Embed Size (px)
Citation preview

Cas cliniques
DOI of or
Departmencal University,
Correspondgery, XuanwuStreet, Xuanwyahoo.cn
Ann Vasc SurDOI: 10.1016/� Annals of V�Edit�e par ELS
Shunt m�esent�erico-jugulaire pour syndromede Budd-Chiari: Un cas avec suivi �along terme
Hong Yong Duan, Xin Wu, Zhong Gao Wang, Jian Zhang, Jian Xin Li, Yong Quan Gu,
Heng Xi Yu, Bing Chen, P�ekin, R.P. de Chine
Objectif : Nous rapportons un cas de shunt m�esent�erico-jugulaire pour syndrome de Budd-Chiari (BCS) avec suivi �a long terme.M�ethodes : Une femme de 32 ans s’est pr�esent�ee �a un stade tardif de BCS. Elle a �et�e trait�eeavec un shunt m�esent�erico-jugulaire pour soulager son hypertension portale. Avec un suivi de17 ans, elle a eu une grossesse, une p�eriode puerp�erale, et a �et�e diagnostiqu�ee avec lupus�eryth�emateux syst�emique diss�emin�e. Elle a repris le travail en tant qu’infirmi�ere de salled’op�eration et a une vie normale. Son pontage reste perm�eable.Conclusion : Un shunt m�esent�erico-jugulaire est moins agressif chirurgicalement avec uneperm�eabilit�e �a long terme meilleure que d’autres shunts. Il peut etre employ�e pour traiter lespatients graves avec BCS qui ne sont pas candidats �a une intervention.
Budd-Chiari syndrome (BCS) is a clinical condition
caused by hepatic venous outflow obstruction loca-
ted anywhere from the hepatic veins to the supra-
hepatic inferior vena cava (IVC), and even below
the right atrium, regardless of the cause of the obs-
truction.1,2 The clinical symptoms and histopa-
thologic features of this syndromewere described by
Budd in 1845 and Chiari in 1899.3 With respect to
etiology, BCS can be classified as primary and
secondary types. The former is caused by endolu-
minal venous lesions, such as thromboses and webs,
while the latter is caused by external invasion or
compression, such as malignant tumors or large
cysts.2 The risk factors for primary BCS include
iginal article: 10.1016/j.avsg.2010.02.050.
t of Vascular Surgery, Xuanwu Hospital, Capital Medi-P�ekin, R.P. de Chine.
ence : Zhong Gao Wang, Department of Vascular Sur-Hospital, Capital Medical University, No.45 Changchunu District, Beijing, P.R. China, E-mail: zhonggaowang@
g 2010; 24: 953.e1-953.e5j.acvfr.2011.02.022ascular Surgery Inc.EVIER MASSON SAS
myeloproliferative diseases, a Factor V Leiden
mutation, antiphospholipid syndrome, Behcet’s
disease, paroxysmal nocturnal hemoglobinuria, oral
contraceptive use, and pregnancy.1,4-6 The basic
therapeutic strategies consist of medical mana-
gement, interventional techniques, transjugular
intrahepatic portosystemic shunts (TIPS), various
surgical shunts, and liver transplantation.
We report a case of a 32-year-old woman with
BCS. A mesojugular shunt was placed to relieve
her severe portal hypertension. Over a 17-year
follow-up, she had a pregnancy and normal deli-
very. She was diagnosed with systemic lupus
eythematosus (SLE) and ileotyphus during the
follow-up. Her graft has remained patent as of the
last visit.
CASE REPORTS
A 32-year-old woman was admitted to our hospital on
February 24, 1992 because of abdominal distention, short
breath, lassitude, and jaundice. Shewas anoperating room
nurse with an 8-year history of menoxenia and acyesis
after marriage. She denied any tobacco and alcohol or
hepatotoxic drug consumption. She had no history of
1036.e15

1036.e16 Cas cliniques Annales de chirurgie vasculaire
heart and lung disease. In January 1991, the patient was
admitted to another hospital because of jaundice and asci-
tes. An inferior cavography revealed total occlusion of the
IVC involving the supra-hepatic portion. She was then
diagnosed with BCS. She had no effective treatment until
admission to our hospital. On admission, she was afebrile,
the heart rate was 119/min, the respiratory rate was 28/
min, and the blood pressure was 120/96 mm Hg. Chest
percussion revealed a flat note on the right lower chest.
Superficial varices on the thoracoabdominal wall with
upward blood flow were noted. The liver was 5 cm below
the right costal margin and the shifting dullness was clear.
Palpationof the spleenwasnot apparent because of ascites.
The abdominal girth was 91 cm. She had moderate edema
and varicose veins in both lower limbs.
The blood cell count was as follows: total leukocyte,
5 � 109/L; erythrocytes, 3.83 � 1012/L; platelets, 118 �109/L; and hemoglobin, 117 g/L. The liver function tests
revealed the following: a normal glutamate pyruvate
transaminase; serum albumin, 26 g/L; total bilirubin, 68.4
mmol/L; and direct bilirubin, 47.88 mmol/L. She had nor-
mal renal function and was euglycemic. The coagulation
function tests revealed a prothrombin time of 20.5 sec and
a prothrombin activity of 36.4%. The hepatitis B surface
antigen and fecal occult bloodwerenegative.A chestX-ray
revealed a right pleural effusion. An abdominal Doppler
ultrasound showed an enlarged liver and spleen, a
moderate amount of ascites, and long-segment IVC
thrombosis. An upper gastroenterography revealed a
grade III varicose vein of the esophagus. According to the
history and results, a diagnosis of BCS was established and
her liver function was Child-Pugh stage C or Wang’s IV
according to the severity of the BCS (the most severe
category).1 Considering her severe disease and risk, she
was treated with a mesojugular shunt through a tunnel
posterior to the sternum. The graft used was of 14 mm
inner diameter and 28 cm long externally supported by
expanded polytetrafluoroethylene (Gore Tex, Newark,
DE) prosthesis, as previously described.7 Approximately
4,800 mL of flavescens ascites was drained when the
abdomen was opened. After establishment of blood flow
through the mesojugular shunt, her portal blood pressure
decreased from51-37 cmof awater column.After surgery,
she was treated with warfarin (2.5 mg/d) until she achie-
ved pregnancy. She resumed her work as an operating
room nurse (including night-shift), even though the third
author (the surgeonwho performed the procedure) firmly
suggested that ‘‘no nightshifts in the OR.’’ Thus, she
resumed her normal life until the time of this writing.
In addition, during her visit to a local hospital or our cli-
nic, we found out that she was pregnant and sponta-
neously delivered a healthy baby girl at term in the
second year postoperatively. In the 5th postoperative
year, she was healthy and her graft was patent, as confir-
med by Doppler ultrasound. The ultrasound showed
that the maximal and minimal blood flow rates were
0.46 m/sec and 0.16 m/sec, respectively.
In October 2004, the patient was admitted because of
macrohematuria and fever. The diagnoses of SLE and
ileotyphus were made based on the 1997 ARA criteria
and hemoculture, respectively. During the hospitaliza-
tion, a Doppler ultrasound showed that the portal flow
was completely retrograde and the graft was patent. A
bone marrow biopsy was performed and no abnormality
was found. Other laboratory studies were as follows: pro-
tein C and S, normal; antithrombin III, 72% (normal
range: 77-127%); positive anticardiolipin antibody, and
elevated erythrocyte sedimentation rate, 81 mm/hr. The
liver function tests were normal. She was given aspirin
(75 mg/d) at the time of discharge.
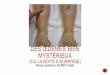
In May 2009, she was called for a follow-up. She had a
well-proportioned build with slightly dilated veins on the
abdominal wall (Fig. 1) and slight varicose veins on both
lower extremities. The newest Doppler ultrasound sho-
wed that the graft was patent with a maximal blood flow
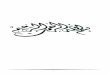
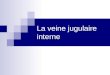
rate of 0.99 m/sec. Computed tomography angiography
showed that the graft was patent and the contrastmedia in
the cross-section was clearly seen (Fig. 2).
DISCUSSION
BCS is a rare disease. According to Rajani et al.8 the
incidence and prevalence of BCS in Western
populations were 0.8 per million per year and 1.4
per million, respectively. In Japan, the incidence
and prevalence were estimated to be 0.2 per million
per year and 2.4 per million in 1989, respectively.9
In Shandong province of China, the prevalence was
about 64 per million in 1988;1 however, the natio-
nal estimate was scanty. The prognosis of untreated
patients with symptomatic BCS is poor. About 90%
of the patients die in 3 years.4Medical therapy alone
had a higher mortality compared with surgical
shunts,10 which can reverse the hepatic congestion
and prevent the cirrhosis.1,11 We have established
classification for BCS as described previously on the
basis of site and extent of occlusive lesions so as to
conveniently select the means for surgical treat-
ment.1,12 In brief, the lesions are divided into three
types: (1) web or short-segment stenosis or occlu-
sion in the suprahepatic IVC, (2) long-segment
stenosis or occlusion in the IVC involving the
suprahepatic portion of the IVC, and (3) involve-
ment of the hepatic veins alone. Furthermore, the
first two types can be divided into sub-types
according to the status (i.e., whether or not the
hepatic vein is involved). The third type can also be
divided into two sub-types according to the extent
of the hepatic vein involved. The lesion of our
patient belongs to the second type (long-segmental
occlusion of the IVC). Surgical shunts play an
essential role for patients with this type. However,
there is no possibility for placing a cavoatrial or
mesoatrial shunt for this patient because both

Fig. 1. Photo: A The patient has a somewhat slender
configuration and well-proportioned body build 17 years
after surgery; B Slightly dilated veins appear on the
abdomen, since the IVC hypertension was not effectively
relieved by the mesojugular shunt.
Vol. 24, No. 7, 2010 Cas cliniques 1036.e17
require a thoracotomy. In consideration of the
patient’s poor preoperative condition, a retrosternal
mesojugular shunt was placed through an upper
abdominal incision to isolate the superior mesen-
teric vein (SMV), and a small cervical incision to
isolate the right internal jugular vein. The graft was
planted into a tunnel posterior to the sternum. The
abdominal side of the prosthesis was used for a
prosthesis-SMV anastomosis, and the cervical part
was used for a prosthesis-internal jugular venous
anastomosis. Both of them were in an end-to-side
fashion. Those maneuvers are relative easy and
safe for a skilled vascular surgeon to complete. This
patient had a rather excellent outcome 17 years
after the mesojugular shunt, indicating that this
approach reached our expected purpose, i.e., not
only to properly relieve her portal hypertension but
also to avoid significant surgical trauma. Compared
with other types of shunts, the mesojugular shunt
has the particular advantage of treating severely ill
patients with BCS.7,12 Theoretically, the long-term
patency of the mesojugular shunt should be the
poorest since it has the longest distance for shunt-
ing, requires amuch longer length of prosthesis, and
has a greater chance for inducing grafting throm-
bosis.3 In this case, the prosthetic length was 28 cm
in length, and after surgery this patient had a pre-
gnancy, a postpartum period and SLE, all of which
are hypercoagulable states and could theoretically
easily cause graft failure due to thrombosis. The
graft is still patent as of this writing. Our prosthetic
IVC study indicated that for an endothelialization
prosthesis, the 100 day patency was 100%.13 Up to
17 years later, the adequacy of endothelialization of
the graft is not clear, however, it can be presumed
that there is proper endothelialization on the inner
surface of this particular graft according to our series
on venous grafts,13 and no remarkable neointima is
formed according to the cross-sections of the graft
(Figs. 2C, D). We therefore can expect a much
longer patency in this still young and healthy
patient. Thus, it is of paramount importance to have
a close and successive observation of this case. A
20-, 25-, or 30-year patency could be identified for
such a long venous prosthesis. Clinically, in our
experience, 5- and 10-year patencies of cavoatrial
shunts are 79.8 and 57.1%, respectively.7 The
patency duration of this patient’s graft is now much
longer than those mentioned. We had another male
patient with BCS of the second type with severe
status. He underwent the same operation as the
female patient. His graft was patent until he died of
hepatic cancer in the 12th year after the shunt
operation. We attribute this satisfactory result to the
pump-like action, i.e., the graft between the heart
and the sternum is rhythmically compressed by the
heart. The action provides additional compression
and relaxation, which propels the blood flow to run
from the SMV in the abdomen to the internal
jugular vein. That is to say, an extra-mechanism for
propelling the blood flow is formed, in addition to a
pressure gradient tapering from the abdominal side

Fig. 2. Computed tomography angiography follow-up 17 years after surgery. A, B Show the patent graft in a longi-
tudinal view; C, D Show the graft in different cross-sections.
1036.e18 Cas cliniques Annales de chirurgie vasculaire
of the mesojugular shunt to the jugular venous side,
which drives the blood from the portal vein to the
systemic vein. Thus, both mechanisms together
create a rather excellent effect as it does in this case.
Although surgical shunts have been increasingly
substituted by TIPS after 1993,14 surgical shunts are
still a good choice for patients who cannot be treated
with TIPS in experienced hospitals. This case report
is a good example of this. Surgical shunts can also be
used for correcting TIPS failure.15
In conclusion, the mesojugular shunt could
have a satisfactory long-term patency, and thus we

Vol. 24, No. 7, 2010 Cas cliniques 1036.e19
suggest using it to treat severe patients with BCS
without the possibility for intervention.
REFERENCES
1. Wang ZG, Jones RS. Budd-Chiari syndrome. Curr Probl Surg
1996;33:83-211.
2. Janssen HL, Garcia-Pagan JC, Elias E, et al. Budd-Chiari syn-
drome: a review by an expert panel. J Hepatol 2003;38:
364-371.
3. Chung RT, Iafrate AJ, Amrein PC, et al. Case records of the
Massachusetts General Hospital. Case 15-2006. A 46-year-
old woman with sudden onset of abdominal distention.
N Engl J Med 2006;354:2166-2175.
4. Valla DC. Primary Budd-Chiari syndrome. J Hepatol 2009;50:
195-203.
5. Mohanty D, Shetty S, Ghosh K, et al. Hereditary thrombo-
philia as a cause of Budd-Chiari syndrome: a study from
Western India. Hepatology 2001;34:666-670.
6. Valla DC. Budd-Chiari syndrome and veno-occlusive disease/
sinusoidal obstruction syndrome. Gut 2008;57:1469-1478.
7. Wang ZG, Zhang FJ, Meng QY, et al. Evolution of mana-
gement for Budd-Chiari syndrome: a team’s view from 2564
patients. ANZ J Surg 2005;75:55-63.
8. Rajani R, Melin T, Bj€ornsson E, et al. Budd-Chiari synd-
rome in Sweden: epidemiology, clinical characteristics and
survivaldan 18-year experience. Liver Int 2009;29:253-259.
9. Okuda H, Yamagata H, Obata H, et al. Epidemiological and
clinical features of Budd-Chiari syndrome in Japan. J Hepatol
1995;22:1-9.
10. Ulrich F, Pratschke J, Neumann U, et al. Eighteen years
of liver transplantation experience in patients with
advanced Budd-Chiari syndrome. Liver Transpl 2008;14:
144-150.
11. Menon KV, Shah V, Kamath PS. The Budd-Chiari syn-
drome. N Engl J Med 2004;350:578-585.
12. Wang ZG, Zhang FJ, Li XQ, et al. Management of Budd-
Chiari syndrome: what is the best approach? J Gastroen
Hepatol 2004;19:S212-S218.
13. Wang ZG, Zhang H, Pu LQ, et al. Can endothelial seeding
enhance patency and inhibit neointimal hyperplasia?
Experimental studies and clinical trial of endothelial seeded
venous prostheses. Int Angiol 2000;19:259-269.
14. Ochs A, Sellinger M, Haag K, et al. Transjugular intrahepatic
portosystemic stent-shunt (TIPS) in the treatment of Budd-
Chiari syndrome. J Hepatol 1993;18:217-225.
15. Rossle M, Olschewski M, Siegerstetter V, et al. The Budd-
Chiari syndrome: outcome after treatment with the trans-
jugular intrahepatic portosystemic shunt. Surgery 2004;135:
394-403.