Embed Size (px)
Citation preview
1
Les mLes mééthodes thodes
de supplde supplééances hances héépatiques patiques
Dr Bernard GoubauxDr Bernard Goubaux
RRééanimation animation medicomedico--chirurgicalechirurgicale et transplantationet transplantation
Hôpital de lHôpital de l’’Archet Archet
CHU de NiceCHU de Nice

2
IntroductionIntroduction
•• InsuffisancesInsuffisances hhéépatiquespatiques aiguaiguëëss: : ddééfifi ththéérapeutiquerapeutique. .
•• MortalitMortalitéé spontspont: 70 : 70 àà 90 % 90 % selonselon ll’’âgeâge et et ll’é’étiologietiologie . .
•• La La TxTx hhéépatiquepatique orthotopiqueorthotopique restereste ll’’unun des des seulsseuls
traitementstraitements efficacesefficaces::
•• maismais intervention intervention majeuremajeure, , cocoûûteuseteuse, non , non ddéénunuééee de de risquesrisques
••limitlimitééee par la par la ppéénurienurie de de greffonsgreffons. .
••traitement immunosuppresseur traitement immunosuppresseur àà vie vie
••supprime la possibilitsupprime la possibilitéé de rde rééggéénnéération du foie dration du foie d’’origine du origine du
patient. patient.

3
Inscription en liste dInscription en liste d’’attente pour attente pour TxTx hhéépatiquepatique
Patients en attente de greffe hépatique aux USA: Source UNOS
4
SupplSupplééance hance héépatiquepatique
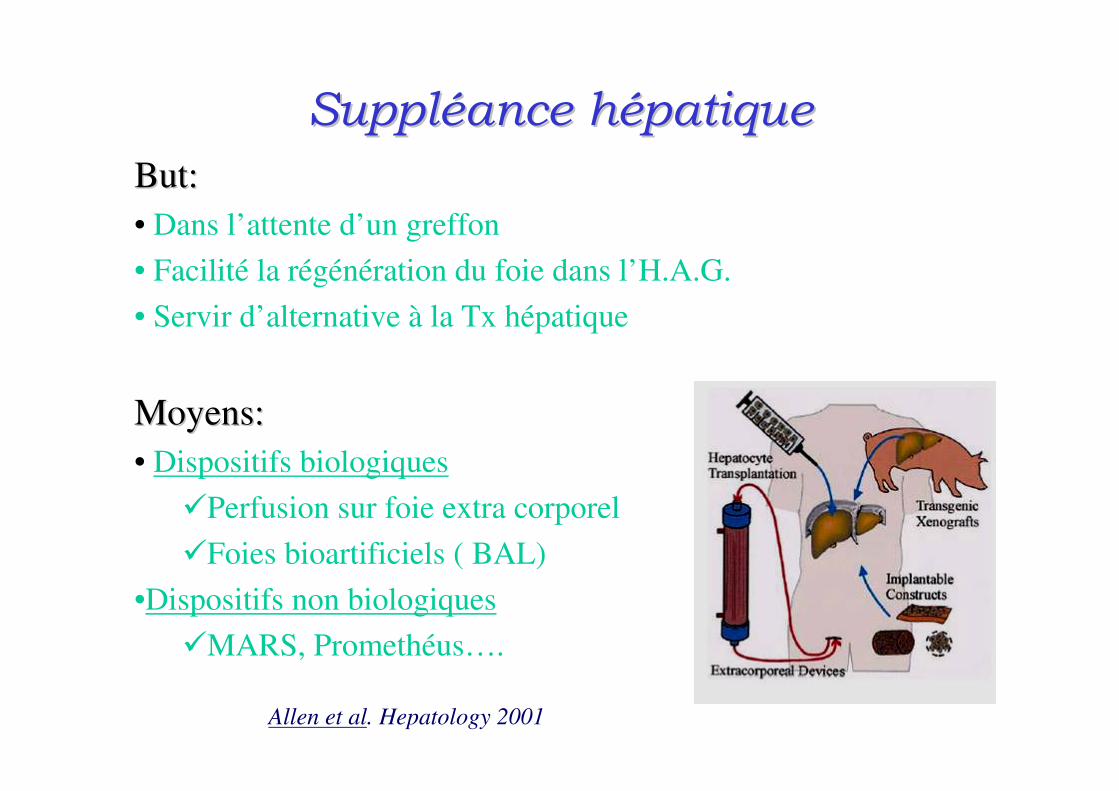
But:But:
• Dans l’attente d’un greffon
• Facilité la régénération du foie dans l’H.A.G.
• Servir d’alternative à la Tx hépatique
Moyens:Moyens:
• Dispositifs biologiques
�Perfusion sur foie extra corporel
�Foies bioartificiels ( BAL)
•Dispositifs non biologiques
�MARS, Promethéus….
Allen et al. Hepatology 2001
5
SupplSupplééance hance héépatique: Historiquepatique: Historique
•Fin des années 50: boyat d’hépatocytes (Sorrentino et al)
•1957 circulation croisée chien homme (Hori et al)
•1958 principe de la perfusion sur foie extra corporel isolé (Otto)
•1959 Premier BAL ( Mikami)
•1970 travaux de Wolf et Munklet à partir d’hepatocytes tumoraux
•1987 1ére publi. d’un BAL avec hépatocytes isolés ( Matsumara)
•2000 Stange : MARS®
•2003 Rifai : Prometheus ®
Le foie extra corporelLe foie extra corporel
6

7
Perfusion sur foie extra corporelPerfusion sur foie extra corporel
•• Foie en dFoie en déérivation rivation àà ll’’extextéérieurrieur
•• Humain ou animalHumain ou animal
•• Quelques cas dQuelques cas déécrits crits ( ( HoriHori 1958; Chari 1994)1958; Chari 1994)
•• Pb thrombotiques, immunologiques, Pb thrombotiques, immunologiques, ééthiquesthiques
8
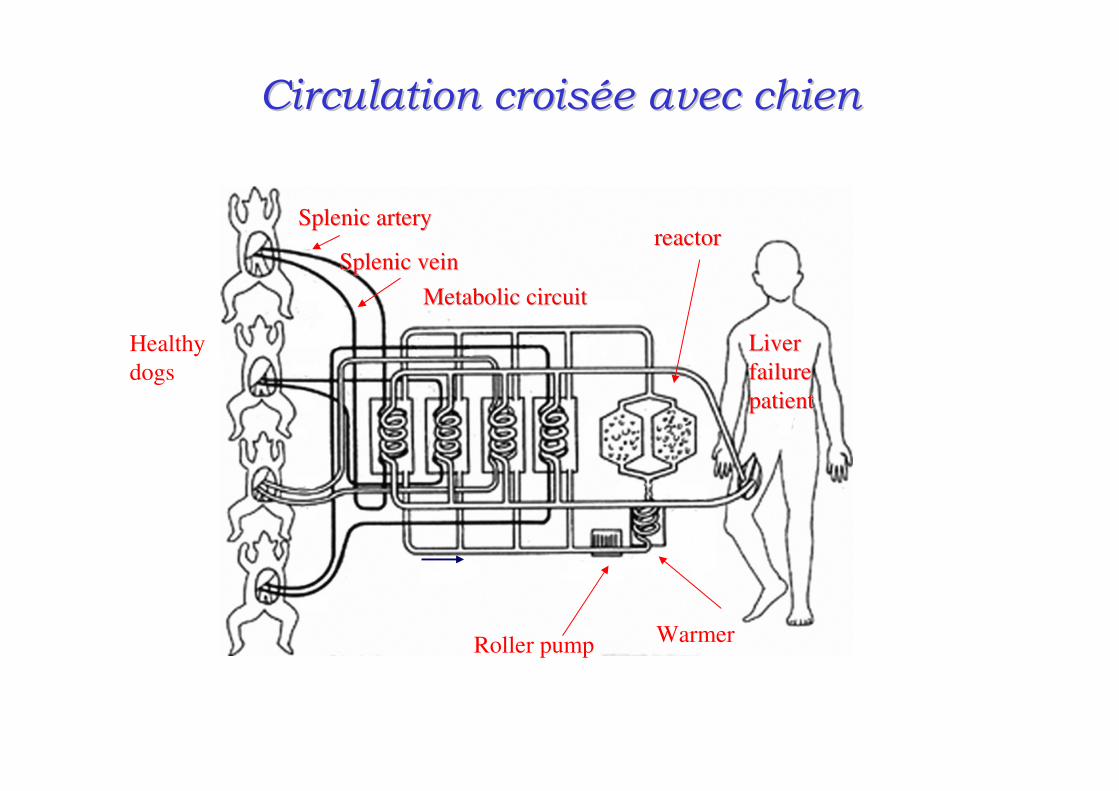
Circulation croisCirculation croiséée avec chiene avec chien
LiverLiver
failurefailure
patientpatient
reactorreactor
WarmerRoller pump
MetabolicMetabolic circuitcircuit
Healthy
dogs
SplenicSplenic arteryartery
SplenicSplenic veinvein
Cross dialysis treatment using four living dogs Hori et al; 1958

9
Perfusion sur Foie ex vivoPerfusion sur Foie ex vivo
The Venovenous Circuit for ex Vivo Pig-Liver Perfusion
Chari RS et al, N. Engl J Med 1994
10
Transplantation dTransplantation d’’hhéépatocytes isolpatocytes isolééss
• Organes cibles: rate, poumon;V. Porte, péritoine;11
• Hépatocytes allo ou xénogénique 22
• Protégés par encapsulation ou enrobés d’un hydrogel
• Surtout études animales 33
• Limites: délai de 2-3 jours pour efficacité maxi.
• Quelques études pédiatriques 44
1 Regimbo JM et al: Gastroenterol Clin Biol 2002
2 Mai G.et al: Xenotransplantation 2005
3 Tsuruga Y et al: Transplant Proc 2008
4 Dhawan A. et al: J. Inherit Metab dis. 2006

Foie Foie BioartificielBioartificiel : B.A.L.: B.A.L.
12
Foie Foie bioartificielbioartificiel -- principesprincipes
Début du concept: Wolf et Munklet milieu 70’s
Le principe commun:
Hépatocytes vivants
Dispositif extracorporel les mettant en relation directe
avec la circulation générale du patient.
Les performances des BAL sont directement liés à la qualité du
bio reacteur.

13
• Milieu propice pour développement et metab. des
hepatocytes
• Transport bidirectionnel entre hepatoc et le sang
• Haut débit de sang
• Protection des hépatoc. contre syst immunitaire de l’hôte
Foie Foie bioartificielbioartificiel –– Cahier des chargesCahier des charges
Plusieurs types de Plusieurs types de bioreacteursbioreacteurs::
•A fibre creuses
•Milieu avec cellules encapsulées
•Milieu avec cellules en suspension
Plusieurs types cellules:Plusieurs types cellules:
• hépatocytes humains
• hépatocytes de Porc

• Hépatocytes:
– Humains : pas de division cellulaire
– Humains transformés ( hépatoblastome C3A)
– Humains immortalisés ( stade de la recherche pure)
– Xenogéniques ( Porc )
• Stockage des hépatocytes
– Culture cellulaire
– Congélation+++
Foie Foie bioartificielbioartificiel –– Cahier des chargesCahier des charges

15
BioreacteurBioreacteur de premide premièère gre géénnéérationration
Représentation schématique des fibres creuses
du foie bio-artificiel
16
SystSystèèmes en cours dmes en cours d’’essais cliniquesessais cliniques

17
http://http://www.hepatix.comwww.hepatix.com
ExtracorporealExtracorporeal LiverLiver AssistAssist DeviceDevice
Sussman NL Transplan Proc. 1993

18
MELS MELS BioreacteurBioreacteur
Vue 3D du Vue 3D du rrééseau de seau de fibresfibres
Module contenant les cellules
Membrane de
dialyse
separateur
plasma
Module de dialyse àl’albumine
8 patients traités entre 8 et 46h
Tous transplantés
Survie à 3 ans:100%
Sauer et al ; J Hepatol 2003
Modular Extracorporeal Liver Support

19
HepatAssistHepatAssist DemetriouDemetriou
Système hybride : hepatocytes et colonne de charbon
Circe Biomedical

20
Algenix Liver 2000
http://hugroup.cems.umn.edu/Research/bal
The technology used in Algenix's LIVERX2000
has been licensed by the University of
Minnesota-USA

21
Amsterdam medical center Bioartificial Liver
AMCAMC--BAL BAL
Schematic representation of the bioartificial liver support system.
Plasma was obtained from the recipient by a centrifugal plasma-separator. To prevent cellular
immunological problems, two plasma filters were included. When blocked, these filters can
easily be replaced during the extra-corporal artificial liver procedure. Different filter types
(various material properties and cut-off) can be applied without changing the bioreactor design.

22
B.A.L.: le futurB.A.L.: le futur
Les législation européenne sur les
xenotransplantation interdisent l’utilisation
d’hépatocytes animaux dans les applications
cliniques des BAL.
Le futur des BAL est le développement et la
culture de lignées cellulaires d’hépatocytes
humain.
23
Les systLes systèèmes de supplmes de supplééances hances héépatiquespatiques

24
Les dispositifs non spLes dispositifs non spéécifiquescifiques
•• HHéémodialyse conventionnellemodialyse conventionnelle–– Toxines produites par lToxines produites par l’’IHCIHC: haut PM et hydrophobes: haut PM et hydrophobes
•• HHéémoperfusionmoperfusion sur colonne de charbon actifsur colonne de charbon actif–– Absorbe Absorbe substsubst lipophiles ou non ionislipophiles ou non ionisééeses11
–– TrblsTrbls coagulationcoagulation
•• EchangesEchanges plasmatiques.plasmatiques.–– A bas volume: pas dA bas volume: pas d’’efficacitefficacitéé sur sur encephalopathieencephalopathie 22
–– A haut volume: plus efficace mais rien sur la survieA haut volume: plus efficace mais rien sur la survie 33
1Yatzidis H. Proc Eur Dial Transplant Assoc 1964
2 Iwai H et al Crit Care Med. 1998
3 Clemmesen JO et al. AM J Gastroenrol.2001
25
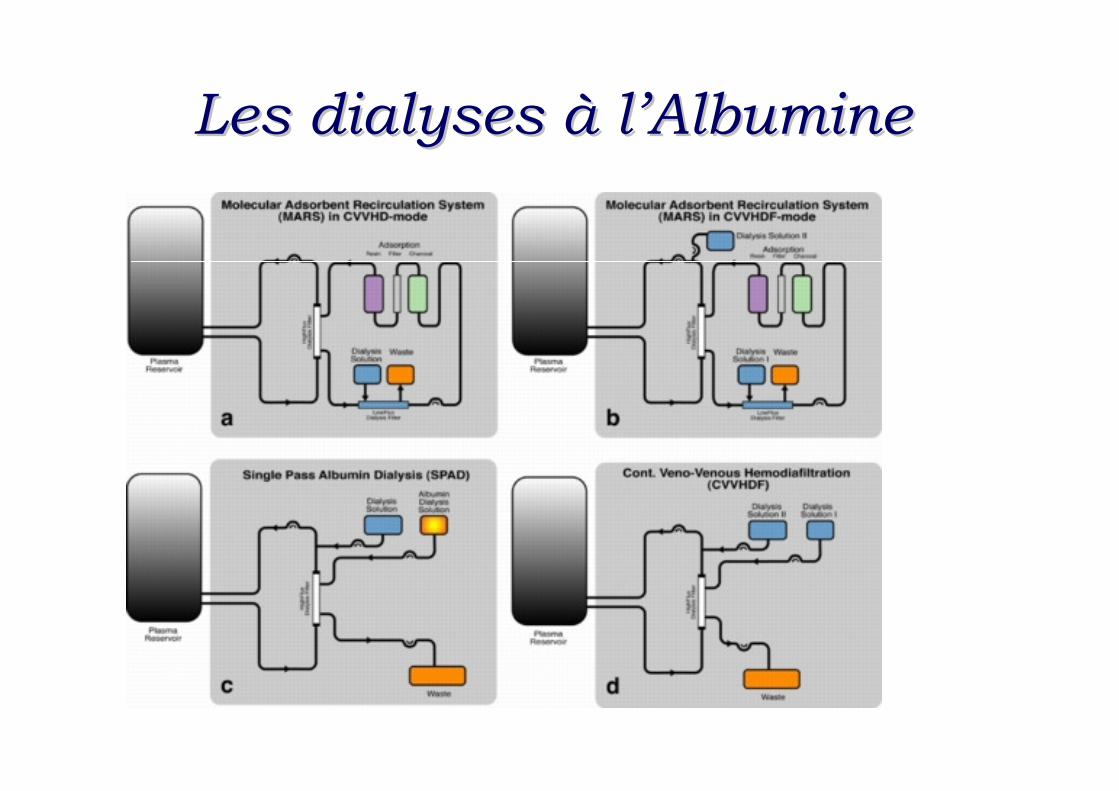
Les dialyses Les dialyses àà ll’’AlbumineAlbumine
26
Dialyse Dialyse àà ll’’Albumine: PrincipesAlbumine: Principes
•• DDéétoxification du sangtoxification du sang
•• Albumine: adsorbant sAlbumine: adsorbant séélectiflectif
•• EliminationElimination de fade faççon son séélective les toxines lilective les toxines liéées es àà ll’’AlbAlb..
•• Pas de fonction de synthPas de fonction de synthèèsese
Dialyse hépatique utilisant le pouvoir de fixation de l’A.H..
27
La dialyse simple: SPADLa dialyse simple: SPAD
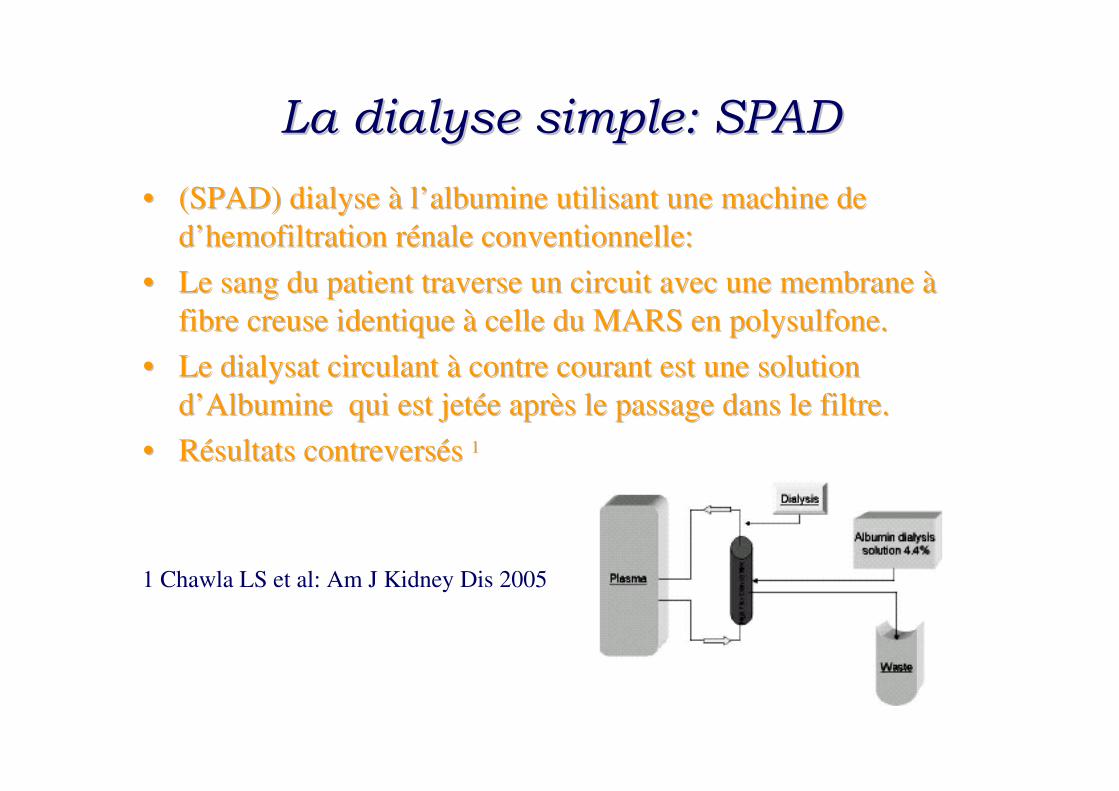
•• (SPAD) dialyse (SPAD) dialyse àà ll’’albumine utilisant une machine de albumine utilisant une machine de
dd’’hemofiltrationhemofiltration rréénale conventionnelle:nale conventionnelle:
•• Le sang du patient traverse un circuit avec une membrane Le sang du patient traverse un circuit avec une membrane àà
fibre creuse identique fibre creuse identique àà celle du MARS en celle du MARS en polysulfonepolysulfone. .
•• Le dialysat circulant Le dialysat circulant àà contre courant est une solution contre courant est une solution
dd’’Albumine qui est jetAlbumine qui est jetéée apre aprèès le passage dans le filtre. s le passage dans le filtre.
•• RRéésultats sultats contreverscontreversééss 11
1 Chawla LS et al: Am J Kidney Dis 2005

SystSystèèmeme SPADSPAD : : ProtocoleProtocole de de misemise en routeen routeMatMatéérielriel ::
••PrismaflexPrismaflex
••Set avec Membrane HF 1400 Set avec Membrane HF 1400 HospalHospal (1.4m(1.4m22))
PrPrééparationparation dudu dialysatdialysat //albuminealbumine ::
••RetirerRetirer 800ml 800ml dd’’hhéémosolmosol apraprèès s avoiravoir rrééuniuni le le compartimentcompartiment bicarbicar et le et le compartimentcompartiment
ioniqueionique
•• bienbien mméélangerlanger
••RemplacerRemplacer le le liquideliquide soustraitsoustrait par 800ml par 800ml dd’’albuminealbumine humainehumaine àà 20%20%
••Concentration finale 32g/l ( 3.2%)Concentration finale 32g/l ( 3.2%)
HHéémofiltrationmofiltration ::
••CVVHDFCVVHDF
••Debit sang 150 ml/minDebit sang 150 ml/min
••DialysatDialysat 1000 ml/h1000 ml/h
••PertesPertes 0 0
••Restitution 0Restitution 0
••DurDurééee de la sde la sééance 10heures (2 ance 10heures (2 hhéémosolsmosols))
Surveillance Surveillance selonselon feuillefeuille de de recueilrecueil
Unité de réanimation et Transplantations
Archet II-CHU de Nice

SPAD et Prismaflex

S.P.A.D.
CorrelationsCorrelations betweenbetween thethe levellevel beforebefore a single a single passpass albuminalbumin dialysisdialysis
(SPAD) session (SPAD) session andand thethe amountamount ofof substance substance extractedextracted duringduring thethe
subsequentsubsequent SPAD session (SPAD session (n n = 37) for (A) bile = 37) for (A) bile acidsacids andand (B) (B)
bilirubinbilirubin
KarimaKarima BenyoubBenyoub,1 ,1
Michel Muller,2 AurMichel Muller,2 Auréélie lie
Bonnet,1Bonnet,1
RRéémy Simon,1 Mathieu my Simon,1 Mathieu
Gazon,1 Serge Gazon,1 Serge DuperretDuperret,1,1
FrFrééddééric ric AubrunAubrun,1 ,1 andand
Jean Paul Viale1Jean Paul Viale1
1Hospices Civils de Lyon, 1Hospices Civils de Lyon,
Hôpital Croix Rousse,Hôpital Croix Rousse,
2Centre Hospitalier de la 2Centre Hospitalier de la
rréégion dgion d’’Annecy, 1,Annecy, 1,
METZMETZ--TESSYTESSY
74374, France74374, France

31
Le système Prometheus( Fresinius Medical Care)
Un principe: Un principe:
FPSA:FPSA:FractionatedFractionated Plasma Plasma SeparationSeparation andand
AbsorptionAbsorption
Quatre Quatre ééllééments:ments:
••AlbuflowAlbuflow filterfilter: : plasmaphplasmaphéérrèèsese
••PromethPrometh 01: fixe les compos01: fixe les composéés insolubles s insolubles
( sels biliaires, ( sels biliaires, phenolsphenols, AAA..), AAA..)
••PromethPrometh 02: r02: réésines sines ééchangeuses dchangeuses d’’anionsanions
••Membrane de dialyse conventionnelle.Membrane de dialyse conventionnelle.
Falkenhagen et al Artif Organs 1999
Evenepoel P. et al Blood purif 2005

Le système Prometheus
•• Contrôle du circuit extra corporel Contrôle du circuit extra corporel
par moniteur de dialyse par moniteur de dialyse
conventionnelle conventionnelle
( 4800H =( 4800H =FreseniusFresenius medicalmedical care)care)

Prometheus: résultats
Evenepoel P. et al Blood purif 2005
EtudeEtude multicentrique multicentrique ""HeliosHelios ""

Etude Helios•• 145 patients 145 patients withwith ACLF ACLF werewere randomizedrandomized to to eithereither SMT or additive SMT or additive
treatmenttreatment withwith PrometheusPrometheus. .
•• PrometheusPrometheus therapytherapy waswas initiatedinitiated for 3 for 3 weeksweeks, , andand thethe primaryprimary endend points points
werewere 2828-- andand 9090--day day survivalsurvival. .
•• ResultsResults
–– ThereThere werewere nono significantsignificant differencesdifferences in in baselinebaseline characteristicscharacteristics concerningconcerning
MELD score, age or MELD score, age or etiologyetiology ofof underlyingunderlying chronicchronic liverliver diseasedisease. .
–– In In thethe intentionintention--toto--treattreat analysisanalysis, , survivalsurvival on on dayday 28 28 waswas 66 versus 63% (p = 66 versus 63% (p =
0.70; SMT plus 0.70; SMT plus PrometheusPrometheus vs SMT) vs SMT) andand on on dayday 90 90 waswas 47 versus 38% (p = 47 versus 38% (p =
0.35), 0.35), respectivelyrespectively. .
–– In a In a predefinedpredefined subgroupsubgroup analysisanalysis, a , a significantsignificant survivalsurvival benefitbenefit waswas observedobserved
underunder FPSA FPSA therapytherapy in patients in patients withwith HRS type I (p = 0.04) or MELD score more HRS type I (p = 0.04) or MELD score more
thanthan 30 (p = 0.02 30 (p = 0.02
Rifai K, Kribben A, Gerken G et al. Extracorporeal liver support by fractionated plasma separation and absorption
(Prometheus®) in patients with acute-on-chronic liver failure (HELIOS study): a prospective randomized
controlled multicenter study. J. Hepatol.52(S1),S3 (2010).
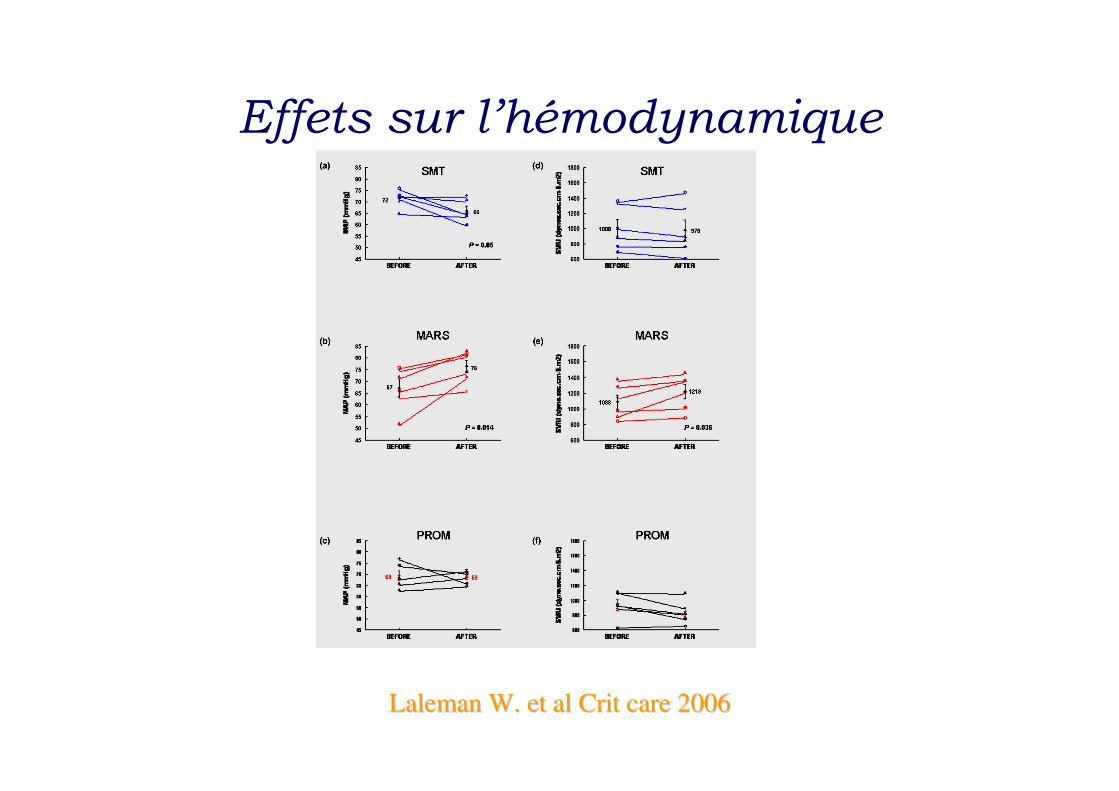
Effets sur l’hémodynamique
LalemanLaleman W. et W. et alal CritCrit care 2006care 2006

36
MolecularMolecular Absorbant Absorbant RecirculatingRecirculating SystemSystem
•• Le moniteur MARS gLe moniteur MARS gèère le circuit clos re le circuit clos
dd’’Albumine 20% (500 ml). Albumine 20% (500 ml).
•• Un appareil dUn appareil d’’hhéémodialyse conventionnelmodialyse conventionnel
•• Une membrane MARS Flux semiUne membrane MARS Flux semi-- permpermééable able
àà fibres creusesfibres creuses
•• Une cartouche de rUne cartouche de réésine dsine d’’absorption des absorption des
toxinestoxines
•• Une colonne dUne colonne d’’absorption par charbon actifabsorption par charbon actif
•• LL’’albumine est en partie ralbumine est en partie rééggéénnéérréée en les e en les
traversant .traversant .
•• Une membrane Une membrane DiafluxDiaflux traditionnelle dtraditionnelle d ’’EEREER
MARS® Gambro Hospal
Stange J; Mitzner S Int J Artif Organs 1996
37
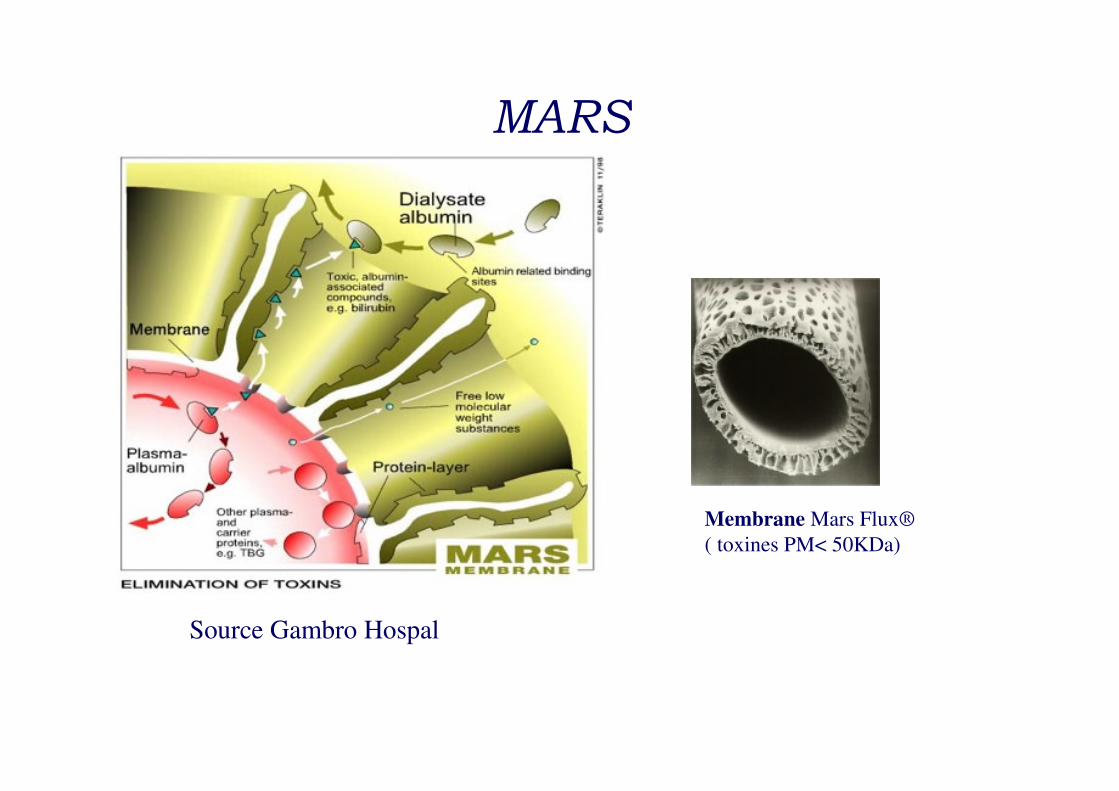
MARS
Source Gambro Hospal
Membrane Mars Flux®
( toxines PM< 50KDa)

PRISMARS
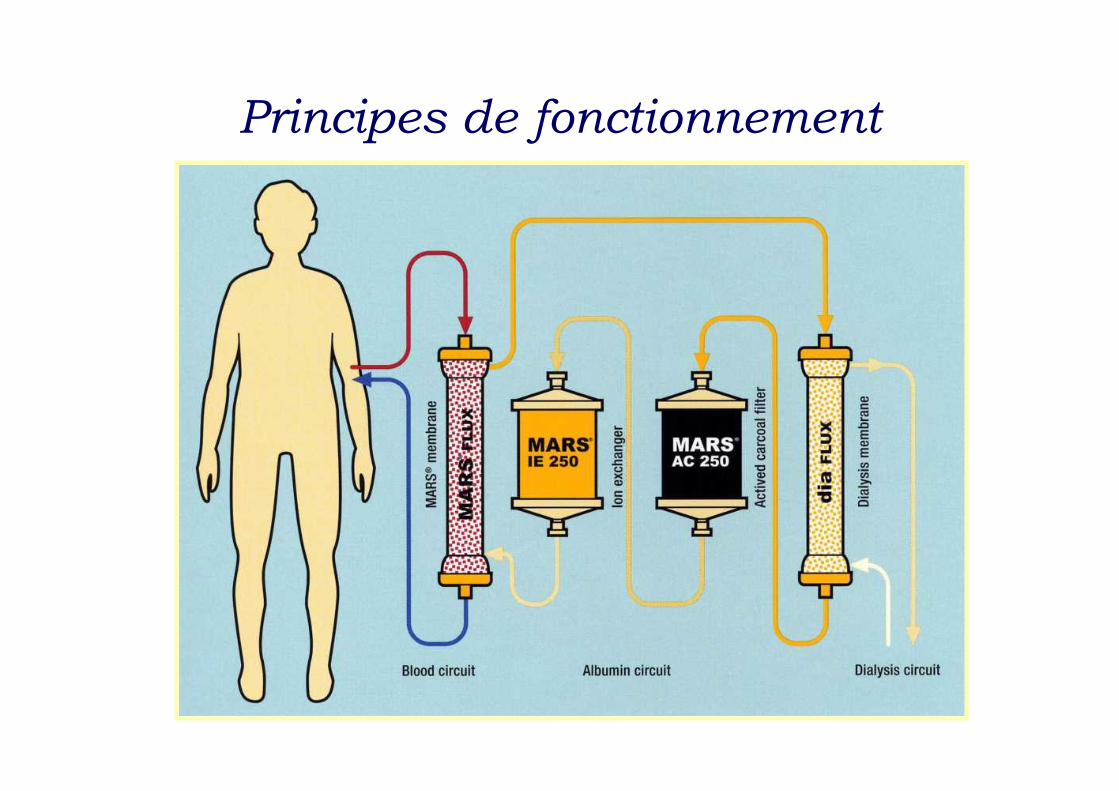
Principes de fonctionnement
Principales substances éliminées par le MARS
• Molécules à haute affinité pour l’albumine– Bilirubine
– Acides Biliaires
– Benzodiazépines
– Cuivre
– Acides Gras à Chaîne moyenne
– Acide arachidonique
– Tryptophane
– TNF alpha
– Ammoniac
– Calci bloqueurs
• Molécules éliminées par l’hémodiafiltration– Urée, créatinine
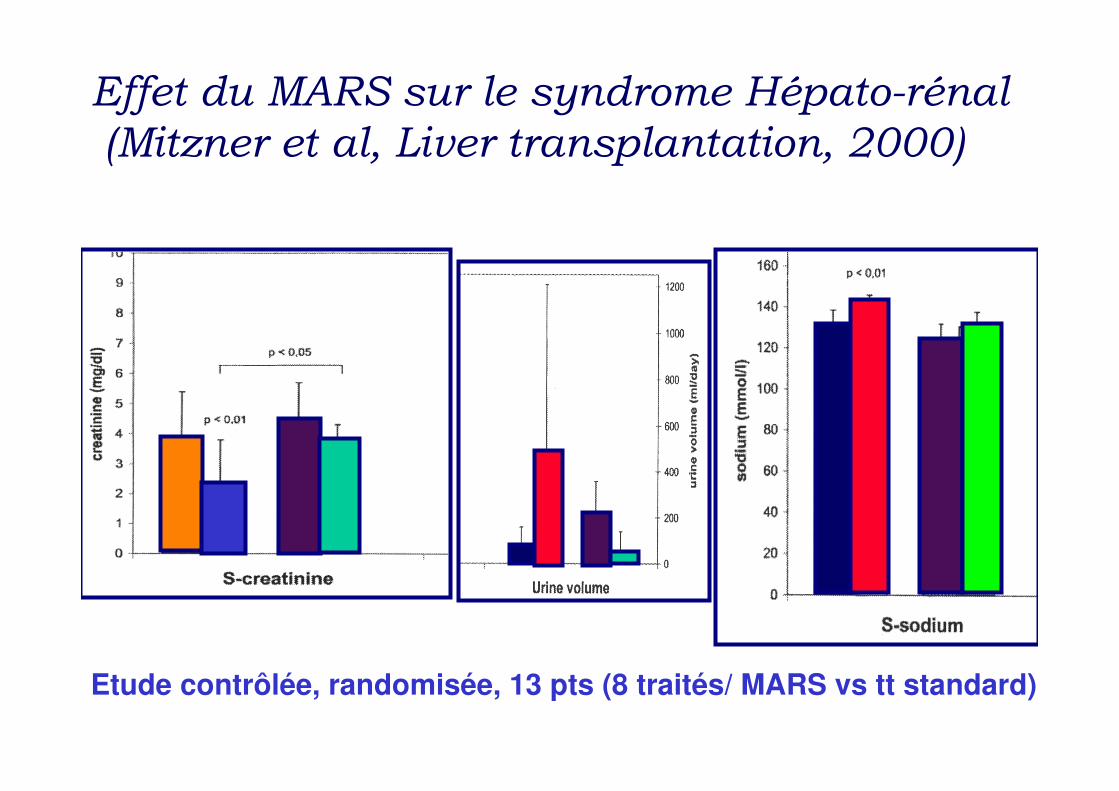
Etude contrôlée, randomisée, 13 pts (8 traités/ MARS vs tt standard)
Effet du MARS sur le syndrome Hépato-rénal
(Mitzner et al, Liver transplantation, 2000)

MARS & Tt standard
Contrôle (Tt standard)
Effet du MARS sur lEffet du MARS sur l’’encencééphalopathiephalopathie
Heemann et al, Hepatology, 2002Heemann et al, Hepatology, 2002

Effets secondaires
• Thrombopénie
• Activation de la fibrinolyse
• hypotension

Contre indications
•• CIVDCIVD
•• Saignement actifSaignement actif
•• Sepsis non contrôlSepsis non contrôléé
•• Absence de projet thAbsence de projet théérapeutiquerapeutique
•• AOCLF en phase terminale sans AOCLF en phase terminale sans TxTx hep. prhep. préévuevue
Kantola T et al . Prognostic factors in MARS-treated patientsWorld J Gastroenterol2009

MARS et HAA
8 pts (47.75 ans, 388 pts (47.75 ans, 38--61)61)
Cirrhose OH + HAA (PBH)Cirrhose OH + HAA (PBH)
Nombre de sNombre de sééance MARS: 5.75 ance MARS: 5.75 ++ 3.2 (33.2 (3--12)12)
Jalan et al, J Hepatol 2003
Changes in bilirubin concentration. The dashed lines represent the treatments with MARS.
(a) A representative course of serum bilirubin (from patient 2) over time in the five patients who survived to leave hospital.
(b) A representative course of serum bilirubin (from patient 6) over time in one of the patients who died in hospital.
Etude fulmar
Ile de France
Lille
Strasbourg
Rennes
Lyon
Bordeaux
Toulouse
Montpellier Nice
Besançon
PHRC* National*Projet Hospitalier de Recherche Clinique
16 Centres
Promoteur :
- DRCD / AP-HPDirection de Recherche Clinique
Assistance Publique-Hôpitaux de Paris
- Gambro/Hospal
- Laboratoires LFB
Critères Inclusion/ Exclusion
•• CritCritèèresres dd’’InclusionInclusion
•• Patients Patients ayantayant uneune hhéépatitepatite FulminanteFulminante ouou subfulminantesubfulminante
•• Age Age ≥≥ 18 18 -- 70 years70 years
•• CritCritèèresres de transplantation de transplantation hhéépatiquepatique ::–– CritCritèèresres de de BeaujonBeaujon ouou
–– CritCritèèresres dudu KingKing’’s colleges college
•• ConsentementConsentement ééclairclairéé patient patient ouou famillefamille
•• CritCritèèrere dd’’exclusionexclusion
•• Sepsis Sepsis sséévvèèrere non non contrcontrôlôléé
•• PressionPression aortiqueaortique moyennemoyenne <40mmHg (<40mmHg (malgrmalgréé inotropesinotropes))
•• Les Les contrecontre--indications indications absoluesabsolues àà la transplantationla transplantation
•• Infection VIHInfection VIH
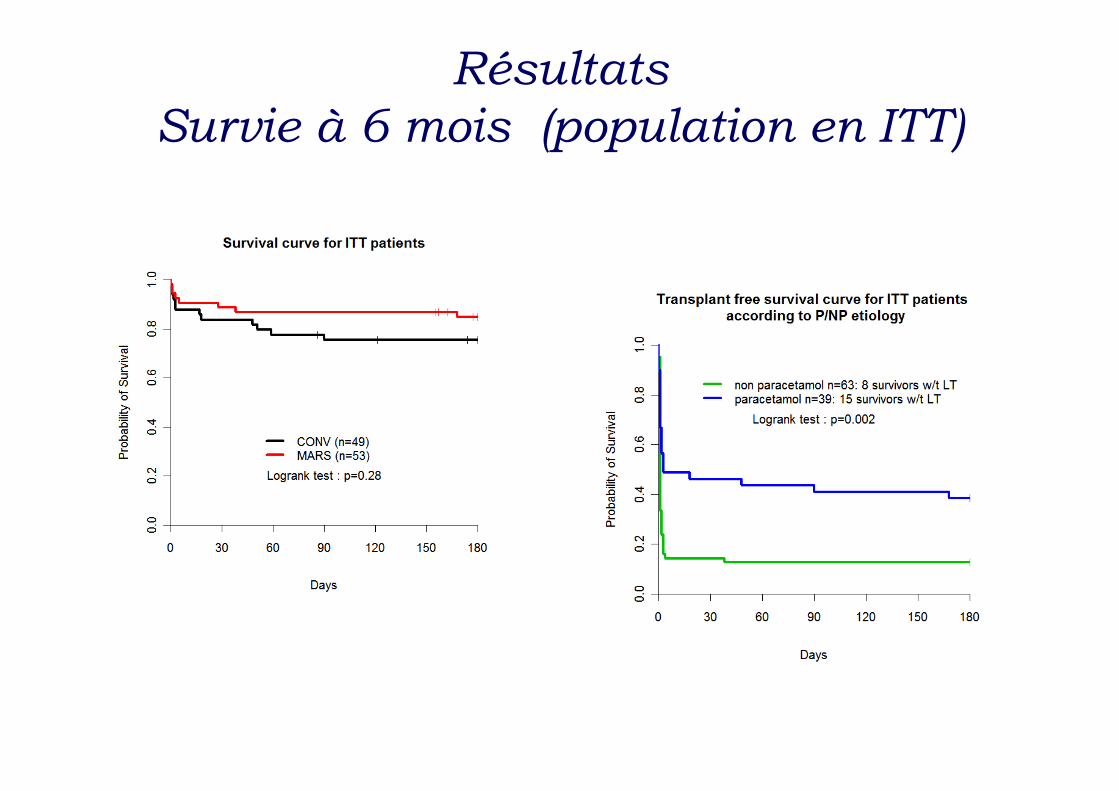
Résultats
Survie à 6 mois (population en ITT)

Etude Fulmar
•• TheThe interpretationinterpretation ofof resultsresults isis mademade difficultdifficult by by thethe factfact thatthat 68 68 ofof thethe 102 102
patients patients werewere transplantedtransplanted withwith a a medianmedian delaydelay ofof 16.2 h 16.2 h betweenbetween listing listing andand
incision, incision, accordinglyaccordingly resultingresulting in a short in a short pretransplantationpretransplantation studystudy phase in phase in
mostmost patients.patients.[*][*]
•• Du fait du dDu fait du déélai court (16h) lai court (16h) randomisationrandomisation--transplantationtransplantation au cours de cette au cours de cette
éétude tude
•• Le MARSLe MARS®® devrait devrait être encore être encore éévaluvaluéé
–– HHéépatite par intoxication au paracpatite par intoxication au paracéétamoltamol
–– Si contreSi contre--indication indication àà la transplantationla transplantation
–– PPéériode longue driode longue d’’attente sur la liste de greffeattente sur la liste de greffe
–– Greffon marginal: stGreffon marginal: stééatose satose séévvèère, fibrosere, fibrose……))
* Saliba F, Camus C, Durand F et al. Randomized controlled multicenter trial evaluating the
efficacy and safety of albumin dialysis with MARS® in patients with fulminant and
subfulminant hepatic failure. Presented at: The 59th Annual meeting of the American
Association for the Study of Liver Diseases. CA, USA, 31 October–4 November 2008
Etude Relief
•• 189 patients189 patients withwith ACLF ACLF werewere randomizedrandomized to to eithereither SMT or additive SMT or additive
treatmenttreatment withwith MARS. MARS.
•• MARS MARS therapytherapy waswas scheduledscheduled overover 21 21 daysdays; ;
•• TheThe primaryprimary endend point point waswas 2828--day day survivalsurvival. .
•• ResultsResults: :
–– ThereThere werewere nono significantsignificant differencesdifferences concerningconcerning baselinebaseline characteristicscharacteristics
betweenbetween thethe groups, groups, althoughalthough thethe numbernumber ofof patients patients withwith (MELD) scores (MELD) scores
andand spontaneousspontaneous bacterialbacterial peritonitisperitonitis waswas higherhigher in in thethe MARS group.MARS group.
–– In In thisthis studystudy, age, MELD score , age, MELD score andand spontaneousspontaneous bacterialbacterial peritonitisperitonitis werewere
independentindependent riskrisk factorsfactors for for increasedincreased mortalitymortality. .
–– In In thethe MARS group a MARS group a higherhigher reductionreduction ofof creatininecreatinine andand bilirubinbilirubin levelslevels
waswas observedobserved, , andand HE HE improvedimproved significantlysignificantly in in comparisoncomparison to SMT.to SMT.
–– HoweverHowever, , nono survivalsurvival benefitbenefit couldcould bebe observedobserved in in thethe MARS group MARS group
Bañares R, Nevens F, Larsen FS et al. Extracorporeal liver support with the molecular adsorbent recirculating system
(MARS) in patients with acute-on-chronic liver failure. The RELIEF trial. J. Hepatol.52(S1),S459–S460 (2010).

L’expérience niçoise
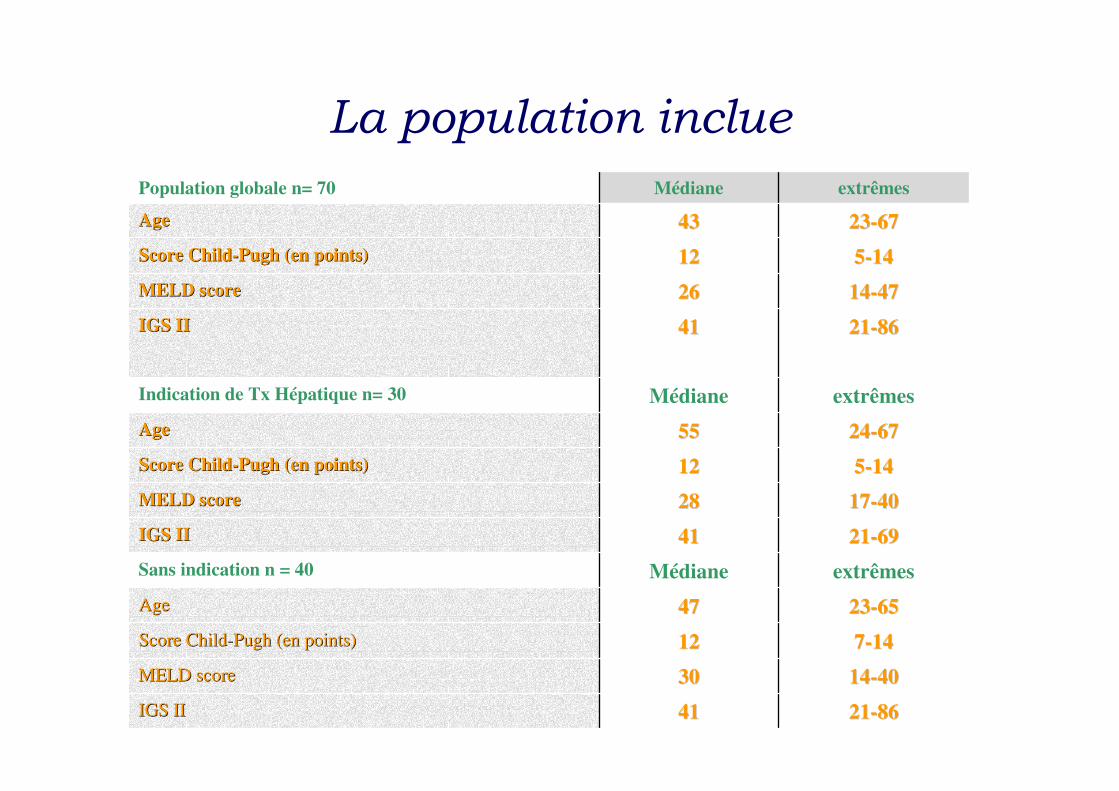
La population inclue
Population globale n= 70 Médiane extrêmes
AgeAge 4343 2323--6767
Score ChildScore Child--Pugh (en points)Pugh (en points) 1212 55--1414
MELD scoreMELD score 2626 1414--4747
IGS IIIGS II 4141 2121--8686
Indication de Tx Hépatique n= 30 Médiane extrêmes
AgeAge 5555 2424--6767
Score ChildScore Child--Pugh (en points)Pugh (en points) 1212 55--1414
MELD scoreMELD score 2828 1717--4040
IGS IIIGS II 4141 2121--6969
Sans indication n = 40 Médiane extrêmes
AgeAge 4747 2323--6565
Score ChildScore Child--Pugh (en points)Pugh (en points) 1212 77--1414
MELD scoreMELD score 3030 1414--4040
IGS IIIGS II 4141 2121--8686
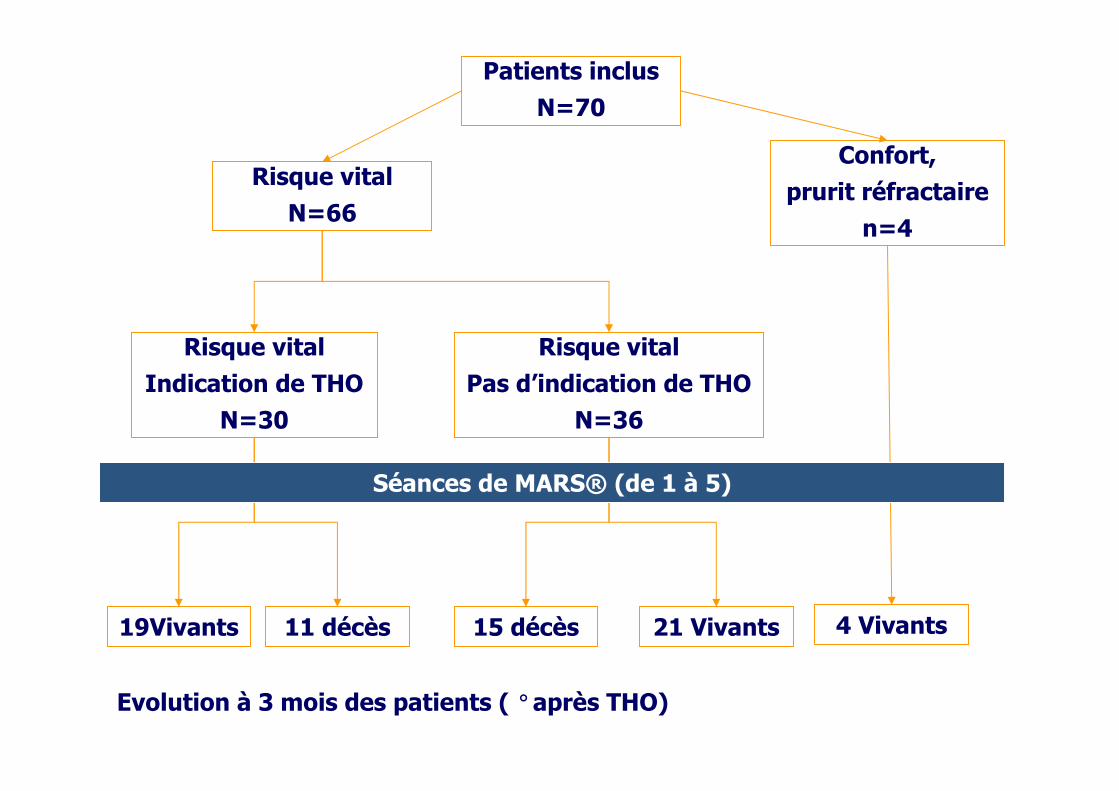
Patients inclus
N=70
Risque vital
N=66
Confort,
prurit réfractaire
n=4
Risque vital
Pas d’indication de THO
N=36
Risque vital
Indication de THO
N=30
19Vivants 11 décès 15 décès 21 Vivants 4 Vivants
Evolution à 3 mois des patients ( °après THO)
Séances de MARS® (de 1 à 5)

54
Conclusion
•• Insuffisance hInsuffisance héépatique Aigue: patique Aigue: gravitgravitéé--mortalitmortalitéé
•• TrtTrt de rde rééfféérence : rence : txtx hhéépatiquepatique
•• MAIS: MAIS:
–– PPéénurie de greffonnurie de greffon
–– Pas tous Pas tous ééligibleligible
•• Alternatives:Alternatives:
–– Ambitieuses: le Foie Ambitieuses: le Foie BioartificielBioartificiel
–– Raisonnables: Dialyse Raisonnables: Dialyse àà ll’’Albumine.Albumine.