Embed Size (px)
Citation preview

Université de Liège
Faculté de Psychologie, Logopédie et des Sciences de l’éducation
MALORIE TOUCHÈQUE
En vue de l’obtention du titre de Docteur en Sciences Psychologiques et
de l’Education
Anne-Marie ETIENNE
Promoteur
Christina DUNCAN
Gilles DUPUIS
Fabienne LEMETAYER
Liesbet GOUBERT
Pierre MISSOTTEN
Jury de thèse
QUALITÉ DE VIE DES ENFANTS ATTEINTS DE
MUCOVISCIDOSE
Rôle des émotions et interactions triadiques ?
Thèse présentée par
Année académique 2015-2016


“The ultimate measure of a man is not where he stands in moments of
comfort and convenience, but where he stands at times of challenge and
controversy”
– Martin Luther King –


Remerciements
“ Les mots manquent aux émotions ”
– Victor Hugo / Le dernier jour d’un condamné –
Je souhaite remercier toutes les personnes qui ont contribué, de près ou de
loin, à l’élaboration de ce travail de recherche.
Je désire adresser mes premiers remerciements au Professeure Anne-Marie
Etienne, promotrice de ce travail de thèse, pour m’avoir offert la possibilité de
découvrir le monde passionnant de la recherche scientifique. Ses précieux
conseils, ses connaissances cliniques et scientifiques, sa disponibilité, ses
encouragements et sa bienveillance m’ont permis d’évoluer dans une ambiance
de travail agréable, et ainsi, d’avancer sereinement le long de ce parcours
doctoral.
C’est avec beaucoup de gratitude que je souhaite également remercier
Pierre Missotten et Fabienne Lemétayer, membres de mon comité
d’accompagnement. Merci Pierre pour tes conseils avisés et tes relectures
approfondies depuis les prémices du mémoire jusqu’à l’aboutissement de cette
thèse. Au cours de ces six années de suivi régulier, tu m’as aiguillée,
encouragée, mais aussi positivement déstabilisée, et je t’en suis grandement
reconnaissante. Fabienne, je vous remercie pour vos conseils judicieux tout au
long de ces quatre années ainsi que vos relectures et précieux encouragements
dans la dernière ligne droite. J’associe également à ces remerciements, le
professeur Gilles Dupuis. Bien que n’ayant pas fait partie du comité
d’accompagnement, nos échanges d’idées et votre aide précieuse en statistique
ont rythmé ces quatre années de thèse.
Chers membres du jury, je vous remercie chaleureusement pour l’intérêt
que vous avez porté à ce travail et le temps que vous avez consacré à sa lecture.
J’espère qu’il en ressortira un débat constructif.

REMERCIEMENTS
Christina, thank you for giving me the opportunity to join your lab for a
year and enjoy the academic life at WVU. This unique professional and personal
experience has made me the woman I am today. During this year, you were a
mentor and a mother to me and I am so grateful for having you in my life. I just
hope you enjoyed this experience as much as I did. I also would like to thank
Christina’s lab students: Margo, Janelle, Paul, Ellen, Katie for their patience in
teaching me English and their help in my research project. Thank you Courtney
for being such a wonderful undergraduate student during data collection and
thank you for editing the English part of this dissertation. Thank you to my
other Morgantown friends, Ron, Daniel, Nipat, Frankie, Cameron R., Rebecca,
Lauren, Cameron F. etc. for letting me be a part of your life. Finally, thank you
the Anderson’s family: Loren, Sarah, Solenne and Annika for sharing their home
with me. I miss you all.
I also would like to thank Nicole Silva. You were and still are like a sister to
me. To be in a country, surrounded by people who don’t speak the same
language and don’t share the culture was hard. But in the middle of this chaos,
I’ve found you, a smart, kind and funny woman. Thank you for making my stay
in Morgantown AWESOME! I love you.
J’adresse toute ma gratitude aux directeur(trice)s et instituteur(rice)s des
écoles primaires/secondaires, en Belgique et aux USA, qui ont apporté leur aide
pour le recrutement des familles d’enfants tout-venant. Un grand merci aux
équipes médicales des différents centres pour la mucoviscidose qui ont accepté
de collaborer à ce projet de recherche : le Centre Hospitalier Régional de la
Citadelle, le Centre Hospitalier Chrétien de l’Espérance, l’Hôpital Universitaire
des Enfants Reine Fabiola, l’UZ Brussel, le West Virgina University’s Mountain
State Cystic Fibrosis Center, et l’Antonio J. and Janet Palumbo Cystic Fibrosis
Center at Children’s Hospital of Pittsburgh. Et puis, un énorme merci aux
enfants et aux parents qui ont été assez généreux que pour accepter de
participer à cette recherche.

REMERCIEMENTS
Je remercie chaleureusement mes lectrices de l’ombre, Sylvie, Céline,
Justine et Courtney pour leur aide, ô combien précieuse, dans la chasse aux
fautes d’orthographe, de grammaire, de conjugaison et autres erreurs de
français (ou d’anglais).
Mes pensées vont également à mes chers et chères collègues, Isa, Cindy,
Muriel, Céline, Béné, Marie B., Julien, Aurélie, Jonathan, Megan, Marie G., Anne-
Lise, Trecy, Lise, Gaïd, Helen, Orianne, Emilie S., etc. Que l’on se connaisse
depuis quatre ans ou depuis quelques mois, vous avez égayé mon quotidien à
l’université et avez fait de ces quatre années une aventure humaine inoubliable.
Je garderai en mémoire les temps de midi, les pauses café pour certains ou
chocolat pour d’autres et les nombreux fous rires que l’on a partagés. Vous me
manquerez beaucoup. Un merci tout particulier à mes deux collègues de
bureau, Béné et Céline pour leur soutien sans faille, leur écoute attentive et
leurs mots réconfortants. On en a partagé des joies et des peines ! Quatre ans
plus tard, ce ne sont pas des collègues que je perds mais des amies que je gagne.
MERCI à mes deux potos, Miguel et Florent, pour les moments de pure
bonheur musical et les innombrables fous rires; à mes amis liégeois, Emilie S.,
Mary, Ken et Marie-Ange, pour les moments magiques autour d’un verre, d’un
film ou d’un bon repas et leur fidélité à toute épreuve; à la joyeuse clique du
badminton, Christine, Adeline, Cindy, Thibaut, Vincent et Arnaud, pour m’avoir
accueillie à bras ouverts dans votre bande et pour les instants de vie partagés
(soirées arrosées, nuits à l’appart, petits déjeuners les lendemains de veille,
etc). Pourvu que ça dure… Une attention particulière à Adeline et Arnaud, pour
l’aide précieuse qu’ils m’ont apportée lors de la finalisation de cette thèse
(fonction recherche grrr !!!). Ce n’était pas du gâteau !
Et merci à ma meilleure amie, Charlotte. Son soutien inconditionnel, sa
présence réconfortante dans les mauvaises épreuves de la vie, ses coups de
téléphone quotidiens (ou presque) via Viber, elle à Mont, moi à Morgantown
(6h de décalage horaire quand même !) et ses soupes au potiron du lundi soir

REMERCIEMENTS
ont donné un sens au mot amitié. Un GRAND merci ma poule. Sans oublié
Joshua ! Que de moments de folies depuis sa naissance ; enfin quelqu’un qui
apprécie mes talents de chanteuse et mon esprit enfantin ! Je vous aime.
Qu’aurait été cette thèse sans la présence réconfortante de mes deux
compagnons, Charlotte et Morgan ; sans leur contribution à la mise en page de
ce document, leur acharnement, journalier et nocturne, à me distraire et leur
douce fourrure qui a le pouvoir d’essuyer mes larmes dans les moments de
doute.
Enfin, mes plus tendres remerciements vont à ma famille. Merci à mes
parents, Léopold et Maryline, d’être toujours là pour moi, dans les bons comme
dans les mauvais moments, de me soutenir quoi qu’il arrive et de m’encourager
quel que soit mes choix. Votre amour inconditionnel est un moteur pour
l’avenir et m’encourage à croire en mes rêves. Merci à mes frères, Florian et
Logan, pour leur capacité à me rendre fière en un seul regard, leur complicité
fraternelle et leur humour légendaire. Sachez que le statut de grande sœur est
le plus beau cadeau qu’il m’a été donné de recevoir. Merci à vous quatre. Je vous
aime plus que tout.
Merci à tous,
Malorie



Table des
matières


Table des matières
Preface ( IN ENGLISH) .............................................................................................. - 25 -
PARTIE 1: CADRE THEORIQUE
Chapitre 1 – La mucoviscidose : la maladie et ses traitements ........... - 33 -
1. La mucoviscidose : une anomalie génétique .............................................. - 33 -
2. Incidence et pronostic ......................................................................................... - 34 -
3. Le diagnostic ........................................................................................................... - 35 -
3.1. Le dépistage néonatal ................................................................................ - 36 -
3.2. Le test de la sueur ........................................................................................ - 37 -
3.3. Le test génétique .......................................................................................... - 38 -
3.4. Le test du potentiel nasal.......................................................................... - 39 -
3.5. Diagnostic anténatal ................................................................................... - 39 -
4. Les symptômes ....................................................................................................... - 40 -
4.1. L’atteinte respiratoire ................................................................................ - 40 -
4.2. L’atteinte digestive ...................................................................................... - 41 -
4.3. Autres complications ................................................................................. - 42 -
5. Les traitements....................................................................................................... - 44 -
5.1. L’atteinte respiratoire ................................................................................ - 44 -
5.1.1. L’antibiothérapie ................................................................................ - 45 -
5.1.2. La kinésithérapie ................................................................................. - 47 -
5.2. L’atteinte digestive ...................................................................................... - 48 -
5.3. Les implications ............................................................................................ - 51 -
En résumé…………………………………………………………………………………………- 53 -

TABLE DES MATIÈRES
Chapitre 2 – Mesurer la qualité de vie chez l’enfant ................................. - 57 -
1. Définition de la QV ................................................................................................ - 57 -
1.1. Le caractère multidimensionnel de la QV .......................................... - 58 -
1.2. Le caractère subjectif de la QV ............................................................... - 60 -
2. Mesurer la QV chez l’enfant .............................................................................. - 61 -
2.1. Problèmes conceptuels relatifs à la notion de QV .......................... - 61 -
2.1.1. Confusion entre les notions d’état de santé, de statut fonctionnel
et de QV……………………………………………………………………………………..- 61 -
2.1.2. Notion de but ........................................................................................... - 63 -
2.2. Considérations méthodologiques relatives à la QV ....................... - 64 -
2.2.1. Auto- vs hétéro- évaluation ................................................................ - 64 -
2.2.2. La création d’un format et d’un design approprié à l’âge de
l’enfant…. ................................................................................................................... - 66 -
2.2.3. Les outils génériques vs spécifiques .............................................. - 69 -
3. Les instruments de mesure de la QV ............................................................. - 71 -
En résumé… ....................................................................................................................... - 76 -
Chapitre 3 – Modèles d’ajustements à la maladie en pédiatrie………- 81 -
1. Le modèle de l’autorégulation du comportement de maladie ............ - 81 -
2. Le modèle transactionnel du stress et du coping ..................................... - 85 -
3. Le modèle intégratif et multifactoriel ........................................................... - 89 -
En résumé…………………………………………………………………………………………- 92 -

TABLE DES MATIÈRES
Chapitre 4 – L’enfant et la maladie: perspective développementale- 97 -
1. L’approche cognitive de la conceptualisation de la maladie ............... - 98 -
1.1. La théorie piagétienne du développement cognitif de l’enfant - 98 -
1.2. Les stades de compréhension du concept de maladie selon Bibace
et Walsh (1980) ........................................................................................................ - 100 -
1.3. Stade de compréhension des causes de la maladie Selon Koopman
et al. (2004) ................................................................................................................ - 103 -
2. L’approche biologique de la conceptualisation de la maladie .......... - 105 -
2.1. Vers le développement d’une théorie naïve de la biologie ....... - 106 -
2.1.1. Distinction entre les vivants et les non-vivants ....................... - 106 -
2.1.2. Distinction entre le corps et l’esprit ............................................. - 107 -
2.1.3. Compréhension des causes des phénomènes biologiques - 108 -
2.2. Modèles biologiques et conceptualisation de la maladie .......... - 109 -
En résumé… ..................................................................................................................... - 112 -
Chapitre 5 – Le rôle des facteurs parentaux sur l’ajustement de l’enfant
malade .............................................................................................................................. - 117 -
1. Le modèle transactionnel du stress et du coping (TSC) de Thompson et
al. (1992) .......................................................................................................................... - 118 -
2. Inclusion des pères dans la recherche en pédiatrie .............................. - 122 -
Résumé… .......................................................................................................................... - 124 -
Chapitre 6 – Objectifs de recherche ................................................................. - 129 -
Chapter 6 – Research objectives (IN ENGLISH)……………………………..- 133 -

TABLE DES MATIÈRES
PARTIE 2: METHODOLOGIE
Chapitre 7 – Procédure de recherche des différentes études ........... - 141 -
1. En Belgique ............................................................................................................ - 141 -
1.1. Etude 1 : Validation d’un format tablette (iPad) de l’ISQV-E ... - 141 -
1.2. Etude 2 : QV des enfants atteints de mucoviscidose ................... - 142 -
1.2.1. Etude 2.a: recrutement des familles du groupe « muco » - 143 -
1.2.2. Etude 2.b: recrutement des familles du groupe contrôle . - 147 -
2. Aux États-Unis d’Amérique ............................................................................. - 147 -
2.1. Etude 3 : Validation d’une version anglaise de l’ISQV-E format
tablette .......................................................................................................................... - 148 -
2.2. Etude 4 : QV des enfants américains .................................................. - 150 -
2.2.1. Etude 4.a: Recrutement des familles du groupe « muco »- 150 -
2.2.2. Etude 4.b: Recrutement des familles du groupe contrôle - 152 -
PART 3: RESEARCH STUDIES
Chapter 8 – A comparison of a tablet version of the Quality of Life
Systemic Inventory for Children (QLSI-C) to the standard paper
version .............................................................................................................................. - 158 -
1. Introduction........................................................................................................... - 159 -
2. Method ..................................................................................................................... - 161 -
2.1. Participants and study design .............................................................. - 161 -
2.2. Measures ....................................................................................................... - 162 -
2.3. Statistical analysis ..................................................................................... - 165 -
3. Results ...................................................................................................................... - 166 -
3.1. Score equivalence ...................................................................................... - 166 -
3.2. Internal consistency reliability ............................................................ - 166 -
3.3. Test-retest reliability ............................................................................... - 166 -
4. Discussion............................................................................................................... - 167 -

TABLE DES MATIÈRES
Chapter 9 – Anxiety, depression and quality of life in school-aged
children with cystic fibrosis: A cross-cultural study .............................. - 174 -
1. Introduction........................................................................................................... - 175 -
2. Method ..................................................................................................................... - 177 -
2.1. Study design and subjects ...................................................................... - 177 -
2.2. Measures ....................................................................................................... - 178 -
2.3. Statistical analyses .................................................................................... - 179 -
3. Results ...................................................................................................................... - 180 -
3.1. Descriptive statistics ................................................................................ - 180 -
3.2. Disease group comparisons for psychosocial measures ........... - 180 -
3.3. Association between anxiety, depressive symptoms and QOL
........................................................................................................................... - 181 -
4. Discussion............................................................................................................... - 182 -
Acknowledgements ...................................................................................................... - 183 -

TABLE DES MATIÈRES
Chapter 10 – Applying the Common Sense Model of Self-Regulation to
pediatric cystic fibrosis: Identifying psychosocial factors associated
with quality of life ...................................................................................................... - 186 -
1. Introduction........................................................................................................... - 187 -
2. Method ..................................................................................................................... - 190 -
2.1. Study design and subjects ...................................................................... - 190 -
2.2. Measures ....................................................................................................... - 191 -
2.3. Statistical analyses .................................................................................... - 194 -
3. Results ...................................................................................................................... - 195 -
3.1. Descriptive statistics ................................................................................ - 195 -
3.2. Bivariate correlations .............................................................................. - 195 -
3.3. Mediation analysis..................................................................................... - 195 -
3.3.1. Mediation of coping strategies between cognitive illness
representation and QOL ................................................................................... - 195 -
3.3.2. Mediation of coping strategies between emotional illness
representation and QOL ................................................................................... - 196 -
3.3.3. Mediation of psychological disturbance between emotional
illness representation and QOL ..................................................................... - 196 -
3.3.4. Mediation of psychological disturbance between coping
strategies and QOL .............................................................................................. - 199 -
4. Discussion............................................................................................................... - 202 -
Acknowledgements ...................................................................................................... - 206 -

TABLE DES MATIÈRES
Chapter 11 – Parenting stress, parental illness perception and coping
strategies associated with quality of life in children with cystic
fibrosis: The mediating role of parental adjustment ............................. - 210 -
1. Introduction........................................................................................................... - 211 -
2. Method ..................................................................................................................... - 214 -
2.1. Study design and subjects ...................................................................... - 214 -
2.2. Measures ....................................................................................................... - 217 -
2.3. Statistical analyses .................................................................................... - 219 -
3. Results ...................................................................................................................... - 219 -
3.1. Demographics ............................................................................................. - 219 -
3.2. Descriptive statistics ................................................................................ - 220 -
3.3. Bivariate correlations .............................................................................. - 220 -
3.4. Mediation analyses.................................................................................... - 221 -
3.4.1. Mediation of parental QOL between parenting stress and QOL
in children with CF .............................................................................................. - 222 -
3.4.2. Mediation of parental QOL between parental illness
perception and QOL in children with CF ................................................... - 223 -
3.4.3. Mediation of parental QOL between parental coping strategies
and QOL in children with CF ........................................................................... - 223 -
4. Discussion............................................................................................................... - 224 -
Acknowledgements ...................................................................................................... - 227 -

TABLE DES MATIÈRES
DISCUSSION (IN ENGLISH) ........................................................................................ - 231 -
1. Theory summary ................................................................................................. - 231 -
2. Results summary ................................................................................................. - 234 -
3. Related topics........................................................................................................ - 237 -
3.1. Using e-Health assessment in pediatric ........................................... - 237 -
3.2. Evidence for our definition and measurement of the QOL ....... - 240 -
3.3. Resilience in chronically ill children and their family ................ - 243 -
3.4. Emotions, cognitions and coping in children with chronic disease
……………………………………………………………………………………………………- 245 -
3.5. Role of mothers and fathers in pediatric chronic disease ........ - 246 -
4. Strengths, limitations & futures perspectives ......................................... - 247 -
4.1. Strengths ....................................................................................................... - 247 -
4.2. Limitations.................................................................................................... - 248 -
4.3. Future perspectives .................................................................................. - 249 -
5. Implications for practice .................................................................................. - 251 -
CONCLUSION ................................................................................................................. - 257 -
Bibliographie ................................................................................................................ - 263 -
ANNEXES
Annexe 1 : Le modèle des systèmes de contrôle (Dupuis et al., 1989)
………………………………………………………………………………………………............- 293 -
Annexe 2 – Validation of the French version of the Parenting Stress
Index – Short Form (Fourth Edition) ............................................................... - 298 -



Preface


- 25 -
Preface
Cystic Fibrosis (CF) is the most common life-shortening recessively
inherited disease among Caucasian population, currently affecting about
70,000 people worldwide (Cystic Fibrosis Foundation, 2013). Each year,
about one in 2,850 babies born with this medical condition in Belgium
(Farrell, 2008), representing 5% of live births1. Advances in medical
research have led to improved treatment and subsequently, increased long-
term survival in CF; patients’ life expectancy today being in the early 40s
(Royce & Carl, 2011). However, the complex, time-intensive daily treatment
regimens still present considerable psychosocial challenges (Besier &
Goldbeck, 2011).
Despite well-established literature on psychosocial health in adolescent
and adult patients with CF, research studies on adjustment to CF in
childhood are limited. To our knowledge, thirteen studies have been
conducted among children (< 12 years old) with CF. Eleven of these
researches have investigated quality of life2 (QOL) and psychological
disturbance3 (i.e. anxiety and depressive symptoms); variables such as
coping strategies and cognitive processes (e.g. illness representations) was
not examined. Of these eleven studies, five highlighted relevant findings for
this research project. Main results are the following: (a) children with CF
reported a poorer QOL than healthy peers (Kianifar et al., 2013; Thomas, et
al., 2006); (b) children with CF demonstrated higher rates of anxiety than
the background population (Bregnballe, Thastum, & Schiotz, 2007);
1 Based on birth data in Belgium (Office de la Naissance et de l'Enfance, 2012). 2 Driscoll, Schatschneider, McGinnity, & Modi, 2012; Groeneveld et al., 2012;
Havermans, Vreys, Proesmans, & De Boeck, 2006; Hegarty, MacDonald, Watter, &
Wilson, 2009; Kianifar et al., 2013; Thomas, Mitchell, O’Rourke and Wainwright,
2006; Tluczek et al. 2013; Ziaian et al., 2006. 3 Bennett et al., 2008 ; Bregnballe, Thastum, & Schiotz, 2007 ; Driscoll et al., 2012 ; Kostakou et al., 2014.

PREFACE
- 26 -
however they did not differ regarding their rates of depressive symptoms
(Bregnballe, et al., 2007) and emotional/behavioral functioning (Kostakou
et al., 2014); (c) increased anxiety in children with CF was associated with
lower QOL (Driscoll, Schatschneider, McGinnity and Modi, 2012). Finally,
the two remaining studies have examined the relation between parental
factors and adjustment in school-aged children with CF (Thompson,
Gustafson, Hamlett, & Spock, 1992; Thompson, Gustafson, George, & Spock,
1994); they highlighted the role of maternal adjustment in the adjustment
of children with CF. Therefore, this research project aims to fill a gap in the
pediatric CF literature by expanding our understanding of individual and
family risk factors associated with a poor QOL in school-aged children with
CF (8 -12 years old). Thus, this work is divided into four sections: Theory,
Methodology, Research studies and Discussion.
The first section (Theory) splits into six chapters providing the
theoretical background of this dissertation as well as objectives and
hypothesis. Chapter one introduces the medical aspects of CF. Chapter two
aims to define the concept of QOL and discuss conceptual and
methodological challenges related to its measurement. Chapter three
presents theoretical frameworks available in health psychology when
studying adjustment to illness. Chapter four offers a developmental
perspective by exposing the conceptualization of illness in childhood.
Chapter five describes a conceptual framework for understanding the role
of parental factors in the child adjustment to chronic disease and discusses
the inclusion of fathers in pediatric research. Chapter six exposes the four
sub-objectives of this research project.
The second section (Methodology) consists of one chapter, the chapter
seven, that presents the research procedures for all studies conducted in
the context of this dissertation.
The third section (Research studies) is divided into four chapters that
show findings from this research project. Chapter eight presents the

PREFACE
- 27 -
validation a new electronic format (tablet) of the Quality of Life Systemic
Inventory for Children (QLSI-C©). Chapter nine examines emotional well-
being and QOL in school-aged children with CF. Chapter ten investigates
psychosocial factors associated with QOL in pediatric CF using the
Common-Sense Model of Self-Regulation (Leventhal, Meyer, & Nerenz,
1980). Chapter eleven examines whether parental QOL acts as a mediator of
the relation between parenting variables and QOL in children with CF using
the Transactional Stress and Coping model (Thompson, Gustafson, Hamlett,
& Spock, 1992).
Finally, the fourth section (Discussion) summarizes the theory and the
main results of research studies and discusses questions raised by findings
from these studies as well as the strengths, limitations, future perspectives
and clinical implications of this research project.


PARTIE 1
Cadre théorique
Chapitre 1
La mucoviscidose : la maladie et ses traitements
Chapitre 2
Mesurer la qualité de vie chez l’enfant
Chapitre 3
Modèles d’ajustement à la maladie en pédiatrie
Chapitre 4
L’enfant et la maladie : perspective développementale
Chapitre 5
Le rôle des facteurs parentaux sur l’ajustement de l’enfant malade
Chapitre 6
Objectifs de recherche


Chapitre 1
La mucoviscidose :
La maladie et ses
traitements


- 33 -
Chapitre 1 La mucoviscidose : La maladie et ses traitements
Afin de mieux saisir l’importance de l’impact de la mucoviscidose et de
ses traitements sur la vie quotidienne de l’enfant, il est essentiel
d’appréhender le caractère médical de cette maladie. Ainsi, ce chapitre sera
consacré à la présentation de cette pathologie et s’articulera autour de
différents éléments: l’anomalie génétique, l’incidence et le pronostic, le
diagnostic, les symptômes et, enfin, les traitements. Deux ouvrages ont
principalement été pris en exemple dans la rédaction de ce chapitre, à
savoir celui de Lebecque et Baran (2002) et celui d’Orenstein, Spahr, et
Weiner (2012).
1. La mucoviscidose : une anomalie génétique
La fibrose kystique, ou mucoviscidose, est une maladie héréditaire
causée par une anomalie génétique présente sur le chromosome 7. Ce gène
défectueux provoque l’absence ou le mauvais fonctionnement d’une
protéine (protéine CFTR) présente au niveau de la membrane de
nombreuses cellules, perturbant le transport du sel et de l’eau de part et
d’autre de la membrane. Ce dysfonctionnement affecte principalement le
système respiratoire et digestif via la formation d’un mucus épais qui
obstrue les petits tubes et canaux. La mucoviscidose est la maladie
génétique la plus fréquente dans la population caucasienne (Dahan &
Verellen, 2002; Weiner, Frizzell, & Orenstein, 2012). Bien qu’il s’agisse
d’une maladie héréditaire, les parents d’un enfant atteint de mucoviscidose
ne sont pas atteints par cette maladie mais porteurs sains d’un gène
déficient (présence d’un gène CFTR sur un des deux chromosomes 7). C’est
la présence du gène défectueux sur les deux chromosomes 7 qui détermine
si l’enfant est atteint de mucoviscidose. Ainsi, pour qu’un enfant soit atteint

PARTIE THÉORIQUE
- 34 -
de mucoviscidose, il faut que ses deux parents soient porteurs du gène
déficient et que chaque parent lui transmette ce gène. Concrètement,
lorsque les deux parents sont porteurs sains d’une mutation du gène
défectueux, le risque d’avoir un enfant malade est, pour chaque grossesse,
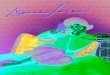
de 1 sur 4 (voir Figure 1).
Figure 1 – Mode de transmission autosomique récessif de la mucoviscidose
(Centre Muco de Liège, 2009b)
2. Incidence et pronostic
En Belgique, la mucoviscidose affecte un nouveau-né sur 2500 et
environ 1 personne sur 25 (4%) est porteuse « saine » d’une anomalie du
gène CFTR (cf. section 1) (Dahan & Verellen, 2002). Malgré les avancées
médicales en matière de traitement, la mucoviscidose est toujours une
maladie incurable ; elle entraîne le décès le plus souvent d’adultes mais
aussi de jeunes enfants ou d’adolescents (90% des décès dus à l’atteinte
pulmonaire) (Lebecque, 2002). Depuis la découverte du gène responsable
de la maladie (CFTR) en 1989, d’énormes progrès scientifiques ont été

CHAPITRE 1 – LA MUCOVISCIDOSE
- 35 -
réalisés. Ainsi, les patients atteints de mucoviscidose à l’heure actuelle
peuvent espérer être quadragénaire, alors qu’il y a environ 50 ans, cette
maladie était fatale dès l’enfance. Voici quelques chiffres pouvant en
attester : en 1940, l’espérance de vie était inférieure à 1 an (Cystic Fibrosis
Foundation, 2013), elle était de 10 ans en 1960 (Lebecque, 2002), de 29.4
ans en 1992, de 31.3 ans en 2002 et de 41.1 ans en 2012 (Cystic Fibrosis
Foundation, 2013). En Belgique, plus de la moitié (54.7%) des patients
atteints de mucoviscidose à l’heure actuelle ont atteint l’âge adulte (>
18ans) (Belgian Cystic Fibrosis Registry, 2014).
3. Le diagnostic
Les critères de diagnostic de la mucoviscidose ont été redéfinis pour la
dernière fois en 1998 lors d’une réunion de consensus (Rosenstein &
Cutting, 1998) et sont présentés Tableau 1. Puisqu’un diagnostic précoce
débouche sur une amélioration du pronostic, l’établissement du diagnostic
constitue une phase très importante pour la santé du patient atteint de
mucoviscidose. Dans la majorité des cas, le diagnostic posé avant l’âge d’un
an.
Tableau 1 – Critères de diagnostic de la mucoviscidose d’après le consensus
établi par Rosenstein et Cutting (1998) (d’après Leal & Lebecque, 2002)
1. La présence de symptômes évocateurs de la maladie (voir Tableau 2)
OU la présence de mucoviscidose dans la fratrie
OU un dépistage néonatal positif (voir 2.1)
+
2. Au moins deux tests de la sueur positifs (voir 2.2)
OU l’identification de deux mutations de gène CFTR à l’aide d’analyses
génétiques (voir 2.3)
OU la présence d’une anomalie de la différence de potentiel au niveau
nasal (voir 2.4)

PARTIE THÉORIQUE
- 36 -
3.1. Le dépistage néonatal
Une analyse de sang, qui consiste à prélever un petit échantillon de sang
dans le talon (ou sur le dos de la main) du bébé, est effectuée chez tous les
nouveau-nés avant leur sortie de la maternité afin de détecter certaines
maladies graves (test de Guthrie). Cependant, bien que le dépistage de la
mucoviscidose soit systématique dans certains pays (ex. France, Etats-Unis,
Espagne, Italie, Pologne, etc.), il ne l’est pas en Belgique. Il appartient à
chaque hôpital belge de demander à inclure le dépistage de la
mucoviscidose dans le test de Guthrie (Frédéric Pierart1, communication
personnelle, 23 septembre 2015). Lorsqu’il est effectué, le dépistage
néonatal de la mucoviscidose permet la détection des concentrations
élevées d’une enzyme pancréatique, appelée trypsine immuno-réactive
(TIR), qui pourrait indiquer la présence de la maladie. Cependant, cet
examen à lui seul ne permet pas de poser le diagnostic de mucoviscidose en
raison de sa faible spécificité et de son manque de sensibilité. A peine un
nouveau-né sur 10 dont le dosage est anormal à la naissance sera atteint de
mucoviscidose et environ 10% des nouveau-nés ne seront pas dépistés par
cette analyse de sang. Ainsi, des analyses complémentaires doivent être
réalisées afin d’établir le diagnostic (Centre Muco de Liège, 2009a; Leal &
Lebecque, 2002).
1 Le Dr. Pierart est le pédiatre responsable du centre Muco de Liège sur le site du Centre Hospitalier Chrétien de l’Espérance.

CHAPITRE 1 – LA MUCOVISCIDOSE
- 37 -
Tableau 2 – Symptomatologie compatible avec un diagnostic de
mucoviscidose (Rosenstein & Cutting, 1998)
1. Atteinte respiratoire chronique :
a. Infection respiratoire persistante par des germes évocateurs de
mucoviscidose : Staphylococcus aureus, Haemophilus influenzae,
Pseudomonas aeruginosa, Burkholderia cepacia.
b. Une toux chronique et expectorations abondantes.
c. Anomalies radiologiques persistantes au niveau du thorax
(bronchectasies, infiltrats, atélectasies, hyperinflation, etc.).
d. Une obstruction chronique des voies aériennes (respiration
sifflante, rétention anormale de l’air dans les poumons).
e. Une polypose nasale, la documentation (RX ou CT) d’anomalies
persistantes des sinus.
f. Un hippocratisme digital (malformation du doigt et des ongles).
2. Atteinte digestive :
a. Intestinale : occlusion intestinale du nourrisson ou équivalent
(iléus méconial), prolapsus rectal.
b. Pancréatique : insuffisance pancréatique exocrine, épisodes
récidivants de pancréatite.
c. Hépatique : hépatite chronique (cirrhose biliaire focale, cirrhose
multilobulaire, etc.).
d. Nutritionnelle : retard de croissance, œdème avec
hypoprotéinémie, manifestations traduisant une carence en
vitamines liposolubles (ADEK).
3. Symptômes traduisant une perte d’électrolytes : coup de chaleur
avec déshydratation hyponatrémique, hypokaliémique et
hypochlorémique, alcalose métabolique chronique.
4. Stérilité masculine par absence congénitale des canaux déférents.
3.2. Le test de la sueur
Le test de la sueur est l’élément central du diagnostic de mucoviscidose.
Il est réalisé pour confirmer ce dernier après avoir observé la présence de
symptômes évocateurs de la pathologie ou en cas de mucoviscidose dans la
fratrie ou d’un dépistage néonatal positif. Il est indolore, rapide (environ 1
heure) et donne des résultats dans un court laps de temps (< 24 heures). Le
principe de ce test consiste à recueillir la sueur du bras ou de la jambe du

PARTIE THÉORIQUE
- 38 -
jeune enfant et d’analyser sa teneur en chlorure de sodium (ex. 3 à 5 fois
plus salée que dans la population générale) (Leal & Lebecque, 2002; Spahr,
Orenstein, & Weiner, 2012b). Le test est dit positif lorsque l’on observe des
taux élevés de chlorure dans la sueur (> 60 mmol/l). La majorité des
patients atteints de mucoviscidose ont des valeurs comprises entre 60 et
110 mmol/l. Un test est dit négatif lorsque l’on observe un taux de chlorure
égal ou inférieur à 40 mmol/l. En ce qui concerne les nouveau-nés de moins
de 6 mois, le taux de chlorure doit être interprété différemment. Ainsi, chez
ces nourrissons, une concentration de chlorure inférieure à 30 mmol/l est
considérée comme normale. Par contre, lorsque la valeur est supérieure à
30 mmol/l, il est recommandé de réaliser des tests supplémentaires (ex.
répéter le test de la sueur ou réaliser un test génétique) (Spahr et al.,
2012b).
3.3. Le test génétique
Le test génétique consiste en une recherche des deux mutations du gène
CFTR afin de déterminer de quelle manière ces mutations affectent la
production et le fonctionnement de la protéine CFTR ou du canal chlore.
Actuellement, près de deux milliers de mutations du gène CFTR sont
connues. Les manifestations et le degré de sévérité de la maladie dépendent
des mutations du gène CFTR dont le patient est porteur. L’analyse génétique
ne permet d’identifier que les mutations les plus fréquentes du gène CFTR
(une vingtaine en Belgique). Cependant, une mutation rare échappera à
l’analyse génétique. La mutation la plus fréquente à l’échelle mondiale est la
mutation Delta-F508 (DF508). À l’issue du test génétique, les deux
mutations auront pu être reconnues chez environ 73% des patients (dont
50% de patients possédant les deux mutations DF508/DF508), une seule
mutation aura été identifiée chez environ 25% des patients et aucune
mutation n’aura été découverte chez 2% des patients, c’est-à-dire que 2%

CHAPITRE 1 – LA MUCOVISCIDOSE
- 39 -
des patients sont porteurs de mutations rares qui échappent au test
génétique et dont les manifestations cliniques sont inconnues. L’analyse
génétique étant coûteuse et longue (jusqu’à plusieurs semaines), elle est
pratiquée soit lorsque le test de la sueur s’est révélé positif soit pour
confirmer le diagnostic de mucoviscidose lorsque le test de la sueur a
démontré des résultats mitigés. (Dahan & Verellen, 2002; Leal & Lebecque,
2002; Spahr et al., 2012b).
3.4. Le test du potentiel nasal
Dans certaines situations ambiguës (ex. test à la sueur mitigé ou
analyses génétiques non concluantes), la mesure de la charge électrique (ou
différence de potentiel) au niveau nasal est utilisée afin de confirmer le
diagnostic. Les patients atteints de mucoviscidose ont une large charge
électrique contrairement aux personnes saines qui révèlent des valeurs
beaucoup plus basses. Ce test est tout aussi efficace que le test à la sueur
pour poser un diagnostic mais il est techniquement très compliqué, requiert
un opérateur expérimenté et l’interprétation des résultats peut être délicate
en raison d’interférences potentielles (inflammation de la muqueuse nasale
ou médicaments). De plus, seuls certains centres spécialisés en
mucoviscidose sont équipés pour réaliser ce test (Leal & Lebecque, 2002;
Spahr et al., 2012b).
3.5. Diagnostic anténatal
Bien que l’outil diagnostic essentiel de la mucoviscidose soit presque
toujours le test de la sueur, il existe une exception très importante où
l’étude génétique permettra à elle seule d’établir le diagnostic ; il s’agit du
diagnostic anténatal. Tous les parents d’un enfant atteint de mucoviscidose
savent qu’à chaque grossesse, il existe un risque sur quatre d’avoir un
enfant malade. Cependant, en cas de nouvelle grossesse, il est possible pour

PARTIE THÉORIQUE
- 40 -
les parents ayant déjà un enfant atteint de mucoviscidose de savoir, avant
trois mois de gestation, si l’enfant à naître sera ou non atteint de l’affection
grâce à l’étude génétique. En cas de diagnostic positif, il sera donné la
possibilité aux parents d’interrompre ou non la grossesse (Dahan &
Verellen, 2002).
4. Les symptômes
4.1. L’atteinte respiratoire
L’appareil respiratoire est le système le plus affecté chez les patients
atteints de mucoviscidose (cf. Tableau 2). L’atteinte pulmonaire est
progressive ; à la naissance, les poumons d’un enfant atteint de
mucoviscidose semblent normaux et c’est au fur et à mesure du temps,
variable d’un enfant à l’autre, qu’ils évoluent vers une destruction
progressive. Ces problèmes pulmonaires résultent de la perturbation du
transport du sel et du liquide au travers de la membrane cellulaire des voies
aériennes qui conduit à la formation d’un mucus sec et épais.
L’accumulation de ce mucus épais, difficile à évacuer, dans les petits tubes
et canaux des voies respiratoires (ex. bronchioles, bronches) provoque une
obstruction progressive et participe à la création d’un milieu favorable à la
prolifération des bactéries ainsi qu’aux infections et inflammations
multiples. Bien que les voies supérieures de l’appareil respiratoire soient
touchées (inflammation des sinus, polype nasal), ce sont les voies
inférieures du système respiratoire, à savoir les poumons, qui sont les
déterminants majeurs de la santé et de l’espérance de vie de la majorité des
patients atteints de mucoviscidose. En effet, l’atteinte pulmonaire est
responsable de plus de 95% des symptômes et complications liés à la
maladie et du décès dans plus de 95% des cas. La sévérité de l’atteinte
pulmonaire se mesure, entre autres, par le volume expiratoire maximal en 1

CHAPITRE 1 – LA MUCOVISCIDOSE
- 41 -
seconde (Forced Expiratory Volume, FEV1) qui correspond au volume d’air
expiré pendant la première seconde (Weiner & Orenstein, 2012).
4.2. L’atteinte digestive
Les organes du système gastro-intestinal (pancréas, intestins, vésicule
biliaire, foie et œsophage) sont également touchés chez les patients atteints
de mucoviscidose (cf. Tableau 3). La majorité des symptômes de l’atteinte
digestive étant liés à l’insuffisance pancréatique exocrine2 (85-90% des
cas), seule cette condition médicale sera présentée dans cette section.
Normalement, la fonction exocrine du pancréas aide à l’absorption et la
digestion des aliments via la production d’enzymes pancréatiques. Le
pancréas exocrine produit également un liquide riche en bicarbonate qui
aide à neutraliser le reflux gastrique. Chez les patients atteints de
mucoviscidose, le suc pancréatique, anormalement épais et acide, entraîne
(a) une obstruction des canaux pancréatiques empêchant le passage d’une
quantité suffisante d’enzymes dans l’intestin et (b) des lésions des glandes
qui produisent les enzymes digestives. Ce déficit dans la production
d’enzymes pancréatiques conduit à une malabsorption de certains types
d’aliments (ex. graisses et protéines) et des vitamines liposolubles3 A-D-E-K.
A la naissance, 50% des nouveau-nés atteints de mucoviscidose sont en
insuffisance pancréatique exocrine, 79% des nourrissons le deviennent
dans les six premiers mois de vie et 90% des enfants le sont à l’âge de 9 ans
(Lindblad et al., 2012).
2 En plus de la fonction exocrine, le pancréas assure une fonction endocrine qui régule le taux de sucre dans le sang via la production d’insuline. L’atteinte de la fonction endocrine conduit à du diabète chez les patients. Contrairement à la fonction exocrine, l’atteinte de la fonction endocrine apparaît plus tard. Le diabète associé à la mucoviscidose est rare en-dessous de l’âge de 10 ans. Son incidence est de 26% entre 10 et 20 ans, elle augmente encore de 10 à 20 % entre 20 et 30 ans et continue d’augmenter de 10 à 20% chaque décennie (Lindblad, Weiner, & Orenstein, 2012). 3 Liposoluble = soluble dans les graisses

PARTIE THÉORIQUE
- 42 -
Plusieurs symptômes résultent de l’insuffisance pancréatique exocrine
(Bauraind & Lebecque, 2002; Fulton, Yann, Weiner, & Orenstein, 2012) :
Un inconfort intestinal : Des gaz intestinaux, des ballonnements et
des crampes d’estomac.
Des anomalies des selles : elles sont fréquentes, diarrhéiques,
grasses, parfois huileuses, malodorantes et anormalement
volumineuses suite à la malabsorption des graisses.
Des signes de malnutrition : ils se manifestent par des problèmes de
croissance et un faible poids. L’indice de masse corporelle (IMC),
calculé sur base de la taille et du poids du patient, est un indice
important de la sévérité de l’atteinte digestive.
Tableau 3 – Symptomatologie de l’atteinte digestive dans la mucoviscidose
(Lindblad et al., 2012)
Organes Condition médicale Incidence (%)
Pancréas Insuffisance pancréatique 85-90
Pancréatite 1
Diabète 204
Foie et vésicule biliaire Cirrhose biliaire 1-4
Lithiase biliaire 10
Œsophage et estomac Reflux gastro-œsophagien 10-20
Ulcères 1-10
Intestins Iléus méconial 10
Péritonite méconiale 1
Équivalent d’Iléus méconial 10-30
Prolapsus rectal 10-20
Invagination intestinale 1
4.3. Autres complications
Outre les symptômes respiratoires et digestifs, d’autres complications
apparaissent chez les patients atteints de mucoviscidose :
4 Cystic Fibrosis Foundation (2013)

CHAPITRE 1 – LA MUCOVISCIDOSE
- 43 -
Maladie des os (incidence : 14.8%5) : une faible densité minérale
osseuse peut être observée chez les patients atteints de mucoviscidose
qui se traduit par une ostéopénie et, dans son stade plus avancé, une
ostéoporose, augmentant ainsi le risque de fracture. Ces problèmes
sont moins fréquents chez les enfants que chez les adolescents et les
adultes atteints de mucoviscidose. Ces problèmes de minéralisation
osseuse sont principalement dus à la malabsorption des vitamines
liposolubles (notamment la vitamine D), la malnutrition, l’inactivité
physique, les infections chroniques, la prise d’anti-inflammatoires (ex.
glucocorticoïdes). Un retard de puberté, fréquent chez les enfants
atteints de mucoviscidose, associé à des hormones sexuelles
(progestérone, œstrogène, testostérone) en faible quantité, sont
également responsables d’une faible densité minérale osseuse
(Weiner & Orenstein, 2012).
Problèmes aux articulations (incidence : 2.9%6) : les patients
atteints de mucoviscidose peuvent également présenter, bien que peu
communes, des manifestations rhumatologiques telles que l’ostéo-
arthropathie hypertrophiante (plus fréquente chez les patients avec
une atteinte sévère des poumons) ou l’arthrite (Weiner & Orenstein,
2012).
Infertilité masculine (incidence : 95-98%7) : les garçons et les
hommes atteints de mucoviscidose présentent une malformation
congénitale des canaux déférents, ceux-ci étant formés de manière
incomplète ou étant complètement obstrués, qui rend impossible le
passage des spermatozoïdes (= stérilité). Les femmes atteintes de
mucoviscidose, quant à elles, présentent une fertilité normale bien que
légèrement diminuée ; il est plus difficile pour une femme atteinte de
5 Cystic Fibrosis Foundation (2013) 6 Cystic Fibrosis Foundation (2013) 7 Devreker, Englert, and Steinfeld (2002)

PARTIE THÉORIQUE
- 44 -
mucoviscidose d’être enceinte que pour une femme de la population
générale en raison du mucus épais qui tapisse le col de l’utérus dont la
perméabilité varie en fonction du cycle menstruel (Devreker et al.,
2002; Weiner & Orenstein, 2012).
Dépression: le fardeau et les exigences de traitement liés à la
mucoviscidose peuvent entrainer une dépression chez 12% des
patients, et ce à tout âge. Lorsque l’on considère seulement la
population d’adultes atteints de mucoviscidose, l’incidence de la
dépression s’élève à 22.2% (Cystic Fibrosis Foundation, 2013).
5. Les traitements
5.1. L’atteinte respiratoire
L’objectif majeur du traitement lié à l’atteinte pulmonaire est de
soulager l’obstruction des poumons via l’évacuation du mucus et de
combattre les infections et les inflammations (Weiner & Orenstein, 2012).
Le tableau 4 reprend les principaux traitements disponibles associés aux
problèmes des voies respiratoires de la mucoviscidose. Seules
l’antibiothérapie et la kinésithérapie, piliers du traitement symptomatique
de l’atteinte pulmonaire, seront approfondies dans ce chapitre.

CHAPITRE 1 – LA MUCOVISCIDOSE
- 45 -
Tableau 4 – Principaux éléments dans le traitement de l’atteinte
respiratoire (Lebecque & Baran, 2002b)
1. Antibiothérapie – cf. 3.2.1
2. Kinésithérapie – cf. 3.2.2
3. Vaccinations – vaccin contre la grippe ; cette infection virale est
responsable d’une détérioration considérable, parfois irréversible, chez
les patients atteints de mucoviscidose
4. Fluidifiants – Ils aident à fluidifier le mucus afin de prévenir et
combattre l’obstruction des bronches et des poumons
5. Bronchodilatateurs – Ils dilatent les bronches et les bronchioles pour
combattre les complications dues à l’encombrement des voies
respiratoires
6. Anti-inflammatoires – traitement complémentaire ; ils aident à
combattre l’inflammation des voies respiratoires mais leur efficacité
reste à prouver et son utilisation en routine à long terme n’est
actuellement pas recommandée.
7. Oxygénothérapie – L’administration prolongée d’oxygène est proposée
aux patients qui présentent une hypoxémie importante au réveil, à
l’effort ou durant le sommeil.
8. Transplantation pulmonaire – en cas d’insuffisance respiratoire en
phase terminale
5.1.1. L’antibiothérapie
L’utilisation d’antibiotiques est probablement le facteur le plus
déterminant de l’espérance de vie et de la qualité de vie du patient atteint
de mucoviscidose en raison de sa grande efficacité à réduire les infections
des voies respiratoires et, par conséquent, à protéger la santé des poumons
(Weiner & Orenstein, 2012). L’antibiothérapie a pour objectif principal de
prévenir la colonisation chronique des bronches et des poumons par
certains germes et de limiter la prolifération des bactéries présentes chez
les patients colonisés. Cet objectif est crucial pour le pronostic du patient
atteint de mucoviscidose puisqu’une antibiothérapie précoce permet
d’éviter ou de postposer la colonisation chronique qui participe à la

PARTIE THÉORIQUE
- 46 -
destruction progressive des poumons. Les antibiotiques sont généralement
prescrits lors d’exacerbations pulmonaires ; celles-ci étant fréquentes chez
le patient atteint de mucoviscidose. Ainsi, l’antibiothérapie est souvent
répétée, voire parfois continue, sur de longues périodes. Une
antibiothérapie adéquate implique des examens bactériologiques, pratiqués
à intervalles réguliers, au moins trimestriellement, des sécrétions
respiratoires. Les germes les plus régulièrement mis en évidence au niveau
des expectorations et qui tendent à s’installer sont le Staphylococcus aureus
et Pseudomonas aeruginosa, ce dernier influençant défavorablement le
pronostic (Lebecque & Baran, 2002a). Le germe Burkholderia cepacia est
encore plus redouté mais l’incidence de celui-ci est rare en Belgique (3.6%)
(Belgian Cystic Fibrosis Registry, 2014).
Conditions d’utilisation. Les antibiotiques sont principalement utilisés
en cas d’infections des voies respiratoires (= exacerbations pulmonaires).
Les infections virales, bien qu’insensibles aux antibiotiques, favorisent
l’invasion des poumons par les bactéries. Ainsi, l’antibiothérapie est
également utilisée dans ce contexte pour son rôle de protection des
poumons contre l’infection bactérienne. L’antibiothérapie est répétée (à
chaque exacerbation pulmonaire) et souvent maintenue pendant de longues
périodes (Lebecque & Baran, 2002a). A titre d’exemple, les antibiotiques
par voie de nébulisation sont souvent prescrits quotidiennement ;
l’antibiothérapie par voie orale s’étale sur une période de deux à trois
semaines et est souvent répétée ; l’antibiothérapie par voie intraveineuse
est, quant à elle, épisodique (cf. ci-dessous pour les différentes voies
d’administration) (Frédéric Pierart, communication personnelle, 23
septembre 2015).
Voie d’administration. Les antibiotiques sont administrés par voie
orale, par inhalation ou par voie intraveineuse. En cas d’exacerbations
pulmonaires, le médecin prescrit dans un premier temps des antibiotiques
par voie orale et par voie de nébulisation. Les antibiotiques par voie

CHAPITRE 1 – LA MUCOVISCIDOSE
- 47 -
intraveineuse sont envisagés dans un second temps, lorsque la prise par
voie orale ou par voie d’inhalation n’a pas fonctionné ou ne fonctionne pas
assez vite. Généralement, l’administration d’antibiotiques par voie
intraveineuse nécessite une hospitalisation (minimum 14 jours) (Weiner &
Orenstein, 2012).
Effets secondaires. L’antibiothérapie est généralement bien tolérée
même si chaque antibiotique peut entraîner l’un ou l’autre effet secondaire,
souvent mineur au regard des bénéfices recueillis (Lebecque & Baran,
2002a).
5.1.2. La kinésithérapie
La kinésithérapie est une autre composante importante du traitement
symptomatique de l’atteinte pulmonaire. Elle consiste en l’élimination des
sécrétions trop épaisses qui s’accumulent dans les voies bronchiques,
favorisent les infections et inflammations multiples et participent à la
destruction progressive des poumons (Reychler & Opdekamp, 2002;
Weiner & Orenstein, 2012). La kinésithérapie est le traitement de la
mucoviscidose le plus contraignant car elle est souvent quotidienne, voire
même biquotidienne en fonction de la sévérité de l’atteinte pulmonaire, et
demande beaucoup de temps (au minimum 20 minutes par séance). En plus
de la contrainte temporelle, l’inconfort, une certaine lassitude, voire des
difficultés relationnelles avec le(s) thérapeute(s) conduisent dans la
majorité des cas à des problèmes de compliance au traitement. Ainsi,
l’adhérence à la kinésithérapie constitue l’un des enjeux majeurs de la prise
en charge des patients atteints de mucoviscidose (Reychler & Opdekamp,
2002). Les différentes techniques de kinésithérapie utilisées chez les
patients atteints de mucoviscidose sont présentées dans le Tableau 5.
Actuellement, aucune de ces techniques n’a démontré sa supériorité par

PARTIE THÉORIQUE
- 48 -
rapport à une autre et l’association de plusieurs de ces méthodes est
fréquente (Reychler & Opdekamp, 2002).
5.2. L’atteinte digestive
La prise en charge nutritionnelle est un élément essentiel du traitement
de la mucoviscidose car les patients qui présentent une meilleure nutrition
ont moins de problèmes de croissance, une meilleure fonction pulmonaire
et une espérance de vie plus élevée que les patients souffrant de
malnutrition. La prise en charge nutritionnelle du patient atteint de
mucoviscidose comporte trois composantes principales (Bauraind, De
Gorter, & Saussez, 2002) :
L’ingestion d’enzymes pancréatiques par voie orale (Lipases,
amylases et protéases) facilite l’absorption et la digestion des graisses,
des sucres et des protéines. Leur ingestion se fait pendant le repas et
est nécessaire à chaque prise d’aliments (repas ou collation) (Bauraind
et al., 2002).
Régime hypercalorique : les besoins énergétiques des patients
atteints de mucoviscidose sont supérieurs à ceux de la population
générale ; l’alimentation doit être équilibrée, hypercalorique (fournir
120 à 140% des apports caloriques recommandés) et sans restrictions
de graisses. Si les apports nutritionnels ne sont pas suffisants à la prise
de poids, des milkshakes ou compléments nutritionnels
hypercaloriques peuvent être utilisés (Bauraind et al., 2002).

CHAPITRE 1 – LA MUCOVISCIDOSE
- 49 -
Tableau 5 – Les différentes techniques de kinésithérapie utilisées chez les patients atteints de mucoviscidose (Reychler
& Opdekamp, 2002; Weiner & Orenstein, 2012)
I. La kinésithérapie respiratoire dite « classique »1 :
a) Drainage postural – consiste à éliminer les sécrétions visqueuses en plaçant le patient dans différentes
positions, chaque position permettant l’accès à un segment précis du poumon, de sorte à optimaliser l’action
de la pesanteur et y à accélérer le flux expiratoire2.
b) Percussions et vibrations – consiste, respectivement, à décoller les sécrétions et à diminuer la viscosité du
mucus.
II. Les techniques d’augmentation du flux expiratoire3
a) Drainage autogène4 – consiste en plusieurs séries de respirations contrôlées : série 1 : très peu d’air dans les
poumons ; série 2 : une quantité normale d’air dans les poumons ; série 3 : grande quantité d’air dans les
poumons. Cette technique nécessite un grand apprentissage avant d’être pleinement efficace.
b) « Active cycle of breathing technique » – cette méthode repose sur des techniques d’expirations
forcées incluant la répétition de trois phases : une respiration contrôlée (respiration calme et lente ; souvent à
travers le nez) ; des expansions thoraciques (inspirations profondes) ; des expirations forcées (expirations
fortes et rapides avec la bouche ouverte).
1 Ces techniques sont de moins en moins utilisées car elles sont très complexes à réaliser pour atteindre l’efficacité désirée (Marc-Antoine Wuidart, kinésithérapeute du centre muco de Liège, communication personnelle, 30 septembre 2015) 2 Mécanisme par lequel les secrétions sont acheminées vers le pharynx pour y être expectorées (Reychler & Opdekamp, 2002). 3 Le patient est capable d’utiliser ces techniques seul ; elles favorisent l’autonomie du patient. 4 En Belgique, il s’agit de la technique la plus pratiquée en association avec d’autres techniques utilisant un appareillage (ex. flutter®, voir suite du tableau) (Marc-Antoine Wuidart, communication personnelle, 30 septembre 2015)

PARTIE THÉORIQUE
- 50 -
Tableau 5 (suite) – Les différentes techniques de kinésithérapie utilisées chez les patients atteints de mucoviscidose
(Reychler & Opdekamp, 2002; Weiner & Orenstein, 2012)
III. Autres techniques (utilisation d’appareillage) :
a) Pression expiratoire positive (PEP) – cette technique consiste à respirer à travers un masque ou un
embout buccal avec une résistance. La pression expiratoire résultante est renvoyée vers les voies aériennes
afin de les maintenir ouvertes durant l’expiration et d’aider le patient à l’expectoration (cf. Acapella®,
Quake®).
b) Compressions thoraciques à haute fréquence – elles sont administrées à l’aide d’une sorte de gilet de
sauvetage relié à un appareil qui le gonfle et le dégonfle rapidement. Ce mécanisme provoque des vibrations
qui diminuent la viscosité du mucus déjà décollée. Ce matériel est coûteux et son intérêt n’a pas encore été
démontré.
c) Flutter® – dispositif en forme de pipe contenant une bille qui vibre lors de l’expiration du patient. Les
vibrations sont alors renvoyées vers les voies respiratoires et permettent la diminution de la viscosité du
mucus déjà décollé.
d) Ventilation à percussions intra-pulmonaires – vise à décoller les sécrétions à l’aide d’un embout buccal
qui délivre des petites rafales d’air (Percussionaire®) ; le matériel est coûteux et des études
supplémentaires sont nécessaires pour préciser les indications et contre-indications dans le traitement de
la mucoviscidose.

CHAPITRE 1 – LA MUCOVISCIDOSE
- 51 -
Prise de vitamines liposolubles A-D-E-K : en raison de leur
malabsorption, des suppléments de vitamines liposolubles sont
prescrits quotidiennement (A-D-E-K) (Bauraind et al., 2002). La
vitamine A aide à combattre les infections, prévient les défauts de
vision dans l’obscurité ainsi que les problèmes de croissance et de
formation osseuse. La vitamine D est nécessaire dans la minéralisation
des os (absorption du calcium et du phosphore) et intervient dans le
bon fonctionnement de nombreux organes. La vitamine E prévient des
problèmes neuromusculaires et protège les poumons de
l’inflammation. Enfin, la vitamine K prévient des problèmes de
coagulation, notamment en cas d’atteinte hépatique ; la protéine de la
coagulation étant produite dans le foie (Fulton et al., 2012).
5.3. Les implications
La mucoviscidose et ses traitements exigent une certaine discipline et
une organisation de la vie quotidienne, cela est dû principalement au fait
que l’essentiel de la prise en charge se fait à domicile. Ces exigences de
traitements ont des répercussions dans divers domaines chez l’enfant
malade ainsi que chez ses parents et demandent certains aménagements de
la vie quotidienne (Jeanbaptiste & Matossian, 2002). En voici quelques
exemples :
Aménagement de l’environnement de l’enfant :
L’école. Bien que l’enfant atteint de mucoviscidose aille à l’école
normalement, l’enseignant doit savoir qu’il est sujet à un certain
absentéisme scolaire en raison de son suivi médical ou des phases
d’hospitalisation. Il est important de bien accompagner les enseignants,
les camarades de classe et leurs parents afin d’éviter d’éventuels conflits ou
incompréhension (brochures et kits éducatifs disponibles sur le site de

PARTIE THEORIQUE
- 52 -
l’association muco : http://www.muco.be/fr/muco-lecole) (Jeanbaptiste &
Matossian, 2002).
Les loisirs, les amis et les vacances. Des activités telles que les
vacances ou les visites à un ami sont également profitables à l’enfant,
malade ou non. Cependant, ces activités impliquent la prise de
certaines dispositions afin d’intégrer le traitement de façon optimale.
Par exemple, en vacances, il faut prévoir un kinésithérapeute sur place
et s’organiser pour que les activités n’interfèrent pas avec le
traitement. Si l’on part en avion, il est préférable de téléphoner à la
compagnie pour s’assurer que la pressurisation des cabines est telle
que l’enfant malade aura assez d’oxygène, etc. Lorsque l’enfant malade
déloge, certains arrangements doivent également être pris afin de
s’assurer que le traitement soit pris correctement (ex. bien informer
les parents des amis) et que la kinésithérapie soit effectuée
(Jeanbaptiste & Matossian, 2002; Spahr, Orenstein, & Weiner, 2012a).
Aménagement de l’environnement des parents :
Le temps de travail. La majorité des traitements ayant lieu à domicile,
une partie de la responsabilité de la prise en charge de l’enfant malade
repose désormais sur les épaules des parents. Ainsi, il est très fréquent
que l’un des deux parents, souvent la mère, réduise son temps de
travail (mi-temps, voire pause-carrière) afin de répondre à toutes les
exigences du traitement.

CHAPITRE 1 – LA MUCOVISCIDOSE
- 53 -
En résumé…
La mucoviscidose est une maladie génétique qui entraîne de
nombreuses complications et limite l’espérance de vie du patient.
Cependant, le pronostic des patients atteints de mucoviscidose s’est
considérablement amélioré au cours des dernières décennies. Le suivi des
patients dans un centre spécialisé pour la mucoviscidose et une
antibiothérapie plus adaptée sont les principaux facteurs impliqués dans
l’amélioration du pronostic global de la maladie. L’attention accrue au statut
nutritionnel ainsi qu’une meilleure reconnaissance de formes moins sévères
de la maladie apportent également leur contribution dans l’amélioration
des chiffres de survie (Lebecque, 2002). Bien que l’espérance de vie ait
augmenté, les exigences des traitements associés à la mucoviscidose posent
encore d’importants problèmes psychosociaux (Besier & Goldbeck, 2011).
Dans ce contexte, l’évaluation de la QV chez ces patients prend tout son sens
et devient un paramètre essentiel permettant d’évaluer l’impact de la
maladie et de ses traitements sur la vie du patient (Abbott, Webb, & Dodd,
1997; Royce & Carl, 2011). Désormais, l’objectif des équipes soignantes
dans les centres spécialisés pour la mucoviscidose est double : d’une part,
ils cherchent à accroître encore l’espérance de vie des jeunes patients et,
d’autre part, à promouvoir leur QV (Royce & Carl, 2011). Cependant, la QV
des enfants (< 12 ans) a été sous-investiguée en comparaison à celle des
adultes et des adolescents atteints de mucoviscidose. Ce constat a éveillé
notre intérêt à mesurer la QV en pédiatrie.


Chapitre 2
Mesurer la qualité de
vie chez l’enfant


- 57 -
Chapitre 2 Mesurer la qualité de vie chez l’enfant
Afin de mieux comprendre la notion de QV et les difficultés liées à son
évaluation chez l’enfant, ce chapitre propose une discussion des propos
généraux associés à ce concept. Tout d’abord, la première section
s’intéresse à la définition du concept de QV. Ensuite, la deuxième section
présente les problèmes conceptuels et méthodologiques relatifs à son
évaluation. Enfin, la troisième section recense les instruments de mesure de
la QV disponibles chez l’enfant.
1. Définition de la QV1
Chez l’adulte, bien que de nombreuses conceptions de cette notion aient
été élaborées (cf. recensement des définitions in Dupuis et al., 2000)(Davis
et al., 2006), aucun consensus n’a été établi ; chaque chercheur
appréhendant ce concept selon les diverses perspectives fondées sur les
préoccupations propres à son champ d’investigation (Trudel, Leduc, &
Dumont, 2012). Parmi les définitions les plus fréquemment citées dans la
littérature, on retrouve celle proposée par l’OMS: « La QV est la perception
qu'a un individu de sa place dans l'existence, dans le contexte de la culture
et du système de valeurs dans lequel il vit en relation avec ses objectifs, ses
attentes, ses normes et ses inquiétudes. C'est un concept très large,
influencé de manière complexe par la santé physique du sujet, son état
1 NB : la QV au sens où nous l’entendons dans ce travail de thèse inclut également le concept
plus spécifique de QV relative à la santé (« HRQOL »). En effet, divers facteurs peuvent
influencer la QV (ex. santé, ressources économiques, maison, conditions politiques, statut
socio-économique, etc.). Cependant, les facteurs relatifs à la santé sont généralement évalués
sous le concept plus restreint de « QV relative à la santé ». Ainsi, ce concept fait partie
intégrante de la QV et représente « la perception subjective par l’individu de l’impact d’un
état de santé, incluant la maladie et de ses traitements, sur son fonctionnement physique,
psychologique et sociale » [Traduction libre] (Leidy, Revicki, & Genesté, 1999).

PARTIE THEORIQUE
- 58 -
psychologique, son niveau d'indépendance, ses relations sociales ainsi que
sa relation aux éléments essentiels de son environnement. » [Traduction
libre] (WHOQOL Group, 1993)(p.153).
Bien que l’OMS se préoccupe abondamment de la QV, à l’heure actuelle,
il n’existe aucune définition considérant les spécificités de la période de
l’enfance. C’est pourquoi, partant de la littérature, mais aussi des outils
existants chez l’adulte, et malgré la diversité des définitions proposées,
nous faisons le choix de nous appuyer sur deux éléments centraux de la QV :
son caractère multidimensionnel et subjectif (Eiser & Morse, 2001b, 2001c;
Lemetayer, 2012; Matza, Swensen, Flood, Secnik, & Leidy, 2004).
1.1. Le caractère multidimensionnel de la QV
Il est aujourd’hui reconnu que la QV s’appréhende au travers de
diverses dimensions. La définition de l’OMS, citée ci-dessus (WHOQOL
Group, 1993), indique clairement le caractère multidimensionnel du
concept. Il en va de même pour Davis et al. (2006) : « la QV se définit par
son caractère multidimensionnel incluant des aspects tels que le
fonctionnement physique, cognitif, social et émotionnel » [Traduction libre]
ou pour Upton, Lawford, et Eiser (2008) : « la QV renvoie à la satisfaction
éprouvée par un individu dans les diverses sphères de vie, incluant le bien-
être physique, sociale, économique et psychologique » [Traduction libre].
Bien qu’il existe une grande hétérogénéité dans le nombre de
dimensions à évaluer et dans leur contenu au sein de la littérature sur la QV
chez l’adulte, le monde scientifique s’accorde sur l’évaluation d’au moins
trois dimensions (Bruchon-Schweitzer & Boujut, 2014) :

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 59 -
La dimension physique : cette dimension fait référence à la santé
physique de l’individu (état de santé) ainsi qu’à ses capacités
fonctionnelles2 (Bruchon-Schweitzer & Boujut, 2014).
La dimension psychologique : la santé psychologique de l’individu
regroupe des composantes telles que les émotions ou affects positifs,
les affects négatifs, l’estime de soi, les capacités cognitives (ex.
mémoire, capacités attentionnelles et d’apprentissage, etc.) et l’image
corporelle ou l’apparence perçue (Bruchon-Schweitzer & Boujut,
2014).
La dimension sociale : la composante sociale de la QV comprend les
relations et les activités sociales (Bruchon-Schweitzer & Boujut, 2014).
Qu’en est-il chez l’enfant ? Appréhende-t-il la QV sur base des mêmes
dimensions que l’adulte (physique, psychologique et sociale) ? Une revue de
littérature sur les outils génériques et spécifiques disponibles chez les
enfants met en évidence que les domaines de QV pertinents chez l’adulte le
sont également chez l’enfant (Eiser & Morse, 2001c). Cependant, bien que ce
caractère multidimensionnel soit applicable à la QV en pédiatrie, il existe
des différences quant à certains aspects spécifiques de la vie de l’enfant.
Contrairement à l’adulte, chez qui le fonctionnement social est souvent
évalué en fonction du nombre et de la qualité de ses contacts sociaux (amis,
collègues), l’enfant évolue dans de multiples contextes sociaux incluant la
famille, le groupe de pairs, l’école et la communauté (hôpitaux, voisins,
etc.) ; chacun de ces contextes sociaux pouvant influencer la QV de l’enfant
(Matza et al., 2004; Spieth & Harris, 1996). Ainsi, le contexte social joue un
rôle différent et, peut-être plus important, dans la QV de l’enfant que dans
celle de l’adulte (Matza et al., 2004).
2 Le statut fonctionnel correspond à la capacité de l’individu à réaliser les activités de la vie quotidienne et à accomplir ses rôles sociaux (Veillette, Demers, & Dutil, 2007).

PARTIE THEORIQUE
- 60 -
1.2. Le caractère subjectif de la QV
La littérature sur la QV chez l’adulte met en évidence l’expérience
subjective de l’individu comme l’un des éléments centraux de l’évaluation
de la QV ; en d’autres termes, la QV doit évaluer le point de vue de l’individu
(Eiser & Morse, 2001b). À titre d’exemples, voici quelques définitions
indiquant clairement le caractère subjectif du concept. D’après Oleson
(1990), la QV se définit comme « la perception subjective de satisfaction ou
de bonheur par rapport à divers domaines de vie importants pour
l’individu » [Traduction libre]. Pour d’autres, la QV renvoie « […] à
l’ensemble des satisfactions/insatisfactions éprouvées par un sujet à propos
de sa vie actuelle en général » (Gerin, Dazord, Cialdella, Leizorovicz, &
Boissel, 1991). La définition de l’OMS citée ci-dessus reflète également le
caractère subjectif de la QV: c’est « la perception qu'a un individu de sa
place dans l'existence, dans le contexte de la culture et du système de
valeurs dans lequel il vit en relation avec ses objectifs, ses attentes, ses
normes et ses inquiétudes » [Traduction libre].
Qu’en est-il chez les enfants ? Sont-ils capables de rapporter des
informations fiables quant à leur QV ou faut-il avoir recours à l’hétéro-
évaluation (ex. parents, professeurs, professionnels de la santé) ? Certaines
études démontrent que les parents sont en mesure d’identifier des
problèmes comportementaux observables (ex. bien-être physique) mais
éprouvent des difficultés à rapporter des informations fiables sur les
problèmes émotionnels de leur enfant (Eiser & Morse, 2001a; Gordon H.
Guyatt, Juniper, Griffith, Feeny, & Ferrie, 1997). De plus, les parents
manquent d’informations quant à l’expérience de l’enfant à l’école ou aux
interactions sociales de l’enfant avec ses amis (Pickard & Knight, 2005). La
question, souvent controversée, de l’évaluation de la QV via des

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 61 -
questionnaires d’auto- vs hétéro- évaluation sera discutée plus tard dans ce
chapitre (cf. section 2.1.1).
2. Mesurer la QV chez l’enfant
Mesurer la QV chez l’enfant présente un certain nombre d’avantages tels
que le support à la communication entre le patient et l’équipe
soignante (Varni, Burwinkle, & Lane, 2005), l’évaluation de la qualité des
soins médicaux (Varni et al., 2005), l’identification des problèmes
psychosociaux (Grootenhuis, Koopman, Verrips, Vogels, & Last, 2007;
Matza et al., 2004; Spieth & Harris, 1996; Varni et al., 2005),
l’amélioration de la prise de décisions cliniques (ex. changement de
traitement (Eiser & Morse, 2001c; Spieth & Harris, 1996), une approche
centrée sur la perspective de l’enfant (Eiser & Morse, 2001b; Leidy,
Revicki, & Genesté, 1999) et l’évaluation de l’efficacité d’un nouveau
traitement ou d’une nouvelle intervention (Eiser & Morse, 2001b; Leidy
et al., 1999). Cependant, lors du développement ou de l’utilisation des
mesures de QV chez les enfants, cliniciens et chercheurs se heurtent à
certaines considérations conceptuelles et méthodologiques.
2.1. Problèmes conceptuels relatifs à la notion de QV
2.1.1. Confusions entre les notions d’état de santé,
de statut fonctionnel et de QV
Il existe une confusion autour de la définition de la QV et de son
évaluation en raison de son chevauchement avec d’autres concepts voisins
dont l’état de santé et le statut fonctionnel (Eiser & Morse, 2001c).
Cependant, en dépit du recouvrement qu’il existe entre ces trois notions,
celles-ci ne sont pas interchangeables (Drotar, 2004).

PARTIE THEORIQUE
- 62 -
Le statut fonctionnel correspond à la capacité de l’individu de réaliser
les activités de la vie quotidienne dans divers domaines de vie : physique
(ex. subvenir à ses besoins et maintenir une bonne santé), social (ex.
accomplir ses rôles sociaux) et psychologique (ex. maintenir un certain
bien-être psychologique) (Eiser & Morse, 2001b) (Wilson & Cleary,
1995). Contrairement aux mesures de QV qui évaluent l’expérience
subjective de l’individu, les mesures de statut fonctionnel évaluent les
capacités fonctionnelles (autonomie) de l’individu ainsi que ses
comportements observables (ex. les mesures du statut fonctionnel évaluent
ce que l’individu est en réalité capable de faire et non pas ce qu’il pense qu’il
est capable de faire) (Eiser & Morse, 2001b).
Selon l’OMS, « la santé est un état de complet bien-être physique, mental et
social, et qui ne consiste pas seulement en une absence de maladie ou
d'infirmité » (Organisation Mondiale de la Santé, 1946) (p.100). La santé est
un concept assez large incluant des mesures du statut fonctionnel, de l’état
physique (douleur, dextérité, dysfonctionnement biologique ou
physiologique, etc.) et du bien-être psychologique. Ces mesures peuvent
également faire partie des mesures de QV. Cependant, contrairement aux
mesures de santé, l’originalité des questionnaires de QV est l’évaluation de
la perspective du patient. Ainsi, les mesures de QV ajoutent une dimension
subjective à l’évaluation de l’état de santé de l’individu (Eiser & Morse,
2001b).
Certains questionnaires souvent recensés parmi les mesures de la QV
évaluent en réalité l’état de santé ou le statut fonctionnel de l’enfant (ex.
Child Health Questionnaire ; the Child Health and Illness Profile, etc.) (cf.
Eiser & Morse, 2001b ; Solans et al., 2008) (cf. section 3). Par conséquent,
nous recommandons une certaine prudence lors du choix de l’instrument
de mesure afin de s’assurer que ce dernier évalue bien le concept qu’il est
censé mesurer en fonction de l’objectif de recherche.

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 63 -
2.1.2. Notion de but
La plupart des questionnaires de QV chez l’enfant (auto- et hétéro-
évaluation, générique ou spécifique) évalue ce concept en termes d’état (ex.
comment je me sens ?) sans prendre en considération les attentes de
l’enfant (ex. comment je voudrais me sentir ?) ni l’importance qu’il attribue
à chaque domaine de vie (Missotten, Etienne, & Dupuis, 2007; Touchèque,
Etienne, Missotten, & Dupuis, in press). A titre d’exemples, les définitions
suivantes suggèrent la nécessité d’aller au-delà cette simple notion d’état et
de considérer les attentes de l’individu. En 1984, Calman (1984) proposait
de définir la QV comme étant la « différence et l’écart entre les attentes
d’une personne et son expérience vécue » [Traduction Trudel et al., 2012].
D’après Cella et Cherin (1988), la QV renvoie à « l’évaluation des patients et
à leur satisfaction quant à leur niveau actuel de fonctionnement en
comparaison à ce qu’ils perçoivent comme étant possible ou idéal »
[Traduction Trudel et al., 2012]. Dupuis, Perrault, Lambany, Kennedy et David
(1989), quant à eux, vont encore plus loin et suggèrent une définition de la
QV qui tienne compte des objectifs de l’individu tout en considérant que
chaque objectif n’a pas la même importance (c’est-à-dire l’organisation
hiérarchique des objectifs selon la priorité que leur accorde l’individu).
Ainsi, d’après ces auteurs, « la QV, à un moment donné dans le temps, est
l’état qui correspond à un niveau atteint par une personne dans la poursuite
continuelle de ses buts organisés hiérarchiquement ». Enfin, la définition de
la QV selon l’OMS confirme également la nécessité d’aller au-delà cette
simple notion d’état : « La QV est la perception qu'a un individu de sa place
dans l'existence, dans le contexte de la culture et du système de valeurs
dans lequel il vit en relation avec ses objectifs, ses attentes, ses normes et
ses inquiétudes […] » [Traduction libre] (WHOQOL Group, 1993).

PARTIE THEORIQUE
- 64 -
2.2. Considérations méthodologiques relatives à la QV
2.2.1. Auto- vs hétéro- évaluation
L’utilisation de questionnaires d’auto- vs hétéro-évaluation chez les
enfants a largement été débattue (Etienne, Dupuis, Spitz, Lemetayer, &
Missotten, 2011; Riley, 2004). Lors de l’auto-évaluation, l’enfant rapporte
lui-même les informations sur sa QV. Cette méthode a pour avantage
d’évaluer l’expérience subjective de l’individu. Cependant, la fiabilité des
informations rapportées par l’enfant est parfois questionnable (Matza et al.,
2004). L’hétéro-évaluation, quant à elle, est réalisée par une tierce personne
qui est, dans la majorité des cas, le parent ; parfois par un professionnel de
la santé ou un enseignant. Elle offre l’avantage d’obtenir des informations
plus fiables lorsque l’enfant est trop jeune ou incapable de répondre au
questionnaire. Par contre, elle va à l’encontre du caractère subjectif de la QV
et peut ne pas refléter la perspective de l’enfant (Matza et al., 2004). Les
avantages et inconvénients de ces deux méthodes d’évaluation sont
présentés de manière plus détaillée dans le Tableau 1.
Par ailleurs, certains auteurs suggèrent d’obtenir des informations à la
fois de l’enfant et de ses parents (Connolly & Johnson, 1999; Eiser & Morse,
2001a). La combinaison de l’auto- et de l’hétéro-évaluation permet de
pallier aux inconvénients (cf. Tableau 1) de chacune de ces méthodes. Elle
offre également la possibilité d’évaluer le degré d’accord entre les réponses
fournies par l’enfant et celles du parent afin de relever les éventuelles
inconsistances entre la perception de chacun. Cependant, cette approche a
également ses inconvénients tels que celui d’alourdir le processus de
recrutement ou celui du choix lorsque les réponses de l’enfant et des
parents divergent (Matza et al., 2004).

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 65 -
Tableau 1 – Avantages et Inconvénients de l’auto- vs hétéro-évaluation
Auto-évaluation Hétéro-évaluation (cf. parents-report)
Avantages Cohérence avec la conceptualisation de la QV
(caractère subjectif). L’auto-évaluation fournit des
informations quant à l’expérience subjective de
l’enfant (Matza et al., 2004).
Validité des informations chez les jeunes enfants.
Fournit des informations plus fiables lorsqu’il s’agit de
jeunes enfants (âge non spécifié par l’auteur) ou
d’enfants incapables de rapporter des informations
fiables (ex. enfants avec un déficit ou un handicap)
(Matza et al., 2004).
Inconvénients
Difficulté à évaluer les concepts complexes ou
abstraits. Les jeunes enfants (de 5 à 8 ans) sont
capables de fournir des informations fiables sur des
concepts concrets (ex. douleur) (Connolly &
Johnson, 1999; Kalish, 2005; Riley, 2004).
Cependant, la fiabilité des informations qu’ils
fournissent à propos de concepts complexes et
abstraits (ex. en bonne santé, irritable, estime de
soi) est questionnable ; ces derniers s’acquièrent
plus tard : 9-10 ans (Landgraf & Abetz, 1996; Matza
et al., 2004; Rebok et al., 2001).
Incohérence avec la conceptualisation de la QV
(caractère subjectif). La perception individuelle de
l’enfant n’est pas évaluée (Matza et al., 2004).
Inconsistance des réponses fournies par l’enfant vs le
parent. Le degré d’accord entre les informations
fournies par l’enfant et celle fournies par le parent varie
de faible à modéré. Ainsi, les informations fournies par le
parent peuvent ne pas représenter la perception de
l’enfant (Matza et al., 2004; Varni et al., 2005; Jan L.
Wallander et al., 2001).

PARTIE THEORIQUE
- 66 -
En résumé, ces différentes méthodes d’évaluation (auto-évaluation,
hétéro-évaluation et mixte) présentent toutes un intérêt certain. Ainsi, la
décision relative à l’utilisation d’une échelle d’auto-évaluation, d’hétéro-
évaluation ou d’une combinaison des deux dépend de divers facteurs : les
caractéristiques individuelles de l’enfant (ex. âge, habilités cognitives,
langage), les domaines de QV que l’on souhaite évaluer, le type de maladie
ainsi que la conception et les objectifs de l’étude (Matza et al., 2004). À titre
indicatif, nous recommandons de privilégier l’utilisation de questionnaires
d’auto-évaluation de la QV chez les enfants de plus de 8 ans et d’opter pour
une combinaison des deux méthodes pour les plus jeunes enfants (< 8 ans).
Telle que suggérée par Eiser, Mohay, et Morse (2000), nous partageons
l’idée que l’utilisation seule de questionnaires d’hétéro-évaluations de la QV
représente une certaine incrédulité face à la réalité selon laquelle la
perception des enfants sur le monde et leurs priorités dans la vie seraient
différentes de celle de l’adulte.
2.2.2. La création d’un format et d’un design
approprié à l’âge de l’enfant
Certains éléments formels sont à prendre en considération lors de la
construction ou de l’utilisation d’un outil d’évaluation chez l’enfant.
Le niveau de compréhension de l’enfant : la fiabilité des informations
fournies par l’enfant est influencée par ses habiletés cognitives et
langagières (Wallander, Schmitt & Koot, 2001). Comme mentionné dans le
Tableau 1, les concepts abstraits peuvent être difficile à comprendre pour
un enfant de 5-6 ans qui aura besoin de plus d’assistance pour compléter le
questionnaire par rapport à un enfant de 9-10 ans (Rebok et al., 2001).
Ainsi, lorsqu’un instrument de mesure est développé, il est essentiel
d’évaluer la pertinence de l’outil en termes de vocabulaire, d’instructions,

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 67 -
de structures de phrases et de contenu afin de déterminer l’âge minimum
pour l’administration du questionnaire (Matza et al., 2004).
Le format de réponse : Dans leur article, Rebok et al. (2001)
conduisent différentes études qui ont pour objectif de déterminer, chez des
enfants âgés entre 5 et 11 ans (n=114), leur capacité à répondre à des
questions relatives à leur santé, présentées sous différents formats. Bien
que cette étude ne soit pas spécifique à l’évaluation de la QV, elle n’en reste
pas moins instructive lorsque l’on souhaite obtenir des informations quant
au format de réponse à adopter dans le contexte de l’évaluation chez
l’enfant. Les résultats de cette étude révèlent que les échelles de réponses
en trois, quatre et cinq points peuvent être utilisées par tous les enfants
sans confusion. Les auteurs montrent également que les enfants préfèrent :
(1) les échelles visuelles analogiques (VAS) composées de cercles plutôt que
de lignes ; (2) les cercles de tailles graduées (ex. petit, moyen et grand
cercles) plutôt que les cercles de même taille ; (3) quatre propositions de
réponse plutôt que trois ; et (4) deux illustrations de part et d’autre de la
VAS pour les réponses extrêmes plutôt qu’une seule illustration. Cette
recherche met en évidence l’importance d’adapter le format des
questionnaires relatifs à l’état de santé ou de QV lorsqu’ils sont destinés à
une population d’enfants.
La longueur de l’échelle : En raison de la grande variabilité des
capacités attentionnelles chez l’enfant, il est important d’évaluer si la
longueur de l’échelle est appropriée à son âge. En règle générale, les enfants
plus âgés sont capables de compléter des questionnaires avec un plus grand
nombre d’items que les enfants plus jeunes (Matza et al., 2004). À titre
d’exemple, Wallander et al. (2001) proposent 14 items pour les enfants
entre 4 et 7 ans, 23 items pour ceux entre 8 et 11 ans et 41 items pour les
adolescents entre 12 et 16 ans.
Le période de rappel : La majorité des questionnaires exigent de
l’enfant qu’il décrive son état de santé au cours d’une période de rappel

PARTIE THEORIQUE
- 68 -
spécifique (ex. une semaine ou deux mois). Cependant, cette capacité de
l’enfant à répondre au sein d’une période spécifique est influencée par des
différences développementales (ex. perception du temps ou mémoire). Bien
que les enfants de 8 à 11 ans soient capables de répondre aux questions en
se référant à des expériences qui se sont déroulées dans un délai de quatre
semaines, les enfants plus jeunes (< 8 ans) peuvent éprouver quelques
difficultés à se rappeler des symptômes ou des comportements relatifs à un
si large laps de temps (Rebok et al., 2001; Wallander et al., 2001).
Méthode d’administration (autonomie) : En fonction de l’âge de
l’enfant, celui-ci peut réclamer plus ou moins d’indépendance par rapport à
la complétion du questionnaire. Par exemple, les jeunes enfants peuvent
avoir besoin d’assistance pour lire les items ou comprendre comment
répondre au questionnaire alors que les enfants plus âgés complètent les
questionnaires (papier-crayon, ordinateur ou en ligne) avec plus
d’autonomie (Matza et al., 2004). Les auteurs ne précisent pas l’âge moyen à
partir duquel l’enfant devient plus autonome dans le remplissage d’un
questionnaire. Cependant, notre expérience dans l’évaluation d’enfants
démontre qu’ils sont capables de répondre de manière indépendante à des
questions relatives à leur QV au-delà de l’âge de 10 ans.
En conclusion, l’une des stratégies qui permettrait de pallier les
différences liées à l’âge de l’enfant est le développement de diverses formes
de questionnaires ciblant les différents groupes d’âge dans la période de
l’enfance (ex. une forme pour les enfants de 4-7 ans, de 8-12 ans et de 13-17
ans). Ces diverses formes se différencient en termes de contenu, de nombre
d’items, de format de réponse et d’autonomie dans le remplissage du
questionnaire (Matza et al., 2004; Wallander et al., 2001).

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 69 -
2.2.3. Les outils génériques vs spécifiques
Deux grands types d’outils peuvent être utilisés pour évaluer la QV chez
les enfants : les outils génériques et les outils spécifiques. Les mesures
génériques de la QV sont conçues pour être applicables à tous les sous-
groupes de population (ex. enfants sains ou malades) et permettent la
comparaison entre ces groupes. Les mesures spécifiques, quant à elles,
évaluent des domaines qui ne sont applicables qu’à un seul groupe (ex.
enfants atteints d’une maladie chronique spécifique) et permettent
d’appréhender les problèmes relatifs à la QV qui découlent des
changements associés à cette condition particulière (Davis et al., 2006). Les
avantages et les inconvénients de ces deux types de mesures sont présentés
dans le Tableau 2. Un troisième type d’outil, appelé outil modulaire, est
également disponible pour l’évaluation de la QV chez l’enfant. Il inclut une
mesure générique ainsi qu’un module additionnel spécifique à une maladie.
Cette troisième approche combine les avantages des deux outils classiques
(génériques et spécifiques). Elle s’avère notamment intéressante lorsque
l’on souhaite à la fois comparer un groupe d’enfants atteints d’une maladie
particulière à la population générale et considérer l’impact spécifique de
cette maladie sur les divers domaines de QV pertinents pour ce type de
population.
Ces diverses considérations conceptuelles et méthodologiques mettent
en évidence le véritable challenge auquel chercheurs et cliniciens doivent
faire face lors du développement d’outils d’évaluation appropriés à la
période de l’enfance.

PARTIE THEORIQUE
- 70 -
Tableau 2 – Avantages et inconvénients des outils génériques et des outils
spécifiques
Mesures génériques Mesures spécifiques
Avantages Est applicable à toute
population (Varni et al.,
2005)
Permet la comparaison : (1)
entre groupes d’enfants
malades ; (2) entre un
groupe d’enfants malades et
un groupe d’enfants sains
(population générale) (Varni
et al., 2005)
Est sensible aux
changements spécifiques liés
à une maladie donnée (Varni
et al., 2005)
Fournit, au niveau
individuel, des informations
spécifiques quant aux
symptômes et à l’impact du
traitement associés à une
maladie donnée (Varni et al.,
2005)
Inconvénients Est insensible aux aspects
spécifiques d’une maladie
(Varni et al., 2005)
Ne mesure pas les
symptômes spécifiques
d’une maladie donnée ni les
effets secondaires du
traitement (Varni et al.,
2005)
Ne permet pas la
comparaison entre
différents groupes d’enfants
malades ou entre un groupe
d’enfants malades et la
population générale (Varni
et al., 2005)

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 71 -
3. Les instruments de mesure de la QV
Afin d’examiner l’adéquation des outils d’évaluation de la QV chez
l’enfant âgé de 0 à 12 ans, un recensement de ces derniers a été réalisé.
Seules les mesures génériques de la QV seront prises en considération dans
cette section. Ces derniers ont été identifiés en utilisant deux stratégies de
recherche. Premièrement, un certain nombre d’outils a été repéré sur base
d’articles investiguant la mesure de la QV chez l’enfant (cf. Connolly &
Johnson, 1999 ; Eiser & Morse, 2001b, 2001c ; Matza et al., 2004 Ravens-
Sieberer et al., 2006; Solans et al., 2008). Deuxièmement, une recherche a
été lancée via la base de données PsycINFO (2002 to 2015) afin d’identifier
les articles publiés entre 2008 (année de parution du dernier article de
revue : Solans et al., 2008) et 2015, en utilisant les mots-clés suivants:
« children », « quality of life », « measurement », « assessment ». Cette
stratégie a donné lieu à 614 résumés d’articles. Ces deux stratégies de
recherche ont donné lieu à l’identification de 25 outils génériques (Figure
1). Pour être inclus, les outils identifiés devaient évaluer la QV ou la QV
relative à la santé en pédiatrie (0-12 ans). Les instruments qui sont utilisés
pour évaluer la QV mais qui en réalité mesurent l’état de santé ou le statut
fonctionnel de l’enfant ont été exclus. Ainsi, parmi les 25 mesures
génériques identifiées, 10 d’entre elles ont été exclues1 ; les 15 mesures
restantes étant présentées dans le Tableau 3.
1 Questionnaires exclus: Children's Health Ratings Scale (CHRS); Sickness Impact
Profile (SIP); Infant/Toddler Quality of Life Questionnaire (ITQOL); Warwick child
health and morbidity profile (WCHMP); Perceived Illness experience (PIE); Child
Health questionnaire (CHQ); Functional Status II (FSIIR); Comprehensive health
status classification system for preschool children (CHSCS-PS); Child Health and
Illness Profile – Child Edition (CHIP-CE); TACQOL et TAPQOL.

PARTIE THEORIQUE
- 72 -
Auto-évaluation
(6)
Auto-évaluation
(5)
Hétéro- et auto-évaluation
(16)
Hétéro- et auto-évaluation
(9)
Hétéro- évaluation
(3)
Hétéro-évaluation
(1)
Figure 1 – Répartition des outils d’évaluation de la QV chez l’enfant selon deux catégories : génériques vs spécifiques et hétéro- vs
auto-évaluation.
n = 7 Exclusion : n = 2 n = 1

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 73 -
Bien que la majorité des outils présentés aient été validés (qualités
psychométriques : fidélité et validité), peu font état de fondements
conceptuels solides. Sur les 15 outils génériques recensés, seulement trois
se basent sur un modèle théorique explicite : l’Exqol (« Discrepancy theory »),
l’ISQV-E (Modèle des systèmes de contrôle) et le Nordic QOLQ (Modèle de
Lindström). Cependant, la validité et la fidélité du Nordic QOLQ n’a pas été
testée (cf. Solans et al., 2008). Par conséquent, seuls l’Exqol et l’ISQV-E
possèdent à la fois de bonnes qualités psychométriques et un fondement
théorique. La « Discrepancy theory » postule qu’une pauvre QV résulte de
l’écart entre la situation actuelle (« comment je suis ») et la situation idéale
(« comment je voudrais être ») (Eiser, Cotter, Oades, Seamark, & Smith,
1999). Le modèle des systèmes de contrôle1 s’articule autour de l’idée que
tous les comportements humains sont contrôlés et maintenus par la
poursuite d’objectifs. Dans un tel système, la mesure de la QV s’appuie sur la
comparaison que l’individu fait entre sa situation actuelle et sa situation
désirée (objectif) (Dupuis et al., 1989). Ainsi, tant l’Exqol que l’ISQV-E
considèrent la notion d’objectif dans l’évaluation de la QV. De plus, tous
deux évaluent la QV en termes de subjectivité (ex. questionnaires d’auto-
évaluation) et de multi-dimensionnalité. Cependant, contrairement à
l’Exqol, l’ISQV-E possède l’avantage d’être un outil modulaire (cf. section
2.2.3.).
En résumé, parmi les différents outils d’évaluation de la QV en pédiatrie,
peu offrent à la fois de bonnes qualités psychométriques et des bases
conceptuelles solides (ex. modèle théorique et définition claire et
opérationnelle de la QV). Ainsi, nous recommandons une certaine prudence
lors du choix d’un outil d’évaluation de la QV chez l’enfant afin de considérer
au mieux ses avantages et ses inconvénients ainsi que son adéquation avec
l’objectif de recherche (ou clinique).
1 L’ISQV-E ayant servi de mesure de la QV dans cette thèse de doctorat, des informations
plus détaillées quant au modèle qui le sous-tend sont disponibles en annexe (Annexe 1).

PARTIE THEORIQUE
- 74 -
Tableau 3 – Outils d’évaluation de la QV disponibles chez l’enfant
Outils de QV Auteur(s) Âge (année) No. d’items
OUTILS GÉNÉRIQUES : AUTO-ÉVALUATION
AUQUEI (c) Manificat & Dazord (1997) 4-12 27
Exqol(c) Eiser et al. (1999) 6-11 16
GCQ(c) Collier, MacKinlay, & Phillips (2000) 6-14 25
PQ-LES-Q* Endicott, Nee, Yang, & Wohlberg (2006) 6-17 15
ISQV-E (a, c) Etienne et al. (2011) 8-12 20
OUTILS GÉNÉRIQUES : AUTO- ET HÉTÉRO-ÉVALUATION
Nordic QOLQ Lindström & Eriksson (1993) 2-18 74
CQOL Graham, Stevenson, & Flynn (1997) 9-15 15
KINDL-R(a) Ravens-Sieberer & Bullinger (1998) 4-17 40/24/12 †
PedsQL(a) Varni, Seid, & Rode (1999) 2-12 23
HAY (a, c) Le Coq, Colland, Boeke, Bezemer, & van Eijk (2000) 8-12 32
TedQL* Lawford, Volavka, & Eiser (2001) 3-8 22
DISABKIDS (a,b) Petersen, Schmidt, Power, & Bullinger (2005) 4-16 37/12/6 †
KIDSCREEN The KIDSCREEN Group Europe (2006) 8-18 52/27/10 †
QoML* Gong, Young, Dempster, Porepa, & Feldman (2007) 10mo-18 3
OUTILS GÉNÉRIQUES : HÉTÉRO-ÉVALUATION
CLQI Beattie and Lewis-Jones (2006) 5-16 12
† Il existe différentes versions du questionnaire avec plus ou moins d’items en fonction de sa longueur (version longue vs courte), de l’âge de
l’enfant (jeune enfant vs enfants plus âgés vs adolescents) ou de la méthode d’évaluation (parents vs enfants/adolescents).
*Le caractère subjectif et multidimensionnel de ces instruments n’a pas pu être déterminé (article non accessible).

CHAPITRE 2 – MESURER LA QV CHEZ L’ENFANT
- 75 -
** Outil d’hétéro-évaluation; une version d’auto-évaluation est disponible pour les enfants de 12-13 ans.
(a) Outils modulaires.
(b) Uniquement destinés aux maladies chroniques.
(c) Outils d’évaluation de la QV tenant compte de la notion de but.
AUQUEI – Autoquestionnaire de Qualité de vie Enfant Imagé; Exqol – Exeter Quality of Life Measure; GCQ – Generic Children’s
Quality of Life Measure; PQ-LES-Q – Pediatric Quality of Life Enjoyment and Satisfaction Questionnaire; ISQV-E© – Inventaire
Systémique de Qualité de vie ; Nordic QOLQ – Nordic Quality of Life Questionnaire for children; CQOL – Child Quality of Life
Questionnaire; PedsQL – Pediatric Quality of Life Inventory; HAY – How Are You; QoML – The Quality of My Life questionnaire; CLQI
– Children’s Life Quality Index; CFQ-R – Cystic Fibrosis Questionnaire Revised

PARTIE THEORIQUE
- 76 -
En résumé…
La mesure de la QV chez l’enfant représente encore à l’heure actuelle un
challenge pour les chercheurs et les cliniciens, en raison des problèmes
conceptuels et méthodologiques qu’elle pose. D’un point de vue conceptuel,
il existe une confusion quant à la définition de la QV. En effet, initialement
développée chez l’adulte, il n’existe pas de définition considérant les
spécificités relatives à la période de l’enfance (ex. manque de précision
quant au contenu des domaines de QV à évaluer) (Eiser & Morse, 2001c).
Par conséquent, certains outils disponibles n’évaluent pas à proprement dit
la QV mais plutôt des concepts voisins (ex. statut fonctionnel ou santé
physique). De plus, peu d’outils offrent une assise théorique solide et
intègrent la notion d’objectifs dans l’évaluation de la QV. À ces problèmes
conceptuels s’ajoutent des considérations méthodologiques qui incluent :
l’utilisation de questionnaires d’auto- vs hétéro-évaluation ; l’adaptation du
format de l’outil en fonction de l’âge de l’enfant (ex. niveau de
compréhension, nombres d’items, format de réponses, autonomie dans la
complétion de l’échelle) ; et l’utilisation d’outils génériques vs spécifiques.
Malgré ces challenges, la mesure de la QV représente un objectif
thérapeutique important dans la prise en charge des enfants atteints de
mucoviscidose. Elle fournit à l’équipe soignante des informations
importantes relatives à l’impact de la maladie et des traitements sur la vie
quotidienne de l’enfant. Ainsi, la QV est considérée, dans ce projet de
recherche, comme un critère d’ajustement à la maladie chez l’enfant. Le rôle
des divers facteurs prédicteurs de celle-ci sera étudié à la lumière des
modèles théoriques d’ajustement à la maladie disponibles en psychologie
de la santé.



Chapitre 3
Modèles d’ajustement
à la maladie en
pédiatrie


- 81 -
Chapitre 3 Modèles d’ajustement à la maladie en pédiatrie
Il existe de nombreux modèles théoriques en psychologie de la santé.
Selon les issues à prédire, ces modèles peuvent être divisés en deux
catégories : (a) les modèles qui prédisent des comportements de santé (ex.
arrêter de fumer, réduire sa consommation d’alcool, adhérer à un
traitement, etc.) tels que le modèle des croyances de santé (Rosenstock,
Strecher, & Becker, 1988), le modèle transthéorique du changement
(Prochaska & DiClemente, 1982), la théorie de l’action raisonnée (Ajzen &
Fishbein, 1980) et la théorie du comportement planifié (Ajzen & Madden,
1986) ; (b) les modèles qui prédisent l’ajustement à la maladie (ex. QV).
Dans ce chapitre nous nous intéresserons aux principaux modèles
théoriques appartenant à cette deuxième catégorie, à savoir : le modèle
d’autorégulation du comportement de maladie (Leventhal, Meyer, & Nerenz,
1980), le modèle transactionnel du stress et du coping (Lazarus & Folkman,
1984) et le modèle intégratif et multifactoriel (Bruchon-Schweitzer &
Dantzer, 1994). Ces modèles théoriques ont été développés auprès d’une
population d’adultes. À l’heure actuelle, aucune adaptation à une population
pédiatrique n’a été réalisée. Une tentative de modélisation chez l’enfant sera
exposée ultérieurement (cf. Chapitre 10).
1. Le modèle de l’autorégulation du comportement de
maladie (Leventhal et al., 1980)
Le modèle d’autorégulation du comportement de maladie, décrit par
Leventhal et al. (1980), propose un cadre théorique qui permet de
comprendre comment l’individu fait face à une menace pour sa santé (ex.
une maladie) (Leventhal, Diefenbach, & Leventhal, 1992). Ce modèle se base

PARTIE THEORIQUE
- 82 -
sur une approche en termes de résolution de problème qui se décrit en trois
stades (voir Figure 1).
D’abord, l’individu donne un sens au problème et évalue la menace pour
sa santé en développant deux représentations parallèles, bien qu’inter-
reliées : cognitive et émotionnelle (stade 1 : l’interprétation). Le
développement de représentations cognitives (= croyances) de la maladie
se construit sur base de cinq dimensions (Ogden, 2014; Weinman &
Figueiras, 2002): l’identité : désignation de la maladie et des symptômes
associés ; les causes : perception du patient quant aux causes de la maladie ;
les conséquences : croyances quant à la manière dont la maladie va
influencer physiquement, socialement et psychologiquement le patient ; la
chronologie : perception du patient quant à la durée de la maladie (ex. crise
aigüe, condition chronique) ; et la contrôlabilité : croyances quant à la
possibilité de guérir ou de contrôler la maladie. Parallèlement au
développement de ces représentations cognitives, ce premier stade
d’interprétation entraîne également un changement dans l’état émotionnel
de l’individu (= représentation émotionnelle de la maladie) (Leventhal et al.,
1992).
Ensuite, sur base de ces représentations (cognitives et émotionnelles),
l’individu met en place des stratégies de coping pour faire face à cette
menace (stade 2 : le coping) (Leventhal et al., 1992). Les stratégies de
coping1 désignent des réponses cognitives (ex. évaluation de la situation
stressante, de ses ressources, recherche d’information), affectives (ex.
expression ou répression de la peur, de la détresse, etc.) ou
comportementales (ex. résolution de problème) mises en œuvre par un
1 Les stratégies de coping sont à différencier du concept d’adaptation. L’adaptation
est un concept large, qui comprend toutes les réactions des organismes vivants face
aux conditions changeantes de leur environnement. Au contraire, le coping est un
concept spécifique ne concernant que les réactions à des changements dans
l’environnement évalués comme menaçants (ou stressants) (Bruchon-Schweitzer,
2001).

CHAPITRE 3 – MODÈLES D’AJUSTEMENT CHEZ L’ENFANT
- 83 -
individu pour tolérer, réduire ou maîtriser la situation problématique (ex.
menace pour la santé) (Bruchon-Schweitzer, 2001; Ogden, 2014). Il s’agit de
tentatives conscientes et volontaires pour affronter des problèmes actuels
ou récents (Bruchon-Schweitzer, 2001).
Enfin, l’individu évalue l’efficacité des stratégies de coping mise en place
en relation avec l’issue de santé désirée (ex. QV satisfaisante, bien-être
psychologique, etc.) afin d’en déterminer soit la maintenance soit le
changement (stade 3 : l’évaluation) (Leventhal et al., 1992).
Parallèlement à l’élaboration de ce modèle, Lazarus et Folkman (1984),
auteurs de référence de la théorie cognitive du stress et du coping,
développent un modèle centré sur les relations entre la personne et
l’environnement. Selon ces auteurs, les stratégies de coping sont mises en
place sur base d’un processus d’évaluation de la situation stressante et non
sur base des représentations de la maladie ; celles-ci n’étant pas prises en
considération dans le modèle proposé par Lazarus et Folkman (1984).

PARTIE THEORIQUE
- 84 -
Figure 1 – Le modèle d’autorégulation du comportement de maladie de Leventhal et al. (1980)
Boucle de rétroaction
Boucle de rétroaction
Représentation
cognitive
(Identité, causes,
conséquences,
chronologie,
contrôlabilité)
Évaluation Stratégies de coping
Évaluation
Menace pour la santé (ex. maladie)
Représentation
émotionnelle
(réactions
émotionnelles) Stratégies de
coping
ÉTAPE 1 ÉTAPE 2 ÉTAPE 3

CHAPITRE 3 – MODÈLES D’AJUSTEMENT CHEZ L’ENFANT
- 85 -
2. Le modèle transactionnel du stress et du coping
(Lazarus & Folkman, 1984)
Selon la théorie cognitive du stress et du coping, le stress se définit
comme « une transaction particulière entre la personne et l’environnement
dans lequel celui-ci est évalué comme débordant ses ressources et pouvant
mettre en danger son bien-être » (Lazarus & Folkman, 1984) (p. 19). Cette
transaction entre l’individu et son environnement se déroule en deux
phases : (1) l’évaluation de la situation stressante; et (2) l’élaboration des
stratégies de coping (voir Figure 2).
L’évaluation (phase 1) est un processus cognitif par lequel l’individu
évalue l’évènement stressant (évaluation primaire) et ses ressources
disponibles pour y faire face (évaluation secondaire) (Bruchon-Schweitzer,
2001). Ces deux processus sont aussi importants l’un que l’autre et
n’entretiennent pas un ordre spécifique, malgré leur appellation. En effet, ils
sont en constante interaction afin de déterminer si la situation est
stressante ou non (Lazarus & Folkman, 1984). Lors de l’évaluation primaire,
l’individu cherche à donner du sens à la situation et à évaluer quel impact
elle peut avoir sur lui. Selon la conception de Lazarus et Folkman (1984), ce
ne sont pas les caractéristiques objectives de l’évènement stressant qui
modulent la transaction entre l’individu et son environnement mais bien
l’expérience subjective (ex. stress perçu) vis-à-vis de cet évènement. Ainsi,
un même évènement stressant est évalué de façon différente selon chaque
individu (Bruchon-Schweitzer, 2001; Spitz, 2002). Une situation stressante
peut être évaluée comme une perte, une menace ou un défi (Bruchon-
Schweitzer, 2001; Spitz, 2002): les évaluations de perte (affective,
matérielle, corporelle, etc.) s’accompagnent d’émotions négatives telles que
la tristesse, la honte ou la colère ; les évaluations de menace (perte
potentielle) s’accompagnent d’émotions négatives telles que l’anxiété et la
peur ; et les évaluations de défi (un challenge) s’accompagnent d’émotions

PARTIE THEORIQUE
- 86 -
positives telles que l’excitation, la fierté et la joie. Après avoir appréhendé
la situation stressante, l’individu évalue les ressources personnelles (ex.
contrôle perçu) et sociales (ex. soutien social perçu) dont il dispose (=
évaluation secondaire) (Bruchon-Schweitzer, 2001).
Ensuite, sur base de ce processus d’évaluation, l’individu détermine ce
qu’il peut mettre en place pour faire face à la situation en élaborant des
stratégies de coping (phase 2). Selon Lazarus and Folkman (1984) (p.141),
les stratégies de coping se définissent par « l’ensemble des efforts cognitifs et
comportementaux, constamment changeants, déployés pour gérer des
exigences spécifiques internes et/ou externes qui sont évaluées par la
personne comme consommant ou excédant ses ressources ». Selon eux, le
coping a deux fonctions principales : modifier le problème à l’origine du
stress (cf. coping centré sur le problème) et réguler les réponses
émotionnelles associées à l’évènement stressant (cf. coping centré sur
l’émotion). Ainsi, ces auteurs identifient deux types de stratégies de coping:
(a) le coping centré sur le problème vise à diminuer les exigences de la
situation et/ou à augmenter les ressources de l’individu pour mieux faire
face à l’évènement stressant. Le coping centré sur le problème sera utilisé
lorsque l’individu pense que la situation est contrôlable (Bruchon-
Schweitzer, 2001) ; et (b) le coping centré sur l’émotion vise à gérer les
réactions émotionnelles associées à la situation stressante. Il ne modifie pas
le problème mais permet de se modifier soi-même afin de mieux supporter
la situation problématique (Bruchon-Schweitzer, 2014). Il existe de
nombreuses stratégies de régulation des émotions (ex. consommation de
substances, l’engagement dans diverses activités, expression des émotions,
etc.). Ces stratégies de coping sont généralement utilisées lorsque l’individu
perçoit la situation comme étant incontrôlable (Bruchon-Schweitzer, 2001).
Lazarus et Folkman (1984) proposent une classification dichotomique des
stratégies de coping (centrées sur le problème vs l’émotion). Il est important
de relever qu’il existe d’autres types de classification (ex. approche vs

CHAPITRE 3 – MODÈLES D’AJUSTEMENT CHEZ L’ENFANT
- 87 -
évitement, etc.) voire une absence de classification où chaque stratégie est
évaluée de manière individuelle. Il existe donc un certain nombre de
questionnaires de stratégies de coping tant chez l’adulte que chez l’enfant ;
tous utilisant une classification différente. Ainsi, lors de l’évaluation de ces
stratégies, il est important pour le chercheur ou le clinicien de choisir une
échelle qui utilise une classification adaptée aux objectifs de recherche ou
thérapeutiques.
En résumé, Lazarus et Folkman (1984) mettent en évidence
l’importance des transactions entre la personne et l’environnement. Cet
élément central sera repris plus tard par Bruchon-Schweitzer et Dantzer
(1994) comme l’une des composantes principales de leur modèle intégratif
et multifactoriel en psychologie de la santé.

PARTIE THEORIQUE
- 88 -
Figure 2 - Le modèle transactionnel du stress et du coping (Lazarus & Folkman, 1984) (reproduction d’après Bruchon-Schweitzer,
2001)
Feedback Déterminants personnels
(croyances, motivations,
traits de personnalité, lieu
de contrôle – attribution
externe vs. interne)
Déterminants
environnementaux
(nature de l’évènement,
imminence, durée,
contrôlabilité,
disponibilité) et sociaux
(réseau social)
Stratégies de coping
(centrées sur les
problèmes ou les
émotions)
Issues de
santé (ex. QV)
Évaluation primaire
(ex. stress perçu) et
secondaire (ex.
contrôle perçu ou
soutien social perçu)

CHAPITRE 3 – MODÈLES D’AJUSTEMENT CHEZ L’ENFANT
- 89 -
3. Le modèle intégratif et multifactoriel (Bruchon-
Schweitzer & Dantzer, 1994)
Le modèle intégratif et multifactoriel de Bruchon-Schweitzer et Dantzer
(1994) a été élaboré afin d’intégrer les divers facteurs que l’on considérait
souvent séparément lorsque l’on étudiait les issues de santé (ou critères
d’ajustement), qu’elles soient biomédicales (ex. statut fonctionnel, santé
physique) ou psychologiques (ex. détresse émotionnelle, QV) (Bruchon-
Schweitzer, 2002) (cf. Figure 3). Ces facteurs peuvent être répertoriés selon
deux catégories : les prédicteurs et les transactions individu-contexte.
La première catégorie (prédicteurs ou antécédents) regroupe les
antécédents environnementaux et sociodémographiques (c’est-à-dire, ce
que l’individu subit) ainsi que des antécédents psychosociaux et
biomédicaux (c’est-à-dire, ce que l’individu est). Parmi les antécédents
environnementaux, on retrouve la culture, l’environnement familial, le
réseau social, les évènements de vie stressants, etc. Les variables
sociodémographiques sont représentées par l’âge, le sexe, le niveau socio-
économique, la profession, certains modes de vie à risque (ex. problèmes
alimentaires, alcool, tabac, manque de sommeil, etc.), etc. Les antécédents
psychosociaux se divisent en deux catégories, à savoir les facteurs de
vulnérabilités ou traits pathogènes (ex. affectivité négative, névrosisme,
hostilité, etc.) et les facteurs protecteurs ou traits immunogènes (ex.
optimisme, résilience, auto-efficacité, etc.). Les problèmes de santé, quant à
eux, sont un exemple d’antécédents biomédicaux.
La deuxième catégorie représente les transactions entre l’individu et
l’environnement, à savoir les processus d’évaluation primaire et secondaire
ainsi que les stratégies de coping (cf. section 2 : modèle transactionnel du
stress et du coping de Lazarus et Folkman, 1984). Bruchon-Schweitzer et

PARTIE THEORIQUE
- 90 -
Dantzer (1994) postule que cette deuxième catégorie joue un rôle
modérateur ou médiateur1 entre les prédicteurs et les issues de santé.
1 La variable médiatrice explique la relation entre la variable indépendante et la
variable dépendante en réduisant significativement ou en annulant la relation entre
ces dernières. La variable modératrice, quant à elle, affecte la direction ou
l’intensité de la relation entre la variable indépendante et la variable dépendante.
Ainsi, les médiateurs expliquent comment ou pourquoi certains effets apparaissent
alors que les modérateurs déterminent dans quel cas ils se déclarent (Baron &
Kenny, 1986).

CHAPITRE 3 – MODÈLES D’AJUSTEMENT CHEZ L’ENFANT
- 91 -
Figure 3 – Le modèle intégratif et multifactoriel (Bruchon-Schweitzer &
Dantzer, 1994)
Antécédents
environnementaux
Événements de vie
stressants
Réseau social
Antécédents
sociodémographiques
Antécédents
psychosociaux
Type A, Type C
Hostilité
Névrosisme
Dépression
Anxiété
Affectivité négative
Optimisme
Lieu de contrôle interne
Auto-efficacité
Endurance
Sens de la cohérence
Résilience
Affectivité positive
Antécédents
biomédicaux
Fonctionnement de
divers systèmes
physiologiques
(neurologiques,
endocriniens,
immunitaires, etc.)
Stratégies
d’ajustement
Coping centré sur
l’émotion
Coping centré sur le
problème
Evaluation
Stress perçu
Contrôle perçu
Soutien social
perçu
Bien-être
subjectif
(Satisfaction,
bonheur, qualité
de vie, subjective)
Etat de santé
physique
Antécédents
(ou
prédicteurs)
Transactions individu-
contexte
(rôle modérateur ou
médiateur)
Issues
(ou critères)

PARTIE THEORIQUE
- 92 -
En résumé…
Les différents modèles présentés dans ce chapitre offrent tous la
possibilité d’étudier la QV en tant qu’indicateur de l’ajustement du patient à
sa maladie ; chacun ayant sa propre spécificité. Leventhal et al. (1980)
considèrent les représentations cognitives et émotionnelles de la maladie
comme les éléments centraux de leur modèle d’autorégulation. Lazarus et
Folkman (1984), quant à eux, offrent un solide cadre conceptuel pour les
recherches sur le stress et mettent à l’avant-plan le rôle des stratégies de
coping dans la gestion de celle-ci. Enfin, Bruchon-Schweitzer et Dantzer
(1994) ont élaboré un modèle qui intègre des facteurs que l’on considérait
souvent séparément lorsque l’on étudiait les issues biomédicales (ex. statut
fonctionnel, santé physique) ou psychologiques de la santé (ex. QV). Il s’agit
des facteurs environnementaux (évènement de vie stressant, réseau social
et facteurs sociodémographiques), psychosociaux (traits de personnalité et
antécédents biomédicaux) et processuels (ou transactionnels ; cf. Lazarus &
Folkman, 1984) (Bruchon-Schweitzer, 2002). Cependant, ces modèles ont
été initialement développés auprès d’une population d’adultes ; aucun
d’entre eux n’étant applicable dans un contexte pédiatrique. Aussi, une
adaptation de ces modèles d’ajustement chez l’enfant permettrait de
renforcer l’assise théorique des recherches en médecine somatique infantile
(cf. Chapitre 10 : tentative de modélisation chez l’enfant). La difficulté d’une
telle perspective réside dans le fait que, contrairement à l’adulte, l’enfant est
un être en plein développement. Par conséquent, une modélisation de
l’ajustement de l’enfant à la maladie nécessite la prise en compte de
certaines considérations développementales (ex. niveau de
conceptualisation de la maladie).



Chapitre 4
L’enfant et la maladie :
perspective
développementale


- 97 -
Chapitre 4 L’enfant et la maladie : perspective développementale
La compréhension du développement du concept de maladie chez
l’enfant représente un enjeu important pour les professionnels de la santé
en pédiatrie. D’une part, elle permet à l’équipe médicale de transmettre à
l’enfant les informations appropriées selon son âge afin de lui permettre de
mieux comprendre sa maladie (Siegal & Peterson, 2005). D’autre part, une
meilleure compréhension de la maladie par l’enfant permet : (a) de prévenir
ou de réduire les réactions émotionnelles négatives liées à l’annonce d’un
diagnostic, au début d’un nouveau traitement, à l’hospitalisation, etc.
(Koopman, Baars, Chaplin, & Zwinderman, 2004) et (b) de promouvoir
l’engagement de l’enfant dans certains comportements qui seront
bénéfiques pour sa santé (ex. compliance au traitement) (Rushforth, 1999).
Historiquement, il existe deux approches pionnières qui apportent un
éclairage sur la compréhension de l’enfant des processus de causes, de
prévention et de traitement de la maladie : (1) les théories du
développement cognitif et (2) les théories de la biologie (Myant & Williams,
2005).
La première partie de ce chapitre exposera la conceptualisation de la
maladie chez l’enfant selon les théories du développement cognitif.
Inévitablement, une première section sera dédiée à la théorie piagétienne
du développement cognitif de l’enfant. Celle-ci servira de point de départ à
la deuxième et troisième section qui porteront sur deux approches centrées
sur le développement d’une théorie des stades de compréhension du
concept de maladie chez l’enfant. Ensuite, la seconde partie de ce chapitre
présentera la conceptualisation de la maladie selon les théories relatives au
développement des notions de biologie. La première section parlera du
développement d’une théorie naïve de la biologie chez l’enfant pour ensuite

PARTIE THEORIQUE
- 98 -
basculer sur la deuxième section qui abordera le concept de maladie d’après
les modèles biologiques.
1. L’approche cognitive de la conceptualisation de
la maladie
1.1. Prérequis : La théorie piagétienne du développe-
ment cognitif de l’enfant
Les recherches sur la compréhension par l’enfant du fonctionnement de
son anatomie, du concept de santé et celui de maladie ont toutes comme
point commun leur étroite relation avec la théorie piagétienne du
développement cognitif (cf. Piaget & Inhelder, 1969) (Rushforth, 1999).
Cette théorie s’articule autour que l’idée que le développement de
l’intelligence humaine (ou l’acquisition des connaissances) se fait par des
adaptations successives du sujet à son environnement. L’ordre de
succession de ces acquisitions est constant et les structures construites à un
stade donné deviennent parties intégrantes des structures du stade suivant.
Ainsi, Piaget décrit quatre stades du développement de l’intelligence :
1. Le stade sensori-moteur (0 à 2 ans) : L’enfant interagit et comprend
le monde qui l’entoure via ce qu’il perçoit et ce qu’il fait. Il est capable
de comprendre qu’un objet continue d’exister en dehors de son champ
de vision et de se souvenir d’objets, de gestes ou de personnes
pendant un certain temps (Bee & Boyd, 2003).
2. Le stade préopératoire (2 à 7 ans) : la pensée précède désormais
l’action. Entre 2 et 4 ans, période de la pensée symbolique, l’enfant est
capable de faire une représentation mentale des objets et des
évènements. A ce stade, il considère les choses selon sa propre
perspective sans se rendre compte qu’il existe d’autres points de vue
(= égocentrisme). La pensée animiste gouverne également cette

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 99 -
période : l’enfant donne des caractéristiques humaines aux objets et
aux évènements. Entre 4 et 7 ans, période de la pensée intuitive,
l’enfant devient progressivement capable d’envisager les choses
comme étant de plus en plus extérieures à lui. Son raisonnement est
intuitif, c’est-à-dire centré sur les aspects perceptifs (ex. concept de
conservation: l’apparence change mais la quantité reste identique).
L’enfant ne parvient pas encore à faire des liens entre les différents
éléments. Durant cette période, la pensée de l’enfant est caractérisée
par une moralité hétéronome ou de contrainte (= les règles sont
inflexibles et imposées par l’autorité, c’est la conséquence de l’action
qui prime sur le caractère intentionnel et qui détermine si l’action est
positive ou négative) et ils croient en une justice immanente (=
enfreindre une règle entraîne une punition immédiate) (Bee & Boyd,
2003).
3. Le stade des opérations concrètes (7 à 11-12 ans) : L’enfant est
désormais capable de faire la différence entre lui et les autres (interne
vs externe) et il raisonne de manière logique. Il est capable d’extraire
de ses observations des règles internes, c’est-à-dire de manipuler
mentalement les objets entre eux (Bee & Boyd, 2003).
4. Le stade des opérations formelles (à partir de 11-12 ans) : L’enfant
est capable de manipuler mentalement autant les idées que les objets.
Il raisonne sur des concepts abstraits ou des hypothèses (Bee & Boyd,
2003).
Selon la théorie piagétienne, l’acquisition des connaissances est
interdépendante d’un domaine à l’autre et les difficultés de
conceptualisation de la maladie chez l’enfant reflètent une immaturité
intellectuelle globale (Rushforth, 1999).

PARTIE THEORIQUE
- 100 -
1.2. Les stades de compréhension du concept de
maladie selon Bibace et Walsh (1980)
Sur des travaux de Piaget et Inhelder (1969), Bibace et Walsh (1980)
proposent une théorie des stades de la conceptualisation de la maladie chez
l’enfant. L’objectif de leur démarche était d’offrir un guide dédié aux
praticiens sur la compréhension cognitive du concept de maladie chez
l’enfant afin de les aider à déterminer quel était le niveau d’explications
approprié à fournir à l’enfant selon son âge (Rushforth, 1999).
Sur base des résultats de vastes études pilotes, Bibace et Walsh (1980)
développent un protocole de recherche qui inclut trois groupes d’enfants de
4, 7 et 11 ans ; chaque groupe d’âge correspondant à un stade piagétien (4
ans = période préopératoire ; 7 ans = période des opérations concrètes ; 11
ans = période des opérations formelles). Le protocole, dit « Concept of
Illness Protocol », consiste en 12 séries de questions qui servent à
déterminer les connaissances de l’enfant à propos de plusieurs maladies
fréquentes (ex. le rhume, la rougeole, la crise cardiaque, les maux de tête, la
douleur, la propre maladie de l’enfant ou la maladie d’un ami). Les enfants
ont été interviewés dans un cadre scolaire en utilisant la méthode clinique
de Piaget, c’est-à-dire que le questionnement de l’enfant était conçu de telle
sorte que leurs réponses reflétaient leur raisonnement plutôt qu’une
pensée dichotomique oui/non (ex. « Qu’est-ce qu’un rhume ? », « Pourquoi
les personnes attrapent-elles un rhume ? », « Comment les personnes
attrapent-elles un rhume ? »). Chaque réponse de l’enfant était ensuite
attribuée à une catégorie d’explications.
Bibace et Walsh (1980) identifièrent trois grandes catégories
correspondant aux stades piagétiens : préopératoire – opérations concrètes
– opérations formelles. Au sein de ces trois catégories, les auteurs
identifièrent deux sous-catégories. Par conséquent, en plus d’une catégorie
d’explications nommée « Incompréhension », qui caractérise les enfants au

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 101 -
stade sensori-moteur, Bibace et Walsh (1980) identifièrent six catégories
d’explications de la maladie (cf. Tableau 1).
Tableau 1 – Description des stades de la conceptualisation de la maladie
(Bibace & Walsh, 1980)
Catégorie 0 : Incompréhension
Explication du stade préopératoire
Catégorie 1 : Phénoménisme
Cause = phénomène externe et concret (ex. le soleil, dieu). Incapacité à
expliquer de quelle manière ce phénomène cause la maladie.
Catégorie 2 : Contagion
Cause = proximité avec un objet ou une personne (pas de contact). Absence
d’explication du lien entre la cause et la maladie ou parfois l’enfant évoque la
« magie »
Explication du stade des opérations concrètes
Catégorie 3 : Contamination
Cause = personne, objet ou action externe qui est « mauvaise » ou
« dangereuse » pour le corps. L’enfant est désormais capable d’expliquer le
lien entre la cause et la maladie : soit il a été en contact physique avec la
personne ou l’objet, soit il s’est engagé physiquement dans une action
dangereuse (maladie = externe).
Catégorie 4 : Internalisation
Cause = externe (personne ou objet) ; maladie = interne. L’enfant explique le
lien entre la cause et la maladie par processus interne (ex. avaler ou respirer)
mais l’explication est non spécifique.
Explication du stade des opérations formelles
Catégorie 5 : Explication physiologique
Cause = évènement externe ; maladie = non-fonctionnement ou
dysfonctionnement d’un processus ou organe interne.
Catégorie 6 : Explication psycho-physiologique
Cause = évènement externe ou problème psychologique ; maladie = non
fonctionnement ou dysfonctionnement d’un processus ou organe interne. A
ce stade, l’enfant prend conscience que les pensées ou les sentiments peuvent
également affecter le fonctionnement du corps.
Aucune information n’a été fournie concernant une catégorisation
différente en fonction d’une maladie donnée (ex. l’enfant acquiert-il les
connaissances relatives à la conceptualisation d’un rhume plus rapidement

PARTIE THEORIQUE
- 102 -
que celles par rapport à la conceptualisation d’une rougeole ?). La
répartition des explications des enfants parmi les six catégories proposées
est présentée dans le Tableau 2.
Tableau 2 – Répartition des explications (%) des enfants de chaque groupe
d’âge parmi les six catégories (Bibace & Walsh, 1980)
Stades piagétiens Catégorie 4 ans 7 ans 11 ans
Sensori-moteur 0 : Incompréhension 4
Préopératoire 1 : Phénoménologique
2 : Contagion 54
Opérations concrètes 3 : Contamination 38 63 4
4 : Internalisation 4 29 54
Opérations formelles 5 : Physiologique 8 34
6 : Psycho-physiologique 8
Au vu de ces pourcentages, on observe une incohérence entre les
explications fournies par les enfants d’un certain âge et leur appartenance
théorique à un stade piagétien. Par exemple, une majorité des enfants de 11
ans (58%), choisis par les auteurs en raison de leur appartenance au stade
des opérations formelles, fournissent des explications du stade des
opérations concrètes. De plus, on observe que bien qu’une majorité des
enfants de 4 ans (54%), choisis par les auteurs pour leur appartenance au
stade préopératoire, fournissent une explication de leur période
d’appartenance supposée, 42% fournissent une explication du stade des
opérations concrètes. Ces observations posent question quant à
l’adéquation de la classification choisie par Bibace et Walsh (1980).

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 103 -
1.3. Stade de compréhension des causes de la maladie
Selon Koopman et al. (2004)
Sur base des travaux de Bibace et Walsh (1980), Koopman et al. (2004)
réalisent une étude visant à examiner les connaissances des enfants (groupe
diabétique vs groupe contrôle) par rapport à différents types de maladies
(ex. rhume, diabète, infection) et à des concepts qui y sont associés (ex.
douleur, aller à l’hôpital ou chez le médecin, devenir malade, etc.). La
méthodologie utilisée est similaire à celle de l’étude de Bibace et Walsh
(1980). En effet, une série de 18 questions (de type « Pourquoi ? »
« Comment ? ») à propos de l’identité d’une maladie donnée, de ses causes,
de ses conséquences, de sa durée et du contrôle perçu par l’enfant sur celle-
ci, a été posée à ces derniers. Les résultats de cette étude démontrent que le
développement du concept de maladie dans les deux groupes (diabète vs
contrôle) est cohérent avec les stades du développement piagétien et les
phases de conceptualisation de la maladie développées par Bibace et Walsh
(1980). L’apport de cette étude réside en la mise en relation du
développement du concept de maladie chez l’enfant avec son niveau de
développement perceptuel (cf. Werner, 1948). Ainsi, sur base de la
catégorisation proposée par Bibace et Walsh (1980) et des travaux de
Werner (1948), Koopman et al. (2004) développe un modèle, le modèle TEC
(« Through the Eyes of the Child »), permettant d’appréhender le
développement de la compréhension des causes de la maladie chez l’enfant
(cf. Tableau 3).

PARTIE THEORIQUE
- 104 -
Tableau 3 – Le modèle « Through the Eyes of the Child » et ses assises théoriques (reproduction Koopman et al.,
2004).
Stades piagétiens (Piaget
& Inhelder, 1969)
Développement perceptuel
(Werner, 1948)
Catégorie selon Bibace et
Walsh (1980)
Modèle Tec (Koopman
et al., 2004)
1 : Sensori-moteur
(0-2 ans)
1 : Incompréhension 1 : Invisible
2 : Préopératoire
(2-7 ans)
1 : Global
(perception du tout)
2 : Phénoménologique 2 : Distance
3 : Contagion 3 : Proximité
3 : Opérations concrètes
(7-11 ans)
2 : Analytique
(perception des parties)
4 : Contamination 4 : Contact
5 : Internalisation 5 : Internalisation
4 : Opérations formelles
(à partir de 11 ans)
3 : Synthétique
(les parties deviennent intégrées
au tout)
6 : Physiologique 6 : Processus corporel
7 : Psycho-physiologique 7 : Corps et esprit

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 105 -
Bien que le modèle TEC propose une dénomination des catégories
différentes, les explications rangées dans ces dernières correspondent à la
classification utilisée par Bibace et Walsh (1980). Ainsi, ce nouveau modèle
n’apporte pas de réponses à la question soulevée à la section précédente
quant à l’adéquation de la catégorisation choisie par Bibace et Walsh
(1980). Cette réflexion conduit à l’idée que la compréhension du concept de
maladie n’est peut-être pas nécessairement dictée par l’âge ou les stades du
développement cognitif. Aussi, un nouvel éclairage quant au développement
de ce concept est proposé par l’approche biologique.
2. L’approche biologique de la conceptualisation
de la maladie
Selon la perspective piagétienne du développement cognitif, les
structures cognitives associées aux différents domaines de connaissances
sont interdépendantes, c’est-à-dire que l’acquisition des connaissances dans
un domaine particulier peut entraîner l’amélioration des performances
dans un autre domaine (Wellman & Gelman, 1992). Ainsi, la confusion,
l’incompréhension ou la compréhension partielle de certains concepts, tels
que la maladie ou la santé, sont des conséquences inévitables d’une
immaturité intellectuelle globale (Rushforth, 1999). Kister et Patterson
(1980) sont les premiers auteurs à suggérer que la compréhension du
concept de santé et de maladie n’est pas nécessairement dictée par l’âge ou
les stades du développement cognitif mais pourrait dépendre de
l’augmentation des connaissances dans un domaine particulier tel que la
biologie. Trois ans plus tard, dans leur revue des concepts piagétiens,
Gelman et Baillargeon (1983) suggèrent la possibilité que les structures
cognitives soient spécifiques à un domaine particulier plutôt
qu’interdépendantes aux différents domaines. A priori, le développement de
notre compréhension se ferait au travers de trois grands domaines qui, à

PARTIE THEORIQUE
- 106 -
eux seuls, engloberaient la plupart du monde extérieur avec lequel on
interagit : la physique, la psychologie et la biologie. C’est la construction
d’une théorie naïve de la biologie qui permettrait à l’enfant de comprendre
des concepts tels que la maladie (Wellman & Gelman, 1992). L’attention
portée à la compréhension de la biologie pour expliquer la
conceptualisation de la maladie chez l’enfant s’est d’autant plus accrue
depuis les travaux de Carey (1985); (Carey, 1995). Selon elle, le
raisonnement des enfants sur les phénomènes biologiques est gouverné par
la pensée animiste, non pas parce qu’ils font preuve d’une immaturité
intellectuelle globale comme l’affirmait Piaget, mais parce qu’ils ne
possèdent pas les connaissances spécifiques au domaine de la biologie
(Inagaki & Hatano, 2006).
2.1. Vers le développement d’une théorie naïve de la
biologie
Selon Inagaki and Hatano (2006), il existe trois composantes
essentielles au développement des connaissances dans le domaine de la
biologie : (a) la distinction entre vivants et non vivants ; (b) la distinction
entre corps et esprit ; (c) la compréhension des mécanismes internes
permettant le raisonnement causal sur des phénomènes biologiques.
2.1.1. Distinction entre les vivants et les non-vivants
D’après Carey (1985, 1995), jusqu’à l’âge de 6 ans, les enfants
apprennent une masse de faits à propos du monde biologique (ex. les
animaux sont vivants, les bébés viennent du ventre de leur maman, les
médicaments aident à se sentir mieux, etc.) constituant ainsi une sorte de
dictionnaire qui les aide à prendre des décisions et à apprendre de
nouveaux faits. Cependant, ce n’est qu’à partir de 7 ans que l’enfant parvient
à établir des connexions entre les différents faits biologiques afin de

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 107 -
construire une structure conceptuelle cohérente et unifiée, à savoir une
théorie de la biologie. Selon Carey, la construction de cette théorie se fait au
travers d’un processus de « changement conceptuel ». L’un des
changements conceptuels les plus importants des connaissances
biologiques de l’enfant est la création de la catégorie « chose vivante » à
partir de deux catégories initialement séparées : plantes et animaux. À
partir de là, d’autres changements conceptuels surviennent tels que la
précision du concept de non-vivants. L’enfant est désormais capable de
différencier le concept de « mort » (= arrêt du fonctionnement du corps) du
concept « inanimé » (ex. l’ordinateur n’est pas vivant) ou « irréel » (ex.
Cendrillon n’est pas vivante).
Une étude réalisée par Gelman (1990) met en évidence, quant à elle, une
acquisition rapide de la distinction inanimé vs animé. Dès l’âge de 3 ans,
l’enfant est capable de différencier des animaux (ex. animaux non familiers,
mammifères, etc.) d’objets (ex. statues, objets à roulettes, etc.) en
distinguant s’ils sont capables ou non de mouvements auto-initiés.
2.1.2. Distinction entre le corps et l’esprit
Carey (1985) affirme que les enfants avant l’âge de 10 ans sont
incapables de différencier le domaine de la biologie et celui de la
psychologie. Cependant, d’autres études suggèrent que l’enfant est capable
de distinguer les phénomènes biologiques des phénomènes psychologiques
à un âge beaucoup moins avancé. Dans leur étude, Inagaki et Hatano (1993)
démontrent que des enfants de 4 et 5 ans reconnaissent l’indépendance
entre le fonctionnement des organes du corps et l’intention d’une personne.
Ainsi, les auteurs concluent que l’enfant, dès l’âge de 6 ans, considère le
domaine de la biologie comme étant autonome et séparé de celui de la
psychologie. Par ailleurs, dans une autre étude, Inagaki (1997) confirme les
observations ci-dessus en démontrant que c’est entre l’âge de 3 et 4 ans que

PARTIE THEORIQUE
- 108 -
l’enfant prend conscience des processus qui sous-tendent notre
fonctionnement biologique interne et devient donc capable de différencier
les processus biologiques involontaires et les états mentaux (ex. l’enfant
reconnaît que les battements de cœur sont indépendant de notre volonté).
En résumé, le jeune enfant (3 à 5 ans) est déjà capable de faire la distinction
entre les fonctions physiques et les fonctions mentales (psychologiques)
mais, à ce stade, il est incapable de comprendre que les fonctions mentales
peuvent parfois être à l’origine des phénomènes biologiques. En effet, selon
une étude menée par Notaro, Gelman et Zimmerman (2001), les enfants
d’âge préscolaire jusqu’à environ 7-8 ans n’envisagent pas qu’un problème
psychologique puisse être la cause d’un problème biologique. Entre l’âge de
7-8 ans et celui de 10-11 ans, l’enfant commence à envisager la possibilité
d’une cause psychologique à un problème biologique mais à un moindre
niveau que la cause physique. Ce n’est qu’à partir de 10-11 ans que l’enfant
accepte les causes psychologiques et physiques puissent être à l’origine
d’un phénomène biologique.
2.1.3. Compréhension des causes des phénomènes
biologiques
D’après Carey (1985), les enfants de moins de 10 ans expliquent les
phénomènes biologiques sur base d’une « causalité intentionnelle », c’est-à-
dire que c’est l’intention d’une personne qui cause le phénomène biologique
(ex. je vais grandir parce que je le veux) alors que les enfants plus âgés et les
adultes utilisent une « causalité mécanique », c’est-à-dire que ce sont les
mécanismes physiologiques qui expliquent les processus biologiques
internes. Cependant, Inagaki et Hatano (1987) suggèrent que les enfants de
5-6 ans sont capables de reconnaitre que la croissance d’une chose vivante
va au-delà du contrôle intentionnel. Quelques années plus tard, ces auteurs
proposent l’existence d’une forme intermédiaire de causalité, la « causalité

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 109 -
vitaliste » (ex. le phénomène biologique est expliqué par la transmission ou
l’échange d’énergie vitale). Celle-ci serait utilisée par les enfants réticents à
l’utilisation de la causalité intentionnelle mais pas encore capables d’utiliser
la causalité mécanique (Inagaki & Hatano, 1993). D’après plusieurs études,
les enfants âgés de 6 ans préfèrent une explication des phénomènes
biologiques en termes d’énergie vitale (Inagaki, 1995; Inagaki & Hatano,
1993, 2002). Par exemple, les enfants de 6 ans choisissent ce type
d’explications : « Si le sang ne vient pas dans les mains, elles mourront,
parce que le sang ne leur aura pas apporté de l’énergie » ou « si on ne
mange pas, on mourra car on perdra de l’énergie » (Inagaki & Hatano,
2005 ; p. 27).
2.2. Modèles biologiques et conceptualisation de la
maladie
Suite à la découverte selon laquelle les enfants possèdent une théorie
naïve de la biologie, des travaux de recherche se sont intéressés à la
conceptualisation biologique de la maladie chez l’enfant (><
conceptualisation cognitive, cf. Bibace et Walsh, 1980). La majorité des
études dans ce domaine a particulièrement porté son attention sur la
compréhension de la causalité d’une maladie au travers de la
compréhension de différentes notions : (a) le processus de contagion et de
contamination ; et (b) les germes en tant qu’agent invisible de la cause
d’une maladie. La compréhension de ces concepts permet la construction
d’une théorie cohérente sur le principe d’infection. L’infection est un
processus par lequel certains agents infectieux (ex. germes) sont transmis,
via un contact physique, d’un objet inanimé ou d’un vivant (personne,
plante, animal) (= contaminant) à un hôte qui devient malade suite à cette
transmission (= contagion). La contagion et la contamination sont les
processus les plus familiers aux jeunes enfants puisqu’une grande majorité

PARTIE THEORIQUE
- 110 -
des maladies qui les touche sont des maladies infectieuses (rhume,
varicelle, rougeole, etc.). Par conséquent, les croyances du jeune enfant (3 à
5 ans) à propos de l’infection fournissent des informations importantes par
rapport à leur compréhension du concept de maladie puisqu’il semble que,
selon eux, l’infection définit la maladie (Kalish, 2005).
Les études réalisées sur cette thématique démontrent que: (a) les
enfants d’âge préscolaire sont capables de comprendre les processus de
contagion et de contamination comme causes d’une maladie (Kister &
Patterson, 1980; Michael Siegal, 1988) ; (b) ils comprennent les bases
physiques des processus de contagion et de contamination; c’est le contact
physique avec un contaminant qui rend malade (Kalish, 1997, 2005) ; (c) ils
comprennent que les agents infectieux peuvent être invisibles à l’œil nu (ex.
germes) (Au, Sidle, & Rollins, 1993; Rosen & Rozin, 1993); (d) ils évoquent
les germes comme cause de maladie (Kalish, 1996, 2005; Springer & Ruckel,
1992) ; (e) les enfants, à partir de l’âge de 5 ans, reconnaissent que l’aspect
physique des activités quotidiennes (ex. manger fruits et légumes, aérer sa
chambre, aller coucher tôt, etc.) ainsi que les mauvais comportements (ex.
mentir, faire mal à quelqu’un, etc.) affectent la propension de la personne à
être malade ; bien que les facteurs biologiques jouent une part plus
importante que les facteurs psychologiques/sociaux dans la vulnérabilité
d’un individu à déclarer une maladie (Inagaki, 1997). Cependant, en
parallèle à ces habilités, les enfants d’âge préscolaire ne sont pas encore
capables de reconnaitre que la maladie est un effet différé du contact avec
l’agent infectieux (ex. les germes). L’enfant pense qu’il devient malade après
avoir touché l’objet contaminé (Kalish, 1997). Ainsi, ils ne sont pas
conscients du processus biologique interne (c’est-à-dire, ce qui se passe à
l’intérieur du corps) qui sous-tend le processus de contagion et de
contamination via les germes (Kalish, 1997, 2005; Solomon & Cassimatis,
1999). Au et Romo (1999) supportent également cette observation auprès
d’enfants plus âgés (5 à 12 ans).

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 111 -
La majorité de ces études s’est focalisée sur les enfants d’âge
préscolaire. Qu’en est-il de l’évolution de cette conceptualisation biologique
de la maladie chez les enfants d’âge scolaire ? Bien que les travaux de
recherche sur les modèles biologiques et le concept de maladie soient en
pleine expansion, il est important pour les chercheurs de ne pas relâcher
leurs efforts s’ils souhaitent apporter davantage de preuves à l’encontre
d’une conceptualisation cognitive de la maladie et ainsi créer une théorie
biologique des stades du développement (de l’âge préscolaire à l’âge adulte
en passant par l’adolescence) du concept de maladie.

PARTIE THEORIQUE
- 112 -
En résumé…
Deux approches alimentent le débat sur le développement du concept
de maladie chez l’enfant. La première approche est sous-tendue par la
théorie du développement cognitif (Piaget & Inhelder, 1969) qui postule
que l’acquisition des connaissances est interdépendante d’un domaine à
l’autre et que les difficultés de conceptualisation de la maladie chez l’enfant
reflètent une immaturité intellectuelle globale. En revanche, la seconde
approche postule que l’acquisition des connaissances est spécifique à un
domaine particulier et que le développement du concept de maladie chez
l’enfant dépend de l’augmentation des connaissances dans le domaine de la
biologie. Alors que Carey (1985, 1995), pionnière des travaux de recherche
basés sur cette perspective, affirme que les notions de biologie n’émergent
pas avant l’âge de 10 ans, d’autres études suggèrent que certaines
connaissances biologiques (processus de contamination et de contagion, les
germes en tant qu’agents infectieux invisibles) s’acquièrent bien plus tôt
(Inagaki & Hatano, 2005; Kalish, 2005; Solomon & Cassimatis, 1999). La
théorie de la biologie apporte un éclairage allant à l’encontre d’une
conceptualisation de la maladie selon les théories piagétiennes. Cependant,
les résultats des travaux de recherche ne sont pas suffisamment étayés,
notamment en raison du manque d’information sur les enfants d’âge
scolaire et les adolescents, que pour abandonner les théories du
développement cognitif lors de nos tentatives de compréhension de la
conceptualisation de la maladie chez l’enfant.
Ces considérations développementales sur la conceptualisation de la
maladie chez l’enfant mettent en évidence l’importance à accorder aux
représentations de la maladie. Nous émettons l’hypothèse que des
représentations incomplètes pourraient entraîner des croyances erronées
et des préoccupations infondées chez les enfants atteints d’une maladie

CHAPITRE 4 – PERSPECTIVE DÉVELOPPEMENTALE
- 113 -
donnée et ainsi, jouer un rôle sur leur ajustement. Dans cette perspective, le
modèle d’autorégulation du comportement de maladie de Leventhal et al.
(1980), considérant les représentations de la maladie comme éléments
centraux du modèle, servira de cadre conceptuel à notre projet de
recherche. Une tentative d’adaptation du modèle à une population d’enfant
sera exposée ultérieurement (cf. Chapitre 10).
Par ailleurs, ces différentes approches sur le développement du concept
de maladie chez l’enfant, qu’elles soient cognitives ou biologiques,
fournissent des repères quant au niveau de connaissances acquises à un
certain âge. Cependant, d’autres facteurs peuvent influencer la
conceptualisation de la maladie chez l’enfant tels que les expériences
d’apprentissage (ex. transmission d’informations relatives à la maladie par
l’équipe médicale ou encore les parents, renforcement ou imitation par
observation de comportements ou de croyances relatives à la maladie) (cf.
Théorie de l’apprentissage de Skinner et Bandura in Bideaud, Houdé, &
Pedinielli, 2002). Les théories de l’apprentissage soulignent l’interaction
constante entre les comportements d’un individu, son fonctionnement
cognitif et son environnement (ex. la famille). Le rôle du parent en tant que
« guide » pour les enfants dans leur apprentissage afin qu’ils atteignent un
niveau supérieur de pensée et d’action est largement reconnu (cf. théorie
classique du développement de Vygotsky in Bideaud, Houdé, & Pedinielli,
2002). Ainsi, il est important de considérer les contributions
environnementales, telles que les facteurs parentaux, à l’expérience de
l’enfant par rapport à sa maladie (ex. pensées, comportements et émotions).


Chapitre 5
Le rôle des facteurs
parentaux sur
l’ajustement de
l’enfant malade


- 117 -
Chapitre 5 Le rôle des facteurs parentaux sur l’ajustement de
l’enfant malade
Parmi les prédicteurs de l’ajustement de l’enfant à une maladie
chronique, le rôle des facteurs contextuels familiaux a reçu une attention
accrue au cours de ces 20 dernières années. En utilisant le modèle
transactionnel du stress et du coping (TSC) (Thompson, Gustafson, Hamlett,
& Spock, 1992), de nombreuses études ont démontré la relation
transactionnelle entre l’ajustement des parents et celui de l’enfant (Chaney
et al., 1997; Colletti et al., 2008; Hocking & Lochman, 2005). Le modèle TSC
propose un cadre théorique permettant de comprendre l’influence de
l’ajustement des parents à la maladie chronique de leur enfant sur
l’ajustement de l’enfant lui-même à sa propre maladie et réciproquement.
Cependant, ce modèle ainsi que de nombreuses études investiguant la
relation entre l’ajustement des parents et de l’enfant à la maladie chronique
se sont exclusivement centrés sur le rôle des mères (Dewey & Crawford,
2007; Hayes & Savage, 2008; Hodgkinson & Lester, 2002; Thompson &
Gustafson, 1996).
Par conséquent, la première partie de ce chapitre aura pour objectif de
présenter le modèle TSC développé par Thompson et al. (1992) ; ce modèle,
en plus du modèle de Leventhal et al. (1980), servira de cadre conceptuel au
présent travail de recherche. La deuxième partie de ce chapitre exposera la
problématique relative à la non-inclusion des pères dans les recherches en
pédiatrie et l’importance de considérer leur rôle dans l’ajustement de
l’enfant à la maladie chronique.

PARTIE THEORIQUE
- 118 -
1. Le modèle transactionnel du stress et du coping
(TSC) de Thompson et al. (1992)
Bien qu’initialement développé pour investiguer le rôle de l’ajustement
maternel et des processus cognitifs individuels sur l’ajustement
psychologique des enfants atteints de mucoviscidose (Thompson et al.,
1992), le modèle TSC s’applique à d’autres maladies chroniques de l’enfance
(Chaney et al., 1997; Colletti et al., 2008; Hocking & Lochman, 2005;
Thompson, Gil, Burbach, Keith, & Kinney, 1993; Thompson, Gustafson, & Gil,
1995). Dans ce modèle, la maladie chronique représente un facteur de
stress potentiel auquel l’enfant malade et sa famille tentent de s’adapter. La
relation maladie–ajustement n’est pas une relation directe ; les transactions
entre les caractéristiques de la maladie (ex. indice sévérité), les
caractéristiques sociodémographiques (ex. âge, sexe, niveau socio-
économique), les processus d’adaptation chez l’enfant et chez la mère
jouent un rôle de médiateur dans la relation entre la maladie et l’ajustement
à celle-ci (cf. Figure 1). Cependant, ce sont les processus d’adaptation qui
sont au centre du modèle ; ils sont considérés comme les principaux
médiateurs de la relation maladie–ajustement, plus que ne le sont les
caractéristiques biomédicales et sociodémographiques. Les processus
d’adaptation inclus dans le modèle TSC sont les suivants : (1) les processus
cognitifs : l’évaluation du stress, les attentes quant à l’efficacité du
traitement et le contrôle perçu ; (2) les stratégies de coping ; (3) le
fonctionnement familial. Le choix de ces derniers, à l’exception du
fonctionnement familial, a été guidé par la théorie cognitive du stress et du
coping de Lazarus et Folkman (1984). Ces processus d’adaptation
influencent respectivement l’ajustement de la mère et celui de l’enfant ; ces
derniers s’influençant de façon réciproque.

CHAPITRE 5 – FACTEURS PARENTAUX
- 119 -
Figure 1 – Le modèle transactionnel du stress et du coping (reproduction d’après Thompson, Gustafson, George, and Spock , 1994)
Processus cognitifs
(ex. évaluation du
stress, attentes en
termes d’efficacité et
de contrôle)
Paramètres
démographiques
(ex. âge et sexe de
l’enfant, niveau
socio-économique)
Paramètres de la
maladie (ex. nature,
sévérité)
AJUSTEMENT
MATERNEL
Strategies de
coping
Fonctionnement
familial
PROCESSUS D’ADAPTATION MATERNEL
PROCESSUS D’ADAPTATION CHEZ L’ENFANT AJUSTEMENT DE
L’ENFANT
Strategies de
coping
Processus cognitifs
(ex. attentes en termes
d’efficacité et de
contrôle)
†
†
† Relations étudiées dans le cadre de cette thèse de doctorat.

PARTIE THEORIQUE
- 120 -
L’ensemble du modèle n’a pas été pas testé dans le cadre de ce travail de
recherche ; seul le rôle des processus d’adaptation et de l’ajustement des
parents sur l’ajustement de l’enfant a été pris en considération. Plus
spécifiquement, sur base du modèle TSC, quatre variables ont été étudiées :
le stress parental et la perception de la maladie (cf. processus cognitifs du
modèle TSC), les stratégies de coping et le fonctionnement familial.
Le stress parental se définit comme le niveau de stress engendré par les
exigences associées au rôle de parent (Abidin, 2012). Des études ont
démontré qu’un niveau élevé de stress parental était associé à des
difficultés d’ajustement chez l’enfant atteint d’une maladie chronique (ex.
cancer, diabètes, asthme) (Colletti et al., 2008; Czyzewski, Mariotto,
Bartholomew, LeCompte, & Sockrider, 1994; Kazak & Barakat, 1997;
Mullins et al., 2007).
La perception de la maladie1 représente le développement de croyances
parentales sur la maladie de l’enfant en termes d’identité, de causes, de
chronologie, de conséquence et de contrôlabilité (cf. Leventhal et al., 1980).
Les études investiguant la relation entre la perception parentale de la
maladie et l’ajustement de l’enfant sont limitées. Deux études réalisées
auprès d’une population d’enfants asthmatiques mettent en évidence
qu’une perception négative de la maladie par le parent est associée à une
moindre QV des enfants (Chateaux & Spitz, 2005 ; Fonseca & Spitz, 2011).
Les stratégies de coping se réfèrent aux efforts cognitifs et
comportementaux mis en œuvre par l’individu pour faire face à une
situation stressante (Lazarus & Folkman, 1984). Peu d’études ont examiné
la relation entre les stratégies de coping des parents et l’ajustement de
l’enfant. De plus, ces études rapportent des résultats divergents. Certains
1 Bien que cette variable ne fasse pas partie intégrante du modèle TSC, elle
représente un processus cognitif et permet de garder une certaine cohérence
vis-à-vis des variables choisies chez l’enfant (ex. représentation cognitive de la
maladie – modèle d’autorégulation de Leventhal et al., 1980 ; Ch. 3).

CHAPITRE 5 – FACTEURS PARENTAUX
- 121 -
auteurs démontrent que les stratégies de coping des parents sont associées
à la QV des enfants atteints d’asthme (Sales, Fivush, & Teague, 2008) alors
que d’autres ne trouvent aucun lien entre les stratégies des parents et
l’ajustement de l’enfant atteint de cancer (Frank, Blount, & Brown, 1997).
Le fonctionnement familial est un élément important à considérer, étant
donné que la majorité du traitement des enfants atteints de mucoviscidose
a lieu à domicile. L’exigence des traitements associés à cette maladie
implique une certaine organisation de l’environnement familial (Herzer et
al., 2010). Il a été démontré que la cohésion familiale, l’expressivité et
l’organisation sont des éléments qui influencent positivement le
fonctionnement psychologique et l’ajustement de l’enfant atteint de
mucoviscidose (Szyndler, Towns, van Asperen, & McKay, 2005).
Comme le montrent les résultats ci-dessus, les études examinant le rôle
des facteurs familiaux sur l’ajustement des enfants atteints de
mucoviscidose sont minoritaires. De plus, aucune étude, à notre
connaissance, ne considère le rôle médiateur de l’ajustement des parents
sur la relation entre les processus d’adaptation de ces derniers et
l’ajustement de l’enfant atteint de cette pathologie. Ce manque de littérature
sur la relation entre les facteurs parentaux et l’ajustement des enfants en
âge scolaire atteints de mucoviscidose apporte un argument en faveur de
notre projet de recherche. Dans cette perspective, le modèle TSC offre une
assise théorique solide pour l’étude des facteurs contextuels familiaux
influençant l’ajustement de l’enfant à la maladie chronique. Cependant, ce
modèle présente l’inconvénient, comme beaucoup d’autres modèles ou
d’études sur l’ajustement à la maladie chronique, de ne pas considérer le
rôle des variables paternelles sur l’ajustement de l’enfant.

PARTIE THEORIQUE
- 122 -
2. Inclusion des pères dans la recherche en
pédiatrie
Il est largement admis que le contexte familial joue un rôle important
dans le développement de l’enfant. Bien qu’il existe une longue tradition de
recherche sur cette thématique, les études ont porté beaucoup moins
d’attention au rôle du père (Wilson & Prior, 2011); ce n’est que récemment
que les chercheurs ont déplacé leur intérêt de l’interaction mère-enfant à
d’autres aspects du système familial, à savoir l’interaction père-enfant et
l’influence du degré d’implication du père dans l’éducation sur le
développement normal de l’enfant. (Buckley & Schoppe-Sullivan, 2010;
Lamb, 2010). Cette attention portée aux pères émerge notamment en raison
du changement lié aux attentes relatives à leur rôle au sein de nos sociétés
modernes. Bien que la vision traditionnelle du père en tant que gagne-pain
de la famille continue d’exister (Hauari & Hollingworth, 2009), elle a
diminué et on leur reconnaît aujourd’hui un rôle beaucoup plus
large (Doucet, 2001; Dulac, 2000; Lamb, 2010; Pelchat, Lefebvre, &
Perreault, 2003; Traustadottir, 1991).
Par ailleurs, les études démontrent de nombreux avantages de
l’implication des pères sur le développement normal de l’enfant, et ce à tous
les stades du développement: des interactions père–enfant et père–
adolescent plus positives (Lamb, 2010) ; un meilleur développement
psychosocial dans l’enfance et une meilleure santé mentale à l’âge adulte
(Lamb, 2010) ; un niveau plus élevé de compétences cognitives, une
meilleure réussite scolaire (Flouri & Buchanan, 2004; McBride, Schoppe-
Sullivan, & Ho, 2005; Wilson & Prior, 2011), et une amélioration de la
réussite professionnelle à l’âge adulte (Lamb, 2010) ; de meilleures
compétences sociales se marquant par de meilleures interactions avec la
fratrie (Lamb, 2010; Volling & Belsky, 1992) et le groupe de pairs ainsi que
moins de difficultés d’ajustement à l’école (Lamb, 2010; Parke et al., 2002) ;

CHAPITRE 5 – FACTEURS PARENTAUX
- 123 -
moins de problèmes comportementaux (Flouri & Buchanan, 2003) ; et une
augmentation des responsabilités sociales, des capacités d’empathie, de
contrôle de soi, d’estime de soi, de maturité sociale (Lamb, 2010).
Le changement sociétal lié aux attentes relatives au rôle du père ainsi
que les bienfaits de leur implication sur le développement de l’enfant
donnent des arguments en faveur de la recherche sur cette thématique.
Cependant, les études considérant le rôle des pères sont encore une
minorité en comparaison à celles sur le rôle des mères (Dewey & Crawford,
2007; Hayes & Savage, 2008; Hodgkinson & Lester, 2002; Thompson &
Gustafson, 1996 ; Wilson & Prior, 2011). Ce constat est valable tant pour les
recherches sur développement normal de l’enfant que pour celles sur le
développement de l’enfant malade (ex. maladies chroniques). Ce
phénomène peut s’expliquer par diverses raisons : (a) les mères sont
généralement plus impliquées dans la gestion des soins de l’enfant et dans
les interactions avec l’équipe médicale (Eiser, 1993; Gray, 2003); (b) elles
passent généralement plus de temps que les pères à s’occuper des enfants
(Eiser, 1993; Hofferth, Pleck, Stueve, Bianchi, & Sayer, 2002); et (c) elles
sont plus accessibles aux chercheurs car ce sont souvent les mères qui
accompagnent leurs enfants aux visites à l’hôpital (Dewey & Crawford,
2007; Eiser, 1993). Il en résulte donc que les pères sont sous-investigués
dans les recherches en pédiatrie (Phares, Lopez, Fields, Kamboukos, &
Duhig, 2005).

PARTIE THEORIQUE
- 124 -
Résumé…
Le modèle TSC propose un cadre théorique permettant de comprendre,
au-delà des facteurs individuels propres à l’enfant, l’influence des facteurs
parentaux sur l’ajustement de celui-ci à la maladie chronique. Initialement,
ce modèle ne considère que l’influence des facteurs maternels sur
l’ajustement de l’enfant ; or, ce chapitre démontre l’importance de
l’inclusion des pères dans les recherches en pédiatrie. Ainsi pour mieux
comprendre comment les facteurs parentaux influencent l’ajustement de
l’enfant atteint d’une maladie chronique (ex. mucoviscidose), il est essentiel,
que ce soit en tant que clinicien ou en tant que chercheur, de porter son
attention non plus exclusivement sur le rôle des mères mais aussi sur celui
des pères (Ievers & Drotar, 1996; Phares et al., 2005). A partir de ce constat,
le modèle TSC a été adapté afin d’y inclure les variables paternelles (cf.
Figure 2). Cette adaptation du modèle TSC sert de cadre conceptuel à ce
travail de thèse pour l’évaluation de l’influence des facteurs parentaux sur
l’ajustement de l’enfant atteint de mucoviscidose (cf. Chapitre 11).

CHAPITRE 5 – FACTEURS PARENTAUX
- 125 -
Figure 2 – Adaptation du modèle transactionnel du stress et du coping (reproduction d’après Thompson et al., 1994)
Paramètres
démographique
s (ex. âge et sexe
de l’enfant, niveau
socio-
économique)
Paramètres de
la maladie (ex.
nature, sévérité)
AJUSTEMENT
MATERNEL
PROCESSUS D’ADAPTATION PARENTAL
(ex. Stress parental, perception de la
maladie, stratégies de coping)
PROCESSUS D’ADAPTATION CHEZ
L’ENFANT
AJUSTEMENT
DE L’ENFANT
AJUSTEMENT
PATERNEL


Chapitre 6
Objectifs de recherche


- 129 -
Chapitre 6 Objectifs de recherche (VERSION FRANÇAISE)
L’objectif de cette thèse de doctorat est d’étudier la QV des enfants
atteints de mucoviscidose en âge scolaire (8 à 12 ans). Cet objectif général
se décompose en quatre sous-objectifs qui sont répartis en deux parties.
PARTIE 1 : ETUDE DE VALIDATION
Le premier sous-objectif consiste en la validation d’un nouveau format
d’administration (version tablette) de l’outil de QV utilisé pour cette
recherche, l’Inventaire Systémique de Qualité de Vie pour Enfants (ISQV-
E©). Cette étude reflète notre volonté de créer un outil au format et au
design approprié à l’âge de l’enfant. Bien que l’ISQV-E offre déjà l’avantage
de tenir compte d’un certain nombre de considérations méthodologiques
énoncées au chapitre 2 (ex. fondement conceptuel et définition
opérationnelle de la QV – cf. Annexe 1 ; auto-évaluation ; approche
modulaire ; différentes formes ciblant différents groupes d’âge), ce travail
de thèse propose une amélioration du format original de l’outil (planche en
bois). Les qualités psychométriques du nouveau format de l’ISQV-E (version
tablette) ainsi que les avantages liés à l’utilisation d’un outil numérique
seront présentés au chapitre 8.
PARTIE 2 : ETUDES SUR LA QV
Le deuxième sous-objectif vise à investiguer le bien-être émotionnel (le
niveau d’anxiété-état et -trait et les symptômes dépressif) et la QV des
enfants atteints de mucoviscidose en comparaison à un groupe d’enfants
tout-venant. Cette étude est motivée par l’observation suivante : les

PARTIE THEORIQUE
- 130 -
informations concernant le bien-être psychologique des enfants en âge
scolaire atteints de cette pathologie sont limitées, surtout en comparaison à
un groupe contrôle. Bien que certaines études aient mis en évidence la
présence de symptômes dépressifs et d’anxiété chez ces enfants (Lawler,
Nakielny, & Wright, 1966; Teicher, 1969; Tropauer, Franz, & Dilgard, 1977),
la pertinence des résultats de celles-ci, datant de plus d’une trentaine
d’années, pose question à l’heure actuelle compte tenu des avancées
scientifiques (ex. traitement plus efficace). Plus récemment, seulement trois
études, à notre connaissance, ont examiné l’anxiété (Bregnballe, Thastum, &
Schiotz, 2007), les symptômes dépressifs (Bregnballe et al., 2007) et la QV
(Kianifar, Bakhshoodeh, Hebrani, & Behdani, 2013) des enfants atteints de
mucoviscidose en comparaison à un groupe contrôle. Ainsi, l’objectif de
cette deuxième étude, présentée au chapitre 9, est de réaliser un état des
lieux actuel des connaissances sur le bien-être émotionnel et la QV des
enfants atteints de cette pathologie.
Guidé par certaines considérations développementales, le troisième
sous-objectif de ce travail de recherche est d’examiner le rôle de certains
facteurs individuels sur la QV des jeunes patients atteints de mucoviscidose.
En effet, bien que la période de l’enfance soit caractérisée par d’importants
changements cognitifs (Ernst, Johnson, & Stark, 2010), la plupart des
contributions sur le développement du concept de maladie suggèrent que
les représentations de cette dernière sont incomplètes avant l’âge de 11-12
ans (cf. Chapitre 4). Sur base de ces informations, nous émettons
l’hypothèse qu’une représentation incomplète de la maladie entraînerait
des croyances erronées et des préoccupations infondées chez les enfants
atteints de mucoviscidose ; celles-ci pouvant jouer un rôle sur l’ajustement à
cette dernière (ex. QV). Ainsi, sur base du modèle de l’autorégulation de
Leventhal et al. (1980), le chapitre 10 investiguera l’influence des
représentations de la maladie (cognitives et émotionnelles), des stratégies
de coping et d’un critère d’ajustement intermédiaire (cf. bien-être

CHAPITRE 6 – OBJECTIFS
- 131 -
émotionnel) sur la QV des enfants atteints de mucoviscidose. Une
adaptation du modèle à une population pédiatrique sera également
proposée.
Enfin, les facteurs individuels ayant été étudiés, le quatrième sous-
objectif de cette thèse vise à examiner le rôle des facteurs
environnementaux sur la QV des enfants atteints de mucoviscidose. Parmi
ces facteurs, l’influence des variables parentales a reçu une attention
particulière. En effet, de nombreuses recherches en pédiatrie ont démontré
une relation entre l’ajustement des parents et celui de l’enfant (cf. Chaney et
al., 1997; Colletti et al., 2008; Hocking & Lochman, 2005). Cependant,
malgré cet engouement, le rôle des pères a été sous-investigué et l’inclusion
de ces derniers dans les études se révèle être, encore à l’heure actuelle, un
défi pour les chercheurs (Phares, Lopez, Fields, Kamboukos, & Duhig, 2005).
Ainsi, sur base du modèle transactionnel du stress et du coping de
Thompson et al. (1992), l’étude présentée au chapitre 11 examinera le rôle
des processus d’adaptation des pères ET des mères (stress parental,
représentations de la maladie et stratégies de coping) ainsi que de leur QV
sur celle des enfants atteints de mucoviscidose.


- 133 -
Chapter 6 Research objectives (ENGLISH VERSION)
The overall purpose of this research project is to examine quality of life
(QOL) in school-aged children with CF (8-12 years old). This objective spits
into four sub-objectives divided into two parts.
PART 1: VALIDATION STUDY
The first sub-objective aims to validate a new format (tablet version) of
the measure used to assess QOL in this research: the Quality of Life
Systemic Inventory for Children (QLSI-E©). This study is the result of our
will to create a better age-appropriate format of the tool. Despite the QLSI-E
offers many advantages considering methodological issues in pediatric
assessment (see chapter 2; conceptual framework and operationalized QOL
definition – see Appendix 1; self-report, modular approach, different forms
depending on age groups), this research project was the opportunity to
make improvements in regards the original format of the measure (wood
board). Psychometric properties of the QLSI-E’s new format (tablet version)
and the advantages of using a technology-based approach is presented in
chapter 8.
PART 2: QOL STUDIES
The second sub-objective aims to investigate emotional well-being (i.e.
state- and trait-anxiety, depressive symptoms) and QOL in school-aged
children with CF in comparison to a healthy control group. In general, data
on psychological well-being in children with CF are limited, especially in
comparison to a healthy control group. Although early researches found a

THEORY
- 134 -
high incidence of anxiety and depression in children with CF (Lawler,
Nakielny, & Wright, 1966; Teicher, 1969; Tropauer, Franz, & Dilgard, 1977,
relevance of these findings, over 30 years old, is questionable given the
advances that have been made in the medical treatment of CF. More
recently, only three studies, to our knowledge, examined anxiety
(Bregnballe et al., 2007), depressive symptoms (Bregnballe et al., 2007) and
QOL (Kianifar et al., 2013) in children with CF in comparison to a control
group. Therefore, the purpose of this study is to offers a state-of-the-art on
emotional well-being and QOL in pediatric CF (see chapter 9).
Guided by some developmental considerations, the third sub-objective
of this research project aims to examine the role of individual factors in QOL
of youths with CF. Although childhood is characterized by evolving
cognitive skills and knowledge (Ernst et al., 2010), most of the contributions
in children’ conceptualization of illness suggests that illness representation
of school-aged children is incomplete (see chapter 4). Based on this finding,
we hypothesized that incomplete representation at this age may lead to
possible misinformation and unfounded concerns about CF; which in turn
may impact children’s health outcome (i.e. QOL). Thereby, based on the
Common Sense Model of Self-Regulation (Leventhal et al., 1980), this study
examines the influence of illness representation (i.e. cognitive and
emotional), coping strategies and an intermediate emotional outcome (i.e.
emotional well-being) on QOL in school-aged children with CF (see chapter
10). An adapted model was also developed when applying in pediatric
populations.
Finally, individual factors being previously studied, the fourth sub-
objective aims to examine the role of contextual factors on QOL in youths
with CF. Since numerous studies have demonstrated the robust
transactional relation between parent and child adjustment (see Chaney et
al., 1997; Colletti et al., 2008; Hocking & Lochman, 2005), family contextual
factors have received a great deal of attention in this research project.

CHAPTER 6 – OBJECTIVES
- 135 -
However, fathers are underrepresented in pediatric research; most studies
examining almost exclusively the role of mothers. In addition, inclusion of
fathers in studies still poses considerable challenges for researchers
(Phares et al., 2005). Thus, guided by the Transactional Stress and Coping
Model (Thompson et al., 1992), this study examines whether adaptational
processes in mothers AND fathers (i.e. parenting stress, illness perception,
coping strategies) and parental QOL are related to the QOL in children with
CF (see chapter 11).


PARTIE 2
Méthodologie
Chapitre 7
Procédure de recrutement des différentes études


Chapitre 7
Procédure de
recrutement des
différentes études


- 141 -
Chapitre 7 Procédure de recrutement des différentes études
Comme mentionné dans le chapitre 6 (Objectifs de recherche), cette
thèse de doctorat se divise en deux parties : (a) la validation d’un nouveau
format (tablette) de l’outil de QV utilisé dans le cadre de cette recherche, à
savoir l’ISQV-E et (b) l’étude de la QV chez les enfants en âge scolaire
atteints de mucoviscidose. La phase de recrutement, initialement prévue en
Belgique, a été répliquée lors d’un séjour de recherche d’un an aux États-
Unis d’Amérique. Ainsi, la première partie de ce chapitre exposera la
méthodologie utilisée pour les diverses études réalisées en Belgique. La
deuxième partie, quant à elle, présentera les procédures de recherche
utilisées dans le cadre des études mises en place aux États-Unis d’Amérique.
1. En Belgique
1.1. Etude 1 : Validation d’un format tablette (iPad) de
l’ISQV-E (Touchèque et al., in press)
Contexte. Après de fructueuses discussions avec le groupe de recherche
interuniversitaire (Université de Liège en Belgique - l’Université de Lorraine
en France et Université du Québec à Montréal) sur l’ISQV-E, il a été décidé
que cette thèse était l’occasion d’améliorer l’outil en créant un nouveau
format de l’ISQV-E disponible sur tablette (cf. objectif 1 ; chapitre 6). Une
application pour tablette (iPad) a ainsi été développée avec l’aide d’un
informaticien et ensuite testée auprès d’une population d’enfants afin de
valider ce nouveau support.
Critère d’inclusion. Pour participer à l’étude : (1) l’enfant devait être
âgé entre 8 et 12 ans ; (2) l’enfant devait être francophone ; (3) l’enfant ne
devait pas présenter de problèmes de santé.

MÉTHODOLOGIE
- 142 -
Outils. Les participants ont dû compléter l’ISQV-E.
Procédure. Après avoir obtenu l’accord du comité d’éthique de
l’Université de Liège et celui de l’échevin de l’Instruction Publique de la ville
de Liège, différentes écoles primaires et secondaires de la province de Liège
ont été contactées ; sept d’entre elles ont accepté de participer à ce projet de
recherche. La procédure de recrutement consistait en la distribution, par les
écoles, de lettres d’information et de consentement éclairé à destination des
parents. Le formulaire de consentement devait être retourné à l’école en
communiquant leurs coordonnées téléphoniques et en précisant si oui ou
non les parents consentaient à la participation de son enfant à l’étude dans
un délai de 15 jours. Le chercheur contactait ensuite les parents ayant
donné leur accord afin de fixer un rendez-vous au domicile de l’enfant pour
l’évaluation de ce dernier. Après un intervalle de deux semaines, ces mêmes
enfants étaient à nouveau évalués mais uniquement pour établir la fidélité
test-retest de l’ISQV-E (20 min).
Cette étude de validation est en cours de publication dans une revue
anglophone : Psychological Assessment (cf. Ch 8.).
1.2. Etude 2 : QV des enfants atteints de mucoviscidose
Contexte. Cette étude a pour objectif d’examiner le bien-être
émotionnel et la QV des enfants atteints de mucoviscidose, en comparaison
à un groupe contrôle (cf. objectif 2 ; chapitre 6) ainsi que d’identifier le rôle
des facteurs individuels (cf. objectif 3 ; chapitre 6) et parentaux (cf. objectif
4 ; chapitre 6) sur la QV de ces enfants. Pour réaliser ces objectifs, deux
échantillons ont été collectés : a) des familles ayant un enfant atteint de
mucoviscidose et b) des familles ayant un enfant sans problèmes de santé.

CHAPITRE 7 – PROCÉDURE DE RECRUTEMENT
- 143 -
1.2.1. Etude 2.a : recrutement des familles ayant un
enfant atteint de mucoviscidose
Critères d’inclusion. Pour participer : (a) l’enfant devait porter le
diagnostic de mucoviscidose depuis au moins un an; (b) l’enfant devait être
âgé entre 8 et 12 ans ; (c) la mère ET le père de l’enfant devaient tous les
deux participer à l’étude – les parents séparés/divorcés étaient également
invités à participer à condition que chacun des deux parents aie des
contacts réguliers avec l’enfant ; (d) les participants devaient parler
français.
Outils. Le protocole de l’étude est présenté dans le Tableau 1.
Procédure. Quatre centres spécialisés pour la mucoviscidose en
Belgique et un centre en France ont été contactés : (1) le Centre
Mucoviscidose de Liège, collaboration entre le Centre Hospitalier Chrétien
(CHC) de l’Espérance et le Centre Hospitalier Régional (CHR) de la
Citadelle ; (2) le Centre Mucoviscidose (ULB) de l’Hôpital Universitaire des
Enfants Reine Fabiola (HUDERF) ; (3) le Centre Mucoviscidose de l’UZ
Brussel ; (4) le Centre Mucoviscidose des Cliniques Universitaires Saint-Luc
(UCL Bruxelles) et (5) le Centre Mucoviscidose du Centre Hospitalier
Régional Universitaire (CHRU) de Lille. Le centre de l’UCL n’a pas été en
mesure d’apporter son aide au projet en raison d’une restructuration du
personnel médical qui rendait difficile l’implication de l’équipe soignante
dans le processus de recrutement. Le centre de Lille avait donné son accord
pour participer au projet de recherche mais l’aboutissement de cette
collaboration n’a pas eu lieu en raison des complications liées aux comités
d’éthiques français (ex. lourdeur de la procédure administrative, long délai
de traitement des dossiers). Trois centres ont donc participé à cette
recherche : le CHC et CHR, l’ULB et l’UZ. Les accords auprès des comités
d’éthique de ces différents hôpitaux ont été obtenus dans les trois mois qui
ont suivi l’introduction des dossiers (date d’accord : 13 Mars 2012 ; Etude

MÉTHODOLOGIE
- 144 -
multicentrique ; numéro de protocole: B412201213307). Après l’obtention
de l’accord, tous les participants potentiels ont été informés du projet de
recherche via une lettre envoyée à l’ensemble des familles éligibles par leur
centre de référence. Les hôpitaux ont ensuite fourni au chercheur la liste
des familles qui rencontraient les critères d’inclusion. Toutes les familles
qui sélectionnées ont été contactées par le chercheur via un appel
téléphonique. Ceci dans le but de leur expliquer brièvement l’étude et leur
demander s’ils étaient intéressés de participer à ce projet de recherche. Une
visite à domicile était ensuite convenue avec les familles intéressées afin de
remplir les questionnaires. Lors de l’évaluation, les instructions étaient
dans un premier temps fournies aux parents afin qu’ils remplissent leurs
questionnaires de manière autonome pendant que le chercheur remplissait
les questionnaires avec l’enfant, dans une pièce séparée. Lorsque les
parents étaient tous les deux présents lors de l’évaluation, les
questionnaires de chaque participant étaient rendus en main propre au
chercheur le jour même de l’évaluation. Dans le cas d’un parent absent lors
du rendez-vous à domicile, le parent présent expliquait les consignes à
l’autre parent qui remplissait les questionnaires dans les jours qui suivaient
l’évaluation et les renvoyait ensuite au chercheur par courrier.

CHAPITRE 7 – PROCÉDURE DE RECRUTEMENT
- 145 -
Tableau 1 – Protocole de recherche des études 2.a et 2.b
Questionnaires PARENTS Auteurs – Version originale Auteurs – Traduction française
Parenting Stress Index Short form 4th
edition (PSI-4-SF)
Abidin (2012)
Touchèque, Etienne, Stassart, and Catale (in
press)1
Family Environment Scale (FES) Moos and Moos (1981) Auteur inconnu, disponible sur
http://www.mindgarden.com/96-family-
environment-scale#horizontalTab4 ou via
l’auteur de la version originale
Coping Health Inventory for Parents
(CHIP)
McCubbin et al. (1983)
Missotten, P. (non publié)
Brief Illness Perception Questionnaire
(BIPQ)*
Broadbent, Petrie, Main, and
Weinman (2006)
Auteur inconnu, publié sur :
http://www.uib.no/ipq/
Dad’s Active Disease Support (DADS) Wysocki and Gavin (2006) Touchèque, M. (non publié)
Inventaire Systémique de Qualité de
Vie (ISQV)
Dupuis et al. (1989) NA
*non inclus dans le protocole de recherche chez les familles du groupe contrôle
1 La validation française du PSI-SF 4e édition a été réalisée au cours de ce travail de recherche. L’article écrit a été accepté pour publication
en tant que « Brief report » et sera publié début 2016 dans « Journal of Community Psychology » (voir annexe 2).

MÉTHODOLOGIE
- 146 -
Tableau 1 (suite) – Protocole de recherche des études 2.a et 2.b
Questionnaires ENFANTS Auteurs – Version originale Auteurs – Traduction française
State Trait Anxiety Index for
Children (STAIC)
Spielberger, Edwards, Lushene,
Montuori, and Platzek (1973)
Turgeon and Chartrand (2003)
Child Depression Inventory (CDI) Kovacs & Beck (1977) – CDI-I
Kovacs (2010) – CDI-II
Mack and Morr (1982)
Children’s Illness Perception
Questionnaire (CIPQ) *
Walker, Papadopoulos, Lipton, and
Hussein (2006)
Touchèque, M. (non publié)
Kidcope Spirito, Stark, and Williams (1988) Touchèque, M. (non publié)
Learning Experience Questionnaire
(LEI) **
Muris, Merckelbach, and Meesters
(2001)
Stassart, C. (non publié)
Inventaire Systémique de Qualité de
Vie pour Enfants (ISQV-E©)
M. Touchèque et al. (in press) – version
tablette
NA
* Non inclus dans le protocole de recherche chez les familles du groupe contrôle
** Le LEI était inclus dans le protocole de recherche en Belgique. Cependant, le protocole a dû être réévalué afin d’optimiser la phase
de recrutement aux USA. En effet, l’évaluation ayant lieu lors des visites de routine à l’hôpital, la LEI a été retiré afin de réduire le
temps de passation.

CHAPITRE 7 – PROCÉDURE DE RECRUTEMENT
- 147 -
1.2.2. Etude 2.b : recrutement des familles ayant un
enfant sans problème de santé
Critères d’inclusion. Pour participer : (a) l’enfant ne devait pas
présenter de problèmes de santé ; (b) l’enfant devait être âgé de 8 à 12 ans ;
(c) la mère et le père de l’enfant devaient tous les deux participer à l’étude –
les parents séparés/divorcés étaient également invités à participer à
condition que chacun des deux parents aie des contacts réguliers avec
l’enfant ; (d) les participants devaient parler français.
Outils (idem étude 2.a). Le protocole de l’étude est présenté dans le
Tableau 1.
Procédure (idem étude 1). Les familles ayant donné leur accord pour
participer ont été recrutées sur base d’un appariement selon l’âge et le sexe
des enfants de l’étude 3.a. Un rendez-vous au domicile de la famille était fixé
afin de compléter les questionnaires.
2. Aux États-Unis d’Amérique
Contexte générale du séjour de recherche aux USA. La phase de
recrutement de l’étude 2 ayant abouti à un faible échantillon (n=20
familles), un séjour à l’étranger d’une durée d’un an a été envisagé afin
d’augmenter la taille de l’échantillon et ainsi, favoriser la publication
scientifique de nos études. Ce séjour a également permis d’introduire une
dimension culturelle au projet de recherche en repérant les spécificités
propres à chaque culture (Belge vs Américaine) en termes de gestion et de
vécu de la maladie par l’enfant et ses parents. Ce séjour de recherche a
débuté le 1er Octobre 2013 à West Virginia University (WVU) au sein du
laboratoire de psychologie pédiatrique dirigé par le Dr. Christina Duncan.
Lors de ce séjour, au-delà des bénéfices liés au recrutement, il m’a été offert
l’opportunité de participer aux activités académiques de l’université
d’accueil (ex. présentations de cas cliniques, conférence, etc.), d’assister à

MÉTHODOLOGIE
- 148 -
différents cours (ex. « Evidence-based therapy in children and adolescents »),
de participer à l’écriture d’articles scientifiques en collaboration avec le
laboratoire de recherche et d’assister à des conférences internationales
(Touchèque, 2014).
2.1. Etude 3 : Validation d’une version anglaise de
l’ISQV-E format tablette
Contexte. Ce séjour de recherche représentait une belle opportunité de
valider le nouveau format tablette de l’ISQV-E en une version adaptée à une
population anglophone. Bien que cette étude de validation ne faisait pas
partie des objectifs de départ de ce séjour, elle s’est progressivement mise
en place suite à diverses réflexions lors de réunions d’équipe à WVU et avec
l’accord du Dr. Anne-Marie Etienne, promotrice de thèse.
Critères d’inclusion. Pour participer à l’étude : (1) l’enfant devait être
âgé entre 8 et 12 ans ; (2) l’enfant devait parler anglais ; (3) l’enfant ne
devait pas présenter de problèmes de santé.
Outils. Le protocole utilisé est présenté dans le tableau 2.
Procédure. La méthodologie de recherche a été soumise à l’Insitutional
Review Board (IRB) de WVU (accord le 22 Août 2014 ; numéro de protocole:
1311126057). Le recrutement a eu lieu au sein de trois écoles de l’état de
Virginie-Occidentale. La procédure consistait en la distribution, par les
écoles, de lettres d’information et de consentements éclairés à destination
des parents. Le formulaire de consentement devait être retourné à l’école en
précisant si oui ou non les parents consentaient à la participation de son
enfant à l’étude. Après réception des formulaires et l’estimation du nombre
d’enfants à évaluer, plusieurs journées de recrutement ont été
programmées dans les écoles afin de compléter les questionnaires. Lors de
ces journées, les élèves dont les parents avaient donné leur accord, étaient
appelés par groupe de deux afin de leur présenter l’étude, de compléter le

CHAPITRE 7 – PROCÉDURE DE RECRUTEMENT
- 149 -
formulaire de consentement et les questionnaires. Trois chercheurs étaient
présents à trois endroits différents de l’école. A l’arrivée des deux étudiants,
chacun d’entre eux se rendait auprès d’un chercheur afin de compléter le
formulaire de consentement ainsi que les questionnaires nécessitant d’être
remplis individuellement. Ensuite, les deux étudiants se déplaçaient à la
troisième table afin de compléter le reste des questionnaires qui pouvait
être administrés en groupe. Au même moment les deux élèves suivants
entraient dans la pièce, et ainsi de suite. L’évaluation durait
approximativement 45 min : 25 min en individuel et puis 20 min en groupe.
Après un intervalle de deux semaines, ces mêmes enfants étaient à nouveau
évalués mais uniquement pour établir la fidélité test-retest de l’ISQV-E (20
min).
Tableau 2 – Protocole de recherche pour l’étude 2
State-Trait Anxiety Inventory for Children (STAIC)*
Children’s Depression Inventory 2 (CDI-II)*
Pediatric Quality of Life Inventory (PedsQL)*
Trail Making Task (TMT)**
Quality of Life Systemic Inventory for Children (QLSI-C©)**
*Questionnaires complétés en individuel
**Questionnaires complétés en groupe
Ces données n’ont pu être exploitées telles quelles pour une étude de
validation en raison de son faible échantillon. Cependant, une partie de ces
dernières (STAIC, CDI-II et ISQV-E) a été utilisée afin de constituer un
groupe contrôle pour l’étude 4.b. L’autre partie des données récoltées (TMT
et PedsQL) n’a pas pu être utilisée dans le cadre de ce projet de recherche.

MÉTHODOLOGIE
- 150 -
2.2. Etude 4 : QV des enfants américains
2.2.1. Etude 4.a : Recrutement des familles ayant un
enfant atteint de mucoviscidose
Critères d’inclusion. Pour participer : (a) l’enfant devait porter le
diagnostic de mucoviscidose depuis au moins un an; (b) l’enfant devait être
âgé entre 8 et 12 ans ; (c) la mère et le père de l’enfant devaient tous les
deux participer à l’étude – les parents séparés/divorcés étaient également
invités à participer à condition que chacun des deux parents aie des
contacts réguliers avec l’enfant ; (d) les participants devaient parler anglais.
Outils. Le protocole utilisé est présenté dans le tableau 1.
Procédure. Trois hôpitaux ont été contactés: (1) WVU’s Mountain State
Cystic Fibrosis Center (Morgantown, WV), (2) The OU Cystic Fibrosis Center
at Children’s Hospital of Oklahoma City et (3) The Antonio J. and Janet
Palumbo Cystic Fibrosis Center at Children’s Hospital of Pittsburgh. Suite à
un changement survenu dans la réglementation de l’hôpital concernant la
venue de chercheurs ou étudiants externes à des fins d’observation ou
d’expérimentation, l’hôpital d’Oklahoma n’a pas été en mesure d’apporter
son aide à ce projet de recherche. Deux hôpitaux ont donc participé à cette
recherche : ceux de WVU et de Pittsburgh. Après avoir obtenu l’accord de
ces derniers, les démarches relatives des comités d’éthique ont été
entamées. La règlementation relative au comité d’éthique des USA diffère de
celle de la Belgique. Aux USA, il n’y a pas de dossier à remettre pour chaque
hôpital ou Université participante. Un seul dossier doit être rempli via une
plateforme en ligne et envoyé à l’Institutional Review Board (IRB) de
l’Université de l’étudiant, à savoir WVU. Les différents hôpitaux participants
doivent signer un accord qui doit être ensuite téléchargé sur la plateforme.
Une fois l’accord de tous les hôpitaux participants téléchargé et le dossier
en ligne rempli, l’IRB de l’Université se charge de réviser le projet de

CHAPITRE 7 – PROCÉDURE DE RECRUTEMENT
- 151 -
recherche. En raison de la lourdeur de la procédure de soumission du
dossier à l’IRB, l’accord pour débuter le recrutement a été donné en date du
3 Mai 2014 (étude multicentrique ; numéro de protocole : 1310112099).
Après obtention de l’accord par l’IRB, le recrutement des familles, lors des
visites de routine dans leur centre pour la mucoviscidose, a débuté. Dans un
premier temps, les familles étaient approchées par leur médecin qui leur
expliquait brièvement l’étude et leur proposait de rencontrer le chercheur
et son assistant (undergraduate student de WVU) pour discuter plus en
détails de l’étude. Les familles ayant marqué leur accord étaient ensuite
vues par les chercheurs afin que leur soient fournies les explications
complètes de l’étude et afin de leur proposer de participer. Deux possibilités
étaient offertes aux familles qui acceptaient de participer : soit ils
remplissaient les questionnaires sur place, le jour-même, soit ils les
remplissaient lors de leur prochaine consultation (2-3 mois plus tard) s’ils
n’étaient pas disponibles en ce premier jour. Peu importe l’option choisie,
l’évaluation avait lieu au centre lors d’une visite de routine. L’assistant se
chargeait de fournir les instructions aux parents afin qu’ils remplissent
leurs questionnaires de manière autonome pendant que le chercheur
remplissait les questionnaires avec l’enfant, dans une pièce séparée.
Lorsque les parents étaient tous les deux présents, les questionnaires de
chaque participant étaient rendus en main propre au chercheur le jour de
l’évaluation. Dans le cas d’un parent absent lors du rendez-vous, le parent
présent reprenait les questionnaires à domicile et expliquait les consignes à
son conjoint (ou ex-conjoint). Celui-ci remplissait ensuite les questionnaires
dans les jours suivants l’évaluation et les renvoyait finalement au chercheur
par courrier.

MÉTHODOLOGIE
- 152 -
2.2.2. Etude 4.b : Recrutement des familles ayant un
enfant sans problème de santé
Contexte. Le timing étant trop court, le recrutement des familles ayant
un enfant sain n’a pas été réalisé au cours du séjour de recherche à WVU.
Cependant, les enfants recrutés dans le cadre de l’étude 1 ont été appariés
selon l’âge et le sexe aux enfants de l’étude 4.a afin de constituer un groupe
contrôle.
Outils et procédure (idem étude 3). Le protocole de l’étude est
présenté dans le Tableau 2. Seules les échelles d’anxiété, de symptômes
dépressifs et de QV ont été utilisées dans le cadre de cette étude 4.b.



PART 3
Research studies
Chapter 8
A comparison of a tablet version of the Quality of Life Systemic Inventory
for Children (QLSI-C) to the standard paper version
Chapter 9
Anxiety, depression and quality of life in school-aged children with Cystic
Fibrosis: A cross-cultural study
Chapter 10
Applying the Common-Sense Model of Self-Regulation to Pediatric Cystic
Fibrosis: Identifying Psychosocial Factors Associated with Quality of Life
Chapter 11
Parenting stress, parental illness perception and coping strategies
associated with Quality of life in children with Cystic Fibrosis: the mediating
role of parental adjustment


Chapter 8
A comparison of a tablet version
of the Quality of Life Systemic
Inventory for Children (QLSI-C)
to the standard paper version
Touchèque, M., M.A., Etienne, A.-M., PhD., Missotten, P., PhD., & Dupuis, G,
PhD. 1
1 Touchèque, M., Etienne, A.-M., Missotten, P., & Dupuis, G. (2015). A
comparison of a tablet version of the Quality of Life Systemic Inventory for
Children (QLSI-C©) to the standard paper version. Psychological Assessment,
27(4).

RESEARCH STUDIES
- 158 -
Abstract
Integration of e-Health technologies for purposes of both assessment and
intervention has recently become an interest area in pediatric psychology. The
purpose of this study is to present psychometric characteristics of a
technology-based (i.e., tablet administration) approach for measuring quality of
life (QOL) in children. Eighty children (8-12 years) completed the Quality of Life
Systemic Inventory for Children (QLSI-C©) twice over a two-week delay, in a
crossover design that used paper and tablet-based modes of administration.
Equivalence of scores across methods was examined using Intraclass
correlation coefficients (ICC), augmented by paired t-test and Pearson’s
correlations. Test-retest reliability was assessed using paired t-test and
Pearson’s correlations while internal consistency was assessed using
Cronbach’s coefficient. Results showed a good concordance across methods of
administration (ICCs = .72 to .91; r = .56 to .83). Paired t-test showed no
significant differences between the tablet and paper version of the QLSI-C.
Internal consistency reliability yielded acceptable Cronbach’s alphas for all
QLSI-C scores, with all α >.70. Test-retest reliability for the tablet-administered
QLSI-C was good (r = .66 to .90). Paired t-test showed no significant difference
between time 1 and 2 for the QLSI-C scores, except for the state score. Findings
established the reliability of the tablet-administered QLSI-C scores. This
technology approach to assessment is more attractive for children, decreases
time for administration, and enhances the ease of scoring. These advantages
might encourage both clinicians and researchers to consider using e-Health
developments in assessment in pediatric psychology.
Keywords: Assessment; quality of life; reliability; technology-based
questionnaire; children.

CHAPTER 8 –VALIDATION OF THE TABLET-ADMINISTERED QLSI-C
- 159 -
1. Introduction
In the past two decades, various evaluation methods have been
employed to assess quality of life (QOL) and health-related quality of life
(HRQOL) in pediatrics: self- versus proxy-report questionnaires and generic
versus specific tools. Use of self- versus proxy-report questionnaires have
been broadly debated in clinical pediatrics and child health research
(Etienne et al., 2011; Riley, 2004). Literature indicates that children as
young as 6 years old can successfully report valuable information about
their own health (Abbott & Gee, 2003; Riley, 2004). However, QOL of
school-aged children is relatively under-investigated (Raat,
Mangunkusumo, Landgraf, Kloek, & Brug, 2007; J. L. Wallander & Varni,
1998). Use of generic versus specific QOL tools is also a controversial issue.
Generic instruments are designed to be applicable to all population
subgroups, it can be used to measure (and compare) QOL for numerous
chronic illnesses; however, they may not be sensitive to particular aspects
of the disease. Unfortunately, disease-specific measures cannot be used to
compare results across diseases or conditions (G. H. Guyatt & Jaeschke,
1990; Tian-hui, Lu, & Michael, 2005). Thus, a modular perspective is more
and more encouraged to combine advantages of both usual tools (generic
and specific) (Eiser & Jenney, 2007; Eiser & Morse, 2001c; Missotten et al.,
2007).
Most of QOL (self- and proxy-report; generic and specific)
questionnaires estimate this concept as a current state (i.e. How I feel about
my health, for example in the past two weeks) without considering the
child’s expectations (i.e. How I would like to feel in the future) and the
child’s evaluation of life priorities (individual perception of the importance
of each life domains) (Missotten et al., 2007). However, the World Health
Organization’s QOL definition goes beyond the single concept of current
state; it represents “an individual’s perception of their position in life in the

RESEARCH STUDIES
- 160 -
context of the culture and value systems in which they live and in relation to
their goals, expectations, standards and concerns. It is a broad ranging
concept affected in a complex way by the person’s physical health,
psychological state, level of independence, social relationships, and their
relationship to salient features of their environment.” (WHOQOL Group,
1993)(p.153). Therefore, it would be important to include these notions in
child-focused measures of QOL.
Based on these shortcomings, the Quality of Life Systemic Inventory for
Children (QLSI-C©) (Etienne et al., 2011) was developed. The QLSI-C is a
self-report measure of QOL, based on a modular approach, appropriate for
children aged 8 to 12 years that considers QOL as the difference between
the current state and the child’s expectations, weighted by the importance
assigned for each life domain. The theoretical model behind the QLSI
(Dupuis et al., 1989) were inspired by the systemic approach on biologic
systems and cybernetics and the definition of the QOL were based on the
notion of discrepancy and the Aristotelian notion of happiness. In this
model, all human activities are oriented towards an end (a goal), that
certain ends are subordinated to others but that the ultimate end is the
pursuit of happiness (G. Dupuis et al., 2000). Thus, Dupuis et al. (1989)
have defined QOL as follow: ‘‘QOL is, at a given time, a state that
corresponds to the level attained by a person in his pursuit of hierarchically
organized goals’’.
Data from the original QLSI-C, as from other (HR)QOL questionnaires,
are traditionally collected on paper format but integration of e-Health
technologies for purposes of assessment has recently become an interest
area in pediatric psychology (Ritterband & Palermo, 2009). Most of
technology-based QOL measures for children use an online mode of
administration (PedsQL, Exeter HRQL, KIDSCREEN-27, etc.) whereas
development of application for Androids for assessment purposes is rare.
The development of a tablet format of the QLSI-C was preferred in a web-

CHAPTER 8 –VALIDATION OF THE TABLET-ADMINISTERED QLSI-C
- 161 -
based mode of administration for the following reasons: (1) the touch
screen is more attractive, especially for children; (2) no need to have
internet access; (3) a tablet is easier to carry, especially in the context of
data collection in hospitals or at home. Further, most of health-related
questionnaires using technology (i.e. computer questionnaire) are self-
administrated mode of data collection (Raat, Mangunkusumo, Landgraf, et
al., 2007; Vallejo, Jordán, Díaz, Comeche, & Ortega, 2007; Young et al., 2009).
In contrast, the QLSI-C preferred a face-to-face interview method. This
mode of administration demonstrated a better data quality in comparison
to self-administration (Bowling, 2005). First, motivation to respond and
give an accurate respond can be enhanced by the interviewer. Second, face-
to-face interview is the least burdensome method for the respondents.
Third, interviewers have a higher control over the questionnaire. Fourth,
interactions between respondent and interviewer are enhanced and thus,
more information may be obtained in face-to-face interview than other
situations (Bowling, 2005). Thus, the new tablet format of the QLSI-C
combines advantages of the usual face-to-face interview with a mode of
administration using technology.
The purpose of this study is to examine the score equivalence between
the QLSI-C modes of administration and assess the reliability of the tablet-
administered QLSCI-C scores in order to replace the original format by the
tablet format.
2. Method
2.1. Participants and study design
Children were recruited from seven elementary schools in the area of
Liège (Belgium). To be included, children had to be: (a) 8 to 12 years of age;
(b) French-speaking; (c) and without a chronic illness, injury, or health
condition. The total sample consists of 80 children (40 girls and 40 boys)

RESEARCH STUDIES
- 162 -
aged 8 to 12 years (M=9.75; SD=1.53). Majority of children came from a
rural environment (n=70). Among the seven elementary schools which
participated to the study, three schools were located in an urban
environment (295 potential children) and four were located in a rural
environment (430 potential children). Nine percent of the total sample
reported that they never used a tablet (n=7). When analysed by preference
of mode of administration, 58% have no preference (n=23), 40% preferred
the tablet format (n=16) and only 2% preferred the paper format (n=1).
Children were approached at their school by the distribution of
newsletters for their parents. When parents consented their child’s
participation, the research assistant contacted them to schedule a home
visit. Children were required to complete the Quality of Life Systemic
Inventory for Children (QLSI-C©) twice over a two week delay, in a
crossover design that used paper and tablet-based modes of administration.
Children were randomly assigned to one of four groups: 25% of the sample
used tablet formats at both time (group 1); 25% used tablet format and
then paper format (group 2); 25% used paper format and then tablet format
(group 3); and 25% used paper formats at both time (group 4). The ration
of males to females is relatively equal within the four groups. This random
assignment of 20 children per group was based on a priori power analyses
(Faul, Erdfelder, Buchner & Lang, 2009). According these analyses, a sample
size of 20 was adequate to give the study a power of 80 to detect medium to
large effect sizes when comparing means (Cohen’s d = .67) or using
correlations (Cohen’s q = .56).
2.2. Measures
Quality of Life Systemic Inventory for Children (QLSI-C©); paper
version (Etienne et al., 2011). QLSI-C is an assessment tool of QOL based
on a modular approach for children 8 to 12 years aged. The generic scale

CHAPTER 8 –VALIDATION OF THE TABLET-ADMINISTERED QLSI-C
- 163 -
consists on a 20-items scale representing life domains of children. Specific
modules of six additional items (e.g. (Touchèque & Etienne, 2013) can be
added to the generic scale. Each domain is presented in both words and
pictures and the response sheet consists of three wooden boards.
The first board is a Visual Analog Scale representing a circle from the
best possible situation to the worst possible situation. For each item, the
child uses a full arrow to indicate on the circle his/her current state (“how
happy are you NOW?”) and a dotted arrow to indicate his/her personal goal
(“Where would you like to be?”). These arrows are positioned in reference
to the ideal situation (i.e. to be perfectly happy with my health) which is at
the same place on the circle for everyone. On the second board, the child
indicates whether she/he thinks that, in the last few days, her/his current
situation has been stable or is moving closer to or away from the ideal
situation. If the situation is improving or deteriorating, the child has to
specify the speed of improvement or deterioration and choose between the
following possibilities: a walker (=very slowly), a cyclist (=slowly), a car
(=quickly) or a plane (=very quickly).On the third board, the child indicates,
on a 7-point Likert scale, how important each domain is to her/him from
“essential” to “not important at all”.
Four overall scores are calculated: state, goal, rank and gap. The state
score is the difference between the current situation and the ideal situation;
a high score indicates that the current situation is far from the ideal. The
goal score is the difference between expectations and the ideal situation; a
high score indicates that the desired situation is far from the ideal. The rank
score reflects the priorities assigned to each life domain; a high score
indicates difficulties prioritizing life domains. The gap score, representing
the score of QOL, is the difference between the present situation (state) and
the child’s expectations (goal), weighted by the speed of improvement and
deterioration and the importance (rank) assigned for each life domains; a

RESEARCH STUDIES
- 164 -
low score reflects a better QOL. The QLSI-C has good reliability and validity,
with alphas for each score ranging from .71 to .92 (Etienne et al., 2011).
Quality of Life Systemic Inventory for Children (QLSI-C©); tablet
version. An App of the QLSI-C on a tablet computer has been developed.
The App that we developed is only available for iPads (Apple product) but
we would like to extend it to other tablets in the future. Each domain of the
QLSI-C is still presented in both words and pictures but the child answers
on the tablet (see Figure 1) instead of answering on three wooden boards.
Children slide their finger on the tablet to place arrows on the circle and
choose the speed of improvement or deterioration and the importance of
the domain. They can change the position of the arrows and their answers
as many times as they wish. Children can also go back to a previous
question if they want to change their answers afterwards. Note that the
design of the response sheet on tablet sticks to the design of the wooden
boards. Instructions and scoring for the tablet version are the same as the
paper version, except for the rank score. As a reminder, this score reflects
the priorities assigned to each life domain and was rated using a 7-point
Likert scale. On the tablet version, the child rates each domain using a 5-
point Likert scale instead of 7. Researchers who developed the QLSI-C
noticed that children had difficulties to understand the difference between
the three last possibilities of the 7-point Likert scale (less important – not
important – not important at all) and suggested to modify the Likert scale
from 7 to 5-point for the new format. Thus, we remove the three last
options and replace them by one option only (“not very or not important”).
Note that we standardized the paper and the tablet format using a 5-point
Likert scale in the analyses for both mode of administration. Once children
have finished the questionnaire, they validate to save the data on the tablet.
Then, results in a excel file are exported from the tablet to an email address.
Finally, results from the excel file can be copy/paste in the scoring sheet.

CHAPTER 8 –VALIDATION OF THE TABLET-ADMINISTERED QLSI-C
- 165 -
Figure 1 – The tablet-administered QLSI-C: Item 1
2.3. Statistical analysis
Analyses were performed using a statistical program (SPSS 20.0) (IBM
Corp., 2011). Equivalence of scores across method of administration was
examined using Intraclass correlation coefficients (ICC), augmented by
paired t-test and Pearson’s correlations. Test-retest reliability was assessed
using paired t-test and Pearson’s correlations while internal consistency
was assessed using Cronbach’s coefficient. The Fisher-Bonett test was used
to compare alpha levels across method. Level of significance was set at p
<.05. Note that six outliers from group 2 and 3 were excluded from the
subsequent analyses based on regression diagnostics and other indices
(standard errors, Cook’s Distance and residual).

RESEARCH STUDIES
- 166 -
3. Results
3.1. Score equivalence
ICCs between methods of administration were high, ranging from .72
and .91, for the all QLSI-C scores (i.e. (Cicchetti, 1994). Paired t-test showed
no significant differences in mean score between paper and tablet format
and Pearson correlations between methods were moderate to high, ranging
from .56 to .83 (See Table 1).
3.2. Internal consistency reliability
Both paper and tablet administration yielded acceptable Cronbach’s
alphas for all scores, with all α >.75 (i.e. (Nunnally & Bernstein, 1994).
Cronbach’s alphas for the scores of the paper version (n=40) were: state: α
= .89, goal: α = .91, rank: α = .82, gap: α = .77. Cronbach’s alphas for the
scores of the tablet version (n=39) were: state: α = .87, goal: α = .92, rank: α
= .79, gap: α = .80. Cronbach α comparison using the Fisher-Bonett test
based on Kim and Feldt (2008) showed no significant differences between
the group that completed the paper version of the QLSI-C and the group that
completed the tablet version.
3.3. Test-retest reliability
Table 2 presents results of the test-retest reliability analysis for the
tablet-administered QLSI-C scores. QLSI-C scores of the tablet version
demonstrated good test-retest reliability. However, despite a high test-
retest correlation (r = .90), we found a significant difference between time 1
and 2 for the state score (i.e. child’s current situation). As regard with the
paper version, Pearson correlation coefficients between scores suggested
good test-retest reliability (state: r = .70; goal: r = .87; gap: r = .64; rank: r =

CHAPTER 8 –VALIDATION OF THE TABLET-ADMINISTERED QLSI-C
- 167 -
.73). No significant difference in means exists between time 1 and 2 for the
paper-administered QLSI-C scores.
4. Discussion
The purpose of this study was to compare the tablet-administered QLSI-
C with its original paper version. Scores derived through paper and tablet
administration were comparable, with high correlations and no difference
between methods. The good concordance of the QLSI-C scores across
methods of administration establishes the score equivalence of the tablet-
administered QLSI-C in comparison to the original paper format. All
Cronbach’s alpha exceeded .70 suggesting a good internal consistency of the
tablet-administered QLSI-C scores. In addition, comparison in alpha levels
showed no differences between methods of administration. Test-retest
analyses for the tablet-administered QLSI-C demonstrated stability over
time for the goal, gap and rank scores. However, we found a difference
between time 1 and 2 for the state score, suggesting that the children’s
current situation has changed within two weeks. This phenomenon may be
explained by an observation we have made during face-to-face interviews
with children suggesting that children’s perception of well-being can
quickly change depending on everyday life events (e.g. being bothered by
sibling, eating something he/she doesn’t like, etc.). Moreover, although most
of QOL questionnaires, including the QLSI-C, assess the well-being of the
child in the past two weeks or months, we observed that it is recent events
(i.e. from the same day or the day before) that make a difference in how
children respond to the QLSI-C. Thus, it might be difficult for children to
answer questions considering their overall mood of the past few weeks
without being focused on events of the day only. This phenomenon can
especially be an issue with questionnaires assessing QOL as a current state.

RESEARCH STUDIES
- 168 -
Table 1 - Equivalence of scores across method of administration
N† Mean
differences
(SD)
95% CI* Paired
t-test
p-
value
Cohen’s d
[95% CI]
Pearson
r**
Intermethod
ICCs***
QLSI-C state 34 -0.39 (7.58) [-3.03 – 2.26] -.298 .768 .04 [-2.34 – 2.42] .72 .84
QLSI-C goal 34 0.22 (3.44) [-.97 – 1.42] .383 .704 .04 [-1.35 – 1.42] .83 .91
QLSI-C rank 34 0.01 (0.17) [-.05 – .07] .265 .792 .05 [-0.01 – 0.10] .60 .76
QLSI-C gap 34 -0.08 (1.17) [-.49 – .32] -.413 .683 07 [-0.23 – 0.36] .56 .72 † Six outliers from group 2 and 3 were excluded.
*95% Confidence Interval Estimates for mean differences
**All p<.001
***Two-way mixed; absolute agreement
Table 2 - Two-week test-retest reliability of the tablet- administered QLSI-C
N Tablet T1
Mean (SD)
Tablet T2
Mean (SD)
95% CI* Paired
t-test
p-
value
Cohen’s d
[95% CI ]
Pearson
r**
QLSI-C state 20 15.38 (11.58) 11.64 (9.56) [1.36 – 6.11] 3.288 .004 .36 [-2.85 – 3.57] .90
QLSI-C goal 20 7.59 (6.55) 6.26 (6.64) [-.97 – 3.63] 1.211 .241 .21 [-1.79 – 2.20] .72
QLSI-C rank 20 1.59 (0.16) 1.61 (0.18) [-.09 – .05] -.641 .529 .12 [0.07 – 0.17] .66
QLSI-C gap 20 2.55 (4.52) 2.38 (6.13) [-1.91– 2.26] .175 .863 .03 [-1.59 – 1.66] .69
*95% Confidence Interval Estimates for mean differences
**All p<.001

CHAPTER 8 –VALIDATION OF THE TABLET-ADMINISTERED QLSI-C
- 169 -
As a result, it might be important to consider, when assessing children’s
well-being, to first briefly assess their day mood, including recent events,
which may influence their well-being at the time of the assessment.
Overall, results from this study provided support for the reliability of
the tablet –administered QLSI-C scores. Our findings confirm the results of
previous studies that have demonstrated good psychometric properties of
online-administered questionnaires scores in school-aged children and
adolescents in comparison to their original paper version using the
Activities Scale for Kids (ASK) and the Pediatric Quality of Life Inventory
(PedsQL) (Young et al., 2009), the Child Health Questionnaire – Child Form
(CFQ-CF) (Raat, Mangunkusumo, Landgraf, et al., 2007), the Asthma and
Fruit Questionnaire (Mangunkusumo et al., 2006), the KIVPA,
(Mangunkusumo et al., 2005) and respiratory questionnaires (Raat,
Mangunkusumo, Mohangoo, Juniper, & Van Der Lei, 2007).
Strength of the current study is the application of a randomized
crossover design that allows the comparison of indicators of reliability at
both group and individual level (Garcia, Benet, Arnau, & Cobo, 2004).
Interval time between the two assessments was long enough to allow the
participant to forget all previously provided answers at the second
assessment. Moreover, based on a priori power analyses (see Method), the
sample size was sufficient to address the research questions about score
equivalence between administration modes and reliability of the tablet-
administered QLSI-C scores. However, generalization of findings from our
research is limited. First, post hoc power analyses (Faul, Erdfelder, Buchner,
& Lang, 2009) showed that our study is underpowered given our actual
sample size and effect sizes. Nevertheless, given the small effect sizes
reported in this study, to yield a power of 0.8, we would need more than a
thousand participants to detect small inter- and intra- method differences
which would suggest low practical significance. Second, because response
rates were low and most children who participated in the study came from

RESEARCH STUDIES
- 170 -
a rural environment, this research do not allow us to presume that our
achieve sample is representative of the French-speaking children in
Belgium. The overall low completion rates in this study may be explained by
the fact that reasons for participating were altruistic; no financial payment
or compensation was provided to participants in this research. However, it
has been showed that financial payment was the most important motivator
for healthy volunteer studies (Chang, Hendricks, Slawsky, & Locastro,
2004). Another possible explanation for low response rates is that parents
are often asked to participate to studies via their child’s school and get tired
of participating. Third, validity of the tablet-administered QLSI-C was not
investigated in this study. Thus, further support for the new format,
including criterion-related validity studies, is needed. Future research
should replicate this study with a larger sample size, a more heterogeneous
sampling and, to a larger extent, with other population (e.g. clinical
populations).
In conclusion, the tablet format of QLSI-C appears valid in comparison
to the original paper format. Thus, both formats of the QLSI-C can be used
for assessment purposes; the choice of the version depends on the research
design or the clinical practice. The original format of the QLSI-C, although it
offers more control on the encoding, is expensive to produce and difficult to
carry. The tablet format, despite computer-related problems, showed major
advantages. First, this medium allows the incorporation of colors, smileys,
graphics and sounds within the questionnaire to make it fun and interesting
for the children to complete. Second, it makes fast, simple and convenient
testing. Third, the electronic scoring eliminates manual data entry and thus,
reduces transcription errors as well as workload by researchers. Therefore,
results from this research combined with the advantages offered by the
tablet format provide more support for the eHealth assessment modality
and encourage both clinicians and researchers to consider using eHealth
technologies in assessment in pediatric psychology.



Chapter 9
Anxiety, depression and quality
of life in school-aged children
with Cystic Fibrosis: A cross-
cultural study
Malorie Touchèque, M.A., Christina Duncan, PhD., Courtney Bee, David
Orenstein, M.D., Kathryn Moffett, M.D., Georges Casimir, M.D., PhD., Anne
Malfroot, M.D., & Anne-Marie Etienne, PhD.1
1 In submission

RESEARCH STUDIES
- 174 -
Abstract
Background. Data on emotional well-being and QOL in children with CF are
limited. This study aims to examine anxiety, depressive symptoms and quality
of life (QOL) in children with CF in comparison to healthy youth. Method.
Thirty-six children with CF (20 Belgians and 16 Americans) and 36 matched
healthy controls participated in the study. Using a cross-sectional design, all
children (8-12 years) completed measures of anxiety, depressive symptoms
and quality of life. Results. In the United-States, children with CF reported
similar level of anxiety, depressive symptoms and QOL than healthy children. In
Belgium, children with CF reported similar level of anxiety, higher rates of
depressive symptoms and a poorer QOL than the control group. In both
countries, higher anxiety and depressive symptoms are related to poorer QOL.
Conclusion. Literature on psychological functioning in children with CF has
produced mixed results. Further research should investigate the influence of
cultural background in the explanation of these results.
Keywords: emotional well-being; quality of life; youth; culture; control group.

CHAPTER 9 – EMOTIONAL WELL-BEING AND QOL IN PEDIATRIC CF
- 175 -
1. Introduction
Advances in research have led to improved treatment and subsequently,
increased long-term survival in Cystic Fibrosis (CF); however, the complex,
time-intensive daily treatment regimens can present considerable
psychosocial challenges (Besier & Goldbeck, 2011). In general, data on
emotional well-being and QOL in school-aged children with CF are limited,
especially in comparison to a healthy control group. Early researches found
a high incidence of anxiety and depression in children with CF (Lawler et al.,
1966; Teicher, 1969; Tropauer et al., 1977); however, many studies
exploring this type of research are over 30 years old, suggesting their
findings may be less relevant given the advances that have been made in the
medical treatment of CF. More recently, findings on anxiety in children with
CF showed that these children were more anxious than children in the
background population (Bregnballe et al., 2007). These same authors found
similar rates of depressive symptoms in children with CF than the general
population (Bregnballe et al., 2007). With regard to QOL, a recent study
showed that children with CF reported a poorer QOL than the background
population (Kianifar, Bakhshoodeh, Hebrani, & Behdani, 2013). This lack of
literature on emotional well-being and QOL support the importance of
studying school-age period in children with CF. Ernst et al. (2010) also
supported this research perspective by justifying that children with CF
experience specific struggles related to school-age period that may impact
their psychological health. Major concern during this developmental period
is the peer relationship. Specifically, because children’s identity and sense of
competence develops through peer comparison (Reis, Collins, & Berscheid,
2000), children with CF begin to recognize their CF-related differences
(D'Auria, Christian, & Richardson, 1997). In addition, they have to cope with
substantial treatment burden; school-aged children with CF spend more
than one hour/day completing treatment-related tasks (Ziaian et al., 2006).

RESEARCH STUDIES
- 176 -
As examples, these challenges can influence the child’s experience of illness
by representing risk for psychological distress (Ernst et al., 2010).
In addition, illness experience is also strongly influenced by culture.
Indeed, it may vary among populations or from one country to another
according to differences in cultural heritage, value systems, family
structure, medical systems, values regarding the communication of illness,
health care providers, etc. (Levenstein et al., 2001). These cultural factors
shape illness by influencing beliefs about disease etiology, appropriate
treatments, proper self-care and preventive treatment, and appropriate
doctor and patient conduct as well as perceptions of symptoms and
emotional states (Shaw, Huebner, Armin, Orzech, & Vivian, 2009). Although
illness experience is culturally constructed, cross-cultural studies are
limited in pediatric CF. Only one research, the International
Depression/Anxiety Epidemiological Study (TIDES), has been conducted in
eight European countries and in the United-states to assess depression and
anxiety in patients with CF and their caregivers (Duff et al., 2014). However,
this study does not include patients less than 12 years of age. According
Ortega and Calderon (2000), failing to accommodate cultural differences
when providing physical or psychosocial health care is associated with
more severe disease outcomes.
To our knowledge, no studies (cross-cultural or not) have been
conducted to assess emotional well-being and QOL in school-aged children
with CF; especially in comparison with a control group. Moreover, no
studies have examined the relation between psychological disturbance (i.e.
anxiety and depressive symptoms) and QOL in a population of pediatric CF.
Therefore, this study aims to examine anxiety, depressive symptoms and
QOL in a multicultural sample (i.e. Belgium and USA) of children with CF in
comparison to healthy youth. This overall objective is divided into two sub-
aims: A) Compare anxiety, depressive symptoms and QOL between children
with CF and healthy youth in a matched control group. Based on previous

CHAPTER 9 – EMOTIONAL WELL-BEING AND QOL IN PEDIATRIC CF
- 177 -
research and clinical experience, we hypothesized that children with CF
report more anxiety and depressive symptoms as well as a poorer QOL than
the background population; B) Investigate the relation of anxiety and
depressive symptoms with QOL in school-aged children with CF. Since
anxiety and depression are considered to influence QOL (DeMaso et al.,
2004; Dupuis et al., 2000; Havermans, Colpaert, & Dupont, 2008; Tsao,
Meldrum, Kim, & Zeltzer, 2007; Yohannes, Willgoss, Fatoye, Dip, & Webb,
2012; Zeller & Modi, 2006), we postulate that higher levels of anxiety and
depressive symptoms are related to poorer QOL.
2. Method
2.1. Study design and subjects
Using a cross-sectional design, participants were recruited at CF centers
in Belgium in the United States. Ethics Committee in both countries
approved research procedures. Inclusion criteria were that the child must:
(a) have a diagnosis of CF for at least one year; (b) be between 8 and 12
years old; and (c) be French- or English-speaking. Children who met the
inclusion criteria were asked to participate either during their routine CF
clinic appointment (in the USA) or over the telephone (in Belgium). The
researcher then obtained written assent and consent from the child and
parent, respectively during the clinic appointment (USA) or a home visit
(Belgium), after which children completed study questionnaires. In the
United States, 32 children with CF were approached for this study and 12
children refused to participate because they were not interested in taking
part to the study. Among the 20 children who agreed to participate, 2 did
not complete the study (dropout: 10%). The participation rate (56.25%)
yielded a sample of 18 American children with CF. However, 2 participants
were removed from the analyses because they did not matched (age and

RESEARCH STUDIES
- 178 -
sex) with an American children without medical conditions. Thus, the total
sample consisted of 16 American children with CF. In Belgium, 36 children
with CF were approached for this study and 16 children refused to
participate. Thereby, the total sample consisted of 20 Belgian children with
CF (participation rate: 55.56%).
This study also involved a matched (age & sex) control group of Belgian
(n=20) and American (n=16) children without medical conditions.
Participants were recruited from schools where consent forms were sent
home to parents of relevant students (ages 8-12), signed and returned to
the school, indicating whether parents agreed to their child’s participation.
Matched students with parental consent subsequently completed the study
questionnaires either during a home visit (in Belgium) or in small groups
during school (in USA).1
2.2. Measures
State-Trait Anxiety Inventory for Children (STAIC) (Spielberger et
al., 1973). The STAIC consists of two 20-item self-report scales measuring
state anxiety (i.e., temporal feelings of fear or worry) and trait anxiety (i.e.,
general tendency for child to be anxious) in children 8-14 years of age. With
each item rated on a 3-point Likert-type scale, the total raw score for both
scales ranges from 20 to 60. Higher raw scores indicate higher levels of
anxiety.
Children’s Depression Inventory (CDI) (Kovacs & Beck, 1977);
revised version (CDI-2) (Kovacs, 2010). The CDI is a 27-item (CDI; used
in Belgium) or a 28-item (CDI-2; used in the USA) self-report measure using
a 3-point response scale and assessing symptoms of depression in youths 7
to 17 years old. For each item, three statements are proposed and the child
is asked to select the one that best describes his/her feelings for the
1 See chapter 7 for more details about procedure.

CHAPTER 9 – EMOTIONAL WELL-BEING AND QOL IN PEDIATRIC CF
- 179 -
previous two weeks. Both versions yield a Total score as well as subscale
scores and provide standardized T-scores allowing comparison of scores
across versions. The total scale T-scores were used in this study and range
from 34 to 100, with higher scores indicating more depressive symptoms.
Quality of Life Systemic Inventory for Children (QLSI-C©) – Tablet
version (Touchèque et al., in press). The QLSI-C is a 20-item self-report
assessment tool of QOL, based on a modular approach, for children 8-12
years of ages. It covers the child’s physical, emotional, cognitive, social and
family functioning. Using a Visual Analog Scale, for each life domain,
children indicate their rating for the present situation and their
expectations using a circle, as well as a rating for its importance. QLSI-C
evaluates QOL in terms of difference (gap) between the present situation
(state) and the child’s expectations (goal), weighted by the importance
(rank) assigned for each life domain. Thus, four overall scores are
calculated: state, goal, rank and gap. For the purpose of this research, only
the gap score was used because it represents the QOL. The gap score ranges
from -100 to 100; a low (or negative) score reflects a better QOL (Etienne et
al., 2011).
2.3. Statistical analyses
Analyses were conducted using SPSS 20.0 (IBM Corp., 2011). When
distributions were non-normal, we ran non-parametric analyses in addition
to parametric analyses. Because parametric and non-parametric results
converged, we reported the parametric statistics. Sample t-tests were used
to investigate differences in means between the CF group and the control
group. Pearson’s correlations were used to examine the relation of anxiety
and depressive symptoms with QOL. For all analyses, the level of statistical
significance was p<.05.

RESEARCH STUDIES
- 180 -
3. Results
3.1. Descriptive statistics
Thirty-six children with CF (23 boys, 13 girls; M age = 10.25, SD = 1.31),
including 20 Belgians and 16 Americans, and 36 matched (for culture, age
and gender) healthy controls participated in the study. Mean scores for
level of anxiety, depressive symptoms and QOL in children with CF and
healthy children from both countries are displayed in Table 1.
3.2. Disease group comparisons for psychosocial
measures
We ran four sample t-tests where the independent variable is the
disease group (CF vs healthy) and the dependent variables are: state-
anxiety, trait-anxiety, depressive symptoms and QOL. We replicate this
procedure twice: in the Belgian and the American group. Statistics and p-
values are reported in Table 1. In Belgium, children with CF reported
similar scores of anxiety (i.e. state and trait) than healthy children whereas
children with CF showed a poorer QOL (t = 2.982; p = .005) than their
matched control group. Note that the difference between children with CF
and their healthy peers on the depressive symptoms scale approached
significance (t = 2.003; p = .052). In the United States, there was no
statistical difference between the CF and the control group for level of
anxiety, depressive symptoms and QOL.

CHAPTER 9 – EMOTIONAL WELL-BEING AND QOL IN PEDIATRIC CF
- 181 -
Table 1 - Descriptive statistics for anxiety, depression and QOL in the CF group
and the control group
Variables* n CF group
M (SD)
n Control
group
M (SD)
Sample t-
test
p
Belgium
STAIC-state 20 29.40 (3.83) 20 27.90 (3.91) 1.226 .228
STAIC-trait 20 33.50 (6.10) 20 33.25 (5.88) .132 .896
CDI 20 51.10 (7.23) 20 47.25 (4.64) 2.003 .052
QLSI-C 20 4.35 (4.46) 20 1.25 (1.34) 2.982 .005
USA
STAIC-state 16 27.63 (3.65) 16 27.81 (4.94) -.122 .904
STAIC-trait 16 32.25 (8.31) 16 37.69 (8.41) -1.840 .076
CDI 16 49.44 (9.05) 16 54.56 (8.53) -1.648 .110
QLSI-C 15† 1.76 (1.44) 15 1.93 (1.57) -.301 .766
*Raw scores were used for the STAIC and QLSI-C scale whereas T-scores were used for the CDI. †Missing data: one child did not want to finish the study package and did not complete the QLSI-C
3.3. Association between anxiety, depressive symptoms
and QOL
Pearson’s correlations are displayed in Table 2. Results showed that
level of anxiety and depressive symptoms are related to QOL in American
and Belgian children with CF; higher rates of anxious and depressive
symptoms being related to poorer QOL.
Table 2 – Correlations between anxiety, depressive
symptoms and QOL in children with CF
Quality of life
Belgian children with CF
State-anxiety .59**
Trait-anxiety .75**
Depressive symptoms .75**
American children with CF
State-anxiety .71**
Trait-anxiety .54*
Depressive symptoms .72**
** p < .01; * p < .05

RESEARCH STUDIES
- 182 -
4. Discussion
The study aims to (a) compare anxiety, depressive symptoms and QOL
between children with CF and healthy youth in a matched control group and
(b) investigate the relation of anxiety and depressive symptoms with QOL in
school-aged children with CF. With regard to group (CF vs healthy)
comparisons, findings from this research showed that level of anxiety in
both Belgian and American children with CF are similar to their healthy
peers; which is not in line with Bregnballe et al. (2007). With respect to
depressive symptoms, Belgian and American children with CF reported
similar rates of depressive symptoms than matched healthy youth. These
results are consistent with findings from Bregnballe et al. (2007). As
regards QOL, findings from our research showed that children with CF
reported a poorer QOL than healthy children in Belgium while no difference
was found between the two groups in the USA. Results from the Belgian
group replicated findings of Kianifar et al. (2013). First, these conflicting
results might be explained by cultural differences. Indeed, studies have
been conducted in different countries: Denmark (Bregnballe et al., 2007),
Iran (Kianifar et al., 2013), United-States and Belgium (this study). This
explanation would support the assumption that cultural background (e.g.
health care systems, cultural values, etc.) may influence psychosocial health
in pediatric CF. Second, the use of somewhat different data collection
procedures for each country (at home vs clinic context vs at school) may
explain a part of the different patterns of results across countries. Future
research should guarantee similar procedures.
Regarding the relation of anxiety and depressive symptoms with QOL,
results showed that higher rates of anxious and depressive symptoms are
related to poorer QOL in children with CF from both countries, which are
consistent with the literature (DeMaso et al., 2004; Dupuis et al., 2000;
Havermans et al., 2008; Tsao et al., 2007; Yohannes et al., 2012; Zeller &

CHAPTER 9 – EMOTIONAL WELL-BEING AND QOL IN PEDIATRIC CF
- 183 -
Modi, 2006). These findings encourage to consider the role of emotional
well-being when studying (researchers) or promoting (clinicians) QOL in
children with CF. Thereby, before concluding a poor QOL in these youths, it
might be relevant to assess psychological disturbance and control if this
variables might not explained a poor QOL.
In sum, although generalization of our findings is limited given the small
sample size, this study sheds light on a missing literature in pediatric CF. To
our knowledge, no recent studies have examined psychosocial health in
school-aged children with CF. In addition, no studies have investigated the
relation between anxiety, depressive symptoms and QOL in this population.
Thus, it would be important to replicate this study with a larger sample size
for both the CF group and the control group. Moreover, this study suggests
that ethnic and cultural background may uniquely impact psychosocial
issues in school-aged children; however, cultural influence is
misunderstood and further investigations are needed.
Acknowledgements
Authors would thank Dr. Jean-Paul Sacré and Dr. Frédéric Pierart from the CF
Center of Liege (Belgium), Dr. Jonathan Spahr and Dr. Daniel Weiner from the
CF Center at the Children’s Hospital of Pittsburgh, Linda Baer (nurse
coordinator) and Alliene Farley (dietician) from West Virginia University’s
Mountain State CF Center, as well as Ellen Manegold from West Virginia
University Department of Psychology, for their kind assistance in data
collection. This study was a part of a 4-year research project entitled, “Quality
of life in children with cystic fibrosis” supported by the Health Psychology Unit
at the University of Liège (Belgium).


Chapitre 10
Applying the Common-Sense
Model of Self-Regulation to
Pediatric Cystic Fibrosis:
Identifying Psychosocial Factors
Associated with Quality of Life
Malorie Touchèque, M.A., Christina Duncan, PhD., Courtney Bee, David
Orenstein, M.D., Kathryn Moffett, M.D., Georges Casimir, M.D., PhD., Anne
Malfroot, M.D., & Anne-Marie Etienne, PhD.1
1 In submission

RESEARCH STUDIES
- 186 -
Abstract
Objective: Based on the common sense model of self-regulation (CSM), this
study aims to examine mediational relations of the cognitive and emotional
pathway of the CSM in a pediatric population with cystic fibrosis (CF). Method:
Using a cross-sectional design, 38 children with CF aged between 8 and 12
years participated in the study. All children were asked to complete
questionnaires assessing psychological disturbance, coping strategies, illness
perception and QOL. Results: The mediational role of coping strategies
between representation of illness and QOL was not confirmed. However, results
showed that psychological disturbance mediates the effect of emotional illness
representation and emotion-focused coping strategy on QOL.Conclusion:
Findings suggest that the CSM needs to be adapted when applied with a
pediatric population. Future research should explore the possibility that illness
representation and coping behaviors exist at the same level and can
independently impact health outcome in school-aged children with CF.
Keywords: common-sense model; mediator; quality of life; school-aged
children; cystic fibrosis

CHAPTER 10 – CSM IN CHILDREN WITH
- 187 -
1. Introduction
Due to recently developed therapies, long-term survival in cystic
fibrosis (CF) has notably increased and patients’ life expectancy with CF
today is in the early 40s (Royce & Carl, 2011). However, complex, time-
intensive daily treatment regimens still pose substantial psychosocial
challenges (Besier & Goldbeck, 2011). As a result, quality of life (QOL)
measurement in CF represents a key parameter to quantify and evaluate the
impact of both the disease and its treatment on the patient’s life (Abbott et
al., 1997; Royce & Carl, 2011).
Few studies have been conducted on QOL in school-aged children with
CF; they have focused on assessing effects of age, gender and disease
severity on QOL (Groeneveld et al., 2012; Hegarty, MacDonald, Watter, &
Wilson, 2009; Thomas, Mitchell, O’Rourke, & Wainwright, 2006), evaluating
agreement between parent- and child-report of QOL (Groeneveld et al.,
2012; Hegarty et al., 2009; Thomas et al., 2006), comparing QOL between
children with CF and a control group (Kianifar et al., 2013) as well as
between inpatients and outpatients with CF (Hegarty et al., 2009), and
examining the relation of treatment time and hassles to health-related QOL
in children with CF (Ziaian et al., 2006).
The common sense model of self-regulation (CSM) described by
Leventhal et al. (1980) provides a framework for understanding factors that
may influence quality of life in people experiencing illness. The CSM
describes three stages in the processing of new information. First,
individuals make sense of the problem and assess the threat to their health
by developing two parallel, yet interrelated, representations of the threat:
cognitive and emotional (stage 1: interpretation). The cognitive
representation is the development of illness cognitions according its cause,
timeline, consequences and controllability. The emotional representation is
the changes in the individual’s emotional state resulting from the illness.

RESEARCH STUDIES
- 188 -
Second, individuals generate and execute appropriate action in response to
difficulties that may arise from the illness and/or its treatment (stage 2:
coping). Finally, individuals assess how successful the coping stage has been
in relation to desired outcome (stage 3: appraisal). Although the
components of the CSM have been examined in various chronic diseases
(Costanzo, Lutgendorf, & Roeder, 2011; Griva, Myers, & Newman, 2000;
Horne & Weinman, 2002; Knowles, Wilson, Connell, & Kamm, 2011;
Scharloo et al., 1998), most of these studies have focused on adolescents
and adult patients. This observation is due to the fact that the CSM was
initially addressed to adult patients (Leventhal et al., 1980; Meyer,
Leventhal, & Gutmann, 1985). Thus, prior to applying the CSM to a pediatric
population, some considerations should be raised. Although childhood is
characterized by evolving cognitive skills and knowledge (Ernst et al.,
2010), most of the contributions in children’ conceptualization of illness
suggests that illness representation of school-aged children is incomplete
(Au & Romo, 1999; Piaget & Inhelder, 1969). Based on this finding, we
hypothesized that possible misinformation and unfounded concerns about
CF may impact children’s health outcome (i.e. QOL). Moreover, since school-
aged children have reached an advanced level of emotional development
(e.g. emotional regulation, expression and understanding of complex
emotions) (Housiaux & Lahaye, 2008), we believed that emotional reactions
to the disease may also influence child’s health outcome.
Guided by these considerations about children’s cognitive and
emotional development and the CSM as a theoretical framework (see Figure
1), the purpose of this exploratory study is to test the relations on both the
cognitive and emotional pathways in a multicultural sample of school-aged
children with CF. Therefore, this study aims to examine whether: (a) coping
strategies mediate the effect of cognitive and emotional illness
representation on QOL; (b) psychological disturbance mediates the effect of
emotional illness representation and coping strategies on QOL.

CHAPTER 10 – CSM IN CHILDREN WITH
- 189 -
Figure 1 – Schematic representation of Leventhal et al.’s (1980) Common Sense Model of Self-regulation based on variables used in
the present study
Feedback loop
Feedback loop
Cognitive illness
representation
(Timeline,
consequence, control)
Illness outcome
Quality of life
Problem-focused coping strategies
Emotional outcome
Psychological
disturbance
Illness stimuli
(i.e. disease severity,
somatic symptoms,
etc.)
Emotional illness
representation Emotion-focused coping strategies

RESEARCH STUDIES
- 190 -
2. Method
2.1. Study design and subjects
Using a cross-sectional design, two independent participant samples of
children with CF were collected in Belgium and the United States. The
research procedures were approved by Ethic Committees in both countries.
In Belgium, all potential CF participants were mailed a letter of information
from the CF Center that described the study and its requirements. Then,
hospitals provided the researcher with a list of children who met the
inclusion criteria. Inclusion criteria were that the child must: (a) have a
diagnosis of CF for at least one year; (b) be between the ages of 8 and 12
years; and (c) be French-speaking. The researcher telephoned parents of all
potential participants to briefly describe the study and ask if they were
interested in scheduling a home visit for their child to take part in the study.
Thirty-six children with CF were eligible for this study. Sixteen children
refused to participate because they were not interested in taking part in the
study. Thus, the total sample consisted of 20 Belgian children with CF
(participation rate: 56%).
In the United States, children were recruited during their routine CF
clinic appointment at their CF center. Inclusion criteria were the same as
those for the Belgian sample; however, children must be English-speaking
(rather than French). When patients met inclusion criteria, their medical
provider asked the family if they were interested in talking to a researcher
about the research. When a family agreed, a member of the research team
briefly described the study, its requirements, and participant rights. The
research team member then obtained assent and consent from the child and
parent, respectively. Children were given the option to: (a) complete study
measures during and/or after their clinic appointment; (b) schedule a later
date with research staff to complete study measures in the principal

CHAPTER 10 – CSM IN CHILDREN WITH
- 191 -
investigator's research laboratory or at the participant’s home. A total of 32
children with CF were approached for this study. Twelve children refused to
participate because they were not interested in taking part in the study
(33%) or they did not have enough time to complete measures during or
after their clinic appointment (67%). Among the 20 children who agreed to
participate, 2 did not want to finish the study questionnaires (dropout:
10%). Thus, the participation rate (56.25%) yielded a sample of 18
American children with CF.
2.2. Measures
Background Information Form. All children completed a form asking
about their sociodemographic data (e.g. grade level, age). Medical staff
provided information about recent medical data (e.g. forced expiratory
volume in one second, FEV1) for participants with CF.
State-Trait Anxiety Inventory for Children (STAIC) (Spielberger et
al., 1973). The STAIC consists of two 20-item self-report scales, one each
for measuring state- and trait- anxiety in children between the ages of 8 and
14. Children rate each item using a 3-point Likert scale. The total raw score
ranges from 20 to 60 for each scale. A high total raw score indicates a high
level of anxiety.
Children’s Depression Inventory (CDI) (Kovacs & Beck, 1977);
revised version (CDI-2) (Kovacs, 2010). The CDI is a 27-item (CDI; used
in Belgium) or a 28-item (CDI-2; used in the USA) self-report measure
assessing symptoms of depression in youths 7 to 17 years old. For each
item, three statements are proposed and the child is asked to select the one
that best describes his/her feelings for the previous two weeks. Both
versions yield raw scores and standardized T-scores allowing comparison
of scores across versions. The total scale T-scores, ranging from 34 to 100+,

RESEARCH STUDIES
- 192 -
were used in this study. Higher T-scores indicate higher levels of depressive
symptoms.
Kidcope – Younger version (Spirito et al., 1988). The Kidcope is a 15-
item self-report measure assessing coping strategies employed by children
7 to 12 years old. First, the child reports a major health-related problem (in
children with CF) that has bothered them in the past month. Then, for each
item, children indicate if they have used the relevant strategy when
encountering problems. If they use the strategy, they then indicate its
efficacy on a 3-point Likert scale. Originally, investigators identified 10
coping strategies: problem-solving, distraction, social support, social
withdrawal, cognitive restructuring, self-criticism, blaming others,
emotional regulation, wishful thinking, and resignation. However, the
“emotional regulation” coping consisted of two items that had very different
endorsement patterns – one item was concerned with yelling, screaming, or
getting mad and the other was concerned with calming oneself – and can be
considered as independent variables (X²=.997; p=.318). The two items were
not related to each other (r=.02; p=.331) and were correlated differently
with the others coping strategies. Thus, for the purpose of this study, we
referred to the first item as emotional outburst and the second as
relaxation, as suggested by Cheng and Chan (2003).
Children’s Illness Perception Questionnaire (CIPQ) (Walker et al.,
2006). The CIPQ is a 26-item self-report instrument for children 7 to 12
years old adapted from the Illness Perception Questionnaire for adults
(John Weinman, Petrie, Moss-morris, & Horne, 1996). It consists of two
separate sections. The first section (16 items) assesses children’s illness
beliefs regarding the timeline, consequences and control/cure of their
illness and the second section (10 items) measures children’s beliefs
regarding the causal aspects of their disease. For each item, the child
answers on a dichotomous scale (‘‘true’’ or ‘‘false’’). For the purpose of this
study, only scores of the first section were entered into the analyses. For the

CHAPTER 10 – CSM IN CHILDREN WITH
- 193 -
timeline subscale, scores range from 0 to 4; the higher the score is, the
longer the illness will last. For the consequences subscale, scores range
from 0 to 7; a higher score indicates more consequences. For the control
subscale, scores range from 0 to 5; the higher the score is, the less children
control their illness.
Quality of Life Systemic Inventory for Children (QLSI-C©) – Tablet
administration (Touchèque et al., in press). QLSI-C is a self-report
assessment tool of QOL, based on a modular approach, for children 8 to 12
years of age. It consists of a 20-item generic scale representing multiple
domains of life. QLSI-C evaluates QOL in terms of difference (gap) between
the present situation (state) and the child’s expectations (goal), weighted by
the importance (rank) assigned for each life domain. Thus, four overall
scores are calculated: state, goal, rank and gap. For the purpose of this
research, only the gap score, representing QOL and ranging from -100 to
100, was used; a low (or negative) score reflects a better QOL (Etienne et al.,
2011). Note that a CF-specific module (i.e. six additional items) was
developed (Touchèque & Etienne, 2014) and that item 1, namely emotional
functioning, was used to assess the emotional illness representation as the
CIPQ did not examine this component. The instruction of the CF-specific
item (e.g. “I feel worried or concerned when I think about my disease”) was
similar to the items of the IPQ-R related to the emotional representation
(e.g. “My illness does not worry me”) (Moss-Morris et al., 2002). Thus, based
on our clinical experience, we postulated that the state score of emotional
functioning assesses children’s emotional reactions to CF-related problems.
The state score ranges from 0 to 100; a higher score suggest that children
worried about their disease.

RESEARCH STUDIES
- 194 -
2.3. Statistical analyses
Statistical analyses were conducted using SPSS 20.0 (IBM Corp., 2011)
and mediation analyses were performed using the PROCESS macro for SPSS
(Hayes, 2013). Pearson’s correlations were performed to identify the
potential effects of demographic/illness parameters on QOL, so that these
effects could be controlled for in subsequent analyses. Then, four mediation
analyses were tested, with QOL being the outcome variable for each
mediation: (1) the mediation of coping strategies between cognitive illness
representation and QOL; (2) the mediation of coping strategies between
emotional illness representation and QOL; (3) the mediation of
psychological disturbance between emotional illness representation and
QOL; (4) the mediation of psychological disturbance between coping
strategies and QOL.
To consider a variable as a mediator, three criteria need to be met: (a)
the independent variable must significantly predict the dependent variable;
(b) the mediator must significantly predict the dependent variable; (c) the
independent variable must predict the mediator. The analysis of mediation
succeeded when after controlling for the effects of the mediator on the
dependent variable, the relation between the independent and the
dependent variable is significantly reduced (i.e. partial mediation) or does
no longer exist (i.e. complete mediation) (Baron & Kenny, 1986).
Note that we created a composite score (i.e. average) labelled
“psychological disturbance” including scores of trait-anxiety and depressive
symptoms. Level of significance for all analyses was set at p<.05.

CHAPTER 10 – CSM IN CHILDREN WITH
- 195 -
3. Results
3.1. Descriptive statistics
Thirty-eight children with CF (23 boys, 15 girls), including 20 Belgians
and 18 Americans, participated in the study (M age = 10.26; SD = 1.37). The
forced expiratory volume in 1 second predicted (FEV1%) was 90.71%
(SD=12.51).
3.2. Bivariate correlations
Statistical covariates were identified by examining the relation of
demographic/illness parameters (i.e. child’s age, sex, culture and FEV1)
with QOL in children with CF. Child’s cultural background (0=Americans;
1=Belgians) and child’s sex (0=girls; 1=boys) were significantly related to
QOL (Culture: r = -.39, p = .017; Sex: r = -.33, p = .046); Being a Belgian child
with CF and a boy was related to poorer QOL. Therefore, the potential
effects of child’s culture and sex were controlled in the subsequent analyses.
3.3. Mediation analysis
3.3.1. Mediation of coping strategies between
cognitive illness representation and QOL
We ran three simple regression analyses to examine whether the three
subscales of the CIPQ (i.e. Timeline, Consequences and Control) predict the
QOL in children with CF. Since none of the subscales was a significant
predictor of the QOL (Timeline: β = .19; t = 1.231; p = .227; Consequences: β
= .05; t = .313; p = .756; Control: β = .03; t = .196; p = .846), we did not run
an analysis of mediation to test whether coping strategies mediate the effect
of illness perception on QOL.

RESEARCH STUDIES
- 196 -
3.3.2. Mediation of coping strategies between
emotional illness representation and QOL
We ran a simple regression analysis to examine whether the emotional
illness representation predicts QOL in children with CF. Result revealed the
regression of emotional illness representation on QOL after controlling for
covariates was a marginal trend toward significance (β = .36; t = 2.033; p =
.051). Since this analysis barely missed statistical significance, we decided
to continue to test for mediation. Then, we run eleven simple regressions to
test whether each coping strategy (see methods) predicts QOL in children
with CF. Results showed that only emotional outburst coping was a
significant predictor of the QOL after controlling for covariates (β = .40; t =
2.682; p = .011). Finally, we performed a logistic regression (i.e. outcome =
binary variable) to examine whether emotional illness representation
predicts emotional outburst coping. Results revealed that, after controlling
for covariates, emotional representation of the illness did not predict the
use of emotional outburst coping (β = 1.14; Wald’s χ² = 1.099; p = .294). As a
result, we cannot test the mediational model in which emotional outburst
coping mediates the relation between emotional illness representation and
QOL.
3.3.3. Mediation of psychological disturbance
between emotional illness representation and
QOL
Results from previous regression analyses showed that emotional
illness representation predicted QOL after controlling for covariates (β =
.36; t = 2.033; p = .051). Thus, we ran a simple regression analysis to test
whether psychological disturbance predicts QOL in children with CF.
Results revealed that psychological disturbance was a significant predictor
of the QOL after controlling for covariates (β = .57; t = 4.791; p < .001).. We

CHAPTER 10 – CSM IN CHILDREN WITH
- 197 -
also ran a simple regression analysis to examine whether emotional illness
representation predicts psychological disturbance. Results showed that
emotional illness representation predicted psychological disturbance after
controlling for covariates (β = 1.17; t = 2.832; p = .008).
Since all criteria were met for a mediation effect, we ran an analysis of
mediation to test whether psychological disturbance mediates the relation
between emotional illness representation and QOL in children with CF. The
unconditional indirect effect was significant (see Table 1). Emotional
representation of the illness predicted psychological disturbance, which in
turn predicted QOL in children with CF: higher psychological disturbance is
associated with poorer QOL. After controlling for the mediator, the relation
of emotional illness representation to QOL reduced from from β = .36 (p =
.051) to β = .02 (p = .813) (see Figure 2).
Table 1 – Unconditional Indirect effect of emotional representation on QOL
through psychological disturbance (n=35; bootstrap resamples = 10,000)
Mediator variable model (VD = Psychological disturbance)
Predictor Β SE t P
Intercept -.73 .35 -2.08 .046
Emotional representation 1.17 .41 2.83 .008
Culture .02 .32 .05 .958
Child’s sex .46 .35 1.30 .204
Dependent variable model (VD = QOL)
Predictor Β SE t P
Intercept .71 .08 9.39 < .001
Emotional representation .02 .09 .24 .813
Psychological disturbance .17 .04 4.64 < .001
Culture -.13 .06 -2.02 .052
Child’s sex -.10 .07 -1.39 .174
Bootstrap results for indirect effect of emotional representation on QOL
Β SE 95% BCa CI
Psychological disturbance .20 .09 (.0502, .4012)

RESEARCH STUDIES
- 198 -
Figure 2 – Mediation of psychological disturbance between emotional illness representation and QOL in children with CF
Emotional representation
Mediator Psychological disturbance
Quality of life
β = 1.17 ; SE =.41 ; p=.008
β = .02 ; SE =.09 ; p = .813b
β = .17 ; SE = .04 ; p < .001 b
β = .36 ; SE = .11 ; p = .051a
β = .57 ; SE = .35 ; p < .001a
a Direct effect in the regression model b Effects in the mediation model

CHAPTER 10 – CSM IN CHILDREN WITH
- 199 -
3.3.4. Mediation of psychological disturbance
between coping strategies and QOL
Results from previous regressions analyses showed that QOL in
children with CF was predicted by emotional outburst coping (β = .40; t =
2.682; p = .011) and psychological disturbance (β = .57; t = 4.791; p < .001).
Thereby, we ran a simple regression to examine whether emotional
outburst coping predicts psychological disturbance. Results revealed that
emotional illness representation predicted psychological disturbance after
controlling for covariates (β = .91; t = 2.642; p = .013).
Since all criteria were met for a mediation effect, we ran an analysis of
mediation to test whether psychological disturbance mediates the relation
between emotional outburst coping and QOL in children with CF. The
unconditional indirect effect was significant (see Table 2). Emotional
outburst coping predicted psychological disturbance, which in turn
predicted QOL in children with CF: higher psychological disturbance is
associated with poorer QOL. After controlling for psychological disturbance,
the relation of emotional outburst coping to QOL reduced from β = .40
(p=.011) to β = .11 (p=.205) (see Figure 3).

RESEARCH STUDIES
- 200 -
Table 2 - Unconditional Indirect effect of emotional outburst coping on QOL
through psychological disturbance (n=37; bootstrap resamples = 10,000)
Mediator variable model (VD = Psychological disturbance)
Predictor Β SE t P
Intercept -.33 .26 -1.28 .208
Emotional outburst coping .91 .34 2.64 .013
Culture .13 .31 .42 .676
Child’s sex .06 .30 .19 .849
Dependent variable model (VD = QOL)
Predictor Β SE t P
Intercept .69 .06 11.97 .000
Emotional outburst coping .11 .08 1.29 .205
Psychological disturbance .15 .04 3.86 < .001
Culture -.13 .07 -1.95 .060
Child’s sex -.13 .07 -2.02 .052
Bootstrap results for indirect effect of emotional outburst coping on QOL
Β SE 95% BCa CI
Psychological disturbance .13 .06 (.0401, .2809)

CHAPTER 10 – CSM IN CHILDREN WITH
- 201 -
Figure 3 – Mediation of psychological disturbance between emotional outburst coping strategy and QOL in children with CF
Emotional outburst coping
Mediator Psychological disturbance
Quality of life β = .11 ; SE = .08 ; p = .205a
β = .15 ; SE = .04 ; p < .001b
β = .91 ; SE =.34 ; p = .013
β = .40 ; SE =.88 ; p = .011b
β = .57 ; SE = .35 ; p < .001a
a Direct effect in the regression model b Effects in the mediation model

RESEARCH STUDIES
- 202 -
4. Discussion
Based on the Common Sense Model of Self-Regulation (Leventhal et al.,
1980), the purpose of this study was to test whether: (a) coping strategies
mediate the effect of cognitive and emotional illness representation on QOL;
and (b) psychological disturbance mediates the effect of emotional illness
representation and coping strategies on QOL. First, the assumption of the
Leventhal’s Common Sense Model that coping acts as a mediator between
cognitive illness representation and appraisal outcome (i.e. QOL) could not
be confirmed. Findings reported from this research indicate that illness
perception was not a significant predictor of the QOL in children with CF.
According some studies (Carey, 1995; Eiser, 1989; Kister & Patterson,
1980), children’s concept of illness depends on the acquisition of knowledge
about their illness. In the case of CF, children are not self-managing their
disease; parents do. As a result, children with CF might have reduced their
understanding of their disease and treatments requirements. The
development of children’s concept of illness may also be influenced by their
own health histories (Campbell, 1975). Children diagnosed with a disease at
an early age or at birth may not be able to fully understand the concept of
illness since they have never experienced being healthy. Thus, we postulate
that even though school-aged children with CF might not have developed a
comprehensive illness representation, it did not impact their QOL; however,
since the school-aged period allows the development of beliefs and
expectations related to the illness, assessment of cognitive representation
of illness during this period may facilitate development of psycho-
educational interventions to address misinformation and unfounded
concerns about CF and empower children to self-management (Ernst et al.,
2010).

CHAPTER 10 – CSM IN CHILDREN WITH
- 203 -
Our results also suggest that emotional illness representation has a
direct effect on QOL that is not explained by the use of coping strategies in
children with CF. This is consistent with a meta-analytic review of the CSM
indicating that illness representation may be associated with outcomes
independently of coping strategies (Hagger & Orbell, 2003). In addition, our
results indicate that use of coping strategies was not a strong predictor of
the QOL in children with CF since only the use of emotional outburst as a
strategy to cope with a CF-related problem was associated with a poorer
QOL. Despite the lack of associations for other specific coping strategies, the
significant effect of emotional outburst on QOL illustrates the potential
importance of examining individuals’ coping strategies rather than using
taxonomies (i.e. approach vs avoidance; problem-focused vs emotion-
focused) in a pediatric CF population. Similar conclusions have been
suggested by Edgar and Skinner (2003) and Spirito et al. (1988).
Second, the results reported from this study showed that psychological
disturbance was a robust predictor of the QOL suggesting that children with
CF experiencing more psychological disturbance had a poorer QOL. This
result is in line with a study showing that having higher symptoms of
anxiety and depression was associated with poorer health-related QOL in
adults with CF (Havermans et al., 2008). In addition, psychological
disturbance was an important mediating factor of the relation between
emotional illness representation and QOL as well as between emotion-
focused coping strategies (i.e. emotional outburst) and QOL. Thus,
psychological disturbance appears to be a major construct in determining
QOL in children with CF which could be targeted for intervention.
The strength of this current study is the application of a theoretical
framework in pediatric CF that sheds light on the relations between illness
representation, coping strategies and appraisal outcomes (i.e. QOL).
However, there are some limitations to this study. First, the design used in
this research was cross-sectional which is not sufficient to demonstrate the

RESEARCH STUDIES
- 204 -
temporal ordering of effects. Second, different sample collection procedures
were used and may account for a part of the culture effect in the study.
Future research should guarantee similar procedures. Third, generalization
of findings is limited. It would be important to replicate this study with a
larger sample size.
In conclusion, this study did not provide support for the hypothesis that
coping strategies mediates the relation between illness representations (i.e.
emotional or cognitive) and QOL. However, findings from this research
highlight the importance of the emotional pathway in determining QOL in
children with CF, with psychological disturbance mediating the effect of
emotional illness representation and emotion-focused coping strategies (i.e.
emotional outburst) on QOL. Based on our findings, we developed an
adaptation of the Leventhal’s Common Sense Model when applying in
pediatric populations (see Figure 4). However, this adapted model only
includes individual factors that influence QOL in children with CF.
Additional research is needed to further examine the role of parental or
family factors in determining QOL in children with CF. Overall, these results
expand our understanding of risk factors associated with a poor QOL in
children with CF. Therefore, our findings have implications for developing
intervention strategies targeted specific needs and concerns in school-aged
children with CF.

CHAPTER 10 – CSM IN CHILDREN WITH
- 205 -
Figure 4 – Schematic representation of Leventhal et al.’s (1980) Common Sense Model of Self-regulation adapted to children with
chronic disease
Feedback loop
Feedback loop
Cognitive illness
representation Timeline
Consequence
Control
Outcome 2
Quality of life
Outcome 1
Psychological
disturbance
Illness stimuli
(i.e. disease
severity, somatic
symptoms, etc.)
Coping
strategies
Emotional
illness
representation

RESEARCH STUDIES
- 206 -
Acknowledgements
Authors would thank Dr. Jean-Paul Sacré and Dr. Frédéric Pierart from the CF
Center of Liege (Belgium), Dr Jonathan Spahr and Dr. Daniel Weiner from the
CF Center at the Children’s Hospital of Pittsburgh, Linda Baer (center
coordinator) and Alliene Farley (dietician) form the WVU’s Mountain State CF
Center as well as Ellen Manegold from West Virginia University for their kind
assistance in data collection. This study was a part of a 4-years research
entitled “Quality of life in children with cystic fibrosis” supported by the Health
Psychology Unit at the University of Liège (Belgium).



Chapter 11
Parenting stress, parental illness
perception and coping strategies
associated with Quality of life in
children with Cystic Fibrosis: the
mediating role of parental
adjustment
Malorie Touchèque, M.A., Christina Duncan, PhD., Ellen Manegold, David
Orenstein, M.D., Kathryn Moffett, M.D., Georges Casimir, M.D., PhD., Anne
Malfroot, M.D., & Anne-Marie Etienne, PhD.1
1 In process

RESEARCH STUDIES
- 210 -
Abstract
Objective. This study aims to examine whether parental quality of life (QOL)
acts as a mediator of the relation between parenting variables and QOL in
children with CF. Method. Using a cross-sectional design, 26 families having a
child with CF (8 to 12 years old) participated in the study. Parents (mothers
AND fathers) completed parenting stress, illness perception, coping strategies
and QOL questionnaires. Children completed a QOL measure. Results.
Parenting variables did not predict QOL in children with CF, except parenting
stress in mothers. The mediational role of parental QOL between parenting
variables and the child’s QOL was not confirmed. There was no specific effect of
mothers- and fathers- related variables on the child’s QOL. Conclusion. This
study is one of the first to apply a theoretical framework to pediatric CF.
Further investigation are needed to better understand the specific role of
mothers- and fathers- related variables on children adjustment.
Keywords: school-aged children; quality of life; gender differences; parenting
variables; cystic fibrosis

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 211 -
1. Introduction
Due to advances in scientific and medical research as well as newer
treatment protocols, life expectancy in patients with cystic fibrosis (CF) has
notably increased such as average survival age today is in the early 40s
(Royce & Carl, 2011). In this context, medical providers in CF care centers
seek not only to improve patients’ health but also to enhance their QOL,
which is regarded with equal importance to medically beneficial therapies
(Royce & Carl, 2011). Therefore, it is widely accepted that quality of life
(QOL) is a key outcome parameter that describes the patients’ perception of
the impact of a disease on his or her well-being and functioning in physical,
mental, emotional, social, and everyday life domains (Bullinger, Schmidt,
Petersen, & Ravens-Sieberer, 2006). QOL also represents a
conceptualization of adjustment to chronic disease (Stanton, Collins, &
Sworowski, 2001). However, QOL in children with CF under the age of 12
years has been under-investigated in comparison to QOL in adolescent and
adult patients.
Family variables have received a great deal of attention as predictors of
child adjustment in the context of chronic disease (Thompson & Gustafson,
1996). Utilizing Thompson and Gustafson’s Transactional Stress and Coping
(TSC) model (Thompson et al., 1992), numerous studies have demonstrated
the robust transactional relation between parent and child adjustment
(Chaney et al., 1997; Colletti et al., 2008; Hocking & Lochman, 2005).
Originally applied to CF in childhood (Thompson et al., 1994), the TSC
model provides a theoretical framework for understanding how the child
and mothers attempt to adapt to chronic disease. This model posits that
maternal and child adjustment affect each other reciprocally and are
influence by different adaptational processes (i.e. stress appraisal, beliefs
and coping strategies) (Hocking & Lochman, 2005). Specifically, we are
interested in the role of three parental adaptational processes (i.e.

RESEARCH STUDIES
- 212 -
parenting stress, illness perception, coping strategies) and parental
adjustment (i.e. QOL) as predictors of the QOL in children with CF.
Parenting stress is defined as the level of stress related to demands of
parenthood, including stress attributable to parental distress, dysfunctional
parent-child interactions and difficult child characteristics (Abidin, 2012).
Findings from previous studies showed that higher levels of parenting
stress was consistently associated to poor adjustment in children with a
chronic disease (i.e. cancer, diabetes, asthma) (Colletti et al., 2008;
Czyzewski et al., 1994; Kazak & Barakat, 1997; Mullins et al., 2007).
Parental illness perception is the development of parental beliefs
related to their child’s illness according its identity, cause, timeline,
consequences and controllability (Leventhal et al., 1980). Literature that
examined the relation between parental perception of their child’s disease
and the child adjustment is scarce. Available studies found that parental
illness perception was related to quality of life in children with asthma
(Chateaux & Spitz, 2005; Fonseca & Spitz, 2011). However, no studies have
examined the relation between parental illness perception and QOL in
children with CF.
Coping strategies refer to the individuals’ cognitive and behavioral
efforts to manage stressful situations (Lazarus & Folkman, 1984). Very few
studies have examined the relation between parental coping strategies and
the child adjustment to chronic disease. Moreover, these studies have
produced mixed results. For instance, Sales et al. (2008) found that parental
coping was related to children’s asthma-related quality of life whereas
Frank et al. (1997) found no association between parental coping and child
adjustment to cancer. To our knowledge, no studies have examined the
relation between parental coping and adjustment in children with CF.
Several studies have demonstrated an association between parent and
child adjustment (Chaney et al., 1997; Colletti et al., 2008; Hocking &
Lochman, 2005). However, these studies used psychological distress as a

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 213 -
conceptualization of adjustment to chronic disease in childhood whereas
literature revealed the multifaceted nature of the concept of adjustment
(Stanton, Revenson, & Tennen, 2007). No studies have examined the
relation between parent and child adjustment using another
conceptualization such as QOL.
The TSC model as well as most studies examining how parents manage
the care of children with a chronic disease have focused almost exclusively
on the role of mothers (Dewey & Crawford, 2007; Hayes & Savage, 2008;
Hodgkinson & Lester, 2002; Thompson & Gustafson, 1996). This
phenomenon can be explained by different reasons: (a) mothers are
traditionally more involved in the care management of the child and the
interactions with medical staff (Eiser, 1993); (b) they spend likely more
time at home (Eiser, 1993); and (c) they have also been more accessible to
researchers because they are usually the ones who bring their children to
clinic visits (Dewey & Crawford, 2007; Eiser, 1993). As a result, fathers are
underrepresented in pediatric research (Phares et al., 2005). Studies have
suggested the important of fathers’ inclusion in pediatric research because
factors that influence parental adjustment may differ for mothers and
fathers (Dewey & Crawford, 2007; Phares et al., 2005). However, specific
studies on how mothers- and fathers- related variables may play a different
role in their child’s adjustment to a chronic disease are scarce. Thus, to
better understand how parental adjustment influence adjustment in
children with CF, there is a need to move beyond an exclusive focus on
mothers and to include fathers as well (Ievers & Drotar, 1996; Phares et al.,
2005).
Guided by the TSC model, the purpose of this study is to test some
relations from our adapted version of this model (see Figure 1) in a
multicultural sample of families having a child with CF (8 to 12 years old).
Therefore, this study aims to examine whether parental QOL acts as a
mediator of the relation between parenting variables (i.e. parenting stress,

RESEARCH STUDIES
- 214 -
illness perception, coping strategies) and the child’s QOL while considering
the specific effect of both mothers- and fathers- related variables on the
child’s QOL.
2. Method
2.1. Study design and subjects
Using a cross-sectional design, children with CF and their parents were
recruited from CF centers in Belgium and the United States. The research
procedures were approved by ethic committee in both countries. In
Belgium, all potential participants were informed of the study and its
requirements by receiving a letter of information from their CF center.
Then, hospitals provided to the researcher a list of families of children with
CF who met the inclusion criteria. All potential participants were
approached by the researcher over phone call to briefly describe the study
and ask the parent if they were interested to participate. We scheduled a
home visit with families who agreed to participate. First, instructions were
given to parents. Then, the researcher completed questionnaires with the
child in a separate room while parents were completing their study
package. Parents had to send back questionnaires via mail if they did not
finish their questionnaires at the end of the evaluation with the child.
Inclusion criteria include: (a) children must have a diagnosis of CF for at
least one year; (b) children must be aged between 8 and 12 years; (c)
children with CF and their parents must be French-speaking; (d) both
mothers and fathers must participate to the study. Thirty six families were
eligible for this study. Sixteen families were not interested in taking part in
the study. Among the 20 families who agreed to participate, 3 were not
included in the study because of missing data; parents did not send back
their questionnaires to the researcher (dropout: 15%). Thus, total sample

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 215 -
consisted of 17 families (including child, mother and father) having a child
with CF (participation rate: 47.2%).
In the United States, families were recruited during their routine CF
clinic appointment in their CF center. Inclusion criteria were the same as
those for the Belgian sample; however, families must be English-speaking
(rather than French). When participants met inclusion criteria, their
medical provider asked the families if they were interested in talking to a
researcher about this study. If the families agree, a member of the research
team briefly described the study, its requirements, and participant rights.
The research team member then obtained consent from parents and assent
from the child. Families were given the option to: (a) complete study
measures during and after their clinic appointment; (b) schedule an
appointment with research staff to complete study measures at a later date
in the principal investigator's research laboratory or at the participant’s
home. Thirty two families of children with CF were eligible for this study.
Twelve families refused to participate because they were not interested in
taking part in the study or they did not have enough time to complete
measures during or after their clinic appointment. Among the 20 families
who agreed to participate, 11 were not included in the study because the
study package was incomplete: children did not want to finish the study
questionnaires (n=2) or parents did not send back their study measures to
the researcher (n=9) (dropout: 55%). Thus, the participation rate (28.13%)
yielded a sample of 9 American families having a child with CF.

RESEARCH STUDIES
- 216 -
Figure 1 –Schematic representation of our adapted version of the Transactional Stress and Coping model (reproduction from
Thompson, Gustafson, George, & Spock, 1994)
Parenting
stress
Demographic
parameters
(i.e. child’s
gender, age)
Illness
parameters
Adjustment
outcome in
fathers (i.e.
QOL)
Illness
perception
Coping
strategies
Parental adaptational processes
Child adaptational processes Child adjustment
outcome (i.e. QOL)
†
†
† Relations examined in the present study
†
Adjustment
outcome in
mothers (i.e.
QOL)
†

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 217 -
2.2. Measures
Parenting Stress Index – Short Form – Fourth Edition (PSI-4-SF)
(Abidin, 2012; M. Touchèque et al., in press). The PSI-4-SF is a 36-item
self-report measure assessing stress related to demands of parenthood. The
PSI-4-SF is divided into three subscales consisting of 12 items each:
Parental Distress (PD), Parent-Child Dysfunctional Interaction (PCDI) and
Difficult Child (DC). Using a 5-point Likert scale, parents indicate the degree
to which they agree with each statement. Total score was used in this study;
a high total score indicates a high level of parenting stress. The PSI-4-SF
showed good internal consistency with Cronbach alphas around .79 for all
subscales (Abidin, 2012; M. Touchèque et al., in press).
Brief Illness Perception Questionnaire (BIPQ) (Broadbent et al.,
2006). The BIPQ is a 9-item scale developed from the Illness Perception
Questionnaire (John Weinman et al., 1996) to rapidly assess cognitive and
emotional illness representations in adults. Each item represents a
dimension of the representation of illness (i.e. consequences, timeline,
personal control, treatment control, identity, emotional response,
understanding, concerns and cause). Participants answer each item using a
0-to-10 response scale except the causal question which is assessed by an
open-ended response item. The overall score is used in this research and
represents the degree to which the illness is perceived as threatening or
benign; a higher score reflects a more threatening view of the illness. The
instrument has good test-retest reliability and validity (Broadbent et al.,
2006).
Coping Health Inventory for Parents (CHIP) (McCubbin et al.,
1983). The CHIP is a 45-item checklist that provides self-report information
about how parents perceive their overall response to the management of
family life with a chronically ill child. The respondent is asked to indicate if
they have used the different strategies (Frequency: 0 = No; 1 = Yes). If they

RESEARCH STUDIES
- 218 -
use the strategy, they have to indicate how helpful (from 0 “not helpful” to 3
“extremely helpful”) each coping strategy has been in managing the illness
situation. There are three subscales: pattern I: maintaining family
integration, cooperation, and an optimistic definition of the situation;
pattern II: maintaining social support, self-esteem, and psychological
stability; and pattern III: understanding the medical situation through
communication with other parents and consultation with medical staff. For
the purpose of this research, only the frequency scale was used. The total
score for the frequency scale ranges from 0 to 19 (pattern I), 0 to 18
(pattern II) and 0 to 8 (pattern III); a high score indicates a high frequency
of use of the strategy. The instrument has good psychometric properties;
Cronbach’s alphas indicated reliabilities ranging from .71 to .79 (McCubbin
et al., 1983).
Quality of Life Systemic Inventory (QLSI©) (Dupuis et al., 1989). The
QLSI evaluates QOL through 28 items clustered into nine life domains in
adults: physical health, cognitive functioning, social and familial
environment, couple relationship, leisure, work, housework, emotional
functioning, and spirituality. It evaluates QOL in terms of difference (gap)
between the current situation (state) and the participant’s expectations
(goal), weighted by the importance (rank) assigned for each life domains.
Thus, four overall scores are calculated: state, goal, rank and gap. Each of
these scores can be calculated for all nine subscales and the total scale. For
the purpose of this research, only the gap score of the total scale was used
because it represents the QOL. The gap score ranges from -100 to 100; a low
(or negative) score reflects a better QOL. The QLSI has good reliability and
validity, with a Cronbach’s alpha of .87 for the gap score (G. Dupuis et al.,
2012).
Quality of Life Systemic Inventory for Children – tablet version
(QLSI-C©) (Touchèque et al., in press). QLSI-C is a self-report assessment
tool of QOL based on a modular approach for children 8 to 12 years aged. It

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 219 -
consists of a 20-items generic scale representing domains of life and
covering the child’s physical, emotional, cognitive, social and family
functioning. Scoring for the QLSI-C is similar to the QLSI (four scores: state,
goal, gap, rank). Only the gap score (i.e. QOL score) was used in this study.
As the QLSI, it ranges from -100 to 100; a low (or negative) score reflects a
better QOL. The QLSI-C has adequate reliability and validity, with a
Cronbach’s alpha of .71 for the gap score (Etienne et al., 2011).
2.3. Statistical analyses
Statistical analyses were conducted using SPSS 20.0 (IBM Corp., 2011)
while mediation analyses were performed using the PROCESS macro for
SPSS (Hayes, 2013). Sample t-tests were used to investigate differences in
means between mothers and fathers. Pearson’s correlations were
performed to identify the potential effects of demographic/illness
parameters on QOL in children with CF, so that these effects could be
controlled for in subsequent analyses. Then, simple regression and
mediation analyses were computed to test the mediations considered in this
research (see results). Level of significance for all analyses was set at p<.05.
3. Results
3.1. Demographics
Twenty six triads of children with CF (58% male – M age = 10.42 years;
SD = 1.17 – M FEV1 (% predicted) = 92; SD = 12.27) and their parents,
including 17 triads in Belgium and 9 triads in the United States, participated
in the study. Parents’ demographic parameters are summarized in Table 1.

RESEARCH STUDIES
- 220 -
Table 1 – Demographic data in families of children with CF
Mothers (n=26) Fathers (n=26)
Mean age 38.62 years
(SD = 3.81)
41.54 years
(SD = 3.95)
Education level
High school or less 42.3% 50%
Bachelor’s degree 38.5% 23.1%
Master’s degree 19.2% 26.9%
Marital status
Married/in couple 84.6%
Divorced/separated 15.4%
3.2. Descriptive statistics
Descriptive statistics for parenting variables (i.e. parenting stress,
illness perception, coping strategies) and QOL in parents and children with
CF are reported in Table 2. Comparisons between mothers and fathers of
children with CF using sample t-tests revealed no significant difference for
all the studied variables.
3.3. Bivariate correlations
Statistical covariates were identified by examining the relation of
demographic/illness parameters (i.e. child’s age, sex, culture, and FEV1,
mothers and fathers’ level of education) with children’s QOL. There was no
significant association of demographic/illness parameters with the child’s
QOL.

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 221 -
Table 2 – Descriptive statistics for the studied variables in families having a child
with CF
N Mean (SD)
Parents variables Mothers Fathers
Parenting stress 26 79.00 (23.94) 77.42 (25.06)
Illness perception 26 47.00 (8.61) 44.38 (9.91)
Coping I (frequency) 26 17.58 (1.53) 18.04 (1.22)
Coping II (frequency) 26 16.23 (1.93) 17.00 (1.72)
Coping III (frequency) 26 7.19 (1.30) 7.27 (1.56)
Quality of life 26 5.03 (3.39) 4.01 (2.89)
Children variables
Quality of life 25 3.46 (4.23)
3.4. Mediation analyses
To explore the mediation of parental QOL between parenting variables
(i.e. parenting stress, illness perception, coping strategies) and the child’s
QOL, three criteria need to be met: (a) parenting variables must
significantly predict child’s QOL; (b) parental QOL must significantly predict
the child’s QOL; (c) parenting variables must predict the parental QOL.
Simple regression analyses are summarized in Table 3. In this research,
three mediation analyses were considered: (1) the mediation of parental
QOL between parenting stress and the child’s QOL; (2) the mediation of
parental QOL between parental illness perception and the child’s QOL; (3)
the mediation of parental QOL between parental coping strategies and the
child’s QOL. The analysis of mediation succeeded when after controlling for
the effects of the parenting QOL on child’s QOL, the relation between
parenting variables and child’s QOL is significantly reduced (i.e. partial
mediation) or does no longer exist (i.e. complete mediation) (Baron &
Kenny, 1986).

RESEARCH STUDIES
- 222 -
Table 3 – Simple regression models predicting the influence of parenting
variables on QOL in children with CF
Dependent variable (i.e. child’s QOL)
Predictors B SE B Β T p r
Mothers
Parenting stress .090 .031 .519 2.910 .008 .52
Illness perception .164 .095 .338 1.723 .098 .34
Coping I (frequency) -.603 .563 -.218 -1.072 .295 -.22
Coping II (frequency) -.698 .434 -.318 -1.609 .121 -.32
Coping III
(frequency)
-.486 .665 -.151 -.732 .472 -.15
Quality of life .136 .263 .107 .518 .609 .11
Fathers
Parenting stress .020 .035 .116 .561 .580 .12
Illness perception .071 .086 .168 .819 .421 .17
Coping I (frequency) -.797 .701 -.231 -1.136 .268 -.23
Coping II (frequency) -.328 .620 -.110 -.529 .602 -.11
Coping III
(frequency)
-.433 .548 -.163 -.790 .438 -.16
Quality of life -.580 .296 -.393 -1.959 .064 -.39
3.4.1. Mediation of parental QOL between parenting
stress and QOL in children with CF
We ran a two regression analyses to examine whether the total score of
the PSI-4-SF (mothers and fathers) predict the QOL in children with CF.
Results showed that parenting stress in mothers was a significant predictor
of the child’s QOL (β = .52; t = 2.910; p = .008) whereas parenting stress in
fathers did not predict the child’s QOL (β = .12; t = .561; p = .580). This
result suggests that higher levels of parenting stress predict a worse QOL in
children with CF. Thereby, we run a simple regression analysis to test
whether mothers’ QOL predicts the child’s QOL. Results revealed that QOL
in mothers was not a significant predictor of the child’s QOL (β = .11; t =

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 223 -
.518; p = .609). Given these results, we did not run an analysis of mediation
to test whether parental QOL mediates the effect of parenting stress on the
child’s QOL.
3.4.2. Mediation of parental QOL between parental
illness perception and QOL in children with CF
We ran two regression analyses to examine whether the total score of
the BIPQ (mothers and fathers) predict the QOL in children with CF. Results
showed that illness perception in both mothers and fathers did not predict
the child’s QOL (mothers: β = .34; t = 1.723; p = .098; fathers: β = .17; t =
.819; p = .421). Since illness perception in mothers and fathers was not a
significant predictor of the child’s QOL, we cannot test the mediational
model in which parental QOL mediates the relation between parental illness
perception and the child’s QOL.
3.4.3. Mediation of parental QOL between parental
coping strategies and QOL in children with CF
We ran three simple regression analyses to examine whether the three
coping strategies (i.e. CHIP: pattern I, II and III) in mothers predict QOL in
children with CF. We replicate the procedure to test whether coping
strategies in fathers is a predictor of the QOL in children with CF. Results
revealed that none of the coping strategies in mothers and fathers was a
significant predictor of the QOL in children with CF. In consequence, we did
not run an analysis of mediation to test whether parental QOL mediates the
effect of parental coping strategies on the child’s QOL.

RESEARCH STUDIES
- 224 -
4. Discussion
Guided by the TSC model (Thompson & Gustafson, 1996), the purpose
of this study is to test the mediating role of parental QOL between parenting
variables (i.e. parenting stress, illness perception, coping strategies) and
QOL in children with CF. First of all, descriptive statistics indicated that
mothers and fathers of children with CF report similar level of parenting
stress, comparable representation of their child’s disease, symmetric use of
coping strategies and equivalent QOL. Previous researches on gender
differences in adapting to a child’s chronic disease have produced mixed
results. Related to childhood cancer, mothers and fathers reports of anxiety
and depressive symptoms and QOL did not differ (Frank, Brown, Blount, &
Bunke, 2001; Goldbeck, 2001). In contrast, others studies showed that
mothers reported more adjustment difficulties than fathers of children with
chronic disease (i.e. CF, juvenile rheumatoid arthritis, asthma, diabetes, etc.)
(Besier et al., 2011; Dewey & Crawford, 2007; Driscoll, Montag-Leifling,
Acton, & Modi, 2009; Quittner, DiGirolamo, Michel, & Eigen, 1992; Timko,
Stovel, & Moos, 1992). Some studies demonstrated that mothers and fathers
reported similar level of parenting stress (Yeh, 2002) whereas others
showed that mothers reported greater parenting stress than fathers
(Iwamoto, Santos, Skare, & Spelling, 2008; Quittner et al., 1992). In contrast
to our results, studies related to coping strategies to chronic disease in
childhood revealed consistent findings; mothers use more various coping
strategies and coped more effectively than fathers (Abbott, 2003; Dewey &
Crawford, 2007; Goldbeck, 2001). Therefore, the specific role of gender in
parenting a child with a chronic disease still needs further investigations.
Second, the assumption based on the Transactional Stress and Coping
model (Thompson & Gustafson, 1996) that parental QOL mediated the
effect of parenting variables (i.e. parenting stress, illness perception, coping
strategies) on the QOL in children with CF was not confirmed. None of the

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 225 -
parenting variables did predict the QOL in children with CF, except
parenting stress in mothers. This results is consistent with a group of
research in chronic disease in childhood (i.e. diabetes, cancer) indicating a
link between maternal processes (i.e. parenting stress, parental
overprotection, perceived child vulnerability) and child adjustment (Colletti
et al., 2008; Hullmann, Wolfe-Christensen, Meyer, McNall-Knapp, & Mullins,
2010; Moreira, Frontini, Bullinger, & Canavarro, 2014). Overall, findings
from our research suggest a poor influence of the parenting variables on the
QOL in children with CF. In addition, our findings did not confirm the
transactional relation between parent and child adjustment (i.e. QOL) which
is not consistent with previous research (Chaney et al., 1997; Colletti et al.,
2008; Hocking & Lochman, 2005; Thompson et al., 1992). These
observations might be explained by methodological issues. Literature
provides nuanced conceptualization of adjustment revealing the
multifaceted nature of the concept (Stanton et al., 2007). Whereas most of
studies on adjustment to chronic disease in childhood have typically
focused on psychological distress (i.e. anxiety or depressive symptoms), the
current study examined the contribution of another conceptualization of
adjustment (i.e. QOL). Our methodological choice might account for the
absence of link between parents and child adjustment. Moreover, the
identity of the disease (i.e. time of diagnosis) may be another possible
explanation to our findings. All children included in our research were
diagnosed with CF few months after birth whereas children with cancer (on
treatment; Mean age of diagnosis = 6 years old) or diabetes (diagnosed after
age of 8 years), for example, lived without the disease for a period of time.
In contrast to other parents of children with chronic illness, parents of
children with CF develop child-rearing practices that include the disease.
Therefore, children with CF are used to a certain level of distress or
uncertainty in their parents because they have to deal with the constant
worry of the unpredictability of CF since their child’s birth. This

RESEARCH STUDIES
- 226 -
phenomenon might explain the absence of link between parenting variables
and QOL in children with CF.
Findings from the current study should be considered preliminary due
to several limitations. First, the design used in this research was cross-
sectional which is not sufficient to demonstrate the causal relation between
parental variables and children’s adjustment. In addition, because of the
transactional nature of the parent-child relation (Thompson & Gustafson,
1996), it would be interesting to examine the reciprocal influences between
parents and child. Second, the generalization of the findings is limited by the
small sample size. Further studies would benefit from a larger sample.
Third, although a majority of families who consented to participate
completed the study, 15% Belgian families and 55% American families
dropped out suggesting that selection bias may have affected the results.
Fourth, we used different sample collection procedures (Belgium: home vs
United States: hospital) which may influence findings from this study.
Future researches should guarantee similar procedures.
In conclusion, at the present, studies examining the relation between
fathers’ variables and child adjustment in pediatric chronic disease are
scarce. When research attempts to include fathers, they represent a
minority (15% or less). Even though this study did not highlight differences
between mothers and fathers in their way to influence the child’s
adjustment, we believe in the importance of including both parents in
pediatric research (see Phares et al., 2005). This absence of relation may be
explained by the fact that we choose the QOL as conceptualization of
adjustment in both parents and children. Therefore, future research could
examine the mediating role of another parental adjustment outcome (ex.
anxiety or depressive symptoms) between parenting variables and QOL in
children with CF.

CHAPTER 11 – TSC MODEL IN FAMILIES OF CHILDREN WITH CF
- 227 -
Acknowledgements
Authors would thank Dr. Jean-Paul Sacré and Dr. Frédéric Pierart from the CF
Center of Liege (Belgium), Dr Jonathan Spahr and Dr. Daniel Weiner from the
CF Center at the Children’s Hospital of Pittsburgh, Linda Baer (center
coordinator) and Alliene Farley (dietician) form the WVU’s Mountain State CF
Center as well as Courtney Bee from West Virginia University for their kind
assistance in data collection. This study was a part of a 4-year research project
entitled, “Quality of life in children with cystic fibrosis” supported by the Health
Psychology Unit at the University of Liège (Belgium).


Discussion


- 231 -
Discussion
Guided by theoretical considerations (see Part 1: theory), the overall
purpose of this research is to explore quality of life (QOL) and its predictors
(individual and family contextual) in school-aged (8-12 years old) children
with CF. Furthermore, this objective spits into four sub-aims; each sub-aim
having been the subject of a research study (see Chapter 8, 9, 10 & 11). This
discussion section presents: (1) a summary of the theory (2) a summary of
the main results for each study; (2) the questions raised by our findings, (3)
the strengths and limitations of our research as well as future perspectives;
and (4) the clinical implications.
1. Theory summary
The five chapters of theory presented at the beginning of this work
provide a theoretical framework for the research topic addressed in this
dissertation (i.e. QOL in children with CF). Chapter 1 (i.e. CF) attempts to
describe a particular chronic disease, namely CF, to those without a
rigorous medical background. It brings to light the difficulties of daily
treatment regimens used to treat CF; many of which are complex and time-
intensive. (Besier & Goldbeck, 2011) Therefore, management of the disease
may uniquely impact patient’s life. As a result, medical providers in CF care
centers seek not only to improve patients’ health but also to enhance their
QOL, which is regarded with equal importance to medically beneficial
therapies (Royce & Carl, 2011). However, QOL in children with CF under the
age of 12 years has been under-investigated in comparison to QOL in
adolescent and adult patients. Therefore, this chapter demonstrates the
relevance for studying QOL in a pediatric CF population.
Chapter 2 (i.e. Measurement of the QOL in children) highlights conceptual
and methodological considerations when assessing QOL in a pediatric

DISCUSSION
- 232 -
population. It shows that confusion exists about the definition and the
assessment of the QOL in children. Moreover, pediatric researchers and
clinicians face age-related issues, such as questionnaires being
developmentally appropriate for all ages, when measuring QOL in children
(e.g. level of comprehension, self vs proxy report, adaptation of the format)
as well as issues about the use of generic vs specific tool. Although
measuring QOL in children still poses some challenges, it represents an
important therapeutic goal in the management of a chronic disease. This
assessment provides the patients’ perception of the disease impact on his or
her well-being; thus evaluating functioning in physical, mental, emotional,
social, and everyday life domains (Bullinger et al. 2006; Royce & Carl, 2011).
Thus, QOL was considered, in this research project, as a conceptualization of
adjustment to CF in childhood.
Chapter 3 (i.e. theoretical models of adjustment to chronic disease)
presents theoretical models available in health psychology to predict
health-related outcomes such as QOL: the Common Sense Model of Self-
Regulation (Leventhal et al., 1980); the Transactional Model of Stress and
Coping (Lazarus & Folkman, 1984); and the Integrative and Multifactorial
Model. (Bruchon-Schweitzer, 2002) However, these models were initially
developed using adult populations. An adaptation for their application in
childhood would strengthen the theoretical basis in pediatric research.
Since children are still undergoing development, this perspective should
take into account some developmental considerations.
Chapter 4 (i.e. conceptualization of illness in children) presents the
development and understanding of the concept of illness in children based
on two approaches. On one hand, the cognitive approach postulates that
difficulties in conceptualization of illness in childhood reflect an overall
intellectual immaturity; the development of the illness concept being
incomplete before the age of 11-12 years. However, on the other hand, the
biological approach postulates that the development of the concept of

DISCUSSION
- 233 -
illness in childhood depends on the increase of knowledge in the domain of
biology. Some authors suggest that notions of biology do not emerge until
the age of 10 years (Carey, 1985, 1995) whereas others assert that certain
biological knowledge (e.g. contagion and contamination processes, germs as
infectious agents) appear in preschoolers (Inagaki & Hatano, 2005; Kalish,
2005; Solomon & Cassimatis, 1999). Overall, both approaches suggest that
conceptualization of illness in childhood is incomplete; thus possibly
leading to misinformation and unfounded concerns about CF which, in turn,
may influence children’s health outcome such as QOL. Therefore, illness
representation appears to be important to assess when studying QOL in
children with CF. Moreover, although these approaches provide some
fundamentals, other theories highlight the constant interactions between
individual’s behaviors, cognitive functioning and environment (e.g. family
contextual factors) (i.e. learning theories: Skinner and Bandura in Bideaud,
Houdé, & Pedinielli, 2002). Thereby, it also seems essential to consider
environmental contributions, such as parental factors, to children’s
experience of illness.
Chapter 5 (i.e. role of family contextual factors on children’s adjustment
to chronic disease) describes a theoretical model for understanding the role
of family contextual factors (i.e. parental variables) in children’s adjustment
to chronic disease: the Transactional Stress and Coping Model (Thompson
et al., 1992). However, this model focuses exclusively on the role of
mothers, whereas the importance of inclusion of fathers in pediatric has
been demonstrated (Phares et al. 2005). Therefore, to better understand
how parental variables influence children’s adjustment to a chronic disease
(e.g. CF), there is a need to move beyond an exclusive focus on mothers and
consider the role of both parents (Ievers & Drotar, 1996; Phares et al.,
2005). Guided by this observation, an adapted version of the model,
including both maternal and parternal variables, was tested (see Chapter
11).

DISCUSSION
- 234 -
2. Results summary
Study 1 entitled “A comparison of a Tablet version of the Quality of life
Systemic Inventory for Children (QLSI-C) to the standard paper version”
aimed to examine psychometric characteristics of a technology-based (i.e.,
tablet administration) approach for measuring quality of life (QOL) in
school-aged (8-12 years old) children by (a) investigating the score
equivalence between the QLSI-C modes of administration (tablet format vs
original paper format); (b) assessing the internal consistency of the tablet-
administered QLSCI-C scores; (c) examining the test-retest reliability of the
tablet-administered QLSCI-C scores.
Study 2 entitled “Anxiety, depression and quality of life in school-aged
children with Cystic Fibrosis: A cross-cultural study” aimed to (a) compare
anxiety, depressive symptoms and QOL between children with CF and
healthy youth in a matched control group and (b) investigate the relation of
anxiety and depressive symptoms with QOL in a multicultural sample (i.e.
Belgium and USA) of school-aged children with CF.
Study 3 entitled “Applying the Common-Sense Model of Self-Regulation to
Pediatric Cystic Fibrosis: Identifying Psychosocial Factors Associated with
Quality of Life” aimed to examine mediational relations of the cognitive and
emotional pathway of the Common Sense Model of Self-Regulation (CSM) in
a pediatric population with cystic fibrosis (CF). This studies aim is to
investigate whether: (a) coping strategies mediate the effect of emotional
and cognitive illness representation on QOL; (b) psychological disturbance
mediates the effect of emotional illness representation and coping
strategies on QOL.
Study 4 entitled “Parenting stress, parental illness perception and coping
strategies associated with Quality of life in children with Cystic Fibrosis: the
mediating role of parental adjustment” aims to examine whether parental
QOL acts as a mediator of the relation between parenting variables and QOL

DISCUSSION
- 235 -
in children with CF in a multicultural sample of families having a child with
CF (8 to 12 years old). Guided by the Transactional Stress and Coping
model, the purpose of this study is to test whether parental QOL acts as a
mediator of the relation between parenting variables (i.e. parenting stress,
illness perception, coping strategies) and the child’s QOL while considering
the specific effect of both mother- and father- related variables on the
child’s QOL.
In order to provide a comprehensive and succinct vision of the findings
highlighted in this dissertation, a summary of the main results is presented
Table 1.
Table 1 – Main findings of the studies presented in this dissertation
Results
Study 1 The good concordance of the QLSI-C scores across
methods of administration establishes the score
equivalence of the tablet-administered QLSI-C in
comparison to the original paper format.
Internal consistency reliability yielded acceptable
Cronbach’s alphas for all QLSI-C scores, with all α >.70.
Test-retest analyses for the tablet-administered QLSI-C
demonstrated stability over time for all QLSI-C scores,
except the state score

DISCUSSION
- 236 -
Table 1 (suite) – Main findings of the studies presented in this dissertation
Results
Study 2 In the United-States, children with CF reported similar
level of anxiety, depressive symptoms and QOL than
healthy children.
In Belgium, children with CF reported similar level of
anxiety, higher rates of depressive symptoms and a
poorer QOL than the control group.
In both countries, higher anxiety and depressive
symptoms are related to poorer QOL.
Study 3 The mediational role of coping strategies between the
cognitive and emotional representation of illness and QOL
was not confirmed.
Psychological disturbance mediates the effect of
emotional illness representation on QOL.
Psychological disturbance mediates the effect of emotion-
focused coping strategy on QOL.
Study 4 Mothers and fathers of children with CF did not differ in
terms of parenting stress, illness perception, coping
strategies and QOL.
None of the variables in fathers did predict QOL in
children with CF.
Parenting stress in mothers predicted QOL in children
with CF.
The mediational role of parental QOL between parenting
variables and the child’s QOL was not confirmed.

DISCUSSION
- 237 -
3. Related topics
Findings from our studies raised questions for discussion. Although
some issues were debated in our manuscripts, this section gives a view of
the discussed topics from a different angle. Study 1 has inspired the
discussion of two related topics: use of electronic health-related measures
(e-Health) for gathering information from children with a chronic illness
(see 3.1.) and evidence for a definition and a measurement of the QOL in
terms the discrepancy between the current situation and the expected (see
3.2.). Study 2 has led to discuss the notion of resilience in pediatric chronic
disease (see 3.3.). Study 3 has led to consider cognitions, behaviors and
emotions through the eyes of those with a chronic disease that are still
undergoing development (see 3.4.). Finally, study 4 has inspired the
discussion of the influence of both mothers and fathers in the child
adjustment to a chronic disease (see 3.5.).
3.1. Using e-Health assessment in pediatric
Study 1 provides support for our technology-based (i.e. tablet
administration) approach for measuring QOL in school-aged children using
the Quality of Life Systemic Inventory for Children (QLSI-C©). Since
technology (i.e. computers, cell phones, Internet, etc.) has infiltrated
modern life, using it for assessment purposes in pediatric psychology has
major advantages for children and interviewers. First, today’s children are
exposed to smartphones and digital tablets at birth. This growing
prevalence of technologies in our society makes them appealing to many
children. For example, this medium allows the incorporation of colors,
smileys, graphics and sounds within the questionnaire to make it fun and
interesting for the child to complete. Our research experience supports this
observation by highlighting that the use of e-Health technology for

DISCUSSION
- 238 -
assessment purposes in pediatric psychology increases the motivation of
children to participate in the study. This proves very useful in the
recruitment of participants with a chronic disease (i.e. CF) where children
and their families are often overwhelmed with research studies. Second, it
makes fast, simple and convenient testing. This argument can also be useful
in the recruitment speech to increase the child’s motivation. Third, the
electronic scoring eliminates manual data entry and thus, reduces
transcription errors as well as workload by researchers. In addition to these
benefits related to e-Health technology, using a tablet format of the QLSI-C
(i.e. application for Androids) instead of a web- or computer-based mode of
administration (e.g. PedsQL, Exeter HRQL, KIDSCREEN-27, etc.) offers the
following advantages: the touch screen is more attractive, especially for
children; there is no need to have internet access; and the tablet is easy to
carry, especially in the context of data collection in hospitals or at home.
However, e-Health researchers may encounter logistical issues when
developing, testing and disseminating these technology-based assessment
tools in the pediatric population. Recently, Wu, Steele, Connelly, Palermo,
and Ritterband (2014) reviewed the key challenges associated with the
development and the implementation of e-Health interventions. Based on
their commentary, an overview of the tasks and considerations for
planning, developing, testing and disseminating e-Health assessment tools
is provided hereafter. When planning the e-Health assessment tool creation,
researchers face challenges associated with assembling a team for
collaboration (e.g. at minimum a pediatric psychologist and a technology
developer/programmer are needed) and discussing financial
considerations. The choice of the programmer may depend on the financial
resources available. For example, hiring an internal programmer (i.e. within
the academic or hospital-based institution) are of lower cost, more familiar
with institutional technology policies and more easily accessible than
external programmers (i.e. commercial consultants); however, they may not

DISCUSSION
- 239 -
have the programming experience required for the project. The choice of
the programmer also depends on which support the researcher wants to
use for the program or application development. For example, only some
programmers have the experience in the development of applications for
Apple products (i.e. iOS). As a result, before selecting the technology
developers, it may be important to consider the support that will be used
for the e-Health tool development (e.g. smartphones, tablets, computers,
Apple products, etc.). When team members are selected, communication
between them is essential to share a common understanding of the content
and design elements of the application. Again, this stage is guided by
financial considerations. Since development of programs and applications
are usually expensive, researchers have to prioritize which elements will be
designed in the current project based on their budget. Note that in addition
to the salary support for technology development, ongoing technical
support needs to be included in the budget. In summary, challenges that e-
Health pediatric researchers have to face at this stage are: (1) selecting the
technology developer depending on the best cost-benefit ratio and support
for the e-Health tool and (2) getting financial resources for the current
project.
When designing the program or application, pediatric researchers have
to consider ethical concerns including issues of recruitment, informed
consent, debriefing, privacy and confidentiality, data security, participant
safety (i.e. how to disclosure of abuse, suicidal thoughts or other behaviors
of concern will be addressed) (Henderson, Law, Palermo, & Eccleston,
2012). Especially, these considerations are important in case of a self-
administered e-Health tool (e.g. web-based questionnaires) in comparison
to a face-to-face interview using a technology-based assessment tool (e.g.
our tablet-administered QLSI-C) where the interviewer ensure participant
security, privacy and safety. Moreover, researchers may face logistical
issues when creating the e-Health assessment tool. For example, each

DISCUSSION
- 240 -
product (Apple, windows, etc.) has its own policy regarding the
development of a program or an application (e.g. buy a developer license).
Another concern to take into account when implementing a technology-
based assessment tool is the data management (e.g. prevent missing or
inaccurate data, consider data storage and exportation, monitor incoming
data for accuracy); especially when collecting data online with a large
number of participants (Wu et al., 2014).
Finally, the dissemination of a pediatric e-Health assessment tool also
requires some considerations such as how to share the program or
application with the scientific community. Some of these situations may
include partnership with a commercial entity or freely distributed,
marketing to clinicians and researchers at conferences, etc. (Wu et al.,
2014).
In conclusion, the choice of using a handwritten or a technology-based
questionnaire administration depends on a cost-benefit analysis. Creating
and testing pediatric focused e-Health assessment tools raise many
challenges. However, results from the study 1 (i.e. score equivalence across
modes of administration: original version vs tablet version. Reliability of
the tablet-administered QLSI-C) combined with the advantages offered by
the tablet format provide support for the eHealth assessment modality and
encourage both clinicians and researchers to consider using eHealth
technologies in assessment in pediatric psychology.
3.2. Evidence for our definition and measurement of the
QOL
Considerable diversity exists in the conceptualization of the QOL in the
pediatric population with no consensus being established (Eiser & Morse,
2001c; Matza et al., 2004; Wallander, Schmitt & Koot, 2001). Thenceforth,
we adopted the conceptualization of Dupuis et al. (1989) for the definition

DISCUSSION
- 241 -
and the measurement of the QOL in this research project. The theoretical
framework that supported this conceptualization is inspired by the
systemic approach on biologic systems, cybernetics and the definition of
QOL, based on the notion of discrepancy and the Aristotelian notion of
happiness. In this model, all human activities are oriented towards an end
(a goal), that certain ends are subordinated to others but that the ultimate
end is the pursuit of happiness (Dupuis et al., 1989). Therefore, Dupuis et al.
(1989) have defined QOL as follow: ‘‘QOL is, at a given time, a state that
corresponds to the level attained by a person in his pursuit of hierarchically
organized goals’’. The measure of the QOL (i.e. QLSI-C©) developed on the
basis of this approach considers QOL as the difference between the current
state as well as the child’s expectations, weighted by the speed of
improvement, deterioration and the importance assigned for each life
domains. In contrast to most of QOL questionnaires that estimate this
concept as a current state, the QLSI-C goes beyond this single concept taking
into consideration the child’s expectations and evaluating their priorities
(i.e. individual perception of the importance of each life domains) in the
QOL measurement.
First, evidence for this definition and measurement of the QOL was
provided by findings from study 1. While the QOL score (i.e. gap score) was
stable over time (i.e. two week-intervals), the state score showed temporal
instability after a period of two weeks. My experience during face-to-face
interviews with children has suggested that children’s perception of well-
being can quickly change depending on everyday life events (e.g. being
bothered by sibling, eating something he/she doesn’t like, etc.). Moreover,
we observed that it is difficult for children to answer QOL questions
considering their overall mood over the past few weeks because it is recent
events (i.e. from the same day or the day before) that make a difference in
how children respond to the QLSI-C. Thus, measuring QOL as a current state
appears to be highly dependent on children’s perception that day whereas

DISCUSSION
- 242 -
estimating QOL as a difference between the child’s current situation and his
or her expectations seems to be more stable.
Second, the QOL definition and measurement as conceptualize by
Dupuis et al. (1989) is supported by the fact that the QLSI-C follows most of
the guidelines established by Wallander, Schmitt and Koot (2001) for
evaluating QOL measures in children. First, the QLSI-C is based on a
theoretical framework (see Appendix 1) that operationalizes a clear and
generic definition of the QOL (see above). Second, it includes broadly
encompassing QOL domains (physical, psychological and social) applicable
to all children. Third, it recognizes the subjective nature that defines the
concept of QOL by using a self-report mode of administration providing
information about the child’s perspective. Indeed, the QLSI-C defines the
QOL as the discrepancy between the child’s current situation and the
expected (i.e. objectives); these situations are positioned in reference to the
ideal situation (i.e. to be perfectly happy with […]) which is conceptualized
differently in each child. Third, the QLSI-C, in contrast to most QOL
measures, assesses the importance assigned to each life domain and the
satisfaction on domains is weighted by the perceived importance to the
child. Fourth, the QLSI-C demonstrates satisfactory psychometric
characteristics for the original and tablet version providing norms for the
general population (Etienne et al., 2011; Touchèque et al., in press). Fourth,
because the QLSI-C is based on a modular approach, it allows comparison
between the background population and a specific group of children such as
a pediatric cancer population (Missotten, Fonseca, Dupuis, Spitz, & Etienne,
2012; Lemétayer, Lanfranchi, & Chastagner, 2015). Fifth, the QLSI-C
recognize explicitly that children are developing beings by providing
different forms of the questionnaire depending on the child’s age (i.e. 8-12
years old: QLSI-Children version; 13-18 years old: QLSI-Adolescent version;
18-64 years old: QLSI adult version; and 65+ years old: QLSI-Senior
version). The children version has different items set, response formats (e.g.

DISCUSSION
- 243 -
illustrations) and support (i.e. tablet administration for the children version
vs paper and pencil administration for the other version).
3.3. Resilience in chronically ill children and their family
Findings from study 2 raised questions about the notion of resilience in
children with CF. Indeed, results revealed that level of anxiety and rates of
depressive symptoms in school-aged children with CF are similar to their
healthy peers. Although children with CF have much to overcome, findings
from study 2 suggest they develop into psychologically well-adapted
individuals and, thereby, are referred to as resilient.
Resilience is a psychosocial construct referring to the maintenance of
psychological and physical well-being by individual despite experiences of
significant adversity (Luthar, Cicchetti, & Becker, 2000; Yi, Vitaliano, Smith,
Yi, & Weinger, 2008). It includes three components: interpersonal (i.e. self-
esteem, optimism, self-efficacy, self-mastery), coping (i.e. assertiveness,
endurance, kindness, resourcefulness, autonomy, responsibility, flexibility)
and intrapersonal (i.e. intimacy, sensitivity, tactful social skills and
cooperation) (Kim, Unpublished doctoral dissertation1). This construct is
worth exploring in the context of a chronic disease such as CF, since school-
aged children experience many adversities that may prevent the
accomplishment of normal developmental task (Ernst, Johnson, & Stark,
2010). Peer- and treatment- related challenges are the major issues that
school-aged children with CF have to face. Some of which, may have
profound and lasting effects on their psychological adjustment (Ernst,
Johnson, & Stark, 2010). Peer relationships play an essential role in
psychosocial development of school-aged children because their identity
and sense of competence begin to develop through a process of peer
comparison (Reis, Collins, & Berscheid, 2000). School-aged children with CF
1 Cited by Kim & Yoo (2010)

DISCUSSION
- 244 -
develop concerns about “being different” (e.g. frequent coughing, more
fatigue, school absences, treatment requirement, etc.) than their peers and
realize at a deeper level the impact of their disease on multiple aspects of
their life (D'Auria, Christian, & Richardson, 1997). In addition to these
psychosocial challenges, school-aged children with CF have to deal with the
time intensive nature of disease management that may interfere with school
and peer-related demands of childhood (Modi et al., 2006). This treatment
burden may compromise health-related behaviors (e.g. adherence) in
school-aged children with CF (Ernst, Johnson, & Stark, 2010). For these
reasons, CF in childhood could be a significant risk factor affecting healthy
growth and development. However, despite the multitude of challenges,
study 2 suggests that children with CF remain psychologically healthy.
Therefore, using the resilience paradigm might be an interesting approach
to adopt in pediatric CF. Using this approach, will allow health professionals
who seek to identify the strengths and abilities of children with illness, help
individuals solve problems by utilizing their own strengths and resources
(Dong H. Kim & Yoo, 2010).
Although the concept of resilience has been studied in childhood, most
of literature available is in a pediatric cancer population (e.g. Brody &
Simmons, 2007; Kim & Yoo, 2010; McCubbin, Balling, Possin, Frierdich, &
Bryne, 2002; Orbuch, Parry, Chesler, Fritz, & Repetto, 2005; Phipps, 2007).
To date, no studies have investigated this concept in children with CF.
However, we hypothesize that the concept of resilience might be employed
to explain the level of adjustment in children with a chronic illness such as
CF. Therefore, it would be an interesting perspective to examine resilience,
identify individual (e.g. personality) or contextual (e.g. school, family,
friends, etc.) factors associated with this concept in order to better
understand variables that help children to be well-adapted despite
adversity.

DISCUSSION
- 245 -
3.4. Emotions, cognitions and coping in children with
chronic disease
Childhood is the most important period of development in human life.
Therefore, emotions, cognitions, and behaviors in children are
interconnected with age-related factors; thus possibly playing a role in
shaping adaptational process to stressful situation (e.g. illness). In
particular, relations between affectivity, beliefs and coping as well as their
influence on health outcomes (e.g. QOL) in children experiencing a chronic
disease might be different than in adult patients. For instance, study 3
revealed that coping strategies did not act as a mediator of the relation
between illness representations (i.e. emotional and cognitive) and QOL in
school-aged children with CF. Therefore, in contrast to the Common Sense
Model of Self-Regulation (Leventhal et al., 1980) that involves a sequence of
three stages (i.e. 1: illness representations – 2: coping – 3: appraisal), we
suggested that children with CF develop three parallel, yet interrelated,
types of information processing based on their emotional reactions,
cognitions and coping strategies; which in turn, influence emotional and
health-related outcome (see Chapter 10; Figure 4). In addition, findings
from study 3 highlighted that emotional pathway (i.e. emotional illness
representations, emotions-focused coping and psychological disturbance)
might play an important role in determining QOL in school-aged children
with CF. This hypothesis is in line former research which suggests that
understanding emotions emerges first in childhood and supports the ability
to understanding the minds and to relate actions to beliefs (Dunn, 2000;
Dunn, Brown, Slomkowski, Tesla, & Youngblade, 1991; Hughes & Dunn,
1998). However, further investigations are need since there remains a lack
of clear empirical evidence on how the three constructs are associated
longitudinally (i.e. causal relations) in pediatric childhood.

DISCUSSION
- 246 -
3.5. Role of mothers and fathers in pediatric chronic
disease
Surprisingly, finding from study 4 revealed no strong relation between
parenting behaviors (i.e. parenting stress, illness perception and coping
strategies) in both parents and QOL in children with CF, which is not
consistent with previous researches in childhood chronic disease (Chaney
et al., 1997; Colletti et al., 2008; Hocking & Lochman, 2005; Hullmann et al.,
2010; Moreira et al., 2014; Thompson et al., 1992). This absence of relation
might be explained by methodological issues. For instance, literature
provides nuanced conceptualization of adjustment revealing the
multifaceted nature of the concept (Stanton et al., 2007). The current study
examined the contribution of one conceptualization of adjustment (i.e. QOL)
while most of studies on adjustment to chronic disease in childhood have
typically focused on psychological distress (i.e. anxiety or depressive
symptoms). Therefore, our methodological choice might account for the
absence of link between parents and child adjustment.
Moreover, findings from study 4 also highlighted the absence of specific
effect of sex (female caregiver vs male caregiver) on QOL in children with
CF. For example, we did not confirm our hypothesis suggesting that QOL in
these young patients would be influenced by different parenting variables
depending on sex or that the direction of the relation between parenting
variables and QOL in youths with CF would be different depending on sex.
In addition, study 4 revealed no differences in parenting variables between
mothers and fathers of children with CF. These results may be explained by
conceptual issues, such as confusion between sex and concept of gender.
For instance, our hypotheses was based on the gender role theory (i.e. Bem,
1981) that posits a difference between the role of fathers and mothers in
the domains of housework and child rearing based on gender divisions in
social structures and family roles (Russell & Saebel, 1997). For example,

DISCUSSION
- 247 -
mothers are more nurturing, warm and predictable while fathers are more
physical, unpredictable, challenging and initiating play when it comes to
child rearing (Le Camus, 1995). These gender differences result in the
socialization in a “masculine” and “feminine” sex-types behaviors and
characteristics in childhood (Russell & Saebel, 1997). Masculinity refers to
aggressiveness, action, self-confidence, dominance and competition and is
aimed at the male sex. Femininity refers to emotionality, warmth, empathy
and creativity and is aimed at the female sex (Spence & Helmreich, 1980).
Therefore, although it is widely accepted that mothers and fathers interact
differently with their child (i.e. complementarity roles), our findings might
suggest that parents would adopt symmetric gender-related roles when
facing adversity such as caring for a child with life-threatening, time-
consuming chronic disease.
4. Strengths, limitations & futures perspectives
4.1. Strengths
Strengths of this research project are highlighted hereafter. First, the
application of theoretical frameworks (CSM – Leventhal et al., 1980; TSC –
Thompson et al. 1992) in pediatric CF sheds light on individual and family
contextual factors that influence health outcome (i.e. QOL) in children with
CF. In addition, given the limited literature on psychosocial functioning in
children with CF, this dissertation offers state-of-the-art information that
would be helpful to CF health care teams in their interaction with children
and their families. Second, this research project proves innovative due to
the inclusion of the father’s perspective. This allows research to move
beyond an exclusive focus on mother’s perspective in the understanding of
how parental variables influence QOL in children with CF. Third, the
methodology used was carefully reviewed to appropriately apprehend
concepts addressed in this research project. For instance, measures used in

DISCUSSION
- 248 -
this dissertation have been selected based on their psychometric properties
(i.e. available validation study), their appropriateness for the studied age
group (8 to 12 years old), their appropriateness for both a clinical and a
non-clinical population, their relevance in a context of a chronic disease and
their frequency of use in the literature. Fourth, this study provides a unique
perspective, pulling samples from both a European population and a North
American population. Although few differences were discovered, this aspect
can be used to the health-care professional’s advantage; making the
distinction between the varying needs of both populations may in turn
improve health outcomes (e.g. QOL) in the future.
4.2. Limitations
This study suffers from some limitations. First, the design used in this
research project was cross-sectional which is not sufficient to demonstrate
causal relations of individual (see study 3) and family contextual (see study
4) factors with QOL in children with CF. Therefore, future research should
consider longitudinal studies to assess, for example, the causal relation
between psychological disturbance and health outcome (e.g. QOL) in
children with CF.
Second, the generalization of the findings is limited by the small sample
size in all CF studies presented in this research (study 2, 3, and 4). Further
studies would benefit from a larger sample. However, it is worth to mention
that while it is clear that American CF families who participated in this
research project are not representative of the American CF population,
Belgian CF families included in these studies are representative of the
French-speaking Belgian population. Around fifty children with CF are
between the age of 8 and 12 years in the French-speaking side of Belgium
(i.e. Wallonia) (Belgian Association against Cystic Fibrosis, personal

DISCUSSION
- 249 -
communication, January 2012). Therefore, despite the small sample size,
our sample represents 40% (n=20) of the CF population in Wallonia.
Third, selection bias may be occurred in studies from this research
project. Indeed, participation rates for study 4 were 47% in Belgium and
28% in the United States. In addition, among the families who consented to
participate in the study 4, 15% Belgian families and 55% American families
dropped out (i.e. did not send study package back). Since one of the
inclusion criteria was to have both parents (mothers AND fathers) to
participate in the study, we hypothesize that both parents (especially
fathers) who participated in the study were more involved in the
management of the disease than parents who did not participate. Therefore,
a selection bias may have affected the results. For instance, it may explain
findings in study 4 that showed no difference between mothers and fathers
of children with CF as well as no difference in their way to influence QOL in
children with CF.
Fourth, different sample collection procedures (Belgium: home vs
United States: hospital) were used and may account for a part of the culture
effect in the study. Since being at the hospital may cause anxiety or stress in
some children, we hypothesize that children with CF who completed the
research protocol at home may have felt more comfortable in reporting
some difficulties than children with CF who completed the study at the
hospital. This hypothesis would explain findings in study 1 showing that
Belgian children with CF reported a higher rate of depressive symptoms
and a poorer QOL than American children with CF. Future researches
should guarantee similar research procedures.
4.3. Future perspectives
This section aims to suggest new perspectives for future research. First,
the TSC model posits a transactional relation between the parent and child

DISCUSSION
- 250 -
adjustment. However, this study only examined the influence of parenting
variables on QOL in children with CF without considering the impact of the
child adjustment on parenting variables. Thereby, because of the
transactional nature of the parent-child relation in the TSC model, it would
be interesting to examine the reciprocal influences between the parents and
the child in future research as well as the influence of the father’s
adjustment on the mother’s adjustment, and vice versa.
Second, discussion with CF medical teams and clinical observations
made during this research project suggest that dealing with medical aspects
of CF (e.g. pulmonary and digestive issues, treatment hassles, etc.) is the
priority for CF health staff and parents of children with CF; psychological
concerns being secondary. In addition, children with CF are not self-
managing their disease; parents do. Therefore, combining psychosocial
variables with a medical variable that represents a priority for CF teams and
families (e.g. treatment adherence, physical activities) in pediatric
psychology studies might be an interesting perspective for future research.
Third, we believe that QOL measurement in terms of discrepancy
between the child’s current situation and his or her expectations is
appropriate in pediatric health psychology. However, literature related to
goal setting and achievement in pediatric chronic disease is limited.
Therefore, future QOL studies in pediatric chronic disease should consider
not only the child’s subjective perception but also his or her aspirations (see
Campbell, Converse, & Rodgers, 1976) (WHOQOL Group, 1993). Moreover,
goal setting and goal achievement notions might be an interesting
perspective for future research investigating health outcome in children
with chronic disease.
Fourth, at the present, studies examining the relation between fathers’
variables and child adjustment in pediatric chronic disease are scarce.
When research attempts to include fathers, they represent a minority (15%
or less). Even though study 4 did not highlight specific effect of parents’ sex

DISCUSSION
- 251 -
in relation to QOL in children with CF, we believe in the importance of
including both mothers and fathers in pediatric research. Since the previous
debate (see section 3.5.) highlighted that the gender effect (masculinity vs
femininity characteristics) might be more relevant than sex effect (male vs
female), future research could investigate the relation of family roles and
behaviors with QOL in children with CF.
Fifth, future research could also examine whether QOL in children with
CF was associated with parental characteristics rather than gender-related
characteristics. For instance, we hypothesize that some parents,
independently of their sex, are distinguished from other parents depending
on parental dimensions (e.g. parents with a high level of parenting stress
and a threatening perception of the disease vs parents with a low level
parenting stress and a less threatening perception of the disease); thus
possibly being associated with QOL in children with CF.
5. Implications for practice
Literature is insufficient in regard to psychosocial well-being in school-
aged children with CF. Therefore, usefulness of this dissertation is based on
the fact that it has shed light on a missing piece in pediatric CF literature.
Implications of findings from this research project will be discussed in this
section.
First, psychometric characteristics of the tablet version of the Quality of
Life Systemic Inventory for Children (QLSI-C©) has been demonstrated in the
study 1 (see chapter 8). Advantages of the use of technology for assessment
purposes in pediatric psychology have been discussed in section 2.1. of this
chapter. In addition to these advantages, the use of the QLSI-C has a clinical
advantage. In contrast to most QOL measurement, the QLSI-C provides
different scores: the state score (i.e. current situation), the goal score (i.e.
child’s aspirations), the rank score (i.e. importance assigned to each life

DISCUSSION
- 252 -
domains) and the gap score (i.e. QOL composite score based on a
multiplicative model). These scores can be useful in clinical practice with
children because they help to determine at which level the child’s problem
lies. For example, children may have a poor QOL because: (1) their
expectations are too high; (2) they cannot prioritize their life domains (i.e.
all domains are assessed as essential); or (3) their expectations are realistic
but their current situation is problematic. This QOL assessment tool helps
the clinician to determine at what level to intervene in their clinical work
with children.
Second, this research project highlighted that children with CF and their
families develop into psychologically well-adapted individuals despite the
adversity (i.e. managing the CF and its treatments). Indeed, literature
showed very few studies assessing the efficacy of interventions or
psychoeducation promoting well-being in children with CF (e.g. Christian &
D'Auria, 2006). Most of the available intervention-based studies aim to
improve adherence to CF treatment in children (e.g. vitamin intake, chest
therapy, antibiotics, etc.) (e.g. Downs, Roberts, Blackmorel, Le Souëf, &
Jenkins, 2006; Powers et al., 2003; Powers et al., 2005; Stark, Mackner,
Kessler, Opipari, & Quittner, 2002; Stark et al., 2003; Stark, Quittner,
Powers, & et al., 2009).
This resilience in school-aged children with CF may be explained by the
fact that the school-age period is one of relative disease latency with many
school-aged children being free from recurrent exacerbations and in-patient
treatment (Duff, 2001); which might suggest a low prevalence of
psychological disturbance in school-aged children with CF. Moreover, as
school-age children are still developing, management of CF may have a
greater impact on children’s developmental tasks rather than be at the
origins of psychological difficulties at this stage (Duff, 2001). Therefore,

DISCUSSION
- 253 -
school-age period may facilitate psychoeducation2 that targets challenges
characterized by this period in pediatric CF. First, as school-age period is
characterized by evolving social skills (e.g. development of children’s
identity and sense of competence through peer comparisons), this period
offers an opportunity for CF teams to help children develop or enhance
their social behavior repertoire leading to greater confidence in navigating
awkward social situations related to their CF (Ernst et al., 2010). Second, as
school-aged children’s cognitive skills expand, their conceptualization of
illness evolves and they develop belief and expectations related to their
disease. Thus, school-age period may be one of communication between
health professionals and children to address possible misinformation and
unfounded fears or concerns about CF (Ernst et al., 2010). Third, school-age
period is one of development of essential components of self-management
throughout the life span (e.g. sense of ownership, self-efficacy, control,
sense of involvement) (Ernst et al., 2010). However, the opportunity to
develop these skills seems to be missed frequently by CF care providers.
During CF clinic visits, children felt to be marginalized by staff with the
interaction to be only between their parent and the provider. Children with
CF also reported that their own health priorities were not addressed but
focused toward the parents’ desired outcome (Savage & Callery, 2007).
In summary, results from our research project revealed that school-
aged children with CF were well-adapted despite experiencing a chronic
disease. However, the evolving social and cognitive skills during this period
make this an optimal time to engage children in collaboration with CF
health teams and work together to develop goal-driven behaviors linked to
children’s own values in order to promote self-management across the life-
span (Ernst et al., 2010).
2 Psychoeducational interventions aim to provide patients with information
about their disease, its treatment and its consequences as well as enhance skills
to cope with disease-related problems (Bonsack, Rexhaj, & Favrod, 2015).

- 254 -

Conclusion


- 257 -
Conclusion
The purpose of this 4-year research project was to examine QOL and its
predictors (i.e. individual and parental) in school-aged children (8 to 12
years old) with CF. However, psychological adjustment to CF within this age
group is largely unknown, especially regarding QOL. Consequently, the
studies conducted within this project shed light on a missing literature in
pediatric CF.
Measurement of QOL in children still poses conceptual and
methodological issues. However, the assessment tool used in this
dissertation (i.e. QLSI-C©) has been developed in taking to account these
challenges and is applicable in clinical and non-clinical populations. The
validation of a new format (i.e. tablet version) of the QLSI-C presented in
this research project demonstrated the reliability of a technology-based
approach and its implications for practice and research.
Once the tablet-administered QLSI-C was validated, studies conducted
within this dissertation attempted to better understand psychological well-
being (i.e. QOL, anxiety, depressive symptoms) in children with CF and
investigate individual and parental factors influencing their QOL. First,
findings from this research highlighted that, overall, our multicultural
sample of school-aged children with CF develop into psychologically well-
adapted individuals. However, the different patterns of results between
Belgian and American children with CF from this research support the
findings according to which illness experience is culturally constructed (i.e.
Kleinman et al., 2006). It suggests the importance of cross-cultural studies
and the development of culturally-appropriate measures in research among
chronically ill patients. Second, based on the Common Sense Model of Self-
Regulation (CSM) (Leventhal et al., 1980), this dissertation also examined
the role of illness representation (i.e. emotional and cognitive), coping
strategies and psychological functioning (i.e. anxiety and depressive

CONCLUSION
- 258 -
symptoms) in the QOL in children with CF. Results revealed the importance
of the emotional pathway, especially the mediational role of psychological
functioning, in the QOL of our young patients. Guided by these findings, an
adaptation of the Leventhal’s CSM was suggested when applying in
pediatric populations. Finally, after considering the role of individual factors
in the QOL in children with CF, an additional study investigated the role of
parental factors. Based on the Transactional Stress and Coping model (TSC)
(Thompson & Gustafson, 1996), the role of parenting stress, parental illness
perception and parental coping strategies in the QOL of youths with CF was
examined while considering the gender effect (mothers vs fathers).
Surprisingly, parental factor did not appear to be a strong predictor of the
QOL in these patients. However, although mother- and father-related
variables did not contribute to the QOL in our pediatric CF sample (except
mother’s parenting stress), inclusion of both mothers and fathers in
pediatric research is strongly encouraged given their respective importance
in the child’s development.
In summary, findings from this 4-year research project fill a gap in the
pediatric CF literature by expanding our understanding of individual and
family risk factors associated with a poor QOL in school-aged children with
CF.



Bibliographie


- 263 -
Bibliographie
Abbott, J. (2003). Coping with cystic fibrosis. Journal of the Royal Society of Medicine, 96 (43), 42-50.
Abbott, J., & Gee, L. (2003). Quality of life in children and adolescents with cystic fibrosis: implications for optimizing treatments and clinical trial design. Paediatric Drugs, 5(1), 41-56.
Abbott, J., Webb, K., & Dodd, M. (1997). Quality of life in cystic fibrosis. Journal of the Royal Society of Medicine, 90(31), 37-42.
Abidin, R. R. (2012). Parenting Stress Index (PSI) manual (4rd ed.). Lutz, FL: Psychological Assessment Resources.
Ajzen, I., & Fishbein, M. (1980). Understanding Attitudes and Predicting Social Behavior Englewood Cliffs, NJ: Prentice-Hall.
Ajzen, I., & Madden, T. J. (1986). Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology, 22(5), 453-474. doi: http://dx.doi.org/10.1016/0022-1031(86)90045-4
Aristote. (1987). The Nichomachean Ethics. New York Oxford University Press.
Ashby, W. R. (1952). Design for a Brain. New York John Wiley.
Au, T. K., & Romo, L. (1999). Mechanical causality in children's "Folkbiology". In D. Medin & S. Atran (Eds.), Folkbiology (pp. 355-401). Cambridge: MIT Press.
Au, T. K., Sidle, A. L., & Rollins, K. B. (1993). Developing an intuitive understanding of conservation and contamination: Invisible particles as a plausible mechanism. Developmental Psychology, 29(2), 286-299. doi: 10.1037/0012-1649.29.2.286
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173-1182. doi: 10.1037/0022-3514.51.6.1173
Bauraind, O., De Gorter, F., & Saussez, M. (2002). Aspects nutritionnels. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives (pp. 109-114). Louvain-la-Neuve, Belgique: Academia-Bruylant.
Bauraind, O., & Lebecque, P. (2002). L'atteinte digestive. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives. Louvain-la-Neuve, Belgique: Academia-Bruylant.
Beattie, P. E., & Lewis-Jones, M. S. (2006). A comparative study of impairment of quality of life in children with skin disease and children with other

BIBLIOGRAPHIE
- 264 -
chronic childhood diseases. British Journal of Dermatology, 155(1), 145-151. doi: 10.1111/j.1365-2133.2006.07185.x
Bee, H., & Boyd, D. (2003). Psychologie du développement: Les âges de la vie (2e Edition). Bruxelles, Belgique: De Boeck.
Belgian Cystic Fibrosis Registry. (2014). Summary Report 2011. Brussels, Belgium: Scientific Institute of Public Health.
Bem, S. L. (1981). Gender schema theory: A cognitive account of sex typing. Psychological Review, 88(4), 354-364. doi: 10.1037/0033-295x.88.4.354
Bennett, D. S., Snooks, Q., Llera, S., Vogel, K., Conklin, D., & Varlotta, L. (2008). Monitoring and Internalizing Symptoms Among Youths With Cystic Fibrosis. Children's Health Care, 37(4), 278-292. doi: 10.1080/02739610802437426
Bertalanffy, L. (1973). Théorie générale des systèmes. Paris: Dunod.
Besier, T., Born, A., Henrich, G., Hinz, A., Quittner, A. L., Goldbeck, L., & The, T. S. G. (2011). Anxiety, depression, and life satisfaction in parents caring for children with cystic fibrosis. Pediatric Pulmonology, 46(7), 672-682. doi: 10.1002/ppul.21423
Besier, T., & Goldbeck, L. (2011). Anxiety and depression in adolescents with CF and their caregivers. Journal of Cystic Fibrosis, 10(6), 435-442. doi: http://dx.doi.org/10.1016/j.jcf.2011.06.012
Bibace, R., & Walsh, M. E. (1980). Development of Children's Concepts of Illness. Pediatrics, 66(6), 912-917.
Bideaud, J., Houdé, O., & Pedinielli, J.-L. (2002). L'homme en développement. Paris, France: Presses Universitaires de France.
Bonsack, C., Rexhaj, S., & Favrod, J. (2015). Psychoéducation : définition, historique, intérêt et limites. Annales Médico-psychologiques, revue psychiatrique, 173(1), 79-84. doi: http://dx.doi.org/10.1016/j.amp.2014.12.001
Bowling, A. (2005). Mode of questionnaire administration can have serious effects on data quality. Journal of Public Health, 27(3), 281-291. doi: 10.1093/pubmed/fdi031
Bregnballe, V., Thastum, M., & Schiotz, P. (2007). Psychosocial problems in children with cystic fibrosis. Acta Paediatr, 96, 58 - 61.
Broadbent, E., Petrie, K. J., Main, J., & Weinman, J. (2006). The Brief Illness Perception Questionnaire. Journal of Psychosomatic Research, 60(6), 631-637. doi: 10.1016/j.jpsychores.2005.10.020
Brody, A. C., & Simmons, L. A. (2007). Family Resiliency During Childhood Cancer: The Father's Perspective. Journal of Pediatric Oncology Nursing, 24(3), 152-165. doi: 10.1177/1043454206298844

BIBLIOGRAPHIE
- 265 -
Bruchon-Schweitzer, M. (2001). Le coping et les stratégies d'ajustement face au stress. Recherche en soins infirmiers, 67, 68-83.
Bruchon-Schweitzer, M. (2002). Un modèle intégratif en psychologie de la santé. In G.-N. Fischer (Ed.), Traité de psychologie de la santé (pp. 47-72). Paris: Dunod.
Bruchon-Schweitzer, M. (2014). Les processus transactionnels: stress, contrôle, soutien social et coping. In M. Bruchon-Schweitzer (Ed.), Psychologie de la santé: Concepts, méthodes et modèles. Paris: Dunod.
Bruchon-Schweitzer, M., & Boujut, E. (2014). Bonheur, Satisfaction de la vie, Bien-être, Santé et Qualité de vie. In M. Bruchon-Schweitzer & E. Boujut (Eds.), Psychologie de la santé: Concepts, méthodes et modèles (pp. 3-82). Paris, France: Dunod.
Bruchon-Schweitzer, M., & Dantzer, R. (1994). Introduction à la psychologie de la santé. Paris: PUF.
Buckley, C. K., & Schoppe-Sullivan, S. J. (2010). Father Involvement and Coparenting Behavior: Parents’ Nontraditional Beliefs and Family Earner Status as Moderators. Personal Relationships, 17(3), 413-431. doi: 10.1111/j.1475-6811.2010.01287.x
Bullinger, M., Schmidt, S., Petersen, C., & Ravens-Sieberer, U. (2006). Quality of life—evaluation criteria for children with chronic conditions in medical care. Journal of Public Health, 14(6), 343-355. doi: 10.1007/s10389-006-0066-0
Calman, K. (1984). Quality of life in cancer patients--an hypothesis. Journal of medical ethics, 10(3), 124-127.
Campbell, J. D. (1975). Illness Is a Point of View: The Development of Children's Concepts of Illness. Child Development, 46(1), 92-100.
Campbell, A., Converse, P. E., & Rodgers, W. L. (1976). The Quality of American Life: Perceptions, Evaluations and Satisfactions. New York: Russell Sage Foundation.
Carey, S. (1985). Conceptual change in childhood. Cambridge, MA: MIT Press.
Carey, S. (1995). On the origin of causal understanding. In D. Sperber, D. Premack & A. J. Premack (Eds.), Causal cognition (pp. 268-301). Oxford: Oxford University Press.
Cella, D., & Cherin, E. (1988). Quality of life during and after cancer treatment. Comprehensive therapy, 14(5), 69-75.
Centre Muco de Liège. (2009a). Maladie: diagnostic. Retrieved June 5, 2015, from http://www.muco.be/fr/mucoviscidose/diagnostic
Centre Muco de Liège. (2009b). Maladie: transmission. Retrieved June 5, 2015, from http://www.mucoliege.be/pages/5_1.html

BIBLIOGRAPHIE
- 266 -
Chaney, J. M., Mullins, L. L., Frank, R. G., Peterson, L., Mace, L. D., Kashani, J. H., & Goldstein, D. L. (1997). Transactional Patterns of Child, Mother, and Father Adjustment in Insulin-Dependent Diabetes Meelitus: A Prospective Study. Journal of Pediatric Psychology, 22(2), 229-244. doi: 10.1093/jpepsy/22.2.229
Chang, B.-H., Hendricks, A. M., Slawsky, M. T., & Locastro, J. S. (2004). Patient recruitment to a randomized clinical trial of behavioral therapy for chronic heart failure. BMC Medical Research Methodology, 4, 8-8. doi: 10.1186/1471-2288-4-8
Chateaux, V., & Spitz, E. (2005). Perceptions de l'asthme par les enfants et leurs parents: impact sur la qualite de vie et l'adhérence d'enfants asthmatiques. Unpublished doctoral dissertation, Université Paul Verlaine, Metz, France.
Cheng, S.-T., & Chan, A. C. M. (2003). Factorial Structure of the Kidcope in Hong Kong Adolescents. The Journal of Genetic Psychology, 164(3), 261-266. doi: 10.1080/00221320309597982
Christian, B. J., & D'Auria, J. P. (2006). Building Life Skills for Children With Cystic Fibrosis: Effectiveness of an Intervention. Nursing Research, 55(5), 300-307.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6(4), 284-290. doi: 10.1037/1040-3590.6.4.284
Colletti, C. J. M., Wolfe-Christensen, C., Carpentier, M. Y., Page, M. C., McNall-Knapp, R. Y., Meyer, W. H., . . . Mullins, L. L. (2008). The relationship of parental overprotection, perceived vulnerability, and parenting stress to behavioral, emotional, and social adjustment in children with cancer. Pediatric Blood & Cancer, 51(2), 269-274. doi: 10.1002/pbc.21577
Collier, J., MacKinlay, D., & Phillips, D. (2000). Norm values for the Generic Children's Quality of Life Measure (GCQ) from a large school-based sample. Quality of Life Research, 9(6), 617-623. doi: 10.1023/a:1008915700210
Connolly, M. A., & Johnson, J. A. (1999). Measuring Quality of Life in Paediatric Patients. [Article]. PharmacoEconomics, 16(6), 605-625.
Costanzo, E. S., Lutgendorf, S. K., & Roeder, S. L. (2011). Common-Sense Beliefs about Cancer and Health Practices Among Women Completing Treatment for Breast Cancer. Psycho-oncology, 20(1), 53-61. doi: 10.1002/pon.1707
Cystic Fibrosis Foundation. (2013). Patient Registry: 2012 Annual Data Report. Bethesda, Maryland.

BIBLIOGRAPHIE
- 267 -
Czyzewski, D. I., Mariotto, M. J., Bartholomew, L. K., LeCompte, S. H., & Sockrider, M. M. (1994). Measurement of quality of well being in a child and adolescent cystic fibrosis population. Medical Care, 32, 965-972.
D'Auria, J. P., Christian, B. J., & Richardson, L. F. (1997). Through the looking glass: children's perceptions of growing up with cystic fibrosis. Can J Nurs Res, 29(4), 99-112.
Dahan, K., & Verellen, C. (2002). Génétique : implications concrètes. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives (pp. 175-178). Louvain-la-Neuve, Belgique: Academia-Bruylant.
Davis, E., Waters, E., Mackinnon, A., Reddihough, D., Graham, H. K., Mehmet-Radji, O., & Boyd, R. (2006). Paediatric quality of life instruments: a review of the impact of the conceptual framework on outcomes. Developmental Medicine & Child Neurology, 48(4), 311-318. doi: 10.1017/s0012162206000673
DeMaso, D. R., Lauretti, A., Spieth, L., Van Der Feen, J. R., Jay, K. S., Gauvreau, K., . . . Berul, C. I. (2004). Psychosocial factors and quality of life in children and adolescents with implantable cardioverter-defibrillators. The American Journal of Cardiology, 93(5), 582-587. doi: http://dx.doi.org/10.1016/j.amjcard.2003.11.022
Devreker, F., Englert, Y., & Steinfeld, S. (2002). L'atteinte d'autres organes. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives (pp. 47-51). Louvain-la-Neuve, Belgique: Academia-Bruylant.
Dewey, D., & Crawford, S. (2007). Correlates of Maternal and Paternal Adjustment to Chronic Childhood Disease. Journal of Clinical Psychology in Medical Settings, 14(3), 219-226. doi: 10.1007/s10880-007-9069-4
Doucet, A. (2001). “You See the Need Perhaps More Clearly Than I Have”. Journal of Family Issues, 22(3), 328-357. doi: 10.1177/019251301022003004
Downs, J. A., Roberts, C. M., Blackmorel, A. M., Le Souëf, P. N., & Jenkins, S. C. (2006). Benefits of an education programme on the self-management of aerosol and airway clearance treatments for children with cystic fibrosis. Chronic Respiratory Disease, 3(1), 19-27. doi: 10.1191/1479972306cd100oa
Driscoll, K. A., Montag-Leifling, K., Acton, J. D., & Modi, A. C. (2009). Relations between depressive and anxious symptoms and quality of life in caregivers of children with cystic fibrosis. Pediatric Pulmonology, 44(8), 784-792. doi: 10.1002/ppul.21057
Driscoll, K. A., Schatschneider, C., McGinnity, K., & Modi, A. C. (2012). Application of Dyadic Data Analysis in Pediatric Psychology: Cystic Fibrosis Health-Related Quality of Life and Anxiety in Child–Caregiver

BIBLIOGRAPHIE
- 268 -
Dyads. Journal of Pediatric Psychology, 37(6), 605-611. doi: 10.1093/jpepsy/jss063
Drotar, D. (2004). Validating measures of pediatric health status, functional status, and health-related quality of life: key methodological challenges and strategies. Ambulatory Pediatrics, 4(4), 358-364.
Duff, A. J. A. (2001). Psychological interventions in cystic fibrosis and asthma. Paediatric Respiratory Reviews, 2(4), 350-357. doi: 10.1053/prrv.2001.0171
Duff, A. J. A., Abbott, J., Cowperthwaite, C., Sumner, C., Hurley, M. A., & Quittner, A. (2014). Depression and anxiety in adolescents and adults with cystic fibrosis in the UK: A cross-sectional study. Journal of Cystic Fibrosis, 13(6), 745-753. doi: http://dx.doi.org/10.1016/j.jcf.2014.02.010
Dulac, G. (2000). « La fragilité de la paternité dans la société québécoise: les paradoxes du père nécessaire et du père abject ». Défi jeunesse, 6(3), 17-23.
Dupuis, G., Marois, D., & Etienne, A.-M. (2012). La mesure de la qualité de vie : le modèle des systèmes de contrôle, une approche théorique pratique pour parler du bonheur. Revue Francophone de Clinique Comportementale et Cognitive, 17(1), 4-14.
Dupuis, G., Perrault, M. C., Lambany, E., Kennedy, E., & David, P. (1989). A new tool to assess quality of life : the Quality of Life Systemic Inventory. Quality of Life and Cardiovasular Care, 5(1), 36-45.
Dupuis, G., Taillefer, M.-C., Etienne, A.-M., Fontaine, O., Bovin, S., & Von Turk, A. (2000). Measurement of quality of life in cardiac rehabilitation. In J. Jobin, F. Maltais, P. LeBlanc, C. Simard & H. Kinetics (Eds.), Advances in cardiopulmonary rehabilitation (pp. 247-273). Champain, IL: Human Kinetics.
Dunn, J. (2000). Mind-reading, emotion understanding, and relationships. International Journal of Behavioral Development, 24(2), 142-144.
Dunn, J., Brown, J., Slomkowski, C., Tesla, C., & Youngblade, L. (1991). Young Children's Understanding of Other People's Feelings and Beliefs: Individual Differences and Their Antecedents. Child Development, 62(6), 1352-1366. doi: 10.2307/1130811
Edgar, K. A., & Skinner, T. C. (2003). Illness Representations and Coping as Predictors of Emotional Well-being in Adolescents with Type 1 Diabetes. Journal of Pediatric Psychology, 28(7), 485-493. doi: 10.1093/jpepsy/jsg039
Eiser, C. (1989). Children's concepts of illness: Towards an alternative to the “Stage” approach. Psychology & Health, 3(2), 93-101. doi: 10.1080/08870448908400369

BIBLIOGRAPHIE
- 269 -
Eiser, C. (1993). Growing up with a chronic disease: The impact on children and their families. London: Jessica Kingsley Publishers.
Eiser, C., Cotter, I., Oades, P., Seamark, D., & Smith, R. (1999). Health-related quality-of-life measures for children. International Journal of Cancer, 83(S12), 87-90. doi: 10.1002/(sici)1097-0215(1999)83:12+<87::aid-ijc16>3.0.co;2-o
Eiser, C., & Jenney, M. (2007). Measuring quality of life. Archives of Disease in Childhood, 92, 348–350.
Eiser, C., Mohay, H., & Morse, R. (2000). The measurement of quality of life in young children. Child: Care, Health and Development, 26(5), 401-414.
Eiser, C., & Morse, R. (2001a). Can parents rate their child's health-related quality of life? Results of a systematic review. Quality of Life Research, 10(4), 347-357. doi: 10.1023/a:1012253723272
Eiser, C., & Morse, R. (2001b). Quality-of-life measures in chronic diseases of childhood. Health Technology Assessment, 5(4), 156. doi: 10.3310/hta5040
Eiser, C., & Morse, R. (2001c). A review of measures of quality of life for children with chronic illness. Archives of Disease in Childhood, 84(3), 205-211. doi: 10.1136/adc.84.3.205
Endicott, J., Nee, J., Yang, R., & Wohlberg, C. (2006). Pediatric Quality of Life Enjoyment and Satisfaction Questionnaire (PQ-LES-Q): Reliability and Validity. Journal of the American Academy of Child & Adolescent Psychiatry, 45(4), 401-407. doi: http://dx.doi.org/10.1097/01.chi.0000198590.38325.81
Ernst, M. M., Johnson, M. C., & Stark, L. J. (2010). Developmental and Psychosocial Issues in Cystic Fibrosis. Child and Adolescent Psychiatric Clinics of North America, 19(2), 263-283. doi: 10.1016/j.chc.2010.01.004
Etienne, A. M., Dupuis, G., Spitz, E., Lemetayer, F., & Missotten, P. (2011). The Gap Concept as a Quality of Life Measure: Validation Study of the Child Quality of Life Systemic Inventory. Social Indicators Research, 100(2), 241-257.
Lemétayer, F., Lanfranchi, J.B., Chastagner, P. (2015) . The goal concept as a measure to differentiate children survivors of cancer from unsorted children. International Journal of Child, Youth and Family Studies, 6(4.1), 709-729.
Farrell, P. M. (2008). The prevalence of cystic fibrosis in the European Union. Journal of Cystic Fibrosis, 7(5), 450-453. doi: http://dx.doi.org/10.1016/j.jcf.2008.03.007
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41, 1149-1160.

BIBLIOGRAPHIE
- 270 -
Flouri, E., & Buchanan, A. (2003). The role of father involvement in children's later mental health. Journal of Adolescence, 26(1), 63-78. doi: http://dx.doi.org/10.1016/S0140-1971(02)00116-1
Flouri, E., & Buchanan, A. (2004). Early father's and mother's involvement and child's later educational outcomes. British Journal of Educational Psychology, 74(2), 141-153. doi: 10.1348/000709904773839806
Fonseca, M., & Spitz, E. (2011). Qualité de vie chez les enfants atteints de cancer: impact des perceptions de la maladie des enfants et des parents sur la qualité de vie. Unpublished doctoral dissertation, Université Paul Verlaine, Metz, France.
Frank, N. C., Blount, R. L., & Brown, R. T. (1997). Attributions, Coping and, Adjustment in Children with Cancer. Journal of Pediatric Psychology, 22(4), 563-576. doi: 10.1093/jpepsy/22.4.563
Frank, N. C., Brown, R. T., Blount, R. L., & Bunke, V. (2001). Predictors of affective responses of mothers and fathers of children with cancer. Psycho-oncology, 10(4), 293-304. doi: 10.1002/pon.526
Fulton, J. A., Yann, I., Weiner, D. J., & orenstein, D. (2012). Nutrition. In D. Orenstein, J. E. Spahr & D. J. Weiner (Eds.), Cystic Fibrosis: A Guide for Patient and Family. Philadelphia, PA: Wolters Kluwer: Lippincott Williams & Wilkins.
Garcia, R., Benet, M., Arnau, C., & Cobo, E. (2004). Efficiency of the cross-over design: an empirical estimation. Statistics in Medicine, 23(24), 3773-3780. doi: 10.1002/sim.2072
Gelman, R. (1990). First Principles Organize Attention to and Learning About Relevant Data: Number and the Animate-Inanimate Distinction as Examples. Cognitive Science, 14(1), 79-106. doi: 10.1207/s15516709cog1401_5
Gelman, R., & Baillargeon, R. (1983). A review of some Piagetian concepts. In J. H. Flavell & E. M. Markman (Eds.), Handbook of Child Psychology (pp. 167-230). New York: John Wiley.
Gerin, P., Dazord, A., Cialdella, P., Leizorovicz, A., & Boissel, J. (1991). Le questionnaire Profil de la qualité de la vie subjective (PQVS): premiers éléments de validation. Thérapie, 46(2), 131-138.
Henderson, E. M., Law, E. F., Palermo, T. M., & Eccleston, C. (2012). Case Study: Ethical Guidance for Pediatric e-health Research Using Examples From Pain Research With Adolescents. Journal of Pediatric Psychology, 37(10), 1116-1126. doi: 10.1093/jpepsy/jss085
Goldbeck, L. (2001). Parental coping with the diagnosis of childhood cancer: gender effects, dissimilarity within couples, and quality of life. [Article]. Psycho-Oncology, 10(4), 325-335. doi: 10.1002/pon.530

BIBLIOGRAPHIE
- 271 -
Gong, G. W. K., Young, N. L., Dempster, H., Porepa, M., & Feldman, B. M. (2007). The Quality of My Life questionnaire: the minimal clinically important difference for pediatric rheumatology patients. The Journal of Rheumatology, 34(3), 581-587.
Graham, P., Stevenson, J., & Flynn, D. (1997). A new measure of health-related quality of life for children: Preliminary findings. Psychology & Health, 12(5), 655-665. doi: 10.1080/08870449708407412
Gray, D. E. (2003). Gender and coping: the parents of children with high functioning autism. Social Science & Medicine, 56(3), 631-642. doi: 10.1016/s0277-9536(02)00059-x
Griva, K., Myers, L. B., & Newman, S. (2000). Illness perceptions and self efficacy beliefs in adolescents and young adults with insulin dependent diabetes mellitus. Psychology & Health, 15(6), 733-750. doi: 10.1080/08870440008405578
Groeneveld, I., Sosa, E., Pérez, M., Fiuza-Luces, C., Gonzalez-Saiz, L., Gallardo, C., . . . Lucia, A. (2012). Health-related quality of life of Spanish children with cystic fibrosis. Quality of Life Research, 21(10), 1837-1845. doi: 10.1007/s11136-011-0100-8
Grootenhuis, M. A., Koopman, H. M., Verrips, E. G. H., Vogels, A. G. C., & Last, B. F. (2007). Health-related quality of life problems of children aged 8–11 years with a chronic disease. Developmental Neurorehabilitation, 10(1), 27-33. doi: 10.1080/13682820600691017
Guyatt, G. H., & Jaeschke, R. (1990). Measurements in clinical trials: choosing the appropriate approach. In B. Spilker (Ed.), Quality of life assessments in clinical trials (pp. 37-46). New York: Raven Press.
Guyatt, G. H., Juniper, E. F., Griffith, L. E., Feeny, D. H., & Ferrie, P. J. (1997). Children and Adult Perceptions of Childhood Asthma. Pediatrics, 99(2), 165-168. doi: 10.1542/peds.99.2.165
Hagger, M. S., & Orbell, S. (2003). A Meta-Analytic Review of the Common-Sense Model of Illness Representations. Psychology & Health, 18(2), 141-184. doi: 10.1080/088704403100081321
Hauari, H., & Hollingworth, K. (2009). Understanding fathering: Masculinity, diversity and change. New York: Joseph Rowntree Foundation.
Havermans, T., Colpaert, K., & Dupont, L. J. (2008). Quality of life in patients with Cystic Fibrosis: Association with anxiety and depression. Journal of Cystic Fibrosis, 7(6), 581-584. doi: http://dx.doi.org/10.1016/j.jcf.2008.05.010
Havermans, T., Vreys, M., Proesmans, M., & De Boeck, C. (2006). Assessment of agreement between parents and children on health-related quality of life in children with cystic fibrosis. Child: Care, Health and Development, 32(1), 1-7. doi: 10.1111/j.1365-2214.2006.00564.x

BIBLIOGRAPHIE
- 272 -
Hayes, A. F. (2013). Introduction to mediation, moderation and conditional process analysis. New York: Guilford Press.
Hayes, C. C., & Savage, E. (2008). Fathers’ Perspectives on the Emotional Impact of Managing the Care of Their Children With Cystic Fibrosis. Journal of Pediatric Nursing, 23(4), 250-256. doi: 10.1016/j.pedn.2007.09.002
Hegarty, M., MacDonald, J., Watter, P., & Wilson, C. (2009). Quality of life in young people with cystic fibrosis: effects of hospitalization, age and gender, and differences in parent/child perceptions. Child: Care, Health and Development, 35(4), 462-468. doi: 10.1111/j.1365-2214.2008.00900.x
Herzer, M., Godiwala, N., Hommel, K. A., Driscoll, K., Mitchell, M., Crosby, L. E., . . . Modi, A. C. (2010). Family Functioning in the Context of Pediatric Chronic Conditions. Journal of Developmental and Behavioral Pediatrics, 31(1), 26-34.
Hocking, M. C., & Lochman, J. E. (2005). Applying the Transactional Stress and Coping Model to Sickle Cell Disorder and Insulin-Dependent Diabetes Mellitus: Identifying Psychosocial Variables Related to Adjustment and Intervention. Clinical Child and Family Psychology Review, 8(3), 221-246. doi: 10.1007/s10567-005-6667-2
Hodgkinson, R., & Lester, H. (2002). Stresses and coping strategies of mothers living with a child with cystic fibrosis: implications for nursing professionals. Journal of Advanced Nursing, 39(4), 377-383. doi: 10.1046/j.1365-2648.2002.02299.x
Hofferth, S. L., Pleck, J., Stueve, J. L., Bianchi, S., & Sayer, L. (2002). The demography of fathers: What fathers do. In C. S. Tamis-LeMonda & N. Cabrera (Eds.), Handbook of father involvement (pp. 63-90). Mahwah, NJ: Erlbaum.
Horne, R., & Weinman, J. (2002). Self-regulation and Self-management in Asthma: Exploring The Role of Illness Perceptions and Treatment Beliefs in Explaining Non-adherence to Preventer Medication. Psychology & Health, 17(1), 17-32. doi: 10.1080/08870440290001502
Housiaux, M., & Lahaye, M. (2008). Les compétences émotionelles chez l'enfant. In O. Luminet (Ed.), Psychologie des émotions Bruxelles, Belgique: De Boek.
Hughes, C., & Dunn, J. (1998). Understanding mind and emotion: longitudinal associations with mental-state talk between young friends. Developmental Psychology, 34(5), 1026.
Hullmann, S., Wolfe-Christensen, C., Meyer, W., McNall-Knapp, R., & Mullins, L. (2010). The relationship between parental overprotection and health-related quality of life in pediatric cancer: the mediating role of perceived child vulnerability. Quality of Life Research, 19(9), 1373-1380. doi: 10.1007/s11136-010-9696-3

BIBLIOGRAPHIE
- 273 -
IBM Corp. (2011). IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.
Ievers, C., & Drotar, D. (1996). Family and parental functioning in cystic fibrosis. J Dev Behav Pediatr, 17, 48 - 55.
Inagaki, K. (1995). Young children's spontaneous vitalistic explanation for bodily phenomena. Paper presented at the fifty-ninth meeting of the Japanese Psychology Association, Okinawa, Japanese.
Inagaki, K. (1997). Emerging distinction between naive biology and naive psychology. In H. M. Wellman & K. Inagaki (Eds.), The emergence of core domains of thought: Children's reasoning about physical, psychological, and biological phenomena (pp. 27-44). San Fransisco: Jossey-Bass.
Inagaki, K., & Hatano, G. (1987). Young Children's Spontaneous Personification as Analogy. Child Development, 58(4), 1013-1020. doi: 10.2307/1130542
Inagaki, K., & Hatano, G. (1993). Young Children's Understanding of the Mind-Body Distinction. Child Development, 64(5), 1534-1549. doi: 10.1111/j.1467-8624.1993.tb02969.x
Inagaki, K., & Hatano, G. (2002). Young children's naive thinking about the biological world. New York: Psychology Press.
Inagaki, K., & Hatano, G. (2005). Children's understanding of mind-body relationship. In M. Siegal & C. C. Peterson (Eds.), Children's Understanding of Biology and Health. New York: Cambridge University Press.
Inagaki, K., & Hatano, G. (2006). Young Children's Conception of the Biological World. Current Directions in Psychological Science, 15(4), 177-181. doi: 10.1111/j.1467-8721.2006.00431.x
Iwamoto, V., Santos, S. H., Skare, T. L., & Spelling, P. F. (2008). Evaluation of psychological stress in primary caregivers of patients with juvenile idiopathic arthritis. J Pediatr (Rio J), 84(1), 91-94. doi: doi:10.2223/JPED.1738
Jeanbaptiste, A.-C., & Matossian, A. (2002). La maladie et la vie quotidienne, au fil du temps. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives. Louvain-la-Neuve, Belgique: Academia-Bruylant.
Kalish, C. (1996). Causes and Symptoms in Preschoolers' Conceptions of Illness. Child Development, 67(4), 1647-1670. doi: 10.1111/j.1467-8624.1996.tb01819.x
Kalish, C. (1997). Preschoolers' understanding of mental and bodily reactions to contamination: What you don't know can hurt you, but cannot sadden you. Developmental Psychology, 33(1), 79-91. doi: 10.1037/0012-1649.33.1.79

BIBLIOGRAPHIE
- 274 -
Kalish, C. (2005). What young children's understanding of contamination and contagion tells us about their concepts of illness. In M. Siegal & C. C. Peterson (Eds.), Children's Understanding of Biology and Health. New York: Cambridge University Press.
Kazak, A. E., & Barakat, L. P. (1997). Brief Report: Parenting Stress and Quality of Life During Treatment for Childhood Leukemia Predicts Child and Parent Adjustment After Treatment Ends. Journal of Pediatric Psychology, 22(5), 749-758. doi: 10.1093/jpepsy/22.5.749
Kianifar, H.-R., Bakhshoodeh, B., Hebrani, P., & Behdani, F. (2013). Qulaity of Life in Cystic Fibrosis Children. Iranian Journal of Pediatrics, 23(2), 149-153.
Kim, D. H. (Unpublished doctoral dissertation). Development of an instrument to measure resilience of children with chronic illness. Yonsei University. Seoul, Korea.
Kim, S., & Feldt, L. S. (2008). A Comparison of Tests for Equality of Two or More Independent Alpha Coefficients. Journal of Educational Measurement, 45(2), 179-193. doi: 10.1111/j.1745-3984.2008.00059.x
Kim, D. H., & Yoo, I. Y. (2010). Factors associated with resilience of school age children with cancer. Journal of Paediatrics and Child Health, 46(7-8), 431-436. doi: 10.1111/j.1440-1754.2010.01749.x
Kister, M. C., & Patterson, C. J. (1980). Children's Conceptions of the Causes of Illness: Understanding of Contagion and Use of Immanent Justice. Child Development, 51(3), 839-846. doi: 10.2307/1129472
Knowles, S. R., Wilson, J. L., Connell, W. R., & Kamm, M. A. (2011). Preliminary examination of the relations between disease activity, illness perceptions, coping strategies, and psychological morbidity in Crohn's disease guided by the common sense model of illness. Inflammatory Bowel Diseases, 17(12), 2551-2557. doi: 10.1002/ibd.21650
Koopman, H. M., Baars, R. M., Chaplin, J., & Zwinderman, K. H. (2004). Illness through the eyes of the child: the development of children's understanding of the causes of illness. Patient Education and Counseling, 55(3), 363-370. doi: http://dx.doi.org/10.1016/j.pec.2004.02.020
Kovacs, M. (2010). Children's Depression Inventory 2nd Edition. North Tonawanda, NY: Multi-Health Systems.
Kovacs, M., & Beck, A. T. (1977). An empirical clinical approach toward a definition of childhood depression In J. G. Schultirbrand & A. Rasken (Eds.), Depression in childhood (pp. 1-27). New York: Raven Press.
Lamb, M. E. (2010). The role of the father in child development. Fifth Edition. Hoboken, New Jersey: john Wiley & Sons, Inc.
Landgraf, J. M., & Abetz, L. N. (1996). Measuring health oucomes in pediatric populations: issues in psychometrics and applications. In B. Spilker (Ed.),

BIBLIOGRAPHIE
- 275 -
Quality of life and pharmacoeconomics in clinical trials (pp. 793-802). Philadelphia, PA: Lippincott-Raven Publishers.
Lawford, J., Volavka, N., & Eiser, C. (2001). A generic measure of Quality of Life for children aged 3-8 years: results of two preliminary studies. Developmental Neurorehabilitation, 4(4), 197-207. doi: 10.1080/13638490210124033
Lawler, R. H., Nakielny, W., & Wright, N. A. (1966). Psychological Implications of Cystic Fibrosis. Canadian Medical Association Journal, 94(20), 1043-1046.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York, NY, USA: Springer Publishing Company.
Le Camus, J. (1995). Pères et bébés. Paris: L'Harmattan.
Le Coq, E. M., Colland, V. T., Boeke, A. J. P., Bezemer, D. P., & van Eijk, J. T. M. (2000). Reproducibility, Construct Validity, and Responsiveness of the “How Are You?” (HAY), a Self-Report Quality of Life Questionnaire for Children with Asthma. Journal of Asthma, 37(1), 43-58. doi: 10.3109/02770900009055427
Leal, T., & Lebecque, P. (2002). Le diagnostic. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives (pp. 15-20). Louvain-la-Neuve, Belgique: Academia-Bruylant.
Lebecque, P. (2002). Pronostic. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives (pp. 53-57). Louvain-la-Neuve, Belgique: Academia-Bruylant.
Lebecque, P., & Baran, D. (2002a). Antibiothérapie. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives (pp. 101-108). Louvain-la-Neuve, Belgique: Academia-Bruylant.
Lebecque, P., & Baran, D. (2002b). L'atteinte respiratoire. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives. Louvain-la-Neuve, Belgique: Academia-Bruylant.
Lebecque, P., & Baran, D. (2002). La mucoviscidose : La maladie, le traitement, les perspectives. Louvain-la-Neuve, Belgique: Academia-Bruylant.
Leidy, N. K., Revicki, D. A., & Genesté, B. (1999). Recommendations for Evaluating the Validity of Quality of Life Claims for Labeling and Promotion. Value in Health, 2(2), 113-127. doi: 10.1046/j.1524-4733.1999.02210.x
Lemetayer, F. (2012). Editorial. Revue Francophone de Clinique Comportementale et Cognitive, 17(1), 2-3.
Levenstein, S., Li, Z., Almer, S., Barbosa, A., Marquis, P., Moser, G., Sperber, A., Toner, B. & Drossman, D. A. (2001). Cross-cultural variation in disease-

BIBLIOGRAPHIE
- 276 -
related concerns among patients with inflammatory bowel disease. Am J Gastroenterol, 96(6), 1822-1830.
Leventhal, H., Diefenbach, M., & Leventhal, E. (1992). Illness cognition: Using common sense to understand treatment adherence and affect cognition interactions. Cognitive Therapy and Research, 16(2), 143-163. doi: 10.1007/bf01173486
Leventhal, H., Meyer, D., & Nerenz, D. (1980). The common sense representation of illness danger. In S. Rachman (Ed.), Medical Psychology (Vol. 2, pp. 7-30). New York: Pergamon Press.
Lindblad, D. S., Weiner, D. J., & Orenstein, D. M. (2012). The Gastrointestinal Tract. In D. Orenstein, J. E. spahr & D. J. Weiner (Eds.), Cystic Fibrosis: A Guide for Patient and Family. Philadelphia, PA: Wolters Kluwer: Lippincott Williams & Wilkins.
Lindström, B., & Eriksson, B. (1993). Quality of life among children in the Nordic countries. Quality of Life Research, 2(1), 23-32. doi: 10.1007/bf00642886
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The Construct of Resilience: A Critical Evaluation and Guidelines for Future Work. Child Development, 71(3), 543-562.
Mack, C., & Morr, L. (1982). Versions françaises d'échelles d'évaluation de la dépression: Les échelles CDI et ISC de Maria Kovacs. Neuropsychiatrie de l'Enfance, 30, 627-652.
Mangunkusumo, R. T., Duisterhout, J. S., De Graaff, N., Maarsingh, E. J., De Koning, H. J., & Raat, H. (2006). Internet Versus Paper Mode of Health and Health Behavior Questionnaires in Elementary Schools: Asthma and Fruit as Examples. Journal of School Health, 76(2), 80-86. doi: 10.1111/j.1746-1561.2006.00072.x
Mangunkusumo, R. T., Moorman, P. W., Van Den Berg-de Ruiter, A. E., Van Der Lei, J., De Koning, H. J., & Raat, H. (2005). Internet-administered adolescent health questionnaires compared with a paper version in a randomized study. Journal of Adolescent Health, 36(1), 70.e71-70.e76. doi: http://dx.doi.org/10.1016/j.jadohealth.2004.02.020
Manificat, S., & Dazord, A. (1997). Evaluation de la qualité de vie de l'enfant : validation d'un questionnaire, premiers résultats. Expansion Scientifique Française, 45(3), 106-114.
Matza, L. S., Swensen, A. R., Flood, E. M., Secnik, K., & Leidy, N. K. (2004). Assessment of Health-Related Quality of Life in Children: A Review of Conceptual, Methodological, and Regulatory Issues. Value in Health, 7(1), 79-92. doi: 10.1111/j.1524-4733.2004.71273.x
McBride, B. A., Schoppe-Sullivan, S. J., & Ho, M.-H. (2005). The mediating role of fathers' school involvement on student achievement. Journal of Applied

BIBLIOGRAPHIE
- 277 -
Developmental Psychology, 26(2), 201-216. doi: http://dx.doi.org/10.1016/j.appdev.2004.12.007
McCubbin, M., Balling, K., Possin, P., Frierdich, S., & Bryne, B. (2002). Family Resiliency in Childhood Cancer*. Family Relations, 51(2), 103-111. doi: 10.1111/j.1741-3729.2002.00103.x
McCubbin, H. I., McCubbin, M. A., Patterson, J. M., Cauble, A. E., Wilson, L. R., & Warwick, W. (1983). CHIP. Coping Health Inventory for Parents: An Assessment of Parental Coping Patterns in the Care of the Chronically Ill Child. Journal of Marriage and Family, 45(2), 359-370.
Meyer, D., Leventhal, H., & Gutmann, M. (1985). Common-sense models of illness: The example of hypertension. Health Psychology, 4(2), 115-135. doi: 10.1037/0278-6133.4.2.115
Missotten, P., Etienne, A.-M., & Dupuis, G. (2007). La qualité de vie infantile: état actuel des connaissances. Revue Francophone de Clinique Comportementale et Cognitive, 12(4), 16-27.
Missotten, P., Fonseca, M., Dupuis, G., Spitz, E., & Etienne, A.-M. (2012). Une approche modulaire d’évaluation de la qualité de vie en oncologie pédiatrique : les versions française et portugaise de l’Inventaire Systémique de Qualité de Vie pour Enfants (ISQV-E©). Revue Francophone de Clinique Comportementale et Cognitive, 17(1), 15-33.
Modi, A. C., Lim, C. S., Yu, N., Geller, D., Wagner, M. H., & Quittner, A. L. (2006). A multi-method assessment of treatment adherence for children with cystic fibrosis. Journal of Cystic Fibrosis, 5(3), 177-185. doi: http://dx.doi.org/10.1016/j.jcf.2006.03.002
Modi, A. C., & Quittner, A. L. (2003). Validation of a Disease-Specific Measure of Health-Related Quality of Life for Children with Cystic Fibrosis. Journal of Pediatric Psychology, 28(8), 535-546. doi: 10.1093/jpepsy/jsg044
Moos, R. H., & Moos, B. (1981). Family Environment Scale. Palo Alto, CA: Consulting Psychologist Press.
Moreira, H., Frontini, R., Bullinger, M., & Canavarro, M. (2014). Family Cohesion and Health-Related Quality of Life of Children with Type 1 Diabetes: The Mediating Role of Parental Adjustment. Journal of Child and Family Studies, 23(2), 347-359. doi: 10.1007/s10826-013-9758-6
Moss-Morris, R., Weinman, J., Petrie, K., Horne, R., Cameron, L., & Buick, D. (2002). The Revised Illness Perception Questionnaire (IPQ-R). Psychology & Health, 17(1), 1-16. doi: 10.1080/08870440290001494
Mullins, L. L., Wolfe-Christensen, C., Hoff Pai, A. L., Carpentier, M. Y., Gillaspy, S., Cheek, J., & Page, M. (2007). The Relationship of Parental Overprotection, Perceived Child Vulnerability, and Parenting Stress to Uncertainty in Youth with Chronic Illness. Journal of Pediatric Psychology, 32(8), 973-982. doi: 10.1093/jpepsy/jsm044

BIBLIOGRAPHIE
- 278 -
Muris, P., Merckelbach, H., & Meesters, C. (2001). Learning Experiences and Anxiety Sensitivity in Normal Adolescents. Journal of Psychopathology and Behavioral Assessment, 23(4), 279-283. doi: 10.1023/a:1012783504852
Myant, K. A., & Williams, J. M. (2005). Children’s Concepts of Health and Illness: Understanding of Contagious Illnesses, Non-Contagious Illnesses and Injuries. Journal of Health Psychology, 10(6), 805-819. doi: 10.1177/1359105305057315
Notaro, P. C., Gelman, S. A., & Zimmerman, M. A. (2001). Children's Understanding of Psychogenic Bodily Reactions. Child Development, 72(2), 444-459. doi: 10.1111/1467-8624.00289
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory (3rd ed). New York: McGraw-Hill
Office de la Naissance et de l'Enfance. (2012). Rapport 2010 de la Banque de Données Médico-Sociales : Fédération Wallonie-Bruxelles. Retrieved from http://www.one.be/uploads/tx_ttproducts/datasheet/Rapport_BDMS_2012_BD.pdf
Ogden, J. (2014). Les représentations de la maladie. In J. Ogden (Ed.), Psychologie de la santé. Louvain-La-Neuve, Belgique: De Boek.
Oleson, M. (1990). Subjectively Perceived Quality of Life. Image: the Journal of Nursing Scholarship, 22(3), 187-190. doi: 10.1111/j.1547-5069.1990.tb00205.x
Orbuch, T. L., Parry, C., Chesler, M., Fritz, J., & Repetto, P. (2005). Parent-Child Relationships and Quality of Life: Resilience Among Childhood Cancer Survivors. Family Relations, 54(2), 171-183. doi: 10.2307/40005247
Orenstein, D., Spahr, J. E., & Weiner, D. J. (2012). Cystic Fibrosis: A Guide for Patient and Family. Philadelphia, PA: Wolters Kluwer: Lippincott Williams & Wilkins.
Organisation Mondiale de la Santé. (1946). La consistution de l'Organisation Mondiale de la Santé. Actes officiels de l'Organisation mondiale de la Santé, 2, 100.
Ortega, A. N., & Calderon, J. G. (2000). Pediatric asthma among minority populations. Curr Opin Pediatr, 12(6), 579-583.
Parke, R. D., McDowell, D. J., Kim, M., Killian, C., Dennis, J., Flyer, M. L., & Wild, M. N. (2002). Father’s contributions to children’s peer relationships. In C. S. Tamis-LeMonda & N. Cabrera (Eds.), Handbook of father involvement (pp. 141-166). Mahwah, NJ: Erlbaum.
Pelchat, D., Lefebvre, H., & Perreault, M. (2003). Differences and similarities between mothers’ and fathers’ experiences of parenting a child with a

BIBLIOGRAPHIE
- 279 -
disability. Journal of Child Health Care, 7(4), 231-247. doi: 10.1177/13674935030074001
Petersen, C., Schmidt, S., Power, M., & Bullinger, M. (2005). Development and pilot-testing of a health-related quality of life chronic generic module for children and adolescents with chronic health conditions: A European perspective. Quality of Life Research, 14(4), 1065-1077. doi: 10.1007/s11136-004-2575-z
Phares, V., Lopez, E., Fields, S., Kamboukos, D., & Duhig, A. M. (2005). Are Fathers Involved in Pediatric Psychology Research and Treatment? Journal of Pediatric Psychology, 30(8), 631-643. doi: 10.1093/jpepsy/jsi050
Phipps, S. (2007). Adaptive Style in Children with Cancer: Implications for a Positive Psychology Approach. Journal of Pediatric Psychology, 32(9), 1055-1066. doi: 10.1093/jpepsy/jsm060
Piaget, J., & Inhelder, B. (1969). The psychology of the child. New York Basic Books.
Pickard, A. S., & Knight, S. J. (2005). Proxy Evaluation of Health-Related Quality of Life: A Conceptual Framework for Understanding Multiple Proxy Perspectives. Medical Care, 43(5), 493-499.
Powers, W. (1973). Behavior : The Control of Perception. Chicago: Aldine.
Powers, S. W., Byars, K. C., Mitchell, M. J., Patton, S. R., Schindler, T., & Zeller, M. H. (2003). A Randomized Pilot Study of Behavioral Treatment to Increase Calorie Intake in Toddlers With Cystic Fibrosis. Children's Health Care, 32(4), 297-311. doi: 10.1207/s15326888chc3204_5
Powers, S. W., Jones, J. S., Ferguson, K. S., Piazza-Waggoner, C., Daines, C., & Acton, J. D. (2005). Randomized Clinical Trial of Behavioral and Nutrition Treatment to Improve Energy Intake and Growth in Toddlers and Preschoolers With Cystic Fibrosis. Pediatrics, 116(6), 1442-1450. doi: 10.1542/peds.2004-2823
Prochaska, J. O., & DiClemente, C. C. (1982). Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy, Theory, Research, and Practice, 19, 276-288.
Quittner, A. L., DiGirolamo, A. M., Michel, M., & Eigen, H. (1992). Parental Response to Cystic Fibrosis: A Contextual Analysis of the Diagnosis Phase. Journal of Pediatric Psychology, 17(6), 683-704. doi: 10.1093/jpepsy/17.6.683
Raat, H., Mangunkusumo, R., Landgraf, J., Kloek, G., & Brug, J. (2007). Feasibility, reliability, and validity of adolescent health status measurement by the Child Health Questionnaire Child Form (CHQ-CF): internet administration compared with the standard paper version. Quality of Life Research, 16(4), 675-685. doi: 10.1007/s11136-006-9157-1

BIBLIOGRAPHIE
- 280 -
Raat, H., Mangunkusumo, R. T., Mohangoo, A. D., Juniper, E. F., & Van Der Lei, J. (2007). Internet and written respiratory questionnaires yield equivalent results for adolescents. Pediatric Pulmonology, 42(4), 357-361. doi: 10.1002/ppul.20576
Ravens-Sieberer, U., & Bullinger, M. (1998). Assessing health-related quality of life in chronically ill children with the German KINDL: first psychometric and content analytical results. Quality of Life Research, 7(5), 399-407. doi: 10.1023/a:1008853819715
Ravens-Sieberer, U., Erhart, M., Wille, N., Wetzel, R., Nickel, J., & Bullinger, M. (2006). Generic health-related quality-of-life assessment in children and adolescents. PharmacoEconomics, 24(12), 1199-1220.
Rebok, G., Riley, A., Forrest, C., Starfield, B., Green, B., Robertson, J., & Tambor, E. (2001). Elementary school-aged children's reports of their health: A cognitive interviewing study. Quality of Life Research, 10(1), 59-70. doi: 10.1023/a:1016693417166
Reis, H., Collins, W., & Berscheid, E. (2000). The relationship context of human behavior and development. Psychol Bull, 126, 844 - 872.
Reychler, G., & Opdekamp, C. (2002). La kinésithérapie. In P. Lebecque & D. Baran (Eds.), La mucoviscidose : La maladie, le traitement, les perspectives (pp. 89-99). Louvain-la-Neuve, Belgique: Academia-Bruylant.
Riley, A. W. (2004). Evidence That School-Age Children Can Self-Report on Their Health. Ambulatory Pediatrics, 4(4), 371-376. doi: http://dx.doi.org/10.1367/A03-178R.1
Ritterband, L. M., & Palermo, T. M. (2009). Introduction to the Special Issue: eHealth in Pediatric Psychology. Journal of Pediatric Psychology, 34(5), 453-456. doi: 10.1093/jpepsy/jsp008
Rosen, A. B., & Rozin, P. (1993). Now you see it, now you don't: The preschool child's conception of invisible particles in the context of dissolving. Developmental Psychology, 29(2), 300-311. doi: 10.1037/0012-1649.29.2.300
Rosenstein, B. J., & Cutting, G. R. (1998). The diagnosis of cystic fibrosis: A consensus statement. The Journal of Pediatrics, 132(4), 589-595. doi: 10.1016/s0022-3476(98)70344-0
Rosenstock, I. M., Strecher, V. J., & Becker, M. H. (1988). Social Learning Theory and the Health Belief Model. Health Education & Behavior, 15(2), 175-183. doi: 10.1177/109019818801500203
Royce, F. H., & Carl, J. C. (2011). Health-related quality of life in cystic fibrosis. Current Opinion in Pediatrics, 23(5), 535-540. doi: 10.1097/MOP.0b013e32834a7829

BIBLIOGRAPHIE
- 281 -
Rushforth, H. (1999). Practitioner Review: Communicating with Hospitalised Children: Review and Application of Research Pertaining to Children's Understanding of Health and Illness. Journal of Child Psychology and Psychiatry, 40(5), 683-691. doi: 10.1111/1469-7610.00485
Russell, A., & Saebel, J. (1997). Mother–Son, Mother–Daughter, Father–Son, and Father–Daughter: Are They Distinct Relationships? Developmental Review, 17(2), 111-147. doi: http://dx.doi.org/10.1006/drev.1996.0431
Sales, J., Fivush, R., & Teague, G. W. (2008). The Role of Parental Coping in Children with Asthma's Psychological Well-being and Asthma-related Quality of Life. Journal of Pediatric Psychology, 33(2), 208-219. doi: 10.1093/jpepsy/jsm068
Savage, E., & Callery, P. (2007). Clinic consultations with children and parents on the dietary management of cystic fibrosis. Social Science & Medicine, 64(2), 363-374. doi: http://dx.doi.org/10.1016/j.socscimed.2006.09.003
Scharloo, M., Kaptein, A. A., Weinman, J., Hazes, J. M., Willems, L. N. A., Bergman, W., & Rooijmans, H. G. M. (1998). Illness perceptions, coping and functioning in patients with rheumatoid arthritis, chronic obstructive pulmonary disease and psoriasis. Journal of Psychosomatic Research, 44(5), 573-585. doi: 10.1016/s0022-3999(97)00254-7
Shaw, S., Huebner, C., Armin, J., Orzech, K., & Vivian, J. (2009). The Role of Culture in Health Literacy and Chronic Disease Screening and Management. Journal of Immigrant and Minority Health, 11(6), 460-467. doi: 10.1007/s10903-008-9135-5
Siegal, M. (1988). Children's Knowledge of Contagion and Contamination as Causes of Illness. Child Development, 59(5), 1353-1359. doi: 10.2307/1130497
Siegal, M., & Peterson, C. C. (2005). Children's Understanding of Biology and Health. New York: Cambridge University Press.
Solans, M., Pane, S., Estrada, M.-D., Serra-Sutton, V., Berra, S., Herdman, M., . . . Rajmil, L. (2008). Health-Related Quality of Life Measurement in Children and Adolescents: A Systematic Review of Generic and Disease-Specific Instruments. Value in Health, 11(4), 742-764. doi: 10.1111/j.1524-4733.2007.00293.x
Solomon, G. E. A., & Cassimatis, N. L. (1999). On facts and conceptual systems: Young children's integration of their understandings of germs and contagion. Developmental Psychology, 35(1), 113-126. doi: 10.1037/0012-1649.35.1.113
Spahr, J. E., Orenstein, D., & Weiner, D. J. (2012a). Daily Life. In D. Orenstein, J. E. Spahr & D. J. Weiner (Eds.), Cystic Fibrosis: A Guide for Patient and Family (pp. 195-203). Philadelphia, PA: Wolters Kluwer: Lippincott Williams & Wilkins.

BIBLIOGRAPHIE
- 282 -
Spahr, J. E., Orenstein, D. M., & Weiner, D. J. (2012b). Making the diagnosis. In D. M. Orenstein, J. E. Spahr & D. J. Weiner (Eds.), Cystic Fibrosis: A guide for patients and family. Philadelphia, PA Wolters Kluwer: Lippincott Williams & Wilkins.
Spence, J. T., & Helmreich, R. L. (1980). Masculine Instrumentality and Feminine Expressiveness: Their Relationships with Sex Role Attitudes and Behaviors. Psychology of Women Quarterly, 5(2), 147-163. doi: 10.1111/j.1471-6402.1980.tb00951.x
Spielberger, C. D., Edwards, C. D., Lushene, R. E., Montuori, J., & Platzek, D. (1973). State-trait anxiety inventory for children ("How I feel questionnaire"): Professional manual. Redwood, CA: Mind Garden.
Spieth, L. E., & Harris, C. V. (1996). Assessment of Health-Related Quality of Life in Children and Adolescents: An Integrative Review. Journal of Pediatric Psychology, 21(2), 175-193. doi: 10.1093/jpepsy/21.2.175
Spirito, A., Stark, L. J., & Williams, C. (1988). Development of a Brief Coping Checklist for Use with Pediatric Populations. Journal of Pediatric Psychology, 13(4), 555-574.
Spitz, E. (2002). Les stratégies d'adaptation face à la maladie chronique. In G.-N. Fischer (Ed.), Traité de psychologie de la santé. Paris: Dunod.
Springer, K., & Ruckel, J. (1992). Early beliefs about the cause of illness: Evidence against immanent justice. Cognitive Development, 7(4), 429-443. doi: http://dx.doi.org/10.1016/0885-2014(92)80002-W
Stanton, A. L., Collins, C. A., & Sworowski, L. A. (2001). Adjustment to chronic illness: theory and research. In A. Baum, T. A. Revenson & J. E. Singer (Eds.), Handbook of Health Psychology (pp. 387–403). Mahwah, NJ: Erlbaum.
Stanton, A. L., Revenson, T. A., & Tennen, H. (2007). Health Psychology: Psychological Adjustment to Chronic Disease. Annual Review of Psychology, 58(1), 565-592. doi: doi:10.1146/annurev.psych.58.110405.085615
Stark, L. J., Mackner, L. M., Kessler, J. H., Opipari, L. C., & Quittner, A. L. (2002). Preliminary Findings For Calcium Intake in Children With Cystic Fibrosis Following Behavioral Intervention for Caloric Intake. Children's Health Care, 31(2), 107-118. doi: 10.1207/s15326888chc3102_2
Stark, L. J., Opipari, L. C., Spieth, L. E., Jelalian, E., Quittner, A. L., Higgins, L., . . . Duggan, C. (2003). Contribution of behavior therapy to dietary treatment in cystic fibrosis: A randomized controlled study with 2-year follow-up. Behavior Therapy, 34(2), 237-258. doi: http://dx.doi.org/10.1016/S0005-7894(03)80015-1
Stark, L. J., Quittner, A. L., Powers, S. W., & et al. (2009). RAndomized clinical trial of behavioral intervention and nutrition education to improve

BIBLIOGRAPHIE
- 283 -
caloric intake and weight in children with cystic fibrosis. Archives of Pediatrics & Adolescent Medicine, 163(10), 915-921. doi: 10.1001/archpediatrics.2009.165
Szyndler, J. E., Towns, S. J., van Asperen, P. P., & McKay, K. O. (2005). Psychological and family functioning and quality of life in adolescents with cystic fibrosis. Journal of Cystic Fibrosis, 4(2), 135-144. doi: 10.1016/j.jcf.2005.02.004
Teicher, J. D. (1969). Psychological Aspects of Cystic Fibrosis in Children and Adolescents. California Medicine, 110(5), 371-374.
The KIDSCREEN Group Europe. (2006). The KIDSCREEN Questionnaires - Quality of life questionnaires for children and adolescents. Lengerich, Germany: Pabst Science Publishers.
Thomas, C., Mitchell, P., O’Rourke, P., & Wainwright, C. (2006). Quality-of-life in children and adolescents with cystic fibrosis managed in both regional outreach and cystic fibrosis center settings in queensland. The Journal of Pediatrics, 148(4), 508-516.e501. doi: 10.1016/j.jpeds.2005.11.040
Thompson, R. J., Gil, K. M., Burbach, D. J., Keith, B. R., & Kinney, T. R. (1993). Role of child and maternal processes in the psychological adjustment of children with sickle cell disease. Journal of Consulting and Clinical Psychology, 61(3), 468-474. doi: 10.1037/0022-006x.61.3.468
Thompson, R. J., & Gustafson, K. E. (1996). Adaptation to chronic childhood illness. Washington, DC: American Psychological Association.
Thompson, R. J., Gustafson, K. E., George, L. K., & Spock, A. (1994). Change Over a 12-Month Period in the Psychological Adjustment of Children and Adolescents with Cystic Fibrosis. Journal of Pediatric Psychology, 19(2), 189-203. doi: 10.1093/jpepsy/19.2.189
Thompson, R. J., Gustafson, K. E., & Gil, K. M. (1995). Psychological adjustment of adolescents with cystic fibrtosis or sickle cell disease and their mothers. In J. L. Wallander & L. Siegel (Eds.), Advances in Pediatric Psychology II: Behavioral Perspectives on Adolescent health (pp. 232-247). New York, NY, USA: Guilford Press.
Thompson, R. J., Gustafson, K. E., Hamlett, K. W., & Spock, A. (1992). Psychological Adjustment of Children with Cystic Fibrosis: The Role of Child Cognitive Processes and Maternal Adjustment. Journal of Pediatric Psychology, 17(6), 741-755. doi: 10.1093/jpepsy/17.6.741
Tian-hui, C., Lu, L., & Michael, M., K. . (2005). A systematic review: How to choose appropriate health-related quality of life (HRQOL) measures in routine general practice? Journal of Zhejiang University Science B, 6(9), 936-9340.
Timko, C., Stovel, K. W., & Moos, R. H. (1992). Functioning Among Mothers and Fathers of Children with Juvenile Rheumatic Disease: A Longitudinal

BIBLIOGRAPHIE
- 284 -
Study. Journal of Pediatric Psychology, 17(6), 705-724. doi: 10.1093/jpepsy/17.6.705
Tluczek, A., Becker, T., Grieve, A., Laxova, A., Rock, M. J., Gershan, W. M., Green, C. G., & Farrell, P. M. (2013). Health-Related Quality of Life in Children and Adolescents with Cystic Fibrosis: Convergent Validity with Parent Reports and Objective Measures of Pulmonary Health. Journal of developmental and behavioral pediatrics : JDBP, 34(4), 252-261. doi: 10.1097/DBP.0b013e3182905646
Touchèque, M. (2014). Rapport interne de séjour de recherche. Document non publié. Université de Liège, Liège, Belgique.
Touchèque, M., & Etienne, A.-M. (2013). Reliability and validity of the Quality of Life Systemic Inventory for Children (QLSI-C): Preliminary result of a modular assessment tool of quality of life using e-Health technologies. Paper presented at the The annual conference of the Society of Pediatric Psychology, Philadelphia, PA.
Touchèque, M., & Etienne, A.-M. (2014). Assessment using e-Health technologies in pediatric Cystic Fibrosis: Developing a CF-specific module for the Quality of Life Systemic Inventory for Children (QLSI-C). Paper presented at the North American Cystic Fibrosis Conference, Atlanta, GA.
Touchèque, M., Etienne, A.-M., Missotten, P., & Dupuis, G. (in press). A comparison of a tablet version of the Quality of Life Systemic Inventory for Children (QLSI-C) to the standard paper version. Psychological Assessment.
Touchèque, M., Etienne, A.-M., Stassart, C., & Catale, C. (in press). Validation of the French Version of the Parenting Stress Index – Short Form (Fourth Edition). Journal of Community Psychology.
Traustadottir, R. (1991). Mothers Who Care. Journal of Family Issues, 12(2), 211-228. doi: 10.1177/019251391012002005
Tropauer, A., Franz, M., & Dilgard, V. (1977). Psychological Aspects of the Care of Children with Cystic Fibrosis. In R. Moos (Ed.), Coping with Physical Illness (pp. 201-218): Springer US.
Trudel, J. G., Leduc, N., & Dumont, S. (2012). Évolution du concept de qualité de vie en oncologie et de sa mesure à travers le temps. Psycho-Oncologie, 6(4), 201-208. doi: 10.1007/s11839-012-0392-4
Tsao, J. C. I., Meldrum, M., Kim, S. C., & Zeltzer, L. K. (2007). Anxiety Sensitivity and Health-Related Quality of Life in Children With Chronic Pain. The Journal of Pain, 8(10), 814-823.
Turgeon, L., & Chartrand, E. (2003). Psychometric properties of the French-Canadian version of the State-Trait Anxiety Inventory for Children. Educational and Psychological Measurement, 63(1), 172-181.

BIBLIOGRAPHIE
- 285 -
Upton, P., Lawford, J., & Eiser, C. (2008). Parent–child agreement across child health-related quality of life instruments: a review of the literature. Quality of Life Research, 17(6), 895-913. doi: 10.1007/s11136-008-9350-5
Vallejo, M. A., Jordán, C. M., Díaz, M. I., Comeche, M. I., & Ortega, J. (2007). Psychological Assessment via the Internet: A Reliability and Validity Study of Online vs Paper-and-Pencil Versions of the General Health Questionnaire-28 (GHQ-28) and the Symptoms Check-List-90-Revised (SCL-90-R). J Med Internet Res, 9(1), e2. doi: 10.2196/jmir.9.1.e2
Varni, J. W., Burwinkle, T. M., & Lane, M. M. (2005). Health-related quality of life measurement in pediatric clinical practice: An appraisal and precept for future research and application. Health and Quality of Life Outcomes, 3, 34-34. doi: 10.1186/1477-7525-3-34
Varni, J. W., Seid, M., & Rode, C. A. (1999). The PedsQL™: Measurement Model for the Pediatric Quality of Life Inventory. Medical Care, 37(2), 126-139.
Veillette, N., Demers, L., & Dutil, E. (2007). [Description of the practice of occupational therapy in emergency rooms in Quebec] [French]. Canadian Journal of Occupational Therapy, 74(4), 348-358.
Volling, B. L., & Belsky, J. (1992). The Contribution of Mother-Child and Father-Child Relationships to the Quality of Sibling Interaction: A Longitudinal Study. Child Development, 63(5), 1209-1222. doi: 10.2307/1131528
Walker, C., Papadopoulos, L., Lipton, M., & Hussein, M. (2006). The importance of children's illness beliefs: The Children's Illness Perception Questionnaire (CIPQ) as a reliable assessment tool for eczema and asthma. Psychology, Health & Medicine, 11(1), 100-107. doi: 10.1080/13548500500155792
Wallander, J. L., Schmitt, M., & Koot, H. M. (2001). Quality of life measurement in children and adolescents: Issues, instruments, and applications. Journal of Clinical Psychology, 57(4), 571-585. doi: 10.1002/jclp.1029
Wallander, J. L., & Varni, J. W. (1998). Effects of pediatric chronic physical disorders on child and family adjustment. J Child Psychol Psychiatry, 39(1), 29-46.
Weiner, D. J., Frizzell, R. A., & Orenstein, D. M. (2012). The basic defect. In D. M. Orenstein, J. E. Spahr & D. J. Weiner (Eds.), Cystic Fibrosis: A Guide for Patient and Family. Philadelphia, PA: Wolters Kluwer: Lippincott Williams & Wilkins.
Weiner, D. J., & Orenstein, D. (2012). Other Systems. In D. Orenstein, J. E. Spahr & D. J. Weiner (Eds.), Cystic Fibrosis: A Guide for Patient and Family. Philadelphia, PA: Wolters Kluwer: Lippincott Williams & Wilkins.
Weiner, D. J., & Orenstein, D. M. (2012). The Respiratory System. In D. Orenstein, J. E. Spahr & D. J. Weiner (Eds.), Cystic Fibrosis: A Guide for

BIBLIOGRAPHIE
- 286 -
Patient and Family. Philadelphia, PA: Wolters Kluwer: Lippincott Williams & Wilkins.
Weinman, J., & Figueiras, M. J. (2002). La perception de la santé et de la maladie. In G.-N. Fischer (Ed.), Traité de psychologie de la santé. Paris: Dunod.
Weinman, J., Petrie, K. J., Moss-morris, R., & Horne, R. (1996). The illness perception questionnaire: A new method for assessing the cognitive representation of illness. Psychology & Health, 11(3), 431-445. doi: 10.1080/08870449608400270
Wellman, H. M., & Gelman, S. A. (1992). Cognitive Development: Foundational Theories of Core Domains. Annual Review of Psychology, 43(1), 337-375. doi: 10.1146/annurev.ps.43.020192.002005
Werner, H. (1948). Comparative psychology of mental development. Chicago: Follett Publishing Company.
WHOQOL Group. (1993). Study protocol for the World Health Organization project to develop a quality of life assessment instrument (WHOQOL). Quality of Life Research, 2, 153–159.
Wiener, N. (1948). Cybernetics. New York: John Wiley.
Wilson, I. B., & Cleary, P. D. (1995). Linking clinical variables with health-related quality of life: A conceptual model of patient outcomes. JAMA, 273(1), 59-65. doi: 10.1001/jama.1995.03520250075037
Wilson, K. R., & Prior, M. R. (2011). Father involvement and child well-being. Journal of Paediatrics and Child Health, 47(7), 405-407. doi: 10.1111/j.1440-1754.2010.01770.x
Wu, Y. P., Steele, R. G., Connelly, M. A., Palermo, T. M., & Ritterband, L. M. (2014). Commentary: Pediatric eHealth Interventions: Common Challenges During Development, Implementation, and Dissemination. Journal of Pediatric Psychology. doi: 10.1093/jpepsy/jsu022
Wysocki, T., & Gavin, L. (2006). Paternal Involvement in the Management of Pediatric Chronic Diseases: Associations with Adherence, Quality of Life, and Health Status. Journal of Pediatric Psychology, 31(5), 501-511. doi: 10.1093/jpepsy/jsj042
Yeh, C.-H. (2002). Gender differences of parental distress in children with cancer. Journal of Advanced Nursing, 38(6), 598-606. doi: 10.1046/j.1365-2648.2000.02227.x
Yi, J. P., Vitaliano, P. P., Smith, R. E., Yi, J. C., & Weinger, K. (2008). The role of resilience on psychological adjustment and physical health in patients with diabetes. British journal of health psychology, 13(Pt 2), 311-325. doi: 10.1348/135910707x186994
Yohannes, A. M., Willgoss, T. G., Fatoye, F. A., Dip, M. D., & Webb, K. (2012). Relationship Between Anxiety, Depression, and Quality of Life in Adult

BIBLIOGRAPHIE
- 287 -
Patients With Cystic Fibrosis. Respiratory Care, 57(4), 550-556. doi: 10.4187/respcare.01328
Young, N. L., Varni, J. W., Snider, L., McCormick, A., Sawatzky, B., Scott, M., . . . Nicholas, D. (2009). The Internet is valid and reliable for child-report: An example using the Activities Scale for Kids (ASK) and the Pediatric Quality of Life Inventory (PedsQL). Journal of Clinical Epidemiology, 62(3), 314-320. doi: http://dx.doi.org/10.1016/j.jclinepi.2008.06.011
Zeller, M. H., & Modi, A. C. (2006). Predictors of Health-Related Quality of Life in Obese Youth. Obesity, 14(1), 122-130. doi: 10.1038/oby.2006.15
Ziaian, T., Sawyer, M. G., Reynolds, K. E., Carbone, J. A., Clark, J. J., Baghurst, P. A., . . . French, D. J. (2006). Treatment burden and health-related quality of life of children with diabetes, cystic fibrosis and asthma. Journal of Paediatrics and Child Health, 42(10), 596-600. doi: 10.1111/j.1440-1754.2006.00943.x


Annexes


Annexe 1
Le modèle des systèmes de
contrôle (Dupuis et al., 1989)


Annexe 1 Le modèle des systèmes de contrôle (Dupuis et al., 1989)
En l’absence de modèle intégré, cette recherche doctorale prend son
appui théorique sur le modèle des systèmes de contrôle et la définition de la
QV qui sous-tend le développement de l’Inventaire Systémique de Qualité de
Vie (ISQV) (Dupuis et al., 1989).
L’approche proposée par Dupuis et al. (1989) se base sur la notion
aristotélicienne du bonheur telle que présentée dans l’Éthique à Nicomaque
(Aristote, 1987). On y mentionne que toute activité humaine est orientée
vers des objectifs et que l’individu cherche à atteindre ces objectifs afin
d’arriver à une fin parfaite et ultime qui serait, selon Aristote, « le
bonheur ». Ainsi, dans chaque domaine de vie, le but ultime de nos actions
est d’atteindre le bonheur (Dupuis, Marois, & Etienne, 2012). Dès lors, en
s’inspirant également de la cybernétique (Wiener, 1948) et de l’approche
systémique des systèmes biologiques (Ashby, 1952; Bertalanffy, 1973;
Powers, 1973), le modèle développé par Dupuis et al. (1989) s’articule
autour de l’idée que tous les comportements humains sont contrôlés et
maintenus par la poursuite des objectifs. Ainsi, la mesure de la QV s’appuie
sur un modèle des systèmes de contrôle qui organise et donne du sens aux
comportements de l’individu (Dupuis et al., 2012).
Dans un tel système de contrôle (voir Figure 1), l’individu compare sa
situation actuelle avec sa situation désirée (objectif). L’absence d’écart
entre les deux situations démontre la satisfaction de l’individu. En revanche,
lorsque l’écart est supérieur à 0, l’individu adopte des comportements qui
visent à le réduire (= boucle de rétroaction négative). Ce dernier peut exister
entre la situation actuelle et les objectifs de l’individu afin d’arriver à un état
de satisfaction ou à un sentiment de contrôle (= mécanisme de contrôle) ;
tout en considérant que chaque objectif n’a pas la même importance (c’est-
à-dire, l’organisation hiérarchique des objectifs selon la priorité que leur

ANNEXE 1
accorde l’individu). Cependant, il est possible que les comportements que
met en place l’individu pour se rapprocher de ses buts soient inefficaces et
produisent dès lors l’effet inverse, à savoir l’augmentation de l’écart entre
sa situation actuelle et ses buts (= boucle de rétroaction positive). Cet
éloignement des buts cause une perte de contrôle qui engendre de la
frustration, de la colère ou de l’anxiété (Dupuis et al., 2012).
Figure 1 – Modèle des systèmes de contrôle (adapté de Dupuis et al., 2000)
Ainsi, le modèle des systèmes de contrôle comporte quatre composantes
principales : la situation actuelle – les buts – l’écart – et la dynamique du système
(boucles de rétroaction et hiérarchisation des objectifs). Sur base de ces
composantes, une définition opérationnelle de la qualité de vie peut être
présentée : « La qualité de vie, à un moment donné dans le temps, est l’état qui
correspond à un niveau atteint par une personne dans la poursuite continuelle de
ses buts organisés hiérarchiquement » (Dupuis et al., 1989).
Frustration, colère, anxiété
Situation actuelle
Évaluation et comparaison
Écart = 0 Écart > 0
ENVIRONNEMENT Augmentation, maintien ou diminution des
comportements
Augmentation de la satisfaction
Situation désirée
Boucle de rétroaction négative
Boucle de rétroaction positive



Annexe 2
Validation of the French Version
of the Parenting Stress Index –
Short Form (Fourth Edition)
Malorie Touchèque, Anne-Marie Etienne, Céline Stassart & Corinne Catale1
1 Accepted for publication in Journal of Community Psychology

ANNEXE 2
Abstract
Introduction: The Parenting Stress Index (PSI) is widely used to measure
stress related to the demands of parenthood. Unfortunately, no French
adaptation and validation of the PSI Short Form (Fourth Edition) had yet been
published. This study examine the factor structure and the psychometric
properties of the French translation of the PSI-4-SF. Method: Sample consists
of 210 parents of children aged 5 to 12 years old. Factor structure of the PSI-4-
SF was investigated using confirmatory factor analysis (CFA). Three models
were tested, with one, two and three dimensions. Internal consistency
reliability and validity were also examined. Results: CFA showed that the
original three-factor solution most closely approximated our data despite the
imperfection of the model fit indices. Results also indicated a good internal
consistency reliability and validity. Conclusion: The French version of the PSI-
4-SF shows promise as a valuable instrument for assessing parenting stress in
the French-speaking population.
Keywords: Parenting Stress Index; parent-child interaction; assessment tool;
factor analytic structure; psychometric properties; validation.

ANNEXE 2
1. Introduction
All parents must cope with the day-to-day stressors related to the
demands of parenthood and, consequently, experience parenting stress that
leads to negative feelings toward the self and the child (Deater-Deckard,
1998). Although there are numerous definitions of parenting stress, a
central element is the discrepancy, whether real or not, between the
perceived demands of the parenting role and parents’ perception of having
access to the resources they need to meet the demands of parenthood
(Deater-Deckard & Scarr, 1996). This specific domain of stress represents a
major study subject as it has been claimed to be important in the
development of dysfunctional parent-child interactions and a major risk
factor for adult and child psychopathology (Deater-Deckard, 1998).
Therefore, reducing parenting stress is important not only at an individual
level, to improve the parent’s psychological health, but also at a broader
level, because it may improve the efficacy of individual, family-based and
community-based interventions targeting the child’s behavioural problems
(Kazdin, 1995).
The most common measure of parents’ level of distress and parent-child
relationship is the Parenting Stress Index (PSI) (Abidin, 2012). The PSI has
been used in studies on a wide range of topic such as at-risk family (Wen,
Korfmacher, Hans, & Henson, 2010) or ethnic minorities (Franco, Pottick, &
Huang, 2010) as well as children with disruptive behaviour problems
(Semke, Garbacz, Kwon, Sheridan, & Woods, 2010) or developmental
disabilities (Hassall, Rose, & McDonald, 2005). In clinical and research
settings, a shortened 36-item PSI (PSI-SF; Abidin, 1995) is often used
instead of the long form of the PSI (120 items) which is overly lengthy and
time-consuming for screening purposes. Recent validation studies showed
conflicting results regarding the structural validity of the PSI-SF. Two
studies concluded that a single- or a two-factor model (Deater-Deckard &
Scarr, 1996; Haskett et al., 2006) for the PSI-SF provided a better solution

ANNEXE 2
than the initial three-factor model (Abidin, 1995). Another study reported
that, although fitting imperfectly, the three-factor solution most closely
approximated the data (Reitman et al., 2002). However, these studies have
been performed in specific groups (i.e. parents of toddlers, ethnically
diverse abusive parents and low-income mothers); some not representative
of the general population.
The PSI-SF has been translated into many languages (Arabic, Chinese,
Dutch, German, Italian, Portuguese, Swedish, Spanish, etc.), including
Canadian French, but no standard French version of the PSI-SF was
previously available. French language in Canada slightly differs from the
French language in Europe (France, Belgium or Switzerland) in terms of
vocabulary, pronunciation and grammar. Given that, the validation of a
standard European French version would facilitate the use of the PSI-SF on
the other side of the Atlantic.
The purpose of this study was to examine the psychometric properties
of the French translation of the PSI-SF (Fourth edition; PSI-4-SF). The factor
structure of the French version of the PSI-4-SF in a large sample of parents
with children aged 5 to 12 years old were examined using confirmatory
factor analyses (CFA). Three models were tested: a three- two- and single-
factor model. Moreover, the reliability and validity of the best model of fit
was assessed.
2. Method
2.1. Research design and Participants
We used a cross-sectional design with three samples collected from the
background population and one sample of parents having a child with a
chronic disease (i.e. Cystic Fibrosis). Samples characteristics are presented
table 1.

ANNEXE 2
Table 1 – Sample Characteristics
Participants (n) Assessment purpose Parents’ age Mode of data collection
Sample 1 163 mothers;
47 fathers
Factor structure;
reliability
M= 38.91; SD= 4.82 Online survey
Sample 2 19 mothers;
19 fathers
Criterion-related and
construct validity
M= 42.63; SD= 5.43 Face-to-face interview
Sample 3 18 mothers;
17 fathers
Discriminant validity M= 39.89; SD= 4.49 Face-to-face interview
Sample 4* 18 mothers;
17 fathers
Discriminant validity M= 43.29; SD= 5.36 Face-to-face interview
*Parents of children with Cystic Fibrosis; matched (child’s age and sex) with sample 3.

ANNEXE 2
2.2. Measures
Parenting Stress Index – Short Form (PSI-4-SF) (Abidin, 2012). The
PSI-4-SF is a 36-item questionnaire using a 5-point response scale and
divided into three subscales (12 items each) labelled Parent Distress (PD),
Parent-Child Dysfunctional Interaction (PCDI) and Difficult Child (DC). A
high total score indicates a high level of parenting stress. The PSI-4-SF was
translated from English to French following the steps of the back-
translation approach (Hambleton, Merenda & Spielberger, 2004).
State-Trait anxiety Inventory for Children (STAIC) (Spielberger,
1973). The STAIC consists of two 20-item self-report scales using a 3-point
response scale and measuring state- and trait-anxiety in children. A high
total score indicates a high level of anxiety.
Children Depression Inventory (CDI) (Kovacs & Beck, 1977). The
CDI is a 27-item self-report measure using a 3-point response scale
assessing symptoms of depression in youths 7 to 17 years old. A high total
score indicates a high level of depression.
Family Environment Scale – Form R (FES) (Moos & Moos, 1981).
The FES is a 90-item true-false scale measuring the family environment.
This scale consists of 10 subscales that can be clustered into 3 underlying
domains: Relationship; Personal Growth; and System maintenance. A high
score indicates the presence of the domain in the family environment.
2.3. Statistical Analysis
Structural validity of the French translation of the PSI-4-SF was
assessed using LISREL 8.80 (Jöreskog & Sörbom, 2006). According Gorsuch
(1983), the ratio participants per item should be at least five suggesting a
minimum of 180 participants for this study. Weighted Least Square (WLS)
estimation was applied to the covariance matrices and goodness of fit was
tested with several indices: the normed χ², the Standardized Root Mean

ANNEXE 2
Square Residual (SRMR), the Root Mean Square Error of Approximation
(RMSEA), the Comparative Fit Index (CFI), the Non-Normed Fix Index
(NNFI) and the Goodness of Fit Index (GFI). The Expected Cross-Validation
Index (ECVI) and the Akaike Information Criterion (AIC) was used to
compare models. Internal consistency and validity of the best model of fit
were assessed using SPSS (version 20.0).
3. Results
3.1. Structural validity
CFA have been conducted on the full sample (n=210) given the fact that
we did not found significant differences between mothers and fathers. We
tested several structural models on the PSI-4-SF and compared them to
each other: Model A examined the fit of the original three-factor model
(Abidin, 2012); Model B tested a two-factor model (i.e. Deater-Deckard &
Scarr, 1996; Haskett et al., 2006); and Model C examined the fit of a single-
factor model (i.e. Deater-Deckard & Scarr, 1996). Goodness-of-fit indices for
the three models tested are presented in Table 2.
Considering model comparison and despite the fact that none of the
models had a good fit, Model A provided the best fit to the data. It showed
statistically significant standardized factor loadings for all items (p < .05).
Standardized factor loadings ranged from .45 to .82 on factor I (PD),
excluding item 6 which showed loading (.29) below the salient loading
(Gorsuch, 1983). Factor loadings ranged from .41 to .84 on factor 2 (PCDI)
and from .49 to .84 on factor 3 (DC). Note that we reran the analyses
without the item 6. Given that the results did not show any significant
changes, we did not exclude the item in order to be consistent with the
initial scale.

ANNEXE 2
Table 2 – Goodness-of-Fit Indices for the Three Models Tested
Models χ² Df Normed
χ²
RMSEA RMSEA
90%CI
SRMR NNFI GFI CFI AIC ECVI
Model A:
three factors
1729.674 591 2.93 .096 .091-.101 .11 .90 .91 .91 1879.674 8.99
Model B:
two factors
1863.346 593 3.14 .101 .096-.106 .11 .89 .91 .90 2009.346 9.61
Model C:
one factor
2334.064 594 3.93 .118 .113-.123 .13 .85 .87 .86 2474.064 11.86
Note: n = 210; Number of items: 36; Estimation method: DWLS
Acceptable values of fit: Normed χ²<3 (Kline, 2005); SRMR<.10 (Kline, 2005); RMSEA<.08 (Jöreskog & Sörbom, 2006); NNFI>.90
(Hu & Bentler, 1999); GFI>.90 (Cole, 1987); CFI>.90 (Hu & Bentler, 1999); AIC and ECVI=lower value (Browne & Cudeck, 1989)

ANNEXE 2
3.2. Descriptive statistics and internal consistency
reliability
Descriptive statistics for the four different samples and Cronbach’s
alpha coefficients for the model A of the PSI-4-SF total score and its
subscales are displayed in Table 3. Comparisons of the three samples from
the background population highlighted that the sample collected using an
online survey reported higher scores than the samples collected using a
face-to-face mode of administration (sample 1 vs 2: p=.001; sample 1 vs 3:
p<.001). However, there is no significant difference between the two
samples collected using a face-to-face interview (p=.245).
3.3. Concurrent validity
Series of multiple regressions were performed and the following
variables were entered simultaneously for each subscale of the PSI-4-SF:
child’s sex, child’s age, level of education, child’s anxiety and child’s
depression. None of the variables made significant contributions in the PD
subscale. Children’s level of depression (β=.57; t=3.25; p=.003) made a
significant contribution in the PCDI subscale, accounting for 39% of the
variance. Similarly, a linear combination of children’s anxiety (β=-.37; t=-
2.19; p=.035) and level of depression (β=.70; t=4.26; p<.001) accounted for
44% of the variance in the DC factor.
3.4. Divergent validity
We computed Pearson’s correlations between the PSI-4-SF and a test
that do not measure the same construct, the FES. Results showed no
significant correlations.

ANNEXE 2
Table 3 – Descriptive Statistics and Cronbach’s Alpha values
Sample 1
(n=210)
Sample 2
(n=38)
Sample 3
(n=35)
Sample 4
(n=35)
Based on sample 1
Mean (SD) Mean (SD) Mean (SD) Mean (SD) α Inter-
correlation*
Total Stress 82.57 (17.58) 72.08 (13.52) 68.46 (12.80) 81.23 (26.70) .89 .18
Parental Distress 27.78 (7.67) 24.89 (4.35) 22.91 (4.82) 25.83 (9.58) .81 .27
Parent-Child
Dysfunctional
Interaction
24.47 (6.67) 22.24 (5.93) 21.37 (5.38) 25.86 (10.38) .79 .25
Difficult Child 30.32 (7.26) 24.95 (5.58) 24.17 (5.00) 29.54 (9.65) .79 .23
*All inter-correlations are statistically significant at p < .001.

ANNEXE 2
3.5. Discriminant validity
An analysis of variance was used to assess how the PSI-4-SF
discriminates between a group of parents having a child with Cystic Fibrosis
(CF) (i.e. sample 4) and a group of parents having a child without medical
issues (i.e. sample 3). We found significant differences between these
populations for the Total stress (F(1,68)=6.51; p=.01; η²=.087), the factor 2
(F(1,68)=5.16; p=.03; η²=.070) and the factor 3 (F(1,68)=8.55; p=.01;
η²=.112); with parents of children with CF scoring higher than parents of
children without medical conditions.
4. Discussion
This study presents the first application and validation of the PSI-4-SF
in a European French-speaking population. Regarding its factor structure,
the original three-factor solution proposed by Abidin (2012) most closely
approximated our data despite the imperfection of the model fit indices.
This finding is consistent with results reported by Reitman et al. (2002).
However, two previous studies failed to find support for the proposed three
dimensions of the scale (Deater-Deckard & Scarr, 1996; Haskett et al.,
2006). These controversial findings revealed problems with the
instrument’s current factor structure, both for the English and the French
version, and suggest it may need some modification before it fits the data
well. The PSI-SF was originally developed through a series of exploratory
factor analyses based on the full-length PSI. Results indicated that 25 items
primarily loaded on Factor 1, 18 items loaded on Factor 2 and 14 items
loaded on Factor 3 (Abidin, 1995). In addition, with regard to the
composition of the factors, 4 items that were retained on Factor 3 had a
secondary loading on Factor 2 and 1 item retained on Factor 2 had a
secondary loading on Factor 3; these secondary loadings turned out to be
higher than their primary loadings. Although the replication of the factor

ANNEXE 2
structure showed that the three-factor solution of the PSI-4-SF is relatively
stable (Abidin, 2012), Abidin’s decision to keep the 12 items on each factors
in order to allow for equivalence in subscales length might have weakened
the factor structure of the PSI-4-SF. These findings suggest that new
explorations of the PSI-SF factor structure might be useful to understand
why the original three-factor solution has not fitted the data well in any
studies examining the factor structure of this scale.
The psychometric properties of the French version of the PSI-4-SF using
the three-factor model were also assessed. Results showed a good internal
consistency, with all the reliability coefficients exceeded .79. Findings also
provided support for the validity of the PSI-4-SF in a French-speaking
population. Note that comparisons between methods of administration
(online vs face-to-face) revealed that the assessment of parenting stress, as
measured by the PSI-4-SF, is sensitive to the social desirability bias.
The present study suffers from several limitations. First, our
participants were all parents of preschool- and school-aged children.
Because the challenges of parenting change over time, future researches
should examine the psychometric properties of the PSI-4-SF with a sample
of parents of toddlers or adolescents. Second, the evaluation of the validity
is not fully resolved because not all validity ratings were investigated in this
research; for example predictive validity and convergent validity were not.
Third, the test-retest reliability of the French version of the PSI-4-SF was
not assessed. Fourth, none of the models appears to provide a very optimal
fit. Future studies are clearly needed to further investigate the factor
structure of the PSI-4-SF.
In conclusion, the French version of the PSI-4-SF has an acceptable
reliability and validity as a measure of parenting stress. Regarding its
structural validity, although CFA pointed to the three-factor model as the
best fit, corroborating Abidin’s conceptualization, none of the models
presented in this study appears to be optimal. Studies among English-

ANNEXE 2
speaking parents presented the same imperfection of the factor structure.
That issue might be solve by simply adding few more items in the different
factors as it was in the original exploratory analyses computed by Abidin
(1995). Therefore, additional studies are needed to further ensure the
factor structure of the PSI-4-SF and confirm it constitutes a valid measure of
parenting stress for French- and English-speaking clinicians and
researchers.
5. References
Abidin, R. R. (1995). Parenting Stress Index (PSI) manual (3rd ed.).
Charlottesville, VA: Pediatric Psychology Press.
Abidin, R. R. (2012). Parenting Stress Index (PSI) manual (4th ed.). Lutz, FL:
Psychological Assessment Resources.
Browne, M. W., & Cudeck, R. (1989). Single sample cross-validation indices for
covariance structures. Multivariate Behavioral Research, 24, 445–455.
doi:10.1207/s15327906mbr2404_4
Cole, D. A. (1987). Utility of confirmatory factor analysis in test validation
research. Journal of Consulting and Clinical Psychology, 55, 584–594.
doi:10.1037/0022-006x.55.4.584
Deater-Deckard, K. (1998). Parenting stress and child adjustment: Some old
hypotheses and new questions. Clinical Psychology: Science and
Practice, 5, 314–332. doi:10.1111/j.1468–2850.1998.tb00152.x
Deater-Deckard, K., & Scarr, S. (1996). Parenting stress among dual-earner
mothers and fathers: Are there gender differences? Journal of Family
Psychology, 10, 45–59. doi:10.1037/0893-3200.10.1.45
Franco, L. M., Pottick, K. J., & Huang, C.-C. (2010). Early parenthood in a
community context: neighborhood conditions, race–ethnicity, and
parenting stress. Journal of Community Psychology, 38(5), 574-590. doi:
10.1002/jcop.20382
Gorsuch, R. L. (1983). Factor analysis (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum
Hambleton, R., Merenda, P., & Spielberger, C. (2004). Adapting Educational and
Psychological Tests for Cross-Cultural Assessment. Mahwah, NJ:
Lawrence Erlbaum.
Haskett, M. E., Ahern, L. S., Ward, C. S., & Allaire, J. C. (2006). Factor structure
and validity of the Parenting Stress Index – Short Form. Journal of
Clinical Child and Adolescent Psychology, 35, 302–312.
doi:10.1207/s15374424jccp3502_14

ANNEXE 2
Hassall, R., Rose, J., & McDonald, J. (2005). Parenting stress in mothers of
children with an intellectual disability: the effects of parental cognitions
in relation to child characteristics and family support. Journal of
Intellectual Disability Research, 49(6), 405-418. doi: 10.1111/j.1365-
2788.2005.00673.x
Hu, L. T., & Bentler, P. M. (1995). Evaluating model fit. In R. H. Hoyle (Ed.),
Structural equation modeling: Concepts, issues, and applications (pp. 76-
99). Thousand Oaks, CA: Sage.
Jöreskog, K. G., & Sörbom, D. (2006). LISREL 8.80 for Windows (computer
software). Lincolnwood, IL: Scientific Software International, Inc.
Kazdin, A. E. (1995). Child, parent and family dysfunction as predictors of
outcome in cognitive-behavioral treatment of antisocial children.
Behaviour Research and Therapy, 33, 271–281.
doi:http://dx.doi.org/10.1016/0005-7967(94)00053-M
Kline, R. B. (2005). Principles and practice of structural equation modeling. New
York: Guilford.
Kovacs, M., & Beck, A. T. (1977). An empirical clinical approach towards
definition of childhood depression. In J. G. Sculterbrandt & A. Raskin
(Eds.), Depression in childhood: Diagnosis, treatment and conceptual
models (pp. 1–25). New York: Raven Press.
Moos, R. H., & Moos, B. (1981). Family Environment Scale. Palo Alto, CA:
Consulting Psychologist Press.
Reitman, D., Currier, R. O., & Stickle, T. R. (2002). A critical evaluation of the
Parenting Stress Index – Short Form (PSI-SF) in a Head Start
population. Journal of Clinical Child and Adolescent Psychology, 31, 384–
392. doi:10.1207/s15374424jccp3103_10
Semke, C. A., Garbacz, S. A., Kwon, K., Sheridan, S. M., & Woods, K. E. (2010).
Family involvement for children with disruptive behaviors: The role of
parenting stress and motivational beliefs. Journal of School Psychology,
48(4), 293-312. doi: http://dx.doi.org/10.1016/j.jsp.2010.04.001
Spielberger, C. D. (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto,
CA: Consulting Psychologist Press.
Wen, X., Korfmacher, J., Hans, S. L., & Henson, L. G. (2010). Young mothers'
involvement in a prenatal and postpartum support program. Journal of
Community Psychology, 38(2), 172-190. doi: 10.1002/jcop.20358




![La Santa Sede - w2.vatican.va · Scrittura [3], questa la costante ed universale tradizione della Chiesa; questa la solenne definizione del Concilio Tridentino che proclama e conferma](https://img.pdfslide.fr/doc/110x75/5c6e20c509d3f20e3e8c4f6c/la-santa-sede-w2-scrittura-3-questa-la-costante-ed-universale-tradizione.jpg)