Embed Size (px)
Citation preview

Cas cliniques
DOI of or1Vascular
Hospital, Turi2Vascular
pital, Asti, Ita
CorrespondSurgery Unit,Turin, Italy, E
Ann Vasc SurDOI: 10.1016/� Annals of V�Edit�e par ELS
Rupture d’un an�evrysme vrai g�eant de l’art�eretibiale post�erieure de 6 cm de diam�etre
Emanuele Ferrero,1 Michelangelo Ferri,1 Andrea Viazzo,1 Andrea Gaggiano,2
Giuseppe Berardi,1 Salvatore Piazza,1 Pia Cumbo,1 Claudio Castagno,1 Alberto Pecchio,1
Franco Nessi,1 Asti et Turin, Italie
Les an�evrysmes vrais de l’art�ere tibiale sont rares et leur rupture est tr�es rare. Nous rapportonsle cas d’un homme de 59 ans qui, apr�es un �episode d’endocardite bact�erienne, a pr�esent�e unan�evrysme tibial post�erieur rompu. �A notre connaissance, c’est le premier cas d’une v�eritablerupture d’un an�evrysme g�eant de l’art�ere tibiale post�erieure (diam�etre, 6 cm). Le traitement s’estcompos�e de l’an�evrysmectomie avec ligature art�erielle. Un ult�erieur de 24 mois a �et�e fait avecde bons r�esultats.
True aneurysms of tibial artery are uncommon and
it is really rare rupture. The etiology is unclear:
fibromuscular fibrodysplasia, trauma, atherosclero-
sis, inflammation, infection, and other pathological
processes are also probably involved. As all aneu-
rysm, they can evolve to thrombosis and distal
embolism more than to rupture. The literature
reports only 14 cases of posterior tibial artery and
only one case of tibial artery aneurysm rupture.
CASE REPORT
On March 6, 2007, a 59-year-old man presented to our
hospital for treatment of bacterial endocarditis (mitral
valve vegetations demonstrated on echocardiography).
Patient medical history: McArdle’s disease, hyperten-
sion, dyslipidemia, on October 2006 onset of evening
fever regressed without specific treatment (no ematic or
iginal article: 10.1016/j.avsg.2010.01.016.
and Endovascular Surgery Unit, Mauriziano Umberto In, Italie.
and Endovascular Surgery Unit, Cardinal Massaia Hos-lie.
ence : Emanuele Ferrero, Vascular and EndovascularMauriziano Umberto I Hospital, Largo Turati 62, 10128-mail: [email protected]
g 2010; 24: 1134.e9-1134.e13j.acvfr.2011.04.007ascular Surgery Inc.EVIER MASSON SAS
lymphatic pathologies neither infectious diseases found
with the exception of doubtful positive for Parvovirus), on
February diagnosis of spondylodiscitis (diagnosticated by
magnetic resonance and confirmed by bone scan and
positron emission tomography imaging) and under anti-
biotic treatment (ceftriaxone and amikacin), on February
diagnosis deep vein thrombosis (DVT) of the left lower leg
under therapy with low molecular weight heparin
(LMWH). During hospitalization hewas given appropriate
antibiotic therapy, and the patient underwent color flow
color duplex ultrasound study (DUS) to check the DVT.
The DUS confirmed the presence of DVT of the left lower
leg and showed a 28-mm diameter aneurysm of the pos-
terior tibial artery to a length of 25 mm never diagnosed
before (Fig. 1). The arterial lumen was patent with little
eccentric mural thrombus, the diameter of undiseased
proximal and distal posterior tibial artery was regular, and
velocity spectral analysis identified distal stenosis and poor
flows at level of posterior tibial artery and peroneal artery;
the analysis of anterior tibial artery identified no stenosis
with regular distal flow. A computed tomography (CT)
scan, performed for evaluation of thoracic, abdomen, and
legs, confirmed the presence of both spondylodiscitis that
left posterior tibial artery aneurysm (diameter, 30 mm;
Fig. 2). The patient, few days after the CT scan, developed
an intracerebral hemorrhage (presumably due to rupture
of cerebral mycotic aneurysm) with consequent coma
state associated to right hemiplegia and aphasia, it was
necessary to perform a cranial decompression with
hematoma evacuation. Therefore, given the clinical con-
dition of the patient (comatose state, hemiplegia, enteral
nutrition through a nasogastric tube, breathing through a
1226.e5

Fig. 2. Computed tomography scan showing the pos-
terior tibial artery true aneurysm (3 cm diameter).
Fig. 1. Color duplex sonography showing the aneurysm
in the posterior tibial artery (2.8 cm diameter).
1226.e6 Cas cliniques Annales de chirurgie vasculaire
tracheostomy tube), the left tibial artery aneurysm has
become a secondary issue, and it was decided tomonitor it
over time. Two months after cerebral bleeding, the pa-
tient presented clinical and neurological improvement,
although his general condition remained critical (per-
cutaneous endoscopic gastrostomy tube placement was
thought necessary for nutrition) but the echocardio-
graphy control scan revealed no more valvular vegeta-
tions. At 8 months after the diagnosis of tibial aneurysm,
the patient was referred to our attention for the detection
of a sudden swelling of the left calf with pulsating mass
associated; the urgent DUS showed a 60-mm diameter
aneurysm of the posterior tibial artery ruptured. The
patient underwent surgery, through medial approach the
giant left tibial posterior aneurysm was detected (Fig. 3)
and was found the rupture of the posterior wall of the
aneurysm. The patient was successfully treated with
aneurysmectomy and surgical arterial ligation under spi-
nal anesthesia. Before, during, and after surgery there was
a regular pulse at the dorsal artery of the left foot. Thus,
both for regular blood supply of the foot (guaranteed by
the anterior tibial artery) and for the suspicion of a
mycotic aneurysm, we felt that the treatment by pro-
sthetic graft or by vein graft was inappropriate because of a
high risk of superinfection and subsequent prosthetic
detachment; hence, we considered the surgical ligation of
the posterior tibial artery as an acceptable treatment. The
postoperative course was uneventful, the patient under-
went intravenous antibiotic therapy for at least 6 weeks.
The patient had no ischemic signs in the lower left leg.
Histologic examination showed wall aneurysmal dilata-
tion with disappearance of the inner limiting tunic,
fibrosis of the medial tunic with atrophy of muscle fibers,
elastic fibers fragmentation of external tunic and fibrosis
limiting periadventitial tunic and hyaline sclerosis of
subintimal plaque; it also showed the absence of inflam-
matory elements in the material examined. At 24 months
follow-up neither foot nor digital ischemia has been
observed; the patient has no paresthesias, pain, dis-
comfort, or leg limitation. A 24 months duplex
scan follow-up examination revealed good patency
of the anterior tibial artery without stenosis, no pseudo-
aneurysm or recurrent aneurysm of the posterior tibial
artery.
DISCUSSION
The aneurysms of the infrapopliteal arteries are rare,
lots of them appear as false and are associated with
trauma or iatrogenic injury.1 True aneurysms of the
posterior tibial artery are really rare, only 14 isolated
case reports in the literature, and themajority of these
were described as either idiopathic or degenerative in
origin. The etiology is unclear: traumatic events,
collagen matrix alterations, infection, inflammation,
fibromuscular dysplasia are more commonly invol-
ved thanatherosclerosis.2 Themycotic etiology iswell
documented and reported in literature,3-6 usually
mycotic aneurysms occur most frequently in the
intracranial arteries (65%), followed by visceral
arteries and vessels of the upper and lower limbs. In
our case thepatientdidnot suffer fromatherosclerotic
disease, vasculitic disorders, or trauma of the leg.
Initially, we thought that this unusual aneurysm
originated from an embolic vegetation that had
settled on the vessel wall and caused erosion and
subsequent mural weakness with consequent rup-
ture; moreover, the intracerebral hemorrhage was
presumably caused due to the rupture of another
mycotic aneurysm, and the histologic examination
was negative (no microbiological examination was
performed). For diagnosis of tibial aneurysm the color
flow duplex ultrasound is usually sufficient (as in our
case); with an accurate evaluation of the run-in and
the run-off it is possible to proceed with repair,
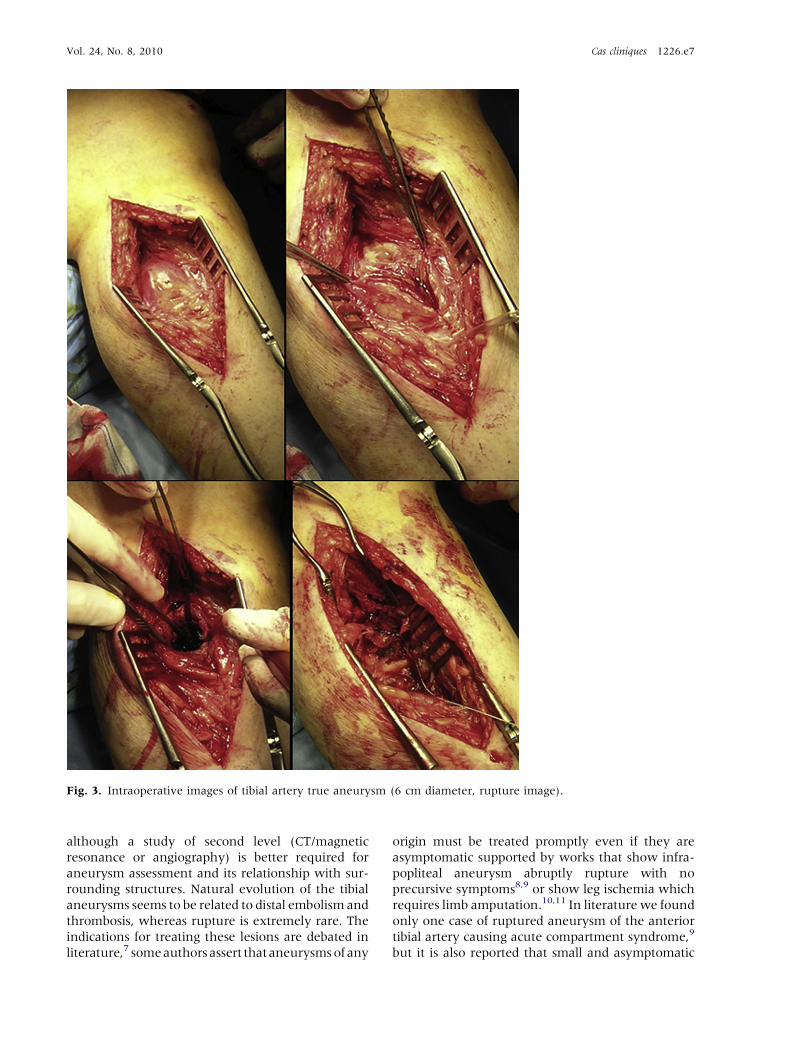
Fig. 3. Intraoperative images of tibial artery true aneurysm (6 cm diameter, rupture image).
Vol. 24, No. 8, 2010 Cas cliniques 1226.e7
although a study of second level (CT/magnetic
resonance or angiography) is better required for
aneurysm assessment and its relationship with sur-
rounding structures. Natural evolution of the tibial
aneurysms seems to be related to distal embolism and
thrombosis, whereas rupture is extremely rare. The
indications for treating these lesions are debated in
literature,7 someauthors assert thataneurysmsof any
origin must be treated promptly even if they are
asymptomatic supported by works that show infra-
popliteal aneurysm abruptly rupture with no
precursive symptoms8,9 or show leg ischemia which
requires limb amputation.10,11 In literature we found
only one case of ruptured aneurysm of the anterior
tibial artery causing acute compartment syndrome,9
but it is also reported that small and asymptomatic
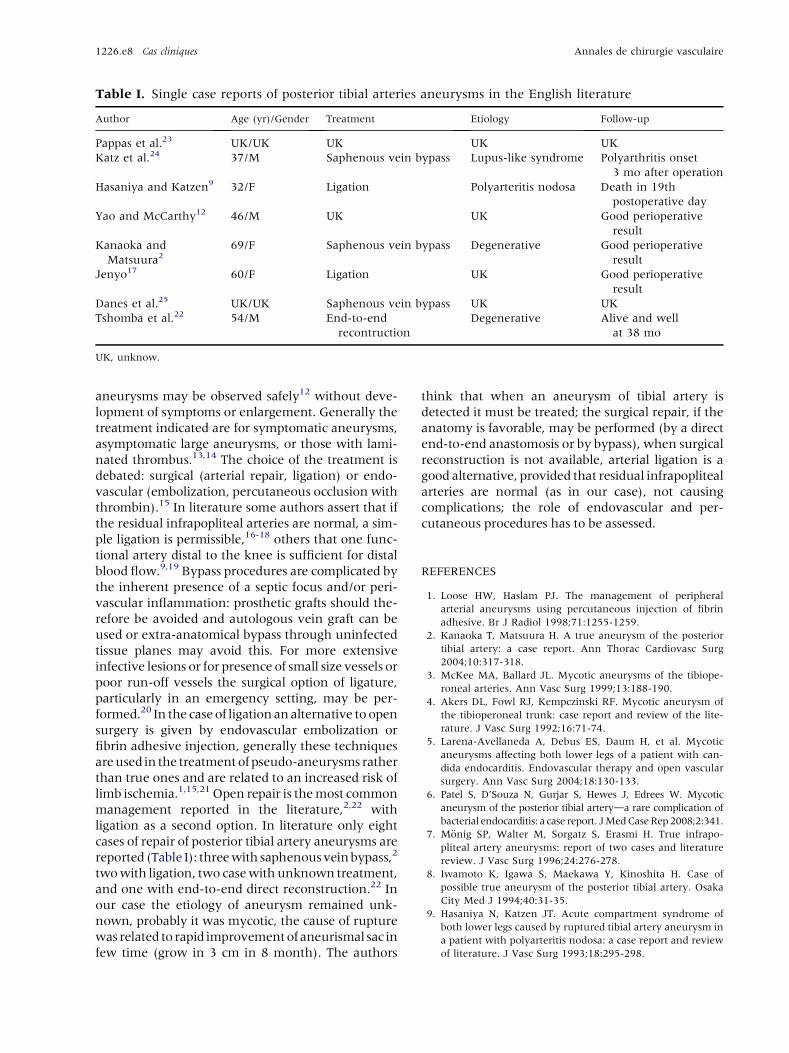
Table I. Single case reports of posterior tibial arteries aneurysms in the English literature
Author Age (yr)/Gender Treatment Etiology Follow-up
Pappas et al.23 UK/UK UK UK UK
Katz et al.24 37/M Saphenous vein bypass Lupus-like syndrome Polyarthritis onset
3 mo after operation
Hasaniya and Katzen9 32/F Ligation Polyarteritis nodosa Death in 19th
postoperative day
Yao and McCarthy12 46/M UK UK Good perioperative
result
Kanaoka and
Matsuura269/F Saphenous vein bypass Degenerative Good perioperative
result
Jenyo17 60/F Ligation UK Good perioperative
result
Danes et al.25 UK/UK Saphenous vein bypass UK UK
Tshomba et al.22 54/M End-to-end
recontruction
Degenerative Alive and well
at 38 mo
UK, unknow.
1226.e8 Cas cliniques Annales de chirurgie vasculaire
aneurysms may be observed safely12 without deve-
lopment of symptoms or enlargement. Generally the
treatment indicated are for symptomatic aneurysms,
asymptomatic large aneurysms, or those with lami-
nated thrombus.13,14 The choice of the treatment is
debated: surgical (arterial repair, ligation) or endo-
vascular (embolization, percutaneous occlusion with
thrombin).15 In literature some authors assert that if
the residual infrapopliteal arteries are normal, a sim-
ple ligation is permissible,16-18 others that one func-
tional artery distal to the knee is sufficient for distal
blood flow.9,19 Bypass procedures are complicated by
the inherent presence of a septic focus and/or peri-
vascular inflammation: prosthetic grafts should the-
refore be avoided and autologous vein graft can be
used or extra-anatomical bypass through uninfected
tissue planes may avoid this. For more extensive
infective lesions or for presence of small size vessels or
poor run-off vessels the surgical option of ligature,
particularly in an emergency setting, may be per-
formed.20 In the caseof ligationanalternative toopen
surgery is given by endovascular embolization or
fibrin adhesive injection, generally these techniques
areused in the treatmentof pseudo-aneurysms rather
than true ones and are related to an increased risk of
limb ischemia.1,15,21 Open repair is themost common
management reported in the literature,2,22 with
ligation as a second option. In literature only eight
cases of repair of posterior tibial artery aneurysms are
reported (Table I): threewith saphenousveinbypass,2
twowith ligation, two casewithunknown treatment,
and one with end-to-end direct reconstruction.22 In
our case the etiology of aneurysm remained unk-
nown, probably it was mycotic, the cause of rupture
was related to rapid improvementof aneurismal sac in
few time (grow in 3 cm in 8 month). The authors
think that when an aneurysm of tibial artery is
detected it must be treated; the surgical repair, if the
anatomy is favorable, may be performed (by a direct
end-to-end anastomosis or by bypass), when surgical
reconstruction is not available, arterial ligation is a
good alternative, provided that residual infrapopliteal
arteries are normal (as in our case), not causing
complications; the role of endovascular and per-
cutaneous procedures has to be assessed.
REFERENCES
1. Loose HW, Haslam PJ. The management of peripheral
arterial aneurysms using percutaneous injection of fibrin
adhesive. Br J Radiol 1998;71:1255-1259.
2. Kanaoka T, Matsuura H. A true aneurysm of the posterior
tibial artery: a case report. Ann Thorac Cardiovasc Surg
2004;10:317-318.
3. McKee MA, Ballard JL. Mycotic aneurysms of the tibiope-
roneal arteries. Ann Vasc Surg 1999;13:188-190.
4. Akers DL, Fowl RJ, Kempczinski RF. Mycotic aneurysm of
the tibioperoneal trunk: case report and review of the lite-
rature. J Vasc Surg 1992;16:71-74.
5. Larena-Avellaneda A, Debus ES, Daum H, et al. Mycotic
aneurysms affecting both lower legs of a patient with can-
dida endocarditis. Endovascular therapy and open vascular
surgery. Ann Vasc Surg 2004;18:130-133.
6. Patel S, D’Souza N, Gurjar S, Hewes J, Edrees W. Mycotic
aneurysm of the posterior tibial arteryda rare complication of
bacterial endocarditis: a case report. JMedCaseRep2008;2:341.
7. M€onig SP, Walter M, Sorgatz S, Erasmi H. True infrapo-
pliteal artery aneurysms: report of two cases and literature
review. J Vasc Surg 1996;24:276-278.
8. Iwamoto K, Igawa S, Maekawa Y, Kinoshita H. Case of
possible true aneurysm of the posterior tibial artery. Osaka
City Med J 1994;40:31-35.
9. Hasaniya N, Katzen JT. Acute compartment syndrome of
both lower legs caused by ruptured tibial artery aneurysm in
a patient with polyarteritis nodosa: a case report and review
of literature. J Vasc Surg 1993;18:295-298.

Vol. 24, No. 8, 2010 Cas cliniques 1226.e9
10. Carey LC, Stremple JF. An aneurysm of the anterior tibial
artery. Angiology 1967;18:117-121.
11. Tempest HV, Wilson YG. Acute forefoot ischemia: an
unreported complication of dorsalis pedis artery aneurysm.
Eur J Vasc Endovasc Surg 2001;22:472-473.
12. Yao JST, McCarthy WJ. Multiple arterial aneurysms: a
seven-year follow-up. Contemp Surg 1987;31:73-78.
13. Mukherjee D. Posterior approach to the peroneal artery.
J Vasc Surg 1994;19:174-178.
14. Ballard JL, Bunt TJ, Malone JM. Management of small
artery vascular trauma. Am J Surg 1992;164:316-319.
15. Corso R, Carrafiello G, Intotero M, Solcia M. Large iatrogenic
pseudoaneurysm of the posterior tibial artery treated with
sonographically guided thrombin injection. Am J Roentgenol
2003;180:1479-1480.
16. Marmorale A, Sapienza P, Gallo P, et al. Aneurysms of the
infrapopliteal arteries. JR Coll Surg Edinb 1995;40:
324-326.
17. Jenyo MS. Silent posterior tibial artery aneurysm. J Cardio-
vasc Surg 1987;28:456-459.
18. Borozan PG, Walker HS 3rd, Peterson GJ. True tibial artery
aneurysms: case report and literature review. J Vasc Surg
1989;10:457-459.
19. Bedford RF, Woolman H. Complication of percutaneous
radial artery cannulation. Anesthesiology 1973;38:228-236.
20. Kelly G, Eiseman B. Civilian vascular injuries. J Trauma
1975;15:507-514.
21. Schneider PA, Abcarian PW, Leduc JR, et al. Stentgraft
repair of mycotic superficial femoral artery aneurysm using
a Palmaz stent and autologous saphenous vein. Ann Vasc
Surg 1998;12:282-285.
22. Tshomba Y, Papa M, Marone EM, et al. A true posterior
tibial artery aneurysmda case report [review]. Vasc Endo-
vasc Surg 2006;40:243-249.
23. Pappas G, James JM, Bernatz PE. Femoral aneurysms.
JAMA 1964;190:489-493.
24. Katz SG, Kohl RD, Razack N. Bilateral infrapopliteal artery
aneurysms. Ann Vasc Surg 1992;6:168-170.
25. Danes SG, Drezner AD, Tamim PM. Posterior tibial artery
aneurysm: a case report. Vasc Endovasc Surg 40:328-330.