Embed Size (px)
Citation preview

Original articleArticle original
� 2011 CEOPublished by / Edite par Elsevier Masson SAS
All rights reserved / Tous droits reserves
Ankylosis of permanent first molars:Genetics or environment? A case report of adiscordant twin pair
Ankylose des premi�eres molaires permanentes :origine g�en�etique ou environnementale ? Rapportde cas d’une paire de jumeaux discordants
Julia COHEN-LEVY
255, rue Saint-Honor�e, 75001 Paris, France
Available online: 2 February 2011 / Disponible en ligne : 2 fevrier 2011
SummaryThe rare condition of secondary retention has been reported inthe literature as being of genetic origin, with some authorssuggesting an autosomal dominant pattern. We report theunusual case of two monozygotic biamniotic, bichorionicmale twins, who were discordant for permanent first molarsecondary retention, involving ankylosis. Twin A showed nor-mal occlusion and eruption patterns, whereas Twin B dis-played a left open bite, in relation with a totally submergedprimary second molar leading to retention of the underlyingpremolar (35), and severe infraocclusion of the adjacent per-manent molar (36). After orthodontic failure to close the openbite, ankylosis of 36 was confirmed, whereas 26 becameseverely infraoccluded.The mother had a history of bilateralmolar ankylosis and presented reduced posterior alveolarheight. Discordance in this twin pair demonstrates that envi-ronmental influences, in addition to epigenetic and localfactors, may play a role in secondary retention, which isdifficult to diagnose and challenging to treat.
� 2011 CEO. Published by Elsevier Masson SAS. All rightsreserved
76
R�esum�e
La r�etention secondaire est une pathologie rare qui a �et�erapport�ee dans la litt�erature comme �etant d’origineh�er�editaire, certains auteurs ayant sugg�er�e un sch�emaautosomique dominant. Nous d�ecrivons ici le cas inhabituelde deux fr�eres jumeaux monozygotes bi-chorioniques,bi-amniotiques, qui pr�esentaient une discordance de lar�etention secondaire de premi�eres molaires permanentesankylos�ees. Le jumeau A pr�esentait une occlusion et unsch�ema d’�eruption normaux alors que, chez le jumeau B onobservait une infraclusion gauche et l’inclusion compl�eted’une deuxi�eme molaire temporaire, la r�etention de lapr�emolaire sous-jacente (35) et une sous-occlusion s�ev�erede la molaire permanente voisine. Apr�es l’�echec de la trac-tion orthodontique, l’ankylose de 36 a �et�e confirm�ee et 26s’est trouv�ee en infraclusion s�ev�ere. La m�ere avaitdes ant�ec�edents d’ankylose molaire bi-lat�erale et pr�esen-tait une hauteur alv�eolaire post�erieure r�eduite. La discor-dance chez ces jumeaux souligne l’importance desinfluences environnementales, associ�ees a des facteurs�epi-g�en�etiques locaux, qui peuvent jouer un role dans lar�etention secondaire, anomalie difficile a diagnostiquer etcompliqu�ee a traiter.� 2011 CEO. Edite par Elsevier Masson SAS. Tous droitsreserves
*Correspondence and reprints / Correspondance et tir�es a part.
e-mail address / Adresse e-mail : [email protected]
International Orthodontics 2011 ; 9 : 76-91doi:10.1016/j.ortho.2010.12.007

Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants
Key-words
·Ankylosis.
·Twins. ·Dizygotic. ·Orthodontics.IntroductionThe eruption process is a complex phenomenon in whichmultiple genetic, molecular and cellular factors are impli-cated [1]. In most cases, arrested tooth eruption is attributedto a physical obstacle in the path of eruption such as super-numerary teeth, crowding, odontogenic tumors and kysts, or amodified position or axial orientation of the tooth germ.However, malfunction of the eruptive mechanism itself canalso occur.
Primary retention is defined as an arrest of the eruption pro-cess before the crown has penetrated the oral mucosa, due toan alteration of the dental follicle, when there is no obviousmechanical interference with eruption [2,3]. Secondary reten-tion refers to the cessation of eruption after emergence: thetooth is fully formed but is unable to reach the occlusal planeand appears to submerge in relation to adjacent teeth thatcontinue to erupt [3–6].
This condition is associated with focal ankylosis, which typ-ically occurs after partial eruption of the tooth into the oralcavity, probably due to a localized alteration of the periodontalligament, or an impairment in its repair process [7]. Fusion ofthe alveolar bone to the cementum and/or dentin occurs wherethere has been a break in the continuity of the desmodontumand, histologically, a portion of the ligament is replaced bycalcified tissue [4].Early diagnosis of ankylosis is challenging as percussiontests are only clinically reliable in about one third of cases[4,5] and depend heavily on the clinician’s judgment of thequality of sounds [8]. This test has proven to be accurate onincisors when more than 20% of the radicular surface isankylosed [6], and appears then to be more sensitive thanradiographic examination [7–9]. As the ankylotic areas aresmall in the first stages, tooth mobility can appear almostnormal, while the eruption process has already stopped[8,9]. A study by Raghoebar et al. claimed that radiographsshowed the loss of periodontal ligament space in one third ofcases [4], and the authors concluded that infraocclusion wasthe most reliable sign for accurate diagnosis of secondaryretention.Molar ankylosis has major clinical repercussions, especiallyin children: while the maxilla and mandible are developing,the ankylosed tooth fails to erupt to meet its counterparts,resulting in progressive infraocclusion. The severity of thelateral open bite depends on the age at ankylosis onset, andworsens sometimes to become total submergence. The adverseeffects expand to the entire occlusion: exaggerated tipping of
International Orthodontics 2011 ; 9 : 76-91
Mots-cl�es
·Ankylose.
·Jumeaux.·Monozygote.
·Orthodontie.
Introduction
L’�eruption dentaire est un ph�enom�ene complexe impliquant denombreux facteurs g�en�etiques, mol�eculaires et cellulaires [1].Dans la plupart des cas, les troubles de l’�eruption sontattribu�es a un obstacle physique situ�e sur le chemind’�eruption, comme une dent surnum�eraire, un fort encombre-ment, une tumeur ou un kyste odontog�ene, voire une modifi-cation de position ou d’orientation axiale du germe. Par ail-leurs, un dysfonctionnement du m�ecanisme �eruptif lui-memepeut etre mis en cause.La r�etention primaire est ainsi d�efinie comme l’interruption duprocessus d’�eruption avant que la couronne n’ait pu p�en�etrerla muqueuse buccale, a la suite d’une alt�eration du folliculedentaire et en l’absence de tout obstacle m�ecaniquea l’�eruption [2,3]. La r�etention secondaire se d�efinit commel’arret de l’�eruption apr�es l’�emergence de la dent. La dent estcompl�etement form�ee mais se trouve dans l’incapacit�ed’atteindre le plan d’occlusion et paraıt sous-�evolu�ee par rap-port aux dents voisines qui continuent leur �eruption [3–6].Cette anomalie est associ�ee une l’ankylose localis�ee qui seproduit habituellement apr�es l’�eruption partielle dans la cavit�eorale, probablement en raison d’une alt�eration locale du liga-ment parodontal ou d’une anomalie de son processus der�eparation [7]. La fusion de l’os alv�eolaire avec le c�ement et/ou la dentine se produit au niveau d’une rupture de continuit�edesmodontale, et, sur le plan histologique, cette partie duligament est remplac�ee par du tissu calcifi�e [4].Le diagnostic pr�ecoce de l’ankylose s’av�ere difficile dans lamesure ou les tests de percussion ne sont cliniquement fiablesque dans un tiers des cas [4,5] et d�ependent fortement dujugement du clinicien sur la qualit�e des sons [8]. Le test n’amontr�e sa fiabilit�e que lorsque plus de 20 % de la surfaceradiculaire est ankylos�ee [6]. Il semblerait en revanche etrealors plus sensible que les examens radiographiques [7–9].Comme les zones ankylos�ees sont r�eduites lors des premiersstades, la mobilit�e dentaire peut paraıtre quasi normale bienque le processus d’�eruption se soit d�eja arret�e [8,9]. Une�etude a ainsi r�ev�el�e que les radiographies montraient uneperte d’espace desmodontal dans un cas sur trois [4] ; l’auteura conclu que, pour obtenir un diagnostic fiable de la r�etentionsecondaire, l’infraclusion constituait le signe le plus sur.L’ankylose de molaires a des r�epercussions cliniques impor-tantes, sp�ecialement chez l’enfant. Alors que la croissancemaxillo-mandibulaire se poursuit, une dent ankylos�ee ne peutatteindre ses antagonistes, d�eclenchant une infraclusion pro-gressive. La s�ev�erit�e de la b�eance lat�erale d�epend de l’ageauquel l’ankylose a d�ebut�e et �evolue parfois vers une r�e-inclu-sion compl�ete. Les effets s’�etendent a l’ensemble de l’arcade :
77

Julia COHEN-LEVY
the adjacent teeth, overeruption of the antagonist, local spaceloss [10], and a shift of the dental midline to the affected side[11].According to the clinical situation, the patient’s age andacceptance, different treatment approaches have been sug-gested [12–22]:– no treatment, in mild infraocclusion cases, showing no evo-lution, for adult patients. Observation is nevertheless requiredto check for over-eruption of the opposite tooth and tipping ofthe surrounding teeth. Proper information should be given tofamily of young patients refusing treatment, as the abnormalitybecomes more severe with age, and is associated with lack ofdevelopment of the alveolar process. Secondary malocclusionsare likely to develop with adverse effects on arch length[10,11,15], and the tendency of the tongue to fill the lateralopen-bite;
– prosthetic build-up is possible if the infraocclusion is lessthan 5 mm and growth is fully completed [17]. For prostheticand functional reasons, adjacent teeth should not show ecces-sive tipping, and the antagonist no overeruption;
– surgical luxation can be planned in order to release the pointof ankylosis, followed by orthodontic traction, provided thatthere is adequate space available for the involved tooth toerupt, and that its development and status make it worthwhile[15]. Several case reports in adult patients have demonstratedfavorable outcomes, even if the risk of ankylosis recurrenceremains [13,16,18,19];– surgical luxation followed by intentional replantation;These two surgical procedures, requiring optimal conserva-tion of the root morphology and blood supply, carry the riskof tooth or mandibular fracture. Differences in gingival mar-gin level may occur because the gingival tissues proliferateless quickly than the immediate repositioning of the tooth[21].Technical aspects have been well described in the dentaltraumatology field, as ankylosis is commonly found in theincisor region following luxation. Extra difficulty can beexpected when dealing with molars, at least from the surgicaland endodontic standpoint;
– segmental osteotomy, which involves sectioning the alveolarbone, followed by vertical repositioning of the fragment, usingbone grafts, if necessary. The limiting factor is the severity ofthe openbite because of the limited stretching properties ofsoft tissues [22];
– corticotomy or alveolar distraction techniques, when anky-losis occurs in single or multiple teeth [22]. Several authorshave reported the use of miniature-distractor devices [20–22],and a recent case report presented the successful treatmentand long-term stability of a severe unilateral openbite requir-ing 7 mm of vertical displacement [22]. The clinical resultssuggested enhancement of the blood supply, gingival contour
78
version excessive des dents voisines, �egression des dentsantagonistes, fermeture de l’espace [10], et d�eport de lam�ediane du cot�e affect�e [11].Diff�erentes approches th�erapeutiques ont �et�e propos�ees enfonction de la situation clinique, de l’age du patient et de sondegr�e de coop�eration [12–22] :– l’abstention th�erapeutique, chez les adultes dont l’infraclu-sion l�eg�ere ne donne aucun signe d’�evolution. Il est cepen-dant n�ecessaire de surveiller l’�egression de l’antagoniste etla version des dents adjacentes. Une information claire doitetre fournie a la famille des jeunes patients qui refuseraientle traitement puisque l’anomalie s’aggrave avec l’age ets’associe a l’absence de d�eveloppement du proc�esalv�eolaire. Des malocclusions secondaires sont suscepti-bles de se d�evelopper avec des r�epercussions d�el�et�eressur la longueur d’arcade [10,11,15]. La langue aura�egalement tendance a combler l’infraclusion lat�erale ;– une r�ehabilitation proth�etique si l’infraclusion fait moins de5 mm et que la croissance est achev�ee [17]. Pour des raisonsproth�etiques et fonctionnelles, les dents voisines ne devraientpas pr�esenter de version excessive, ni l’antagoniste une�egression ;– une luxation chirurgicale afin de mobiliser la zoneankylos�ee, suivie d’une traction orthodontique, a conditionque le diast�eme soit suffisant pour permettre l’�eruption de ladent, et que son �etat et son d�eveloppement en vaillent la peine[15]. Plusieurs rapports de cas chez des patients adultes ont�et�e couronn�es de succ�es, meme s’il subsiste un risque der�ecidive de l’ankylose [13,16,18,19] ;– une luxation chirurgicale suivie d’une r�eimplantationintentionnelle ;Ces deux gestes chirurgicaux, exigeant la conservation maxi-male de la morphologie radiculaire et un bon apport sanguin,comportent un risque de fracture dentaire ou mandibulaire.Des diff�erences d’alignement des collets peuvent en r�esulter,puisque la prolif�eration des tissus gingivaux est plus lente quele repositionnement de la dent [21].Les aspects techniques de cette solution ont �et�e bien d�ecritsen traumatologie car l’ankylose est fr�equemment rencontr�eesur les incisives lux�ees. Le traitement des molaires risquecependant d’etre plus compliqu�e, dumoins en ce qui concerneles aspects chirugicaux et endodontiques.– l’ost�eotomie segmentaire. Elle implique une section de l’osalv�eolaire, dont le fragment est ensuite repositionn�e vertica-lement, en �eventuelle association a une greffe osseuse.Face a une infraclusion s�ev�ere, le recours a cette techniqueest limit�e en raison de l’�elasticit�e r�eduite des tissus mous[22] ;– la corticotomie ou distraction alv�eolaire, lorsque l’ankyloseaffecte une a plusieurs dents [22]. Diff�erents auteurs ontrapport�e l’utilisation de distracteurs miniaturis�es [20–22] etun rapport de cas r�ecent a montr�e le succ�es, stable a longterme, du traitement d’une infraclusion unilat�erale s�ev�eren�ecessitant 7 mm de mouvement vertical [22]. Les r�esultatscliniques laissent supposer une meilleure irrigation sanguine
International Orthodontics 2011 ; 9 : 76-91

Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants
and aesthetic outcome as opposed to conventional surgerywith immediate repositioning [21];
– surgical extraction, followed by orthodontic closure or pros-thetic replacement [18,23]. This option has been qualified asaggressive by some authors [18], but should be considered asthe treatment of choice for ankylosed second molars if thethird molars have not yet formed their roots, as a spontaneousmesial drift of the immature tooth to the extraction site can beexpected. In cases of first permanent molar ankylosis, treat-ment planning must take into account the risk of alveolardefects, and the likely mesioversion of the second molar,requiring further correction.
The etiopathogenesis of secondary retention remains unclear[23], even if a familial occurrence has been often reported[24–29], suggesting a genetic component. When heredity hasbeen involved after pedigree analysis, it appeared to becompatible with an autosomal dominant transmission path[26]. In this article, discordance of secondary retention isreported in a monozygotic male twin pair, in association withtotal submergence of a primary molar. As their mother exhib-ited bilateral ankylosis of her permanent molars, genetic influ-ence cannot be ignored.
Case report
Ten-year-old white male twins were referred to the authors’clinic for treatment of an unerupted permanent first molar inone of them. The twins were biamniotic and bichorionic, asreported by the obstetrician and birth records. They were bornat normal term; delivery was reported to be atraumatic, andtheir medical history normal and concordant for childhooddiseases.
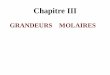
Extra-oral examination showed a perfect match of facial fea-tures (figs. 1 and 2). No mirror image was found between them.
Zygosity diagnosis was based on the concordance of physicalcharacteristics: standing height, ear shape, iris pattern, haircolour, tooth size and on their reported blood group.
Diagnosis
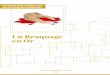
Orthodontic evaluation revealed a bilateral Angle class Imolar relationship, normal incisor overbite and overjet. TwinA showed normal occlusion and eruption patterns. A slightmandibular midline shift to the left, and minor diastemas wereobserved (fig. 3).
Twin B had a left open bite in relation with a totally submergedmandibular primary second molar (75) and adjacent first
International Orthodontics 2011 ; 9 : 76-91
et un r�esultat plus probant au niveau du contour gingival et del’esth�etique g�en�erale qu’avec la chirurgie traditionnelle avecrepositionnement imm�ediat [21] ;– l’avulsion chirurgicale, suivie de fermeture orthodontique oude restauration proth�etique [18,23]. Selon certains auteurs[18], cette technique constituerait une option agressive.Cependant, elle devrait etre consid�er�ee comme le traitementde choix en cas de deuxi�emes molaires ankylos�ees lorsqueles troisi�emes molaires n’ont pas encore �elabor�e leurs racinespuisque l’on peut s’attendre a unem�esialisation spontan�ee dela dent immature en direction du site d’extraction. En ce quiconcerne l’ankylose des premi�eres molaires permanentes, leplan de traitement doit tenir compte du risque d’un d�efautalv�eolaire et de la m�esioversion probable de la deuxi�ememolaire, qui peut n�ecessiter une correction suppl�ementaire.L’�etiopathog�enie de la r�etention secondaire n’a toujours pas�et�e clairement �etablie [23],meme si une occurrence familiale asouvent �et�e rapport�ee [24–29], ce qui laisse supposer unecomposante g�en�etique. Lorsque l’h�er�edit�e a �et�e impliqu�eed’apr�es des arbres g�en�ealogiques, elle semblait compatibleavec unmode de transmission autosomal dominant [26]. Danscet article, nous rapportons une discordance relative der�etention secondaire chez deux jumeaux monozygotes.Comme leur m�ere pr�esente une ankylose bilat�erale desmolaires permanentes, l’influence g�en�etique ne peut cepen-dant pas etre ignor�ee.
�Etude de cas
Des jumeaux caucasiens ag�es de dix ans ont �et�e address�esau cabinet de l’auteur pour le traitement d’une premi�eremolaire pemanente non �evolu�ee chez l’un d’entre eux. Selonl’obst�etricien et les documents relatifs a l’accouchement, lesjumeaux �etaient biamniotiques et bichorioniques. Ils �etaientn�es a terme et l’accouchement a �et�e atraumatique. Leursanamn�eses �etaient normales et concordantes pour les mala-dies infantiles.L’examen extra-oral a r�ev�el�e une concordance parfaite destraits du visage (fig. 1 et 2). Aucun signe d’image inverse(sym�etrie miroir) n’a �et�e relev�e entre eux.Le diagnostic de zygosit�e a �et�e fond�e sur cette concordancede traits physiques : taille, forme des oreilles, configuration del’iris, couleur des cheveux, dimensions des dents et groupesanguin d�eclar�e.
Diagnostic
L’�evaluation orthodontique a r�ev�el�e une relation molaire deClasse I d’Angle bilat�erale, et un surplomb et recouvrementincisifs normaux. Le jumeau A pr�esentait une occlusion et dessch�emas d’�eruption normaux, avec un l�eger d�ecalage vers lagauche de la m�ediane mandibulaire et des diast�emes discrets(fig. 3).Le jumeau B pr�esentait une infraclusion gauche en relationavec la r�einclusion apparente de la deuxi�eme molaire
79

[(Figure_1 a–c)TD$FIG]
Figure 1 a–c: extraoral views of Twin A.Figure 1 a–c : vues extra-orales du jumeau A.
Julia COHEN-LEVY
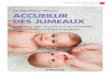
molar secondary retention (36), with the tip of the buccal cuspshaving emerged from the gingiva. Adjacent teeth showedexcessive tipping and relative under-eruption. The upper leftmolars (26) showed moderate infraclusion, approximately1.5 mm from the occlusal plane, whereas the right side wasnormal. Percussion tests were negative (fig. 4).
Panoramic radiography demonstrated a full complement ofpermanent teeth. Twin A had normal eruption patterns,whereas Twin B showed the retention of 35, close to theinferior border of the mandible, under severely infraoc-cluded 75.
[(Figure_2 a–c)TD$FIG]
Figure 2 a–c: extraoral views of Twin B.Figure 2 a–c : vues extra-orales du jumeau B.
80
temporaire (75) et une r�etention secondaire de la premi�eremolaire adjacente (36) dont les pointes des cuspides vestibu-laires �emergaient de la gencive. Les dents voisines accusaientune version exag�er�ee et une infraposition relative. La molairesup�erieure gauche (26) montrait une infraclusion mod�er�ee,d’a peu pr�es 1,5 mm par rapport au plan d’occlusion, alorsque le cot�e droit �etait normal. Les tests a la percussion �etaientn�egatifs (fig. 4).La radiographie panoramique a montr�e une formule dentairecompl�ete. Le jumeau A avait un sch�ema d’�eruption normaltandis que le jumeau B pr�esentait l’inclusion de 35, prochedu rebord basilaire, sous 75 en infraclusion s�ev�ere.
International Orthodontics 2011 ; 9 : 76-91

[(Figure_3 a–e)TD$FIG]
Figure 3 a–e: intraoral views of Twin A.Figure 3 a–e : vues intra-orales du jumeau A.
[(Figure_4 a–e)TD$FIG]
Figure 4 a–e: intraoral views of Twin B.Figure 4 a–e : vues intra-orales du jumeau B.
International Orthodontics 2011 ; 9 : 76-91 81
Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants

[(Figure_5 a)TD$FIG]
Figure 5 a: Twin A: panoramic radiograph (June 2006); b: Twin B: panoramic radiograph (October 2005). Tooth maturation stage is slightlydifferent because of the interval between records.Figure 5 a : radiographie panoramique du jumeau A (juin 2006) ; b : radiographie panoramique du jumeau B (Octobre 2005). Le stade de
maturation dentaire est l�eg�erement different en raison du d�ecalage entre les deux panorex.
Julia COHEN-LEVY
The adjacent permanent molar, 36, seemed to be following anormal eruption path, with no radiologically-detectable bar-rier. However, it remained approximately one centimeterbelow the occlusal plane, showing a slight distal root curvature(fig. 5).The mother had a history of tooth ankylosis and submergedmolars, some of which had been extracted. She showed a largebilateral posterior openbite with a conspicuous tongue andcheek suction habit. We supposed that the tooth must havebeen in acceptable occlusion at some time because it had arestorative filling, consistent with the diagnosis of secondaryretention (fig. 6).
[(Figure_6 a–c)TD$FIG]Figure 6 a–c: intraoral views of the twins’ mother; d: panoramic X-Rayinfraocclusion of 16, severe infraocclusion of 26, with adjacent distal prFigure 6 a–c : vue intra-orale de la m�ere des jumeaux ; d : radiographie
associ�ee a une l�eg�ere infraocclusion de la 16, a une infraocclusion s�ev�ere
adjacente.
82
La molaire permanente voisine, 36, semblait suivre une voied’�eruption normale sans aucun obstacle radiologiquementd�etectable. N�eanmoins, elle restait a peu pr�es a 1 cm en des-sous du plan d’occlusion, avec l’amorce d’une courbure radi-culaire distale (fig. 5).La m�ere pr�esentait des ant�ec�edents d’ankylose et d’inclusionmolaire, dont certaines avaient �et�e extraites. Elle pr�esentaitune infraclusion post�erieure bilat�erale importante et uned�eglutition primaire avec tic d’aspiration des joues et pulsionlinguale. Nous avons suppos�e que la dent en infraclusion avaitdu se trouver, par le pass�e, en occlusion puisque qu’elle avaitrecu une obturation, ce qui renforcait le diagnostic d’uner�etention secondaire (fig. 6).
of the twins’ mother, showing posterior open bite, in relation to mildemolar inclination and infraposition.panoramique de la m�ere des jumeaux. Notez la b�eance post�erieure,
de la 26 et d’une inclinaison et infraposition distales de la pr�emolaire
International Orthodontics 2011 ; 9 : 76-91

Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants
Treatment objectives
The failure of orthodontics alone to correct posterior openbiteshas previously been reported and extrusion of teeth appears tobe possible where there has been a mechanical barrier inter-fering with eruption. As percussion tests were normal, wehypothezied that a lateral tongue thrust during swallowingmight be acting as a mechanical obstacle and that the paraf-unction had further exacerbated by the large gap created bythe submerged primary molar. Twin B was given a lingualretainer for night-time, and asked to perform functional train-ing in order to achieve a normal swallowing pattern.Conventional orthodontic treatment was then planned toaccelerate eruption.
The patient was scheduled for removal of the reimpacteddeciduous molar under local anesthesia, as it was impedingthe premolar’s path of eruption.
Treatment plan and follow-up
An orthodontic extrusion force was directly applied on themolar, using a 0.017 � 0.025 inch TMA� device fixed on alingual arch (fig. 7). Vertical elastics were worn at night inorder to avoid increasing the lateral open-bite, from the lin-gual arch to an upper palatal arch. After six months treatment,orthodontic extrusion and an attempt to close the posterioropen bite appeared to be unsuccessful, despite the tongueprotrusion habit having been been eliminated. The impactedpremolar had started to erupt in a normal pathway, until itreached the mesial face of 36. Ankylosis of both upper andlower left permanent first molars was confirmed, as theireruption stopped while adjacent teeth continued to erupt(figs. 8–10).Surgical extraction of the left permanent first molars wasplanned; priority was given to 36, which was removed underlocal anesthesia without complications. Follow-up appoint-ments for the tongue-retainer were scheduled and, 10 monthslater, the previously impacted premolar was set in correctocclusion. The upper left molar, that had become completelysubmerged, was then extracted under local anesthesia. Theright side remained normal (figs. 11 and 12).The need for a long observation period and further orthodonticcorrection was explained to the patient and family.Appointments were scheduled to assess second molar evolu-tion. After one year, spontaneous closure of the anteriordiastemas occurred in both twins (figs. 13 and 14). Whencomparing the last panoramic radiographs (figs. 15), the rela-tionship of the left lower molar and premolars, which wereinitially at the same level, had clearly changed. . . a sign ofarrested eruption. On the upper left side, the second molarspontaneously mesialized. Its evolution appears more favor-able but still needs to be carefully monitored.
International Orthodontics 2011 ; 9 : 76-91
Objectifs de traitement
L’�echec de l’orthodontie seule pour corriger les infraclusionspost�erieures a d�eja �et�e rapport�ee et l’�egression dentaire for-c�ee ne semble etre une option de traitement que lorsqu’unobstacle m�ecanique s’oppose a l’�eruption. Puisque les testsa la percussion �etaient normaux, nous avons suppos�e qu’uneinterposition linguale lat�erale lors de la d�eglutition pouvait agircomme un obstacle m�ecanique, interposition pouvant etreentretenue par l’espace important cr�e�e par l’enfouissementde la molaire temporaire. Le jumeau B a ainsi port�e une enve-loppe linguale nocturne, parall�element a des exercices fonc-tionnels afin de retrouver une d�eglutition mature. Ensuite, untraitement orthodontique conventionnel a �et�e pr�evu pouracc�el�erer l’�eruption.Rendez-vous a �et�e pris pour extraire la molaire temporairer�eincluse qui empechait l’�evolution de la pr�emolaire, sousan�esth�esie locale.
Plan de traitement et suivi
Une force d’�egression orthodontique a �et�e appliqu�ee sur lamolaire en utilisant un arc sectionnel 0,017 x 0,025 TMA� fix�ea un arc lingual (fig. 7). Pour �eviter d’aggraver l’infraclusionlat�erale, le patient a port�e des �elastiques verticaux la nuit entrel’arc lingual et un arc palatin. Apr�es six mois de traitement,l’�egression orthodontique et la tentative de fermer l’infraclu-sion semblaient s’av�erer un �echec, malgr�e l’�elimination del’interposition linguale. La pr�emolaire incluse avait commenc�ea rejoindre un trajet d’�eruption normal jusqu’a atteindre lapartie m�esiale de 36. L’ankylose des premi�eres molaires per-manentes gauches sup�erieure et inf�erieure a �et�e confirm�eepuisque leur �eruption s’�etait arret�ee alors que d’autres dentscontinuaient a �evoluer (fig. 8–10).L’extraction chirurgicale des premi�eres molaires permanentesgauches a �et�e d�ecid�ee. Priorit�e a �et�e donn�ee a 36 qui a �et�eavuls�ee sous anesth�esie locale, sans complications. Des ren-dez-vous de suivi ont �et�e pr�evus et, dix mois plus tard, lapr�emolaire initialement retenue s’est positionn�ee en bonneocclusion. La molaire sup�erieure gauche, compl�etementenfouie, a �et�e extraite sous anesth�esie locale. Le cot�e droit�etait toujours normal (fig. 11 et 12).La n�ecessit�e de respecter une longue p�eriode d’observation etde r�ealiser de nouvelles corrections orthodontiques a �et�eexpliqu�ee au patient et a la famille. Des rendez-vous ont �et�epr�evus afin d’�evaluer l’�evolution des deuxi�emes molaires.Apr�es un an, la fermeture spontan�ee des diast�emesant�erieurs s’est effectu�ee chez les deux jumeaux (fig. 13 et14). En comparant les derni�eres radiographies panoramiques(fig. 15), nous avons pu observer que la relation de la molaireet des pr�emolaires inf�erieures gauches, qui se trouvaient intia-lement au meme niveau, avait consid�erablement �evolu�e. . .signe d’un arret du processus d’�eruption. La deuxi�ememolaire sup�erieure gauche s’est m�esialis�ee de faconspontan�ee. Son �evolution paraıt plus favorable mais doit tou-jours etre suivie avec attention.
83

[(Figure_7)TD$FIG]
Figure 7: Orthodontic extrusion device: a: lingual archwire; b: palatal archwire; c: left lateral view; d: it was assumed that orthodontictraction accelerated root resorption of the primary molar.Figure 7 : Dispositif d’�egression orthodontique ; a : arc lingual soutenant un fil rectangulaire TMA� ; b : arc palatin ; c : vue de profil gauche ;
d : nous pr�esumons que la traction orthodontique a acc�el�er�e la r�esorption radiculaire de la molaire temporaire.
[(Figure_8)TD$FIG]
Figure 8: Twin B control panoramic radiograph, after 6 monthstreatment.Figure 8 : Radiographie panoramique de controle du jumeau B apr�es
six mois de traitement.
84 International Orthodontics 2011 ; 9 : 76-91
Julia COHEN-LEVY

[(Figure_9 a,b)TD$FIG]
Figure 9 a,b: Twin B pre-treatment lateral cephalograph, and control cephalograph (same radiologist).Figure 9 a,b : c�ephalogramme lat�eral avant traitement du jumeau B et c�ephalogramme de controle (meme radiologue).
Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants
Discussion
In the normal population, teeth exhibiting secondary retentionare usually deciduous molars, but permanent molars can beinvolved, in rare cases, with a prevalence of about 0.06%[24,25].
The developmental disturbance affecting the periodontal lig-ament and causing ankylosis might be genetic, as reports of afamilial tendency abound [26–35]. However, it could be theresult of a combination of factors: disturbances in local metab-olism, history of trauma, viral infection [35], chemical orthermal irritation, jaw surgery, and abnormal pressure fromthe tongue. The concomitance of arrested molar eruption withinfraocclusion of deciduous molars, as presented in this casestudy, has been previously reported. Both abnormalities maybe connected with a local metabolic disturbance [33].
Pylik and Alfter [31] studied tooth eruption impairment infour generations of the same family and assumed there to bea multifactorial genetic cause. Raghoebar et al., on the otherhand, found that when there was familial occurrence, pedi-grees were compatible with an autosomal dominant inheri-tance, with no evidence of reduced penetrance [26]. Boskerand Nijenhuis provisionally ascribed the causing gene to bein the same linkage group as the gene locus of blood group P[30].
International Orthodontics 2011 ; 9 : 76-91
Discussion
Dans la population normale, les dents pr�esentant uner�etention secondaire sont g�en�eralement des molaires tempo-raires. N�eanmoins, dans de rares cas, des molaires perma-nentes peuvent �egalement etre impliqu�ees, avec une pr�eva-lence d’environ 0,06 % [24,25].Les troubles du d�eveloppement qui affectent le ligament paro-dontal et qui provoquent l’ankylose sont peut-etre d’origineh�er�editaire, puisqu’il existe de nombreux rapports de cas met-tant en cause une origine familiale [26–35]. Cependant, ilspourraient �egalement r�esulter d’une combinaison defacteurs : perturbations au niveau du m�etabolisme local, trau-matisme, infection virale [35], irritation chimique ou thermique,chirurgie orthognathique et une pression anormale exerc�eepar la langue. La pr�esence concomitante d’une ankylosemolaire et de celle des molaires temporaires, telle que nousla pr�esentons dans ce cas, a d�eja �et�e rapport�ee. Il est possibleque les deux anomalies soient reli�ees a une perturbation dum�etabolisme local [33].Pylik et Alfter [31] ont trouv�e une perturbation de l’�eruptiondentaire au sein des quatre g�en�erations d’unememe famille etont conclu a une cause g�en�etique multifactorielle. Pour leurpart, Raghoebar et al. ont trouv�e que, face a des cas touchantune meme famille, les arbres g�en�etiques indiquaient unh�eritage autosomique dominant sans aucun signe dep�en�etrance r�eduite [26]. Bosker et Nijenhuis ont provisoire-ment attribu�e le g�ene responsable au meme locus g�en�etiqueque celui du groupe sanguin P [30].
85

[(Figure_11 a)TD$FIG]
Figure 11 a: intraoral photograph showing total submergence of upper left first molar; b: intraoral photograph showing spontaneous eruption ofthe lower bicuspid; c: intraoral view of the occlusion on the right side.Figure 11 a : vue intra-orale montrant la totale submergence de la premi�ere molaire sup�erieure gauche ; b : vue intra-orale montrant l’�eruption
spontan�ee de la pr�emolaire inf�erieure ; c : vue intra-orale de l’occlusion cot�e droit.
[(Figure_10)TD$FIG]
Figure 10: Local superimposition after 6 months treatment: man-dibular and maxillary first molars show no eruption movement.Figure 10 : Superposition locale apr�es six mois de traitement : les
premi�eres molaires mandibulaires et maxillaires ne montrent aucun
signe d’�emergence.
Julia COHEN-LEVY
Secondary retention has been reported in twins [32,36]: in thefirst case, described by Helpin and Duncan, there was a nearlyidentical pattern of distribution and severity of ankylosis: oneof the twins had four ankylosed teeth while the other had five.In the second publication by Radlanski and Freesmeyer, the
86
La r�etention secondaire a �et�e rapport�ee chez des jumeaux[32,36]. Dans un premier cas, d�ecrit par Helpin et Duncan, ilsont trouv�e une r�epartition et une s�ev�erit�e d’ankylose presqueidentiques. L’un des jumeaux avait quatre dents ankylos�eestandis que l’autre en avait cinq. Dans un deuxi�eme article de
International Orthodontics 2011 ; 9 : 76-91

[(Figure_12 a)TD$FIG]
Figure 12 a: occlusion on the left side of casts; b: occlusal view on casts.Figure 12 a : occlusion du cot�e gauche des moulages ; b : Vue occlusale sur moulages.
[(Figure_13 a–e)TD$FIG]
Figure 13 a–e: intraoral photographs of twin A at age 13.Figure 13 : Vues intra-orales du jumeau A a 13 ans.
Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants
twins were dizygotic but required treatment for a nearly iden-tical openbite due to ankylosis of the permanent molars.
Discordance in this twin pair was therefore unexpected, espe-cially in view of the mother’s occlusion and panoramic radio-graph which revealed bilateral molar ankylosis, thus suggest-ing a genetic predisposition. Unfortunately, the family refusedto accept DNA testing, so doubt persists regarding the twinszygosity status, although comparisons of facial features and
International Orthodontics 2011 ; 9 : 76-91
Radlanski et Freesmeyer, les jumeaux �etaient dizygotes maisavaient besoin d’un traitement pour une infraclusion presqueidentique due a une ankylose des molaires permanentes.La discordance entre ces deux jumeaux �etait donc inattendue,surtout a la vue de l’occlusion et de la radiographie panorami-que de la m�ere qui pr�esentait une ankylose molaire bilat�erale,laissant ainsi soupconner une pr�edisposition g�en�etique.Malheureusement, la famille n’a pas autoris�e des tests ADN,laissant persister des doutes quant au statut zygotique, bien
87

[(Figure_14 a–e)TD$FIG]
Figure 14 a–e: intraoral photographs of twin B at age 13.Figure 14 a–e : vues intra-orales du jumeau B a 13 ans.
[(Figure_15 a)TD$FIG]
Figure 15 a: panoramic before upper first molar extraction; b: panoramic 18 months after upper first molar extraction.Figure 15 a : panorex avant extraction de la premi�ere molaire sup�erieure ; b : panorex 18 mois apr�es extraction de la premi�ere molaire
sup�erieure.
Julia COHEN-LEVY
tooth morphology can provide accurate means of distinguish-ing between monozygotic and dizygotic twin pairs [37–39].
Genetic and environmental influences could explain whymonozygotic twins might not be identical phenotypically[40]: differential placental implantation and nutrition, differ-ential transplacental infections as possible environmentaleffects, post-zygotic mutations, discordance for imprintablegenes (maternal or paternal), or a slight difference in methyl-ation degree of autosomal genes [41,42].
88
que la comparaison des traits du visage et de la morphologiedentaire puisse fournir un moyen fiable pour distinguer entredes paires de jumeaux mono- et dizygotes [37–39].Les influences g�en�etiques et environnementales peuventexpliquer pourquoi des jumeaux monozygotes ne sont pasph�enotypiquement identiques [40] : la diff�erence d’implanta-tion et de nutrition placentaires, les diverses infections trans-placentaires en tant qu’�eventuelles influences environnemen-tales, les mutations post-zygotiques, la discordance pour lesg�enes soumis a empreinte (maternelle ou paternelle), ou unel�eg�ere diff�erence du degr�e de m�ethylation des g�enes autoso-miques [41,42].
International Orthodontics 2011 ; 9 : 76-91

Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants
The twins were dichorionic and diamniotic, signifying that theplacenta, chorion and amnion were all doubled during preg-nancy, and that the twinning event occurred in the early stagesof development, before the blastocyst stage. Chorion type is animportant variable that can affect the prenatal environment ofmonozygotic twin pairs, leading to differences in growth anddevelopment. As in twin pregnancies, vascular disruptions arecommon, creating an imbalance in nutrition between co-twins,and possibly explaining some of the divergent clinical featuresof these individuals.
Viral attacks on the nerve paths have also been implicated indelaying dental development and eruption [43]. However, asthe medical history of both twins was concordant, this hypoth-esis was abandoned. Recently, Bang et al. [44] found aconnection between unilateral secondary retention of perma-nent teeth, dental malformation and the innervation pattern,suggesting a possible role for the nerve supply in the affectedregion: we could argue that trophic differences during preg-nancy, through placenta anastomoses, might account for theobserved differences.
Conclusion
The etiopathogenesis of secondary retention is not fully under-stood, but heredity has often been involved. In this case report,two dichorionic, diamniotic male twins were discordant forsecondary retention of permanent first molars, while theirmother had a history of bilateral molar ankylosis. This findinghighlights the possibility that environmental influences, inaddition to epigenetic and local factors, may play a role insecondary retention. Chorionicity may also be an importantfactor, as environmental influences in utero play a significantrole in tooth development.
Conflict of interest
None
References/R�ef�erences
1. Wise GE, King GJ. MechaniRes 2008;87(5):414–34.
2. Proffit WR, Vig KW. PrimaAm J Orthod 1981;80:173–9
International Orthodontics 2011 ; 9 : 76-91
Les jumeaux �etaient bichoriaux et biamniotiques, ce qui sig-nifie que le placenta, le chorion et l’amnios �etaient dupliqu�espendant la grossesse et que la g�emellit�e s’est d�eclench�eependant les premiers stades du d�eveloppement, avant lestade blastocyste. Le type de chorion est une variable impor-tante qui peut influer sur l’environnement pr�enatal de paires dejumeaux monozygotes, donnant lieu a des diff�erences auniveau de la croissance et du d�eveloppement. Dans les gros-sesses g�emellaires, les perturbations sont fr�equentes et peu-vent cr�eer un d�es�equilibre d’apport nutritif entre les deuxjumeaux et peut-etre expliquer certaines des divergencescliniques entre eux.Des attaques virales ont �egalement �et�e impliqu�ees dans leretard du d�eveloppement et d’�eruption dentaires [43].Cependant, comme les ant�ec�edents m�edicaux des deuxjumeaux �etaient concordants, cette hypoth�ese a �et�eabandonn�ee. R�ecemment, Becktor et al. [44] ont trouv�e unerelation entre la r�etention secondaire unilat�erale des dentspermanentes, les malformations dentaires et le sch�ema destrajets nerveux, laissant supposer un role �eventuel de l’inner-vation dans la zone affect�ee.
Conclusion
Si l’�etiopathog�enie de la r�etention secondaire n’est pasenti�erement connue, l’h�er�edit�e a n�eanmoins �et�e souvent miseen cause. Dans ce rapport de cas, deux fr�eres jumeaux,diamniotiques et dichorioniques �etaient discordants pour lar�etention secondaire des premi�eres molaires permanentesalors que leur m�ere pr�esentait une ankylosemolaire bilat�erale.Cette observation souligne la possibilit�e que les influencesenvironnementales puissent jouer un role dans la r�etentionsecondaire, en plus des facteurs g�en�etiques et �epig�en�etiques.La chorionicit�e pourrait �egalement constituer un facteur impor-tant puisque les influences trophiques in utero jouent un rolesignificatif dans le d�eveloppement dentaire.
Conflit d’int�eret
Aucun
sms of tooth eruption and orthodontic tooth movement. J Dent
ry failure of eruption: a possible cause of posterior open-bite.0.
89

3. Raghoebar GM, Boering G, Vissink A, Stegenga B. Eruption disturbances of permanentmolars: a review. J Oral Pathol Med 1991;20:159–66.
4. Raghoebar GM, Boering G, Jansen HW, Vissink A. Secondary retention of permanentmolars: a histologic study. J Oral Pathol Med 1989;18:427–31.
5. Raghoebar GM, Boering G, Vissink A. Clinical, radiographic and histological character-istics of secondary retention of permanent molars. J Dent 1991;19(3):164–70.
6. Andersson L, Bloml€of L, Lindskog S, Feiglin B, Hammarstr€om L. Tooth ankylosis: clinical,radiographic and histological assessments. Int J Oral Surg 1984;13:423–31.
7. Brown WA. Resorption of permanent teeth. Br J Orthod 1982;9:212–20.8. Campbell KM, Casas MJ, Kenny DJ, Chau T. Diagnosis of ankylosis in permanent incisors
by expert ratings. Periotest and digital sound wave analysis. Dent Traumatol 2005;21(4):206–12.
9. Stenvik A, Stermer Beyer-Olsen EM, Abyholm F, Haanaes HR, Gerner NW. Validity of theradiographic assessment of ankylosis. Evaluation of long-term reactions in 10 monkeyincisors. Acta Odont Scand 1990;48:265–9.
10. Becker A, Karnei-R’em RM. The effects of infraocclusion: Part 1. Tilting of the adjacentteeth and local space loss. Am J Orthod Dentofacial Orthop 1992;102(3):256–64.
11. Becker A, Karnei-R’em RM, Steigman S. The effects of infraocclusion: Part 3: Dental archlength and the midline. Am J Orthod Dentofacial Orthop 1992;102(5):427–33.
12. Kurol J. Impacted and ankylosed teeth: why, when, and how to intervene. Am J OrthodDentofacial Orthop 2006;129(4 Suppl.):S86–9.
13. LimWH, KimHJ, Chun YS. Treatment of ankylosed mandibular first permanent molar. AmJ Orthod Dentofacial Orthop 2008;133(1):95-101.
14. Marechaux SC. The problems of treatment of early ankylosis: report of case. ASDC J DentChild 1986;53:63–6.
15. Paleczny G. Treatment of the ankylosed mandibular permanent first molar: a case study. JCan Dent Assoc 1991;57(9):717–9.
16. Skolnick IM. Ankylosis of maxillary permanent first molar. J Am Dent Assoc 1980;100(4):558–60.
17. Mullally BH, Blakely D, Burden DJ. Ankylosis: an orthodontic problem with a restorativesolution. Br Dent J 1995;179:1126–30.
18. Geiger AM, Bronsky MJ. Orthodontic management of ankylosed permanent posterior teeth:a clinical report of three cases. Am J Orthod Dentofacial Orthop 1994;102:543–8.
19. Chaushu S, Becker A, Chaushu G. Orthosurgical treatment with lingual orthodontics of aninfraoccluded maxillary first molar in an adult. Am J Orthod Dentofacial Orthop 2004;125(3):379–87.
20. Razdolsky Y, El-Bialy TH, Dessner S, Buhler Jr. JE. Movement of ankylosed permanentteeth with a distraction device. J Clin Orthod 2004;38(11):612–20.
21. Alcan T. A miniature tooth-borne distractor for the alignment of ankylosed teeth. AngleOrthod 2006;76:77-83.
22. Susami T, Matsuzaki M, Ogihara Y, Sakiyama M, Takato T, Sugawara Y, Matsumoto S.Segmental alveolar distraction for the correction of unilateral open-bite caused by multipleankylosed teeth: a case report. J Orthod 2006;33(3):153–9.
23. Biederman W, Chem B. Etiology and treatment of tooth ankylosis. Am J Orthod1962;48:671–4.
24. Prece JW. The incidence of unerupted permanent teeth and related clinical cases. OralSurg 1985;59:420–5.
25. Grover PS, Lorton L. The incidence of unerupted permanent teeth and related clinicalcases. Oral Surg Oral Med Oral Pathol 1985;59:420–5.
26. Raghoebar GM, Ten Kate LP, Hazenberg CA, Boering G, Vissink A. Secondary retention ofpermanent molars: a report of five families. J Dent 1992;20(5):277–82.
27. Pelias MZ, Kinnebrew MC. Autosomal dominant transmission of ankylosed teeth, abnorm-alities of the jaws, and clinodactyly. A four-generation study. Clin Genet 1985;27:496-500.
28. Cozza P, Gatto R, Ballanti F, De Toffol L, Mucedero M. Case report: severe infraocclusionankylosis occurring in siblings. Eur J Paediatr Dent 2004;5(3):174–8.
90 International Orthodontics 2011 ; 9 : 76-91
Julia COHEN-LEVY

29. Bosker H, Tenkate LP, Nuenhuis LE. Familial reinclusion of permanent molars. Clin Genet1978;13:314–20.
30. Bosker H, Nijenhuis LE. Possible linkage between a gene causing reinclusion of molar 1and blood group P. Cytogenetics Cell genet 1975;14:255–6.
31. Pytlik W, Alfter G. Impairment of tooth eruption. Pathogenetic aspects. J Orofac Orthop1996;57(4):238–45.
32. Helpin ML, Duncan WK. Ankylosis in monozygotic twins. ASDC J Dent Child 1986;53(2):135–9.
33. Baccetti T. Tooth anomalies associated with failure of eruption of first and second perma-nent molars. Am J Orthod Dentofacial Orthop 2000;118(6):608–10.
34. Proff P, Bayerlein T, Fangh€anel J, Allegrini Jr. S, Gedrange T. Morphological and clinicalconsiderations of first and second permanent molar eruption disorders. Ann Anat 2006;188(4):353–61.
35. Bang E, Kjaer I, Christensen LR. Etiologic aspects and orthodontic treatment of unilaterallocalized arrested tooth-development combined with hearing loss. Am J Orthod DentofacOrthop 1995;108(2):154–61.
36. Radlanski RJ, Freesmeyer WB. Bilateral open bite in dicygotic twins. A combined ortho-dontic-prosthetic approach. J Orofac Orthop 2002;63(4):339–47.
37. Townsend GC, Richards LC, Brown T, Burgess VB. Twin zygosity determination on thebasis of dental morphology. J Forensic Odontostomatol 1988;6(1):1-15.
38. Kabban M, Fearne J, Jovanovski V, Zou L. Tooth size and morphology in twins. Int JPaediatr Dent 2001;11(5):333–9.
39. Townsend GC, Richards L, Hughes T, Pinkerton S, Schwerdt W. The value of twins indental research. Aust Dent J 2003;48(2):82–8.
40. Townsend GC, Richards L, Hughes T, Pinkerton S, Schwerdt W. Epigenetic influences mayexplain dental differences in monozygotic twin pairs. Aust Dent J 2005;50(2):95-100.
41. Machin GA. Some causes of genotypic and phenotypic discordance in monozygotic twinpairs. Am J Med Genet 2001;102(3):306–7.
42. Martin NG, Boomsma D, Machin G. A twin-pronged attack on complex traits. Nat Genet1997;17:387–92.
43. Becktor KB, Bangstrup MI, Rølling S, Kjær I. Unilateral primary or secondary retention ofpermanent teeth and dental malformations. Eur J Orthod 2002;24:205–14.
44. Bang E, Kjær I, Christensen LR. Etiological aspects and orthodontic treatment of unilaterallocalized arrested tooth development combined with hearing loss. Am J Orthod DentofacOrthop 1995;108:154–61.
International Orthodontics 2011 ; 9 : 76-91 91
Ankylosis of permanent first molars: Genetics or environment? A case report of a discordant twin pairAnkylose des premi�eres molaires permanentes : origine g�en�etique ou environnementale ? Rapport de cas d’une paire de jumeaux
discordants