Embed Size (px)
Citation preview

71
COLUNA/COLUMNA. 2008;7(1):71-75
Chordomas of cervical spine: surgical managementstrategies and outcome
Cordomas da coluna cervical: método cirúrgico e resultados
Cordomas de la columna cervical: estrategiasde manejo quirúrgico y resultados
ARTIGO ORIGINAL / ORIGINAL ARTICLE
Amit Kohli1
Ram Chaddha1
Sharookh P. Vatchha1
ABSTRACTObjectives: chordomas of cervical spineare rare tumors but are the primarymalignant tumors of the spine. AsChordomas has poor sensitivity toradiotherapy and chemotherapy itrequires surgical resection. The purposeof this study was to determine the suitablemethods for removal of the tumorscompletely and outcome over time inpatients undergoing complete en blocexcision. Methods: a retrospective studyof twelve patients from October 2003 toAugust 2007 between the ages of 45-75years who presented with gradual onsetof neck pain and upper extremityweakness. All patients were clinicallyevaluated and preoperatively underwentDigital X-Rays, CT scans and contrastenhanced MR imaging. All patientsunderwent tumors resection and spinalinstrumentation. All cases were followedup clinically and radiographically fordetermination of their status. Results:eleven patients were available for follow-up. All patients underwent an anterior
RESUMOObjetivos: os tumores da coluna cervicalsão raros, mas são tumores malignos pri-mários da coluna. Como os cordomasapresentam baixa sensibilidade à radio-terapia e à quimioterapia requerem ci-rurgia para sua ressecção. O objetivodeste estudo é determinar os métodosadequados para a remoção total dostumores e conhecer os resultados parao paciente no período posterior à suaretirada. Métodos: foi realizado umestudo retrospectivo de 20 pacientes,de Outubro de 2003 a Agosto de 2007,com idade entre 45 e 75 anos, os quaisapresentavam uma gradual dor nopescoço e uma importante fraqueza nasextremidades superiores. Todos ospacientes foram avaliados clinicamentee no período pré-operatório por meiode radiografia digital, tomografiacomputadorizada e por imagem deressonância magnética com contraste.Todos os pacientes foram submetidosà ressecção dos tumores e instrumen-tação da coluna vertebral. Todos os
RESUMENObjetivos: los tumores de la columnacervical son raros, siendo tumoresprimarios malignos de la columna.Como los cordomas presentan bajasensibilidad a la radioterapia y a laquimioterapia requieren cirugía para suresección. El objetivo de este estudioes determinar los métodos adecuadospara la remoción total del tumores yconocer los resultados de los pacientesen el período posterior a su retirada.Métodos: fue realizado un estudioretrospectivo de 20 pacientes, deOctubre de 2003 a Agosto de 2007, conedad entre 45 y 75 años, que presentaronun dolor gradual en el cuello y unadebilidad importante en las extremidadessuperiores. Todos los pacientes fueronevaluados clínicamente y en el preope-ratorio fue realizada radiografía digital,tomografía computarizada y resonanciamagnética de contraste. Todos los pa-cientes fueron sometidos a la reseccióndel tumores y a la instrumentación dela columna vertebral. Todos los casos
Study carried out at Lilavati Hospital and Research Centre, Bandra (west), Mumbai, India.
1Orthopaedics from the Department of Orthopedics Lilavati Hospital and Research Centre, Bandra (west), Mumbai, India.
Recebido: 20/01/2008 Aprovado: 20/02/2008
48_col_7_1.pmd 14/3/2008, 18:0471

COLUNA/COLUMNA. 2008;7(1):71-75
72 Kohli A, Chaddha R, Vatchha SP
stabilization procedure combined withinterbody fusion (seven with iliac crestand five with Interbody cages) whereasone required an occipitocervical fusion.At the time of this submission, there weretwo signs of recurrence. Discussion: theuncontrolled growth of chordoma iscommonly the cause of death. En blocexcision of the lesion, sometimescombined with radiation therapy as anadjuvant, obtained the best results.Conclusion: chordoma occur in mostcases directly from the vertebral body. Enbloc excision of these tumors even ifmarginal seems to be the most effectivetreatment combined with megavoltageradiation which can be administered as anadjuvant.
KEYWORDS: Chordoma/surgery;Orthopedic procedures/methods; Spinal neoplasms/surgery
casos foram acompanhados clínica eradiograficamente para determinar suaevolução. Resultados: 11 pacientes es-tavam disponíveis para o acompanha-mento. Todos os pacientes submeteram-se ao procedimento de estabilização an-terior da coluna com fusão inters-somática, sete deles com enxerto do ossoilíaco, cinco com “cages” interssomá-ticos, enquanto que um pacientenecessitou de fusão occipto-cervical.No grupo de pacientes estudadosobservaram-se duas recidivas dotumores. Conclusão: a falta de controledo crescimento do cordoma da colunacervical é uma comum causa de óbito.A conduta de retirada do bloco de lesão,às vezes combinada com a radiação e aterapia obtém bons resultados. O cor-doma ocorre em muitos casos direta-mente no corpo vertebral. A remoçãodo bloco dos tumores parece ser o maisefetivo tratamento combinado comirradiação de megavoltagem que éadministrada como coadjuvante aotratamento cirúrgico.
DESCRITORES: Cordomas/cirurgia;Procedimentos ortopédicos/métodos; Neoplasias dacoluna vertebral/cirurgia
fueron acompañados clínica y radiográ-ficamente para determinar su evolución.Resultados: 11 pacientes estaban dis-ponibles para acompañamiento. Todoslos pacientes se sometieron al procedi-miento de estabilización anterior de lacolumna con fusión intersomática, sietede ellos con injerto de hueso iliaco, cincocon “cages” intersomáticos, mientrasque un paciente necesitó de fusiónoccípito-cervical. En el grupo de pa-cientes estudiados se observaron dosrecidivas de tumores. Conclusión: lafalta de control de crecimiento de lacordoma de la columna cervical es unacausa común de óbito. La conducta deretirada del bloque de la lesión, algunasveces combinada con la radiación y laterapia ocasiona buenos resultados. Lacordoma ocurre en muchos casosdirectamente en el cuerpo vertebral. Laremoción del bloque del tumor pareceser el tratamiento más efectivo combi-nado con la irradiación de megavoltageque es administrada como coadyuvanteal tratamiento quirúrgico.
DESCRIPTOREs: Cordoma/cirurgía;Procedimientos Ortopédicos/métodos; Neoplasias de lacolumna vertebral/cirurgía
INTRODUCTIONChordoma is a low grade malignant tumors accounting forabout 1% to 4% of all malignant bone tumors. It originatesfrom the remnants of the notochord. It is predominantlyfound in the clivus (50%), followed by the sacral spine (15%).Only rarely is this tumors seen in cervical spine accountingfor 6% of all chordoma1. Cervical spine Chordomas presentsignificant surgical challenges because of the importantanatomical structures present in this area. The tumors growsslowly by infiltrating cancellous bone, is seen typically inadults and the elderly. At the time of initial presentation, thecervical chordoma usually shows infiltration into theparavertebral and epidural compartments. It has a markedtendency toward recurrence following intralesional excisionor biopsy. Metastasis is usually seen in the brain, skin, lungs,bone or internal organs. Rate of metastasis varies from 0%to 5%2. Survival seems to be more affected by the localspread rather than by metastasis. Magnetic resonanceimaging and computed tomography have made thediagnosis of the size of the tumors faster and easier1, they
also play an important role in improving the prognosis ofchordoma by discovering small tumors, which can besubmitted to en bloc resection4-5.
In this study we present twelve cases with isolatedcervical spine Chordomas. All patients at the time ofpresentation had evidence of tumors extension. In this studywe determine the suitable methods for removal of the tumorscompletely and outcome over time in patients undergoingcomplete en bloc excision.
METHODSWe retrospectively analyzed twelve patients with cervicalchordoma from October 2003 to August 2007 at the LilavatiHospital and Research Centre, Mumbai. All data wasobtained from hospital records, including preoperative andsequential postoperative clinical findings, radiologicaldetails and pictures and details of the status of the patienttill the last follow-up. Neurological deficit was assessed byFrankel grading.
48_col_7_1.pmd 14/3/2008, 18:0472

73
COLUNA/COLUMNA. 2008;7(1):71-75
Out of the twelve patients studied eight were males andfour were females. Mean age at diagnosis was 60 years.Follow-up duration ranged from 12 to 36 months. The slowand gradual onset of pain was the most consistentcomplaint; all patients presented with neck pain and upperextremity symptoms. Upper extremity symptoms ranged fromhand tingling and numbness to overt weakness. One patientpresented with difficulty in swallowing.
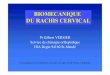
All patients preoperatively underwent standard X-rays,CT scans to assess the degree of bone destruction andcervical spine instability and contrast enhanced MRI toevaluate bone and soft tissue involvement, and nuclear bonescan to check for metastasis, we used MR angiography toevaluate the patency of vertebral artery in addition to acomplete preoperative workup (Figure 1-2).
Based on the preoperative images we staged all tumors byusing the oncological staging system devised by Enneking etal. and the extent of the lesion was described according to theWeinstein- Borian- Biagini (WBB) system. According to theEnneking staging system, the lesions were classified as 1A (4cases) and 1B (8 cases)3. The tumors arose mostly central inthe body and invaded the whole vertebrae. Chordomas appearlate on standard X-Rays, the radiographic pattern is mostlyradiolucent with scanty ossifications and huge masses in thesurrounding soft tissues. The discs were spared. MRI and CTscan proved useful in detecting lesions which were not seenon radiographs, the MRI signal is hypo dense in T1 weightedand hyper intense in T2 weighted images. In six cases completevertebral collapse occurred. We planned our surgical approachbased on a variety of factors including tumors location, extent,area of cord compression and degree of instability. In all of thetwelve surgical interventions, two were done by combinedanterior and posterior approach; these had pure anterior, middleand posterior column involvement. Ten were done by anteriorapproach; these had anterior and middle column involvement.
The treatment performed on twelve cases included› En bloc resections in four cases, the margins were
contaminated at some point and for this reason radiationtherapy was performed as an adjuvant in these cases.
› En bloc resection of the vertebral body (vertebrectomy)could be performed in five cases (Figure 3).
› Intralesional extra capsular excision with adjuvantradiation therapy was performed in three cases.
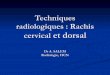
Specimens obtained during resection were sent forhistopatholgical analysis in all cases (Figure 4). Spinalinstrumentation was performed when surgery causedinstability or for reconstruction of spine after tumors removal.All patients in this series underwent spinal stabilization.Combined anterior and posterior reconstruction was performedin two cases; the vertebral body was replaced by autogenousiliac bone graft in seven cases and by interbody cages in fivecases along with anterior plating (Figure 5).
Post-operative care included immobilization of the operatedspine with a SOMI brace or a hard cervical collar (Philadelphia)for three months post surgery. The duration of hospital stayfollowing surgery ranged from five to 14 days. A contrast
enhanced MR imaging study was obtained at 6 weeks in allpatients to evaluate the status of the tumors. Follow-up evaluationwas on outpatient basis at 6 weeks post tumors excision alongwith a fresh digital X-ray, further follow-ups were at 3, 6, 9 and 12months along with fresh X-Rays for assessment of spinalalignment and integrity of the instrumentation and to check forfusion. Successful fusion required the presence of bridgingtrabeculae across the fused levels. A contrast
enhanced MR imaging study was obtained in all patientsat 3, 6 and 12 months post excision to check for early tumorsrecurrence. Once fusion was established, the patients wereweaned off the brace to a soft cervical collar.
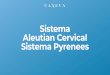
Figure 2Patient underwent C6body excision +decompression withinterbody iliac crestbone graft andstabilization
Figure 158 years lady: MRI saggital (A) and axial (B) cuts showing C6chordoma with cord compression
Figure 3Microscopic picture of same
patient showing largepolyhedral cells with
eccentric nuclei and largemucoid foci with a chondroid
appearance
Figure 5Patient underwent C2 excision with a two
stage antero-posterior occipito-cervical fusion
Figure 460 year old lady withchordoma of C2 vertebrae
Chordomas of cervical spine: surgical management strategies and outcome
A
B
48_col_7_1.pmd 14/3/2008, 18:0473

COLUNA/COLUMNA. 2008;7(1):71-75
74
RESULTSAll patients were analyzed using the Frankel grading.The evolution of the chordomas is known for elevenpatients. All patients were submitted to clinical andimaging studies during their follow-ups to determine therelationship between treatment and outcome. In allpatients in this study the tumors were resected using astandard anterior cervical approach for anterior andmiddle column tumours and posterior approach forinvolvement of posterior elements. Of the eleven patientsavailable at follow-up their were two cases of localrecurrence. The mean follow-up duration has been 24months in this study. Three patients were treated byintralesional extra capsular excision with adjuvantradiation therapy, at one year there was one case of localrecurrence which required chemotherapy, this patient isbeing treated and one patient of this group was lost tofollow-up. En bloc excision was performed in five cases,there was no recurrence at 48 months in this group ofpatients. Of the four patients who underwent En blocresections with contaminated margins and adjuvantradiation therapy there was one patient (25%) with localrecurrence at 24 months follow-up which requiredexcision along with radiation therapy.
Chordomas are a frequent cause of cord compressionbecause of the slow growth which expands toward theepidural space compressing the dura. In all cases asignificant improvement in the neurological symptomsarose following decompression and excision of thetumors. Seven patients received postoperative radiationtherapy of these two patients with local recurrence alsounderwent chemotherapy.
DISCUSSIONDuring the period of this study (2003 to 2007), twelvechordomas of the cervical spine were treated at Lilavatihospital. Chordomas of cervical spine always arise withinthe vertebral body, they constitute 1 to 4% of malignantbone tumors6. After plasmacytomas they are the mostfrequent primary malignant tumors in the spine, thecervical region constitutes 6 to 7% of cases. Chordomasare locally aggressive and have a tendency to recur.Metastases are noted in approximately 30% of cases7-8.As it is slow growing tumors it is detected late and oftenoccupies most of the vertebrae at the t ime ofpresentation, chordomas are often destructive. Latediagnosis makes it difficult to provide appropriatetreatment. According to the oncological stagingproposed by Enneking, chordomas are classified asstage 1A/1B lesions3. Aggressive resection is thetreatment of choice.
The main problem in the treatment of chordoma islocal recurrence. The uncontrolled growth of thesetumors is commonly the cause of death. The treatmentof chordomas in the cervical spine consists of radicalexcision and stabilization, followed by adjuvant
radiotherapy and chemotherapy9. Proton beam radiationis the modality that has been used extensively for thetreatment of chordomas10-11.
In this study five patients who underwent En blocexcisions of the tumors had no recurrence at 48 months.The results of this study thus confirms most of theconclusions of the literature and stresses the point thatEn bloc resection with tumors free margin seems to bethe procedure of choice to allow a disease free interval.It has been reported that the margin free, en bloc tumorsresection is the treatment of choice for Chordomas8,12.This requires the tumors be confined within the vertebralbody, as it is slow growing tumors it is detected lateand often occupies the epidural space after penetratingthe vertebral body at the time of presentation, removingsuch large tumors in the cervical spine in an en blocmanner when the lesion extends well beyond the spinewould be associated with significant morbidity. The maindisadvantage in resecting cervical spine chordomaresult from the involvement of the vertebral artery andthe duramater13. In this study we were able to achievetumors eradication in three such cases with intralesionalexcision and adjuvant radiation therapy, one out of threepatients from this group has had a disease free intervalafter a follow-up of 36 months, this being a reasonablemethod of choice when en bloc resection is not feasiblein tumors with intradural and soft tissue involvement.In 4 cases the margins were contaminated and in thesecases adjuvant radiation therapy was given obtaining adisease free interval for 36 months in three out of fourpatients.
CONCLUSIONChordomas in cervical spine are rare tumors. They arisedirectly from the vertebral body and tend to expandthe whole body. At presentation, the majority ofpatients had tumors beyond the vertebral body, thistumors spread beyond the vertebral body makes itdifficult to perform an en bloc resection of the body asthe margins would never be disease free, consideringthe risk benefit ratio as the surgical risk presumablyexceeds the benefit. In this study the patients withcervical chordoma presented with nonspecif icsymptoms of neck pain with radicular and myelopathicchanges. The result of this study indicates that enbloc resection of chordoma in some areas seems to bethe most effective treatment in local control of thisdisease in combinat ion with s tabi l izat ion andreconstruction of the spine. In cases when en blocexcis ion is not feasible that is in cases withinvolvement of vital neurological structures a completeexcision that is piecemeal removal of the tumors is aviable technique combined with megavoltage radiationtherapy or proton beam radiation.
Kohli A, Chaddha R, Vatchha SP
48_col_7_1.pmd 14/3/2008, 18:0474

75
COLUNA/COLUMNA. 2008;7(1):71-75
REFERÊNCIAS1. Nöel G, Feuvret L, Calugaru V,
Dhermain F, Mammar H, Haie-MéderC, et al. Chordomas of the base of theskull and upper cervical spine. Onehundred patients irradiated by a 3Dconformal technique combiningphoton and proton beams. ActaOncol. 2005; 44(7): 700-8.
2. Boriani S, Weinstein JN, Biagini R.Primary bone tumors of the spine.Terminology and surgical staging.Spine. 1997; 22(9): 1036-44.
3. Enneking WF, Spanier SS, GoodmanMA. A system for the surgical stagingof musculoskeletal sarcoma. ClinOrthop Relat Res. 1980; (153): 106- 20.
4. Bas T, Bas P, Prieto M, Ramos V, BasJL, Espinosa C. A lumbar chordomatreated with a wide resection. EurSpine J. 1994; 3(2): 115-7.
5. Boriani S, Chevalley F, Weinstein JN,Biagini R, Campanacci L, De Iure F,Piccill P. Chordoma of the spine abovethe sacrum. Treatment and outcome in21 cases. Spine. 1996; 21(13): 1569-77.
6. Catton C, O’Sullivan B, Bell R,Laperriere N, Cummings B, FornasierV, Wunder J. Chordoma: long-termfollow-up after radical photonirradiation. Radiother Oncol. 1996;41(1):67-72.
7. Cummings BJ, Hodson DI, Bush RS.Chordoma: the results of megavoltageradiation therapy. Int J Radiat OncoBiol Phys. 1983; 9(5): 633-42.
8. Bjornsson J, Wold LE, Ebersold MJ,Laws ER. Chordoma of the mobilespine. A clinicopathologic analysis of 40patients. Cancer. 1993; 71(3): 735-40.
9. Bilsky MH, Yamada Y, Yenice KM,Lovelock M, Hunt M, Gutin PH,Leibel SA. Intensity-modulatedstereotactic radiotherapy ofparaspinal tumors: a preliminaryreport. Neurosurgery. 2004; 58(4):823-30; discussion 830-1.
10. Mindell ER. Chordoma. J Bone JointSurg Am. 1981; 63(3): 501-5.
11. Suit HD, Goiten M, Munzenrider J,Verhey L, Davis KR, Koehler A, et al.Definitive radiation therapy forchordoma and chondrosarcoma of baseof skull and cervical spine. JNeurosurg. 1982; 56(3): 377-85.
12. Fujita T, Kawahara N, Matsumoto T,Tomita K. Chordoma in the cervicalspine managed with en bloc excision.Spine. 1999; 24(17): 1848-51.
13. Sen C, Eisenberg M, Casden AM,Sundaresan N, Catalano PJ.Management of the vertebral artery inexcision of extradural tumors of thecervical spine. Neurosurgery. 1995;36(1): 106-15; discussion 115-6.
Correspondence
Dr. Amit Kohli
802-Green Blaze CHSL,
Near IDBI Bank
Juhu-Versova link road,
Andheri (West), Mumbai-400053
INDIA
Tel.: + 91-9820504676
E-mail: [email protected]
Chordomas of cervical spine: surgical management strategies and outcome
48_col_7_1.pmd 14/3/2008, 18:0475