-
8/15/2019 PLEURAL MCQS MEDICINE
1/17
Page 1 of 17
DR. RAJENDRAN’S INSTITUTE OF MEDICAL EDUCATION
+91 93888 52220
PNEUMOTHORAX (12 MCQs)
1) Pressure in the pleural space
a. Negative during inspiration and positive during
expiration
b. Negative during expiration and positive during
inspiration
c. Negative during both inspiration and expiration
d. Positive during both inspiration and expiration
Ans: (c)
In normal subjects, the pressure in the pleural space is
negative with respect to the
alveolar pressure during the entire respiratory cycle. The
pressure gradient between the
alveoli and the pleural space—the transpulmonary pressure—is the
result of the inherent
elastic recoil of the lung. During spontaneous breathing, the
pleural pressure is also
negative with respect to the atmospheric pressure. The
functional residual capacity, or
resting end-expiratory volume of the lung, is the volume at
which the inherent outward pull
of the chest wall is equal to, but opposite in direction to, the
inward pull (recoil) of the
lung.
-
8/15/2019 PLEURAL MCQS MEDICINE
2/17
Page 2 of 17
2) What is the main physiologic consequence of a
pneumothorax?
a. Decrease in the vital capacity
b. Hypercapnia
c. Mediastinal shift
d. Infection
Ans: (a)
The main physiologic consequences of a pneumothorax are a
decrease in the vital
capacity and the arterial PO2. In patients without underlying
major lung disease, the
decrease in the vital capacity is usually well tolerated. If the
lung function of the patient is
abnormal before the development of the pneumothorax, the
decrease in vital capacity may
lead to respiratory insufficiency with alveolar hypoventilation
and respiratory acidosis.
3) Pneumothorax causes -
a. Chest pain
b. Dyspnea
c. Ventilation-perfusion mismatch
d. Arterial hypoxemia
e. All of the above
-
8/15/2019 PLEURAL MCQS MEDICINE
3/17
Page 3 of 17
Ans: (e)
A pneumothorax is defined as air in the pleural space, between
the parietal and visceral pleura.This condition may be caused by
trauma or underlying lung disease, but sometimes happens
spontaneously without obvious cause. When a pneumothorax
develops, there is loss of the
negative intrapleural pressure that is needed for lung
inflation, and the lung on the affected side
collapses and cannot expand properly. This collapse leads to a
ventilation-perfusion mismatch
because there is continued perfusion of a poorly ventilated
lung.
Arterial hypoxemia can occur with 50% collapse of the lung. If
there is a continued air leak with
increasing positive intrapleural pressure, this can lead to a
tension pneumothorax and can lead to
compromise of venous return to the heart, decreasing cardiac
output, and causing hemodynamic
collapse.
Patients who develop a pneumothorax usually complain of sudden
onset of dyspnea and pleuritic
chest pain. However, the condition may be asymptomatic in 10% of
cases. Signs of a tension
pneumothorax (see below) include respiratory distress,
tachypnea, distended neck veins, pulsus
paradoxus, displacement of the point of maximal cardiac impulse,
and trachea shift.
PNEUMOTHORAX - ESSENTIALS OF DIAGNOSIS
● Pleuritic chest pain
● Acute-onset dyspnea
● Decreased breath sounds on affected side
● Plain x-ray is usually diagnostic. Expiratory films may
demonstrate small pneumothoraces
that are not visible on inspiratory films. See x-ray below.
● Chest CT will often be helpful in identifying associated
pathology, such as pneumocystis
pneumonia or differentiating pneumothorax from emphysematous
blebs in patients with
COPD.
-
8/15/2019 PLEURAL MCQS MEDICINE
4/17
Page 4 of 17
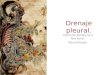
X-ray – There is complete translucency on the left with absence
of vascular markings, diagnostic of a
pneumothorax. The collapsed left lung appears as a left hilar
mass.
Hydropneumothorax – Horizontal fluid level on the left
-
8/15/2019 PLEURAL MCQS MEDICINE
5/17
Page 5 of 17
4) What is the cause of primary spontaneous pneumothorax?
a. Chronic bronchitis
b. Emphysema
c. Subclinical lung disease
d. A and b are true
e. Nonpenetrating chest injuries
Ans: (c)
Spontaneous pneumothorax is one that occurs without trauma to
the thorax. Primary
spontaneous pneumothorax occurs in the absence of underlying
lung disease. Primary
spontaneous pneumothoraces are usually due to rupture of apical
pleural blebs (small cystic
spaces that lie within or immediately under the visceral
pleura). Primary spontaneous
pneumothoraces occur almost exclusively in smokers. This
suggests that these patients have
subclinical lung disease. Secondary spontaneous pneumothorax
occurs when there is underlyinglung disease. In tension
pneumothorax, the pressure in the pleural space is positive
throughout
the respiratory cycle.
Traumatic pneumothorax results from penetrating or
nonpenetrating chest injuries.
TREATMENT OPTIONS
● Observation
● Supplemental oxygen
● Simple aspiration of the pneumothorax
● Simple tube thoracostomy
● Tube thoracostomy with instillation of a pleurodesing
agent
● Thoracoscopy with oversewing of the blebs and pleurodesis
-
8/15/2019 PLEURAL MCQS MEDICINE
6/17
Page 6 of 17
● Open thoracotomy
5) False about primary spontaneous pneumothorax
a. Usually due to rupture of an emphysematous bullae
b. Equally common in men and women
c. Recurrence occur in < 10 %
d. Thoracotomy with pleural abrasion can prevent recurrences in
up to 75%
e. All
Ans: (e) All are false.
Pneumothorax due to rupture of an emphysematous bullae is
secondary spontaneouspneumothorax. Primary spontaneous pneumothorax
is due to rupture of apical pleural blebs.
These are small cystic spaces that lie within, or immediately
under, the visceral pleura. It occurs
almost exclusively in smokers. It suggests that these patients
have subclinical lung disease. 50%
will have a recurrence.
The initial treatment for primary spontaneous pneumothorax is
simple aspiration. If the lung does
not expand with aspiration, or if the patient has a recurrent
pneumothorax, thoracoscopy with
stapling of blebs and pleural abrasion is indicated.
Thoracoscopy or thoracotomy with pleural
abrasion is almost 100% successful in preventing
recurrences.
TREATMENT OF SPONTANEOUS PNEUMOTHORACES
-
8/15/2019 PLEURAL MCQS MEDICINE
7/17
Page 7 of 17
● Treatment varies depending on the patient's condition, the
degree of collapse, the
cause, and the estimate of the chance of recurrence.
● Small (< 20–25%), stable, asymptomatic pneumothoraces in
otherwise healthy
patients can be observed. Complete resolution usually occurs
within several weeks.
Air is normally reabsorbed at a rate of 1–1.25% per day.
● Larger asymptomatic pneumothoraces taking longer than 2–3
weeks to resolve
place the patient at risk for developing trapped lung as a
result of deposition of
fibrin on the visceral pleura. These patients, as well as
patients with symptoms or
pneumothoraces associated with pleural effusions, should have
them evacuated.
● In highly selected patients, this can be accomplished with
simple aspiration . The
immediate and 2-hour delayed chest radiographs should show
reexpansion of lung.
Small breaks in the visceral pleural seal once the lung
collapses, but they can reopen
with reexpansion. The chance of recurrence is 20–50% with this
method. Follow-up
x-ray is therefore mandatory after 24 hours.
● Most patients with significant pneumothoraces (> 30%)
require placement of a
closed-chest catheter (8–20F) for reexpansion. This catheter
then can be placed
either to underwater suction drainage or to a Heimlich (one-way)
valve.
● Chest tubes should be placed in the midaxillary line at the
level of the fifth
intercostal space (nipple line).
● Pleurodesis - Patients with air leaks lasting longer than 7
days, patients who do not
fully reexpand their lungs, patients with large bullae or poor
pulmonary function,
and patients with bilateral or recurrent pneumothoraces are
candidates for
pleurodesis or surgical intervention.
-
8/15/2019 PLEURAL MCQS MEDICINE
8/17
Page 8 of 17
● Following a single episode, the risk of a recurrent
pneumothorax is 40–50%. After
two episodes, the risk increases to 50–75%, and with three
previous episodes, the
risk is in excess of 80%. Currently, most first-time patients
are treated initially with
simple chest tube drainage; however, with subsequent
recurrences, additional
therapy generally is indicated.
6) Treatment of secondary spontaneous pneumothorax
a. Wait till absorbed
b. Simple aspiration
c. Tube thoracostomy
d. Pleural abrasion
Ans: (c)
Most secondary spontaneous pneumothoraces are due to chronic
obstructive pulmonary disease.
Secondary pneumothoraces may also be due to pneumonia, cystic
fibrosis, asthma, or
tuberculosis. Pneumothoraces have been reported with virtually
every lung disease.
Pneumothorax in patients with lung disease is more
life-threatening than it is in normal
individuals. This is because of the lack of pulmonary reserve in
these patients. Almost all patients
with secondary spontaneous pneumothorax should be treated with
tube thoracostomy and the
instillation of a sclerosing agent such as doxycycline or talc.
See 2 figures below.
Tube thoracostomy and the instillation of a sclerosing agent
such as doxycycline or talc are
needed for almost all patients with secondary spontaneous
pneumothorax.
-
8/15/2019 PLEURAL MCQS MEDICINE
9/17
Page 9 of 17
Indications for thoracoscopy with bleb resection and pleural
abrasion are a persistent air leak, an
unexpanded lung after 3 days of tube thoracostomy, or a
recurrent pneumothorax.
7) Indications for thoracoscopy in secondary spontaneous
pneumothorax
a. Persistent air leak
b. Unexpanded lung after 3 days of tube thoracostomy
c. Recurrent pneumothorax
d. All
-
8/15/2019 PLEURAL MCQS MEDICINE
10/17
Page 10 of 17
Ans: (d)
8) False about traumatic pneumothorax
a. Nonpenetrating chest trauma does not cause pneumothorax
b. Treated with tube thoracostomy
c. Insertion of central intravenous catheter can cause traumatic
pneumothorax
d. All
e. None
Ans: (a)
Pneumothorax can result from both penetrating and nonpenetrating
chest trauma.
Traumatic pneumothoraces should be treated with tube
thoracostomy unless they are
very small. If a hemopneumothorax is present, one chest tube
should be placed in the
superior part of the hemithorax to evacuate the air, and another
should be placed in the
inferior part of the hemithorax to remove the blood.
Iatrogenic pneumothorax is a type of traumatic pneumothorax. It
is becoming more
common. The leading causes are transthoracic needle aspiration,
thoracentesis, and the
insertion of central intravenous catheters. The treatment
depends on the degree of
distress - observation, supplemental oxygen, aspiration, or tube
thoracostomy.
-
8/15/2019 PLEURAL MCQS MEDICINE
11/17
Page 11 of 17
9) True about tension pneumothorax
a. Usually occurs during mechanical ventilation
b. Cardiac output is reduced
c. Enlarged hemithorax with no breath sounds
d. Diagnosis is confirmed by needle insertion
e. All
Ans: (e)
Tension pneumothorax usually occurs during mechanical
ventilation or during resuscitative
efforts. Difficulty in ventilation during resuscitation or high
peak inspiratory pressures during
mechanical ventilation strongly suggests the diagnosis.
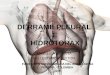
In tension pneumothorax, the pressure in the pleural space is
positive throughout the respiratory
cycle. See figure below. The positive pleural pressure is
life-threatening. Ventilation is severelycompromised. The positive
pressure is transmitted to the mediastinum. This results in
decreased
venous return to the heart and reduced cardiac output. If the
tension in the pleural space is not
relieved, the patient is likely to die from inadequate cardiac
output or marked hypoxemia.
-
8/15/2019 PLEURAL MCQS MEDICINE
12/17
Page 12 of 17
Diagnostic findings are enlarged hemithorax with no breath
sounds and shift of the mediastinum
to the contralateral side. Diagnosis is confirmed by needle
insertion.
Tension pneumothorax is a medical emergency. If the tension in
the pleural space is not relieved,the patient is likely to die from
inadequate cardiac output or marked hypoxemia. A large-bore
needle should be inserted into the pleural space through the
second anterior intercostal space. If
large amounts of gas escape from the needle after insertion, the
diagnosis is confirmed. The
needle should be left in place until a thoracostomy tube can be
inserted.
ESSENTIALS OF DIAGNOSIS - TENSION PNEUMOTHORAX
● Shift of cardiac apex to opposite side
● Shift of the trachea to opposite side
● Jugular venous distension
-
8/15/2019 PLEURAL MCQS MEDICINE
13/17
Page 13 of 17
10) False about tension pneumothorax
a. Most commonly due to COPD
b. USS is better than x-ray to detect small pneumothorax
c. May present as typical SVC obstruction
d. Bronchial breathing is typical
e. All are false
Ans: (e) All are false.
Tension pneumothorax usually occurs during mechanical
ventilation or resuscitative
efforts.
The positive pleural pressure is life threatening. Tension
pneumothorax presents with
chest pain and dyspnea.
The diagnosis is made by enlarged hemithorax with no breath
sounds and shift of the
mediastinum to the contralateral side.
11) Treatment of tension pneumothorax
a. Small bore needle inserted
b. Site of insertion is point of maximum resonance
-
8/15/2019 PLEURAL MCQS MEDICINE
14/17
-
8/15/2019 PLEURAL MCQS MEDICINE
15/17
Page 15 of 17
pneumothoraces, with sensitivities as low as 36–48% in some
studies. Tension pneumothorax can
develop when an injury to the lung parenchyma or bronchus acts
as a 1-way valve, allowing air to
enter the pleural cavity but preventing it from escaping. A
tension pneumothorax can develop
rapidly and is greatly exacerbated by positive-pressure
ventilation, posing a great danger to
intubated patients. Rapid detection of pneumothoraces in trauma
patients is critical, and bedsideultrasonography is a fast,
reliable means of accomplishing this task.
Findings suggestive of pneumothorax
The presence of a pneumothorax is characterized by the absence
of 2 findings: (1) the absence of
pleural (lung) sliding, and (2) the absence of comet-tail
artifacts. The lung point is difficult to
identify, but is pathognomonic for a pneumothorax and can be
used to measure the size of the
pneumothorax.
Absence of pleural sliding
In normal persons, the pleural line represents both the parietal
and visceral layers of the pleura,
and back-and-forth sliding of that line is easily visualized
during the respiratory cycle. In the
presence of a pneumothorax, air accumulates between the 2 layers
and blocks transmission of
sound waves, so that the sliding is not visualized. This
phenomenon can be seen in real time in
the 2-D mode but is more easily visualized by viewing a still
image in M-mode.
The appearance of normal lung has been described as the seashore
sign. See figure below.
This term refers to the change in appearance between soft tissue
and lung, divided by the pleural
-
8/15/2019 PLEURAL MCQS MEDICINE
16/17
Page 16 of 17
line, a change resembling that between sand and sea waves. In
the presence of a pneumothorax,
this demarcation is lost, and the appearance on M-mode imaging
is described as the stratosphere
sign . See figure below.
Absence of comet tails
Comet tails are artifacts that are created when ultrasound waves
bounce off the interface between
the opposing visceral and parietal layers of the pleura. They
appear as hypoechoic vertical
ray-like projections off the pleural line and are parallel to
the rib shadows. The presence of air in
the pleural space inhibits the propagation of sound waves,
preventing the appearance of comet
tails. The presence of comet tails is 60% specific for the
absence of pneumothorax. Combined
with the absence of lung sliding, the absence of comet tails has
a negative predictive value of
100% and a specificity of 96.5%.
Lung point
The lung point is pathognomonic for the presence of a
pneumothorax. See figure below. The lung
point is the actual point at which the normal lung pattern (ie,
lung sliding and comet-tail artifacts)
is replaced by a pattern consistent with a pneumothorax (ie, no
lung sliding and no comet-tailartifacts). Although it is the most
specific sign of pneumothorax, it is also the hardest to
visualize
and may require an experienced operator to locate. Finding both
transition zones (from normal
lung to pneumothorax and then back again) allows calculation of
pneumothorax size.
-
8/15/2019 PLEURAL MCQS MEDICINE
17/17
Page 17 of 17
● For video click
https://www.youtube.com/watch?v=Xxdedx1HtHo
● Disorders of the Pleura > PNEUMOTHORAX
o Harrison's Principles of Internal Medicine, 19e, Chapter
316.
● Pneumothorax
o Fishman's Pulmonary Diseases and Disorders, 5e, Chapter 78
● Pneumothorax
o Tintinalli’s Emergency Medicine: A Comprehensive Study Guide,
8e, Chapter 68
https://www.youtube.com/watch?v=Xxdedx1HtHo