Embed Size (px)
Citation preview
le
La v a l e u r de la c y t o l o g i e g a s t r i q u e d a n s le c a n c e r g a s t r i q u e super f i c i e l , c a n c e r invasi f e t les 16sions a s s o c i 6 e s
D. AMADORI, A. RAVAIOLI, M. LIVERANI, R. RIDOLFI, A. SARAGONI Oncology Department, L. Pierantoni Hospital, Forli (Italy)
The value of gastric cytology in advanced and early gastric cancer and related lesions
RI~SUMI~
Les donn6es de la litt6rature montrent les indications et les limites de la cytologie gastrique dirig6e dans le cancer gastrique superficiel et invasif et dans les 16sions et conditions pr6canc6reuses.
L'analyse des donn6es recueillies confirme l'accroissement de la pr6cision diagnostique, r6sultant de la cytologie dirig6e, dans le cancer gastrique, tant invasif que superficiel.
Les auteurs rapportent leur exp6rience de l'association cytologie et biopsie dans une s6rie de 3 393 cas.
La sensibilit6 et la sp6cificit6 de la cytologie sont respectivement de 0,92 et 0,98.
La corr61ation cytologie et biopsie a 6t6 6valu6e sur 449 pi~ces de r6section chirurgicale r6alis6e chez des patients pour lesquels la comparaison cytologie-biopsie a 6t6 effectu6e sur bases du diagnostic histo-pathologique des pi~ces de r6section chirurgicale.
Les.valeurs des taux de sensibilit6 et de sp6cificit6 de la cytologie et de la biopsie s6par6es sont significativement am61ior6es par la combinaison des deux m6thodes tant dans les cancers invasifs que dans les cancers superficiels.
S U M M A R Y
The data f rom literature on the indications and limits o f gastric aimed cytology in advanced and early gastric cancer and in precancerous conditions and lesions are reported.
The analysis o f these data confirms that the use o f aimed cytology in gastric pathology improves the diagnostic accuracy in both advanced and early gastric carcinoma.
The authors report their experience on 3 393 cases in which both aimed cytology and biopsy were carried out.
The sensitivity and the specificity o f cytology resulted 0.92 and 0.98 respectively.
Cytological and bioptic correlations were analyzed on 449 resected cases in which cytology and biopsy were compared with the histological diagnosis on surgical specimens.
The values o f sensitivity and o f specificity o f cytology and biopsy separately considered were significantly improved by the combined use o f the two methods both in advanced and in early gastric carcinoma.
INTROD UCTION
Depuis longtemps, la cytologie gastrique, utili- sant du mat6riel obtenu par diverses m6thodes exfoliatives ou abrasives [7, 22, 23, 29, 43] fait partie des techniques de diagnostic du carcinome et des 16sions associ6es.
Cette m6thode a donn6 de meilleurs r6sultats et une pr6cision diagnostique sup6rieure dans le can-
cer gastrique invasif plut6t que le cancer gastrique superficiel et les 16sions associ6es [1, 2, 11, 25, 26, 30, 38].
La large diffusion des techniques endoscopiques a permis le pr61~vement d'6chantillons obtenus pour cytologie par brossage au niveau d'une 16sion macroscopiquement d6celable (tableaux 1, 2, 3, 4) [3, 8, 11, 14, 16, 17, 21, 24, 27, 31, 32, 34, 35, 36, 37, 38, 39, 40, 42, 44, 46].
Tir6s ~ part : D; Dino AMADORI , Oncology Department, G.B. Morgagni, L. Pierantoni Hospital, V. Forlanini 1, 47100 Forli (Italy).
Mots-clds : cancer gastrique superficiel, cytologie, endoscopie, 16sions pr6canc6reuses.
Key-words:cy to logy , endoscopy, early gastric cancer, pre- cancerous lesions.
Acta Endoscopica Volume 15 - N ~ 4 - 1985 307
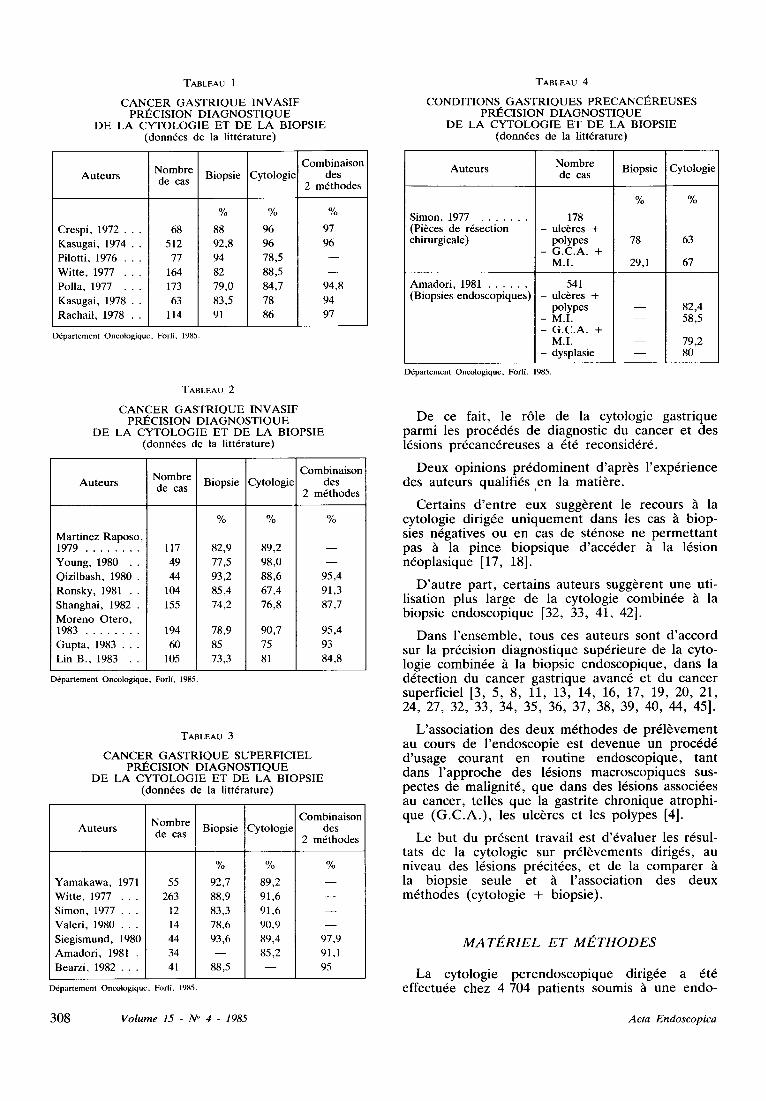
TABLEAU 1
C A N C E R G A S T R I Q U E I N V A S I F PRI~CISION D I A G N O S T I Q U E
D E L A C Y T O L O G I E ET D E L A B I O P S I E donn6es de la litt6rature)
Auteurs
Crespi, 1972 . . .
Kasugai, 1974 . .
Pilott i , 1976 . . .
Witte, 1977 . . .
Polla, 1977 . . .
Kasugai, 1978 . .
Racha i | , 1978 . .
Nombre Biopsie Cytologie de cas
Combinaison des
2 m6thodes
% % %
68 88 96 97
512 92,8 96 96
77 94 78,5 - -
164 82 88,5 - -
173 79,0 84,7 94,8
63 83,5 78 94
114 91 86 97
D6partement Oncologique, For l l , 1985.
TABLEAU 2
C A N C E R G A S T R I Q U E I N V A S I F PRI~CISION D I A G N O S T I Q U E
D E L A C Y T O L O G I E ET D E L A B I O P S I E (donn6es de ia litt6rature)
Nombre Auteurs de cas Biopsie Cytologie
Combinaison des
2 m6thodes
% % %
Martinez Raposo , 1979 117 82,9 89,2
Young, 1980 . . 49 77,5 98,0
Qizi lbash, 1980 . 44 93,2 88,6
Ronsky , 1981 . . 104 85,4 67,4
Shanghai, 1 9 8 2 . 155 74,2 76,8
Moreno Otero, 1983 194 78,9 90,7
Gupta, 1983 . . . 60 85 75
Lin B., 1983 . . 105 73,3 81
D6partement Oncologique, For l i , 1985.
95,4
91,3
87,7
95,4
93
84,8
TABLEAU 3
C A N C E R G A S T R I Q U E S U P E R F I C I E L PRI~CISION D I A G N O S T I Q U E
D E LA C Y T O L O G I E ET D E LA B I O P S I E donn6es de la litt6rature)
Auteurs Combinaison
Nombre Biopsie iCytologie des de cas
2 m6thodes
Y a m a k a w a , 1971
Witte, 1977 . . .
Simon, 1977 . . .
Valeri, 1980 . . .
Siegismund, 1980
Amadori, 1981 .
Bearzi, 1 9 8 2 . . .
D6partemcnt Oncologique, For l l , 1985.
% % %
55 92,7 89,2 - -
263 88,9 91,6 - -
12 83,3 91,6 - -
14 78,6 90,9 - -
44 93,6 89,4 97,9
34 - - 85,2 91,1
41 88,5 95
TABLEAU 4
C O N D I T I O N S G A S T R I Q U E S P R E C A N C t ~ R E U S E S PRI~CISION D I A G N O S T I Q U E
D E L A C Y T O L O G I E ET D E LA B I O P S I E (donn6es de la litt6rature)
Auteurs Nombre de cas
Simon, 1977 (Pi~ces de r6section chirurgicale)
Amadori, 1981 (Biopsies endoscopiques)
Biopsie Cytologie
% %
178 - ulc6res +
polypes 78 63 - G .C .A. +
M.I. 29,1 67
541 - ulc~res +
polypes - M.I. - G .C .A . +
M.I. - dysplasie
m
m
82,4 58,5
79,2 80
D6partement Oncologique, ForlL 1985.
De ce fait, le r61e de la cytologie gastrique parmi les proc6d6s de diagnostic du cancer et des 16sions pr6canc6reuses a 6t6 reconsid6r6.
Deux opinions pr6dominent d'apr~s l'exp6rience des auteurs qualifi6s en la mati~re.
Certains d'entre eux sugg~rent le recours ~i la cytologie dirig6e uniquement dans les cas ~ biop- sies n6gatives ou en cas de st6nose ne permettant pas ~ la pince biopsique d'acc6der h la 16sion n6oplasique [17, 18].
D'autre part, certains auteurs sugg~rent une uti- lisation plus large de la cytologie combin6e ~ la biopsie endoscopique [32, 33, 41, 42].
Dans l'ensemble, tous ces auteurs sont d'accord sur la pr6cision diagnostique sup6rieure de la cyto- logie combin6e h la biopsie endoscopique, dans la d6tection du cancer gastrique avanc6 et du cancer superficiel [3, 5, 8, 11, 13, 14, 16, 17, 19, 20, 21, 24, 27, 32, 33, 34, 35, 36, 37, 38, 39, 40, 44, 45].
L'association des deux m6thodes de pr61~vement au cours de l'endoscopie est devenue un proc6d6 d'usage courant en routine endoscopique, tant dans l'approche des 16sions macroscopiques sus- pectes de malignit6, que dans des 16sions associ6es au cancer, telles que la gastrite chronique atrophi- que (G.C.A.) , les ulc~res et les polypes [4].
Le but du pr6sent travail est d'6valuer les r6sul- tats de la cytologie sur pr616vements dirig6s, au niveau des 16sions pr6cit6es, et de la comparer la biopsie seule et ~ l'association des deux m6thodes (cytologie + biopsie).
MATE, R I E L E T ME, T H O D E S
La cytologie perendoscopique dirig6e a 6t6 effectu6e chez 4 704 patients soumis h une endo-
308 V o l u m e 1 5 - N ~ 4 - 1 9 8 5 A c t a Endoscopica
scopie gastrique dans notre h6pital entre 1971 et 1984.
Les frottis cytologiques, obtenus par brossage de la muqueuse gastrique sous contr61e visuel, ont 6t6 color6s selon la m6thode de Papanicolaou, exa- min6s au microscope /~ fort grossissement et clas- s6s selon les crit6res morphologiques usuels [2, 3, 9, 10, 11, 19, 28] (tab. 5, 6).
TABLEAU 5
P A T H O L O G I E C E L L U L A I R E EN C Y T O L O G I E G A S T R I Q U E
M O D I F I C A T I O N S BI~NIGNES
Caract6res cytologiques Alt6rations cellulaires
Inflammatoire Diff6renciation modifi6e :
R6g6n6ratif Modifications d'inhibition Atrophique de la maturat ion
(degr6s variables)
M6taplasie intestinale Diff6renciation anormale : - Ceilules de type absorbante - Goblet cells
R6gress i f - D6g6n6ratif Cariorexie, pycnose, n6crose, vacualisation
D6partement Oncologique, Forli, 1985.
TABLEAU 6
P A T H O L O G I E C E L L U L A I R E EN C Y T O L O G I E G A S T R I Q U E
M O D I F I C A T I O N S A T Y P I Q U E S
Caract6res cytologiques Alt6rations cellulaires
Dysplasie Degr6s variables d'atypies cellulaires
Malignit6 - cellules de type diff6renci6 - cellules de type indiff6renci6
D6partement Oncologique, Forli, 1985.
Les corr61ations cyto-histologiques ont 6t6 analy- s6es sur un total de 3 393 cas cons6cutifs, 6tudi6s dans notre D6par tement en y associant biopsie et cytologie.
La sensibilit6, la sp6cificit6, les taux de F.P. (faux positifs), F.N. (faux n6gatifs) de la cytologie et de la biopsie et des m6thodes combin6es, ont 6t6 ainsi 6valu6es sur 449 cas gastrectomis6s (pi6ces de r6section chirurgicale) comportant 130 16sions b6nignes, 319 cancers gastriques invasifs et 70 cancers gastriques superficiels.
Les donndes cytologiques des 16sions pr6canc6- reuses ont 6t6 6tudi6es chez 501 cas diagnostiqu6s par la biopsie.
R E S U L TATS
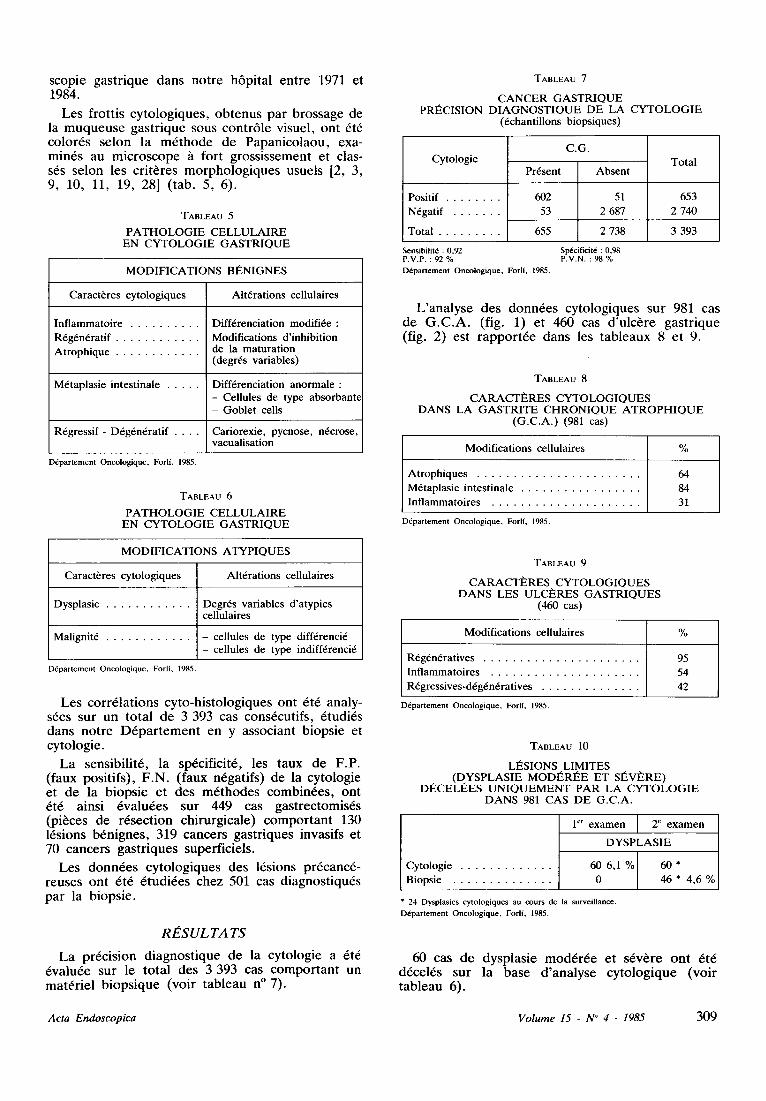
La pr6cision diagnostique de la cytologie a 6t6 6valu6e sur le total des 3 393 cas comportant un mat6riel biopsique (voir tableau n ~ 7).
TABLEAU 7
C A N C E R G A S T R I Q U E PRI~CISION D I A G N O S T I Q U E D E LA C Y T O L O G I E
Cytologie
6chantillons biopsiques)
Positif 602
�9 N6gatif . . . . . . . . 53
�9 Total . . . . . . . . . . 655
Sensibilit~ : 0,92 P.V.P. : 92 % D6partement Oncologique, Forli, 1985.
C.G. Total
Pr6sent Absent
51 653
2 687 2 740
2 738 3 393
Sp6cificit6 : 0,98 P.V.N. : 98 %
L'analyse des donn6es cytologiques sur 981 cas de G.C.A. (fig. 1) et 460 cas d'ulc6re gastrique (fig. 2) est rapport6e dans les tableaux 8 et 9.
TABLEAU 8
CARACTI~RES C Y T O L O G I Q U E S DANS LA G A S T R I T E C H R O N I Q U E A T R O P H I Q U E
(G.C.A. ) (981 cas)
Modifications cellulaires %
Atrophiques 64
M6taplasie intestinale 84
. Inflammatoires . . . . . . . . . . . . . . . . . . . . . . 31
D6partement Oncologique, ForlL 1985.
TABLEAU 9
CARACTI~RES C Y T O L O G I Q U E S D A N S LES U L C E R E S G A S T R I Q U E S
(460 cas)
Modifications cellulaires %
R6g6n6ratives 95
Inflammatoires 54
. R6gressives-d6g6n6ratives . . . . . . . . . . . . . . . 42
D6partement Oncologique, Forli, 1985.
TABLEAU 10
LI~SIONS LIMITES �9 ( D Y S P L A S I E MODt~RI~E ET SI~VI~RE)
DECELI~ES U N I Q U E M E N T PAR LA C Y T O L O G I E D A N S 981 CAS D E G.C.A.
Cytologie
�9 Biopsie . . . . . . . . . . . . . . .
I er examen 2 e examen
D Y S P L A S I E
60 6 , 1 % 6 0 *
0 46 * 4,6 %
* 24 Dysplasies cytologiques au cours de la surveillance. D~partement Oncologique, Forli, 1985.
60 cas de dysplasie mod6r6e et s6v6re ont 6t6 d6cel6s sur la base d'analyse cytologique (voir tableau 6).
A c t a E n d o s c o p i c a V o l u m e 15 - N ~ 4 - 1 9 8 5 309
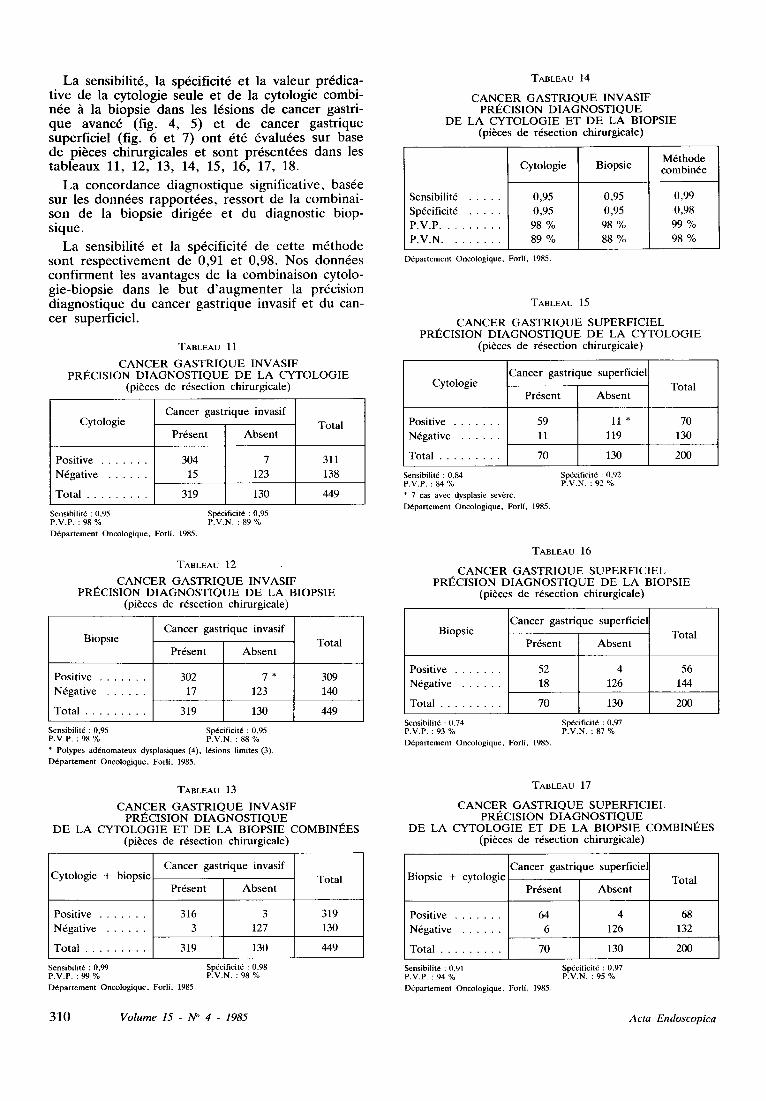
La sensibilit6, la sp6cificit6 et la valeur pr6dica- tive de la cytologie seule et de la cytologie combi- n6e h la biopsie dans les 16sions de cancer gastri- que avanc6 (fig. 4, 5) et de cancer gastrique superficiel (fig. 6 et 7) ont 6t6 6valu6es sur base de pi~ces chirurgicales et sont pr6sent6es dans les tableaux 11, 12, 13, 14, 15, 16, 17, 18.
La concordance diagnostique significative, bas6e sur les donn6es rapport6es, ressort de la combinai- son de la biopsie dirig6e et du diagnostic biop- sique.
La sensibilit6 et la sp6cificit6 de cette m6thode sont respectivement de 0,91 et 0,98. Nos donn6es confirment les avantages de la combinaison cytolo- gie-biopsie dans le but d'augmenter la pr6cision diagnostique du cancer gastrique invasif et du can- cer superficiel.
TABLEAU 11
C A N C E R G A S T R I Q U E I N V A S I F P R I ~ C I S I O N D I A G N O S T I Q U E D E L A C Y T O L O G I E
(p i~ces d e r 6 s e c t i o n c h i r u r g i c a l e )
C y t o l o g i e
P o s i t i v e
�9 N 6 g a t i v e . . . . . . .
�9 T o t a l . . . . . . . . . .
C a n c e r g a s t r i q u e i n v a s i f
P r 6 s e n t A b s e n t
304 7
15 123
319 130
T o t a l
311
138
449
Sensibilit6 : 0 , 95 Sp~ci f ic i t~ : 0,95 P.V.P. : 98 % P.V.N, : 89 % D6partement Oncologique, ForlL 1985.
TABLEAU 12
C A N C E R G A S T R I Q U E I N V A S I F P R I ~ C I S I O N D I A G N O S T I Q U E D E L A B I O P S I E
(p i~ces d e r 6 s e c t i o n c h i r u r g i c a l e )
B i o p s i e
P o s i t i v e
�9 N 6 g a t i v e . . . . . . .
�9 T o t a l . . . . . . . . . .
C a n c e r g a s t r i q u e i n v a s i f
P r 6 s e n t A b s e n t
302 7 *
17 123
319 130
T o t a l
309
140
449
Sensibilit6 : 0,95 Sp~Scificit6 : 0,95 P.V.P. : 98 % P,V.N. : 88 % * Polypes ad6nomateux dysplasiques (4), 16sions limites (3). D6partement Oncologique, Forli, 1985.
TABLEAU 13
C A N C E R G A S T R I Q U E I N V A S I F P R I ~ C I S I O N D I A G N O S T I Q U E
D E L A C Y T O L O G I E E T D E L A B I O P S I E C O M B I N I ~ E S (p i~ces d e r 6 s e c t i o n c h i r u r g i c a l e )
C y t o l o g i e + b i o p s i e
P o s i t i v e
�9 N 6 g a t i v e . . . . . . .
. T o t a l . . . . . . . . . .
C a n c e r g a s t r i q u e i n v a s i f
T o t a l P r 6 s e n t A b s e n t
316 3 319
3 127 130
319 130 449
Sensibiht6 : 0,99 Sp~cificit6 : 0,98 P.V.P. : 99 % P.V.N. : 98 % D6partement Oncologique, Forli, 1985.
TABLEAU 14
C A N C E R G A S T R I Q U E I N V A S I F P R I ~ C I S I O N D I A G N O S T I Q U E
D E L A C Y T O L O G I E E T D E L A B I O P S I E (p i~ces d e r 6 s e c t i o n c h i r u r g i c a l e )
Sens ib i l i t6
Sp6c i f ic i t6
P . V . P .
�9 P . V . N . . . . . . . . .
C y t o l o g i e
0 ,95
0 ,95
98 %
89 %
B i o p s i e
0 ,95
0 ,95
98 %
88 %
M 6 t h o d e c o m b i n 6 e
0 ,99
0 ,98
99 %
98 %
D6partement Oncologique, Forli, 1985.
TABLEAU 15
C A N C E R G A S T R I Q U E S U P E R F I C I E L P R I ~ C I S I O N D I A G N O S T I Q U E D E L A C Y T O L O G I E
(p i~ces d e r 6 s e c t i o n c h i r u r g i c a l e )
C a n c e r g a s t r i q u e supe r f i c i e l C y t o i o g i e
P r 6 s e n t A b s e n t
Pos i t i ve 59 11 *
�9 N 6 g a t i v e . . . . . . . 11 119
�9 T o t a l . . . . . . . . . . 70 130
T o t a l
70
130
200
SensibilitE : 0,84 P.V.P. : 84 % * 7 cas avec dysplasie severe. D6partement Oncologique, Forli, 1985,
sp6cificit6 : 0,92 P.V.N. : 92 %
TABLEAU 16
C A N C E R G A S T R I Q U E S U P E R F I C I E L P R I ~ C I S I O N D I A G N O S T I Q U E D E L A B I O P S I E
(p i~ces d e r 6 s e c t i o n c h i r u r g i c a l e )
B i o p s i e
P o s i t i v e
�9 N 6 g a t i v e . . . . . . .
�9 T o t a l . . . . . . . . . .
C a n c e r g a s t r i q u e s u p e r f i c i e l
P r 6 s e n t A b s e n t
52 4
18 126
7 0 130
T o t a l
56
144
200
Sensibilit~ : 0,74 Sp6cificitd : 0,97 P.V.P. : 93 % P.V.N. : 87 % Ddpartement Oncologique, Forlf, 1985.
TABLEAU 17
C A N C E R G A S T R I Q U E S U P E R F I C I E L P R I ~ C I S I O N D I A G N O S T I Q U E
D E L A C Y T O L O G I E E T D E L A B I O P S I E C O M B I N I ~ E S (p i~ces d e r 6 s e c t i o n c h i r u r g i c a l e )
B i o p s i e + c y t o l o g i e
Pos i t i ve
. N 6 g a t i v e . . . . . .
. T o t a l . . . . . . . . .
C a n c e r g a s t r i q u e s u p e r f i c i e l
P r 6 s e n t A b s e n t
64 4
6 126
7 0 130
T o t a l
68
132
200
Sensibilit6 : 0,91 P.V.P. : 94 % Ddpartement Oncologique. Forlf, 1985.
Sp6cificit6 : 0,97 P.V.N. : 95 %
310 V o l u m e 15 - N ~ 4 - 1 9 8 5 A c t a E n d o s c o p i c a
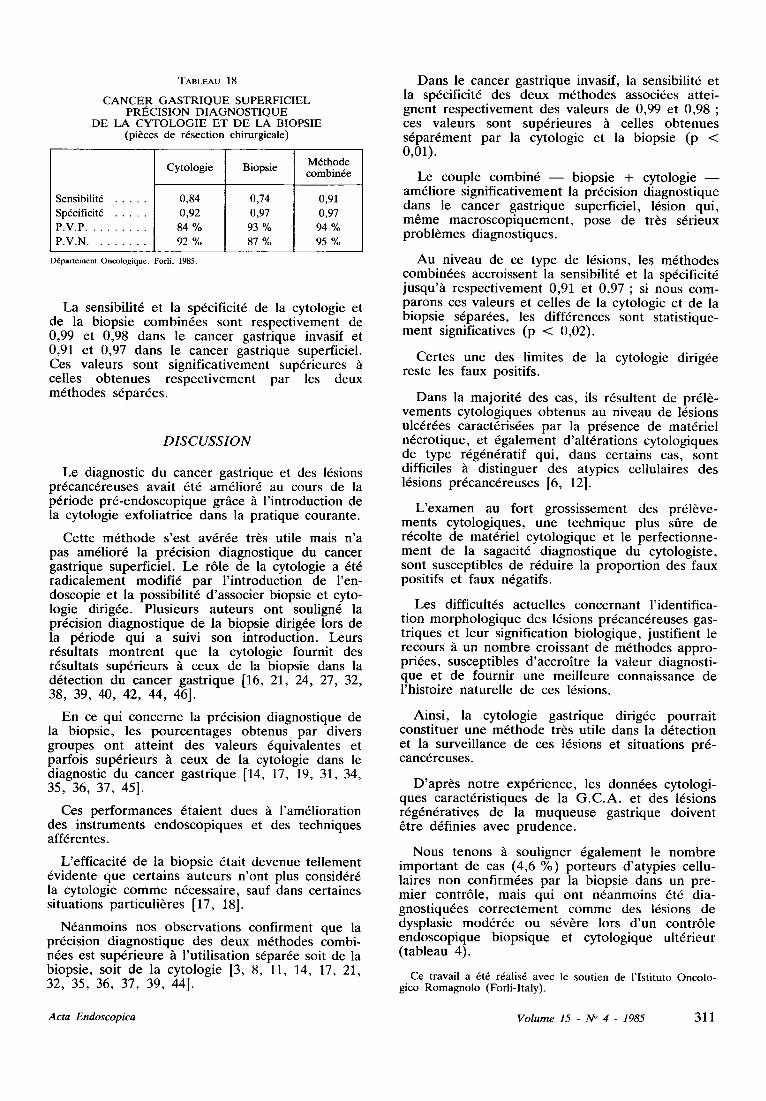
TABLEAU 18
CANCER G A S T R I Q U E SUPERFICIEL PRI~CISION DIAGNOSTIQUE
DE LA CYTOLOGIE ET DE LA BIOPSIE (pi~ces de r6section chirurgicale)
Sensibilit6 Sp6cificit6 P.V.P.
. P.V.N . . . . . . . . .
Cytologic
0,84 0,92 84 % 92 %
Biopsie
0,74 0,97 93 % 87 %
M6thode combin6e
0,91 0,97 94 % 95 %
D6partement Oncologique, Forli, 1985.
La sensibilit6 et la sp6cificit6 de la cytologic et de la biopsie combin6es sont respectivement de 0,99 et 0,98 dans le cancer gastrique invasif et 0,91 et 0,97 dans le cancer gastrique superficiel. Ces valeurs sont significativement sup6rieures celles obtenues respectivement par les deux m6thodes s6par6es.
D I S C U S S I O N
Le diagnostic du cancer gastrique et des 16sions pr6canc6reuses avait 6t6 am61ior6 au cours de la p6riode pr6-endoscopique grglce h l'introduction de la cytologic exfoliatrice dans la pratique courante.
Cette m6thode s'est av6r6e tr~s utile mais n'a pas am61ior6 la pr6cision diagnostique du cancer gastrique superficiel. Le r61e de la cytologie a 6t6 radicalement modifi6 par l'introduction de l'en- doscopie et la possibilit6 d'associer biopsie et cyto- logie dirig6e. Plusieurs auteurs ont soulign6 la pr6cision diagnostique de la biopsie dirig6e lors de la p6riode qui a suivi son introduction. Leurs r6sultats montrent que la cytologic fournit des r6sultats sup6rieurs ~ ceux de la biopsie dans la d6tection du cancer gastrique [16, 21, 24, 27, 32, 38, 39, 40, 42, 44, 46].
En ce qui concerne la pr6cision diagnostique de la biopsie, les pourcentages obtenus par divers groupes ont atteint des valeurs 6quivalentes et parfois sup6rieurs ~ ceux de la cytologie dans le diagnostic du cancer gastrique [14, 17, 19, 31, 34, 35, 36, 37, 45].
Ces performances 6taient dues h l'am61ioration des instruments endoscopiques et des techniques aff6rentes.
L'efficacit6 de la biopsie 6tait devenue tellement 6vidente que certains auteurs n'ont plus consid6r6 la cytologie comme n6cessaire, sauf dans certaines situations particuli~res [17, 18].
N6anmoins nos observations confirment que la pr6cision diagnostique des deux m6thodes combi- n6es est sup6rieure ~t l'utilisation s6par6e soit de la biopsie, soit de la cytologic [3, 8, 11, 14, 17, 21, 32, 35, 36, 37, 39, 44].
Dans le cancer gastrique invasif, la sensibilit6 et la sp6cificit6 des deux m6thodes associ6es attei- gnent respectivement des valeurs de 0,99 et 0,98 ; ces valeurs sont sup6rieures h celles obtenues s6par6ment par la cytologic et la biopsie (p < 0,01).
Le couple combin6 - - biopsie 4- cytologie - - am61iore significativement la pr6cision diagnostique dans le cancer gastrique superficiel, 16sion qui, m6me macroscopiquement, pose de tr~s s6rieux probl~mes diagnostiques.
Au niveau de ce type de 16sions, les m6thodes combin6es accroissent la sensibilit6 et la sp6cificit6 jusqu't~ respectivement 0,91 et 0,97 ; si nous com- parons ces valeurs et celles de la cytologie et de la biopsie s6par6es, les diff6rences sont statistique- ment significatives (p < 0,02).
Certes une des limites de la cytologic dirig6e reste les faux positifs.
Dans la majorit6 des cas, ils r6sultent de pr61~- vements cytologiques obtenus au niveau de 16sions ulc6r6es caract6ris6es par la pr6sence de mat6riel n6crotique, et 6galement d'alt6rations cytologiques de type r6g6n6ratif qui, dans certains cas, sont difficiles tt distinguer des atypies cellulaires des 16sions pr6canc6reuses [6, 12].
L'examen au fort grossissement des pr61~ve- ments cytologiques, une technique plus sfire de r6colte de mat6riel cytologique et le perfectionne- ment de la sagacit6 diagnostique du cytologiste, sont susceptibles de r6duire la proportion des faux positifs et faux n6gatifs.
Les difficult6s actuelles concernant l'identifica- tion morphologique des 16sions pr6canc6reuses gas- triques et leur signification biologique, justifient le recours tt un nombre croissant de m6thodes appro- pri6es, susceptibles d'accroitre la valeur diagnosti- que et de fournir une meilleure connaissance de l'histoire naturelle de ces 16sions.
Ainsi, la cytologic gastrique dirig6e pourrait constituer une m6thode tr6s utile dans la d6tection et la surveillance de ces 16sions et situations pr6- canc6reuses.
D'apr6s notre exp6rience, les donn6es cytologi- ques caract6ristiques de la G.C.A. et des 16sions r6g6ndratives de la muqueuse gastrique doivent 6tre d6finies avec prudence.
Nous tenons fa souligner 6galement le nombre important de cas (4,6 %) porteurs d'atypies cellu- laires non confirm6es par la biopsie dans un pre- mier contr61e, mais qui ont n6anmoins 6t6 dia- gnostiqu6es correctement comme des 16sions de dysplasie mod6r6e ou s6v6re lors d'un contr61e endoscopique biopsique et cytologique ult6rieur (tableau 4).
Ce travail a 6t6 r6alis6 avec le soutien de l'Istituto Oncolo- gico Romagnolo (Forli-Italy).
A c t a E n d o s c o p i c a V o l u m e 15 - N ~ 4 - 1985 311
RI~FI~RENCES
1. AMADORI D., RAVAIOLI A., SARAGONI A., MAR- TUZZI M . - - Aspetti citologici della gastrite atrofica associata a carcinoma gastrico. Pathologica 1973, L X V : 341-346.
2 . A M A D O R I D . - - La citologia gastrica nelle lesioni beni- gne : flogosi-iperplasia-atrofia metaplasia intestinale. Atti Corso Naz. Citologia diagnostica, Forli 2-7 Aprile 1979.
3. AMADORI D., RAVAIOLI A., SARAGONI A., ZOLI W. - - Cyto-morphological aspects and cito-histological cor- relations in pre-neoplastic alterations and in malignancies of gastric mucosa. Acta Endoscopica 1981, X ! : 155-164.
4. AMADORI D., RAVAIOLI A., CASADEI GIUNCHI D., RASI F., MALTONI M. - - La citologia nella diagno- si e nel controllo della gastrite cronica. Giornale ltaliano End. Dig. 1983, 6:19-24.
5. AMADORI D., RAVAIOLI A., RIDOLFI R., GENTI- LINI P. - - Tumori dello stomaco. Citologia. Trattato di Clinica Oncologica 1983, H : 913-929, Piccin Ed., Padova.
6. BAJTAI A., SIMON L., FIGUS I.A. - - Some particular aspects of gastric cytology. Comparison of cytology and histology. Arch. Geschwulstforsch 1977, 47/8:728-737.
7. BEALE L.S. - - The microscope in Medicine 2 "d Ed. 1958, J., and Churchill L.T.D.
8 . BEARZI I., RANALDI R . - - Early gastric cancer and morphologic study of 41 cases. Tumori 1982, 68 : 223-233.
9. BIGOTTI A., CRESPI M., DI MAq'TEO S. - - The main criteria of judgement in the morphological diagnosis of chronic gastritis in its various stages. Pro. 2nd. World Congress of Gastrointestinal Endoscopy 1972, Piccin Ed., Padova.
10. CRESPI M., BIGOTI'I A.D., DI MATTEO S. - - The value of abrasive gastric cytology in the grading and fol- low-up of chronic gastritis. Pro 2nd. World Congress of Gastrointestinal Endoscopy 1972, Piccin ED.PD.
11. CRESPI M. - - Cytological screening of gastric carcinoma. Current views in gastroenterology. Symposia and Round Table Conferences of the 10th International Congress of Gastroenterology. Budapest, 1976.
12. DZIURA B.R., OTIS R., HUKILL P., GOLDBLAT1 ~ P . , D A M J A N O V I . - - Gastric brushing cytology : an ana- lysis of cells from bening and malignant ulcers. Acta Cyt. 1977, 21 : 187-190.
13. GRAHAM D.Y., SPJUT H.J., ESTRADA R.G. - - Directed cytology of the esophagus and stomach, a compa- rison of 3 rapid collection methods. Gastroint, Endoscopy 1978, 24 - 277-280.
14. GUPTA J.R., JAIN A.K., A G R A W A L B.K., GUPTA S. - - Gastroscopic cytology and biopsies in diagnosis of gastric malignancies. J. of Surg. Oncology 1983, 22 : 62-64.
15. HENNING N., WITTE S. - - Atlante di citodiagnostica gastroenterologica. Editrice Internazionale ~ Arti e Scienze ~ Roma 1970.
16. KASUGAI T., KOBAYASHI S. - - Evaluation of biopsy and cytology in the diagnosis of gastric cancer. Am. J. Gastroenterol 1974, 60 : 199-203.
17. KASUGAI T., KOBAYASHI S., KUNO N. - - Endoscopic cytology of the esophagus, stomach and pan- creas, Acta Cyt. 1978, 22 : 327-330.
18. KOBAYASHI S., YOSHII Y., KASUGAI T. - - Selective use of brushing cytology in gastrointestinal strictures, Gas- troint. Endosc. 1972, 19 : 77-78.
19. KOBAYASHI S., YOSHII Y., KASUGAI T. - - Biopsy and cytology in the diagnosis of early gastric cancer. 10 year experience with direct vision techniques at a Japanese Institution. Endoscopy 1976, 8 : 53-58.
20. KOBAYASHI S., KASUGAI T. - - Brushing cytology for the diagnosis of gastric cancer involving the cardia or the lower esophagus. Acta Cyt. 1978, 22 : 155-158�9
21. LIN B.P.C., H A R M A D A P.A. - - Gastric and esophageal brush cytology. Pathology 1983, 15 : 393-397.
22. LOEPER M. BINET E. - - Le cytodiagnostic des affec- tions de l'estomac. Bull. Soc. M~d. H6p. Paris 31, 563, 1911.
23. MARINI G. - - Uber die diagnose des magenkarzinoms auf Grund der cytologischen untersuchung des spuiwassers. Eigene Beobachtungen und pathologischen zelleninhalt des magens. Arch�9 Verdan, 1909, 15 : 251-255.
24. MARTINEZ-RAPOSO A., MORENO OTERO R., RODRIGUEZ-CORTES J., PAJARES GARCIA J.M., JIMENEZ JIMENEZ E . - - Volor diagnostico comparati- vo de la citologia exfoliativa, biopsia y endoscopia en las lesiones malignas del estomago. Revista Clinica Espahola 1979, 152 : 299-302.
25. MARTUZZI M., A MA D O RI D., SARAGONI A. - - Citodiagnostica oncologica su liquido di lavaggio gastrico. Boll. Soc. It. Patol. 1969, XI, Fasc. I.
26. MARTUZZI M., A M A D O R I D., SARAGONI A, - - Le cytodiagnostic du cancer gastrique. Revue de Cytologie Clinique 1971, 4 : 9-16.
27. MORENO OTERO R., MARTINEZ-RAPOSO A., CANTERO T., PAJARES J . M . - - Exfoliative cytodiagno- sis of gastric adenocarcinoma. Comparison with biopsy and endoscopy. Acta Cyt. 1983, 27 : 485-488.
28. NIEBURGS H.E. - - Diagnostic cell pathology in tissue and smears Grune. Stratton, New York, 1967.
29. PANICO F.G., PAPANICOLAOU G.N., COOPER W.A. - - Abrasive ballon for exfoliation of gastric cancer cells. J .A.M.A. 1950, 143 : 1308.
30. PAPANICOLAOU G.N., COOPER W.A. - - Cytology of gastric fluid in diagnosis of carcinoma of the stomach. J. Natl. Cancer Ist. 1947, 7 : 357-360.
31. PILO'ITI S. - - Biopsia e citologia gastrica. Min. gastroen- terol. 1976, 22 : 42-48.
32, PROLLA J.C., REILLY R.W., KIRSNER J.B., CO- CKERHAM L . - - Direct-vision Endoscopic cytology and biopsy in the diagnosis of esophageal and gastric tumours : current experience. Acta Cyt. 1977, 21 : 399-402.
33. PROLLA J.C. - - Diagnostic cytology of early gastric cancer. Proc. of the Symposium 4th World Congress of Digestive Endoscopy. 1979, 14:289-291. Brazil.
34. QIZILBASH A., HARNARINE C., CASTELLI M. - - Early Gastric Carcinoma. Arch. Pathol. Lab. Med. 1977, 101 : 610-614.
35. RACHAIL-ARNOUX M., RACHAIL M., PEDOTI~I C., MOURIQUAND C. - - Fiberoptically controlled gastric cytology: its value and limitations�9 Arch. Geschwulst- forsch. 1978, 48/1 : 70-73.
36. RON SKY R., FRIE P., KULHANKOVA S., LOYDA Z., JIRASEK A., HUSLAROVA A., KOTSCLIK J., DVORAK M. - - Fiber endoscopy and complementary methods in the diagnosis of gastric cancer Part. 2, brush cytology , . Unitr. Lek. 1981, 27 (11) : 1068-1072.
37. SIEGISMUND G., OSTERTAG H. ATAY Z. - - The advantage of combined target biopsy and contact smear cytology in the diagnosis of early gastric carcinoma. Can- cer Cytology 1980, 20 : 18-25.
38. SIMON L., BAJTAI A., FIGUS I., VASKO J. - - Clini- cal value of exfoliative and abrasive cytology in the dia- gnostics of gastric cancer and precanceroses. Arch. Ges- chwulst-forsch. 1977, 47/8 : 719-727.
39. SHANGAI COOPERATIVE GROUP (CHINA). - - Gut 1982, 23 : 774-776.
�9 40. VALERI F.V., VALERI V., MODENA J.L.P., CENE- VIVA R., NETO J.B., OLIVEIRA J.S.M., CASTEL- FRANCHI P . L . - - Early Gastric Cancer : combined ana- lysis of endoscopy, cytology and histology. In : Prevention and Detection of cancer. Part. II, Detection Vol. 2, Cancer Detection in Specific sites. Nieburgs H.E. ed. New York, Marcel Dekker Inc. 1303, 2456 pp., 1980.
312 Volume 15 - N ~ 4 - 1985 Acta Endoscopica
41. w r I T E S. - - Gastroenteroiogical cytodiagnosis. Editorial. Acta Hepatogastroenterol. 1975, 22 : 137-139.
42. WI'FI'E S. - - Die Bedeutung der Zytologie bei der dia- gnostik nicht-maligner Schleimhautver~inderungen des ma- gens. Arch. GeschwulsOCorsch 1977, 47/8 : 748-754.
43. YAMADA T., MATSUMOTO S., SAUKAWA H., and SEING Y. - - Clinical evaluation of proteolytic enzyme method in gastric cytodiagnosis especially in the detection of early cancer. Acta Cyt. 1968, 8 : 27-31.
44. Y A M A K A W A M., PANISH J., BERCI G., MORGEN-
45.
46.
STERN L., SOHMA S., KIDOKORO T., HAYASHIDA T. - - The correlation of target biopsy and contact smear cytology under direct visual control in malignant gastric lesions. Gastrointestinal Endoscopy 1971, X V I I : 164-168.
YOSHII Y., TAKAHASHI J., Y A M A O K A Y., KASU- GAI T. - - Significance of imprint smear in cytologic diagnosis of malignant tumours of the stomach. Acta Cyt. 1970, 14 : 249-253.
YOUNG J.A., HUGUES H.E. - - Three year trial of endoscopic cytology of the stomach and duodenum. Gut 1980, 21 : 241-246.
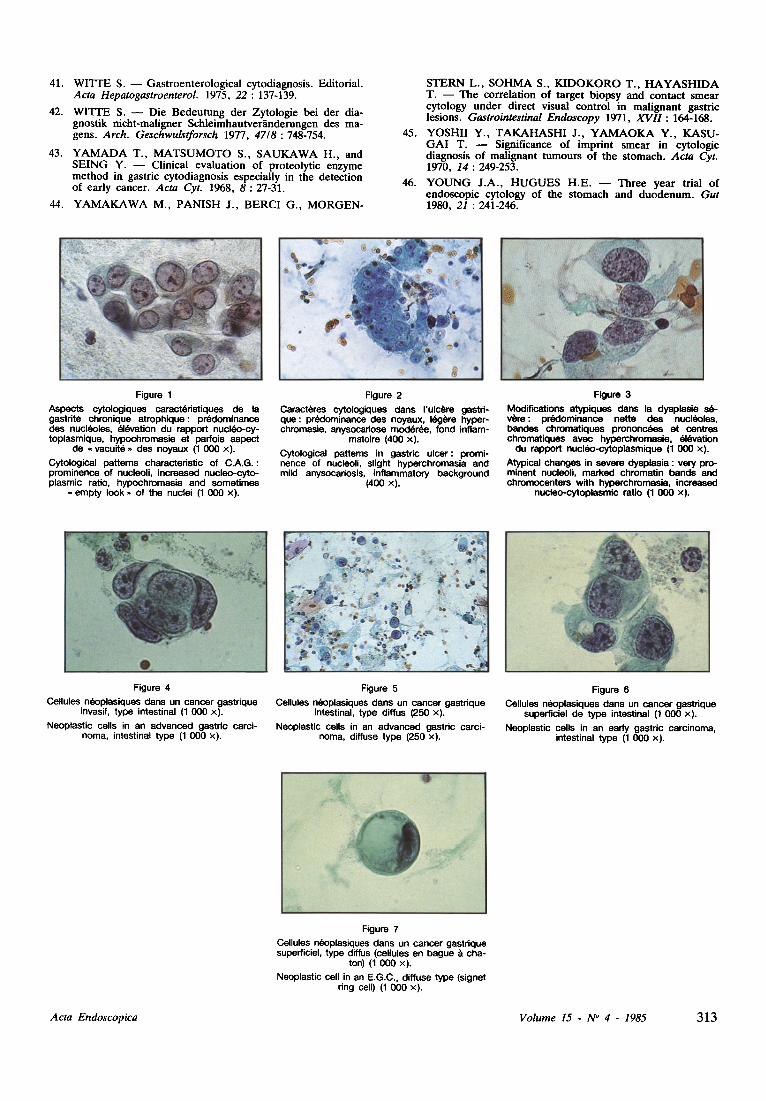
Figure 1 Aspects cytologiques caract(~ristiques de la gastrite chronique atrophique: prddominanca des nucldoles, ~l~vation du rapport nucl(~o-cy- toplasmique, hypochromesie et parfois aspect
de ~ vacuit(~ ~ des noyaux (1 000 x). Cytological patterns characteristic of C.A.G. : prominence of nucleoli, increased nucleo-cyto- plasmic ratio, hypochromasia and sometimes
,, empty look - of the nuclei (1 000 x).
Figure 2 Caract6res cytologiques dans I'ulc~re gastri- que: pr6clominance des noyaux, I~g~re hyper- chromasie, anysocariose mod~rde, fond inflam-
matoire (400 x). Cytological patterns in gastric ulcer: promi- nence of nucleoli, slight hyperchromasia and mild anysocariosis, inflammatory background
(400 x).
Figure 3 Modifications atypiques dans la dysplesie s ~ v6re : pr~clominance nette des nucl(~Joles, bandes chromatiques p r o n o n ~ et centres chromatiques aveo hyperchromasie, ~l~vation
du rapport nucl~o-cytoplasmique (1 000 x). Atypical changes in severe dysplesia : very pro- minent nucleoli, marked chromatin bands and chromocenters with hyperchromesia, increased
nucleo-cytoplesmic ratio (1 000 x).
Figure 4 Cellules ndoplasiques darts un cancer gastrique
invasif, type intestinal (1 000 x). Neoplastic cells in an advanced gastric carci-
noma, intestinal type (1 000 •
Figure 5 Cellules n~oplasiques dans un cancer gastrique
intestinal, type diffus (250 x). Neoplastic cells in an advanced gastric carci-
noma, diffuse type (250 x).
Figure 6 Cellules nl~oplasiques dans un cancer gastrique
superficiel de type intestinal (1 000 x). Neoplastic cells in an early gastric carcinoma,
intestinal type (1 000 x).
Figure 7 Cellules n~oplasiques dans un cancer gastdque superficiel, type diffus (cellules en hague & cha-
ton) (1 000 • Neoplastic cell in an E.G.C., diffuse type (signet
ring cell) (1 000 x).
Acta Endoscopica Volume 15 - N ~ 4 - 1985 313

INTRODUCTION
Gastric cytology has been applied for a long time in the diagnosis and research of carcinoma and related lesions, using exfoliative or abrasive mate- rial obtained by various blind methods [7, 22, 23, 29, 43].
This method has given better results and diagnos- tic accuracy in the advanced gastric carcinoma rather than in early gastric cancer and related lesions [1, 2, 11, 25, 26, 30, 38].
The introduction of a wide-spread use of fibreop- tic endoscopic procedures has allowed the aimed collection of cytological samples by the brushing of the endoscopically detected lesions (tab. 1, 2, 3, 4) [3, 8, 11, 14, 16, 17, 21, 24, 27, 31, 32, 34, 35, 36, 37, 38, 39, 40, 42, 44, 46].
An important change in the role of gastric cyto- logy among diagnostic procedures of carcinoma and its precursors has been thus achieved.
Two predominant opinions emerge from the experience of the authors concerned in this matter.
TABLE 1
A D V A N C E D G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y O F C Y T O L O G Y
A N D BIOPSY (data from literature)
Authors N. Cases Biopsy Cytology Combined
Crespi, 1972 . . .
Kasugai, 1974 . .
Pilotti, 1976 . . .
Witte, 1977 . . .
Polla, 1977 . . .
Kasugai, 1978 . .
Rachail, 1978 . .
% % %
68 88 96 97
512 92.8 96 96
77 94 78.5 - -
164 82 88.5 - -
173 79.0 84.7 94.8
63 83.5 78 94
114 91 86 97
Oneology department. Forli. 1985.
TABLE 2
A D V A N C E D G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y O F C Y T O L O G Y
A N D BIOPSY (data from literature)
Authors N. Cases Biopsy Cytology Combined
% % %
Martinez Raposo, 1979 117 82.9 89.2
Young, 1980 . . 49 77.5 98.0
Qizilbash, 1980. 44 93.2 88.6 95.4
Ronsky, 1981 . . 104 85.4 67.4 91.3
Shanghai, 1982 . 155 74.2 76.8 87.7
Moreno Otero, 1983 194 78,9 90,7 95,4
Gupta , 1983 . . . 60 85 75 93
Lin B., 1983 . . 105 73.3 81 84.8
Oncology department, Fofll, 1985.
TABLE 3
E A R L Y G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y OF C Y T O L O G Y
Authors
Yamakawa, 1971
Witte, 1977 . . .
Simon, 1977 . . .
Valeri, 1980 . . .
Siegismund, 1980
Amadori , 1981 .
Bearzi, 1982 . . .
A N D BIOPSY (data from literature)
N. Cases Biopsy Cytology Combined
% % %
55 92.7 89.2
263 88.9 91.6 - -
12 83.3 91.6 - -
14 78.6 90.9 - -
44 93.6 89.4 97.9
34 85.2 91.1
41 88.5 95
Oncology department, Forli, 1985.
TABLE 4
G A S T R I C C A N C E R P R E C U R S O R S D I A G N O S T I C A C C U R A C Y OF C Y T O L O G Y
A N D BIOPSY (data from literature)
Authors N. Cases
Simon, 1977 (Surgical specimens)
Amadori , 1981 (Bioptic specimens)
O n c o l o g y department, Forl[, 1985.
Biopsy Cytology
% %
178 - Ulcers +
Polyps 78 63 - C .A.G. +
M.I. 29.1 67
541 - Ulcers +
Polyps - M . I .
- C .A.G. + M.I.
- Dysplasia
- - 82.4 - - 58.5
- - 79.2 - - 80
Some authors suggest the use of aimed cytology mainly in cases with negative bioptic findings and in cases where the presence of stenosis does not allow a biopsy forceps to reach the neoplasm [17, 18].
One the other hand many authors suggest a more wide-spread use of aimed cytology combined with endoscopy and biopsy [32, 33, 41, 42].
It is agreed, however, that the accuracy in the detection of Advanced and Early Gastric Cancer is improved by the combined use of cytology and biopsy during endoscopy [3, 5, 8, 11, 13, 14, 16, 17, 19, 20, 21, 24, 27, 32, 33, 34, 35, 36, 37, 38, 39, 40, 44, 45].
This association of cytology and biopsy during endoscopy is a common procedure in our diagnos- tic practice, both in the lesions with a malignant macroscopic aspect and in the lesions of gastric mucosa related with cancer, such as chronic atro- phic gastritis, ulcers and polyps [4].
314 V o l u m e 15 - N ~ 4 - 1 9 8 5 A c t a E n d o s c o p i c a
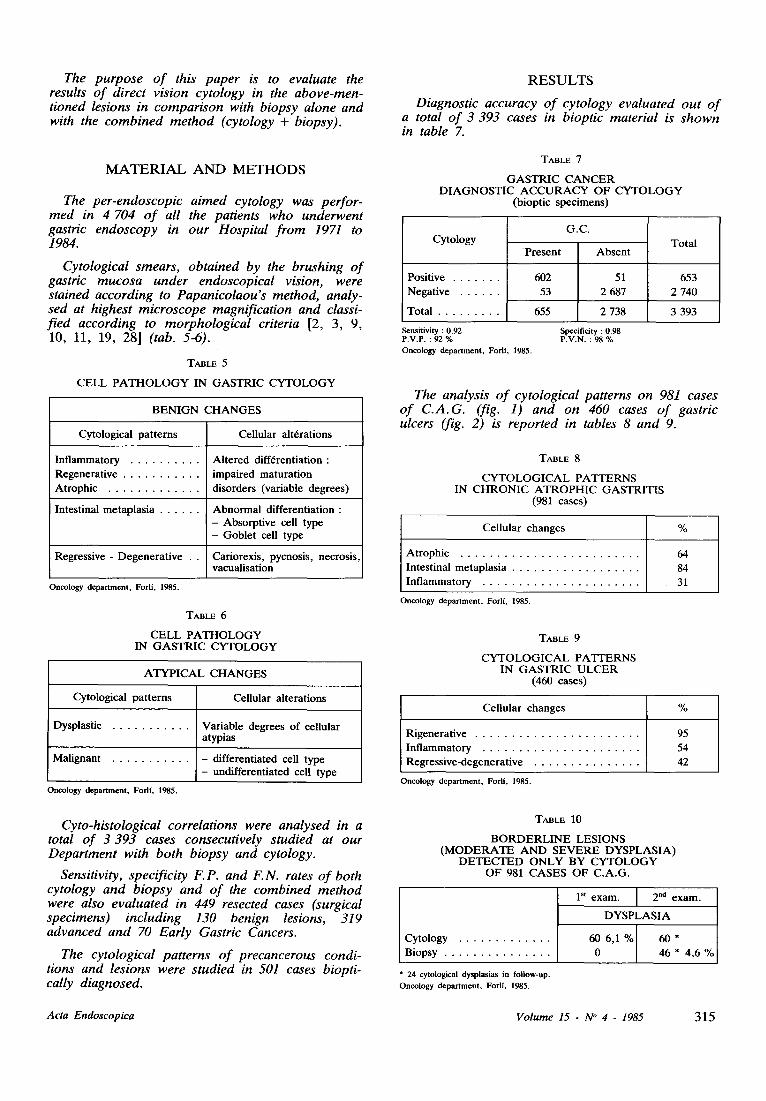
The purpose of this paper is to evaluate the results of direct vision cytology in the above-men- tioned lesions in comparison with biopsy alone and with the combined method (cytology + biopsy).
MATERIAL A N D METHODS
The per-endoscopic aimed cytology was perfor- med in 4 704 o f all the patients who underwent gastric endoscopy in our Hospital from 1971 to 1984.
Cytological smears, obtained by the brushing of gastric mucosa under endoscopical vision, were stained according to Papanicolaou's method, analy- sed at highest microscope magnification and classi- fied according to morphological criteria [2, 3, 9, 10, 11, 19, 28] (tab. 5-6).
TABLE 5
C E L L P A T H O L O G Y IN G A S T R I C C Y T O L O G Y
B E N I G N C H A N G E S
Cytological pa t te rns Cellular al t6rations
In f l ammatory Al te red diff6rentiation :
Regenera t ive impaired matura t ion �9 Atrophic . . . . . . . . . . . . . . disorders (variable degrees)
Intestinal metap las ia A b n o r m a l differentiat ion : - Absorpt ive cell type - Goble t cell type
Regressive - Degene ra t ive . . Cariorexis, pycnosis , necrosis , vacualisat ion
Oncology department, Forli, 1985.
TABLE 6
C E L L P A T H O L O G Y IN G A S T R I C C Y T O L O G Y
A T Y P I C A L C H A N G E S
Cytological pa t t e rns Cellular al terat ions
Dysplastic Variable degrees of cellular atypias
Mal ignant - differentiated cell type - undifferent ia ted cell type
Oncology department, Forli, 1985.
Cyto-histological correlations were analysed in a total of 3 393 cases consecutively studied at our Department with both biopsy and cytology.
Sensitivity, specificity F.P. and F.N. rates o f both cytology and biopsy and of the combined method were also evaluated in 449 resected cases (surgical specimens) including 130 benign lesions, 319 advanced and 70 Early Gastric Cancers.
The cytological patterns of precancerous condi- tions and lesions were studied in 501 cases biopti- cally diagnosed.
RESULTS
Diagnostic accuracy o f cytology evaluated out o f a total of 3 393 cases in bioptic material is shown in table 7.
TABLE 7
G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y O F C Y T O L O G Y
(bioptic spec imens)
Cytology
Positive �9 Negat ive . . . . . . .
Total
P r e s e n t
602
53
655
G.C.
A b s e n t
51
2 687
2 738
Tota l
653
2 740
3 393
Sensitivity : 0.92 Specificity : 0.98 P.V.P. : 92 % P.V.N. : 98 % Oncology department, Forli, 1985.
The analysis of cytological patterns on 981 cases of C.A.G. (fig. 1) and on 460 cases o f gastric ulcers (fig. 2) is reported in tables 8 and 9.
TABLE 8
C Y T O L O G I C A L P A T T E R N S IN C H R O N I C A T R O P H I C G A S T R I T I S
(981 cases)
Cel lular changes
At rophic
Intest inal metap las ia . In f l ammatory . . . . . . . . . . . . . . . . . . . . . . .
Oncology department, Forli, 1985.
%
64
84 31
TABLE 9
C Y T O L O G I C A L P A T T E R N S IN G A S T R I C U L C E R
(460 cases)
Cel lu lar changes %
Rigenera t ive In f l ammato ry
, Regress ive-degenera t ive . . . . . . . . . . . . . . . .
95
54 42
Oncology department, ForlL 1985.
TABLE 10
B O R D E R L I N E L E S I O N S ( M O D E R A T E A N D S E V E R E D Y S P L A S I A )
D E T E C T E D O N L Y B Y C Y T O L O G Y O F 981 C A S E S O F C . A . G .
Cytology Biopsy
1 st e x a m . 2 nd exam.
D Y S P L A S I A
6 0 6 , 1 % 6 0 *
0 46 * 4,6 %
* 24 cytological dysplasias in fol low-up.
Oncology department, Forli, 1985.
A c t a E n d o s c o p i c a V o l u m e 15 - N ~ 4 - 1 9 8 5 315
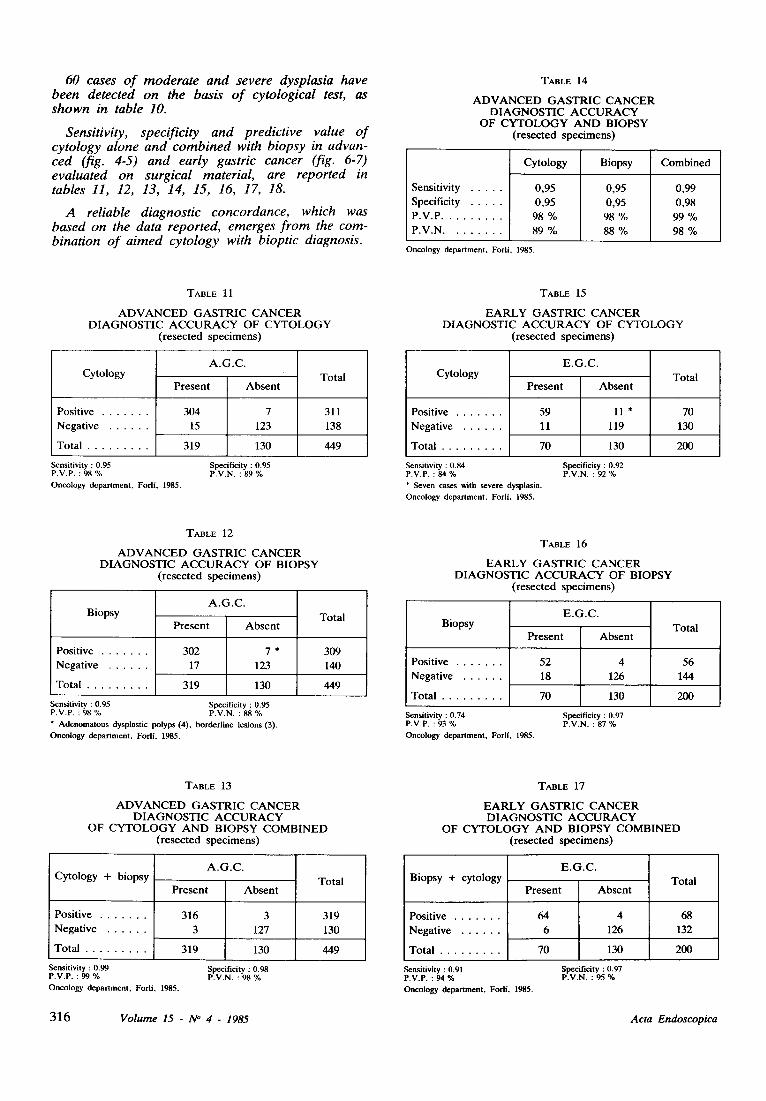
60 cases of moderate and severe dysplasia have been detected on the basis o f cytological test, as shown in table 10.
Sensitivity, specificity and predictive value of cytology alone and combined with biopsy in advan- ced (fig. 4-5) and early gastric cancer (fig. 6-7) evaluated on surgical material, are reported in tables 11, 12, 13, 14, 15, 16, 17, 18.
A reliable diagnostic concordance, which was based on the data reported, emerges from the com- bination o f aimed cytology with bioptic diagnosis.
TABLE 14
A D V A N C E D G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y
O F C Y T O L O G Y A N D B I O P S Y ( r e s e c t e d s p e c i m e n s )
Sens i t iv i ty
Spec i f i c i ty
P . V . P .
P . V . N .
C y t o l o g y
0 , 9 5
0 , 9 5
98 %
89 %
B i o p s y C o m b i n e d
0 ,95 0 ,99
0 ,95 0 , 9 8
98 % 99 %
88 % 98 %
Oncology department, Forll, 1985.
TABLE 11
A D V A N C E D G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y O F C Y T O L O G Y
( r e s e c t e d s p e c i m e n s )
C y t o l o g y
Pos i t i ve
�9 N e g a t i v e . . . . . . .
. T o t a l . . . . . . . . . .
A . G . C .
P r e s e n t A b s e n t
3 0 4 7
15 123
319 130
T o t a l
311
138
4 4 9
Sensitivity : 0.95 Specificity : 0.95 P.V.P. : 98 % P.V.N. : 89 % Oneology department, Forll, 1985.
TABLE 15
E A R L Y G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y O F C Y T O L O G Y
( r e s e c t e d s p e c i m e n s )
C y t o l o g y
Pos i t i ve
�9 N e g a t i v e . . . . . . .
�9 T o t a l . . . . . . . . . .
E . G . C .
P r e s e n t A b s e n t
59 11 *
11 119
7 0 130
T o t a l
70
130
200
Sensitivity : 0.84 P.V.P. : 84 % * Seven cases with severe dysplasia. Oneology department, Forli, 1985.
Specificity : 0.92 P.V.N. : 92 %
TABLE 12
A D V A N C E D G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y O F B I O P S Y
( r e s e c t e d s p e c i m e n s )
B i o p s y
P o s i t i v e
�9 N e g a t i v e . . . . . . .
T o t a l
A . G . C .
P r e s e n t A b s e n t
3 0 2 7 *
17 123
319 130
T o t a l
3 0 9
140
449
Sensitivity : 0.95 Specificity : 0.95 P.V.P. : 98 % P.V.N. : 88 % * Adenomatous dysplastic polyps (4), borderline lesions (3). Oncology department, Fodi. 1985.
TABLE 16
E A R L Y G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y O F B I O P S Y
( r e s e c t e d s p e c i m e n s )
B i o p s y
P o s i t i v e
�9 N e g a t i v e . . . . . . .
�9 T o t a l . . . . . . . . . .
E . G . C .
P r e s e n t A b s e n t
52 4
18 126
7 0 130
T o t a l
56
144
200
Sensitivity : 0.74 Specificity : 0.97 P.V.P. : 93 % P.V.N. : 87 % Oneology department, Forll, 1985.
TABLE 13
A D V A N C E D G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y
O F C Y T O L O G Y A N D B I O P S Y C O M B I N E D ( r e s e c t e d s p e c i m e n s )
C y t o l o g y + b i o p s y
P o s i t i v e
. N e g a t i v e . . . . . . .
T o t a l
A . G . C .
P r e s e n t A b s e n t
3 1 6 3
3 127
3 1 9 130
T o t a l
319
130
449
Sensitivity : 0.99 P.V.P. : 99 % Oncology department, Forli�9 1985.
Specificity : 0.98 P.V.N. : 98 %
TABLE 17
E A R L Y G A S T R I C C A N C E R D I A G N O S T I C A C C U R A C Y
O F C Y T O L O G Y A N D B I O P S Y C O M B I N E D ( r e s e c t e d s p e c i m e n s )
B i o p s y + c y t o l o g y
P o s i t i v e
�9 N e g a t i v e . . . . . . .
�9 T o t a l . . . . . . . . . .
E . G . C .
P r e s e n t A b s e n t
6 4 4
6 126
7 0 130
T o t a l
68
132
200
Sensitivity : 0.91 P.V.P. : 94 % Oncology department, Forli. 1985.
Specificity : 0.97 P.V.N. : 95 %
316 V o l u m e 1 5 - N ~ 4 - 1 9 8 5 A c t a E n d o s c o p i c a
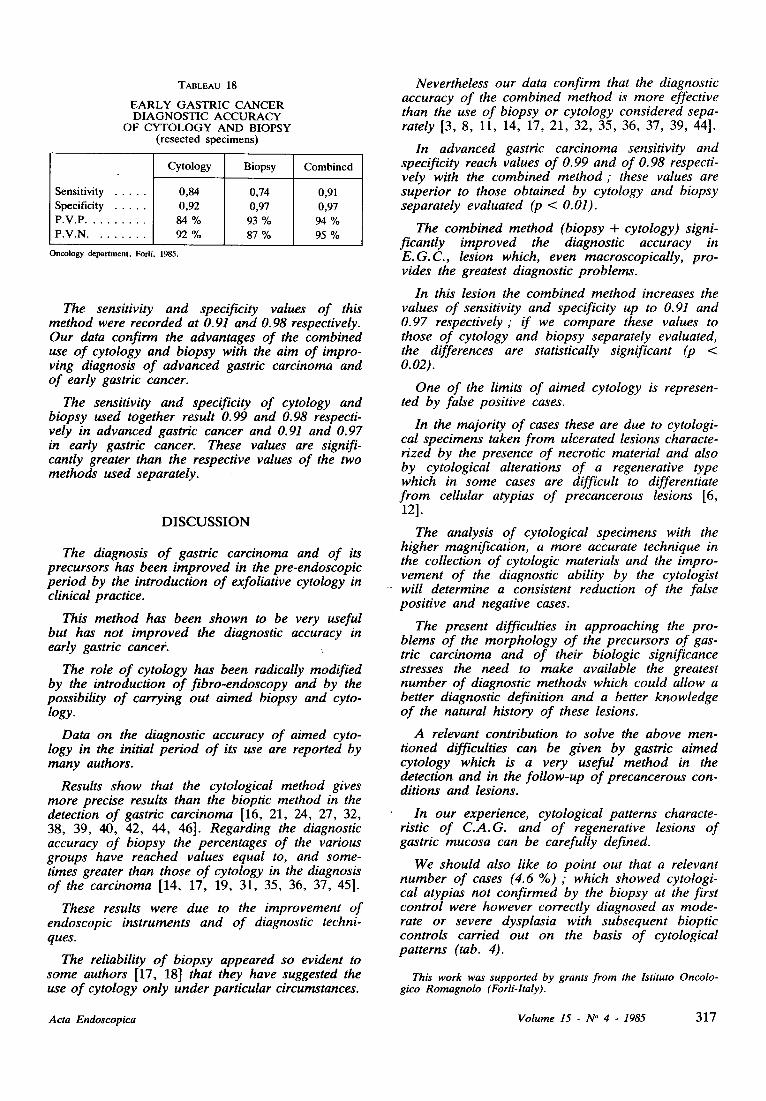
TABLEAU 18
EARLY GASTRIC CANCER DIAGNOSTIC ACCURACY
OF CYTOLOGY AND BIOPSY (resected specimens)
Sensitivity Specificity P.V.P. P.V.N.
Cytology Biopsy Combined
0,84 0,74 0,91 0,92 0,97 0,97 84 % 93 % 94 % 92 % 87 % 95 %
Ontology department, Forli. 1985.
The sensitivity and specificity values of this method were recorded at 0.91 and 0.98 respectively. Our data confirm the advantages of the combined use o f cytology and biopsy with the aim of impro- ving diagnosis o f advanced gastric carcinoma and o f early gastric cancer.
The sensitivity and specificity of cytology and biopsy used together result 0.99 and 0.98 respecti- vely in advanced gastric cancer and 0.91 and 0.97 in early gastric cancer. These values are signifi- cantly greater than the respective values of the two methods used separately.
DISCUSSION
The diagnosis o f gastric carcinoma and of its precursors has been improved in the pre-endoscopic period by the introduction o f exfoliative cytology in clinical practice.
This method has been shown to be very useful but has not improved the diagnostic accuracy in early gastric cance~.
The role o f cytology has been radically modified by the introduction o f fibro-endoscopy and by the possibility o f carrying out aimed biopsy and cyto- logy.
Data on the diagnostic accuracy of aimed cyto- logy in the initial period o f its use are reported by many authors.
Results show that the cytological method gives more precise results than the bioptic method in the detection of gastric carcinoma [16, 21, 24, 27, 32, 38, 39, 40, 42, 44, 46]. Regarding the diagnostic accuracy of biopsy the percentages of the various groups have reached values equal to, and some- times greater than those o f cytology in the diagnosis of the carcinoma [14, 17, 19, 31, 35, 36, 37, 45].
These results were due to the improvement of endoscopic instruments and o f diagnostic techni- ques.
The reliability o f biopsy appeared so evident to some authors [17, 18] that they have suggested the use o f cytology only under particular circumstances.
Nevertheless our data confirm that the diagnostic accuracy o f the combined method is more effective than the use of biopsy or cytology considered sepa- rately [3, 8, 11, 14, 17, 21, 32, 35, 36, 37, 39, 44].
In advanced gastric carcinoma sensitivity and specificity reach values of 0.99 and of O. 98 respecti- vely with the combined method ; these values are superior to those obtained by cytology and biopsy separately evaluated (p < 0.01).
The combined method (biopsy + cytology) signi- ficantly improved the diagnostic accuracy in E.G.C., lesion which, even macroscopically, pro- vides the greatest diagnostic problems.
In this lesion the combined method increases the values of sensitivity and specificity up to 0.91 and 0.97 respectively ; if we compare these values to those of cytology and biopsy separately evaluated, the differences are statistically significant (p < 0.02).
One of the limits o f aimed cytology is represen- ted by false positive cases.
In the majority of cases these are due to cytologi- cal specimens taken from ulcerated lesions characte- rized by the presence of necrotic material and also by cytological alterations o f a regenerative type which in some cases are difficult to differentiate from cellular atypias o f precancerous lesions [6, 121.
The analysis of cytological specimens with the higher magnification, a more accurate technique in the collection of cytologic materials and the impro- vement of the diagnostic ability by the cytologist will determine a consistent reduction of the false positive and negative cases.
The present difficulties in approaching the pro- blems o f the morphology o f the precursors of gas- tric carcinoma and of their biologic significance stresses the need to make available the greatest number of diagnostic methods which could allow a better diagnostic definition and a better knowledge o f the natural history of these lesions.
A relevant contribution to solve the above men- tioned difficulties can be given by gastric aimed cytology which is a very useful method in the detection and in the follow-up of precancerous con- ditions and lesions.
In our experience, cytological patterns characte- ristic of C.A.G. and o f regenerative lesions of gastric mucosa can be carefully defined.
We should also like to point out that a relevant number of cases (4.6 %) ; which showed cytologi- cal atypias not confirmed by the biopsy at the first control were however correctly diagnosed as mode- rate or severe dysplasia with subsequent bioptic controls carried out on the basis o f cytological patterns (tab. 4).
This work was suppor ted by grants f r o m the lstituto Oncolo- gico Romagno lo (Forli-ltaly).
Acta Endoscopica Vo lume 15 - N ~ 4 - 1985 317
September 7-12 1986
8 th CONGRESS OF GASTROENTEROLOGY
6 th CONGRESS OF DIGESTIVE ENDOSCOPY
3 rd CONGRESS OF COLO-PROCTOLOGY
318
For fur ther informat ion see p. X X X V
V o l u m e 15 - N ~ 4 - 1 9 8 5 A c t a E n d o s c o p i c a