Embed Size (px)
Citation preview

OXYGEN CASCADEOXYGEN FLUXOXYGEN DISSOCIATION CURVE
Presented By:Dr. Rony MathewModerators:Dr. Basheer, Dr. Krishnadas

Pressure = nRT V Diffusion of gases
Gases in contact with a liquid
Partial pressure
Properties of Gases

DALTON’s law of partial pressure Total pressure exerted by a gaseous
mixture is equal to the sum of the partial pressures of individual component in a gas mixture
Individual partial pressure exerted by a component gas in a mixture α volume fraction of that gas component in that gas mixture

Composition of Dry Air20.98% O2 78.06% N20.04% CO20.92% Other inert gases
Barometric Pressure at sea level = 1Atm = 760 mmHg
P O2 = 0.21X760 = 160 mmHgP CO2 = 0.004X760 = 0.3mmHg

Atmospheric air ↓ Alveoli ↓ Arterial blood ↓ Tissue capillaries ↓ Mitochondria
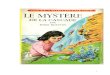
OXYGEN CASCADEIt describes the process of decreasing oxygen tension from atmosphere to mitochondria.

Water vapour pressure at body temp =
47mmHg Thus, Pressure exerted by gas in saturated
moist air = 760-47 = 713mmHg => Partial pressure of O2 in saturated
moist air = 713 x 0.21 = 149 mmHg This is the starting point of O2 cascade.

Down the respiratory tree, O2 tension is
further diluted by the alveolar CO2.
The partial pressure of alveolar oxygen(PAO2 ) is calculated by alveolar gas equation
PAO2= PiO2-PACO2/R PaCO₂ = PACO₂ ( 40mmHg ) as CO₂ is
freely diffusible.

R is RESPIRATORY QUOTIENT(RQ) , the ratio of rate of CO₂ produced to the rate of oxygen uptake.
RQ=VCO₂/VO₂ 200/250=0.8 RQ depends on the metabolic substrate
ie,carbohydrate only diet =1. Protein &fat=0.8
So PAO2 =149-(40/0.8)~100mmHg.

ALVEOLUS TO BLOOD Alveolar PAO2 is 100mmHg. Blood returning
from tissues to heart has low PO2 (40mmHg).
So oxygen diffuses from alveoli to pulmonary capillaries.
After oxygenation,blood moves to pulm. veins→left side of heart→ arterial system → systemic tissues.
In a perfect lung pO₂ of pulm. Venous blood would be equal to pO₂ in the alveolus.

O2 DELIVERY TO TISSUES(DO2)
= [(1.34 x HbxSaO2)+(0.003xPaO2)] x Q
O2 delivery to tissues depends on Hb concentration O2 binding capacity of Hb saturation of Hb amount of dissolved O2 cardiac output (Q)

UNLOADING OF O2 AT TISSUES Initially the dissolved O2 is consumed. Then the sequential unloading of Hb bound O2
occurs. Transport of O2 from the capillaries to tissues is
by simple diffusion. Pasteur point is the critical PO2 at which
delivered O2 is utilised by the tissue & below which the O2 delivery is unable to meet the tissue demands.


O2 CASCADE


FACTORS AFFECTING O2 CASCADE AT EACH
LEVEL

Atmosphere to alveolus
High altitude. At high altitude, the barometric pressure is
less than that at sea level, and thus, even though the FiO2 is 21%,the piO2 is decreased.
Water vapour Higher the water vapour lesser will be the
PiO2 . Upper resp. tract, humidifies inspired air , depends upon temp.

In the alveolus Amount of CO2 in the alveolus depends on
the metabolism & degree of hypoventilation.
Fever,sepsis,malignant hyperthermia increases CO2 production.

Alveous to capillaries
• Ventilation/perfusion mismatch
• Shunt
• Slow diffusion.

VENTILATION /PERFUSION MISMATCH
• in normal lung itself upper zones are over ventilated while lower zones are relatively overperfused and under ventilated.
• pulmonary venous blood is a mixture of pulmonary capillary blood from all the alveoli,hence a lower PO2 than PAO2

SHUNTS
Occur when deoxygenated blood passes unventilated alveoli , without getting oxygenated , to enter the systemic arterial system .
examples of shunts : atelectasis consolidation of lung small airway closure. These effects are overcome by a
compensatory mechanism termed HYPOXIC PULMONARY VASOCONSTRICTION ( HPV ).

SLOW DIFFUSION Normally diffusion is very rapid and is
completed by the time the blood has passed about 1/3 of the way along the pulm. capillary.
Diffusion is affected in pulmonary diseases.


ALVEOLAR ARTERIOLAR GRADIENT : P( A – a )O2
Partial pr of Oxygen in Arterial blood is given by
PaO2=102-age/3 Normal Aa gradient is 5-15mmHg. AA gradient ↑ due to: slow diffusion. atelectasis pulm. Edema congenital heart disease(right to
left shunt)

Aa gradient depends upon: shunt ventilation/perfusion mismatch mixed venous O2 tension Aa gradient directly proportional to shunt
and inversely proportional to mixed venous O2 tension.

Arterial blood to tissue Serum Hb level. Percentage of Hb saturated with O2. Cardiac output. Amount of dissolved oxygen.

OXYGEN CARRIAGE BY BLOOD In two ways
Dissolved in serum.(5%) Combination with Hb(95%)

OXYHEMOGLOBIN
One Hb molecule with its 4 heme group is capable of binding 4 molecules of O2.
1gm of fully oxygenated Hb contains 1.34ml of O2 (vary depending on Fe content)
At an arterial PO2 of 100mmHg,Hb is 98% saturated,thus 15gm of Hb in 100ml blood will carry about 20ml of O2
=1.34ml x 15gm x 98/100=20

DISSOLVED OXYGEN• Henry’s law :states that the
concentration of any gas in a solution is proportional to its partial pressure
• Gas concentration= x partial pressure is the gas solubility coefficient =0.003ml/dl(100ml of blood)/mmHg
for O2
• Dissolved O2 in arterial blood is thus 0.3ml/dl (0.003ml/dl x100mmHg).

Venous blood have an O2 partial pressure of 40mmHg and Hb is 75% saturated.thus it contains about 15ml of O2/100ml
1.34x15x75/100=15
Thus every 100ml of blood passing through the lungs will take up 5ml of O2

OXYGEN CONTENT Total O2 content of blood is the sum of O2
in the solution & that carried by Hb. O2 content=0.003ml O2/dl x PaO2 + 1.34 x Hb x %
saturation of Hb

OXYGEN FLUX Amount of O2 leaving the left ventricle per
minute in the arterial blood . O2 content of arterial blood X cardiac
output O2 content of arterial blood = (O2 bound to
Hb + dissolved O2) i.e 20ml+0.3ml=20.3ml/dl(20.3ml/100ml) So O2 flux=20.3ml/100ml X
5000ml=1000ml

Hb : Anaemic Hypoxia O2 saturation : Hypoxic Hypoxia Cardiac output : Stagnant Hypoxia
Three factors can decrease O2 Flux

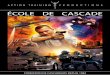
Relates saturation of Hemoglobin (Y axis) to partial pressure of O2 (X axis)
It’s a sigmoid shaped curve with a steep lower portion and flat upper portion
Describes the nonlinear tendency for O2 to bind to Hb.
O2 DISSOCIATION CURVE(ODC)


Ferrous iron in each heme binds with one O2
One Hb molecule can bind 4 molecules of O2
Deoxy Hb : globin units are tightly bound in a tense configuration (T state)
As first molecule of O2 binds, it goes into a relaxed configuration (R state) thus exposing more O2 binding sites 500 times increase in 02 affinity characteristic sigmoid shape of ODC

CHARACTERISTICS OF THE CURVE

SHAPE OF THE CURVE
Characteristic sigmoid shape which offers many physiological advantages
It reflects the physiological adaptation of Hb to take up O2 at higher partial pressures (alveoli) and release oxygen at lower partial pressures (tissues )

The flat upper portion means that even if PO2 falls somewhat, loading of O2 wont be affected much.
Even when red cells take up most of the O2 from alveoli , PO2 drop is less compared to gain in saturation a large PO2 difference still exists for diffusion of O2 to continue

The steep lower part of the curve means peripheral tissues can withdraw large amounts of 02 for only a small drop in capillary PO2.
This maintenance of blood PO2 assists diffusion of 02 into tissue cells

The characteristic points on the curve are:
1) The arterial point PO2=100mmHg and SO2=97.5%
2) The mixed venous point PO2=40mmHg and SO2=75%
3) The P50 PO2=27mmHg and SO2=50%
ANCHOR POINTS IN THE CURVE


It is the partial pressure at which 50% of Hb is saturated.
At a pH of 7.4 , temp 37C , the PO2 at which the Hb is 50% saturated (P50) is 27mmHg
When affinity of Hb for 02 is increased , P50 decreases : shift to left in ODC
When affinity is reduced , P50 increases : shift to right in ODC
P50


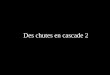
SHIFT OF ODC

Right shift - High P50 (>27mmHg)
Hb has decreased affinity for O2 O2 delivery facilitated at tissue level
Causes: Increase in H+ Increase in temperature Increase in 2,3 DPG Increase in PCO2 Exercise Anaemia Drugs : propranalol , digoxin etc

Left shift - Low P50 (<27mmHg)
Hb has ↑ed affinity for O2 O2 delivery at tissues is decreased
Causes: Low H+ Low temperature Low 2,3 DPG Low PCO2 Variants of normal Hb (fetal Hb, carboxy Hb,
met Hb)

Temperature Increase in temperature decreases Hb-O2
affinity and curve is shifted to right
Decrease in temperature increases affinity and curve shifted to left decreased release of O2
But this wont cause hypoxia because in hypothermia body O2 demand is also less
FACTORS AFFECTING ODC

Hydrogen ions Acidosis decreases Hb-O2 affinity and curve
is shifted to right
Deoxy Hb binds with H+ more actively than does oxy Hb
H+ + HbO2 H.Hb +O2
Advantageous at tissue level

Acute conditions : 0.1 unit Ph change causes 3mm Hg change in P50
Chronic (>2-3 hrs) : depends on compensatory changes in organic phosphate synthesis (2,3 DPG, ATP)

Carbon dioxide Effects attributed to changes in pH
CO2 + H2O H2CO3 H + HCO3
Increase in CO2 shifts curve to right causing more release of O2
BOHR EFFECT


2,3 DPG Produced in red cells by Embden meyerhof
shunt pathway of glycolysis
Normal concentration : 4mmol/l
Binds to deoxyHb and reduces its affinity for O2
ODC is shifted to right
Fetal erythrocytes have lower concn of 2,3 DPG and hence HbF has a higher affinity for O2


FACTORS INCREASING 2,3 DPG
Anaemia Hypoxemia Cardiac failure Chronic acidosis Hyperthyroidism Uremia Cirrhosis liver

FACTORS DECREASING 2,3 DPG
Polycythemia Hyperoxia Chronic alkalosis Hypothyroidism Blood storage
NB: blood stored with ACD anticoagulant loses 2,3 DPG faster (6-7 days) than CPD blood. Effect starts immediately after transfusion and may last for 2-3 days

Physiological situations(1) Exercise ODC for skeletal muscles shifted to right This ensures max O2 delivery for
exercising muscles Factors : Increased CO2 production Increased Temperature Presence of myoglobin (higher O2 affnity)
Other conditions affecting ODC

(2) High Altitude A s distance from sea level increases , partial
pressure of gases in atmosphere decreases
But, volume remains constant eg: 21% for O2
Leads to a progressive reduction in ambient O2 Hypoxia
Compensatory mechanisms net effect is right shift of ODC

Increased alveolar ventilation
Increased Hb production
Increase in 2,3 DPG
Increase in diffusing capacity of lungs
Increase in vascularity of tissues
Increase cellullar use of 02

Congenital Abnormalities
Hemoglobinopathies: ODC shifted to right or left depending on affinity of abnormal Hb to O2
Deficiency of red cell metabolism Pyruvate kinase deficiency : shift to right d/t elevated 2,3 DPG levels

Carbon Monoxide Poisoning Hb has 200 times higher affinity for CO than O2
50% saturated at 0.4mmhg
Displaces O2 from Hb
Increases O2 affinity of those hemoglobin unbound to CO
Together it produces a shift to left in ODC and over all decrease in 02 delivery

Chronic disease states
Cardiopulmonary disease : decreased cardiac output O2 extraction more increased deoxyHb stimultes 2, 3 DPG production shift to right
Anaemia : 2 important compensatory mechanisms
1)increase in CO and oxygen delivery 2)right shift of ODC – increase in 2,3DPG

Acute disease states Shock: Net effect on ODC involves
interaction of pH , PCO2, temperature and many other factors.
2,3DPG & P50 were lower in patients with septic shock.
Shift to left massive transfusions , a/c alkalosis (hyperventilation , bicarbonate administration) , hypothermia , hypophosphatemia etc

A/c MI: right shift with an elevated P50
Hypophosphataemia as occurs in starvation, vomiting, malabsorption etc causes increased Hb-O2 affinity and shift ODC to left

Occurs at feto-maternal interface.
CO2 & other metabolic products from the fetal blood diffuses into maternal blood making maternal blood more acidic & fetal blood more alkaline.
DOUBLE BOHR EFFECT

In maternal side ODC is shifted to right with ↓ed O2 affinity, causing ↑ed O2 release to fetus
In fetal side , there is left shift of ODC, ↑ing O2 affinity
Thus Bohr effect acting in two different directions having a beneficial effect



ODC AND THE ANAESTHESIOLOGIST

ODC helps us to relate PO2 and Hb saturation
A left shift gives a warning that tissue oxygen delivery may be compromised even when there is not much drop in PO2
All inhalational agents including N2O causes shift to right
Intravenous agents have no demonstrable effect on ODC

Among other drugs : propranalol , steroids have been found to be associated with shift to right and improved tissue oxygenation
Blood transfusion : whenever possible, ACD anticoagulated fresh blood (<5-7 days old) should be used and avoid massive transfusions.

Thank you
Thank you