Embed Size (px)
Citation preview

Contents lists available at ScienceDirect
J Ped Surg Case Reports 1 (2013) 398e400
Journal of Pediatric Surgery CASE REPORTS
journal homepage: www.jpscasereports.com
Gastroschisis and multiple intestinal perforations in a pretermneonate
Letícia Feldens a,*, Samanta S. da Silva a, Melissa M. Silva a, Maria Lúcia P. Roenick a, Rodrigo Feldens b,Alexandra C. Ponso a, Valentina O. Provenzi a, João Carlos K. de Souza a, Elinês O. Maciel a,João Vicente Bassols a
aHospital da Criança Conceição (HCC), Porto Alegre, RS CEP 91350-200, BrazilbUniversidade Federal de Ciências Médicas de Porto Alegre, Porto Alegre, RS CEP 90050-170, Brazil
a r t i c l e i n f o
Article history:Received 24 September 2013Received in revised form22 October 2013Accepted 22 October 2013
Key words:GastroschisisBowel perforationPremature infant
* Corresponding author. Rua André Puente, 92/31,Alegre, RS CEP 90035-150, Brazil. Tel.: þ55 51 9249 0
E-mail addresses: [email protected](L. Feldens).
2213-5766Published by Elsevier Inc.http://dx.doi.org/10.1016/j.epsc.2013.10.010
Open access under CC B
a b s t r a c t
Several cases of bowel perforation in patients with intestinal atresia have been reported in the literature.Gastroschisis is known to be associated with multiple intestinal perforations. We report the case of apreterm neonate with gastroschisis who presented with bowel lesions consistent with pneumatosisintestinalis, as well as several small bowel perforations, with no associated intestinal atresia. Rupture ofmembranes 18 h before delivery may have contributed to bacterial contamination and consequentdevelopment of bowel perforations and pneumatosis.
Published by Elsevier Inc. Open access under CC BY license.
Several reports of bowel perforation in infants with gastro-schisis have been published in the literature. The characteristicpresentation is a single perforation associated with small bowelatresia. We report a case of numerous small bowel perforations ina preterm infant with gastroschisis, with concomitant pneuma-tosis intestinalis similar to that found in necrotizing enterocolitis(NEC).
1. Case report
A preterm neonate (gestational age 32 weeks, birth weight1495 g), delivered by Cesarean section, presentedwith gastroschisisand multiple bowel perforations not diagnosed on prenatalultrasound.
Themother had completed five prenatal visits, was not a smokerand did not use any illicit drugs. All serologies were negative andthere was no history of prenatal infections, including vaginal
Bairro Independência, Porto857.r, [email protected]
Y license.
streptococcal infection. Two doses of prenatal corticosteroids wereadministered.
Therewasnoonset of labor. Cesareandeliverywasperformeddueto signs of fetal distress and premature rupture of membranes (18 hbefore delivery). The amniotic fluid was stained with meconium.
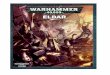
Bowel perforations extended from the duodenum to the ileo-cecal valve. Several areas of pneumatosis intestinalis withimpending perforation were also identified (Figs. 1e4).
Within the first hours of life, surgery was performed, which con-sisted of simple closure of several bowel perforations, small bowelbiopsies, and placement of a silo made from silicone sheets.
The patient remained in critical condition. Despite mechanicalventilation, antibiotic therapy, and vasopressor support, hecontinued to deteriorate and eventually died 48 h after birth.
Postmortem examination revealed transmural necrosis, hem-orrhage, and acute inflammatory reaction in the small bowel.
2. Discussion
A review of the literature yielded only one previous report ofgastroschisis and bowel perforation in the neonatal period. Thepatient described in this report had intestinal atresia and developeda single perforation of the terminal ileum while in utero [1]. Othercases of intestinal perforation in patients with gastroschisis have

Fig. 1. Gastroschisis associated with bowel perforations. Fig. 3. Photomicrograph of a bowel biopsy from the patient, showing edema andinflammatory infiltration (hematoxylineeosin stain, �100 magnification).
L. Feldens et al. / J Ped Surg Case Reports 1 (2013) 398e400 399
been reported in the literature, but most have also been of singleperforation associated with intestinal atresia.
Marked changes in the fetal bowel take place around the 30thweek of pregnancy, when the protein and ferritin levels of amnioticfluid increase, as do levels of inflammatory markers and mono-nuclear cells [2]. In this period, the fetal bowel becomes morepermeable to macromolecules and pathogens.
The multiple perforations and pneumatosis-like lesionsobserved in our patient are suggestive of necrotizing enterocolitis(NEC) developing shortly after delivery. NEC is characterized by aflorid inflammatory reaction that leads to disruption of the intes-tinal mucosal barrier, with subsequent pathogen translocation,inflammation, and tissue injury [3].
The histological hallmarks of NEC are coagulation necrosis andinflammatory reaction. The early stages of NEC are characterized byan inflammatory process that increases blood flow to affected areas.Bacteria cross the mucosal barrier and the byproducts of bacterialmetabolism lead to intramural gas formation (pneumatosis intes-tinalis). As NEC progresses, so does injury to the mucosal andsubmucosal layers, finally extending to all layers of the intestinalwall (transmural involvement). The ischemic bowel wall becomesprogressively thinner and may rupture [3].
Neonates with gastroschisis are known to be susceptible to NEC.It has been suggested that primary defect closure may increase therisk of enterocolitis, perhaps due to increased intra-abdominal
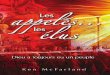
Fig. 2. Bowel lesions similar to necrotizing enterocolitis-associated pneumatosisintestinalis in a neonate with gastroschisis.
pressure, which decreases splanchnic blood flow to bowel loops andconsequently facilitates developmentof bowel ischemia andNEC [4].
The clinical manifestations of NEC tend to develop relatively latein the presence of gastroschisis, as these patients are usually onlyfed after several days of life. Furthermore, the course of NEC is oftencomparatively benign in these patients, and surgical treatment isgenerally not required [4].
Within the first hours of extrauterine life, the neonatal gastro-intestinal tract is exposed to bacteria, particularly those present inthe mother’s vaginal environment [5]. In this case, the history ofrupture of membranes 18 h prior to delivery may have facilitatedbacterial contamination.
However, it remains unclear whether frank invasion by patho-genic bacteria is required for development of NEC or whetheractivation of receptors exposed to bacterial endotoxins andbyproducts is sufficient to trigger bowel inflammation and conse-quent mucosal injury [6].
3. Conclusions
In this premature infant, pre-labor bacterial exposure may haveled to the development of an NEC-like syndrome of bowel mucosalinjury, as, in addition to the intestinal immaturity inherent to
Fig. 4. Appearance of the intestinal villi, showing inflammatory infiltration.

L. Feldens et al. / J Ped Surg Case Reports 1 (2013) 398e400400
preterm birth, the patient had gastroschisis. Prolonged rupture ofmembranes may also have predisposed to bacterial contaminationof the gastrointestinal tract and this uncommonly early develop-ment of the condition.
Although histopathological examination did not show thecoagulation necrosis characteristic of NEC, the gross appearance ofthe patient’s bowel and the presence of multiple perforations werequite consistent with necrotizing enterocolitis. The multiple per-forations in the antimesenteric border were also suggestive ofdiffuse vasospasm, which may have been associated with prema-ture rupture of membranes.
Conflict of interest statementThe authors have indicated they have no conflict of interest
relevant to this article to disclose.
Consent
Written informed consent was obtained from the patient’s nextof kin for publication of this case report and accompanying images.
A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
References
[1] Haberman S, Burgess T, Klass L, Cohn BD, Minkoff HL. Acute bowel perfo-ration in a fetus with gastroschisis. Ultrasound Obstet Gynecol 2000;15:542e4.
[2] Alfaraj MA, Ryan G, Langer JC, Windrim R, Seaward PG, Kingdom J. Does gastricdilation predict adverse perinatal or surgical outcome in fetuses with gastro-schisis? Ultrasound Obstet Gynecol 2011;37:202e6.
[3] Chokshi NK, Guner YS, Hunter CJ, Upperman JS, Grishin A, Ford HR. The role ofnitric oxide in intestinal epithelial injury and restitution in neonatal necrotizingenterocolitis. Semin Perinatol 2008;32:92e9.
[4] Oldham KT, Coran AG, Drongowski RA, Baker PJ, Wesley JR, Polley Jr TZ.The development of necrotizing enterocolitis following repair ofgastroschisis: a surprisingly high incidence. J Pediatr Surg 1988;23:945e9.
[5] Hunter CJ, Upperman JS, Ford HR, Camerini V. Understanding the suscepti-bility of the premature infant to necrotizing enterocolitis (NEC). Pediatr Res2008;63:117e23.
[6] Schnabl KL, Van Aerde JE, Thomson AB, Clandinin MT. Necrotizing enteroco-litis: a multifactorial disease with no cure. World J Gastroenterol 2008;14:2142e61.