Embed Size (px)
Citation preview

G-CSF ET PROPHYLAXIE DES NEUTROPENIES CHIMIO-INDUITES ETAT DES LIEUX ET RECOMMANDATIONS Prof G FREYER MD PhD Oncologie Meacutedicale CH Lyon-Sud et Universiteacute Lyon 1
Cours DES Monaco 2016
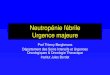
Taux de mortaliteacute chez les patients atteints drsquoun cancer et hospitaliseacutes avec NF
95
Dureacutee moyenne drsquohospitalisation de patients atteints drsquoun cancer et
hospitaliseacutes avec NF
115 jours
Neutropeacutenie feacutebrile et pronostic vital
Kuderer et al Cancer 2006
RISQUE DE MORTALITE PREacuteCOCE et NEUTROPENIE FEBRILE (NF)
Lyman GH et al Cancer 20101165555-5563
Kaplan-Meier curve for early mortality S
urv
iva
l p
rob
ab
ilit
y
Follow-up (months)
0
Log-rank test Chi2(1)=1487 p=00001
Non-FN patients 100
FN patients
1 2 3 4 5 6 7 8 9 10 11 12
095
090
085
Number at risk Non-FN patients 5990 5195 4799 3898 3132 2041 1154 678 357 262 199 146 130
FN patients 5990 5761 5470 4769 3883 2646 1607 1073 663 487 398 325 275
ldquoAU SIEgraveCLE DERNIERrdquo ANNEacuteES 90 GSF(Filgrastim) Decreased the Depth and Duration of Neutropenia
CRITEgraveRE DrsquoENREGISTREMENT
Study day
001
01
05
10
100
1000
0 4 8 12 16 20 24
Start filgrastim
placebo
Placebo (n = 110)
Filgrastim (n = 101)
AN
C ( 1
09L
)
Crawford J et al N Engl J Med 1991325164-170
Median ANC during cycle one
CAE chemotherapy in small-cell lung cancer
Severe neutropenia (ANC 05 x 109L)
CAE = cyclophosphamide
doxorubicinetoposide
0
20
40
60
FN cycle one FN cycle one
Pati
en
ts (
)
1Crawford J et al N Engl J Med 1991325164-170 2Trillet-Lenoir V et al Eur J Cancer 199329A319-324
P lt 00011
P lt 00122
IMPACT DIRECT SUR LA NEUTROPEacuteNIE FEacuteBRILE
Filgrastim Decreased the Incidence of FN
(10 Agrave 13 INJECTIONS EN MOYENNE )
Placebo
Filgrastim
AMM POUR LES PROTOCOLES AVEC RISQUE DE NF gt 40
Etude Pathologie Bras de traitement Neutropeacutenie
Feacutebrile
Hospitalisation
Anti-infectieux
Vogel
n=928
Sein adjuvant
et
meacutetastatique
Doceacutetaxel 3s +
Neulasta
Vs
Doceacutetaxel 3s +
placebo
1
17
1 - 2
14 - 10
Timmer Bonte
n=186
CBPC CDE + ATB prophy
+ G-CSF
Vs
CDE + ATB prophy
18
32
p = 001
CDE Doxorubicine 45 mgm2 + Cyclophosphamide 1000 mgm2 + Etoposide 100 mgm2
Antibioprophylaxie ciprofloxacine + roxithromycine (J4 agrave J13)
G-CSF J4 agrave J13
2005-2006 RISQUE DE NF INTERMEacuteDIAIRE ( 20)
G-CSF et prophylaxie primaire
Vogel CL Wojtukiewicz MZ Carroll RR et al First and subsequent cycle use of pegfilgrastim prevents febrile neutropenia in patients with breast cancer a multicenter double-blind placebo-controlled phase III study J Clin Oncol 200523(6)1178-1184
Timmer-Bonte JN and all Prevention of chemotherapy-induced febrile neutropenia by prophylactic antibiotics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer a dutch randomized phase III study J Clin Oncol 2005237974-7984s
p lt 0001
Recommandations de lrsquoASCO et de lrsquoEORTC
pour lrsquoeacutevaluation de la NF
G-CSF NON
RECOMMANDE
PREVENTION
PAR G-CSF
RECOMMANDEE
Risque de NF ge 20
Risque global de NF ge 20 Risque global de NF lt 20
bull Pour chaque patient le risque de NF doit ecirctre eacutevalueacute en routine avant chaque cycle de chimiotheacuterapie
bull Les protocoles de chimiotheacuterapie dose-denses doivent ecirctre toujours consideacutereacutes comme agrave risque eacuteleveacute de NF (risque de NF ge 20)1
bull Les patients gt 65 ans atteints de LNH et traiteacutes par une chimiotheacuterapie curative doivent ecirctre consideacutereacutes comme agrave risque eacuteleveacute de NF2
ETAPE 1 eacutevaluer le risque de NF associeacute au protocole preacutevu de chimiotheacuterapie
bull Heacutemoglobine lt 12 gdl1
bull Carence nutritionnelle12
bull Chimio-radiotheacuterapie combineacutee2
bull Anteacuteceacutedent de NF12
bull Plaies ouvertes ou infections eacutevolutives2
bull Pas drsquoantibioprophylaxie
bull Acircge ge 65 ans12
bull Mauvais indice fonctionnel12
bull Maladie avanceacutee12
bull Comorbiditeacutes graves2
bull Cytopeacutenies dues agrave lrsquoenvahissement meacutedullaire par la tumeur2
bull Sexe feacuteminin1
ETAPE 2 eacutevaluer les facteurs augmentant le risque de
NF
Risque de NF entre 10 et 20 Risque de NF lt 10
Cet arbre deacutecisionnel est constitueacute par la synthegravese des recommandations 2006 de lrsquoEORTC et de lrsquoASCO
1Aapro MS et al Eur J Cancer 2006422433ndash2453 2Smith TJ et al J Clin Oncol 2006243187ndash3205
Les facteurs de risque souligneacutes correspondent agrave un niveau de
preuve III drsquoapregraves lrsquoEORTC
Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Taux de mortaliteacute chez les patients atteints drsquoun cancer et hospitaliseacutes avec NF
95
Dureacutee moyenne drsquohospitalisation de patients atteints drsquoun cancer et
hospitaliseacutes avec NF
115 jours
Neutropeacutenie feacutebrile et pronostic vital
Kuderer et al Cancer 2006
RISQUE DE MORTALITE PREacuteCOCE et NEUTROPENIE FEBRILE (NF)
Lyman GH et al Cancer 20101165555-5563
Kaplan-Meier curve for early mortality S
urv
iva
l p
rob
ab
ilit
y
Follow-up (months)
0
Log-rank test Chi2(1)=1487 p=00001
Non-FN patients 100
FN patients
1 2 3 4 5 6 7 8 9 10 11 12
095
090
085
Number at risk Non-FN patients 5990 5195 4799 3898 3132 2041 1154 678 357 262 199 146 130
FN patients 5990 5761 5470 4769 3883 2646 1607 1073 663 487 398 325 275
ldquoAU SIEgraveCLE DERNIERrdquo ANNEacuteES 90 GSF(Filgrastim) Decreased the Depth and Duration of Neutropenia
CRITEgraveRE DrsquoENREGISTREMENT
Study day
001
01
05
10
100
1000
0 4 8 12 16 20 24
Start filgrastim
placebo
Placebo (n = 110)
Filgrastim (n = 101)
AN
C ( 1
09L
)
Crawford J et al N Engl J Med 1991325164-170
Median ANC during cycle one
CAE chemotherapy in small-cell lung cancer
Severe neutropenia (ANC 05 x 109L)
CAE = cyclophosphamide
doxorubicinetoposide
0
20
40
60
FN cycle one FN cycle one
Pati
en
ts (
)
1Crawford J et al N Engl J Med 1991325164-170 2Trillet-Lenoir V et al Eur J Cancer 199329A319-324
P lt 00011
P lt 00122
IMPACT DIRECT SUR LA NEUTROPEacuteNIE FEacuteBRILE
Filgrastim Decreased the Incidence of FN
(10 Agrave 13 INJECTIONS EN MOYENNE )
Placebo
Filgrastim
AMM POUR LES PROTOCOLES AVEC RISQUE DE NF gt 40
Etude Pathologie Bras de traitement Neutropeacutenie
Feacutebrile
Hospitalisation
Anti-infectieux
Vogel
n=928
Sein adjuvant
et
meacutetastatique
Doceacutetaxel 3s +
Neulasta
Vs
Doceacutetaxel 3s +
placebo
1
17
1 - 2
14 - 10
Timmer Bonte
n=186
CBPC CDE + ATB prophy
+ G-CSF
Vs
CDE + ATB prophy
18
32
p = 001
CDE Doxorubicine 45 mgm2 + Cyclophosphamide 1000 mgm2 + Etoposide 100 mgm2
Antibioprophylaxie ciprofloxacine + roxithromycine (J4 agrave J13)
G-CSF J4 agrave J13
2005-2006 RISQUE DE NF INTERMEacuteDIAIRE ( 20)
G-CSF et prophylaxie primaire
Vogel CL Wojtukiewicz MZ Carroll RR et al First and subsequent cycle use of pegfilgrastim prevents febrile neutropenia in patients with breast cancer a multicenter double-blind placebo-controlled phase III study J Clin Oncol 200523(6)1178-1184
Timmer-Bonte JN and all Prevention of chemotherapy-induced febrile neutropenia by prophylactic antibiotics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer a dutch randomized phase III study J Clin Oncol 2005237974-7984s
p lt 0001
Recommandations de lrsquoASCO et de lrsquoEORTC
pour lrsquoeacutevaluation de la NF
G-CSF NON
RECOMMANDE
PREVENTION
PAR G-CSF
RECOMMANDEE
Risque de NF ge 20
Risque global de NF ge 20 Risque global de NF lt 20
bull Pour chaque patient le risque de NF doit ecirctre eacutevalueacute en routine avant chaque cycle de chimiotheacuterapie
bull Les protocoles de chimiotheacuterapie dose-denses doivent ecirctre toujours consideacutereacutes comme agrave risque eacuteleveacute de NF (risque de NF ge 20)1
bull Les patients gt 65 ans atteints de LNH et traiteacutes par une chimiotheacuterapie curative doivent ecirctre consideacutereacutes comme agrave risque eacuteleveacute de NF2
ETAPE 1 eacutevaluer le risque de NF associeacute au protocole preacutevu de chimiotheacuterapie
bull Heacutemoglobine lt 12 gdl1
bull Carence nutritionnelle12
bull Chimio-radiotheacuterapie combineacutee2
bull Anteacuteceacutedent de NF12
bull Plaies ouvertes ou infections eacutevolutives2
bull Pas drsquoantibioprophylaxie
bull Acircge ge 65 ans12
bull Mauvais indice fonctionnel12
bull Maladie avanceacutee12
bull Comorbiditeacutes graves2
bull Cytopeacutenies dues agrave lrsquoenvahissement meacutedullaire par la tumeur2
bull Sexe feacuteminin1
ETAPE 2 eacutevaluer les facteurs augmentant le risque de
NF
Risque de NF entre 10 et 20 Risque de NF lt 10
Cet arbre deacutecisionnel est constitueacute par la synthegravese des recommandations 2006 de lrsquoEORTC et de lrsquoASCO
1Aapro MS et al Eur J Cancer 2006422433ndash2453 2Smith TJ et al J Clin Oncol 2006243187ndash3205
Les facteurs de risque souligneacutes correspondent agrave un niveau de
preuve III drsquoapregraves lrsquoEORTC
Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

RISQUE DE MORTALITE PREacuteCOCE et NEUTROPENIE FEBRILE (NF)
Lyman GH et al Cancer 20101165555-5563
Kaplan-Meier curve for early mortality S
urv
iva
l p
rob
ab
ilit
y
Follow-up (months)
0
Log-rank test Chi2(1)=1487 p=00001
Non-FN patients 100
FN patients
1 2 3 4 5 6 7 8 9 10 11 12
095
090
085
Number at risk Non-FN patients 5990 5195 4799 3898 3132 2041 1154 678 357 262 199 146 130
FN patients 5990 5761 5470 4769 3883 2646 1607 1073 663 487 398 325 275
ldquoAU SIEgraveCLE DERNIERrdquo ANNEacuteES 90 GSF(Filgrastim) Decreased the Depth and Duration of Neutropenia
CRITEgraveRE DrsquoENREGISTREMENT
Study day
001
01
05
10
100
1000
0 4 8 12 16 20 24
Start filgrastim
placebo
Placebo (n = 110)
Filgrastim (n = 101)
AN
C ( 1
09L
)
Crawford J et al N Engl J Med 1991325164-170
Median ANC during cycle one
CAE chemotherapy in small-cell lung cancer
Severe neutropenia (ANC 05 x 109L)
CAE = cyclophosphamide
doxorubicinetoposide
0
20
40
60
FN cycle one FN cycle one
Pati
en
ts (
)
1Crawford J et al N Engl J Med 1991325164-170 2Trillet-Lenoir V et al Eur J Cancer 199329A319-324
P lt 00011
P lt 00122
IMPACT DIRECT SUR LA NEUTROPEacuteNIE FEacuteBRILE
Filgrastim Decreased the Incidence of FN
(10 Agrave 13 INJECTIONS EN MOYENNE )
Placebo
Filgrastim
AMM POUR LES PROTOCOLES AVEC RISQUE DE NF gt 40
Etude Pathologie Bras de traitement Neutropeacutenie
Feacutebrile
Hospitalisation
Anti-infectieux
Vogel
n=928
Sein adjuvant
et
meacutetastatique
Doceacutetaxel 3s +
Neulasta
Vs
Doceacutetaxel 3s +
placebo
1
17
1 - 2
14 - 10
Timmer Bonte
n=186
CBPC CDE + ATB prophy
+ G-CSF
Vs
CDE + ATB prophy
18
32
p = 001
CDE Doxorubicine 45 mgm2 + Cyclophosphamide 1000 mgm2 + Etoposide 100 mgm2
Antibioprophylaxie ciprofloxacine + roxithromycine (J4 agrave J13)
G-CSF J4 agrave J13
2005-2006 RISQUE DE NF INTERMEacuteDIAIRE ( 20)
G-CSF et prophylaxie primaire
Vogel CL Wojtukiewicz MZ Carroll RR et al First and subsequent cycle use of pegfilgrastim prevents febrile neutropenia in patients with breast cancer a multicenter double-blind placebo-controlled phase III study J Clin Oncol 200523(6)1178-1184
Timmer-Bonte JN and all Prevention of chemotherapy-induced febrile neutropenia by prophylactic antibiotics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer a dutch randomized phase III study J Clin Oncol 2005237974-7984s
p lt 0001
Recommandations de lrsquoASCO et de lrsquoEORTC
pour lrsquoeacutevaluation de la NF
G-CSF NON
RECOMMANDE
PREVENTION
PAR G-CSF
RECOMMANDEE
Risque de NF ge 20
Risque global de NF ge 20 Risque global de NF lt 20
bull Pour chaque patient le risque de NF doit ecirctre eacutevalueacute en routine avant chaque cycle de chimiotheacuterapie
bull Les protocoles de chimiotheacuterapie dose-denses doivent ecirctre toujours consideacutereacutes comme agrave risque eacuteleveacute de NF (risque de NF ge 20)1
bull Les patients gt 65 ans atteints de LNH et traiteacutes par une chimiotheacuterapie curative doivent ecirctre consideacutereacutes comme agrave risque eacuteleveacute de NF2
ETAPE 1 eacutevaluer le risque de NF associeacute au protocole preacutevu de chimiotheacuterapie
bull Heacutemoglobine lt 12 gdl1
bull Carence nutritionnelle12
bull Chimio-radiotheacuterapie combineacutee2
bull Anteacuteceacutedent de NF12
bull Plaies ouvertes ou infections eacutevolutives2
bull Pas drsquoantibioprophylaxie
bull Acircge ge 65 ans12
bull Mauvais indice fonctionnel12
bull Maladie avanceacutee12
bull Comorbiditeacutes graves2
bull Cytopeacutenies dues agrave lrsquoenvahissement meacutedullaire par la tumeur2
bull Sexe feacuteminin1
ETAPE 2 eacutevaluer les facteurs augmentant le risque de
NF
Risque de NF entre 10 et 20 Risque de NF lt 10
Cet arbre deacutecisionnel est constitueacute par la synthegravese des recommandations 2006 de lrsquoEORTC et de lrsquoASCO
1Aapro MS et al Eur J Cancer 2006422433ndash2453 2Smith TJ et al J Clin Oncol 2006243187ndash3205
Les facteurs de risque souligneacutes correspondent agrave un niveau de
preuve III drsquoapregraves lrsquoEORTC
Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

ldquoAU SIEgraveCLE DERNIERrdquo ANNEacuteES 90 GSF(Filgrastim) Decreased the Depth and Duration of Neutropenia
CRITEgraveRE DrsquoENREGISTREMENT
Study day
001
01
05
10
100
1000
0 4 8 12 16 20 24
Start filgrastim
placebo
Placebo (n = 110)
Filgrastim (n = 101)
AN
C ( 1
09L
)
Crawford J et al N Engl J Med 1991325164-170
Median ANC during cycle one
CAE chemotherapy in small-cell lung cancer
Severe neutropenia (ANC 05 x 109L)
CAE = cyclophosphamide
doxorubicinetoposide
0
20
40
60
FN cycle one FN cycle one
Pati
en
ts (
)
1Crawford J et al N Engl J Med 1991325164-170 2Trillet-Lenoir V et al Eur J Cancer 199329A319-324
P lt 00011
P lt 00122
IMPACT DIRECT SUR LA NEUTROPEacuteNIE FEacuteBRILE
Filgrastim Decreased the Incidence of FN
(10 Agrave 13 INJECTIONS EN MOYENNE )
Placebo
Filgrastim
AMM POUR LES PROTOCOLES AVEC RISQUE DE NF gt 40
Etude Pathologie Bras de traitement Neutropeacutenie
Feacutebrile
Hospitalisation
Anti-infectieux
Vogel
n=928
Sein adjuvant
et
meacutetastatique
Doceacutetaxel 3s +
Neulasta
Vs
Doceacutetaxel 3s +
placebo
1
17
1 - 2
14 - 10
Timmer Bonte
n=186
CBPC CDE + ATB prophy
+ G-CSF
Vs
CDE + ATB prophy
18
32
p = 001
CDE Doxorubicine 45 mgm2 + Cyclophosphamide 1000 mgm2 + Etoposide 100 mgm2
Antibioprophylaxie ciprofloxacine + roxithromycine (J4 agrave J13)
G-CSF J4 agrave J13
2005-2006 RISQUE DE NF INTERMEacuteDIAIRE ( 20)
G-CSF et prophylaxie primaire
Vogel CL Wojtukiewicz MZ Carroll RR et al First and subsequent cycle use of pegfilgrastim prevents febrile neutropenia in patients with breast cancer a multicenter double-blind placebo-controlled phase III study J Clin Oncol 200523(6)1178-1184
Timmer-Bonte JN and all Prevention of chemotherapy-induced febrile neutropenia by prophylactic antibiotics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer a dutch randomized phase III study J Clin Oncol 2005237974-7984s
p lt 0001
Recommandations de lrsquoASCO et de lrsquoEORTC
pour lrsquoeacutevaluation de la NF
G-CSF NON
RECOMMANDE
PREVENTION
PAR G-CSF
RECOMMANDEE
Risque de NF ge 20
Risque global de NF ge 20 Risque global de NF lt 20
bull Pour chaque patient le risque de NF doit ecirctre eacutevalueacute en routine avant chaque cycle de chimiotheacuterapie
bull Les protocoles de chimiotheacuterapie dose-denses doivent ecirctre toujours consideacutereacutes comme agrave risque eacuteleveacute de NF (risque de NF ge 20)1
bull Les patients gt 65 ans atteints de LNH et traiteacutes par une chimiotheacuterapie curative doivent ecirctre consideacutereacutes comme agrave risque eacuteleveacute de NF2
ETAPE 1 eacutevaluer le risque de NF associeacute au protocole preacutevu de chimiotheacuterapie
bull Heacutemoglobine lt 12 gdl1
bull Carence nutritionnelle12
bull Chimio-radiotheacuterapie combineacutee2
bull Anteacuteceacutedent de NF12
bull Plaies ouvertes ou infections eacutevolutives2
bull Pas drsquoantibioprophylaxie
bull Acircge ge 65 ans12
bull Mauvais indice fonctionnel12
bull Maladie avanceacutee12
bull Comorbiditeacutes graves2
bull Cytopeacutenies dues agrave lrsquoenvahissement meacutedullaire par la tumeur2
bull Sexe feacuteminin1
ETAPE 2 eacutevaluer les facteurs augmentant le risque de
NF
Risque de NF entre 10 et 20 Risque de NF lt 10
Cet arbre deacutecisionnel est constitueacute par la synthegravese des recommandations 2006 de lrsquoEORTC et de lrsquoASCO
1Aapro MS et al Eur J Cancer 2006422433ndash2453 2Smith TJ et al J Clin Oncol 2006243187ndash3205
Les facteurs de risque souligneacutes correspondent agrave un niveau de
preuve III drsquoapregraves lrsquoEORTC
Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

0
20
40
60
FN cycle one FN cycle one
Pati
en
ts (
)
1Crawford J et al N Engl J Med 1991325164-170 2Trillet-Lenoir V et al Eur J Cancer 199329A319-324
P lt 00011
P lt 00122
IMPACT DIRECT SUR LA NEUTROPEacuteNIE FEacuteBRILE
Filgrastim Decreased the Incidence of FN
(10 Agrave 13 INJECTIONS EN MOYENNE )
Placebo
Filgrastim
AMM POUR LES PROTOCOLES AVEC RISQUE DE NF gt 40
Etude Pathologie Bras de traitement Neutropeacutenie
Feacutebrile
Hospitalisation
Anti-infectieux
Vogel
n=928
Sein adjuvant
et
meacutetastatique
Doceacutetaxel 3s +
Neulasta
Vs
Doceacutetaxel 3s +
placebo
1
17
1 - 2
14 - 10
Timmer Bonte
n=186
CBPC CDE + ATB prophy
+ G-CSF
Vs
CDE + ATB prophy
18
32
p = 001
CDE Doxorubicine 45 mgm2 + Cyclophosphamide 1000 mgm2 + Etoposide 100 mgm2
Antibioprophylaxie ciprofloxacine + roxithromycine (J4 agrave J13)
G-CSF J4 agrave J13
2005-2006 RISQUE DE NF INTERMEacuteDIAIRE ( 20)
G-CSF et prophylaxie primaire
Vogel CL Wojtukiewicz MZ Carroll RR et al First and subsequent cycle use of pegfilgrastim prevents febrile neutropenia in patients with breast cancer a multicenter double-blind placebo-controlled phase III study J Clin Oncol 200523(6)1178-1184
Timmer-Bonte JN and all Prevention of chemotherapy-induced febrile neutropenia by prophylactic antibiotics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer a dutch randomized phase III study J Clin Oncol 2005237974-7984s
p lt 0001
Recommandations de lrsquoASCO et de lrsquoEORTC
pour lrsquoeacutevaluation de la NF
G-CSF NON
RECOMMANDE
PREVENTION
PAR G-CSF
RECOMMANDEE
Risque de NF ge 20
Risque global de NF ge 20 Risque global de NF lt 20
bull Pour chaque patient le risque de NF doit ecirctre eacutevalueacute en routine avant chaque cycle de chimiotheacuterapie
bull Les protocoles de chimiotheacuterapie dose-denses doivent ecirctre toujours consideacutereacutes comme agrave risque eacuteleveacute de NF (risque de NF ge 20)1
bull Les patients gt 65 ans atteints de LNH et traiteacutes par une chimiotheacuterapie curative doivent ecirctre consideacutereacutes comme agrave risque eacuteleveacute de NF2
ETAPE 1 eacutevaluer le risque de NF associeacute au protocole preacutevu de chimiotheacuterapie
bull Heacutemoglobine lt 12 gdl1
bull Carence nutritionnelle12
bull Chimio-radiotheacuterapie combineacutee2
bull Anteacuteceacutedent de NF12
bull Plaies ouvertes ou infections eacutevolutives2
bull Pas drsquoantibioprophylaxie
bull Acircge ge 65 ans12
bull Mauvais indice fonctionnel12
bull Maladie avanceacutee12
bull Comorbiditeacutes graves2
bull Cytopeacutenies dues agrave lrsquoenvahissement meacutedullaire par la tumeur2
bull Sexe feacuteminin1
ETAPE 2 eacutevaluer les facteurs augmentant le risque de
NF
Risque de NF entre 10 et 20 Risque de NF lt 10
Cet arbre deacutecisionnel est constitueacute par la synthegravese des recommandations 2006 de lrsquoEORTC et de lrsquoASCO
1Aapro MS et al Eur J Cancer 2006422433ndash2453 2Smith TJ et al J Clin Oncol 2006243187ndash3205
Les facteurs de risque souligneacutes correspondent agrave un niveau de
preuve III drsquoapregraves lrsquoEORTC
Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Etude Pathologie Bras de traitement Neutropeacutenie
Feacutebrile
Hospitalisation
Anti-infectieux
Vogel
n=928
Sein adjuvant
et
meacutetastatique
Doceacutetaxel 3s +
Neulasta
Vs
Doceacutetaxel 3s +
placebo
1
17
1 - 2
14 - 10
Timmer Bonte
n=186
CBPC CDE + ATB prophy
+ G-CSF
Vs
CDE + ATB prophy
18
32
p = 001
CDE Doxorubicine 45 mgm2 + Cyclophosphamide 1000 mgm2 + Etoposide 100 mgm2
Antibioprophylaxie ciprofloxacine + roxithromycine (J4 agrave J13)
G-CSF J4 agrave J13
2005-2006 RISQUE DE NF INTERMEacuteDIAIRE ( 20)
G-CSF et prophylaxie primaire
Vogel CL Wojtukiewicz MZ Carroll RR et al First and subsequent cycle use of pegfilgrastim prevents febrile neutropenia in patients with breast cancer a multicenter double-blind placebo-controlled phase III study J Clin Oncol 200523(6)1178-1184
Timmer-Bonte JN and all Prevention of chemotherapy-induced febrile neutropenia by prophylactic antibiotics plus or minus granulocyte colony-stimulating factor in small-cell lung cancer a dutch randomized phase III study J Clin Oncol 2005237974-7984s
p lt 0001
Recommandations de lrsquoASCO et de lrsquoEORTC
pour lrsquoeacutevaluation de la NF
G-CSF NON
RECOMMANDE
PREVENTION
PAR G-CSF
RECOMMANDEE
Risque de NF ge 20
Risque global de NF ge 20 Risque global de NF lt 20
bull Pour chaque patient le risque de NF doit ecirctre eacutevalueacute en routine avant chaque cycle de chimiotheacuterapie
bull Les protocoles de chimiotheacuterapie dose-denses doivent ecirctre toujours consideacutereacutes comme agrave risque eacuteleveacute de NF (risque de NF ge 20)1
bull Les patients gt 65 ans atteints de LNH et traiteacutes par une chimiotheacuterapie curative doivent ecirctre consideacutereacutes comme agrave risque eacuteleveacute de NF2
ETAPE 1 eacutevaluer le risque de NF associeacute au protocole preacutevu de chimiotheacuterapie
bull Heacutemoglobine lt 12 gdl1
bull Carence nutritionnelle12
bull Chimio-radiotheacuterapie combineacutee2
bull Anteacuteceacutedent de NF12
bull Plaies ouvertes ou infections eacutevolutives2
bull Pas drsquoantibioprophylaxie
bull Acircge ge 65 ans12
bull Mauvais indice fonctionnel12
bull Maladie avanceacutee12
bull Comorbiditeacutes graves2
bull Cytopeacutenies dues agrave lrsquoenvahissement meacutedullaire par la tumeur2
bull Sexe feacuteminin1
ETAPE 2 eacutevaluer les facteurs augmentant le risque de
NF
Risque de NF entre 10 et 20 Risque de NF lt 10
Cet arbre deacutecisionnel est constitueacute par la synthegravese des recommandations 2006 de lrsquoEORTC et de lrsquoASCO
1Aapro MS et al Eur J Cancer 2006422433ndash2453 2Smith TJ et al J Clin Oncol 2006243187ndash3205
Les facteurs de risque souligneacutes correspondent agrave un niveau de
preuve III drsquoapregraves lrsquoEORTC
Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Recommandations de lrsquoASCO et de lrsquoEORTC
pour lrsquoeacutevaluation de la NF
G-CSF NON
RECOMMANDE
PREVENTION
PAR G-CSF
RECOMMANDEE
Risque de NF ge 20
Risque global de NF ge 20 Risque global de NF lt 20
bull Pour chaque patient le risque de NF doit ecirctre eacutevalueacute en routine avant chaque cycle de chimiotheacuterapie
bull Les protocoles de chimiotheacuterapie dose-denses doivent ecirctre toujours consideacutereacutes comme agrave risque eacuteleveacute de NF (risque de NF ge 20)1
bull Les patients gt 65 ans atteints de LNH et traiteacutes par une chimiotheacuterapie curative doivent ecirctre consideacutereacutes comme agrave risque eacuteleveacute de NF2
ETAPE 1 eacutevaluer le risque de NF associeacute au protocole preacutevu de chimiotheacuterapie
bull Heacutemoglobine lt 12 gdl1
bull Carence nutritionnelle12
bull Chimio-radiotheacuterapie combineacutee2
bull Anteacuteceacutedent de NF12
bull Plaies ouvertes ou infections eacutevolutives2
bull Pas drsquoantibioprophylaxie
bull Acircge ge 65 ans12
bull Mauvais indice fonctionnel12
bull Maladie avanceacutee12
bull Comorbiditeacutes graves2
bull Cytopeacutenies dues agrave lrsquoenvahissement meacutedullaire par la tumeur2
bull Sexe feacuteminin1
ETAPE 2 eacutevaluer les facteurs augmentant le risque de
NF
Risque de NF entre 10 et 20 Risque de NF lt 10
Cet arbre deacutecisionnel est constitueacute par la synthegravese des recommandations 2006 de lrsquoEORTC et de lrsquoASCO
1Aapro MS et al Eur J Cancer 2006422433ndash2453 2Smith TJ et al J Clin Oncol 2006243187ndash3205
Les facteurs de risque souligneacutes correspondent agrave un niveau de
preuve III drsquoapregraves lrsquoEORTC
Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Reacutesultats
Avec les G-CSF une reacuteduction significative de 46 du risque de NF
Etude Kuderer
JCO 2007 17 essais controcircleacutes 3493 patients
Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Preacutevention de la neutropeacutenie feacutebrile et de ses complications valideacutee en oncologie dans les chimiotheacuterapies fortement neutropeacuteniantes(12)
DEacuteBUT DES ANNEacuteES 2000
PELFIGRASTIM VS G-CSF QUOTIDIENS
(1) Holmes FA et al Blinded randomized multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily
filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage IIIIV breast cancer J Clin Oncol 200220(3)727-31
(2) Green MD et al A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily
filgrastim in patients receiving myelosuppressive chemotherapy Ann Oncol 200314(1)29-35
(
Critegravere principal Reacuteduction comparable de la dureacutee de la
neutropeacutenie seacutevegravere au cycle 1 (12)
Critegraveres secondaires
Reacuteduction comparable de lrsquoincidence de NF sur lrsquoensemble des cycles (12)
NS non significatif
NR diffeacuterence statistique non rapporteacutee
Nombre de patients eacuteligibles sur les critegraveres de lrsquoefficaciteacute
2 eacutetudes de phase III multicentriques randomiseacutees en double aveugle de non infeacuterioriteacute
Objectifs des eacutetudes comparer lrsquoefficaciteacute et la toleacuterance drsquoune dose unique de Neulastareg cycle de chimiotheacuterapie (dose fixe de 6 mg(2) ou dose variable de 100 microgkg(1)) agrave des injections quotidiennes de G-CSF (filgrastim 5 microgkgj)
Patientes atteintes drsquoun cancer du sein reacuteparties en 2 groupes et recevant
- Etude Holmes(1) (n=310) Neulastareg (100 microgkg) (n=154) ou injections quotidiennes de G-CSF (5microgkg) (n=156)
- Etude Green(2) (n=157) Neulastareg (6 mg ) (n=80) ou injections quotidiennes de G-CSF (5microgkg) (n=77)
Etudes Holmes(1) et Green(2)
- Etude Holmes 17 jour avec Neulastareg versus 18 jour avec
filgrastim (diffeacuterence des moyennes 003 j)
- Etude Green 18 jour avec Neulastareg versus 16 jour avec
filgrastim (diffeacuterence des moyennes 023 j)
Reacuteduction des taux drsquohospitalisation et drsquoadministration drsquoantibiotiques en IV (2)
La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

La stimulation preacutecoce par G-CSF au plus tard agrave J3 tels que recommandeacutee
par lrsquoASCO permet une reacuteduction consideacuterable du taux de survenue des
neutropeacutenies feacutebriles
bull Lacy CF et al Drug Information Handbook Hudson OH Lexi-Comp Inc 2001
bull Koumakis et al Oncology 1999 56 28-35
Chimio Nadir constateacute Retour au seuil de NS
Vincristine
Cyclophosphamide
Cisplatin
Docetaxel
Doxorubicin
Paclitaxel
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Jours post chimio
160
330
250
660
750 750
0
20
40
60
80
GCSF agrave J1 GCSF agrave J2 GCSF agrave J3 GCSF agrave J4 GCSF si leucocytes
lt 1000
Pas de GCSF
Dureacutee G-CSF 115 12 135 155 17 0
Peacuteriode de neutropeacutenie seacutevegravere par
type de chimiotheacuterapie
Incidence des NF en fonction du 1er
jour drsquoadministration du GCSF (Haute dose de cyclophosphamide)
Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Lymphome non Hodgkinien Cancer du sein K du poumon
Jours de prophylaxie par Filgrastim
Ris
que d
rsquohospitalis
atio
n
+ 3 jours = 55
de reacuteduction du
risque de NF
Weycker D et al Are shorter courses of filgrastim prophylaxis associated
with increased risk of hospitalization Ann Pharmacother 200640(3)402-7
Le risque drsquohospitalisation pour NF diminue avec le
nombre de jours de preacutevention par filgrastim RESPECT
DES MODALITEacuteS (DUREacuteE) PARAMEgraveTRE ESSENTIEL
DrsquoEFFICACITEacute DES G-CSF QUOTIDIENS
Analyse reacutetrospective preacutes de 12000 patients
Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Von Minckwitz Annals of oncology 07
ndash Etude prospective multicentrique GEPARTRIO n = 1 256
patientes atteintes drsquoun cancer du sein et traiteacutees par le
protocole TAC en neacuteo-adjuvant
bull Ciprofloxacine seule n = 253
bull 6 jours de G-CSF n = 377
bull Neulasta seul n = 305
bull Neulasta + ciprofloxacine n = 321
ndash Critegravere principal incidence de la NF
ndash Critegraveres secondaires incidence de la neutropeacutenie et autres
toxiciteacutes heacutematologiques infections toxiciteacutes non-heacutemato
et hospitalisations
Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Par rapport agrave 6 jours de G-CSF pegfilgrastim
reacuteduit de 61 lrsquoincidence de la NF
18
p lt 0001
61
0
5
10
15
20
7
18
d - G-CSF Pegfilgrastim
Inc
ide
nce
de N
F s
ur
lrsquoe
nse
mb
le
des
cyc
les
61
p lt 0001
bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

bull La NF est associeacutee agrave un accroissement de la
mortaliteacute et des couts1
bull Importance des facteurs de risque lieacutes agrave la patiente agrave la maladie
sous-jacente et au protocole de chimiotheacuterapie utiliseacute
bull Les G-CSF doivent ecirctre administreacutes 24 agrave 72 h apregraves la fin de la
chimiotheacuterapie et doivent ecirctre poursuivis jusqursquoagrave PN 2 agrave 3 109 pour
les G-CSF quotidiens
bull Impact des G-CSF sur le CA 153 eacuteleacutevation transitoire ne devrait pas
entraicircner drsquoinquieacutetude chez le meacutedecin et la patiente
Utilisation des facteurs de croissance
granulocytaires dans le cancer du sein
1 Kuderer et al 2006 Smith et al 2006 Aapro et al 2006 Repetto et al 2003 NCCN 2007
Jared et al 2006
LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

LA PRATIQUE DES SCHEMAS COURTS
EST NON OPTIMALE
Etudes reacutetrospectives comparatives
Daily GCSF initieacute de J6 agrave J11
En moyenne 5 ndash 6 injections
Un risque de NF augmenteacute de 41 (versus Peg)
QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

QUELLE EST LA REALITE DES PRATIQUES
AUJOURDrsquoHUI
GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

GCSF et pathologie myeacuteloiumlde
bull Revue des essais adjuvants (sein) du NSABP ndash Smith RE JCO 2003 21 1195 ndash 1204
bull Doxo 60 Endoxan 600 agrave 2400 ndash 6 essais
bull Risque SMDLAM 1 (HD) vs 02 (standard)
bull Utilisation GCSF = correacutelation agrave lrsquoaugmentation du risque
bull Agents alkylants et doses (anomalies Chr 5711)
bull Facteur confondant = prophylaxie secondaire = reflet drsquoune plus grande fragiliteacute
bull Problegraveme meacutethodo identique eacutetude cas-teacutemoin de Le Deley JCO 2007 20 292 ndash 300 (rocircle de la mitoxantrone et possiblement du GCSF)
GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

GCSF et pathologie myeacuteloiumlde
bull Cancer du sein base de donneacutees SEER ndash Hershman D JNCI 2007 99 196 ndash 205
bull 5510 femmes gt 65 ans traiteacutees en adjuvant
bull SMD LAM = 177 avec GCSF vs 104 sans GCSF (HR 112 ndash 408)
bull Pas drsquoinformation sur la DI ni sur la dose de Cyclo (correacuteleacutee agrave lrsquoutilisation de GCSF)
bull Risque de LAM non confirmeacute dans une eacutetude SEER plus reacutecente et plus vaste [ Patt JC0 2007 ] ni dans lrsquoeacutetude dose-densiteacute CALGB 9741 [ Citron JCO 2003 ]
bull Aucun surcroicirct de risque de SMD LAM (003 ) ou cancer chez les donneurs de CSP mobiliseacutes par GCSF seul ndash sur pregraves de 35 000 donneurs suivis [Pulsipher Ped Blood Cancer 2006 Ries SEER 2006 de La Rubia Haematologica 2008]
GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

GCSF et pathologie myeacuteloiumlde
bull En somme aucune PREUVE de lrsquoeffet inducteur de
SAM LMD par lrsquoutilisation de GCSF mecircme chez les
personnes acircgeacutees
bull Et mecircme un assez grand nombre drsquoarguments contraires
bull Rocircle probablement central de la DI des alkylants
bull Inteacuterecirct du suivi agrave long terme (NFP) des patientes traiteacutees
en adjuvant
JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

JCO 2010 ndash Meacuteta-analyse 12 800 pts
25 eacutetudes controcircleacutees
GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

GCSF usefulness of primary prophylaxis
Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Prophylaxie chez la personne acircgeacutee
Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Mai 2010
Traitement de support
de patientes
Traitement(s) de support primaires EPO
Introduction au 1er cycle Introduction au 4egraveme cycle
G-CSF
Introduction au 1er cycle Introduction au 2nd cycle
Introduction au 3egraveme cycle
3 (n=3)
2 patientes 1 patiente
52 (n=53)
50 patientes 2 patientes 1 patiente
Traitement(s) adjuvant(s) compleacutementaire(s)
Herceptinereg
17 (n=17)
Conseils dieacuteteacutetiques 7 (n=7)
Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Mai 2010
Toxiciteacute heacutematologique
Sur lrsquoensemble des cycles de patientes
Aneacutemie (au moins une) 30 (n=30)
Neutropeacutenie (au moins une) 13 (n=13)1
Neutropeacutenie feacutebrile (au moins une) 5 (n=5)2
Thrombopeacutenie (au moins une) Aucune
1 dont 4 patientes avec grade 4 2 dont 2 patientes avec grade 4
Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Traitement curatif de la NF
bull Reacuteduction probable (Niveau II) des complications
infectieuses de la dureacutee drsquohospitalisation et de la
consommation drsquoantibiotiques
bull Pas drsquoimpact clair sur la survie
La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

La prophylaxie secondaire dans les recommandations
pouvant entraicircner une
La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

La prophylaxie secondaire dans les recommandations
Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

Anticancer Res 2013 Jan33(1)301-7
Granocyte-colony stimulating factor (G-CSF) has
significant efficacy as secondary prophylaxis of
chemotherapy-induced neutropenia in patients with
solid tumors results of a prospective study
Freyer G1 Jovenin N Yazbek G Villanueva C Hussain A
Berthune A Rotarski M Simon H Boulanger V
Hummelsberger M Falandry C
wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

wwwesmo2012org
Study Design
Cycle A (No G-CSF support
Cycle B (Initiation of
G-CSF)
Cycle C Cycle D Cycle E
Chemotherapy regimen
NEUTROPENIC EVENT (NE)
NEUTROPENIC EVENT (NE)
Study Follow up
33
(1) National Comprehensive Guidelines Network Myeloid Growth Factors Available from httpnccnorg
INCLUSION
NE definition (1) FN or Neutropenia that impacted on subsequent
cycle ( ie cycle delay andor dose reduction andor G-CSF use)
wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

wwwesmo2012org
Patients and Disease Characteristics
bull 628 patients included between January and December 2009
bull Data analyzed = 548 evaluable patients
bull Patient characteristics
ndash Age mean ( SD)= 617 123 y (436 gt 65 y)
ndash Gender= 3 1 Male 69 Female
ndash Karnofsky PS 0 -1= 883
ndash Breast cancer= 40
ndash Metastatic disease= 533
34
wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

wwwesmo2012org
Chemotherapy Regimens N=548
FEC 100 52 (95)
Paclitaxel- carboplatin 39 (71)
Folfoxcapecitabine 38 (69)
Docetaxel 100 mgm2 22 (40)
Other 397 (725)
FEC100 5-fluorouracil 500-600mgm2- epirubicin 100mgm2- cyclophosphamide 600mgm2 Folfox 5-fluorouracil- Leucovorin- oxaliplatin other Adriamycincyclophosphamide (AC) Adriamycincyclophosphamide- paclitaxel (AC-T) Caelyx Docetaxel 75 mgm2 Doxorubicin docetaxel Epirubicin FEC75+ Taxotere+ trastuzumab cyclophosphamide-Etoposidecisplatin 5-Fluorouracil- leucovorin- irinotecan (FOLFIRI) 5-FU-leucovorin Gemcitabine Cisplatin Vironelbine Paclitaxel Paclitaxel+ Bevacizumab Taxotere-cyclophosphamide (TC) Taxotere- carboplatin-herceptin (TCH) Taxotere-Adriamycin- Cyclophosphamide (TAC) Bleomycine-Etoposide-Cysplatin (BEF) Topotecan and other
wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

wwwesmo2012org
Incidence of NE N=548 pts all cycles
36
NE FN or neutropenia with a significant impact on the next cycle of chemotherapy cycle delay andor dose
andor prescription of G-CSF FN single temperature ge 383degC orally or ge 380degC over one hour and
neutrophils lt 500mm3 or lt 1000mm3 or decline of neutrophils to le 500mm3 over the next 48h Neutropenic
fever grade 1-3 neutropenia with fever
00
100
200
300
400
500
600
700
800
900
1000
Cycle ACycle B
Cycle CCycle D
Cycle E
1000
212
186
115 129
763
203
173
113 137
77
04 07
02
00
161
05 07
00 03
Percentage of patients
Neutropenic events Neutropenia all grades Neutropenic fever FN
No G-CSF
wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

wwwesmo2012org
Prophylactic strategies developed during the study (N=548 All Cycles)
Prophylactic strategies Cycle B N= 548
Cycle C N=548
Cycle D N=442
Cycle E N=344
Cycle delay (n ) 244 (445) 44 (80) 23 (52) 18 (52)
Dose reduction (n) 122 (223) 27 (49) 17 (38) 12 (35)
Use of prophylactic G-CSF (n ) 466 (850) 413 (754) 332 (751) 247 (718)
Type of G-CSF
Pegfilgrastim 278 (597) 253 (613) 211 (636) 152 (615)
Filgrastim 48 (103) 39 (94) 30 (90) 22 (89
Lenograstim 127 (273) 11 (269) 84 (253) 67 (271)
Biosimilar 10 (21) 9 (22) 6 (18) 6 (24)
Prophylactic strategies included cycle delay andor dose reduction andor prophylactic G-CSF Cycle delay or dose reduction in cycle B to E were relative to the previous cycle while G-CSF use was the proportion of the subjects in the given cycle
37
wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

wwwesmo2012org
Predictive Factors of NE Recurrence (Multivariate Analysis)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy With G-CSF Without G-CSF
Prophylaxis HR ( 95 CI) P value
(Vs no use o G-CSF) 032 ( 024 043) lt 0001
Incidence of NE following the first event in the subsequent cycles according to the prophylactic strategy
with or without G-CSF (Left Panel) and the type of G-CSF Pegylated Vs others (Right Panel)-Kaplan
Meier curve for the time to recurrence of NE N=548 all cycles)
o
f p
atien
ts w
ith
ou
t n
eu
trop
en
ic e
ven
t
0
10
20
30
40
50
60
70
80
90
100
Duration in days
0 50 100 150 200 250 300
Treatment strategy PEGFilgrastim Other G-CSFWithout G-CSF
HR (95 CI) P value
Pegfilgrastim prophylaxis (Vs others)
023 (016 032) lt 0001
38
wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39

wwwesmo2012org
Conclusion bull The study shows that prophylactic strategy
using G-CSF has significant efficacy in reducing the incidence of chemo-induced NE in patients with solid tumors
bull Use of prophylactic G-CSF may be a valuable option for optimal delivery of standard chemotherapy in patients with solid tumors
39




![Toxicité de la radiothérapie - sahgeed.com · Toxicité subaigue : pneumopathie radique ± Dyspnéisante ± Febrile ± W µ [ v v Z} À}oµu ] ] ± Peut Etre léthale guérir sous](https://img.pdfslide.fr/doc/110x75/5b37be177f8b9a5a178ca244/toxicite-de-la-radiotherapie-toxicite-subaigue-pneumopathie-radique-.jpg)