Embed Size (px)
Citation preview

RéférentielsRéférentiels Oncomipp-CBNPC
-CBPC
-Tumeurs Carcinoïdes
-Mésothéliome
N d l lit i-Nodule solitaire pulmonaire
www.oncomip.fr

Animateurs Jean-Marc BACHAUD, Julien MAZIERES,
Pierre MOURLANETTE, Marcel DAHANPierre MOURLANETTE, Marcel DAHAN
Anatomo-pathologistes Isabelle ROUQUETTE, Daniel MESSELET,
Paul CAVERIVIERE
Chirurgie Jean BERJAUD,C u g e Je J U ,
Laurent BROUCHET, Olivier GARCIA
Pneumologues Pierre BAREL, Pascal DEBOVE,
Emmanuel COURAU, Laurence BIGAY-GAME,, ,
Michel FARNY, Christophe HERMANT,
Christine JULIA, Sylvie JULIEN,
François PETUREAU, Gavin PLAT,ç , ,
Anne PRUDHOMME, Christophe RASPAUD
Stéphanie LOZANO
Oncologues Franck BURKI, Nathalie CAUNESg ,
Radiothérapeutes
Bernard COUDERC, Philippe DUDOUET,
Igor LATORZEFFg
Radiologues / Médecins nucléaires Frédéric COURBON, Thierry DUCLOUX,
Nicolas FOURQUET, Jacques GIRON,
Cyril NORMANDy
Réseaux de soins palliatifs Olivier LAMOUR
Epidémiologiste Cyrille DELPIERRE
"

Arbres décisionnels
Littérature récente
S.O.R.
ArbreArbre décisionnel RCP onco-
P ti E i
thoracique
Pratiques locales
Essais cliniques
Lexique Désigne des recommandations et non un standard. Une discussion approfondie en RCP spécialisée est souhaitable



Cancer broncho pulmonairett
Cancer broncho-pulmonairenon à petites cellulesp
Arbres décisionnelsArbres décisionnels

BILAN INITIAL
- Radiographie standard du thorax
- TDM Thorax-Foie-Surrénales APC
-Endoscopie bronchiquep q
OBJECTIFS: Diagnostic pathologique et classification TNMOBJECTIFS: Diagnostic pathologique et classification TNM
RCPTumeur résécable
et patient opérable
Tumeur non résécable
ou patient inopérable
CHIRURGIE NON ENVISAGEECHIRURGIE ENVISAGEE CHIRURGIE NON ENVISAGEE
TRAITEMENT PALLIATIF
RADIOTHERAPIE ou RT-CHM
TEP-FDG
IRM é h li
Examens complémentaires
si suspicion clinique de M+TEP-FDG
IRM encéphalique
(ou à défaut TDM)
si suspicion clinique de M+IRM encéphalique (ou à défaut TDM)

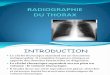
Evaluation pré-opératoire du risque avant chirurgie de résection pulmonaire majeure
Table 1.. Preoperative Tests for Assessing Pulmonary Risk Prior to Major Lung Resection TestValue Range for Low risk PatientsValue Range for Low-risk Patients
FEV1% > 60 %
DLCO% > 60 %
ppoFEV1 > 800 mL
ppoFEV1% > 40 %
ppoDLCO% > 40 %
VO2max during exercise > 15 mL/kg/min
Chest 1999

Stade I• IA → T1 N0
Après bilan initial
• IB → T2 N0Stade II
• IIA → T1 N1Classification
TNM 1998• IIB → T2 N1, T3 N0
Stade III• IIIA → T3 N1, T1-3 N2• IIIB → T4 ou N3
Stade IV
Patient opérableTumeur résécable TEP-FDG systématique
Chirurgie envisagée
y q

Limites de la résécabilité et impact de la nouvelle classificationLimites de la résécabilité et impact de la nouvelle classification
N d l lli d IIIB(T4) à IIIA(T3) i N1 N2 à IIB i N0!
IIIB et IV actuels potentiellement résécables:
• Nodules satellites :passent de IIIB(T4) à IIIA(T3) si N1 ou N2, et à IIB si N0!• T4 par invasion : si N0/1: IIIB>IIIA• Métastase pulmonaire unique ipsilatérale:IV(M1)>T4:IIIA si N0/1 IIIB si N2/3• Métastase pulmonaire unique ipsilatérale:IV(M1)>T4:IIIA si N0/1,IIIB si N2/3• Métastase pulmonaire unique hétérolatérale:M1> M1a
– !Bénéfice du doute(second primitif?) si <N2• >chirurgie ou chir+Rt stéréot. ou chir+radiofréquence…
IIIA non résécables
• IIIA N2 massifs ou persistants après chimiothérapie d’induction:pas de bénéfice de la chirurgiebénéfice de la chirurgie

CHIRURGIE ENVISAGEE
f é GPas de fixation médiastinale en TEP-FDG, M0
Stades I – II et T3N1 TEP-FDG
CHIRURGIELobectomie ou pneumonectomie + prélèvement ganglionnaire médiastinal large et systématique
Examen anapath. définitif
pT1 pN0 pT1pN1 ou pT2pN1 pT3 et/ou pN2pT2 pN0pT1 pN0
Pas de ttt
pT1pN1 ou pT2pN1
Chimiothérapie
pT3 et/ou pN2
Chimiothérapie
pT2 pN0
Pas de ttt Pas de ttt adjuvant*
Chimiothérapie adjuvante
p
± RT adjuvante (à discuter cas par cas si « minimal » N2)
adjuvant*
* Des critères liés au patient et anatomopathologique : taille > 4 cm, embols vasculaires ou lymphatiques, agressivité, etc.. peuvent intervenir dans la décision
** 4 cyles de bithérapie à base de platine à débuter dans les 6 semaines suivants la chirurgie

Tx N0 R0

Stades cliniques actuels <T3N2Stades cliniques actuels <T3N2
• !pronostic très dépendant de la taille du primitifp– ancienT2:
• si>5cm à 7cm• si>5cm à 7cm – et NO:passe de IB à IIA
• Si>3cm à 5cmSi>3cm à 5cm- et N1:passe de IIB à IIA
- si>7cm:devient T3et NO:passe de IIA à IIBet N1:passe de IIB à IIIAet N1:passe de IIB à IIIA

Conséquences de l’amélioration de la discrimination des stades en fonction du pronostic
• Les nouveaux IB sont de meilleur pronosticp– OR:
• Actualisation des données de survie de l’étude• Actualisation des données de survie de l étude CALGB 9633(Strauss;JCO 2008):ne retrouve plus d’avantage de survie après un suivi médian de 74 g pmois!(seule grosse étude non Japonaise spécifique du IB préalablement positive)
– Mais :Taxol-Carbo– Analyse non planifiée: bénéfice persistant si >4cm

Traitements adjuvantsTraitements adjuvantsBé éfi dé t é t d IIA à IIIA• Bénéfice démontré pour stades IIA à IIIA réséqués
Pour les chimiothérapies à base de cisplatine (ou UFT chez les– Pour les chimiothérapies à base de cisplatine (ou UFT chez les Japonais)
– Probablement à appliquer aux actuels IB>7cm
IB• IB:tendance au bénéfice dans la méta-analyse LACE(HR 0,93 95%CI 0,78-1,10)– utiliser la limite de 4cm? 5cm?(futur IIA) 7cm?(futurIIB)– utiliser la limite de 4cm? 5cm?(futur IIA),7cm?(futurIIB)– Attendre sa validation prospective?– Attendre les résultats d’études faites avec la nouvelle
l ifi ti ?classification?– Valider les critères de sélection des patients bénéficiant de la
chimiothérapie adjuvante?(marqueurs de mauvais pronostic , et/ou prédictifs de réponse à la chimiothérapie(ERCC1, RRM1, Beta-tubuline…))

CHIRURGIE ENVISAGEE
é é GFixation médiastinale homolatérale en TEP-FDG, M0
Stade IIIA (T1-3, N2) TEP-FDG
* • ganglion unique
Cas favorables* et concordance TDM/TEP Autres cas (défavorable ou
discordance TDM/TEP) à discuter cas par cas
• ganglion unique • 1er relais anatomique médiastinal
Expertise médiastinale+
CHIRURGIE
Selon école
Expertise
+-
CHIRURGIE
+
CHIMIOTHERAPIE ADJUVANTE
Expertise
médiastinale
+
Cas défavorables-
CHIMIOTHERAPIE NEO-ADJUVANTE
+
CHM et RT concomitante si possible.
Rediscussion de la chirurgie selon
RT post-opératoire si pN2 et/ou pT3
CHIRURGIE downstaging

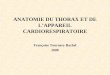
Spécif.Sens.Imagerie
0,86(0,84-0,88)0,51(O,47-0,54)Scanner N=5111
0,85(0,82-0,88)0,74(0,69-0,79)TEP FDGN=2865
11010078M di ti
FNFPSpecSensTechnique
11010078Mediastinoscopie n=6505
S
190.799.584EUS-FNAn=1003
10089TTNA
20010090EBUS-FNA n=918
Chest 2007
10089TTNA n=215

« Selon école »
-Moins d’évidence en faveur de l’induction:Moins d évidence en faveur de l induction:-moins de publications, essais versus chirurgie seule
interrompus…-dernière méta-analyse:n=1507 (Gilligan Lancet 2007):HR
0,88 mais P 0,07
-n’accentue pas le risque chirurgical-peu de risque de progression lors de l’inductionpeu de risque de progression lors de l induction-valeur pronostique majeure du downstaging médiastinal:>première étape avant le choix entre CT-CHIR et CT-RT si cN2 de « bon »pronostic-observance de la chimiothérapie nettement supérieure(>80%) à l’approche adjuvante(<60%)l approche adjuvante(<60%)-Nécessité d’un excellent staging médiastinal-Permet de tester la chimiosensibilité avant résection(chimio péri-Permet de tester la chimiosensibilité avant résection(chimio périopératoire)-discutable:épargne parenchymateuse

Rôle de la chirurgie dans les N2Rôle de la chirurgie dans les N2
EORTC 08941• EORTC 08941 Van Meerbeeck JNCI 2007
– Ct-Rt versus Ct-Chir :pas de survie globale améliorée dans le groupe chirurgicalaméliorée dans le groupe chirurgical
– Downstaging:dans le bras chirurgical:• si N2>N0:29% de survie à 5 anssi N2 N0:29% de survie à 5 ans• Si N2 persistant:7% de survie à 5 ans• (downstaging ana-path :5,2%)
• RTOG 9309 Rusch Lung Cancer 2005CT Rt CT RT i hi id– -CT-Rt con vs CT-RT puis chir: idem
– Chir :moins bien si pneumonectomie


CHIRURGIE ENVISAGEE
é é GFixation médiastinale homolatérale en TEP-FDG, M0
Stade IIIA (T1-3, N2) TEP-FDG
* • ganglion unique non sous-Cas défavorables: à discuter au cas par cas
Expertise médiastinaleMini invasive si possible
• ganglion unique non souscarénaire et• 1er relais anatomique médiastinal
discuter au cas par cas
(N2multisite,
Aire 7)N2 non confirméOu N3:algorithme correspondant
N2 non confirméOu N3:algorithme correspondant
CHIRURGIE
Selon école
CHIMIOTHERAPIE
correspondantcorrespondant
CHIRURGIE
+
CHIMIOTHERAPIE ADJUVANTE
CHIMIOTHERAPIE NEO-ADJUVANTE Restaging
médiastinal invasif
Rediscussion de la chirurgie selon downstaging
RT post-opératoire si pN2 et/ou pT3
CHIRURGIE (si N0/1 et pas de
pneumonectomie)Chimio-radiothérapie si N2

CHIRURGIE ENVISAGEE
é é GFixation médiastinale controlatérale en TEP-FDG, M0
Stade IIIB (T1-3, N3) TEP-FDG
EXPERTISE MEDIASTINALE
(Médiastinoscopie, PTBA, BTO, médiastinotomie, thoracoscopie, etc…)
visant la loge du N3 hyperfixant
+-
RADIO-CHIMIOTHERAPIE (concomitante si possible)
Cf. stade correspondant

Stade I• IA → T1 N0
Après bilan initial
• IB → T2 N0Stade II
• IIA → T1 N1Classification
TNM 1998• IIB → T2 N1, T3 N0
Stade III• IIIA → T3 N1, T1-3 N2• IIIB → T4 ou N3
Stade IV
Patient inopérableTEP-FDG
Chirurgie non envisagée

PATIENT INOPERABLE
Stade I-IIIA après bilan initial
Cas particuliers
(OMS ≥ 3, refus, âge…)
Fonction respiratoire suffisante pour radiothérapie
Fonction respiratoire insuffisante pour
radiothérapie
TEP-FDG
IRM encéphalique ou TDM
M0 M1
p q
ABSTENTION RADIOTHERAPIE*CHIMIOTHERAPIE
± CHIMIOTHERAPIECHIMIOTHERAPIE
* La radiofréquence (thermoablation) peux être discutée au cas par cas mais reste une alternative

RT stéréotoxiqueDonnées patients série de LAGERWAARDDonnées patients, série de LAGERWAARD
Patients (tumeurs) 314 (364)
Homme (%) 59%
Age médian (ans) 74
T1 / T2 (%) 60% / 40%
Confirmation histologique OUI / NON 36% / 64%
Inopérables 84%Inopérables 84%
VEMS médian (% théorique) 57%
Nombre de fractions (équivalent de dose biologique Gy) 39% / 47% / 14%Nombre de fractions (équivalent de dose biologique Gy)3(180) / 5(132) / 8(105)
39% / 47% / 14%
Rechutes locales à 1 an / 2ans / 3 ans 3% / 9% / 11%
Lagerwaard et al. IASLC/ESMO 2008 ; Abstract 30IN

Stade I• IA → T1 N0
Après bilan initial
• IB → T2 N0Stade II
• IIA → T1 N1IIB T2 N1 T3 N0
ClassificationTNM 1998
• IIB → T2 N1, T3 N0Stade III
• IIIA → T3 N1, T1-3 N2IIIB T4 N3• IIIB → T4 ou N3
Stade IV
Stades avancés TEP FDG ?

STADES AVANCES T4 après bilan initial
OMS ≤ 2 OMS > 2
Absence d’épanchement pleuro-péricardique Epanchement pleural ou
péricardique
(cytologie +)(cytologie )TEP-FDG
IRM encéphalique
+/- IRM Thorax +/- médiastino
Futurs M1a
M0 M1
Non résécablePotentiellement
résécable
RADIO-CHM
(concomitanteCHIMIOTHER. RADIOTHERAPIE
ouTRAITEMENT
CHIMIOTHER.
(± symphyse)
CHIRURGIE ou RADIO-CHM
ou séquentielle)
TRAITEMENTSYMPTOMATIQUE
(± symphyse)

STADES AVANCESM1 solitaire après bilan initial
TEP-FDG + IRM +/- biopsies
M0 M1 multiples M1 unique
Autres sitesCas particuliers
ou Non opérable
ou M1 non résecable
M1 encéphale
M1 poumon
A discuter au cas par cas
Cf. stade correspondant
CHIMIOTH.
+ RT symptôme
CHIMIOTH.+/- RT clôture ( h M1)
Chirurgie 2 sites*
Radiothérapie RT symptôme(thorax ± M1) Chimiothérapie
* La radiochirurgie cérébrale peut être discutée dans les M1 uniques cérébrales

STADES AVANCESM1 multiples après bilan initial
OMS ≤ 2 OMS = 4 OMS = 3
CHIMIOTHERAPIE TRAITEMENT
SYMPTOMATIQUEA Discuter