Embed Size (px)
Citation preview

International
Orthodontics
2009 ; 7 : 193-206
193
© 2009. CEO.Édité par / Published by Elsevier Masson SAS.
Tous droits réservés/All rights reserved
Article original
Original article
Comparaison de l’effet du paracétamol
et de l’ibuprofène sur la douleur orthodontique
Comparison of the effect of Paracetamol and Ibuprofène on orthodontic pain
Lahcen OUSEHAL
1
, Amina LAKHDAR
2
, Farid ELQUARS
3
Résumé
Les patients qui vont bénéficier d’un traitement orthodontique peu-vent éprouver une sensation douloureuse désagréable. Ceci a étéprouvé dans plusieurs études.Le contrôle de la douleur durant le traitement orthodontique est inté-ressant, que ce soit pour le praticien ou le patient.L’objectif de notre étude est de comparer l’effet de l’ibuprofène et duparacétamol sur la douleur orthodontique.Pour cela, un échantillon de 56 patients divisés en 2 groupes :
• le groupe A de 27 patients a reçu de l’ibuprofène (Nofène
®
) (2 cpde 300 mg/j pendant 5 j) ;• le groupe B de 29 patients a reçu du paracétamol (Doliprane
®
)(4 cp de 500 mg/j pendant 7 j).Le niveau de douleur est évalué en utilisant l’échelle visuelle analo-gique à 2 h, 6 h, 24 h, 2 j, 3 j et 7 j après insertion du 1
er
arc.Les résultats ont montré qu’il n’y a pas de différence significativeentre l’ibuprofène et le paracétamol en matière de lutte contre ladouleur orthodontique sauf durant les deux premières heures aprèsla pose de l’arc où on note une légère supériorité du paracétamol parrapport à l’ibuprofène. La comparaison en fonction de l’âge et dusexe a montré qu’il n’y a pas de différence significative.Nous pouvons ainsi conclure que le paracétamol et l’ibuprofène sontdes analgésiques de choix dans la lutte contre la douleur liée autraitement orthodontique.
Mots-clés
• Douleur.• Paracétamol.• Ibuprofène.• Orthodontie.
Summary
Patients undergoing orthodontic treatment can experience anunpleasant painful sensation. This has been proven by severalstudies. Controling pain during orthodontic treatment is in the interest ofboth practitioner and patient. The aim of this study was to compare the effect of ibuprofen andparacetamol on orthodontic pain. To this end, a sample of 56 patients was divided into two groups:
• group A comprising 27 patients received ibuprofen (Nofène
®
)(2 x 300mg tablets per day for 5 days);• group B comprising 29 patients received paracetamol (Dol-iprane
®
) (4 x 500mg tablets per day for 7 days). Pain levels were assessed using the visual analog scale at 2h,6h, 24h, day 2, day 3 and day 7 after insertion of the first arch-wire. Results show that there is no significant difference betweenibuprofen and paracetamol regarding control of orthodontic painexcept during the first two hours after archwire insertion whenparacetamol was observed to be slightly more effective than ibu-profen. Comparison by age and gender revealed no significantdifferences. Thus, we can conclude that paracetamol and ibuprofen are pain-killers of choice in the relief of orthodontically-related pain.
Key-words
•
Pain.
•
Paracetamol.
•
Ibuprofen.
•
Orthodontics.
1
Professeur agrégé, département d’orthodontie, faculté de médecine dentaire, Casablanca, Maroc.
2
Docteur en médecine dentaire, département d’orthodontie, faculté de médecine dentaire, Casablanca, Maroc.
3
Professeur de l’enseignement supérieur, département d’orthodontie, faculté de médecine dentaire, Casablanca, Maroc.
Correspondance et tirés à part/Correspondence and reprints:
L. OUSEHAL, département d’orthodontie, faculté de médecine dentaire, Casablanca, [email protected]

Lahcen OUSEHAL, Amina LAKHDAR, Farid ELQUARS
194
International
Orthodontics
2009 ; 7 : 193-206
L
a douleur est une impression anormale et pénible reçue parune partie vivante et perçue par le cerveau. Actuellement, on peutproposer plusieurs définitions de la douleur. Selon Louis et Michel-son, 1994 : « La douleur est une sensation désagréable qui résulte del’action de différents stimuli sur un tissu innervé ou sensoriel » [1].L’association internationale pour l’étude de la douleur (IASP)définit la douleur comme « une sensation désagréable et uneexpérience émotionnelle en réponse à une atteinte tissulaireréelle ou potentielle, ou décrite en ces termes ».La douleur et l’inconfort liés à la mise en bouche d’un appareilorthodontique sont des expériences communes pour les patientsen orthodontie. Il a été rapporté que la peur de la douleur est unfacteur non négligeable dans le découragement des patients endemande de traitement orthodontique [2].Patel [3] avait trouvé qu’une petite mais considérable proportiondes patients (8 %) cesse le traitement à cause de la douleur dansles premières étapes de la thérapie. Burstone [4] avait classifié laréponse douloureuse pendant le traitement orthodontique en 3 dif-férents degrés :• 1
er
degré : produit par une forte pression exercée sur la dentavec un instrument. Ceci est habituellement percu plus facile-ment par l’application de forces dirigées dans la même directionque celles de l’appareillage fixe. Le patient n’est pas conscient dece 1
er
degré de la douleur ; • 2
e
degré : caractérisé par la douleur ou l’inconfort pendant laconsolidation des dents, mais le patient garde la possibilité demastiquer une nourriture normale sans difficulté ; • 3
e
degré : présent lorsque le patient souffre de douleur sponta-née ou est dans l’impossibilité de mastiquer une nourriture deconsistance normale.
Objectif de l’étude
La présence de douleur orthodontique peut se répercuter sur la col-laboration du patient voire l’acceptation du traitement, d’où l’intérêtd’une médication. Une question se pose alors, quel médicament àeffet antalgique prescrire ? Du paracétamol ou un AINS (anti-inflammatoires non stéroïdiens) en l’occurrence l’ibuprofène ? C’estainsi que nous avons pris comme objectif de notre travail de :• comparer l’effet d’un AINS (dans notre étude l’ibuprofène) aveccelui du paracétamol sur la douleur orthodontique ;• choisir ainsi le médicament le plus efficace pour nos patients.
Matériel et méthode
Un échantillon de 56 patients – sélectionnés au hasard parmila population orthodontique du service d’orthodontie du cen-tre de consultation et de traitements dentaires du centre hos-pitalier Ibn Rochd à Casablanca – est divisé en deux groupes.1. Le groupe A est formé de 27 patients qui ont pris 600 mg d’ibupro-fène (Nofène
®
) en 2 doses : (2 cp de 300 mg) par jour pendant 5 jours.
2. Le groupe B est formé de 29 patients qui ont pris 2 g de paracétamol(Doliprane
®
) en 4 doses : (4 cp de 500 mg) par jour pendant 7 jours.
P
ain is an abnormal and unpleasant sensation registered by aliving part of the body and perceived by the brain. Currently, sev-eral definitions of pain are available. According to Louis and Mich-elson, 1994: “Pain is an unpleasant sensation resulting from theaction of various stimuli on an innervated or sensorial tissue” [1].The International Association for the Study of Pain (IASP) definespain as “an unpleasant sensation and an emotional experience inresponse to a tissue aggression which is real, potential ordescribed in those terms”. Pain and the discomfort linked to the oral placement of braces arecommon experiences for orthodontic patients. It has beenreported that fear of pain is a non-negligible factor in discouragingpatients seeking orthodontic treatment [2].
Patel [3] found that a small but considerable proportion of patients(8%) pull out of treatment on account of pain during the earlystages of treatment. Burstone [4] classified pain response duringorthodontic treatment in 3 separate degrees:
• 1
st
degree: caused by an instrument applying strong pressure onthe teeth. This is generally perceived more easily by the applica-tion of forces directed in the same direction as those of the fixedappliance. The patient is not aware of this first degree of pain;
• 2
nd
degree: characterized by pain or discomfort during consoli-dation of the teeth although the patient still has no problem chewingnormal food;• 3
rd
degree: the patient suffers spontaneous pain or is unable tochew normally consistent food.
Aim of the study
Orthodontic pain can have repercussions on patient collaborationand even their decision to accept treatment or not. Hence theneed for medication. A question now arises. Which antalgic drugshould be prescribed? paracetamol? Or a non-steroidal anti-inflammatory (NSAID), or ibuprofen, in effect? Thus, our studyhad the following aims: • to compare the impact on orthodontic pain of an NSAID (ibupro-fen in our study) with that of paracetamol;• to select the most appropriate drug for our patients.
Material and method
A sample of 56 patients selected at random among the orthodon-tic population at the orthodontic consultation and dental treatmentunit of the Ibn Rochd hospital center in Casablanca, Morocco,was divided into two groups. 1. Group A included 27 patients who received 600 mg of ibupro-fen (Nofène
®
) in two doses: 2tb x 300mg per day for 5 days. 2. Group B included 29 patients who received 2 g paracetamol(Doliprane
®
) in 4 doses: 4tb x 500mg per day for 7 days.

Comparaison de l’effet du paracétamol et de l’ibuprofène sur la douleur orthodontique
Comparison of the effect of Paracetamol and Ibuprofène on orthodontic pain
International
Orthodontics
2009 ; 7 : 193-206
195
Aucune sélection n’a été faite concernant le type de dysmorphoseni la technique utilisée.Il a été établi une fiche individuelle pour chaque patient surlaquelle figurent toutes les données utiles à l’étude, à savoir :l’identification, l’âge, le sexe, le médicament utilisé, le question-naire médical et l’échelle visuelle analogique (EVA).Notre étude consiste à évaluer l’effet du paracétamol et de l’ibu-profène sur la perception douloureuse après mise en place du1
er
arc. La première prise du médicament se fait immédiatementaprès l’acte opératoire, l’évaluation de douleur sur l’EVA se fait à2 h, 6 h, 24 h, 2 j, 3 j et à 7 j. L’EVA est une ligne graduée de 10 cm, sur laquelle le patient estcensé mettre une croix. L’extrémité gauche de cette ligne signifiel’absence de douleur alors que l’extrémité droite signifie la pré-sence d’une douleur atroce. Les mesures sont effectuées à l’aide d’une réglette millimé-trée de l’extrémité gauche à la marque. Ces mesures sontenregistrées sur des tableaux facilement utilisables et lisi-bles, avec l’utilisation d’un logiciel statistique (SPSS 11.5)permettant un calcul rapide et sans erreur des fréquences,pourcentages, moyennes arythmiques et écarts types.Le test « t » de Student a été utilisé pour comparer statistique-ment les différentes moyennes.
Résultats
Distribution de l’échantillon
• En fonction du sexe : l’échantillon comporte 39 patients desexe féminin soit 69,6 % et 17 patients de sexe masculin soit30,4 %.• En fonction de l’âge : l’échantillon est divisé en 2 tranchesd’âge, ceux qui ont un âge < 15 ans ne représentent que 21,4 %alors que ceux âgé de plus de 15 ans représente la majorité avecun pourcentage de 78,6 %.• En fonction du médicament : la distribution du paracétamol parrapport à l’ibuprofène est presque identique, soit 48,2 % pour leparacétamol et 51,8 % pour l’ibuprofène.
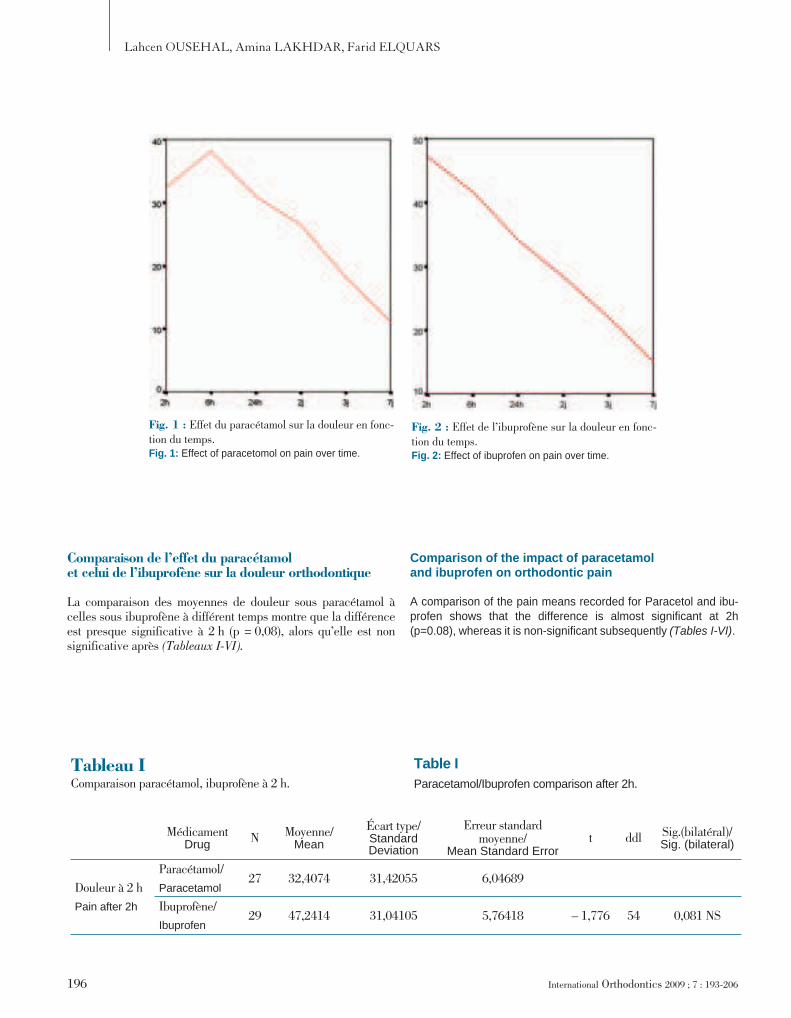
Effet du paracétamol sur la douleur en fonction du temps
L’étude de l’effet du paracétamol sur la douleur orthodon-tique montre qu’il y a une diminution de la perception dou-loureuse à partir du 2
e
jour avec un maximum de douleur 6 haprès la mise en place du 1
er
arc
(fig. 1)
. Cette diminution dedouleur est significative au 3
e
jour et hautement significativeau 7
e
jour.
Effet de l’ibuprofène sur la douleur en fonction du temps
L’ibuprofène diminue la perception douloureuse en fonction dutemps avec un maximum de douleur situé à 2 h, la différence demoyenne de douleur est significative à 6 h et hautement signifi-cative à 24 h, 2 j, 3 j et à 7 j
(fig. 2)
.
No selection was made regarding the type of dysmorphosis or thetechnique adopted. A personal file was draw up for each patienton which was noted all the data of interest to the study, i.e. iden-tity, age, gender, the drug used, the medical questionnaire andthe analog visual scale (AVS).
Our study involved assessing the impact of paracetamol and ibu-profen on pain perception following placement of the first arch-wire. The first drug intake was scheduled immediately after theprocedure. Pain evaluation on the AVS was made at 2h, 6h,24h,day 2, day 3 and day 7 . AVS is a graduated 10cm line on which the patient is requested tomark a cross. The far left of the line signifies no pain where as thefar right indicates unbearable pain.
Measurements are performed using a millimeter-scale ruler fromthe far left up to the mark. The measurements were then noted onconvenient and legible tables using statistics software (SPSS11.5) which performed rapid error-free calculations of frequency,percentages, arhythmic means and standard deviations.
The Student t test was used make statistical comparisons of thedifferent means.
Results
Sample distribution
• By gender: the sample contained 39 female patients (69.6%)and 17 males (30.4%).
• By age: the sample was divided into 2 age groups, those under15 (21.4%) and the majority who were over 15 (78.6%).
• By drug: the distribution of paracetamol versus ibuprofen wasalmost identical, namely 48.2% for paracetamol and 51.8% foribuprofen.
Effect of paracetamol on pain over time
An analysis of the effect of paracetamol on orthodontic painshows that there was a reduction in the perception of pain fromthe 2
nd
day with a pain peak 6 hours after placement of the firstarchwire
(fig. 1)
. This decrease in pain was significant on day 3and highly significant at day 7.
Effect of ibuprofen on pain over time
Ibuprofen reduced pain perception over time with a pain peak at2h. The difference in mean pain was significant at 6h and highlysignificant at 24h, day 2, day 3, and day 7
(fig. 2)
.
Lahcen OUSEHAL, Amina LAKHDAR, Farid ELQUARS
196
International
Orthodontics
2009 ; 7 : 193-206
Comparaison de l’effet du paracétamol et celui de l’ibuprofène sur la douleur orthodontique
La comparaison des moyennes de douleur sous paracétamol àcelles sous ibuprofène à différent temps montre que la différenceest presque significative à 2 h (p = 0,08), alors qu’elle est nonsignificative après
(Tableaux I-VI).
Fig. 1 : Effet du paracétamol sur la douleur en fonc-tion du temps.Fig. 1: Effect of paracetomol on pain over time.
Fig. 2 : Effet de l’ibuprofène sur la douleur en fonc-tion du temps.Fig. 2: Effect of ibuprofen on pain over time.
Tableau IComparaison paracétamol, ibuprofène à 2 h.
Table IParacetamol/Ibuprofen comparison after 2h.
MédicamentDrug N Moyenne/
Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Errort ddl Sig.(bilatéral)/
Sig. (bilateral)
Douleur à 2 h
Pain after 2h
Paracétamol/
Paracetamol27 32,4074 31,42055 6,04689
Ibuprofène/
Ibuprofen29 47,2414 31,04105 5,76418 – 1,776 54 0,081 NS
Comparison of the impact of paracetamol and ibuprofen on orthodontic pain
A comparison of the pain means recorded for Paracetol and ibu-profen shows that the difference is almost significant at 2h(p=0.08), whereas it is non-significant subsequently
(Tables I-VI)
.
Comparaison de l’effet du paracétamol et de l’ibuprofène sur la douleur orthodontique
Comparison of the effect of Paracetamol and Ibuprofène on orthodontic pain
International
Orthodontics
2009 ; 7 : 193-206
197
Perception douloureuse en fonction du sexe
Afin d’évaluer la perception douloureuse, nous avons comparé lamoyenne de douleur entre les filles et les garçons appartenant à
Tableau IIComparaison paracétamol, ibuprofène à 6 h.
Table IIParacetamol/Ibuprofen comparison after 6h.
Médicament/Drug N Moyenne/
Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddl Sig. (bilatéral)Sig. (bilateral)
Douleur à 6 h/
Pain after 6h
Paracétamol/
Paracetamol27 38,1852 34,60773 6,66026 – 0,420 54 0,676 NS
Ibuprofène/
Ibuprofen29 41,7241 28,32452 5,25973
Tableau IIIComparaison paracétamol, ibuprofène à 24 h.
Table IIIParacetamol/Ibuprofen comparison after 24h.
Médicament/Drug N Moyenne/
Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Errort ddl
Sig. (bilatérale)/
Sig. (bilateral)
Douleur à 24 h/
Pain after 24h
Paracétamol/
Paracetamol27 31,0741 26,68466 5,13547 – 0,422 54 0,675 NS
Ibuprofène/
Ibuprofen29 34,1379 27,61563 5,12809
Tableau IVComparaison paracétamol, ibuprofène à 48 h.
Table IVParacetamol/Ibuprofen comparison after 48h.
Médicament/Drug
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standardmoyenne
Mean Standard Errort ddl
Sig. (bilatérale)
Sig. (bilateral)
Douleur à 48 h/
Pain after 48h
Paracétamol/
Paracetamol27 26,5556 25,93532 4,99126 – 0,261 54 0,795 NS
Ibuprofène/
Ibuprofen29 28,4483 28,09752 5,21758
Perception of pain by gender
In order to assess pain perception, we compared the mean painrecorded by girls and boys belonging to the same age groups
Lahcen OUSEHAL, Amina LAKHDAR, Farid ELQUARS
198 International Orthodontics 2009 ; 7 : 193-206
la même tranche d’âge (≤ à 15 ans ; > à 15 ans) et sous le mêmemédicament (paracétamol ou ibuprofène) et ceci à 2 temps (2 h et7 j). Les résultats ont montré que la différence de moyenne estnon significative, permettant de conclure que le sexe ne peut êtreconsidéré comme facteur influençant la perception douloureuse(Tableaux VII-XII).
Tableau VComparaison paracétamol, ibuprofène à 72 h.
Table VParacetamol/Ibuprofen comparison after 72h.
Médicament/Drug
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddl Sig. (bilatérale)Sig. (bilateral)
Douleur à 72 h/
Pain after 72h
Paracétamol/
Paracetamol27 18,2222 20,04674 3,85800 – 0,593 54 0,556 NS
Ibuprofène/
Ibuprofen29 22,1034 27,99406 5,19837
Tableau VIComparaison paracétamol, ibuprofène à 7 j.
Table VIParacetamol/Ibuprofen comparison after 7 days.
Médicament/Drug
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t DdlSig.
(bilatérale)/Sig. (bilateral)
Douleur à 7 j/Pain after 7 days
Paracétamol/
Paracetamol27 11,1111 16,60244 3,19514 – 0,732 54 0,467 NS
Ibuprofène/
Ibuprofen29 15,0690 23,07895 4,28565
Tableau VIIComparaison de la perception douloureuse entre filles et garçons de moins de 15 ans sous paracétamol à 2 h.
Table VIIComparison of pain perception between girls and boys less than 15 under Paracetamol after 2 h.
Douleur en fonction du sexe/
Pain as a function of Gender
N MoyenneMean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
T ddlSig.
(bilatérale)/Sig. (bilateral)
Douleur à 2 h/
Pain after 2h
Fille/Girls
≤ 15 ans Paracétamol/
≤15 yrs Paracetamol
7 35,0000 38,83727 14,67911 0,313 8 0,762 NS
Garçon/Boys
≤ 15 ans Paracétamol/
≤15 yrs Paracetamol
3 26,6667 37,85939 21,85813
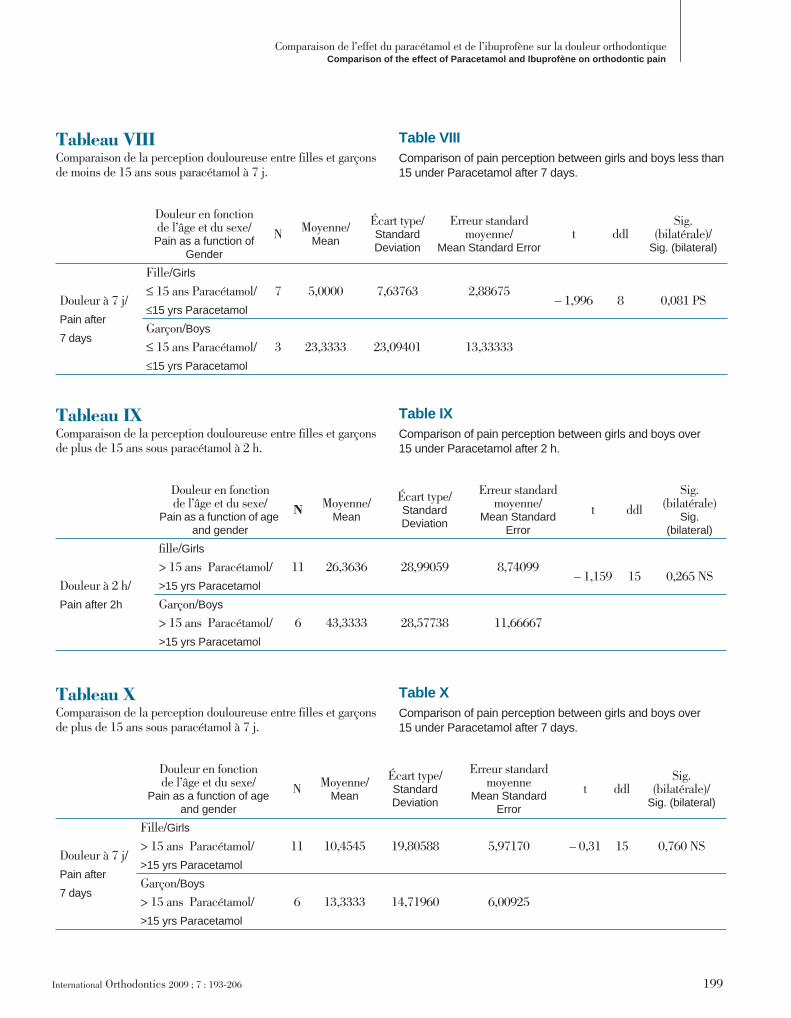
(≤15 yrs; >15 yrs) and receiving the same drug (paracetamol oribuprofen) at two different times (2h and day 7). The results showthat the difference in the means is non-significant and allows usto conclude that gender cannot be considered a factor influencingthe perception of pain (Tables VII-XII).
Comparaison de l’effet du paracétamol et de l’ibuprofène sur la douleur orthodontiqueComparison of the effect of Paracetamol and Ibuprofène on orthodontic pain
International Orthodontics 2009 ; 7 : 193-206 199
Tableau VIIIComparaison de la perception douloureuse entre filles et garçons de moins de 15 ans sous paracétamol à 7 j.
Table VIIIComparison of pain perception between girls and boys less than 15 under Paracetamol after 7 days.
Douleur en fonction de l’âge et du sexe/Pain as a function of
Gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Errort ddl
Sig. (bilatérale)/
Sig. (bilateral)
Douleur à 7 j/
Pain after
7 days
Fille/Girls
≤ 15 ans Paracétamol/
≤15 yrs Paracetamol
7 5,0000 7,63763 2,88675
– 1,996
8
0,081 PS
Garçon/Boys
≤ 15 ans Paracétamol/
≤15 yrs Paracetamol
3 23,3333 23,09401 13,33333
Tableau IXComparaison de la perception douloureuse entre filles et garçons de plus de 15 ans sous paracétamol à 2 h.
Table IXComparison of pain perception between girls and boys over 15 under Paracetamol after 2 h.
Douleur en fonction de l’âge et du sexe/
Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddl
Sig. (bilatérale)
Sig. (bilateral)
Douleur à 2 h/
Pain after 2h
fille/Girls
> 15 ans Paracétamol/
>15 yrs Paracetamol
11 26,3636 28,99059 8,74099
– 1,159
15
0,265 NS
Garçon/Boys
> 15 ans Paracétamol/
>15 yrs Paracetamol
6 43,3333 28,57738 11,66667
Tableau XComparaison de la perception douloureuse entre filles et garçons de plus de 15 ans sous paracétamol à 7 j.
Table XComparison of pain perception between girls and boys over 15 under Paracetamol after 7 days.
Douleur en fonction de l’âge et du sexe/
Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne
Mean Standard Error
t ddlSig.
(bilatérale)/Sig. (bilateral)
Douleur à 7 j/
Pain after
7 days
Fille/Girls
> 15 ans Paracétamol/
>15 yrs Paracetamol
11 10,4545 19,80588 5,97170 – 0,31 15 0,760 NS
Garçon/Boys
> 15 ans Paracétamol/
>15 yrs Paracetamol
6 13,3333 14,71960 6,00925
Lahcen OUSEHAL, Amina LAKHDAR, Farid ELQUARS
200 International Orthodontics 2009 ; 7 : 193-206
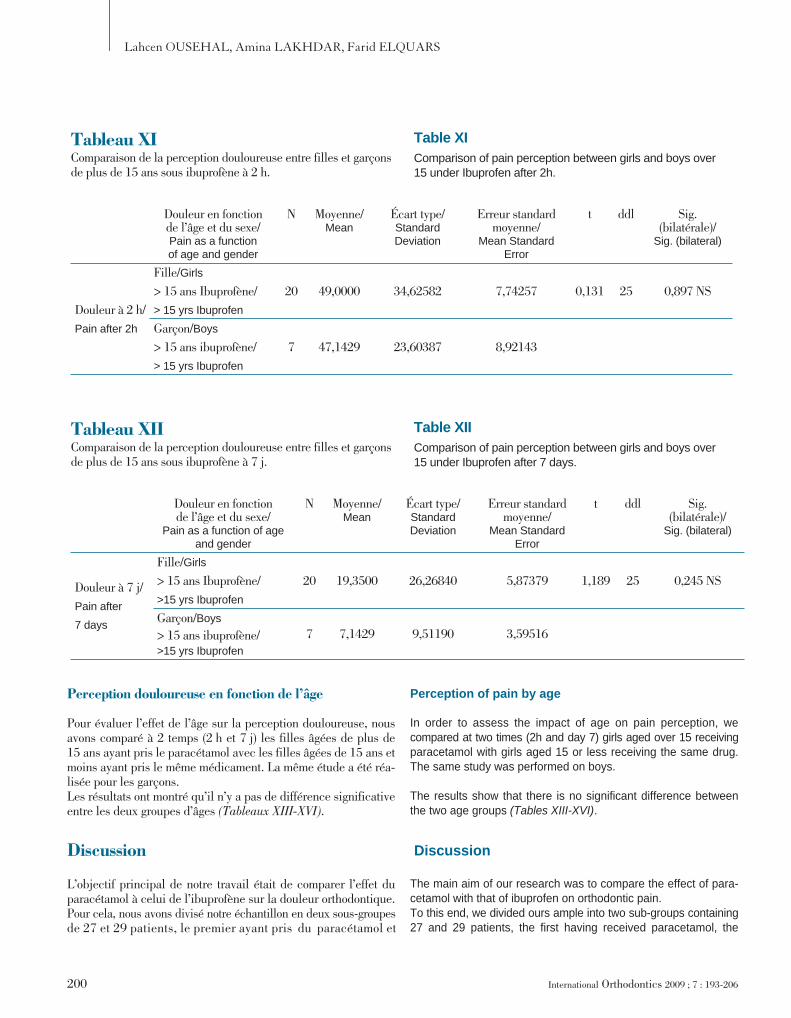
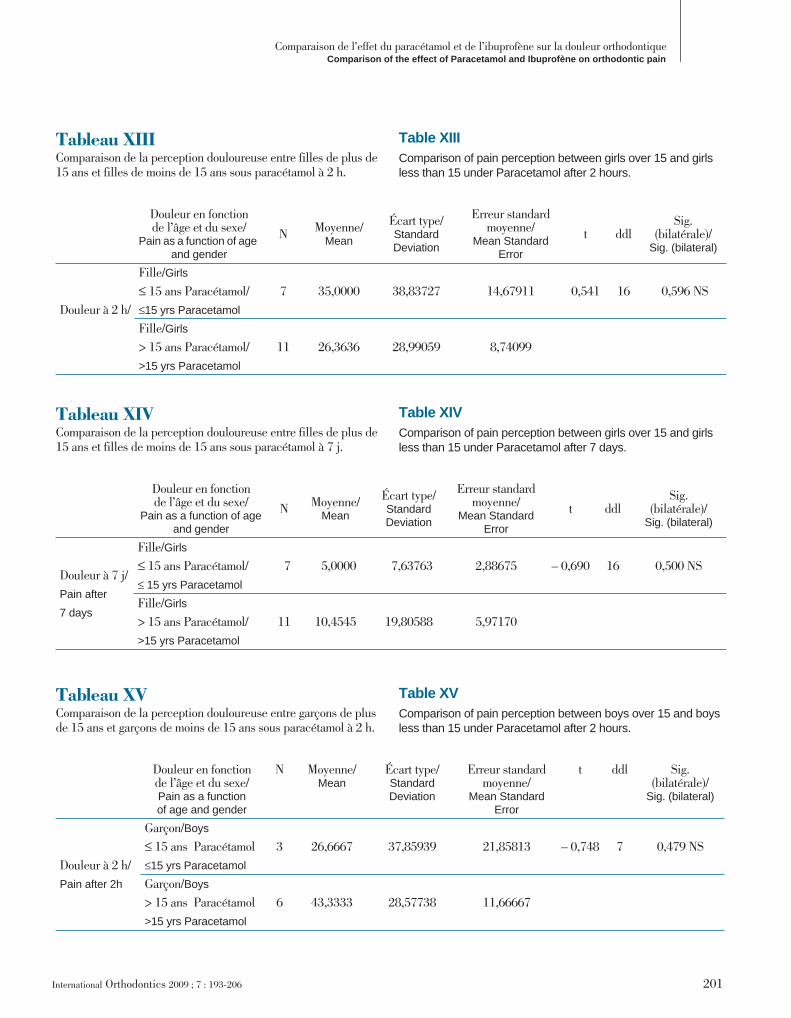
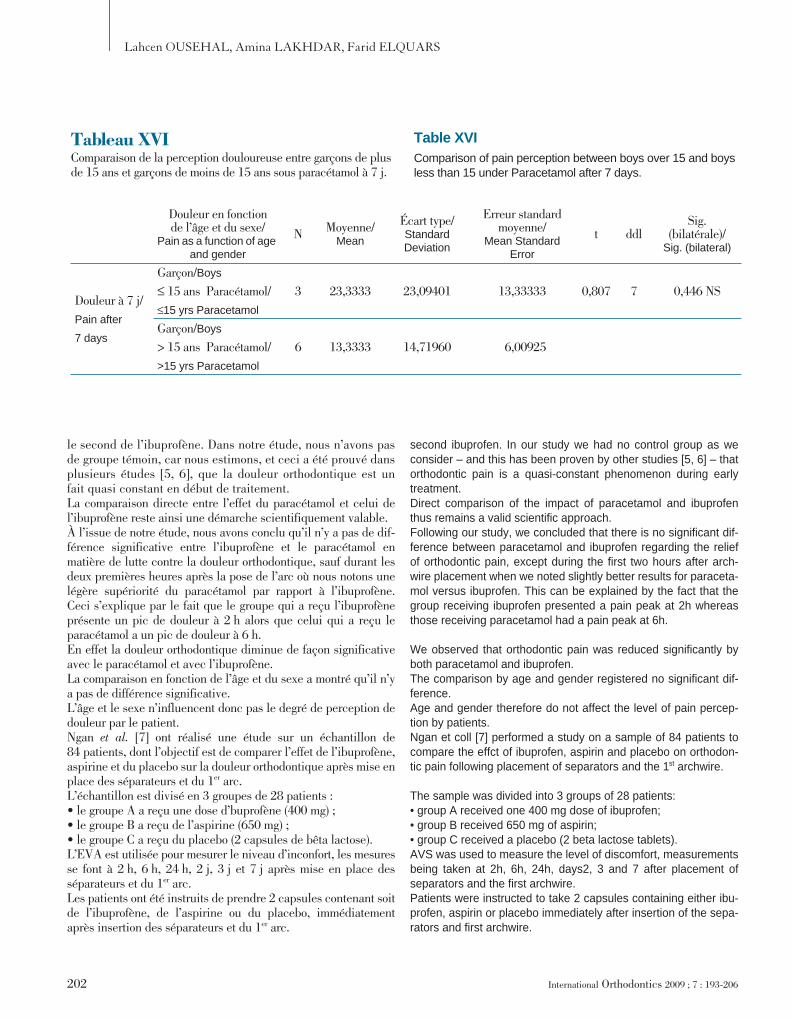
Perception douloureuse en fonction de l’âge
Pour évaluer l’effet de l’âge sur la perception douloureuse, nousavons comparé à 2 temps (2 h et 7 j) les filles âgées de plus de15 ans ayant pris le paracétamol avec les filles âgées de 15 ans etmoins ayant pris le même médicament. La même étude a été réa-lisée pour les garçons.Les résultats ont montré qu’il n’y a pas de différence significativeentre les deux groupes d’âges (Tableaux XIII-XVI).
Discussion
L’objectif principal de notre travail était de comparer l’effet duparacétamol à celui de l’ibuprofène sur la douleur orthodontique.Pour cela, nous avons divisé notre échantillon en deux sous-groupesde 27 et 29 patients, le premier ayant pris du paracétamol et
Tableau XIComparaison de la perception douloureuse entre filles et garçons de plus de 15 ans sous ibuprofène à 2 h.
Table XIComparison of pain perception between girls and boys over 15 under Ibuprofen after 2h.
Douleur en fonction de l’âge et du sexe/Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddl Sig. (bilatérale)/
Sig. (bilateral)
Douleur à 2 h/
Pain after 2h
Fille/Girls
> 15 ans Ibuprofène/
> 15 yrs Ibuprofen
20 49,0000 34,62582 7,74257 0,131 25 0,897 NS
Garçon/Boys
> 15 ans ibuprofène/
> 15 yrs Ibuprofen
7 47,1429 23,60387 8,92143
Tableau XIIComparaison de la perception douloureuse entre filles et garçons de plus de 15 ans sous ibuprofène à 7 j.
Table XIIComparison of pain perception between girls and boys over 15 under Ibuprofen after 7 days.
Douleur en fonction de l’âge et du sexe/
Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddl Sig. (bilatérale)/
Sig. (bilateral)
Douleur à 7 j/
Pain after
7 days
Fille/Girls
> 15 ans Ibuprofène/
>15 yrs Ibuprofen
20 19,3500 26,26840 5,87379 1,189 25 0,245 NS
Garçon/Boys
> 15 ans ibuprofène/>15 yrs Ibuprofen
7 7,1429 9,51190 3,59516
Perception of pain by age
In order to assess the impact of age on pain perception, wecompared at two times (2h and day 7) girls aged over 15 receivingparacetamol with girls aged 15 or less receiving the same drug.The same study was performed on boys.
The results show that there is no significant difference betweenthe two age groups (Tables XIII-XVI).
Discussion
The main aim of our research was to compare the effect of para-cetamol with that of ibuprofen on orthodontic pain. To this end, we divided ours ample into two sub-groups containing27 and 29 patients, the first having received paracetamol, the
Comparaison de l’effet du paracétamol et de l’ibuprofène sur la douleur orthodontiqueComparison of the effect of Paracetamol and Ibuprofène on orthodontic pain
International Orthodontics 2009 ; 7 : 193-206 201
Tableau XIIIComparaison de la perception douloureuse entre filles de plus de 15 ans et filles de moins de 15 ans sous paracétamol à 2 h.
Table XIIIComparison of pain perception between girls over 15 and girls less than 15 under Paracetamol after 2 hours.
Douleur en fonction de l’âge et du sexe/
Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddlSig.
(bilatérale)/Sig. (bilateral)
Douleur à 2 h/
Fille/Girls
≤ 15 ans Paracétamol/
≤15 yrs Paracetamol
7 35,0000 38,83727 14,67911 0,541 16 0,596 NS
Fille/Girls
> 15 ans Paracétamol/
>15 yrs Paracetamol
11 26,3636 28,99059 8,74099
Tableau XIVComparaison de la perception douloureuse entre filles de plus de 15 ans et filles de moins de 15 ans sous paracétamol à 7 j.
Table XIVComparison of pain perception between girls over 15 and girls less than 15 under Paracetamol after 7 days.
Douleur en fonction de l’âge et du sexe/
Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddlSig.
(bilatérale)/Sig. (bilateral)
Douleur à 7 j/
Pain after
7 days
Fille/Girls
≤ 15 ans Paracétamol/
≤ 15 yrs Paracetamol
7 5,0000 7,63763 2,88675 – 0,690 16 0,500 NS
Fille/Girls
> 15 ans Paracétamol/
>15 yrs Paracetamol
11 10,4545 19,80588 5,97170
Tableau XVComparaison de la perception douloureuse entre garçons de plus de 15 ans et garçons de moins de 15 ans sous paracétamol à 2 h.
Table XVComparison of pain perception between boys over 15 and boys less than 15 under Paracetamol after 2 hours.
Douleur en fonction de l’âge et du sexe/Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddl Sig. (bilatérale)/
Sig. (bilateral)
Douleur à 2 h/
Pain after 2h
Garçon/Boys
≤ 15 ans Paracétamol
≤15 yrs Paracetamol
3 26,6667 37,85939 21,85813 – 0,748 7 0,479 NS
Garçon/Boys
> 15 ans Paracétamol
>15 yrs Paracetamol
6 43,3333 28,57738 11,66667
Lahcen OUSEHAL, Amina LAKHDAR, Farid ELQUARS
202 International Orthodontics 2009 ; 7 : 193-206
le second de l’ibuprofène. Dans notre étude, nous n’avons pasde groupe témoin, car nous estimons, et ceci a été prouvé dansplusieurs études [5, 6], que la douleur orthodontique est unfait quasi constant en début de traitement.La comparaison directe entre l’effet du paracétamol et celui del’ibuprofène reste ainsi une démarche scientifiquement valable.À l’issue de notre étude, nous avons conclu qu’il n’y a pas de dif-férence significative entre l’ibuprofène et le paracétamol enmatière de lutte contre la douleur orthodontique, sauf durant lesdeux premières heures après la pose de l’arc où nous notons unelégère supériorité du paracétamol par rapport à l’ibuprofène.Ceci s’explique par le fait que le groupe qui a reçu l’ibuprofèneprésente un pic de douleur à 2 h alors que celui qui a reçu leparacétamol a un pic de douleur à 6 h.En effet la douleur orthodontique diminue de façon significativeavec le paracétamol et avec l’ibuprofène.La comparaison en fonction de l’âge et du sexe a montré qu’il n’ya pas de différence significative.L’âge et le sexe n’influencent donc pas le degré de perception dedouleur par le patient. Ngan et al. [7] ont réalisé une étude sur un échantillon de84 patients, dont l’objectif est de comparer l’effet de l’ibuprofène,aspirine et du placebo sur la douleur orthodontique après mise enplace des séparateurs et du 1er arc.L’échantillon est divisé en 3 groupes de 28 patients : • le groupe A a reçu une dose d’buprofène (400 mg) ;• le groupe B a reçu de l’aspirine (650 mg) ;• le groupe C a reçu du placebo (2 capsules de bêta lactose).L’EVA est utilisée pour mesurer le niveau d’inconfort, les mesuresse font à 2 h, 6 h, 24 h, 2 j, 3 j et 7 j après mise en place desséparateurs et du 1er arc.Les patients ont été instruits de prendre 2 capsules contenant soitde l’ibuprofène, de l’aspirine ou du placebo, immédiatementaprès insertion des séparateurs et du 1er arc.
Tableau XVIComparaison de la perception douloureuse entre garçons de plus de 15 ans et garçons de moins de 15 ans sous paracétamol à 7 j.
Table XVIComparison of pain perception between boys over 15 and boys less than 15 under Paracetamol after 7 days.
Douleur en fonction de l’âge et du sexe/
Pain as a function of age and gender
N Moyenne/Mean
Écart type/Standard Deviation
Erreur standard moyenne/
Mean Standard Error
t ddlSig.
(bilatérale)/Sig. (bilateral)
Douleur à 7 j/
Pain after
7 days
Garçon/Boys
≤ 15 ans Paracétamol/
≤15 yrs Paracetamol
3 23,3333 23,09401 13,33333 0,807 7 0,446 NS
Garçon/Boys
> 15 ans Paracétamol/
>15 yrs Paracetamol
6 13,3333 14,71960 6,00925
second ibuprofen. In our study we had no control group as weconsider – and this has been proven by other studies [5, 6] – thatorthodontic pain is a quasi-constant phenomenon during earlytreatment. Direct comparison of the impact of paracetamol and ibuprofenthus remains a valid scientific approach. Following our study, we concluded that there is no significant dif-ference between paracetamol and ibuprofen regarding the reliefof orthodontic pain, except during the first two hours after arch-wire placement when we noted slightly better results for paraceta-mol versus ibuprofen. This can be explained by the fact that thegroup receiving ibuprofen presented a pain peak at 2h whereasthose receiving paracetamol had a pain peak at 6h.
We observed that orthodontic pain was reduced significantly byboth paracetamol and ibuprofen. The comparison by age and gender registered no significant dif-ference. Age and gender therefore do not affect the level of pain percep-tion by patients. Ngan et coll [7] performed a study on a sample of 84 patients tocompare the effct of ibuprofen, aspirin and placebo on orthodon-tic pain following placement of separators and the 1st archwire.
The sample was divided into 3 groups of 28 patients:• group A received one 400 mg dose of ibuprofen;• group B received 650 mg of aspirin;• group C received a placebo (2 beta lactose tablets). AVS was used to measure the level of discomfort, measurementsbeing taken at 2h, 6h, 24h, days2, 3 and 7 after placement ofseparators and the first archwire. Patients were instructed to take 2 capsules containing either ibu-profen, aspirin or placebo immediately after insertion of the sepa-rators and first archwire.

Comparaison de l’effet du paracétamol et de l’ibuprofène sur la douleur orthodontiqueComparison of the effect of Paracetamol and Ibuprofène on orthodontic pain
International Orthodontics 2009 ; 7 : 193-206 203
77 patients ont complété l’étude des séparateurs, tandis que seule-ment 56 patients ont complété les deux phases d’étude(séparateurs et 1er arc) dont la moyenne d’âge est de 16,6± 6,8 ans.Les résultats ont montré qu’il y a une différence significativedans l’inconfort orthodontique en fonction du groupe de médica-tion et aussi du temps. Le placebo réduit moins l’inconfort en comparaison avec l’ibu-profène à tout temps de l’étude sauf au 7e jour après placementdes séparateurs, de même le placebo réduit moins l’inconfort encomparaison à l’aspirine à 2 h, 6 h, 24 h, 2 j, 3 j et 7 j après pla-cement des séparateurs. En plus, avec l’ibuprofène il y a moinsd’inconfort par rapport aux deux autres médicaments à 6 h, 24 h,2 j et 7 j après placement des séparateurs.Il y a moins d’inconfort avec l’ibuprofène qu’avec le placebo àtous les temps de l’étude après placement du 1er arc.Il y a moins d’inconfort avec l’aspirine qu’avec le placebo à 6 h,24 h, 3 j et 7 j après placement du 1er arc.Il y a moins d’inconfort avec l’ibuprofène qu’avec l’aspirine à 2 h,6 h, 2 j, 3 j et 7 j après placement du 1er arc.La comparaison des moyennes de douleur entre séparateurs et1er arc montre que le plus haut niveau de douleur se produit auniveau du 1er arc. Ceci appuie notre démarche puisque nous noussommes contentés de la douleur qui accompagne la pose du 1er arc.Bird [8] a fait une étude similaire à la nôtre, mais se limitant àl’évaluation de la douleur suite à la mise en place des séparateursorthodontiques. Ils ont trouvé qu’il n’y pas de différence significa-tive entre l’ibuprofène et le paracétamol en matière de contrôle dela douleur orthodontique.Bradley [9] a réalisé une étude clinique sur 159 patients âgésentre 12 et 16 ans divisés en deux groupes qui ont reçu respecti-vement 400 mg d’ibuprofène et 1 g de paracétamol par voie orale,1 h avant et 6 h après la mise en place des séparateurs.L’EVA a été utilisée pour apprécier la douleur orthodontiquedurant une semaine.Les résultats ont montré que la douleur était à son pic 2 h aprèsmise en place des séparateurs et diminuait progressivement avecle temps. De même, l’ibuprofène prescrit en préopératoire et enpostopératoire serait plus efficace dans le contrôle de la douleurorthodontique que le paracétamol.Steen [10] a, quant à lui, étudié le temps de prise de l’ibuprofènepour la douleur orthodontique. Son objectif est d’évaluer l’effet del’ibuprofène en préopératoire dans la réduction de la sévérité dela douleur après placement des séparateurs orthodontiques etsurtout de comparer l’effet de l’ibuprofène préopératoire aveccelui de l’ibuprofène postopératoire et du placebo.Pour cela, un échantillon de 114 patients a été choisi dans « theclinical pool of the university of lowa college of dentistry’s depar-tement of orthodontics », les patients ont été affectés à 3 groupes.Le groupe A a reçu 400 mg d’ibuprofène 1 h avant le placementdes séparateurs et du lactose placebo immédiatement après le ren-dez-vous.Le groupe B a reçu du lactose placebo 1 h avant le placement desséparateurs et 400 mg d’ibuprofène immédiatement après lerendez-vous.
77 patients completed the study with the separators, whereasonly 56 patients (mean age: 16.6±6.8yrs) completed the twophases of the study (separators and 1st archwire).
The results showed that there is a significant difference in orth-odontic discomfort depending on both the medication group andthe time. The placebo reduced discomfort least versus ibuprofen at allstudy times except at day 7 after placement of the separators.Similarly, the placebo reduced discomfort less than aspirin at 2h,6h, 24h, day 2, day 3 and day 7 after separator placement. More-over, less discomfort was experienced with ibuprofen than withthe two other medications at 6h, 24h, 2 days and 7days followingplacement of separators. There was less discomfort with ibuprofen than with the placebo atall study times after placement of the first archwire. There was less discomfort with aspirin than with placebo at 6h,24h, day 3 and day 7 following placement of the 1st archwire. Less discomfort was observed with ibuprofen than with aspirin at 2h,6h, 2 days, 3 days and 7 days after placement of the first archwire.A comparison of mean pain between separators and 1st archwirerevealed that the highest peak occurred following the 1st archwireplacement. This result supports our own approach since we lim-ited our measurements to pain following the placement of the1st archwire.Bird SE [8] undertook a similar study to ours but limited to anassessment of pain following placement of orthodontic separa-tors. They found that there was no significant difference betweenibuprofen and paracetamol as regards control of orthodontic pain.Bradley [9] performed a clinical study on 159 patients between 12and 16 years divided into two groups receiving, respectively,400mg of ibuprofen and 1g of paracetamol per os, 1 hour beforeand 6 hours after separator placement. AVS was used to measure orthodontic pain for one week.
The results showed that pain reached a peak 2 hours after place-ment of the separators and decreased gradually with time. More-over, they demonstrated that ibuprofen prescribed preoperativelyand postoperatively are more effective than paracetamol fororthodontic pain control. Steen Law [10] studies the intake time of ibuprofen for orthodonticpain. His aim was to assess the effect of preoperative ibuprofen inthe reduction of pain severity after placement of orthodontic sepa-rators and, above all, to compare the effect of preoperative ibu-profen with that of postoperative ibuprofen and placebo.
A sample of 144 patients was selected at the “Clinical clinical poolof the University of lowa College of Dentistry’s department of ortho-dontics”. Patients were divided into 3 groups. Group A received 400 mg of ibuprofen 1h before placement of theseparators and a lactose placebo immediately following theappointment. Group B received a lactose placebo 1h before placement of theseparators and 400 mg of ibuprofen immediately following theappointment.

Lahcen OUSEHAL, Amina LAKHDAR, Farid ELQUARS
204 International Orthodontics 2009 ; 7 : 193-206
Le groupe C a reçu du lactose placebo 1 h avant le place-ment des séparateurs et immédiatement après le rendez-vous.L’évaluation de la douleur se fait à l’aide de l’EVA, les patientsvont évaluer leur douleur à 2 h, 6 h, 24 h, 2 j, 3 j et 7 j après pla-cement des séparateurs en mettant une croix sur l’EVA à chaqueévaluation. Seulement 63 patients ont respecté les consignes etont été, par la suite, introduits dans l’étude.Les résultats montrent que la moyenne d’âge est similaire entreles 3 groupes. De plus, il n’y a pas de différence significativedans la distribution du sexe dans les 3 groupes de même quedans la distribution du nombre de séparateurs.Les résultats de son étude ont montré qu’il y a une différencesignificative entre les groupes à 2 h : les sujets qui ont pris del’ibuprofène avant leur rendez-vous rapportent une diminutiondu score de douleur par rapport aux sujets qui ont pris de l’ibu-profène en postopératoire ou du placebo. Ceci expliquerait lasupériorité du paracétamol par rapport à l’ibuprofène à 2 hdans notre étude.Dans les 3 groupes, il y a une augmentation du score de la dou-leur à partir de 2 h jusqu’au pic de douleur situé à 24 h aprèsplacement des séparateurs, puis il y a une diminution graduellede douleur jusqu’au 7e jour.Bernhardt et al. [11] ont réalisé une étude dont l’objectif est decomparer l’effet de l’ibuprofène préopératoire, l’ibuprofène post-opératoire et la combinaison pré- et postopératoire de l’ibupro-fène après mise en place des séparateurs.Pour cela, un échantillon de 140 patients a été divisé en 3 groupes.Le groupe A a reçu 400 mg d’ibuprofène 1 h avant l’insertion desséparateurs et 400 mg d’ibuprofène 6 h après la 1re dose.Le groupe B a reçu 400 mg d’ibuprofène 1 h avant l’insertiondes séparateurs et une capsule de lactose 6 h après la doseinitiale.Le groupe C a reçu une capsule de lactose 1 h avant l’insertiondes séparateurs et 400 mg d’ibuprofène 6 h après l’initialedose.Un questionnaire a été remis à chaque patient. Il contient des fichesd’EVA permettant de mesurer le degré d’inconfort à 2 h, 6 h, au cou-cher, au réveil, à 24 h, 2 j, 3 j et 7 j après placement des séparateurs.Les résultats de l’étude montrent qu’à 2 h après placement desséparateurs, il y a une différence de douleur significative enfaveur du groupe A et B qui ont pris de l’ibuprofène en préopé-ratoire.Le soir de la mise en place des séparateurs, il y a une différencede douleur significative en faveur du groupe B par rapport augroupe C. Le groupe A ne montre pas de différence significativeque ce soit par rapport au groupe B ou C.À partir du 2e jour, tous les patients du groupe A présentent desscores de douleur bas.Polat [12] a comparé l’effet de l’ibuprofène, du paracétamol, del’aspirine et d’un placebo sur la douleur chez des patients porteursd’appareillages orthodontiques. Les résultats ont montré que tous lesantalgiques réduisent la douleur par rapport au placebo. Le groupeayant pris l’aspirine ou le paracétamol a affiché les scores de douleurles plus bas sur l’EVA.
Group C received a lactose placebo 1h prior to placement of theseparators and immediately following the appointment.
Pain assessment was performed using AVS and patient evalu-ated their pain at 2h, 6h, 24h, day 2, day 3 and day 7 after place-ment of the separators by placing a cross on the AVS at eachevaluation. Only 63 patients followed instructions and were sub-sequently allowed into the study. The results showed that a similar mean age between the differentgroups. Moreover, there was no significant difference in genderdistribution or in the distribution of the number of separatorsbetween the three groups. The results of his study showed a significant difference betweenthe groups at 2h. Subjects receiving ibuprofen before theirappointment reported a decrease in their pain score versus sub-jects taking ibuprofen or placebo postoperatively. This wouldexplain the superiority of paracetamol over ibuprofen at 2h in ourstudy.
In the three groups, the pain score increased as of 2h to reach apeak around 24h after placement of the separators, followingwhich there is a gradual decrease in pain up to day 7.
Bernhardt et coll [11] made a study designed to compare theeffect of preoperative ibuprofen, postoperative ibuprofen and acombination of pre- and postoperative ibuprofen following separa-tor placement.They used a sample of 140 patients divided into 3 groups. Group A received 400 g of ibuprofen 1h before insertion of theseparators and 400 g of ibuprofen 6h after the first dose. Group B received 400 g of ibuprofen 1h before insertion of theseparators and a lactose capsule 6h after the initial dose. Group C recieved a capsule of lactose 1h before placement of theseparators and 400 mg of ibuprofen 6h after the initial dose.
A questionnaire was given to each patient containing AVS cardsto measure the level of discomfort at 2h, 6h on going to bed, onwaking, at 24h, day 2, day 3 and day 7 after separator placement. The results of the study showed that 2h after separator placementthere was a significant difference in pain levels in favor of groupsA and B which had taken ibuprofen preoperatively.
On the evening of the day of separator placement, there was asignificant pain difference in favor of group B versus group C.Group A showed no significant difference with either group B orgroup C. From day 2 onwards, all the patients in group A recorded low painscores. Polat [12] compared the effect of ibuprofen, paracetamol, aspirinand a placebo on pain in patients wearing orthodontic appliances.The results showed that all the antalgesics reduce pain versusplacebo. The group receiving aspirin or paracetamol recorded thelowest pain scores on the AVS.

Comparaison de l’effet du paracétamol et de l’ibuprofène sur la douleur orthodontiqueComparison of the effect of Paracetamol and Ibuprofène on orthodontic pain
International Orthodontics 2009 ; 7 : 193-206 205
L’ibuprofène dans le contrôle de la douleur orthodontique
Ngan et al. [7] ont comparé l’ibuprofène, l’aspirine et le placebo.Ils ont conclu que l’ibuprofène est l’analgésique de choix quidiminue la douleur durant le traitement orthodontique.Steen et al. [10] prennent les recherches plus loin et supportentl’utilisation de l’ibuprofène en préopératoire pour l’inconfortorthodontique.En se basant sur ces résultats, Bernhardt et al. [11] suggèrentl’utilisation de l’ibuprofène en pré- et postopératoire qui aentraîné la diminution de la douleur orthodontique en comparai-son avec les doses d’analgésiques prises seules. À partir desrésultats de cette dernière étude, nous concluons que la prise de400 mg d’ibuprofène 1 h avant la mise en place des séparateursréduit le degré de douleur éprouvé après traitement.En effet, les prostaglandines participent à la transmission desstimuli douloureux et augmentent la sensibilité aux stimulianxieux comme la sérotonine, l’histamine, la bradykinine et lasubstance P. D’autre part, les prostaglandines, particulière-ment de série E, stimulent la résorption osseuse pendant lesmouvements orthodontiques dentaires. Étant donné le rôleimportant des prostaglandines dans le mouvement dentaire,l’ibuprofène ne peut être utilisé pour contrôler la douleurorthodontique, car il inhibe la cyclooxygénase et donc la pro-duction de PGE ; il peut inhiber l’activité des ostéoclastesnécessaires au mouvement dentaire.Cependant, le dosage de l’anti-inflammatoire utilisé dans les étudesqui conclut à l’inhibition du mouvement dentaire est beau-coup plus important que la dose utilisée pour anticiper ladouleur orthodontique. En plus, il n’est pas évident quel’inhibition du mouvement dentaire soit due à l’inhibition desprostaglandines.Tout ceci nous amène à conclure que l’ibuprofène est lemeilleur choix pour minimiser l’inconfort lié à la douleurorthodontique.
Conclusion
De nombreuses études ont montré que les patients qui vont béné-ficier d’un traitement orthodontique manifesteront un degrévariable d’inconfort lié au port de l’appareil, mais surtout à ladouleur secondaire au déplacement dentaire.Le caractère subjectif de la douleur fait que sa perception seratrès différente d’un patient à l’autre. Dans certains cas, elle peutmême être la raison de l’abandon du traitement.Aussi, le praticien se doit d’informer le patient, de lui expliquerles différents inconforts avant d’entamer un traitement.À l’issue de notre travail, nous pouvons avancer les recommanda-tions suivantes :• mettre le patient sous médication antalgique de préférence 1 havant la mise en place des séparateurs ou du 1er arc ;• en cas d’absence de contre-indication, choisir un anti-inflam-matoire non stéroïdien, de préférence un ibuprofène ;
Ibuprofen in the control of orthodontic pain
Ngan et coll [7] compared ibuprofen, aspirin and placebo andconcluded that ibuprofen is the antalgesic of choice for the reliefof pain during orthodontic treatment. Steen Law et coll [10] pursued this research still further and sup-ported the use of ibuprofen preoperatively for orthodontic painrelief. Based on these results, Bernhardt et coll [11] suggested the useof ibuprofen pre- and postoperatively as it had reduced orthodon-tic pain in comparison with the doses of antalgesics taken alone.On the basis of the results in this latter study, we conclude that400g of ibuprofen taken 1h before placement of separatorsreduces the level of pain experienced posttreatment.
Effectively, prostaglandins plat a role in transmitting pain stimuliand increase sensitivity to anxiety stimuli such as serotonin, hista-mine, bradykinine and substance P. Furthermore, prostaglandins,particularly series E prostaglandins, stimulate bone resorptionduring orthodontic tooth movements. Given the major role playedby prostaglandins in tooth movement, ibuprofen cannot be usedfor orthodontic pain control as it inhibits cyclo-oxygenase andthus the production of PGE. It can inhibit the activity of the osteo-clasts required for dental movement.
However, the dose of anti-inflammatory agents used in the stud-ies which concluded on tooth movement inhibition is muchgreater than the dose used to relieve orthodontic pain. In addition,it is not clear whether the inhibition of tooth movement was due toprostaglandine inhibition.
All these arguments lead us to conclude that ibuprofen is the bestchoice to minimize discomfort linked to orthodontic pain.
Conclusion
Many studies have shown that the patients undergoing orthodon-tic treatment will experience varying degrees of discomfort asso-ciated with wearing the appliance but, above all, with the paincaused by tooth displacement. The subjective nature of pain means that perception of pain dif-fers from one patient to another. In some cases, it can even leadto treatment being abandoned. Thus, before commencing treatment, practitioners must informpatients, and explain to them the various sources of discomfort. In conclusion to our study, we can advance the following recom-mendations: • administer antalgesic medication to the patient 1h before placingseparators or the 1st archwire; • when not contraindicated, choose a non-steroidal anti-inflammatory,preferably ibuprofen;

Lahcen OUSEHAL, Amina LAKHDAR, Farid ELQUARS
206 International Orthodontics 2009 ; 7 : 193-206
• choisir des arcs souples superélastiques en début de traite-ment, car le maximum de douleur est ressenti avec le 1er arc.Les arcs Ni-Ti, les fils australiens de faible calibre et les arcstressés sont ainsi recommandés.
Références/References
1. Louis P, Michielsens B. Les algies neurogènes. Real Clin 1994;5:229-239.2. Oliver RG, Knappman YM. Attitudes to orthodontic treatment. Br J Orthod 1985;12:179-188.3. Patel V. Non-completion of orthodontic treatment: a study of patients and parental factors
contributing in the hospital service and specialist practice. University of Wales; 1989 heathpark.
4. Burstone CJ. Biomechanics of tooth movement. Philadelphia: Lea & Febiger, 1964.5. Jones M, Chan C. Pain in the early stages of orthodontic treatments. J Clin Orthod 1992;26:311-
313.6. Jones M, Chan C. The pain and discomfort experienced during orthodontic treatment: a rando-
mized clinical trial of two initial aligning archwires. Am J Orthod Dentofacial Orthop 1992;102:373-381.
7. Ngan P, Kess B. The effect of ibuprofen on the level of discomfort in patients undergoing ortho-dontic treatment. Am J Orthod Dentofacial Orthop 1994;106:88-95.
8. Bird SE, Williams K, Kula K. Preoperative acetaminophen vs ibuprofen for control of pain afterorthodontic separator placement. Am J Orthod Dentofacial Orthop 2007;132(4):504-10.
9. Bradley RL, Ellis PE, Thomas P, Bellis H, Ireland AJ, Sandy JR. A randomized clinical trialcomparing the efficacy of ibuprofen and paracetamol in the control of orthodontic pain. Am JOrthod Dentofacial Orthop 2007;132(4):511-517.
10. Steen L, Sandra L. An evaluation of preoperative ibuprofen for treatment of pain associated withorthodontic separator placement. Am J Orthod Dentofacial Orthop 2000;118: 629-635.
11. Bernhardt MK, Southard KA, Batterson KD, Logan HL, Baker KA, Jakobsen JR. The effect ofpreemptive and/or postoperative ibuprofen therapy for orthodontic pain. Am J Orthod Dentofa-cial Orthop 2001;120(1):20-27.
12. Polat O, Karaman AI. Pain control during fixed orthodontic appliance therapy. Angle Orthod2005;75(2):214-219.
• choose flexible super-elastic archwires during early treatmentas the greatest pain is experienced with the initial archwire.Ni-Ti archwires, small-sized Australian wires and braided wiresare also recommended.













![Traitements chirurgico- orthodontiques · Les patients non motivés ou trop fragiles ne doivent pas oper és têré [3, 6, 7] . Préparation orthodontique préchirurgicale Calendrier](https://img.pdfslide.fr/doc/110x75/5f68261673ef3552572c85b4/traitements-chirurgico-orthodontiques-les-patients-non-motivs-ou-trop-fragiles.jpg)




![Traitements chirurgico- orthodontiques€¦ · Les patients non motivés ou trop fragiles ne doivent pas oper és têré [3, 6, 7] . Préparation orthodontique préchirurgicale Calendrier](https://img.pdfslide.fr/doc/110x75/5f68261673ef3552572c85b6/traitements-chirurgico-les-patients-non-motivs-ou-trop-fragiles-ne-doivent-pas.jpg)