Embed Size (px)
Citation preview
Cas clinique
DOI of or
DepartmenJapon.
CorrespondTokyo Medica160-0023, Jap
Ann Vasc Surhttp://dx.doi.or� Annals of V�Edit�e par ELS
�Evaluation perop�eratoire de la perfusionsanguine par angiographie au vertd’indocyanine assist�ee par laser apr�esreconstruction vasculaire ex vivo d’unan�evrysme intra-hilaire de l’art�ere r�enale
Toru Iwahashi, Yukio Obitsu, Nobusato Koizumi, Naozumi Saiki, Satoshi Takahashi,
Hiroshi Shigematsu, Tokyo, Japon
La reconstruction chirurgicale des an�evrysmes intra-hilaires de l’art�ere r�enale (RAAs) est unechirurgie difficile en raison de l’anatomie complexe. Nous pr�esentons un cas de RAA intra-hilairedroit diagnostiqu�e chez un homme de 67 ans. Nous avons fait une reconstruction ex vivo enutilisant une solution de conservation d’organe pour empecher l’insuffisance r�enale post-op�eratoire. Nous avons �evalu�e la perm�eabilit�e de la revascularisation et la perfusion sanguinepar angiographie laser-assist�ee au vert d’indocyanine avec le syst�eme SPY apr�es auto-transplantation. On n’a pas observ�e d’insuffisance r�enale postop�eratoire. Les r�esultatsd�emontrent que la reconstruction ex vivo des RAA intra-hilaires utilisant une solution de con-servation d’organe, et que l’�evaluation de la perm�eabilit�e et de la perfusion sanguine par lesyst�eme SPY sont des m�ethodes efficaces pour pr�eserver la fonction r�enale.
The incidence of renal artery aneurysms (RAAs) is
very rare, occurring at approximately 0.01-0.09%
as reported in an autopsy study1 and at 0.1-0.3%
as described in an angiography study.2 Moreover,
the risk of RAA rupture has been reported to be
2.8-5.6%,3 with a reported mortality rate of 80%
from ruptured RAAs.4 Progress of the endovascular
technique has enabled the treatment of RAAs
located in the main renal artery, but not of those
found in the renal hilum. The surgical arterial
reconstruction of intrahilar RAAs involves many
iginal article: 10.1016/j.avsg.2011.02.019.
t of Vascular Surgery, Tokyo Medical University, Tokyo,
ance : Toru Iwahashi, Department of Vascular Surgery,l University, 6-7-1 Nishishinjuku, Shinjuku-ku, Tokyoon, E-mail: [email protected]
g 2011; 25: 838.e5-838.e8g/10.1016/j.acvfr.2012.07.022ascular Surgery Inc.EVIER MASSON SAS
risks, including difficulty in securing a surgical view,
difficult surgery due to complex anatomy in the
renal hilum, possible ischemia-reperfusion injury of
the kidney, and postoperative renal failure. We
report a case demonstrating that the ex vivo arterial
reconstruction of intrahilar RAA using an organ
preservation solution, and graft patency and organ
blood perfusion evaluation using the SPY� intrao-
perative imaging system (Novadaq Technologies,
Toronto, Canada) are useful methods for preserving
renal function.
CASE REPORT
We describe the case of a 67-year-old man who presented
with fecal occult blood. To determine the cause of the occult
blood, we performed abdominal computed tomography
(CT) during the medical checkup. CT showed a saccular
aneurysm of 25 mmmaximal dimension in the right renal
artery, and specifically located in the right renal hilum. The
patient had been healthy without any evidence of cardio-
vascular risk factors, such as hypertension, hyperlipidemia,
894.e5
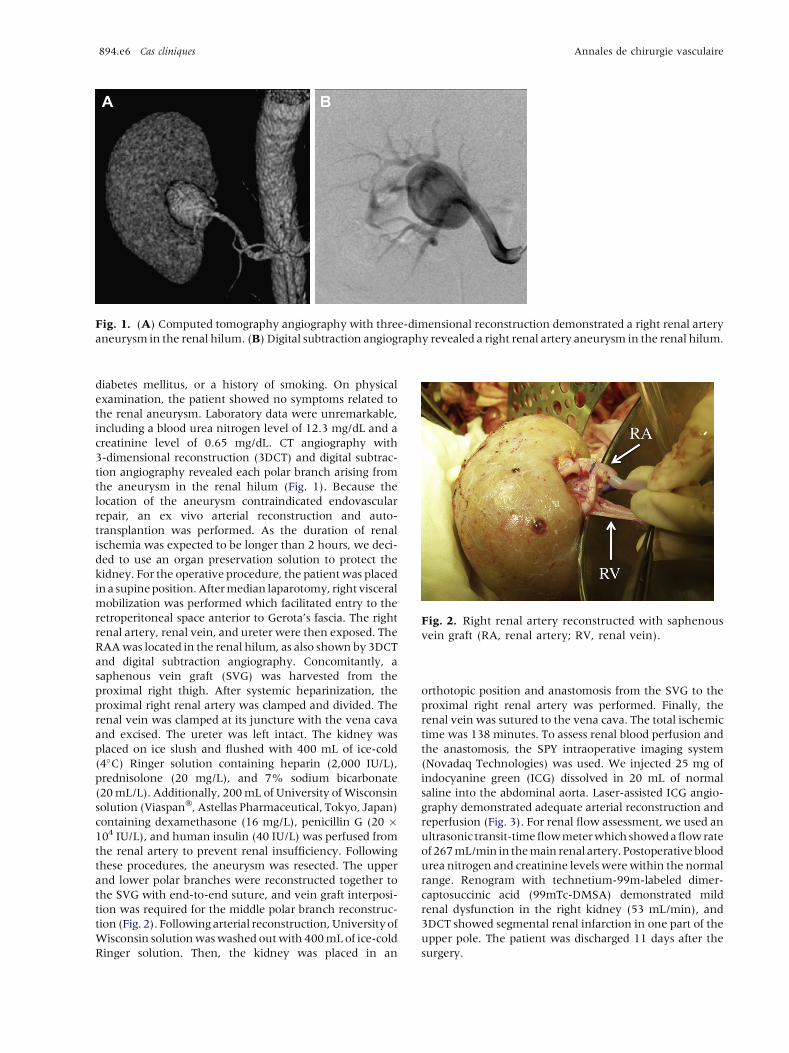
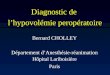
Fig. 1. (A) Computed tomography angiography with three-dimensional reconstruction demonstrated a right renal artery
aneurysm in the renal hilum. (B) Digital subtraction angiography revealed a right renal artery aneurysm in the renal hilum.
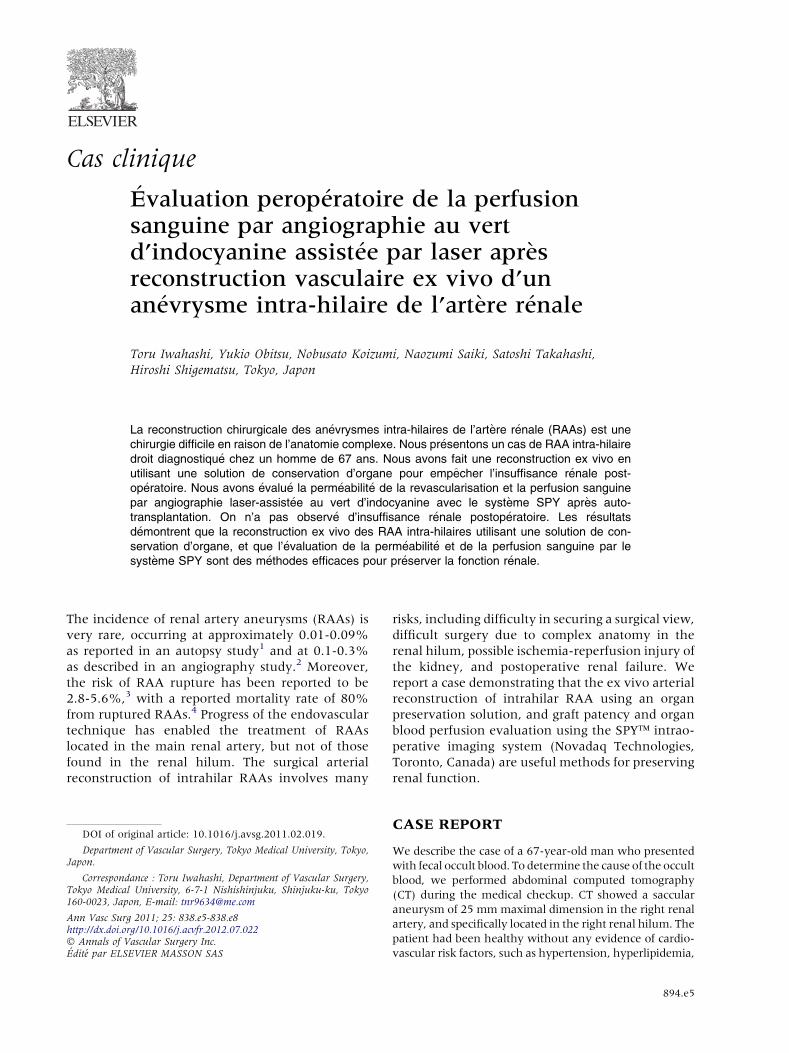
Fig. 2. Right renal artery reconstructed with saphenous
vein graft (RA, renal artery; RV, renal vein).
894.e6 Cas cliniques Annales de chirurgie vasculaire
diabetes mellitus, or a history of smoking. On physical
examination, the patient showed no symptoms related to
the renal aneurysm. Laboratory data were unremarkable,
including a blood urea nitrogen level of 12.3 mg/dL and a
creatinine level of 0.65 mg/dL. CT angiography with
3-dimensional reconstruction (3DCT) and digital subtrac-
tion angiography revealed each polar branch arising from
the aneurysm in the renal hilum (Fig. 1). Because the
location of the aneurysm contraindicated endovascular
repair, an ex vivo arterial reconstruction and auto-
transplantion was performed. As the duration of renal
ischemia was expected to be longer than 2 hours, we deci-
ded to use an organ preservation solution to protect the
kidney. For the operative procedure, the patientwas placed
ina supineposition.Aftermedian laparotomy, right visceral
mobilization was performed which facilitated entry to the
retroperitoneal space anterior to Gerota’s fascia. The right
renal artery, renal vein, and ureter were then exposed. The
RAAwas located in the renal hilum, as also shown by 3DCT
and digital subtraction angiography. Concomitantly, a
saphenous vein graft (SVG) was harvested from the
proximal right thigh. After systemic heparinization, the
proximal right renal artery was clamped and divided. The
renal vein was clamped at its juncture with the vena cava
and excised. The ureter was left intact. The kidney was
placed on ice slush and flushed with 400 mL of ice-cold
(4�C) Ringer solution containing heparin (2,000 IU/L),
prednisolone (20 mg/L), and 7% sodium bicarbonate
(20mL/L). Additionally, 200mL of University ofWisconsin
solution (Viaspan�, Astellas Pharmaceutical, Tokyo, Japan)
containing dexamethasone (16 mg/L), penicillin G (20 �104 IU/L), and human insulin (40 IU/L) was perfused from
the renal artery to prevent renal insufficiency. Following
these procedures, the aneurysm was resected. The upper
and lower polar branches were reconstructed together to
the SVG with end-to-end suture, and vein graft interposi-
tion was required for the middle polar branch reconstruc-
tion (Fig. 2). Followingarterial reconstruction,Universityof
Wisconsin solutionwaswashed outwith 400mLof ice-cold
Ringer solution. Then, the kidney was placed in an
orthotopic position and anastomosis from the SVG to the
proximal right renal artery was performed. Finally, the
renal vein was sutured to the vena cava. The total ischemic
time was 138 minutes. To assess renal blood perfusion and
the anastomosis, the SPY intraoperative imaging system
(Novadaq Technologies) was used. We injected 25 mg of
indocyanine green (ICG) dissolved in 20 mL of normal
saline into the abdominal aorta. Laser-assisted ICG angio-
graphy demonstrated adequate arterial reconstruction and
reperfusion (Fig. 3). For renal flow assessment, we used an
ultrasonic transit-timeflowmeterwhich showedaflowrate
of267mL/min in themain renal artery. Postoperativeblood
urea nitrogen and creatinine levels werewithin the normal
range. Renogram with technetium-99m-labeled dimer-
captosuccinic acid (99mTc-DMSA) demonstrated mild
renal dysfunction in the right kidney (53 mL/min), and
3DCT showed segmental renal infarction in one part of the
upper pole. The patient was discharged 11 days after the
surgery.

Fig. 3. Intraoperative fluorescent angiography after renal vascular reconstruction; 5 and 12 seconds after the injection of
indocyanine green, the renal parenchyma turned bright gradually (RA, renal artery; IVC, inferior vena cava; Ao, aorta).
Vol. 25, No. 6, 2011 Cas cliniques 894.e7
DISCUSSION
The surgical indication for asymptomatic RAAs is cur-
rently not established. However, rupture of small-
diameter RAAs has been reported.5 For most cases,
nephrectomy may be required if the RAAs rupture.
Therefore, experts have suggested the following
indications for the surgical intervention of asympto-
matic RAAs: aneurysmal diameter >20 mm, RAAs
with calcification, enlarging RAAs, and RAAs in
pregnant women.6
Recently, advances in endovascular techniques
have allowed the successful treatment of RAAs.
However, the indications of catheter intervention
remain limited because of the anatomical location,
complexity, and size of aneurysms. In particular,
intrahilar RAAs are difficult to treat by endovascular
therapy.
In situ or ex vivo repair is usually used for the
reconstructionof intrahilarRAAs. If RAAshavemul-
tiple branchvessels, it is expected that reconstruction
may take time. Crutchley et al suggested the use of
hypothermic perfusion when >30-40 minutes of
warm ischemia is anticipated.7 Levy reported that
hypothermic perfusion preserved kidney function
for 120 minutes in dogs.8 Moreover, ex vivo surgery
followed by hypothermic perfusion or perfusion
withorganpreservation solutions, suchasUniversity
of Wisconsin solution, Bretschneider’s Histidine-
Tryptophan-Ketoglutarate (HTK) solution, and
Euro-Collins solution, has been shown to prevent
renal dysfunction caused by ischemia-reperfusion
injury after renal artery reconstruction.7,9 By using
ex vivo vascular reconstruction and an organ pre-
servation solution, we were able to perform arterial
reconstruction with a good operative field without
the constraints of time limitation. By contrast, the
disadvantage of ex vivo repair is the elimination of
collateral blood flow.We speculate that this is one of
the reasons underlying the postoperative segmental
renal infarction at the upper pole.
In addition, we used laser-assisted ICG angio-
graphy to confirm the status of the reconstructed
vessels and the SPY system to verify substantial
renal perfusion. This laser-assisted ICG angiography
system enables fluorescent angiography through
ICG fluorescence (830 nm) by photoradiation laser
at 806 nm.10 The target vessels have been determi-
ned at a resolution of 570 � 485 TV line. Moreover,
this system can observe an area of 75 � 75 mL.
Recently, this system has been used to assess coro-
nary bypass grafts intraoperatively11,12 as well as
vascular reconstruction for parenchymal organ
transplantation.10,13 This technique can also assess
the quality of bypass graft similarly to standard
contrast angiography.14 As compared with contrast
angiography, the advantages of laser-assisted ICG
angiography lie in its ease of setting and avoidance
of nephrotoxicity. The laser-assisted ICG angio-
graphy system can be set up very easily, which
allows extra time to be used for the assessment of
graft patency for about 10 minutes, and there is no
need for any protective clothing. Duplex scanning is
another option for studying anastomosis in patients
with renal insufficiency. This procedure can eva-
luate the main renal artery, but it may become dif-
ficult to evaluate branches to the polar artery.
Moreover, there is a significant training and learn-
ing curve for individuals using duplex scanning,
which is not needed in ICG angiography. However,
laser-assisted ICG angiography also has some limi-
tations. The fluorescence signal is scattered by fat or
muscular tissue and false-positive defects may be
produced. Thus, target vessels should be skeletoni-
zed. Also, it can only visually assess quality of blood
flow. We believe that the combination of laser-
assisted ICG angiography and duplex scanning or
the use of an ultrasonic transit-time flow meter will

894.e8 Cas cliniques Annales de chirurgie vasculaire
complement the limitations of each technique and
enable the evaluation of the morphologic and
functional quality of the reconstruction.
Taken together, laser-assisted ICG angiography is
less invasive for preserving renal function, and
easier to use than angiography with iodine contrast
media. We consider that this technique might be
useful for the intraoperative evaluation of blood
perfusion without impairing renal function.
CONCLUSION
Ex vivo arterial reconstruction of intrahilar RAAs
using anorganpreservation solution is a safemethod
for preserving renal function. In addition, laser-
assisted ICG angiography is useful for the intraope-
rative evaluation of graft anastomosis and organ
blood perfusion without impairing renal function.
The authors are grateful to Assistant Professor Edward F.
Barroga and Professor J. Patrick Barron of the Department of
International Medical Communications of Tokyo Medical
University for reviewing the manuscript.
REFERENCES
1. Charron J, Belanger R, Vauclair R, L�eger C, et coll. Renal
artery aneurysm: polyaneurysmal lesion of kidney. Urology
1975;5:1-11.
2. Hageman JH, Smith RF, Szilagy E, et coll. Aneurysm of the
renal artery: problems of prognosis and surgical manage-
ment. Surgery 1978;84:563-572.
3. Pfeiffer T, Reiher L, Grabitz K, et coll. Reconstruction for
renal artery aneurysm: operative techniques and long-term
results. J Vasc Surg 2003;37:293-300.
4. ThamG, Ekelund L, Herrlin K, et coll. Renal artery aneurysms:
natural history and prognosis. Ann Surg 1983;197:348-352.
5. Henke PK, Cardneau JD, Welling TH 3rd, et coll. Renal
artery aneurysms. A 35-year clinical experience with 252
aneurysms in 168 patients. Ann Surg 2001;234:454-463.
6. PliskinMJ, DresnerML, Hassell LH, et coll. A giant renal artery
aneurysmdiagnosed post partum. J Urol 1990;144:1459-1461.
7. Crutchley TA, Pearce JD, Craven TE, et coll. Branch renal
artery repair with cold perfusion protection. J Vasc Surg
2007;46:405-412.
8. Levy MN. Oxygen consumption and blood flow in the hypo-
thermic, perfused kidney. Am J Physiol 1959;197:1111-1114.
9. Knobloch K, Wiebe K, Lichtenberg A, et coll. Ex vivo repair
and renal autotransplantation for complex renal artery
aneurysms in solitary kidney. Ann Vasc Surg 2005;19:1-4.
10. Sekijima M, Tojimbara T, Sato S, et coll. An intraoperative
fluorescent imaging system in organ transplantation.
Transplant Proc 2004;36:2188-2190.
11. Taggart DP, Choudhary B, Anastasiadis K, et coll. Pre-
liminary experience with a novel intraoperative fluores-
cence imaging technique to evaluate the patency of bypass
grafts in total arterial revascularization. Ann Thorac Surg
2003;75:870-873.
12. Takahashi M, Ishikawa T, Higashidani K, et coll. SPY�: an
innovative intra-operative imaging system to evaluate graft
patency during off-pump coronary artery bypass grafting.
Interact Cardiovasc Thorac Surg 2004;3:479-483.
13. Sanchez EQ, Chinnakotla S, Khan T, et coll. Intraoperative
imaging of pancreas transplant allografts using indocyanine
green with laser fluorescence. Proc (Bayl Univ Med Cent)
2008;21:258-260.
14. Desai ND, Miwa S, Kodama D, et coll. Improving the quality
of coronary bypass surgery with intraoperative angiography.
Validation of a new technique. J Am Coll Cardiol 2005;46:
1521-1525.