Embed Size (px)
Citation preview
SONIA JEAN
INCIDENCE DES FRACTURES AU QUÉBEC ET LEUR SUIVI CLINIQUE
Thèse présentée à la Faculté des études supérieures et postdoctorales de l'Université Laval
dans le cadre du programme de doctorat en epidemiologic pour l'obtention du grade de Philosophiae Doctor (Ph. D.)
DEPARTEMENT DE MEDECINE SOCIALE ET PREVENTIVE FACULTÉ DE MÉDECINE
UNIVERSITÉ LAVAL QUÉBEC
2012
Sonia Jean, 2012

Résumé Les fractures associées à l'ostéoporose constituent un problème de santé publique majeur,
affectant chaque année un nombre croissant d'individus. Le fardeau de ces fractures est non
seulement important en raison de la mortalité et de la morbidité associées à ces fractures,
mais aussi à cause des coûts de soins de santé qui y sont reliés. Dans ce contexte, le
développement d'outils en matière de surveillance de ces fractures s'est révélé essentiel.
Les travaux de cette thèse de doctorat ont pour but d'évaluer la faisabilité de l'utilisation
des données recueillies dans le fichier des services rémunérés à l'acte de la Régie de
l'assurance maladie du Québec (RAMQ) pour l'identification des cas incidents de fracture,
d'établir un portrait populationnel des fractures chez les femmes de 50 ans et plus et de
quantifier leurs impacts en termes de mortalité et d'utilisation des ressources des soins de
santé.
Pour atteindre cet objectif, une première étude rétrospective utilisant le fichier des services
rémunérés à l'acte de la RAMQ nous a permis de vérifier et de comparer l'exactitude de
plusieurs algorithmes utilisés pour l'identification des cas incidents de fracture. Les
résultats de cette étude montrent que l'utilisation de ce fichier pour identifier les cas
incidents de fracture est réalisable. De plus, l'excellente validité de l'algorithme sélectionné
permet d'obtenir des estimateurs précis et valides de l'occurrence des fractures dans la
population.
À l'aide de l'algorithme validé et le jumelage des données provenant des fichiers médico-
administratifs, deux autres études ont été réalisées afin de quantifier les taux d'incidence
des fractures, d'évaluer leurs impacts sur la survie des patientes de 50 ans et plus, et
d'estimer l'utilisation des ressources médicales dans l'année suivant la fracture. Selon les
résultats de ces études, les fractures de fragilisation sont fréquentes chez les femmes de 50
ans et plus. Les fractures de la hanche, du fémur et du bassin sont plutôt rares avant l'âge de
70 ans, mais augmentent substantiellement après cet âge. Tel que prévisible, ces fractures
ont un impact important sur la survie des patientes, lequel peut persister plusieurs années
après la fracture. De plus, ces fractures nécessitent le recours à de nombreuses ressources
médicales puisqu'une grande proportion des femmes présentant ce type de fracture sont
11
hospitalisées. Finalement, nous avons également observé que les · autres fractures
périphériques surviennent fréquemment après l'âge de 50 ans et que certaines de ces
fractures ont aussi un impact sur la survie des patientes. De plus, l'utilisation des ressources
médicales associées aux traitements des fractures périphériques est non négligeable tant sur
le plan des soins cliniques liés aux traitements chirurgicaux et aux consultations médicales,
que sur le plan des hospitalisations.
En conclusion, les résultats de nos travaux montrent qu'il est possible d'utiliser le fichier
des services rémunérés à l'acte de la RAMQ pour effectuer le repérage des cas incidents de
fracture dans la population. L'algorithme développé permet d'élargir la surveillance des
fractures pour englober non seulement les fractures de la hanche, mais aussi 1' ensemble des
sites de fractures associées à 1' ostéoporose. De plus, la méthodologie utilisée, qui repose sur
l'utilisation de l'algorithme validé et le jumelage des données médico-administratives,
permet non seulement d'obtenir des indicateurs sur la prévalence, l'incidence et la
mortalité, mais offre également l'opportunité d'élargir la surveillance à d'autres indicateurs
tels que ceux qui concernent l'utilisation des services de santé. Par conséquent, nous
pouvons conclure que cette méthode permet d'obtenir, de manière efficace et peu coûteuse,
des indicateurs d'une grande qualité, tout en offrant l'opportunité d'effectuer de façon
continue une surveillance populationnelle des fractures au Québec.
Sonia Jean, M.Sc. Sylvie Dodin, M.D., M.Sc.
Directrice
I l l
Abstract Osteoporosis-related fractures represent a major public health problem that is affecting an
increasing number of individuals every year. The burden of these fractures is heavy because
of their association with excess mortality, morbidity and healthcare costs. The development
of fracture surveillance capabilities is therefore essential.
The aims of this thesis were to assess the feasibility of analyzing data collected from a
physician-billing claims database (Régie de Vassurance-maladie du Québec, RAMQ) to
identify incident fracture cases, to establish a population-based description of fractures in
women 50 years of age or older, and to quantify their impact on mortality as well as
healthcare resource utilization.
To achieve our goals first, a retrospective study of the RAMQ physician-billing claims
database compared the accuracy of several algorithms in detecting incident fracture cases.
The results show that the use of this file for fracture case identification is feasible.
Moreover, the excellent validity of the algorithm selected provided accurate and well-
founded estimators of fracture occurrence in the population of women 50 years and over.
Two other studies were performed, with the validated algorithm and linkage of health-
administrative databases, to quantify fracture incidence rates, to evaluate their impact on
patient survival and to assess the health resource utilization in the year after fracture. Our
findings reveal that fragility fractures are common in women 50 years of age or older. Hip,
femur and pelvis fractures are rare before 70 years of age but increase substantially
thereafter. As expected, these fractures have a significant impact on patient survival that
can persist for several years thereafter. They require considerable medical resources since a
large proportion of cases are hospitalized. Finally, according to the results of our studies,
other peripheral fractures occur frequently after the age of 50 years, and some of them
determine patient survival. Moreover, health resource utilization linked with the treatment
of peripheral fractures is significant in terms of clinical care related to surgery, medical
consultations and hospitalizations.
lV
In conclusion, our results show that it is possible to exploit RAMQ physician-billing daims
database to fmd incident fracture cases in the population of women over 50 years of age.
The algorithm developed allows fracture surveillance to be expanded beyond hip fractures
to ali fracture sites related to osteoporosis. Methodology based on the validated algorithm
and the linkage of administrative healthcare databases provides not only indicators of
prevalence, incidence and mortality, but also offers the opportunity to extend scrutiny to
other indicators, such as health resource utilization. Our studies lead us to conclude that this
method offers indicators of high quality, efficiently and inexpensively, with the possibility
of performing continuo us population-based fracture surveillance in Que bec.
Sonia Jean, M.Sc. Sylvie Dodin, M.D., M.Sc.
Director
Avant-Propos La réalisation de cette thèse n'aurait pu être concevable sans l'aide, l'encadrement,
l'encouragement et l'amitié de plusieurs personnes.
En premier lieu, je désire remercier mes directeurs de thèse, les docteurs Sylvie Dodin,
Jacques P. Brown et Bernard Candas qui m'ont conjointement dirigée tout au long de mon
doctorat. Mes remerciements les plus chaleureux vont d'abord au Dr Brown qui m'a
accordé le privilège de travailler à ses côtés pour réaliser mes travaux de doctorat. Son
expertise scientifique mondialement reconnue, ses commentaires judicieux, son attention
soutenue, sa générosité et sa compréhension ont fait de ce projet une expérience formatrice
et enrichissante. Je tiens à lui exprimer ma reconnaissance pour m'avoir offert l'opportunité
d'explorer la recherche scientifique, d'avoir eu confiance en mes capacités et de m'avoir
soutenue pendant toutes ces années. Ma profonde gratitude va également au Dr Candas
pour ses conseils avisés. Grâce à sa rigueur, à sa minutie et à son sens du travail bien fait, il
a été pour moi une référence essentielle. Ce fut pour moi un réel plaisir de le côtoyer tant au
niveau scientifique que personnel. Je tiens également à remercier infiniment la Docteure
Dodin pour son encadrement, ses conseils judicieux et son sens pédagogique qui m'ont
permis de trouver la force de mener à terme ce projet. Je considère avoir reçu une formation
étayée et avoir développé plusieurs qualités scientifiques, et pour cela, je leur serai toujours
reconnaissante.
J'adresse également mes remerciements aux Docteurs Louis Bessette, Etienne Belzile et
Suzanne Morin pour leurs pertinents commentaires. En effet, ils ont toujours pris le temps
de m'aider dans la réalisation de ce projet et de répondre à mes nombreuses interrogations.
Je tiens à leur faire part de ma gratitude pour avoir partagé avec moi leurs savoirs
scientifiques.
Je ne manquerai pas de remercier ma collègue de travail, madame Julie Parrot, pour son
aide technique. Au fil du temps, elle est devenue une amie et a été pour moi d'un grand
soutien moral. J'aimerais lui faire part de toute mon admiration pour son côté très humain et
la remercier pour les nombreuses discussions que nous avons échangées, et aussi pour sa
grande écoute.
VI
Je ne saurai passer sous silence l'appui de mes supérieurs à l'Institut national de santé
publique du Québec (INSPQ) et encore moins celui des chercheurs du programme
Reconnaître l'ostéoporose et ses conséquences au Québec (ROCQ) pour leurs supports
financiers. Grâce à leur soutien, j 'ai pu réaliser ce projet dans des conditions optimales.
Enfin, je remercie mon conjoint, Stéphane Bizier, pour sa compréhension malgré les
concessions et les contraintes qu'il a souvent dû subir durant la réalisation de ce projet, tout
comme je tiens à remercier ma famille et mes trois garçons, Raphaël, Mathieu et Olivier qui
sont souvent perplexes de me voir encore aux études.
vu
A Stéphane, et mes enfants Raphaël, Mathieu et Olivier

IX
Table des matières
RÉSUMÉ I
ABSTRACT m
AVANT-PROPOS v
LISTE DES TABLEAUX xi
LISTE DES FIGURES xm
ABRÉVIATIONS xv
INTRODUCTION 1
CHAPITRE 1 : REVUE DE LA LITTÉRATURE 5
1.1 OSTÉOPOROSE 7
1.2 FRACTURE DE FRAGILISATION 8
1.2.1 Définition 8 1.2.2 Prévalence et incidence des fractures de fragilisation 10 1.2.3 Fractures de la hanche 10 1.2.4 Autres fractures de fragilisation 12 1.2.5 La cascade des fractures 13 1.2.6 Conséquences des fractures de fragilisation 14 1.2.7 Évaluation du risque de fracture 16 1.2.8 Prise en charge 18 1.2.9 Progression et coût des fractures ostéoporotiques 19 1.2.10 Trajectoires cliniques 19 1.2.11 Suivi après une fracture 22
1.3 L E RÔLE DE LA SANTÉ PUBLIQUE 23
1.4 SURVEILLANCE DES FRACTURES DE FRAGILISATION 24
CHAPITRE 2 31
2.1 RÉSUMÉ 33
2.2 ABSTRACT 34
2.3 INTRODUCTION 35
2.4 STUDY DESIGN AND SETTING 36
2.4.1 Study Design 36 2.4.2 Data sources 37 2.4.2 Development and validation of algorithms 40 2.4.2 Assessing the performance ofthe algorithms 43
2.5 RESULTS 43
2.6 CONCLUSION 52
2.7 ACKNOWLEDGMENTS 54
CHAPITRE 3 57
3.1 RÉSUMÉ 59
3.2 ABSTRACT 61
3.3 INTRODUCTION 63
3.4 M E T H O D S 64
3.4.1 Data Sources 64 3.4.2 Identification of fracture cases 65 3.4.3 Statistical analysis 66
3.5 R E S U L T S 68
3.5.1 Fracture incidence rates 68 3.5.2 Fracture associated mortality 72
3.6 DISCUSSION 78
3.7 ACKNOWLEDGMENTS 83
CHAPITRE 4 85
4.1 R É S U M É 87
4.2 ABSTRACT 89
4.3 INTRODUCTION 90
4.4 M A T E R I A L S AND M E T H O D S 91
4.4.1 Study Cohort and Design 91 4.4.2 Data Sources 91 4.4.3 Identification of incident fracture cases 92 4.4.4 Identification of health resources used 93 4.4.5 Assessment ofthe direct medical resources utilization 95
4.5 RESULTS 96
4.6 DISCUSSION I l l
4.7 ACKNOWLEDGMENTS 114
CHAPITRE 5 CONCLUSIONS GÉNÉRALES ET PERSPECTIVES 115
5.1 CONCLUSIONS GÉNÉRALES 117
5.2 PERSPECTIVES 121
BIBLIOGRAPHIE 125
Appendix 1 : Medical services billing and ICD-9 codes selected in the physician claims database 139
Appendix 2: Predictive positive value by fracture site and type of medical service billing code 149
Appendix 3: Classification of primary diagnostic codes at hospitalization observed in Med-Echo 151
Appendix 4: Classification of procedure intervention codes at hospitalization observed in Med-Echo 153
Appendix 5: Selection of hospital admissions8 155
XI
Liste des tableaux
Table 2.1 Table 2.2
Table 2.3 Table 2.4
Table 2.5 Table 2.6
Table 3.1
Table 3.2
Table 3.3 Table 3.4 Table 3.5 Table 3.6 Table 4.1
Table 4.2 Table 4.3
Table 4.4
Table 4.5
Criteria for identification of fracture cases 42 Baseline characteristics of women identified by algorithm 1 and subsets from the administrative database and the ROCQ cohort 46 Positive predictive value ofthe algorithms by fracture site and index claim 48 Concordance between actual anatomical site of fracture reported in the medical chart and site identified via algorithm three 49 Sensitivity ofthe algorithms by fracture site 51 Relative performance of algorithms using likelihood ratios graphs for comparison 52 Distribution and median age at fracture and crude and age-standardized rates, by fracture site 69 Age-specific fracture rates among women > 50 years of age, by fracture site/grouping 71 Median follow-up time (years) and crude mortality rate 72 Relative survival by fracture site at 12, 24, 36 and 48 months 73 Potential YLL, Average YLL and YLL proportion of Years of life lost 77 RRand 95% CI of mortality in 4 years after fracture 79 Distribution of fragility fracture sites identified by algorithm and respective median age at fracture 98 Distribution of claims by fracture type 100 Health resource utilization related to treatment and medical consultation and rate of hospital stay in the year after the osteoporosis-related fracture 101 Health resource utilization related to hospitalization in the year after osteoporosis-related fracture 104 Discharge destination at final admission according to resident status at initial admission 106
xm
Liste des figures Figure 1.1 Taux d'incidence des fractures de la hanche en Ontario 1996/97 11 Figure 2.1 Description of selection of fee-for-service claims in physician-billing
claims databases 39 Figure 2.2 Description of steps used for validation study 45 Figure 3.1 Age-specific incidence rate of fracture, by fracture site 70 Figure 3.2 Relative survival by fracture site 76 Figure 4.1 Selection of fracture cases by RAMQ algorithm 98 Figure 4.2 Fracture treatments by age groups 108 Figure 4.3 Health resource utilization by age groups 109 Figure 4.4 Discharge destinations after hospitalization by age groups 110 Figure 5.1 Fichiers utilisés pour la surveillance des maladies chroniques 122
XV
Abréviations ASBMR American Society for Bone and Minerai Research
CAI Commission d'accès à l'information
CAROC Association canadienne des radiologistes et Ostéoporose Canada
CHMD Canadian Human Mortality Database
CHUQ Centre hospitalier universitaire de Québec
DMO Densité minérale osseuse
EP Emergency physician
FF Fragility fracture
FRAX Fracture risk assessment Tool
GP General Practitioner
ICD-9-CM International classification of diseases, Clinical Modification - 9 Revision
MSSS Ministère de la Santé et des Services sociaux du Québec
OCDE Organisation de coopération et de développement économique
OMS Organisation mondiale de la santé
OS Orthopaedic surgeon
PCD Physician-billing claims database
PMSM Plan ministériel de surveillance multithématique
PPV Positive predictive value
RAMQ Régie de l'assurance maladie du Québec
ROCQ Reconnaître l'ostéoporose et ses conséquences au Québec
Sn Sensitivity
VPP Valeur prédictive positive
YLL Years of life lost
Introduction L'ostéoporose et les fractures qui lui sont associées constituent un problème majeur de
santé publique touchant aussi bien les femmes que les hommes, et dont la prévalence
augmente parallèlement au vieillissement de la population [1]. Au Canada, 15,8% des
femmes de 50 ans et plus et 6,6 % des hommes souffrent d'ostéoporose [2].
L'ostéoporose est une maladie squelettique caractérisée par une faible masse osseuse et par
la détérioration du tissu osseux [3]. L'ostéoporose est traditionnellement perçue comme un
diagnostic clinique posé à la suite d'une mesure de la densité minérale osseuse trop faible.
On ignore ainsi que le principal indicateur de l'ostéoporose est la survenue d'une fracture
de fragilisation, c'est-à-dire une fracture occasionnée par un traumatisme de faible énergie,
par exemple une chute de sa propre hauteur, qui n'aurait pas causé de fracture chez une
personne dont les os sont sains.
Les fractures ostéoporotiques se manifestent essentiellement à partir de 50 ans et, passé cet
âge, elles représentent 81 % de l'ensemble des fractures [4]. Ainsi, quatre fractures sur cinq
sont une manifestation clinique d'ostéoporose associée à un risque élevé de fracture
subséquente. Quoique les conséquences de ces fractures, en termes de morbidité et de
mortalité, soient clairement démontrées, 80 % d'entre-elles ne seront accompagnées ni d'un
diagnostic, ni d'un traitement adéquat [4], et ainsi, ne bénéficieront pas d'une prise en
charge adéquate. Pourtant, la présence d'une première fracture de fragilisation mineure,
telle que la fracture du poignet, double le risque de présenter ultérieurement une fracture
majeure de la hanche [5].
Après 50 ans, 50 % des femmes et 20 % des hommes subiront une fracture associée à
l'ostéoporose au cours de leur vie [6-9]. Toujours après cet âge, pour une femme, le risque
à vie de subir une fracture du poignet, des vertèbres (cliniquement diagnostiquée) ou de la
hanche sont respectivement de 16,0 %, 15,6 % et 17,5 %. Le risque de fracture de la hanche
est donc supérieur aux risques combinés de développer un cancer du sein, de l'utérus ou de
l'ovaire [6].
Dans le domaine des soins de la santé, les fractures associées à l'ostéoporose constituent
non seulement un important facteur de décès et de morbidité, mais aussi, une source
appréciable de dépenses. En effet, environ 20 % des femmes et 30 % des hommes
décéderont dans l'année suivant la survenue d'une fracture de la hanche [10]. Un an plus
tard, 40% des personnes ayant survécu à ces fractures seront toujours incapables de marcher
sans aide et 60 % d'entre-elles auront besoin d'aide pour accomplir leurs activités
quotidiennes [11].
Les fractures associées à l'ostéoporose sont l'une des principales raisons d'hospitalisation
et de transfert dans un établissement de soins de longue durée [12]. Après les troubles
mentaux, la fracture de la hanche, la fracture des vertèbres et les autres fractures sont
respectivement les 2e, 3e et 4e causes d'hospitalisations qui nécessitent les plus longs séjours
[13]. Parmi les patients qui obtiennent leur congé de l'hôpital, à la suite d'une fracture de la
hanche, seulement 44 % d'entre-eux retourneront à la maison, 10 % seront transférés dans
un autre hôpital, 27 % iront dans un établissement de réadaptation et 17 % iront dans un
établissement de soins de longue durée [14]. Au Canada, les coûts des soins actifs
(hospitalisations, soins ambulatoires, médicaments et soins de longue durée) associés aux
fractures liées à l'ostéoporose ont atteint 1,3 milliard de dollars en 1993 [15]. Par
conséquent, l'ampleur de ce problème ainsi que ses conséquences méritent une surveillance
continue à partir de 50 ans.
Depuis une quinzaine d'années, les fractures liées à l'ostéoporose survenant à partir de
l'âge de 50 ans ont enregistré de nombreuses évidences cliniques qui plaident en faveur
d'une surveillance accrue. Cependant, ces fractures ne sont que très peu intégrées dans des
plans de surveillance populationnels. Il devient donc primordial de réaliser des études
épidémiologiques à caractère populationnel afin d'évaluer l'importance du fardeau de ces
fractures au Québec et d'estimer leurs impacts sur le système de santé. Ces études
permettront de développer des indicateurs de surveillance pour suivre l'évolution de ce
problème de santé et, éventuellement, d'évaluer l'efficacité de la mise en place
d'interventions favorisant la prévention (primaire, secondaire et tertiaire) ainsi que la prise
en charge optimale de cette maladie.
Les données médico-administratives, comme celles provenant du fichier des services
médicaux rémunérés à l'acte de la RAMQ, peuvent être très utiles pour la réalisation
d'études épidémiologiques populationnelles portant sur les fractures. En effet, des études
ont montré que les données médico-administratives ont un niveau élevé de fiabilité et de
validité [16, 17] et leur jumelage fournit une source puissante d'information pour étudier les
issues de santé comme le fardeau des maladies et l'utilisation des ressources du système de
santé. Par conséquent, l'utilisation des données provenant du fichier des services médicaux
rémunérés à l'acte de la RAMQ peut permettre la production d'estimateurs fiables de la
prévalence et de l'incidence des fractures associées à l'ostéoporose dans la population. Ces
données peuvent également permettre d'évaluer les trajectoires cliniques et l'utilisation des
ressources médicales du système de soins de santé.
Au Québec, aucune étude, à ce jour, n'a eu recours aux données provenant du fichier des
services rémunérés à l'acte de la RAMQ pour examiner l'impact des fractures liées à
l'ostéoporose sur la santé des populations et sur le système de santé. Par conséquent, les
travaux présentés dans le présent document ont pour but d'évaluer, dans un premier temps,
la fiabilité des données recueillies dans le fichier de la RAMQ pour l'identification des cas
incidents de fracture et, par la suite, établir un portrait populationnel des fractures chez les
femmes de 50 ans et plus et de quantifier leur impact. La réalisation de ce projet sera donc
une première étape vers la mise en place d'un système de surveillance continu des fractures
ostéoporotiques au Québec.
Chapitre 1 : Revue de la littérature
1.1 Ostéoporose L'Organisation mondiale de la santé (OMS) définit l'ostéoporose comme étant « une
maladie squelettique caractérisée par une faible masse osseuse accompagnée d'une
détérioration de la microarchitecture du tissu osseux ayant pour conséquence la fragilité
osseuse et la susceptibilité de subir une fracture de fragilisation » [3]. L'ostéoporose est
classée en deux catégories : primaire et secondaire. L'ostéoporose primaire est
principalement causée par l'âge et une diminution de la sécrétion des estrogènes
(hypoestrogénie) chez la femme [18]. L'ostéoporose primaire est la forme la plus commune
et représente la majorité des cas chez les individus de plus de 70 ans [18]. L'ostéoporose
secondaire est plutôt causée par la prise de certains médicaments (héparine,
glucocorticoïdes) ou par la présence d'autres maladies entraînant la perte osseuse
(syndromes de malabsorption, myélome multiple, insuffisance rénale, arthrite rhumatoïde,
hyperparathyroïdie) [18]. D'autres facteurs peuvent également avoir un impact sur la perte
osseuse. Ces facteurs se caractérisent par une carence en calcium et en vitamine D, une
mauvaise alimentation, un manque d'exercice physique, et par le tabagisme et la
consommation excessive de caféine et d'alcool [19].
L'ostéoporose est une maladie silencieuse sans douleur qui peut se développer sur plusieurs
années. Elle survient plus souvent chez les femmes puisque celles-ci ont une masse osseuse
plus faible que celles des hommes, et ce, à tout âge et qu'il n'y a pas d'équivalent à la
ménopause chez l'homme [20]. Cependant, l'ostéoporose et ses conséquences touchent
également les hommes [21].
Selon une définition récente de l'ostéoporose par les « National Institutes of Health », la
résistance osseuse dépend à la fois de la densité et de la qualité des os [22]. Actuellement,
par manque de méthodes d'évaluation de la qualité des os, la mesure de la densité minérale
osseuse (DMO) est utilisée pour poser le diagnostic de l'ostéoporose. Selon les critères
établis par un groupe de travail de l'OMS, l'ostéoporose est opérationnellement définie par
une valeur de DMO de plus de 2,5 écarts types en dessous de la valeur moyenne des jeunes
femmes adultes [23, 24]. Si l'ostéoporose, telle que définie ci-dessus, s'accompagne d'une
ou de plusieurs fractures de fragilisation, on parlera alors d'ostéoporose sévère [23, 24]. Au
Canada, l'ostéoporose est un problème de santé publique majeur dont la prévalence
augmente avec le vieillissement de la population [1]. Selon l'Étude canadienne
multicentrique sur l'ostéoporose, la prévalence de cette affectation chez les femmes de plus
de 50 ans s'établit à 15,8 % alors que la prévalence chez l'homme est de 6,6 % [2].
Le fardeau de l'ostéoporose tant au plan clinique qu'au plan de la santé publique est associé
à la survenue des fractures de fragilisation causées par cette affection. Bien que le risque de
fracture augmente exponentiellement avec la diminution de la DMO, la plupart des
fractures de fragilisation surviennent chez des patients ne présentant pas les critères
d'ostéoporose tels qu'établis par l'OMS [25]. D'autres facteurs de risque comme l'âge, la
présence d'un antécédent personnel de fracture de fragilisation après l'âge de 40 ans,
l'existence d'une histoire familiale d'ostéoporose et un emploi prolongé de corticostéroïdes
augmentent le risque de subir une fracture de fragilisation et ce, indépendamment de la
densité minérale osseuse [26-28]. En octobre 2010, la société d'ostéoporose du Canada, lors
de sa dernière réunion consensuelle, proposait un nouveau paradigme dans la prévention et
le traitement de l'ostéoporose et des fractures de fragilisation. Dorénavant, l'accent sera mis
sur la prévention des fractures et de leurs conséquences plutôt que sur le traitement d'une
faible densité minérale osseuse, considérée comme étant un facteur de risque parmi
plusieurs [25, 29]. Une approche intégrée, prenant en compte la combinaison des facteurs
de risque clinique et la DMO, est désormais utilisée pour calculer la probabilité de fracture
à 10 ans, favorisant ainsi l'évaluation du risque global de fracture. Cette approche augmente
donc notre capacité à identifier les individus à haut risque de fracture et aide à mieux
orienter les décisions thérapeutiques.
1.2 Fracture de fragilisation 1.2.1 Définition
Définir une fracture de fragilisation n'est pas simple. Une première approche, largement
adoptée pour identifier les fractures de fragilisation, est de considérer les circonstances
ayant conduit à la fracture. Selon ce critère, une fracture de fragilisation est occasionnée par
un traumatisme faible qui n'aurait normalement pas causé de fracture chez une personne
ayant des os sains (par exemple une fracture à la suite d'une chute de sa propre hauteur)
[30]. Selon une récente étude québécoise, chez les femmes de 50 ans et plus, les fractures
de fragilisation associées à un faible traumatisme représentent 81 % de l'ensemble des
fractures [4]. Ainsi, selon cette définition, plus de quatre fractures sur cinq se trouvent être
un signe clinique évident d'ostéoporose.
On peut également définir la fracture de fragilisation de façon plus pragmatique; une
fracture survenant à un site anatomique dont la fréquence de survenue augmente avec l'âge
et la baisse de la DMO [31]. Une étude récente, basée sur une synthèse de la littérature et
sur l'évaluation d'un groupe d'experts, utilise l'association entre la DMO et le risque de
fracture subséquente pour définir une fracture de fragilisation [32]. Selon ces différents
critères, les fractures de fragilisation chez les femmes sont les fractures de la colonne
vertébrale (par écrasement), des côtes, du bassin, de l'humérus, de l'avant-bras, de la
hanche, du péroné, du tibia, de la cheville, de la clavicule, de l'omoplate, du sternum et les
autres fractures fémorales. Les fractures de fragilisation chez l'homme touchent les mêmes
sites, à l'exception des fractures du péroné et du tibia. Ainsi, les fractures au visage, à la
tête, à la colonne cervicale, à la main, et au pied sont classées comme étant non
ostéoporotiques.
Dans les études populationnelles utilisant les bases de données administratives comme
celles du fichier des services médicaux rémunérés à l'acte de la RAMQ, il n'est pas
possible d'identifier les circonstances ayant conduit à la fracture. Par conséquent,
l'identification des fractures de fragilisation doit se baser sur la deuxième définition et
considérer l'ensemble des fractures (à traumatisme faible et élevé) survenant à ces sites
anatomiques, dont la majorité sont des fractures de fragilisation (81 % de l'ensemble des
fractures [4]). De plus, dans les études populationnelles, il a été récemment proposé de
considérer également les fractures causées par un traumatisme élevé puisqu'elles sont
également associées à une diminution de la DMO et augmentent le risque de subir une
fracture subséquente [33].
De façon similaire, il a été également suggéré de ne pas exclure les fractures pathologiques
puisqu'elles ne représentent qu'une faible proportion de l'ensemble des fractures et leur
exclusion pourrait conduire à une sous-estimation du fardeau associé aux fractures
ostéoporotiques [34].
10
1.2.2 Prévalence et incidence des fractures de fragilisation
L'obtention de données fiables sur l'incidence des fractures chez les personnes de 50 ans et
plus est un point de départ important pour quantifier l'importance de l'ostéoporose tant sur
le plan social que sur le plan économique, même s'il est reconnu que certaines fractures ne
sont pas reliées à l'ostéoporose [35]. Ces données permettent de suivre l'évolution de ce
problème de santé publique et constituent des renseignements de base importants
permettant d'évaluer l'impact de la mise en place d'interventions favorisant une prise en
charge optimale de l'ostéoporose et des fractures de fragilisation.
En 2000, une projection mondiale estimait le nombre de fractures de fragilisation à 9
millions, dont 1,6 million se situaient au niveau de la hanche, 1,7 million à l'avant-bras et
1,4 million étaient des fractures vertébrales [36]. À partir de l'âge de 50 ans, entre 40 % et
50 % des femmes blanches subiront une fracture de fragilisation au cours de leur vie [6-9].
Toujours après cet âge, Melton et al. estimaient, en 1993, que le risque à vie de subir une
fracture du poignet, des vertèbres (cliniquement diagnostiquée) ou de la hanche était
respectivement de 16 %, 15,6 % et 17,5 % [6]. Au Canada, on a estimé, sur la base des
tables de survie, que le risque à vie du subir une fracture de la hanche sur la même période
est de 14,0 % chez la femme et de 5,2 % chez l'homme [37, 38].
1.2.3 Fractures de la hanche
Les fractures de la hanche ont été davantage étudiées dans la littérature puisqu'elles sont
associées à une mortalité et une morbidité importantes. Elles constituent une sorte de
baromètre international de l'ostéoporose car elles sont fortement associées à une faible
DMO [39]. D'autre part, comme elles entraînent quasi systématiquement une
hospitalisation, elles sont plus faciles à dénombrer, et peuvent donc facilement faire l'objet
de comparaisons d'un pays à l'autre [39]. En 2007, il y a eu 28 000 hospitalisations pour
une fracture de la hanche au Canada [40]. Selon une projection mondiale, le nombre de cas
incidents de fractures de la hanche passera de 1,26 million en 1990 à 2,6 millions en 2025
[41].
Au Canada, quelques études ont évalué l'incidence des fractures de la hanche mais ces
études se sont limitées à quelques provinces [1, 14, 38]. Selon une étude réalisée au
11
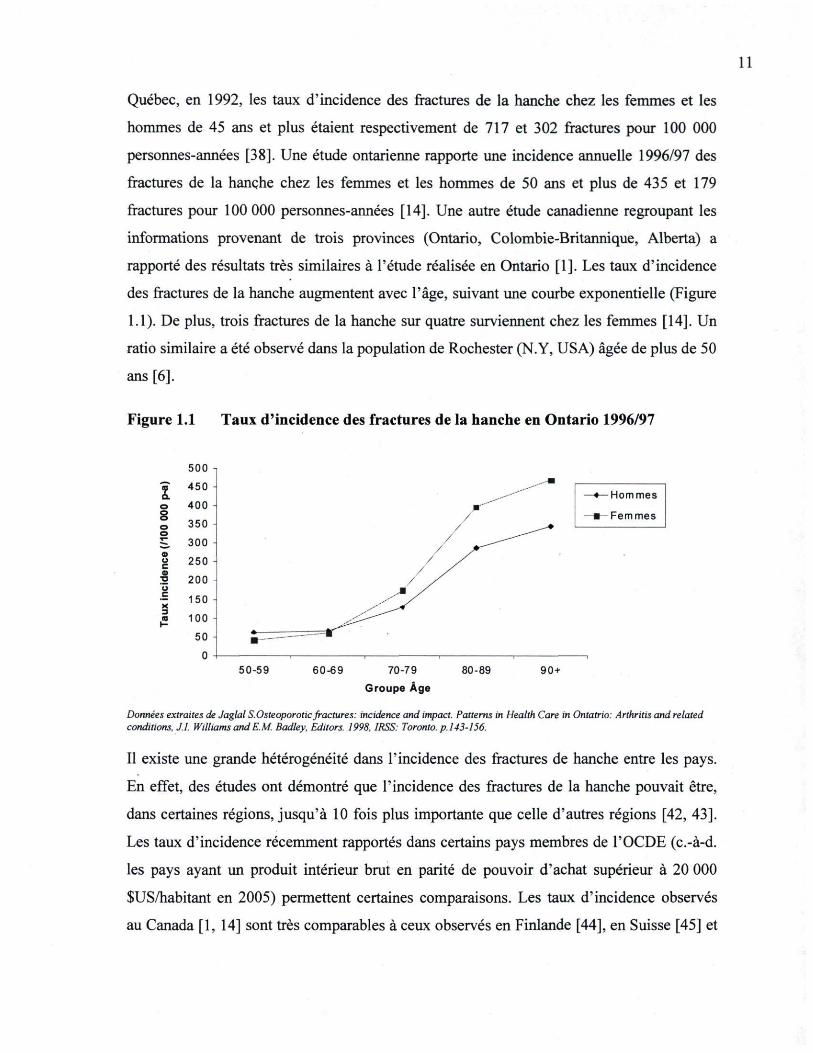
Québec, en 1992, les taux d'incidence des fractures de la hanche chez les femmes et les
hommes de 45 ans et plus étaient respectivement de 717 et 302 fractures pour 100 000
personnes-années [38]. Une étude ontarienne rapporte une incidence annuelle 1996/97 des
fractures de la hanche chez les femmes et les hommes de 50 ans et plus de 435 et 179
fractures pour 100 000 personnes-années [14]. Une autre étude canadienne regroupant les
informations provenant de trois provinces (Ontario, Colombie-Britannique, Alberta) a
rapporté des résultats très similaires à l'étude réalisée en Ontario [1]. Les taux d'incidence
des fractures de la hanche augmentent avec l'âge, suivant une courbe exponentielle (Figure
1.1). De plus, trois fractures de la hanche sur quatre surviennent chez les femmes [14]. Un
ratio similaire a été observé dans la population de Rochester (N-Y, USA) âgée de plus de 50
ans [6].
Figure 1.1 Taux d'incidence des fractures de la hanche en Ontario 1996/97
500 -i f 450 -a. o 400 -S o 350 -o ~_ 300 -o o 250 -o •a 200 -o c X 3
150 -c X 3 (0 100 -H
50 -0
♦—■Hommes
■—Femmes
50-59 60-69 7079
Groupe Âge
80-89 90 +
Données extraites de Jaglal S.Osleoporotic fractures: incidence and impact. Patterns in Health Care in Ontatrio: Arthritis and related conditions, JJ. Williams and EM. Badley. Editors. 1998, IRSS: Toronto, p. 143-156.
Il existe une grande hétérogénéité dans l'incidence des fractures de hanche entre les pays.
En effet, des études ont démontré que l'incidence des fractures de la hanche pouvait être,
dans certaines régions, jusqu'à 10 fois plus importante que celle d'autres régions [42, 43].
Les taux d'incidence récemment rapportés dans certains pays membres de l'OCDE (c.-à-d.
les pays ayant un produit intérieur brut en parité de pouvoir d'achat supérieur à 20 000
$US/habitant en 2005) permettent certaines comparaisons. Les taux d'incidence observés
au Canada [1, 14] sont très comparables à ceux observés en Finlande [44], en Suisse [45] et
12
aux États-Unis [46], mais plus bas que ceux observés au Danemark [47], en Norvège [48],
en Australie [49] et en Espagne [50]. De façon générale, les gens vivant en latitude plus
nordique par rapport à l'équateur avaient une incidence de fractures de la hanche plus
élevée [49].
Plusieurs études réalisées dans les années 80 et 90 rapportent une augmentation de
l'incidence des fractures de la hanche après standardisation des taux d'incidence selon la
distribution d'âge [46, 47, 51-53]. Cependant, d'autres études, dont une récente étude
canadienne, réalisée en 2009 observent plutôt une diminution de l'incidence des fractures
de la hanche standardisée pour la distribution d'âge [44-46, 49, 54-57]. De 1985 à 2005,
l'étude la plus récente rapporte une diminution de l'incidence des fractures de la hanche de
31,8 % chez la femme (de 118,6 à 80,9 fractures par 100 000 personnes-années) et 25,0 %
chez l'homme (de 68,2 à 51,1 fractures par 100 000 personnes-années). Plusieurs facteurs
peuvent expliquer ces changements. Une utilisation plus répandue des mesures préventives
comme l'évaluation de la densité minérale osseuse et l'arrivée des traitements pour
l'ostéoporose peuvent expliquer en partie ces changements. Une étude Ontarienne, évaluant
l'utilisation des tests diagnostiques (c.-à-d. mesure de la densité minérale osseuse par
ostéodensitométrie), rapporte une augmentation de l'utilisation de ce test entre 1992 et 2001
[54]. Ces auteurs ont également observé une augmentation constante de l'utilisation des
médicaments approuvés pour le traitement de l'ostéoporose de 1996 à 2003. Au Canada,
ces médicaments ont été introduits sur le marché en 1996. D'autres facteurs comme
l'augmentation de l'activité physique, la consommation de calcium et de vitamine D, ou les
programmes de prévention des chutes peuvent également expliquer en partie la diminution
de l'incidence des fractures de la hanche observée [58-61]. Finalement, la diminution du
nombre de fumeurs et l'augmentation de l'obésité sont également des facteurs susceptibles
d'avoir contribué à la diminution du nombre de fractures de la hanche observée [62-64].
1.2.4 Autres fractures de fragilisation
La littérature médicale consacre une attention particulière aux fractures de la hanche, des
vertèbres, du poignet et de l'humérus proximal car ces sites sont très majoritairement et
traditionnellement perçus comme étant associés à l'ostéoporose. On retrouve, cependant,
quelques études ayant examiné l'incidence des fractures pour l'ensemble des sites associés
13
à l'ostéoporose [48, 65, 66, 67]. Selon ces études, les quatre sites de fractures les plus
fréquents sont la hanche, les vertèbres, le poignet et l'humérus. Selon une estimation
récente de la distribution de l'incidence des fractures aux États-Unis, 27 % des fractures
étaient des fractures des vertèbres, 19% étaient localisées aux poignets, et 14 % à la hanche.
De plus, l'ensemble des fractures aux autres sites non traditionnellement perçus comme
étant associés à l'ostéoporose (c.-à-d. bassin, humérus, clavicule, tibia, péroné et autres)
représente la plus grande proportion, soit 40 % de l'ensemble des fractures [67]. En général,
les taux d'incidence, selon les différents sites de fracture, sont plus élevés chez les femmes
que chez les hommes. L'incidence des fractures des côtes, de la clavicule, de l'omoplate et
du sternum est cependant plus élevée chez les hommes. À l'exception des fractures de la
hanche et du bassin, l'incidence des fractures augmente linéairement avec l'âge, peu
importe le site. Finalement, puisque l'incidence des fractures de fragilisation (excluant la
fracture de la hanche) est non négligeable, il est essentiel de considérer l'ensemble des sites
de fracture comme étant associés à l'ostéoporose dans l'évaluation de l'incidence des
fractures afin de ne pas sous-estimer l'impact des conséquences de l'ostéoporose.
Une étude a récemment évalué, sur une période de 20 ans (1986-2006), les tendances dans
les taux d'incidence des fractures standardisés pour l'âge et pour les sites majoritairement et
traditionnellement perçus comme étant associés à l'ostéoporose (hanche, avant-bras,
vertèbres et humérus) [68]. Une diminution significative des taux d'incidence des fractures
de la hanche (deux sexes), de l'avant-bras et de l'humérus (femmes seulement) a été
observée, alors que l'incidence des fractures de vertèbres est restée stable.
1.2.5 La cascade des fractures
Plusieurs études épidémiologiques suggèrent que les patients ayant subi une fracture de
fragilisation ou ayant eu une fracture vertébrale radiologiquement confirmée ont un risque
élevé de subir une autre fracture de fragilisation. Klotzbuecher et al. ont effectué une revue
systématique de la littérature et ont calculé le risque de fracture suivant une histoire
préalable de fracture [5]. Selon cette étude, l'association la plus forte a été obtenue entre un
antécédent de fracture vertébrale et le risque d'une nouvelle fracture vertébrale. Les femmes
ayant au moins une fracture vertébrale radiologique ont un risque de nouvelle fracture
vertébrale quatre fois plus élevé que celles n'ayant pas d'antécédent de fracture vertébrale et
14
ce risque augmente avec le nombre de fractures vertébrales antérieures [5]. Globalement,
les femmes ayant une histoire antérieure de fracture (poignet, vertèbres, hanche ou autres)
ont un risque d'une nouvelle fracture deux fois plus élevé par rapport à celles n'ayant aucun
antécédent de fracture [5, 69]. Selon une étude récente, le risque d'une nouvelle fracture
serait 3,5 fois plus élevée chez les hommes ayant un antécédent de fracture
comparativement à ceux qui n'en n'ont pas [69]. De plus, dans les études ayant mesuré
initialement la DMO des patients, l'association entre une histoire antérieure de fracture et le
risque d'une nouvelle fracture est à peine modifiée lorsque les données sont ajustées pour la
mesure de la DMO [26]. Ces résultats suggèrent que la fracture de fragilisation est
probablement le facteur de risque le plus important et que ce facteur de risque prédit de
façon indépendante la survenue d'une nouvelle fracture. En effet, l'existence d'une
première fracture traduit directement la faiblesse osseuse fonctionnelle, le seuil de fracture
est alors atteint et, l'ostéoporose devient une maladie grave et difficile à contrôler. Par
conséquent, il devient essentiel de faire une évaluation de l'ostéoporose et du risque de
fracture particulièrement chez les patients qui présentent un antécédent de fracture.
Suite à la fracture, la douleur, la difformité, la mobilité réduite et la réduction de l'activité
physique entraînent une réduction rapide de la masse osseuse et ainsi, une augmentation du
risque de fracture. Une étude canadienne (Hamilton), menée auprès de patients ayant
présenté une fracture de la hanche, a révélé que 5 % de ces patients subiront une deuxième
fracture de la hanche dans l'année suivant la fracture, et ce pourcentage de deuxième
fracture atteint 9,9 % si l'on ajoute les fractures des vertèbres, du poignet et des côtes [70].
Une étude récente rapporte que les taux d'incidence d'une deuxième fracture de la hanche
chez les femmes et les hommes sont respectivement de 293 et 237 pour 100 000 personnes-
années [71]. Dans cette étude, il est mentionné que les taux d'incidence d'une deuxième
fracture de la hanche sont très élevés dans les 12 mois suivant la première fracture de la
hanche et diminuent par la suite pour atteindre des taux équivalents à ceux observés pour la
survenue d'une première fracture de la hanche [71].
1.2.6 Conséquences des fractures de fragilisation
En plus du risque de fractures subséquentes, les fractures de fragilisation entraînent
également un accroissement du risque de perte d'autonomie, d'une baisse de la qualité de
15
vie et de décès, qui à leur tour, imposent un fardeau important aux femmes, à leurs proches
et au système de santé.
Les fractures associées à l'ostéoporose sont l'une des principales raisons d'hospitalisation
et de transfert dans un établissement de soins de longue durée [12]. Les fractures de
fragilisation entraînent également une augmentation de la mortalité. Selon une étude
réalisée au Québec entre 1981 et 1983, le taux de mortalité dans l'année suivant une
fracture de la hanche est de 22 % [72]. Deux autres études canadiennes plus récentes
rapportent des taux similaires [70, 73]. Selon une revue systématique de la littérature
portant sur les taux de mortalité suivant une fracture de la hanche, le risque de décès suivant
une fracture de la hanche est au moins 2 fois plus élevé comparativement au risque de décès
attendu au même âge dans la population. Les taux de mortalité sont plus élevés chez les
hommes que chez les femmes et cet excès de mortalité peut persister sur plusieurs années
[74]. Un excès de mortalité a également été rapporté chez les patients ayant subi une
fracture des vertèbres [10, 75]. Une augmentation du risque de mortalité suite à une fracture
de l'humérus et du poignet (homme seulement) a été récemment rapportée [76]. De plus,
l'excès de mortalité observé à ces sites est principalement observé au cours des premiers 12
mois suivant la fracture mais peut persister jusqu'à 5 ans et voir même 10 ans suivant la
fracture de la hanche [76, 77].
D'autre part, parmi les patients qui survivent à une fracture, on observe souvent une
diminution considérable de la mobilité ainsi qu'une perte d'autonomie. Effectivement, dans
l'année suivant une fracture de la hanche, 40 % des patients sont toujours incapables de
marcher sans aide et 60 % d'entre eux ont besoin d'aide pour accomplir leurs activités
quotidiennes [11]. Parmi les patients, ayant obtenu leur congé de l'hôpital à la suite d'une
fracture de la hanche, seulement 44 % retournent à la maison, 10 % sont transférés dans un
autre hôpital, 27 % dans un établissement de réadaptation et 17 % dans un établissement de
soins de longue durée [14]. Parmi ceux qui retourneront à domicile, 62,4 % recevront des
services à domicile pour une moyenne de 154 jours [70].
Les fractures ont également une profonde répercussion sur la qualité de vie des patients.
Les auteurs de l'étude canadienne multicentrique sur l'ostéoporose ont observé une
16
diminution significative de la qualité de vie chez les patients ayant subi des fractures
ostéoporotiques comparativement aux patients n'ayant pas subi de fracture [78]. Selon les
résultats de cette étude, les fractures ont un impact important sur les scores des deux
échelles de mesure de la qualité de vie : l'échelle du fonctionnement physique et l'échelle
du rôle des limitations dues aux problèmes de santé. Chez les femmes, les fractures de la
hanche et du bassin ont particulièrement un impact sur l'échelle du fonctionnement
physique alors que chez l'homme, les fractures de la hanche ont un impact sur l'échelle du
rôle des limitations dues aux problèmes de santé [78].
1.2.7 Evaluation du risque de fracture
Depuis la publication des guides de pratique clinique pour le diagnostic et le traitement de
l'ostéoporose en 2002 [79], des changements importants ont été apportés dans les lignes
directrices relatives à la prévention et au traitement de l'ostéoporose et des fractures de
fragilisation. Selon le nouveau paradigme proposé par Ostéoporose Canada dans son guide
de pratique clinique récemment publié en octobre 2010 [29], la prise en charge de
l'ostéoporose va bien au-delà du traitement d'une faible densité osseuse mais vise à
prévenir et à traiter les fractures de fragilisation et leurs conséquences. Une DMO basse est
actuellement considérée comme étant un facteur de risque parmi plusieurs. En effet,
certains facteurs, comme par exemple le fait d'avoir un antécédent personnel de fracture
après l'âge de 40 ans, augmentent le risque de fracture et ce, indépendamment de la DMO.
Il est donc actuellement recommandé d'utiliser une approche intégrée considérant la
combinaison des facteurs de risque clinique et la DMO pour évaluer le risque absolu de
fracture. Cette approche augmente notre capacité à identifier les individus à haut risque de
fracture et aide à mieux orienter la prise de décision thérapeutique. Par conséquent,
l'intégration de nouveaux outils pour l'évaluation du risque de fracture à 10 ans dans la
prise en charge de cette problématique de santé est actuellement recommandée.
Le fardeau global des fractures de fragilisation concerne surtout les femmes et les hommes
de 50 ans et plus. C'est pourquoi, les guides de pratiques cliniques publiés en 2010
recommandent une évaluation des facteurs de risque de l'ostéoporose et des fractures pour
ce groupe d'âge afin d'identifier les individus à risque élevé [29]. Pour évaluer le risque de
fracture, on procède à un bref historique médical et à un examen physique ciblé. La taille
17
doit être mesurée avec précision afin d'évaluer la présence d'une fracture vertébrale.
L'évaluation de la mobilité doit également être effectuée. En présence de facteurs de risque,
une évaluation plus complète est alors nécessaire. Au Canada, il existe actuellement deux
outils de prédiction du risque de fracture ostéoporotique majeure (c'est-à-dire fracture
d'une hanche, d'une vertèbre [clinique], de l'avant-bras ou de la partie proximale de
l'humérus) à dix ans : l'outil CAROC conçu conjointement par l'association Canadienne
des radiologistes et Ostéoporose Canada [80] ainsi que l'outil FRAX de l'Organisation
mondiale de la santé [81]. Ces deux outils utilisent uniquement la DMO ou le score T au
niveau du col fémoral. Ces deux outils sont calibrés en utilisant les mêmes données
canadiennes sur les fractures et sont validés pour la population canadienne [82-84]. Il faut
cependant préciser que ces outils ne sont conçus que pour les femmes et les hommes de
plus de 50 ans n'ayant jamais été traités.
L'outil CAROC définit trois catégories de risque de fracture ostéoporotique majeure à dix
ans : faible (< 10 %), modéré (10 % - 20 %) et élevé (> 20 %) [80, 85]. Cet outil est basé
sur l'âge, le sexe et le score T de la DMO mesurée pour le col fémoral. Certains facteurs de
risque peuvent faire passer le patient à une catégorie de risque supérieure (de faible à
modéré ou de modéré à élevé) et ce, indépendamment de la DMO. Ces facteurs sont la
présence d'antécédent personnel de fracture après l'âge de 40 ans et l'utilisation prolongée
de glucocorticoïdes (plus de trois mois au cours de l'année précédente). Si ces deux facteurs
de risque sont présents, on considère automatiquement le patient à risque élevé de fracture.
L'outil FRAX utilise les mêmes facteurs de risque cliniques et considère également l'indice
de masse corporelle, la fracture de la hanche chez un parent, la polyarthrite rhumatoïde, le
tabagisme actuel et une forte consommation d'alcool. La valeur de la DMO du col fémoral
est une information optionnelle pour l'outil FRAX. Par contre, il a été montré que la
discrimination des fractures est supérieure lorsque le FRAX utilise la valeur de la DMO
comparativement au FRAX n'utilisant pas la mesure de la DMO ou si l'on utilise la mesure
de la DMO seule [86]. Dans 90 % des cas, les résultats avec ces deux outils concordent et
placent les individus dans la même catégorie de risque [80].
18
1.2.8 Prise en charge
Une prise en charge intégrée des patients à risque de fracture est également recommandée
dans les lignes directrices de 2010. Dans le cadre de cette prise en charge intégrée, les
différentes catégories de risque de fracture (faible, modéré et élevé) servent à orienter les
modifications à apporter dans les habitudes de vie et dans les décisions thérapeutiques.
Tous les patients quelque soit leur risque doivent envisager l'intégration d'exercices
d'entrainement pour améliorer l'équilibre et la démarche. Les exercices sont également et
particulièrement recommandés lorsqu'un patient a subi une fracture puisque cela lui
permettra d'améliorer sa fonction physique et réduira la douleur. Les résultats des études les
plus récentes suggèrent un effet modeste de l'exercice sur la DMO [87, 88]. Cependant,
l'effet de l'activité physique sur la prévention des fractures s'explique en majorité par son
effet bénéfique sur la réduction du risque des chutes via l'amélioration de l'équilibre et de
la force musculaire. Un changement majeur des nouvelles lignes directrices concerne les
recommandations en calcium et vitamine D. Une consommation quotidienne en calcium de
1200 mg par jour provenant particulièrement de l'alimentation ou sous la forme de
suppléments au besoin est recommandée. Selon une récente méta-analyse évaluant les effets
du calcium seul ou en combinaison avec la vitamine D sur les fractures, une consommation
combinée de calcium et de vitamine D serait associée à une réduction du risque de fracture
de 12 % (RR 0,88, IC 95 % 0,83-0,95). La réduction était plus importante chez les
personnes âgées les plus adhérentes à la thérapie et parmi celles ayant au moins 1200 mg de
calcium et 800 Ul de vitamine D par jour [89]. Contrairement aux recommandations
touchant les suppléments de calcium, celles concernant la vitamine D sont à la hausse. Les
études épidémiologiques suggèrent en effet que la majorité des canadiens n'ont pas un
apport optimal de vitamine D. La Société d'ostéoporose du Canada recommande entre 400
et 1000 Ul/jour pour les patients de moins de 50 ans et de 800 à 2000 UI/jour pour les
patients de 50 ans et plus [29].
Un traitement pharmacologique est recommandé pour les personnes ayant un risque élevé
de fracture et ceux ayant subi une fracture de la hanche et de la colonne vertébrale [29]. Les
patients présentant un risque modéré et ayant des facteurs de risque additionnels tel qu'un
antécédent familial de fracture ou une fracture du poignet pourraient bénéficier d'un
19
traitement pharmacologique à la lumière d'autres informations cliniques. Actuellement, au
Canada, un nombre croissant d'options thérapeutiques est disponible. De façon générale, les
traitements disponibles sur le marché réduisent le risque de fracture de 30 à 70 % selon
l'âge du patient et les sites de fracture [29, 90]. Finalement, chez les patients à risque élevé
de fracture, les bienfaits des traitements pharmacologiques l'emportent sur les effets
indésirables.
1.2.9 Progression et coût des fractures ostéoporotiques
Ce problème de santé dont l'importance s'accroît avec l'âge est non seulement bien présent
aujourd'hui mais, compte tenu du vieillissement de la population, prendra des proportions
de plus en plus grandes si des stratégies d'intervention ne sont pas mises en place pour
prévenir l'apparition de la première fracture de fragilisation. En 2006, 14% de la
population du Québec avait plus de 65 ans (groupe plus à risque de fracture), en 2056, on
estime qu'elle atteindra 28 % [91]. Parallèlement à ces changements démographiques
importants, on peut facilement entrevoir une augmentation du nombre de patients ayant
subi une fracture de fragilisation que l'on devra traiter.
Les fractures de fragilisation imposent une charge financière non négligeable. En 1997, au
Canada, le traitement d'un patient ayant subi une fracture de la hanche coûtait 21 385 $ si le
patient était de retour chez lui après son hospitalisation. Dans le cas où le patient était
transféré dans un établissement après son hospitalisation, le traitement coûtait le double,
soit 44 156 $ [73]. Au Canada, le coût total du traitement des fractures de la hanche était
chiffré à 650 millions en 1997. On estime qu'en 2041, ce montant devrait atteindre 2,4
milliards [73]. En 1993, les coûts des soins actifs (hospitalisations, soins ambulatoires,
médicaments et soins de longue durée) pour traiter les fractures liées à l'ostéoporose au
Canada ont atteint 1,3 milliard de dollars [15]. Compte tenu de son poids dans la population
canadienne et de l'augmentation des dépenses de santé, on a estimé ce coût à presque 14
milliard en 2007 pour le Québec.
1.2.10 Trajectoires cliniques
L'accroissement du nombre de personnes âgées induit une surcharge des ressources
médicales et financières qui obligent le système de santé canadien à porter une attention
20
particulière sur l'accès aux services de santé et sur leur utilisation. Dans ce contexte, il est
essentiel d'évaluer les trajectoires cliniques et le profil d'utilisation des ressources
médicales chez les personnes ayant subi des fractures de fragilisation. Ces informations
permettront d'identifier l'impact de ces fractures sur les services de santé, et plus
spécialement, leur impact sur les services orthopédiques. Ces renseignements permettront
également de comparer les pratiques en lien avec les recommandations cliniques et,
éventuellement, favoriser une meilleure planification des ressources médicales à consacrer
pour cette problématique. Par ailleurs, des indicateurs de performance et de qualité pourront
être établis et permettront éventuellement d'améliorer les soins des personnes ayant subi
des fractures.
Selon le site de la fracture et la sévérité de cette dernière, le traitement peut impliquer un
médecin spécialiste (orthopédiste) mais dans la majorité des cas, le médecin de famille est
adéquatement formé pour offrir le traitement. Plusieurs fractures (simple, stable et non
déplacée) survenant à certains sites anatomiques (main, pied, tibia, péroné, cheville, bassin,
poignet, humérus, clavicule, vertèbres et côtes) peuvent être efficacement traitées par les
médecins de famille [92-94]. Selon une étude réalisée aux États-Unis, les médecins de
famille peuvent traiter deux tiers des patients ayant subi des fractures et obtiennent
d'excellents résultats cliniques [94]. De plus, selon cette étude, les médecins de famille
ayant une formation et une expérience en orthopédie peuvent traiter un tiers des fractures
nécessitant une chirurgie [94]. Cependant, les médecins de famille ne traitent que peu les
fractures. Selon une étude réalisée en Virginie, seulement 42 % des médecins de famille
offraient des soins aux patients ayant subi des fractures et parmi ceux-ci, 32% seulement
étaient en mesure d'appliquer un plâtre dans leur clinique [95]. Une autre étude révèle que
43 % des patients référés en orthopédie auraient pu être traités par le médecin de famille
[96]. Il semble y avoir un écart important entre les soins que les médecins de famille
pourraient offrir et les soins qu'ils offrent, ce qui conduit à une sur-utilisation des
ressources orthopédiques.
En ce qui concerne la gravité des fractures, beaucoup d'entre-elles nécessiteront une
intervention chirurgicale. En effet, une étude révèle que 46 % de l'ensemble des fractures
sont traitées chirurgicalement et que celles-ci nécessitent davantage de visites
21
comparativement aux fractures ne nécessitant aucune chirurgie [97]. Selon une étude
américaine, plus de 98 % des patients ayant subi une fracture de la hanche auront besoin
d'un traitement chirurgical [98], alors que la majorité des fractures du poignet, de
l'humérus et de la cheville n'en n'ont pas besoin. Cependant, pour ces sites de fracture, des
variations régionales importantes dans le nombre d'interventions chirurgicales ont été
observées [98]. Ces variations régionales peuvent s'expliquer par une perception différente
des bénéfices de la chirurgie par les médecins et les patients ainsi que par le nombre
d'orthopédistes pratiquant dans certaines régions. Selon une étude réalisée par l'Institut
canadien d'information sur la santé, en 2005-2006, il y a eu 28 200 admissions pour une
fracture de la hanche dans les hôpitaux canadiens dont 88 % impliquaient des patients âgés
de plus de 65 ans [99].
Une autre étude réalisée en 1996 a révélé que la durée moyenne d'un séjour hospitalier des
personnes souffrant d'une fracture de la hanche est de 19,1 jours [14], alors que la durée
moyenne d'un séjour hospitalier après une fracture vertébrale a été estimée à 10,1 jours
[13]. De plus, lorsqu'une fracture vertébrale coexiste avec d'autres conditions ayant conduit
à l'hospitalisation, le séjour hospitalier dure en moyenne 2 jours de plus [13]. Après les
troubles mentaux, la fracture de la hanche, la fracture de vertèbres et les autres fractures
sont respectivement les 2e, 3e et 4e cause d'hospitalisation qui nécessitent les plus longs
séjours chez les personnes de plus de 50 ans [13].
La chirurgie est un élément essentiel du traitement des patients ayant subi une fracture de la
hanche. Avant la chirurgie, la majorité des patients sont confinés au lit. Par conséquent, le
délai chirurgical et la mobilisation peuvent entraîner des complications importantes
notamment thromboemboliques, des infections des voies urinaires, des atélectasies
pulmonaires et des plaies de lit [100]. Le délai d'attente pour l'obtention de la chirurgie est
un indicateur de performance important dans le traitement des fractures de la hanche [99].
En effet, des études ont montré que des délais d'attente plus courts avaient des
conséquences favorables sur la santé des patients se traduisant par une diminution de la
mortalité [101, 102], de la douleur, des complications post-chirurgie et de la durée de séjour
[100]. Une étude réalisée au Canada (excluant le Québec) a révélé que les pourcentages de
patients opérés avec un délai d'attente inférieur à 48 ou à 72 heures étaient respectivement
22
de 65 % et 85 % [99]. Des variations régionales dans les délais d'attente ont également été
observées. En effet, les pourcentages de patients opérés avec des délais d'attente inférieurs
à 48 heures pour l'île-du-Prince-Édouard et la Colombie Britannique étaient respectivement
de 78 % et de 71 % alors que ces pourcentages pour le Manitoba et la Saskatchewan étaient
respectivement de 53 % et 56 % [99]. Ces données ne sont pas disponibles pour le Québec.
Des caractéristiques associées aux patients et au système de santé influencent les délais
d'attente. En effet, les hommes en particulier, ont moins de chance d'avoir leur chirurgie
dans un délai inférieur à 48 heures comparativement aux femmes (63 % versus 66 %), et les
patients ayant des comorbidités à l'admission ont plus de risque de voir leur chirurgie
retardée [99]. De plus, les patients admis dans des petits hôpitaux ont plus de chances de
recevoir leur chirurgie dans un délai inférieur à 48 heures (74 %), comparativement aux
patients admis dans des gros hôpitaux (67 %) ou dans des hôpitaux universitaires (57 %)
[99]. Le volume chirurgical a également un impact sur le délai chirurgical. En effet, les
patients admis dans des hôpitaux ayant un faible volume chirurgical (c.-à-d. hôpitaux ayant
admis moins de 137 patients avec une fracture de la hanche en 2005-2006), recevaient plus
souvent leur chirurgie dans un délai inférieur à 48 heures comparativement aux patients
admis dans les hôpitaux ayant un gros volume chirurgical [99]. Malgré le fait que certains
facteurs favorisent l'augmentation du délai chirurgical, cet indicateur de performance peut
servir de baromètre pour mesurer l'efficacité du système de santé dans le traitement des
patients ayant subi des fractures de la hanche.
1.2.11 Suivi après une fracture
Malgré l'existence de recommandations et de lignes directrices canadiennes concernant la
pratique clinique pour le diagnostic et la prévention de l'ostéoporose et des fractures
ostéoporotiques [29, 79, 103, 104], et la disponibilité de traitements efficaces [105-111], la
prise en charge clinique de l'ostéoporose suivant une fracture de fragilisation n'est pas
adéquate. En effet, Papaioannou et al. ont effectué une revue systématique de la littérature
pour évaluer le suivi clinique (diagnostic et traitement) au Canada de l'ostéoporose chez
des patients de 40 ans et plus ayant subi une fracture de fragilisation [112]. Selon cette
étude, la proportion de patients ayant subi une fracture et qui reçoivent un diagnostic
d'ostéoporose (suite à un test ou selon le diagnostic du médecin) varie entre 1,7 % et 50 %,
23
alors que la proportion de patients avec fracture ayant reçu un traitement (thérapie
hormonale, bisphosphonates, calcitonine) varie entre 5,2 % et 37,5 %. Selon une étude
récente menée au Québec auprès de femmes âgées de 50 ans et plus et qui ont subi une
fracture de fragilisation, 80 % d'entre elles n'avaient toujours pas reçu de diagnostic et de
traitement pour l'ostéoporose dans les 12 mois suivant la fracture [4]. Ces données
suggèrent que ces patientes ne bénéficient pas d'une prise en charge clinique adéquate.
Finalement, les auteurs d'une étude évaluant les tendances entre 1996 et 2008 dans le
traitement et le diagnostic de l'ostéoporose dans l'année suivant une fracture de
fragilisation arrivaient à la conclusion que la prise en charge de l'ostéoporose suivant une
fracture ne s'était pas améliorée au cours des 10 dernières années et demeurait sous
optimale. En effet, moins de 20 % des patients recevaient une intervention à la suite de leur
fracture [113]. Ce suivi déficient suite une à fracture est largement reconnu [4, 112, 114-
116] et a même amené le Conseil ontarien des services de santé pour les femmes, dans son
rapport publié en 2003 [117], à qualifier ces absences de suivi d'« occasions d'interventions
manquées ».
1.3 Le rôle de la santé publique Malgré les connaissances scientifiques actuelles et le cumul des évidences qui
favoriseraient le soutien des interventions de santé publique en vue de faire face à cette
problématique de santé, la surveillance des fractures de fragilisation reste encore très peu
intégrée dans les plans de surveillance populationnelle. Or, il s'agit d'un point de départ
essentiel à une approche organisée et scientifique de cette question [12, 118]. Certains
organismes de santé ont déjà commencé à redéfinir l'approche de la gestion des fractures
dans la population. C'est le cas de l'Ontario qui s'est dotée d'un nouveau « Cadre et
stratégie de prévention et de gestion de l'ostéoporose » [12] duquel est issu le rapport
«Élaboration d'un modèle de soins intégré post-fracture» [117]. Parmi les
recommandations, on suggère « la création de l'infrastructure d'une collecte coordonnée
des données sur la population ontarienne atteinte d'ostéoporose ayant subi des chutes et des
fractures ». Ce registre permettrait d'évaluer l'impact des interventions, des programmes
généraux et éducatifs et d'analyser les aspects économiques incluant une analyse de
rentabilité du diagnostic et de la prise en charge de cette maladie. Lorsque le Chirurgien
24
Général du Département de la santé des États-Unis a fait son rapport en 2002 sur
l'ostéoporose et la santé osseuse, il en venait à la même conclusion qu'il fallait obtenir de
meilleures données de surveillance, d'incidence et évaluer l'efficacité des interventions
[118].
1.4 Surveillance des fractures de fragilisation Dans un contexte de contraintes budgétaires et étant donné l'importance de ce problème de
santé, la mise en place d'une surveillance des fractures de fragilisation est incontournable.
Il est primordial de développer des outils permettant d'évaluer l'importance populationnelle
du fardeau des fractures de fragilisation et leur impact sur le système de santé. Des études
épidémiologiques à caractère populationnel aideront à établir l'ampleur et le fardeau de
cette problématique. Ces études permettront également le développement d'indicateurs pour
suivre l'évolution et, ultérieurement, évaluer l'efficacité de la mise en place d'interventions
favorisant la prévention (primaire, secondaire et tertiaire) ainsi que la prise en charge
précoce de cette problématique.
Les données provenant des fichiers des hospitalisations ont été amplement utilisées et sont
considérées valides pour étudier des problématiques de santé nécessitant quasi
automatiquement une hospitalisation comme la fracture de la hanche [38]. Cependant, ce
type de fichier est restreint aux fractures assez sérieuses pour causer l'hospitalisation alors
que ces fractures ne représentent qu'une petite fraction de l'ensemble des fractures [119].
Par conséquent, ce fichier n'est pas représentatif de l'ensemble des fractures survenant dans
la population et ne peut être utilisé pour identifier les fractures de fragilisation.
Au Québec, les résidents bénéficient d'un système public d'assurance santé (Régie de
l'assurance maladie du Québec, RAMQ) qui repose sur l'universalité et la gratuité des soins
et des services de santé. L'un des mandats assumés par la RAMQ est de gérer la
rémunération versée aux professionnels de la santé par le paiement des prestations de
services médicaux rendus par ces derniers. Les professionnels de la santé sont remboursés
pour chaque acte médical posé en soumettant une réclamation à la RAMQ. Le numéro
d'assurance maladie du patient, la date et l'endroit de l'acte médical, le code de la
procédure (code d'acte) correspondant à l'acte médical posé et optionnellement le code du
25
diagnostic CIM-9 sont disponibles sur cette réclamation. Tous les actes médicaux réclamés
à la RAMQ sont enregistrés dans un fichier administratif. Ce fichier des services rémunérés
à l'acte est facilement accessible, dans un format standardisé, depuis plusieurs décennies et
les services médicaux fournis à la très grande majorité de la population y sont enregistrés.
De plus, puisque ce fichier contient les informations concernant les remboursements
effectués aux médecins, la grande majorité des contacts ayant eu lieu avec ces derniers y
sont enregistrés et l'identification de fausse réclamation est peu probable en raison de la
mise en place d'un système de surveillance sophistiqué pour identifier les cas de fraudes
potentiels [120]. Entre 2004 et 2005, ce fichier a collecté et enregistré les réclamations des
services médicaux rendus par 94 % des médecins du Québec et 98 % des 7,5 millions des
résidents du Québec [121]. Malgré le fait que ce fichier ait été peu utilisé pour le repérage
de certaines maladies dans la population, quelques études ont montré que l'utilisation de ce
fichier à cet effet pouvait être valide [120, 122-125].
Une étude publiée en 2000 a examiné la sensibilité de ce fichier à identifier tous les cas de
traumatisme (fractures, déchirures des tissus mous, brûlures, blessures par un corps
étranger, entorses, contusions, éraflures, engelures, etc.) chez les personnes de 65 ans et
plus [120]. De façon générale, la sensibilité de la combinaison du code de procédure de
l'acte médical et du code de diagnostic pour repérer un cas de traumatisme était élevée. La
sensibilité était respectivement de 67,3 % et 81,3 % pour identifier un traumatisme à la
même date ou dans une fenêtre de 17 jours (95,6 % des traumatismes étaient à l'intérieur
d'une fenêtre de -1 jour à +3 jours) entourant la date réelle du traumatisme. Dans cette
même étude, 55,4 % des traumatismes étaient des fractures et la sensibilité variait, selon le
site de fracture, de 26,7 % pour les fractures au visage à 97,2 % pour les fractures de la
hanche. Puisque l'objectif visé par la méthodologie développée dans cette étude était
l'identification des cas de traumatisme, il est donc difficile de généraliser les résultats
obtenus à l'identification des fractures. De plus, seulement la moitié des traumatismes
examinés dans cette étude sont des fractures. Par conséquent, ceci limite l'interprétation des
résultats statistiques obtenus pour l'identification des fractures.
26
À ce jour, aucune étude n'a cherché à utiliser les données provenant de ce fichier pour
étudier l'impact des fractures de fragilisation sur la santé de la population et sur le système
de santé du Québec.
En résumé, à la lumière de la synthèse de la littérature présentée ci-dessus, l'ampleur de
l'ostéoporose et des fractures de fragilisation ainsi que leurs conséquences nécessitent une
surveillance continue à partir de l'âge de 50 ans. Le développement de nos capacités en
matière de surveillance épidémiologique est très utile pour évaluer le fardeau populationnel
associé aux fractures de fragilisation et pour évaluer l'efficacité et l'impact d'interventions
populationnelles visant à prévenir ces fractures et leurs conséquences. C'est pourquoi, il
devient impératif d'évaluer d'abord la faisabilité de l'utilisation des données recueillies
dans le fichier des services rémunérés à l'acte de la RAMQ pour identifier les cas incidents
de fractures. Par la suite, les premiers indicateurs visant à établir un portrait populationnel
des fractures chez les femmes de 50 ans et plus et de quantifier leur impact pourraient être
construits. Ceci serait une première étape vers la mise en place d'un système de
surveillance continu de l'ostéoporose et des fractures de fragilisation au Québec.
L'utilisation des données provenant des fichiers médico-administratifs pour la surveillance
épidémiologique s'avère non seulement une approche pratique, relativement simple,
accessible et peu coûteuse, mais permet en plus d'augmenter la généralisation des résultats
à la population et de minimiser les biais associés aux études de cohorte (biais de sélection,
biais de rappel et la non-réponse) [122, 126]. Ces fichiers peuvent également offrir une
grande opportunité pour mener des études populationnelles sur les fractures de fragilisation.
Cependant, étant donné que ces fichiers sont conçus pour répondre à des besoins d'ordre
administratif, ayant pour but de gérer les soins de santé des patients, leur utilisation à des
fins de surveillance épidémiologique doit d'abord faire l'objet d'une validation. La
validation des données administratives a été identifiée comme une priorité de recherche par
un consortium international [127]. De plus, la validation des algorithmes utilisés pour
identifier les patients ayant certains états de santé est essentielle afin d'éviter les biais de
classification qui peuvent menacer la validité interne et les conclusions des études [126].
Tel que mentionné précédemment, les fichiers des hospitalisations ont été largement
utilisés, mais leur validité est limitée à des problèmes de santé nécessitant une
27
hospitalisation, comme les fractures de la hanche [38, 128], ce qui représente seulement une
petite proportion de toutes les fractures de fragilisation [119]. Puisque les fractures
surviennent généralement dans un contexte aigu et douloureux, elles nécessitent plusieurs
contacts avec le système de santé [128]. Par conséquent, elles devraient être facilement
identifiables en utilisant le fichier des services rémunérés à l'acte de la RAMQ. Les travaux
présentés dans le cadre de ce doctorat répondent ainsi à 3 objectifs.
Objectif 1 : Développer et valider un algorithme d'identification des cas incidents de
fracture à partir du fichier des services rémunérés à l'acte de la RAMQ.
Basée sur l'utilisation du fichier des services rémunérés à l'acte de la RAMQ, une étude
rétrospective, chez les femmes de 50 ans et plus provenant de trois régions sociosanitaires
(Québec, Montréal et Mauricie-Centre du Québec), a été réalisée entre le 1er septembre
2003 et le 31 mars 2006 pour répondre à ce premier objectif. Toutes les réclamations
potentiellement associées à la survenue d'une fracture à un site ostéoporotique enregistrées
dans le fichier de la RAMQ au cours de la période étudiées ont été identifiées. Fondé sur la
combinaison de la spécialité médicale du médecin, du code d'acte correspondant à l'acte
médicale posé et du code de diagnostic CIM-9 disponible sur chaque réclamation, un
groupe d'experts cliniciens a défini trois algorithmes pour l'identification des cas incidents
de fractures. Pour évaluer la validité de ces algorithmes, leurs valeurs prédictives positives
(VPP) et leurs sensibilités ont été calculées.
Le développement d'un algorithme valide pour identifier les cas incidents de fracture à
partir du fichier de la RAMQ permettra d'obtenir des données sur l'incidence des fractures
chez les femmes de 50 ans et plus. Dans le contexte d'une population vieillissante, donc
d'une augmentation de la population plus à risque de subir une fracture associée à
l'ostéoporose, ces informations sur l'incidence des fractures aideront à mieux comprendre
l'ampleur de celles-ci. En outre, ces données permettront non seulement de quantifier le
fardeau que ces fractures représentent sur les individus mais aussi de mesurer leur poids sur
le système de santé.
Objectif 2 : Estimer les taux d'incidence des fractures de fragilisation chez les femmes
de 50 ans et plus au Québec et évaluer leurs impacts sur la mortalité.
28
À partir de l'algorithme développé et validé lors de la réalisation de l'objectif 1, toutes les
patientes de 50 ans et plus provenant des mêmes régions sociosanitaires et ayant subi une
fracture entre le 1er janvier 2004 et le 31 décembre 2005 ont été identifiées. Cette cohorte
représentative de l'ensemble des fractures à survenir dans cette population au cours de la
période étudiée sera utilisée en lien avec les données démographiques pour estimer les taux
d'incidence des fractures de fragilisation. De plus, pour cette cohorte de patientes, des
données sur le statut vital ont également été obtenues via le fichier de la RAMQ jusqu'au
31 décembre 2007. Ces informations sur la mortalité seront utilisées pour évaluer l'impact
des fractures de fragilisation sur la mortalité des patientes.
Finalement, l'obtention d'informations concernant l'utilisation des ressources médicales
liées directement aux traitements des fractures de fragilisation aide à comprendre le fardeau
qu'elles représentent sur les ressources médicales et le système de santé. De plus, ces
informations peuvent être conjointement utilisées avec les données d'incidence afin
d'estimer les besoins en ressources et peuvent également aider les décideurs à planifier
l'allocation des ressources humaines et budgétaires ainsi que l'organisation de soins afin de
maintenir et d'accroître l'efficacité.
Objectif 3 : Évaluer le fardeau associé aux traitements des fractures de fragilisation
chez les femmes de 50 ans en termes d'utilisation des ressources médicales dans
l'année suivant la fracture.
Grâce à l'utilisation de l'algorithme développé et validé précédemment, toutes les patientes
de 50 ans et plus provenant des trois régions sociosanitaires et ayant subi une fracture entre
le 1er janvier 2004 et le 31 décembre 2005 ont été identifiées. Pour établir l'utilisation de
ressources médicales liées à la fracture pour chaque cas incident, l'utilisation des ressources
de santé dans l'année suivant la fracture a été identifiée en utilisant le fichier des services
rémunérés à l'acte de la RAMQ et le fichier des hospitalisations (Med-Echo). Ces données
ont été liées par un identifiant personnel unique afin de créer une cohorte longitudinale sur
l'utilisation des ressources de santé pour tous les cas de fracture. L'estimation de
l'utilisation de ressources directement associées aux traitements de ces fractures dans
l'année suivant la fracture a été calculée et incluait : toutes les réclamations effectuées par
29
les médecins (visite médicale ou procédure correspondant à l'acte médical posé) et
l'information concernant les séjours hospitaliers.
Les résultats des trois principaux objectifs de ce projet de recherche sont présentés sous la
forme d'articles scientifiques en anglais. L'étude de validation en lien avec le
développement d'un algorithme d'identification des cas incidents de fracture est présentée
au chapitre 2. Les résultats en lien avec l'objectif 2 visant à estimer les taux d'incidence des
fractures de fragilisation chez les femmes de 50 ans et plus au Québec et évaluer leurs
impacts sur la mortalité seront présentés dans le chapitre 3. Finalement, les résultats en lien
avec l'objectif 3 visant à évaluer le fardeau associé aux traitements des fractures de
fragilisation en termes d'utilisation des ressources médicales sont présentés au chapitre 4.
31
Chapitre 2
Des algorithmes peuvent être utilisés pour identifier les fractures de fragilisation dans le fichier
des services rémunérés à l'acte
Algorithms can be used to identify fragility fracture cases in physician-claims databases
L'objectif dans ce chapitre est de présenter les résultats de l'étude visant à évaluer la faisabilité et la validité des données recueillies dans le fichier des services rémunérés à l'acte de la RAMQ pour l'identification des cas incidents de fracture.
Les résultats de ce travail ont été publiés dans Osteoporosis International[129f. Les auteurs sont Sonia Jean, Bernard Candas, Etienne Belzile, Suzanne Morin, Louis Bessette, Sylvie Dodin et Jacques P. Brown. Le chapitre comporte l'intégral de l'article publié en anglais.
33
2.1 Résumé OBJECTIF : Développer et valider des algorithmes pour identifier les fractures à partir du
fichier des services rémunérés à l'acte de la RAMQ.
MÉTHODES : Trois algorithmes ont été développés en combinant les informations du
fichier des services médicaux rémunérés à l'acte de la RAMQ telles la spécialité du
médecin, le code d'acte et le code du diagnostic. La validité des algorithmes a été évaluée
par le calcul des valeurs prédictives positives (VPP; par la vérification d'un échantillon de
cas identifiés par l'algorithme dans les dossiers médicaux hospitaliers) et des sensibilités
(par le croisement des cas incidents de fracture identifiés par l'algorithme avec une cohorte
de fractures bien caractérisée).
RÉSULTATS : Les VPP et les sensibilités variaient selon le site de la fracture. Pour la
plupart des sites de fracture, les VPP de l'algorithme 3 étaient supérieures à celle des
algorithmes 1 ou 2. Excepté pour la fracture du genou, les VPP variaient de 0,81 à 0,96. La
sensibilité était faible pour les vertèbres, le sacrum et le coccyx (de 0,40 à 0,50), mais
élevée à tous les autres sites de fracture. Dans 95 % des cas de fractures identifiés par
l'algorithme, le site de la fracture concordait avec le site indiqué au dossier médical
hospitalier du patient. La date de la fracture identifiée par l'algorithme était dans un
intervalle de deux jours de la date réelle de fracture pour 88 % des fractures identifiés par
l'algorithme. Parmi les cas ayant eu une réduction ouverte identifiée par l'algorithme 3 (N =
461), 95 % avaient subi une intervention chirurgicale selon leur dossier médical hospitalier.
CONCLUSION : Les algorithmes utilisant le fichier des services rémunérés à l'acte de la
RAMQ sont précis et fiables pour identifier les fractures à des sites associés à
l'ostéoporose. L'identification de ces fractures dans la population est importante pour aider
à estimer le fardeau associé à l'ostéoporose et l'utilité des programmes visant à réduire les
taux de fractures de fragilisation.
34
2.2 Abstract INTRODUCTION: To develop and validate algorithms that identify fracture events from
a physician-billing claims database (PCDs).
METHODS: Three algorithms were developed using physician's specialty, diagnostic, and
medical services codes used in a PCD from the province of Quebec. Algorithm validity was
assessed via calculation of positive predictive values (PPV; via verification of a sample of
algorithm-identified cases with hospitalization files) and sensitivities (via cross-referencing
respective algorithm-identified fracture cases with a well-characterized fracture cohort).
RESULTS: PPV and sensitivity varied across fracture sites. For most fracture sites, the
PPV with algorithm 3 was higher than with algorithms 1 or 2. Except for knee fracture, the
PPVs ranged from 0.81 to 0.96. Sensitivities were low at the vertebral, sacral, and coccyx
sites (0.40-0.50), but high at all other fracture sites. For 95% of fractures, the fracture site
identified by algorithm agreed with the fracture site from patients' medical records.
Fracture dates identified by algorithm were within two days of the actual fracture date in
88% of fracture cases. Among cases identified by algorithm 3 to have had an open
reduction (N=461), 95% underwent surgery according to their respective medical charts.
CONCLUSION: Algorithms using PCDs are accurate and reliable for identifying incident
fractures associated with osteoporosis-related fracture sites. The identification of these
fractures in the community is important for helping to estimate the burden associated with
osteoporosis and the utility of programs designed to reduce the rates of fragility fracture.
35
2.3 Introduction Osteoporosis is a skeletal disorder characterized by compromised bone strength and an
increased risk of fracture [3]. The clinical manifestation of osteoporosis is fragility fracture
(FF). A 50 year-old Caucasian woman has an estimated 40% lifetime risk of FF [6].
Approximately 81% of all fractures in women >50 years of age can be classified as FFs and
attributed to osteoporosis [4]. FFs are a major public health concern due to their association
with increased mortality, morbidity and healthcare costs [67, 130-132]. Since the majority
of the world's populations are aging, there is an ever-increasing burden of FFs on the
healthcare system. Despite the well-recognized burden of FFs, the diagnosis and treatment
of osteoporosis following a FF is disappointingly low [4, 112, 115, 116].
The development of epidemiological surveillance capabilities is useful for evaluating the
burden associated with FFs and for monitoring the impact of population-based and clinical-
based interventions [12, 118]. Information provided by surveillance systems can be used to
support evidence-based policies and to conduct performance evaluation of health care
services. With respect to FFs, the majority of attention has been given to the study of hip
fractures due to their relative ease of identification in medico-administrative databases and
their disproportionate burden on personal health and treatment costs as compared to other
FFs [67, 133]. Although fracture sites other than the hip may carry a lesser individual
burden, they are of interest to administrators of health programs because of their relatively
greater prevalence in the population and for their significant predictive value for recurrent
FFs, including hip fractures [5].
Population-based administrative databases have been successfully used for case-
identification of medical conditions in the general population [120, 122, 124,125, 128, 134-
137]. Using administrative databases is relatively inexpensive, minimizes usual biases
associated with survey studies (recall bias, nonresponse and subject attrition) and increases
external validity compared with cohort studies [122, 134]. This method also allows for
longitudinal follow-up of individuals over time for disease case and noncase comparisons.
Therefore, healthcare services administrative databases may provide unprecedented
opportunities to conduct population-based studies on FFs. Hospital discharge databases
have been used widely, but their validity is limited to health problems that require
36
hospitalization, such as hip fractures [38, 128], which only represent a small proportion of
all FFs [119].
Physician-billing claims databases (PCDs) are a valid source of information for outcome
assessment [120, 122, 124, 125, 128, 134-137]. Since fractures are typically acute and
painful, they are easily recognized and promptly treated within the healthcare system [128],
and consequently, should be identifiable from PCDs. Using PCDs to identify FFs would
provide a more comprehensive assessment of the total burden of illness associated with FFs
than current methods.
The objectives of this study were to develop, validate, and compare three computerized
algorithms for the identification of fracture cases in women 50 years of age and older using
a PCD. Development of algorithms that reliably and accurately identify FFs would allow
for the creation and maintenance of a population-based surveillance system for FFs.
2.4 Study design and setting 2.4.1 Study Design
This retrospective study is based on physicians' fee-for-service claims to the Quebec
(Canada) provincial database for medical services provided to women 50 years of age and
older between September 1, 2003 and March 31, 2006. A panel of expert clinicians (SM,
EB, LB, SD, JPB) defined several combinations of medical specialty, diagnostic and
medical services codes likely to be related to incident cases of FF. To establish the validity
of the algorithms their respective positive predictive value (PPV) and sensitivity (Sn) were
calculated. To calculate PPV, a random sample of fracture cases identified by the
algorithms (1,506, 1,341 and 1,211 fractures in algorithm 1, 2 and 3 respectively) was
selected and the respective patients' hospital medical charts were reviewed to validate the
diagnosis of a fracture event. To calculate sensitivity, data accrued from a cohort of
confirmed incident fracture cases (1,914 fractures) previously recruited for another study
[138] was obtained and tested against the algorithms to verify that the cases from this
cohort were well-identified by the algorithms.
37
This study focused exclusively on osteoporosis-related fracture sites: fracture occurring at
the vertebra, sacrum, coccyx, pelvis, hip, femur, shoulder, humerus, elbow, forearm, wrist,
knee, tibia, fibula, foot or ankle. While low-trauma fractures represent the vast majority of
fractures [4], both low- and high-trauma fractures were included as it was recently proposed
that both be included as outcomes in osteoporosis trials and observational studies [33], as
were pathological fractures [34]. Craniofacial, hand, finger and toe fractures were excluded
[31].
This project was approved by the Research Ethics Board of the « Centre hospitalier
universitaire de Québec, CHUQ » and approval for linking with clinical and administrative
databases was provided by Québec « Commission d'accès à l'information, CAI »
(http://www.cai.gouv.qc.ca). Personal identifiers were stripped and recoded before
transmission to the study analysts, with the exception of the subset of individuals used to
validate fractures cases from patient hospital medical charts (see below for details).
Authorization to review hospital medical records was granted by the Director of
Professional Services of each institution that supplied records.
2.4.2 Data sources
Provincial physicians' fee-for-service database.
Canadian residents are covered by a universal health insurance plan provided by their
province of residence. In Québec, physicians are remunerated on a fee-for-service basis and
must submit a claim to the Régie de Fassurance-maladie du Québec (RAMQ) for every
clinical service provided. Each claim must include the physician's unique identification
number, the patient's provincial health insurance plan number (NAM), the medical service
billing code for the clinical service, the date and location of the clinical service provided,
and, optionally, a diagnosis coded using the ninth revision of the International
Classification of Diseases, Clinical Modification (ICD-9-CM) codes. All claims are
electronically stored in a provincial administrative database of which the accuracy and
completeness have been previously verified [120, 125]. Medical services codes, being the
basis for payments, are closely monitored, accurately reported, and reliable [120]. However,
as the diagnostic field (ICD-9-CM) of the claim is not mandatory for payments, its use has
38
been cautionary due to its lack of specificity. Between 2004 and 2005, the RAMQ database
collected information from approximately 94% of Quebec-based physicians and almost
98% ofthe residents of Québec [121].
The study dataset was limited to medical services provided to women 50 years of age and
older between September 1, 2003 and March 31, 2006 in three provincial health regions
(Montreal, Québec City and Mauricie). These three regions represent 42% of the total
population of women 50 years of age and older in the province of Québec [121]. A list of
medical service billing codes potentially associated with the occurrence of a fracture at an
osteoporotic site was established by a panel of clinical experts (SM, EB, LB, SD, JPB).
Two main groups of fee-for-service claims were extracted: a) claims associated with
medical service billing codes definitively related to fracture care, i.e. open or closed
reduction of fracture [Criteria 1, Figure 2.1] and b) claims associated with medical services
billing codes not limited to fracture care [i.e. immobilization, consultation, principal visit,
follow-up or emergency room visit by an orthopedic surgeon (OS), emergency physician
(EP), or general practitioner (GP)], but combined with ICD-9-CM fracture codes [Criteria
2, 3 and 4, Figure 2.1]. Immobilization included casting, orthoses and splints. The list of
relevant medical services codes is provided in Appendix 1.
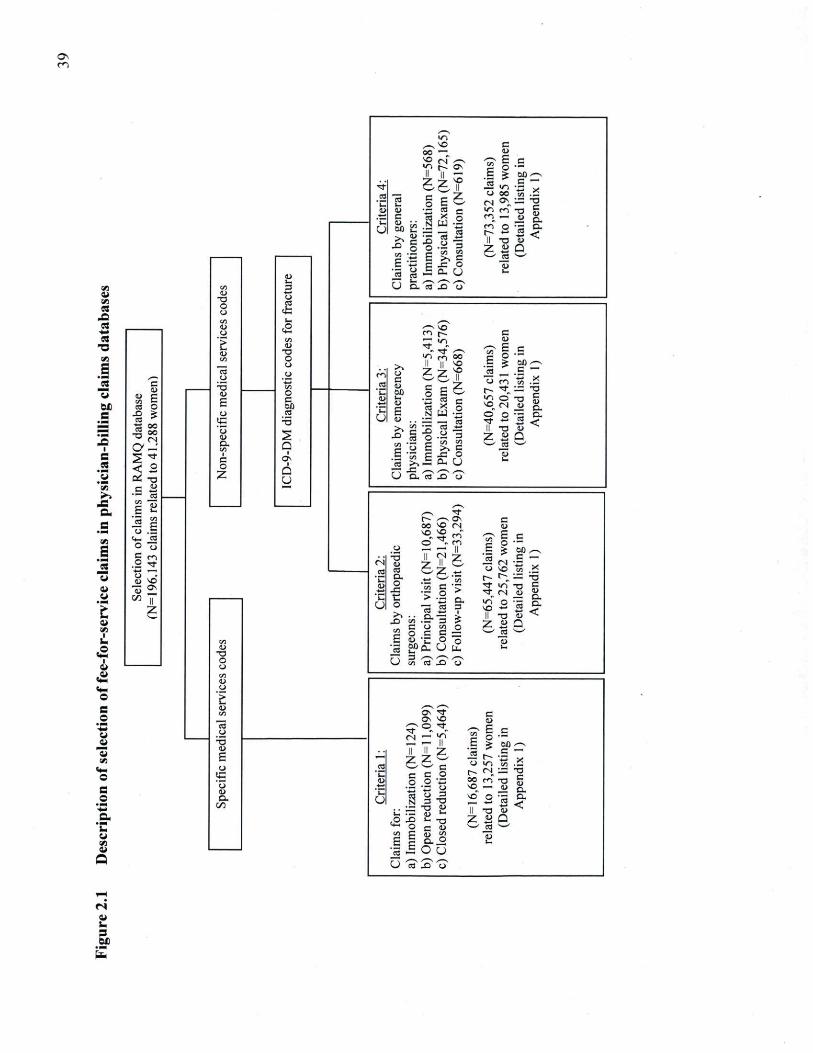
VJ i i VJ a
4X1 m
* m a •a VJ
S es s
e
VJ > J
JS C. S
■ M (Z_
S
ù a
■ .4»
O
e w i i "S « * . O s
_
Q
4r .2 D
'C u
s by
gen
eral
io
ner
s:
no
bil
izat
ion
(N=
56
8)
sica
l Exam
(N
=72,1
65)
isu
ltat
ion
(N=
61
9)
[N=
73,3
52 c
laim
s)
ited
to 1
3,9
85 w
om
en
^Det
aile
d li
stin
g in
Ap
pen
dix
1)
4r .2 D
'C u
s by
gen
eral
io
ner
s:
no
bil
izat
ion
(N=
56
8)
sica
l Exam
(N
=72,1
65)
isu
ltat
ion
(N=
61
9)
[N=
73,3
52 c
laim
s)
ited
to 1
3,9
85 w
om
en
^Det
aile
d li
stin
g in
Ap
pen
dix
1)
c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
U O.'éS' J2 "é? c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
m ca i
5_ '__ U
Cla
ims
by
em
erg
ency
p
hy
sici
ans:
a)
Im
mo
bil
izat
ion (
N=
5,4
13
b) P
hysi
cal E
xam
(N=
34,5
7
c) C
on
sult
atio
n (
N=
66
8)
(N=
40,6
57
cla
ims)
re
late
d to
20
,43
1 w
om
en
(Det
aile
d li
stin
g in
A
pp
end
ix 1
)
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
m ca i
5_ '__ U
Cla
ims
by
em
erg
ency
p
hy
sici
ans:
a)
Im
mo
bil
izat
ion (
N=
5,4
13
b) P
hysi
cal E
xam
(N=
34,5
7
c) C
on
sult
atio
n (
N=
66
8)
(N=
40,6
57
cla
ims)
re
late
d to
20
,43
1 w
om
en
(Det
aile
d li
stin
g in
A
pp
end
ix 1
)
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
c/l (U
•O O U
« O '> U VJ
u 5 u E 0 S u 0 . VJ 1
C O
Z
<L> U 3 O CC
<Ë a
VJ a>
T3 O O O
*_ O C Oû cd
•5 a
1 ON
1 û y
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
.2
u
Cla
ims
by
ort
ho
pae
dic
su
rgeo
ns:
a)
Pri
nci
pal
vis
it (N
= 1
0,6
87)
b) C
onsu
ltat
ion (N
=21,4
66)
c) F
oll
ow
-up v
isit
(N
=33,2
94;
(N=
65
,44
7 c
laim
s)
rela
ted to
25,7
62 w
om
en
(Det
aile
d li
stin
g in
A
pp
end
ix 1
)
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
.2
u
Cla
ims
by
ort
ho
pae
dic
su
rgeo
ns:
a)
Pri
nci
pal
vis
it (N
= 1
0,6
87)
b) C
onsu
ltat
ion (N
=21,4
66)
c) F
oll
ow
-up v
isit
(N
=33,2
94;
(N=
65
,44
7 c
laim
s)
rela
ted to
25,7
62 w
om
en
(Det
aile
d li
stin
g in
A
pp
end
ix 1
)
Sel
ecti
on o
f cla
ims
in R
AM
Q d
atab
ase
(N=
196.1
43 c
laim
s re
late
d to
41
.28
8 w
om
en)
C/5
<L> T1 O O crt U a '> <L>
U T3 C E u
IC ' 5 0 CL
00
.2
u
Cla
ims
by
ort
ho
pae
dic
su
rgeo
ns:
a)
Pri
nci
pal
vis
it (N
= 1
0,6
87)
b) C
onsu
ltat
ion (N
=21,4
66)
c) F
oll
ow
-up v
isit
(N
=33,2
94;
(N=
65
,44
7 c
laim
s)
rela
ted to
25,7
62 w
om
en
(Det
aile
d li
stin
g in
A
pp
end
ix 1
)
C/5
<L> T1 O O crt U a '> <L>
U T3 C E u
IC ' 5 0 CL
00
C/5
<L> T1 O O crt U a '> <L>
U T3 C E u
IC ' 5 0 CL
00
C/5
<L> T1 O O crt U a '> <L>
U T3 C E u
IC ' 5 0 CL
00
■C? «> •*« ^ p .
S r ^ ^ s S
C/5
<L> T1 O O crt U a '> <L>
U T3 C E u
IC ' 5 0 CL
00
.2
U
Cla
ims f
or:
a)
Im
mo
bil
izat
ion (N
=l.
b) O
pen
red
uct
ion (N
=l
c) C
lose
d re
duct
ion
(N=
(N=
16,6
87 c
laii
r re
late
d to
13,2
57 w
(D
etai
led
lis
tin
g A
pp
end
ix 1
)
Cla
ims f
or:
a)
Im
mo
bil
izat
ion (N
=l.
b) O
pen
red
uct
ion (N
=l
c) C
lose
d re
duct
ion
(N=
(N=
16,6
87 c
laii
r re
late
d to
13,2
57 w
(D
etai
led
lis
tin
g A
pp
end
ix 1
)
a _. 3 6X)
40
Recognizing Osteoporosis and its Consequences in Quebec (ROCQ) database.
A population-based cohort of clinically-assessed incident fracture cases recruited in the
same three health regions was needed to assess the sensitivity of the assessed algorithms.
ROCQ is an ongoing patient-health management program aimed at evaluating the
diagnostic and treatment care gaps for osteoporosis following a FF and subsequently
initiating and measuring interventions to decrease these care gaps in women 50 years of age
and over [138]. From September 2003 to September 2005, 18 hospitals, representing 70%
of the orthopedic practice in the three selected health regions, participated in the
recruitment of women who sustained a recent fracture to the ROCQ program. During the
study period, the ROCQ program was successful in recruiting and collecting clinical
information on 2,076 recently-fractured women.
Records of the ROCQ database were transmitted to the RAMQ services analysts and were
then linked to the physician's fee-for-services data set using the NAM as the linking code.
The NAM was then replaced by a coded anonymous unique personal identifier prior to
transmission to the study analyst.
2.4.2 Development and validation of algorithms
Fracture identification.
Three algorithms of incident fracture event identification were assessed using the above-
described PCD (Table 2.1 for all algorithms). Incident fracture was considered to be present
in:
Algorithm 1 : at least one claim associated with: a) medical service billing code limited to
fracture treatment: open reduction, closed reduction, immobilization or b) principal visit
with an OS combined with an ICD-9-CM fracture code or c) consultation with an OS
combined with an ICD-9-CM fracture code.
Algorithm 2: excludes cases of fractures identified by algorithm 1 with only one claim of a
principal visit with an OS. The addition of at least one other claim to the principal visit is
41
required to consider it an incident fracture. The added criteria eliminates cases indentify by
algorithm 1 that are most likely associated to long term follow-up of an old fracture.
Algorithm 3 : excludes fracture cases identified by algorithm 2 that only have one claim for
an OS consultation. The addition of at least one other claim to the consultation is required
to be considered as an incident fracture. Similar to algorithm 2, the added criteria eliminates
cases identified by algorithm 2 corresponding more to a long term follow-up of an old
fracture.
The claim that triggered the identification of a fracture was referred to as the "index claim".
Fracture occurrences were grouped according to the fracture site indicated by the specific
medical service billing code of the index claim or, if not specific to fracture treatment, the
ICD-9-CM code. To establish the complete sequence of medical care for each fracture, the
algorithms used any other claims (emergency room visit, follow-up visit with OS, etc.)
related to the same anatomical site. The date of fracture corresponded to the date ofthe first
claim in the sequence of medical care. For example, a humeral fracture could generate
claims for an emergency room visit, an orthopedic visit with immobilization of the fracture,
and an orthopaedic follow-up visit at four weeks. The algorithm would identify a new
fracture based on the index claim for immobilization. Subsequently, the algorithm would
link the two other claims with the index claim into a single sequence of clinical events. The
date of the first claim (medical care provided at the emergency room) would identify the
date of fracture. Finally, to minimize potential misclassification of the follow-up of a
fracture as a new incident fracture, a period less than or equal to six months between two
clinical sequences related to the same anatomical site for the fracture needed to be observed
in order to be considered a follow-up of the index incident fracture; otherwise it was
considered a new incident fracture event.
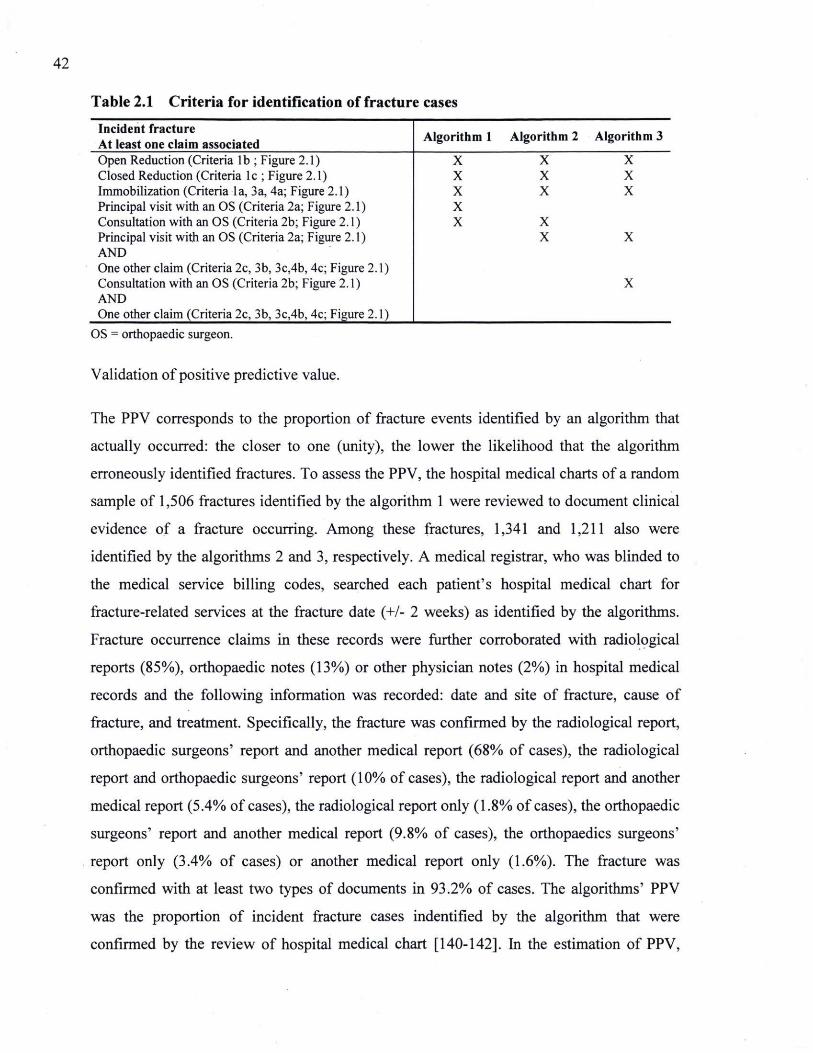
42
Table 2.1 Criteria for identification of fracture cases Incident fracture At least one claim associated Algorithm 1 Algorithm 2 Algorithm 3 Open Reduction (Criteria lb ; Figure 2.1) X X X Closed Reduction (Criteria lc ; Figure 2.1) X X X Immobilization (Criteria la, 3a, 4a; Figure 2.1) X X X Principal visit with an OS (Criteria 2a; Figure 2.1) X Consultation with an OS (Criteria 2b; Figure 2.1) X X Principal visit with an OS (Criteria 2a; Figure 2.1) X X AND One other claim (Criteria 2c, 3b, 3c,4b, 4c; Figure 2.1) Consultation with an OS (Criteria 2b; Figure 2.1) X AND One other claim (Criteria 2c, 3b, 3c,4b, 4c; Figure 2.1)
OS = orthopaedic surgeon.
Validation of positive predictive value.
The PPV corresponds to the proportion of fracture events identified by an algorithm that
actually occurred: the closer to one (unity), the lower the likelihood that the algorithm
erroneously identified fractures. To assess the PPV, the hospital medical charts of a random
sample of 1,506 fractures identified by the algorithm 1 were reviewed to document clinical
evidence of a fracture occurring. Among these fractures, 1,341 and 1,211 also were
identified by the algorithms 2 and 3, respectively. A medical registrar, who was blinded to
the medical service billing codes, searched each patient's hospital medical chart for
fracture-related services at the fracture date (+/- 2 weeks) as identified by the algorithms.
Fracture occurrence claims in these records were further corroborated with radiological
reports (85%), orthopaedic notes (13%) or other physician notes (2%) in hospital medical
records and the following information was recorded: date and site of fracture, cause of
fracture, and treatment. Specifically, the fracture was confirmed by the radiological report,
orthopaedic surgeons' report and another medical report (68% of cases), the radiological
report and orthopaedic surgeons' report (10% of cases), the radiological report and another
medical report (5.4% of cases), the radiological report only (1.8% of cases), the orthopaedic
surgeons' report and another medical report (9.8% of cases), the orthopaedics surgeons'
report only (3.4% of cases) or another medical report only (1.6%). The fracture was
confirmed with at least two types of documents in 93.2% of cases. The algorithms' PPV
was the proportion of incident fracture cases indentified by the algorithm that were
confirmed by the review of hospital medical chart [140-142]. In the estimation of PPV,
43
patients' hospital medical charts were considered as the gold standard. PPVs were
estimated for each fracture site.
Validation of sensitivity.
Sensitivity assesses the capacity of a tool to correctly identify cases. To estimate the
sensitivity of each algorithm, the clinical information collected on the 2,076 women
recruited in the ROCQ program was compared with information provided from the
algorithms for the same women. An algorithm's sensitivity was estimated by the proportion
of actual fractures (ROCQ cohort) that were correctly identified by the algorithms [140-
142]. In the estimation of sensitivity, clinical information from women enrolled in the
ROCQ cohort was used as the gold standard. The sensitivity was calculated by fracture site.
An algorithm with a sensitivity value close to one has almost no false-negative fracture
cases.
The 95% confidence intervals for PPV and sensitivity were calculated by assuming a
normal approximation for a binomial proportion.
2.4.2 Assessing the performance of the algorithms
The overall performance of the algorithms was compared using a graphical representation
of likelihood ratios [143]. Ratios ofthe likelihood of being an actual fracture case over the
likelihood of being disease-free are calculated for those who are and are not identified as
being a fracture case by an algorithm. Graphical representations of these two likelihood
ratio lines for any single algorithm allow for the assessment of their relative performance,
falling into one of the four following categories: overall superiority, superiority for
confirming the absence of a fracture, superiority for confirming the presence of a fracture,
and overall inferiority. Performance comparisons of the three algorithms were performed
for each fracture site grouping.
2.5 Results Overall 196,143 claims related to 41,288 women were extracted from the PCD (Figure 2.1).
Among these women, 57% had less than three claims extracted during the study period with
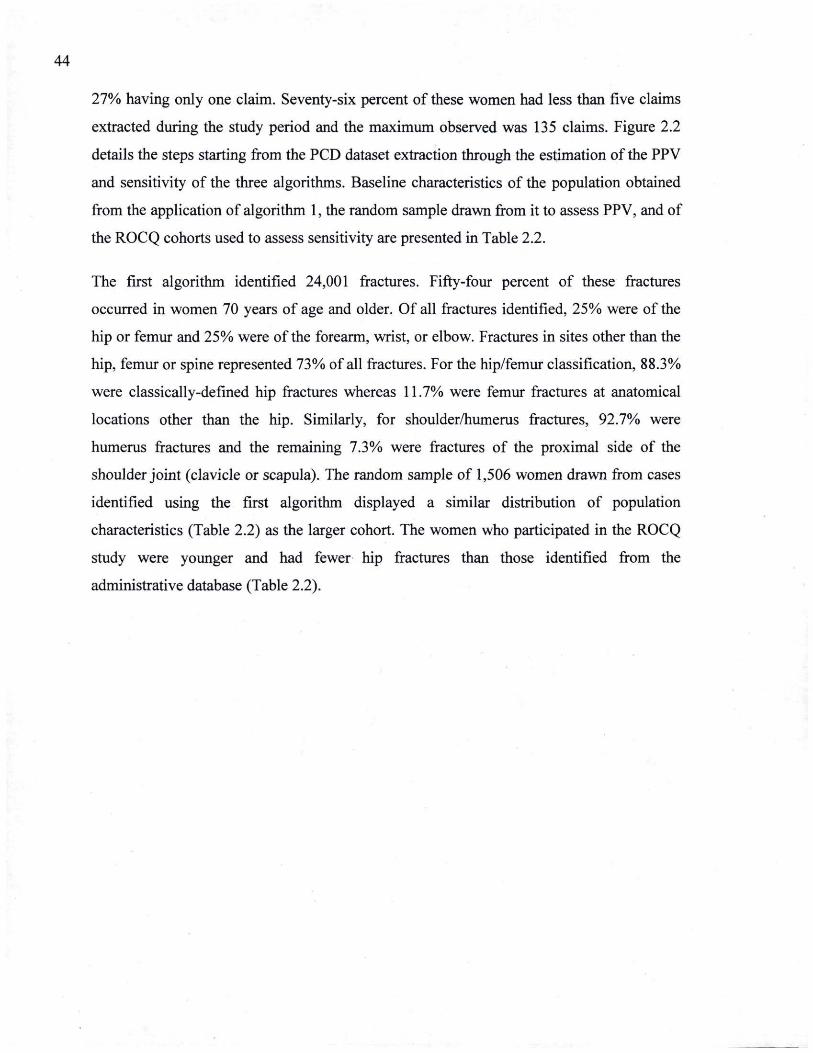
44
27% having only one claim. Seventy-six percent of these women had less than five claims
extracted during the study period and the maximum observed was 135 claims. Figure 2.2
details the steps starting from the PCD dataset extraction through the estimation ofthe PPV
and sensitivity of the three algorithms. Baseline characteristics of the population obtained
from the application of algorithm 1, the random sample drawn from it to assess PPV, and of
the ROCQ cohorts used to assess sensitivity are presented in Table 2.2.
The first algorithm identified 24,001 fractures. Fifty-four percent of these fractures
occurred in women 70 years of age and older. Of all fractures identified, 25% were of the
hip or femur and 25% were ofthe forearm, wrist, or elbow. Fractures in sites other than the
hip, femur or spine represented 73% of all fractures. For the hip/femur classification, 88.3%
were classically-defined hip fractures whereas 11.7% were femur fractures at anatomical
locations other than the hip. Similarly, for shoulder/humerus fractures, 92.7% were
humerus fractures and the remaining 7.3% were fractures of the proximal side of the
shoulder joint (clavicle or scapula). The random sample of 1,506 women drawn from cases
identified using the first algorithm displayed a similar distribution of population
characteristics (Table 2.2) as the larger cohort. The women who participated in the ROCQ
study were younger and had fewer hip fractures than those identified from the
administrative database (Table 2.2).
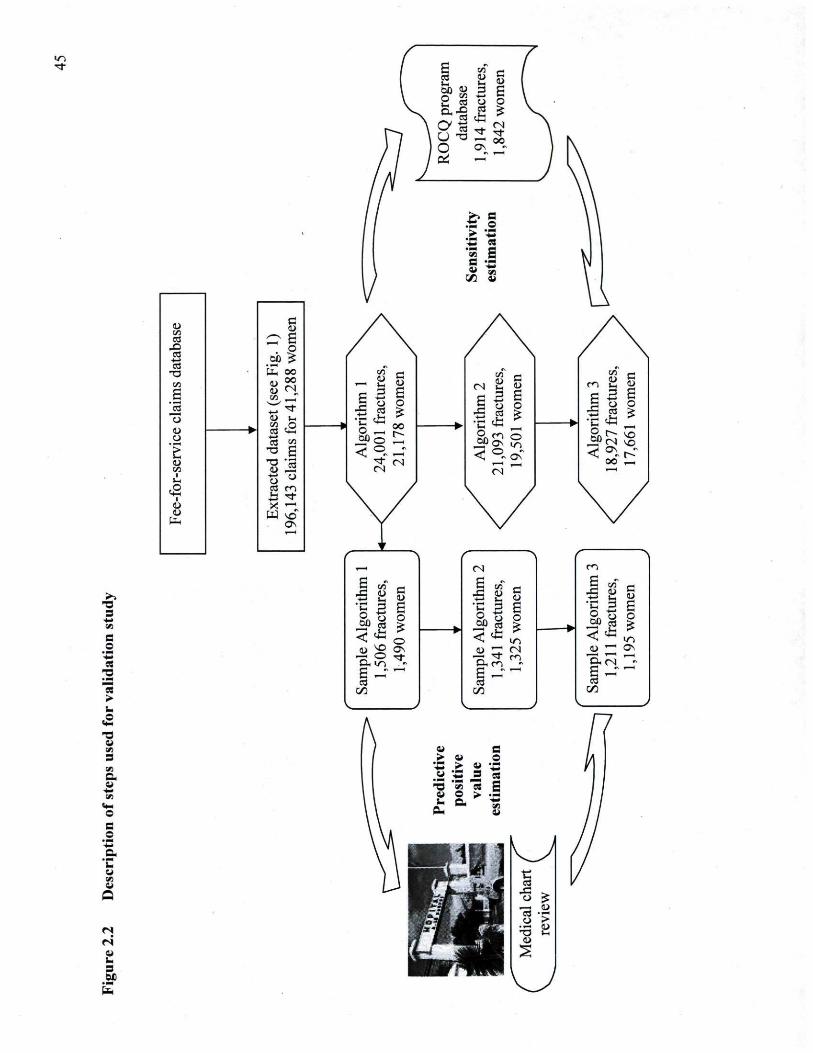
•V.
ID VJ
a ID VJ
a
d u
S? S o
ab JS / iS
a fa oo VJ
B see
1,28
2 « "* o U I H
<D k C/3 O h <D k C/3 O
w <D P C/3 O
w o 53 22 1 •9 g C i? 'â c/3 u 2
■M CJ IH O w
l _9 cd r«"> <•(—1
£ ■* <i> x " l <D
fa PJ SO
Os
/
__ u u
o
3 •M O o3
S+I
O
E o
< © . — i
"* <N (N
(N _. i i s
c <D
3 4—» s y O o
'C o Oû
1 m ON
o
< ■o ON"
(N
m VJ i i I H
4 ^ ^
o CÛ
3 O 03
r
E o
< Os r." OO , H
£ C o « «s o
>
S VJ
a.
© s c •s • _ ■
u 09 i i
Q
1
go
( " r H
C <D c
Alg
ori
t fr
actu
r
Ê o o
(U sg ON
•a ° si&, ir> H <—1
c/_ v
Sam
ple
Alg
ori
thm
2
1,3
41 fr
actu
res,
1,3
25 w
om
en
Sam
ple
Alg
ori
thm
2
1,3
41 fr
actu
res,
1,3
25 w
om
en
r " m S W rt T^ ft_ I H ~ I H D
;ori
ct
u
om
►
<u '—' ON
D.CN ^
s *"* t/_
u c . ; ■> i i o "C .> a u *^H 9 C3 3 'S "S I w O >
PH c B_
LJ ■g c3
A £ O £ _ « rt _o >
u •3 fc-
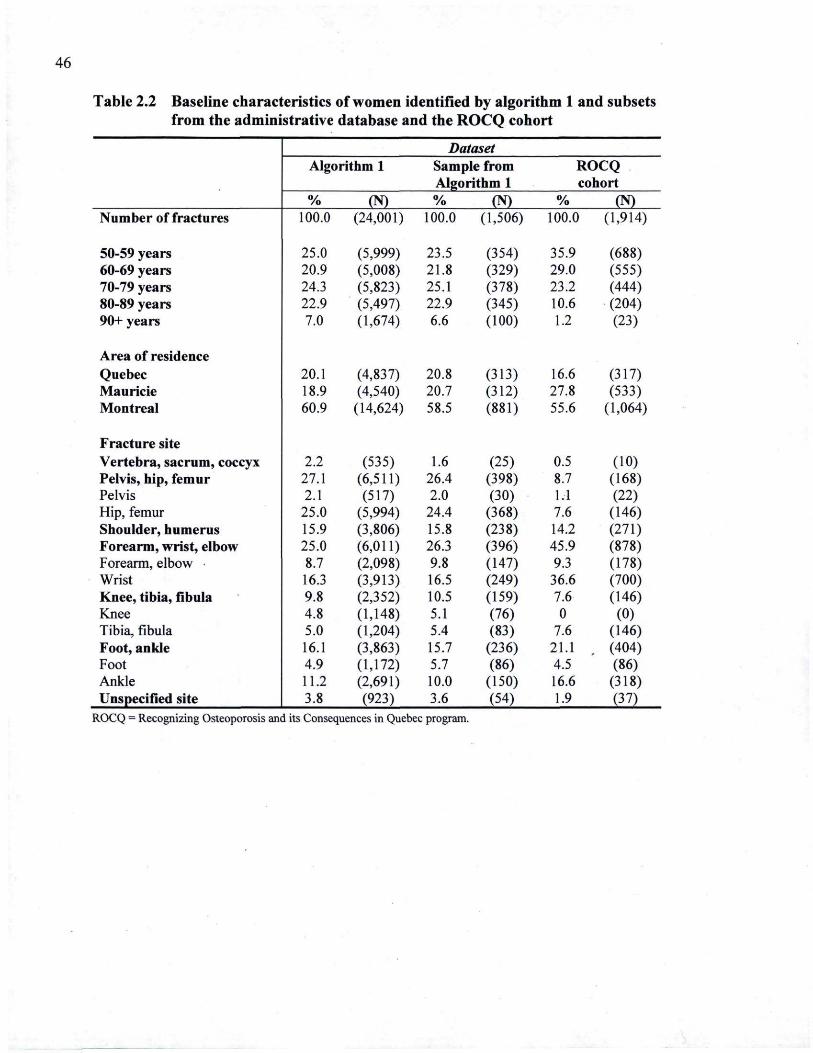
46
Table 2.2 Baseline characteristics of women identified by algorithm 1 and subsets from the administrative database and the ROCQ cohort
Dataset Algorithm 1 Sample .from ROCQ
Algorithm 1 cohort % (N) % (N) % (N)
Number of fractures 100.0 (24,001) 100.0 (1,506) 100.0 (1,914)
50-59 years 25.0 (5,999) 23.5 (354) 35.9 (688) 60-69 years 20.9 (5,008) 21.8 (329) 29.0 (555) 70-79 years 24.3 (5,823) 25.1 (378) 23.2 (444) 80-89 years 22.9 (5,497) 22.9 (345) 10.6 (204) 90+ years 7.0 (1,674) 6.6 (100) 1.2 (23)
Area of residence Quebec 20.1 (4,837) 20.8 (313) 16.6 (317) Mauricie 18.9 (4,540) 20.7 (312) 27.8 (533) Montreal 60.9 (14,624) 58.5 (881) 55.6 (1,064)
Fracture site Vertebra, sacrum, coccyx 2.2 (535) 1.6 (25) 0.5 (10) Pelvis, hip, femur 27.1 (6,511) 26.4 (398) 8.7 (168) Pelvis 2.1 (517) 2.0 (30) 1.1 (22) Hip, femur 25.0 (5,994) 24.4 (368) 7.6 (146) Shoulder, humerus 15.9 (3,806) 15.8 (238) 14.2 (271) Forearm, wrist, elbow 25.0 (6,011) 26.3 (396) 45.9 (878) Forearm, elbow 8.7 (2,098) 9.8 (147) 9.3 (178) Wrist 16.3 (3,913) 16.5 (249) 36.6 (700) Knee, tibia, fibula 9.8 (2,352) 10.5 (159) 7.6 (146) Knee 4.8 (1,148) 5.1 (76) 0 (0) Tibia, fibula 5.0 (1,204) 5.4 (83) 7.6 (146) Foot, ankle 16.1 (3,863) 15.7 (236) 21.1 (404) Foot 4.9 (1,172) 5.7 (86) 4.5 (86) Ankle 11.2 (2,691) 10.0 (150) 16.6 (318) Unspecified site 3.8 (923) 3.6 (54) 1.9 (37)
ROCQ = Recognizing Osteoporosis and its Consequences in Quebec program.
47
Table 2.3 presents the PPVs for the three algorithms by index claim and by fracture site.
The PPV varied according to the index claim. Compared to algorithm 1, the criteria added
in algorithm 2 and 3 improved the PPV noticeably. The PPV was high when the index
claim corresponded to a specific treatment. In fact, when the index claim was designated as
an open reduction, a closed reduction or an immobilization as the most significant medical
treatment, the PPV with algorithm 3 was 0.96, 0.98 and 0.85, respectively. For principal
visit and consultation with an OS, the PPV was 0.71 and 0.80, respectively. The PPV
varied according to fracture site. Compared to algorithm 1, algorithm 3 improved the PPV
noticeably for all fracture sites, except for fractures of the vertebrae, sacrum and coccyx
combined and for fractures of the forearm, wrist and elbow combined. The highest PPVs
are obtained for fractures ofthe wrist or hip/femur with respective values of 0.96 and 0.93.
PPVs for forearm and elbow combined, shoulder and humerus combined, tibia and fibula
combined or for foot and ankle combined were between 0.88 and 0.90. Similar PPV results
were observed for fractures of the vertebra, sacrum, or coccyx combined sites and the
pelvis site (0.82 and 0.81, respectively). The lowest PPV was with the knee site (0.63).
Among the true positives with algorithm 3, the fracture site identified by the algorithm was
concordant with a fracture site in the patients' hospital medical records in 95% of cases.
Moreover, the date of fracture was accurately identified by the algorithm in 66% of the
cohort, and was within two days of the actual date of the fracture in 88% of cases. Ninety-
six percent of open reduction cases as identified by algorithm 3 were confirmed having had
surgery by the patient's hospital medical charts (for a comparison of algorithms please see
Table 2.3).
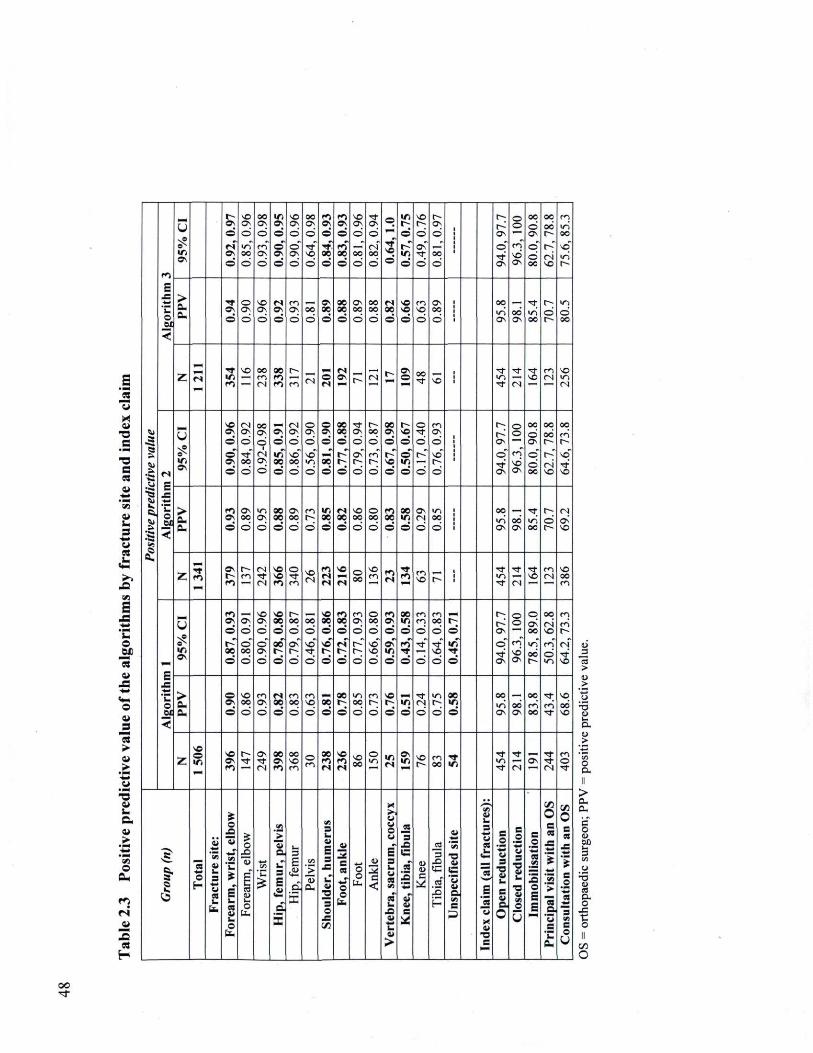
u
i i a e
a c «
a _. 3 ** u
o M
13 a
o i i 2
13 >
fe
i l
c i l fe
o Cu
r i
cs H
«1
« >
1 •e. S!
S ? fi
E _= 'C o <
Û
w. ON
Ov
O
«N ON ©
NO Ov. ©
0 0 o
oo Ov
d m d
u . Ov ©
© Ov ©
ND Ov
d © Ov d
0 0 Ov d tf NO d
ro Ov ©
•tf 00 ©
ro Ov ©
ro 0 0 ©
NO Ov d
OO d
tfON d oo d
©
NO ©
©
r» m ©
NO r ©
Ov
tf d
rOv d
0 0 d
r~
Ov
©
ON
© ©
ro ' NO ON
00 d Cv
© d 0 0
oo oo t ^ r" CN NO
r o I O OO
vo" i r i r
«1
« >
1 •e. S!
S ? fi
E _= 'C o <
> a. Cu
tfON ©
o Ov ©
NO ON d
es OV ©
r o Ov d
0 0 d
Ov 00 ©
0 0 0 0 ©
ov. OO ©
oo 0 0 ©
«S 0 0 ©
N O NO ©
r o NO ©
ov. 0 0 d
OO i r i ON
oo O N
tf Ki 00
c
d d oo
«1
« >
1 •e. S!
S ? fi
E _= 'C o <
Z »N "W m r O
NO OO rr ,
0 0 ro ro r i e
«s «s Ov r CN •r Ov
© oo
tf NO i ■ i
"tf ■ t f
( N
tf NO
r o CN
NO
CN
«1
« >
1 •e. S!
S ? fi
E 4 ^
<
Û
i n ON
NO ON ©
© Ov. ©
<N ON d
oc ©
0 0 ON d <N Ov ©
Ov ©
VJ 0 0 ©
CN Ov d NO OO d
© ON d NO I/O d
© OV ©
ôë ©
0 0 0 0
©
©
tf Ov d Ov
d
r 0 0 d co r
d
0 0 Ov
©
rNO ©
NO ©
© m ©
© tf ©
d
r o Ov d NO
d
Ov
d" Ov
© ©
r o NO Ov
OO d Ov © " d 0 0
oo 0 0 t 4
r"
NO
oq co f
vo" tf NO
«1
« >
1 •e. S!
S ? fi
E 4 ^
<
> û . Cu
ro ON ©
Ov 0 0 ©
i o O N
d 0 0 0 0 ©
ov oo d
r o r ©
i n oe 9
es 0 0 ©
NO 0 0 d
© 0 0 d
ro 0 0 ©
0 0 i n ©
Ov ( N ©
i r . 0 0 d
OO v j Ov
00 Ov
tf i r i 0 0
r— d
<N ON NO
«1
« >
1 •e. S!
S ? fi
E 4 ^
<
Z i f ro
Ov
<*> rco
( N tf ( N
NO NO ro
o tf r o
NO ( N
ro rs rs
NO
rs © OO
NO r o ro
rs •tf ro H
r o NO r*
i i i
■ t f V J
tf ( N
tf NO
c o C J
NO OO CO
«1
« >
1 •e. S!
S ? fi
E x : H
*__ o en
<
Û S?
Ov ©
0 0 ©
Ov d © oo ©
NO O N
d © Ov d
NO 0 0
e 0 0
©
OO d Ov r 4
d
0 0 d NO
d
VO OC ©
NO
©
ro 0 0
©
rs
©
r o
d
r
d
© 00 d NO ND ©
ro OV
©
Ov m ©
0 0 m © ro TT ©
CO r o d ■ t f
d
co 0 0
d ■ t f
NO d
©
m
©
F* Ov
O
Ov
© ©
ro" NO Cv
© as oo i/o" oo •r
oo
NO r o " © V J
r o r o t~ <N
tf NO
«1
« >
1 •e. S!
S ? fi
E x : H
*__ o en
<
> cu cu
© Ov ©
NO OO ©
r o O N
©
f N 0 0 ©
r o 0 0 d
r o NO d
0 0 ©
0 0
©
I O oo ©
CO r
d
NO
© !n ©
•tf CN ©
i o C
d
0 0 m ©
0 0
ON 0 0 Ov
0 0 r o oo
■ t f
r o ■ t f
NO 00 NO
«1
« >
1 •e. S!
S ? fi
E x : H
*__ o en
<
z NO o NC
Ov r4
tf Ov
CN
0 0 Ov r o
oo NO r o
© r o
0 0 ro rs
NO ro rs
NO oo
© KO m
rs ON m NO
r(O 00 m
■ t f V J
tf ( N
Ofi tf" ■ t f
ro © tf
1 — o
iî m* M
u 3
4 * 4 4 1
u .
O £ a i
M 'C
i u cs i i i . o
u
o £
ca D G O
CL.
V i
VJ
'_> i i O . _T 3
E
d £
4 4 —
3 E fi ci 'f
V i
> (U
a,
V i 3
01 E 3 _= C i i
"3 O _=
c « *_r o o
b .
o o
U .
■ _ _ :
c
<
■ > >
u o u
E" 3 _. U cs
es' _. X ! a i U a i >
JS 3
C
S
33 oT a i =
u
_2
_çS 3
IC
a i
' v t ■ a <Si
ç 'S a i
a C 3
BB O . 3 •** U es
<h M E 'Ji •X Oi
■ o C
C , o o 3
■g a i
3 a i a . 0
C
_o
ai 3
■o ai _. •a a i VI
o
Û
C _o
M
.__ J 5 o E E
t » O c es
J =
■ —
'__ "5 a
' û ■ç. Cu
Cfl 0 c es
_= l C
. o 'm* es
ta* "5 V i c o
u
o
> a. a. c o Oû
o <J> a D. o
je
e o
oo
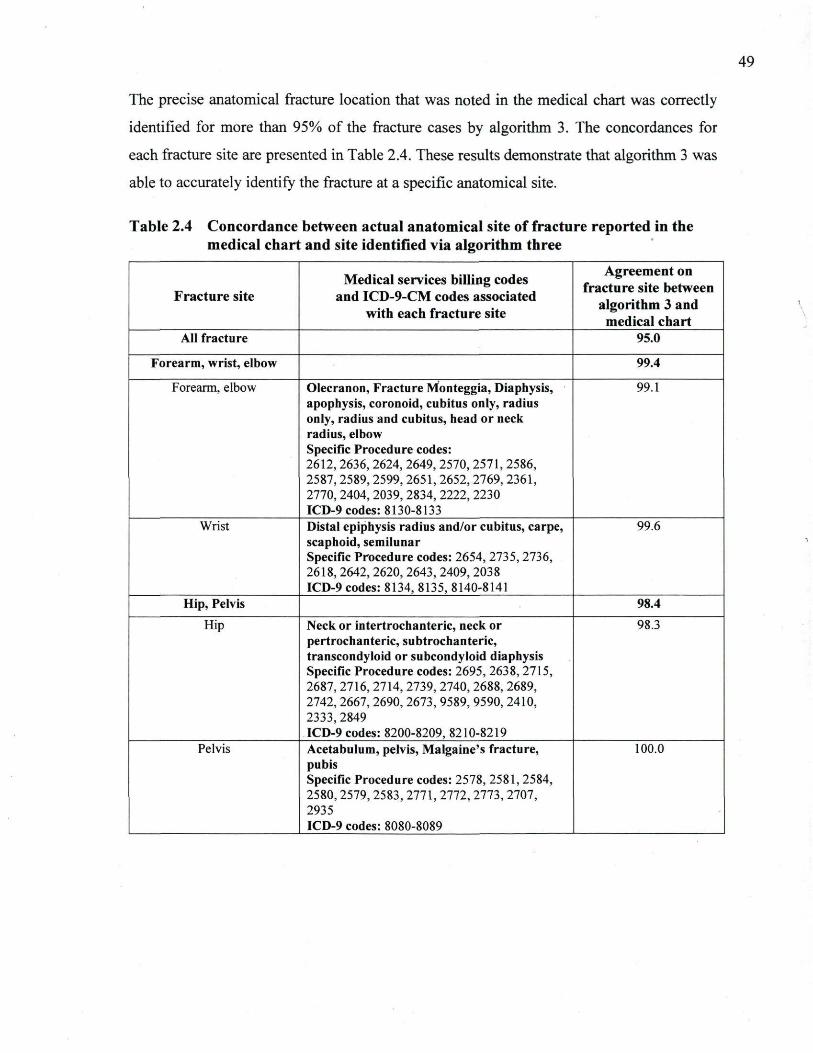
49
The precise .anatomical fracture location that was noted in the medical chart was correctly
identified for more than 95% ofthe fracture cases by algorithm 3. The concordances for
each fracture site are presented in Table 2.4. These results demonstrate that algorithm 3 was
able to accurately identify the fracture at a specific anatomical site.
Table 2.4 Concordance between actual anatomical site of fracture reported in the medical chart and site identified via algorithm three
Fracture site Medical services billing codes
and ICD-9-CM codes associated with each fracture site
Agreement on fracture site between
algorithm 3 and medical chart
All fracture 95.0
Forearm, wrist, elbow 99.4
Forearm, elbow Olecranon, Fracture Monteggia, Diaphysis, apophysis, coronoid, cubitus only, radius only, radius and cubitus, head or neck radius, elbow Specific Procedure codes: 2612, 2636,2624, 2649, 2570, 2571, 2586, 2587, 2589,2599, 2651, 2652, 2769, 2361, 2770, 2404,2039, 2834, 2222, 2230 ICD-9 codes: 8130-8133
99.1
Wrist Distal epiphysis radius and/or cubitus, carpe, scaphoid, semilunar Specific Procedure codes: 2654, 2735,2736, 2618, 2642, 2620, 2643, 2409, 2038 ICD-9 codes: 8134, 8135, 8140-8141
99.6
Hip, Pelvis 98.4 Hip Neck or intertrochanteric, neck or
pertrochanteric, subtrochanteric, transcondyloid or subcondyloid diaphysis Specific Procedure codes: 2695, 2638, 2715, 2687, 2716,2714, 2739, 2740, 2688, 2689, 2742,2667, 2690, 2673, 9589, 9590, 2410, 2333,2849 ICD-9 codes: 8200-8209, 8210-8219
98.3
Pelvis Acetabulum, pelvis, Malgaine's fracture, pubis Specific Procedure codes: 2578, 2581,2584, 2580,2579, 2583, 2771, 2772, 2773, 2707, 2935 ICD-9 codes: 8080-8089
100.0
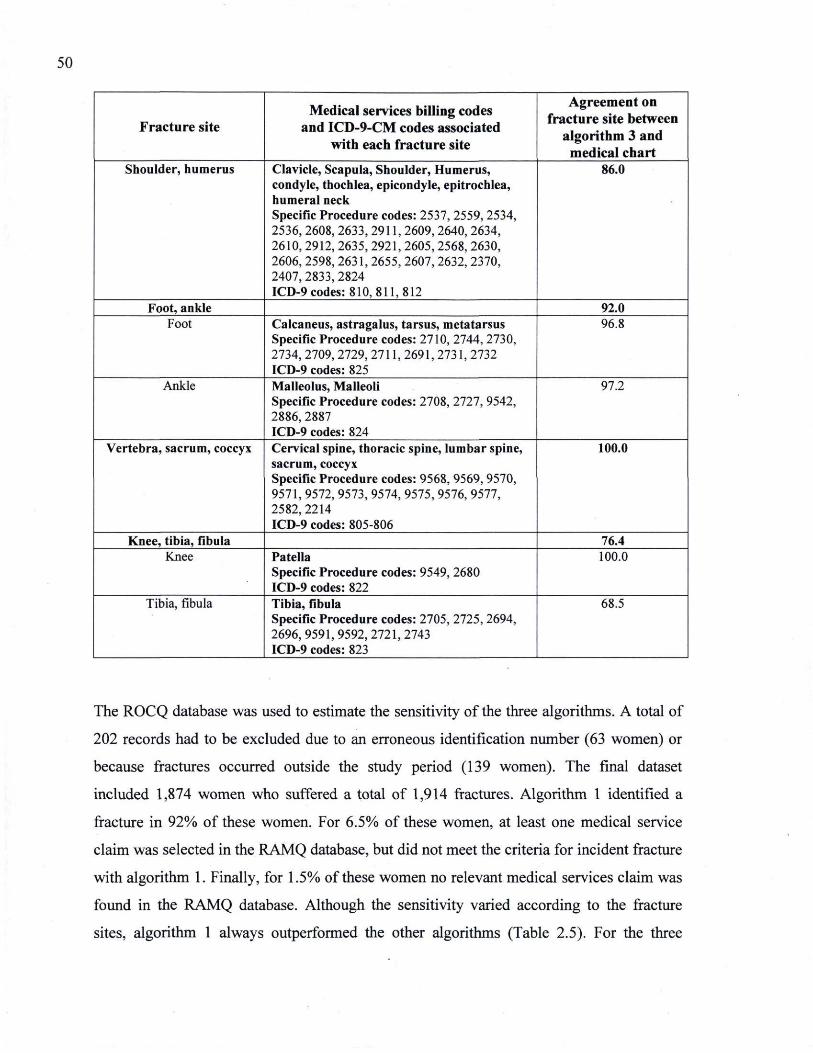
50
Fracture site Medical services billing codes
and ICD-9-CM codes associated with each fracture site
Agreement on fracture site between
algorithm 3 and medical chart
Shoulder, humerus Clavicle, Scapula, Shoulder, Humerus, condyle, thochlea, epicondyle, epitrochlea, humeral neck Specific Procedure codes: 2537, 2559,2534, 2536, 2608,2633, 2911, 2609,2640, 2634, 2610, 2912,2635, 2921, 2605,2568, 2630, 2606, 2598,2631, 2655, 2607,2632, 2370, 2407, 2833, 2824 ICD-9 codes: 810, 811,812
86.0
Foot, ankle 92.0 Foot Calcaneus, astragalus, tarsus, metatarsus
Specific Procedure codes: 2710, 2744,2730, 2734, 2709,2729, 2711, 2691,2731,2732 ICD-9 codes: 825
96.8
Ankle Malleolus, Malleoli Specific Procedure codes: 2708, 2727, 9542, 2886, 2887 ICD-9 codes: 824
97.2
Vertebra, sacrum, coccyx Cervical spine, thoracic spine, lumbar spine, sacrum, coccyx Specific Procedure codes: 9568, 9569, 9570, 9571, 9572, 9573, 9574, 9575, 9576, 9577, 2582,2214 ICD-9 codes: 805-806
100.0
Knee, tibia, fibula 76.4 Knee Patella
Specific Procedure codes: 9549, 2680 ICD-9 codes: 822
100.0
Tibia, fibula Tibia, fibula Specific Procedure codes: 2705, 2725,2694, 2696,9591,9592,2721,2743 ICD-9 codes: 823
68.5
The ROCQ database was used to estimate the sensitivity ofthe three algorithms. A total of
202 records had to be excluded due to an erroneous identification number (63 women) or
because fractures occurred outside the study period (139 women). The final dataset
included 1,874 women who suffered a total of 1,914 fractures. Algorithm 1 identified a
fracture in 92% of these women. For 6.5% of these women, at least one medical service
claim was selected in the RAMQ database, but did not meet the criteria for incident fracture
with algorithm 1. Finally, for 1.5% of these women no relevant medical services claim was
found in the RAMQ database. Although the sensitivity varied according to the fracture
sites, algorithm 1 always outperformed the other algorithms (Table 2.5). For the three
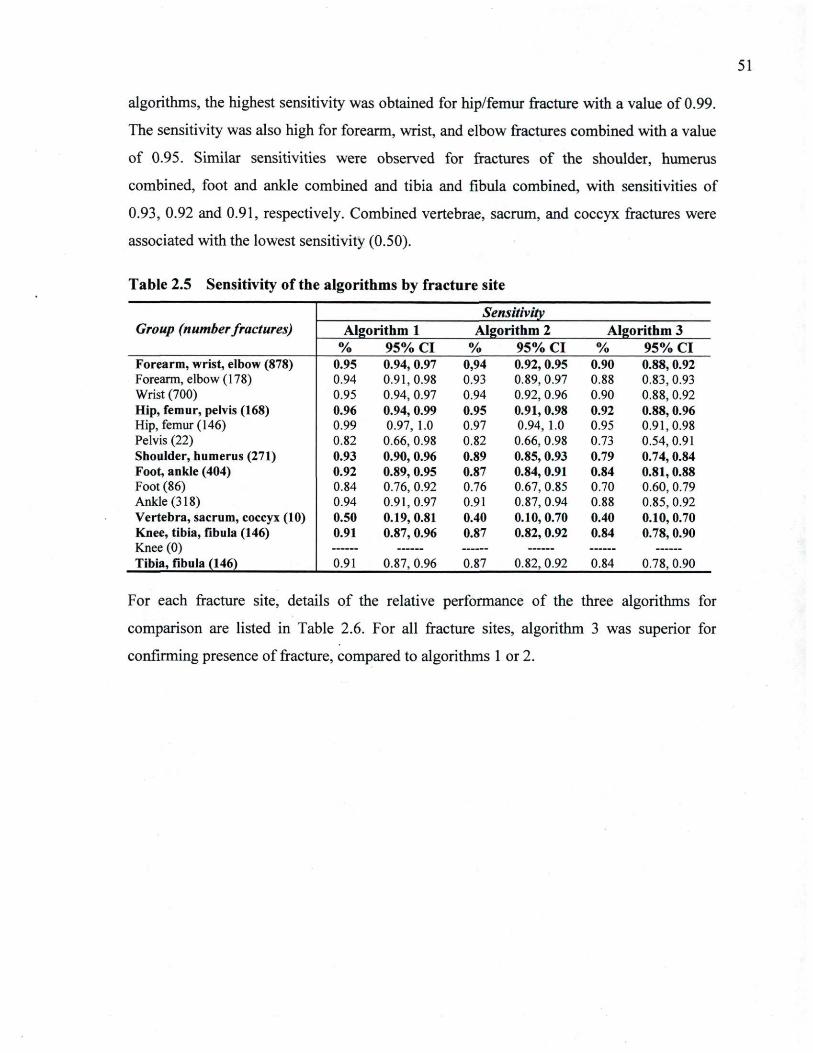
51
algorithms, the highest sensitivity was obtained for hip/femur fracture with a value of 0.99.
The sensitivity was also high for forearm, wrist, and elbow fractures combined with a value
of 0.95. Similar sensitivities were observed for fractures of the shoulder, humerus
combined, foot and ankle combined and tibia and fibula combined, with sensitivities of
0.93, 0.92 and 0.91, respectively. Combined vertebrae, sacrum, and coccyx fractures were
associated with the lowest sensitivity (0.50).
Table 2.5 Sensitivity of the algorithms by fracture site
Sensitivity Group (number fractures) Algorithm 1 Algorithm 2 Algorithm 3
% 9 5 % CI % 9 5 % CI % 9 5 % CI Forearm, wrist, elbow (878) 0.95 0.94, 0.97 0,94 0.92,0.95 0.90 0.88,0.92 Fore-arm, elbow (178) 0.94 0.91,0.98 0.93 0.89, 0.97 0.88 0.83,0.93 Wrist (700) 0.95 0.94, 0.97 0.94 0.92, 0.96 0.90 0.88, 0.92 Hip, femur, pelvis (168) 0.96 0.94, 0.99 0.95 0.91,0.98 0.92 0.88, 0.96 Hip, femur (146) 0.99 0.97, 1.0 0.97 0.94, 1.0 0.95 0.91,0.98 Pelvis (22) 0.82 0.66, 0.98 0.82 0.66, 0.98 0.73 0.54,0.91 Shoulder, humerus (271) 0.93 0.90, 0.96 0.89 0.85, 0.93 0.79 0.74, 0.84 Foot, ankle (404) 0.92 0.89, 0.95 0.87 0.84, 0.91 0.84 0.81,0.88 Foot (86) 0.84 0.76, 0.92 0.76 0.67, 0.85 0.70 0.60, 0.79 Ankle (318) 0.94 0.91, 0.97 0.91 0.87, 0.94 0.88 0.85, 0.92 Vertebra, sacrum, coccyx (10) 0.50 0.19, 0.81 0.40 0.10,0.70 0.40 0.10,0.70 Knee, tibia, fibula (146) 0.91 0.87, 0.96 0.87 0.82, 0.92 0.84 0.78,0.90 Knee (0) Tibia, fibula (146) 0.91 0.87, 0.96 0.87 0.82, 0.92 0.84 0.78, 0.90
For each fracture site, details of the relative performance of the three algorithms for
comparison are listed in Table 2.6. For all fracture sites, algorithm 3 was superior for
confirming presence of fracture, compared to algorithms 1 or 2.
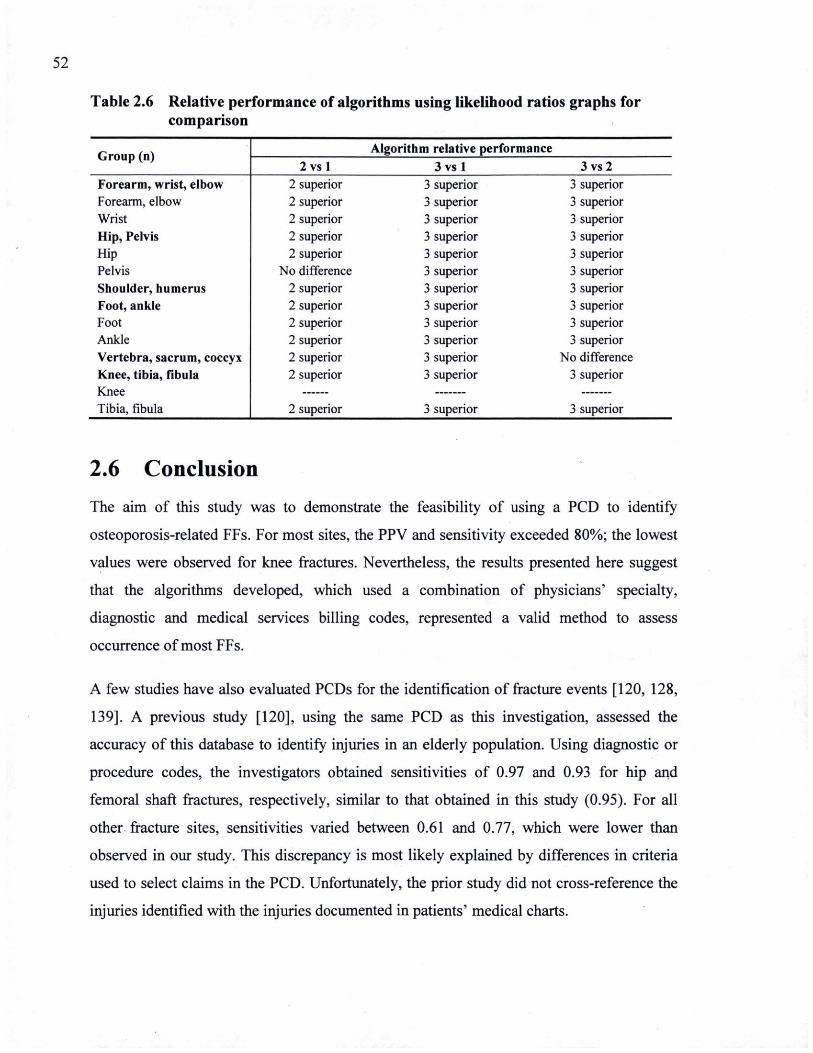
52
Table 2.6 Relative performance of algorithms using likelihood ratios graphs for comparison
Group (n) Algorithm relative performance Group (n) 2 v s l 3 v s l 3vs2
Forearm, wrist, elbow Forearm, elbow
2 superior 2 superior
3 superior 3 superior
3 superior 3 superior
Wrist Hip, Pelvis
2 superior 2 superior
3 superior 3 superior
3 superior 3 superior
Hip Pelvis Shoulder, humerus Foot, ankle
2 superior No difference
2 superior 2 superior
3 superior 3 superior 3 superior 3 superior
3 superior 3 superior 3 superior 3 superior
Foot Ankle Vertebra, sacrum, coccyx Knee, tibia, fibula Knee
2 superior 2 superior 2 superior 2 superior
3 superior 3 superior 3 superior 3 superior
3 superior 3 superior
No difference 3 superior
Tibia, fibula 2 superior 3 superior 3 superior
2.6 Conclusion The aim of this study was to demonstrate the feasibility of using a PCD to identify
osteoporosis-related FFs. For most sites, the PPV and sensitivity exceeded 80%; the lowest
values were observed for knee fractures. Nevertheless, the results presented here suggest
that the algorithms developed, which used a combination of physicians' specialty,
diagnostic and medical services billing codes, represented a valid method to assess
occurrence of most FFs.
A few studies have also evaluated PCDs for the identification of fracture events [120, 128,
139]. A previous study [120], using the same PCD as this investigation, assessed the
accuracy of this database to identify injuries in an elderly population. Using diagnostic or
procedure codes, the investigators obtained sensitivities of 0.97 and 0.93 for hip and
femoral shaft fractures, respectively, similar to that obtained in this study (0.95). For all
other fracture sites, sensitivities varied between 0.61 and 0.77, which were lower than
observed in our study. This discrepancy is most likely explained by differences in criteria
used to select claims in the PCD. Unfortunately, the prior study did not cross-reference the
injuries identified with the injuries documented in patients' medical charts.
53
A study by Ray et al. [128] long-ago demonstrated that Medicare data files (Medicare
inpatient, emergency room, hospital outpatient and physician claims) could be used to
accurately identify fractures in an elderly population. For almost all fracture sites, the PPV
and sensitivity exceeded the values observed in our study. The main reason for their
increased analytical sensitivity was likely due to their use of discharge diagnosis data from
a hospitalization database which increased the validity of their algorithms; further, the
authors acknowledged that their methodology tended to overestimate sensitivity. In another
investigation, the validity of using an administrative claims database to identify vertebral
compression fractures was assessed [139]. In this investigation, medical claims had a high
PPV for the identification of confirmed clinical vertebral fractures, but detected fewer than
half of vertebral fracture cases, since at least half of vertebral fractures did not come to
clinical attention. These results demonstrate why vertebral fractures cannot be accurately
assessed by administrative claims databases because they are not reliably diagnosed by the
health care services, or recognized by the patients [128, 146].
With the overall prevalence of osteoporosis expected to increase in the coming years, the
availability of valid tools for FF observation will become increasingly important. In this
context, a low false-positive rate is important (high PPV). A high sensitivity is desirable
because it suggests that the algorithm is capturing most of the fracture cases. In this study,
with the exception of vertebral fracture, the high PPVs and sensitivities provide support for
using PCDs to establish and maintain surveillance systems for fractures.
A number of limitations of this study need to be addressed. First, the study was not
designed to investigate negative predictive values. Second, the validity was evaluated in a
generally elderly population of women, which represents the highest proportion of women
with fractures, and it is possible that these results could not be generalized to younger
populations or to men. Third, the accuracy of our estimate of PPV primarily depends upon
the quality of the data in hospital medical records (the "gold standard"). Since most
fractures are readily diagnosed, this should not be a major source of error. However, in a
few cases with suspected symptoms consistent with a fracture, we considered that the
fractures were not confirmed by the medical records; consequently, some misclassifications
may have occurred. Fourth, reviews of the radiograph reports were not performed by a
54
second reviewer. Fifth, in our study, no procedure for eliminating fractures related to motor
vehicles accidents or malignancies was used. However, some studies have shown that the
rate of these fractures is quite low and that more that 80% of fractures in patients 50 years
of age and older are related to osteoporosis [4, 146]. Sixth, to minimize the double-coding
of the same fracture, a washout period of six months was used, as proposed by our expert
panel and confirmed by sensitivity analyses. Any new fractures during this washout period
may have filtered out some new subsequent incident fractures. Seventh, the accuracy ofthe
algorithms is dependent ofthe billing codes used for claims, thus any change in coding may
affect its validity. However, the billing codes are generic and easily interchangeable with
billing codes used in any PCD allowing generalizibility of the proposed algorithm for
fracture detection to other PCDs. Eighth, only one medical archivist reviewed the medical
files so it was impossible to assess the agreement between different reviewers. Ninth, the
small sample size for fractures of the vertebra, sacrum, coccyx combined and pelvis sites
limited the ability to draw reliable conclusions concerning these fractures. Vertebral
fractures are most often asymptomatic and do not come to clinical attention [144, 145], thus
largely precluding the use of PCDs for the estimation of the incidence of these fractures.
Finally, this method cannot be utilized in populations that do not use a universal healthcare
plan like that which is found in Quebec. Moreover, in Quebec more than 94% of physicians
are paid directly via the submission of billing claims which may not necessarily be the case
for all provinces in Canada.
In summary, this analysis shows that PCDs are reliable for the identification of incident
non-vertebral fractures. The methodology developed here offers the possibility to establish
and maintain a surveillance program for fractures. This tool may be particularly useful for
describing the burden, resources utilization and economic implication of non-vertebral
osteoporosis-related fractures on the health care system.
2.7 Acknowledgments This work was funded by an unrestricted grant from Sender Canada Inc. It is also part of
the study Recognizing Osteoporosis and its Consequences in Québec (ROCQ, which has
been made possible through the support of founding partners Merck Canada , sanofi-aventis
Canada Inc., and Warner Chilcott, as well as major partner Amgen Canada Inc. and minor
55
partners Eli Lilly Canada Inc. and Novartis Pharma Canada Inc. There are no other
conflicts of interest to declare.
We would like to acknowledge the important contribution of medical archivist
Karine Picard who conducted the review of cases in hospitals' medical records and
Dr. K. Shawn Davison for revision ofthe manuscript.
57
Chapitre 3
Taux d'incidence des fractures et leurs impacts sur la mortalité des femmes au Québec, Canada
Fracture rates and fracture-associated mortality of women in Quebec, Canada
L'objectif de ce chapitre est de présenter les résultats de l'étude réalisée afin de quantifier les taux d'incidence des fractures et d'évaluer leurs impacts sur la survie des patientes de 50 ans et plus.
Les résultats de cette étude ont été présentés au congrès annuel de l'American Society for Bone and Mineral Research (ASBMR) en octobre 2010 sous la forme d'une présentation par affiche. Les auteurs sont Sonia Jean, Bernard Candas, Etienne Belzile, Suzanne Morin, Louis Bessette, Sylvie Dodin et Jacques P. Brown. Le chapitre comporte l'intégral de l'article en anglais.
59
3.1 Résumé OBJECTIF : Comme dans de nombreux pays, aucune donnée de surveillance
populationnelle associée aux fractures de fragilité n'est disponible au Québec; même s'il est
bien connu que cette affection constitue un problème de santé publique important et
croissant. Dans cette étude, les taux d'incidence des fractures non-vertébrales associées à
l'ostéoporose chez les femmes de 50 ans et plus ont été estimés. L'impact de ces fractures
sur la survie des patientes et les années potentielles de vie perdues a été évalué.
MÉTHODES: À l'aide d'un algorithme validé pour le fichier des services rémunérés à
l'acte, nous avons identifié les femmes de 50 ans et plus ayant subi une fracture non-
vertébrale incidente entre le 1 janvier 2004 et le 31 décembre 2005 dans trois régions de
santé de la province de Québec. Le statut vital de ces cas de fracture a également été
déterminé jusqu'au 31 décembre 2007. Les taux d'incidence brut et standardisés pour l'âge
ont été calculés pour chaque site de fracture. Pour évaluer l'impact des différents sites de
fracture sur la mortalité des patientes, la survie relative à 12, 24, 36 et 48 mois suivant la
fracture et les années potentielles de vie perdue ont été estimées.
RÉSULTATS : Durant la période de l'étude, un total de 17 471 fractures ont été
identifiées. Les fractures les plus fréquentes sont celles traditionnellement associées à
l'ostéoporose; celles de la hanche/fémur, du poignet et de l'humérus. Les fractures des bras
et des jambes surviennent plus tôt que les fractures de la hanche/fémur et du bassin. Les
taux d'incidence des fractures du bras augmentent linéairement avec l'âge tandis que les
taux d'incidence des fractures de la jambe demeurent constants selon l'âge. Les fractures de
la hanche/fémur et du bassin sont rares avant l'âge de 70 ans mais augmentent
substantiellement par la suite. Une diminution significative de la survie relative a été
observée chez les femmes présentant une fracture de la hanche/fémur, du bassin, de
l'humérus, de l'avant-bras et du tibia/péroné. Cependant, l'excès de mortalité observé pour
les fractures de l'avant-bras et du tibia/péroné est seulement significatif chez les femmes
ayant plus de 80 ans. Les fractures de la hanche/fémur et du bassin sont associées à la plus
grande perte d'années de vie, étant plus importante durant la première année après la
fracture mais continuent à avoir un impact significatif sur la survie des patientes sur une
période d'au moins 4 ans.
60
CONCLUSION : Les fractures de la hanche et les autres fractures sont fréquentes et sont
associées significativement à une diminution de la survie. Ces fractures on un impact
important sur les individus et sur le système de santé. Par conséquent, dans l'estimation du
fardeau associé aux fractures de fragilisation, ces autres fractures, comme les fractures de
l'humérus et du bassin, doivent être considérées.
61
3.2 Abstract BACKGROUND: As in many countries, no population-based data on fragility fracture
(FF) surveillance in an aging population are available in Quebec, Canada; although they are
well-known to be an important and growing public health issue. In this study, we estimated
the incidence rates of non-vertebral, osteoporosis-related fractures occurring in women
aged 50 years or older. The impact of these fractures on survival and potential years of life
(YLL) was also evaluated.
METHODS: A validated algorithm for physicians' claims databases identified women
aged 50 years or older with an incident non-vertebral fracture between January 1, 2004 and
December 31, 2005, in 3 health regions ofthe province of Quebec. The survival status of
these fracture cases was ascertained until December 31, 2007. Crude and age-standardized
fracture rates were calculated for each fracture site. To evaluate the impact of different
fracture sites on mortality, we estimate relative survival at 12, 24, 36 and 48 months post-
fracture and the potential YLL.
RESULTS: During the study period, a total of 17,471 fractures were identified. The most
frequent fractures were those traditionally associated with osteoporosis - those at the
hip/femur, wrist and humerus. Arm and lower leg fractures occurred earlier than hip/femur
and pelvis fractures. The incidence rates of arm fracture increased linearly with age while
those of lower legs fractures were generally constant over the ages groups studied.
Hip/femur and pelvis fractures were rare before 70 years of age, but increased substantially
thereafter. A significant decrease in relative survival was observed in women who sustained
hip/femur, pelvis, humerus, forearm or tibia/fibula fractures. However, mortality with
forearm and tibia/fibula fractures was only significant in women experiencing fracture at or
after 80 years of age. Hip/femur and pelvis fractures were linked with the greatest YLL,
being most striking in the initial year after fracture, but continuing to have a significant
impact on survival for at least 4 years.
CONCLUSION: Hip and non-hip fractures are common and associated with significant
decreased survival. These fractures have a significant influence on individuals and the
62
healthcare system. Therefore, non-hip fractures, such as humerus and pelvis fractures, must
be included when assessing FF burden.
63
3.3 Introduction Osteoporosis-related fractures, or fragility fractures (FF) represent a major public health
problem that is affecting an increasing number of individuals worldwide every year. These
fractures are also associated with substantially-reduced quality of life [147], excess
morbidity [132] and loss of independence [36, 130]. Their treatment accounts for
considerable clinical resource utilization with a growing financial burden on healthcare
budgets [73]. Moreover, FF lead to shorter lifespan than if they had not occurred [131,
148], even after adjusting for concomitant morbidities [76, 149].
Administrative healthcare databases can be analyzed for epidemiological studies to assess a
number of outcomes, including the incidence rates of medical conditions in the general
population and relationships between diseases, risk factors and outcomes [150-152]. These
databases readily provide population-based information that is free from many ofthe biases
inherent in survey studies and may enable the development of chronic disease surveillance
systems.
Since the majority of fractures require clinical care, characteristics related to their treatment
are commonly recorded in administrative healthcare databases, with other health outcomes
and some demographics information. These data can serve to ascertain the incidence of
fractures within a given geographical area and to investigate relationships with bone
metabolism regulators or excess mortality.
Aging ofthe population, in itself, contributes to a rising number of fractures. Therefore, the
burden of fractures on the healthcare system is increasing significantly. By advising policy
makers about the incidence rates of fractures by demographic subgroups and skeletal sites,
they may better understand their real burden and implement appropriate prevention
programs and services.
The 2 main objectives of the present study were to assess the incidence rates of non-
vertebral, osteoporosis-related fractures occurring in women 50 years of age or older for the
years 2004-2005 and to evaluate their impact on survival and potential years of life lost
64
(YLL). Moreover, the influence of surgical delay on survival was examined for hip
fractures requiring surgery.
3.4 Methods 3.4.1 Data Sources
All Canadians are covered by a universal healthcare administered by their province or
territory of residence. In the province of Quebec, it is administered by the Régie de
l'assurance-maladie du Québec (RAMQ). The RAMQ maintains a computerized
administrative physician fee-for-service claims database containing information related to
physician reimbursement. It includes: each physician's unique identification number, each
patient's unique provincial health insurance number (NAM), clinical service billing codes,
locations where the clinical services were provided and dates, and, optionally, a diagnoses
made as per the 9th revision of the International Classification of Diseases: Clinical
Modification Codes (ICD-9-CM) included in 91% of all RAMQ claims. This database has
been verified previously for accuracy and completeness [120, 125]. In 2004 and 2005,
RAMQ databases collected and stored medical-claims information from approximately
94% of Quebec-based physicians and on almost 98% of 7.5 million residents in the
province of Quebec [121].
In this retrospective cohort study, the RAMQ claims database was accessed to identify
fracture cases requiring clinical care between January 1, 2004 and December 31, 2005,
among women aged 50 years or older. Our study comprised 3 of Quebec's most populated
health regions (Montreal, Quebec City and Mauricie), for a total of 563,656 women aged
50 years or older, representing 42% of the women of that age living in Quebec province
[153]. Mortality data were obtained from the RAMQ databases to establish vital status up
to December 31, 2007, for each woman identified with incident fracture, thereby providing
between 2 to 4 years of follow-up for each fracture case. Cause of death was not available
to us.
This project was approved by the Research Ethics Board of Centre hospitalier universitaire
de Québec of Laval University.
65
3.4.2 Identification of fracture cases
An algorithm developed for the physician fee-for-service claims database (RAMQ) [129],
identified all incident non-vertebral fracture cases during the period of interest. Based on a
panel of clinical experts, the algorithm was designed to first select all medical services
claims potentially associated with fracture treatment: (a) claims with medical services
billing codes definitively related to fracture care (i.e., open and closed reduction), or (b)
claims with medical services billing codes not limited to fracture care (i.e., immobilization,
consultation, principal or follow-up visit with an orthopedic surgeon (OS), emergency
physician (EP), or general practitioner (GP)) if combined with ICD-9-CM diagnosis codes
of fracture. Via these extracted claims, the algorithm considered an incident fracture had
occurred if there was at least one claim associated with (a) fracture treatment (open
reduction, closed reduction, immobilization), (b) principal visit with an OS with at least one
other claim, or (c) consultation with an OS with at least one other claim. The claim
identifying the fracture was referred to as the « index claim ». This algorithm has been
validated previously [129].
Fractures were grouped according to fracture site, indicated by the specific medical service
code of the index claim or, if not specific to fracture treatment, to the ICD-9-CM code. To
establish the complete temporal sequence of medical care for each fracture, the algorithm
identified any other claim (emergency room visit, follow-up visit, etc.) related to the same
anatomical site as the fracture. The date of fracture corresponded to the date of the first
claim in the temporal sequence of medical care. Finally, a 6-month period was established
for « washout period » between two clinical sequences related to the same anatomical
fracture to minimize potential misclassification of fracture follow-up as a new incident
fracture.
In this study, the following fractures were investigated: hip, femur, pelvis, shoulder,
humerus, forearm, elbow, wrist, tibia, fibula, foot and ankle. Vertebra, sacrum and coccyx
fracture were not included in these analyses, since unacceptably low Sn was associated with
the algorithm for the identification of fractures at these sites [129], and vertebral fracture
are under reported in administrative databases [139]. Also, craniofacial, hand, finger, knee
and toe fractures were excluded since they are not linked with osteoporosis [31]. In
66
administrative healthcare databases, no information is available on circumstances
surrounding incident fracture events. Since FF represent the vast majority of fractures in
women aged 50 years or older (approximately 81% of this population [4]) both low- and
high-energy trauma fractures were included in the analyses. Furthermore, both low- and
high-energy trauma fractures have recently been proposed for inclusion as outcomes in
osteoporosis studies as they are similarly associated with decreased bone mineral density
(BMD) and result in increased fracture risk [33]. Pathological fractures were not excluded
since they represent a small proportion and their exclusion may lead to underestimation of
the burden related to osteoporotic fractures [33, 34].
3.4.3 Statistical analysis
Crude and age-specific (5-year interval) fracture incidence rates per 100,000 person-years
are reported by fracture site or site grouping, with their respective 95% confidence intervals
(95% CI). For each fracture site or grouping, fracture incidence was calculated by dividing
the number of fractures identified by the validated algorithm by the total population of
women >50 years of age in the 3 health regions studied. Age-standardized fracture rates
were directly adjusted to the 1991 age-structure ofthe Canadian population [154].
Only women 50 to 99 years old were retained for analysis ofthe impact of non-vertebral FF
on mortality. If more than 1 fracture was identified for the same woman and at the same site
during 2004-2005, only the first fracture was considered. However, since this analysis was
performed for each fracture site separately, if a woman had more than one fracture in 2004-
2005 at different sites, she would contribute to each fracture site grouping. Among women
who were identified to have experienced fractures in 2004-2005 and who died in the
follow-up period, time to death was calculated from the fracture date to the date of death.
Among fracture cases that survived the follow-up period, time to death started on the
fracture date and was censored on December 31, 2007. The cumulative proportion of all-
cause mortality at 12 and 48 months from the fracture date was calculated by life tables. To
assess the impact of each fracture site on survival, relative survival was investigated at 12,
24, 36 and 48 months post-fracture for the entire cohort and by 10-year age groups.
67
Relative survival was calculated as the ratio of observed survival after fracture and
expected survival in the general population for people of the same age group and sex,
according to the Ederer II method. One minus relative survival provides an estimate of
mortality in the studied cohort that is in excess of what is experienced by the general
population ofthe same age group and sex. A relative survival of unity (100%) indicated
that survival after fracture was similar to that in the general population. Relative survival
that does not include unity in the 95% CI means that survival in the studied cohort of
fracture cases is significantly different from survival in the general population.
Expected survival data on the general population were obtained from the Canadian Human
Mortality Database (CHMD) [155], developed to provide detailed and validated Canadian
information on population mortality. Life tables for the province of Quebec were generated
from the CHMD for the years 2004 through 2007, providing expected survival.
The impact of non-vertebral FF on patient life expectancy was calculated for each fracture
case. Potential YLL were computed for each fracture case by subtracting survival time
since fracture from life expectancy at the time of fracture based on life tables for women
from the province of Quebec. Total YLL and average YLL correspond to the sum and mean
of YLL for each fracture case, respectively. The YLL proportion for each fracture case was
calculated and corresponded to the difference between life expectancy and survival, divided
by life expectancy.
To assess the impact of surgical delay on the survival of women with hip/femur fractures,
Cox's proportional hazards modelling was performed with surgical delay considered as
time-dependent variable. Surgical delay was calculated as the number of days between the
fracture date and the date of first open reduction in the RAMQ claims database. To
ascertain the validity of this definition, it was compared to the surgical delay observed in
the hospital discharge database (Med-Echo database; time between the date of admission
and the date of surgery) when surgery was cited in both databases (N=3,351). In 81% of
cases, the 2 measures of surgical delay were identical and corresponded to a Kappa statistic
of agreement of 0.64, indicating satisfactory agreement. Moreover, in more than 90% of
cases, the 2 measures of surgical delay were in a window of 1 day apart, suggesting that
this definition of surgical delay is valid.
68
All statistical analyses were conducted with SAS version 9.3 (SAS Institute, Inc., Cary,
NC, USA).
3.5 Results 3.5.1 Fracture incidence rates
During the 2-year observation period, the algorithm identified a total of 18,927 fractures in
17,661 women in the 3 health regions studied. After eliminating vertebra, coccyx, sacrum
or knee fractures as well as fractures occurring in women less than 50 years of age, 16,376
women had a total of 17,471 eligible fractures.
The total number of fractures, the median (Q1-Q3) age at fracture, and crude and age-
standardized fracture rates (per 100,000 person-years) are reported in Table 3.1 for all
fractures combined and for each fracture site grouping. When all fracture groups were
combined, median age (Q1-Q3) at fracture was 73 (61-82) years. Median age at hip/femur
and pelvis fracture was approximately 10 years older than median age at all other peripheral
fractures. In this cohort, hips/femurs represented 29.6% of all fractures, and non-hip
fractures, 70.4%. The most common fractures identified were those of the hip/femur
(29.6%; crude rate=461.6 fractures/100,000 person-years), wrist (20%; crude rate=312.0
fractures/100,000 person-years), shoulder/humerus (17.1%; crude rate=267.0
fractures/100,000 person-years) and ankle (11.9%; crude rate=186.1 fractures/100,000
person-years). These 4 most frequent fracture sites represented 79% of all fractures. Despite
accounting for only 15% of the female population over 50 years of age, one-third of
fractures occurred in women 80 years of age or older.
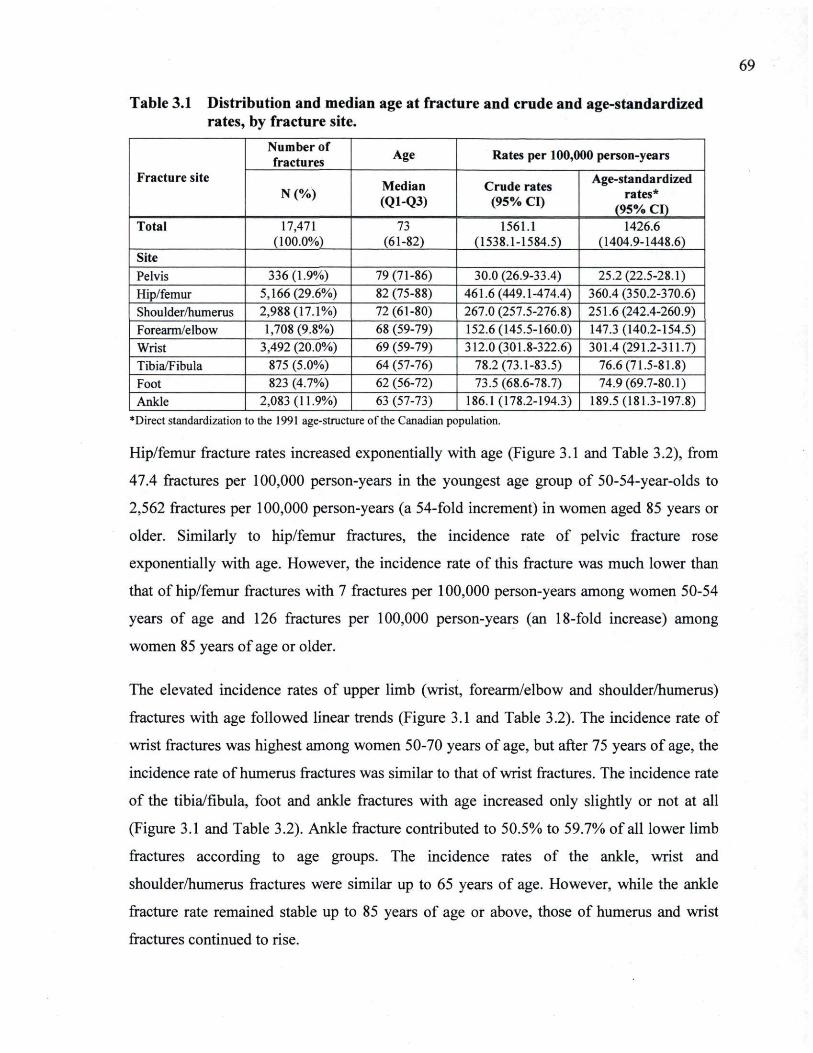
69
Table 3.1 Distribution and median age at fracture and crude and age-standardized rates, by fracture site.
Fracture site
Number of fractures Age Rates per 100,000 person-years
Fracture site N (%) Median
(Q1-Q3) Crude rates
(95% CI)
Age-standardized rates*
(95% CI) Total 17,471
(100.0%) 73
(61-82) 1561.1
(1538.1-1584.5) 1426.6
(1404.9-1448.6) Site Pelvis 336(1.9%) 79(71-86) 30.0(26.9-33.4) 25.2(22.5-28.1) Hip/femur 5,166(29.6%) 82 (75-88) 461.6(449.1-474.4) 360.4 (350.2-370.6) Shoulder/humerus 2,988(17.1%) 72 (61-80) 267.0 (257.5-276.8) 251.6(242.4-260.9) Forearm/elbow 1,708(9.8%) 68 (59-79) 152.6(145.5-160.0) 147.3(140.2-154.5) Wrist 3,492 (20.0%) 69 (59-79) 312.0(301.8-322.6) 301.4(291.2-311.7) Tibia/Fibula 875 (5.0%) 64 (57-76) 78.2(73.1-83.5) 76.6(71.5-81.8) Foot 823 (4.7%) 62 (56-72) 73.5 (68.6-78.7) 74.9(69.7-80.1) Ankle 2,083(11.9%) 63 (57-73) 186.1(178.2-194.3) 189.5(181.3-197.8)
♦Direct standardization to the 1991 age-structure ofthe C-anadi-an population.
Hip/femur fracture rates increased exponentially with age (Figure 3.1 and Table 3.2), from
47.4 fractures per 100,000 person-years in the youngest age group of 50-54-year-olds to
2,562 fractures per 100,000 person-years (a 54-fold increment) in women aged 85 years or
older. Similarly to hip/femur fractures, the incidence rate of pelvic fracture rose
exponentially with age. However, the incidence rate of this fracture was much lower than
that of hip/femur fractures with 7 fractures per 100,000 person-years among women 50-54
years of age and 126 fractures per 100,000 person-years (an 18-fold increase) among
women 85 years of age or older.
The elevated incidence rates of upper limb (wrist, forearm/elbow and shoulder/humerus)
fractures with age followed linear trends (Figure 3.1 and Table 3.2). The incidence rate of
wrist fractures was highest among women 50-70 years of age, but after 75 years of age, the
incidence rate of humerus fractures was similar to that of wrist fractures. The incidence rate
of the tibia/fibula, foot and ankle fractures with age increased only slightly or not at all
(Figure 3.1 and Table 3.2). Ankle fracture contributed to 50.5% to 59.7% of all lower limb
fractures according to age groups. The incidence rates of the ankle, wrist and
shoulder/humerus fractures were similar up to 65 years of age. However, while the ankle
fracture rate remained stable up to 85 years of age or above, those of humerus and wrist
fractures continued to rise.
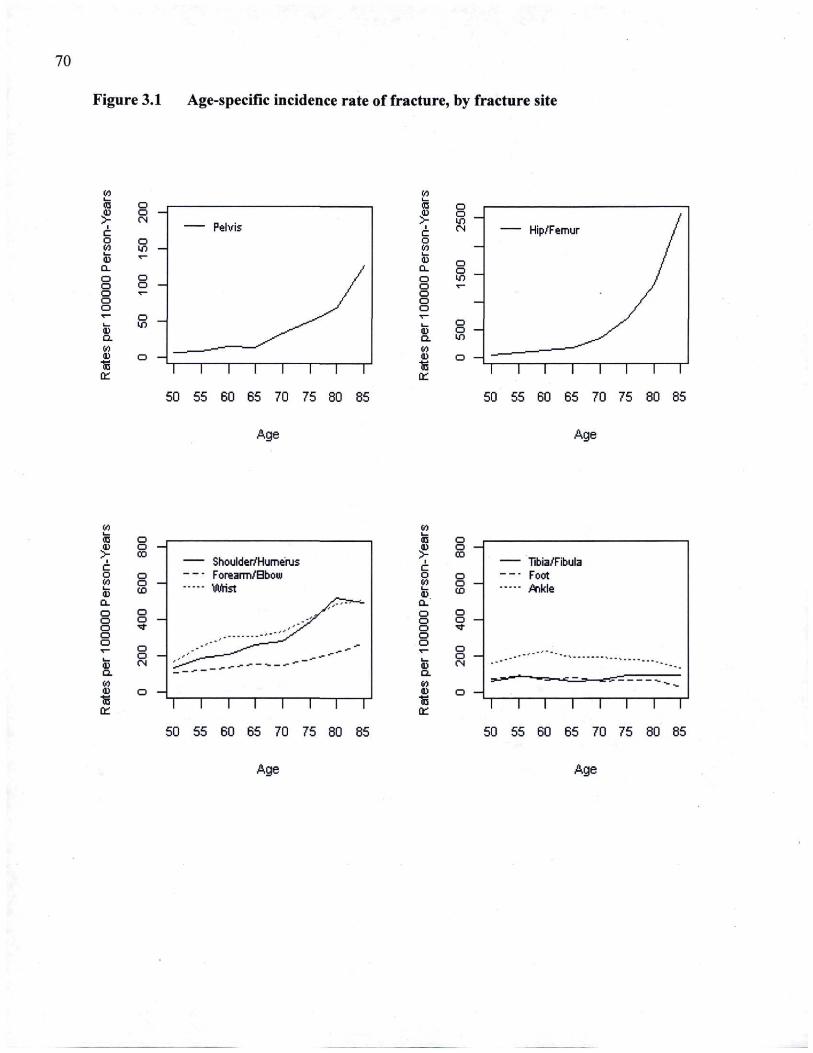
70
Figure 3.1 Age-specific incidence rate of fracture, by fracture site
IA i— OD I i
C o CO I— d Q. o o o o o a. CL IA ■D 1£ ù_ i—i—i—i—i—r
50 55 60 65 70 75 80 85
Age
I c o VS L_
CL o o o o o
ID Q. IA a. tt_ ~i i i i i i i r
50 55 60 65 70 75 80 85
Age
«_ a <i> Q > oo c o <) IA o a. UD
CL
o o o o o "Çf o o
1J o
<K CN O. IA a. o 15 Q_
Shoulder/Humerus Forearm/Bbow WHst
i i i i i i — i — T
50 55 60 65 70 75 80 85
CD o a> o > oo c o CT IA O ID OD
CL
O O o O o ^ f o o O !_. LJ
D. IA 1) O ■s Ct_
Tibia/Fibula Fort jfinkle
— i — i — i — i — i — i — r 50 55 60 65 70 75 80 85
Age Age
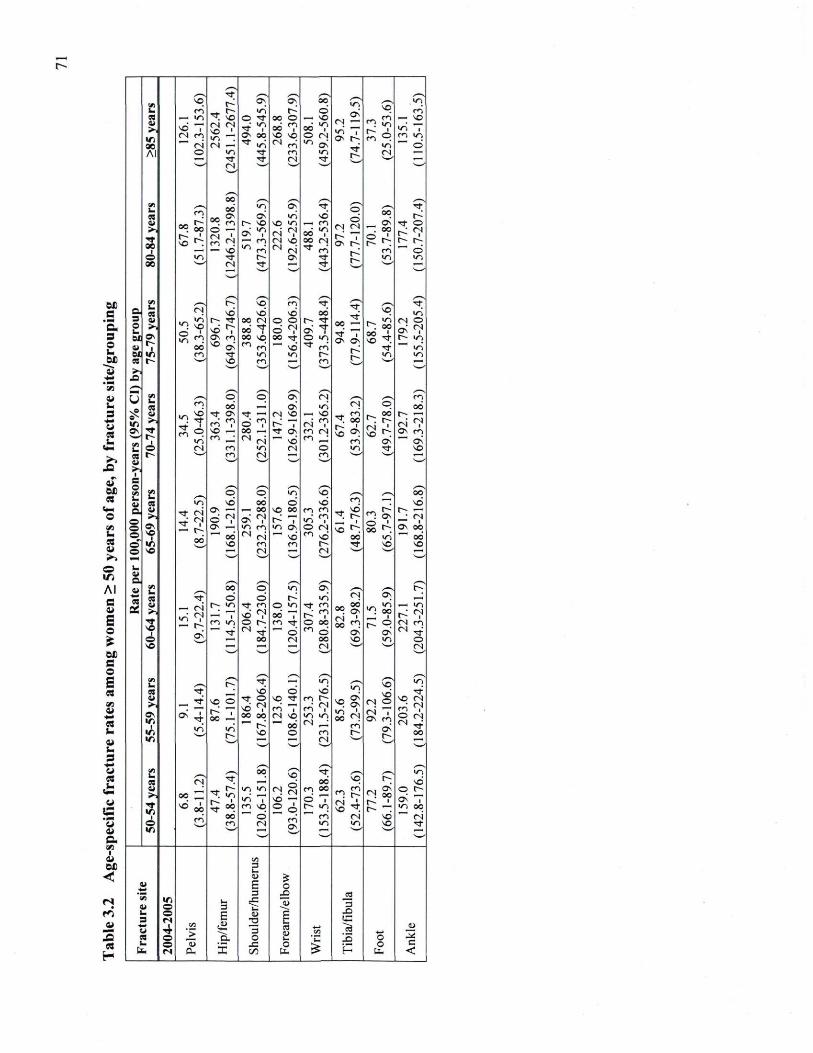
s • — c . 43 o u Sa
"as CJ
s +m a
o
«
o I D A l S a £ o UD C o
s a VJ i i
+m a u i i u s "S
s C VJ I
O M
rn
, . r f ^^
V i vq l ~ O v S? oo vn
vq wn
■ r n r r ^ wn H d O s
O l —
v j T Ov t~.
r f
vq en
es _~ v j r r ^ O r f 00 o — VO O s O l —
v j T Ov t~.
r f
^ . « r i
wn
—. VO
V i 00
vd i r n o i
O l O J vo » VJ . OJ —
r f i O v 0 0
od «J VO VO ™ en
^ v j 0 O i O OJ "> o ;
O s O l —
v j T Ov t~.
r f
^ . « r i
wn
wn "T m wn —' d
A l O «n r f m "O
O s O l —
v j T Ov t~.
r f Ci 4 —
— r r "tf OJ r f
O s O l —
v j T Ov t~.
r f
— O)
oo
a i oo
vo
r n 00 VJ Ov
•r vo v j
v o v j
r ? vd
— m d Ov| O l
r^ T ov r^
r »
0 0
_ G s
r ?
r f O 4 > 1
r f oe
i
oo
vo
00 1
o — Sri — VO
as "♦? — m
oi «2 O l V O N o i
od • ? 0O (N
d Ov| O l
r^ T ov r^
r »
. oo
""' d o v , r f t~ Ov r f
d Ov| O l
r^ T ov r^
r » VJ wn oe ' — 4 4
OJ r f ^ T — ■ ( r f^
d Ov| O l
r^ T ov r^
r » v > ^ — v ^
w
_ /—S ? m \
c V i
•— CB
es F; vd
vq vd
CJ vd
r f
O O r? r f
OO —
r f "T O v O v
r
V O r t wn
3 Ci un O VJ
un t r f oo o i o o t ^ r f
r? r f
OO —
r f "T O v O v
r
r f
(N o O L. 5,
4 > 1
1
un O VJ
vo 1
en oo'
vd ^ ov m * > O s
odr oo vo d 2
0 O q
"~ vd
O VJ ^ m'
r? r f
OO —
r f "T O v O v
r
r f
Ov ^ r wn " "
, wn ©£ V l en r f wn VJ F*
r? r f
OO —
r f "T O v O v
r i ^ l wn
eej t s ' V O m ( H en
r? r f
OO —
r f "T O v O v
r v ^ >—
>> " ^ >44jJ V>J " ^ 4 * * v ^ >>
^ ^^ ^^ U t/3
m O OO
O " Ov" Ov
OJ v j OJ O^
r n oo
iÇ O VJ r t f )
vd r f Ov r f — O l V O « VO
en vo n
OV
t~ •— V J O s
V i r
i
VJ r t f )
r r 1
p v j
~ ï en m i V O — en _ •
oo — M o i
r f O v 1 1 vd
^ ; en O J i m O J m __; en
vo n OV
o i «^ Ov r n
— OV
V J O s
V i o OJ m VJ O l o VJ r f vo
ca t ~ '—' en O l • f i v j ^ i
C i v ^ *
^ s o ^^ ^ N c« V I o p 1/*J vq ,— oo ■
C i 4 . f N
VI vd 00 d vd r n — vd a .
o o o
1 O v V O
1
r r o i OJ
1
rod
O v —
d <7 O v —
" " OO
— o o
O v ' ^ v j e n
vo oo r~ "T V J o v ■"" vd
«H <? o Ol < > vd
• f ?
oo un
r — —i
N
Ov oo ~" oo
o u .
o i OJ
1
rod
V O m f l r^ r f VO VO o v O ■ ~ —
Ci — OJ V — i • ^ s f—H
v ^ ' V
1—J
_. u c s * , /—V a
es Di
V i ■
es r ? oo d
p " d
"1 O v OJ OV K a
es Di 4>V
r f v O
1
un (N OJ
i o
f V J
— 1 C. VJ ~~ r f
r f en V O ^
O t
M r f
O VJ 00 "T C . r f
""" d
r f f < .
r «? o oo "> d
^ , 0O °°. Ov OJ ' oo n
Ov
_ _ l
t P OV
— wn
< ^ ^ o i m " r f
o
(N OJ
i o
■F"« oo OJ 00 VO wn O VO w
"~" ci es V I
^ P r? —; un </n vê* wn
cs r r vd o vd </n vd
O) o o i T Ov m
Ov r
rf" >,
«r, ■
i n
ov
r r ■
r f v j
VO O r^ "T 00 —
wn •T
r f O
vd <7 ■OO 4J0
VO
vq r f en T o i vq " " 00
o
m r ^ O J e n i V J V J
O J _ ; cn OJ
en t—
vd O) o o i T Ov m
Ov r
VO OJ m' «? O O l N r f
O O w 1
—' ^^ _^ _
cs s — v
OJ r f " 00 ^ 4 ^ 4 .
vo
^ ^ VO —
2 P OV
00 vq / 4 4 ^
r wn vd
■>>
TT IT,
i
00 vd 1
00 m'
~ wn r? »
00
wn >n
«i T en vo " " d
^ 4 ^ 4 .
vo
^ ^ VO —
2 P OV
m oo d T ■r «n 1 1 en
n rvN 4 V O ~
OvJ VO
o ( ^ ov" T wn oo " " o^
O
1
00 m'
en O l
^ 4 ^ 4 .
vo
^ ^ VO —
2 P OV VJ VJ VO r f
V i ^ s • ^ 1
^ 4 ^ 4 .
vo
^ ^ VO —
2 P OV
^™ v._^
^^ v—'
Wl 3 U U ^
a» E O ••_■ 3 £ ee) 09 IU
V l o 3 | "53 3
3 o «s E S
T3 g 3
U 1
o
r .
> «S " o .
3 O
es QQ
o c
< u o o t
u a . X t a
O % H o
u . c
<
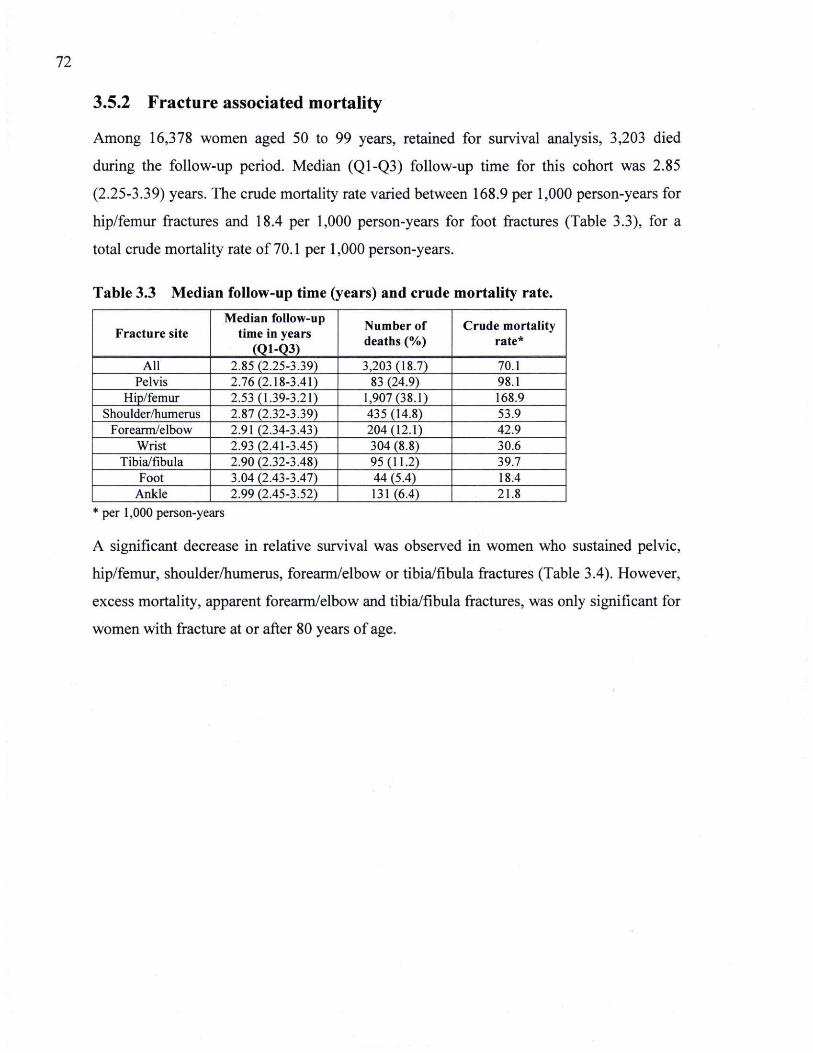
72
3.5.2 Fracture associated mortality
Among 16,378 women aged 50 to 99 years, retained for survival analysis, 3,203 died
during the follow-up period. Median (Q1-Q3) follow-up time for this cohort was 2.85
(2.25-3.39) years. The crude mortality rate varied between 168.9 per 1,000 person-years for
hip/femur fractures and 18.4 per 1,000 person-years for foot fractures (Table 3.3), for a
total crude mortality rate of 70.1 per 1,000 person-years.
Table 3.3 Median follow-up time (years) and crude mortality rate.
Fracture site Median follow-up
time in years (Q1-Q3)
Number of deaths (%)
Crude mortality rate*
All 2.85 (2.25-3.39) 3,203(18.7) 70.1 Pelvis 2.76(2.18-3.41) 83 (24.9) 98.1
Hip/femur 2.53(1.39-3.21) 1,907(38.1) 168.9 Shoulder/humerus 2.87(2.32-3.39) 435 (14.8) 53.9
Forearm/elbow 2.91 (2.34-3.43) 204(12.1) 42.9 Wrist 2.93 (2.41-3.45) 304 (8.8) 30.6
Tibia/fibula 2.90(2.32-3.48) 95(11.2) 39.7 Foot 3.04(2.43-3.47) 44 (5.4) 18.4
Ankle 2.99(2.45-3.52) 131(6.4) 21.8 * per 1,000 person-years
A significant decrease in relative survival was observed in women who sustained pelvic,
hip/femur, shoulder/humerus, forearm/elbow or tibia/fibula fractures (Table 3.4). However,
excess mortality, apparent forearm/elbow and tibia/fibula fractures, was only significant for
women with fracture at or after 80 years of age.
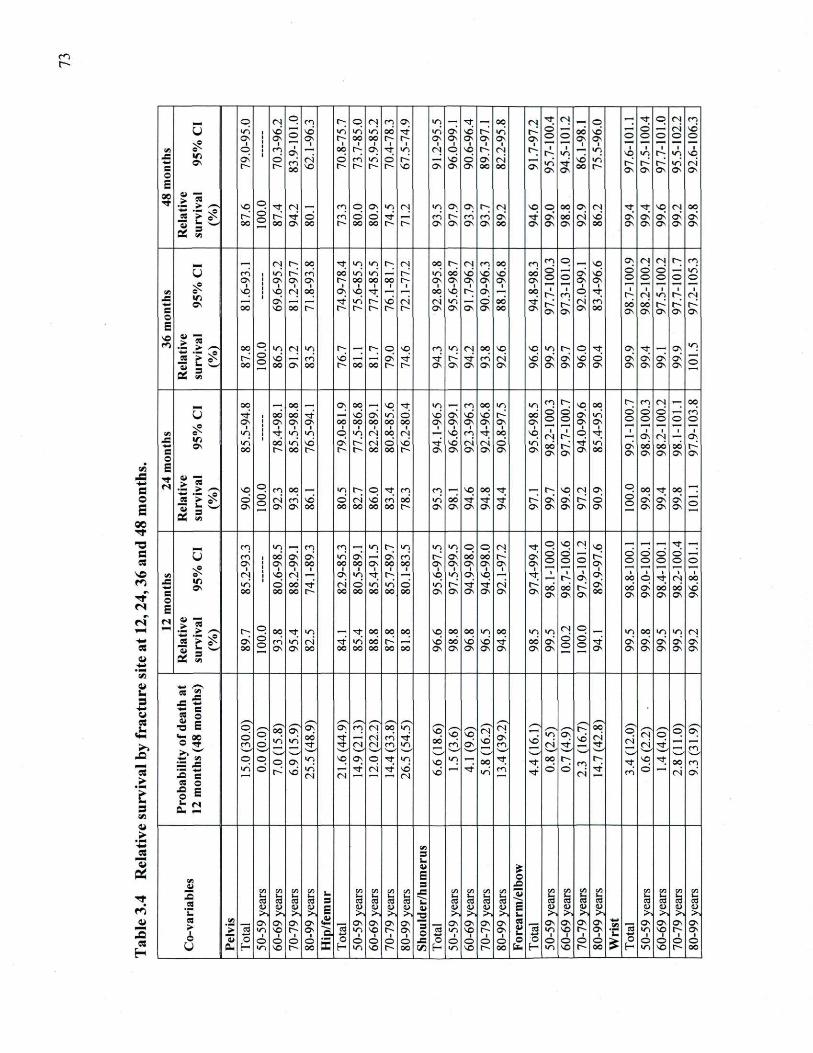
on r
e o
oe ■rt ■o fi es
v * r*.
rs rs
re a "S _s w o «
C
"re fe
s VJ i i > ._ t
_re "3 a: r t r.
re
p Oj p en I"; p O l r n Ov un r f _ oo O J r f Oj _
o — r f p O l m
o wn vd s vd v j un un 0 0 r f un CT^ vd r un ■r^ d o o 0 0 vd o
d o o o i
o vd o
OV
CJv O v s O v r 0 0 0 0 O r^ O v O v O v O N C v O v
d o o
O v O v o d o o o i
o vd o
VI . e C o E
oc r f
OV p m 1
Ov — 0 0 O ; O v r f un Oj p V O O Oj O ; 1 O;
1
un — un vq un i
o 1
un 1
VO VI . e C o E
oc r f
OV d r
d o en
00 •oi VO
d r~ r n
run r
d r VO O v
vd O v d
O v
Ov 00
oi 00
O v un" ON
r f O v
vd 00
un o
C v O v O v un O v
o i C v
VI . e C o E
oc r f
** "fi VO p r f OJ en O O v wn Oj un O v Ov 1 ^ (N V O O OO
°! O l r f r f V O O J 0 0 es > 0 ^ d
o •f~ r f d r n d d r f •1—î m' t4^ en r n Ov' r f Ov' oo o i vd d d d d d * a oo
d o oo O v oo r~ 0 0 0 0 r t ~ O v O v O v O v oo O v O v O v O v 0 0 C v o O v C v O v
— VJ
__ O l O ; 0 0 r f VJ un O ; Oj OO r O l en 0 0 en en p _
VO OV OJ O l O; en
i « Ov
en O v
un Ov
r n OV
00 o
v j 00
un oo 0 0 ■r
un ON
0 0 O v
i
vd O v
vd as
vd os
oo d o
o d O v
i
vd O v
d o
d o d
o O un O
en
C O
E VO r n
i « Ov
vq vq OJ. 0 0 O v vq r f —; — 0 0 vq O ; O v — OO •r~ 1
en o r f i o O)
i 1 1
r s en
C O
E VO r n
i « Ov 0 0
Ov' V O 0 0 r
r f un r r
vd ■r oi o i
O v un Ov S d
O v
oo 00
r f O v O v C v
o i O v
m' 0 0
0 0 C v
oo O v O v OV O v
en
C O
E VO r n
4 * " f i
•Si es >
g 0 0 o d o
un vd
O J un r n vd
. O ; o d
V O
r f
en r f
un O J
r f
oo r n
vq o i
V O
vd un d
o
d o vd
r f
d C v
d r f d d
O v
d un
O
— m oo
o d o
oo O v oo r oo OO f r~ OV OV O v O v O v O v O v O v O v O v O v O v O v av
un
O
— m
oo 0 0 Ov oo vq r f un _ en oo un un en o vo 0 0 r m O J — oo
U s? u .
r f 0 0 O v
oo' O N
r f O v 00
1
vd 00
OV 0 0
un 00
d 00
V D O v
O v O v
i
vd O v
vd O v O v
0 0 O v
d o d
o d O v
un O v
i
d o
d o d
o o
en O
V i
U s? u .
un r f un un o VJ Oj 0 0 OJ — VO m r f OO vq OJ r o r f ■ ■
Ov OJ ■ i
av V i
U s? u . un 0 0 un vd d r^ oi d vd r f " vd o i o i d un oo
O v Ov r f un d
O v
oc av
oo O v
oo O v O v c
o E
r f Ol
U s? u .
oo r oo 0 e~ f 0 0 0 0 0 O v O v O v O v O v O v oo O v Ov O v oo d
O v
oc av
oo O v
oo O v O v c
o E
r f Ol •fil g vq p m oo un O ; p r f m en V O 0 0 r f o VO ( N ov o
0 0 r f 0 0 „
es > g d d o ( N r n vd d oi vd r n oo un 0 0 r f r f r f o^ d d K d d
o d d d O 13 £ fi! w
ON d o O v O v 0 0 0 0 oo 0 0 oo r O v O v O v O v O v O v Ov O v Ov O v
d o O v O v ov O
13 £ fi! w
en un _ en en _
wn r^ un wn un O O O l r f o V O Oj vq — —• — r f —. U S? V l Ov
m' oo O v
Ov' O v
d oo
un oo
d 00 Ov
Ov' 0 0
en oo O s
a^ as
0 0 O v
OO O v Ov
O v O v
d o d
o O O s
d o
d o
d o
d o o
V I J= ** C o E
OJ
U S? V l Ov
OJ VO O J —; O v un r f t ~ — vq V J O v V O — r f i ■ 1 O v o\ ■
« 3 i
o ■
r f ■
es 1
00 V I J= ** C o E
OJ
U S? V l Ov un
00 d 00
0 0 0 0
r f •T
oi oo
d 00
un 00
un 00
d 00
un O v
t : O v
r f OV
r f O v
o i O v O v oo
O v 0 0 O v O v
d oo 0 0
C v d O v O v
0 0 O v
vd av.
V I J= ** C o E
OJ
•Il g •T; p 0 0 r f " . r f 0 0 0 0 0 0 V O 0 0 OO un OO un un Oj p un 0 0 un un Oj es > g O v d
o en un oi r f un 0 0 C~ _î vd 0 0 vd vd r f oo d d
o d o r f d d d d d
3 a — VJ
oo d o
OV O v 0 0 0 0 oo oo 0 0 oo O v O v Ov. O v Ov O v Ov d o
d o O v C v av O v O v O v
3 a — VJ
•** O CS j 2 _s — t i s
■o S
o %r
t i s
■o S
o %r
, v t , f / — s , V __ t i s
■o S
o %r
o d m
p" o
00 v j
' V
Ov un
OV oo' r f
a ? r f r f ,
en (N •oi Ci
00 m' m
un r f un 0 0
vq r n d
oT vd
(N O^ m vd
un
Ci Ov
vd 0 0
o i r £
p" oi OJ
Ci o r t
p m
.>> w v»—^ . _,. d ^ v — ' v ' N — '
^^ *—' ^ s V ■* .^,. !~^ m
— VJ — JS '■5 B
p o o O v un vq O v p r f un vq un — OO r f r f oo o m r r f VO r f 0 0 en — VJ
— JS '■5 B
un d o^ vd un O l OJ
r f o i r f vd OJ
vd F^ r f un r n r f d d o i r f m' d 1
—' oi d « o o
B
b —
VJ B L . C i •S E o
VJ C i 3 J 2
_. C/3 _. en ■— VJ V i V i
_. f V i en V I V i en _. _. V i en VJ V i VJ
3 .2
L L M L . ■—
;u •L ra ;_ f
■•_ L . L U, U L . S fe L_ •L u . u i— 3
.2 ra ra ra ra 3 ra ra ra ra U ra ra C3 ra E ra S fe ra ra ra ra es 3
.2 ID u OJ a E C i Ci a <u CJ <u o; <U (D E a D <u a D C i a IU 'C >> >> >. >> E
>. >. >> >, 2 p ^ >> > v > v u >. >. >. >> 5n >» >. ^ es 4 >
1 — __, O v O v O v O v
E _ O v O v Ov O v 3
o O v O v O v Ov. es __ O v O v O v O v __. O v O v O v Ov es
4 > 1 ]> C3 wn V O o O v
" Q . ra un VO •t Ov 3 o ra un V O O O v L. ra
44»
un i VO
i i O v
i 'C ra un V O i o
1
O v 1
o u O o o o o £ o O O © O JE o O O o d O O O O O O £ o d O o o
U 0 . H v , VO o oo £ H un VO r^ 0 0 (^ H un V O r oo _. H un VO r 0 0 £ f— wn VO o oo
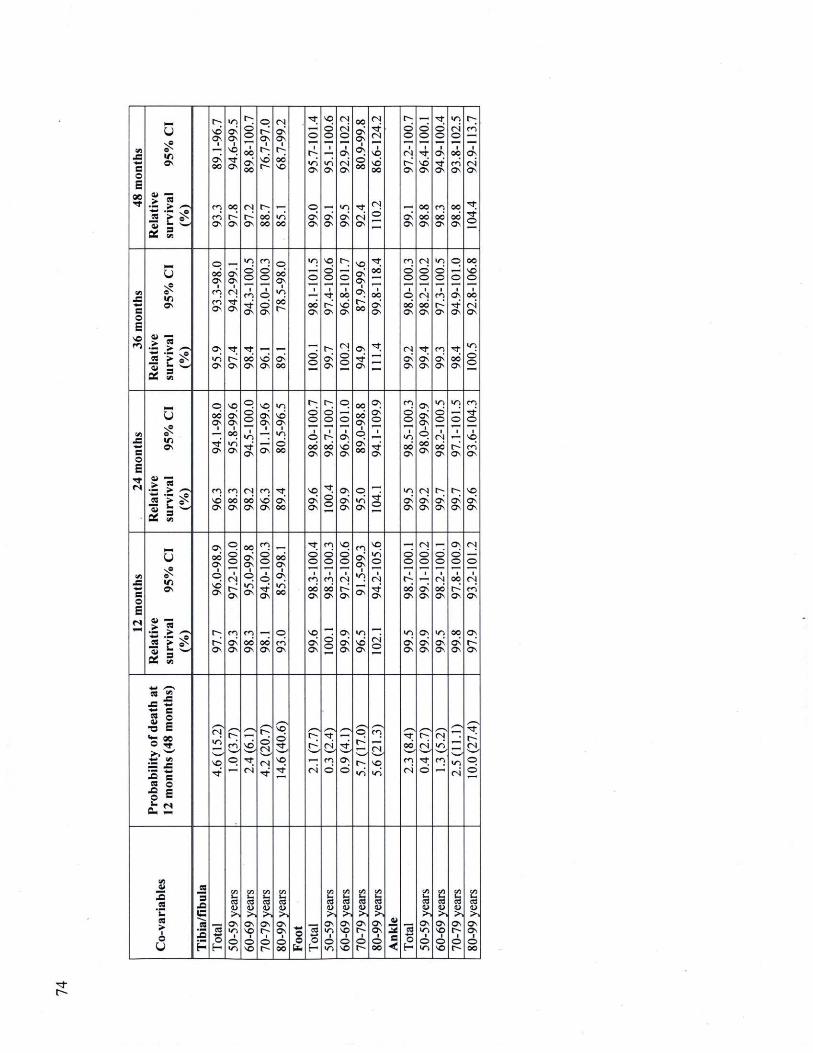
Vi
_= e o E
0 0 r f
Rela
tiv
e su
rviv
al
95%
C
I (%
)
O; vd Ov
■
d oo
rn rn Ov
un d Ov
■ VO r f OV
0 0
Ov
1; d o
OO d oo
Oj r~ OV
O r^ OV
■ t ; vd
O; 0 0 0 0
O l d Ov
i O ; 0 0 VO
un 0 0
r f
o 1
un Ov
O Ov Ov
VO d o
■
wn Ov
d Cv
O l o i ©
■ Ov o i Ov
u n d Ov
0 0 d Ov
1 Ov d oo
r f o i Ov
OJ r f OJ
i vq vd oo
O l d
o
© o
1 Oj
Ov
d OV
© ©
■ r f VD Ov
OO 0 0 Ov
r f © ©
i Ov r f Ov
en oo OV
un o i ©
0 0 r n Ov
0 0 0 0 Ov
O; rn
1 Ov o i Ov
r f r f ©
Vi _= m i S O
E VO r n
U
V i OV
** TS
if* — VJ
p 0 0 Ov
1 rn rn Cv.
Ov un Ov
d Ov OJ r f OV
r f r^ Ov
un d o
■ e n r f Ov
r f OO Ov
en d ©
■ p d Ov
vd Ov
p 0 0 Ov
1 un 0 0 r
d oo
un
o 1
oo Ov
d o
VO d o
i r f
Ov
r
d ov.
©
oo vd
Ov
O l
d ©
vq d Ov
■ Ov O^ o o
e3v r f Ov
r f 0 0
1 oo d
<3v
r f
m © ©
i © 0 0 ov
O l d Ov
O l © ©
1 Oj CO Ov
r f d Ov
VJ © ©
1 en o^ Cv
m d Ov
p
© I
Ov r f Ov.
r f OO Ov
OO vd ©
1 oo o i Ov
un d ©
Vi J= m* e o E
r f OJ
u
OV
« TS É 5 ^ _2 __ ^ u g
w
OS w
O 0 0 OV
1
r f Ov
en vd Cv
VO d Ov
i oo un OV
m 0 0 Ov
O d o
1 u n r f Ov
Oj oo Ov
VO d Ov
i
Ov
m vd Ov
un vd Ov
1 un d oo
r f d 0 0
d o
■ o 0 0 Ov
vq d Ov
d o
i r00 Cv
r f d o
p
S ■
Ov vd
Ov
Ov
d Ov
0 0 0 0 Ov
i © ON oo
p un" Ov
Ov d ©
■
r f Ov
r f ©
m © ©
i un oo Ov
un d Cv.
Ov d OV
i © OO Ov
Oj d Ov
un © ©
■ Oj oo
Cv
O;
d Cv
un
© t
Cv
O ;
d Ov
m r f ©
■ vq rn Ov
VO d Ov
en J =
e o E
OJ
u I D OV
> ra
if? — m
Os 0 0 Ov
1 o vd Ov
r^ Ov
O d o
i Oj o^ OV
m d Ov
OO d Ov
1 p un Ov
en oo Ov
en d o
i o r f Ov
0 0 Ov
0 0 Ov
1 Ov un 0 0
p rn OV
r f d o
■ en 0 0 Ov
VO d Ov
m d o
■ en 00 Cv
d o
VO d o
i Oj t~
Ov
Ov
d Ov
m d Ov un
Ov
un vd Ov
vq un ©
i O l r f Ov
o i ©
d ©
i O ; 0 0 Ov
un d Ov
O l d ©
d
Ov
Ov
d Ov
d ©
O j 0 0 Ov
un d <3V
Ov d ©
i oo t~ ov
0 0 d Ov
OJ
©
1 O j r n Ov
Ov r^ Ov
Pro
bab
ilit
y o
f death
at
12 m
on
ths
(48
mo
nth
s)
O j un
vo r f
rn © r f
o i
0 ^ d Ci O l r f
vq d r f _
VO r f o i
r ? oj, m d
r f v—* Ov d
v '
un
en
Ci vq un
r p 0 0
m o i
K1
d r f ©
' s O)
v j
en un o i
r ?
OJ
© ©
VJ — _= .2 *__ es ■
o
_S
_a ç "ra j a
"ra o
E
en fe a
Ov un
■ o un
cn fe <_> >>
Ov VO
i o VO
en S. ra a >.
Ov ■o
1 o o
en i ra <D >.
Ov Ov
i o 0 0
* 4 _
o o fc
o H
en fe eu >>
OV wn
i O un
en fe eu .>>
Ov VO
i o vO
en u . ra (U
Ov o
1 ©
Vi fe <D >.
OV Ov
i © oo
a
c <
"3 o
i
cn fe a >>
Ov un
■ © un
Vi '~ ra a >>
Ov VO
i © VO
en fe 0) >.
Ov o
1 © o
en
fe >
Ov Ov
i © oo
r t r
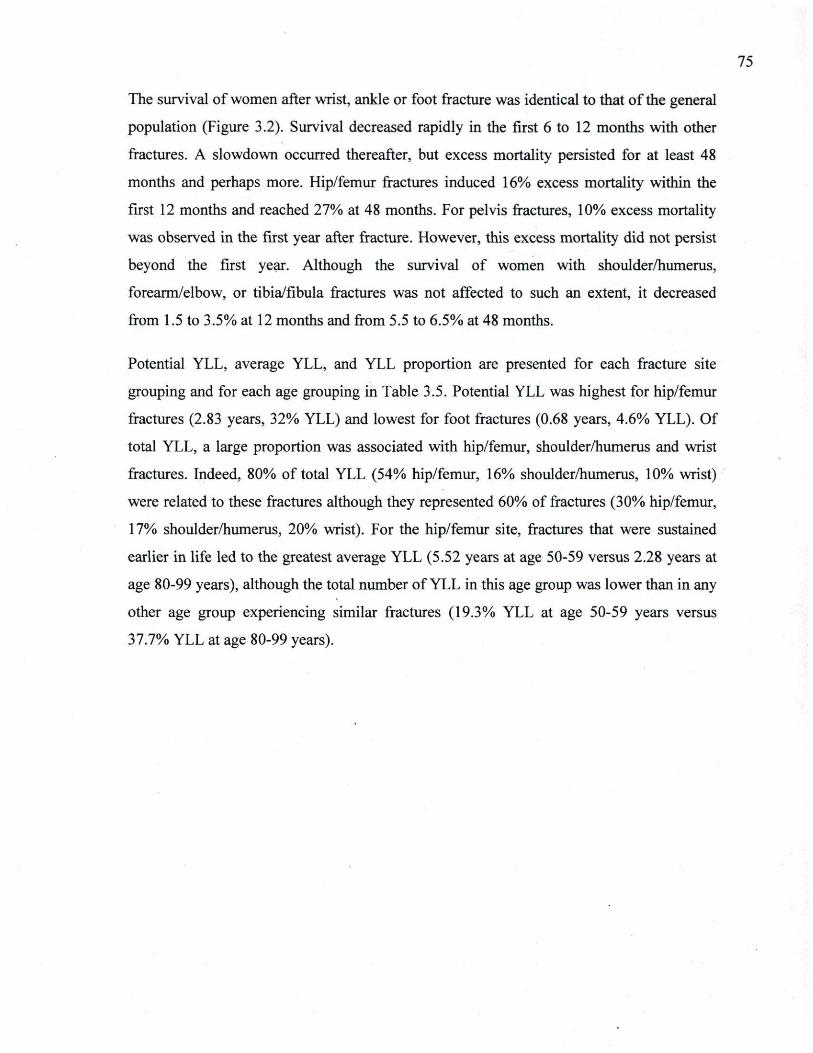
75
The survival of women after wrist, ankle or foot fracture was identical to that ofthe general
population (Figure 3.2). Survival decreased rapidly in the first 6 to 12 months with other
fractures. A slowdown occurred thereafter, but excess mortality persisted for at least 48
months and perhaps more. Hip/femur fractures induced 16% excess mortality within the
first 12 months and reached 27% at 48 months. For pelvis fractures, 10% excess mortality
was observed in the first year after fracture. However, this excess mortality did not persist
beyond the first year. Although the survival of women with shoulder/humerus,
forearm/elbow, or tibia/fibula fractures was not affected to such an extent, it decreased
from 1.5 to 3.5% at 12 months and from 5.5 to 6.5% at 48 months.
Potential YLL, average YLL, and YLL proportion are presented for each fracture site
grouping and for each age grouping in Table 3.5. Potential YLL was highest for hip/femur
fractures (2.83 years, 32% YLL) and lowest for foot fractures (0.68 years, 4.6% YLL). Of
total YLL, a large proportion was associated with hip/femur, shoulder/humerus and wrist
fractures. Indeed, 80% of total YLL (54% hip/femur, 16% shoulder/humerus, 10% wrist)
were related to these fractures although they represented 60% of fractures (30% hip/femur,
17% shoulder/humerus, 20% wrist). For the hip/femur site, fractures that were sustained
earlier in life led to the greatest average YLL (5.52 years at age 50-59 versus 2.28 years at
age 80-99 years), although the total number of YLL in this age group was lower than in any
other age group experiencing similar fractures (19.3% YLL at age 50-59 years versus
37.7% YLL at age 80-99 years).
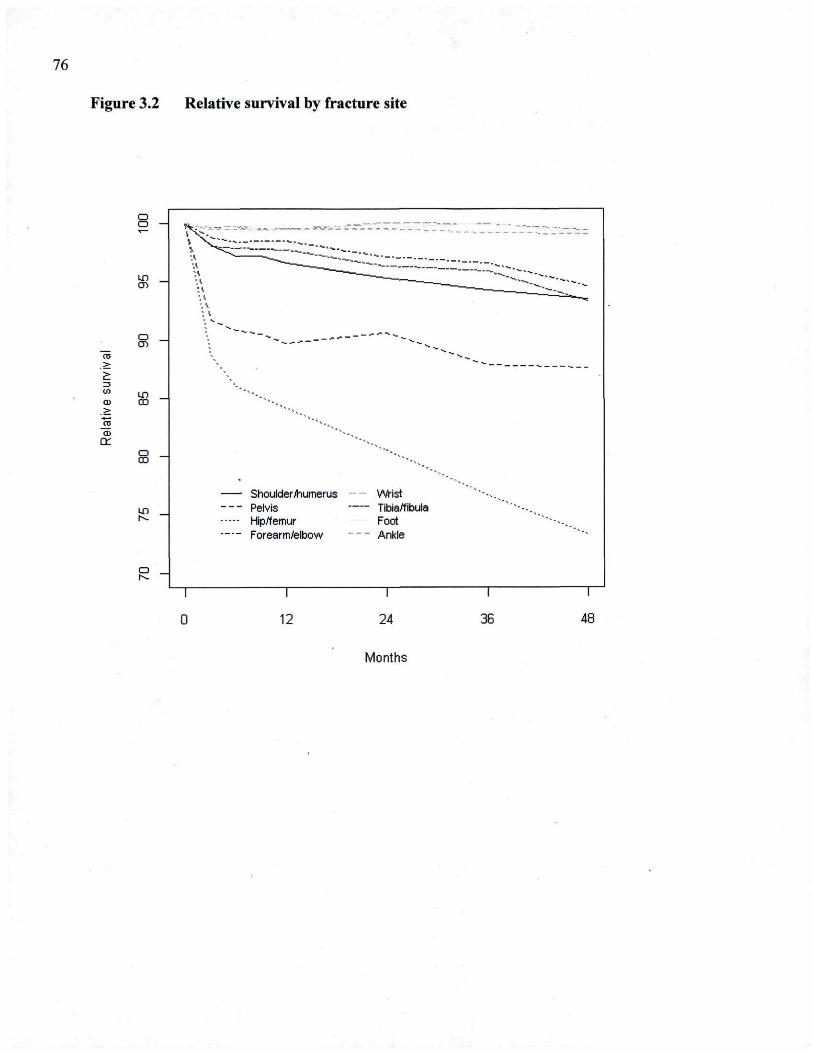
76
Figure 3.2 Relative survival by fracture site
a a — ^ . . 4 . , „ _ „ "~ ~ ™ " " " " ~ "
iX^ ^™J" *"*'" ~» _
'} ^ " — s _ ^ ^ "—— %_ |V 1— — —
un a.
v,\ ^ * _ _ ^ ^
',* ;\ ', \ ; \ , <.
• 4 ,
o \ ^ as > V
, £ 3 VI kn ' " ■ • .
a. co "***., > ". a: '* a j cr
o co
Shoulder/humerus Wrist LD Pelvis Tibia/fibula ■N. Hip/femur Foot
Forearm/elbow Ankle
a i~
12 24 36 48
Months
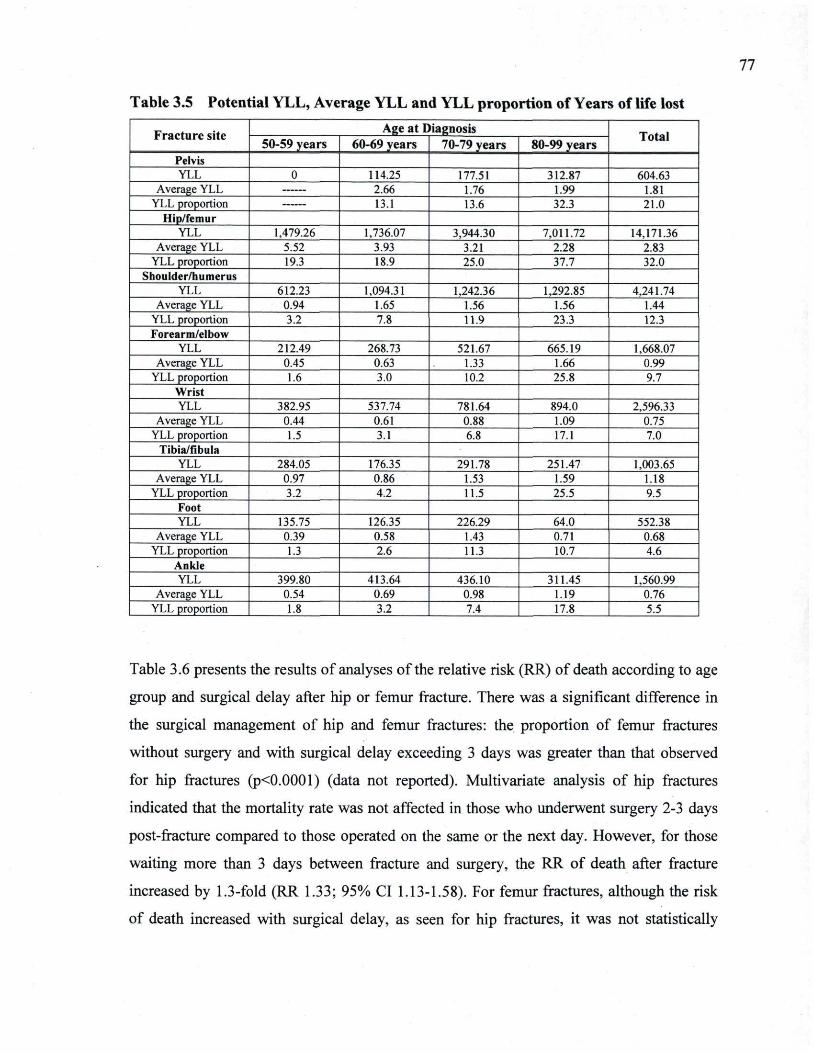
77
Table 3.5 Potential YLL, Average YLL and YLL proportion of Years of life lost
Fracture site Age at Diagnosis Total Frac ture site
50-59 years 60-69 years 70-79 years 80-99 years Total
Pelvis YLL 0 114.25 177.51 312.87 604.63
Average YLL 2.66 1.76 1.99 1.81 YLL proportion 13.1 13.6 32.3 21.0
Hip/femur YLL 1,479.26 1,736.07 3,944.30 7,011.72 14,171.36
Average YLL 5.52 3.93 3.21 2.28 2.83 YLL proportion 19.3 18.9 25.0 37.7 32.0
Shoulder/humerus YLL 612.23 1,094.31 1,242.36 1,292.85 4,241.74
Average YLL 0.94 1.65 1.56 1.56 1.44 YLL proportion 3.2 7.8 11.9 23.3 12.3 Forearm/elbow
YLL 212.49 268.73 521.67 665.19 1,668.07 Average YLL 0.45 0.63 1.33 1.66 0.99
YLL proportion 1.6 3.0 10.2 25.8 9.7 Wrist YLL 382.95 537.74 781.64 894.0 2,596.33
Average YLL 0.44 0.61 0.88 1.09 0.75 YLL proportion 1.5 3.1 6.8 17.1 7.0
Tibia/fibula YLL 284.05 176.35 291.78 251.47 1,003.65
Average YLL 0.97 0.86 1.53 1.59 1.18 YLL proportion 3.2 4.2 11.5 25.5 9.5
Foot YLL 135.75 126.35 226.29 64.0 552.38
Average YLL 0.39 0.58 1.43 0.71 0.68 YLL proportion 1.3 2.6 11.3 10.7 4.6
Ankle YLL 399.80 413.64 436.10 311.45 1,560.99
Average YLL 0.54 0.69 0.98 1.19 0.76 YLL proportion 1.8 3.2 7.4 17.8 5.5
Table 3.6 presents the results of analyses ofthe relative risk (RR) of death according to age
group and surgical delay after hip or femur fracture. There was a significant difference in
the surgical management of hip and femur fractures: the proportion of femur fractures
without surgery and with surgical delay exceeding 3 days was greater than that observed
for hip fractures (p<0.0001) (data not reported). Multivariate analysis of hip fractures
indicated that the mortality rate was not affected in those who underwent surgery 2-3 days
post-fracture compared to those operated on the same or the next day. However, for those
waiting more than 3 days between fracture and surgery, the RR of death after fracture
increased by 1.3-fold (RR 1.33; 95% CI 1.13-1.58). For femur fractures, although the risk
of death increased with surgical delay, as seen for hip fractures, it was not statistically
78
significant, which may be related to the small number of femur fractures in some subgroups
of surgical delay.
3.6 Discussion Over a 2-year period, more than 17,000 fractures were identified in a cohort of women over
50 years of age and residing in Quebec, Canada. The most frequently-occurring fractures
were those traditionally associated with osteoporosis - those at the hip/femur and wrist
(although spine fractures are commonly associated with osteoporosis, they were not
considered in this study) [7, 66]. The temporal sequence of fracture incidence was similar
to what has been described previously, with arm and lower leg fractures generally occurring
earlier in life than hip/femur fractures [7, 66]. Mean age at hip/femur fracture
(approximately 80 years) was similar to that in other large epidemiological investigations
[7, 50]. Before age 70 years, the incidence of hip/femur fractures was relatively low, but
increased exponentially thereafter. The incidence of upper arm fractures
(shoulder/humerus, forearm/elbow, wrist) rose roughly linearly with increasing age, in
agreement with previous reports [8].
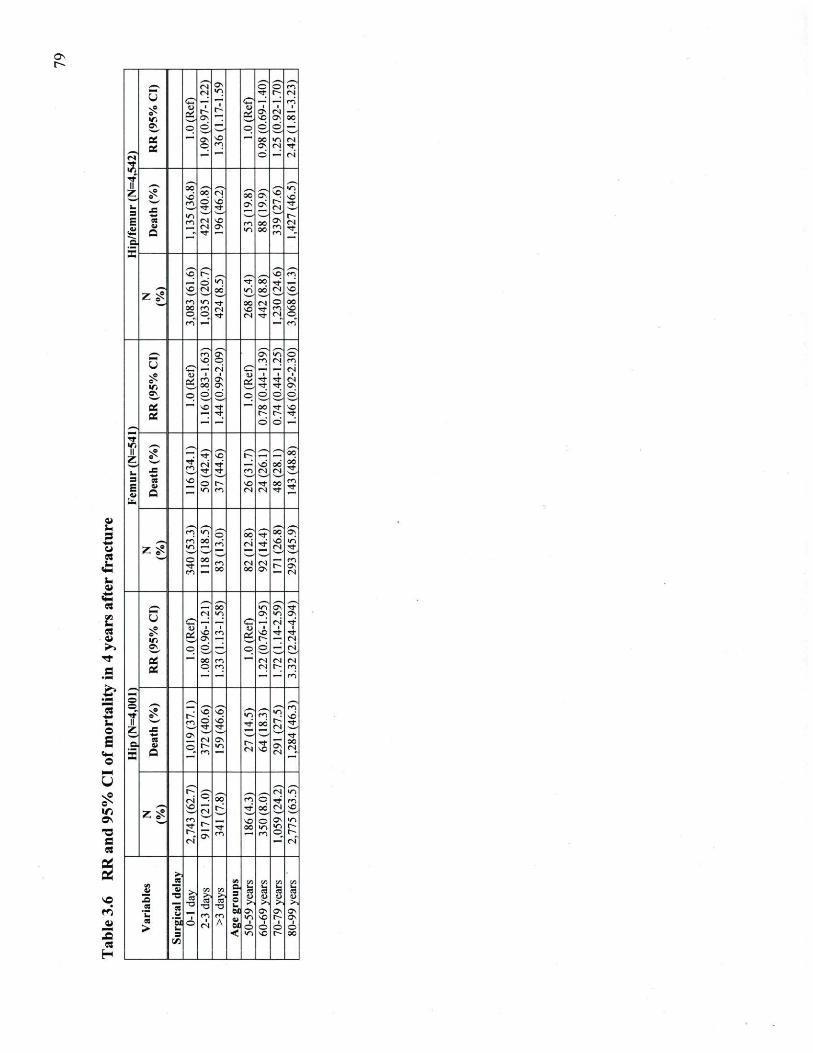
i i u s
•mm «
■ _ _ _
« im es
r f fi £ =■
_. o £
'—C v
_ _ _ ( N C v
O O m
U ( N vn r f 14 f N U O — — c: — — r n
5? u i
r■r g i
Cv 1
t N i
V I
u Ov 1 . g vO C v 0 0
»\ o © — o d d _* Qf —" C v vO
— 0 0 vn «s a p m C v t N r f
f v * a
— — O —' f N
r f V i
r t II II OC vn Z 13 _=
m oo o r f^
t N vd r f^
00 c< CV
t N
vd r r ^
S es Q
m (N t N r f
vO CV m
vn 00 oc
m m
t N r f
c
_s _s , , ,
3" •f» ,—. ,—, Cô r n
__. © V i r? 0 0 r f _'
*— ^c rN oo v i 0 0 t N vO
ZS "—"
' 4 ' — ■
ZS m vn r f 0 0 t N o 0 0
oc m ( N v O ^f m vc o r O r f t N r f t N c_
1 f i "
r n
_. r m O? O v vn o
u vo O m I N m u o _: r i C ,' f N
5? 1
m i
Cv g ■ r f r f
1 f N
V i 0 0 C v g r f r f O v OV o o © o O d O
g 'vO r f r f
00
o r f ro
vO r f
r f
tf. Il Z £ — G" P c. ZT 0 0 Il Z r f
m f N r f —' vd 0 0 00
rf_ 4 4
JC r f m r f r f m < N ( N
00 rf_
4 4
3 E Ci
Q VO O
un m vo (N
r t t N
00 r f
m r f
fc
r n un ô 0? r f se ST zg r n
un 0 0
m ' t N r f vd t N
vn r f
o r f m
oo m 00
t N 00
t N Ov C>
m Ov f N
0 0 vn S: r f
U ( N vn O v vn Ov U CT __' <=? t N r f
S? u i vO Cv
■ m g i
vO r
r f r f f N
o\ o © ,—', o o_ __ f N o CC H —• oo m — t N I N f N
S B o m es r~ m
| '— '— •—' ' r n
•— O , , O m r f * K \q vq vn en vn
vd II ••4W m o vd ^ oc l ~ rf_ Z — i 1
—' r f r f t N C v r f
a. X
es I Q
p (N m
Ov vn •r
<N r f vo t N
00 es
f " p t N vn t N
p 0 0 m © r f r n 4 ^ * 1 vO
—— f ^ T f OC f N VO 7 ^
m f N
VO o Ov * n
^^ r f
f N
4 OC vn vn e~ f ;
C v m m q e~ r i f N
• > 1 es !« V J V J V , V I
VI ° _S es 1 T _
Vi a. g 1 S5 •_> _5 VI °
_S es es
T _ _J TD
_3 T3
o _. > ■ >, >, >, es M av C v 0v O v
I H es
i m m Ci as.
vn v O r C v es
__■ 'S O
( N A Ci as. O
i O
■ o
i O
3 < vn v O t oc
| v:
80
In contrast, the incidence of lower leg fractures (tibia/fibula, foot, and ankle) was generally
constant over the ages studied. This result is consistent with other observational studies and
suggests different aetiologies of these fractures [66]. Moreover, recent evidence indicates
that a significant proportion of ankle fractures are linked with higher body mass index
[156]. Applying a recently-updated definition of an osteoporotic fracture (i.e. fractures
occurring at a site associated with low BMD and which increase in incidence after age 50
years) [31], such observations prompt us to consider these fractures as not being related to
osteoporosis.
Numerous studies have recently reported that the incidence of hip fractures is decreasing
over time, perhaps as a consequence of better treatment or secular changes [54, 57, 157-
162]. Furthermore, there is evidence that the mean age of those who suffer hip fractures is
increasing as people are typically healthier in older age, skewing the incidence curve of
such fractures towards older age [162]. A recently-published report demonstrated a decline
in the age-adjusted incidence of other major osteoporotic fractures (forearm and humerus
but not spine) [68]. However, the aetiology behind these changing trends needs to be
elucidated.
With regard to mortality, we have observed that the highest fracture-associated mortality
follows hip/femur or pelvis fractures, that substantial increases in fracture-related mortality
occur in the first year post-fracture, and that a significantly negative impact of these
fractures on survival persists after 4 years.
These findings are similar to those of many other trials that demonstrated significant
decreases in survival with hip fractures [47, 70, 76, 77, 131, 148, 163-182]. Similar to our
results, a Swedish patient register study concluded that 17-32% of deaths were causally
related to hip fracture [182]. A recent systematic review ofthe literature [174] noted that
hip fracture patients have an excess risk of mortality compared to the general population,
and it persists for several years. Moreover, several studies reported that the greatest risk of
death was within the first 6 months after fracture. A recent meta-analysis concluded that
there was a 5- to 8-fold increase in the risk of mortality in the initial 3 months after hip
fracture, with risk decreasing from that time point but remaining significantly elevated,
even after 10 years of follow-up [148].
81
Increased mortality has been reported across all age groups after low-trauma hip, vertebral
and other major fractures (pelvis, distal femur, proximal tibia, ribs and humerus) [76, 77].
A recent study of healthcare databases from the province of Manitoba, Canada observed
that, after adjustment for age, number of co-morbidities and level of dependence in living
arrangements, major fractures at typical osteoporotic sites (hip, vertebral, humerus, wrist
(men only) and other fractures) are associated with increased mortality across all age
groups, particularly in men [76]. Similarly to our investigation, it discerned the highest
mortality risk 12 months post-fracture, and this risk remained elevated until 5 years after
most fractures, with the highest risks attributed to hip and vertebral fractures. While lower
leg and arm fractures were not linked with as much fracture-related decreases in survival,
they did have a significant impact on mortality, as reported previously [77, 131, 173].
Significant losses in average YLL were associated with hip/femur fractures (average 2.83
years) and pelvic fractures (average 1.81 years). Contrasting with other types of fractures,
the average YLL with hip/femur fractures at an earlier age was greater than later age
fractures. This cohort of women fracturing at the hip/femur or pelvis between 50-70 years
of age may represent a truly frail population. Other peripheral fractures tended to have a
greater impact on average YLL and YLL proportion as age at the time of fracture increased.
For hip and femur fractures, the most common reason for delayed surgery may be related to
the need to stabilize other acute medical conditions, unavailability of operating room time
and/or human resource constraints [101, 183, 184]. In Canada, Ministers of Health from
several provinces consider surgery within 48 hours of admission as a performance indicator
[185], and Federal Government has included it in their wait time reduction strategy [186].
In this study, as reported previously, a small proportion of hip fractures had no surgery
procedure recorded in the database [101]. Similarly to a Canadian study of hospitals outside
Quebec, more than two-thirds (68%) of patients were surgically treated on the day of
fracture or the next day [99]. In this study, a delay of more than 3 days for surgery to repair
a hip fracture was coupled with an overall 58% increase in mortality risk. Surgical delays in
treating hip fractures have been previously linked with a high risk of short-term mortality
[184, 187, 188]. Our analysis has limitations that may be due to our not having adjusted for
pre-existing medical conditions or co-morbidities (i.e. patients for whom surgery was
82
delayed may be sicker than those without delay); however, most studies showed that the
effect of surgical delay persisted, even after adjustment for the severity and number of pre
existing medical conditions [101, 183, 188]. Moreover, shorter time to surgery has been
associated with reduced post-surgery complications, pain, and hospital stay [100, 189].
Thus, a proportion of the hip fracture population not receiving surgical attention promptly
may represent a more morbid segment that would have otherwise had a decreased life
expectancy.
Our study investigated the association between fractures and survival only in women.
Numerous others have presented data showing that men have significantly lower survival
time than women after osteoporotic fractures [76, 77, 148, 168, 170, 181, 190]. Vestergaard
et al. [179] suggested that, if men or women of particular age groups experience significant
losses in expected remaining lifespan consequent to fracture, they should be targeted for
preventive programs. Recent investigations have demonstrated that bisphosphonate therapy
after hip fracture may increase survival time [191], and several studies have indicated that
the decrease in FF rates observed in the past decade may be a consequence of better
preventive approaches to osteoporosis with anti-fracture therapies [54, 157, 159].
Unfortunately, it has repeatedly been documented that, even in high-risk women who have
suffered a FF, osteoporosis remains under-recognized and under-treated [4].
The major strength of our study is the use of population-based data that provide power and
wide population coverage/representation. Other strengths of our analysis include a large,
validated database to assess the relationship between mortality and a number of different
fracture types. The ability to apply a validated algorithm for the identification of fracture
cases was an important asset for our investigation. The algorithm identified inpatient and
outpatient fracture cases, thereby achieving a better understanding of the true burden of FF
not leading to hospitalization.
Our study had some limitations that need to be addressed. Vertebral fractures were not
included in our investigation due to the inability to properly identify them in administrative
databases. This limitation of not being able to identify vertebral fractures from
administrative databases is not unusual as approximately two-thirds of them do not come to
clinical attention [139, 192, 193]. Furthermore, our investigation only included women
83
from 3 health regions that represented 42% of the population in Quebec province; it is
possible that fracture and mortality rates differ in other regions for socio-economic and
regional reasons. Another limitation was that no attempt was made to quantify the trauma
of fracture, with approximately 19% resulting from high-energy trauma events. Patients
suffering high-energy trauma fractures may have a different survival profile from patients
who experience low-energy trauma fractures. No adjustments were made for co
morbidities, surgical delay after fracture, or complications after the index fracture, all of
which may have significant independent impacts on survival time. A few investigations
have reported that survival time after fracture is influenced by the number and severity of
co-morbidities [175, 182]. Therefore, this limitation may have an impact on the magnitude
of the results but does not invalidate our conclusion, since several studies making such
adjustments obtained results similar to ours [182]. However, future work on this
population-based cohort will attempt to include controls for these variables.
In conclusion, we have shown that non-vertebral FFs are common in women above the age
of 50 years, with fractures of the lower leg, particularly the ankles and arms (humerus
forearm/elbow and wrist) occurring frequently after 50 years of age. Hip and pelvis
fractures are rare before 70 years of age but increase substantially thereafter. Hip and pelvis
fractures are associated with the greatest YLL, being most striking in the initial year after
fracture, but continuing to have a significant impact on survival for at least 4 years. Other
fracture types also generally resulted in significantly decreased survival in our cohort of
women.
Osteoporosis-related fractures are an important public health problem, and health
authorities should consider establishing interventions that promote prevention before the
age of 50 years, with targeted approaches for FFs avoidance before the age of 60 years.
3.7 Acknowledgments This research, part of the Recognizing Osteoporosis and its Consequences in Québec
(ROCQ) Study, was made possible through the support of founding partners Merck
Canada, sanofi-aventis Canada Inc., and Warner Chilcott as well as major partner Amgen
Canada Inc. and minor partners Eli Lilly Canada Inc. and Novartis Pharma Canada Inc.
84
These funding sources had no access to the data prior to publication and, no input into
writing ofthe manuscript as well as in the decision to publish the results.
Sonia Jean designed the study, directed its implementation, acquired data, analyzed and
interpreted the data, and drafted the manuscript. Bernard Candas contributed to study
design, helped with its implementation, interpreted the data and drafted the manuscript. All
other authors interpreted the data and reviewed the article critically for intellectual content.
85
Chapitre 4
Utilisation des ressources médicales directement associées aux fractures ostéoporotiques
chez les femmes ménopausées
Direct medical resources utilization associated with osteoporosis-related fractures in postmenopausal women
L'objectif de ce chapitre est de présenter les résultats de l'étude visant à estimer l'utilisation des ressources médicales directement associées aux traitements des fractures, aux consultations médicales et aux hospitalisations dans l'année suivant la fracture..
Les résultats de cette étude ont fait l'objet d'une présentation orale à la conférence annuelle de l '«American Society for Bone and Minerai Research» (ASBMR) en septembre 2011. De plus, la grande qualité de ces travaux a été soulignée par la remise d'un prix honorifique «2011 Young Investigator Award» lors de cette conférence. Les auteurs sont Sonia Jean, Louis Bessette, Etienne L Belzile, K. Shawn Davison, Bernard Candas, Suzanne Morin, Sylvie Dodin et Jacques P. Brown. Le chapitre comporte l'intégral de l'article en anglais.
87
4.1 Résumé OBJECTIF: Estimer l'utilisation des ressources médicales directement associées aux
traitements des fractures ostéoporotiques non-vertébrales et évaluer l'impact de l'âge.
MÉTHODES: Un algorithme précédemment validé pour le fichier des services rémunérés
à l'acte a identifié 15 327 femmes de 50 ans et plus ayant subi une fracture ostéoporotique
incidente à un site non-vertébral entre le 1 janvier 2004 et le 31 décembre 2005. Pour
déterminer l'utilisation des ressources médicales dans l'année suivant la fracture, les bases
de données médico-administratives sur les services de santé offerts aux résidents du Québec
ont été utilisées. Ces données ont été liées par un identifiant personnel unique afin de créer
une cohorte longitudinale sur l'utilisation des ressources médicales pour tous les cas de
fractures. Les proportions des fractures traitées par une réduction ouverte, une réduction
fermée, une immobilisation ou un suivi médical avec un orthopédiste ont été évaluées. Le
nombre moyen des réclamations associées aux consultations avec un orthopédiste ou aux
visites avec d'autres cliniciens ainsi que le taux d'hospitalisation et la durée de séjour ont
été estimés.
RESULTATS: Les fractures de la hanche/fémur utilisent une grande proportion des
ressources médicales puisque la majorité d'entre elles nécessitent une chirurgie (91.1%) et
une hospitalisation (94.5%) avec une durée moyenne de séjour (médiane) de 39.2 (31)
jours. Cependant, les autres fractures non-vertébrales exigent également une proportion
importante des ressources médicales en termes des soins cliniques liés aux traitements
chirurgicaux (27.9%), aux consultations médicales avec un orthopédiste (77.4%) et aux
hospitalisations (27.3% de la durée de séjour totale). Même les fractures du bassin qui
requièrent plutôt un traitement conservateur nécessitent des ressources médicales
importantes en raison de l'hospitalisation d'une grande proportion des personnes atteintes
(64.7%) avec une durée moyenne de séjour (médiane) de 34.2 (26) jours.
Finalement, l'âge est un déterminant important de l'utilisation des ressources médicales. En
effet, l'âge est associé à une augmentation du nombre de visites avec un médecin, de
l'hospitalisation et de la durée d'hospitalisation. Il est également associé à une
augmentation des admissions dans un centre de soins de longue durée et des décès.
88
CONCLUSION: L'utilisation des ressources médicales associées au traitement des
fractures ostéoporotiques est considérable. Avec le vieillissement de la population et
l'augmentation de la prévalence de ces fractures, des stratégies de prise en charge de
l'ostéoporose doivent être introduites afin de réduire le fardeau de cette problématique sur
le système de santé.
89
4.2 Abstract PURPOSE: To assess direct medical resource utilization related to the treatment of non-
vertebral osteoporotic fractures within 1 year post-fracture and to evaluate if age impacts
resource utilization.
METHODS: A previously-validated algorithm for physician claims databases identified
15,327 women aged 50 years or older with incident fracture at non-vertebral osteoporotic
sites between January 1, 2004 and December 31, 2005. Administrative databases ofthe
health services available to all residents in Quebec served to study fracture-related health
resource utilization in the year after fracture. Data were linked by a unique personal
identifier, creating a longitudinal cohort of all fracture cases for health resource utilization.
The proportions of fractures treated by open reduction, closed reduction, immobilization or
follow-up by an (OS) were evaluated. The mean number of claims for consultation with an
OS or other clinicians in inpatient and outpatient visits, the hospitalization rate and length
of stay (LOS) were assessed.
RESULTS: Hip/femur fractures represented the highest rate of resource utilization since
the majority of them required surgery (91.1%) and hospitalization (94.5%) with a mean
(median) LOS of 39.2 (31) days. However, other non-vertebral fracture types needed
significant clinical care related to surgery (27.9%), follow-up consultation with an OS
(77.6%) and hospitalization (27.3% of total LOS). Even pelvic fractures, which often do not
require surgical treatment, commanded high resource utilization due to the high
hospitalization rate (67.4%) with a mean (median) LOS of 34.2 (26) days. Moreover, age
was an important determinant of health resources utilization, being associated with an
increased number of visits to other physicians, hospitalization and length of hospitalization
(LOH), admission to long-term care (LTC) and death.
CONCLUSION: Osteoporosis-related fractures accounted for substantial health care
resource utilization. With an aging population and increased prevalence of these fractures,
strategies for osteoporosis management need to be introduced to reduce the healthcare
burden.
90
4.3 Introduction As in many other industrialized countries, osteoporosis prevalence is high in Canada,
affecting more than 1 in 5 women over the age of 50 years [194]. Osteoporosis is a major
public health problem owing to its association with fragility fractures (low-energy
fractures), particularly those of the spine, hip, humerus and distal forearm [195]. It is
estimated that a 50-year-old woman has a 50% remaining lifetime risk of fragility fracture
[9]. Recently, it has been reported that approximately 81% of all fractures in women >50
years of age can be classified as fragility fractures and attributed to osteoporosis [4].
Until now, the majority of studies have focused on hip fractures because of their
disproportionate burden on individual health status and their socio-economic impact
compared to other fragility fractures [67, 133]. However, some evidence suggests that non-
hip fractures also represent a significant burden, resulting in disability, impaired quality of
life, increased mortality, morbidity as well as significant healthcare costs [10, 36, 76, 130-
132, 196-198].
Recent Canadian studies have observed a reduction in age-standardized rates of hip fracture
in both sexes and of 2 major low-trauma fracture sites (forearm and humerus) in women
[57, 68]. With increased life expectancy, the population most at risk of fractures (i.e. those
65 years and older) is projected to grow from 14% in 2006 to 28% in 2056 [91]. Therefore,
even under the assumption of declining rates, the absolute number of fragility fractures will
continue to rise, imposing a heavy healthcare burden.
Details of direct medical resource utilization required for the treatment of fragility fractures
by skeletal site may help to understand the impact of these fractures on the health care
system. This information can also be analyzed in conjunction with incidence data to project
and estimate the healthcare resources needed and may help policy-makers to plan resource
allocation and care organization to maintain and increase efficiency. The assessment of
resource utilization beyond the initial treatment is essential to understand the care pathway
related to different fractures and is the first step towards the developing and implementing
performance indicators.
91
The purposes of our study were to ascertain the burden related of non-vertebral fragility
fractures by analyzing direct medical resource utilization for their treatment in
postmenopausal women in the year after the fracture and to evaluate if age is a determinant
of medical resource utilization.
4.4 Materials and Methods 4.4.1 Study Cohort and Design
In this population-based, retrospective cohort study, all women aged 50 years or older who
experienced incident non-vertebral osteoporotic fractures between January 1, 2004 and
December 31, 2005, were identified in 3 of Quebec's largest provincial health regions
(Montreal, Quebec City and Mauricie). These 3 regions account for an estimated 42% of
the population of women 50 years of age or older in Quebec province [153]. This cohort of
recently-fractured women was identified from a previous study that validated an algorithm
for fracture case identification [129]. Administrative databases of healthcare services
(RAMQ physician fee-for-service claims and Med-Echo hospital discharge) delivered to
most residents in Quebec were considered to track fracture-related direct medical resource
utilization in the year after fracture. RAMQ database collect and store medical claims
information from approximately 94% of Quebec-based physicians and almost 98% of 7.5
million residents in Quebec province [121].The data from both databases were linked by a
unique personal identifier, creating a longitudinal cohort of health resource utilization for
all fracture cases.
This project was approved by the Research Ethics Board of Centre hospitalier universitaire
de Québec, CHUQ and linkage with these administrative databases was approved by the
Québec Commission d'accès à l'information, (http://www.cai.gouv.qc.ca).
4.4.2 Data Sources
In Canada, physician and hospital services provided to all citizens are covered by a
universal health insurance plan. In Quebec province, this plan is administered by the
RAMQ, which maintains the computerized physician fee-for-service claims database
containing information related to physician reimbursement. It includes: the physicians'
92
unique identification numbers, patients' unique provincial health insurance numbers
(NAM), medical service billing codes for clinical services, dates and locations of the
clinical services provided, and, optionally, diagnoses as per ICD-9-CM codes, included in
91% of all RAMQ claims. The RAMQ also maintains hospital discharge databases (Med-
Echo) containing information on patient demographics, diagnosis and co-morbidities at
admission, care, and destination at discharge provided in general and acute care hospitals
(not including long term care and rehabilitation facilities). Diagnoses are coded using 16
diagnostic codes (ICD-9-CM) before April 1, 2006, and 25 diagnostic codes (ICD-10-CA)
thereafter. Some studies have shown that administrative healthcare databases have a high
level of reliability and validity [16, 17], and their linkage provides a powerful resource
when investigating health issues such as health resource utilization [199].
4.4.3 Identification of incident fracture cases
An algorithm developed for the physician fee-for-service claims database (RAMQ),
identified all incident non-vertebral fracture cases during the period of interest [129]. With
guidance from a panel of clinical experts, the algorithm was designed to first select all
medical services claims potentially associated with fracture treatment: (a) claims with
medical services billing codes definitively related to fracture care (i.e., open or closed
reduction), or (b) claims with medical service billing codes not limited to fracture care (i.e.,
immobilization, consultation, principal or follow-up visit with an orthopaedic surgeon (OS),
emergency physician (EP), or general practitioner (GP)) if they were combined with ICD-9-
CM diagnostic codes of fracture. Using these extracted claims, the algorithm considered an
incident fracture had occurred if there was at least one claim associated with (a) fracture
treatment (open reduction, closed reduction, immobilization), (b) principal visit to an OS
with at least one other claim, or (c) consultation with an OS with at least one other claim.
The claim allowing fracture identification was referred to as the « index claim ». The
validity of this algorithm has been evaluated and published [129].
Fractures were grouped according to fracture site indicated by the specific medical service
code ofthe index claim or, if not specific to the treatment of fracture, to ICD-9-CM codes.
To establish the complete temporal sequence of medical care for each fracture, the
algorithm identified any other claim (emergency room visit, follow-up visit, etc.) related to
93
the same anatomical site as the fracture. The date of fracture corresponded to the date ofthe
first claim in the temporal sequence of medical care. Finally, a 6-month period was
established as « washout period » between 2 clinical sequences related to the same
anatomical fracture to minimize potential misclassification of fracture follow-up as a new
incident fracture.
In administrative databases, no information was available on the circumstances surrounding
the incident fracture event and we could not identify traumatic and pathological fractures.
Since fragility fractures represent the vast majority of fractures in women aged 50 years or
older (approximately 81% of this population) [4], all fracture types (traumatic, non
traumatic, and pathological) were included in the analyses. Furthermore, both low and high-
energy trauma fractures have been proposed recently for inclusion as outcomes in
osteoporosis studies as they are linked with decreased in bone mineral density and result in
increased risk of future fracture [33]. Similarly, pathological fractures were not excluded
since they represent a very small proportion, and their exclusion may lead to
underestimation ofthe burden of osteoporotic fractures [33, 34]. Women who had multiple
fractures, either suffered at the same time or at different times during the assessment period,
were eliminated from the analyses as it was often impossible to accurately ascertain the
resources utilized for each fracture independently. Fractures at the following sites were
investigated in our study: hip, femur, pelvis, shoulder, humerus, forearm, elbow, wrist,
tibia, fibula, foot and ankle. Vertebra, sacrum and coccyx fractures were not included in the
analyses since sensitivity of the algorithm was unacceptably low for the identification of
fractures at these sites [129]. Furthermore, vertebral fractures are generally under-reported
in administrative databases [139]. Also, cranio-facial, hand, finger, patella and toe fractures
were excluded since they are not typically associated with osteoporosis [31].
4.4.4 Identification of health resources used
To assess direct medical resource utilization for the treatment of each fracture, direct
medical resources were identified in both physician fee-for-service claims (RAMQ) and
hospital discharge (Med-Echo) databases. The records for each fracture case retained for
analysis were followed forward in time between January 1, 2004 and December 31, 2007
94
and linked to create a longitudinal cohort of fracture cases for health resource utilization
analysis.
To select claims in the physician fee-for-service claims database, all claims were screened
to ensure they were relevant to fracture treatment. To prevent the addition of claims linked
to subsequent or previous fracture type, claims were only retained if they were billed with
medical service billing codes or ICD-9-CM diagnostic codes directly related to the original
fracture site or a site considered to be affected by the original fracture (i.e. concomitant
site).
To evaluate resource utilization related to hospitalization, all admissions in the hospital
discharge database (Med-Echo) of patients included in the study cohort were screened and
retained if related to fracture treatment and, for re-hospitalization, if related to fracture
treatment (rehabilitation), or complications. Each hospital admission was categorized by
one of the clinical investigators (EB), a practicing orthopaedic surgeon, according to one of
the following criteria:
1- Hospital admission with primary diagnostic codes of fracture (same site,
concomitant site, unspecified site, pathological fracture);
2- Hospital admission with procedure intervention codes of fracture repair (same site);
3- Hospital admission with primary diagnostic codes associated with fracture;
4- Hospital admission with primary diagnostic codes associated with fracture
complication;
5- Hospital admission with secondary diagnostic codes of fracture (same site,
concomitant site, unspecified site);
6- Hospital admission unrelated to fracture.
With the exception of unrelated hospital admissions (criteria 6), lists ofthe diagnostic codes
and procedural intervention codes are presented in Appendices 3 and 4. Hospital admission
was considered as definitely related to fracture if it met any ofthe criteria numbered 1 to 3.
95
Hospital admissions meeting criteria number 4 were considered as probably related to the
fracture, as were hospital admissions meeting criteria number 5 if the admission date was
within 14 days ofthe index fracture for hip/femur and 10 days for other sites. All other
hospital admissions were assumed to be unrelated to the fracture and were not included in
the study. Appendix 5 details the selection of hospital admissions.
In this study, we considered hospitalization as initial hospital admission with any
readmission to another hospital within 1 day. Re-admissions that occurred 2 or more days
after discharge from a previous admission were considered as re-hospitalizations.
Hospitalizations and re-hospitalizations that occurred more than 1 year after the index
fracture were ignored.
4.4.5 Assessment of the direct medical resources utilization
For each fracture retained, our analysis provided an assessment of health service utilization
at the population level. First, medical claims were used to describe all medical services
related to fracture treatment and physician consultation. This information was also used to
describe fracture treatment type, which had a direct impact on medical resource utilization.
Fractures requiring surgery (open reduction) involved operating room utilization, which
necessarily requires many medical resources and, most likely, hospitalization. Closed
reduction of fracture requires more resources than fractures treated by immobilization since
such procedure are performed by OSs. Similarly, fractures requiring immobilization would
likely involve cast room resources, thereby consuming more resources than fractures treated
by conservative observational treatment (i.e. non-weight-bearing protected use or rest with
a follow-up visit to an OS without casting or immobilization). Therefore, in our analysis,
the most resource-intensive fracture treatment was open reduction and internal fixation,
followed by closed reduction, immobilization and, finally, conservative observational
treatment. The proportions of fractures treated by each type of treatment were calculated
according to this classification. Moreover, mean number of outpatient visits to an OS and
mean number of inpatient and outpatient visits to other physicians were evaluated for each
fracture site.
96
All hospitalizations included in the analysis were considered, to assess direct medical
resource utilization for hospitalization. More specifically, the rate of fractures requiring at
least 1 hospitalization directly related to their treatment was determined for each fracture
site. The rate of hospitalization requiring at least 1 re-admission to another hospital within 1
day and the rate of re-hospitalization were also calculated. The lengths of stay at individual
admission (LOS) and length of hospitalization (LOH) that included stays in several
hospitals (initial hospital admission with all re-admissions (for rehabilitation or
complications post-fracture) to another hospital within 1 day) are reported, in days, for
initial hospitalization and fracture-related re-hospitalization. Furthermore, for long term
care (LTC) resident and non-LTC residents at initial admission, the destination at discharge
(acute care, rehabilitation, local community health services center (CLSC), home, LTC,
inpatient death) was ascertained from the last hospitalization related to fracture care
Finally, to evaluate if patient age is an important determinant of heathcare resource
utilizations, all statistics on healthcare resource utilization were calculated by age group.
The statistical significance of the age, we analyzed by Pearson's chi-squared test for
dichotomous variables and by the Wilcoxon test for continuous variables.
All statistical analyses were undertaken with SAS software (version 9.1, SAS Institute,
Cary, NC, USA).
4.5 Results During the study period (2004-2005), the algorithm identified 18,927 incident fractures (in
17,661 women). Vertebra, coccyx and sacrum fractures (N=286) were excluded since
unacceptably low Sn was associated with the algorithm utilized for their identification.
Knee fractures (N=500) not considered as related to osteoporosis, and women less than 50
years old (N=362) when their fracture occurred, were also excluded. Finally, women with
multiple fractures (N=l,186) (same or different events) were excluded since it was not
possible to independently assess the health resources used for each of these fracture events.
Therefore, data on 2,334 women were removed from the analysis, leaving 15,327 women
aged 50 years or older with a single fracture event during the study period (Figure 4.1).
97
The number of fractures by site and the median (Q1-Q3) age of cases are reported in Table
4.1. In this cohort, hip/femur fractures represented 29.6% of all fracture, and non-hip
fractures, 70.4%. The most common fracture sites identified were the hip/femur (29.6%),
wrist (20.6%), shoulder/humerus (17.0%) and ankle (12.0%). When all fracture groups
were combined, median age (Q1-Q3) at fracture was 73 (61-82) years. Median age at
hip/femur fracture was approximately 10 years older than median age at other peripheral
fractures.
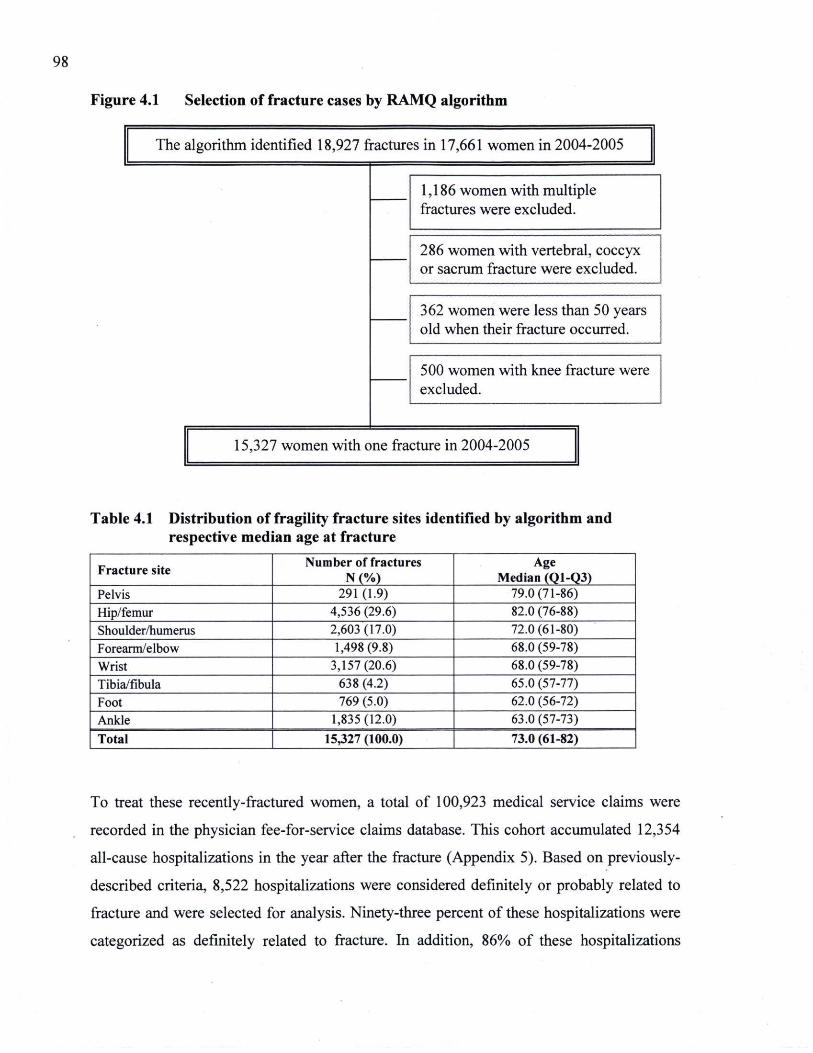
98
Figure 4.1 Selection of fracture cases by RAMQ algorithm
The algorithm identified 18,927 fractures in 17,661 women in 2004-2005
1,186 women with multiple fractures were excluded. 1,186 women with multiple fractures were excluded.
286 women with vertebral, coccyx or sacrum fracture were excluded. 286 women with vertebral, coccyx or sacrum fracture were excluded.
362 women were less than 50 years old when their fracture occurred. 362 women were less than 50 years old when their fracture occurred.
500 women with knee fracture were excluded. 500 women with knee fracture were excluded.
15,327 women with one fracture in 2004-2005
Table 4.1 Distribution of fragility fracture sites identified by algorithm and respective median age at fracture
Fracture site Number of fractures N (%)
Age Median (Q1-Q3)
Pelvis 291 (1.9) 79.0(71-86) Hip/femur 4,536 (29.6) 82.0 (76-88) Shoulder/humerus 2,603(17.0) 72.0(61-80) Forearm/elbow 1,498(9.8) 68.0 (59-78) Wrist 3,157(20.6) 68.0 (59-78) Tibia/fibula 638 (4.2) 65.0 (57-77) Foot 769 (5.0) 62.0 (56-72) Ankle 1,835(12.0) 63.0(57-73) Total 15,327 (100.0) 73.0 (61-82)
To treat these recently-fractured women, a total of 100,923 medical service claims were
recorded in the physician fee-for-service claims database. This cohort accumulated 12,354
all-cause hospitalizations in the year after the fracture (Appendix 5). Based on previously-
described criteria, 8,522 hospitalizations were considered definitely or probably related to
fracture and were selected for analysis. Ninety-three percent of these hospitalizations were
categorized as definitely related to fracture. In addition, 86% of these hospitalizations
99
occurred within a window of 14 days from the fracture date for hip/femur fractures and 10
days for other non-vertebral fractures.
Tables 4.2 and 4.3 report direct medical resource utilization for fracture treatment and
physician consultation. Globally, 43.6% of all claims were for hip/femur fracture treatment
(Table 4.2). Since a large proportion of hip/femur fractures are treated with surgery (91.1%,
Table 4.3), they required 72.1% of all clinical care related to surgery (open reduction). As
expected, when hip/femur fractures were treated by surgery, the hospitalization rate was
very high: 98.3% (data not reported). Therefore, hip/femur fractures consumed a large
proportion of medical consultations with an average of 2.0 outpatient visits to OSs, and 5.4
and 1.5 inpatient, and emergency/outpatient visits to other physicians, respectively.
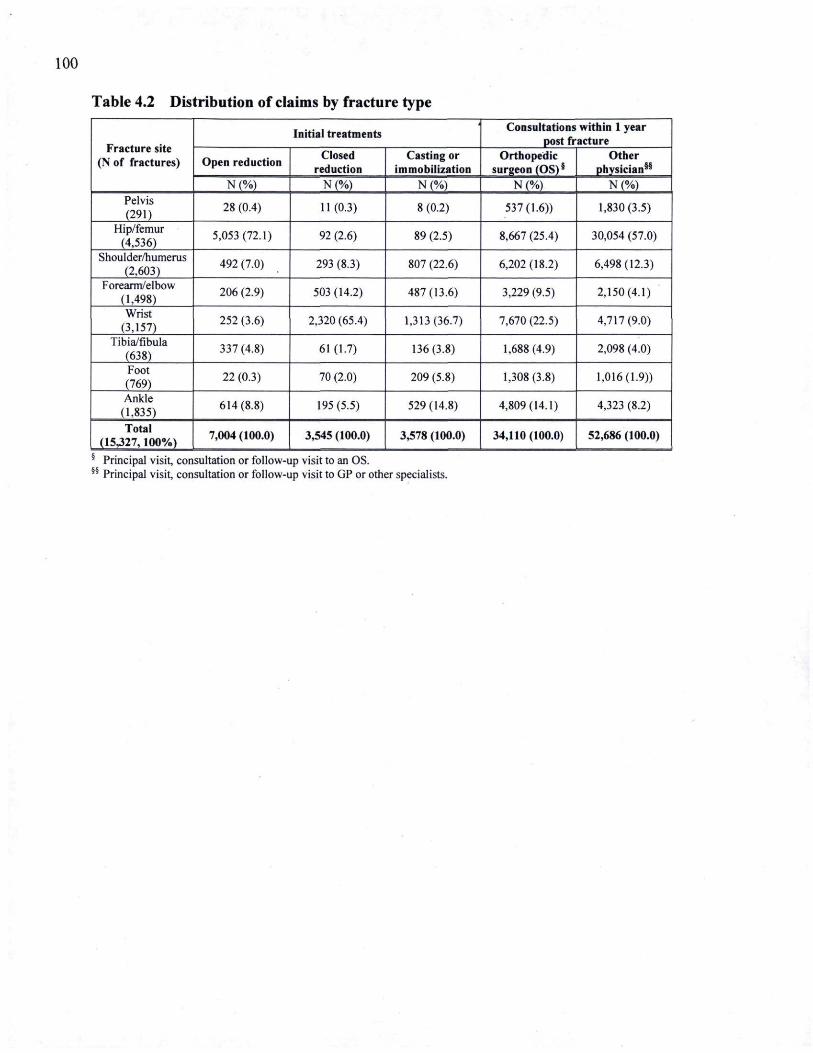
100
Table 4.2 Distribution of claims by fracture type
Fracture site (N of fractures)
Initial treatments Consultations within 1 year post fracture Fracture site
(N of fractures) Open reduction Closed reduction
Casting or immobilization
Orthopedic surgeon (OS)§
Other physician85
Fracture site (N of fractures)
N (%) N (%) N (%) N (%) N (%) Pelvis (291) 28 (0.4) 11(0.3) 8 (0.2) 537(1.6)) 1,830(3.5)
Hip/femur (4,536) 5,053(72.1) 92 (2.6) 89 (2.5) 8,667 (25.4) 30,054 (57.0)
Shoulder/humerus (2,603) 492 (7.0) 293 (8.3) 807 (22.6) 6,202(18.2) 6,498(12.3)
Forearm/elbow (1,498) 206 (2.9) 503 (14.2) 487(13.6) 3,229 (9.5) 2,150(4.1)
Wrist (3,157) 252 (3.6) 2,320 (65.4) 1,313(36.7) 7,670 (22.5) 4,717(9.0)
Tibia/fibula (638) 337 (4.8) 61 (1.7) 136(3.8) 1,688(4.9) 2,098 (4.0)
Foot (769) 22 (0.3) 70 (2.0) 209 (5.8) 1,308(3.8) 1,016(1.9))
Ankle (1,835) 614(8.8) 195 (5.5) 529(14.8) 4,809(14.1) 4,323 (8.2)
Total (15-327,100%) 7,004 (100.0) 3,545 (100.0) 3,578 (100.0) 34,110(100.0) 52,686 (100.0)
§ Principal visit, consultation or follow-§§ Principal visit, consultation or follow-
up visit to -an OS. up visit to GP or other specialists.
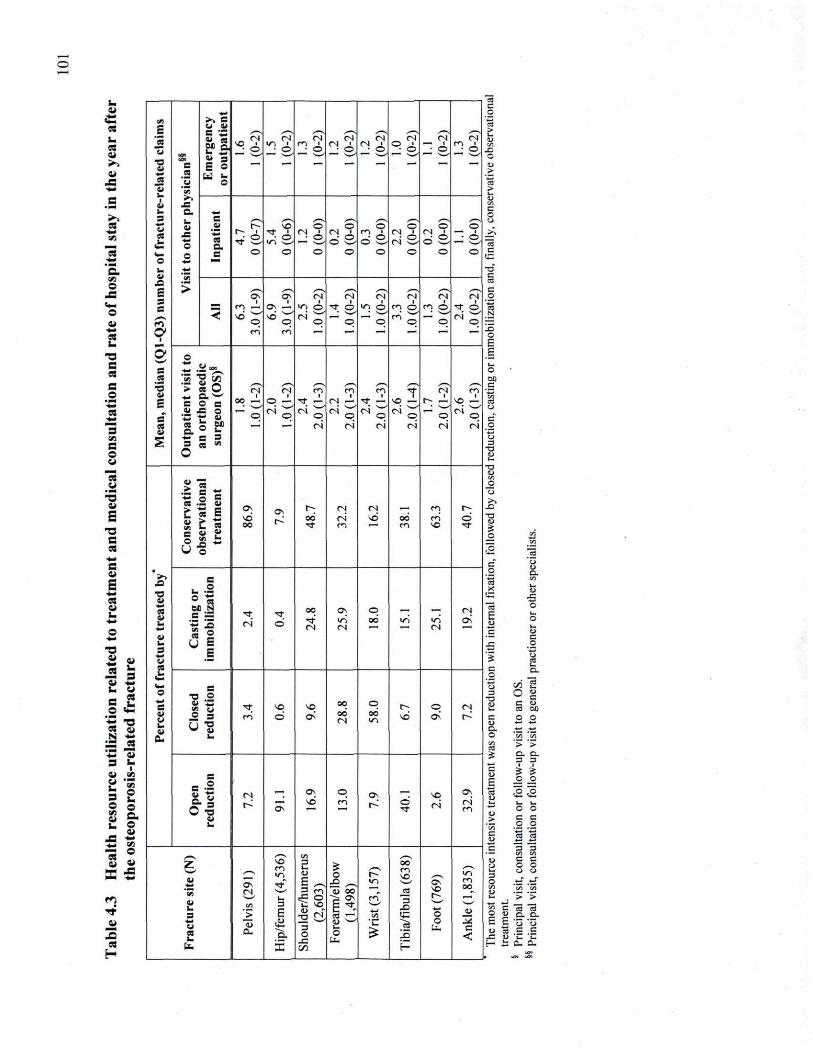
u i i •— ç <s «n 4>> B
_: ZJ
« m. C5 i i >>
J is ■a
B ' ^ a es gg S E o
_ <N (N M <N . r j _ Cr N r j _:
ZJ
« m. C5 i i >>
J is ■a
C0O
B
B ' ^ a es gg S E o
^ O ^ © " ■ é * *6 ^ 6 = ! o • O " ■ 6 V. SJ o u > 3
i i 1\W\ '3 u ë
V. SJ o u > 3
mm "S S
"S S
t i 4S V, c o >, u
3 a. l a
mm B
V, c o
« •mm C i
a. l a V r~ SO O o o o o _ o
fc•mm C i _=
■fc
O
r~ i r f ' ( N i <N " m i r j ■ (N ■ _>. VJ _= ■fc
O a. ^ a v j S , _: ° © s d S ■ o d S • o ~s
"3 •mm
<— o
o B o O o o o o o o c c
C fa C i
_o £ 3 B
>
T_
§ V J O
S
fa C i
_o £ 3 B
> Os » <N <N r j es t s n
T_
§
■ ■ *
fa C i
_o £ 3 B
™ e n —• as J . VJ o r f o v , o en o m O j r f 6 1 o
fa C i
_o £ 3 B
< ___.* ""^ 1 < *o sd '.r' CS ^ c*. CNI i i m p P p O p p p o ~
fc o c . r*. C
i . E
s O s
. 2
o
'S "S ^
| IM O
s ■5 S i
£
• •__ Ci *. ■> es O *. c _
w
B O S
<N i
oo — (N
O ^ ■
r f —.
m i
r j — r f 1 r f
i so —
n ■
r» —. 1 1
fc
■5 S i
£
• •__ Ci *. ■> es O *. c _
w
B O S • s^s • ^^ o C5
■mm G 41 JS O
•■C t _ u
S.» £ *~ p H
P ^ P ™ p N' o ™ o ""' p M
' q c
S es
41 JS O
•■C t _ u
S.» £ — ~* r i r i r i r i r i r i _o
«1 e o
S ■fc C 3 3 CS »
O
o =
T3
u m* a m*
a _>
1 1 1 1 u ■o
E 3 S
e es . s u Z « E I If
Os Os t : ad
r j r i
n sd 0 0
<rj d a
u
e
3 S e
es . s u Z « E I If SO
Os t :
r f m m SO r f a u
_i
«
3 S e
es . s u Z « E I If
S "i ■ *
•3 ■u a. cfl 1 4
B ■s
c a E
« c •3 ■u a. cfl 1 4
B ■s
c a E
« B
, o
c •3 ■u a. cfl 1 4
B ■s
* « ■a o | C
•3 ■u a. cfl 1 4
B ■s
a u
•fc* o
■ f c
cs S __ V fa
B '—
if r f r i
r f O
oo r f ( N
O s v j n
p oc <ri >ri
n
n Os
"3 Ë 3 _g _=
c _. o
c ■o i i
■mm E S
3 mm U SS
B '—
if 5 c
1 _a.
■o i i
■mm E S
3 mm U SS
5 c
1 _a.
•
s o
•** a «
•r
<— o
•m* S
B •s .2 2 o r f SO SO 0 0 p
t ^ o r j
3
î_
O | c u •s oe
°5 X I SJ
C Ci
_2 3 CJ "S
en o Os 0 0 n
oo d OS r^ C
c o o
1 fc* 2
a. fa c ■y, a
'_: !^ ' > ' > o. a. •mm
fc* 2
a. c ■y, a
'_: !^ ' > ' > o. a.
3 u =3 3 1 1
i i i i _. S O VJ i i
i VJ
'VJ O U o a
il J r 3 0 o
S
r j l Os p Os
„ SO as
c u E a J J
_o _o i i i i _. S O VJ i i
i VJ
'VJ O U o a
il J r 3 0 o
S
r~: Os
1 d rn t^ d r f
r i r i m _.
> ■— u . O O c c
m . o c v. .2 .2 _C ■mm a s s •fc«« i i
X
V J
O O
c ■ f c *
u ;_ 3 O 'Si ZJ
•fc«« i i
X
V J
O O
c ■ f c *
z v
■fc
' v i a u 3
Os ( N
SO m V J
VJ 3 C IU
E ^ 2 f>
o O ^ "û oo
0 0 en so
JS oT S O
V J m 00
u ;_ 3 O 'Si ZJ
3 3 _. crt C C o o o o
.ti . t f ' ^ "_5
r r
z v
■fc
' v i a u 3
E «5 ° C so 1> m J 3 O
JS t /5
VJ
3 r
o u t . o E u ^:
. •> > s "3 *3 H a. a. _2
_â U es _. a.
X
«5 ° C so 1> m J 3 O
JS t /5
o o
tu _i B
<
t . o E u ^:
S '5 û o .S .s u C C i : a. o.
102
For pelvic fractures, Tables 4.2 and 4.3 demonstrate that 2.4% of all claims were related to
their treatment and 86.9% received conservative treatment (follow-up visit to an OS only).
Despite the low rate of pelvic fractures treated by surgery (7.2%), they required a high rate
of hospitalization (67.4%, Table 4.4), likely related to older age. Thus, these fractures also
accounted for a significant proportion of medical consultations with an average number of
1.8 outpatient visits to an OS and 4.7 and 1.6 inpatient and emergency/outpatient visits to
other physicians, respectively (Table 4.3).
Non-hip and non-pelvic fractures accounted for a large proportion of medical consultations.
Table 4.3 illustrates that several non-hip fractures had a high rate of clinical care related to
surgery (tibia/fibula 40.1%, ankle 32.9%, shoulder/humerus 16.9%, forearm/elbow 13%,
wrist 7.9, and foot 2.6%), requiring a total of 27.4% (open reduction). Forearm/elbow and
wrist fractures had the highest rate of closed reduction (28.8% and 58.0%, respectively),
which always involved an OS for the procedure. These fractures required a significant
proportion of medical consultations, representing 74.6% of all consultations with an OS
and 43.0% of all consultations with other physicians (Table 4.2). As with hip fractures,
when other fractures were treated by surgery, the hospitalization rate was high, varying
between 90% for foot and 99% for wrist fractures (data not included). The average number
of outpatient visits to an OS was approximately 2 similar to that observed for hip/femur and
pelvis fractures. Moreover, the average number of visits to other physicians varied between
3.3 (tibia/fibula) and 1.3 (foot) and were correlated with the rate of surgeries, due to the
average number of inpatient visits. Therefore, the mean number of claims (Table 4.3) to
treat these fractures was highly correlated with the proportion of fractures treated by
surgery, thus requiring hospitalization.
Table 4.4 details health resource utilization for hospitalization in the year after fracture. As
expected, the highest hospitalization rate was attributed to hip/femur fractures, with 95.4%
of these fractures having at least one hospitalization related to their care. In terms of LOH,
these fractures also had the highest resource utilization rate with a mean (median) LOH of
39.2 days (31 days), representing 73.2% of total LOH related to all fracture care. In
addition, a significant proportion of hip/femur fractures (46.2%) required at least one re-
admission to another hospital within 1 day. Mean (median) LOS of 18.4 days (11 days) for
103
initial hospital admission and mean (median) total LOS was 45.1 days (38 days) for all re-
admissions. Finally, 8.1% of all hospitalization for hip/femur fractures corresponded to re-
hospitalization (rehabilitation or complications) and LOH for these re-hospitalizations was
shorter in duration than the first hospitalization.
Pelvic fractures carried a high rate of medical resource use related to hospitalization, with
67.4% requiring at least 1 hospitalization for their treatment. Mean (median) LOH was 34.2
days (26 days) and 40.6% of these hospitalizations involved at least 1 readmission to
another hospital within 1 day. Mean LOS at initial hospital admission was shorter than for
all readmissions. Mean (median) LOS at initial hospital admission was 18.9 days (13 days)
and mean (median) LOS for all re-admissions was 38.9 days (29 days). Globally, 5.3% of
all hospitalizations related to pelvic fractures were re-hospitalizations.
Non-hip and non-pelvic fractures (so-called peripheral fractures) accounted for a significant
proportion of medical resources used for hospitalization, with 54.2% of tibia/fibula, 41.7%
of ankle, 33.3% of wrist and 30.7% of shoulder/humerus fractures needing at least 1
hospitalization for fracture care. Although somewhat shorter than for hip and pelvic
fractures, mean (median) LOH at these sites was still considerable, with 26.3 days (9 days)
for tibia/fibula, 16.6 days (3 days) for ankle, 8.0 days (1 day) for wrist and 23.5 days (8
days) for shoulder/humerus fractures. Moreover, the rate of these fractures requiring at least
1 re-admission to another hospital within 1 day varied between 12.1% and 29.4%. As with
hip/femur and pelvic fractures, mean LOS at initial admission was shorter than for all re-
admissions. Altogether, non-hip fractures involved 26.8% of total LOS for fracture care.
For all fractures, we observed that a large proportion (between 92% hip/femur and 100%
foot) of all procedural intervention codes related to their treatment (reduction, fixation, etc.)
were assigned during initial hospital admission (data not included). This observation
confirms that initial admissions correspond to the acute period of fracture care. Moreover,
as described above, the high proportion of fractures requiring re-admission to another
hospital within 1 day of a previous admission suggests that after initial admission (acute
care period), a significant proportion of fracture patients remain hospitalized to receive
other care (inpatient rehabilitation).
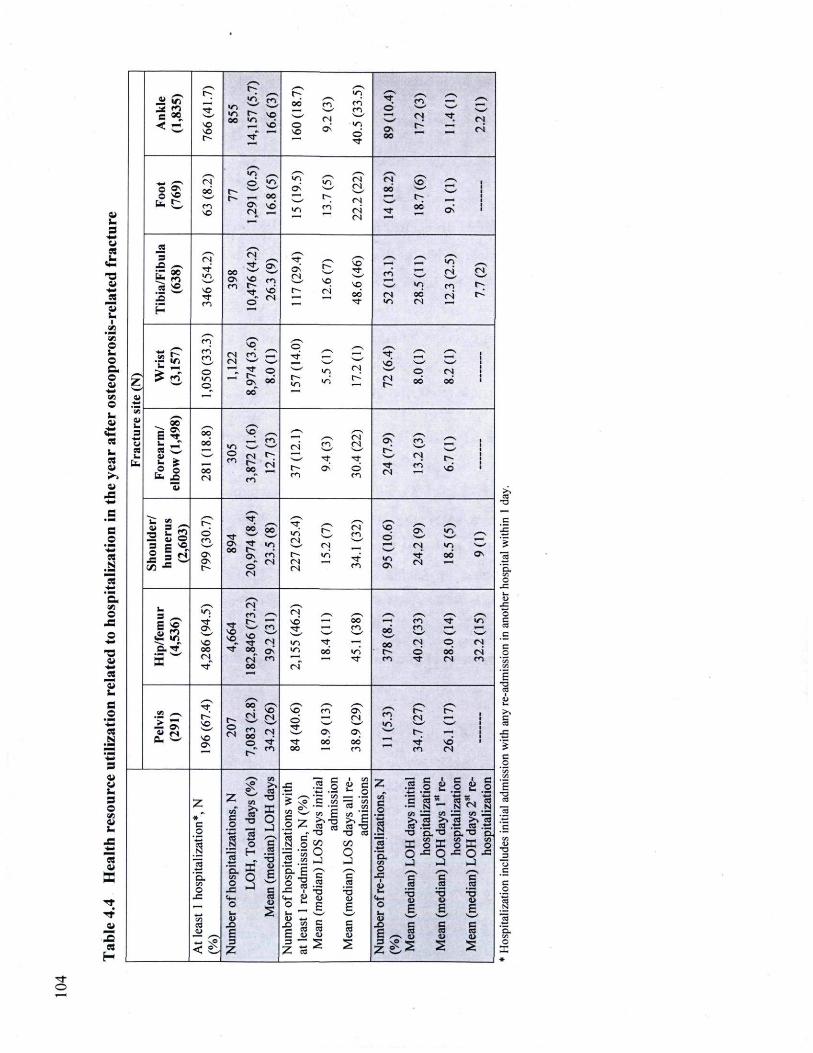
i i U 3
fcU
> <#m
x i i
•mm
_s _. o fa o c o
fcVj O o
4 .
JS
G O
• ■_
■mm
03 | "3 • — C c« O
x a
a im e O
'■mm
.a
E 3 O
I 1
y—N •r-.
.__ en r f V J r-
S S
en O O •ro en en
y—N
r * ©
s s en
• s ._^ s s s~~S
B • = s _ ^ V J
0 0 r-
sq •*—• n — 4 ^ - ^ ci r f rs < c S O
S O r f
sd © S O o-
© r f
Os 00
r- ~ r i
y*"N
-,__ ^ s ^T © S S
V J y—s V , n Cs) s s
SO s s
s s. 0 0 t^. * ^ as n 00 ■> ■* 2*
te. «^ en S O
t~ Os <N
O O
sd V J
t»; r j ri n r f 0 0 Os
_9 S S
s - B —
rT r f V J 00
Os
n r r S O
• w -
en
rf" OS
y—s
S O
r£ ro y—S
V J
ri (N
a » m r-~ sq ^ m t-; a » sO r f en
r f © "
d r j •f» ri oo
r f n V J
O O
n r i l ~
H " ^^
Z •2 £
en en m © V J ©^
r j
S S
sq ci r f f-
00
s s s_* p O C
p r f S_*4
i n
V J
i d r j
r f SO s — '
r j
s s
p oo'
s s
r j 00
■ —
Vi Vi
C i
fa 3
■ w C i es fa te.
Fo
rearm
/ el
bo
w (1
,498)
0 0
0 0
oo n
© c».
s s sq •—' (N r-°°„ en
S S
m r-~ r i
y — \
r i
r~-en
en s—' r f <_s
rT n r f © en
/— Os
r f r j
en
ci
s s
t s sd
C i
fa 3
■ w C i es fa te.
"£_,___ •-SS u ©
r^ © ' en r f
r? 00 r f r-Os © "
/ — s 0 0
r ? «d r j
y—V
t - en ©
s s OS /—
Os Os
-Os oo
r? 00 r f r-Os © "
V J
en n r j
r j
Csj v j r f
en V J Os
es r f n
"1 oo
s — s
Os
n ^
S S r j S S
3 __, V J en S S r j
B $ r f r f •r--
fcH d — oo • ■H en r f V J
B $ Os r f m r f m 0 0
0 0
en *—i T —
«2 in S O
S O S O S O
r f r j r f ^—y 0 0
0 0 tN © r j ~a.rf oo r f 0 0 ^ Os >/-. 0 0 vj
0 0
0 0 © oo r i
a n n" m —-' — r f r». r f n en a r f 0 0 r t
s s r ? 0 0 y — s r—^ s s / - ^ s
59 , I ~ I . r ? S O sq tn O S •fl •d
t~- t~
l a 0- ^
SO
SO Os
© <N
n en 00 ©_
n (N r f
© r f ,
r f
* . 0 0
r j
OS oo
•fl •d
(N
r-r f sd
SO
SO Os
r-" en 0 0 en en r j
s s O S
VJ
i .2 g I VJ
î_ c
fa o Z II s J è |
s VJ S o
en
i T3 ΠO
'43 Ci E §
§ 2
"g % S ce
*3 s_ co ' e >. E CO T 3
J I 1
1 1 - B VJ 'JS > , cfl « .-s
CA ^ Z > . (0 « -B
o 3 1 i
o
T3 ΠO
'43 Ci E §
te rf N O
T3 eo 00
J I 1
T3 D . ■T-I SG "o a "o a
'E. VJ O
J S
■mm VJ
H 'ô.
VJ O
J S <mm
O fa o
H ac o
T3 ΠO
'43 Ci E §
1 S o. Ê
1 « «- __ fa * 1 ) * -
O J / — s
C ra CJ
E -—'
O .—v B CO
■5 C i
E
'S. VJ o
J S 1
O fa
î •5
CJ
Ë
O * - J
E
B es
'■5 Ci B
eo C i
— S S Ë *5 S c_ ™
C Cs3
B (8 O
^ 2
B /*** mm N = 3 3 —
S _> 3 S P S 2 s
!£ '0 S 'E. _: C
E a a
M «r» ___ !H
S
105
Table 4.5 provides details of discharge destination for the last hospitalization for fracture
care in the year after fracture. Among all fracture patients with at least 1 hospitalization for
fracture care (N=7,787), 5.2% (N=407) were LTC residents at initial admission. Ninety
percent of these LTC residents had hip/femur fractures. Among these LTC residents, 91%
returned to LTC at last hospitalization and 6% died. Among non-LTC residents at initial
admission, only 44.8% of hospitalized patients for hip/femur fracture returned home, 25.6%
required rehabilitation or were referred to their CLSC, 18.2% needed LTC and 10.8% died
during hospitalization. Therefore, hip/femur fractures consistently utilized a significant
proportion of health resources after hospitalization.
Similarly, non-LTC residents hospitalized for pelvic fractures required a significant portion
of medical resources after discharge, with only 53.9% returning home, 25.4% needing
rehabilitation or referral to their CLSC, 10.9% admitted to LTC and 9.3% dying during
hospitalization. For other hospitalized peripheral fracture cases, between 10.1% (wrist) and
23.3% (tibia/fibula) required rehabilitation or were referred to their CLSC and between
4.0% (wrist) and 8.1% (foot) were admitted for LTC. Therefore, for peripheral fractures,
medical resource utilization persisted after the last hospitalization.
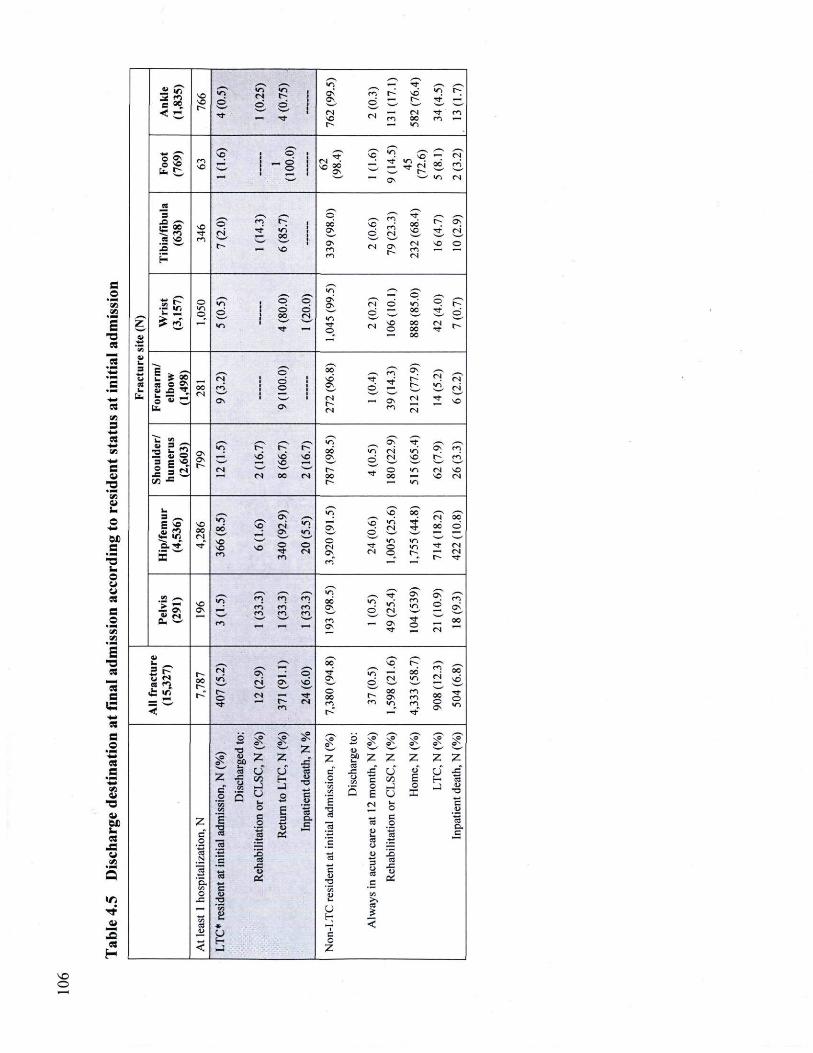
c ' V J VJ
s X
VJ S
■mm «
-fc-VJ
-fc-C i i
X "S
•m.
M B
X fa O w u ss B
%© V l VJ
s X "S B
■ f c -
«5 B
« B 'S VJ i i
X DC i «
S W VJ
r*
« H
_ t . .—. VJ ■ * . v
_S <7T SO SO t - -
d r f
v s n © s s
VJ
o O s
5s r j
.—. r o ©
f~ SD t -
•—-CN
VJ T f
r f r o
_S <7T d r f
1—« r f SO
.—. r o ©
r o 0 0 CO « t-~ — irs
o < *
te. £,
y - 1 * .
s q S* Ç" S" VJ se" ^ CN
o < *
te. £, r o SO v ^ y
_ . © © Ov
mm r t 9 Ë 0 0 r o
w • ' ~ Cs irv CN
es 3 CT e o
r o (N
Os
r f
£oo S : i n es s o
SO r f
Ô
ci r -
r o r f «d
0 0
s o
00 Os
Os r o
SO ©
CS
e o r o (N
Os
0 0 SO
CN ■ro
f"; r f
Os ÇN
O
H r o
e o r o (N
Os CN
^^ «n . — ■
" E © S - . VS CT CT Os
Os
VJ f CT
CN d © v j S" P
g VJ © K
©
VJ
CT 0 0 r f
CT r s s_^
Os Os
VJ f CT
O
fN sO o
0 0
o c 0 0
r j ^
CN r t
©
mm 0 0
__■
3 fa * 25 8 o » a - O r f
_, S" 00 m C_v (N v j
r . 03
fa * 25 8 o » a - O r f 0 0
r j
es» c d
CT CT
d o s
r f O
r f t-4^ ■ r -
(N v j
CN r i 03
te.
0 0 r j
O s C3S
( S
( S — Os
r o CN
CN
r t sO
■O fa 2
^ ^ ^
■O fa 2 y ^ VI Os r f
■O fa 2 Os Os •r-
VJ • t - t - t ~ 00 VJ CN v j Ov r o _XS Ci o Os
Os •r-
s d s d s d Os O
r r
CN SO •r> r o 3 C sO
J ici Os Os •r- n w s o mm
•r-O
r r O VJ CN SO 3 C sO
J ici ( N 0 0 f S oo
O
r r OC iO CN
1/3 ■= r» —— V i
^ ^ ^
' s ? SO 0 0
v s o o G"
S*s O s v s
v j
VJ
O s ©
sO v j CN
o c r t
CN
30 0 0 d
fa- V i n w s o s o CT VJ VS
~ Q . r f r f s o s o SO CT CT e s r f O v j r t CN
S w s o s o SO
r f r o
e s Os CN © e~_ r -
CN r t
ro" "" ""
^ S—s
l a SO a s
s s VJ
r o
y—N
r o r ô r o
r o r o ' r o
e o e o r o
VJ 00 Os
e o OS
O
r? CN
Os r f
S : r o TS
r t O
S : d
CN
r o ■OS
0 0
o *- __ -2 P ea fO
•r-0 0
y—N
n S~V Os e s O s
CT* s d
0 0 r f Os
v j ©
SC
CN 00 VJ
r o CN
0 0
r - " o r f
e s f s e n
r * e s
O 0 0 r o r o
OC Os " 1
m m r o rf"
00 o OS
r f O
^^ ^^ _S ^ ^ O
S g, _S
CS* o s ? S s ?
o x
s s T 3 Z j _ r
—' •_> s s T 3
z Z Z j _ r z i z Z Z z z
* -s B .2
.2 Q H9
U ci s « cd C J S J S u u o J S
* -s B .2
.2 Q H9
V J H O c j • ~ CA
S t/5 E H a * -s B .2
.2 Q H9
J _5 O c j
• ~ CA O J o _ J ZJ * -s B .2
.2 Q H9
u fa
2 c .H
.22 Q E
E CN fa
X c
Z " o
B E 3
■s o . B
r _ ca
5 13 o c o
ZJ
o . c o
'-5 3 ta oi
'S ZJ fa C3 CJ
"cd c
cd
3 ■B ' S 1 CC
c CJ
3 u cd
Ï 0>
'E es fc* ai <u
T3
CJ
3 u cd
â w C VI
o u CJ ■si J S ."2 >v — *33
fa U cd 5
i » J < « O c __ H o < - J Z
O
107
Figure 4.2 discloses that the proportion of surgery increased significantly with age while
less invasive (immobilization and conservative treatment) treatments decreased. In contrast
to hip/femur fractures, pelvic and tibia/fibula fractures were associated with a significant
increment in the proportion of conservative treatment with age and a significant decline in
the proportion of surgery (open reduction) and immobilization. For upper limb fractures,
the proportion of closed reductions increased greatly and significantly with age, while other
types of treatment decreased or remained stable. For all fractures, Figure 4.3 shows that the
average number of visits to an OS fell slightly with age while the average number of visits
to other physicians, the proportion requiring hospitalization and LOS increased
significantly with age. Finally, Figure 4.4 denotes that during the last hospitalization for
fracture care, the proportion of patients discharged to their home decreased significantly
with age while the proportion of patients admitted for LTC or who died increased
significantly with age. Therefore, patient age at the time of fracture is an important
determinant of health resources utilization, and is associated with increased admission for
LTC and death.
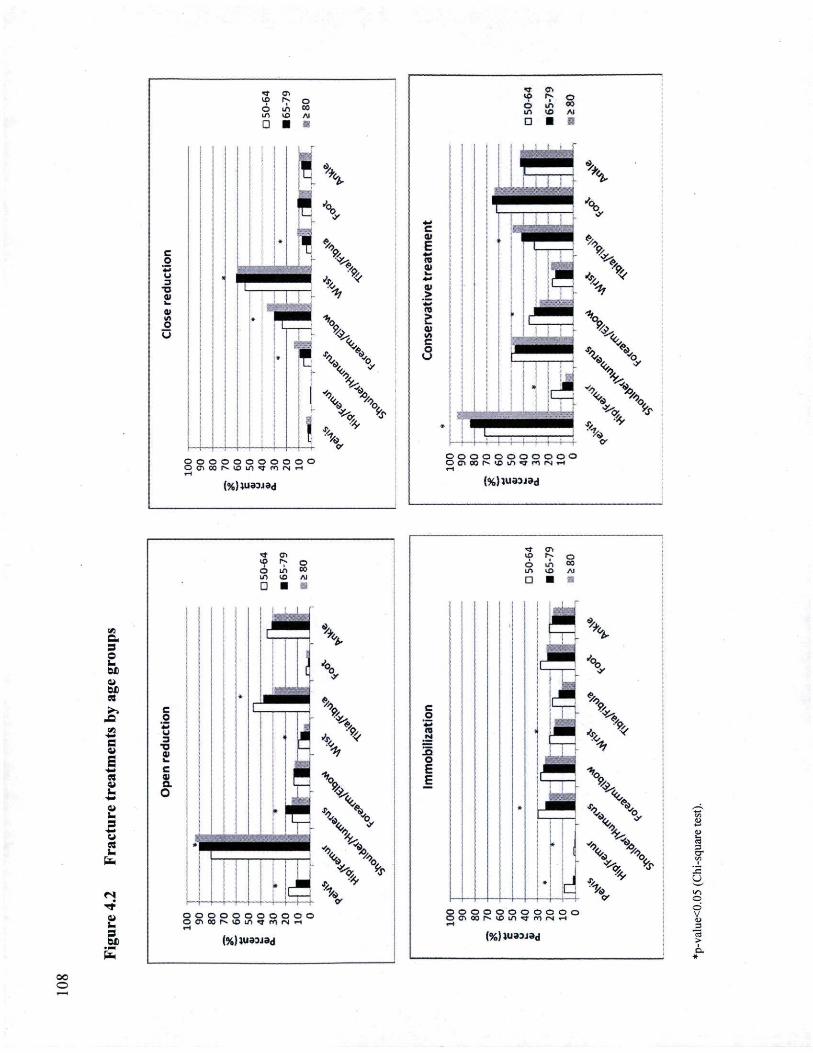
lu 6 VJ
a
7 o U3 Al ■ ■
C o
'+m U 3 T3
<U
o u
j i
* |
\
\
%
X \ \
o o o o o o o o o o o OcT.cor^iOi/'irJ'fOiN.-i H
(%)Wi33ja<l
lu t
m so
O oo Al
C 0) E •*ro
Oi
> ro 0)
c 6
© o o o o o o o o o o ©•ssoor^sDi / s r r rOfN-^- i
{%)lU33i3d
su
a
OS
SO
■
O CO A l
:.:
VJ C. 3 O _. DC
DC es
B
E ■ f c
« .
fa> i i U
m. Um
• r f i i U 3 DC
C O *5 u 3
■a « fa c « a O
o o o o o o o o o o o o e n o M o u i ^ m r M r t
(%}}U83J3d
•q
6 m
CS o oo Al
C O
-Q O
d O o o o o o o o o o o CNOOf'-^un^'mrNr-i
(%)»ua3jad
CT I I
oc o
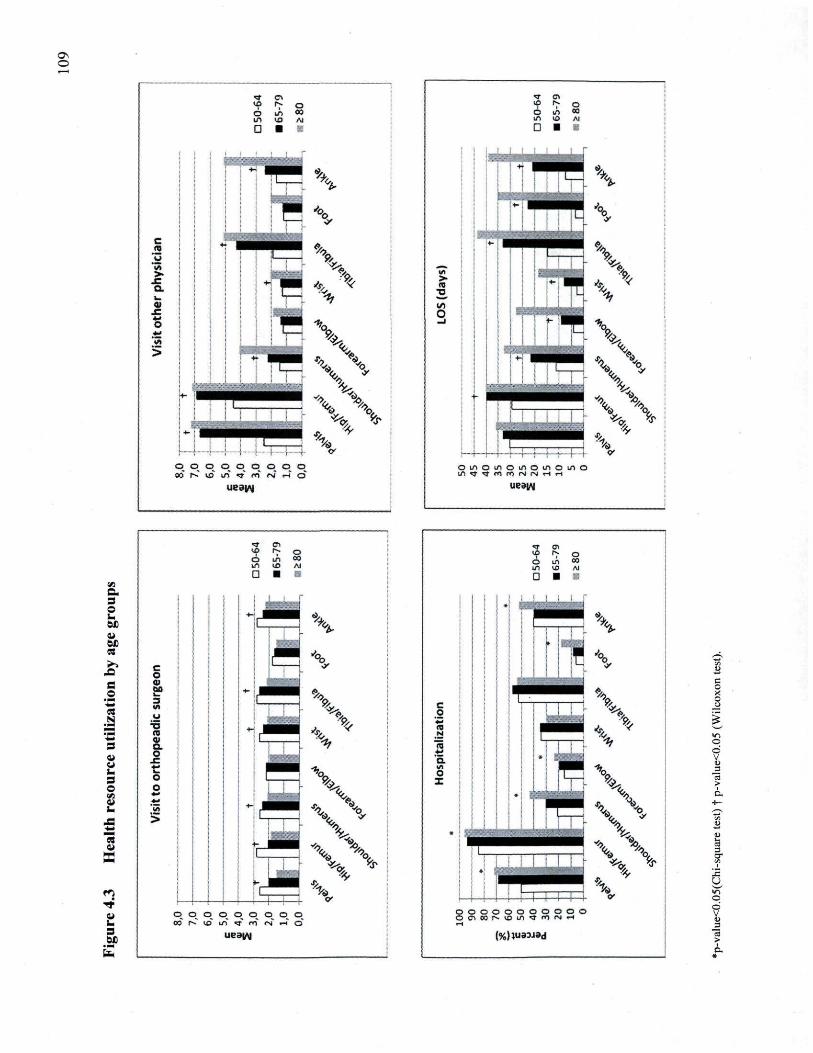
Os O
■a- cr, so I S O o us 00 US «3 Al
0 ■
C ro
'v> >
j e Q. fa <U
C
v ,
>
p o o^ p p p p p o oo |s io «n «t en r«î «J o '
ueaiAj
o
> ._. O
+j
t
\
^
O t / i O i n O i f i O i n O i f l O
uesw
VJ
a 3 O u DC U DC « >> c
O B O
01 00
■*■> W)
.a TÏ ♦ 01 3 CL
W O _c t .
3 o O o en U mm b V>
4S > ■fc
3 v a r i r t U fa 3 DC
O OO
p p p oo r * UJ
o . o_ o^ o^ o o^ l/l" T ro IN H d
o 00 Al
c o
o I
o d V
o o o o o o o o o o o O C S O o r ^ v O i / l ^ f O r v l i H
(%)»U33J3d
U
o d V
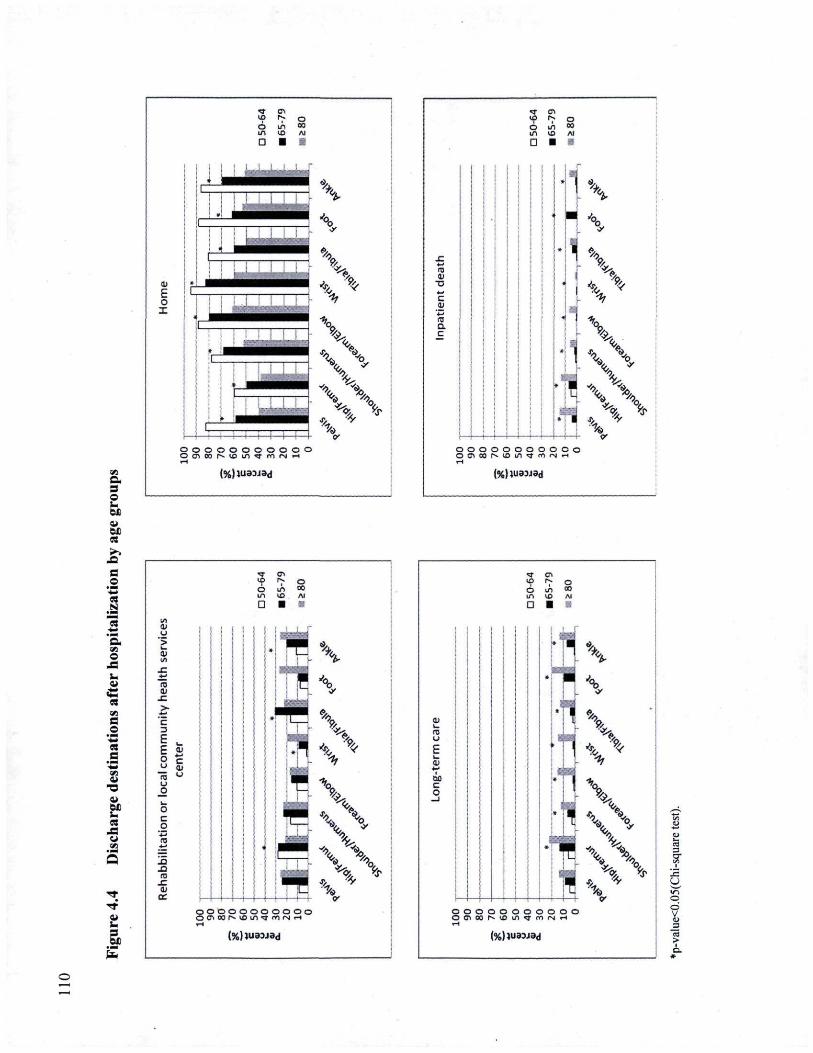
v-y «7 o o vj °o LO I O A l
D ■ ii
ai E O X
o o o o o o o o o o o O O S O O M O l f l l t m i N H
VJ c 3 o I OJ DC «s ■ > >
.-Q B O
• ■_• ■fai
| "es ■ f c
'S. VJ o
ss I » B o
"S es s
°S n o>
X a DC U CS
-S i i VJ
r t r t i i C 3 DC
u
"5
ra OJ
C
C
u s! O C O
J2 J_t ro
JZ d) ce
(%)VJ33JBd
O _i
O co Al ■
ra m
T3 44 c S
ra a c
%
V
X Cj\\
'
V \ \
o o cv 00
o o o o o o o o I f i Cf CT) IN rl
(%)}U3_J3d
1 <n T 7 9 O u. °o in vo Ai
D ■ s
O O O O O O O O O O O O C i c o M O i n ^ r c n i s i H
(%)}U33J3d
O oo
10
■
ro u
60 C O
—1
1 ^rÉ
!
1 I 1"
i m ïtaj
. ■
I ÉÉ
X9* % s .
X
\ O O O O O O O O O O O O O O O M O U l ^ m i N H
J= CJ VJ o d
i (%)}U33_3d
I l l
4.6 Discussion With health administrative databases, we assessed direct medical resource utilization for
fracture treatments, physician consultations and hospitalizations in the year after fragility
fracture. As expected, hip/femur fractures represented the highest resource utilization rate
since the majority of them required surgery and hospitalization. However, other peripheral
fractures accounted for the significant use of clinical care related to surgeries, OS
consultations and hospitalizations. Even with pelvic fractures, which often do not require
surgical treatment, the resource utilization rate was elevated due to the high hospitalization
rate. This study indicated that patient age was an important determinant of health resource
utilization, associated an increased number of visits to other physicians, hospitalizations,
LOH, admissions to LTC and death.
Few investigations provide detailed estimates of health resource utilization for fragility
fracture care and most focus on hip fractures. Any attempt to compare these studies is
limited by differences in healthcare systems, populations, time periods studied, and type of
data sources for estimating health service utilisation.
In our study, the number of physician visits for fracture care was higher for hip and pelvic
fractures compared to other peripheral fractures. This observation is related to the higher
hospitalization rate associated with hip and pelvic fractures, which result in more inpatient
physician visits. A study of MedicAid data (USA) reported approximately 7 outpatient
physician visits in 6 months post-fracture, a number that was constant across different
fracture sites [200]. In the year after fracture, a Canadian study disclosed an average of 4
general practitioner visits and 1 specialist visit for patients residing in the community.
General practitioner visits averaged 7 for patients transferred to LTC [73]. However, unlike
our investigation, which considered only physician visits directly related to fracture care,
the 2 cited studies analized all physician visits in the year after fracture.
Results on the health services burden related to hospitalization in our investigation are
similar in several aspects to those reported previously. First, for each fracture site, a
significant proportion of patients had at least 1 acute hospitalization for fracture care in the
year after fracture and the magnitude of these hospitalizations varied by fracture site. The
112
proportion of patients with at least 1 hospitalization for fracture care ranged from 8.2% for
foot fractures to 94.5% for hip/femur fractures. As suggested by Becker et al. [200], these
variations between fracture sites reflect differences in fracture severity. Second, in this
study, the majority of procedural intervention codes for fracture repair during
hospitalization were assigned during initial admission. This observation indicates that a
greater proportion of initial admissions corresponded to the acute care period. Moreover,
the mean (median) LOS of 18.4 (11) days observed for hip/femur fractures at initial
admission was similar to the mean acute care LOS of 16.7 days recorded in 2005 by Med-
Echo hospital discharge database in a Level I trauma center in Quebec, Canada [201].
Thirdly, it was previously reported that a large proportion of patients hospitalized for
fracture treatment also received inpatient post-acute fracture care [70, 200]. After initial
admission, a large proportion of the fracture cases were transferred admission to another
hospital, suggesting that a significant proportion of post-acute fracture care obtained
rehabilitation and/or chronic care provided by another hospital. This observation is
consistent with the Canadian context where post-fracture rehabilitation is considered to be
an extension of acute care, whereas discharge to LTC occurs when patients fail to be
autonomous [70]. For LTC residents at the time of fracture, their place of residence
remained largely unchanged among survivors, as reported previously[70]. Moreover,
among non-LTC residents, our descriptive analysis of discharge destination after final
hospital admission indicated that a large proportion of fracture patients received post-acute
care services through LTC, rehabilitation care or were referred to their CLSC pointing to an
important role of these services in fracture care. In this study, we observed that 18.2% of
non-LTC patients with hip/femur fractures were transferred to LTC at last hospitalization
for fracture care. Another Canadian study reported that 16.6% of community patients with
hip fracture were admitted to LTC at hospital discharge [14].
A Swiss study, comparing the total number of hospitalization days for osteoporosis and
fragility fractures to those observed for other chronic diseases, reported that osteoporosis in
women accounted for 1.5 times more hospital days than cardiovascular diseases, between 2
and 3 times more than chronic obstructive pulmonary disease and breast cancer, and 6
times more than diabetes [133]. Moreover, in addition to the burden on health resources,
the treatment of these osteoporosis-related fractures represents an economic burden to the
113
healthcare system. Taking the same methodological approach, our earlier work estimated
the average cost of treating acute fractures and post-fracture complications in the year after
fracture to be $46,664 CND per hip/femur fracture, $5,253 for wrist fracture and $10,410
for other peripheral fracture sites [198].
Major strengths of our study were the use of population-based administrative databases,
providing global measurement of healthcare delivery at the population level and access to a
large sample of fracture cases included for each fracture site, allowing a robust estimation.
Moreover, in selecting only medical claims and hospitalizations for fracture care, medical
resource utilization directly attributable to fracture care and representing actual care was
assessed. Secondly, a validated algorithm identified inpatient and outpatient fracture cases,
thereby achieving a better understanding of the true burden related to fragility fractures,
especially those not leading to hospitalization. Moreover, the ability to link the information
on each fracture case from several databases allowed the assessment of fracture impact on
health resource utilization across a continuum of clinical care.
This study had some limitations. First, we had no procedure for eliminating fractures
related to motor vehicle accidents or malignancies. It has been reported that the rate of
motor vehicle accident- and malignancy-related fractures is low. Moreover, the ROCQ
Study, in a subset of the population included in these analyses, indicated that the majority
of fractures (81%) occurring at an osteoporotic site were low-energy trauma fractures [4].
Second, vertebral fractures were not considered in this investigation because of our
inability to properly identify vertebral fractures in administrative databases. This limitation
is not unusual, as approximately two-thirds of vertebral fractures do not come to clinical
attention [139, 192, 193]. Furthermore, our investigation only included women from three
health regions that represented 42% of the female population Quebec province. It is
possible that fractures and direct medical resource utilization differ in other regions in
terms of the socio-economic and regional aspects of medical care. Administrative data
analysis cannot eliminate coding omissions or coding errors. Lack of information regarding
transitions to LTC after the final discharge destination and treatment by home-based
healthcare workers, physical or occupational therapists could also have influenced our
results.
114
This study has implications for health service administrators responsible for coordinating
and prioritizing healthcare delivery. Characterizing the healthcare resource utilization
burden related to fragility fractures is a first step towards better understanding the
determinants of fracture care. This information is essential for resource planning and
organization of healthcare services and may also help to maintain and increase the
efficiency of fracture care.
However, although the burden of osteoporosis-related fractures is high in terms of excess
mortality [10, 76], levels of healthcare used [200], institutionalization [70] and their
associated costs [198], under-recognition of osteoporosis and its consequence remains
problematic [4], despite availability of effective therapy to lower fracture risk. Therefore,
effective public health interventions need to be introduced to improve the diagnosis and
treatment of osteoporosis, particularly in high-risk groups (i.e. those with fragility fracture)
to reduce their impact on the healthcare system.
4.7 Acknowledgments This research part of the Recognizing Osteoporosis and its Consequences in Quebec
(ROCQ) Study, has been made possible through the support of founding partners Merck
Canada, sanofi-aventis Canada Inc, and Warner Chilcott as well as major partner Amgen
Canada Inc. and minor partners Eli Lilly Canada Inc. and Novartis Pharma Canada Inc.
These funding sources had no access to the data prior to publication and no input into
writing ofthe manuscript as well as in the decision to publish the results.
Sonia Jean designed the study, directed its implementation, acquired, analyzed and
interpreted the data, and drafted the manuscript. Bernard Candas contributed to the study
design, helped with its implementation, interpreted the data and drafted the manuscript. All
other authors interpreted the data and reviewed the article critically for intellectual content.
115
Chapitre 5 Conclusions générales et perspectives
117
5.1 Conclusions générales Dans le cadre de ces travaux de doctorat, nous avons d'abord comparé l'exactitude de
plusieurs algorithmes pour identifier les cas incidents de fracture chez les patients de 50 ans
et plus, sur la base des données recueillies dans le fichier des services rémunérés à l'acte de
la RAMQ. L'algorithme que nous avons retenu et validé nous permet de conclure que
l'utilisation des données provenant du fichier de la RAMQ pour identifier les cas incidents
de fracture chez les femmes de 50 ans et plus, et pour effectuer une surveillance continue de
ces fractures est réalisable et raisonnablement précise.
À l'aide de l'algorithme validé, nous avons quantifié l'incidence des fractures de
fragilisation chez les femmes de plus de 50 ans et évalué leurs impacts sur la survie de ces
patientes. Selon nos travaux, les fractures de fragilisation chez les femmes de 50 ans et plus
sont fréquentes et les plus communes sont celles traditionnellement associées à
l'ostéoporose: hanche/fémur, poignet, épaule/humérus et cheville. Notons cependant que
nous n'avons pas inclus dans notre analyse les fractures vertébrales. Nous avons également
observé que les fractures périphériques surviennent fréquemment dès l'âge de 50 ans alors
que les fractures de la hanche/fémur et du bassin sont plutôt rares avant 70 ans, mais leurs
incidences augmentent substantiellement par la suite. Tel qu'attendu, les fractures de la
hanche/fémur et du bassin sont associées à la plus grande perte d'années de vie et l'impact
de ces fractures sur la survie des patientes est particulièrement important durant la première
année mais peut persister plusieurs années après la fracture. Pour les patientes ayant
présenté une fracture de la hanche, nous avons pu identifier certains facteurs ayant un
impact significatif sur la survie de ces patientes; notamment le fait d'être âgée de plus de 80
ans et un délai entre la survenue de la fracture et la chirurgie de plus de 3 jours. Finalement,
selon nos données, certaines fractures périphériques ont également un impact sur la survie
des patientes.
Le jumelage des données provenant du fichier des services médicaux rémunérés à l'acte de
la RAMQ et du fichier des hospitalisations (Med-Echo) des patientes ayant présenté une
fracture identifiée par l'algorithme, nous a permis d'estimer l'utilisation des ressources
médicales directement associées aux traitements des fractures, aux consultations médicales
et aux hospitalisations dans l'année suivant la fracture. Une grande proportion des
118
ressources médicales sont destinées aux fractures de la hanche/fémur qui nécessitent pour la
majorité d'entre elles un traitement chirurgical ainsi qu'une hospitalisation. Bien que les
fractures du bassin requièrent plutôt un traitement conservateur, ces fractures nécessitent
des ressources médicales importantes en raison de l'hospitalisation d'une grande proportion
des patientes présentant une telle fracture. Par ailleurs, en termes de soins cliniques liés aux
traitements chirurgicaux, aux consultations médicales et aux hospitalisations, l'utilisation
des ressources médicales pour les autres fractures périphériques est non négligeable.
Dans cette étude, nous avons identifié certaines limites de la méthodologie que nous avons
utilisée. La principale lacune de nos travaux est liée à l'incapacité de l'algorithme à
identifier adéquatement les fractures vertébrales compte tenu de la sensibilité médiocre de
l'algorithme pour ce site de fracture. D'autres auteurs [139] confirment dans leurs travaux
que les fractures vertébrales sont en général sous-déclarées dans les banques de données
administratives puisque la majorité de ces fractures sont asymptomatiques et reçoivent donc
peu d'attention clinique [144, 145].
D'autre part, dans le cadre de ce travail, aucune procédure n'a été établie pour identifier et
éliminer les fractures traumatiques et pathologiques. Néanmoins, selon une étude récente,
les fractures de fragilisation représentent plus de 81% de l'ensemble des fractures [4]. De
plus, dans les études populationnelles, il a été proposé de ne pas exclure les fractures
traumatiques puisque ces fractures sont également associées à une diminution de la DMO et
augmentent le risque de subir une fracture subséquente [33]. De façon similaire, il est
recommandé de ne pas exclure les fractures pathologiques puisqu'elles représentent une
très faible proportion de l'ensemble des fractures et leur exclusion peut conduire à une
sous-estimation du fardeau associé aux fractures ostéoporotiques [34]. Le manque
d'information sur les facteurs de risque clinique et la possibilité d'erreurs de codage sont
également des limites inhérentes à l'utilisation des banques de données administratives.
Finalement, les autorisations obtenues par la CAI pour la réalisation de ce projet de
recherche limitaient l'accessibilité des données administratives uniquement aux services
médicaux liés aux traitements des fractures. En conséquence, notre capacité d'ajuster pour
d'autres variables importantes comme l'indice de défavorisation sociale et matérielle, les
complications suivant la fracture, les comorbidités, la médication ou la présence d'autres
119
maladies pouvant avoir une impact important sur la survie des patients et l'utilisation des
ressources médicales était réduite.
Malgré les limites mentionnées ci-dessus, les résultats de nos travaux ont des implications
importantes pour la surveillance épidémiologique des fractures. En effet, le développement
et la validation de l'algorithme basés sur l'utilisation du fichier des services médicaux
rémunérés à l'acte de la RAMQ, nous a permis d'obtenir des estimateurs fiables de
l'incidence des fractures. Ces estimateurs sont également représentatifs, généralisables à la
population et permettent d'éliminer les biais de sélection habituellement liés aux études
menées par enquête. Grâce à l'algorithme que nous avons développé, il est désormais
possible d'identifier l'ensemble des fractures, incluant celles qui ne conduisent pas
nécessairement à une hospitalisation, offrant ainsi une meilleure compréhension du fardeau
des fractures. Cette méthodologie permet non seulement d'élargir la surveillance des
fractures aux fractures de la hanche, mais permet également de l'étendre à celles de
l'ensemble des sites de fractures associées à l'ostéoporose. Cette méthodologie, qui repose
principalement sur l'utilisation de l'algorithme validé et sur une approche par jumelage des
données médico-administratives (RAMQ et Med-Echo), permet d'obtenir des indicateurs de
surveillance concernant non seulement la prévalence, l'incidence, et la mortalité, mais offre
également l'opportunité d'élargir la surveillance par le développement d'autres indicateurs
comme ceux sur l'utilisation des services de santé.
Finalement, un autre avantage important de la méthodologie que nous avons privilégiée est
la capacité de jumeler plusieurs banques de données administratives à l'aide d'un identifiant
unique dans le contexte d'un système de santé universel permettant ainsi d'obtenir des
informations sur l'ensemble des contacts des patients avec le système de santé. Bien que
cette méthode repose sur des données collectées à des fins administratives plutôt qu'à des
fins de surveillance, nos travaux nous permettent de conclure que cette méthode permet
d'obtenir, de manière efficace et peu coûteuse, des indicateurs d'une grande qualité. Enfin,
la méthodologie proposée dans ce projet de recherche est facilement reproductible, offrant
ainsi l'opportunité d'effectuer une surveillance continue et populationnelle des fractures au
Québec.
120
Comme le suggère l'analyse des indicateurs issus de nos travaux portant sur l'incidence des
fractures, les fractures de fragilisation, en termes de mortalité et d'utilisation des ressources
médicales, sont lourdes de conséquence. Outre les fractures de la hanche, les autres
fractures de fragilisation sont également fréquentes et imposent, elles aussi, un fardeau
important sur les individus et sur le système de santé en termes de mortalité et d'utilisation
des ressources. Dans le contexte d'une population vieillissante, les données de base que
nous avons générées permettront de suivre l'évolution de ce problème et constituent un
point de départ important pour évaluer l'impact d'interventions favorisant une prise en
charge optimale de l'ostéoporose et des fractures. Récemment, les données sur l'incidence
des fractures et l'utilisation des ressources médicales issues de ce projet de recherche ont
été utilisés afin d'estimer les coûts directement associés aux traitements de ces fractures.
Selon les derniers résultats, récemment, publiés par notre équipe, les fractures de la hanche
représentent une proportion importante des coûts associés aux traitements des fractures de
fragilisation. Le coût moyen par fracture a été estimé à 46,664 $ [198]. Cependant, les coûts
associés aux traitements des autres fractures de fragilisation ne sont pas négligeables. En
effet, les coûts moyens par fracture sont estimés à 5,253 $ pour les fractures du poignet et à
10,410 $ pour les autres fractures périphériques. Selon des extrapolations à l'ensemble de la
province de Québec, les coûts annuels associés aux traitements des fractures de la hanche et
les autres fractures périphériques sont respectivement évalués à 261 et 101 millions. Ces
résultats démontrent donc la pertinence de la méthodologie proposée dans ce projet.
L'information issue de ces indicateurs aide à comprendre le fardeau que représentent les
fractures sur les ressources médicales et sur les budgets du système de santé. Ces
informations sont particulièrement utiles pour les administrateurs des services de santé qui
ont la responsabilité de coordonner et de prioriser les soins de santé. Elles permettent aux
administrateurs de non seulement planifier l'allocation des ressources humaines et
budgétaires mais aussi, l'organisation des soins afin de maintenir et d'accroître son
efficacité. Ces informations permettent la réalisation de l'analyse coût-efficacité afin
d'évaluer des interventions thérapeutiques ou de santé publique visant une gestion optimale
de cette problématique.

121
5.2 Perspectives Avec le vieillissement rapide de la population du Québec, le nombre de personnes atteintes
d'ostéoporose ou ayant subi une fracture associée à l'ostéoporose ne cesse d'augmenter et
place cette problématique de santé parmi les priorités nationales de santé publique. En
2009, l'Institut national de santé publique du Québec recommandait l'intégration de la
surveillance de l'ostéoporose et des fractures au volet « Maladies chroniques » du Plan
ministériel de surveillance multithématique (PMSM) afin d'élaborer et mettre en œuvre la
surveillance de cette problématique de santé au Québec [202]. Ce volet du PMSM vise à
optimiser la surveillance afin de permettre au ministre de la santé d'obtenir en temps
opportun, des mesures statistiques précises relatives à l'incidence, la prévalence, la survie,
la comorbidité et la multimorbidité de certaines maladies chroniques préalablement ciblées
comme étant prioritaires. À ce jour, ce volet du PMSM a retenu les maladies chroniques
suivantes : le cancer, le diabète, les maladies cardiovasculaires, l'asthme et les maladies
pulmonaires obstructives chroniques (MPOC), les maladies ostéoarticulaires, l'ostéoporose,
les troubles mentaux et la démence.
L'approche méthodologique de ce volet du PMSM repose sur le jumelage de
renseignements contenus dans les fichiers médico-administratifs appartenant à la RAMQ ou
au ministère de la Santé et des Services sociaux (MSSS) et est très similaire à la
méthodologie retenue dans nos travaux. L'utilisation d'algorithmes spécifiques propre à
chaque maladie chronique permet d'identifier les individus atteints et de mesurer les
indicateurs retenus pour la surveillance. Brièvement, la méthodologie employée utilise
différents critères de sélection (c.-à-d. diagnostiques, pharmaceutiques, thérapeutiques ou
de cause de décès) pour identifier un sous-ensemble de la population susceptible d'être
atteinte de l'une ou l'autre des maladies chroniques retenues. Par la suite, pour chaque
individu sélectionné, les renseignements contenus dans chacun des fichiers sont extraits.
Cependant, pour certains fichiers, les données sont extraites à la fois pour les individus
sélectionnés et non sélectionnés. Les différents fichiers sont alors jumelés à l'aide d'un
identifiant anonyme et unique à chaque personne. Pour les individus sélectionnés, tous les
renseignements provenant de tous les fichiers sont obtenus pour l'ensemble de la période
ciblée par l'extraction. La réalisation de la première extraction de données a eu lieu en 2010
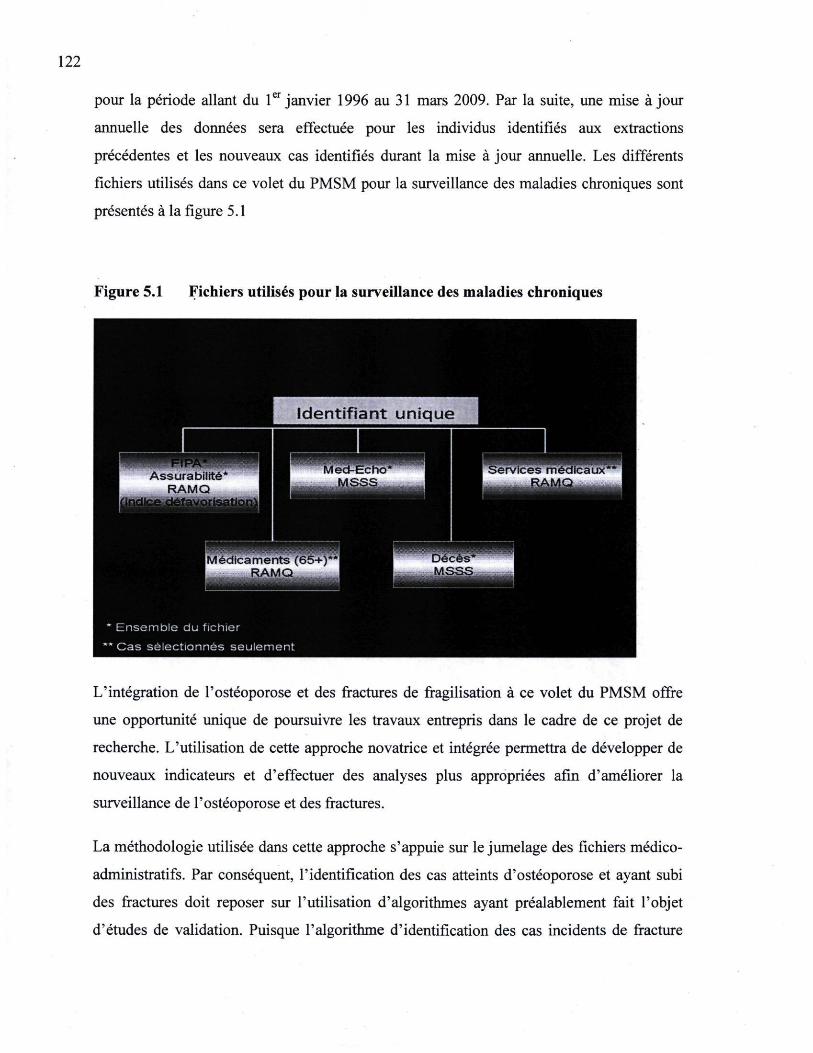
122
pour la période allant du 1er janvier 1996 au 31 mars 2009. Par la suite, une mise à jour
annuelle des données sera effectuée pour les individus identifiés aux extractions
précédentes et les nouveaux cas identifiés durant la mise à jour annuelle. Les différents
fichiers utilisés dans ce volet du PMSM pour la surveillance des maladies chroniques sont
présentés à la figure 5.1
Figure 5.1 Fichiers utilisés pour la surveillance des maladies chroniques
L'intégration de l'ostéoporose et des fractures de fragilisation à ce volet du PMSM offre
une opportunité unique de poursuivre les travaux entrepris dans le cadre de ce projet de
recherche. L'utilisation de cette approche novatrice et intégrée permettra de développer de
nouveaux indicateurs et d'effectuer des analyses plus appropriées afin d'améliorer la
surveillance de l'ostéoporose et des fractures.
La méthodologie utilisée dans cette approche s'appuie sur le jumelage des fichiers médico-
administratifs. Par conséquent, l'identification des cas atteints d'ostéoporose et ayant subi
des fractures doit reposer sur l'utilisation d'algorithmes ayant préalablement fait l'objet
d'études de validation. Puisque l'algorithme d'identification des cas incidents de fracture
123
que nous avons développés présente une excellente validité, il sera utilisé pour identifier les
cas incidents de fracture. Selon les auteurs d'une étude récente de validation effectuée au
Manitoba, il est possible d'identifier les individus souffrant d'ostéoporose sur la base des
données issues des fichiers médico-administratifs avec un niveau acceptable de sensibilité,
de spécificité et de précision [203]. Selon les différents algorithmes développés dans cette
étude, une analyse de validation dans les fichiers administratifs du Québec pourra être
réalisée afin d'obtenir une définition valide pour identifier les cas atteints d'ostéoporose.
L'utilisation de données extraites pour la réalisation du PMSM combinée à ces deux
algorithmes d'identification de cas (ostéoporose et fracture) permettra d'améliorer notre
compréhension de l'ampleur de l'ostéoporose et des fractures ainsi que leurs conséquences.
L'ampleur de cette problématique sera décrite par des estimations de la prévalence et de
l'incidence dans l'ensemble de la population et en fonction de certains déterminants. Ces
nouvelles données permettront non seulement de produire des mesures globales pour
l'ensemble du Québec mais aussi, de mettre en évidence certaines variations selon l'âge, le
sexe (hommes par opposition à femmes), la région sociosanitaire ou la situation
socioéconomique (défavorisation matérielle et sociale) des individus. De plus, l'accès aux
données sur une plus longue période d'observation permettra de suivre l'évolution de ces
mesures dans le temps. Ces informations permettront de mieux quantifier le fardeau global
de l'ostéoporose et des fractures de fragilisation, d'identifier les sous-groupes les plus à
risque et d'effectuer des projections temporelles.
Cette nouvelle approche intégrée permettra également d'améliorer les indicateurs portant
sur l'issue de la maladie (i.e. mortalité, survie et complications), l'utilisation des services de
santé et la consommation des médicaments. En effet, l'accessibilité à une information plus
complète pour les cas sélectionnés (c.-à-d. ensemble des services de santé reçus sur toute la
période) permettra de développer de nouveaux indicateurs sur l'issue clinique de la maladie
comme par exemple l'évaluation des taux de complications médicales à la suite d'une
fracture. Il sera également possible d'effectuer des analyses de comparaison concernant
l'utilisation des services de santé avant et après le diagnostic d'ostéoporose ou de la
survenue d'une fracture. Ces informations permettront également de raffiner les analyses
statistiques afin de prendre en considération d'autres facteurs pouvant avoir un impact sur
124
l'issue clinique de la maladie et de l'utilisation de services de santé, comme par exemple,
l'âge, le sexe, la présence de comorbidité, et l'utilisation de certains médicaments.
Finalement, des analyses portant sur les trajectoires de soins des patientes atteintes
d'ostéoporose ou ayant subi une fracture permettront, d'une part, d'évaluer l'organisation
des systèmes de soins et d'autre part, de développement des indicateurs liés à la
performance du système tels que l'évaluation des délais d'attente pour l'obtention d'une
chirurgie, l'efficacité de la prise en charge, la couverture et l'accès au soins de santé.
Avec le vieillissement de la population, l'augmentation de l'espérance de vie et de
l'amélioration des soins de santé, un nombre de plus en plus important de personnes
risquent maintenant de souffrir simultanément de plusieurs maladies chroniques. Dans ce
contexte, la surveillance doit se préoccuper du vieillissement de la population et du cumul
des maladies chroniques. Par conséquent, la multi-morbidité et la comorbidité représentent
des défis nouveaux et majeurs de surveillance. Dans cette perspective de cumul des
maladies, il est essentiel de mieux comprendre quelles sont les répercussions de ces
comorbidités sur la santé et l'évolution de la santé des individus atteint d'ostéoporose ou
ayant subi une fracture de fragilisation. Ainsi, l'identification des facteurs de risque
communs à l'ostéoporose, aux fractures et à d'autres maladies chroniques permettra de
cibler certaines combinaisons de maladies plus fréquentes méritant une investigation
approfondie.
En conclusion, l'expertise développée dans le projet de recherche combinée à l'approche
méthodologique développé dans le PMSM, permettra la poursuite de la surveillance de
l'ostéoporose et des fractures au Québec. La grande disponibilité de l'information et le
raffinement des méthodes utilisées permettront d'augmenter notre capacité en matière de
surveillance de l'ostéoporose et des fractures de fragilisation, un élément essentiel à une
meilleure compréhension de l'importance populationnelle de cette problématique. Dans ce
nouveau contexte, la surveillance pourra alors dépasser la simple observation des taux
d'incidence, de mortalité et d'hospitalisation pour se rapprocher davantage de son objectif
fondamental, soit de documenter l'évolution de cette problématique de santé afin d'appuyer
la prise de décision, de promouvoir la prévention et d'assurer une meilleur qualité des soins.
125
Bibliographie 1. Papadimitropoulos EA, Coyte PC, Josse RG, Greenwood CE, Current and projected
rates of hip fracture in Canada. CMAJ, 1997. 157(10): p. 1357-63. 2. Tenenhouse A, Joseph L, Kreiger N, Poliquin S, Myrray TM, Blondeau L, Berger
C, Hanley DA, Prior JC; CaMos Researcg Group, Estimation of the prevalence of low bone density in Canadian women and men using a population-specific DXA reference standard: the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos Int, 2000. 11(10): p. 897-904.
3. Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med, 1993. 94(6): p. 646-50.
4. Bessette L, Ste-Marie LG, Jean S, Davison KS, Beaulieu M, Baranci M, Bessant J, Brown JP, The care gap in diagnosis and treatment of women with a fragility fracture. Osteoporos Int, 2008. 19(1): p. 79-86.
5. Klotzbuecher CM, Ross PD, Landsman PB, Abbott TA III, Berger M, Patients with prior fractures have an increased risk of future fractures: a summary ofthe literature and statistical synthesis. J Bone Miner Res, 2000. 15(4): p. 721-39.
6. Melton LJ III, Chrischilles EA, Cooper C, Lane AW, Riggs BL, Perspective. How many women have osteoporosis? J Bone Miner Res, 1992. 7(9): p. 1005-10.
7. Johnell O, Kanis JA, Epidemiology of osteoporotic fractures. Osteoporos Int, 2005. 16 Suppl 2: p. S3-7.
8. Kanis JA, Johnell O, Oden A, Sembo I, Redlund-Johnell I, Dowson A, De Laet C, Jonsson B, Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int, 2000. 11(8): p. 669-74.
9. Sambrook P, Cooper C, Osteoporosis. Lancet, 2006. 367(9527): p. 2010-8. 10. Center JR, Nguyen TV, Schneider D, Sambrook PN, Eisman JA, Mortality after all
major types of osteoporotic fracture in men and women: an observational study. Lancet, 1999. 353(9156): p. 878-82.
11. Magaziner J, Simonsick EM, Kashner TM, Hebel JR, Kenzora JE, Predictors of functional recovery one year following hospital discharge for hip fracture: a prospective study. J Gerontol, 1990. 45(3): p. M101-7.
12. A framework and strategy for the prevention and management of osteoporosis. Report ofthe Strategic Action Working Group on Osteoporosis. 2000, Ontario's Women Health Council: Toronto, p. 49.
13. Papaioannou A, Adachi JD, Parkinson W, Stephenson G, Bédard M, Lengthy hospitalization associated with vertebral fractures despite control for comorbid conditions. Osteoporos Int, 2001.12(10): p. 870-4.
14. Jaglal S, Osteoporotic fractures: incidence and impact. Patterns in Health Care in Ontario: Arthritis and related conditions., ed. J.I. Williams and E.M. Badley. 1998, Toronto: IRSS.
15. Goeree R, O'Brien B, Pettitt D, Cuddy L, Ferraz M, Adachi J, An assessment ofthe burden of illness due to osteoporosis in Canada. J Soc Obstet Gynaecol Can, 1998. 18: p. 15-24.
16. Roos LL, Roos NP, Cageorge SM, Nicol JP, How good are the data? Reliability of one health care data bank. Med Care, 1982. 20(3): p. 266-76.
126
17. Roos LL, Gupta S, Soodeen RA, Jebamani L, Data quality in an information-rich environment : Canada as an example. Can J Aging, 2005. 24(Suppl 1): p. 153-70.
18. Silver J J, Einhorn TA, Osteoporosis and aging. Current update. Clin Orthop Relat Res, 1995(316): p. 10-20.
19. Osteoporosis Action Plan: An Osteoporosis Strategy for Ontario. Report ofthe Osteoporosis Action Plan Committee to the Ministry of Health and Long-Term Care. 2003, Ministry of Health and Long-term Care, Government of Ontario.
20. Glaser DL, Kaplan FS, Osteoporosis. Definition and clinical presentation. Spine (PhilaPa 1976), 1997. 22(24 Suppl): p. 12S-16S.
21. Kanis JA, Johnell O, Oden A, De Laet C, Mellstrom D, Epidemiology of osteoporosis and fracture in men. Calcif Tissue Int, 2004. 75(2): p. 90-9.
22. Osteoporosis prevention, diagnosis, and therapy. NIH Consens Statement, 2000. 17(1): p. 1-45.
23. Kanis JA, Melton LJ, Christiansen C, Johnston CC, Khaltaev N, The diagnosis of osteoporosis. J Bone Miner Res, 1994. 9(8): p. 1137-41.
24. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser, 1994. 843: p. 1-129.
25. Cranney A, Jamal SA, Tsang JF, Josse RG, Leslie WD, Low bone mineral density and fracture burden in postmenopausal women. CMAJ, 2007. 177(6): p. 575-80.
26. Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, Delmas P, Eisman J, Fujiwara S, Garnero P, Kroger H, McCloskey EV, Mellstrom D, Melton LJ, Pols H, Reeve J, Silman A, Tenenhouse A, A meta-analysis of previous fracture and subsequent fracture risk. Bone, 2004. 35(2): p. 375-82.
27. Kanis JA, Johansson H, Oden A, Johnell O, De Laet C, Melton III LJ, Tenenhouse A, Reeve J, Silman AJ, Pols HA, Eisman JA, McCloskey EV, Mellstrom D, A metaanalysis of prior corticosteroid use and fracture risk. J Bone Miner Res, 2004. 19(6): p. 893-9.
28. Kanis JA, Johansson H, Oden A, Johnell O, De Laet C, Eisman JA, McCloskey EV, Mellstrom D, Melton LJ 3rd, Pols HA, Reeve J, Silman AJ, Tenenhouse A, A family history of fracture and fracture risk: a meta-analysis. Bone, 2004. 35(5): p. 1029-37.
29. Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP, Feldman S, Hanley DA, Hodsman A, Jamal SA, Kaiser SM, Kvern B, Siminoski K, Leslie WD, 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. CMAJ, 2010. 182(17): p. 1864-73.
30. Guidelines for pre-clinical evaluation and clinical trial in osteoporosis. 1998, World Health Organization: Geneva, Switzerland, p. 78.
31. Kanis JA, Oden A, Johnell O, Jonsson B, De Laet C, Dawson A, The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporos Int, 2001. 12(5): p. 417-27.
32. Warriner AH, Patkar NM, Curtis JR, Delzell E, Gary L, Kilgore M, Saag K, Which fractures are most attributable to osteoporosis? J Clin Epidemiol, 2011. 64(1): p. 46-53.
33. Mackey DC, Lui LY, Cawthon PM, Bauer DC, Nevitt MC, Cauley JA, Hillier TA, Lewis CE, Barrett-Connor E, Cummings SR, High-trauma fractures and low bone mineral density in older women and men. JAMA, 2007. 298(20): p. 2381-8.
127
34. Curtis JR, Taylor AJ, Matthews RS, Ray MN, Becker DJ, Gary LC, Kilgore ML, Morrisey MA, Saag KG, Warriner A, Delzell E, "Pathologic"fractures: should these be included in epidemiologic studies of osteoporotic fractures? Osteoporos Int, 2009. 20(11): p. 1969-72.
35. Kanis JA, The incidence of hip fracture in Europe. Osteoporos Int, 1993. 3 Suppl 1: p. 10-5.
36. Johnell O, Kanis JA, An estimate ofthe worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int, 2006. 17(12): p. 1726-33.
37. Kanis JA, Johnell O, De Laet C, Jonsson B, Oden A, Ogelsby AK, International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res, 2002. 17(7): p. 1237-44.
38. Levy AR, Mayo NE, Grimard G, Rates of transcervical and pertrochanteric hip fractures in the province of Quebec, Canada, 1981-1992. Am J Epidemiol, 1995. 142(4): p. 428-36.
39. Cummings SR, Melton LJ, Epidemiology and outcomes of osteoporotic fractures. Lancet, 2002. 359(9319): p. 1761-7.
40. Health Indicators 2007, Canadian Institute for health Information: Ottawa. 41. Gullberg B, Johnell O, Kanis JA, World-wide projections for hip fracture.
Osteoporos Int, 1997. 7(5): p. 407-13. 42. Johnell O, Gulberg B, Allender E, Kanis JA, The apparent incidence of hip fracture
in Europe: a study of national register sources. MEDOS Study Group. Osteoporos Int, 1992. 2(6): p. 298-302.
43. Elffors I, Allender E, Kanis JA, Gullberg B, Johnell O, Dequeker J, Dilsen G, Gennari C, Lopes Vaz AA, Lyritis G et al., The variable incidence of hip fracture in southern Europe: the MEDOS Study. Osteoporos Int, 1994. 4(5): p. 253-63.
44. Kannus P, Niemi S, Parkari J, Palvanen M, Vuori I, Jârviven M, Nationwide decline in incidence of hip fracture. J Bone Miner Res, 2006. 21(12): p. 1836-8.
45. Chevalley T, Guilley E, Herrmann FR, Hoffmeyer P, Rapin CH, Rizzoli R, Incidence of hip fracture over a 10-year period (1991-2000): reversal of a secular trend. Bone, 2007. 40(5): p. 1284-9.
46. Zingmond DS, Melton 3r LJ, Silverman SL, Increasing hip fracture incidence in California Hispanics, 1983 to 2000. Osteoporos Int, 2004. 15(8): p. 603-10.
47. Giversen IM, Time trends of age-adjusted incidence rates of first hip fractures: a register-based study among older people in Viborg County, Denmark, 1987-1997. Osteoporos Int, 2006. 17(4): p. 552-64.
48. Finsen V, Jonhsen LG, Trane G, Hansen N, Sneve KS, Hip fracture incidence in central Norway: afollowup study. Clin Orthop Relat Res, 2004(419): p. 173-8.
49. Chang KP, Center JR, Nguyen TV, Eisman JA, Incidence of hip and other osteoporotic fractures in elderly men and women: Dubbo Osteoporosis Epidemiology Study. J Bone Miner Res, 2004.19(4): p. 532-6.
50. Herrera A, Martinez AA, Ferrandez L, Gil E, Moreno A, Epidemiology of osteoporotic hip fractures in Spain. Int Orthop, 2006. 30(1): p. 11-4.
51. Lônnroos E, Kautiainen H, Karppi P, Huusko T, Hartikainen S, Kiviranta I, Sulkava R, Increased incidence of hip fractures. A population based-study in Finland. Bone, 2006. 39(3): p. 623-7.
52. Stephenson S, Langley J, Campbell J, Gillespie W, Upward trends in the incidence of neck of femur fractures in the elderly. N Z Med J, 2003. 116(1185): p. U665.
128
53. Hagino H, Katagiri H, Okano T, Yamamoto K, Teshima R, Increasing incidence of hip fracture in Tottori Prefecture, Japan: trend from 1986 to 2001. Osteoporos Int, 2005.16(12): p. 1963-8. "
54. Jaglal SB, Weller I, Mamdani M, Hawker G, Kreder H, Jaakkimainen L, Adachi JD, Population trends in BMD testing, treatment, and hip and wrist fracture rates: are the hip fracture projections wrong? J Bone Miner Res, 2005. 20(6): p. 898-905.
55. Nymark T, Lauritsen JM, Ovesen O, Rock ND, Jeune B, Decreasing incidence of hip fracture in the Funen County, Denmark. Acta Orthop, 2006. 77(1): p. 109-13.
56. Gehlbach SH, Avrunin JS, Puleo E, Trends in hospital care for hip fractures. Osteoporos Int, 2007.18(5): p. 585-91.
57. Leslie WD, O'Donnell S, Jean S, Lagacé C, Walsh P, Bancej C, Morin S, Hanley DA, Papaioannou A, Trends in hip fracture rates in Canada. JAMA, 2009. 302(8): p. 883-9.
58. Briefel RR, Johnson CL, Secular trends in dietary intake in the United States. Annu Rev Nutr, 2004. 24: p. 401-31.
59. Brownson RC, Boehmer TK, Luke DA, Declining rates of physical activity in the United States: what are the contributors? Annu Rev Public Health, 2005. 26: p. 421-43.
60. Hagenau T, Vest R, Gissel TN, Poulsen CS, Erlandsen M, Mosekilde L, Vestergaard P, Global vitamin D levels in relation to age, gender, skin pigmentation and latitude: an écologie meta-regression analysis. Osteoporos Int, 2009. 20(1): p. 133-40.
61. Gates S., Fisher JD, Cooke MW, Carter YH, Lamb SE, Multifactorial assessment and targeted intervention for preventing falls and injuries among older people in community and emergency care settings: systematic review and meta-analysis. BMJ, 2008. 336(7636): p. 130-3.
62. Katzmarzyk PT, The Canadian obesity epidemic, 1985-1998. CMAJ, 2002.166(8): p. 1039-40.
63. Tremblay MS, Katzmarzyk PT, Willms JD, Temporal trends in overweight and obesity in Canada, 1981-1996. Int J Obes Relat Metab Disord, 2002. 26(4): p. 538-43.
64. Gilmore J, Report on Smoking in Canada, 1985 to 2001, S. Canada, Editor. 2002. 65. Melton LJ 3rd, Crowson CS, O'Fallon WM, Fracture incidence in Olmsted County,
Minnesota: comparison of urban with rural rates and changes in urban rates over time. Osteoporos Int, 1999. 9(1): p. 29-37.
66. Sanders KM, Seeman E, Ugoni AM, Pasco JA, Martin TJ, Skoric B, Nicholson GC, Kotowicz MA, Age- and gender-specific rate of fractures in Australia: a population-based study. Osteoporos Int, 1999.10(3): p. 240-7.
67. Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A, Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res, 2007. 22(3): p. 465-75.
68. Leslie WD, Sadotsafovi M, Lix LM, Azimaee M, Morin S, Metge CJ, Caetano P, Secular decreases in fracture rates 1986-2006 for Manitoba, Canada: a population-based analysis. Osteoporos Int, 2011. 22(7): p. 2137-43.
69. Center JR, Bliuc D, Nguyen TV, Eisman JA, Risk of subsequent fracture after low-trauma fracture in men and women. JAMA, 2007. 297(4): p. 387-94.
129
70. Papaioannou A, Wiktorowicz M, Adachi JD, Goeree R, Papadimitropoulos E, Bédard M, Brazil K, Parkinson W, Weaver B, Mortality, independence in living, and re-fracture, one year following hip fracture in Canadians. J Soc Obstet Gynaecol Can, 2000. 22(8): p. 591-7.
71. Nymark T, Lauritsen JM, Ovesen O, Rock ND, Jeune B, Short time-frame from first to second hip fracture in the Funen County Hip Fracture Study. Osteoporos Int, 2006. 17(9): p. 1353-7.
72. White BL, Fisher WD, Laurin CA, Rate of mortality for elderly patients after fracture ofthe hip in the 1980's. J Bone Joint Surg Am, 1987. 69(9): p. 1335-40.
73. Wiktorowicz ME, Goeree R, Papaioannou A, Adachi JD, Papadimitropoulos E, Economic implications of hip fracture: health service use, institutional care and cost in Canada. Osteoporos Int, 2001. 12(4): p. 271-8.
74. Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C, Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int, 2009. 20(10): p. 1633-50.
75. Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jônsson B, Mortality after osteoporotic fractures. Osteoporos Int, 2004.15(1): p. 38-42.
76. Morin S, Lix LM, Azimaee M, Metge C, Caetano P, Leslie WD, Mortality rates after incident non-traumatic fractures in older men and women. Osteoporos Int, 2011. 22(9): p. 2439-48.
77. Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR, Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA, 2009. 301(5): p. 513-21.
78. Adachi JD, Ioannidis G, Berger C, Joseph L, Papaioannou A, Pickard L, Papadimitropoulos EA, Hopman W, Poliquin S, Prior JC, Hanley DA, Olszynski WP, Anastassiades T, Brown JP, Murray T, Jackson SA, tenenhouse A, The influence of osteoporotic fractures on health-related quality of life in community-dwelling men and women across Canada. Osteoporos Int, 2001. 12(11): p. 903-8.
79. Brown JP, Josse RG, 2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. CMAJ, 2002. 167(10 Suppl): p. Sl-34.
80. Leslie WD, Berger C, Langsetmo L, Lix LM, Adachi JD, Hanley DA, Ioannidis G, Josse RG, Kovacs CS, Towheed T, Kaiser S, Olszynski WP, Prior JC, Jamal S, Kreiger N, Goltzman D, Construction and validation of a simplified fracture risk assessment tool for Canadian women and men: results from the CaMos and Manitoba cohorts. Osteoporos Int, 2011. 22(6): p. 1873-83.
81. Leslie WD, Lix LM, Langsetmo L, Berger C, Goltzman D, Hanley DA, Adachi JD, Johansson H, Oden A, McCloskey E, Kanis JA, Construction of a FRAX(R) model for the assessment of fracture probability in Canada and implications for treatment. Osteoporos Int, 2011. 22(3): p. 817-27.
82. Leslie WD, Lix LM, Johansson H, Oden A, McClosket E, Kanis JA, Independent clinical validation of a Canadian FRAX tool: fracture prediction and model calibration. J Bone Miner Res, 2010. 25(11): p. 2350-8.
83. Leslie WD, Tsang JF, Lix LM, Simplified system for absolute fracture risk assessment: clinical validation in Canadian women. J Bone Miner Res, 2009. 24(2): p. 353-60.
130
84. Fraser LA, Langsetmo L, Berger C, Ioannidis G, Goltzman D, Adachi JD, Papaioannou A, Josse R, Kovaca CS, Olszynski WP, Towheed T, Hanley DA, Kaiser SM, Prior J, Jamal S, Kreiger N, Brown JP, Johansson H, Oden A, McCloskey E, Kanis J A, Leslie WD, Fracture prediction and calibration of a Canadian FRAX(R) tool: a population-based report from CaMos. Osteoporos Int, 2011. 22(3): p. 829-37.
85. Siminoski K, Leslie WD, FRame H, Hodsman A, Josse RG, Khan A, Lentle BC, Lévesque J, Lyons DJ, Tarulli G, Brown JP, Recommendations for bone mineral density reporting in Canada. Can Assoc Radiol J, 2005. 56(3): p. 178-88.
86. Kanis JA, Oden A, Johnell O, Johansson H, De Laet C, Brown J, Burckhardt P, Cooper C, Christiansen C, Cummings S, Eisman JA, Fujiwara S, Glûer C, Goltzman D, Hans D, Krieg MA, La Croix A, McCloskey E, Mellstrom D, Melton LJ 3rd, Pols H, Reeve J, Sanders K, Schott AM, Silman A, Torgerson D, van Staa T, Watts NB, Yoshimura ~N,The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int, 2007. 18(8): p. 1033-46.
87. Schwab P, Klein RF, Nonpharmacological approaches to improve bone health and reduce osteoporosis. Curr Opin Rheumatol, 2008. 20(2): p. 213-7.
88. Park H, Kim KJ, Komatsu T, Park SK, Mutoh Y, Effect of combined exercise training on bone, body balance, and gait ability: a randomized controlled study in community-dwelling elderly women. J Bone Miner Metab, 2008. 26(3): p. 254-9.
89. Tang BM, Eslick GD, Nowson C, Smith C, Bensoussan A, Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: a meta-analysis. Lancet, 2007. 370(9588): p. 657-66.
90. Cranney A, Guyatt G, Griffith L, Wells G, Tugwell P, Rosen C, Meta-analyses of therapies for postmenopausal osteoporosis. LX: Summary of meta-analyses of therapies for postmenopausal osteoporosis. Endocr Rev, 2002. 23(4): p. 570-8.
91. Perspectives démographiques Québec et régions, 2006-2056. 2009, Institut de la statistique du Québec.
92. Medley ES, Shirley SM, Brilliant HL, Fracture management by family physicians and guidelines for referral. J Fam Pract, 1979. 8(4): p. 701-10.
93. Manusov EG. Pearman D, Ross S, Beadling CW, Goff TH, Orthopedic trauma: a family practice perspective. Mil Med, 1990.155(7): p. 314-6.
94. Hatch RL, Rosenbaum CI, Fracture care by family physicians. A review of 295 cases. J Fam Pract, 1994. 38(3): p. 238-44. "
95. Swain R. and Ashley J, Primary care orthopedics and sports medicine in West Virginia. W V Med J, 1995. 91(3): p. 98-100.
96. Roland MO, Porter RW, Mathews JG, Redden JF, Simonds GW, Bewley B, Improving care: a study of orthopaedic outpatient referrals. BMJ, 1991. 302(6785): p. 1124-8.
97. Brinker MR, O'Connor DP, The incidence of fractures and dislocations referred for orthopaedic services in a capitated population. J Bone Joint Surg Am, 2004. 86-A(2): p. 290-7.
98. Sporer SM, Weinstein JN, and Koval KJ, The geographic incidence and treatment variation of common fractures of elderly patients. J Am Acad Orthop Surg, 2006. 14(4): p. 246-55.
131
99. Tracey J, Forte T, Fagbemi J, Chaudhary Z, Wait time for hip fracture surgery in Canada. Healthc Q, 2007. 10(4): p. 24-7.
100. Orosz GM, Magaziner J, Hannan EL, Morisson RS, Koval K, Gilbert M, Mclaughlin M, Halm EA, Wang JJ, Like A, Silberzweig SB, Siu AL, Association of timing of surgery for hip fracture and patient outcomes. JAMA, 2004. 291(14): p. 1738-43.
101. Bottle,A, Aylin P, Mortality associated with delay in operation after hip fracture: observational study. BMJ, 2006. 332(7547): p. 947-51.
102. D'Angelo F, Giudici M, Molina M, Margaria G, Mortality rate after hip hemiarthroplasty: analysis of risk factors in 299 consecutive cases. Journal of orthopedics and traumatology, 2005. 6(3): p. 111-116.
103. Cheung AM, Feig DS, Kapral M, Diaz-Granados N, Dodin S, Prevention of osteoporosis and osteoporotic fractures in postmenopausal women: recommendation statement from the Canadian Task Force on Preventive Health Care. CMAJ, 2004.170(11): p. 1665-7.
104. Brown JP, Fortier M, Canadian consensus conference on osteoporosis, 2006 update. J Obstet Gynaecol Can, 2006. 28(2 Suppl 1): p. S95-S112.
105. Liberman UA, Weiss SR, Broil J, Minne HW, Quan H, Bell NH, Rodriguez-Portales J, Downs RW Jr, DequeKer J, Favus M, Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The Alendronate Phase III Osteoporosis Treatment Study Group. N Engl J Med, 1995. 333(22): p. 1437-43.
106. Cummings SR, Black DM, Thompson DE, Applegate WB, Barett-Connor E, Musliner TA, Palermo L, Prineas R, Rubin SM, Scott JC, Vogt T, Wallace R, Yates AJ, LaCroix AZ, Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA, 1998. 280(24): p. 2077-82.
107. McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C, Adami S, Fogelman I, Diamond T, Eastell R, Meunier JP, Reginster JY, Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med, 2001. 344(5): p. 333-40.
108. Hodsman AB, Hanley DA, Josse R, Do bisphosphonates reduce the risk of osteoporotic fractures? An evaluation ofthe evidence to date. CMAJ, 2002. 166(11): p. 1426-30.
109. Delmas PD, Treatment of postmenopausal osteoporosis. Lancet, 2002. 359(9322): p. 2018-26.
110. Brown TER, Osteoporosis: a pharmacotherapy update. Journal of pharmacy practice, 2003.16(3): p. 164-169.
111. Hauselmann HJ, Rizzoli R, A comprehensive review of treatments for postmenopausal osteoporosis. Osteoporos Int, 2003.14(1): p. 2-12.
112. Papaioannou A, Giangregorio L, Kvern B, Boulos P, Ioannidis G, Adachi JD, The osteoporosis care gap in Canada. BMC Musculoskelet Disord, 2004. 5: p. 11.
113. Leslie WD, Giangregorio LM, Yogendran M, Azimaee M, Morin S, Metge S, Caetano P, Lix LM, A population-based analysis ofthe post-fracture care gap 1996-2008: the situation is not improving. Osteoporos Int, 2011.
114. Hajcsar EE, Hawker G, Bogoch ER, Investigation and treatment of osteoporosis in patients with fragility fractures. CMAJ, 2000.163(7): p. 819-22.
132
115. Giangregorio L, Papaioannou A, Cranney A, Zytaruk N, Adachi JD, Fragility fractures and the osteoporosis care gap: an international phenomenon. Semin Arthritis Rheum, 2006. 35(5): p. 293-305.
116. Elliot-Gibson V, Bogoch ER, Jamal SA, Beaton DE, Practice patterns in the diagnosis and treatment of osteoporosis after a fragility fracture: a systematic review. Osteoporos Int, 2004.15(10): p. 767-78.
117. Development of a model for integrated post-fracture care in Ontario. 2003, Ontario Women's Health Council: Toronto, p. 92.
118. Report ofthe Surgeon General's Workshop on Osteoporosis and Bone Health. 2004, US Department of Health and Human Services, p. 55.
119. Sattin RW, Lambert Huber DA, DeVito CA, Rodriguez JG, Ros A, Bacchelli S, Stevens JA, Waxweiler RJ, The incidence of fall injury events among the elderly in a defined population. Am J Epidemiol, 1990. 131(6): p. 1028-37.
120. Tamblyn R, Reid T, Mayo N, McLeod P, Churchill-Smith M, Using medical services claims to assess injuries in the elderly: sensitivity of diagnostic and procedure codes for injury ascertainment. J Clin Epidemiol, 2000. 53(2): p. 183-94.
121. Outils de recherche de l'information statistique (ORIS). Available from: www.ramp.gouv.qc.ca.
122. Wilchesky M, Tamblyn RM, Huang A, Validation of diagnostic codes within medical services claims. J Clin Epidemiol, 2004. 57(2): p. 131-41.
123. Tamblyn R, Lavoie G, Petrella L, Monette J, The use of prescription claims databases in pharmacoepidemiological research: the accuracy and comprehensiveness ofthe prescription claims database in Quebec. J Clin Epidemiol, 1995. 48(8): p. 999-1009.
124. Kostylova A, Swaine B, Feldman D, Concordance between childhood injury diagnoses from two sources: an injury surveillance system and a physician billing claims database. Inj Prev, 2005. 11(3): p. 186-90.
125. Monfared AA, Lelorier J, Accuracy and validity of using medical claims data to identify episodes of hospitalizations inpatients with COPD. Pharmacoepidemiol Drug Saf, 2006.15(1): p. 19-29.
126. Benchimol EI, Manuel DG, To T, Griffiths AM, Rabeneck L, Guttmann A, Development and use of reporting guidelines for assessing the quality of validation studies of health administrative data. J Clin Epidemiol, 2011. 64(8): p. 821-9.
127. De Coster C, Quan H, Finlayson A, Gao M, Halfon P, Humphries KH, Johansen H, Lix LM, Luthi JC, Ma J, Romano PS, Roos L, Sundararajan V, Tu JV, Webster G, Ghali WA, Identifying priorities in methodological research using ICD-9-CM and ICD-10 administrative data: report from an international consortium. BMC Health Serv Res, 2006. 6(15): p. 77.
128. Ray WA, Griffin MR, Fought RL, Adams ML, Identification of fractures from computerized Medicare files. J Clin Epidemiol, 1992. 45(7): p. 703-14.
129. Jean S.; Candas B, Belzile.E., Morin S, Bessette L, Dodin S, Brown JP, Algorithms can be used to identify fragility fracture cases in physician-claims databases. Osteoporos Int, 2011.
130. Cooper C, The crippling consequences of fractures and their impact on quality of life. Am J Med, 1997.103(2A): p. 12S-17S; discussion 17S-19S.
131. Ioannidis G, Papaioannou A, Hopman WM, khtar-Danesh N, Anastassiades T, Pickard L, Kennedy CC, Prior JC, Olszynski WP, Davison KS, Goltzman D,
133
Thabane L, Gafhi A, Papadimitropoulos EA, Brown JP, Josse RG, Hanley DA, Adachi JD, Relation between fractures and mortality: results from the Canadian Multicentre Osteoporosis Study. CMAJ, 2009.181(5): p. 265-71.
132. Melton LJ III, Adverse outcomes of osteoporotic fractures in the general population. J Bone Miner Res, 2003.18(6): p. 1139-41.
133. Lippuner K, Golder M, Greiner R, Epidemiology and direct medical costs of osteoporotic fractures in men and women in Switzerland. Osteoporos Int, 2005.16 Suppl 2: p. S8-S17.
134. Lix LM, Yogendran MS, Leslie WD, Shaw SY, Baumgartner R, Bowman C, Metge C, Gumel A, Hux J, James RC, Using multiple data features improved the validity of osteoporosis case ascertainment from administrative databases. J Clin Epidemiol, 2008. 61(12): p. 1250-60.
135. Zuckerman IH, Sato M, Hsu VD, Hernandez J J, Validation of a method for identifying nursing home admissions using administrative claims. BMC Health Serv Res, 2007. 7: p. 202.
136. Potter BK, Manuel D, Speechley KN, Gutmanis IA, Campbell MK, Koval JJ, Is there value in using physician billing claims along with other administrative health care data to document the burden of adolescent injury? An exploratory investiation with comparison to self-reports in Ontario. BMC Health Serv Res, 2005. 5.
137. Dendukuri N, McCusker J, Bellavance F, Cardin S, Verdon J, Karp I, Belzile E, Comparing the validity of different sources of information on emergency department visits: a latent class analysis. Med Care, 2005. 43(3): p. 266-75.
138. Bessette L, Ste-Marie LG, Jean S, Davison KS, Beaulieu M, Baranci M, Bessant J, Brown JP, Recognizing osteoporosis and its consequences in Quebec (ROCQ): background, rationale, and methods of an anti-fracture patient health-management programme. Contemp Clin Trials, 2008. 29(2): p. 194-210.
139. Curtis JR, Mudano AS, Solomon DH, Xi J, Melton ME, Saag KG, Identification and validation of vertebral compression fractures using administrative claims data. Med Care, 2009. 47(1): p. 69-72.
140. Bernard PM, Lapointe C, Mesure statistique en epidemiologic 1995: Presses de l'Université du Québec. 175-190.
141. Altman DG, Bland JM, Diagnostic tests 2: Predictive values. BMJ, 1994. 309(6947): p. 102.
142. Altman DG, Bland JM, Diagnostic tests. 1: Sensitivity and specificity. BMJ, 1994. 308(6943): p. 1552.
143. Biggerstaff BJ, Comparing diagnostic tests: a simple graphie using likelihood ratios. Stat Med, 2000. 19(5): p. 649-63.
144. Lentle BC, Brown JP, Khan A, Leslie WD, Lévesque J, Lyons DJ, Siminoski K, Tarulli G, Josse RG, Hodsman A, Recognizing and reporting vertebral fractures: reducing the risk of future osteoporotic fractures. Can Assoc Radiol J, 2007. 58: p. 27-36.
145. Cataldi V; Laporta T; Sverzellati N, De FM, Zompatori M, Detection of incidental vertebral fractures on routine lateral chest radiographs. Radiol Med, 2008.113: p. 968-977.
146. Pentek M, Horvacth C, Boncz I, Falusi Z, Toth E, Sebestyen A, Majer I, Brodszky V, Gulacsi L, Epidemiology of osteoporosis related fractures in Hungary from the
134
nationwide health insurance database, 1999-2003. Osteoporos Int, 2008.19(2): p. 243-9.
147. Papaioannou A, Kennedy CC, Ioannidis G, Sawka A, Hopman WM, Pickard L, Brown JP, Josse RG, Kaiser S, Anastassiades T, Goltzman D, Papadimitropoulos M, Tenenhouse A, Prior JC, Olszynski WP, Adachi JD, The impact of incident fractures on health-related quality of life: 5 years of data from the Canadian Multicentre Osteoporosis Study. Osteoporos Int, 2009. 20(5): p. 703-14.
148. Haentjens P, Magaziner J, Colon-Emeric CS, Vanderschueren D, Milisen K, Velkeniers B, Boonen S, Meta-analysis: excess mortality after hip fracture among older women and men. Ann Intern Med, 2010.152(6): p. 380-90.
149. Vestergaard P, Rejnmark L, Mosekilde L, Increased mortality inpatients with a hip fracture-effect ofpre-morbid conditions and post-fracture complications. Osteoporos Int, 2007. 18(12): p. 1583-93.
150. Crawford AG, Cote C, Couto J, Daskiran M, Gunnarsson C, Haas K, Haas S, Nigam SC, Schuette R, Prevalence of obesity, type II diabetes mellitus, hyperlipidemia, and hypertension in the United States: findings from the GE Centricity Electronic Medical Record database. Popul Health Manag, 2010.13(3): p. 151-61.
151. Van WC, Austin PC, Manuel D, Knoll G, Jennings A, Forster AJ, The usefulness of administrative databases for identifying disease cohorts is increased with a multivariate model. J Clin Epidemiol, 2010. 63: p. 1332-1341.
152. Wirehn AB, Karlsson HM, Carstensen JM, Estimating disease prevalence using a population-based administrative healthcare database. Scand J Public Health, 2007. 35(4): p. 424-31.
153. Institut de la statistique du Québec, Démographie: Données générales, Population du Québec. 2010;
154. Statistique Canada 2011. http://www.12.statcan.ca/francais/census01. Accessed. 155. Department of Demography, Université de Montréal Canada. Canadian Human
Mortality Databae. Available from: http://www.bdlc.umontreal.ca/CHMD/. 156. Bessette L, Jean S, Roy S, Davison KS, Ste-Marie L-G, Brown JP, The relationship
between body mass index and the risk ofpheripheral fragility fracture. JBMR, 2010: p. 24.
157. Fisher AA, O'Brien ED, Davis MW, Trends in hip fracture epidemiology in Australia: possible impact ofbisphosphonates and hormone replacement therapy. Bone, 2009. 45(2): p. 246-53.
158. Mann, E., Icks A, Haastert B, Meyer G, Hip fracture incidence in the elderly in Austria: an epidemiological study covering the years 1994 to 2006. BMC Geriatr, 2008. 8: p. 35.
159. Melton LJ 3rd, Kearns AE, Atkinson EJ, Bolander ME, Achenbach SJ, Huddleston JM, Therneau TM, Leibson CL, Secular trends in hip fracture incidence and recurrence. Osteoporos Int, 2009. 20(5): p. 687-94.
160. Ahlborg HG, Rosengren BE, Jarvinen TL, Rogmark C, Nilsson JA, Sernbo I, Karlsson MK, Prevalence of osteoporosis and incidence of hip fracture in women -secular trends over 30 years. BMC Musculoskelet Disord, 2010. 11(48): p. 48.
161. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB, Incidence and mortality of hip fractures in the United States. JAMA, 2009. 302(14): p. 1573-9.
135
162. Bergstrom U, Jonsson H, Gustafson Y, Pettersson U, Stenlund H, Svensson O, The hip fracture incidence curve is shifting to the right. Acta Orthop, 2009. 80(5): p. 520-4.
163. Fransen M, Woodward M, Norton R, Robinson E, Butler M, Campbell AJ, Excess mortality or institutionalization after hip fracture: men are at greater risk than women. J Am Geriatr Soc, 2002. 50: p. 685-690.
164. Crée MW, Juby AG, Carrière KC, Mortality and morbidity associated with osteoporosis drug treatment following hip fracture. Osteoporos Int, 2003.14(9): p. 722-7.
165. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ, Mortality risk after hip fracture. J Orthop Trauma, 2003. 17(1): p. 53-6.
166. McLeod K, Brodie MP, Fahey PP, Gray RA, Long-term survival of surgically treated hip fracture in an Australian regional hospital. Anaesth Intensive Care, 2005. 33(6): p. 749-55.
167. Farahmand BY, Michaelsson K, Ahlbom A, Ljunghall S, Baron JA, Survival after hip fracture. Osteoporos Int, 2005.16(12): p. 1583-90.
168. Sharma H, Vashishtha P, Sharma R, Gender differences inpatients with hip fracture: a greater risk of morbidity and mortality in men. J Orthop Trauma, 2005. 19(5): p. 365-6; author reply 366.
169. Robbins JA, Biggs ML, Cauley J, Adjusted mortality after hip fracture: From the cardiovascular health study. J Am Geriatr Soc, 2006. 54(12): p. 1885-91.
170. Pande I, Scott DL, O'Neill TW, Pritchard C, Woolf AD, Davis MJ, Quality of life, morbidity, and mortality after low trauma hip fracture in men. Ann Rheum Dis, 2006. 65(1): p. 87-92.
171. Vidal EI, Coeli CM, Pinheiro RS, Camargo KR Jr., Mortality within 1 year after hip fracture surgical repair in the elderly according to postoperative period: a probabilistic record linkage study in Brazil. Osteoporos Int, 2006.17(10): p. 1569-76.
172. Holt G, Smith R, Duncan K, Finlayson DF, Gregori A, Early mortality after surgical fixation of hip fractures in the elderly: an analysis of data from the Scottish hip fracture audit. J Bone Joint Surg Br, 2008. 90(10): p. 1357-63.
173. Piirtola M, Vahlberg T, Lopponen M, Raiha I, Isoaho R, Kivela S J, Fractures as predictors of excess mortality in the aged-a population-based study with a 12-year follow-up. Eur J Epidemiol, 2008. 23(11): p. 747-55.
174. von Friesendorff M, Besjakov J, Akesson K, Long-term survival and fracture risk after hip fracture: a 22-year follow-up in women. J Bone Miner Res, 2008. 23(11): p. 1832-41.
175. de Luise C, Brimacombe M, Pedersen L, Sorensen HT, Comorbidity and mortality following hip fracture: a population-based cohort study. Aging Clin Exp Res, 2008. 20(5): p. 412-8.
176. Haleem S, Lutchman L, Mayahi R, Grice JE, Parker MJ, Mortality following hip fracture: trends and geographical variations over the last 40 years. Injury, 2008. 39(10): p. 1157-63.
177. Holt G, Smith R, Duncan K, Hutchison JD, Gregori A, Gender differences in epidemiology and outcome after hip fracture: evidence from the Scottish Hip Fracture Audit. J Bone Joint Surg Br, 2008. 90(4): p. 480-3.
136
178. Panula J, Pihlajamaki H, Savela M, Jaatinen PT, Vahlberg T, Aarnio P, Kivela SL, Cervical hip fracture in a Finnish population: incidence and mortality. Scand J Surg, 2009. 98(3): p. 180-8.
179. Vestergaard P, Rejnmark L, Mosekilde L, Loss of life years after a hip fracture. Acta Orthop, 2009. 80(5): p. 525-30.
180. Forte ML, Virnig BA, Swiontkowski MF, Bhandari M, Feldman R, Eberly LE, Kane RL, Ninety-day mortality after intertrochanteric hip fracture: does provider volume matter? J Bone Joint Surg Am, 2010. 92(4): p. 799-806.
181. Kannegaard PN, Van Der MS, Eiken P, Abrahamsen B, Excess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survival. Age Ageing, 2010. 39(2): p. 203-9.
182. Kanis JA, Oden A, Johnell O, De Laet C, Jonsson B, Oglesby AK, The components of excess mortality after hip fracture. Bone, 2003. 32(5): p. 468-73.
183. Zuckerman JD, Skovron ML, Koval KJ, Aharonoff G, Frankel VH, Postoperative complications and mortality associated with operative delay in older patients who have a fracture ofthe hip. J Bone Joint Surg Am, 1995. 77(10): p. 1551-6.
184. Simunovic N, Devereaux PJ, Sprague S, Guyatt GH, Schemitsch E, Debeer J, Bhandari M, Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. CMAJ, 2010. 182(15): p. 1609-16.
185. First ever common benchmarks will allow Canadians to measure progress in reducing wait times.2008; Available from: http://www.health.gov.on.ca/english/media/news releases/archives/nr 05/nr 12120 5.html.
186. Health Canada, A 10-year plan to strengthen healthcare. 2008; Available from: http://vvvvw.hc-sc.gc.ca/hcs-sss/delive-T-restatiorL/fptcollab/2004-fmm-ipm/nr-cp 9 16 2 e.html.
187. Kesmezacar H, Ayhan E, Unlu MC, Seker A, Karaca S, Predictors of mortality in elderly patients with an intertrochanteric or a femoral neck fracture. J Trauma, 2010. 68(1): p. 153-8.
188. Shiga T, Wajima Z, Ohe Y, Is operative delay associated with increased mortality of hip fracture patients? Systematic review, meta-analysis, and meta-regression. Can J Anaesth, 2008. 55(3): p. 146-54.
189. Leung F, Lau TW, Kwan K, Chow SP, Kung AW, Does timing of surgery matter in fragility hip fractures? Osteoporos Int, 2010. 21(Suppl 4): p. S529-34.
190. Carpintero P, Lopez P, Leon F, Fluch M, Montera M, Aguilera C, Men with hip fractures have poorer nutritional status and survival than women: a prospective study of 165patients. Acta Orthop, 2005. 76(3): p. 331-5.
191. Lyles KW, Colon-Emeric CS, Magaziner JS, Adachi JD, Pieper CF, Mautalen C, Hyldstrup L, Recknor C, Nordsletten L, Moore KA, Lavecchia C, Zhan J, Mesenbrink P, Hodgson PK, Abrams K, Orloff JJ, Horowitz Z, Eriksen EF, Boonen S, Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med, 2007. 357(18): p. 1799-809.
192. Kroth PJ, Murray MD, McDonald CJ, Undertreatment of osteoporosis in women, based on detection of vertebral compression fractures on chest radiography. Am J Geriatr Pharmacother, 2004. 2(2): p. 112-8.
137
193. Majumdar SR, Kim N, Colman I, Chahal AM, Raymond G, Jen H, Siminoski KG, Hanley DA, Rowe BH, Incidental vertebral fractures discovered with chest radiography in the emergency department: prevalence, recognition, and osteoporosis management in a cohort of elderly patients. Arch Intern Med, 2005. 165(8): p. 905-9.
194. Berger C, Goltzman D, Langsetmo L, Joseph L, Kreiger N, Tenenhouse A, Davison KS, Josse RG, Prior JC, Hanley DA, Peak bone mass from longitudinal data: implications for the prevalence, pathophysiology, and diagnosis of osteoporosis. J Bone Miner Res, 2010. 25(9): p. 1948-57.
195. Lane NE, Epidemiology, etiology, and diagnosis of osteoporosis. Am J Obstet Gynecol, 2006. 194(2 Suppl): p. S3-11.
196. Pike C, Birnbaum HG, Schiller M, Sharma H, Burge R, Edgell ET, Direct and indirect costs of non-vertebral fracture patients with osteoporosis in the US. Pharmacoeconomics, 2010. 28(5): p. 395-409.
197. Shi N, Foley K, Lenhart G, Badamgarav E, Direct healthcare costs of hip, vertebral, and non-hip, non-vertebral fractures. Bone, 2009. 45(6): p. 1084-90.
198. Bessette L, Jean S, Lapointe-Garant MP, Belzile ÉL, Davison KS, Ste-Marie LG, Brown JP, Direct medical costs attributable to peripheral fractures in Canadian post-menopausal women. Osteoporos Int, 2011.
199. Jutte DP, Roos LL, Brownell MD, Administrative record linkage as a tool for public health research. Annu Rev Public Health, 2011. 32: p. 91-108.
200. Becker DJ, Yun H, Kilgore ML, Curtis JR, Delzell E, Gary LC, Saag KG, Morrisey MA, Health services utilization after fractures: evidence from Medicare. J Gerontol A Biol Sci Med Sci, 2010. 65(9): p. 1012-20.
201. Sirois MJ, Cote M, Pelet S, The burden of hospitalized hip fractures: patterns of admissions in a level I trauma center over 20 years. J Trauma, 2009. 66(5): p. 1402-10.
202. Plan ministériel de surveillance multithématique, volet maladies chroniques du thème 1 «Habitudes de vie, comportements et maladies chroniques». 2008, Ministère de la Santé et des Services sociaux. Institut national de santé publique du Québec.
203. Leslie WD, Lix LM, Yogendran MS, Validation of a case definition for osteoporosis disease surveillance. Osteoporos Int, 2011. 22(1): p. 37-46.

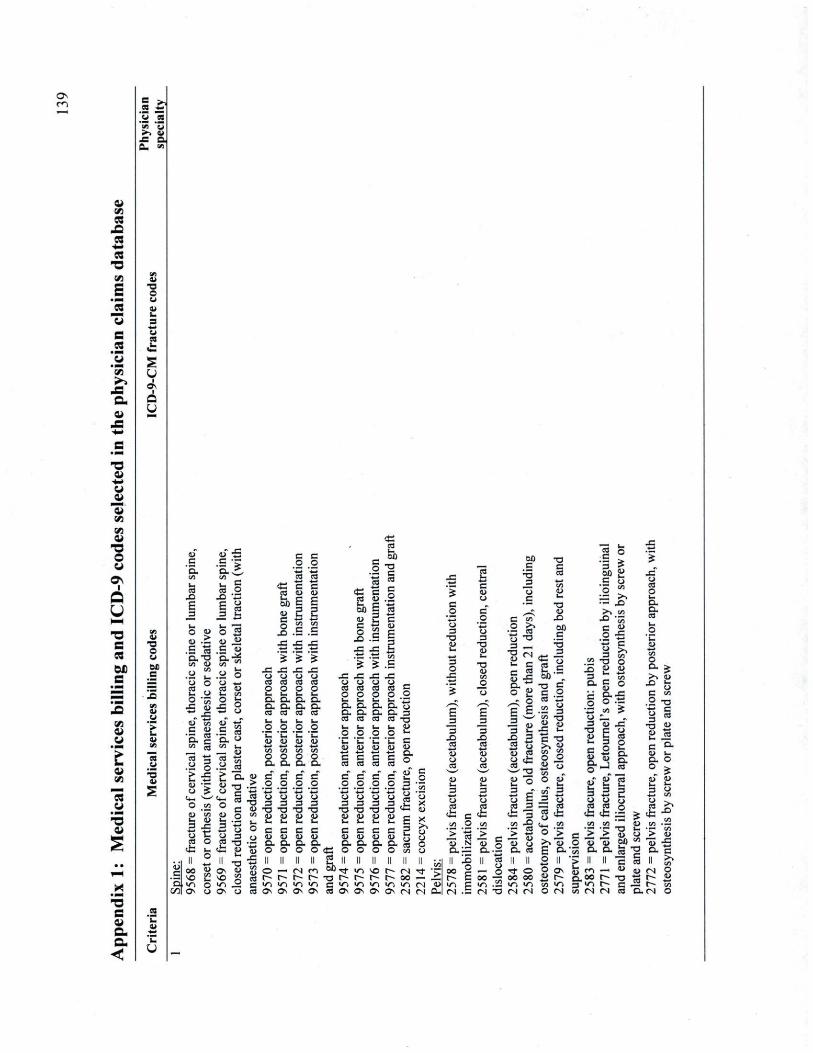
a Vi CQ
mO CQ
■ f c
CQ X ) un en
Ci
£ o • M u CQ D
fa d 3 4fc4>
e u
S £ 'Z> s *5 u >_ 1
_e Os
a à u v _e
■o o
wi a>
■a o o i
a u M X . S CQ bfi s a»
t »
"3
3 s a a.
4>> U
■ a o C i M) e
C3
■5
c
X )
O U> a >
.s 1 g"S .a " I S fa u o - |
■S i> *J, J S Ci t o
■S s _#< ss
11 <u - g
Cfa ^ O VJ
t ' I VJ ,_ C 53 o
X "B S u * ^ ±3 fa r a
o S a _a c a>
' 5 . - *
o o 5 S ■4—> ■■—
C C C CC C i C i fa su
B B OJ 11 o
X .£ .S
c/_ to s s a .2 ô o « eu Ci fa C/
•fi R c i W 4 ^ O
.S ca a « CO fa
— Ci
11
ZJ CS
e D . Q . S
x : o C3
£ D . O . CS
-n o o c a. C L es
il *_ c g es u . 2 fa c ■*—• M E S K C C o S a _o .S S j s JS É .SJS ."t_ en 5 £ .8
. 3 C A JS Ci Ci Ci Ci Cm Cm Cd Cd Ë O O O O O
es
? I % 1) • o c o c •a o 2 "15
T 3 3 fa Ci
.2 .2 .2 .2 'c 'C 'n *fa S B B B t o t o t . t . JS JB
D. a. es fa o
'fa B c es
O . D . a. G. es es
fa fa O o
fa O . 9
ZJ VJ fa c j 3 JS es O
cb fa M O
0 0 «>
rv » E C/_f Os u
5 T3 .2 <fa es .2
SS Ci
2 o <"
i l ë g-g .2 et g B Il mZS
W l _ 2 C Ov o es
> o ô _o o CJ 3 •o c fa c D Q . o
2_ c 6 D . o
SS n ■ o r C >£} es Os
c c CS cs
c c o o o u 3 3
■o a Ci a fa fa e c u <_> o . a . o o
e1> s
3
es T 3 fa V O m*
'fa c
1* c g g .2 f ' S « S a 3 ,2 X 7 3 c e D
3 O
E _ 3 3
■s (D O es
t_ <u
3 X ) CS Jâ-<u o cs
c H S * O en
VJ v j s o t~ ( N "S " S r r i o o — A IT. V J V J V J ( N d> OS O s O s CN t N Pm
o u es es
cfc c sfa en O co
II | n | oo g — o r B oo — ■ n c i r> . S r s . S ( N O
OÛ
a ' S
IS
SS ç 2 sS T 3 3 __
fa c c J o g
s A O
'B e 3
w
•= u
3 t: D 3 es « •£9 s j D eB 2 * CS
^.y " O
15 efc 3
a S ■E D eu CJ D . es
— fa ■ £ es o e
T .
-a CU
X Su c
o
"2 B S .2 C3 4—*
a I en ■ Q u 5
3 fa B T) cn çn O O
a u S o es
X 3 Q .
o 3
T3
fa C a-v a. o
ii i& . __o
> a
i i 3 en
■O O U u c O B _. Û . S O . t i
"s j_r E I i i eu " «
p fa fa
° 3: > % C i B CL o
3 CJ es
cfc
c > o 0>
•a o.
3 E 2 ° .a ^ O Oû
o §
o CS o fa 5, a. CS
e_> •£3 cn O
_^^ > . CL»
X l fa _ 9 C en
. 2 T 3 t l C 3 "
•S « S ts c o. o ( U ÇLI fa fa 3 v j CJ CS
Uefc 1> en
8 n ■> O y ^ fa •* O O Os
o o o o £ r m i f i m « (N <N O (N
a e n
Q . 0 O
en t N
E_ "9 tN es
•i § CU ( N
a.tN
x
JS c >> •_. o CU
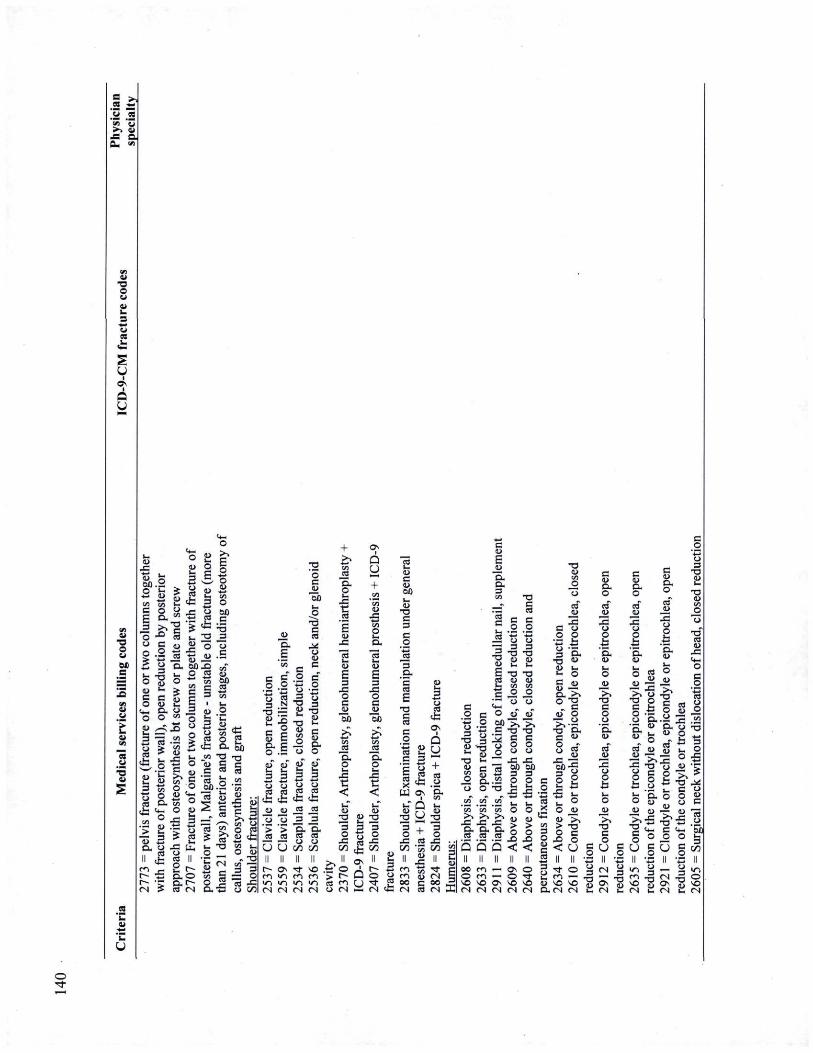
.a .2 'en ' y >> t i
•e ai a.
Ci ■ o o a Ci
u I
Os O U
o
es
■5 a i
. 2 'fa a i
mm 'fa
IU J S
OÛ.2 O fa
en t o
S S B 5. 3 > ,
" S * O C o .2 £ t j t_
3
E £ c o <u
Cfa G . O O U
<*m O
eâ *
g i I a
o •sa <u S D . Çj
es Il efc
? £
> es
ïfc ° __= en ç j "9 'S ca i_
il SX 60 O *T ■ en
£ i o ___ M ô
2 __ .a g
en ^
| s Se! | « O «u _ fa
i 2 S e j
■g fc
es II 2
£ es t N
g g § i •So 3 5 2 °û ca c
« § | a 3
o c .2 û û
+ ? ^ Q M y §■ + g , V J
• S VJ t . IU es J S
O o a .g
X VJ ea t.
IU
c 3
•S en i fa <u JO fa
3 'fa 01
« *: ea O E
8
en T J "o> S C "
•a ! s I
ea i__! y
" •
ea Ç« * | > a
. 2 — fa f N IU s j
' Ç
û û
a
c c .2 2 | I TJ S 2_ S § e o .5
<u X
o fa
a c ca .__ C i C i
ss «
.2 c T J 3 2_ •«
__ i> T J >0) c
s | Û O ^ - -ïï
c <u eu 01
T J C 3 C
,o 3
1 a. 3
en es C L t S
a . . ■ S
u
li O es « . cfc VJ •_. o <u
- TJ VJ " 3
â §
Oj fl} <L> 1> 5 fe B H
3 3 3 3 o o e j c j es es ÇS es
cfc cfc cfc <fc d i q j ro ro
* Ô " o _3 3
">">*& "S ro ro w co — — o o U U oo oo
3 3 C 01 X X CS fa
3 ■ 4 4 O O B fa 3
■ 4 4
B B CJ ZJ B a CS CÛ Oû c
es fc 0 \
cn en C
o 1
Q S es
1 î. o EL SX c 3 '—'
X 2 <
X C <
O) - o CU " 3 3
.sf Il II II II ■>, Il lOv
M î i * « P O J m v j m m > r~ fa.1 v . m ■/. </. es f . CJ t N f N t N t N CJ t N S
11 i __> 2 * fa f N fc
i § Sfc W Ov
ë u § +
X es V J s \ n y
s .2 c il 3 a TJ 3 J > X J ** O)
T J fa 01 C
J I
S.2 JS t j
il § ^ es 0)
| | O o)
i c ,o o 3
T J aj fa
T J <u
T J 01
es 0>
. £ T J
•S 5 O U
___ x ~3 3
_ cn Q O T J S
T J S C
O U
X 0 0 3 P C
1 VJ VI
e n m c i 0 0 c f N es
■V «
_= Il g
4>V 4>V X X ( X SX es es
3 5 tN
tN X
ïï fa cn O
x S .2 x Q <
fa «_ o i W
> a 5 § < ë Il ÇS
c g •2 £ §i 3 O .
O o> •u fa fa O C CJ l s °.^ eu o
T J O . C 0> H mf f j CS
y>g x
é ■ f c fa
fa 5 O Ci Ci l s
i: "v 2 c x o < U
c OJ O . o es" 2 X c j O fc SX Ci
> s T J C O u
'5. O) es" 2 x o O
(U O . O es" c j
c 01 Q . O es" 0)
o o
fc 5. Ci
C i o
>> T J C o CJ
'S. IU es"
J U
JS e j
fî
T J S O
U
C i ■ > .
T J
e §5
a . 0) fa
es o
Ci 4>
^ >> fc O
'a.2 Ci SX fa a
^ o C o
gfc * 3 fa D . O eu
0) 0) —
X C> fc T J Cfa C O O
C
o a o <u ^
x .a o „ fc 3 <__ 2 o x
4t
i! T J __ S 01 O C
es CJ
' ô û
w y j
oo e n —< o s o O m — o "3-
^0 O fa *n —- ..-j
s o s o o s s o s o i i s o * o 5 t N t N t N f N f N C X t N f N fa
< 3 ""> 3 - 3 >rt — -g rn -g tN -S O Os vo Os vo fN fa tN C, CN fa fN
O
CQ f a
!__ s "en ' Z s . i i
J S a QL. ">
01 T J O a
S u
i
i o u
01 ■ o o Ol
c
C i
"> fa 01
es ■5 01
fa o i
c ^o '4W
o 3
TJ IU fa
TJ 01
3 O
il o ,2 C en
~ 3 ea o e j c i Su £ 3 3
CZ_ c j Il fe
00 Cm SO TJ i r , c tN ea
C
p CJ 3
T J «J fa C 01 D . O .
S 5 IU 3
x a-°e£ C ■ -
.2 oh il 2 £ .2 c .a 'S. "3 oi *S T J
5 * O fa
X M a g ■_c «
> O)
O Oû
il .2 ô SÛ c fa 01
(g M Il I
O 3 m 75 ^ __ f N . 5
c c .2 .2 4 i mm Ci Ci 3 3
T J T J 0) 0) fa fa
T J T J 01 0) en en
_2 S. *ë j o T J " T J " ea ea eu eu
X X
O o c c .2 .2 « 'ca o u o o
.2 .2 %-» 'mm O O 3 3
T J T J 0) 0) fa fa C C IU 01
a. a. o o
TJ" TJ" cd fl n U U B X X § Cfa l u J S O O —
£ £ 2 .2 .2 ° a a S CJ CJ 3
S 2
o
0> X 3
O
0 1 X
3
es O)
3 O
■S c 'S °
* z -s * a * i S e C en
— 3 es o .2 <u Sb £ fa S 3 3
V J O Il fe
0 0 CL
O S T J <•. C f N es
JH J H o a Ci Ci ss ss
e j e j
3 3 t/_ C/_
— >/-) en v j s o s o fN tN
is a o x g o c
8 'S 9
&| I K 3 TJ O . Ci
•a fe § I Ci VJ _ 2 •fl a ^J en i fa il 33
«V s •S o £ • - SO 3 ? fN X
3 X «fai O > . C
. t . o VJ p P U
J T J 3 S fe g en O .
01
3 S a fe
3
_ 0)
3eg
gô
■S 2 g x fa 01
3 >v
<i .. mm
£ 5 2 s 3 E w <
01 c Ol Oû
a ss JS
o
Os I
û u
c IU
o es
fc 01 o
_eS Q , 01
+ £ T J es 0>
X
es
0) T J fa es 3 >
O C .£ es O g fc [ M ea I3S ' 3 X > X
W Q U
u g PJ Il Ol M
O m m eu t N T f O o o c f N t N t N t N ca t N
e n <J fN g t N fc
C .2 c t j 2 3 o T J 3 g T3
___ U TJ >-
e «■> C • l o | t j O O • 3 IU IU S t; S £. B 3 SS c i c i Ci P S D . f c fc O __en j n c f ca ça 0 ' O Û ' O O E 6 0 6Û ea eu eu fa mm mm 2 <=
c
01 O O
C O
O 3
T J 01 fa
T J 01
3 T J 0) fa
C .2 s & O
c .5
n 01 ■a. o
CJ •
3 » T J 3
2 V,
e j 3
T J Ol
0) fa en T 3 fa 'en
lose
p
en T J
IU en
X lose
p
en
_o S X o
o o CJ
a. 3?^> «v es > v
3 c T J o o c O
O cn en C O 1 3 en
^ 3
fa x x 5 O 3 3 CS CJ
u u a; VJ i i i VJ a> o j Ol J s J u fa JS SX es 3 3 3
mm JS SX es ej cj
ca ea C i es
TJ C 0>
•2-5 \J3 T J o o> 3 • •a o J J CJ c a" <U 3 D . . t _ O X
3 > v O
3 "S 0 § ■cfl
Cfl
3 3 (2 2 0) u fa fa 3 3
es fc B
g.! •XS X
o 3 3 CJ
T J x )
e ■ C § a .2 CX.2 3 O TJ 2 es 5 en fa T J
2 1 * S o 3 3 S
S i l 3 f c » ro _ fe <*_■ _3 U 3
___ w U
1^1 v.f ? 3 3 x 1 1 « ea .22
o o S S o a £ £ £ Ë £ £ a s o fa es 3 CJ N * v J O \ 0 « S O r - O S O S — fN -"S"
— p*» e s r t P • r o o o o o o o s v . i r . u
. > û « \ 0 * i n w , v i i f i i n i t , v O v _ v O C t N f N f N t N t N f N t N t N f N t N t N t N < N es
VJ ( J S : Ci
01 TJ O
O l SJ
u O l
à u
Ci T J O 01 M
Ol Ci
cs p ■5 01
1 3 es C
O _ 3 _ 3 + cU T J 0> en c
01 S X
3 O
1 a j en
£ 0 ) VJ
O o fa T J T J I VJ en"
01
a. a g CS
3 3 T J
c T J T J
'en CD
X X es '5 'o X 3 3
C
' w
C X X to
O
T J
CJ
T J
C
' w
C 3
S 3 g c 3 O o
01
£ § O 3
t j 3 U
en en ^ O g
c 3 O o
IU
fa 3
"ës VJ en T J T . 3 Q . O . U •a es
IU
fa 3 fa
p 3 a j 01 T J <u 0 1 3 o fc 3
CJ 0 )
fa fa eu e j e j T J o fc 3
CS c T J CS fa
T J es fa
T J 01
T J Ol en
fa C 01 a. o en"
<u 01 fa
T J
T J O S
fa Q fc O s
Ol 0 Û fa
01 fa 3
mm n
i 0 ) fa 3
mm
_o CJ
VJ
_o CJ
en"
fa C 01 a. o en"
en" CD C O
X
VJ ID C
o X
0> en
_o c U ZJ —
o +
1
Q y
I U T J C 3
C i 'EL U
p 3 3
en" CD C O
X
VJ ID C
o X #. c n
+ es 'EL es 0 ) 01 fa fa " S + B
fc x fc ■ 5 es
T J es
T J CS fa
O fa o
CS 3 « S.
c 2 en '5
ea '5 "es fa fa fa
fa fa
B E _ 3 3 3
1
• ' 1
fa 0 1 en > v
3 O
I U en 4>V
O
J H
O
J H
O
J H
fa o fa
o Ê 0 ) 11
iu n . 1 o
B X X CJ CJ C i 0 ) O)
Ê 0 ) 11
iu n . E o
O
o. ' 5 . C i
ts X
a. 'S .
01
0 1 c fa o
I U c fa o
0 1
c fa O
3 O
VJ C
^ O
c o en C
TJ" ' 5
en ^ en
3 'fa '5 ?
E o 1
3 o S en
5 II
T J 3 CS
3 p
"3 4 ^
V i
s II
C
T J T J ea ea eu eu X X Il II C
T J CS eu X Il ••
3
ees
U II
t j 3
T J 01 fa
T J
3
et U II
O o 3
T J
S
x | CJ
a n II
X __ (X ca o o
VJ H Il II
K M . fa
Il II OS fa V J CJ
3 T J a_
S O o 3
T J z j
O s p_4 'E , 3
O eo 0 0 01 C N B o e n Os 0 0 m Q E en
CJ 3
T J a_
m o 3
T J z j
so S O 'E , 3 r 'C — VJ
O a 01 C N » O en m Q E r
CJ 3
T J a_ t ~
o 3
T J z j •r m
'E , 3
r _S S O VJ O S O D . S O S O v * O oo o 4>
t N e t N fa t N C N B . f N s * C N C i tN O ( N f N t N C N N M U.
o c 0)
B B .2 .2 o o 3 3
TJ TJ eu oi fa fa
TJ TJ O) IU en en
_o _o ~ "ë j
3 O
>>§
B fi O o
o 3 3
T J T J IU U fa fa B B Ci 0) a. a. o o
B B es es
eu 01 fi C ea ea
x X O CJ o o
.8.8 fa fa o o
JH JH e j o O) Ci
z z >o oo Os en so so fN tN
O O JH J H o e j CD CD
Z z s o II n ' V J t— 0) — o o 0Û t— SO ea f N t N
J5 SX
TJ
TJ 01
CJ 3
TJ 2_ B 01 a. o
i X CJ o
ëë I l .£
_* o 01
z ȣ. 0) , fa fe rVJ tN
01 >srS
•.n B 'C 'c o
&. _ >, ,>>
VJ X X 2 ^ TJ o ea ca B o> O) ea X X 4 fa fa
s o o
o 01
c c eu o i
c j
T J £ ÇU C i C i •s U CJ c ca ca
SX SX Q " SU
01 mm
.£ fa o
4 _ _ *
o 01
* a Il vU
2 « f N Oû
C C es es
X X o CJ O O
ëë OJ I U D . D .
fa fa O O
_ 5 M e j C i 01 C i
Z z II II
O v o c i ■«r
r t ~ I N t N
I
TJ (U C O) E 01 o
X TJ
J g fa £ o p mm Q .
B S c
3
E VJ Ci (
u .a § _ro w .s o. 2 t> B 3 3 fa en o
. o U O fa fa J fa i
es Q
X g.a 11 a. t . fa o
0) TJ IU 0> Z 3
I I «■>
J L£
0O a i 0 0 o SO C f N 3
ea o o JJ a • P * 'C fc 0 0 «o
S . S R fa 3 S
x £ fc oi ' S 5 en" 3 Z s w II J so i ; r~ t N C X f N
CN «fr
«fr S fcJ 0 3 mm p « S . 01
J = D. eu
Ci T J O CJ
Ol es
.fa
Q U
Ol T J O Ol 0 * C
p ■5 01
.2 'fa C i
'fa U
.2 OÛ mm Vi C e j 3 3 O JH fa fa
01 T J CJ è CJ
O O
T J > T J fa a 01 "cS 01 O 0) 3
OJ CL
IU t s fa 3 en _.
3 OJ CL
en 3 O _o O _o
3 OJ CL _o . O ôb
e j SO o O CJ ■a es fc
01
fa m" .a" vî en" en" fa vi 01 CÛ CS
cy") GA en 'en Ov CD > v
01 CÛ CS >. >v >v >> Q " O
X
01 CÛ CS
X X X X Q 01 C n . _ J
o. D CL a. y fa 3 es 3 S .2 es _ „ c
3 3 C p Oû • — *
C T J X ) T J T J C " O + CJ
CS
fc 2
T J ts D .
T J T J T J 2 S VJ CJ CS
fc CS
'5 .s' J3 es '5 'Ô 8 3 en
01 Os 3 > v .s'
>> es
>> > s — ,>. X i Q
p G 01
fa T 3 'an C i
x T J en
C i X
T J T J ■a "» E o
en i
Q e 01
fa 3 O
'an C i
x C O
en C i
X 3 O
C O
■a "» E o
O fa y es E
3
CJ CS
fc O to O to CJ 01 ■a ° SX
es E
3
CJ CS
fc X 3
01 c
X 3
CD C
X 3
X 3
s O O 3 M +
en
T J C CS
3
CJ CS
fc en CS en CS en C en fa en
d . 3 en
T J C CS Ov
fa O
T J 'o >>
w 3 O
X y
"S
fa O
T J '5 > v
3 O
X mm
fa O
r2 'o >v
^O
ts X
>mG
fa O
T J '5 >.
^" fa 0 0 O
.8 TJ
If
X 3 "S c j es
CD X ■44y en O fa S X
C
es C
i Q y + T J fa T J fa T J ~5 " O
^" fa 0 0 O
.8 TJ
If O — E cs .s C O C o C E
01
c
^" fa 0 0 O
.8 TJ
If CS E cs 'en
O X O X O E 01 o .. o "es o X 1)
O en
X CJ en
X CJ en x CJ
en en o
• | a fa o
H W X 3 es fa '1 3
es fa '5 C es fa fa
C CS fa
en o
• | a c E
CD ,e£ p. en
(U C
H II
c" _o i
II fi" .o
1
II o
" c S II 3 H fr II
01
E JJ
ta
ll I X II II
es 13
f CJ 3
T J ZJ
O u 3
T J 01
r i E Ov O o o. o cn Ov fa Ol
oi SO
CJ 3
T J ZJ
Os u 3
T J 01
r~ B OO P Ov CL n «T c Ol c SO
CJ 3
T J ZJ SO
u 3
T J 01
so p V J en i n 3 «t en OO Ol Ol c <N fa rs fa t N p
Os O Os en t N ( N ( N Oû
Ol c
W» _UJ «. Î * _ :
CL
SZ CJ
E I fc
o X
CJ
o 01
CL CS
3 O
(S T J 01
C
,2 O 3
T3 01
'43 O o 3
TJ 0>
C
O es O fa CL
% es X
cS ea Ç = o i =
H
eu 3 (U s s
cL.a a - s SM fa S
O <c o g g S IH fa2 3 fa 3 © 3
t j ° O « [ S es fa ca " ô
l B
C ' S C £ M
ta. g_ta_ w g || u || fa ea
fa 3 _ Os _e O e .2 «r T5 «g £ X _? > * <S __ Os ? t N w H
C O
o 3
a 01
fa T J 01
■Si c j fa^ 3 *-
TJ 3 (U O
3 CJ O fa
i?i_>X C C ' S
o o £ ea ea w 3 3
3 X X X
E E H II II II
>/. v . ^
O f N Os r r s o f N f N f N
mm 3 T3
TJ 2 S_ 6b C 3
8-1 o fc 3
c ,2 o 3
T J OJ
C . o
CJ 3
TJ (U
£ °o c S..S i O J H CL O °
s s O S S p — _eo
S 3 « g x e x B .S «O 3 ?
_2 S 3 .2
o fa •3 "3 ' I E
0)
E .S w * X * 3 O 3 S R S x sox S ooS fa T J fa O p O
X t j _ 3
CD
CL
Pv X CL
'£. Ol
£ x o
_2 3
X US
S o
X
o X
.2 £ 3 •H o Il "3 so Ë Os <U so S f N E
. a w en w .S <u
C O
3 T J 2_ C Ol CL O
3 X
3 O
O X S es .Se. a
CS c o
'5b g m
o
c p mm CJ 3
T J ZJ fa
T ! 01
es en ca
3 j l H c H Il fr II
" " 2 vN os £ os •r. tô >n Os O OS
es SX &> „ JS X
M II
•BÊ £> fa O
tN A tN
O " o i e n
o f ~ w tN
es Oû es fc Vi es fa O en en 3 ■" CD O) C X ca ■■
I i ca c
U ea Il «
O OJ r— eu t N Oû
01 T J O Ol Ol
Ol 05
à S U
I
l Q U
Ci T J O Ol OD
01 0
' > fa 01
T J 01
3 O 01 = a 3 i 0) 5. > .
X c o
T J Oi
TJ OJ
T J
CS 00 cs
3 CD
§ JJ cs u «r rf N
» a a S
£ O £ O fa Ç3
'mm J S P u t s 3 CO CJ
1 &3 B S
c
C f <° a M VJ CL fa 3 o a, 73 - « ao
a a « 3 3 fc ca ca VJ oo oo =3
2 2 °o is ts c en cn • — ca ca T J fa fa 3 O O — en en X 3 3 CD (U Ci *—' C C en ea ca 3 U U en ca ca ca U O f
g> II II II ■ 3 O «fr Os fa en en o .
.fa f r~ t~ CL fN fN CN
C S SX O
3 OJ
CS CJ
T J 3 CS
CS 5b CS fc Vi cs 00
p TJ p
CJ X 0>
— y VJ SJ VJ
C C
C o
o ,p
3 . — ^ o II s
OS § PJ TJ N 2
01 > <u
O <u c O
c" ,2 CJ 3
T J 01 fa
TJ <U Vi p
CJ
CD X
3 p '5 § .• 3 CJ fa — _? __ ^ _
X cs £ ea c
.2 c o 3 . 2 TJ
T J .a TJ cu a cs u T J —
T J CS CS S <- h en X v o y >
S y O O) cfl cfl en c/i 3 3 3 Cfl Cfl Cfl
fe fe fe ro ro ro
* — ■ * — > > — •
ro ro ro 0 M M O <D <D
2 2_> n n n
_ _ CN Q Os C l C i O s o f t~
Cfa CN CN CN
3 ,2
CJ 3
TJ 01
C 2 £ V -2 o mG 3 CJ "S 3 O) T J
C O M
' c c CJ 1 )
3 £ ^ 3 cS eu — i, o i . _
es __ i_ _ — g fi CL 01
C 01 a. o
x a ._• — fc o o
I 0)" c O
3 S 3 S o> . 2
" S 2 Ê S 0> g
3 •*
O r ju ? "3 en cs 3 £ — fa o eu eu O) 3 _ fa es h 5
f f N SO P» t N « f 0 0 0 0 f v j o o o o tN Os tN tN
. 2 'fa 01
T J <U C Q . O O 0 1
X 0 0
O v\
o CJ
~hm SS
VJ . 2 fa en O P C T 3 O fa
fi o c o E cs
fi 3 '3 o <"
X X
a $ g Ol O) E E ' 3 ' 3 Cfl Cfl
JU en c j
_E "> O) JS CL O fa fa O o O) 01 fa fa 3 3
es 3 3 CIJ CL E
3 en X
O o oi <U
fa fa 3 3
X E
, S_ 2 s s CL
- S M CL 3
^ f a es X « e" " 3 fa 3 CS S
a B3 ea ça es c u fc fa fa *-O O TJ u o» 2 fa fa fi 3 3 CC
mm mm a , yv y» "V
01 CL CL 3
ta. ta. ta. ta. ta. ta —
o X fa OJ] 3 3 E > eH O fa > O c M en <u fa fi 3 aj c i x n i fc fa
O Ol a CL
3
3 (B Ë f c
fa o
CL T J ID
' Ô 01 CL
3 X
a a ca 2 3 ts x
fc o ci,'f i fa. fa fa o o o ZJ ZJ ZJ
fa fa fa 3 3 3
■fa. f a f a O O O cs c_ e_
fc fc fc
O O) X £
3 eu o_ fa
o cs fc T J
<D C
fi <u
TJ
T J C CS
eu eu
es
P SX
O 3 JJ o P B
Os Os Ov — >n SO OO O O O O — oo oo oo oo
l l l l o o o o <o SO 00 o © O © — oo oo oo oo
— VJ — tN
VJ
© o — CN
— — — OS v* OO OS O
— — — — f N oo oo oo oo oo
I I I I I o o o o o en * f oo os o oo oo oo oo oo
m — en — tN r o fN fN fN oo oo oo
I I I O O O — tN m t N t N f N 0 0 0 0 0 0
3 2
fc II Os e n « t v j f N f N 0 0 0 0
I I o o « f V J t N CN oo oo
f N 0 0 'JS
y ^ ^ Ë +- SS o c m
CD ' f i P
1.1*1 e
3 J r .s o a.
y ^ ^ E O c o 3 2 ». 2 fi p
'mm 2 ca
! # ! e
3 Jr
•8 o $^ S fi fi o o o
en en en ' ■ > ' > ' >
.£ .£ .£ ca ca ca ._.
US 2 2 s o tN rvO vo t s
mm mm mm 4 - i i
o> CJ
O i t 3 2 7, ■a I S iH".! c
3 JF .£ o a. cn en en
'> '> "> CL CL Q . 3 3 3
3 3 3 r en rn en n C C 3
O O O cs U U U
" 3 II II II en O O vn O
SO r SO O U Ov Ov Ov
o > s 3 £."3 "Ô "Ô 3 t u ta. ta. > Il II II
P fN "0- OS ES i n SO fN U. Os OS Os
<N
«fr T f
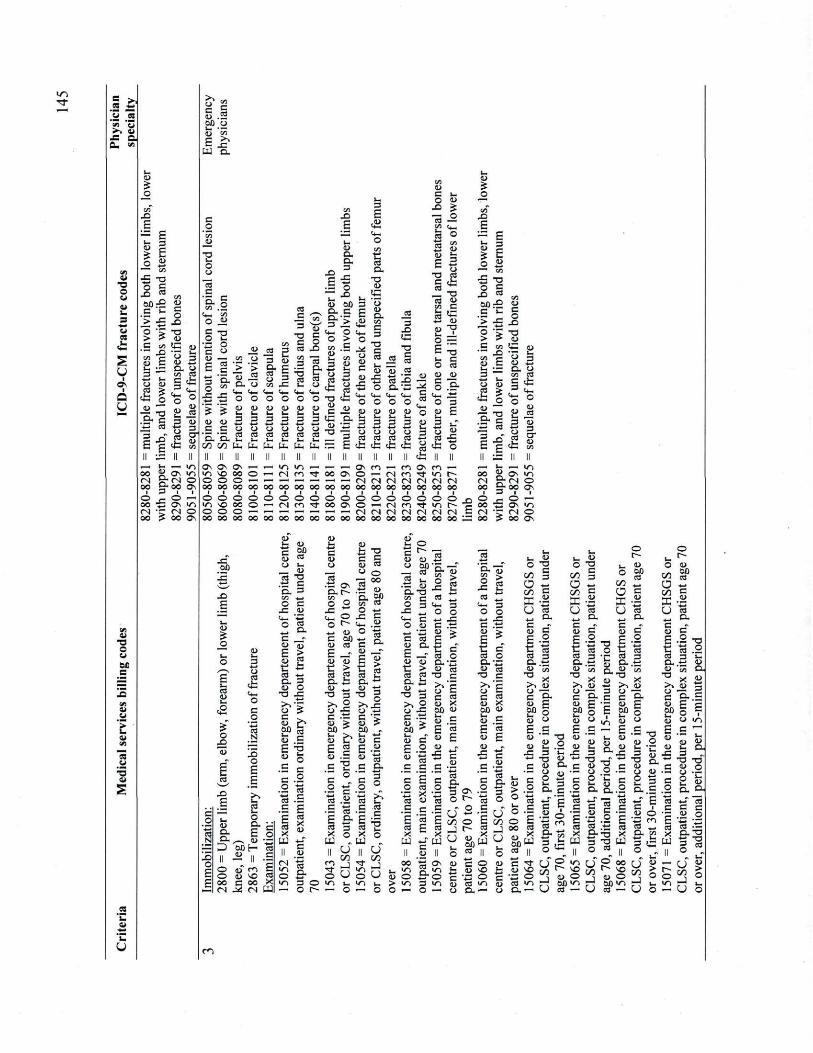
«fr CQ —*
p CS
■>■> C i JS a Cu vi
a T J O Ol 01
fa 3
01
cs
u I
I
Q
u
01 o o 01
> fa 01
cs e j
"S 01
.2 'fa 01
OJ
a o """"
W X )
£ — E B H o
3
tfl X o o E
X es Oû X
c 'fa ■ > X t—t
o > ' i c en
"— X en 0) J fa 3 ■ '
fa O 0> es
fc j2 CD s . a
01 c o
X
T J 01
fc s 3 x S S
U 3 a a CL 2 en ca §fc , <fa O °
(U
11 Ji
1 ï ov m o <N © £•00 os - © m~
•is Os VJ • r tN o ? 00 Os
>v CJ c 01
en C
.2 Su p fa 01 'en E >v
X
faCL
IU CL CL 3
O X
T J 01
01 3 O
X
S ts a> E
T J
i
0)
o
X
£
en 'en
es 3
O JD O 3
3
2 T J fa T J
Ç O VJ T J Ç
C CJ JD es 2 Ol
Ë 3
X
es OJ
E mm 3 •v
"es S
'5. en
en J> CD CL
CJ
> JS CJ
3 CL cs CJ en
2 Ol
Ë 3
X
en 3
T J es fa 5 fr
o X X
'1 'I (U eu C C
'E-'S. Cfl Cfl
o o eu oi
fa fa 3 3 o o es ea
O O
CD IU
H o o a ro 3 èrt
ta. ta. ta. ta. ta. ta — c f c
0) 0 0 3 CJ
Ou CL 3 fa
g J> o
E fa
CD CL VJ ss 3
CS 3
X O
> O fa1
en _g J H T J
i fa 0)
x o
T J CD fa 3
O ca
fc
en CD fa 3 *• CJ es
O CJ C ID
J S
T J
i fa 0)
x o
JS
ts CL
1 CS
X
T J 01 3
fc p
fa o ID
fa O (U
fa O 01
fa o CJ
<*G Ci "B. 3 fa
fa 3
mm 3 T J "31 U CJ CJ o
CJ cs fc
_ T3
es eu __ c I | £3 o 3 E T J fa c O es
3
E 01
Os OS Os 4 — i VJ SO 00 © © © o — oo oo oo oo
l l l l © © © © IO SO oo © © © o — 0 0 OO OO 0 0
- H VS — tN
© © -m fN
— « — I3v « f 00 Ov O 0 0 0 0 0 0 0 0
l l l l © © © o « r oo i3s © OO OO 0 0 o o
cs es es fc fc fc Il II II
en — en —• fN en fN CN CN oo oo oo
■ i i © © © — tN en fN tN fN oo oo oo
Ci O)
fi c__
O £ t. 3 3 2 il fc II Os en « r v j CN CN oo oo
I I o © « r v j CN CN oo oo
JD "g, mm
3 E O)
x
fc T )
° £ _o ca 00 tS C fa j> 3 3 '> > > SS VJ IU c
CJ O)
ea > fc I J. .—' 3- = -D ca
OJ c o
x T J
2 t f a 0)
o S IU fi
& 2 en ca , 'fa o ° 2__2 3 01
m-> - -li cfc i o
r(N oo
i © _Q f" c fN C oo —
fa — V) 2 os io g-IN © g - 00 OS 3 i i
O — fi Os i o r M O ? OO I3v
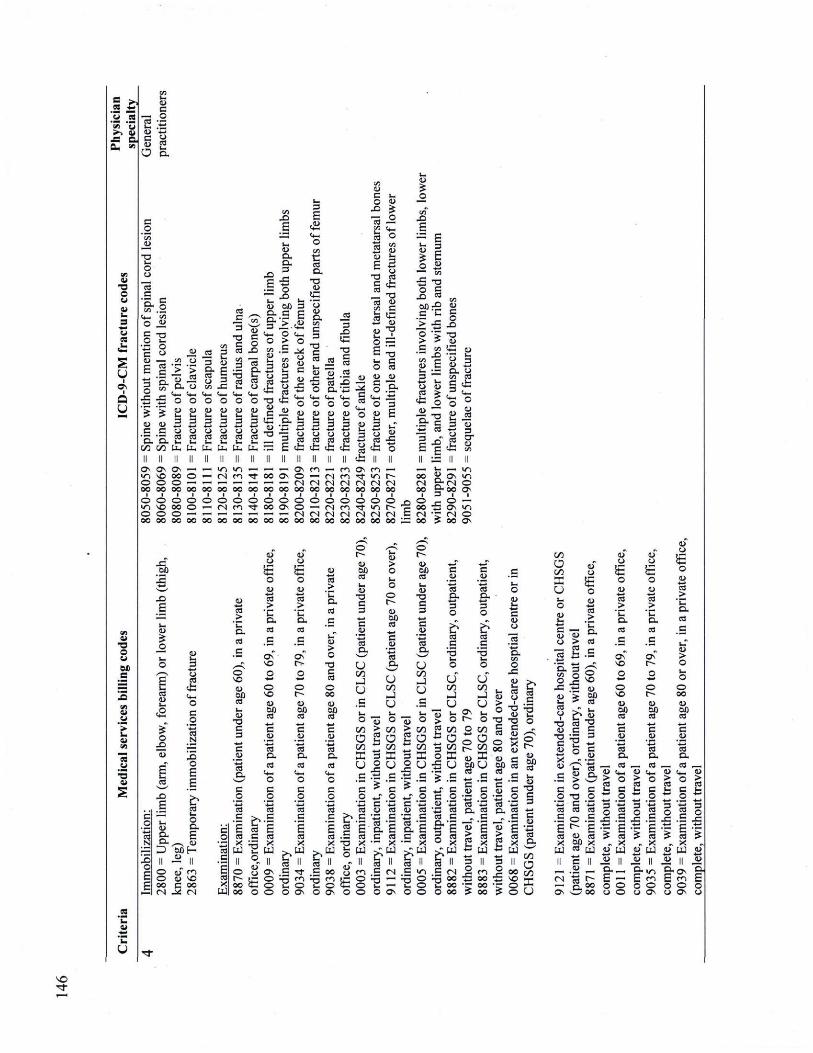
fCQ m m * p M "S ' 3 4>> 01 _= a a.
01 T J O Ol 01
Ol cs .fa
a u
01 ■o o Ci oc c
01 01
es O l
.2 'fa 01
c 13 2 fa .~tS Ci mm C o> u eo O B,
CS C '5. 3
VJ .Si fa en O _2 C O
X E
es C
X E
CD CL
O X
s SX
T J CJ
0 1 c o
X 13 en
i s CJ
8 JH ,—. en " o ea er •r' c > >
• s <o _2 fr a. o _ fa fa
fi o o ' 5 CD eu ? fa fa a i SS S3 d f a —4 C CJ c j
■ S ca ea CL fa fa cfl ta. ta.
en
fi 2 3 Ci
fa fa o O IU 01
fa fa 3 3 O) o ca ea
S. fi 3 O) c3 ea
£fc 0 TJ 01 g 5 .£ 3 fa ■R eu
Oû 3 .£ E >..t&
ta. ta. ta. ta. —
O . C °
■S JH VJ 2 eu Ci fa C ea ,**
y f a fa
fa Q P Ci CL fa
■IG 3 3 £ Ë fc
*__ 3
< " mt
cx _2 __ 3
S x fi
c "S g .2 S OJ ^ .cJ 3 ts x o a ' û
fa fa (4_ o o o
Ci es
fc TJ
CD C
IG 01
T J
01 O)
H fa O
S 3 3 4> S .? ■fa ■" S fa fa K
es fa O JJ 01
T J
p P+G 3 E
i o
? i I 3 '—' en x a *» s j o £ rs cS 0Û:£ C fa > 3 ° S > > C en «■s O) C
O CJ -
cs cs cs fc fc fc
O s O s O s •—i V J SO 00 © © © © — OO OO 0 0 0 0
l l l l © © © © VJ SO 00 © o © © •— oo oo oo oo
X Oû
— vs — CN
© © — CN
mm — i— ov en — c . «fr oo o © — tN en — — — tN fN tN CN 00 oo OO 00 00 00 00
l l l l l l l © © © © © © © «]■ 400 os © i—i tN en — — — CN CN CN CN oo oo oo oo oo oo oo
3 2 i . ca
gfc fc II •Os C . «fr I O CN f N oo oo
■ i © © «fr I O (N tN oo oo
O CJ ea >
fc I •» ro
1°"
» y cfl ro § f c , <fa O °
IU
eu es S 13 il fc s
r 0 0 t N t N oo OO
© X E
© r
X E 0 0
( N
X E CN
0 0 X 0 0
eu O
cs CD
O X
o CS fc fa O c
p ts N
X o Ë Ë
X E i
c p
O) o CL c
o ts CL E c o
.2 CL s s Ci OÛ H es
X II JJ il C
o E
o Ol" en Ë o E o CJ SO cs
E 0 0 ( N JH
0 0 CN
X W
es >
'fa C L
CS C
© SO CD Oû es fa 01
T J C 3
3 01
i CL C O
'mG es C
CJ CJ
h -o B ts >
'fa a, es .g Os" SO
© SO 01 O Û es C 2
'ts CL es
C O
0 1 CJ
o p ts >
'fa a . es c
Ov"
© r
O)
8P c
CD
CL es fa O C
JO ts c
es > 'fa
C L
CS C CD > O
TJ
i o 00 0)
s? m J C ID
'te. CL CS
© t--
CJ Oû CS fa CJ
T J C 3 mm C
.2 'mG es OU cfl J U
es X ta
cs x
fa'U
k II .£ «t O en t . © O Os
c o
1 — »
es c Ë es X
S n £ «> fa © O Os
O Cfl O Cfl X U p c o ca
ç?.B
CJ > o
© <D
S1
t—» c
.2 ts a
U cfl I U fa o
cfl a Cfl X U _g c O
'i c
2 os -o gCN © a oo ov _ © —
fc Os IO T (N O > oo Os
o f
(U m J Oû C ea eu CJ
T J C 3
mm B
.2 ta S U cfl ■_J U B
es 3 3 O
es S
3 . 2 ts fr 3 O
£ es C
TJ
U Cfl 1 U
J o fa <*•> fc O 3 a o X
3 U
OS
U VI 1 U
O 01 fc c 01 o
o X
O)
c
2 cfl
ç cfl
O Û O cs
fa CS CJ o
o "S "S m.-. -2 __ TJ TJ O E
3 es eu s •
S *°0 0 Ci
S .£ £ . £ + _ . .£
CU (J 0 0 es es
CD Oû es
es C Ë
es
es CL p
T J X fa O ta
ll C I
6 C D " CJ
ta
ll C I
es C
e © ©
T J fa o © O
*J o c fi <u ea « 3 ca . CL E c ea
■- x es H C i o "P S t . © o ©
*" E c o a fi
il ° X ■cpq
.S (N a 00 fa oo O 00
c . CJ C
fi 2 ea fi
•3 5 C fa
■a c i
3
C 2 'ta o .
g Ë 2 x fi m 3 n g 1 o K S o O
Cfl
a Cfl _C U o s a
o JS 01 fa es e j i
T J CJ
T J C IU
■ t . X (U
es >
'fa 13 C L > es
S .s
es X
ta.
s S1
.C fe
11 ° c
TJ O C fi es es
O .E < - Ë 2„ « oo x es rjq c (U
CS _> 'fa CL CS Ç
Os" SO
O SO 01 Oû CS mm C
.2 ts CL
OJ o £ o 01 ts >
'fa CL CS c
es >
'fa a. es
p Ov"
c-9 o
IU > o
© r 01 Oû cs 3 eu
ï s.
O 0 0 CJ Oû es c
.2 ts SX
!___« ro _ < a r— ro — W '-*_ U ^ 4 ^ O C4_, 1>
> o > o > o > rt _ cd _ ^ rt fc g fc § fc § fc il es 3 -s es 2 O
x .fa x .5 x .5 x . f i g . f i g .*_ £ S 5 cd S ca ï s S
X X X y oT t_J oT [ j j oT taJ «u 6 i t i « « ï
« . 2 — o — & CN
Os «3SS
= . m gos gJ E _ E c j E ÇQ c o © o © o © o o © o Os ej Os o
SO «fr
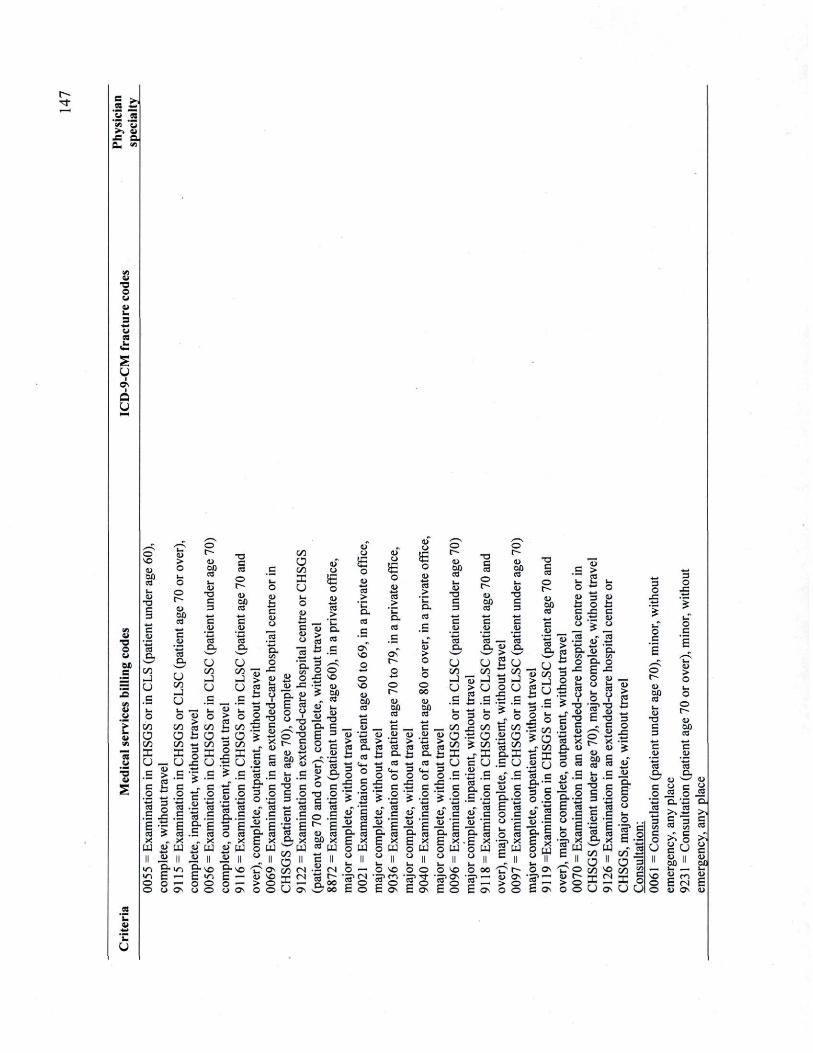
fr»
a . VJ
a TJ O 01 01 fa 3
U i i
a u
01 TJ o 01
B
> fa 01
cs J J
■ 5 Ci
© SO CJ 0Û CS fa Ol
T J c 3
CS O
Cfl ml u p fa o
Cfl O c f l X u
<u > o
© f
01
fa CJ
T J C
© r
01 00 es mm fi
.2 mm CS
a
U Cfl - I O fa — fa P
sz p ta a .
U V J _ ) U
T J C CS
©
<D 0 Û CS mm sz
p fi es a. U Cfl J u
c f l
a Cfl X
ID CJ
£ o
o
P fa 0) fi O 3 sz eu o
IU
i's CJ g ca
• 3 fc C
CS X
UJ
V J
a Cf l X
— o > .8 ca ~ fc £
<u S cfl fc a ■3 Cf l o *
x U
> Cm . fi Cfl
13
o
"3 * fc S g T > o JA x 3 S g * x
^ J IU c ss 5. ea
en _ . __
c j
fa O «J ta > 'C CL CS c
Ov SO
« a fr
.2 fi '5 c _ a .Si
"S E
? ca x
« PJ _•» n
cs ea . 8
3 § ., X
U [ j j O ||
êa g f| 3 E O ea
X p u i a M
fa CO . fa
§ 1 «" c Ë g g 8 rR o PJ U II
CL
£ em o V u T J
« O) © "g f g § ) | sr « fa c CJ — 3
3 § ■ 2
3 y t 2 ©
X so • g IU 15 Oû
y ca 01 fa
01 o
£ o (U ts >
*fa CL es c
Ov"
<u CJ
£ o CD
4W CS >
' fa Q . cs C
© r
01 0 0 es fa Ol
T J C
T J C CS
©
01 Oû CS
CD > O
01 O) JJi T J CL C
© SO 01 Oû es
C a
Ci fi > CS ça C L
fc
fi o © t"~4
CJ Oû es
© oo 01 Oû es
g-io g-so E — £ vs o — o o U OS o o
■ s o ^ a a "mm E — a so o — > © O Os O ©
fi s •Si fi
3 2 « CL x
ww
rt n
X X*
U as
fa es eu CL > w
° C T J O C fi es es O .£ ^ E B . ca o û x eo a j
01
C ? o o
ca fi fa ° 2 I s « c fi
ra
— £ g a Ë ,*, o PJ <> n
_ c IU p ea « fi CL mm CO
11 « c s g g g E x 5 PJ <J II
_ c IU o> > fi ea es fi omm CO g « J S o fi c i 2 g g 3 i g a Ë rï. O PJ 0) n
c .2 ts a. U rt __ •—J 13
Ë fi fe t i
° § — vV X
g O fi
fc I . j 3 _ U o .£ s
X _ eo . f i
3 CL £ .2 .g ta
eu c <U mm . 3 -C"
g. i g. £ x E o P J o y v r v
.2 « — fr > îfc °_ ri
3
c s
o rOl o û es fa 01
T ! C 3
3 .2 mm CS CL
O — O SO
ÏSÏ8 fc © E C3S
O o IS? «fr
E o s
O SO o S? g •S' E © E
cfl E O 2 ¥ 3 X sx U .£ .8 » c tu
.2 3 . 3 Ë c o 1 s * • § > PJ g Il
oo e — > Os O
U rt 13 J > U g c fc '• 1 ° x
Cfl fi O ? Cfl ,
U «3
3 3 g g
PJ S « 2
r O
if o E
T J c CS
© r
t>
eo CS
fi 4> ea > o, 5 u * Cfl 3
u 3 .£ ? fa mm
O fi cfl .2 O ta cfl p. X S U o c u"
' a î o a.
fi £ n o
es 3 CJ £ m. 3 .2 x ca ffl £
— i > — > Os O
£ > ~ es fa fa fa O ° O 0) 3 IU fc O fc C X C o> .fi a> o > o
I «J CL U CL en _ en O g . O
X g X eu O <u
i £ i V o ¥
T J = > T 3 OJ 2 Ol
T J E T J C c U —v Ci
mm ^ s mm x f C x Ci a
g &g eo ea " C fa C .— u C T J c O g O
' C 3 '5
| g.E Ë fi Ë eo 2 « X O X
II g II O r f l s o
S x ™ O U OS
3 o
X
CL
© r
CJ 0 0 ea fa CJ
T J c 3
c J J
t s a .
c o
o
"f £ Ë 2 O rt r X o U U
3 o
X
o 3
<U > O fa o
©
01 Oû CS
c .2 mm es CL
O) s s o c 2
2 o j . C L ' f i CL
' >s c
es
O c CD Oû
>>f i fi 73 eo g
ëô
E CN E
fa 01
O
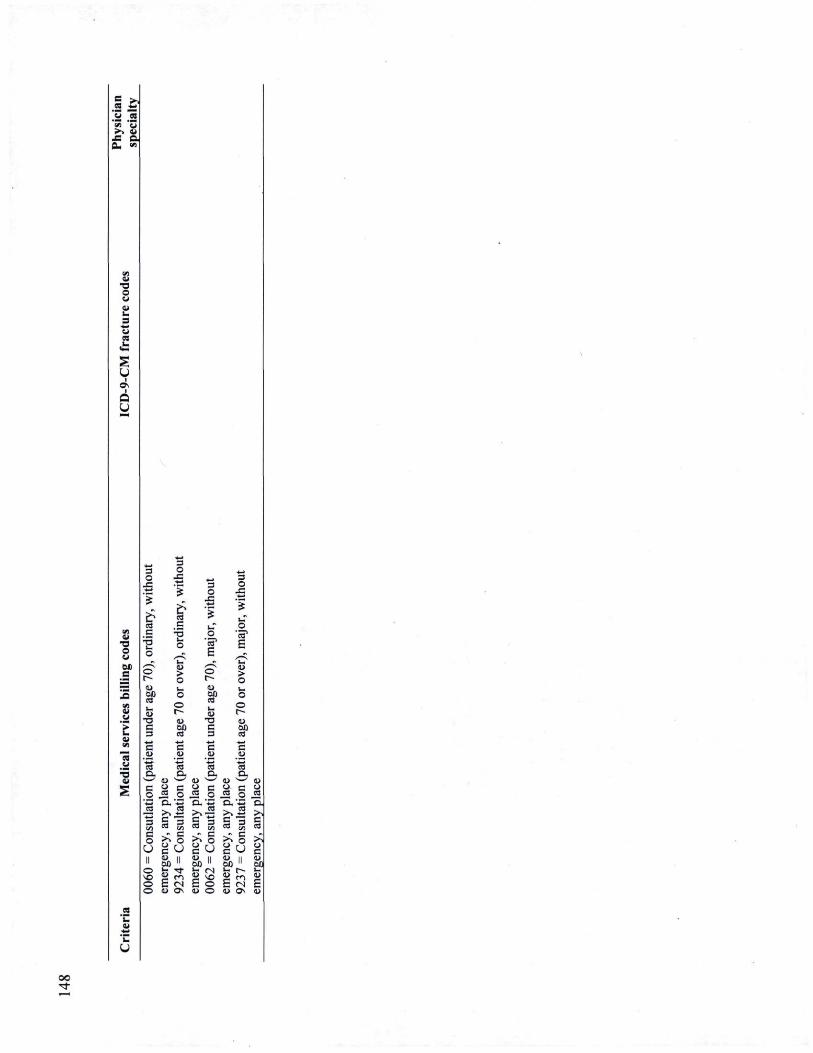
.a .2 'en * o ■>. V £ a O. -
01 T J O Ol
Ol es
û
01 T J O CJ
cs p T J 01
3 O 3
o
I c
T J fa O
3 O
X
3 O
X
ea c
1 o o" •f» o> 0 0 CO
fa CJ
T J c
•3 *
01 > o
© CJ 0Û es
■ * -
3 CD
O "S
1
Ë s s O r~ o i 00 es fa 01
T J C 3
■II C 0)
o •g
1
Ë
01 > O
©
01 0 0 es
mm c <u
•a CL
a s s 9 c CS o a' i
• > s f i
g S gu eu M 00 " ïi en E <N IU O s
es CL
01 v — y
CJ C CS O CL 'zz ,>» JS C CS
+* SJ en
>. C O
CJ
c U 01 II 00 II
fa <N 01
E SO 01
E © Ol ©
ts CL
U s_j j , u c U co o S c 73 c ea S « .» c .« ■>> O > s ss s J ss IU M u oo " OÛ fa r ^ fa
E CN E O) OS 01
00 «t
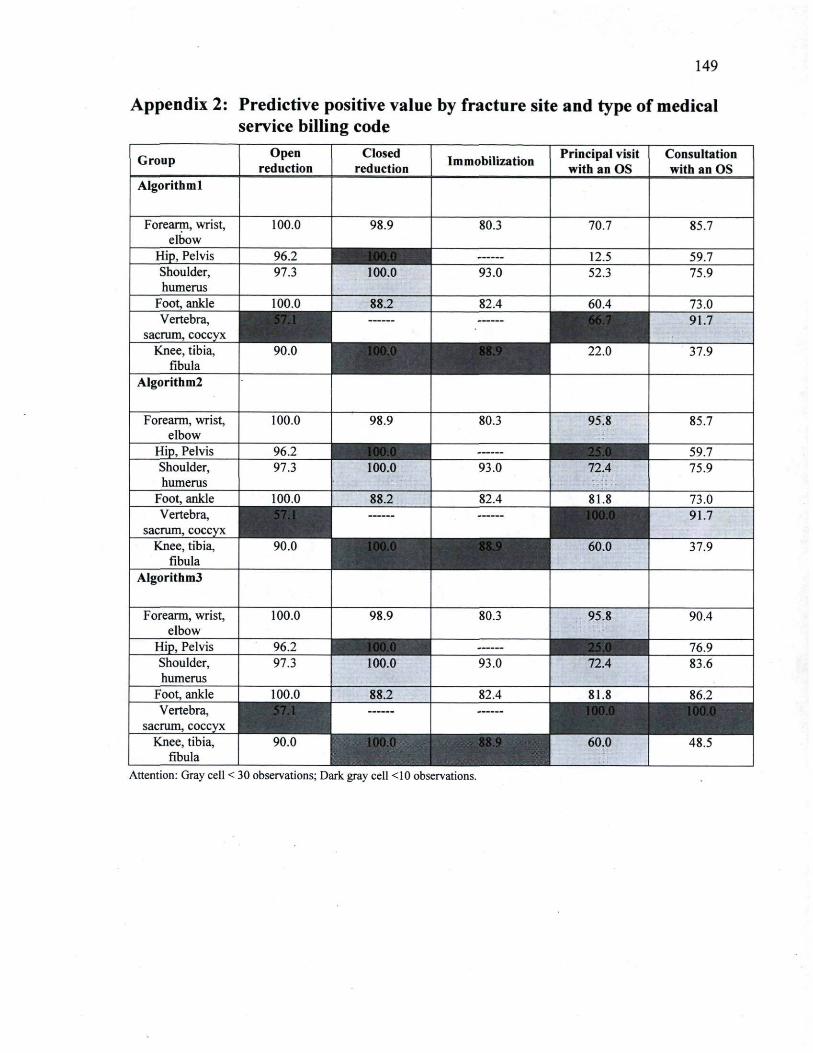
149
Appendix 2: Predictive positive value by fracture site and type of medical service billing code
Group Open reduction
Closed reduction Immobilization Principal visit
with an OS Consultation with an OS
Algorithm.
Forearm, wrist, elbow
100.0 98.9 80.3 70.7 85.7
Hip, Pelvis 96.2 100.0
12.5 59.7 Shoulder, humerus
97.3 100.0 93.0 52.3 75.9
Foot, ankle 100.0 88.2 82.4 60.4 73.0 Vertebra,
sacrum, coccyx 91.7
Knee, tibia, fibula
90.0 22.0 37.9
Algorithm!
Forearm, wrist, elbow
100.0 98.9 80.3 95.8 85.7
Hip, Pelvis 96.2 59.7 Shoulder, humerus
97.3 100.0 93.0 72.4 75.9
Foot, ankle 100.0 88.2 82.4 81.8 73.0 Vertebra,
sacrum, coccyx 91.7
Knee, tibia, fibula
90.0 60.0 37.9
Algorithm3
Forearm, wrist, elbow
100.0 98.9 80.3 95.8 90.4
Hip, Pelvis 96.2 76.9 Shoulder, humerus
97.3 100.0 93.0 72.4 83.6
Foot, ankle 100.0 88.2 82.4 81.8 86.2 Vertebra,
sacrum, coccyx Knee, tibia,
fibula 90.0 100.0 60.0 48.5
Attention: Gray cell < 30 observations; D-ark gray cell <10 observations.
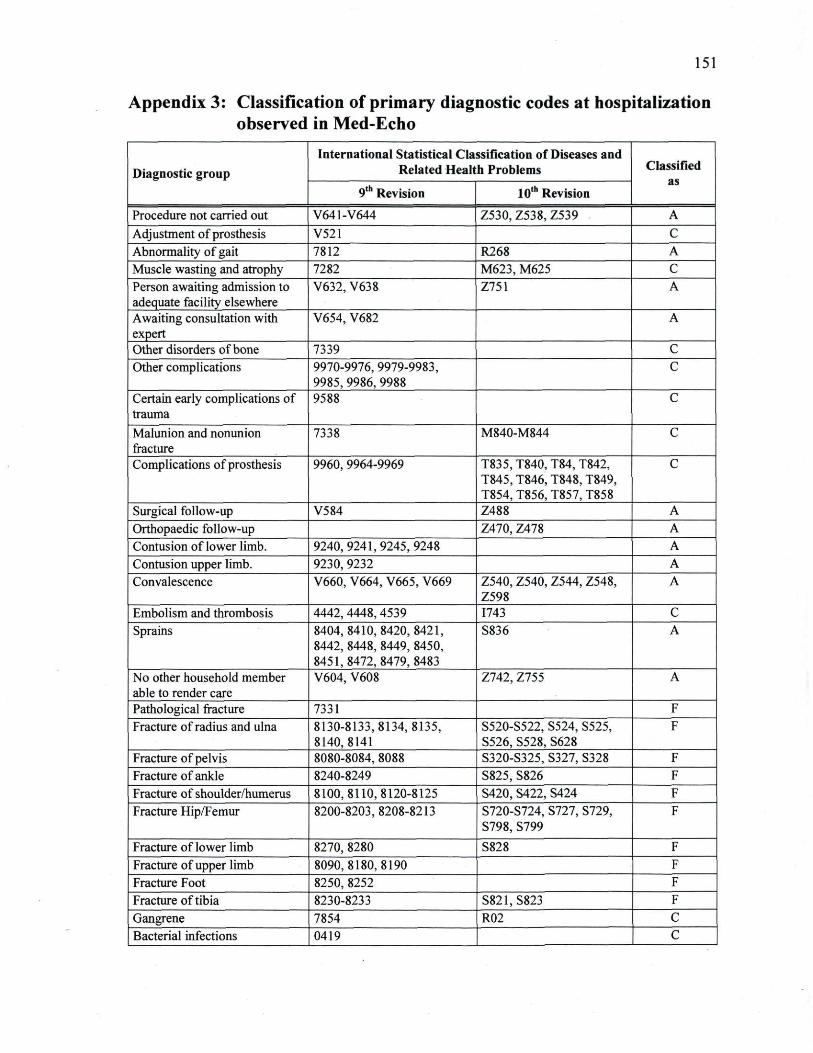
151
Appendix 3: Classification of primary diagnostic codes at hospitalization observed in Med-Echo
Diagnostic group International Statistical Classification of Diseases and
Related Health Problems Classified as Diagnostic group
9th Revision 10th Revision
Classified as
Procedure not carried out V641-V644 Z530, Z538, Z539 A Adjustment of prosthesis V521 C Abnormality of gait 7812 R268 A Muscle wasting and atrophy 7282 M623, M625 C Person awaiting admission to adequate facility elsewhere
V632, V638 Z751 A
Awaiting consultation with expert
V654, V682 A
Other disorders of bone 7339 C Other complications 9970-9976, 9979-9983,
9985, 9986, 9988 C
Certain early complications of trauma
9588 c Malunion and nonunion fracture
7338 M840-M844 c Complications of prosthesis 9960, 9964-9969 T835, T840, T84, T842,
T845, T846, T848, T849, T854, T856, T857, T858
c
Surgical follow-up V584 Z488 A Orthopaedic follow-up Z470, Z478 A Contusion of lower limb. 9240,9241,9245,9248 A Contusion upper limb. 9230, 9232 A Convalescence V660, V664, V665, V669 Z540, Z540, Z544, Z548,
Z598 A
Embolism and thrombosis 4442,4448,4539 1743 C Sprains 8404, 8410, 8420, 8421,
8442, 8448, 8449, 8450, 8451,8472,8479,8483
S836 A
No other household member able to render care
V604, V608 Z742, Z755 A
Pathological fracture 7331 F Fracture of radius and ulna 8130-8133,8134,8135,
8140,8141 S520-S522, S524, S525, S526, S528, S628
F
Fracture of pelvis 8080-8084, 8088 S320-S325, S327, S328 F Fracture of ankle 8240-8249 S825, S826 F Fracture of shoulder/humerus 8100,8110,8120-8125 S420, S422, S424 F Fracture Hip/Femur 8200-8203,8208-8213 S720-S724, S727, S729,
S798,S799 F
Fracture of lower limb 8270, 8280 S828 F Fracture of upper limb 8090,8180,8190 F Fracture Foot 8250, 8252 F Fracture of tibia 8230-8233 S821,S823 F Gangrene 7854 R02 C Bacterial infections 0419 C
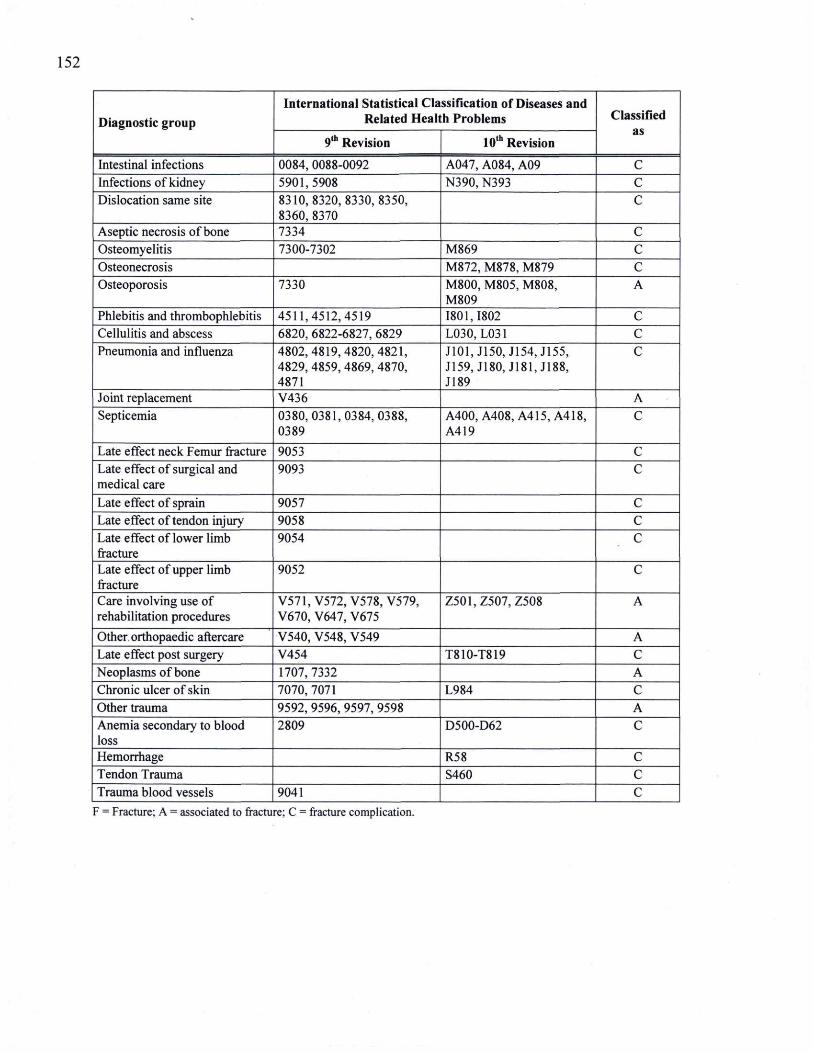
152
Diagnostic group International Statistical Classification of Diseases and
Related Health Problems Classified as Diagnostic group
9th Revision 10th Revision
Classified as
Intestinal infections 0084, 0088-0092 A047, A084, A09 C Infections of kidney 5901, 5908 N390, N393 C Dislocation same site 8310,8320,8330,8350,
8360, 8370 c
Aseptic necrosis of bone 7334 c Osteomyelitis 7300-7302 M869 c Osteonecrosis M872, M878, M879 c Osteoporosis 7330 M800, M805, M808,
M809 A
Phlebitis and thrombophlebitis 4511,4512,4519 1801,1802 C Cellulitis and abscess 6820, 6822-6827, 6829 L030, L031 C Pneumonia and influenza 4802,4819,4820,4821,
4829, 4859, 4869, 4870, 4871
J101.J150, J154,J155, J159, J180, J181, J188, J189
C
Joint replacement V436 A Septicemia 0380,0381,0384,0388,
0389 A400, A408,A415,A418, A419
C
Late effect neck Femur fracture 9053 C Late effect of surgical and medical care
9093 C
Late effect of sprain 9057 C Late effect of tendon injury 9058 C Late effect of lower limb fracture
9054 C
Late effect of upper limb fracture
9052 C
Care involving use of rehabilitation procedures
V571, V572, V578, V579, V670, V647, V675
Z501,Z507, Z508 A
Other, orthopaedic aftercare V540, V548, V549 A Late effect post surgery V454 T810-T819 C Neoplasms of bone 1707, 7332 A Chronic ulcer of skin 7070,7071 L984 C Other trauma 9592, 9596, 9597, 9598 A Anemia secondary to blood loss
2809 D500-D62 C
Hemorrhage R58 C Tendon Trauma S460 C Trauma blood vessels 9041 C
F = Fracture; A = associated to fracture; C = fracture complication.
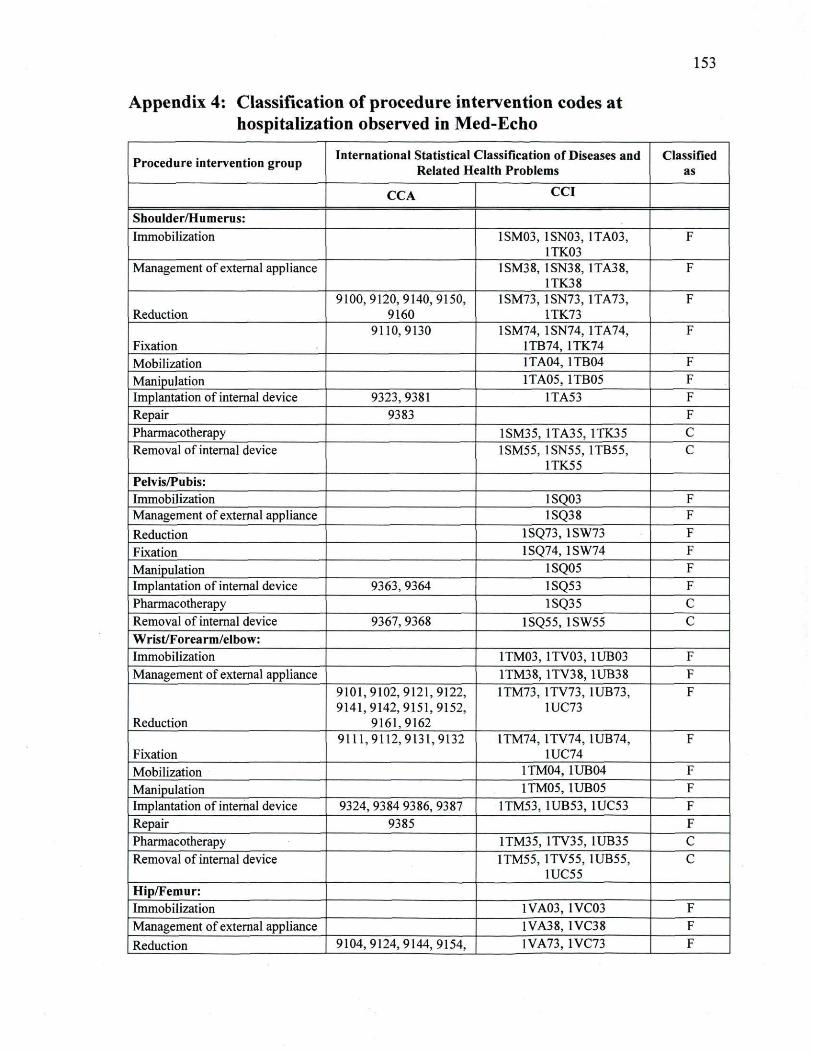
153
Appendix 4: Classification of procedure intervention codes at hospitalization observed in Med-Echo
Procedure intervention group International Statistical Classification of Diseases and Related Health Problems
Classified as
CCA CCI
Shoulder/Humerus: Immobilization 1SM03, 1SN03, 1TA03,
1TK03 F
Management of external appliance 1SM38, 1SN38, 1TA38, 1TK38
F
Reduction 9100,9120,9140,9150,
9160 1SM73, 1SN73, 1TA73,
1TK73 F
Fixation 9110,9130 1SM74, 1SN74, 1TA74,
1TB74, 1TK74 F
Mobilization 1TA04, 1TB04 F Manipulation 1TA05, 1TB05 F Implantation of internal device 9323,9381 1TA53 F Repair 9383 F Pharmacotherapy 1SM35, 1TA35, 1TK35 C Removal of internal device 1SM55, 1SN55, 1TB55,
1TK55 C
Pelvis/Pubis: Immobilization 1SQ03 F Management of external appliance 1SQ38 F Reduction 1SQ73, 1SW73 F Fixation 1SQ74, 1SW74 F Manipulation 1SQ05 F Implantation of internal device 9363, 9364 1SQ53 F Pharmacotherapy 1SQ35 C Removal of internal device 9367, 9368 1SQ55, 1SW55 C Wrist/Forearm/elbow: Immobilization 1TM03, 1TV03, 1UB03 F Management of external appliance 1TM38, 1TV38, 1UB38 F
Reduction
9101,9102,9121,9122, 9141,9142,9151,9152,
9161,9162
1TM73, 1TV73, 1UB73, 1UC73
F
Fixation 9111,9112,9131,9132 1TM74, 1TV74, 1UB74,
1UC74 F
Mobilization 1TM04, 1UB04 F Manipulation 1TM05, 1UB05 F Implantation of internal device 9324, 9384 9386, 9387 1TM53, 1UB53, 1UC53 F Repair 9385 F Pharmacotherapy 1TM35, 1TV35, 1UB35 C Removal of internal device 1TM55, 1TV55, 1UB55,
1UC55 C
Hip/Femur: Immobilization 1VA03, 1VC03 F Management of external appliance 1VA38, 1VC38 F Reduction 9104,9124,9144,9154, 1VA73, 1VC73 F
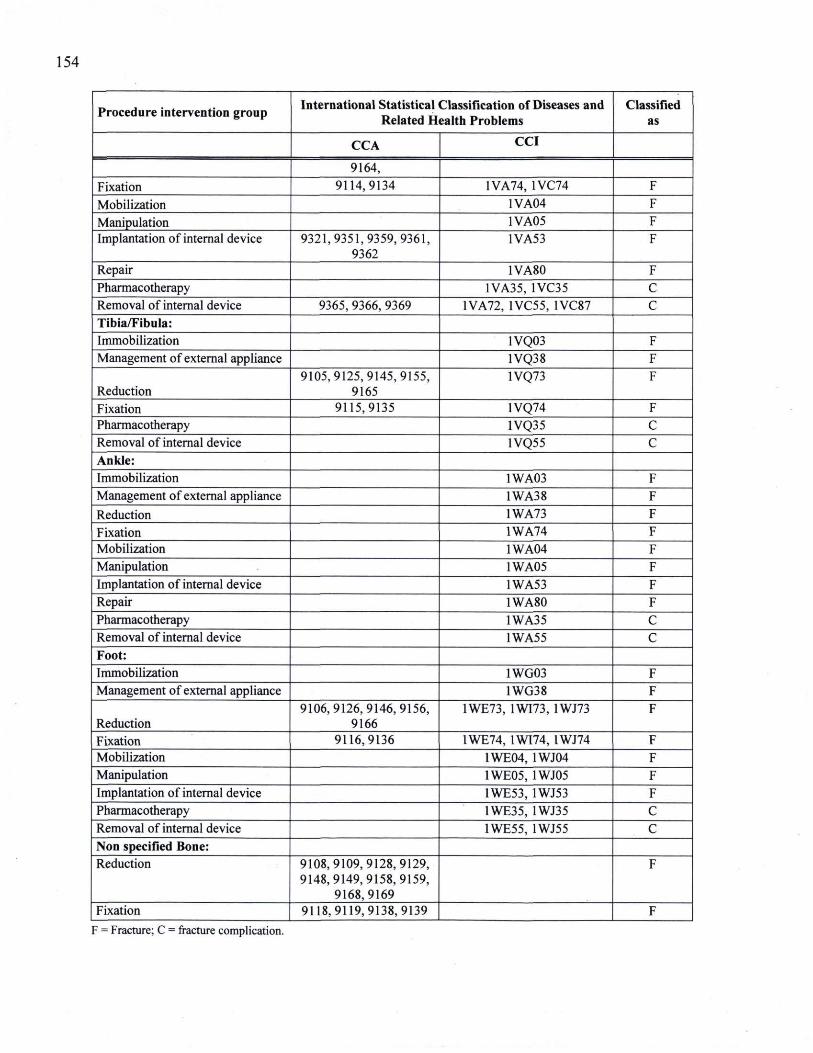
154
Procedure intervention group International Statistical Classification of Diseases and Related Health Problems
Classified as
CCA CCI
9164, Fixation 9114,9134 1VA74, 1VC74 F Mobilization 1VA04 F Manipulation 1VA05 F Implantation of internal device 9321,9351,9359,9361,
9362 1VA53 F
Repair 1VA80 F Pharmacotherapy 1VA35, 1VC35 C Removal of internal device 9365, 9366, 9369 1VA72, 1VC55, 1VC87 C Tibia/Fibula: Immobilization 1VQ03 F Management of external appliance 1VQ38 F
Reduction 9105,9125,9145,9155,
9165 1VQ73 F
Fixation 9115,9135 1VQ74 F Pharmacotherapy 1VQ35 C Removal of internal device 1VQ55 C Ankle: Immobilization 1WA03 F Management of external appliance 1WA38 F Reduction 1WA73 F Fixation 1WA74 F Mobilization 1WA04 F Manipulation 1WA05 F Implantation of internal device 1WA53 F Repair 1WA80 F Pharmacotherapy 1WA35 C Removal of internal device 1WA55 C Foot: Immobilization 1WG03 F Management of external appliance 1WG38 F
Reduction 9106,9126,9146,9156,
9166 1WE73, 1WI73, 1WJ73 F
Fixation 9116,9136 1WE74, 1WI74, 1WJ74 F Mobilization 1WE04, 1WJ04 F Manipulation 1WE05, 1WJ05 F Implantation of internal device 1WE53, 1WJ53 F Pharmacotherapy 1WE35, 1WJ35 C Removal of internal device 1WE55, 1WJ55 C Non specified Bone: Reduction 9108,9109,9128,9129,
9148,9149,9158,9159, 9168,9169
F
Fixation 9118,9119,9138,9139 F F = Fracture; C = fracture complication.
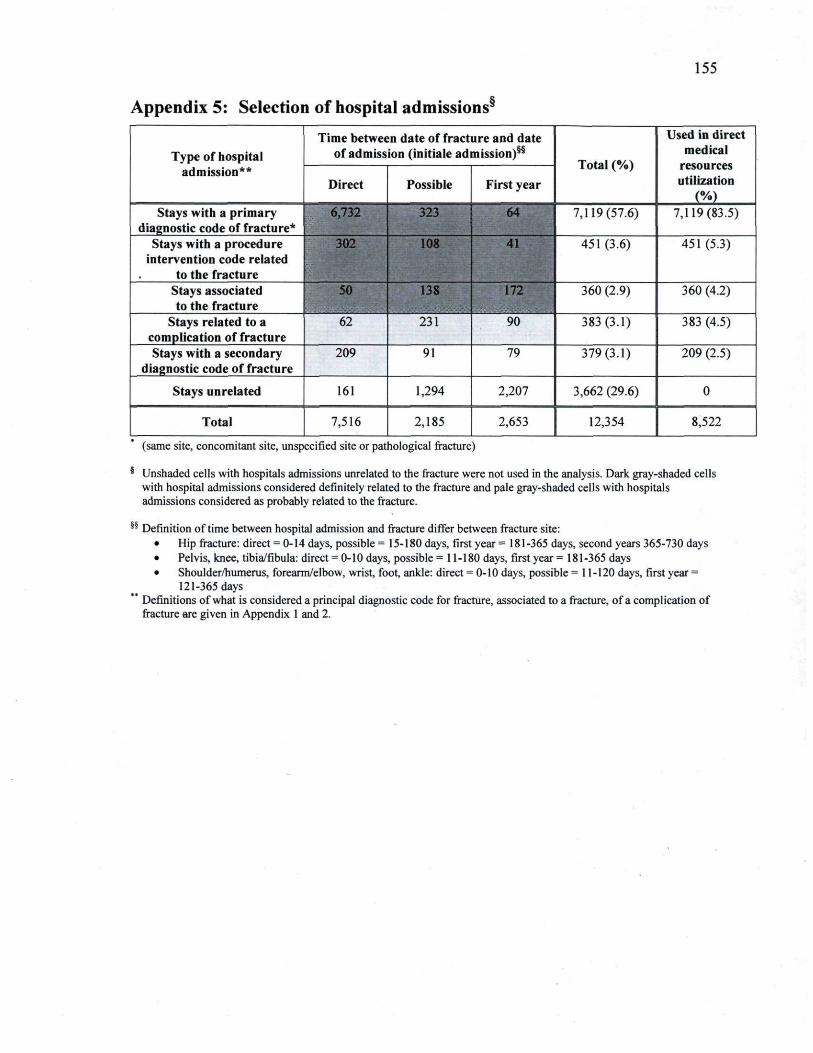
155
Appendix 5: Selection of hospital admissions®
Type of hospital admission**
Time between date of fracture and date of admission (initiale admission)55
Total (%)
Used in direct medical
resources utilization
(%)
Type of hospital admission**
Direct Possible First year
Total (%)
Used in direct medical
resources utilization
(%) Stays with a primary
diagnostic code of fracture* 6,732 323 64 7,119(57.6) 7,119(83.5)
Stays with a procedure intervention code related
to the fracture
302 108 41 451(3.6) 451 (5.3)
Stays associated to the fracture
50 138 172 360 (2.9) 360 (4.2)
Stays related to a complication of fracture
62 231 90 383(3.1) 383 (4.5)
Stays with a secondary diagnostic code of fracture
209 91 79 379(3.1) 209 (2.5)
Stays unrelated 161 1,294 2,207 3,662 (29.6) 0
Total 7,516 2,185 2,653 12,354 8,522
(same site, concomitant site, unspecified site or pathological fracture)
§ Unshaded cells with hospitals admissions unrelated to the fracture were not used in the analysis. Dark gray-shaded cells with hospital admissions considered definitely related to the fracture and pale gray-shaded cells with hospitals admissions considered as probably related to the fracture.
§§ Definition of time between hospital admission -and fracture differ between fracture site: • Hip fracture: direct = 0-14 days, possible = 15-180 days, first year = 181-365 days, second years 365-730 days • Pelvis, knee, tibia/fibula: direct = 0-10 days, possible = 11-180 days, first year = 181-365 days • Shoulder/humerus, forearm/elbow, wrist, foot, ankle: direct = 0-10 days, possible = 11-120 days, first year =
121-365 days Definitions of what is considered a principal diagnostic code for fracture, associated to a fracture, of a complication of fracture are given in Appendix 1 and 2.