Embed Size (px)
Citation preview

Le t ra i tement par laser des malformations vasculaires du tube digestif
V. M A U N O U R Y *, J . M . B R U N E T A U D **, D . C O C H E L A R D ***, A . C O R T O T **** , J.C. P A R I S ****
* C e n t r e M u l t i d i s c i p l i n a i r e d e T r a i t e m e n t p a r L a s e r , C . H . R . L i l l e ( F r a n c e ) ** U n i M I . N . S . E . R . M . 279 , L i l l e
*** L a b o r a t o i r e d e b i o m a t h ~ m a t i q u e s , f a c u l M d e p h a r m a c i e , L i l l e **** C l i n i q u e de s M a l a d i e s d e l ' A p p a r e i l D i g e s t i f , C . H . R . L i l l e
Laser treatment for vascular malformations of the digestive tract
Tratamiento de las malformaciones vasculares del tracto digestive con laser
RI~SUMI~
Les r6sultats du traitement par photocoagulation laser des malformations vasculaires h6morragiques du tube digestif sont rapport6s chez 67 malades. Le but du traitement 6tait : a) d'arr6ter le saignement et de pr6venir sa r6cidive lorsqu'il 6tait dO h des angiomes isol6s gastroduod6naux (43) ou coliques (12), b) de r6duire les transfusions sanguines lorsqu'il 6tait dO ~ une maladie angiomateuse syst6matis6e (Rendu-Osler : 10, syndrome de Bean : 2). Le laser argon a 6t6 le plus souvent utilis6 pour coaguler sans volatiliser sauf en cas d'h6morragie active, de nouveau saignement d 'un angiome d6j~ trait6 par le laser argon et pour les angiomes tub6reux, oO le laser Nd Y A G a 6t6 utilis6. Le traitement initial a permis la correction stable de la spoliation sanguine dans 100 % des cas sans complications imm6diates ou retard6es en dehors d'une perforation colique non li6e au tir laser. Treize pour cent des malades avec des angiomes isol6s ont resaign6 soit de nouveaux angiomes qui ont 6t~ retrait6s avec succ~s (4 malades), soit de cause non identifi~e (3 malades). La qualit6 de vie des malades avec maladie de Rendu- Osier a 6t6 transform6e bien qu'une ou plusieurs r6cidives h6morragiques soient survenues chez 66 % d'entre eux. Cette 6tude confirme l'efficacit6 et la s6curit6 de la photocoagulation par laser des malformations vasculaires digestives h6morragiques.
S U M M A R Y
The results o f laser treatment for bleeding vascular malformations o f digestive tract are reported in 67 patients. The aim o f the treatment was : a) to stop the hemorrhage and to prevent its recurrence when the angiomas were isolated in the upper tract (43) or in the colon (12), b) to reduce the blood transfusions in patients with Osler-Rendu disease (10) or Bean syndrom (2). The argon laser was usually used to coagulate without to vaporize excepted in active bleeding, recurrence after a previous argon laser treatment and for tuberous angiomas in which the Nd Y A G laser was used. The success rate was 100 % after initial treatment without immediate or lasted complications excepted one perforation not due to the laser shot itself. Thirteen percent o f patients with isolated angiomas recurred from new angiomas successfully retreated in 4 patients or from non-identified origin in 3 patients. The quality o f life was actually improved in patients with Osler-Rendu disease although 66 % o f them recurred. This study is in favor o f the efficiency and safety o f laser treatment for bleeding vascular malformations.
R E S U M E N
Se describen los resultados del tratamiento con laser de malformaciones vasculares hemorragicus del tubo digestivo en 67 pacien- tes. El objectivo del tratamiento fuP. : a. - - Detenci6n de la hemorragia o prevenci6n de recidivas en los casos de angiomas gastroduodenales (43) o col6nicos (12) aislados, b. - - Reducci6n del mimero de transfusiones sangulneas cuando se trataba de una enfermedad angiomatosa sisMmica (Rendu-Osler (10), sindrome de Bean (2). El laser empleado corn mayor frecuencia fu# el de argon, con el fin de coagular sin volatizar, excepto en los casos de hemorragia activa, de resangrado de un angioma ya tratado con laser argon y e n los casos de angioma tuberoso ; en todos ellos se utiliz6 el laser ND-YAG. El tratamiento inicial permiti6 la detenci6n estable del 100 % de casos sin complicaciones immediatas o a largo plazo, si se exceptaa un caso de perforaci6n de colon, no relacionada con el tratumiento con laser. De los pacientes portadors de angiomas aislados un 13 % resangr6, siendo debida dicha hemorragia a nuevos angiomas que fueron tratados con ~xito en 4 cusos ; en 3 pacientes no se pudo identificar la causa de la recidiva hemorrtigica. La calidad de vida de los pacientes ufectos de enfermedad de Rendu-Osler fu~ mejorada, si bien en un 66 % de casos una o varias recidivas reaparecieron. Este estudio confirma la eficacia y segurudad de la fotocoagulati6n con laser en los pacientes portadores de malforma- ciones vasculares del tubo digestivo.
Las malformaciones vasculares (MV) del tracto gatrointestinal (GI) pueden set responsable de hemorragias agudas o de anemia cr6nica. El tratamiento era quirurgico. En la actualidad tiende a set conservador gracias a la endoscopia (24). Aportamos nuestra experiencia de 8 ahos y medio de tratamiento endosc6pico en el Centro de Laser de Lille.
Tir6s h part : V. M A U N O U R Y , Centre Multidiseiplinaire de Traitement par Laser, H6pital C.-Huriez, C.H.R. 59037 Lille Cedex (France).
Mots-cl~s : angiome digestif, photocoagulation laser.
Key-words : laser photocoagulation, vascular malformations.
Palabrus-clave : angioma digestivo, fotocoagulacion con laser.
Acta Endoscopica Volume 1 8 - N ~ 2 - 1988 73
IN T ROD UCTION
Les malformations vasculaires du tube digestif peuvent 6tre responsables d'un saignement soit patent et parfois abondant, soit mod6r6 ou occulte mais volontiers r6cidivant. Depuis quelques ann6es [24], leur coagulation per-endoscopique tend ~ se substituer au traitement chirurgical sou- vent trop limit6 ou excessivement mutilant. Nous rapportons ici notre exp6rience de leur photocoa- gulation par laser ces huit derni6res ann6es.
M A L A D E S E T ME, THODES
Malades
Nous avons trait6 67 malades (32 hommes et 35 femmes) ; trente neuf pr6sentaient une h6morragie digestive active ou r6cente et 28 une an6mie ferri- prive rapport6es ~ des angiomes digestifs sur les crit6res suivants : a) stigmates d'h6morragie active ou r6cente au niveau d'un ou plusieurs angiomes l'endoscopie, b)his toire d'h6morragies digestives ou d'an6mie ferriprive sans autre 6tiologie que des angiomes constamment retrouv6s. Nous avons r6parti ces 67 malades en 5 groupes (tableau I ) : les 2 premiers rassemblaient ceux qui pr6sentaient des angiomes gastro-duod6naux, soit isol6s (grou- pe I), soit dans le cadre d'une maladie de Rendu- Osier (groupe II), les 2 suivants ceux avec des angiomes coliques, droits (groupe III) ou gauches (groupe IV), le dernier (groupe V) ceux avec un syndrome de Bean (~, Blue rubber bled naevus syndrom ~ : phacomatose caract6ris6e par des angiomes caverneux du tube digestif et parfois de la peau).
TABLEAU I
T R A I T E M E N T P A R P H O T O C O A G U L A T I O N L A S E R DES M A L F O R M A T I O N S V A S C U L A I R E S D U T U B E
D I G E S T I F ; R I ~ P A R T I T I O N D ES 67 M A L A D E S EN F O N C T I O N D E L A L O C A L I S A T I O N DES A N G I O M E S
E T D U C A D R E N O S O L O G I Q U E
N
i G r o u p e I . . . 43
Groupe II . . . 10
Groupe III . . 8
Groupe IV . . 4
Groupe V . . . 2
Le syndrome de Bean ~hacomatose caract6ris6e ~arfois de la peau.
Age moyen (ans)
Local isat ion Nosologie
71 Gastro- duod6nale
56 Gastro- duod6nale
71 Colique droi te
37 rectum et colon gauche
13 pan-digest if syndrome de Bean *
Blue Rubber 3led Naevus Syndrom) est une Jar des angiomes caverneux du tube digestif et
isol6e
R e n d u Osler
isol6e
isol6e
Seize malades (24 %) pr6sentaient des facteurs de morbidit6 associ6s : trois traitements anticoagu-
lants, six insuffisances r6nales chroniques dont 2 en h6modialyse, deux r6tr6cissements aortiques, une thrombocyt6mie et une maladie de Willebrant, deux traitements anti-inflammatoires au long cours, et une hypertension portale.
Le but du traitement 6tait : a) d'arr6ter le sai- gnement digestif et de pr6venir sa r6cidive Iors- qu'il 6tait dO ~ des angiomes isol6s (groupes I, III et IV), b) de r6duire les transfusions sanguines en pr6venant ainsi les accidents d'incompatibilit6 Iors- que les h6morragies 6taient dues ~ une maladie angiomateuse syst6matis6e (groupes II et V).
Mdthode
Nous avons utilis6 les endoscopes GIF Q et CF LB3W (Olympus, Tokyo, Japon). Les sondes laser 6taient prot6g6es par une insuflation d'azote (1,5 l/mn). En endoscopic haute, la sonde laser avait un diam~tre ext6rieur de 1,6 mm ; l'6vacua- tion de l'azote s'effectuait par le canal op6rateur laiss6 ouvert. En endoscopie basse, elle avait un diam~tre de 2,2 mm et le gaz s'6vacuait par une sonde plac6e le long de l'endoscope dans le rectum.
Dans le tractus digestif sup6rieur, nous avons ie plus souvent utilis6 un laser argon (Lasersonics 770, Santa Clara, Californie) ~ une puissance de 4 W e n sortie de fibre, avec un spot de 2 mm de diam6tre (densit6 de puissance 125 W / cm2), en tir de plusieurs secondes, pour coaguler sans volatili- ser. Nous avons rarement utilis6 un laser Nd:YAG (YM 101, Cilas, Marcoussis, France) en cr6neaux de 1 s, puissance 50 W, avec un spot identique (densit6 de puissance 1 600 W/ cm L) en cas de saignement actif, de r~cidive apres un premier traitement par le laser argon et pour les angiomes tub6reux. Dans le colon, l'utilisation du laser Nd:YAG a 6t6 encore plus exceptionelle : nous n'avons trait6 ainsi que les angiomes tub6reux du colon gauche, et en compl6ment du laser argon, un angiome du caecum particuli6rement h6morra- gique.
Le traitement 6tait r6alis6 sans pr6m6dication et en ambulatoire lorsque le malade n'6tait pas hos- pitalis6 du fait de son h6morragie. Le plus grand nombre d'angiomes, en commenqant par les plus d6clives, 6tait trait6 ~t chaque s6ance. Lorsque le traitement provoquait un saignement, nous ne retraitions l'angiome qu'apr6s son tarissement spontan6. Les malades 6taient revus syst6matique- ment les semaines suivantes pour v6rifier la des- truction des 16sions coagul6es et 6ventuellement traiter des angiomes initialement m6connus. Une simple surveillance clinique et biologique (h6mo- gramme) 6tait assur6e par la suite sauf pour les malades du groupe II qui avaient une endoscopic syst6matique t o u s l e s 3 mois, avec traitement de nouveaux angiomes le cas 6ch6ant ; parall61ement, le traitement des localisations nasales en cas de maladie de Rendu Osier 6tait effectu6 au laser argon [17] par nos coll6gues O.R.L.
74 V o l u m e 1 8 - N ~ 2 - 1 9 8 8 A c t a E n d o s c o p i c a
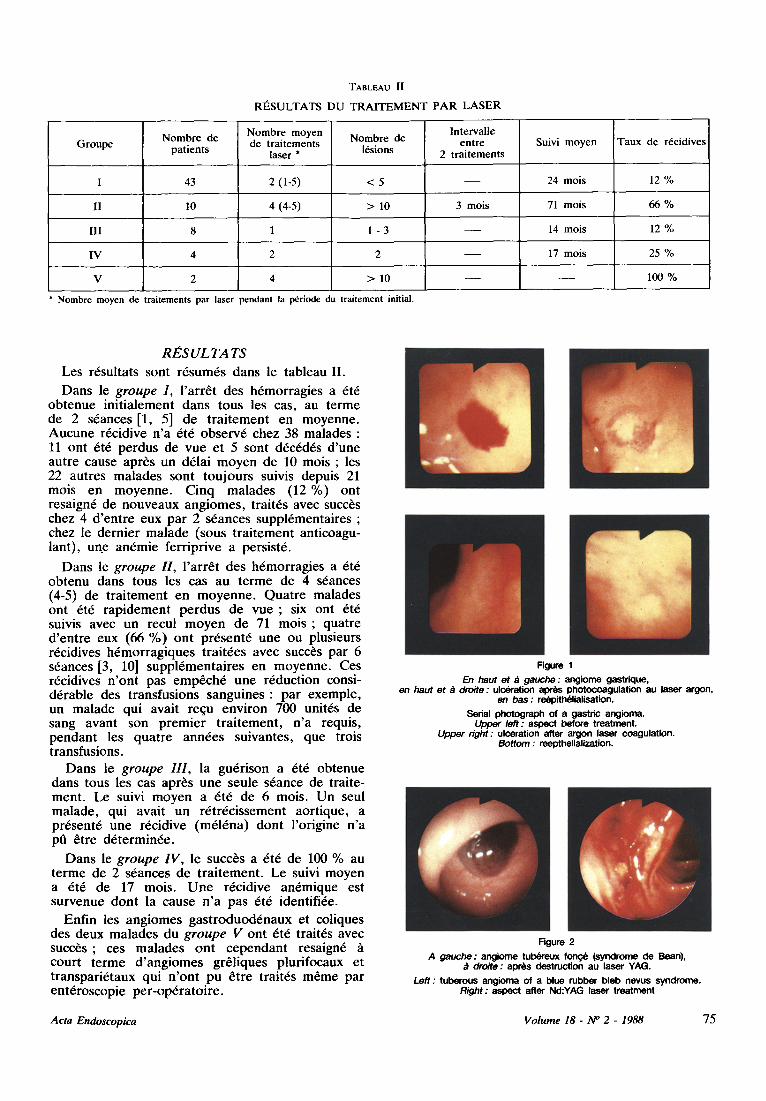
TABLEAU II
RI~SULTATS DU TRAITEMENT PAR LASER
Groupe Nombre de patients
Nombre moyen de traitements
laser * Nombre de
16sions
lntervalle entre
2 traitements Suivi moyen Taux de rdcidives
I 43 2 (1-5) < 5 24 mois 12 %
II 10 4 (4-5) > 10 3 mois 71 mois 66 %
III 8 1 1 - 3 14 mois 12 %
IV
V
17 mois
> 10
25 %
I00 %
Nombre moyen de traitements par laser pendant la p~riode du traitement initial.
R E S U L T A TS
Les r6sultats sont r6sum6s dans ie tableau II.
Dans le g r o u p e I , l 'arr6t des h6morragies a 6t6 obtenue init ialement dans t o u s l e s cas, au te rme de 2 s6ances [1, 5] de t ra i tement en moyenne. Aucune r6cidive n 'a 6t6 observ6 chez 38 malades : 11 ont 6t6 perdus de vue et 5 sont d6c6d6s d 'une autre cause apr/~s un d61ai moyen de 10 mois ; les 22 autres malades sont toujours suivis depuis 21 mois en moyenne . Cinq malades (12 %) ont resaign6 de nouveaux angiomes , trait6s avec succ6s chez 4 d 'en t re eux par 2 s6ances suppl6mentaires ; chez le dernier malade (sous t ra i tement anticoagu- lant), un.e an6mie ferr iprive a persist6.
Dans le g r o u p e H, l 'arr6t des h6morragies a 6t6 obtenu dans t o u s l e s cas au t e rme de 4 s6ances (4-5) de t ra i tement en moyenne . Qua t re malades ont 6t6 rap idement perdus de v u e ; six ont 6t6 suivis avec un recu| m o y e n de 71 m o i s ; quatre d 'en t re eux (66 %) ont pr6sent6 une ou plusieurs r6cidives h6morragiques trait6es avec succ~s par 6 s6ances [3, 10] suppl6menta i res en moyenne. Ces r6cidives n 'on t pas emp6ch6 une r6duction consi- d6rable des transfusions sanguines : par exemple , un malade qui avait requ environ 700 unit6s de sang avant son p remie r t ra i tement , n 'a requis, pendant les quatre ann6es suivantes, que trois transfusions.
Dans le g r o u p e I I I , la gu6rison a 6t6 obtenue darts tous les cas apr~s une seule s6ance de traite- ment . Le suivi moyen a 6t6 de 6 mois. Un seul malade , qui avait un r6tr6cissement aort ique, a pr6sent6 une r6cidive (m616na) dont l 'origine n 'a pfi 6tre d6termin6e.
Dans le g r o u p e I V , le succ~s a 6t6 de 100 % au te rme de 2 s6ances de t ra i tement . Le suivi moyen a 6t6 de 17 mois. U n e r6cidive an6mique est survenue dont la cause n ' a pas 6t6 identifi6e.
Enfin les angiomes gas t roduod6naux et coliques des deux malades du g r o u p e V ont 6t6 trait6s avec succ6s ; ces malades ont cependant resaign6 court t e rme d ' ang iomes gr61iques plurifocaux et t ranspari6taux qui n 'on t pu 6tre trait6s m6me par ent6roscopie per -op6ra to i re .
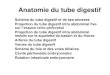
Figure 1 En haut et .~ gauche : angiome gastrique,
en haut et ~ droite : ulceration apr~s photoeoagulation au laser argon, en bas : re~pitl~lialisation.
Serial photograph of a gastric angioma. Upper left : aspect before treatment.
Upper r ight: ulceration after argon laser coagulation. Bottom : reepthelialization.
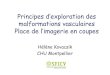
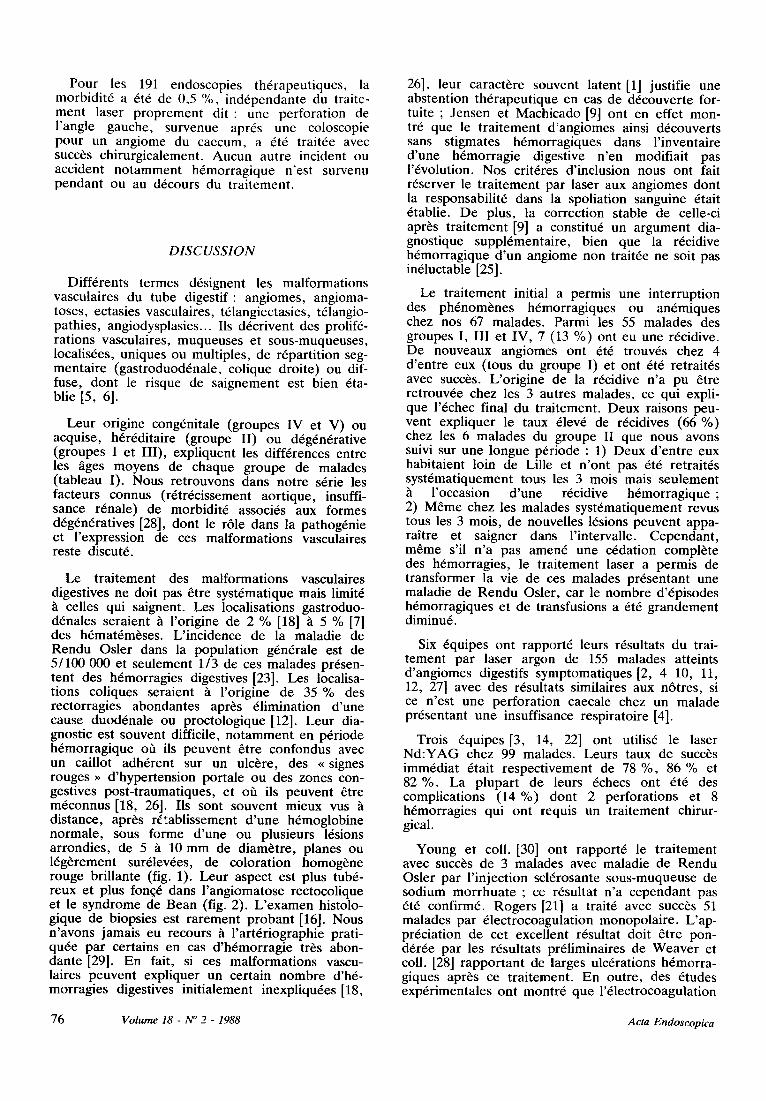
Figure 2
A gauche : angiome tul~reux f o n ~ (syndrome de Bean), droite : aprils destruction au laser YAG.
Left : tuberous angioma of a blue rubber bleb nevus syndrome, Right: aspect after Nd:YAG laser treatment
Acta Endoscopica Volume 18- N ~ 2 - 1988 75
Pour les 191 endoscopies th6rapeutiques, la morbidit6 a 6t6 de 0,5 %, ind6pendante du traite- ment laser proprement di t : une perforation de l'angle gauche, survenue apr6s une coloscopie pour un angiome du caecum, a 6t6 trait6e avec succ6s chirurgicalement. Aucun autre incident ou accident notamment h6morragique n'est survenu pendant ou au d6cours du traitement.
DISCUSSION
Diff6rents termes d6signent les malformations vasculaires du tube digestif : angiomes, angioma- toses, ectasies vasculaires, t61angiectasies, t61angio- pathies, angiodysplasies... Ils d6crivent des prolif6- rations vasculaires, muqueuses et sous-muqueuses, localis6es, uniques ou multiples, de r6partition seg- mentaire (gastroduod6nale, colique droite) ou dif- fuse, dont le risque de saignement est bien 6ta- blie [5, 6].
Leur origine cong6nitale (groupes IV et V) ou acquise, h6r6ditaire (groupe II) ou d6g6n6rative (groupes I et III), expliquent les diff6rences entre les ages moyens de chaque groupe de malades (tableau I). Nous retrouvons dans notre s6rie les facteurs connus (r6tr6cissement aortique, insuffi- sance r6nale) de morbidit6 associ6s aux formes d6g6n6ratives [28], dont le r61e dans la pathog6nie et l'expression de ces malformations vasculaires reste discut6.
Le traitement des malformations vasculaires digestives ne doit pas 6tre syst6matique mais limit6
celles qui saignent. Les localisations gastroduo- d6nales seraient ~ l'origine de 2 % [18] h 5 % [7] des h6mat6m~ses. L'incidence de la maladie de Rendu Osier dans la population g6n6rale est de 5/100 000 et seulement 1/3 de ces malades pr6sen- tent des h6morragies digestives [23]. Les localisa- tions coliques seraient h l'origine de 35 % des rectorragies abondantes apr6s 61imination d'une cause duod6nale ou proctologique [12]. Leur dia- gnostic est souvent difficile, notamment en p6riode h6morragique o/~ ils peuvent 6tre confondus avec un caillot adh6rent sur un ulc6re, des ~ signes rouges ~ d'hypertension portale ou des zones con- gestives post-traumatiques, et off ils peuvent 6tre m6connus [18, 26]. Ils sont souvent mieux vus distance, apr6s r~tablissement d'une h6moglobine normale, sous forme d'une ou plusieurs 16sions arrondies, de 5 h 10 mm de diam6tre, planes ou 16g6rement sur61ev6es, de coloration homog6ne rouge brillante (fig. 1). Leur aspect est plus tub6- reux et plus fon~6 dans l'angiomatose rectocolique et le syndrome de Bean (fig. 2). L'examen histolo- gique de biopsies est rarement probant [16]. Nous n'avons jamais eu recours ta l'art6riographie prati- qu6e par certains en cas d'h6morragie tr~s abon- dante [29]. En fait, si ces malformations vascu- laires peuvent expliquer un certain nombre d'h6- morragles digestives initialement inexpliqu6es [18,
26], leur caract6re souvent latent [1] justifie une abstention th6rapeutique en cas de d6couverte for- tuite ; Jensen et Machicado [9] ont en effet mon- tr6 que le traitement d'angiomes ainsi d6couverts sans stigmates h6morragiques dans l'inventaire d'une h6morragie digestive n'en modifiait pas l'6volution. Nos crit6res d'inclusion nous ont fait r6server le traitement par laser aux angiomes dont la responsabilit6 dans la spoliation sanguine 6tait 6tablie. De plus, la correction stable de celle-ci apr~s traitement [9] a constitu6 un argument dia- gnostique suppl6mentaire, bien que la r6cidive h6morragique d'un angiome non trait6e ne soit pas in61uctable [25].
Le traitement initial a permis une interruption des ph6nom6nes h6morragiques ou an6mlques chez nos 67 malades. Parmi les 55 malades des groupes I, III et IV, 7 (13 %) ont eu une r6cidive. De nouveaux angiomes ont 6t6 trouv6s chez 4 d'entre eux (tous du groupe I) et ont 6t6 retrait6s avec succ~s. L'origine de la r6cidive n'a pu 6tre retrouv6e chez les 3 autres malades, ce qui expli- que l'6chec final du traitement. Deux raisons peu- vent expliquer le taux 61ev6 de r6cidives (66 %) chez les 6 malades du groupe II que nous avons suivi sur une longue p6riode : 1) Deux d'entre eux habitaient loin de Lille et n'ont pas 6t6 retrait6s syst6matiquement tous les 3 mois mais seulement ta l'occasion d'une r6cidive h6morragique ; 2) M6me chez les malades syst6matiquement revus tousles 3 mois, de nouvelles 16sions peuvent appa- raitre et saigner dans l'intervalle. Cependant, m~me s'il n'a pas amen6 une c6dation compl6te des h6morragies, le traitement laser a permis de transformer la vie de ces malades pr6sentant une maladie de Rendu Osier, car le nombre d'6pisodes h6morragiques et de transfusions a 6t6 grandement diminu6.
Six 6quipes ont rapport6 leurs r6sultats du trai- tement par laser argon de 155 malades atteints d'angiomes digestifs symptomatiques [2, 4 10, 11, 12, 27] avec des r6sultats similaires aux n6tres, si ce n'est une perforation caecale chez un malade pr6sentant une insuffisance respiratoire [4].
Trois 6quipes [3, 14, 22] ont utilis6 le laser Nd:YAG chez 99 malades. Leurs taux de succ6s imm6diat 6tait respectivement de 78 %, 86 % et 82 %. La plupart de leurs 6checs ont 6t6 des complications (14 %) dont 2 perforations et 8 h6morragies qui ont requis un traitement chirur- gical.
Young et coll. [30] ont rapport6 le traitement avec succ6s de 3 malades avec maladie de Rendu Osier par l'injection scl6rosante sous-muqueuse de sodium morrhuate ; ce r6sultat n'a cependant pas 6t6 confirm6. Rogers [21] a trait6 avec succ6s 51 malades par 61ectrocoagulation monopolaire. L'ap- pr6ciation de cet excellent r6sultat doit 6tre pon- d6r6e par les r6sultats pr61iminaires de Weaver et coll. [28] rapportant de larges ulc6rations h6morra- giques apr6s ce traitement. En outre, des 6tudes exp6rimentales ont montr6 que l'61ectrocoagulation
76 V o l u m e 18 - N ~ 2 - 1 9 8 8 A c t a E n d o s c o p i c a
monopolaire 6tait peu reproductible [15]. L'61ec- trocoagulation multipolaire (Bicap, ACMI, USA), comme la coagulation par sonde chauffante (Hea- ter Probe, Olympus, Japon), n'ont pas cet incon- v6nient. Jensen et coll. [10, 11] ont montr6 une efficacit6 et une s6curit6 comparables des traite- ments par Heater Probe, Bicap ou laser argon; cette derni~re technique est apparue cepen- dant [11] plus rapide et plus facile en cas d'angiomes multiples.
Notre exp6rience confirme l'efficacit6 et la s6cu- rit6 de la photocoagulation par laser argon des malformations vasculaires digestives accessibles en endoscopie. Elle permet un contr61e satisfaisant des h6morragies digestives de la maladie de Rendu Osier ; chez ces malades, un traitement r6gulier est souhaitable. Les accidents rapport6s dans la litt6rature avec le laser Nd:YAG justifient la pru- dence dans son utilisation pour le traitement des angiomes.
R~F~RENCES
1. BOLEY S.J., SAMMARTANO R., ADAMS A., DIBIASE A., KLEINHAUS S., SPRAYREGEN S. - - On the nature and etiology of vascular ectasias of the colon. Gastroenterology, 1977, 72, 650-660.
2. BOWERS J.H., DIXON J.A.. - - Argon laser photocoagu- lation of vascular malformations in the GI tract. Gastroin- test. Endosc., 1982, 28, 2, 126 (abstr).
3. BOWN S.G., SWAIN C.P., STOREY D.W., COLLINS C., MATTHEWSON K., SALMON P.R., CLARK C.G. - - Endoscopic laser treatment of vascular anomalies of the upper gastrointestinal tract. Gut, 1985, 26, 1338-1348.
4. CELLO J.P., GRENDELL J.H. - - Endoscopic laser treat- ment for gastrointestinal vascular ectasias. Ann. Intern. Med., 1986, 104, 352-354.
5. DELMONT J., RAMPAL P., LJUNGGREN B. - - Angio- dysplasies d~g6n6ratives du colon droit. Sem. H6p. Paris, 1978, 54, 1331-1335.
6. FARUP P.G., ROSSELAND A.R. , STRAY N. - - Locali- zed telangiopathy of the stomach and duodenum diagnosed and treated endoscopically. Case reports and review. En- doscopy, 1981, 13, 1-6.
7. FLEISCHER D. - - Etiology and prevalence of severe persistent upper gastrointestinal bleeding. Gastroenterology, 1983, 84, 538-543.
8 . G U N N L A U G S S O N O . - - Angiodysplasia of the stomach and duodenum. Gastrointest. Endosc., 1985, 31, 251-254.
9 . J E N S E N D . M . , M A C H I C A D O G . A . - - Endoscopic treat- ment of incidental angioma in patients with severe gastroin- testinal bleeding. Gastrointest. Endosc., 1985, 31, 158 (abs- tract).
10. JENSEN D.M., MACHICADO G.A., REEDY T.E., ELASHOFF J. - - Bleeding U G I angioma: endoscopic coagulation and outcome. Gastrointest. Endosc., 1986, 32, 142 (abstract).
11. JENSEN D.M., MACHICADO G.A., SILPA M.L. - - Treatment of GI angiomata with argon laser, heater probe, or bipolar electrocoagulation. Gastrointest. Endosc., 1984, 30, 134 (abstract).
12. JENSEN D.M., M A C H I C A D O G.A., TAPIA J.I. - - Emergent colonoscopy in patients with severe hematoche- zia. Gastrointest. Endosc., 1983, 29, 177 (abstract).
13. JENSEN D.M., MACHICADO G.A., TAPIA J.I, BEI- LIN D . B . - - Endoscopic treatment of hemangiomata with argon laser in patients with gastrointestinal bleeding. Gas- troenterology, 1982, 82, 1093 (abstract).
14. JOHNSTON J.H. - - Complications following endoscopic laser therapy. Gastrointest. Endosc., 1982, 28, 2, 135 (abs- tract).
15. JOHNSTON J.H., JENSEN D.M., MA U T N E R W. - - Comparison of endoscopic electrocoagulation and laser photocoagulation of bleeding canine gastric ulcers. Gas- troenterolog~, 1982, 82, 904-910.
16. MITSUDO S.M., BOLEY S.J., B R A N D T L.J. - - Vascu- lar ectasias of the right colon in the elderly: a distinct pathologic entity. Human. Pathol., 1979, 10, 585-600.
17 PIQUET J.J., B R U N E T A U D J.M., M O S Q U E T L., BURNY A., TON J. - - Laser /t argon et maladie de Rendu Osier. Journal Fran~ais d'Oto-Laryngologie, 1985, 34, 325-326.
18. QUINTERO E., PIQUE J.M., BOMBI J .A. , ROS E., BORDAS J.M., RIVES A., TERES J., RODES J. - - U p - per gastrointestinal bleeding caused by gastroduodenal vas- cular malformations. Dig. Dis. Sc., 1986, 31, 897-905.
19. RICHARDSON J.D., MAX M.H., FLINT L.M., SCHWEISINGER W., HOWARDM. , AUST J.B. - - Bleeding vascular malformations of the intestine. Surgery, 1978, 84, 430-436.
20. ROGERS B.H.G. - - Endoscopic diagnosis and therapy of mucosal vascular abnormalities of the gastrointestinal tract occuring in elderly patients and associated with cardiac, vascular and pulmonary disease. Gastrointest. Endosc., 1980, 26, 134-138.
21. ROGERS B.H.G. - - Endoscopic electrocoagulation of vas- cular abnormalities of the gastrointestinal tract in 51 pa- tients. Gastrointest. Endosc., 1982, 28, 2, 142 (abstract).
22. RUTGEERTS P., VAN GOMPEL F., G E B O E S K., VANTRAPPEN G., BROECKAERT L., C O R E M A N S G. - - Long term results of treatment of vascular malforma- tions of the gastrointestinal tract by Nd:YAG laser photo- coagulation. Gut., 1985, 26, 586-593.
23. SMITH C.R., BARTHOLOMEW R.G, CAIN J.C. - - Hereditary hemorrhagic telangiectasia and gastrointestinal hemorrhage. Gastroenterology, 1963, 44, 1-6.
24. SUDRY P., B R U N E T A U D J.M., PARIS J.C., BRE- T A G N E J.F., DANIELOU F., B O U R E T J.F., LE BO- DIC M . F . , LE BODIC L . - - La photocoagulation par laser ~ argon des angiomes digestifs : h propos de quinze cas. Gastroenterol. Clin. Biol., 1981, 5, 426-432.
25. TEDESCO F.J., GRIFFIN J.W., KHAN A.Q. - - Vascu- lar ectasia ow the colon : clinical, colonoscopic and radio- graphic features. J. Clin. Gastroenterol., 1980, 2, 233-238.
26. THOMPSON J.N., SALEM R.R., H E M I N G W A Y A.P., REES H.C., HODGSON H.J.F., WOOD C.B., ALLI- SON D . J . , S P E N C E R J. - - Specialist investigation of obscure gastrointestinal bleeding. Gut, 1987,28, 47-51.
27. WAITMAN A.M., GRANT D.Z., C H A T E A U F. - - Argon laser photocoagulation treatment of patients with acute and chronic bleeding secondary to telang acute and chronic bleeding secondary to telangiectasia. Gastrointest. Endosc., 1982, 28, 153 (abstract).
28. W E A V E R G.A. , ALPERN H.D., DAVIS J.S., R A M S E Y W . J . , R E I C H E L D E R F E R M . - - Gastrointestinal angio- dysplasia associated with aortic valve disease: part of a spectrum of angiodysplasia of the gut. Gastroenterology, 1979, 77, 1-11.
29. WOLFF W.I., GROSSMAN M.B., SHINYA H. - - Angio- dysplasia of the colon : diagnosis and treatment. Gastroen- terology, 1977, 72, 329-333.
30. Y O U N G W., GIBBERT V., FEINSTAT T., T R U D E A U W. - - The recurrent upper gastrointestinal bleeding in hereditary hemorrhagic telengiectasia successfully treated by endoscopic sclerotherapy. Gastrointest. Endosc., 1982, 28, 2, 148 (abstract).
Acta Endoscopica Volume 18 - N ~ 2 - 1988 77
Vascular malformations (VM) of the gastrointesti- nal tract (GI) can be responsible of acute digestive hemorrhages or chronic anemia. The treatment was previously surgical. It tends now to be conservative with endoscopic treatment [ 2 4 ] . We report our 8 years experience with endoscopic laser treatment at the Lille Laser Center.
P A T I E N T S A N D M E T H O D
P a t i e n t s
Sixty seven patients (32 males and 35 females) were referred to the Laser Center for endoscopic treatment of a VM. Thirty nine presented recently with an active hemorrhage and 28 with chronic anemia from GI blood loss. The VM was conside- red as the cause of the digestive hemorrhage because 1) stigmata of hemorrhages were seen during endoscopy at the VM, or 2) VM were the only abnormality found during repeated endoscopies for multiple digestive hemorrhages.
The patients were divided into five groups (Table I). Group I and H had an upper GI VM (group I : no familial history, group H : Osier - Weber - Rendu syndrome, O-W-R). Group III and IV patients had colonic VM (group 3 : right colon, group 4 : left colon). Group V patients had a blue rubber bleb nevus syndrome (B-R-B-N). This syn- drome consists of cavernous angiomas distributed throughout the entire digestive tract along with non- digestive localizations such as skin vascular tumors.
TABLE I
B R E A K D O W N OF THE PATIENTS BY LOCALIZATION AND ETIOLOGY
No. Mean age Localization Etiology
G r o u p e I . . . 43 71
G r o u p e I I . . . 10 56
G r o u p e I I I . . 8 71
G r o u p e I V . . 4 37
G r o u p e V . . . 2 13
u p p e r G I
u p p e r G I
r i gh t colon
left colon
entire tract
isolated
O - W - R *
isolated
isolated
B - R - B - N *
O-W-R is Osler-Weber-Rendu syndrome and B-R-B-N is blue rubber bled nevus syndrome.
Associated treatments and diseases were found in sixteen patients (24 %) and included 3 with anti- thrombotic and 2 with steroid treatments, 6 chronic renal failures, 2 aortic valvular stenosis, one throm- bocytemia, one Willebrand's disease, and one por- tal hypertension. The goals of the treatment were 1) to stop the blood loss and to prevent recurrence in group L III and IV patients, and 2) to reduce the blood transfusion rate in the group H and V patients.
M e t h o d s
An argon laser (770, Cooper Lasersonics, Santa Clara, Calif.) was mainly used for coagulation of VM with a 4 W continuous beam (spot size 2 mm, irradiance 125 W/cm2). The Nd:YAG laser was used (YAG 101, Cilas Marcoussis, France) with a 50 W beam (spot size 2 mm, irradiance 1600 W/cm 2, exposure time 1 s). The Nd:YAG laser was used in only 3 circumstances : actively bleeding VM in the upper G1 tract, local recurrence after an argon treatment in the upper GI tract, and caver- nous VM (Blue rubber bleb nevus syndrome) in upper and lower GI tract.
Olympus GIF Q and CF LBW3 endoscopes (Olympus Corp., Tokyo, Japan) were used for laser treatment. Nitrogen was used to protect the fiber tip. For upper GI endoscopy, the argon and Nd:YAG laser fibers were inserted in a 1.6 external diameter catheter. The small diameter of the cathe- ter allowed the gas to escape through the biopsy channel of the GIF Q endoscope during the laser treatment. For lower GI endoscopy, a canula was introduced in the rectum along side the endoscope to evacuate the gas.
Patients were treated without sedation and as outpatients, except when they were hospitalized for an active hemorrhage or for colonic preparation. The maximum number of VM was treated during each treatment session. The treatment was tempora- rily interrupted when the treatment induced bleee- ding from the VM. The VM was further retreated when it had stopped bleeding spontaneously. The patients were reendoscoped and retreated every two weeks until complete disappearance of the VM. Then, they were clinically followed, except group H patients who were systematically reendoscoped and eventually retreated every 3 months. These group H patients also bled frequently from VM in the nose and were treated with the argon laser by our ENT collegues [ 1 7 ] .
R E S U L T S
Results are summarized in Table II.
G r o u p I p a t i e n t s
All the 43 patients stopped bleeding after an average of 2 laser treatment sessions (range 1-5). No recurrence was observed in the 11 patients who were lost to follow up after an average period of 10 months, in the 5 patients who deceased from other causes after an average period of 10 months and in the 22 patients who are still followed during an average period of 21 months. A recurrent hemor- rhagic episode was observed in 5 patients (12 %). Four were successfully retreated. A chronic anemia persisted in the fifth patients who was under anti- thrombotic treatment.
7 8 Volume 18 - N ~ 2 - 1988 Acta Endoscopica
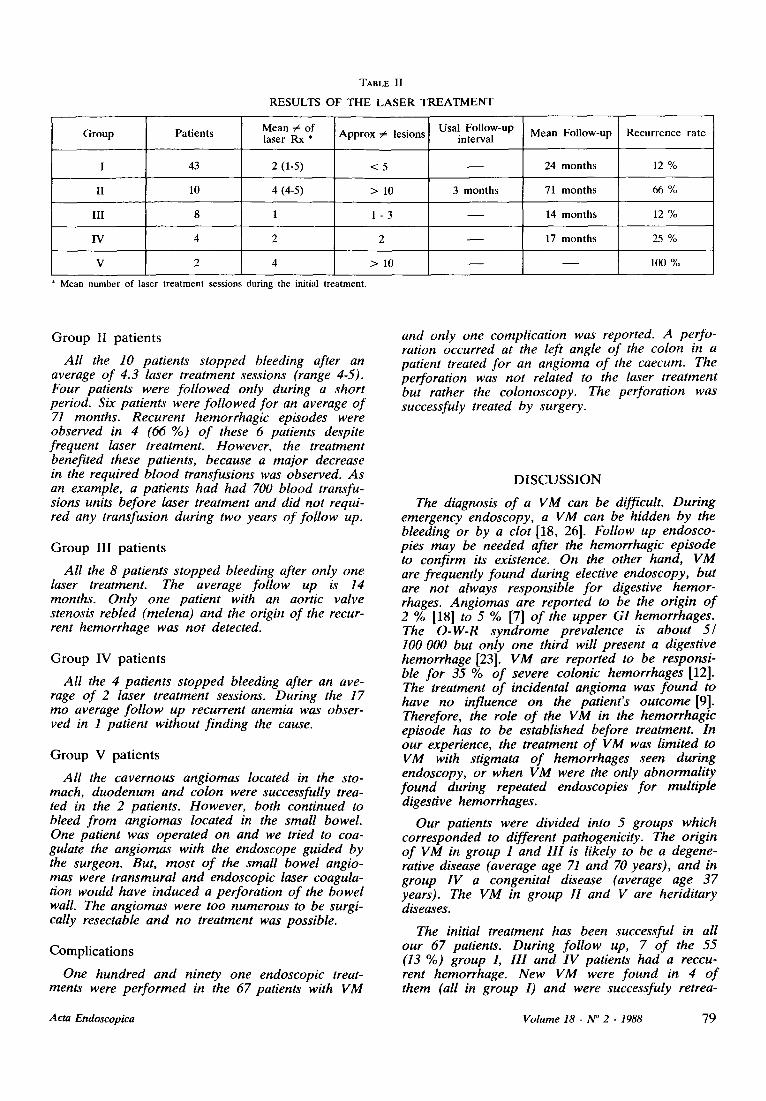
TABLE II
RESULTS OF THE LASER TREATMENT
Group
II
III
IV
V
Patients
43
10
Mean ~ of laser Rx *
2 (1-5)
4 (4-5)
Approx # lesions
< 5
> 10
1 - 3
Usal Follow-up interval
3 months
Mean Follow-up
24 months
71 months
14 months
Recurrence rate
12 %
66 %
12%
4 2 2 17 months 25 %
2 4 > 10 100 %
Mean number of laser treatment sessions during the initial treatment.
G r o u p II patients
All the 10 patients stopped bleeding after an average of 4.3 laser treatment sessions (range 4-5). Four patients were followed only during a short period. Six patients were followed for an average of 71 months. Recurent hemorrhagic episodes were observed in 4 (66 %) of these 6 patients despite frequent laser treatment. However, the treatment benefited these patients, because a major decrease in the required blood transfusions was observed. As an example, a patients had had 700 blood transfu- sions units before laser treatment and did not requi- red any transfusion during two years of follow up.
G r o u p I I I patients
All the 8 patients stopped bleeding after only one laser treatment. The average follow up is 14 months. Only one patient with an aortic valve stenosis rebled (melena) and the origin of the recur- rent hemorrhage was not detected.
G r o u p I V patients
All the 4 patients stopped bleeding after an ave- rage of 2 laser treatment sessions. During the 17 mo average follow up recurrent anemia was obser- ved in I patient without finding the cause.
G r o u p V patients
All the cavernous angiomas located in the sto- mach, duodenum and colon were successfully trea- ted in the 2 patients. However, both continued to bleed from angiomas located in the small bowel. One patient was operated on and we tried to coa- gulate the angiomas with the endoscope guided by the surgeon. But, most of the small bowel angio- mas were transmural and endoscopic laser coagula- tion would have induced a perforation of the bowel wall. The angiomas were too numerous to be surgi- cally resectable and no treatment was possible.
Compl icat ions
One hundred and ninety one endoscopic treat- ments were performed in the 67 patients with VM
and only one complication was reported. A perfo- ration occurred at the left angle of the colon in a patient treated for an angioma of the caecum. The perforation was not related to the laser treatment but rather the colonoscopy. The perforation was successfuly treated by surgery.
D I S C U S S I O N
The diagnosis of a VM can be difficult. During emergency endoscopy, a VM can be hidden by the bleeding or by a clot [18, 26]. Follow up endosco- pies may be needed after the hemorrhagic episode to confirm its existence. On the other hand, VM are frequently found during elective endoscopy, but are not always responsible for digestive hemor- rhages. Angiomas are reported to be the origin of 2 % [18] to 5 % [7] of the upper GI hemorrhages. The O-W-R syndrome prevalence is about 5/ 100 000 but only one third will present a digestive hemorrhage [23]. VM are reported to be responsi- ble for 35 % of severe colonic hemorrhages [12]. The treatment of incidental angioma was found to have no influence on the patient's outcome [9]. Therefore, the role of the VM in the hemorrhagic episode has to be established before treatment. In our experience, the treatment of VM was limited to VM with stigmata of hemorrhages seen during endoscopy, or when VM were the only abnormality found during repeated endoscopies for multiple digestive hemorrhages.
Our patients were divided into 5 groups which corresponded to different pathogenicity. The origin of VM in group I and III is likely to be a degene- rative disease (average age 71 and 70 years), and in group IV a congenital disease (average age 37 years). The VM in group H and V are heriditary diseases.
The initial treatment has been successful in all our 67 patients. During follow up, 7 of the 55 (13 %) group L 1II and IV patients had a reccu- rent hemorrhage. New VM were found in 4 of them (all in group I) and were successfuly retrea-
Acta Endoscopica Volume 18 - N ~ 2 - 1988 79

ted. In the 3 other patients the origin of the reccu- rent bleeding could not be identified and therefore was not treated. Two reasons can explain the high recurrence rate (66 %) in the 6 group H patients who were followed. 1) Two of them were living far aways f rom Lille and were not reendoscoped every 3 months, but only after a new hemorrhage. 2) Even in the regularly treated patients, new lesions can appear between two treatments. Howe- ver, all these 6 patients benefited from the treatment and had their quality o f life greatly improved as assessed by reduction in bleeding episodes and transfusion.
Argon laser treatment o f VM was reported with similar results in 6 other studies with a total o f 155 patients [2, 4, 10, 11, 12, 27]. A caecal perforation in a patient with pulmonary insufficiency [4] was the unique complication.
Three studies [22, 3, 14] reported the N d : Y A G laser experience in 99 patients with VM. The imme- diate success rates was limited respectively to 82 %, 78 % and 86 %. Most o f the failures corresponded
to complications. Two perforations and 8 laser- induced hemorhhages required surgical treatment.
Endoscopic non laser treatments exist. Bipolar electrocoagulation (BICAP, Circon-ACML Stam- ford, Connecticut) and thermal coagulation (Heater probe, Olympus, Tokyo) were reported to be very efficient and safe [11]. Sclerotherapy is another modality of endoscopic treatment for VM [30], but has not been widely used.
In conclusion, argon laser photocoagulation is a safe and efficient method o f treatment for digestive vascular malformations. In patients with Osler - Weber - Rendu disease, repeated treatments are needed. Even so, a total control o f the hemor- rhages may be not obtained. But, the quality of life o f these patients still remains greatly improved. Several complications were reported in the literature with Nd: YA G lasers. Therfore, the use of Nd: YA G laser is strictly limited in our institution to 1) acti- vely bleeding VM in the upper GI tract, 2) local recurrence after argon treatment in the upper GI tract, and 3) cavernous VM (Blue rubber bleb nevus syndrome) in upper and lower GI tract.
80 V o l u m e 18 - N ~ 2 - 1 9 8 8 A c t a E n d o s c o p i c a