Upload
others
View
4
Download
0
Embed Size (px)
Citation preview
REVIEW
Therapeutic applications of the carbonic anhydrase inhibitors
Claudiu T SupuranUniversità degli Studi, Laboratorio di Chimica Bioinorganica, Rm 188, Via della Lastruccia 3, I-50019 Sesto Fiorentino (Firenze), ItalyTel.: +39 055 457 3005;Fax: +39 055 457 3385;E-mail: [email protected]
part of
Keywords: anticancer drug, antiglaucoma agent, antiobesity agent, carbonic anhydrase, enzyme inhibitor, isozyme, sulfamate, sulfamide, sulfonamide, tumor-progression marker
10.2217/14750708.4.3.355 © 2
Inhibitors of the zinc enzyme carbonic anhydrase (CA) targeting different isozymes among the 15 presently reported in humans have various therapeutic applications. These enzymes are efficient catalysts for the hydration of carbon dioxide to bicarbonate and protons, playing crucial physiological/pathological roles related to acid–base homeostasis, secretion of electrolytes, transport of ions, biosynthetic reactions and tumorigenesis. Many CA inhibitors have been reported as antiglaucoma, anticancer and antiobesity agents, or for the management of a variety of neurological disorders, including epilepsy and altitude disease. Furthermore, some CA isozymes appear to be valuable markers of tumor progression in a variety of tissues/organs. Various CAs present in pathogens such as Plasmodium falciparum, Helicobacter pylori, Mycobacterium tuberculosis, Candida albicans and Cryptococcus neoformans, have started to also be investigated recently as drug targets. Recent progress in all these areas, as well as in the characterization of new such enzymes isolated in many other organisms/tissues, in addition to their detailed catalytic/inhibition mechanisms, are reviewed herein, together with the therapeutic use of these enzyme inhibitors and drug-design studies for obtaining such new-generation derivatives with improved activity.
Among the zinc enzymes extensively studied,the carbonic anhydrases (CAs) occupy a specialplace for several reasons. These enzymes areubiquitous in all kingdoms, starting witharchaea, bacteria, algae and green plants, andending with superior animals, including verte-brates [1–8]. Their physiological function isessential for these organisms, as CAs catalyze avery simple physiological reaction, the inter-conversion between CO2 and bicarbonate anda proton [1–8]. This reaction is critical for respi-ration and transport of CO2 between metabo-lizing tissues and excretion sites, secretion ofelectrolytes in a variety of tissues and organs,pH regulation and homeostasis, CO2 fixation(for algae and green plants), several metabolicbiosynthetic pathways (in vertebrates), tumori-genesis and signal transduction [1–8]. Inhibition(and also activation) of these enzymes may beexploited clinically in the treatment or preven-tion of a variety of disorders [1–3]. In conse-quence, CA inhibitors (CAIs) possess a varietyof applications in therapy [1]. In mammals, 16different α-CA isozymes or CA-related pro-teins (CARPs) have been described, with verydifferent subcellular localization and tissue dis-tribution [1–8]. There are several cytosolicforms (CA I–III and CA VII), five membrane-bound isozymes (CA IV, CA IX, CA XII,CA XIV and CA XV), two mitochondrial
forms (CA VA and CA VB), as well as asecreted CA isozyme (in saliva and milk;CA VI). Among the membrane-bound CAs,isoforms CA IV and XV are anchored to mem-branes by means of glycosylphosphatidyl-inositol (GPI) tails, whereas isozymes IX, XIIand XIV are transmembrane proteins possess-ing just one transmembrane domain [1–8]. How-ever, all these five isozymes have their active siteoutside the cell, and are thus commonly knownas extracellular CAs [1–8].
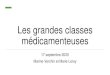
Catalytic/inhibition mechanismIsozymesOver the phylogenetic tree, CAs are encodedby several (probably four) distinct, evolution-arily unrelated gene families: the α-CAs(present in vertebrates, bacteria, algae andcytoplasm of green plants); the β-CAs (pre-dominantly in bacteria, algae and chloroplastsof both mono- as well as dicotyledons); theγ-CAs (mainly in archaea and some bacteria);and the δ-CAs, evidenced so far in somemarine diatoms (Figure 1) [1–8].
CAs are metalloenzymes and most of themhave a Zn(II) ion within their active sites,although the δ-CAs seem to be Cd(II) enzymesand the γ-CAs use Zn(II), Co(II) or Fe(II) as ametal ion cofactor [1–8]. The metal ion of CAs isessential for catalysis [1–8]. X-ray crystallographic
007 Future Medicine Ltd ISSN 1475-0708 Therapy (2007) 4(3), 355–378 355
REVIEW – Supuran
356
data carried out mainly on the α-CA family ofenzymes showed that the metal ion is situated atthe bottom of a 15-Å deep active-site cleft,being coordinated by three histidine residues(His94, 96 and 119) and a H2O/OH- ion [1–8].The Zn-bound water is also engaged in H-bondinteractions with the hydroxyl moiety ofThr199, which in turn is bridged to the carbox-ylate moiety of Glu106 (these amino acids areconserved in all α-CAs currently known [1–5]).These interactions enhance the nucleophilicityof the Zn-bound H2O/OH- ion, and orient thesubstrate (CO2) in a favorable location fornucleophilic attack (Figure 1A) [1–5].
The first x-ray crystallographic structure of amember of the β-CA family has been deter-mined by Mitsuhashi and colleagues for theenzyme isolated from the red algae Porphyrid-ium purpureum (Figure 1B) [9]. This CA monomeris composed of two internally repeating struc-tures, being folded as a pair of fundamentallyequivalent motifs of an α/β-domain and threeprojecting α-helices. The motif is very distinctfrom that of either α- or γ-CAs. This
homodimeric CA appeared like a tetramer witha pseudo 2–2–2 symmetry. The active-siteZn(II) ion was shown to be coordinated by aCys–Asp–His–Cys tetrad that is strictly con-served among the β-CAs, and no H2O mole-cule was found in the Zn-liganding radius,indicating that the Zn(OH)2 mechanism in α-and γ-CAs is not directly applicable to the casein β-CAs [9]. This first report was soon fol-lowed by another, in which the structure of the‘cab’-type β-CA from the archaeon Methano-bacterium thermoautotrophicum (Cab) has beendetermined to a resolution of 2.1 Å (Figure 1C)[10]. Cab exists as a dimer with a subunit foldsimilar to that observed in ‘plant’-type β-CAs.The active-site zinc ion was shown to be coor-dinated by the amino acid residues Cys32,His87 and Cys90, with the tetrahedral coordi-nation completed by a H2O molecule [10]. Themajor difference between plant- and cab-typeβ-CAs is in the organization of the hydropho-bic pocket (except for the aforementioned Zncoordination). The structure also revealed aHEPES buffer molecule, bound 8 Å away from
Figure 1. Metal ion coordination sphere in the four classes of carbonic anhydrases.
(A) α-carbonic anhydrases (CAs; hCA II numbering). (B) Porphyridium purpureum and Escherichia coli β-CAs. (C) Pisum sativum chloroplast and Methanobacterium thermoautotrophicum β-CAs. (D) γ-class CA from Methanosarcina thermophila (M = Zn(II), Co(II) or Fe(II) – which can be either tetra-, penta- or hexa-coordinated by additional water molecules; Cam numbering of the His residues) and δ-class CA from Thalassiosira weissflogii (M = Cd(II) or Zn(II) – the exact geometry of the metal ion is not known).
N
NH
O
O
Zn SS
N
NH
Zn SS
OH2
NNH
NH
N
NH
M2+
OHH2O
NNH N
NH
N
NH
NH
O
O
O
H
OH
OH
Zn2+
-A B
C D
Thr199
Glu106
His94
His96
His119
Asp residue
Cys residue
Cys residue
Cys residue
Cys residue
His residue
His residueHis81
His122
His117
M = Zn, Co, Fe or Cd
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
the active-site Zn, which suggests a possibleproton-transfer pathway from the active site tothe solvent [10]. The structure of the β-CA fromthe dicotyledonous plant Pisum sativum at1.93 Å resolution has also been reported(Figure 1C) [11]. The molecule assembles as anoctamer with a novel dimer-of-dimers-of-dim-ers arrangement. Two distinct patterns of con-servation of active-site residues were observed,implying two potentially mechanistically dis-tinct classes of β-CAs. The active site is locatedat the interface between two monomers, withCys160, His220 and Cys223 binding the cata-lytic Zn ion and residues Asp162 (oriented byArg164), Gly224, Gln151, Val184, Phe179and Tyr205 interacting with the substrate ana-logue, acetic acid [11]. The substrate-bindinggroups have a one-to-one correspondence withthe functional groups in the α-CA active site,with the corresponding residues being closelysuperposable by a mirror plane. Therefore,despite differing folds, α- and β-CAs have con-verged upon a very similar active-site designand are likely to share a common mechanism ofaction [11].
The prototype of the γ-class of CA has beencharacterized from the methanogenic archaeonMethanosarcina thermophila (Figure 1D) [12]. Thecrystal structures of Zn-containing and Co-sub-stituted γ-CA from M. thermophila werereported in the unbound form and cocrystallizedwith sulfate or bicarbonate. Relative to the tetra-hedral-coordination geometry seen at the activesite in the α-CAs, the active site of γ-CA containsadditional metal-bound water ligands, so thatthe overall coordination geometry is trigonalbipyramidal for the Zn-containing enzyme andoctahedral for the Co-substituted enzyme [12].Ligands bound to the active site make contactswith the side chain of Glu62 in a manner thatsuggests this side chain to be protonated. In theuncomplexed Zn-containing enzyme, the sidechains of Glu62 and Glu84 appear to share aproton; additionally, Glu 84 exhibits multipleconformations. This suggests that Glu84 mayact as a proton shuttle, which is an importantaspect of the reaction mechanism of α-CAs, forwhich a histidine active-site residue generallyperforms this function (usually His64) [1–8].
X-ray absorption spectroscopy at the ZnK-edge indicates that the active site of the marinediatom, Thalassiosira weissflogii CA, is strikinglysimilar to that of mammalian α-CAs. The Zn hasthree histidine ligands and a single H2O mole-cule, being quite different from the β-CAs of
higher plants in which zinc is coordinated by twocysteine thiolates, one histidine and a H2O mole-cule [13]. The diatom CA shows no significantsequence similarity with other CAs and may rep-resent an example of convergent evolution at themolecular level [13]. In the same diatom, an unu-sual discovery has been made: the first Cd-con-taining enzyme, which is a CA-type protein [14].The marine diatom, T. weissflogii, growing underconditions of low Zn, typical of the marine envi-ronment, and in the presence of Cd, led toincreased levels of cellular CA activity, althoughthe levels of TWCA1, the major intracellularZn-requiring isoform of CA in T. weissflogii,remained low [14]. 109Cd labelling comigrates witha protein band that showed this CA activity to bedistinct from TWCA1 on native polyacrylamidegel electrophoresis (PAGE) of radiolabeledT. weissflogii cell lysates. The levels of the Cd pro-tein were modulated by CO2 in a manner that isconsistent with a role for this enzyme in carbonacquisition. Purification of the CA-active fractionleads to the isolation of a Cd-containing proteinof 43 kDa, being clear that T. weissflogii expressesa Cd-specific CA, which, particularly under con-ditions of Zn limitation, can replace the Znenzyme TWCA1 in its carbon-concentratingmechanism [14]. This enzyme is considered tobelong to the δ-CA class (Figure 2).
The catalytic mechanism is well understoodfor the α-CAs, and will be discussed in detailhere. The active form of the enzyme is the basicone, with hydroxide bound to Zn(II)(Figure 1A & 2A) [1–8]. This strong nucleophileattacks the CO2 molecule bound in a hydro-phobic pocket in its neighbourhood (the elusivesubstrate-binding site comprises residuesVal121, Val143 and Leu198 [1–8]) (Figure 2B),leading to formation of bicarbonate coordinatedto Zn(II) (Figure 2C). The bicarbonate ion is thendisplaced by a water molecule and liberated intosolution, leading to the acid form of the enzyme,with water coordinated to Zn(II) (Figure 2D),which is catalytically inactive [1–8]. In order toregenerate the basic form A, a proton-transferreaction from the active site to the environmenttakes place, which may be assisted either by active-site residues (such as His64 – the proton shuttle inisozyme CA II) or by buffers present in themedium [1–8]. The process may be schematicallyrepresented by Equations 1A & B.
The rate-limiting step in catalysis is the sec-ond reaction, that is, the proton transfer thatregenerates the Zn-OH- species of the enzyme(Figure 3) [1–8].
357www.futuremedicine.com
REVIEW – Supuran
358
Equations
Figure 2. Schematicfor α-carbonic anhy
A. EZn2+–OH + CO2
B. EZ
-
Zn2+
-OH
His11His96His94
Zn2+
OH2
His119
His96His94
-BH+ B
A
D
Two main classes of CAIs are known: themetal-complexing anions (inorganic inhibitors),and the unsubstituted sulfonamides and theirderivatives (e.g., sulfamates or sulfamides) – theorganic inhibitors. All inhibitors of interest fortheir therapeutic applications bind to the Zn(II)ion of the enzyme, either by substituting thenonprotein Zn ligand (Figure 3A) or by adding themetal coordination sphere (Figure 3B), generatingtrigonal-bipyramidal species [1–8]. Sulfonamides,which are the most important CAIs, bind in atetrahedral geometry of the Zn(II) ion (Figure 3A),in a deprotonated state, with the nitrogen atomof the sulfonamide group coordinated to Zn(II).Anions may bind either in tetrahedral geometryof the metal ion or as trigonal-bipyramidaladducts, such as the thiocyanate adduct shownin Figure 3B [1–8].
X-ray crystallographic structures are availablefor many adducts of sulfonamide/sulfamate/sulfa-mide inhibitors with various isozymes [1–8,15–24].In all these adducts, the deprotonated sulfona-mide is coordinated to the Zn(II) ion of theenzyme, and its NH moiety participates in a Hbond with the Oγ of Thr199, which in turn isengaged in another H bond to the carboxylate
group of Glu106 [15–17]. One of the oxygenatoms of the SO2NH moiety also participates ina H bond with the backbone NH moiety ofThr199 [15–24]. In Figure 4, the crystal structures ofthe human isoform hCA II adducts with the sim-plest compounds incorporating a sulfamoyl moi-ety (sulfamide and sulfamic acid, respectively) areshown as examples of the binding of sulfona-mide, sulfamate and sulfamide inhibitors [15].The binegatively charged (NH)SO32- sulfamateion and the monoanion of sulfamideNHSO2NH2- were shown to bind to the Zn(II)ion within the enzyme active site [15]. These twostructures provide some close insights into whythis functional group (the sulfonamide) appearsto have unique properties for CA inhibition:
• It exhibits a negatively charged and mostlikely monoprotonated N coordinated to theZn(II) ion
• Simultaneously, this group forms a H bond asdonor to the oxygen Oγ of the adjacentThr199
• A H bond is formed between one of the SO2oxygens to the backbone NH of Thr 199
Thus, the basic structural elements explainingthe strong affinity of the sulfonamide moiety forthe Zn(II) ion of CAs were delineated in alldetails by using these simple compounds as proto-typical CAIs, without the need to analyze theinteractions of the organic scaffold, usuallypresent in other inhibitors (generally belonging tothe aromatic/heterocyclic sulfonamide class [15]).Despite important similarities of the binding ofthese two inhibitors to the enzyme with that ofaromatic/heterocyclic sulfonamides of the typeRSO2NH2 previously investigated, the absenceof a C–SO2NH2 bond in sulfamide/sulfamicacid leads to a different H-bond network in theneighborhood of the catalytical Zn(II) ion,which was shown to be useful for the drugdesign of more potent CAIs, possessing differ-ent Zn-binding functions than the classicalsulfonamides [15].
A very important discovery in parasitic CAshas been reported by Krungkrai and colleagues,who discovered the presence of at least two differ-ent CAs in Plasmodium falciparum, the protozoacausing malaria [25]. Red cells infected withP. falciparum contained CA amounts approxi-mately twice as high as those of normal red cells.The three developmental forms of the asexualstages (i.e., ring, trophozoite and schizont) wereisolated from their host red cells and found tohave stage-dependent CA activity. This enzyme
representation of the catalytic mechanism drase-catalyzed CO2 hydration.
EZn2+–HCO3 EZn2+–OH2 + HCO3
EZn2+–OH + H+n2+–OH2
H2O- -
-
O
O
9
-Zn2+
O
O
OH
His119
His96His94
Zn2+
-OH
His119
His96His94
+ CO2
+ H2O
- HCO3
B
C
-
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
Figure 3. Carbonic a(sulfonamide) and i
Figure 4. Adducts osimplest sulfonamid
(A) Sulfamic acid hCA II-determined by x-ray crys
Zn2+
-HN
S
R
O
O
His
His96His94
EZn2+–OH2 + I
EZn2+–OH2 + I
Tetrahedral add(sulfonamide)
A
A
B
was then purified to homogeneity by using multi-ple steps of fast-liquid chromatographic tech-niques, showing a Mr of 32, being active inmonomeric form (the human red cell enzyme wasalso purified for comparison with the parasiteenzyme in this study) [25]. The parasite–enzymeactivity was sensitive to well-known sulfonamideCAIs, such as sulfanilamide and acetazolamide
(AZ). The kinetic properties and amino-terminalsequences of the purified enzymes from the para-site and host red cell were found to be different,indicating that the purified protein was a distinctprotein (i.e., P. falciparum CA). In addition, theaforementioned enzyme inhibitors showed anti-malarial effect against in vitro growth of P. falci-parum [25]. This very important contributionshows that CAIs may represent valuable futuredrugs for the treatment of malaria.
CAIs & their applicationsThere are at least 16 clinically used drugs/orphandrugs reported to possess significant CA inhibi-tory properties (Figures 5 & 6) [1,26–28], and manyother such derivatives belonging to the sulfona-mide, sulfamate or sulfamide classes are con-stantly reported, designed and synthesized bymeans of rational drug-design processes [29–49].
Compounds used clinically, such as AZ(Figure 5A), methazolamide (Figure 5B), ethox-zolamide (Figure 5C), the orphan drug benzola-mide (Figure 5D) and dichlorophenamide (DCP;Daranide®) (Figure 5E), have been known formany years and were initially developed in thesearch for diuretics [26]. Although their diureticuse was not extensive [26–28], it was found thatsuch enzyme inhibitors could be employed for thesystemic treatment of glaucoma [26]. Thus, manysuch drugs (e.g., AZ, methazolamide and DCP)are still presently used in ophthalmology (see dis-cussion later in the text), whereas two novel deriv-atives, dorzolamide (Figure 5F) and brinzolamide(Figure 5G) have been developed in the 1990s astopically acting antiglaucoma agents [26–28].
The antitumor sulfonamide indisulam(Figure 5H) is in Phase II clinical development forthe treatment of solid tumors [50], whereas theantiepileptic sulfamate topiramate (Figure 6A) [51]and sulfonamide zonisamide (Figure 6B) [22] wererecently shown to possess significant inhibitoryproperties against many physiologically relevantCA isozymes. The same is true for the anti-psychotic sulpiride (Figure 6C) [52]. The sulfamatespossessing steroidal-like scaffolds COUMATE-667 (Figure 6D) [53] and EMATE (Figure 6E) [54]were initially discovered as steroid sulfatase (STS)inhibitors [53] and subsequently shown to be lownanomolar CAIs. These compounds are also inclinical development for the treatment of breasttumors in which both STS and some CA iso-zymes are overexpressed [1,53,54]. The sulfonamidecyclooxygenase (COX)-2 inhibitors celecoxib(Figure 6F) [55] and valdecoxib (Figure 6G) [23] alsoact as potent inhibitors of many CA isozymes,
nhydrase inhibition mechanism by organic norganic (anion) inhibitors.
f human carbonic anhydrase II with the es.
(HO)SO2(NH2) and (B) sulfamide hCA II-SO2(NH2)2, tallography [15].
119
-
Zn2+
OH2N
S
C
His119
His96His94
EZn2+–I + H2O
EZn2+–OH2(I)
(substitution reaction)
(addition reaction)
Tetrahedral adduct
uct
Trigonal-bipyramidal adduct
Trigonal-bipyramidal adduct(thiocyanate)
B
359www.futuremedicine.com
REVIEW – Supuran
360
Figure 5. Chemical c
A
D
G
N
N
O
Acetazolam
N
SC6H5
OO
Benzolamid
O
and some of their clinical applications (e.g., theprevention of some gastrointestinal tumors) arecorrelated with the strong inhibition of someCAs [23,55]. The sulfimine artificial sweetener sac-charin (Figure 6H) is also a very potent inhibitor ofseveral physiologically relevant mammalian CAisoforms (Table 1) [56].
Examples of inhibitory effects of some of theseclinically used drugs against the mammalian iso-forms CA I–XIV are shown in Table 1. Data inTable 1 show that only isoform III is not suscepti-ble to inhibition by sulfonamides and sulfamates,whereas all other CA isoforms possessing catalyticactivity – CA I, II, IV, VA, VB, VI, VII, IX, XII,XIII and XIV (CA XV is not present in humans)– are appreciably inhibited by many of the clini-cally used drugs, with inhibition constants inmany cases in the low nanomolar range. Thesevery diverse inhibition profiles of the various iso-zymes with derivatives discussed above mayexplain the very different clinical applications of
the CAIs, ranging from diuretics and antiglau-coma agents, to anticancer, antiobesity andantiepileptic drugs [1–8,26,27].
Applications of CAIs in ophthalmologyCAIs constitute an important class of drugs in thearmamentarium of antiglaucoma agents [1,2,26,27].In addition to the classical, systemically used sul-fonamides (AZ, methazolamide, DCP and ethox-zolamide [1,2,26,27]), two topically acting agentsbecame available in the last years, dorzolamide andbrinzolamide [1,2,26,27]. The two drugs are effectivein reducing intraocular pressure (IOP) by20–25%, and show fewer side effects comparedwith the systemically applied sulfonamides [1,2].Still, the observed side effects, including stinging,burning or reddening of the eye, blurred vision,pruritus, and bitter taste, may lead, in many cases,to patient noncompliance and the need to useother drugs, or to develop topically acting sulfona-mides possessing less side effects. All but the last
ompounds.
E F
B C
H
S
N
S
N
OO
ide
S
NN
S
N
N
O
OO
Methazolamide
N
S SN
O
O O
Ethoxzolamide
S
NN
S
N
OO
e
SS
Cl
Cl
O
ONN
O
O
Dichlorophenamide
S S
S N
O
O
O O
N
Dorzolamide
NS S
N
S N
O
O
O O
N
NS
S
OO
NCl
O
ON
IndisulamBrinzolamide
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
Figure 6. Chemical c
O
O
O
O
S OO
NCO
Va
A
D
side effects mentioned above are probably due tothe fact that dorzolamide and brinzolamide aresalts of weak bases (secondary amines) with a verystrong acid (HCl), so that the pH of the drug solu-tion is rather acidic (generally around 5.5). Thus,many studies were reported ultimately for thedevelopment of topically acting sulfonamide CAIsthat can be formulated in solution at near neutralpH [31,32,34,35,37,38,44,45,47]. Conversely, many clini-cal studies regarding the two drugs from this classavailable up to now (dorzolamide and brinzola-mide), alone or in combination with other agents,were reported in the last few years [57–61]. Thus, in
a randomized, double-blind study the efficacy ofdorzolamide 2% and brinzolamide 1% in loweringIOP and in evaluating side effects were recentlyreported [57]. IOP decreased significantly frombaseline for both drugs, with no statistically signif-icant differences between dorzolamide 2% andbrinzolamide 1% either before or after eye-dropadministration. The most frequent side effect wasocular pain in the case of dorzolamide 2% andblurred vision in brinzolamide 1%. The resultssuggested that dorzolamide 2% and brinzolamide1% have similar IOP-lowering efficacies with dif-ferent side effects [57]. The nonselective β-blocker
ompounds.
O
O
OO
SN
O
O
Topiramate
NO
S
O
O
N
Zonisamide
N
S
N
OO
OO
NSulpiride
O O
UMATE-667
O
O
S OO
NEMATE
NN
F
F
F
S NO
O
Celecoxib
S NO
O
O N
ldecoxib
S
N
O
O O
Saccharin
E F
B C
HG
361www.futuremedicine.com
REVIEW – Supuran
362
Table 1. Inhibition dsaccharin against is
Isozyme
5A*
hCA I‡ 250
hCA II‡ 12
hCA III‡ 3.105
hCA IV‡ 74
hCA VA‡ 63
hCA VB‡ 54
hCA VI‡ 11
hCA VII‡ 2.5
hCA IX‡ 25
hCA XII§ 5.7
mCA XIII‡ 17
hCA XIV‡ 41
The isoforms CA VIII, X and*Refers to the figure numb‡Full-length enzyme.§Catalytic domain.¶The data against the full-h: Human; m: Murine isozy
timolol and dorzolamide both lower IOP, but thetwo agents have different mechanisms of actionand their effects are additive when administeredtogether [58]. Therefore, these drugs are frequentlyused concomitantly to treat patients with open-angle glaucoma who have not adequatelyresponded to first-line therapy (β-blockers or sul-fonamide CAIs). A barrier to good compliancewith concomitant therapy is the need to adminis-ter five or six drops of medication on two or fouroccasions during the day. Timolol 0.5% and dor-zolamide 2.0% have therefore been combined in asingle formulation, reducing the number ofadministrations required to two per day [58]. Clini-cal trials in patients with glaucoma have demon-strated that dorzolamide 2%/timolol 0.5%(dorzolamide/timolol) is superior to monotherapywith the individual components [58]. When dor-zolamide/timolol administered twice daily wascompared with concomitant treatment with dor-zolamide 2% and timolol 0.5%, each administeredtwice daily for 90 days, both regimens resulted inmarked lowering of trough IOP (measured justbefore the morning dose) compared with baseline(reduction in IOP = 4.2 mmHg). When the com-bined formulation was compared with a concomi-tant regimen that included dorzolamide 2% threetimes a day and timolol 0.5% twice daily, the con-comitant regimen was slightly more efficacious
than the combined regimen, after 90 days: IOPwas lowered by 3.6 mmHg in the combined groupversus 4.1 mmHg in the concomitant group. Dor-zolamide/timolol has been compared with con-comitant administration of timolol 0.5% and theIOP-lowering miotic drug, pilocarpine 2.0%. Thisnon-blind, patient-preference study found thatboth regimens reduced IOP. However, the dorzola-mide/timolol combination was preferred bypatients because of reduced frequency and severityof adverse effects and less frequent administration[58]. Dorzolamide/timolol was well tolerated inclinical trials, the adverse effects reflected those ofthe individual components and no additional tol-erability issues were identified. However, thepotential for timolol to cause cardiorespiratoryeffects must be considered when prescribing thiscombination, whereas dorzolamide, being a sul-fonamide, can cause allergic reactions in those whoare hypersensitive to this class of drug [58].
Similarly, the additive effect of latanoprost0.005% in patients who have uncontrolled IOPusing timolol 0.5% and dorzolamide 2% has beeninvestigated [59]. Latanoprost had an additive effectwhen used as a third drug for patients on timololand dorzolamide who were in need of further IOPreduction. These results suggested that latanoprostmay be very effective in some patients with poorlycontrolled glaucoma on multiple therapy [59].
ata with the clinically used sulfonamides, the clinically used sulfamate (topiramate) and ozymes I–XIV.
Ki (nM)
5B* 5C* 5E* 5F* 5G* 6A* 6H*
50 25 1200 50000 45000 250 18540
14 8 38 9 3 10 5950
1.105 5000 NT 8000 NT NT NT
6200 93 15000 8500 NT 4900 7920
65 25 630 42 50 63 10060
62 19 21 33 30 30 7210
10 43 79 10 0.9 45 935
2.1 0.8 26 3.5 2.8 0.9 10
27 34 50 52 37 58¶ 103
3.4 22 50 3.5 3.0 3.8 633
19 NT 23 18 NT 47 12100
43 25 345 27 24 1460 773
XI are devoid of catalytic activity and probably do not bind sulfonamides as they do not contain Zn(II) ions [1].
er from Figures 5 & 6.
length enzyme is of 1590 nM. me; NT: Not tested (no data available).
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
The reduction in IOP by topical dorzolamide2% and oral methazolamide (5 mg/kg) in dogshas also been investigated in order to determineif the combination of both drugs would reduceIOP more than either drug administered alone.Topical dorzolamide 2%, administered twiceand three times a day, significantly decreasedIOP in glaucomatous dogs on the first day(twice daily 7.6 mmHg and three times a day16.4 mmHg), which was greater by day 5 (twicedaily 10.4 mmHg and three times daily13.9 mmHg). Oral methazolamide also signifi-cantly lowered IOP in both eyes. Oral meth-azolamide combined with topical dorzolamide2% (instilled in the eye from day 3 to 5) also sig-nificantly lowered IOP of both eyes for all daysand, for day 5, the mean IOP was decreased by7.9 mmHg (methazolamide plus dorzolamide)and 7.5 mmHg (methazolamide only). Topicaldorzolamide (instilled in the drug eye for day1–5) combined with oral methazolamide(administered from day 3 through to day 5) sig-nificantly lowered IOP in the eye on day 1(5 pm, 9.6 mmHg), for day 3 (11 am and 5 pm)and for all of day 5 for both eyes (5 pm: controleye 9.5 mmHg; drug eye 9.0 mmHg). Topicaldorzolamide (2%) instilled three times a dayproduced similar IOP declines compared withthe combination of oral methazolamide anddorzolamide 2% administered twice daily. Thus,dorzolamide (2%) instilled twice or three timesa day caused significant decreases in IOP inglaucomatous dogs. Twice-daily instillationscaused progressive declines in IOP from day 1 today 5. Dorzolamide (2%) combined with oralmethazolamide (5 mg/kg twice daily) producedsimilar but not additional declines in IOP [60].
A comparison study of topical brinzolamide1% twice daily with dorzolamide 2% twice daily,each given with timolol 0.5% twice daily, hasalso been reported [61]. Both treatment regimenssignificantly reduced IOP at all time points:brinzolamide plus timolol by -3.6 to -5.3 mmHg(-14.2 to -21.9%) and dorzolamide plus timololby -3.6 to -5.1 mmHg (-14.1 to -21.2%). Clini-cally relevant IOP reductions (decreases5 mmHg or greater or absolute IOP values of21 mmHg or less) were manifested by50–89.3% of patients under brinzolamide plustimolol and by 43.9–85.4% under dorzolamideplus timolol. The treatments were equivalent inmean IOP lowering. In general, both regimenswere well tolerated. However, more patientsexperienced at least one adverse event with dor-zolamide plus timolol (32.8%) compared with
brinzolamide plus timolol (14.7%). In addition,more patients experienced ocular discomfort(stinging and burning) after dorzolamide plustimolol (13.1%) than after brinzolamide plustimolol (1.7%) in this study [61].
Medical treatment of cystoid macular edema(CME) is another major indication for CAIs [1,62].Initial observations were based on experimentaldata that suggested that AZ can increase fluidabsorption across the retinal pigment epithelium[1,62]. CAIs have also been shown to possess otherdirect effects, both on retinal and retinal pig-ment epithelial cell function, by inducing anacidification of the subretinal space, a decrease ofthe standing potential as well as an increase inretinal adhesiveness [1,62]. It is thought that acid-ification of the subretinal space is responsible forthe increase in fluid resorption from the retina.Several clinical studies have suggested thatpatients with CME due to retinitis pigmentosaand uveitis may react more favorably to treat-ment with CAIs than other etiologies, such asdiabetic maculopathy or macular edema afterretinal vein occlusion [1,62]. A normal clinicalstarting dose of systemic CAI is 500 mg/day,which should be continued for at least 1 monthto see an effect on CME [62].
Recently, the involvement of CA I (an abun-dant isoform with a rather unknown physiologicfunction [1]) in eye pathology has emerged [63].Thus, it is known that excessive retinal vascularocclusion/permeability contributes to thepathogenesis of proliferative diabetic retinopa-thy and diabetic macular edema, leading causesof vision loss in adults. Using mass spectros-copy-based proteomics, Gao and colleaguesdetected 117 proteins in human vitreous andelevated levels of extracellular CA I in vitreousfrom individuals with diabetic retinopathy, sug-gesting that retinal hemorrhage and erythrocytelysis contribute to the diabetic vitreous pro-teome [63]. Intravitreous injection of CA I in ratswas then shown to increase retinal vessel leakageand to cause intraretinal edema. CA I-inducedalkalinization of vitreous increased kallikreinactivity and its generation of factor XIIa revealeda new pathway for contact system activation.CA I-induced retinal edema was decreased bycomplement 1 inhibitor, a neutralizing antibodyto prekallikrein- and bradykinin-receptor antag-onism. Subdural infusion of CA I in ratsinduced cerebralvascular permeability, suggest-ing that extracellular CA I could have broad rel-evance to neurovascular edema [63]. Inhibition ofthe enzyme activity of the extracellular CA I by
363www.futuremedicine.com
REVIEW – Supuran
364
sulfonamide/sulfamate/sulfamide inhibitorscould thus provide new therapeutic opportuni-ties for the treatment of hemorrhage-inducedretinal and cerebral edema, a highly relevantmedical problem.
CAIs & cancerThere are many connections between CA andcancer [1,2,64,65]. Some CA isozymes are predomi-nantly found in cancer cells, lacking from theirnormal counterparts [1,2,64,65]. CA IX was shownto be highly overexpressed in many cancer typesand was present in few normal tissues in a quitelimited amount [64,65]. CA IX expression isstrongly induced by hypoxia present in manytumors, being regulated by the hypoxia-induci-ble factor (HIF) transcription factor and corre-lated with a poor response to classical chemo-and radio-therapies [64,65]. CA IX was recentlyshown to contribute to acidification of thetumor environment by efficiently catalyzing thehydration of CO2 to HCO3- and protons withits extracellularly situated active site [66], leadingboth to the acquisition of metastasic phenotypesand chemoresistance with weakly basic anti-cancer drugs [66,67]. Thus, Svastova and col-leagues proved that CO2 is a significant source ofacidity in tumors (in addition to lactic acid) [66],thereby indicating the relevant contribution ofCA IX in the tumor acidification processes. Thisseminal study provided the first evidence for therole of CA IX in the control of the extracellularpH (pHe) in tumors [66]. It was shown that CAIX can acidify the pH of the culture medium inhypoxia but not in normoxia. This acidificationcould be perturbed by deletion of the enzymeactive site or by inhibiting the CA IX catalyticdomain with selective sulfonamide CAIs, whichwere shown to bind only to hypoxic cells express-ing CA IX [66]. These findings suggested thathypoxia regulates both expression and activity ofCA IX in order to enhance the extracellular acid-ification processes, which may have importantimplications for tumor progression [66]. Con-versely, inhibition of this enzymatic activity byspecific and potent inhibitors was shown torevert these processes, establishing a clear-cutrole for CA IX in tumorigenesis and proving thisenzyme to be a druggable target. The develop-ment of a wide range of potent and selectiveCA IX inhibitors might thus provide useful toolsfor highlighting the exact role of CA IX inhypoxic cancers, to control the pH (im)balanceof tumor cells and to develop novel diagnostic ortherapeutic applications for the management of
such tumors. Indeed, both fluorescent inhibitors[67] or positively charged, membrane-imper-meant sulfonamides [68] that were shown toinhibit only these extracellular CAs have recentlybeen developed as CA IX inhibitors and used asproof-of-concept tools for demonstrating thatCA IX constitutes a novel and interesting targetfor anticancer drug development, as well as forimaging purposes of hypoxic tumors [67–69].
The design of fluorescent sulfonamides thatpreferentially inhibit the activity of CA IX,showing reduced penetration through theplasma membranes and binding to hypoxiccells expressing CA IX, was reported by Cecchiand colleagues [67]. These inhibitors representpromising candidates for developing anticancertherapies based on tumor-associated CA iso-zyme inhibition and offer very interesting toolsfor imaging and further investigation ofhypoxic tumors, due to the fact that they onlyaccumulate in such tissues [66,67].
A series of positively charged, membrane-impermeant sulfonamides were obtained byreaction of aminobenzolamide [5-(4-aminoben-zenesulfonylamino)-1,3,4-thiadiazole-2-sulfon-amide] with tri-/tetra-substituted pyrilium saltspossessing alkyl, aryl or combinations of alkyland aryl groups at the pyridinium ring [68]. Thecompounds were assayed for the inhibition offour physiologically relevant isozymes: thecytosolic hCA I and II, the membrane-anchoredbCA IV and the membrane-bound, tumor-asso-ciated isozyme hCA IX. They showed potentinhibitory activity against all investigated iso-zymes, although with different profiles. ForCA I, the derivatives showed inhibition con-stants in the range of 3–12 nM, for CA II in therange of 0.20–5.96 nM, against CA IV in therange of 2.0–10.3 nM and against CA IX in therange of 3–45 nM. These compounds weredemonstrated to be membrane impermeant dueto the permanent positive charge present intheir molecules. Some of these derivatives werealso tested for their inhibitory activity againstthe Cl-/HCO3- anion exchanger (AE)1. Twoderivatives showed inhibitory activity in the lowmicromolar range, whereas one compound wasinactive at these concentrations. The high affin-ity of these derivatives for the tumor-associatedisozyme CA IX and their membrane impermea-bility make this type of CAI an interesting can-didate for the selective inhibition of only thetumor-associated isozyme and not the cytosolictypes, for which they also show high potency.Furthermore, it was proved for the first time in
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
this study that the CA–AE metabolon can beinhibited by the same type of sulfonamidederivatives [68].
In a recent report, the drug design, synthesis,and transepithelial transport of a group ofthioureido sulfonamide CAIs, which have beenobtained by reaction of isothiocyanate-substi-tuted aromatic sulfonamides with amines, wasalso investigated [69]. These compounds havepotent inhibitory properties against CA IX withKi values in the range of 10–37 nM and Papp val-ues greater than 0.34 × 10-6 cm/s for the absorp-tive transepithelial transport in Caco-2 cells. Inthese cells, one of these compounds was shownto be a substrate for efflux transporters such asp-glycoprotein (p-gp). p-gp activity is not likelyto be rate limiting for intestinal absorption, butmight be useful when targeting hypoxic tumorsexpressing both p-gp and CA IX [69].
Indisulam is a sulfonamide anticancer drugdiscovered at Eisai Co. and is in Phase II clinicaldevelopment for the treatment of solid tumors[5–7]. The combination of indisulam with variousantitumor drugs, such as carboplatin, oxalipla-tin, capecitabine or their salts, for the preventionor treatment of cancer was recently reported [27].Indisulam is a cell-cycle inhibitor and a potentCAI. The combinations have been found to havestrong synergistic activity. The human breastcancer cell line HBC4 was implanted subcutane-ously in nude mice and, when tumor volumereached 114 mm3, the mice were treated withindisulam at dosages of:
• (I) 30.625 mg/kg/day for 5 days
• (II) 1.3125 mmol/kg/day for 14 days orsequentially with (I) on day 1–5
• (II) on day 6–19
The minimum relative tumor volume (mRTV)between the treatment groups was determined andit was found that (II) alone elicited no reductionin tumor growth, while the mRTV for (I) and thecombination groups were 24 and 18% of originaltumor size, respectively. Out of 18 mice dividedequally among the groups, the only tumor-freemouse was in the combination group [27]. Novelsulfonamide-containing indole compounds struc-turally related to indisulam, their pharmacologi-cally acceptable salts and their hydrates wereclaimed by Eisai scientists [27]. In addition, neovas-cularization inhibitors, anticancer agents, metasta-sis inhibitors and anti-inflammatory agents for thetreatment of rheumatoid arthritis comprising thesecompounds as the active component were alsoclaimed [27].
Parkkila’s group investigated the effect of AZ,a potent CAI (Table 1), on the invasive capacity offour renal carcinoma cell lines (Caki-1, Caki-2,ACHN and A-498) [70]. It was found that AZ10 µM inhibited the relative invasion rate ofthese cell lines by between 18 and 74%. TheCaki-2 and ACHN cell lines displayed the high-est responsiveness, and their responses clearlydepended on the AZ concentration in the cul-ture medium. Immunocytochemical and west-ern blotting results identified the presence ofCA isozyme II in the cytoplasm of all four celllines and CA XII on the plasma membrane inthree of four cell lines. Because AZ alonereduced invasiveness of these cancer cellsin vitro, it was concluded that the CAs over-expressed in renal cancer cells contribute toinvasiveness [70]. This valuable study constitutedanother demonstration that CAIs may be usedin the management of tumors that overexpressone or more CA isozymes.
In a series of important studies [71–78],Parkilla’s, Pastorek’s and Harris’ groups investi-gated the expression of various CA isozymes(mainly CA IX and XII) and hypoxia as markersof tumor progression in different organs/tissues.CA IX was shown to be expressed in the baso-lateral plasma membrane of normal biliary epi-thelial cells, but not in hepatocytes. Pastorek’sgroup recently showed that, in the biliary epi-thelial tumors, immunostaining for CA IX wasmainly localized at the basolateral surface of theepithelial cells, as in normal mucosa [71]. All non-invasive dysplastic lesions and 57% of invasivelesions of the gall bladder expressed this isozyme.In the liver, 78% of cholangiocellular malignantlesions showed a positive reaction for CA IX,whereas only 33% of hepatocellular carcinomasshowed a weak immunoreaction [71]. The con-clusion was that abnormal expression of CA IXmay be linked to malignant transformation ofhepatobiliary cells, this enzyme being a promis-ing marker for biliary differentiation in hepato-biliary neoplasms [71]. In another study [72], thesame group examined the expression of CA IXin non-small-cell lung cancers. Of 107 casesanalyzed, 39 (36.4%) had strong mem-brane/cytoplasmic expression of CA IX andwere grouped as positive. The staining was con-fined around areas of necrosis, and a significantassociation of CA IX expression with the extentof necrosis was noted. Nevertheless, 38 out of 74cases with focal or extensive necrosis did notexpress this enzyme [72]. A direct association ofCA IX expression with epidermal growth factor
365www.futuremedicine.com
REVIEW – Supuran
366
receptor, c-erbB-2 and MUC1 expression wasalso noted. Survival analysis showed that CA IXexpression is related to poor prognosis. Multi-variate analysis also revealed that CA IX expres-sion was a significant prognostic factorindependent of angiogenesis. It was concludedthat CA IX is an important molecule in non-small-cell lung cancer, the upregulation of whichoccurs in highly hypoxic/necrotic regions of thetumors. The expression of CA IX was linked tothe expression of a constellation of proteinsinvolved in angiogenesis, apoptosis inhibition,and cell–cell adhesion disruption, whichexplained the strong association of this enzymewith poor clinical outcome [72].
A similar study was then reported in a cohortof patients with invasive breast cancer [73]. Themajority of patients were treated with adjuvanthormonal or chemotherapy. The frequency ofCA IX expression, its association with recog-nized prognostic factors and the relationshipwith outcome was evaluated by univariate andmultivariate statistical analyses. CA IX expres-sion was present in 49 (48%) out of 103 cases.The level of CA IX expression was found to besignificantly associated with tumor necrosis(p < 0.001), higher grade and negative estrogenreceptor status [73]. CA IX expression was associ-ated with worse relapse-free survival and overallsurvival in an unselected cohort of patients withinvasive breast carcinoma. The potential role ofCA IX as a marker of hypoxia within breast car-cinomas was also indicated by a significantassociation with necrosis [73].
There is increasing evidence that hypoxia-reg-ulated gene expression influences tumor aggres-siveness, contributing to the poorer outcome ofpatients with hypoxic tumors [74]. The role of thetranscriptional complex HIF-1 as an importantmediator of hypoxia-regulated gene expression isone of the best documented pathways. Recently,it has emerged that certain tumor-associated CAscan be added to the list of known HIF-respon-sive genes [72–74]. In such a study, it was provedthat the tumor-associated CA IX is correlatedwith the level of hypoxia in human cervicaltumors [74]. There was a significant positive corre-lation between the level of tumor hypoxia and theextent of CA IX expression. A retrospective studyof 130 squamous cell cervical carcinomas demon-strated that a semiquantitative immunohisto-chemical analysis of CA IX expression in tumorbiopsies is a significant and independent prog-nostic indicator of overall survival and metastasis-free survival after radiation therapy [74]. These
studies provided clinical evidence that CA IXexpression is upregulated in hypoxic human cer-vical tumors and is associated with a poor prog-nosis. CA IX may act as an intrinsic marker oftumor hypoxia and poor outcome after radiationtherapy. The level of CA IX expression may beused to aid in the selection of patients whowould benefit most from hypoxia-modificationtherapies or bioreductive drugs [74]. CA12, thegene encoding isozyme XII, has also been identi-fied as a hypoxia-inducible gene [75]. The expres-sion of CA IX and CA XII in relation to necrosisand early breast tumor progression in 68 cases ofductal carcinoma has been recently examined[75]. CA IX expression was rare in normal epithe-lium and benign lesions, but was present focallyin ductal carcinomas (50% of cases) and in asso-ciated invasive carcinomas (29%). In compari-son, CA XII was frequently expressed in normalbreast tissues (89%), in ductal carcinomas (84%)and in invasive breast lesions (71%). NeitherCA IX nor CA XII expression was associatedwith regional or overall proliferation. Assessmentof mammographic calcification showed thatCA XII expression was associated with theabsence of calcification. These results demon-strate that induction of CA IX and CA XIIoccurs in regions adjacent to necrosis in thesetumors [75]. Furthermore, these data suggestedthat proliferation status does not influenceexpression of either CA isozyme in breast tissues,that hypoxia may be the dominant factor in theregulation of CA IX and that factors related todifferentiation, as determined by tumor grade,dominated the regulation of CA XII. The exist-ence of differential regulation and associationswith an aggressive phenotype may be importantin the development of selective CAIs useful toprevent/treat tumor invasion [1,2,67]. In anotherstudy, the expression and localization of CA IXin head and neck squamous cell carcinoma(HNSCC) was examined and related to the loca-tion of tumor microvessels, angiogenesis, necro-sis and stage [76]. CA IX was induced by hypoxiain three HNSCC cell lines and overexpressed inHNSCC tumor tissue. Overexpression waslocalized to the perinecrotic area of the tumoron immunostaining, and the percentage area ofthe tumor expressing CA IX was significantlyhigher with more tumor necrosis and advancedstage. CA IX was overexpressed in HNSCCbecause of hypoxia and may be a potentialbiomarker for hypoxia in this tumor. Overex-pression may help to maintain the intracellularpH, giving tumor cells a survival advantage and
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
enhancing resistance to radiotherapy and chem-otherapy. Thus, CA IX is considered a potentialtarget for future therapy in HNSCC [76]. In arecent study, the localization of isozymes CA I,II, IX and XII in normal large intestine andcolorectal tumors has been investigated [77].While the normal mucosa of the large intestineshowed high expression for CA I and II, theintensity of the immunostaining for both iso-zymes decreased in benign lesions and was veryweak in malignant tumors. The reciprocal pat-tern of expression observed for these cytoplasmicisozymes and transmembrane CA IX and XII inintestinal tissue specimens supported the sugges-tion that CA IX and XII may be functionallyinvolved in tumor progression to malignancyand/or in invasion [77]. While CA I and II wereshown to be prominent in normal colorectalmucosa, playing a role in regulation of pHhomeostasis and water and ion transport, loss ofexpression of these cytoplasmic isozymes wasshown to consistently accompany progression tomalignant transformation [77].
In another study, the presence of CA XIIalong the human nephron and collecting duct,together with its cellular and subcellular local-ization, have been investigated [78]. CA XII hasbeen revealed to be present in the basolateralplasma membrane of the epithelial cells in thethick ascending limb of Henle and distal convo-luted tubules, and in the principal cells of thecollecting ducts. A weak basolateral signal wasalso detected in the epithelium of the proximalconvoluted tubules. In addition to the normalkidney specimens, this immunohistochemicalstudy included 31 renal tumors [78]. CA XIIshowed moderate or strong plasma membrane-associated expression in most oncocytomas andclear-cell carcinomas. The segmental, cellularand subcellular distribution of CA XII along thehuman nephron and collecting duct suggestedthat it may be one of the key enzymes involvedin normal renal physiology, particularly in theregulation of water homeostasis [78]. Highexpression of CA XII in some renal carcinomasmay contribute to its role in von Hippel–Lindaucarcinogenesis [78,79].
Breast carcinoma is the most frequent cancerin women and is the second leading cause ofdeath [75]. Choroid metastasis of breast carci-noma can be found either at presentation or inremission, being also frequently encountered indisseminated breast cancer with multiple-organmetastasis. It has recently been proposed that theedema-reducing effect of AZ might be used for
fluid removal from the retina to the choroid. In a40-year-old female patient on adjuvant chemo-therapy for breast cancer with an isolatedchoroid metastasis, clinical and radiologicalremission was achieved after orbital radio-therapy, chemotherapy and AZ treatment [75].Thus, AZ may possess another, only slightlyexplored up to now, beneficial clinical use inpatients with choroid metastasis [75].
CAIs in obesityObesity, a multifactorial disorder characterizedby an excess of adipose tissue, represents a chal-lenging medical problem in Western countries,with, for example, 65% of the US populationaffected [8]. Developing countries, such as China,are also not immune to this epidemic, since itwas reported that obesity doubled in women andalmost tripled in men from 1989 to 1997 in thiscountry [8]. Obesity is caused by an excessivelypositive energy balance, with the energy intakeexceeding the expenditure, but the exact etiologyof the disease is largely unknown [8]. Althoughdiet, physical activity and behavioral modifica-tions should theoretically help in controlling thiscondition, very rarely, patients undergoing thesestrategies can lose more than 5–10% of theirbody weight and maintain this loss for a suffi-ciently long period in order to experienceimprovements in blood pressure, plasma lipidlevels, blood glucose and diabetic control [8].Thus, phamacological interventions for thetreatment of obesity are essential. Paradoxically,the drugs available for the treatment of obesityare very few, their mechanism of action hardlyunderstood and their side effects generally quiteserious [8].
Among the many CA isozymes evidenced sofar in diverse organisms all over the phyloge-netic tree, CA VA and CA VB are present inmitochondria and are shown to be involved inseveral biosynthetic processes, such as ureagene-sis [1–8], gluconeogenesis [1–8] and lipogenesis(both in vertebrates, such as rodents, as well asinvertebrates, such as the locust [8,80–83]).Indeed, in several important biosynthetic proc-esses involving pyruvate carboxylase (PC),acetyl CoA carboxylase (ACC) and carbamoylphosphate synthetases I and II, HCO3- and notCO2, is the real substrate of these carboxylatingenzyme. The provision of enough HCO3- isassured mainly by catalysis involving the mito-chondrial isozymes CA VA and CA VB (proba-bly assisted by the high-activity cytosolicisozyme CA II) (Figure 7) [8,84–89].
367www.futuremedicine.com
REVIEW – Supuran
368
Thus, mitochondrial PC is needed for theefflux of acetyl groups from the mitochondria tothe cytosol where the fatty acid biosynthesistakes place [82]. Practically, pyruvate is carboxy-lated to oxaloacetate in the presence of bicarbo-nate and PC. The bicarbonate needed for thisprocess is generated under the catalytic influenceof the mitochondrial isozymes (CA VA and/orCA VB). The mitochondrial membrane isimpermeant to acetyl-CoA, which reacts withoxaloacetate, leading to citrate, which is there-after translocated to the cytoplasm by means ofthe tricarboxylic acid transporter. In the cytosol,the citrate is cleaved and regenerates acetyl-CoAand oxaloacetate. As oxaloacetate is unable tocross the mitochondrial membrane, its decarbox-ylation regenerates pyruvate, which can be thentransported into the mitochondria by means ofthe pyruvate transporter (Figure 7) [8]. The acetyl-CoA generated in the cytosol is in fact used forde novo lipogenesis, by carboxylation in the pres-ence of ACC and bicarbonate, with formation ofmalonyl-CoA. The HCO3- needed in this proc-ess is furnished by the CA II-catalyzed conver-sion of CO2 to HCO3-. Subsequent stepsinvolving the sequential transfer of acetyl groupslead to longer-chain fatty acids [8]. As a whole,
several CA isozymes are critical to the entireprocess of fatty acid biosynthesis: CA VA and/orCA VB within the mitochondria (to provideenough substrate to PC) and CA II within thecytosol (for providing sufficient substrate toACC). It was, in fact, demonstrated that inhibi-tion of CAs by sulfonamides (e.g., trifluoro-methanesulfonamide [TFM], a very potent butunstable CAI [8]) can decrease lipogenesis in adi-pocytes in cell culture [82,83]. In such experi-ments, an indiscriminate inhibition of all CAisozymes present in these tissues is achieved bythe used inhibitor, such as, for example, TFM orAZ [82–84].
Topiramate is an antiepileptic drug possessingpotent anticonvulsant effects due to a multi-factorial mechanism of action: CA inhibition,blockade of sodium channels and kain-ate/α-amino-3-hydroxy-5-methylisoxazole-4-pro-pionic acid (AMPA) receptors, CO2 retentionsecondary to inhibition of the red cell and brainCA isozymes, as well as enhancement of γ-ami-nobutyric acid (GABA)ergic transmission [51]. Aside effect of this drug observed in obese patientswas the loss of body weight [90], although nopharmacological explanation of this phenome-non has been provided. Furthermore, topiramate
Figure 7. The transfer of acetyl groups from the mitochondrion to the cytosol (as citrate) for the provision of substrate for de novo lipogenesis.
All steps involving bicarbonate also need the presence of carbonic anhydrase (CA) isozymes: CA VA and CA VB in the mitochondrion and CA II in the cytosol (see discussion in the text).Adapted from [13].
Mitochondrion Cytosol
Oxaloacetate
[Citrate]c
[Pyruvate]c
Ac-CoA
HCO3-
-CO2
-CO2
CoA
Malonyl-CoA
Fatty acids
ACC
Pyruvate transporter
Tricarboxylate transporterTherapyTherapy
Oxaloacetate
[Citrate]m
Krebs cycle
[Pyruvate]m
Ac-CoA
HCO3-
-CO2PC
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
was shown to reduce energy and fat gain in lean(Fa/?) and obese (fa/fa) Zucker rats [91]. Con-versely, our group recently demonstrated thattopiramate is a very potent (low nanomolar)inhibitor of several CA isozymes, such as CA I,II, IV, VA and VAB, and the x-ray crystal struc-ture of its complex with hCA II has also beendetermined, revealing the basical molecularinteractions that explain the high affinity oftopiramate for the CA active site [51].
Considering these in vitro findings and thereported clinical side effects of the drug thatcaused weight loss in humans and animals [90,91],we also investigated in detail the inhibition ofthe mitochondrial isozymes hCA VA [92] andhCA VB [93] with this drug, showing the com-pound to be a good inhibitor of both (Ki in therange of 30–63 nM). Thus, we hypothesizedthat the inhibition of mitochondrial and/orcytosolic CA isozymes leading to impaired lipidbiosynthesis may represent a means of control-ling weight loss with pharmacological agentssuch as topiramate or any other sulfamate/sul-fonamide CAIs that show effective CA VA/CAVB/CA II inhibition profiles. As a consequence,selective inhibition of mitochondrial CA iso-zymes (CA VA and CA VB) may lead to dimin-ished lipid biosynthesis and a novelpharmacological approach for the treatment ofobesity [8].
Recently, Lynch’s group showed that theantipsychotic drug olanzapine (1–8 mg/kg),but not clozapine, increased body weight infemale rats only [94]. Weight changes weredetectable within 2–3 days and were associatedwith hyperphagia starting approximately 24 hafter the first dose. Chronic administration ofthe drug (12–29 days) led to adiposity, hyper-leptinemia and mild insulin resistance, but nolipid abnormalities or changes in D2-receptordensity were observed. Topiramate, which hasreversed weight gain from atypical antipsy-chotics in humans [95], also attenuated weightgain in rats. Olanzapine, but not clozapine,acutely lowered plasma glucose and leptin [94].Indeed, patients treated with atypical antipsy-chotic drugs commonly gain excess weight.Because obesity is associated with considerablemorbidity and decreased life expectancy, treat-ment of weight gain in these patients is criti-cal. Topiramate was shown to promote weightloss in healthy obese subjects, patients withbipolar disorder, eating disorder and schizo-phrenia, without aggravation of theirpsychotic symptoms [95].
Zonisamide, is another antiepileptic drugused as adjunctive therapy for refractory partialseizures [96]. Owing to its multiple mechanismsof action, it shows a broad spectrum of anti-convulsant activity and has been shown to beeffective in several types of seizures, including par-tial and generalized seizures, tonic–clonic seizuresand absence seizures in patients unresponsive toother anticonvulsants [96]. Recent clinical studieshave demonstrated additional potential for itstherapeutic use in neuropathic pain, bipolar disor-der, migraine, obesity, eating disorders and Par-kinson’s disease, similarly to topiramate [96,97].Being an aliphatic sulfonamide, we have investi-gated whether this compound will also interactwith the CAs [22].
Unill recently, zonisamide was considered toact as a weak CAI, with a Ki of 4.3 µM againstthe cytosolic isozyme hCA II [22]. We proved thatthis is not true. Indeed, testing zonisamide inclassical assay conditions of CO2 hydrase activityof hCA II, with incubation times for the enzymeand inhibitor solution of 15 min, a Ki of10.3 µM has been obtained. However, when theincubation time between enzyme and inhibitorwas increased to 1 h, the obtained Ki was35.2 nM, of the same order of magnitude as thatof the clinically used sulfonamides/sulfamatesAZ, methazolamide, ethoxzolamide and topiram-ate (Ki values in the range of 5.4–15.4 nM). Inhi-bition of the human mitochondrial isozyme hCAVA with these compounds has also been tested bymeans of a dansylamide competition-bindingassay, which showed zonisamide and topiramateto be effective inhibitors, with Ki values in therange of 20.6–25.4 nM [22]. The x-ray crystallo-graphic structure of the adduct of hCA II withzonisamide has also been examined at a resolu-tion of 1.70 Å, showing that the sulfonamidemoiety participates in the classical interactionswith the Zn2+ ion, through coordination to thedeprotonated sulfonamide moiety, and also inter-acting with the Thr199 and Glu106 residues.The benzisoxazole ring of zonisamide has beenshown to be oriented toward the hydrophobicarea of the active site, establishing a large numberof strong van der Waals interactions (
REVIEW – Supuran
370
zonisamide therapy was started at 100 mg/dayorally, with a gradual increase to 400 mg/day anda further increase to 600 mg/day for patients los-ing less than 5% of body weight at the end of12 weeks [99]. The zonisamide group (n = 19)had a mean weight loss of 9.2 kg (1.7 kg; 9.4%loss) at week 32 compared with 1.5 kg (0.7 kg;1.8% loss) for the placebo group (n = 17).Zonisamide was well tolerated, with few adverseeffects [53]. In this preliminary trial, zonisamideand hypocaloric diet resulted in greater weightloss than placebo and hypocaloric diet in thetreatment of obesity [99].
Miscellaneous applications of CAIsSince CAs are ubiquitous enzymes, their inhibi-tion may have other types of applications inaddition to those already mentioned above.Thus, CAIs have been used in the treatment ofthe primary periodic paralyses (PPs), but theirefficacy has not been demonstrated in double-blind, placebo-controlled trials [100]. Therefore,the efficacy of DCP, a potent CAI in the treat-ment of episodic weakness in primary PPs, hasrecently been tested [69]. Two multicenter, rand-omized, double-blind, placebo-controlled cross-over trials, one involving 42 subjects withhypokalemic periodic paralysis (HypoPP) andthe other involving 31 subjects with potassium-sensitive periodic paralysis (PSPP) have been per-formed. In each trial, two 8-week treatment peri-ods were separated by an active washout periodof at least 9 weeks. The primary outcome varia-ble in the HypoPP trial was the occurrence of anintolerable increase in attack severity or fre-quency; the primary outcome variable in thePSPP trial was the number of attacks per week.The HypoPP trial had 13 subjects who exhibiteda preference for either DCP or placebo, and 11of these preferred DCP. In the PSPP trial, DCPsignificantly reduced attack rates relative to pla-cebo [69,100]. DCP also significantly reducedattack rates relative to placebo in the HypoPPsubjects. It was concluded that the drug is effec-tive in the prevention of episodic weakness inboth HypoPP and PSPP [100].
Essential tremor (ET) is another commonmovement disorder that often causes functionaldisability, potentially leading to physical andemotional difficulties [101]. The paucity of dataavailable regarding the underlying pathophysio-logic mechanism of ET hinders the develop-ment of innovative approaches topharmacotherapeutic treatments. Options fordrug therapy include the use of primidone,
β-adrenergic blockers, alcohol, benzodiazepines,gabapentin and CAIs, but few detailed studiesin this field are available [101]. In this context, itmust be mentioned that, although long sus-pected from histochemical evidence for CAactivity on neurons and observations that CAIsenhance the extracellular alkaline shifts associ-ated with synaptic transmission, an extracellularCA located in the brain had not been identifieduntil recently [102]. A candidate for this CA wassuggested by the recent discovery of membraneCA XIV, whose mRNA is expressed in mouseand human brain as well as several other tissues.CA XIV was found by immunostaining on neu-ronal membranes and axons in both mouse andhuman brain. The highest expression was seenon large neuronal bodies and axons in the anter-olateral part of pons and medulla oblongata.Other CA XIV-positive sites included thehippocampus, corpus callosum, cerebellar whitematter and peduncles, pyramidal tract andchoroid plexus. These observations madeCA XIV a likely candidate for the extracellularCA postulated to have an important role inmodulating excitatory synaptic transmission inbrain [102].
By inhibition of CA activity, the regionalblood flow (rBF) in organs increases as hyper-capnia develops [1,103]. However, the effects ofAZ-induced vasodilation have not been esti-mated with respect to vessel size and organsuntil recently [103]. The aim of a recent studywas solely to determine the diameter of the cap-illaries in various organs that respond to CAinhibition by AZ. While the systolic blood pres-sure (SBP), pH, hemoglobin concentration andbase excess did not change, the partial pressureof arterial O2 (PaO2) increased significantly andthe partial pressure of arterial CO2 (PaCO2)decreased significantly with AZ. The rBF wascalculated by using three different sizes (15, 25,and 50 µM) of colored microspheres (CMs).The rBF measured with 15-µM CMs in thebrain, kidneys and liver increased in response toAZ, and the rBF in these organs differedbetween size of CM. However, the rBF, calcu-lated by using the different sizes of CM in thestomach and abdominal muscle, did not changeafter the administration of AZ. AZ-inducedvasodilation occurred in all sizes of vessels in theliver, the small- and medium-sized vessels inkidneys and in the larger capillaries in the brain[103]. Thus, CAIs may be successfully used asdiagnostic tools in magnetic resonance imagingor positron-emission tomography [1,103].
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
The study by Komai and colleagues wasdesigned in order to clarify the effect of Zn defi-ciency on NaCl preference, the lingual trigeminaland taste nerves transduction and CA activity ofthe tongue surface and salivary gland [104]. MaleSprague–Dawley rats, 4 weeks old, were dividedinto four groups and fed Zn-deficient, low-Znand Zn-sufficient diets with free access and pair-feeding. After taking part in the preference testsfor 42 days, the rats took part in the chorda tym-pani and lingual trigeminal nerve recordings,then finally they were sacrificed and the tongueand submandibular gland were excised to meas-ure CA activity. NaCl preference increased onlyafter 4 days of the feeding of Zn-deficient andlow-Zn diets, which means that the taste abnor-mality appeared abruptly in Zn deficieny, even inmarginal deficiency. Reduced CA activities of thetaste-related tissues in the Zn-deficient groupparalleled well with the decreased taste andlingual trigeminal nerve sensitivities [104].
The secretory isozyme CA VI was previouslyidentified as an essential component of mamma-lian saliva [1], and recently it has been shown to bean elementary component of human milk [105].The 42-kDa glycopolypeptide purified fromhuman milk in CAI affinity chromatographyshared 100% homology with salivary CA VI inthe protein sequence analysis (40% coverage),and its digestion with PNGase F (N-glycosidase)resulted in a polypeptide backbone similar in sizeto salivary CA VI. Quantification of CA VI inmilk using a time-resolved immunofluorometricassay revealed an approximately eight-times-higher concentration in human colostrum thanin mature milk, the latter corresponding to thelevels previously detected in human saliva. Thehigh concentration in the colostrum, in particu-lar its functional and structural stability in anacidic milieu and its growth-supporting role inthe taste buds, suggested that milk CA VI is anessential factor in normal growth and develop-ment of the infant alimentary tract [105]. Thissecretory isozyme of human origin, hCA VI, hasbeen cloned, expressed and purified in a bacterialexpression system recently [106]. The kineticparameters for the CO2 hydration reactionproved that hCA VI possessed a significant cata-lytic activity for the physiological reaction in thesame order of magnitude as the ubiquitous iso-form CA I or the transmembrane, tumor-associ-ated isozyme CA IX. A series of sulfonamides andone sulfamate have been tested for their interac-tion with this isozyme. Simple benzenesulfona-mides were rather ineffective hCA VI inhibitors,
with Ki values in the range of 1090–6680 nM.Better inhibitors were detected among derivativesbearing 2- or 4-amino-, 4-aminomethyl or4-hydroxymethyl moieties or among halogenatedsulfanilamides (Ki values of 608–955 nM). Someclinically used compounds, such as AZ, meth-azolamide, ethoxzolamide, DCP, dorzolamide,brinzolamide, topiramate, sulpiride and indisu-lam, or the orphan drug benzolamide, showedeffective hCA VI inhibitory activity, with Ki val-ues of 0.8–79 nM. The best inhibitors were brin-zolamide and sulpiride (Ki values of0.8–0.9 nM), the latter compound also being aCA VI-selective inhibitor. The metallic tastereported as a side effect after the treatment withsystemic sulfonamides may be due to the inhibi-tion of the salivary CA VI. Some of the com-pounds investigated in this study might be usedas additives in toothpastes for reducing the acidi-fication produced by the relevant CO2 hydraseactivity of enamel CA VI, which leads to the for-mation of protons and HCO3- and may play arole in carcinogenesis [106].
An immune-mediated reaction to pancreaticstructures has been postulated for the pathogen-esis of chronic pancreatitis (CP) [107]. Severalreports demonstrate the presence of antibodiesto the pancreatic ductal epithelium in somepatients suffering from CP. Serum antibodies toCA I (anti-CA I) and II (anti-CA II) were shownto be present in patients affected by idiopathicCP. A significant correlation between anti-CA Iand anti-CA II serum levels in control subjectsand in CP patients has been observed. No corre-lation was found between serum antibody levelsand any of the following variables: length of dis-ease, alcohol consumption, smoking habits,pancreatic surgery, pancreatic calcifications, dia-betes and steatorrhea. Serum levels of anti-CA Iand anti-CA II are thus quite elevated inpatients suffering from CP [107].
Seizures are one of the most common neuro-logical disorders. The triggering mechanisms bywhich seizures occur remain unclear, but arerelated to a rapid change in ionic composition,including an increase in intracellular potassiumconcentration and pH shifts within the brain [108].pH buffering of extra- and intra-cellular spaces ismainly carried out by the CO2/HCO3-buffer, theequilibration of the two species being assured bythe many CA isoforms present in the brain (e.g.,CA I, II, IV, VB, VII, XII and XIV) [108–110].Some CAIs, such as AZ and methazolamide,have been used as anticonvulsants in the treat-ment of epilepsy, with rather scarce success [108].
371www.futuremedicine.com
REVIEW – Supuran
372
Both these sulfonamides are used either in com-bination therapy with other antiepileptic medi-cations in both children and adults or inrefractory epilepsy [108–110]. AZ might be usefulin partial, myoclonic, absence and primary gen-eralized tonic–clonic seizures uncontrolled byother classical antiepileptic drugs [110]. However,such sulfonamides did not provide effectivelong-term therapy for epileptic patients due toreasons currently not well understood [108–110].
Zonisamide is a synthetic 1,2-benzisoxazole-3-methanesulfonamide with potent anticonvul-sant properties [111]. The sulfamoyl group onzonisamide was expected to suppress seizures ina similar way to AZ through inhibition of CA,but it was claimed that CA inhibition does notappear to be the primary mechanism of actionof this drug [111]. Zonisamide prevents repetitiveneuronal firing by blockade of voltage-sensitiveNa+ channels. It also reduces voltage-dependentT-type Ca2+ channels, facilitating dopaminergicand serotoninergic neurotransmission [111].However, it has recently been reported thatzonisamide is also quite an effective CAI againstmany of the physiologically relevant isoforms[22]. It is unknown at this point to what extentthe CA inhibitory properties of the drug have acontribution to its antiepileptic action.
Topiramate is a sulfamate fructopyranosederivative currently available for the treatment ofpartial-onset epilepsy [112]. As an antiepilepticdrug, it is known to be clinically effective againstsimple or complex partial seizures and also againstgeneralized tonic–clonic seizures [112]. Besides itsability to block the voltage-gated Na+ channel, topotentiate GABAergic transmission and to blockthe kainate/AMPA receptor, topiramate occupiesa particular place among the new anticonvulsantsdue to its ability to inhibit CA [113]. In thisrespect, topiramate-induced changes of GABA-ergic depolarizations were supposed to be basedon a decreased intracellular HCO3- concentra-tion, which may be caused by an inhibition ofneuronal CA [112,114]. It has been reported byour group that topiramate strongly inhibits sev-eral CA isoforms, among which are the cytosolicCA II and CA VII present in the brain [51,115].Moreover, its x-ray crystallographic structure incomplex with hCA II revealed a tight associa-tion, with a network of seven strong H bondsfixing the inhibitor within the active site, inaddition to Zn(II) coordination through theionized sulfamate moiety [51]. The inhibitoryeffect of topiramate on interstitial and intracel-lular CAs could modify extra- and intra-cellular
activity-dependent pH changes, as demonstratedfor other CAIs [116]. Such pH shifts might have adeep impact on neuronal excitability becausemany ion channels, gap junctions and neuro-transmitter receptors are highly sensitive tochange in pH [112]. Local administration of AZhas a similar effect to systemic administration oftopiramate or AZ, suggesting that the effect ofthese drugs on the initial alkalinization isthrough inhibition of central CA [117]. Bothdrugs decreased initial alkalinization, whichwould be consistent with an antiepileptic effect,and may actually contribute to their antiepilepticactions in vivo [117]. However, the change in pHregulation is not a fundamental anticonvulsantmechanism since carbamazepine and phenytoin,two antiepileptic drugs, have no effect on thealkalinization [117]. Thus, the effect of CA inhibi-tion on the antiepileptic action of topiramate isnot well understood.
CAIs were also shown to be effective in theprevention and treatment of mountain sicknessand high-altitude cerebral edema [118–120]. Theseconditions affect, to varying degrees, all travellersto high altitudes, being characterized by a com-bination of symptoms such as headache, insom-nia, anorexia, nausea, dizziness, vomiting,dyspnea, muscle weakness, oliguria, peripheraledema and retinal hemorrhage [118–120]. In moreserious cases, pulmonary or cerebral edema werealso observed [118–120]. The primary cause ofmountain sickness is related to reduced oxygencontent in the air at high altitudes, which leadsto hypoxemia and all the symptoms mentionedabove. AZ, alone or in combination with dexam-ethasone, is useful in markedly reducing thesesymptoms, due to the increased arterial oxygenconcentrations after red blood cell/brain enzymeinhibition by the sulfonamide drug [118–120]. It isnot clear whether methazolamide or other clini-cally used CAIs may have a better mode of actioncompared with AZ in preventing acute moun-tain sickness, since few comparative studies havebeen reported [120].
ConclusionCAs continue to be surprising enzymes, as manyexciting new discoveries are constantly emerging,even though these are quite ‘old’ enzymes, beingfirst discovered in 1933, and thoroughly investi-gated since then. In the last few years, a host ofinteresting such reports have been made, first of allregarding the catalytic/inhibition mechanism aswell as isolation/characterization of new isozymes,in addition to CAs of nonvertebrate origin.
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
future science groupfuture science group
The x-ray crystallographic structure adducts ofhCA II with the simplest sulfonamides (sulfamideand sulfamate) have been reported. These com-pounds are considered to be the mother of all sul-fonamides, since they incorporate in theirstructure the essential Zn-binding functionpresent in all potent CAIs currently known, with-out any other aromatic/heterocyclic scaffold gen-erally present in other inhibitors investigated indetail. The x-ray crystallographic structures ofmany hCA II and I adducts with sulfonamidesand sulfamates currently reported ultimatelyhelped in a better understanding of the molecularinteractions between the inhibitor and theenzyme, which may lead to a rational drug designof inhibitors with reduced side effects and selectiv-ity for the target isoform. Among these structures,there are also those with some widely used clinicalagents, some of which have originally beendesigned for other applications, such as the anti-epileptics topiramate and zonisamide, the antitu-mor sulfonamide indisulam, the antipsychoticsulpiride, the steroid sulfatase inhibitors COU-MATE and EMATE, the COX-2 inhibitorscelecoxib and valdecoxib and the artificial sweet-ener saccaharin. All these compounds show appre-ciable inhibition (in the low nanomolar range) ofsome physiologically relevant human CAs.
In the last few years, most of the catalyticallyactive isozymes have been investigated in detailfor their inhibition profile against the mostimportant classes of CAIs, the sulfonamides, sul-famates and sulfamides. This is highly importantin the search of isozyme-selective compoundsand for reducing side effects of the presentlyavailable drugs. Indeed, physiologically quite rel-evant isoforms, such as CA IV, VA, VB, VII, IX,XII, XIII and XIV, have been investigated for thefirst time in detail for their inhibition with manytypes of such compounds, and several importantdrug-design studies have also been reported inwhich compounds with selectivity for one orother such isozymes were obtained. However, todate, few compounds show a good selectivity forany CA isoform with clinical relevance, althoughimportant advances have been reported in thedesign of compounds with a good selectivityratio for CA VA over CA II, CA IX over CA II orCA XIII over CA II (CA II is the ubiquitous, cat-alytically very effective isoform, and this is thereason why many-times its inhibition is regardedas detrimental).
In targeting the tumor-associated isoformCA IX, important advances have been reportedin the design of fluorescence labels and of
membrane-impermeant compounds that inhibitonly the membrane-associated isoforms (e.g.,CA IX) and not cytosolic (e.g., CA I and II). Byusing fluorescent CAIs, a proof-of-concept studyshowing the role of CA IX in the tumor acidifica-tion processes was reported, and the fact that thisphenomenon may be reversed by inhibiting thecatalytic activity of the enzyme with CA IX-selec-tive and potent inhibitor. Furthermore, B-con-taining CA IX inhibitors have been reported,which may be useful in B neutron capture ther-apy. In another important study, hypoxia-activat-able CA IX prodrugs containing disulfide bondswere reported. Such bulky, dimeric sulfonamidesare very weak CA I, II and IX inhibitors, but byreduction in hypoxic conditions present intumors, they lead to thiols that act as lownanomolar inhibitors of these isozymes.
Various ophthalmologic and antiobesity appli-cations of the CAIs were also reported in the pat-ent and scientific literature, together with novelderivatives that act as anticonvulsants.
There are currently very few pharmacologicalapproaches for the treatment of obesity, and mostare unsatisfactory. Furthermore, this disease iswidespread both in the developed and developingworld, and the number of affected individuals isconstantly increasing. Thus, new and effectiveapproaches are needed for the development ofantiobesity agents possessing different mecha-nisms of action. A new approach for the treat-ment and prophylaxis of obesity may be based onthe inhibition of CAs, enzymes involved in severalsteps of de novo lipogenesis, both in the mito-chondria and the cytosol of cells. Topiramate andzonisamide, clinically used antiepileptic drugsalso showing strong CA inhibitory properties,possess a highly desired side effect in obesepatients – induction of weight loss. It has beenrecently proved by our groups that both topiram-ate and zonisamide act as very potent in vitroinhibitors of several CA isozymes (includingCA II, CA VA and CA VB), and that this mightexplain their antiobesity effects. A program ofdesigning such antiobesity sulfonamide CAIs alsocould lead to the detection of several interestinglead molecules. CAIs targeting isozymes involvedin lipogenesis may represent a new approach forthe treatment and prevention of obesity.
Several important findings relate to the fullstructural characterization of CAs belonging tothe β- and γ-families (characteristic of bacteria,plants and Archaea, respectively). Rather shock-ing was the finding that, in some β-CAs, there isno H2O molecule or OH- coordinated to the
373www.futuremedicine.com
REVIEW – Supuran
374
catalytically essential Zn(II) ion, making theseenzymes quite different to those belonging tothe α- and γ-CA families. Thus, the catalyticmechanism of β-CAs is not fully understood atthis time.
Many novel representatives of CAs belongingto the three families mentioned above were iso-lated and characterized in some other organismsless investigated up to now, such as bacteria (e.g.,Helicobacter pylori, Neisseria gonorrheae,Escherichia coli and Mycobacterium tuberculosis)fungi (Candida albicans and Cryptococcus neofor-mans) or in the protozoa causing malaria(P. falciparum). However, few inhibition studiesof these enzymes are currently available. Thesediscoveries may soon have important therapeuticconsequences in the treatment of infectionscaused by pathogenic agents, in cases wherepotent and selective inhibitors for the pathogenicover the host enzymes could be detected.
The data presented herein clearly show thatCAs and their inhibitors may play an essentialrole in the development of new therapeuticapproaches against a multitude of disorders, inaddition to the classical ones for which suchagents were and are still in use.
Future perspectiveAs CAs are widespread enzymes in most organismsall over the phylogenetic tree, and as they deal withsome of the very simple substrates (such as CO2and HCO3-), it is rather probable that the futurewill see the discovery of many new representativesof these catalysts in many different species. In fact,the recent reports of genomes of many bacterial(pathogenic) species revealed a high number ofCAs belonging to the α-, β-, γ- and/or δ-CA gene
families in most of them, although the non-mam-malian CAs are highly uninvestigated at thepresent time. Thus, in my opinion, there will bemajor breakthroughs in this field with the discov-ery of many new such enzymes and/or novel genefamilies encoding for CAs.
It is less probable that novel CAs will be discov-ered in mammalians/humans, since the entiregenome of such species has already been analyzedin detail, and 15 isozymes was detected in pri-mates, and 16 in nonprimates. However, thephysiological function of many of these isoformsis currently largely not understood, and we esti-mate that important progress will occur in thisfield, especially considering the fact that all theseisozymes have now been characterized, from thebiochemical point of view, and their inhibitionprofiles have also been investigated with manyclasses of organic and inorganic inhibitors. As aconsequence, it is possible that new CAIs will bedeveloped, some of them with selectivity for vari-ous isoforms. Indeed, the presently available drugsbelonging to this class indiscriminately inhibitmost isozymes. It is probable that the future willsee the development of isozyme-selective inhibi-tors for isozymes I, II, VA, VB, VII, IX, XII, XIIIand XIV, which will lead to drugs with less sideeffects. It is also probable that many new such tar-gets belonging to the bacterial/fungal/protozoanCAs will be validated and lead to novel types ofagents fighting diseases provoked by such patho-gens. The first results already obtained in this fieldare very promising.
AcknowledgementsResearch from the author’s laboratory was financed in part by anEU grant of the 6th framework programme (EUROXY project).
Executive summary
• Carbonic anhydrases (CAs) are widespread enzymes in bacteria, archaea and eukaryotes that catalyze a critically important physiologic reaction – hydration of CO2 to HCO3- and protons.
• These enzymes are inhibited by several classes of compounds, such as sulfonamides, sulfamates and sulfamides, among others.
• A number of such derivatives are clinically used inhibitors, such as acetazolamide, methazolamide, ethoxzolamide, dichlorophenamide, dorzolamide, brinzolamide, topiramate, zonisamide, sulpiride, celecoxib and valdecoxib. Several compounds are in clinical development, such as indisulam and COUMATE-667.
• CA inhibitors (CAIs) are used in therapy as antiglaucoma, diuretic, antiobesity and antitumor drugs/diagnostic tools. Some compounds are also used as anticonvulsants or for the treatment of other neurological disorders.
• Most presently available CAIs show undesired side effects due to indiscriminate inhibition of CA isoforms other than the target.
• Many new CAIs are being developed in the search of isozyme-selective compounds as potential drugs with less side effects.
• Bacterial, fungal and protozoan CAs present in many pathogens have recently started to be considered as potential targets for the development of inhibitors with therapeutic applications.
Therapy (2007) 4(3) future science groupfuture science group
Therapeutic applications of the carbonic anhydrase inhibitors – REVIEW
Bibliography1. Supuran CT, Scozzafava A, Conway J:
Carbonic Anhydrase: its Inhibitors and Acti