Embed Size (px)
Citation preview
8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 1/17
Stem Cells in the Treatmentof Heart Disease
Stefan Janssens
Division of Cardiology and Vesalius Research Center, VIB, Gasthuisberg University Hospital, University of Leuven, B-3000 Leuven, Belgium;email: [email protected]
Annu. Rev. Med. 2010. 61:287–300
The Annual Review of Medicine is online atmed.annualreviews.org
This article’s doi:10.1146/annurev.med.051508.215152
Copyright c 2010 by Annual Reviews. All rights reserved
0066-4219/10/0218-0287$20.00
Key Wordscardiac stem cells, neovascularization, cardiomyogenesis, regenerativemedicine (myocardial repair), transdifferentiation
Abstract
Progenitor cells residing in bone marrow, adipose tissue, and skeleta
muscle or circulating in the blood are capable of improving myocardiafunction in preclinical models. In contrast, early clinical studies usin
bone marrow cells have shown mixed results and reflect our incompletunderstanding of underlying mechanisms. Recent identification of var
ious cardiac precursor cells has suggested an endogenous reservoir fo
cell-based repair. However, confronted with massive cardiac cell lossinventive strategies and enabling technologies are required to mobilize or deliver functionally competent progenitor cells to sites of injury
or to effectively stimulate endogenous repair. We review our presenknowledge in this promising and rapidly evolving development in car
diovascular medicine and highlight obstacles as well as opportunities.
287

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 2/17
AMI: acutemyocardial infarction
INTRODUCTION
Theuseofhumanstemcellsisbecomingpivotalfor the development of new therapeutic strate-
gies for many organ-specific diseases, which arecharacterized by abrupt or progressive loss of
function and for which existing therapies areinadequate. Many significant human diseases
with limited options for a definitive cure arecharacterized by the loss or malfunction of spe-cific cell types in the body. This is especially
true for diseases associated with aging, includ-ing Alzheimer’s and Parkinson’s disease, type II
diabetes, heart failure, osteoarthritis, and au-toimmune and hematopoietic disorders. The
potential use of stem cells is also attractive formedical conditions resulting from acute dam-
age to cells, e.g., infarction, trauma, and burns.In cardiology, the emerging field of treat-
ment called regenerative medicine or cell ther-apy has focused for many years on the develop-
ment of methods to either induce replacementof damaged cells with stem cells to replenish
the deficit or (at least) use stem cells to mediate
functional repair via paracrine, trophic effects(1). However, there is currently a growing un-
derstanding that in the course of evolution, theheart, like many adult solid organs, harbors a
population of endogenous progenitor cells, po-tentially capable of regenerating the parenchy-
mal cells of the tissue when properly activated(2). Importantly, for any cell therapy to be suc-
cessful, equal efforts are required (a) to developbiomaterials, (b) to study signaling cues that will
facilitate sustained cross-talk between cells andtheir specific microenvironment, and (c ) to de-
velop enabling technologies for successful clin-
ical applications.
THE UNMET CLINICAL NEEDIN HEART DISEASE
Despite state-of-the-art interventional andmedical therapy for myocardial infarction (MI)
andheart failure, clinical outcome remains poorin post-MI patients with reduced left ventricu-
lar (LV) function. The one-year mortality rateis 13%, and the incidence of the combined
endpoint of death, recurrent infarction, or
hospitalization for heart failure is 26%
These sobering results are based on caremonitoring of patients included in randomiz
controlled trials, where implantable automa
defibrillators, resynchronization devices, apharmacological treatment with beta blo
ers, angiotensin converting enzyme (ACinhibitors, or angiotensin receptor block
and spironolactone are optimally implement Most likely, clinical outcome in daily pract
outside the setting of randomized trials is evmore dismal.
Advanced heart disease results from abrupt or progressive loss of contractile m
ocytes, which in western societies is most ten caused by an acute or chronic reduction
coronary blood flow. Therefore, soon after
firstpromisingresultsfrommixedmononuclebone marrow cells or selected subpopulatio
in small-animal models of cardiac ischemic jury (4), translational studies in patients w
heart disease were initiated. In addition to thencouraging preclinical studies, the observ
chimerism in the human heart (5, 6) furthstimulated clinical researchers to explore aut
ogous mononuclear bone marrow cell transstrategies in ischemic heart disease.
EARLY CLINICAL EXPERIENCE
Initial trials of autologous bone marrow cedocumented safety and feasibility both in
tients with acute myocardial infarction (AMand in those with chronic ischemia and
ported a modest, beneficial effect on recupation of LV function (7, 8, 9). By virtue
their exploratory design andemphasis on safethese studies were not randomized, and th
lacked a control population undergoing bomarrow aspiration followed by intracoron
infusion of vehicle or infusion of an irre
vant cell type. Again, the encouraging resuof this first clinical experience have accel
ated subsequent introduction of larger randoized controlled trials. By 2006, four indepe
dent randomizedstudiesusing autologous bomarrow–derived progenitor cells had be
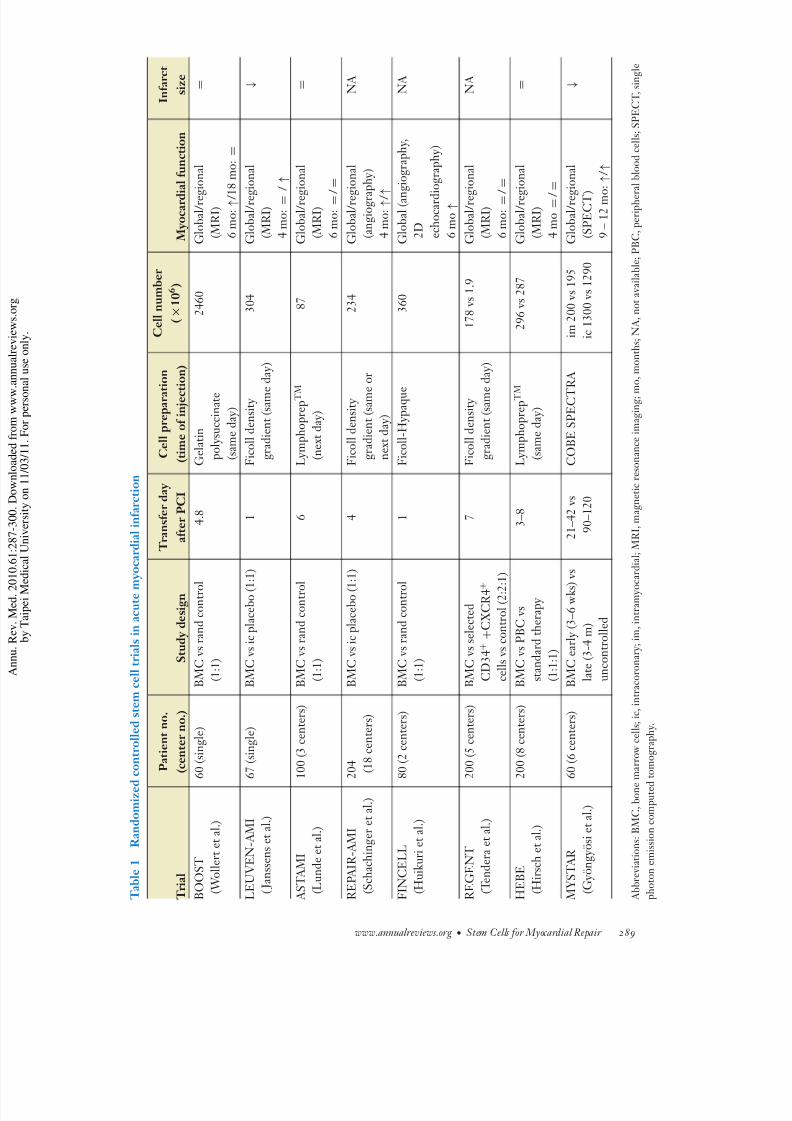
reported in AMI patients ( Table 1). T
288 Janssens
8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 3/17

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 4/17
PCI: percutaneouscoronary intervention
LVEF: left ventricularejection fraction
common objective was to investigate whether
or not intracoronary infusion of autologous
bone marrow cells conferred incremental ben-efit beyond state-of-the-art reperfusion ther-
apy and postinfarction pharmacological ther-apy. Inherent to the early stage of development,
the studies differed in design, patient numbers,cell preparation methods, timing of cell trans-
fer after percutaneous coronary intervention(PCI), and imaging modalities.
The BOOST study was the first random-ized controlled study to report a significant
improvement in global LV function recovery after six months, expressed as a 6% incremen-
tal increase in LV ejection fraction (LVEF)
evaluated using magnetic resonance imaging(MRI) in patients who had received intracoro-
nary cell infusion after a median of 4.8 daysfollowing index PCI (10). The authors at-
tributed the transient cell-mediated benefit toenhanced regional contraction in the infarct
border zones. The study was, however, notplacebo-controlled; the control group did not
undergo bone marrow aspiration, nor a sec-ond coronary intervention with repeated stop
flow conditions. Moreover, functional recovery at six months was confined to the cell trans-
fer group and—somewhat unexpectedly—not
observed in control patients. Of note, one andfive years later, global LV function in patients
who had received cell transfer was the same asthat in patients who had received state-of-the-
art treatment (11). The relatively small numberof patients, the absence of a control group un-
dergoing repeat coronary infusions, andthe rel-atively mild reduction in LV function after the
index infarction need to be considered when in-terpreting these results.
Two subsequent double-blind randomizedplacebo-controlled studies, conducted at the
universities of Leuven and Frankfurt (12, 13)in a similar AMI population, addressed some
of these confounding variables associated with
bone marrow aspiration and a second catheter-ization. The increase in global LV function
recovery in patients randomized to cell transferabove and beyond the increase in control
patients receiving state-of-the-art therapy
ranged from 1.2% to 2.5% supplemen
increase in LVEF. In addition, patients ceiving cell transfer had a significantly grea
reduction in infarct size for a similar arearisk, as assessed using repeated MRI, an
greater recovery of regional systolic functi
Importantly, these beneficial effects wsustained at one-year follow-up (14, 15).
Whereas bone marrow cell isolation, preration, and characterization protocols w
similar in the Leuven and Frankfurt stuies, this was not the case for the Norw
gian ASTAMI study ( Table 1). The latter walso not placebo-controlled and concluded
100 post-AMI patients that mononuclear bomarrow–derived cell transfer did not incre
global LV function recovery or reduce infasize at six months as evaluated by MRI (1
Although the reasons for these divergent fin
ings are still unclear, significant differencestrial design, isolation, and characterization
the stem cell preparation need to be conside(17). Indeed, a head-to-head comparison of
cell infusate in the Repair-AMI and the A TAMI studies revealed important difference
bone marrow cell functionality, depending laboratory procedures (17, 18).
The Frankfurt Repair-AMI trial was a mticenter study involving 18 different sites w
a central core laboratory for bone marrow cprocessing (13). Cell transfer was therefore n
always performed on the same day after the
dex PCI but ranged from three to seven da whereas patients in the Leuven study receiv
placebo or bone marrow cell infusion at 2after the first intervention. Interestingly, wh
data were stratified by time of cell transfer aby severity of LV dysfunction at baseline,
benefit was predominantly observed in patiereceiving delayed cell transfer and in patie
with a baseline LVEF below the median vaof 49%. The latter observation is in agr
ment with our own findings of significanenhanced metabolic recovery in AMI patie
with large infarctions receiving cell transfer.
though the studieswere not powered to primily evaluate the effects of MI size, there wa
significant interaction between infarct sever
290 Janssens

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 5/17
and subsequent benefit from cell transfer. The
best results were observed in patients suffer-
ing from large infarctions with more depressedglobal ejection fractions (incremental increase
in LVEF of 5%–6%). Because of the smallernumber of patients, we failed to detect a signif-
icant difference in global functional recovery but did observe significantly greater improve-
ment in regional contractile function in the in-farct core and border zones, using both MRI
and tissue Doppler analysis (19). Interestingly,strain rate and MRI-based wall-motion analysis
in all infarcted segments with a >50% trans-mural extent of myocardial necrosis confirmed
a significant benefit up to one year after cell
transfer (15). We cannot exclude that by givingthe cells sooner after the index infarction, we
may have missed a more favorable time pointfor cell transfer, especially in view of the high
incidence of microvascular obstruction that isobserved in the early phase of reperfusion and
that may limit homing, engraftment, and sur- vival of infused cells.
As highlighted in editorial comments thataccompanied these pioneering studies, the best
focus for future cell therapy efforts, therefore, would be in patients with severe ischemic car-
diomyopathy (anterior infarctions and signif-
icant LV dysfunction) (20, 21). This focus isconsistent with the unmet clinical need in this
expanding population and represents the primetarget in second-generation clinical trials.
A major point of discussion, however, re-mains whether or not the absolute incremen-
tal increase in LVEF of 1.2% to 2.5% or thefavorable effect on coronary flow reserve (22),
infarct remodeling, and recovery of regionalLV function translate into a meaningful clini-
cal benefit at longer-term follow-up and justify the additional costs of cell-based interventions.
Although only adequately powered prospectiveclinical trials can provide the answers, the ques-
tion echoes earlier discussions on the benefit of
changes in LVEF of similar magnitudeobtained with beta blockers and ACE inhibitors in heart
failure (23).
STEMI: ST-segmeelevation myocardiainfarction
SECOND-GENERATION RANDOMIZED CLINICAL TRIALS
The common objective of the first four land-
mark trials was to investigate incremental ben-efit of autologous bone marrow cell transfer
on global LV function recovery beyond state-of-the-art therapy for ST-segment elevation
myocardial infarction (STEMI). In contrast,the most recent randomized studies also ad-dressed (a) cell transfer in AMI patients re-
ceiving thrombolysis (24), (b) the added valueof CD34+CxCR4-selected hematopoietic stem
cells(25),(c )selectionofalternativecontrolcellsandsurrogate primary end points (26), (d )more
restrictive inclusion criteria, and (e) differenttiming (early or late) and cell delivery routes
(combined intramyocardial and intracoronary injection) (27) ( Table 1).
The FINCELL study is a multicenter ran-domized placebo-controlled trial including 80
patients with STEMI treatedwith thrombolysis
followed by PCI and stenting 2–6 days after theacute coronary event (24). Patients were ran-
domly assigned to receive intracoronary mixedbone marrow cells or placebo solution infused
into the infarct-related coronary artery imme-diately after stenting. This study confirmed that
intracoronary administration of bone marrowcells is safe in STEMI patients treated with
thrombolytic therapy followed by PCI and isassociated with an incremental improvement of
global LVEF measured by LV angiography (7.1 vs 1.2%, p = 0.05) and 2D echocardiography
(4.0 vs −1.4%, p = 0.03). In this study, how-
ever, the biological significance of the observedchanges in LVEF remains unclear as baseline
values indicated virtually preserved global LV function before cell infusion.
The Polish REGENT trial, in contrast, wasa randomized but not placebo-controlled mul-
ticenter trial including 200 AMI patients withbaseline LVEF ≤40% undergoing primary
PCI (25). Patients were randomly assigned toselected CD34+CXCR4+ bone marrow cell
infusion, unselected mononuclear cell infusion,or control (ratio 2:2:1). The median time
www.annualreviews.org • Stem Cells for Myocardial Repair 291

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 6/17
between PCI and cell infusion was seven days
(range 3–12 days), and the median number
of infused CD34+CXCR4+ cells was 1.9 ×
106 in the selected cell group versus 1.78 ×
106 in the unselected mononuclear cell group. At six months, the increase in LVEF observed in
the cell treatment groups was not significantly different from the increase in control patients.
Of note, and consistent with the Repair-AMIstudy, a post hoc analysis in patients whose
initial LVEF was below the median value of 37% indicated a more pronounced (∼5%)
increase in global function recovery followingcell transfer. Importantly, the design of the
study did not allow evaluation of potential
benefits of bone marrow cell enrichmentstrategies, because the number of injected
CD34+CxCR4+ cells did not differ betweenthe two cell arms of this study. Moreover,
the primary endpoint analysis using repeated MRI was performed in only ∼60% of included
patients (117 of 200 patients), which reducedthe power to detect cell-mediated differences
in global function recovery. The HEBE trial is also a multicenter
randomized but not placebo-controlled trialincluding 200 STEMI patients undergoing
primary PCI (26). Patients in eight medical
centers in the Netherlands were randomized tointracoronary bone marrow–derived mononu-
clear cell infusion, mononuclear peripheralblood cell infusion, or primary PCI alone
(ratio 1:1:1). Cell aspiration and intracoronary infusion were performed 3–8 days after primary
PCI. Despite promising results in the pilottrial (28, 29), intracoronary infusion of bone
marrow–derived cells failed to improve re-gional myocardial function recovery (primary
endpoint) and global LV function and LV remodeling (secondary endpoints) in first-time
large-STEMI patients undergoing PCI. The
reasons for these negative findings are unclear,and although we are still awaiting data on
infarct remodeling in this carefully executedstudy with serial MRI analysis in 189 of 200 pa-
tients, we can only speculate that the functionalcapacity of cells and/or their ability to home,
engraft, and survive in ischemic myocardium
is insufficient to mediate detectable biologi
effects. MYSTAR was a randomized multicen
open-label trial including 60 patients w
LVEF <45% after AMI (27). Bone marroderived mononuclear cells were delivered
combined intramyocardial injection and intcoronary infusion at either 3–6 weeks (ear
or 3−4 months (late) after AMI. This studemonstrated feasibility, safety, and efficacy
combined delivery of a large number of atologous bone marrow–derived mononucl
cells in patients after AMI with severely dpressed LV function. Early and late treatm
both resulted in an improvement in infarct sand global systolic function recovery, and
benefit was sustained at 9–12 months. Ho
ever, in the absence of a randomized contgroup, the biological significance is uncl
Prospective randomized controlled trials wbe required, including the ongoing multice
ter SWISS-AMI trial in 150 STEMI patiencomparing early, late, or no cell transfer af
PCI. Taken together, these recently reported
als, some of which are still ongoing, confithat treatment with bone marrow–derived c
is safe and feasible in AMI patients and in ptients with ischemic cardiomyopathy. Howev
the use of selected bone marrow stem cedid not show an additional benefit over mix
mononuclear bone marrow cells or state-
the-art reperfusion and pharmacological thapy, despite selection of patients with mo
pronounced LV dysfunction (REGENT aHEBEstudies).Itisdifficulttoreconcilethea
parently discrepant results in the above stud with the earlier-stated best window of opp
tunity for cell therapy, but limitations in studesign or conduct may account for some of
variability. Moreover, accumulating data poto reduced functionality of bone marrow c
in patients with severe and advanced ischemheart disease (30), and these recent obser
tions may well have affected the outcome
REGENT and HEBE, which specifically tgeted patients with large MIs and likely mo
advanced atherosclerotic disease.
292 Janssens

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 7/17
UNRESOLVED QUESTIONS ON MECHANISMS OF ACTION:CARDIOPROTECTION VERSUSCARDIOMYOGENESIS?
Until recently, the major premise in preclini-
cal tests was that circulating or bone marrow–derived progenitor cells could potentially re-
populate the injured myocardium and undergomilieu-dependent differentiation to form vas-cular cells and cells with a cardiomyocyte-like
phenotype (31). Improvements in cardiac func-tion following adult mononuclear stem or pro-
genitor cell injection in preclinical models wereinitially ascribed to cardiac and vascular regen-
eration via such autocrine transdifferentiationmechanisms (4). However, theplasticity of adult
stem cells remains debatable, with more recentdata questioning the validity of the cardiomyo-
genic potential of these cells (32). Based on ob-servations in genetically engineered mice al-
lowing unambiguous tracking of both donor
lineage and cardiac phenotype with a singlemolecular marker, the prevailing view among
stem cell scientists and developmental biolo-gists is that cardiac transdifferentiation after
direct injection of hematopoietic stem cells is very limited (33, 34). Moreover, limited reten-
tion, engraftment, and survival of transferredcells in clinical and preclinical studies alike fa-
vor paracrine effects via secreted trophic factorsthat may stimulate nutrient blood supply, re-
duce apoptotic cardiomyocyte death,or activateresidual cardiac resident stem cells (Figure 1)
(35, 36). Differentiation into cardiomyocyteshas only been clearly demonstrated in embry-
onic stem cells (37) and cardiac resident stem
cells (38, 39). More recent preclinical stud-ies in mice have likewise suggested that in-
tracardiac injection of in vitro expanded adultmesenchymal stem cells exerted a beneficial
effect on the infarcted myocardium by enhanc-ing neoangiogenesis rather than via true car-
diac regeneration (40). Thus, despite initialreports of cardiomyogenic potential, many sub-
sequent studies in mice, rats, and pigs have con-cludedthatbonemarrow–derived or circulating
CSC: cardiac stemcell
progenitor cells may improve cardiac function
indirectly via release of trophic factors that en-
hance angiogenesis and rescue cardiomyocytesat risk in the infarct border zone (35, 41, 42).
Similarly, the limited improvement in globalsystolic function recovery in clinical studies
with adult mononuclear bone marrow cells hastraditionally been ascribed to insufficient hom-
ing, engraftment, and survival of transplantedcells into the ischemic and hostile milieu. To
a certain extent, this may relate to faulty ex-trapolation of the data from small animals to
the human, failure to properly account forthe difference in size between rodent and hu-
man, and the unknown nature, functionality,
and number of true stem cells administered(43).
In addition, most of the cell transplantation–based therapeutic approaches used so far are
predicated on the concept that the adulthuman myocardium does not have intrinsic
regenerative capacity because the workingmyocytes are terminally differentiated cells
with no regenerative capacity. Recently, how-ever, the adult myocardium has been found
to harbor a population of resident pluripotentcells with the characteristics of true cardiac
stem cells, i.e., self-renewing, clonogenic,
and multipotent. Several groups have iden-tified cardiac stem cells possessing growth
factor–receptor systems and reported differentmembrane markers or transport proteins.
These endogenous cardiac stem cells (CSCs)are able to regenerate the contractile myocytes
and endothelial and smooth muscle cells of the microvasculature, but their numbers vary
substantially between species, and it is unclear whether they constitute phenotypic variations
of a unique cell type (38, 44). The very recentdemonstration that human ISL1 heart progen-
itors, isolated from second-heart-field-derivedstructures in embryonic life, are capable of self-
renewal, expansion, and differentiation into the
major cell types in the heart provides anotherimportant model system for ES-cell-derived
cardiomyogenesis (55). All these discoveries
www.annualreviews.org • Stem Cells for Myocardial Repair 293

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 8/17
Functional repair
Stem cell transfer
Myocardial
injury/damagePCI (CABG-MedR/)
Trophiceffects
Cardiac regeneration
Stimulation/maturation of cardiac stem cells
Transdifferentiation?
Ischemia Necrosis Remodeling
Cardiac muscle Skeletal muscle Adipose tissueBone marrow
CardioprotectionCMC apoptosisCMC oxidative stressCMC metabolismNeovascularizationFibrosis/matrix remodeling
Figure 1
Cell-based myocardial functional repair. Abbreviations: PCI, percutaneous coronary intervention; CABGcoronary artery bypass grafting; CMC, cardiomyocyte.
have opened novel therapeutic avenues for
physiologically meaningful regeneration of the myocardium damaged by ischemic orinflammatory events or by congenital defects
(1, 45, 46). The problem is that these reservoirs of cells
are usually overridden in patients with AMI,
advanced coronary artery disease, and chronicheart failure. Despite this limited capacity for
regeneration of myocardium, the existence of these repair mechanisms suggests that cardiac
repair may be achieved therapeutically in these
clinical settings, given the appropriate stim-ulation (in situ activation, multiplication anddifferentiation of the eCSCs) and/or adoptive
transfer of (stem) cells involved in these pro-cesses (47, 48). Cardiac repair via endogenous
CSCs represents a major target for translationalresearch in the years to come.
THE QUEST FOR THE OPTIMA
CELL SOURCE: AUTOLOGOUS VERSUS ALLOGENEIC,EXOGENOUS VERSUSENDOGENOUS PROGENITOR CELLS?
Autologous cell therapies, even if their clical efficacy were markedly superior, suffer fr
relative complexity and face significant cconstraints posedby the need to make the tre
ment affordable to large numbers of candate patients. Moreover, the clinical requi
ment for a readily available (“off-the-shel
treatment that can be prepared and admintered in the majority of catheterization la
oratories during the acute phase of the dease remains a major challenge ( Table 2).
circumvent some of these obstacles, a ra
294 Janssens
8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 9/17
8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 10/17
Basic research:Stem/progenitor celldifferentiation andmaturation
Interaction:Cells, microenvironment,and biomaterials
Tissue generation: Tissue organization
Enablingtechnologies:• Biomarkers• Imaging technologies• High-throughput• technologies• Model systems• Bioreactors
Regenerative
therapies:• Clinical validation
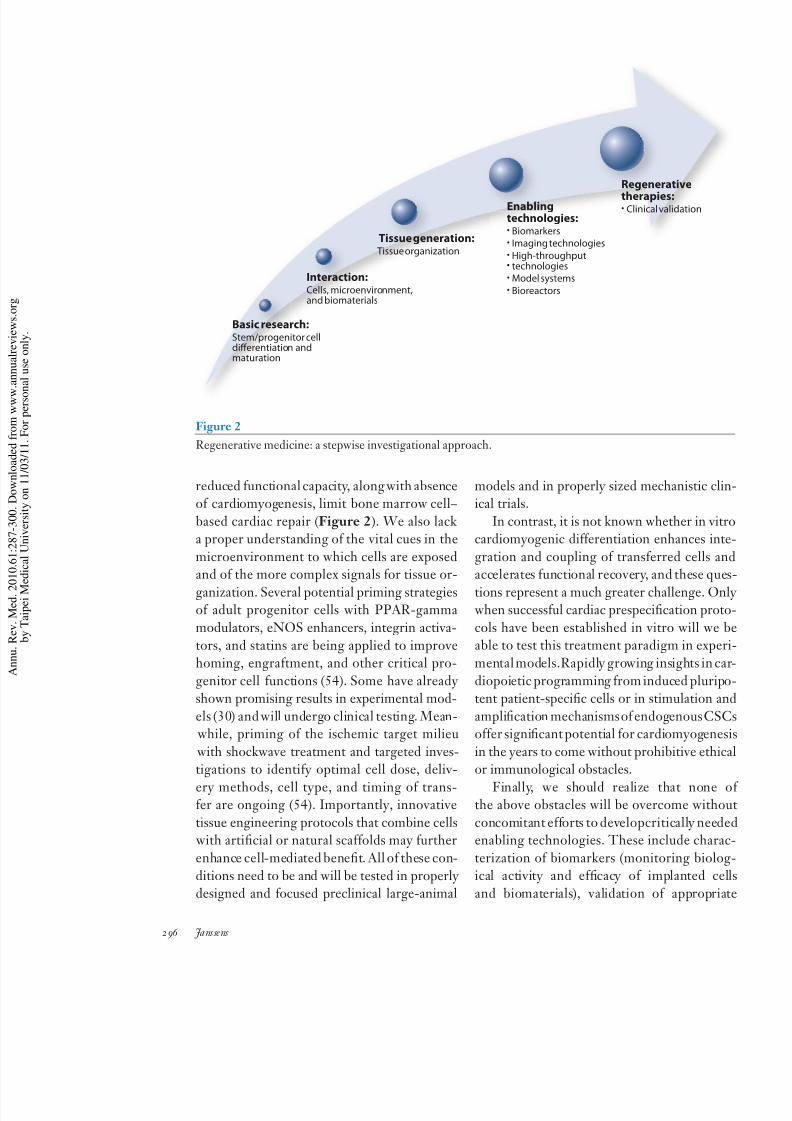
Figure 2
Regenerative medicine: a stepwise investigational approach.
reduced functional capacity, along with absenceof cardiomyogenesis, limit bone marrow cell–
based cardiac repair (Figure 2). We also lack a proper understanding of the vital cues in the
microenvironment to which cells are exposedand of the more complex signals for tissue or-
ganization. Several potential priming strategiesof adult progenitor cells with PPAR-gamma
modulators, eNOS enhancers, integrin activa-
tors, and statins are being applied to improvehoming, engraftment, and other critical pro-
genitor cell functions (54). Some have already shown promising results in experimental mod-
els (30) and will undergo clinical testing. Mean- while, priming of the ischemic target milieu
with shockwave treatment and targeted inves-tigations to identify optimal cell dose, deliv-
ery methods, cell type, and timing of trans-fer are ongoing (54). Importantly, innovative
tissue engineering protocols that combine cells with artificial or natural scaffolds may further
enhance cell-mediated benefit. All of these con-
ditions need to be and will be tested in properly designed and focused preclinical large-animal
models and in properly sized mechanistic clical trials.
In contrast, it is not known whether in vicardiomyogenic differentiation enhances in
gration and coupling of transferred cells aaccelerates functional recovery, and these qu
tions represent a much greater challenge. O when successful cardiac prespecification pro
cols have been established in vitro will weable to test this treatment paradigm in expe
mental models.Rapidly growing insights in c
diopoietic programming from induced pluritent patient-specific cells or in stimulation a
amplification mechanismsof endogenousCSoffer significant potential for cardiomyogene
in the years to come without prohibitive ethior immunological obstacles.
Finally, we should realize that none the above obstacles will be overcome with
concomitant efforts to developcritically needenabling technologies. These include char
terization of biomarkers (monitoring bioloical activity and efficacy of implanted c
and biomaterials), validation of appropri
296 Janssens

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 11/17
imaging modalities (molecular imaging tools),
high-throughput techniques (screens of small
moleculescapable of specifying andguiding dif-ferentiation processes), model systems (mim-
icking interactions between stem cells and localenvironment), and bioreactors (cell amplifica-
tion procedures under GMP conditions).
CONCLUSIONS
Many of the cell-based treatment protocolshave proven modestly effective at best. Al-
though they are interesting from the point of view of advancing a new paradigm for the treat-
ment of ischemic heart disease and heart fail-
ure, none is poised to solve the severe pub-lic health problem of advanced cardiac disease
yet. So far, most bone marrow cell transfer issafe and might constitute a valuable treatment
option for patients with large MI and signifi-cantly impaired LV function. The absolute in-
cremental increase in global function recovery following cell transfer is modest, and at least
three randomized trials failed to show signif-
icant changes in surrogate endpoints. Underthese circumstances, judicious clinical devel-
opment of cell-based cardiac repair requires
stepwise investigations of the critical limita-tions to functional recovery, as we understand
it today. At an early stage, this will best beaccomplished through collaborative studies on
cell-enhancement strategies involving expertcenters andwill benefitfrom standardized oper-
ational procedures for progenitor cell procure-ment, processing, and functional evaluation. At
the same time, cross-talk between clinicians,basic scientists, and developmental stem cell
biologists will be indispensable in this rapidly progressing field of medicine. Preclinical stud-
ies in relevant large-animal models are needed
to define our best options. It is very likely that new and better progenitor cell populations
will be identified in the near future and thatcardiac prespecification or endogenous CSC
activation will become a realistic treatmentoption.
DISCLOSURE STATEMENT
Dr. Janssens is a group leader at VIB and holds a named chair financed by AstraZeneca at
KU-Leuven, Belgium.
ACKNOWLEDGMENTS
Dr. Janssens is supported by a research grant from the Flemish Institute for Scientific Research,
FWO and the University of Leuven, Belgium (GOA).
LITERATURE CITED
1. Kajstura J, Urbanek K, Rota M, et al. 2008. Cardiac stem cells and myocardial disease. J. Mol. Cell Cardiol.
45(4):505–13
2. Leri A, Kajstura J, Anversa P, et al.2008. Myocardial regenerationand stem cell repair. Curr. Probl. Cardiol.
33(3):91–153
3. Pfeffer MA, McMurray JJ, Velazquez EJ, et al. 2003. Valsartan, captopril, or both in myocardial infarction
complicated by heart failure, left ventricular dysfunction, or both. N. Engl. J. Med. 349(20):1893–9064. Orlic D, Kajstura J, Chimenti S, et al. 2001. Bone marrow cells regenerate infarcted myocardium. Nature
410(6829):701–5
5. Quaini F, Urbanek K, Beltrami AP, et al. 2002. Chimerism of the transplanted heart. N. Engl. J. Med.
346(1):5–15
6. Deb A, Wang S, Skelding KA, et al. 2003. Bone marrow–derived cardiomyocytes are present in adult hu-
man heart: a study of gender-mismatched bone marrow transplantation patients. Circulation 107(9):1247–
49
www.annualreviews.org • Stem Cells for Myocardial Repair 297

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 12/17
8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 13/17
Intracoronary Infusion of Selected Population of Stem Cells in Acute Myocardial Infarction (REGENT)
Trial. Eur. Heart J. 30(11):1313–21
26. Piek JJ. 2008. Intracoronary infusion of mononuclear cells after primary percutaneous coronary inter-
vention: the HEBE trial. Circulation; AHA Scientific Sessions. November 10, 2008
27. Gyongyosi M, Lang I, Dettke M, et al. 2009. Combined delivery approach of bone marrow mononuclear
stem cells early and late after myocardial infarction: the MYSTAR prospective, randomized study. Nat.
Clin. Pract. Cardiovasc. Med. 6(1):70–81
28. Hirsch A, Nijveldt R, Van Der Vleuten PA, et al. 2008. Intracoronary infusion of autologous mononuclear
bone marrow cells in patients with acute myocardial infarction treated with primary PCI: pilot study of the multicenter HEBE trial. Catheter. Cardiovasc. Interv. 71(3):273–81
29. Van Der Laan A, Hirsch A, Nijveldt R, et al. 2008. Bone marrow cell therapy after acute myocardial
infarction: the HEBE trial in perspective, first results. Neth. Heart J. 16(12):436–39
30. Sasaki K, Heeschen C, Aicher A, et al. 2006. Ex vivo pretreatment of bone marrow mononuclear cells
with endothelial NO synthase enhancer AVE9488 enhances their functional activity for cell therapy. Proc.
Natl. Acad. Sci. USA 103(39):14537–41
31. Haider H, Ashraf M. 2005. Bone marrow stem cell transplantation for cardiac repair. Am. J. Physiol. Heart
Circ. Physiol. 288(6):H2557–67
32. Scherschel JA, Soonpaa MH, Srour EF, et al. 2008. Adult bone marrow-derived cells do not acquire
functional attributes of cardiomyocytes when transplanted into peri-infarct myocardium. Mol. Ther.
16(6):1129–37
33. Balsam LB, Wagers AJ, Christensen JL, et al. 2004. Haematopoietic stem cells adopt mature haematopoi-etic fates in ischaemic myocardium. Nature 428(6983):668–73
34. Murry CE, Soonpaa MH, Reinecke H, et al. 2004. Haematopoietic stem cells do not transdifferentiate
into cardiac myocytes in myocardial infarcts. Nature 428(6983):664–68
35. Murry CE, Reinecke H, Pabon LM. 2006. Regeneration gaps: observations on stem cells and cardiac
repair. J. Am. Coll. Cardiol. 47(9):1777–85
36. Wollert KC. 2008. Cell therapy for acute myocardial infarction. Curr. Opin. Pharmacol. 8(2):202–10
37. Laflamme MA, Gold J, Xu C, et al. 2005. Formation of human myocardium in the rat heart from human
embryonic stem cells. Am. J. Pathol. 167(3):663–71
38. Torella D, Ellison GM, Karakikes I, et al. 2007. Resident cardiac stem cells. Cell Mol. Life Sci. 64(6):661–73
39. Tateishi K, Ashihara E, Takehara N, et al. 2007. Clonally amplified cardiac stem cells are regulated by
Sca-1 signaling for efficient cardiovascular regeneration. J. Cell Sci. 120(Pt. 10):1791–800
40. Silva GV, Litovsky S, Assad JA, et al. 2005. Mesenchymal stem cells differentiate into an endothelialphenotype, enhance vascular density, and improve heart function in a canine chronic ischemia model.
Circulation 111(2):150–56
41. Laflamme MA, Murry CE. 2005. Regenerating the heart. Nat. Biotechnol. 23(7):845–56
42. Goodell MA, Jackson KA, Majka SM, et al. 2001. Stem cell plasticity in muscle and bone marrow. Ann.
NY Acad. Sci. 938:208–18; discussion 218–20
43. Nadal-Ginard B, Fuster V. 2007. Myocardial cell therapy at the crossroads. Nat. Clin. Pract. Cardiovasc.
Med. 4(1):1
44. Mendez-Ferrer S, Ellison GM, Torella D, et al. 2006. Resident progenitors and bone marrow stem cells
in myocardial renewal and repair. Nat. Clin. Pract. Cardiovasc. Med. 3(Suppl. 1):S83–89
45. Rota M, Padin-Iruegas ME, Misao Y, et al. 2008. Local activation or implantation of cardiac progenitor
cells rescues scarred infarcted myocardium improving cardiac function. Circ. Res. 103(1):107–16
46. Tillmanns J, Rota M, Hosoda T, et al. 2008. Formation of large coronary arteries by cardiac progenitorcells. Proc. Natl. Acad. Sci. USA 105(5):1668–73
47. Passier R, van Laake LW, Mummery CL. 2008. Stem-cell-based therapy and lessons from the heart.
Nature 453(7193):322–29
48. Rubart M, Field LJ. 2008. Stem cell differentiation: cardiac repair. Cells Tissues Organs 188(1–2):202–11
49. Sanz-Ruiz R, Fernandez-Santos E, Dominguez-Munoa M, et al. 2009. Earlytranslation of adipose-derived
cell therapy for cardiovascular disease. Cell Transplant. 18(3):245–54
50. Meliga E, Strem BM, Duckers HJ, et al. 2007. Adipose-derived cells. Cell Transplant. 16(9):963–70
www.annualreviews.org • Stem Cells for Myocardial Repair 299

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 14/17
51. Assmus B, Honold J, Schachinger V, et al. 2006. Transcoronary transplantation of progenitor cells a
myocardial infarction. N. Engl. J. Med. 355(12):1222–32
52. Menasche P, Alfieri O, Janssens S, et al. 2008. The Myoblast Autologous Grafting in Ischemic Cardiom
opathy (MAGIC) trial: first randomized placebo-controlled study of myoblast transplantation. Circula
117(9):1189–200
53. Hofmann M, Wollert KC, Meyer GP, et al. 2005. Monitoring of bone marrow cell homing into
infarcted human myocardium. Circulation 111(17):2198–202
54. Dimmeler S, Burchfield J, Zeiher AM. 2008. Cell-based therapy of myocardial infarction. Arteriosc
Thromb. Vasc. Biol. 28(2):208–1655. Bu L, Jiang X, Martin-Puig S, et al. 2009. Human ISL1 heart progenitors generate diverse multipot
cardiovascular cell lineages. Nature 460:113–17
300 Janssens

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 15/17
Annual Review
Medicine
Volume 61, 201Contents
Using Genetic Diagnosis to Determine Individual
Therapeutic Utility
C. Thomas Caskey p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 1
Emotion Recollected in Tranquility: Lessons Learned
from the COX-2 Saga
Tilo Grosser, Ying Yu, and Garret A. FitzGerald p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
17Progressive Multifocal Leukoencephalopathy in Patients on
Immunomodulatory Therapies
Eugene O. Major p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 35
The Future of Antiplatelet Therapy in Cardiovascular Disease
Carlo Patrono and Bianca Rocca p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 49
Pharmacogenetics of Warfarin
Farhad Kamali and Hilary Wynne p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 63
Heparin-Induced ThrombocytopeniaGowthami M. Arepally and Thomas L. Ortel p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 77
Regulation of Phosphate Homeostasis by PTH, Vitamin D, and FGF23
Clemens Bergwitz and Harald J¨ uppner p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 91
Alveolar Surfactant Homeostasis and the Pathogenesis of Pulmonary
Disease
Jeffrey A. Whitsett, Susan E. Wert, and Timothy E. Weaver p p p p p p p p p p p p p p p p p p p p p p p p p p p p 105
Diagnosis and Treatment of Neuropsychiatric Disorders
Katherine H. Taber, Robin A. Hurley, and Stuart C. Yudofsky p p p p p p p p p p p p p p p p p p p p p p p p p p p 121
Toward an Antibody-Based HIV-1 Vaccine
James A. Hoxie p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 135
HIV-1 Vaccine Development After STEP
Dan H. Barouch and Bette Korber p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 153
Growing Up with HIV: Children, Adolescents, and Young Adults with
Perinatally Acquired HIV Infection
Rohan Hazra, George K. Siberry, and Lynne M. Mofenson p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 169
v

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 16/17
H5N1 Avian Influenza: Preventive and Therapeutic Strategies
Against a Pandemic
Suryaprakash Sambhara and Gregory A. Poland p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
Revascularization for Coronary Artery Disease: Stents Versus Bypass
Surgery
Spencer B. King III, John Jeffrey Marshall, and Pradyumna E. Tummalap p p p p p p p p p
Controversies in the Use of Drug-Eluting Stents for Acute Myocardial
Infarction: A Critical Appraisal of the Data
Rahul Sakhuja and Laura Mauri p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
Arrythmogenic Cardiomyopathy: Etiology, Diagnosis, and Treatment
Srijita Sen-Chowdhry, Robert D. Morgan, John C. Chambers,
and William J. McKenna p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
Contemporary Use of Ventricular Assist Devices
Cesare M. Terracciano, Leslie W. Miller, and Magdi H. Yacoub p p p p p p p p p p p p p p p p p p p p p p p
Stress Cardiomyopathy
Yoshihiro J. Akashi, Holger M. Nef, Helge M¨ ollmann, and Takashi Ueyama p p p p p p p p
Stem Cells in the Treatment of Heart Disease
Stefan Janssens p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
Biological Mechanisms Linking Obesity and Cancer Risk:
New Perspectives
Darren L. Roberts, Caroline Dive, and Andrew G. Renehan p p p p p p p p p p p p p p p p p p p p p p p p p p
Hepatocellular Carcinoma: Novel Molecular Approaches for
Diagnosis, Prognosis, and Therapy Augusto Villanueva, Beatriz Minguez, Alejandro Forner, Maria Reig,
and Josep M. Llovet p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
Molecular Diagnosis and Therapy of Kidney Cancer
W. Marston Linehan, Gennady Bratslavsky, Peter A. Pinto, Laura S. Schmidt,
Len Neckers, Donald P. Bottaro, and Ramaprasad Srinivasan p p p p p p p p p p p p p p p p p p p p p p p
Myelodysplastic Syndromes
Bart L. Scott and H. Joachim Deeg p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
Nanotechnology Applications in Surgical Oncology
Sunil Singhal, Shuming Nie, and May D. Wang p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
Emerging Molecular Targets for the Treatment of Nonalcoholic Fatty
Liver Disease
Giovanni Musso, Roberto Gambino, and Maurizio Cassader p p p p p p p p p p p p p p p p p p p p p p p p p p
Metabolic Surgery to Treat Type 2 Diabetes: Clinical Outcomes
and Mechanisms of Action
Francesco Rubino, Philip R. Schauer, Lee M. Kaplan, and David E. Cummings p p p p p
v i C on te nt s

8/3/2019 Annu. Rev. Med. 2010, 61, 287–300
http://slidepdf.com/reader/full/annu-rev-med-2010-61-287300 17/17
Genetic Aspects of Pancreatitis
David C. Whitcomb p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 413
Anorexia Nervosa: Current Status and Future Directions
Evelyn Attia p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 425
Structural Variation in the Human Genome and its Role in Disease
Pawel Stankiewicz and James R. Lupski p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p
437
Surgical Innovations Arising from the Iraq and Afghanistan Wars
Geoffrey S.F. Ling, Peter Rhee, and James M. Ecklund p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 457
Medicare Part D: Ongoing Challenges for Doctors and Patients
Gretchen Jacobson and Gerard Anderson p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 469
Indexes
Cumulative Index of Contributing Authors, Volumes 57–61 p p p p p p p p p p p p p p p p p p p p p p p p p p p 477
Cumulative Index of Chapter Titles, Volumes 57–61 p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p p 481
Errata
An online log of corrections to Annual Review of Medicine articles may be found at
http://med.annualreviews.org/errata.shtml