Embed Size (px)
Citation preview

Dr Aziz ZAANAN Hôpital Européen Georges Pompidou
Université Paris Descartes
Cancer du rectum avec métastases synchrones

Cancer du rectum métastatique
• Situation clinique complexe
• Traitement tumeur rectale : symptômes/complications
• Traitement des métastases : conditionne le pronostic
• Fonction :
- tumeur primitive : Haut vs Moyen-Bas rectum Marge résection circonférentielle
- métastases : résécables ou non

Cancer du rectum métasta.que Faut-il privilégier:
Le traitement loco-régional?
Le traitement systémique?
Risque de progression des lésions secondaires
hépatiques, pulmonaires...
Risque de progression de la tumeur primitive
douleurs++, troubles neurologiques...

1ière situation: Cancer du rectum et
métastases résécables

Deux ques(ons : • Comment traiter ? -‐ le cancer rectal ? -‐ les métastases ?
• Quand réséquer ? -‐ Chirurgie en un ou deux temps ? -‐ Avant ou après CT ?
Métastases résécables
à Stratégie à discuter en RCP

Traitement du bas et moyen rectum
MRC : marge de résection circonférentielle TME : exérèse complète du mésorectum RCT : radio-chimiothérapie avec 5FU ou capécitabine RT : radiothérapie
Chirurgie avec TME
Evaluation du stade pré-opératoire : Toucher rectal, IRM, TDM, +/- Echoendoscopie
T1-2N0 T3N0 et MRC > 1 mm T4N0 - TxN+ T3N0 et MRC < 1 mm
RCT (5FU ou capécitabine) Options: RT 25 Gy ou chirurgie d’emblée
RCT (5FU ou capécitabine)
TNCD

Traitement des métastases résécables
FOLFOX péri-opératoire
Articles
1212 www.thelancet.com/oncology Vol 14 November 2013
stent. One patient in the perioperative chemotherapy group died suddenly (intercurrent death from unknown origin) while on protocol treatment before planned surgery, and the investigator reported the serious adverse event as possibly related to protocol treatment. In the surgery-only group, of the three patients who died from further cancer treatments, one died from septic shock while receiving FOLFIRI (folinic acid, fl uorouracil, and irinotecan) after progression, one died from port-catheter-related sepsis after starting second-line chemotherapy for progression, and one died from complications of further surgery for progression. Causes of deaths were reviewed by the study coordinator to assess their possible relation to protocol treatment and further cancer treatments.
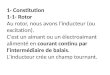
Overall survival in all randomly assigned patients did not diff er signifi cantly between groups (HR 0·88, 95% CI 0·68–1·14; p=0·34) nor did overall survival in eligible patients (HR 0·87, 95% CI 0·66–1·14; p=0·30; table 3). Kaplan-Meier curves for overall survival in all randomly assigned patients and all eligible patients are shown in fi gure 2. In all randomised patients, median overall survival was 61·3 months (95% CI 51·0–83·4) in the perioperative chemotherapy group and 54·3 months (41·9–79·4) in the surgery-only group. In the eligible population median overall survival was 63·7 months (52·7–87·3) and 55·0 months (41·9–79·4) in the perioperative chemotherapy and surgery-only groups, respectively. In all randomised patients, the absolute diff erence between groups in the proportion of patients with 5-year overall survival was 3·4% (95% CI –7·1 to 13·8); in all eligible patients it was 4·1% (–6·6 to 14·8).
The results of sensitivity analyses for overall survival are presented in the appendix. Updated results on PFS are displayed in table 4 and fi gure 3.
Of patients who had cancer progression (130 [71%] in the surgery-only group vs 124 [68%] in the perioperative chemotherapy group), 100 (77%) in the surgery-only group received chemotherapy as part of fi rst treatment for progression compared with 73 (59%) patients in the
Patients(N)
Deaths(n [%])
HR (95% CI) Median overall survival (months [95% CI])
Estimated 5 year overall survival (% [95% CI])
p value (log-rank)*
Primary analysis in randomly assigned patients 0·34
Perioperative chemotherapy 182 107 (59%) 0·88 (0·68–1·14) 61·3 (51·0–83·4) 51·2% (43·6–58·3)
Surgery only 182 114 (63%) 1·00 54·3 (41·9–79·4) 47·8% (40·3–55·0)
Sensitivity analyses
Eligible patients 0·30
Perioperative chemotherapy 171 101 (59%) 0·87 (0·66–1·14) 63·7 (52·7–87·3) 52·4% (44·6–59·7)
Surgery only 171 109 (64%) 1·00 55·0 (41·9–79·4) 48.3% (40·6–55·6)
Resected patients 0·35
Perioperative chemotherapy 152 84 (55%) 0·87 (0·64–1·17) 77·5 (59·4–94·6) 57·3% (49·0–64·8)
Surgery only 152 90 (59%) 1·00 73·3 (53·7–95·5) 54·4% (46·1–62·0)
HR=hazard ratio. *p value comparing overall survival between groups over the whole period of the study.
Table 3: Overall survival
Number at riskSurgery only
Perioperative chemotherapy
0 1 2 3 4 5 6 7 8
182182
167165
138145
116120
94107
7988
7272
5866
Overall log-rank test: p=0·340
10
20
30
50
70
90
100
40
60
80
Over
all s
urvi
val (
%)
A All randomly assigned patients
Number at riskSurgery only
Perioperative chemotherapy
0 1 2 3 4 5 6 7 8
171171
159158
133139
111114
91103
7686
6970
5664
Years since randomisation
Overall log-rank test: p=0·3030
10
20
30
50
70
90
100
40
60
80
Over
all s
urvi
val (
%)
B All eligible patients
Surgery onlyPerioperative chemotherapy
Figure 2: Overall survivalKaplan-Meier curves of overall survival in all randomly assigned patients (A) and all eligible patients (B) per treatment group.
Articles
www.thelancet.com/oncology Vol 14 November 2013 1213
perioperative chemotherapy group (p=0·0029), 52 (40%) in the surgery-only group versus 57 (46%) in the perioperative group had repeat surgery, three (2%) versus 11 (9%) had radiotherapy, and eight (6%) versus 14 (11%) received symptomatic treatment (appendix). Only data for fi rst therapy for progression can be reported because data for further successive treatments were not obtained systematically.
The results of the competing-risk analysis and the analysis of cancer-specifi c survival showed a trend towards an increased diff erence in favour of the perioperative chemotherapy group, especially with respect to the long-term results, but this diff erence was not statistically signifi cant (appendix).
DiscussionOur long-term overall survival analysis showed that there was no signifi cant diff erence in overall survival between perioperative chemotherapy and surgery alone; however, median overall survival was longer in the perioperative group, and a greater proportion of patients were alive at 5 years than in the surgery alone group (panel).
The failure to show a signifi cant diff erence in overall survival might be explained by several reasons. First, this trial was designed to detect a PFS benefi t and was not powered for overall survival, which was a secondary endpoint. The 4·1% absolute survival benefi t at 5 years in the eligible population is similar to other positive adjuvant trials in primary colorectal cancer. The MOSAIC trial15 reported a 4·2% overall survival benefi t at 6 years of follow-up. Of patients with stage III colon cancer (672 patients in the FOLFOX4 group and 675 in the LV5FU2 [bolus plus continuous-infusion fl uorouracil plus folinic acid] group), the probabilities of surviving at 6 years were 72·9% in the FOLFOX4 group and 68·7% in the LV5FU2 group (HR 0·80, 95% CI 0·65–0·97; p=0·023). Because a relatively large sample size was used (1347 patients with stage III cancer), generating signifi cant results, these fi ndings led to the establishment of oxaliplatin as standard of care for adjuvant treatment of stage III colon cancer. The National Surgical Adjuvant Breast and Bowel Project (NSABP) C-07 trial16 (FULV [fl uorouracil plus
folinic acid] vs FLOX [FULV plus oxaliplatin]) and a multicentre colorectal cancer trial17 comparing XELOX (capecitabine plus oxaliplatin) with bolus fl uorouracil plus folinic acid as adjuvant therapy showed signifi cant
Patients (N)
Patients with progression events (n [%])
HR (95% CI) Median PFS (months [95% CI])
Estimated 3 year PFS (% [95% CI])
p value (log-rank)
Randomly assigned patients 0·068
Perioperative chemotherapy 182 136 (75%) 0·81 (0·64–1·02) 20·0 (15·9–27·6) 38·2% (31·1–45·2)
Surgery only 182 139 (76%) 1·00 12·5 (9·7–17·7) 30·3% (23·7–37·1)
Eligible patients 0·035
Perioperative chemotherapy 171 129 (75%) 0·78 (0·61–0·99) 20·9 (17·1–28·9) 39·0% (31·7–46·3)
Surgery only 171 134 (78%) 1·00 12·5 (9·7–18·2) 29·9% (23·2–36·9)
PFS was measured according to the protocol defi nition of the primary endpoint. HR=hazard ratio. PFS=progression-free survival.
Table 4: Progression-free survival (long-term update)
Number at riskSurgery only
Perioperative chemotherapy
0 1 2 3 4 5 6 7 8
182182
89123
6681
5367
4556
4250
3542
3039
Overall log-rank test: p=0·0680
10
20
30
50
70
90
100
40
60
80
Prog
ress
ion-
free s
urvi
val (
%)
A All randomly assigned patients
Number at riskSurgery only
Perioperative chemotherapy
0 1 2 3 4 5 6 7 8
171171
85120
6379
5065
4254
3948
3240
2837
Years since randomisation
Overall log-rank test: p=0·0350
10
20
30
50
70
90
100
40
60
80
Prog
ress
ion-
free s
urvi
val (
%)
B All eligible patients
Surgery onlyPerioperative chemotherapy
Figure 3: Progression-free survival (long-term update)Kaplan-Meier curves of progression-free survival in all randomly assigned patients (A) and all eligible patients (B) per treatment group.
Nordlinger B et al, Lancet 2008 Nordlinger B et al, Lancet Oncol 2013
Survie globale Survie sans progression

Stratégie thérapeutique
Référence ?
pas de standard validé
TNCD

Options thérapeutiques
• RCT suivie d’une proctectomie + hépatectomie • En 1 ou 2 temps (si 2 temps, préférer le reverse) • Intérêt d’une RCT avec oxali ?
• RT courte (5x5) puis chimio péri-opératoire avec chirurgie du primitif et des métastases en 1 temps
• Chimio péri-opératoire des méta hépatiques suivie du traitement du rectum
Stratégie doit toujours être discuté en RCP
TNCD

2ième situation: Cancer du rectum et
métastases non résécables

Situation n°1: Tumeur primitive Symptomatique
• Quel traitement de 1ère intention pour traiter les symptômes ?
• Chirurgie • Chimiothérapie • Radio-chimiothérapie • Autres (endoscopique, …)
Toutes les options peuvent se discuter Il n’y a pas d’essai randomisé qui comparent ces options

Chirurgie 1ère
• Avantage : - contrôle des symptômes rectaux > 95%
• Inconvénients : - risque de résection R1-R2 - morbidité : 4-33% fistule anastomotique : facteur de mauvais pronostic - mortalité : 0-11% - retarde le contrôle des métastases
Chu QD et al, J Surg Oncol 2002 ; Nash GM et al, Ann Surg Oncol 2002 ; Benoist S et al, Br J Cancer 2005 ; Scheer MGW et al, Ann Oncol 2008 ; Tougeron D et al, GCB 2009 ; Declety G et al, ESMO 2009 ; Cellini C et al, World J Surg 2010 ; Smith JD et al, Ann Surg Oncol 2013

Radiochimiothérapie 1ère
• Avantage : - contrôle des symptômes rectaux 70-95%
• Inconvénients : - dose intensité de la chimiothérapie non optimale pour le contrôle des métastases
Tougeron D et al, Gastroenterol Clin Biol 2009 ; Crane CH et al, Int J Radiation Oncology Biol Phys 2001

Chimiothérapie 1ère
• Avantage : - efficacité immédiate sur métastases et tumeur rectale - adaptation de la stratégie en fonction de l’évolution : RT (5x5) ou RCT résection secondaire (primitif +/- méta)
• Inconvénients :
- Pas de comparaison avec la radiothérapie sur le contrôle des symptômes
Scoggins CR et al, Ann Surg Oncol 1999 ; Tebbut NC et al, GUT 2003 ; Michel P et al, GCB 2004 ; Benoist S et al, Br J Cancer 2005 ; Tougeron D et al, GCB 2009 ; Declety G et al, ESMO 2009 ; Poultsides GA et al, JCO 2009

En l’absence de complications relevant d’une chirurgie ou d’un traitement endoscopique en urgence, la radio-chimiothérapie représente l’option la plus appropriée si pas de menace des lésions secondaires.
RPC Gastroentérol Clin Biol 2005
Recommandations HAS-INCa 2011
Situation n°1: Tumeur primitive Symptomatique

La chimiothérapie première représente l’option la plus appropriée: - elle permet de traiter sans délai la maladie métastatique, … traitement adapté à la réponse (traitement local ou 2ème ligne)
RPC Gastroentérol Clin Biol 2005
Recommandations HAS-INCa 2011
Situation n°2: Tumeur primitive Asymptomatique
• Quel traitement de 1ère intention ?

Essai FFCD 1102 : FOLFIRINOX dans le K du rectum métasta(que non résécable
• Le cancer du rectum métasta.que est un vrai challenge thérapeu.que
avec un besoin de contrôle des métastases + tumeur primi.ve • Etude de phase II, FFCD, mul.centrique • Valida.on du concept d’une chimiothérapie de L1 agressive
Bachet JB. et al., ASCO 2016, P 3513
l FOLFIRINOX regimen : – oxalipla.n 85 mg/m2 d1 + – irinotecan 180 mg/m2 d1 + – leucovorin 400 mg/m2 d1 followed by – 5FU 400 mg/m2 bolus d1 and – 5FU 2,400 mg/m2 46h con.nuous infusion biweekly
Therapeu.c strategy according to inves.ga.ons’ choice
FOLFIRINOX (4 cycles) FOLFIRINOX (4 cycles)
CT scan rectal MRI
Inclusion
CT scan rectal MRI
CT scan rectal MRI

Bachet JB. et al., ASCO 2016, P 3513
Réponse Objec(ve Revue centralisée après 4 cycles
Réponse Objec(ve Revue centralisée après 8 cycles
61 pa(ents : -‐ Réponse par(elle n = 30 (46,9%) -‐ Stabilité n = 29 (45,3%)* -‐ Maladie progressive n = 2 (3.1%) -‐ Non evaluable n = 3 (4.7%)
64 pa(ents : -‐ Réponse par(elle n = 55 (86%) -‐ Stabilité n = 5 (7.8%) -‐ Maladie progressive n = 4 (6.2%)* -‐ Non evaluable n = 0 (0%)
-‐100,0
-‐80,0
-‐60,0
-‐40,0
-‐20,0
0,0
20,0
40,0
Pa(ents
Essai FFCD 1102 : FOLFIRINOX dans le K du rectum métasta(que non résécable

Evalua(on après 8 cycles Evalua(on après 4 cycles 20
0
-‐20
-‐40
-‐60
-‐80
-‐100
N=47
Bachet JB. et al., ASCO 2016, P 3513
• PFS : 10.9 [8.8-‐12.3] • Bon contrôle des symptômes
liés à la tumeur primi.ve
l Evalua(on de la réponse de la tumeur primi(ve : Volume-‐IRM
N=48 20
0
-‐20
-‐40
-‐60
-‐80
-‐100
Essai FFCD 1102 : FOLFIRINOX dans le K du rectum métasta(que non résécable

Cas clinique 1 Monsieur R, 62 ans
• HTA modérée
• Rectorragies et ténesme
• Coloscopie et biopsies : adénocarcinome circonférentiel de 8 à 12 cm de la marge anale
• IRM : tumeur rectum T3N+
• TDM TAP : présence de 3 métastases hépatiques dans les 2 lobes : – 2 dans le VI – 1 dans le III

Monsieur R, 62 ans
1. Que proposez-vous ?

Monsieur R, 62 ans
Traitements combinés et successifs choisis en RCP : perspective curative
• Les métastases hépatiques sont a priori
résécables Importance d’une chimiothérapie péri-opératoire
Traitement optimal pré-opératoire par RT/RCT
Tumeur du rectum localement évolué et symptomatique

Monsieur R, 62 ans
• Radio-chimiothérapie avec chimiothérapie efficace sur les métastases : FOLFOX + radiothérapie 45 Gy TDM à 2 mois : diminution de 30 à 50 % des métastases
Résection antérieure du rectum 4 semaines après la fin de la RCT et 2 semaines après arrêt de la chimiothérapie Reprise de la chimiothérapie 5 semaines après la résection
4 nouveaux cycles puis TDM: stable Résection hépatique du lobe gauche hépatique avec
segmentectomie du VI Reprise de la chimiothérapie jusqu’à 12 cycles au total

Cas clinique 2 Mr D…72 ans
• Antécédents : – Insuffisance coronarienne. Pontage en 2008. – HTA équilibrée et hypercholestérolémie
• Douleurs de l’hypochondre droit Echographie : grosses lésions en cocarde dans les 2 lobes doit du foie, petite ascite
• TDM : métastases hépatiques et pulmonaires • Biopsie sous échographie : adénocarcinome • Coloscopie et biopsies : adénocarcinome de 9
à 12 cm de la marge anale (RAS muté). • Bio: ACE=500 ; LDH: 10N; Bili: 1.1 N

Mr D…72 ans

1. Que proposez-vous ?
Mr D…72 ans

Mr D…72 ans
Les métastases hépatiques symptomatiques engagent à court terme le pronostic vital
Importance d’une chimiothérapie intensive
Radio-chimiothérapie ultérieure ?
L’indication d’un traitement local sera envisagée secondairement

• Chimiothérapie par FOLFIRINOX – Contrôle à 2 mois :
• Pas de douleurs ni d’ictère • Réponse 50 % métastases hépatiques, disparition de
l ’ascite • Disparition complète de la lésion rectale
– Contrôle à 4 mois : • Stable • Neuropathie
• 5FU entretien 4 mois Puis progression hépatique
• Chimiothérapie par FOLFIRI + bev 8 mois puis progression
• Reprise du FOLFOX
Mr D…72 ans
Cancer du rectum Métastases symptomatiques

Conclusion
• Pas d’attitude consensuelle dans la majorité des cas
(Pas d’étude contrôlée randomisée)
• Décision en fonction de la taille, la masse tumorale, les symptômes...
• Discussion multi-disciplinaire+++

• Options multiples : - 1 temps ou 2 temps (reverse) - résection primitif +/- précédée de RT 5x5 ou RCT - chimiothérapie péri-op, d’intervalle ou adjuvante
Métastases résécables

Métastases non résécables
Lésion primitive Symptomatique
Radio-chimiothérapie chimiothérapie systémique
Primitif peu ou non symptomatique
Chimiothérapie systémique

Merci de votre attention