Embed Size (px)
Citation preview

Camille . S -Cécile .T – Maëlle . D - Marion. R
12 février 2010
LES ENJEUX STRATÉGIQUES DANS LE SECTEUR
DE LA THROMBOSE
Le dernier congrès de l’ESC à Barcelone a permis la
présentation de très nombreux résultats positifs sur de
nouveaux antithrombotiques ou antiagrégants
plaquettaires: le dabigatran avec l’étude RELY, le
prasugrel avec l’étude TRITON TIMI 38, le ticagrelor
avec l’étude PLATO
INTRODUCTION
Reminder of thrombosis
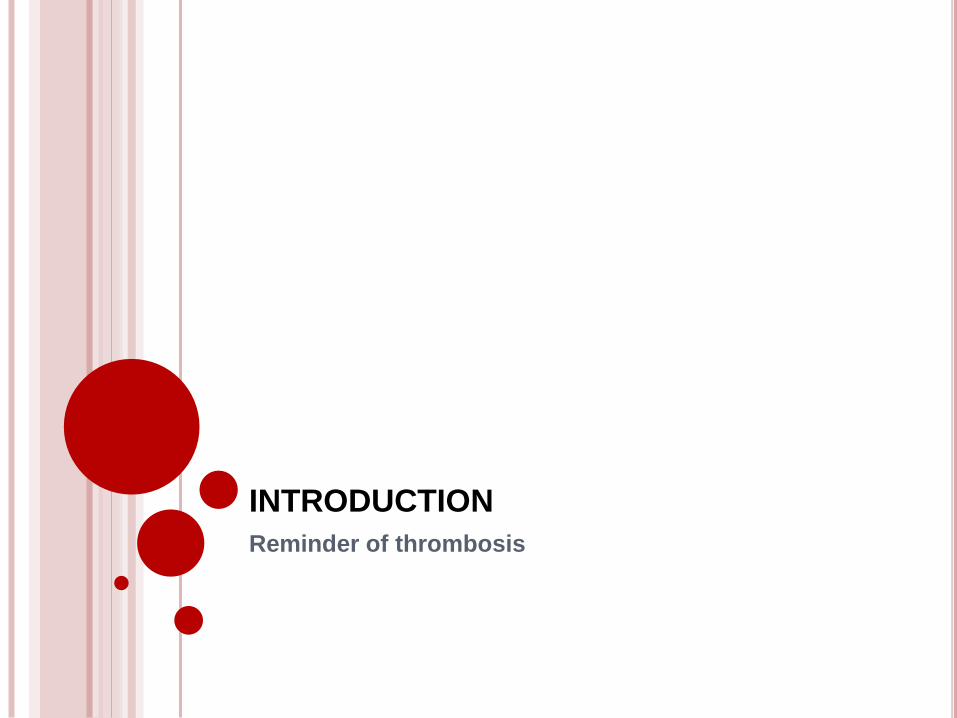
THROMBOSIS, BASIC POINTS
o Thrombosis = formation of a blood clot(thrombus) inside a blood
vessel, obstructing the flow of blood through the circulatory system.
o Virchow's triad :
o 2 subtypes :
- Veinous thrombosis
- Arterial thrombosis
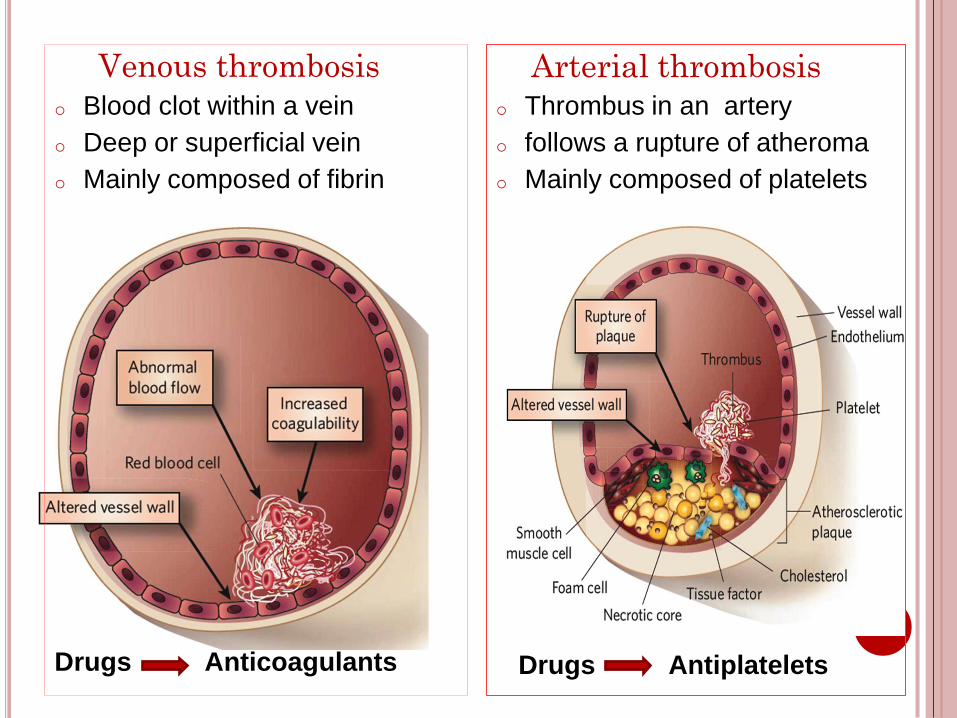
Venous thrombosis
o Blood clot within a vein
o Deep or superficial vein
o Mainly composed of fibrin
Drugs Anticoagulants
Arterial thrombosis
o Thrombus in an artery
o follows a rupture of atheroma
o Mainly composed of platelets
Drugs Antiplatelets
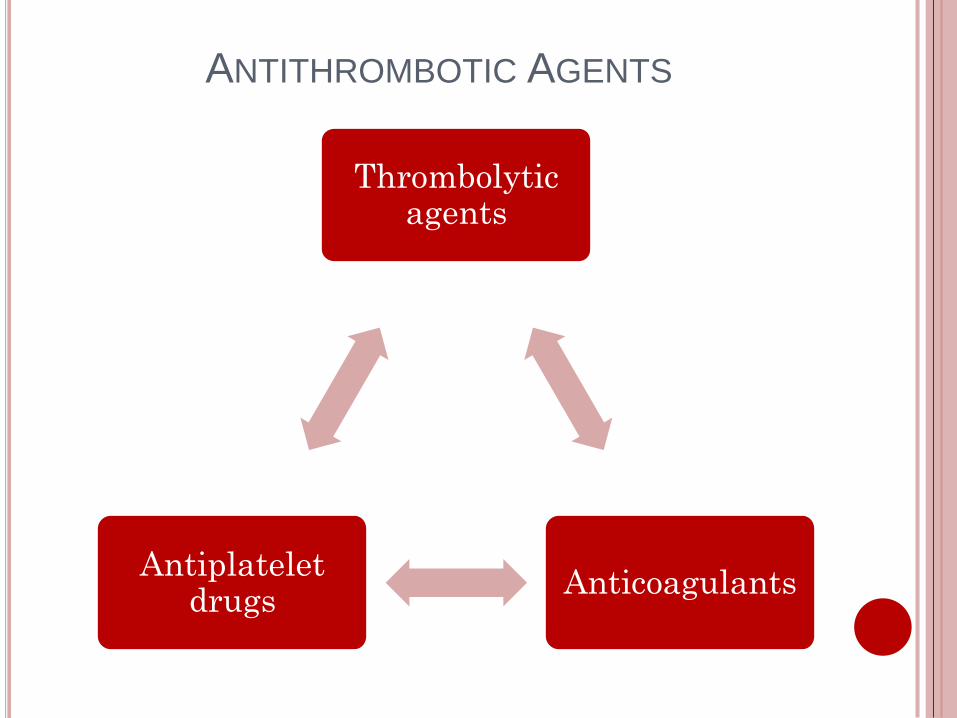
ANTITHROMBOTIC AGENTS
Thrombolytic agents
AnticoagulantsAntiplatelet
drugs
1ST PART
Antiplatelets in Acute Coronary
Syndrom (ACS)
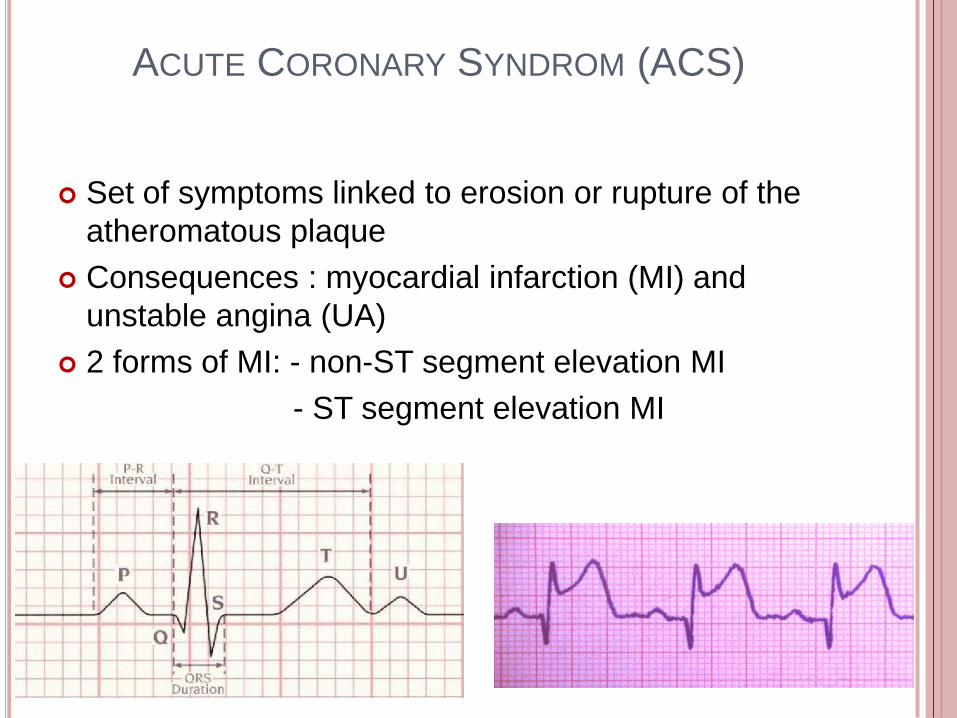
ACUTE CORONARY SYNDROM (ACS)
Set of symptoms linked to erosion or rupture of the
atheromatous plaque
Consequences : myocardial infarction (MI) and
unstable angina (UA)
2 forms of MI: - non-ST segment elevation MI
- ST segment elevation MI
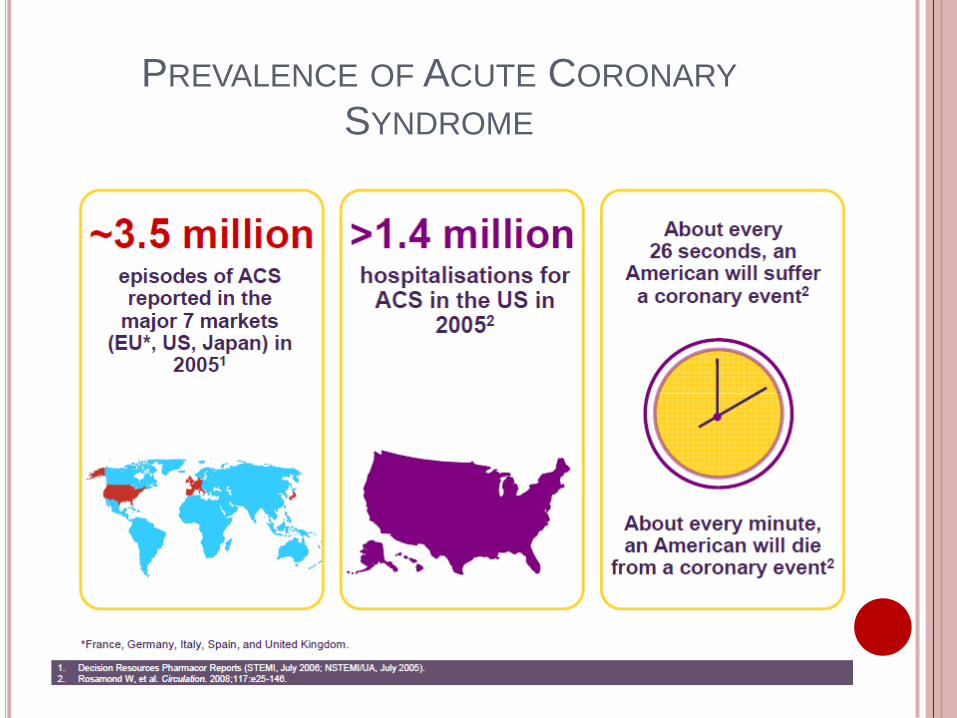
PREVALENCE OF ACUTE CORONARY
SYNDROME
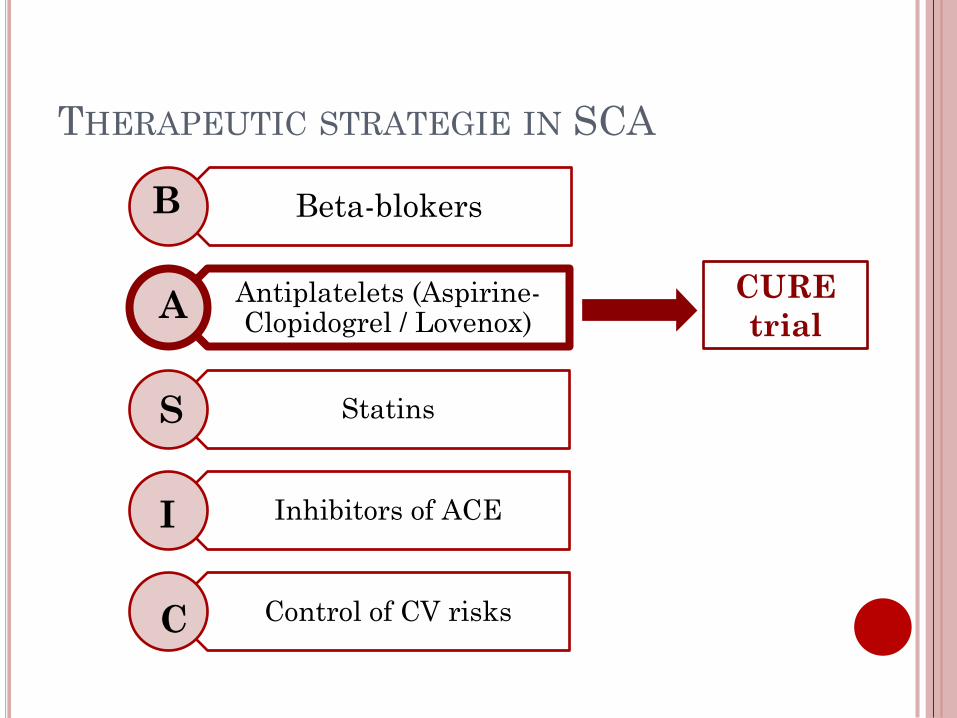
THERAPEUTIC STRATEGIE IN SCA
Beta-blokers
Antiplatelets (Aspirine-Clopidogrel / Lovenox)
Statins
Inhibitors of ACE
Control of CV risks
B
C
A
I
S
CURE
trial
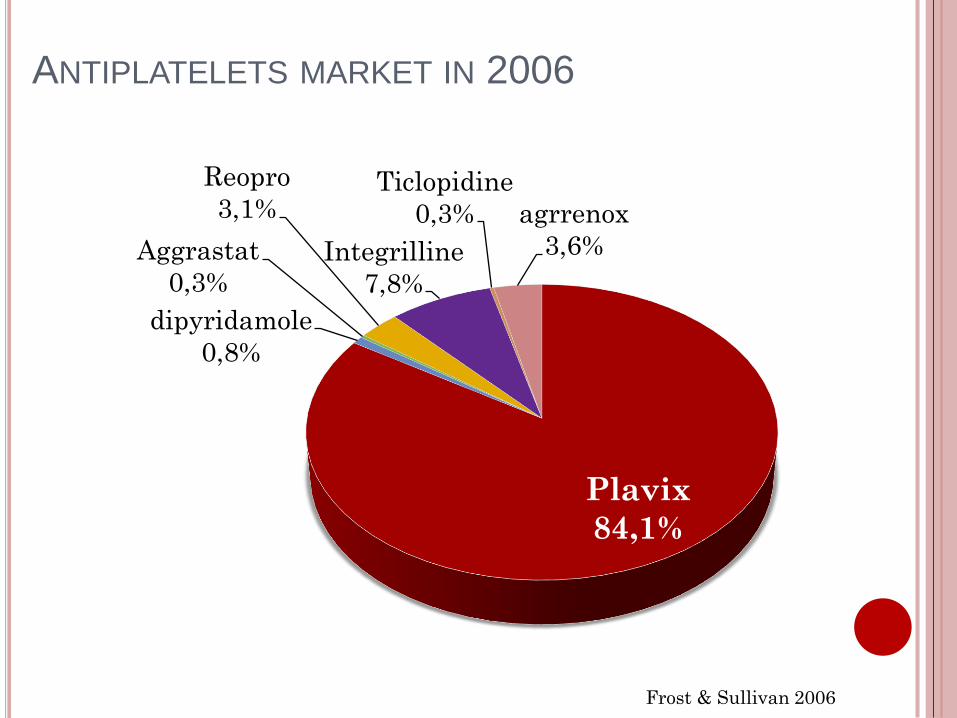
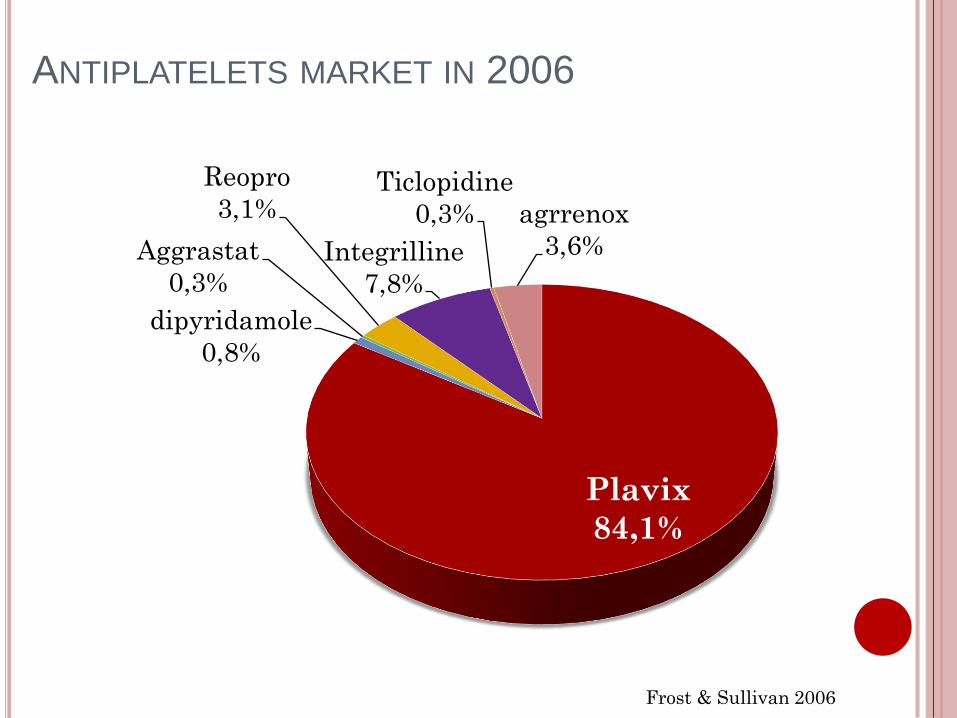
ANTIPLATELETS MARKET IN 2006
Plavix
84,1%
dipyridamole
0,8%
Aggrastat
0,3%
Reopro
3,1%
Integrilline
7,8%
Ticlopidine
0,3% agrrenox
3,6%
Frost & Sullivan 2006
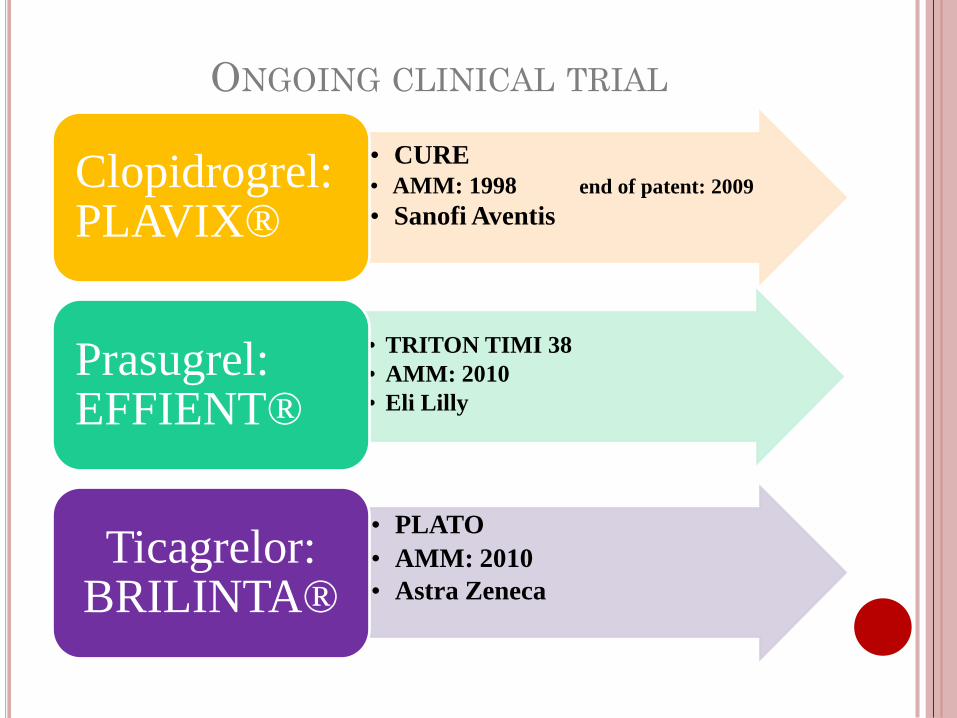
• CURE
• AMM: 1998 end of patent: 2009
• Sanofi Aventis
Clopidrogrel: PLAVIX®
• TRITON TIMI 38
• AMM: 2010
• Eli Lilly
Prasugrel: EFFIENT®
• PLATO
• AMM: 2010
• Astra Zeneca
Ticagrelor: BRILINTA®
ONGOING CLINICAL TRIAL
CLOPIDOGREL
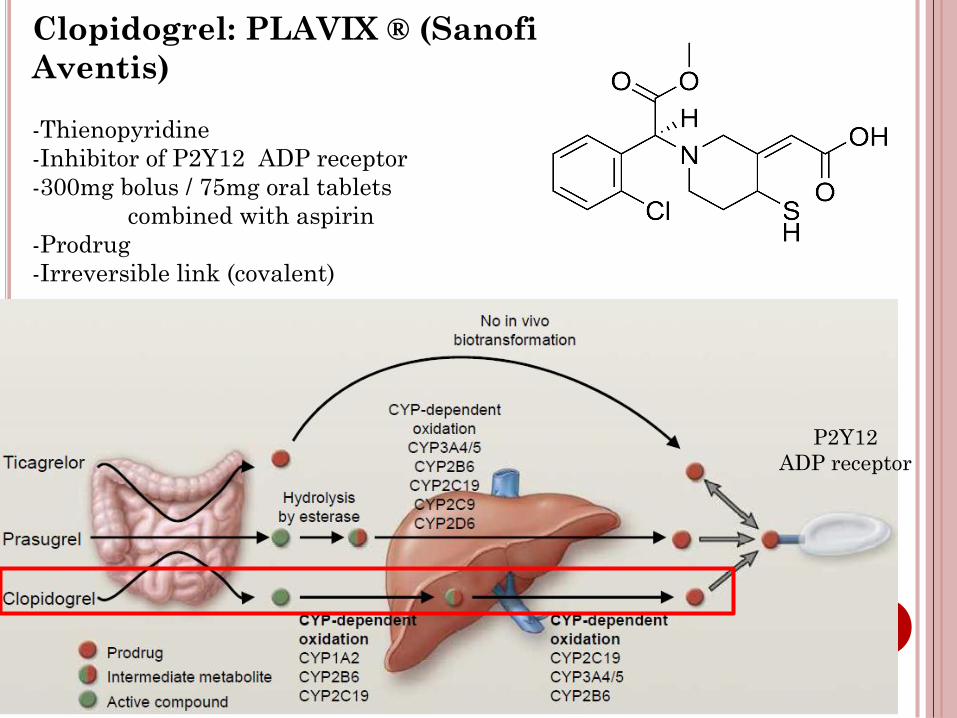
Clopidogrel: PLAVIX ® (Sanofi
Aventis)
-Thienopyridine
-Inhibitor of P2Y12 ADP receptor
-300mg bolus / 75mg oral tablets
combined with aspirin
-Prodrug
-Irreversible link (covalent)
P2Y12
ADP receptor
S
N
Cl
H COOCH3
S
N
Cl
H COOCH3
O
N
Cl
H COOCH3
SH
HOOC
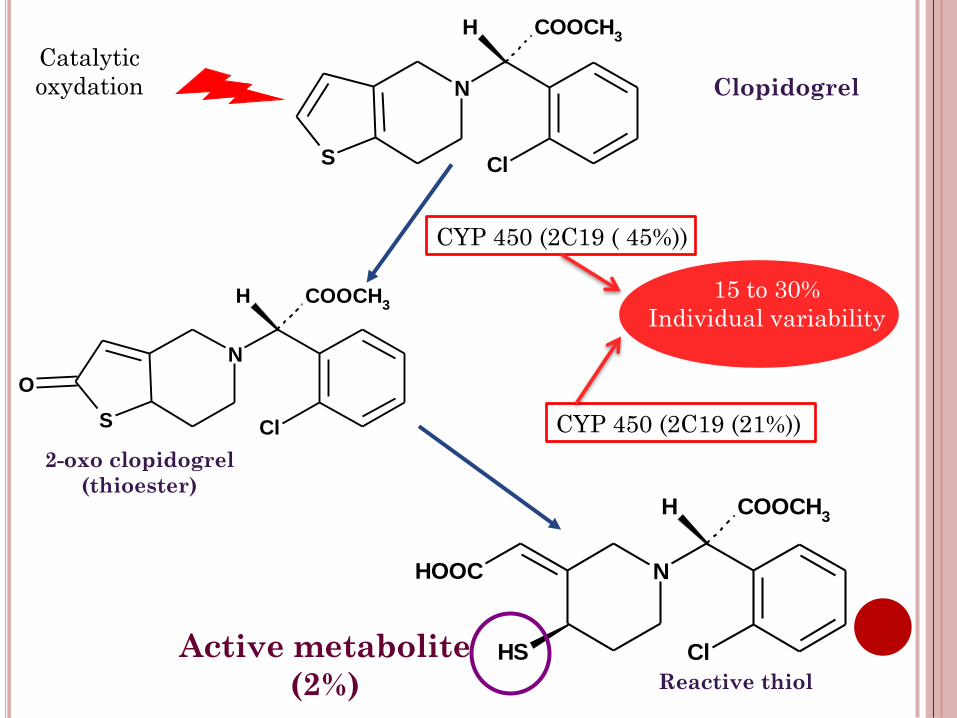
2-oxo clopidogrel
(thioester)
Reactive thiol
Active metabolite
(2%)
Clopidogrel
Catalytic
oxydation
CYP 450 (2C19 ( 45%))
CYP 450 (2C19 (21%))
15 to 30%
Individual variability
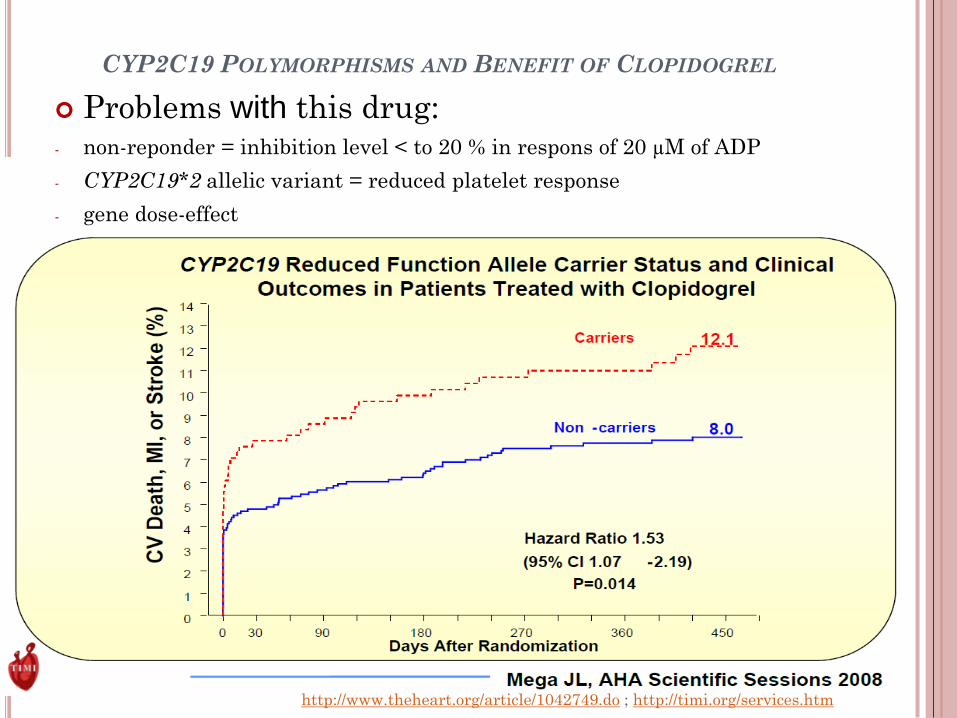
CYP2C19 POLYMORPHISMS AND BENEFIT OF CLOPIDOGREL
Problems with this drug:- non-reponder = inhibition level < to 20 % in respons of 20 µM of ADP
- CYP2C19*2 allelic variant = reduced platelet response
- gene dose-effect
http://www.theheart.org/article/1042749.do ; http://timi.org/services.htm
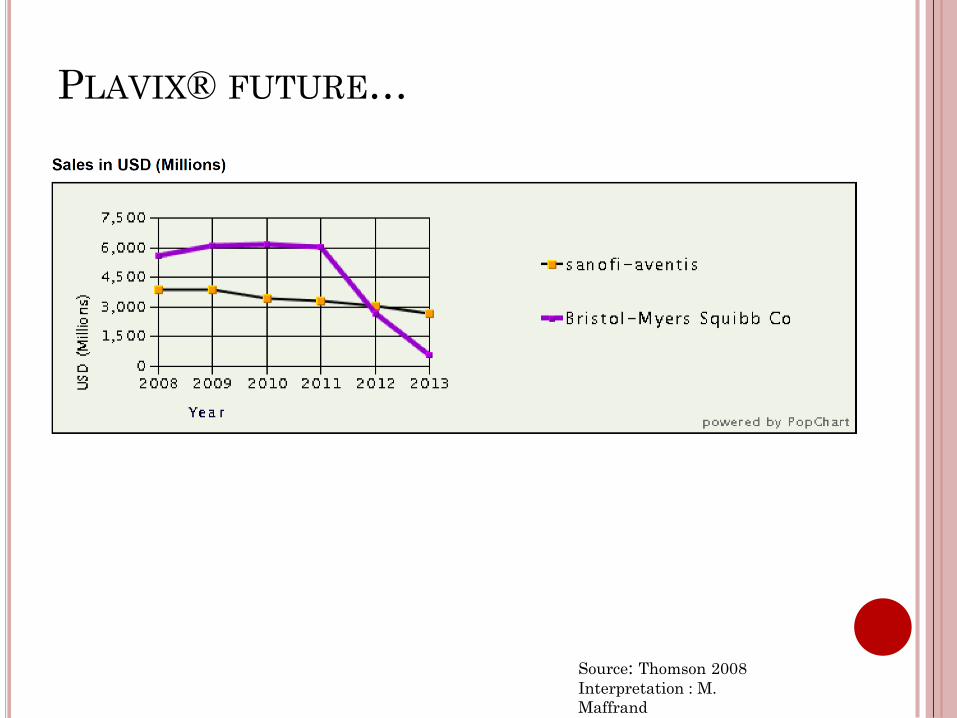
PLAVIX® FUTURE…
Source: Thomson 2008
Interpretation : M.
Maffrand
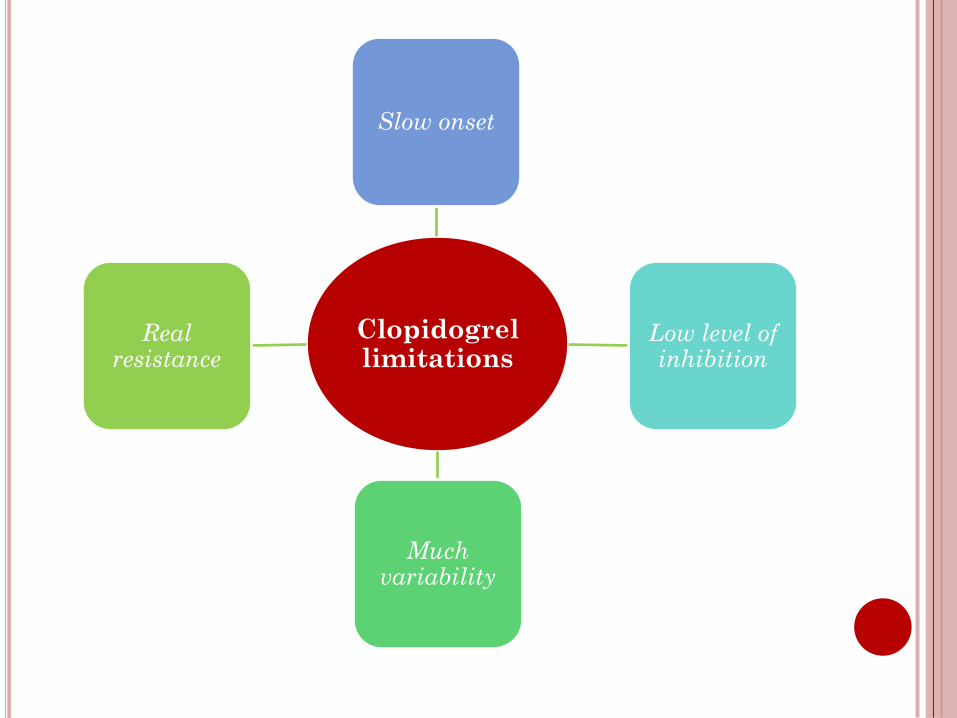
Clopidogrellimitations
Slow onset
Low level of inhibition
Much variability
Real resistance
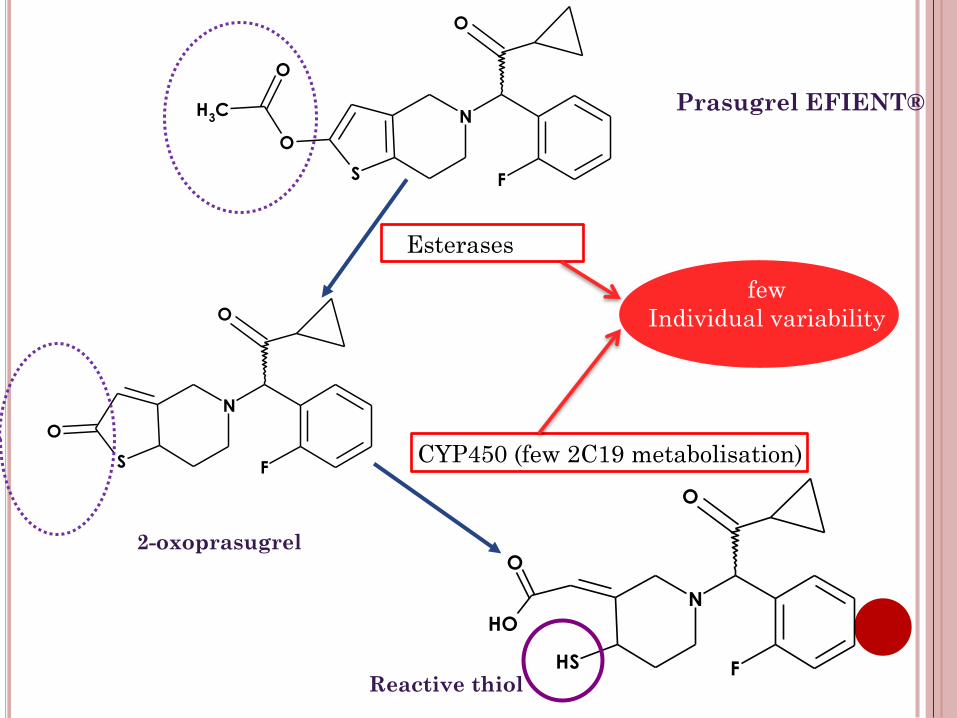
PRASUGREL
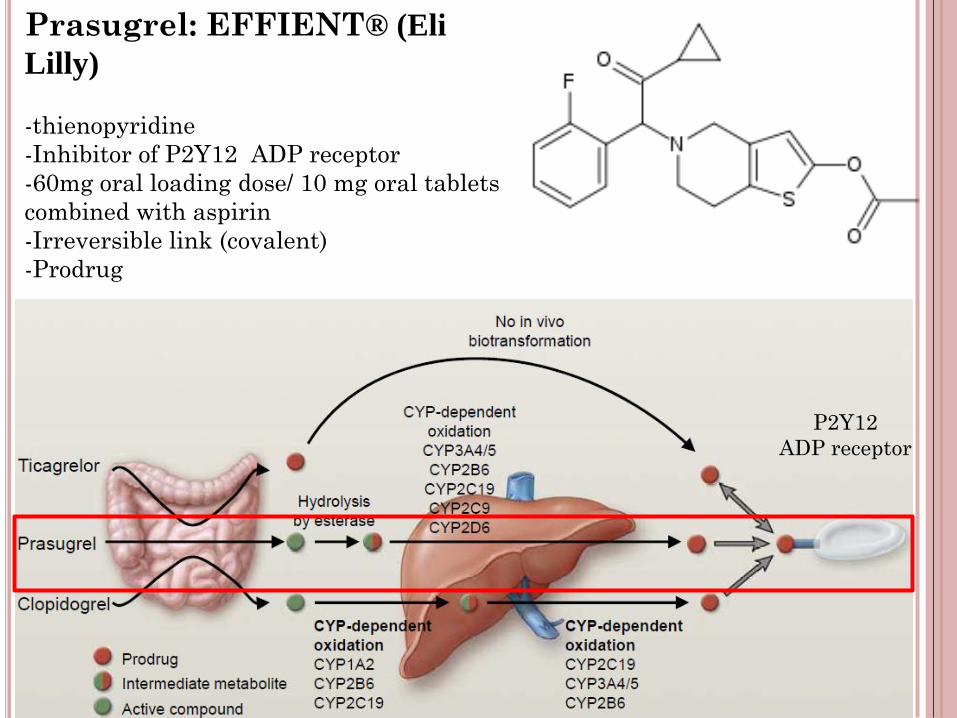
Prasugrel: EFFIENT® (Eli
Lilly)
-thienopyridine
-Inhibitor of P2Y12 ADP receptor
-60mg oral loading dose/ 10 mg oral tablets
combined with aspirin
-Irreversible link (covalent)
-Prodrug
P2Y12
ADP receptor
S
N
F
O
CH3
O
O
S
N
F
O
O
SH
N
F
O
O
OH
Prasugrel EFIENT®
Esterases
CYP450 (few 2C19 metabolisation)
2-oxoprasugrel
few
Individual variability
Reactive thiol

TRITON TRIAL
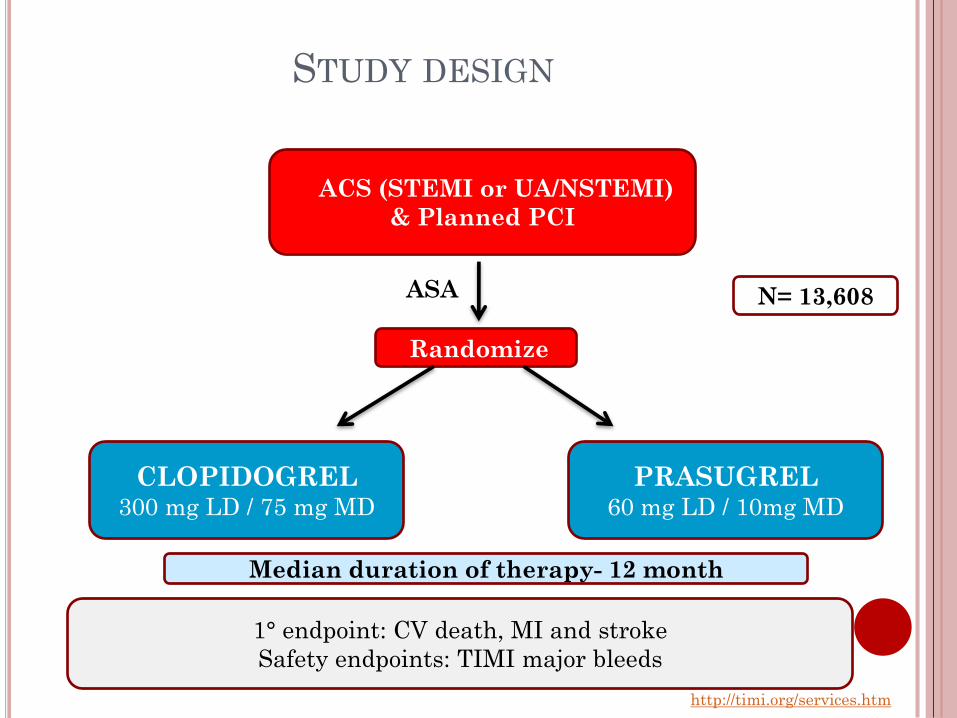
ACS (STEMI or UA/NSTEMI)
& Planned PCI
Randomize
PRASUGREL 60 mg LD / 10mg MD
CLOPIDOGREL300 mg LD / 75 mg MD
N= 13,608ASA
Median duration of therapy- 12 month
1° endpoint: CV death, MI and stroke
Safety endpoints: TIMI major bleeds
STUDY DESIGN
http://timi.org/services.htm
http://timi.org/services.ht
m
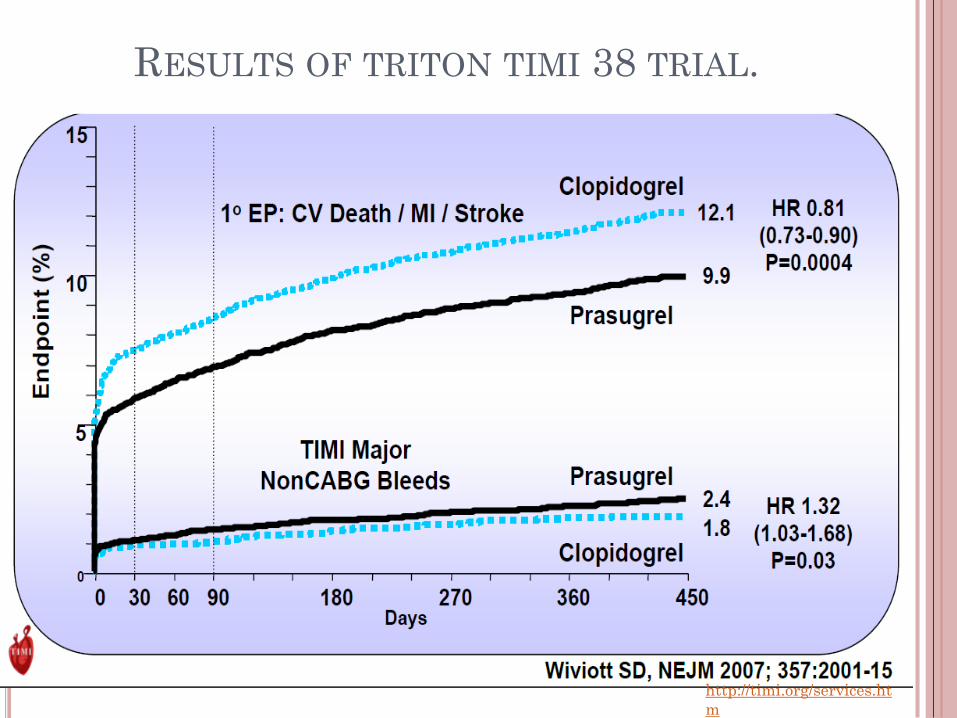
RESULTS OF TRITON TIMI 38 TRIAL.
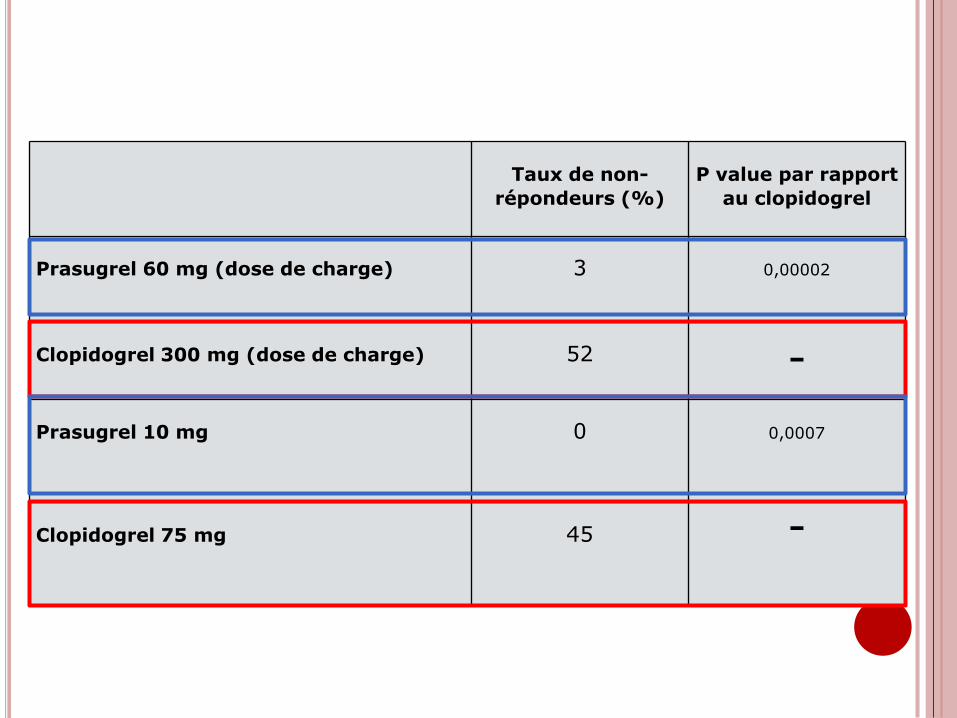
Taux de non-
répondeurs (%)
P value par rapport
au clopidogrel
Prasugrel 60 mg (dose de charge) 3 0,00002
Clopidogrel 300 mg (dose de charge) 52 -
Prasugrel 10 mg 0 0,0007
Clopidogrel 75 mg 45 -
http://timi.org/services.htm
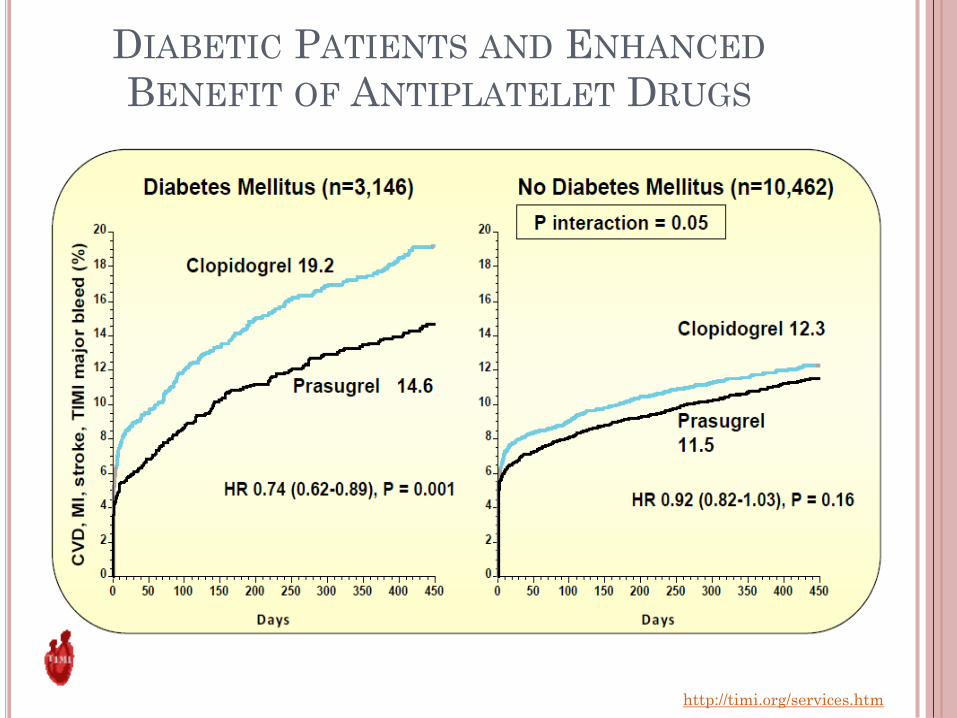
DIABETIC PATIENTS AND ENHANCED
BENEFIT OF ANTIPLATELET DRUGS
http://timi.org/services.htm
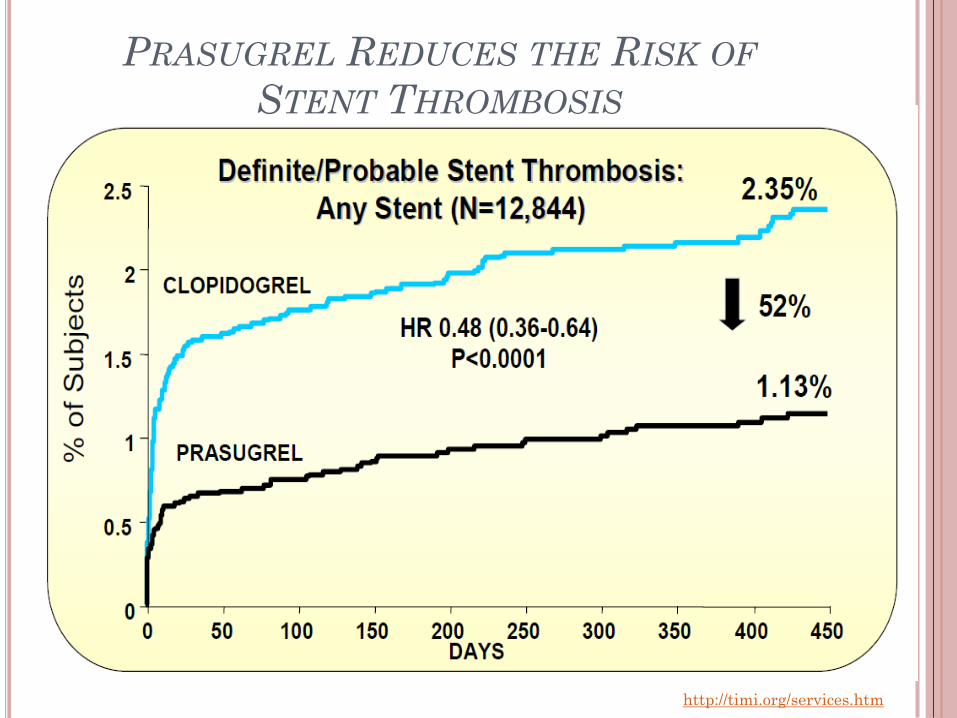
PRASUGREL REDUCES THE RISK OF
STENT THROMBOSIS
PRASUGREL PROFILE
Prasugrel advantages
- A significant reduction in CV death, MI and
stroke (19%)
- An earlier and sustained benefits
- Less non reponders
- good response of diabetes patients
Prasugrel Inconvenients
- Not a reversible drug
- Significant increase in serious bleeding (32% increase)
- Doses adjustement for < 60kg and > 75 years (5mg?)
- Contre-indication in stroke.
TICAGRELOR
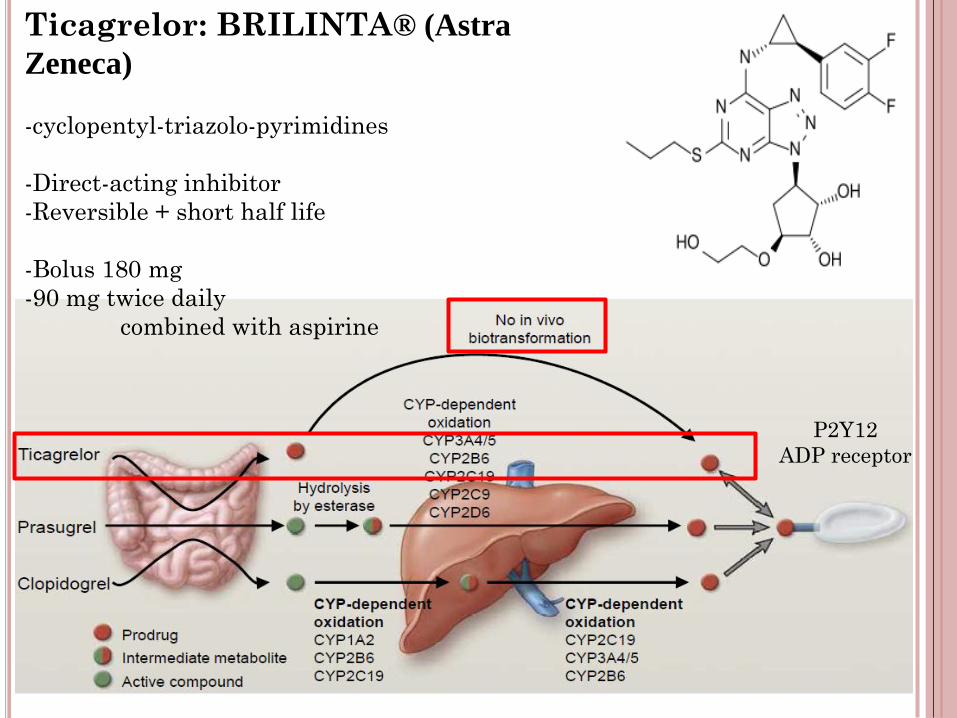
Ticagrelor: BRILINTA® (Astra
Zeneca)
-cyclopentyl-triazolo-pyrimidines
-Direct-acting inhibitor
-Reversible + short half life
-Bolus 180 mg
-90 mg twice daily
combined with aspirine
P2Y12
ADP receptor
PLATO TRIAL
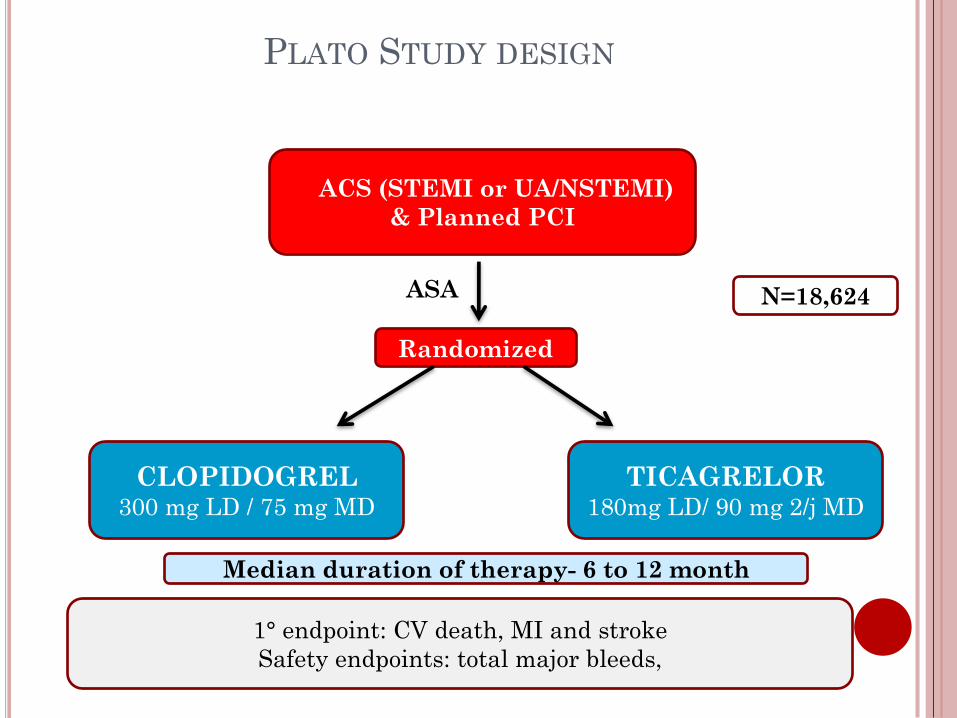
PLATO STUDY DESIGN
ACS (STEMI or UA/NSTEMI)
& Planned PCI
Randomized
TICAGRELOR 180mg LD/ 90 mg 2/j MD
CLOPIDOGREL300 mg LD / 75 mg MD
N=18,624ASA
Median duration of therapy- 6 to 12 month
1° endpoint: CV death, MI and stroke
Safety endpoints: total major bleeds,
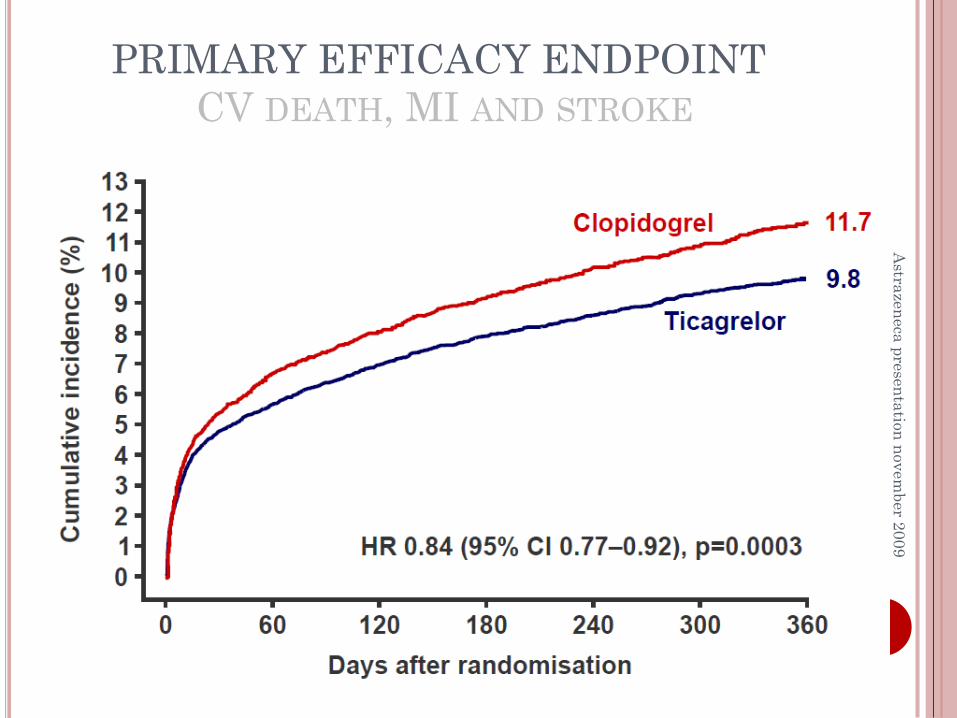
PRIMARY EFFICACY ENDPOINT
CV DEATH, MI AND STROKE
Astra
zen
eca
pre
sen
tatio
nn
ovem
ber
20
09
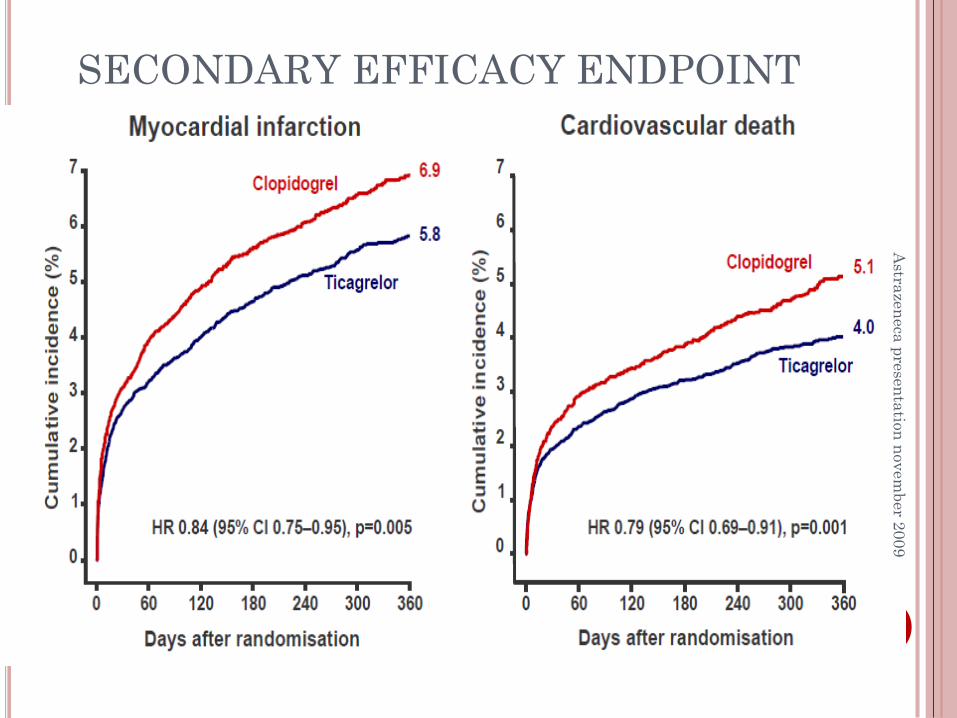
SECONDARY EFFICACY ENDPOINTA
strazen
eca
pre
sen
tatio
n n
ovem
ber 2
00
9
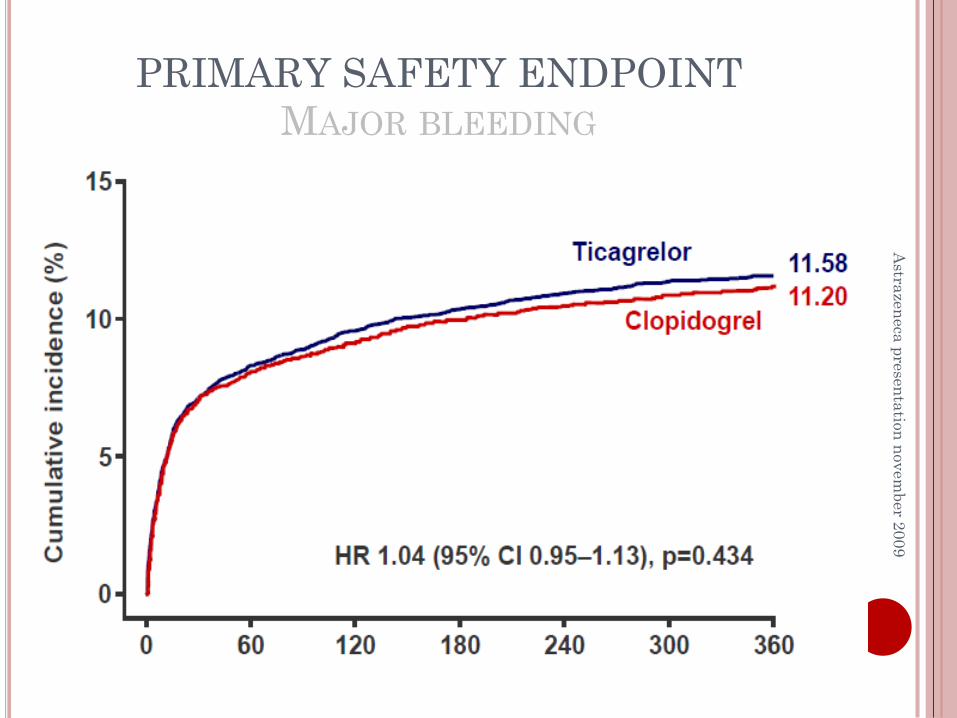
PRIMARY SAFETY ENDPOINT
MAJOR BLEEDING
Astra
zen
eca
pre
sen
tatio
n n
ovem
ber 2
00
9
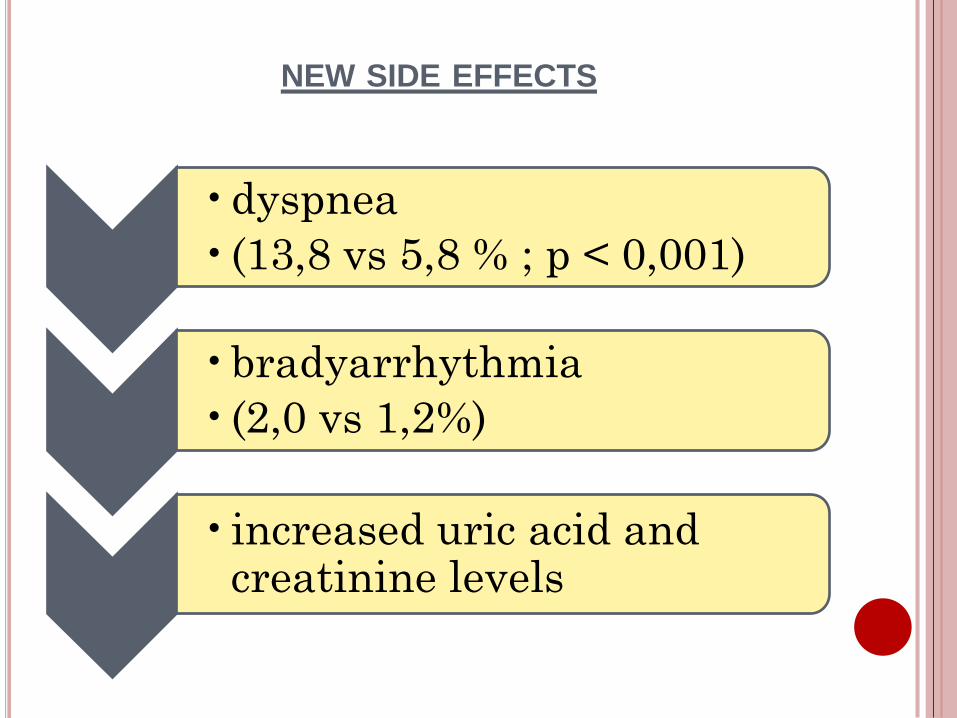
NEW SIDE EFFECTS
•dyspnea
•(13,8 vs 5,8 % ; p < 0,001)
•bradyarrhythmia
•(2,0 vs 1,2%)
•increased uric acid and creatinine levels
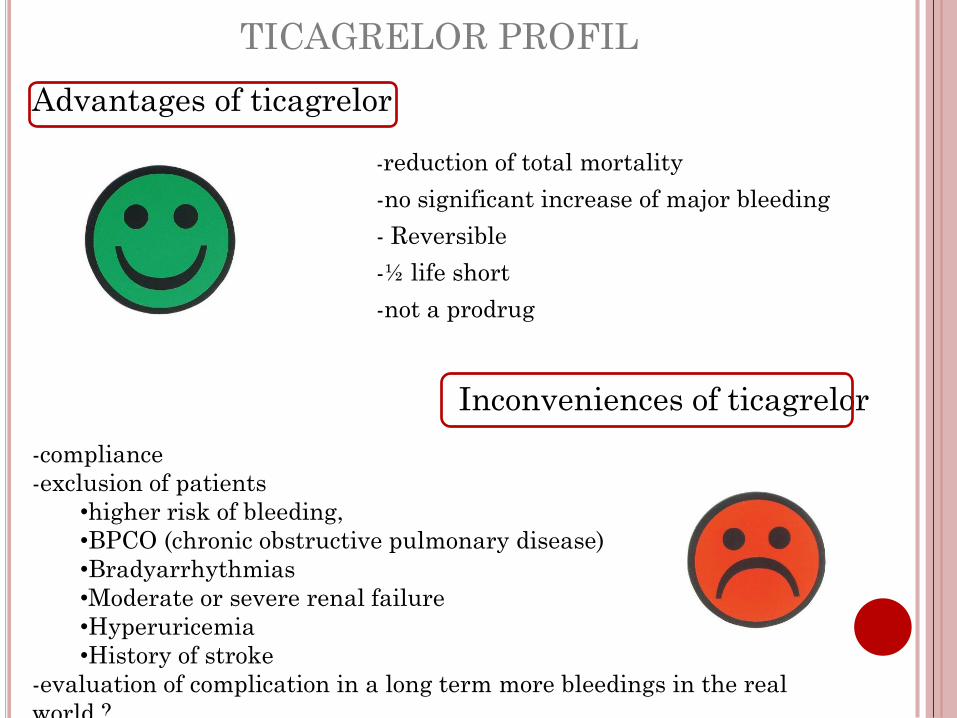
TICAGRELOR PROFIL
-reduction of total mortality
-no significant increase of major bleeding
- Reversible
-½ life short
-not a prodrug
Inconveniences of ticagrelor
-compliance
-exclusion of patients
•higher risk of bleeding,
•BPCO (chronic obstructive pulmonary disease)
•Bradyarrhythmias
•Moderate or severe renal failure
•Hyperuricemia
•History of stroke
-evaluation of complication in a long term more bleedings in the real
world ?
Advantages of ticagrelor
Dr Albert Schömig (Munich,
Germany)
“now we have a new and better
alternative to standard treatment
to prevent patients with myocardial
infarction from new myocardial
infarction, and also to improve their
chances of survival “
UCLA cardiologist Dr. Gregg C.
Fonarow
"Ticagrelor represents an
important new treatment advance
for the management of patients
with acute coronary syndromes."
Dr. Byron Lee, a
cardiologist from the
University of California at
San Francisco
“ I expect this new drug to
get FDA approval very
soon.”
Steen D. Kristensen, MD, of
Aarhus University, Skejby,
Denmark
“a promising drug “
Med 2009;361. DOI 10.1056/NEJMe0906549
European Soiety of Cardiology Congress 2009; Aug.
29-Sept. 2, 2009; Barcelona
Schomig said. "We have now the opportunity to choose between three drugs, clopidogrel, prasugrel [Effient] and ticagrelor, in patients with acute coronary syndromes, taking into account the advantages and disadvantages of each one"
2ND PARTAnticoagulants in Atrial Fibrillation (AF)
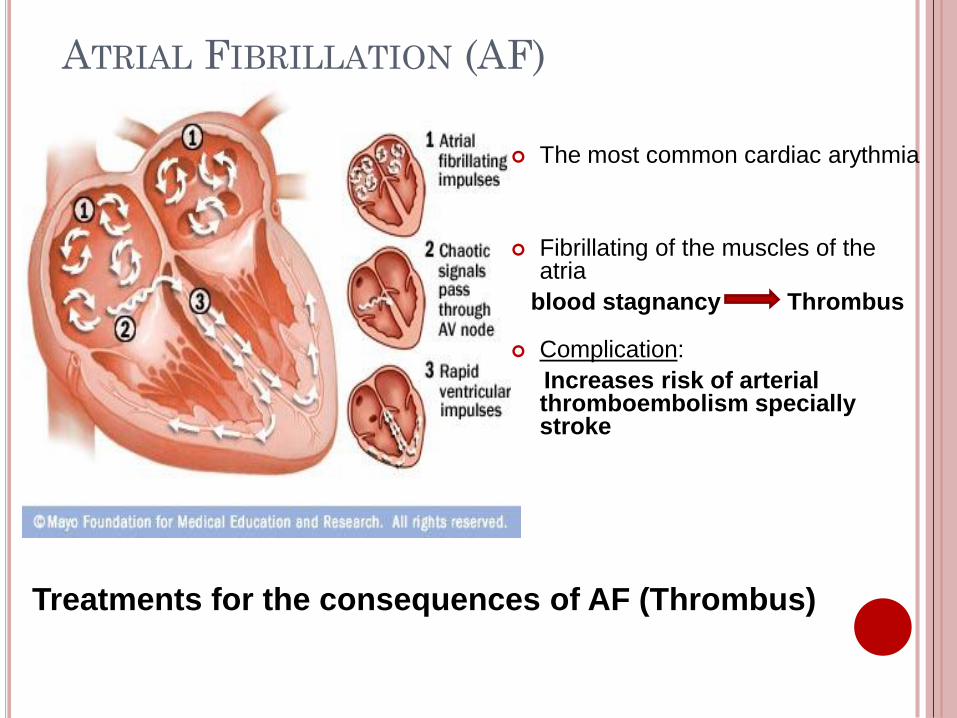
ATRIAL FIBRILLATION (AF)
The most common cardiac arythmia
Fibrillating of the muscles of the atria
blood stagnancy Thrombus
Complication:
Increases risk of arterialthromboembolism speciallystroke
Treatments for the consequences of AF (Thrombus)
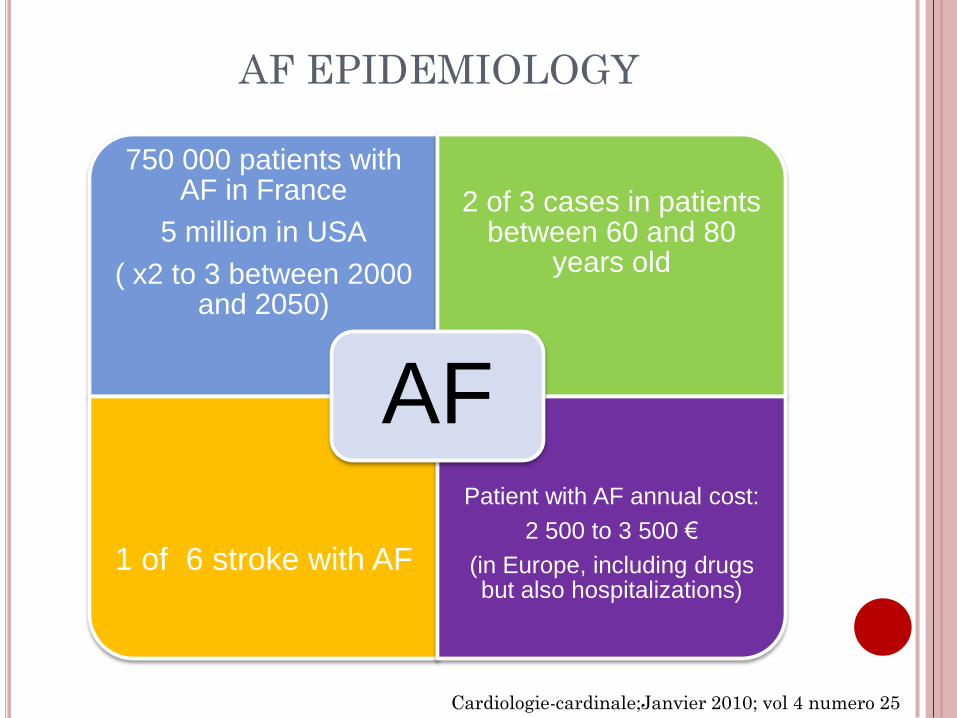
AF EPIDEMIOLOGY
750 000 patients withAF in France
5 million in USA
( x2 to 3 between 2000 and 2050)
2 of 3 cases in patients between 60 and 80
years old
1 of 6 stroke with AF
Patient with AF annual cost:
2 500 to 3 500 €
(in Europe, including drugsbut also hospitalizations)
AF
Cardiologie-cardinale;Janvier 2010; vol 4 numero 25
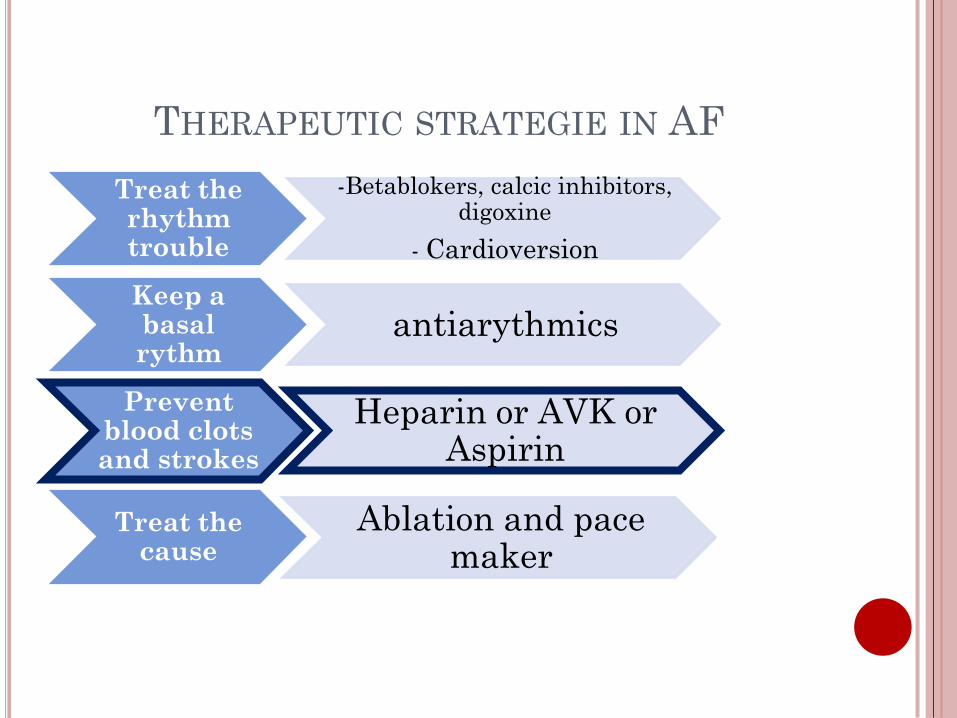
THERAPEUTIC STRATEGIE IN AF
Treat the rhythm trouble
-Betablokers, calcic inhibitors, digoxine
- Cardioversion
Keep a basal rythm
antiarythmics
Prevent blood clots and strokes
Heparin or AVK or Aspirin
Ablation and pace maker
Treat the cause
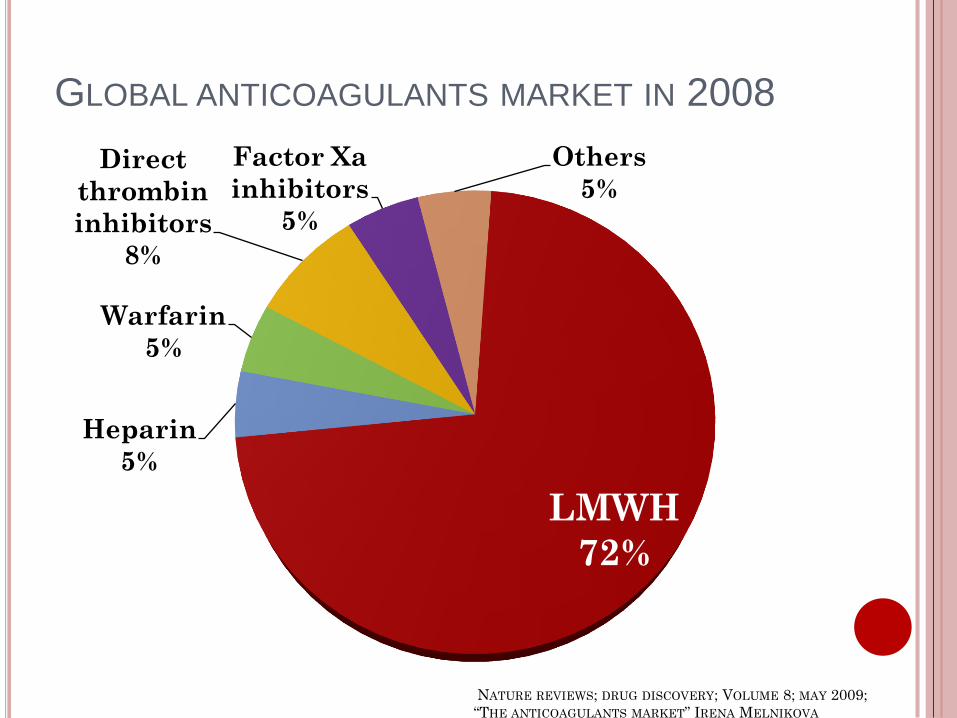
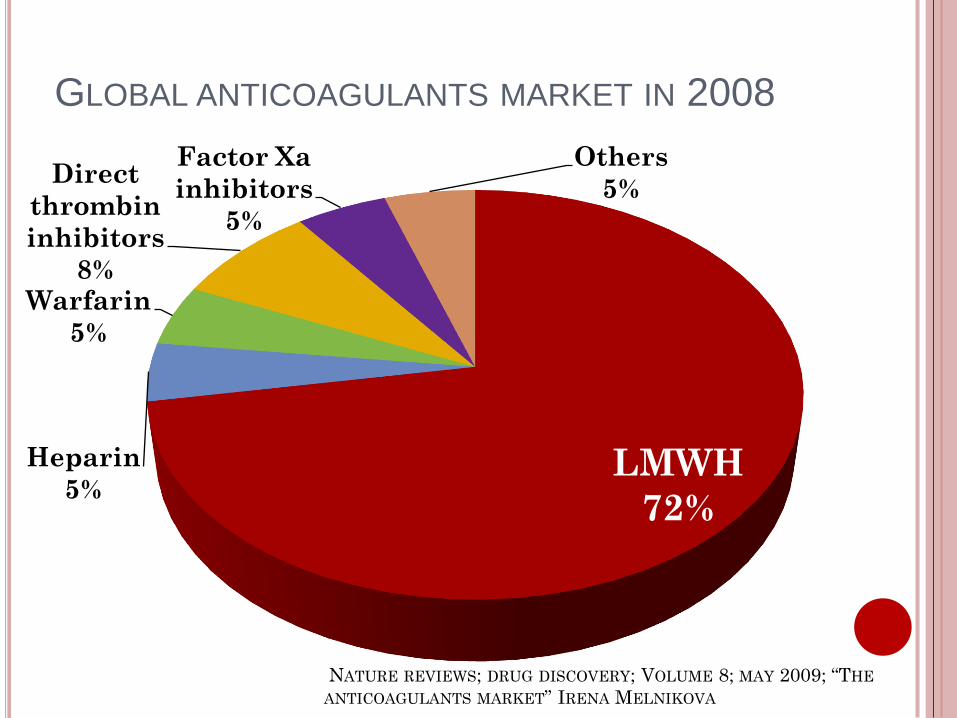
GLOBAL ANTICOAGULANTS MARKET IN 2008
LMWH
72%
Heparin
5%
Warfarin
5%
Direct
thrombin
inhibitors
8%
Factor Xa
inhibitors
5%
Others
5%
NATURE REVIEWS; DRUG DISCOVERY; VOLUME 8; MAY 2009;
“THE ANTICOAGULANTS MARKET” IRENA MELNIKOVA
WARFARIN
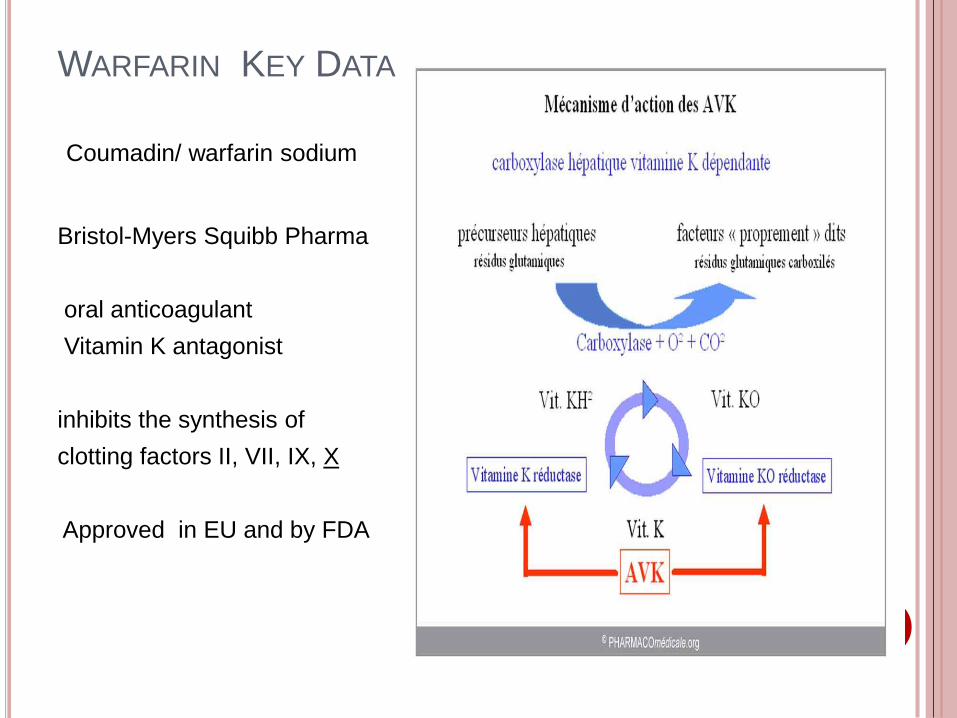
WARFARIN KEY DATA
Coumadin/ warfarin sodium
Bristol-Myers Squibb Pharma
oral anticoagulant
Vitamin K antagonist
inhibits the synthesis of
clotting factors II, VII, IX, X
Approved in EU and by FDA
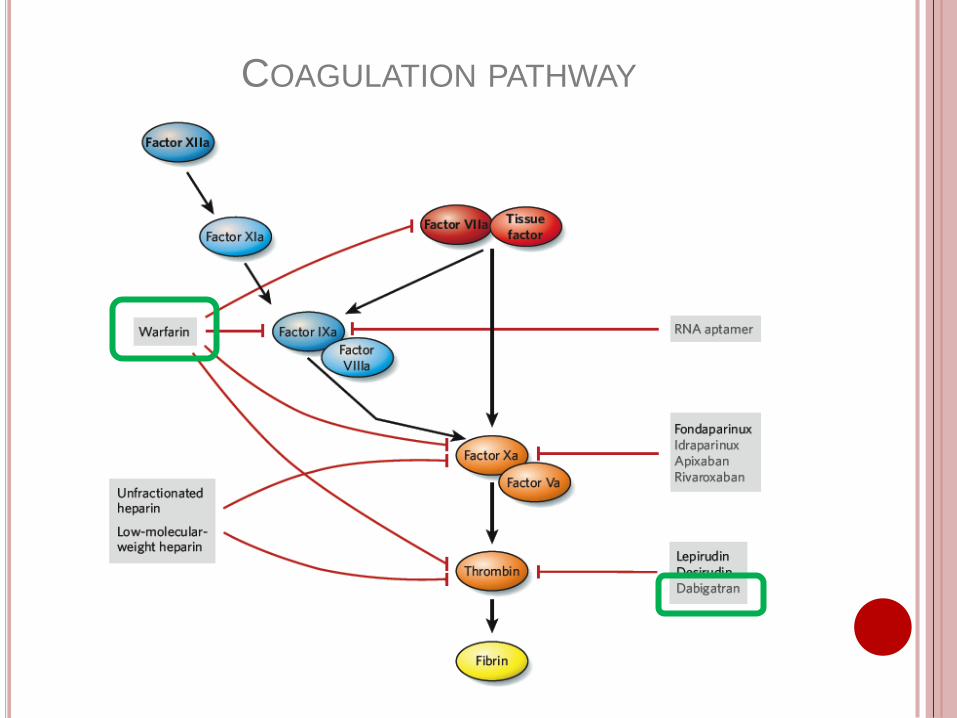
COAGULATION PATHWAY
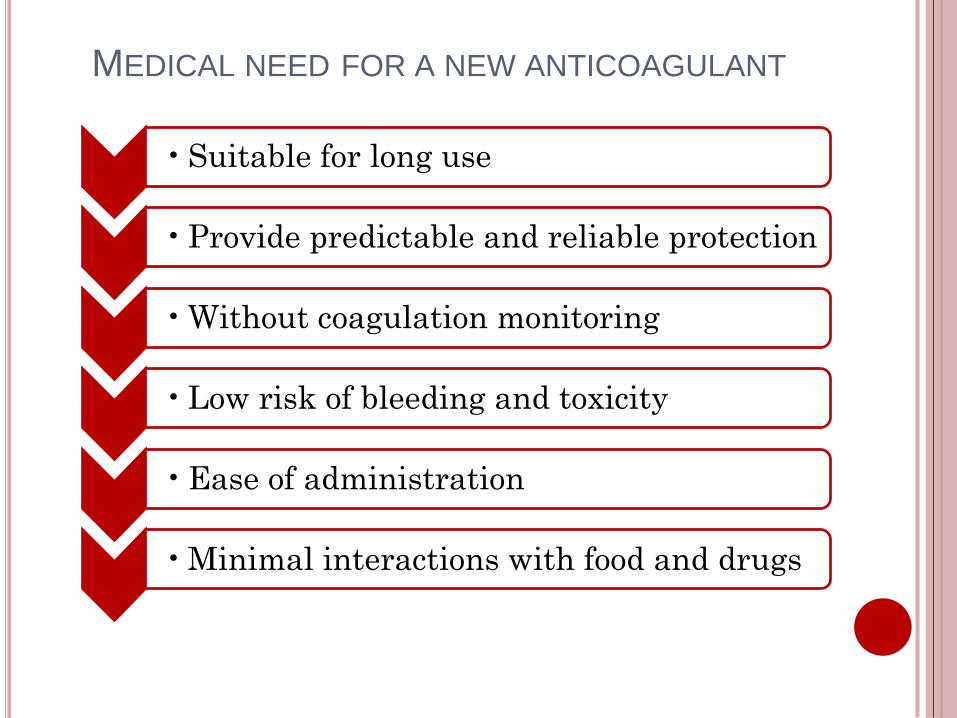
• Suitable for long use
• Provide predictable and reliable protection
• Without coagulation monitoring
• Low risk of bleeding and toxicity
• Ease of administration
• Minimal interactions with food and drugs
MEDICAL NEED FOR A NEW ANTICOAGULANT
DABIGATRAN ETEXYLATE
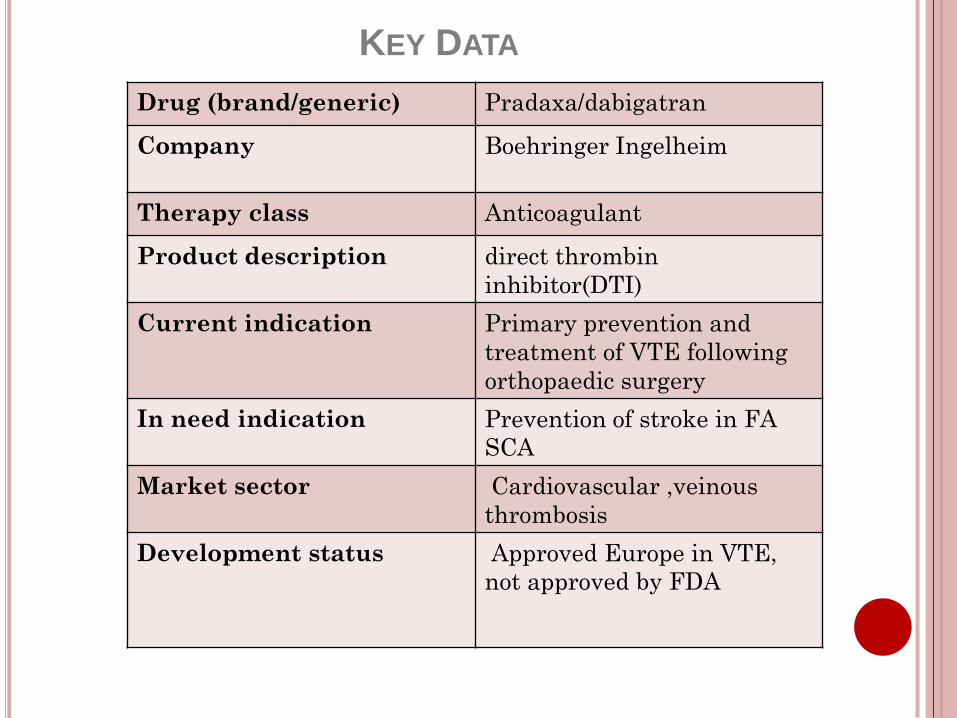
Drug (brand/generic) Pradaxa/dabigatran
Company Boehringer Ingelheim
Therapy class Anticoagulant
Product description direct thrombin
inhibitor(DTI)
Current indication Primary prevention and
treatment of VTE following
orthopaedic surgery
In need indication Prevention of stroke in FA
SCA
Market sector Cardiovascular ,veinous
thrombosis
Development status Approved Europe in VTE,
not approved by FDA
KEY DATA
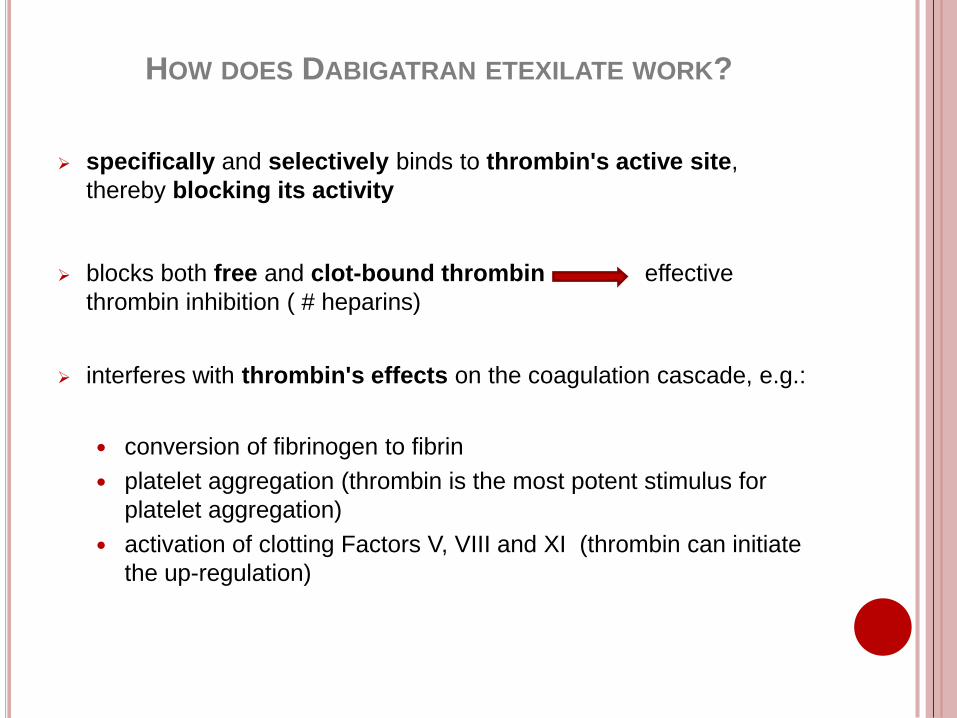
HOW DOES DABIGATRAN ETEXILATE WORK?
specifically and selectively binds to thrombin's active site,
thereby blocking its activity
blocks both free and clot-bound thrombin effective
thrombin inhibition ( # heparins)
interferes with thrombin's effects on the coagulation cascade, e.g.:
conversion of fibrinogen to fibrin
platelet aggregation (thrombin is the most potent stimulus for
platelet aggregation)
activation of clotting Factors V, VIII and XI (thrombin can initiate
the up-regulation)
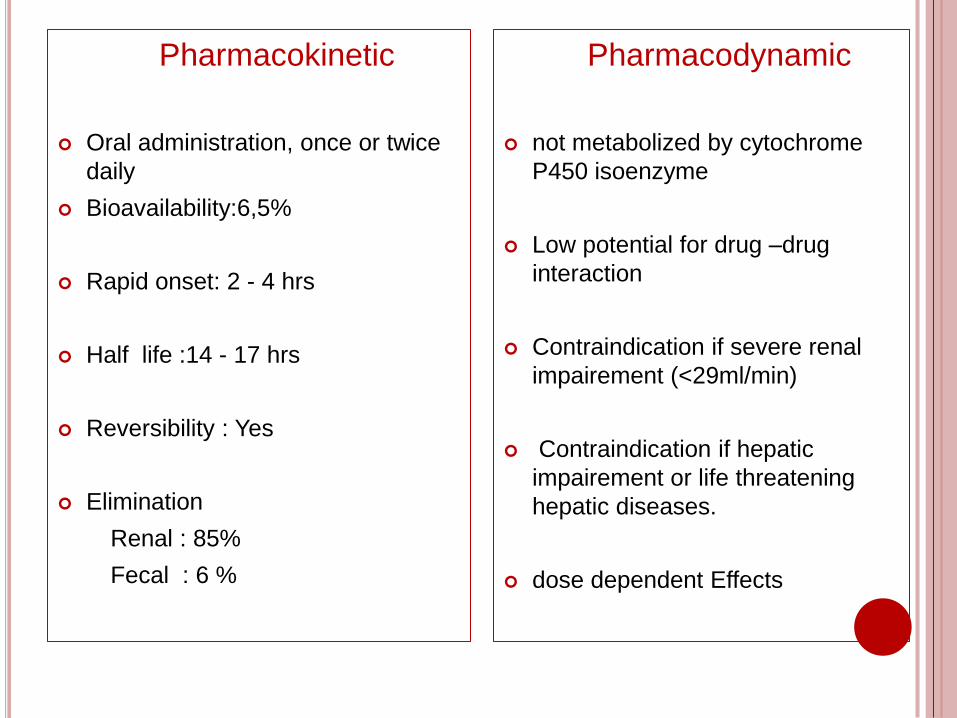
Pharmacokinetic
Oral administration, once or twice
daily
Bioavailability:6,5%
Rapid onset: 2 - 4 hrs
Half life :14 - 17 hrs
Reversibility : Yes
Elimination
Renal : 85%
Fecal : 6 %
Pharmacodynamic
not metabolized by cytochrome
P450 isoenzyme
Low potential for drug –drug
interaction
Contraindication if severe renal
impairement (<29ml/min)
Contraindication if hepatic
impairement or life threatening
hepatic diseases.
dose dependent Effects
RELY TRIAL
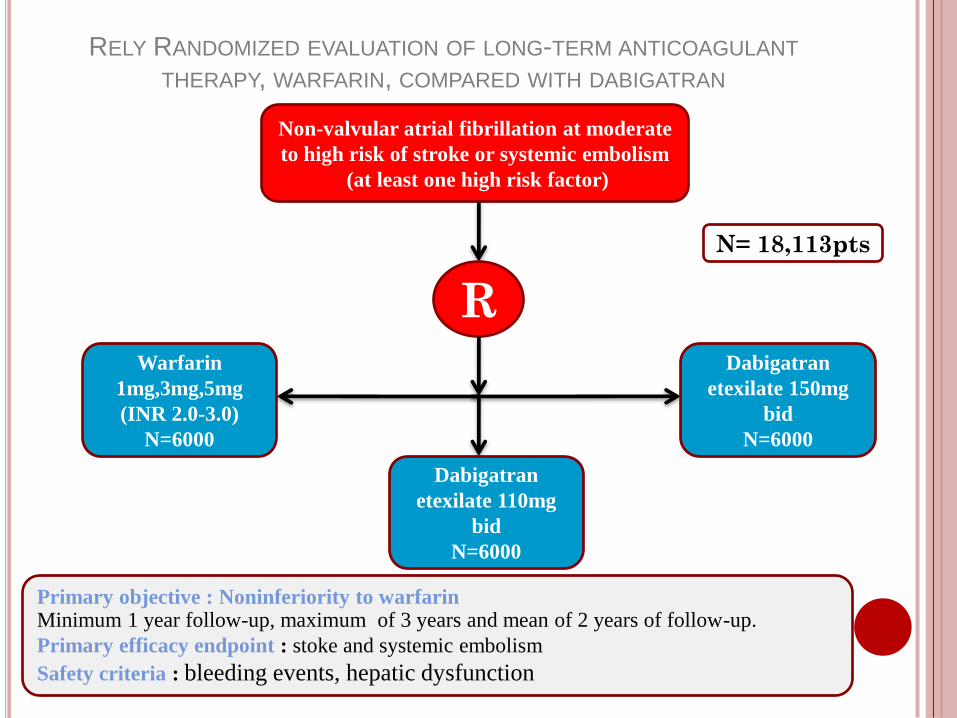
RELY RANDOMIZED EVALUATION OF LONG-TERM ANTICOAGULANT
THERAPY, WARFARIN, COMPARED WITH DABIGATRAN
Non-valvular atrial fibrillation at moderate
to high risk of stroke or systemic embolism
(at least one high risk factor)
R
Dabigatran
etexilate 110mg
bid
N=6000
Dabigatran
etexilate 150mg
bid
N=6000
Warfarin
1mg,3mg,5mg
(INR 2.0-3.0)
N=6000
Primary objective : Noninferiority to warfarinMinimum 1 year follow-up, maximum of 3 years and mean of 2 years of follow-up.
Primary efficacy endpoint : stoke and systemic embolism
Safety criteria : bleeding events, hepatic dysfunction
N= 18,113pts
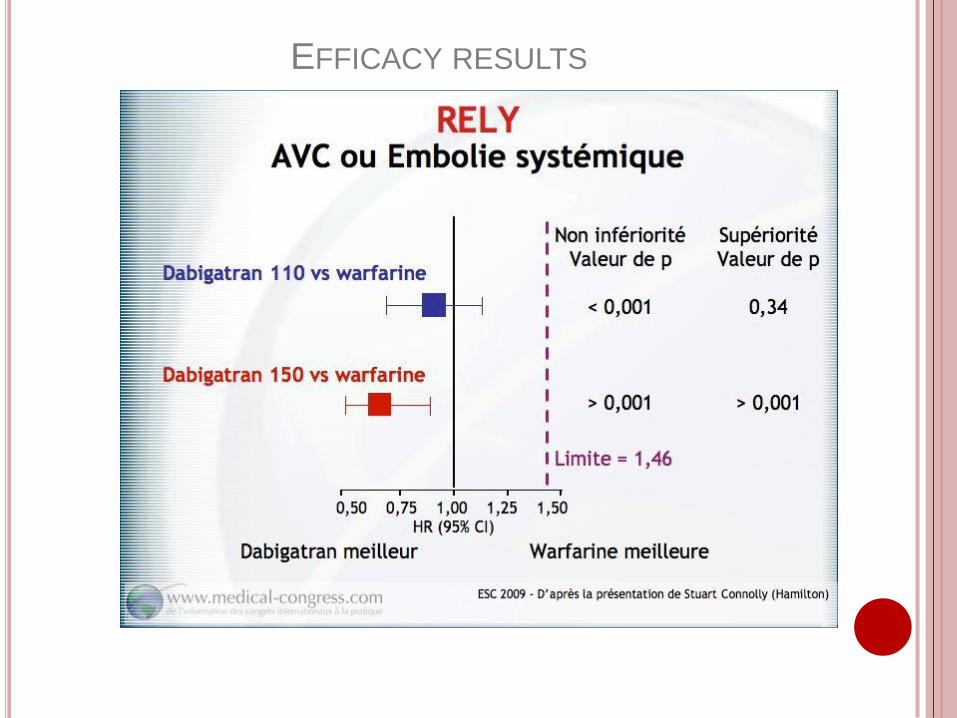
EFFICACY RESULTS
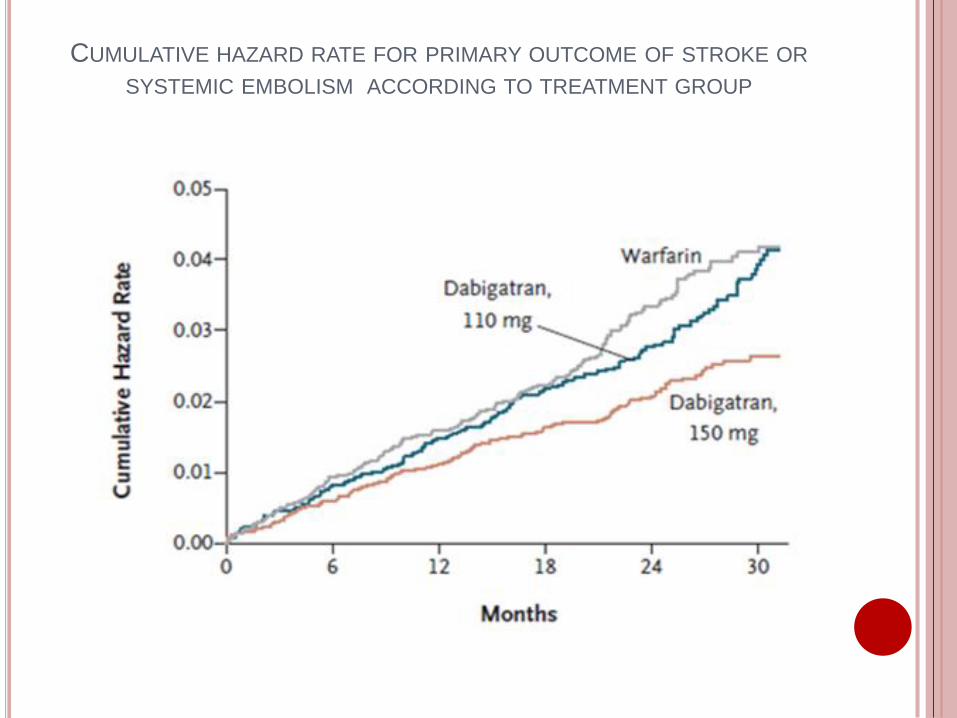
CUMULATIVE HAZARD RATE FOR PRIMARY OUTCOME OF STROKE OR
SYSTEMIC EMBOLISM ACCORDING TO TREATMENT GROUP
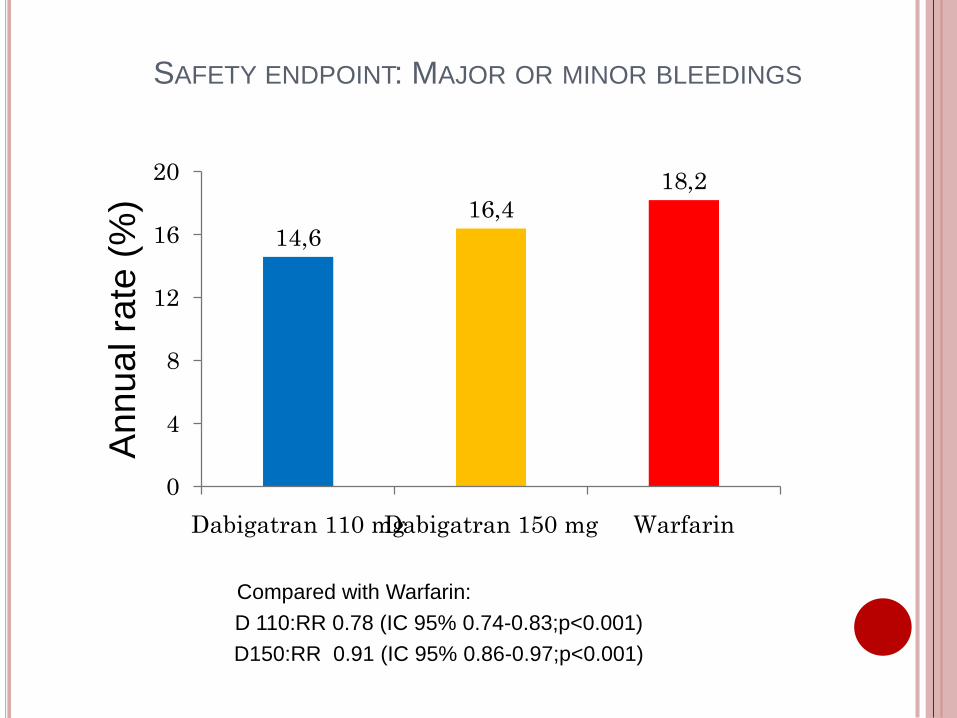
SAFETY ENDPOINT: MAJOR OR MINOR BLEEDINGS
Compared with Warfarin:
D 110:RR 0.78 (IC 95% 0.74-0.83;p<0.001)
D150:RR 0.91 (IC 95% 0.86-0.97;p<0.001)
14,6
16,4
18,2
0
4
8
12
16
20
Dabigatran 110 mgDabigatran 150 mg Warfarin
An
nu
alra
te (
%)
D 110mg D 150mg Warfarin D 110 mg vs Warfarin D 150 mg vs Warfarin
TTR Annual
rate
Annual
rate
Annual
rate
RR
IC 95% p
RR
IC 95% p
All
patients
0.23% 0 .30% 0.740.31
0.20-0.74 0.001
0.40
0.27-0.60 <0.001
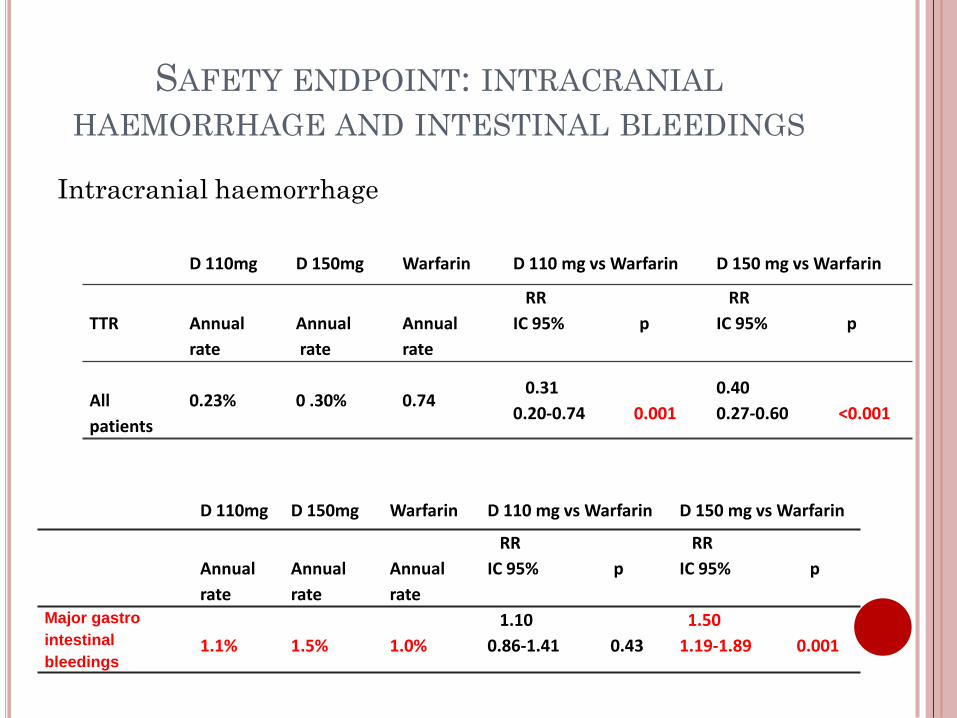
SAFETY ENDPOINT: INTRACRANIAL
HAEMORRHAGE AND INTESTINAL BLEEDINGS
Intracranial haemorrhage
D 110mg D 150mg Warfarin D 110 mg vs Warfarin D 150 mg vs Warfarin
Annual
rate
Annual
rate
Annual
rate
RR
IC 95% p
RR
IC 95% p
Major gastro
intestinal
bleedings1.1% 1.5% 1.0%
1.10
0.86-1.41 0.43
1.50
1.19-1.89 0.001
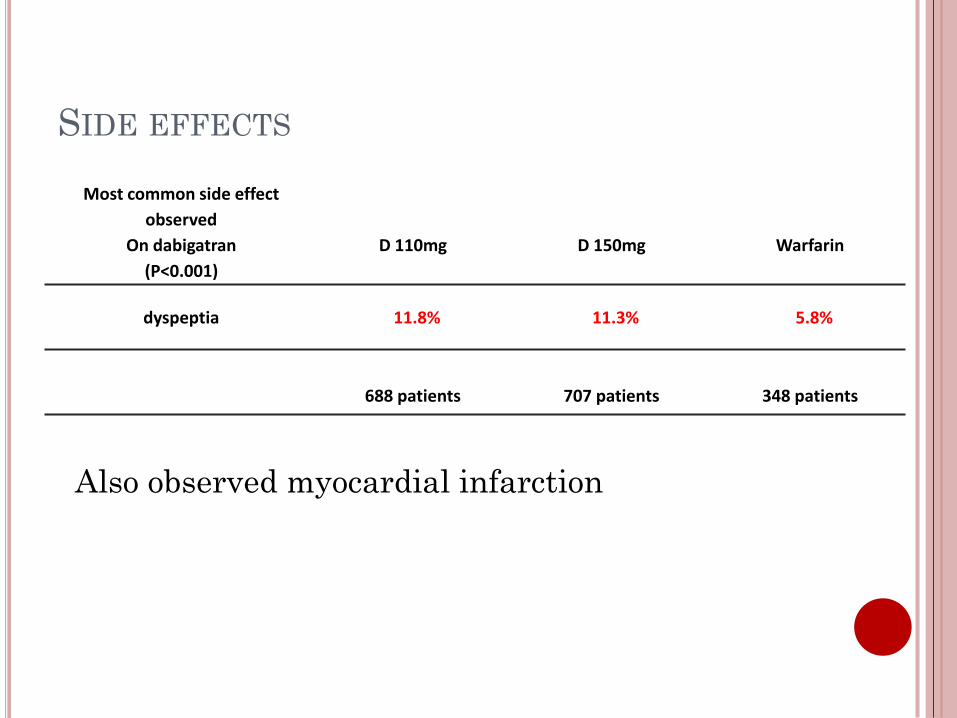
Most common side effect
observed
On dabigatran
(P<0.001)
D 110mg D 150mg Warfarin
dyspeptia 11.8% 11.3% 5.8%
688 patients 707 patients 348 patients
SIDE EFFECTS
Also observed myocardial infarction
DABIGATRAN PROFILE
Dabigatran advantages
-Oral therapy ,fixed dose
-Rapid onset of action
-No food and drug interactions
-Wide therapeutic window
-No coagulation monitoring
Dabigatran Inconvenients
-No antidote (half-life 17 hrs)
-C.I if severe renal impairement
-dyspectic symptoms
-risk of major gastrointestinal bleeding
Warfarin is a tough comparator,but the challenge for competitor products is now even tougher
Waiting for the NDA in the indication (FA)
Other trials are ongoing
A real revolution for the practicians
Dabigatran Market
2/3 of patients with AF important market
Untreated Patients with medium or high risk of AF
Patients taking aspirin instead of warfarin
Patients unstable with Warfarin
Maybe patients well balanced on Warfarin
Doses adaptation with Dabigatran according to safety profile
DISCUSSION

DISCUSSION
Anticoagulants
GLOBAL ANTICOAGULANTS MARKET IN 2008
LMWH
72%
Heparin
5%
Warfarin
5%
Direct
thrombin
inhibitors
8%
Factor Xa
inhibitors
5%
Others
5%
NATURE REVIEWS; DRUG DISCOVERY; VOLUME 8; MAY 2009; “THE
ANTICOAGULANTS MARKET” IRENA MELNIKOVA
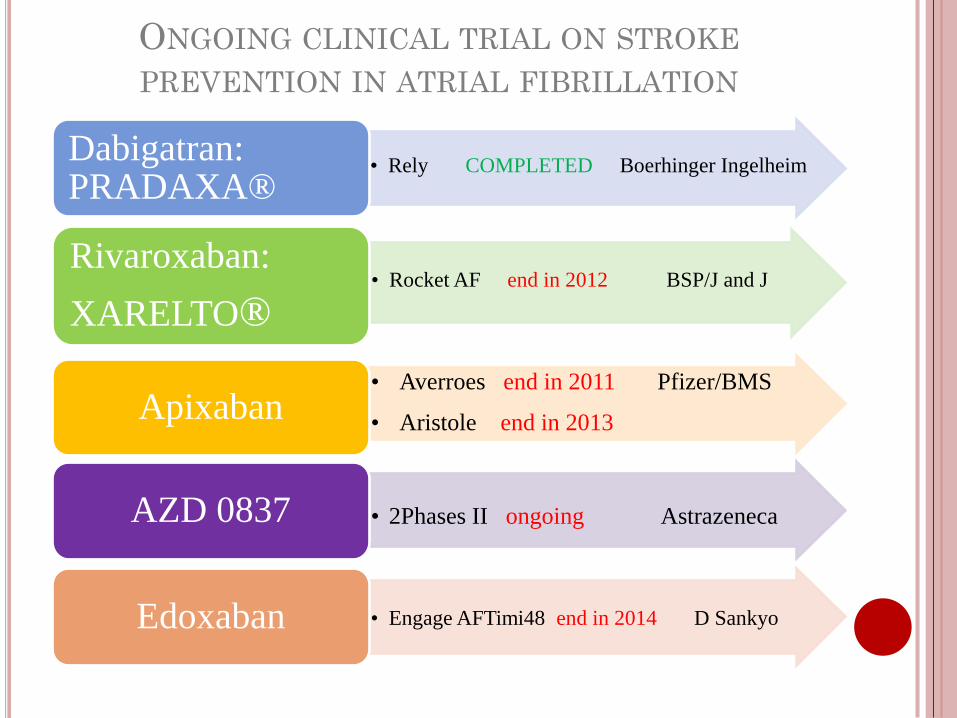
• Rely COMPLETED Boerhinger IngelheimDabigatran: PRADAXA®
• Rocket AF end in 2012 BSP/J and JRivaroxaban:
XARELTO®
• Averroes end in 2011 Pfizer/BMS
• Aristole end in 2013 Apixaban
• 2Phases II ongoing Astrazeneca AZD 0837
• Engage AFTimi48 end in 2014 D SankyoEdoxaban
ONGOING CLINICAL TRIAL ON STROKE
PREVENTION IN ATRIAL FIBRILLATION
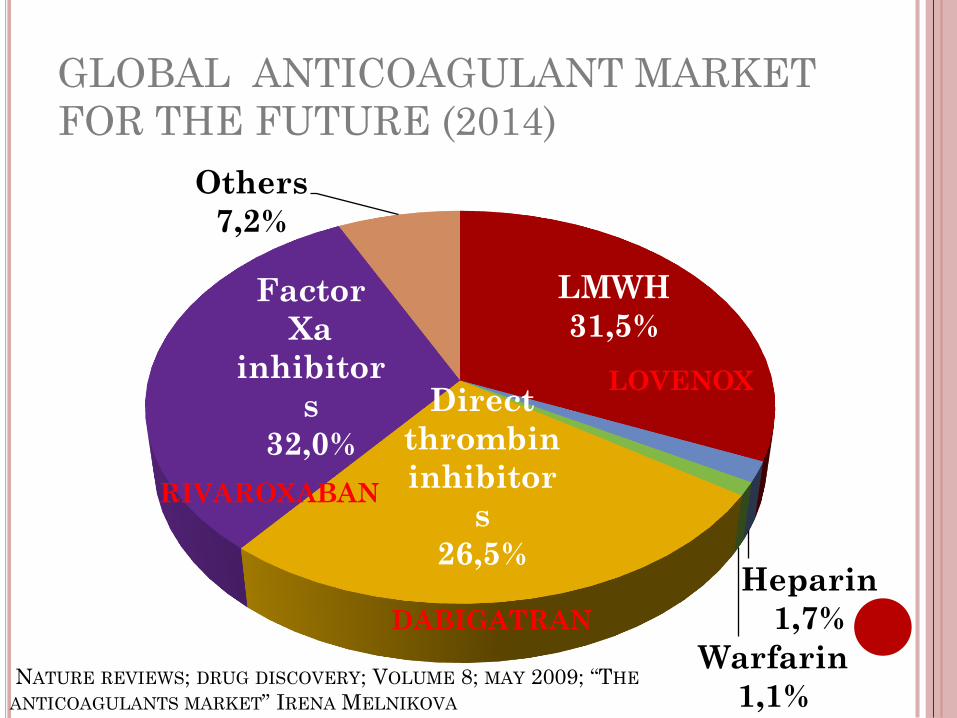
GLOBAL ANTICOAGULANT MARKET
FOR THE FUTURE (2014)
LMWH
31,5%
Heparin
1,7%
Warfarin
1,1%
Direct
thrombin
inhibitor
s
26,5%
Factor
Xa
inhibitor
s
32,0%
Others
7,2%
RIVAROXABAN
LOVENOX
DABIGATRAN
NATURE REVIEWS; DRUG DISCOVERY; VOLUME 8; MAY 2009; “THE
ANTICOAGULANTS MARKET” IRENA MELNIKOVA
DISCUSSION
Antiplatelets
ANTIPLATELETS MARKET IN 2006
Plavix
84,1%
dipyridamole
0,8%
Aggrastat
0,3%
Reopro
3,1%
Integrilline
7,8%
Ticlopidine
0,3% agrrenox
3,6%
Frost & Sullivan 2006
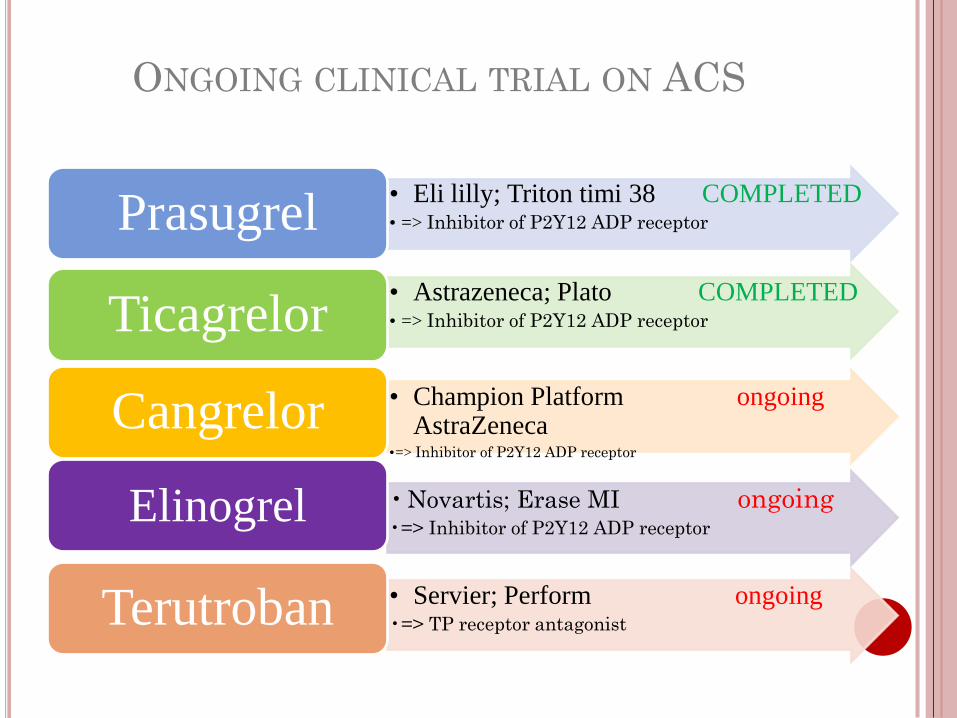
ONGOING CLINICAL TRIAL ON ACS
• Eli lilly; Triton timi 38 COMPLETED• => Inhibitor of P2Y12 ADP receptorPrasugrel
• Astrazeneca; Plato COMPLETED• => Inhibitor of P2Y12 ADP receptorTicagrelor
• Champion Platform ongoingAstraZeneca
•=> Inhibitor of P2Y12 ADP receptor
Cangrelor
• Novartis; Erase MI ongoing•=> Inhibitor of P2Y12 ADP receptor
Elinogrel
• Servier; Perform ongoing•=> TP receptor antagonistTerutroban
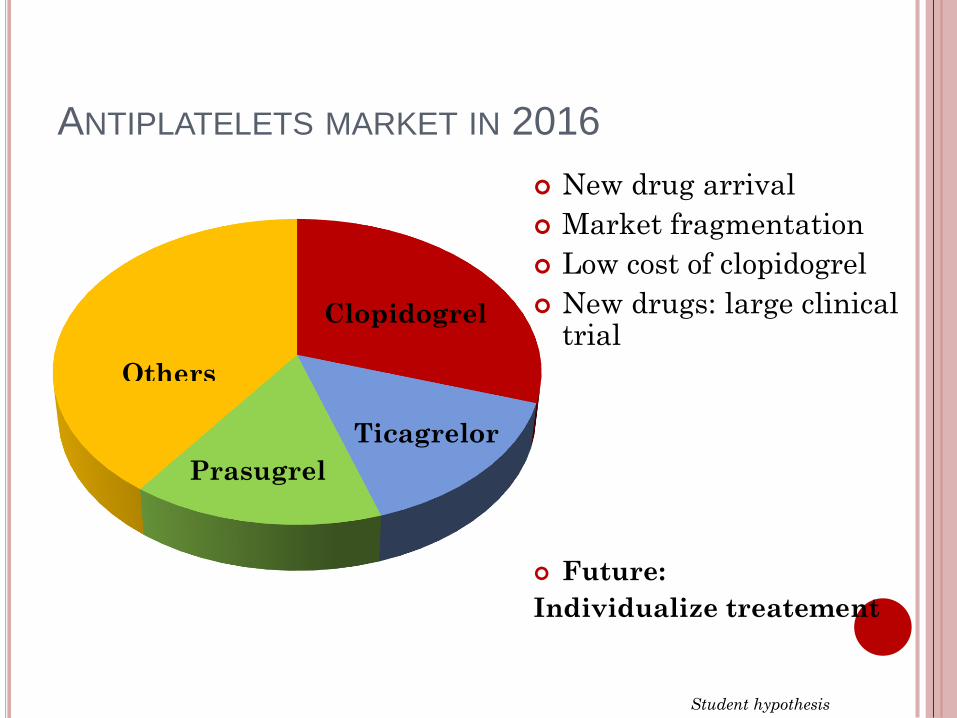
ANTIPLATELETS MARKET IN 2016
Ticagrelor
Others
Clopidogrel
New drug arrival
Market fragmentation
Low cost of clopidogrel
New drugs: large clinicaltrial
Future:
Individualize treatement
Prasugrel
Student hypothesis
DISCUSSION
Global market
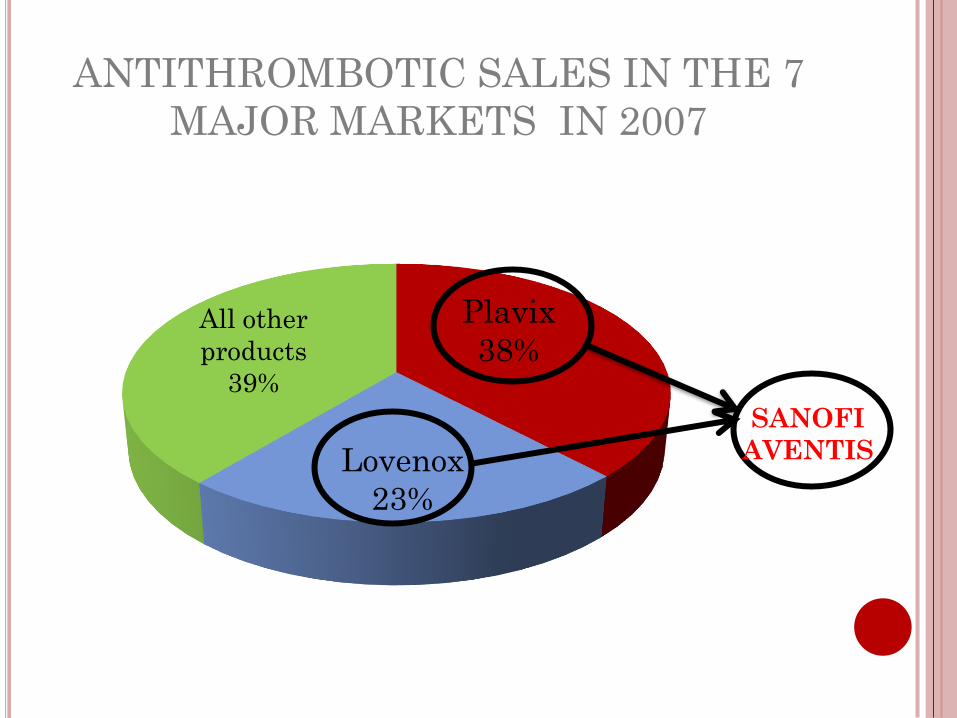
ANTITHROMBOTIC SALES IN THE 7
MAJOR MARKETS IN 2007
Plavix
38%
Lovenox
23%
All other
products
39%
SANOFI
AVENTIS
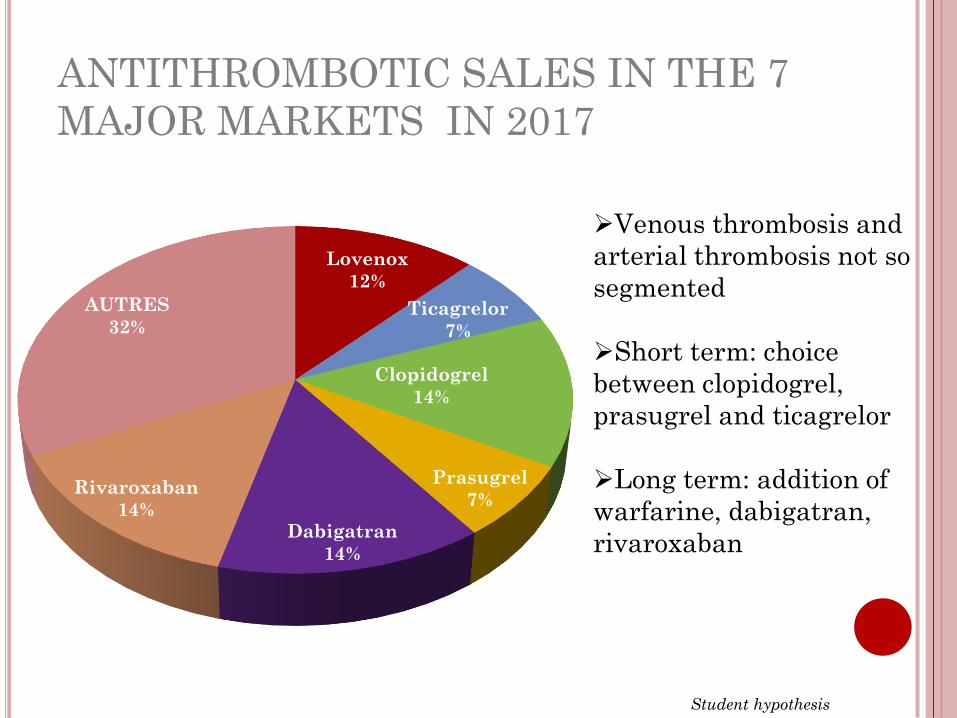
ANTITHROMBOTIC SALES IN THE 7
MAJOR MARKETS IN 2017
Lovenox
12%
Ticagrelor
7%
Clopidogrel
14%
Prasugrel
7%
Dabigatran
14%
Rivaroxaban
14%
AUTRES
32%
Student hypothesis
Venous thrombosis and
arterial thrombosis not so
segmented
Short term: choice
between clopidogrel,
prasugrel and ticagrelor
Long term: addition of
warfarine, dabigatran,
rivaroxaban
THANK YOU FOR YOUR ATTENTION
IS THERE ANY QUESTION?