Embed Size (px)
Citation preview
Mise à jour sur le traitement de l’infarctus et sur lesanti‐plaquettaires
Focus sur les indications de transfert pour angioplastie coronarienne et sur les inhibiteurs des récepteurs de l’ADP
Jean‐Pierre Déry, MD, MSc, FRCP(C)
Objectifs
Au terme de la conférence, le participant sera en mesure de :
• 1. Déterminer la place, les indications et la procédure de l’angioplastie rapide post‐thrombolyse.
• 2. Reconnaître les indications, la durée et la sécurité de la trithérapie anticoagulante post‐endoprothèse coronarienne.
• 3. Discuter de la controverse sur l’association des IPP avec le clopidogrel.
• 4. Discuter de la place des nouveaux antiplaquettaires oraux (prasugrel, ticagrelor) post‐endoprothèse coronarienne.
Conflits d’intérêt
• Subvention de recherche (>50,000$)– Eli Lilly Canada (prasugrel, abciximab)– Astra‐Zeneca (ticagrelor)
• Subventions de recherche (<50,000$)– Sanofi‐Aventis (clopidogrel)– BMS (clopidogrel)
• Advisory boards– Eli Lilly, Astra‐Zeneca, Sanofi‐Aventis
• Conférencier– Astra‐Zeneca, BMS, Sanofi‐Aventis
Plan
• Traitement de l’infarctus avec ↑ST– Qui et quand référer pour angioplastie primaire– Qui et quand référer post‐thrombolyse
• Traitement du patient en FA référé pour coro– Comment balancer les risques hémorragiques et ischémiques
• Non‐réponse au clopidogrel– Rôle des interactions médicamenteuses et des polymorphismes génétiques
• Nouveaux anti‐plaquettaires– Le clopidogrel a‐t‐il encore sa place?
Angioplastie primaire:Thrombolyse vs angioplastie primaire
• Points à prendre en considération:– Facteurs influençant l’efficacité de la thrombolyse
• Durée des symptômes• Localisation / étendue de l’infarctus • Choc cardiogénique
– Facteurs influençant la sécurité de la thrombolyse• Âge• Présence de contre‐indications relatives
– Délai du transfert• PCI‐related delay (door‐to‐balloon − door‐to‐needle)
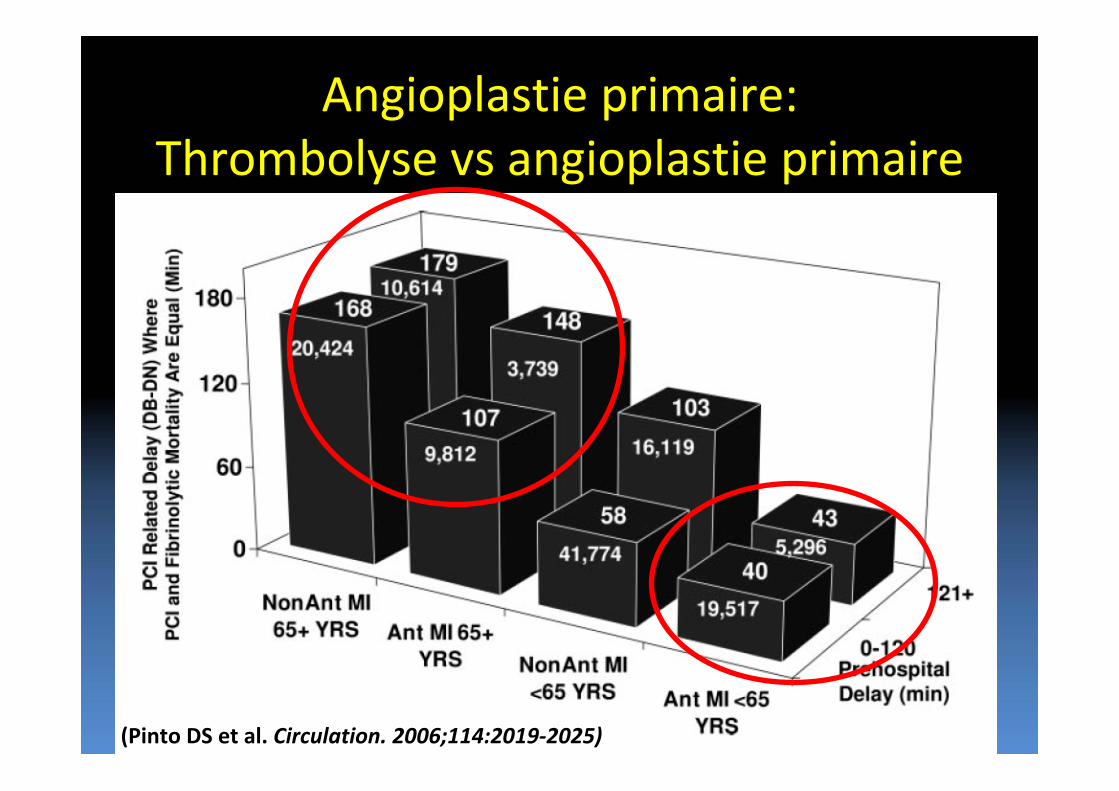
Angioplastie primaire:Thrombolyse vs angioplastie primaire
(Pinto DS et al. Circulation. 2006;114:2019‐2025)
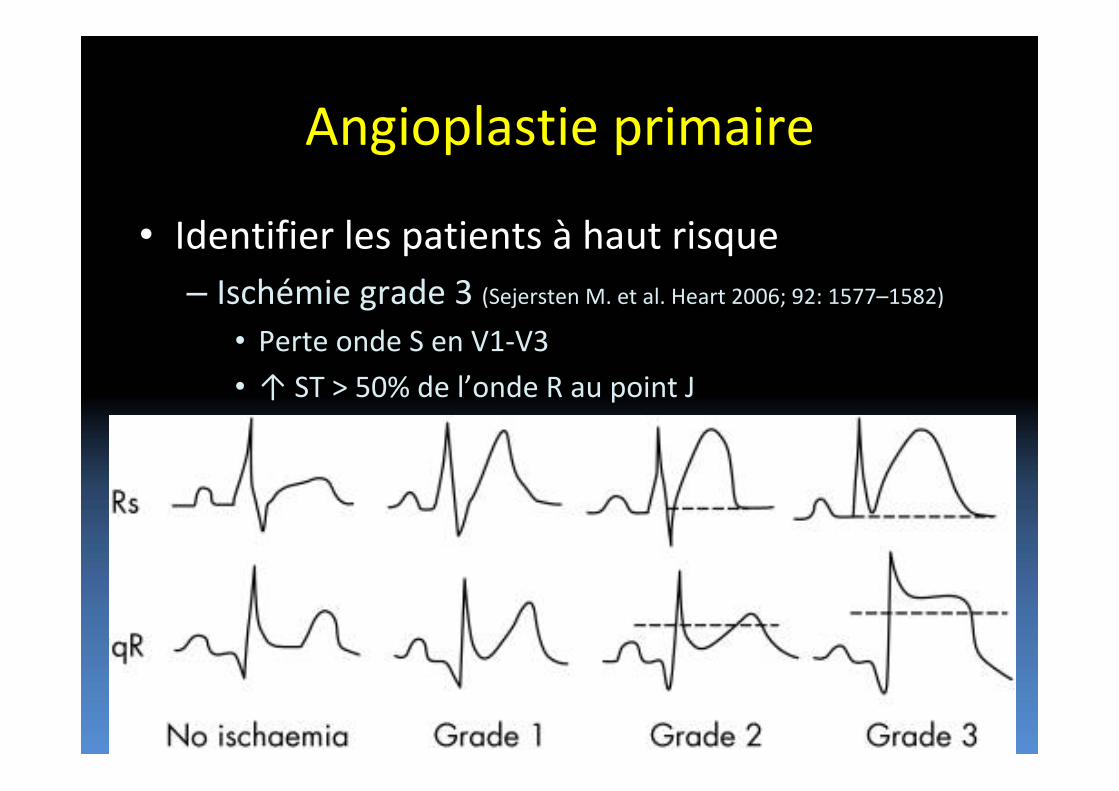
Angioplastie primaire
• Identifier les patients à haut risque– Ischémie grade 3 (Sejersten M. et al. Heart 2006; 92: 1577–1582)
• Perte onde S en V1‐V3
• ↑ ST > 50% de l’onde R au point J
Angioplastie primaire:Thrombolyse vs angioplastie primaire
• Symptômes < 3 heures– Si délai relatif à l’angioplastie < 60 min(distance < 30 min)
• Thrombolyse ou transfert– Si délai relatif à l’angioplastie > 60 min (distance > 30 min)
• Thrombolyse• Transfert si:
– Contre‐indication absolue à la thrombolyse– Choc cardiogénique– Diagnostic incertain– Contre‐indication relative à la thrombolyse etinfarctus peu étendu
Angioplastie primaire:Thrombolyse vs angioplastie primaire
• Symptômes ≥ 3 heures et < 12 heures– Si délai relatif à l’angioplastie < 60 min(distance < 30 min)
• Transfert– Si délai relatif à l’angioplastie > 60 min (distance > 30 min)
• Thrombolyse• Transfert si:
– Contre‐indication relative à la thrombolyse ouinfarctus peu étendu
– Contre‐indication absolue à la thrombolyse– Choc cardiogénique– Diagnostic incertain
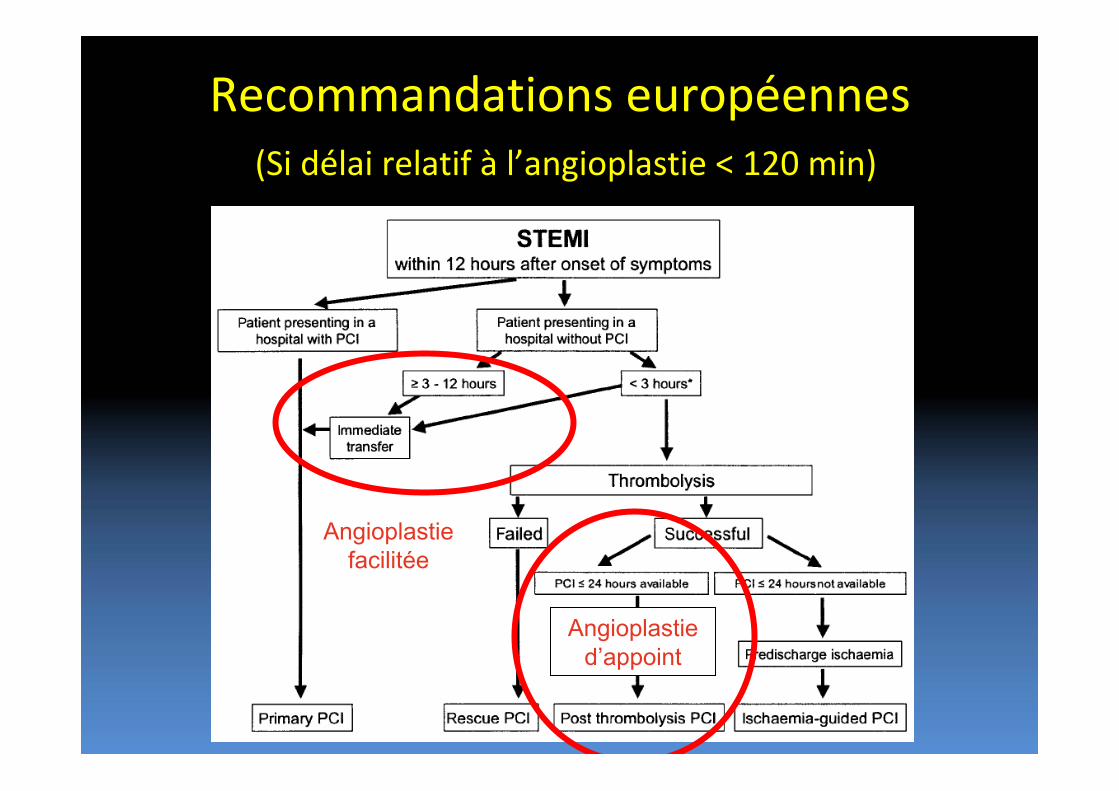
Recommandations européennes(Si délai relatif à l’angioplastie < 120 min)
Angioplastiefacilitée
Angioplastied’appoint

Angioplastie facilitée
• Définition:– Administration d’un médicament pendant le transport en vue de l’angioplastie primaire
• TNK: Pas d’avantage (ASSENT‐IV)
• Abciximab: Pas d’avantage (FINESSE)
Angioplastie d’appoint
• Définition:– Recours à l’angioplastie dans les heures suivant une thrombolyse réussie
– Nombreuses études• CAPITAL‐AMI (Ottawa)• WEST (Alberta)• TRANSFER‐AMI (Ontario)• CARESS‐in‐AMI• GRACE‐2• NORDISTEMI• SIAM‐3
Angioplastie d’appoint
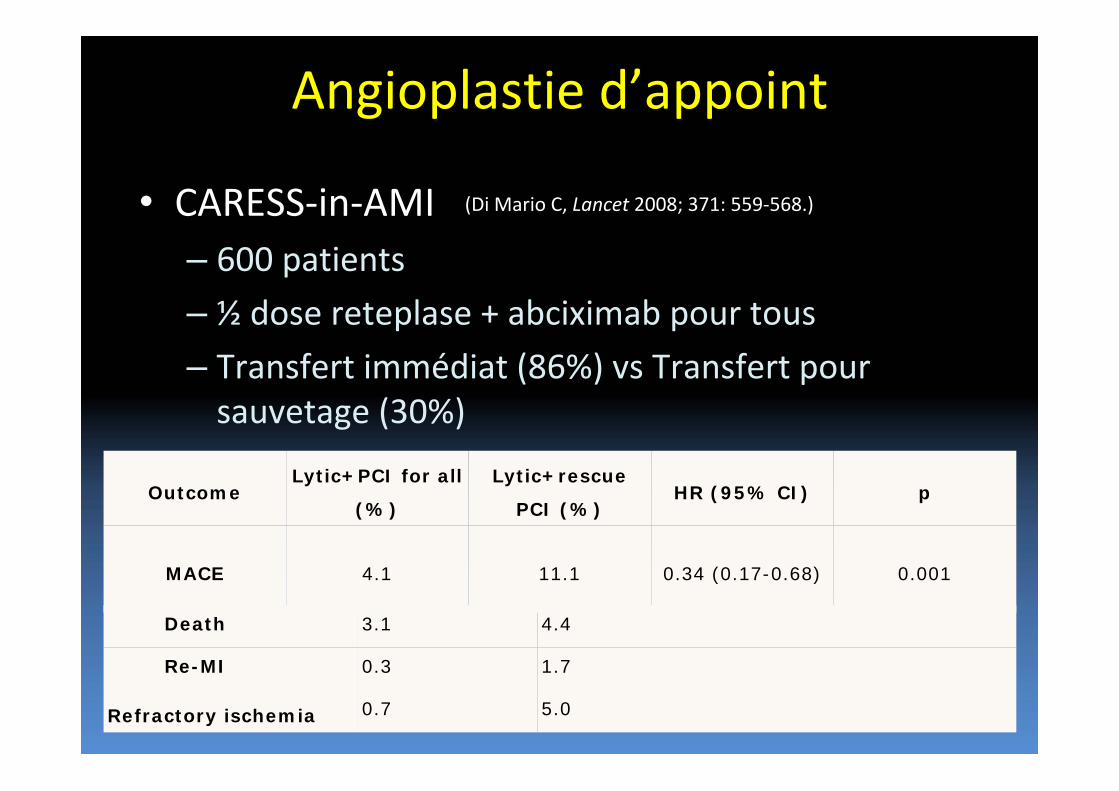
• CARESS‐in‐AMI– 600 patients
– ½ dose reteplase + abciximab pour tous
– Transfert immédiat (86%) vs Transfert pour sauvetage (30%)
OutcomeLytic+PCI for all
(%)
Lytic+rescue
PCI (%)HR (95% CI) p
MACE 4.1 11.1 0.34 (0.17-0.68) 0.001
Death 3.1 4.4
Re-MI 0.3 1.7
Refractory ischemia 0.7 5.0
(Di Mario C, Lancet 2008; 371: 559‐568.)
Angioplastie d’appoint
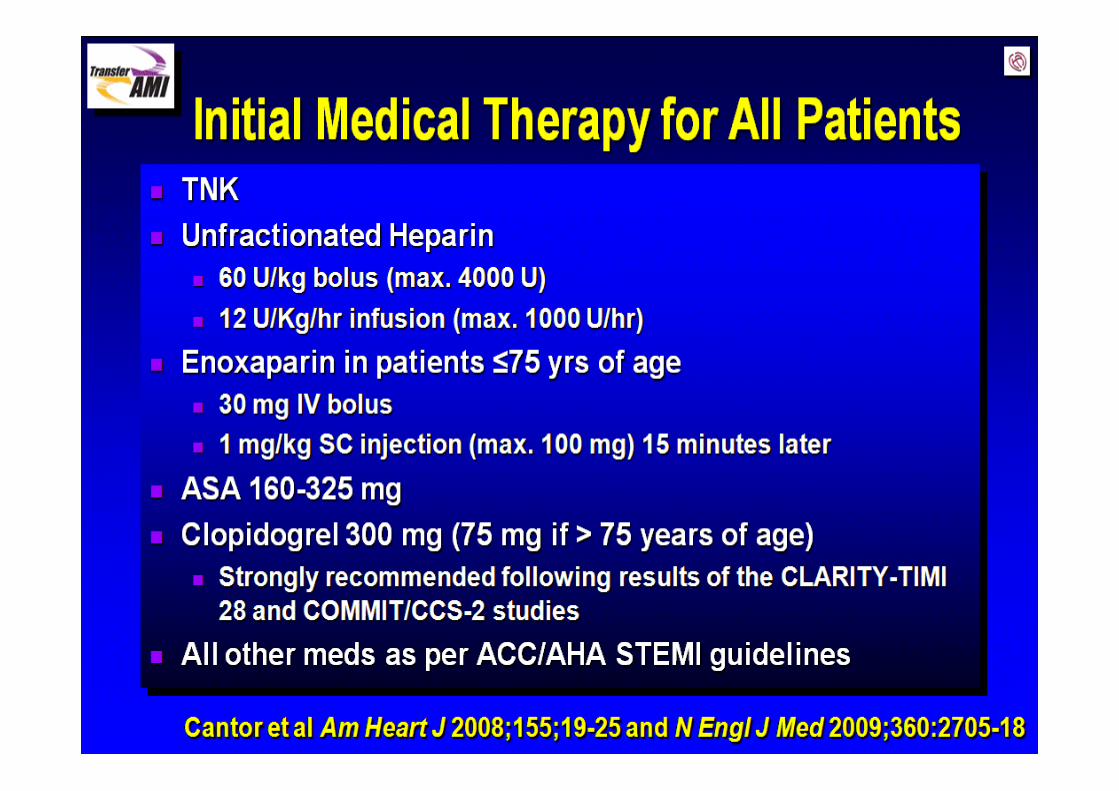
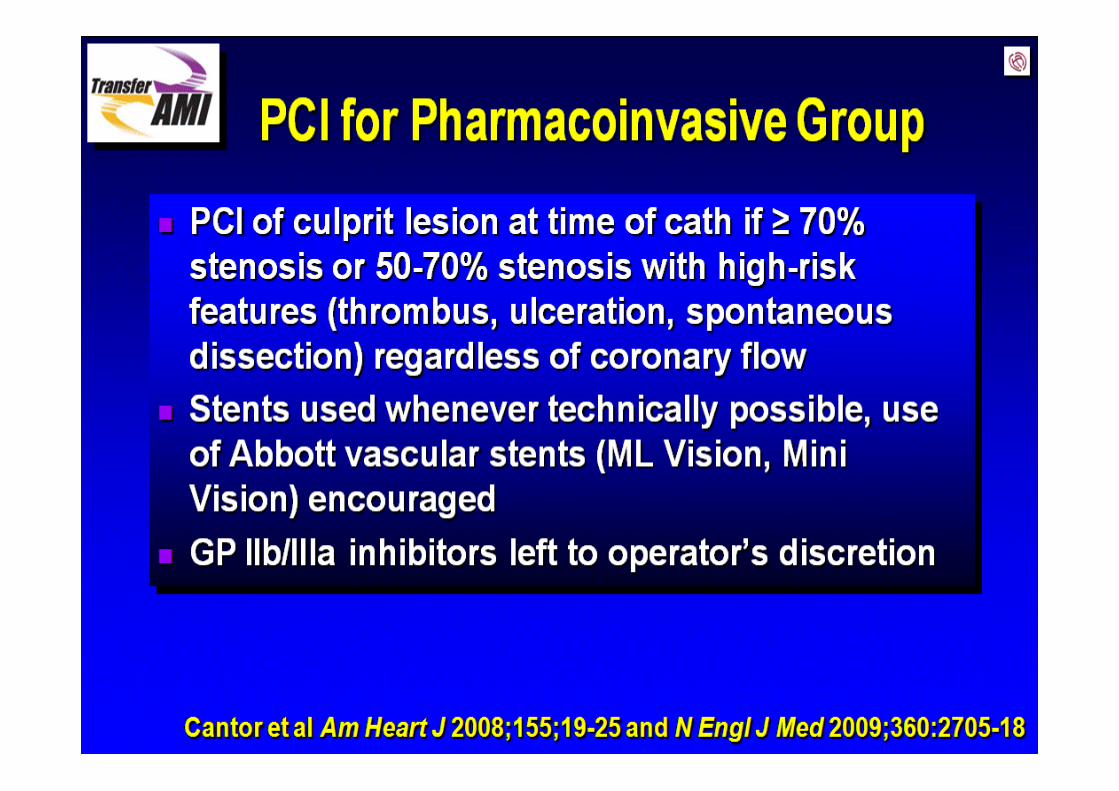
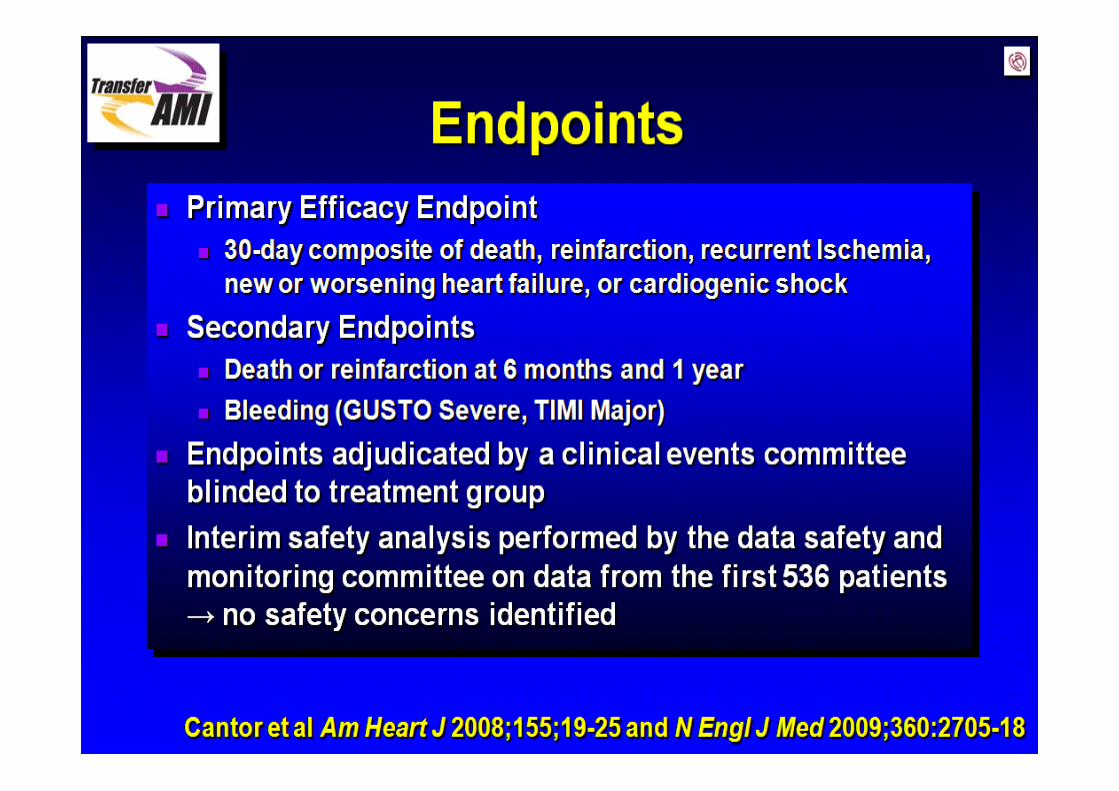
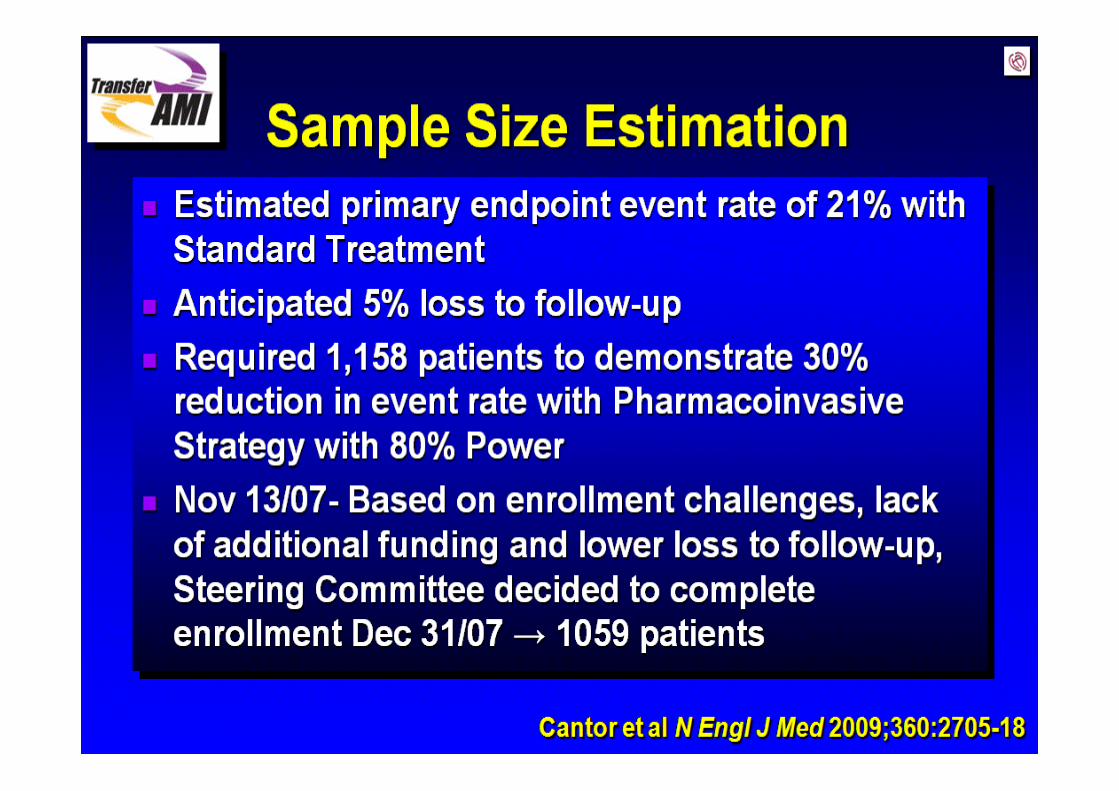
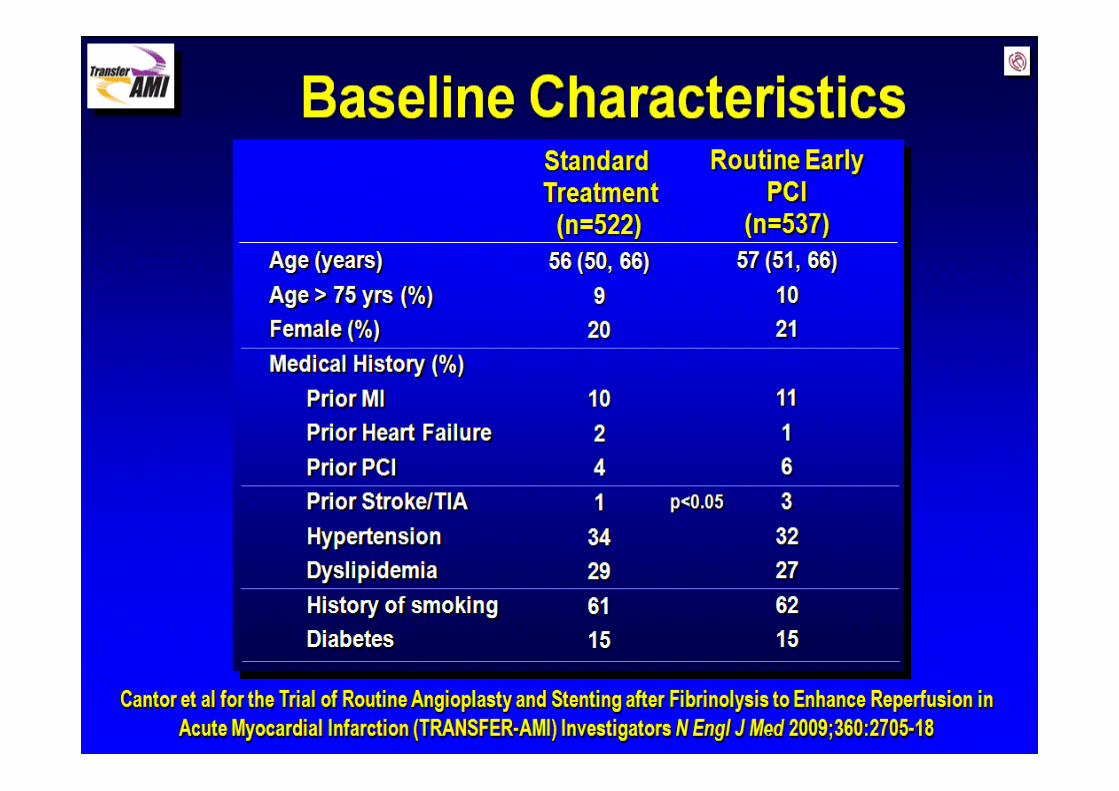
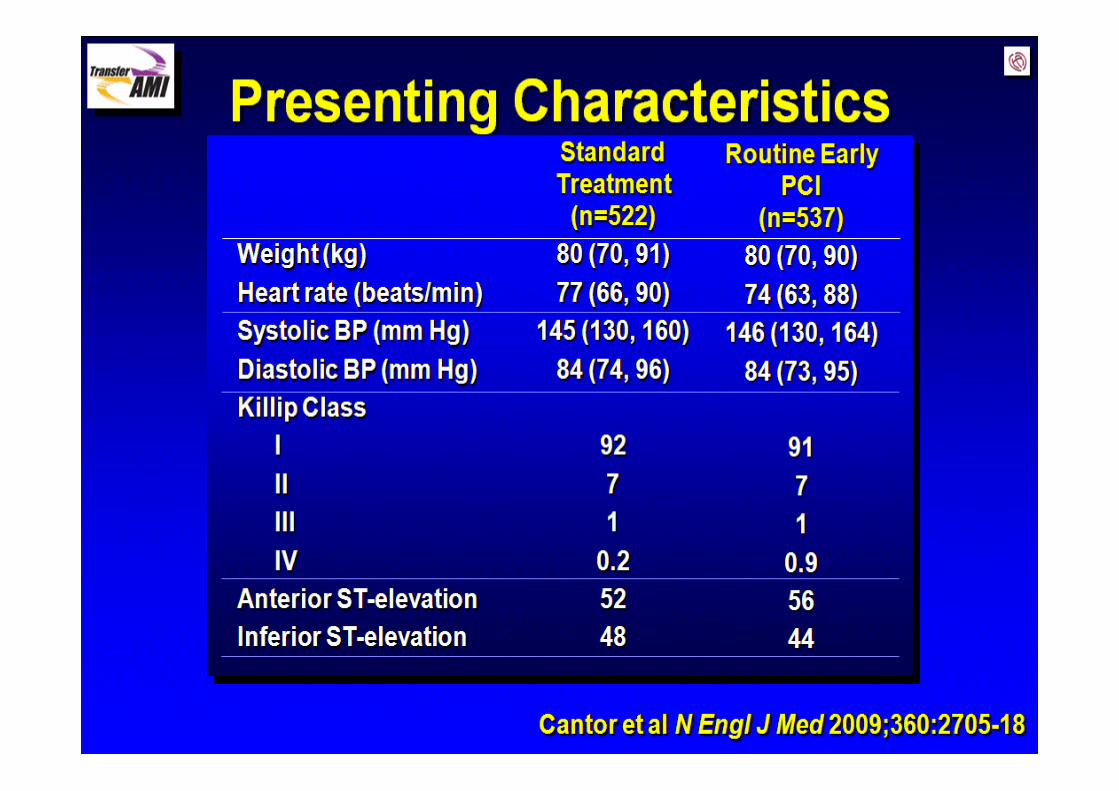
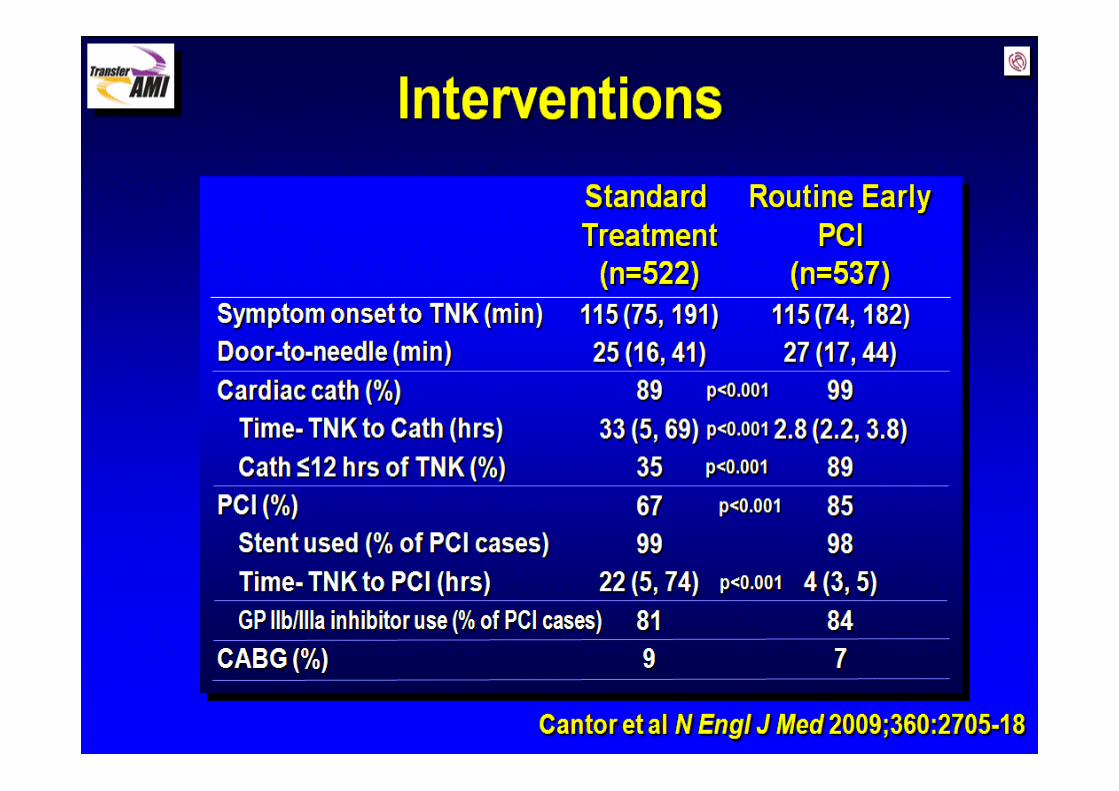
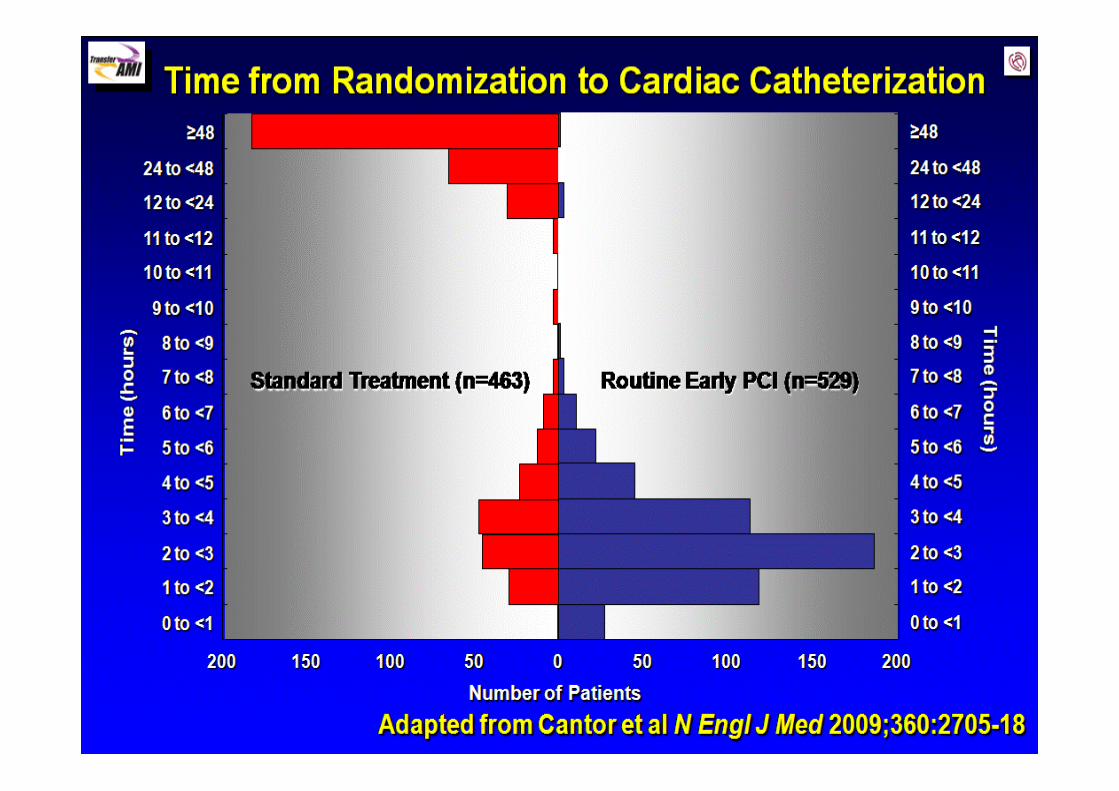
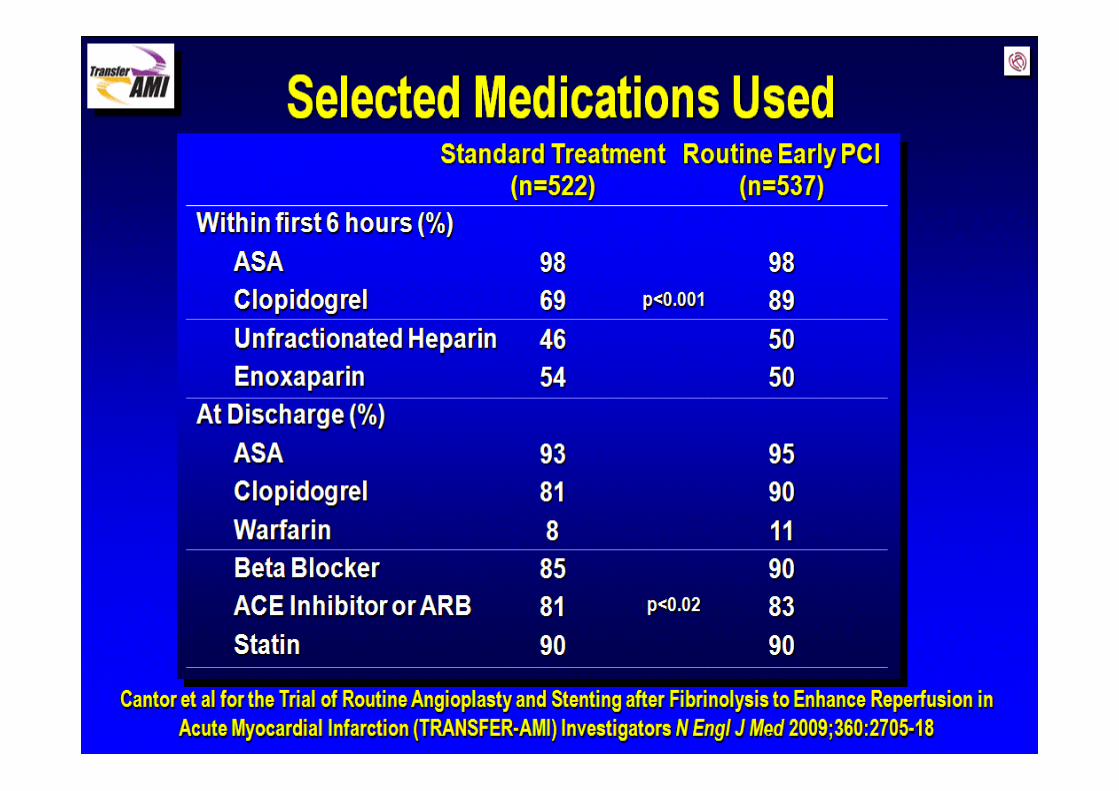
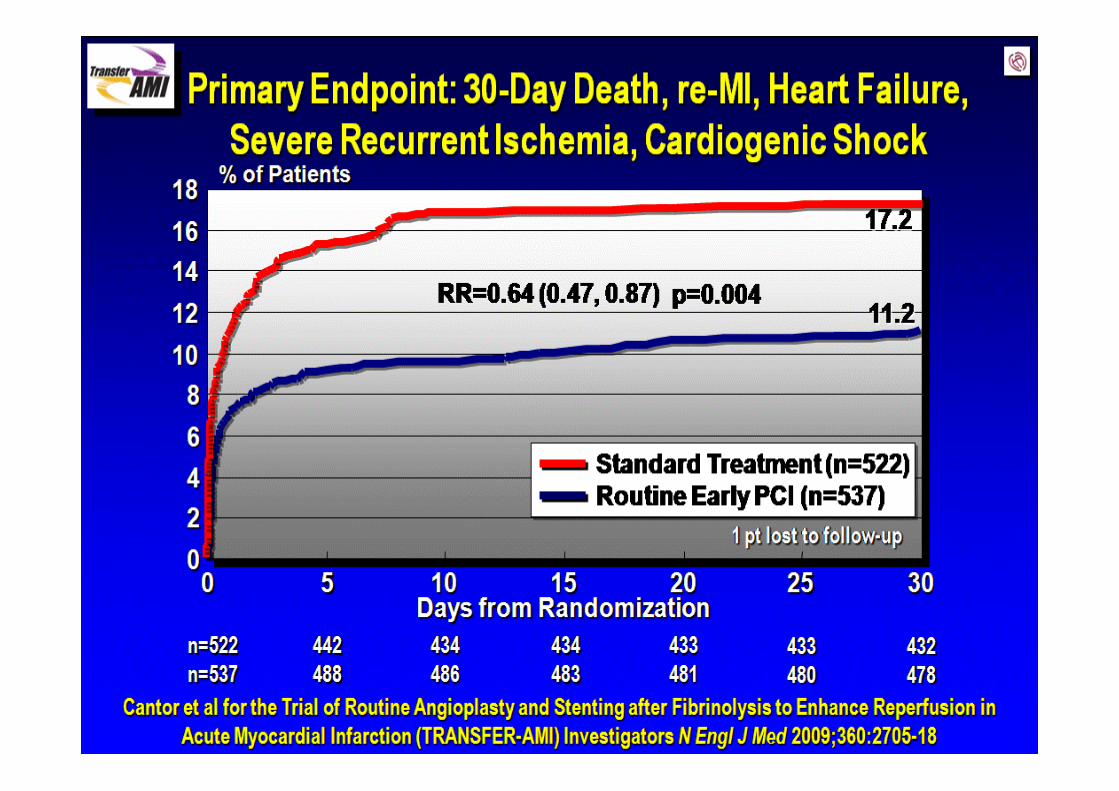
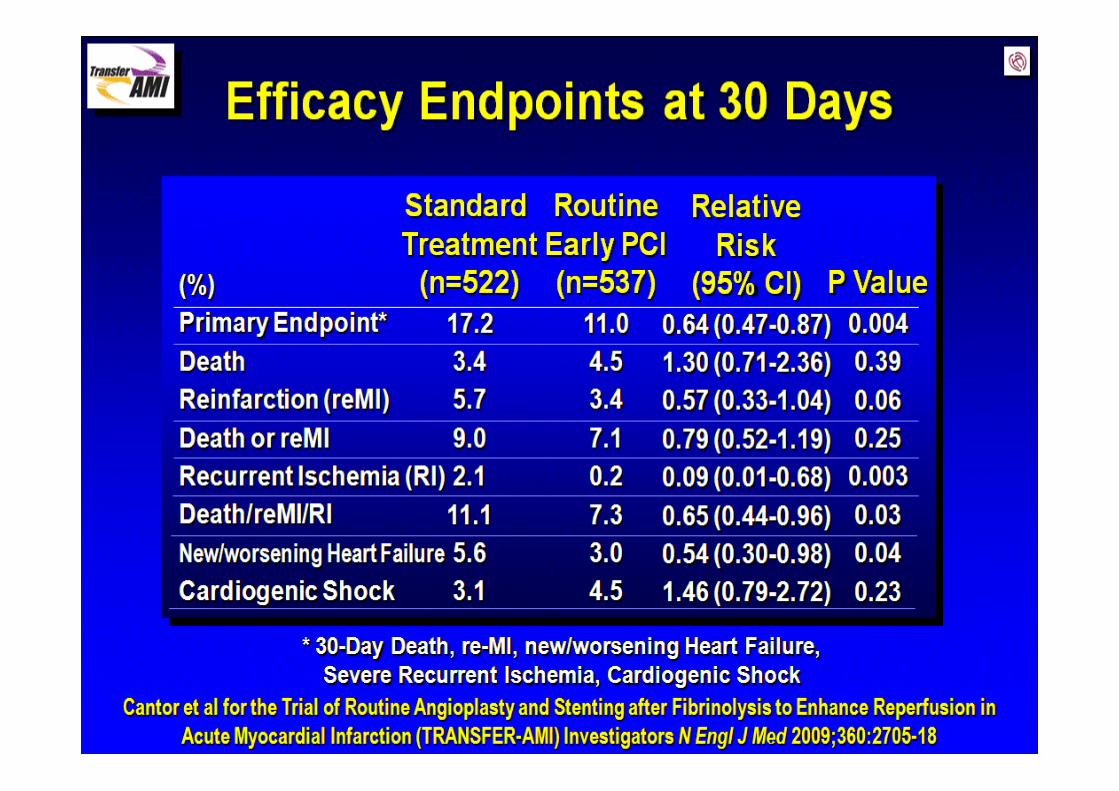
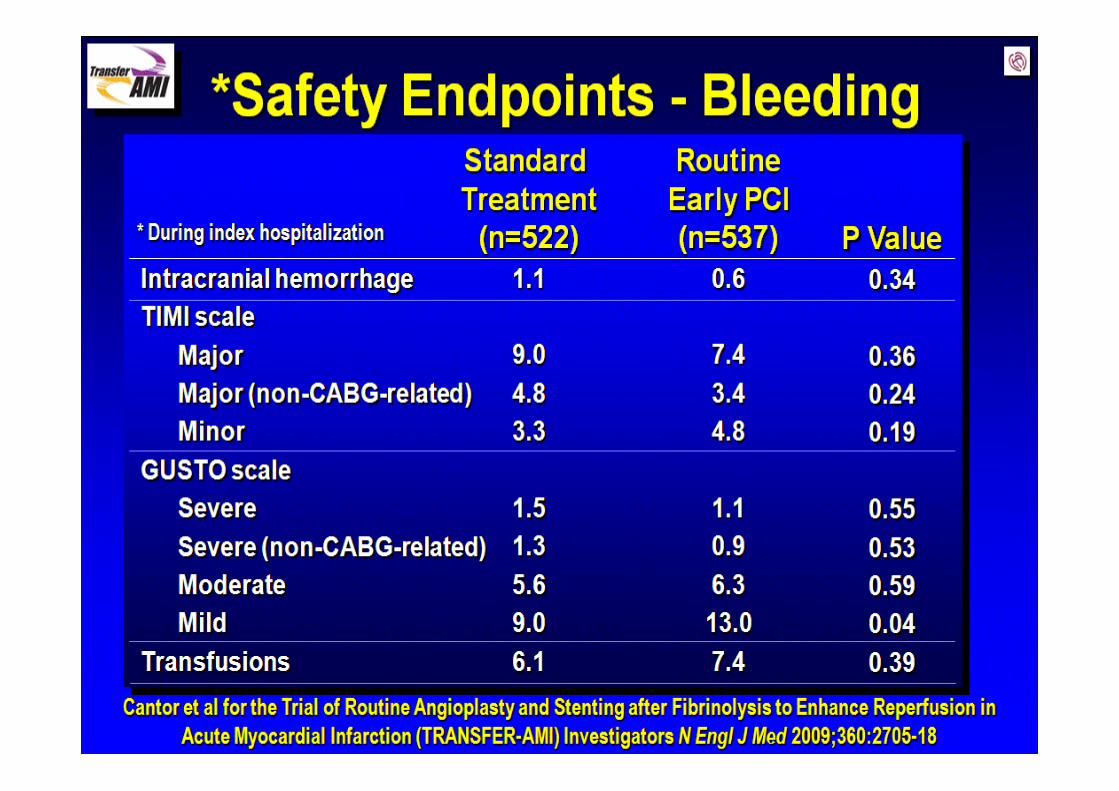
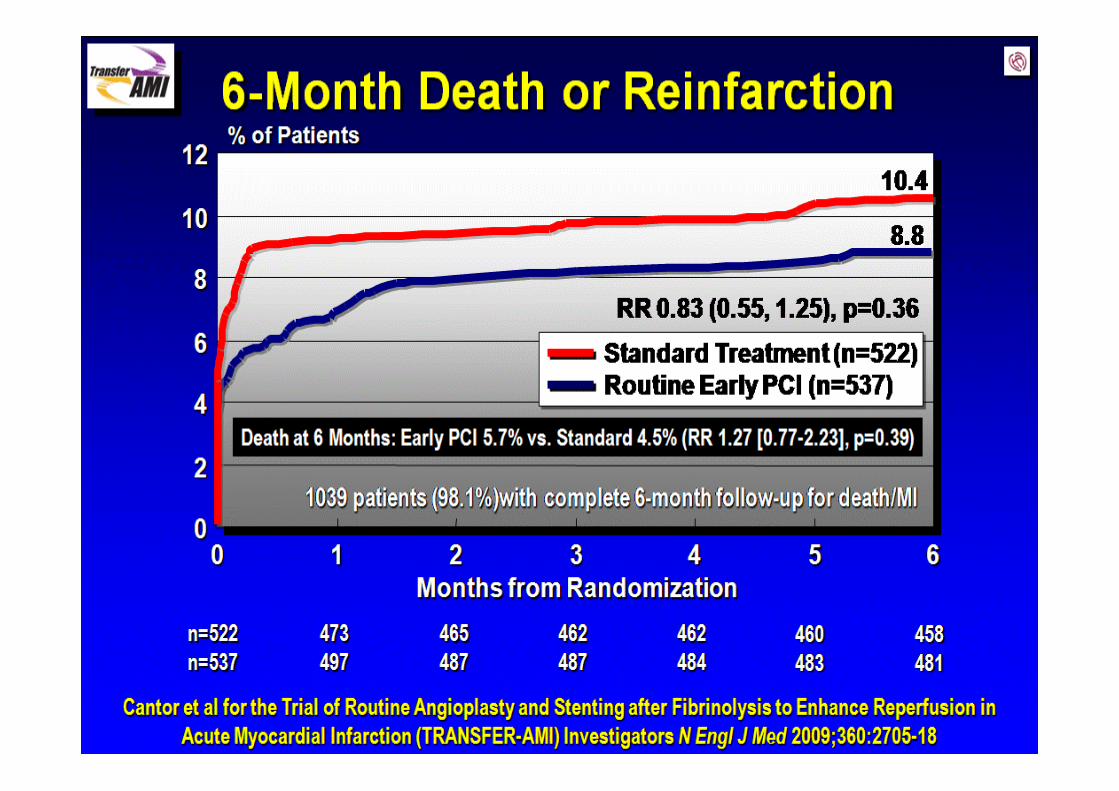
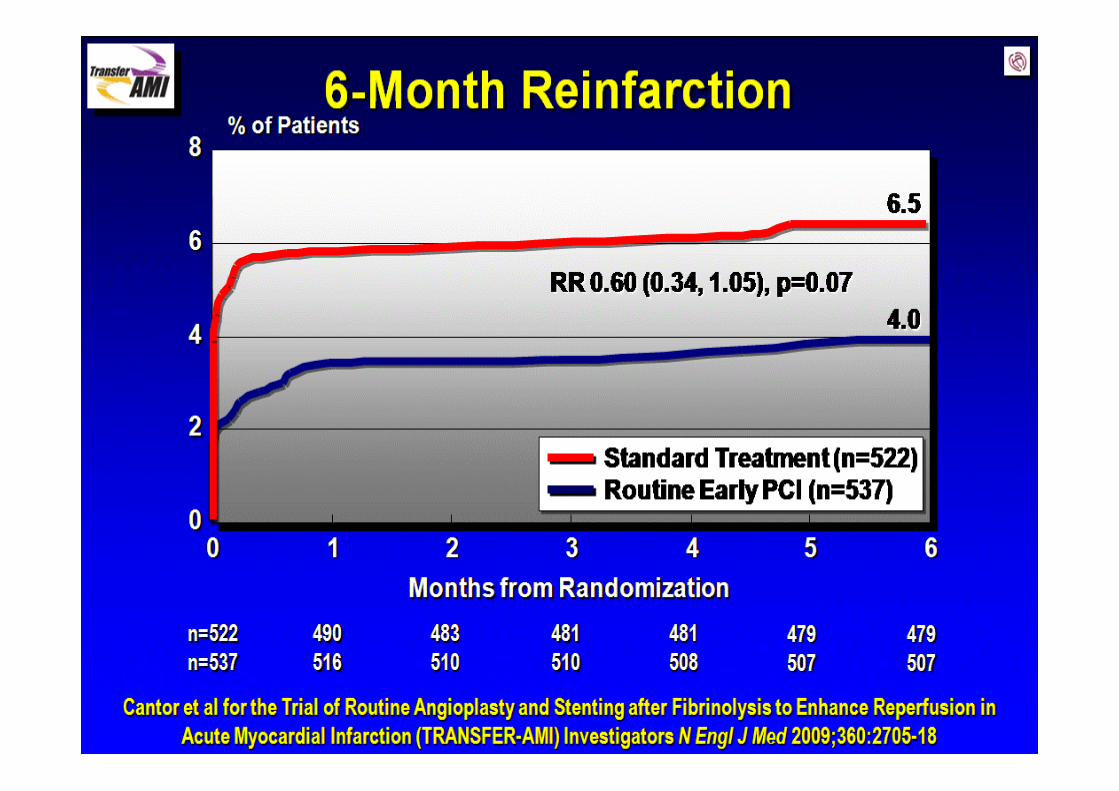
• TRANSFER‐AMI (Cantor W, et al. N Engl J Med 2009;360:2705‐18.)
– 1059 patients thrombolysés
– Randomisation:• Angioplastie < 6 heures (98,5% des pts)
• Angioplastie si indiquée (88,7% des pts)– Utilisation libérale si échec à la thrombolyse
• Site internet: www.chrc.net/TAMI
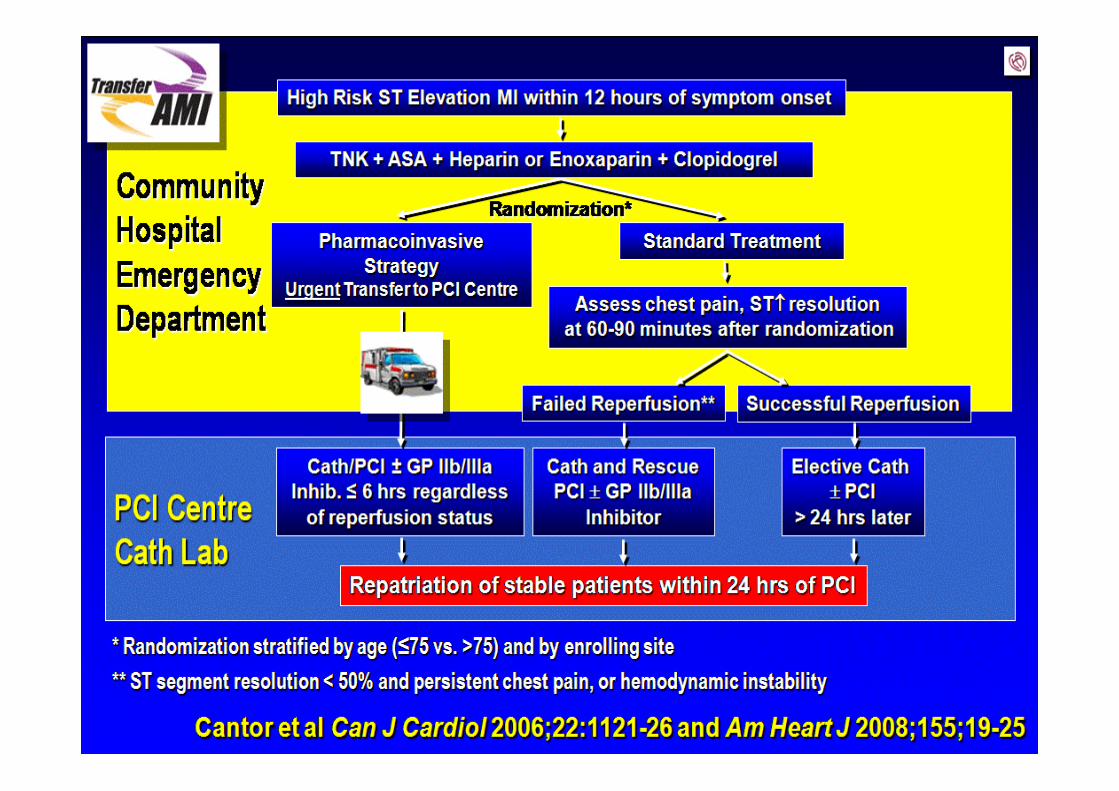

Angioplastie d’appointRecommandations
• Étant donné les problèmes logistiques d’un transfert immédiat, il est probablement préférable de:– Transférer immédiatement les patients à haut risque post‐thrombolyse (si PCI possible < 6h)
• Score TIMI / territoire étendu / Killip ≥ 2 / ischémie Gr 3
– Transférer pour sauvetage les patients qui n’ont pas reperfusé dans les 30‐60 min post‐thrombolyse
– Transférer tous les autres patients dans les 24‐48 heures
Angioplastie primaire et d’appoint
• Période de question
Traitement du patient en FA subissant une angioplastie coronarienne
• Recommandations européennes(Lip GY et al. Eur Heart J 2010;May 6)
– Faire le pont avec héparine augmente le risque de saignement au site d’accès artériel
– Il semble plus sécuritaire de procéder sans cesser l’anticoagulation plutôt que d’administrer l’héparine
– Favoriser l’accès radial
– Pas nécessaire d’administrer de l’héparine au moment de l’angioplastie si INR 2.0 – 3.0
– Il faut prétraiter avec ASA et clopidogrel
– GP2b3a ne devraient pas être administrés
Traitement du patient en FA subissant une angioplastie coronarienne
• Recommandations européennes(Lip GY et al. Eur Heart J 2010;May 6)
– ASA + coumadin = pas suffisant contre la thrombose de tuteur
– ASA + clopidogrel = pas suffisant pour FA
– La triple thérapie est associée à un risque accru de saignement• ↑ de 3‐8x selon les études
– Un IPP devrait être administré et l’INR visé entre 2.0 et 2.5
– Les tuteurs pharmacoactifs devraient être utilisés seulement si une thérapie alternative (tuteurs non‐pharmacoactifs, pontages, traitement médical) ne peut être envisagée.
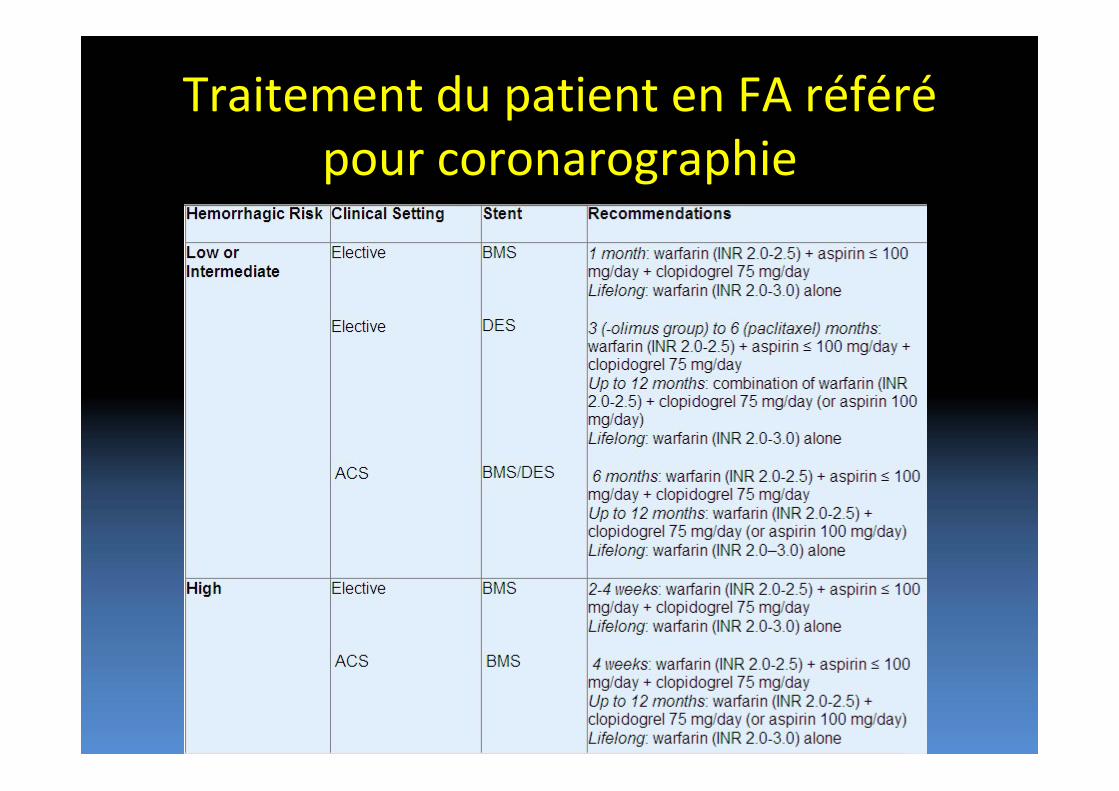
Traitement du patient en FA référépour coronarographie
Triple thérapie antithrombotique
• Période de question
• Autres références:– Zinn A. Am J Cardiol. 2009 Sep 7;104(5 Suppl):49C‐54C.
– Pasceri et al. Catheter Cardiovasc Interv. 2010 May 1;75(6):936‐42

Résistance au clopidogrel
• Variabilité interindividuelle de la réponse au clopidogrel– Facteurs génétiques et
– Interactions médicamenteuses• Focus sur les inhibiteurs de la pompe à proton (IPP)
Méthodes d’analyse de l’efficacité du clopidogrel
‐ Gold standard:
‐ Mesures de l’agrégation plaquettaire par agrégométrie optique (light transmittance aggregometry) (ou par impédance)‐ Mesures:
‐ RPA (residual platelet aggregation)
‐ IPA (% inhibition of platelet aggregation)
‐ Autres méthodes spécifiques aux inhibiteurs de l’ADP:
‐ VASP (vasodilator stimulated phosphoprotein)‐ Mesure:
‐ PRI (platelet reactivity index)
‐ VerifyNow point‐of‐care assay ‐ Mesure: rectivité plaq. résiduelle (RPR)
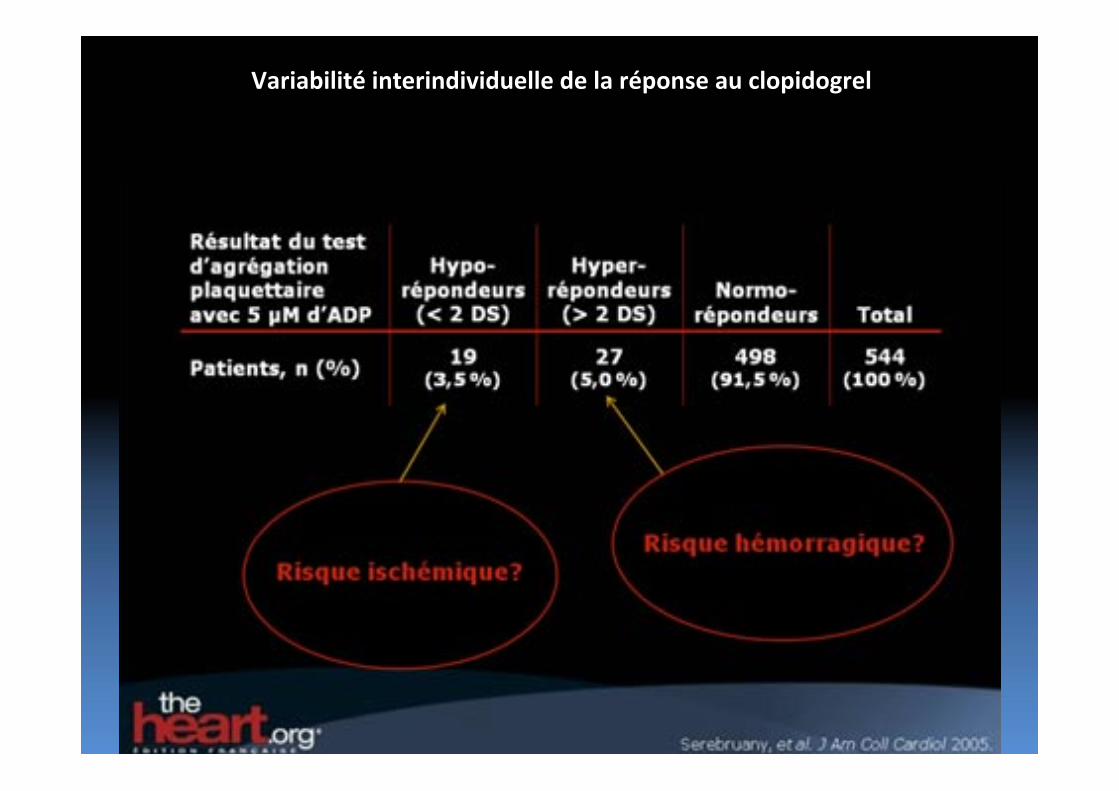
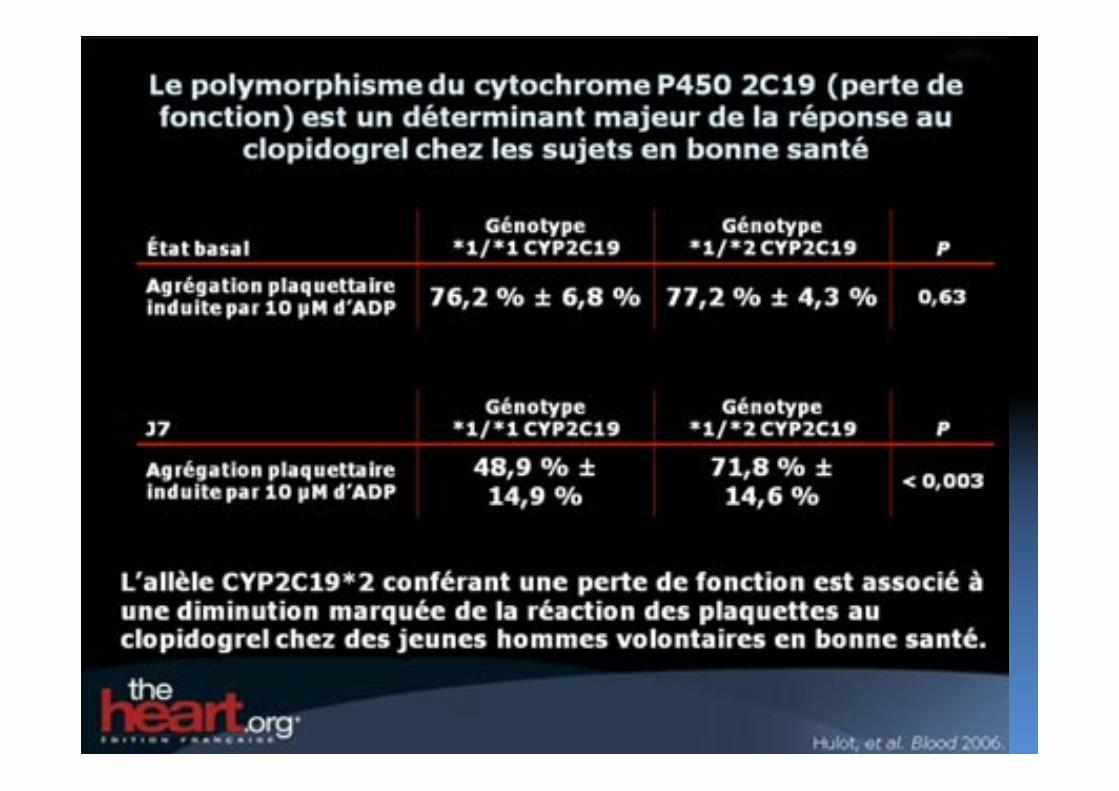
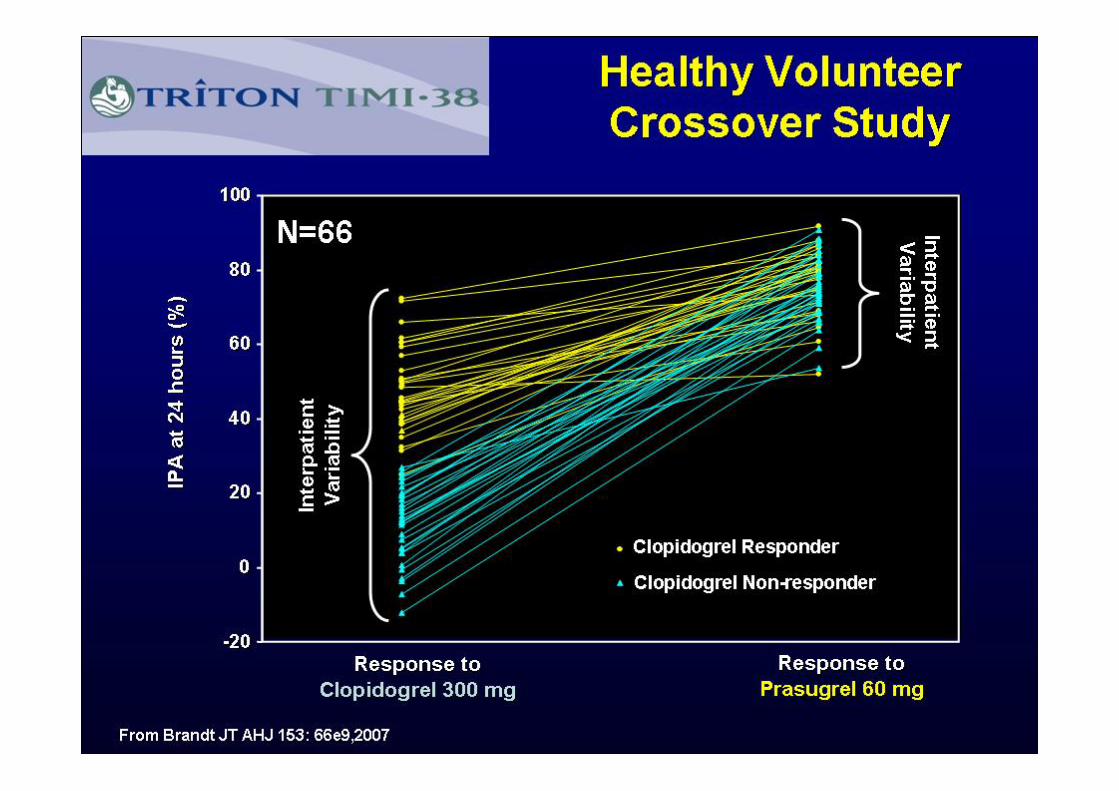
Variabilité interindividuelle de la réponse au clopidogrel
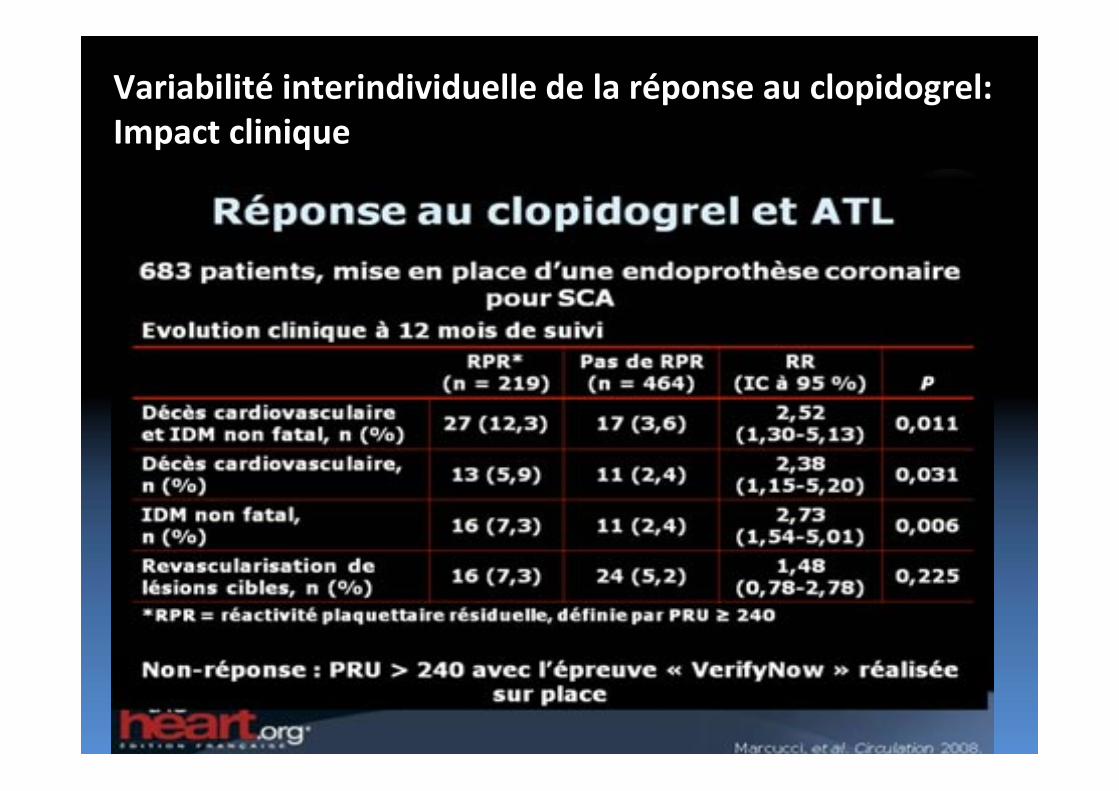
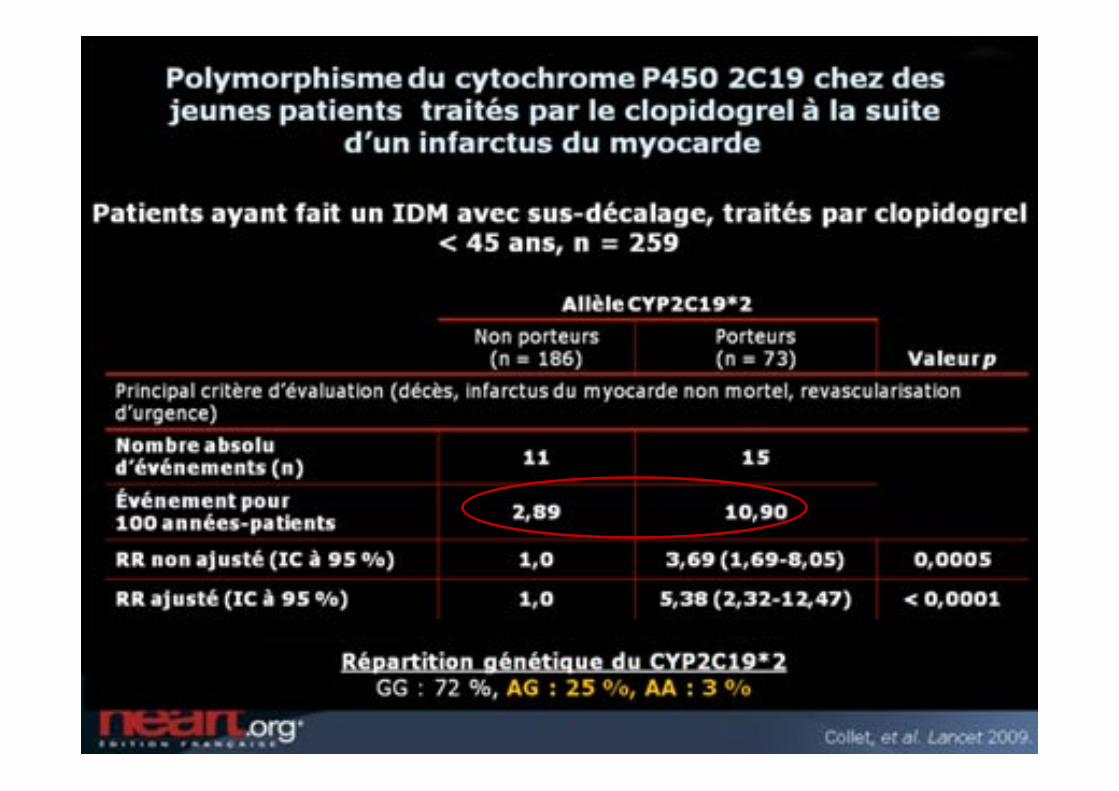
Variabilité interindividuelle de la réponse au clopidogrel:Impact clinique
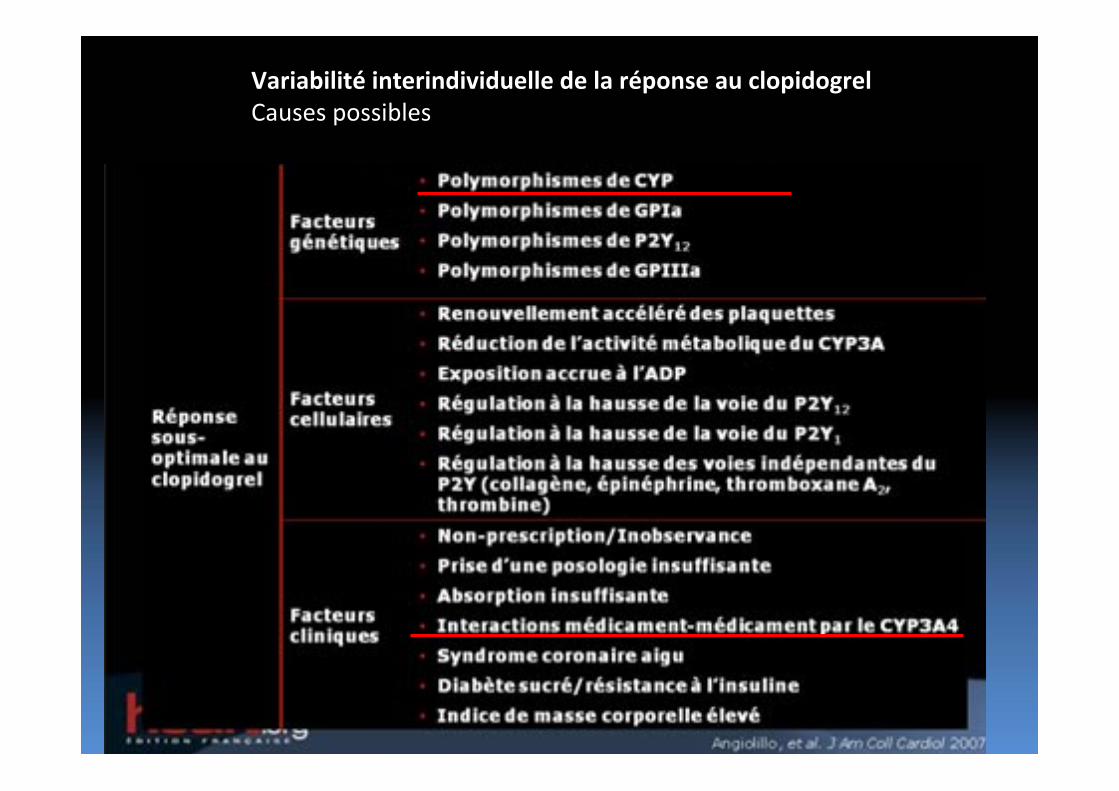
Variabilité interindividuelle de la réponse au clopidogrelCauses possibles
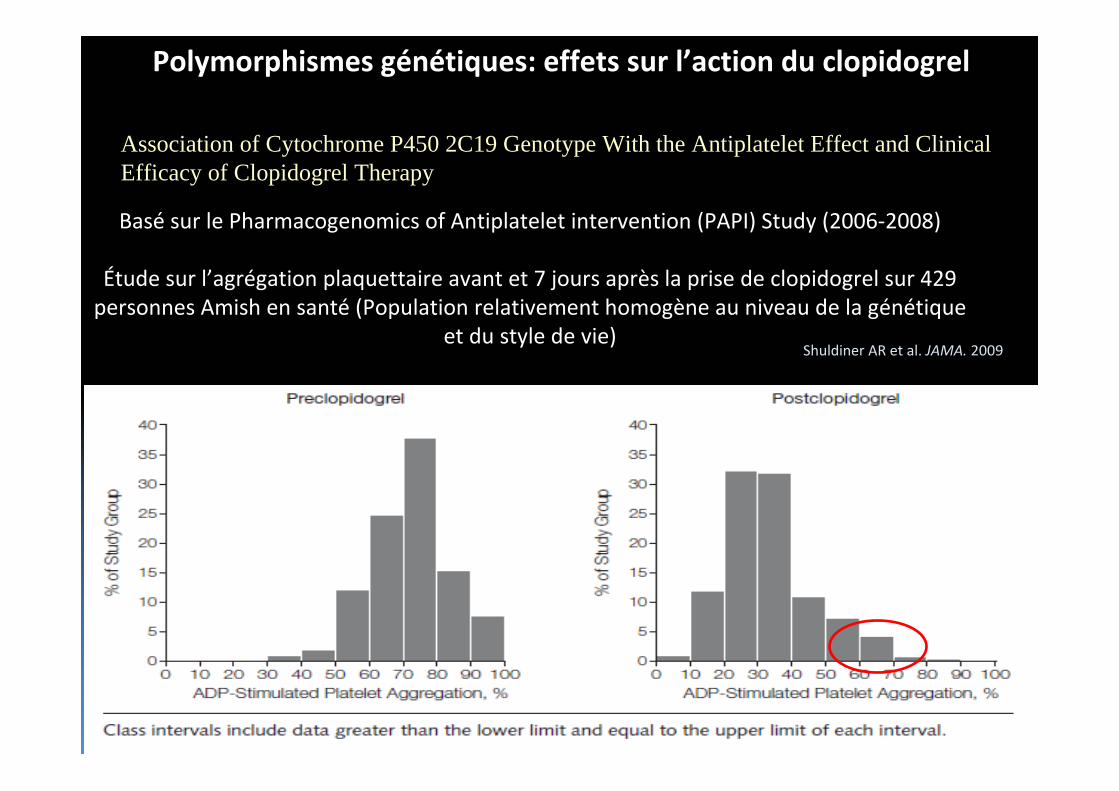
Polymorphismes génétiques: effets sur l’action du clopidogrel
Association of Cytochrome P450 2C19 Genotype With the Antiplatelet Effect and Clinical Efficacy of Clopidogrel Therapy
Shuldiner AR et al. JAMA. 2009
Basé sur le Pharmacogenomics of Antiplatelet intervention (PAPI) Study (2006‐2008)
Étude sur l’agrégation plaquettaire avant et 7 jours après la prise de clopidogrel sur 429 personnes Amish en santé (Population relativement homogène au niveau de la génétique
et du style de vie)
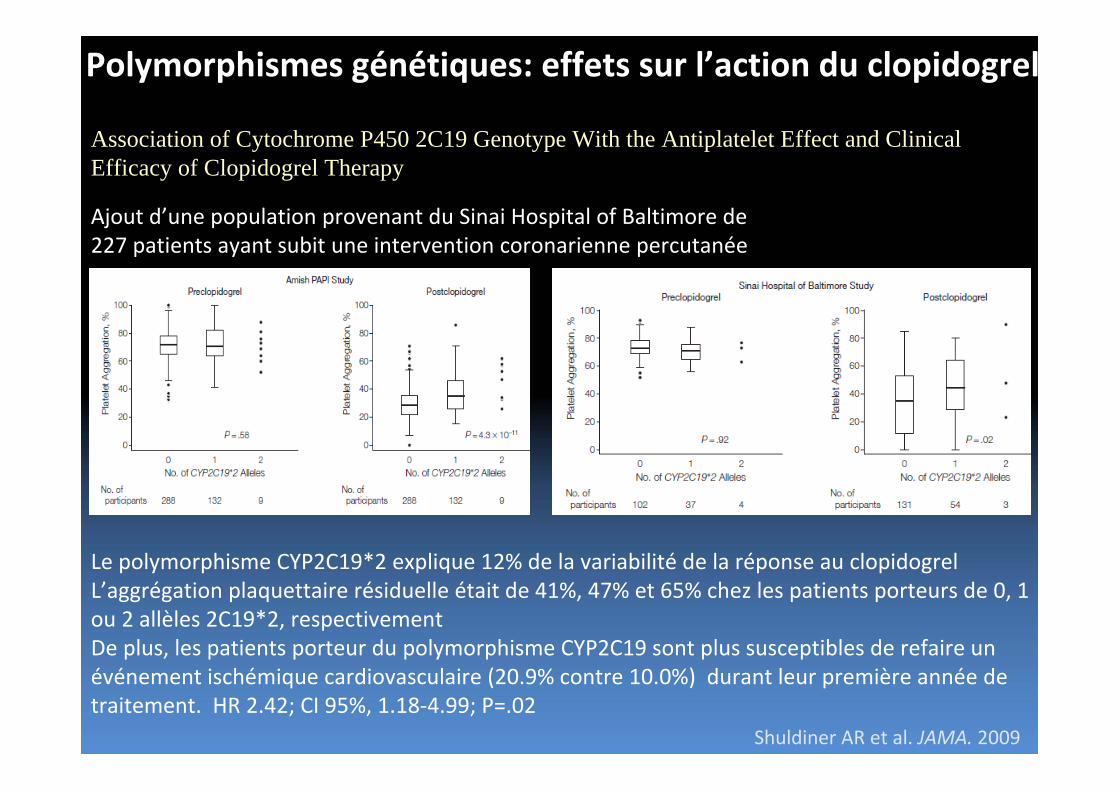
Polymorphismes génétiques: effets sur l’action du clopidogrel
Association of Cytochrome P450 2C19 Genotype With the Antiplatelet Effect and Clinical Efficacy of Clopidogrel Therapy
Ajout d’une population provenant du Sinai Hospital of Baltimore de227 patients ayant subit une intervention coronarienne percutanée
Le polymorphisme CYP2C19*2 explique 12% de la variabilité de la réponse au clopidogrelL’aggrégation plaquettaire résiduelle était de 41%, 47% et 65% chez les patients porteurs de 0, 1 ou 2 allèles 2C19*2, respectivementDe plus, les patients porteur du polymorphisme CYP2C19 sont plus susceptibles de refaire un événement ischémique cardiovasculaire (20.9% contre 10.0%) durant leur première année de traitement. HR 2.42; CI 95%, 1.18‐4.99; P=.02
Shuldiner AR et al. JAMA. 2009
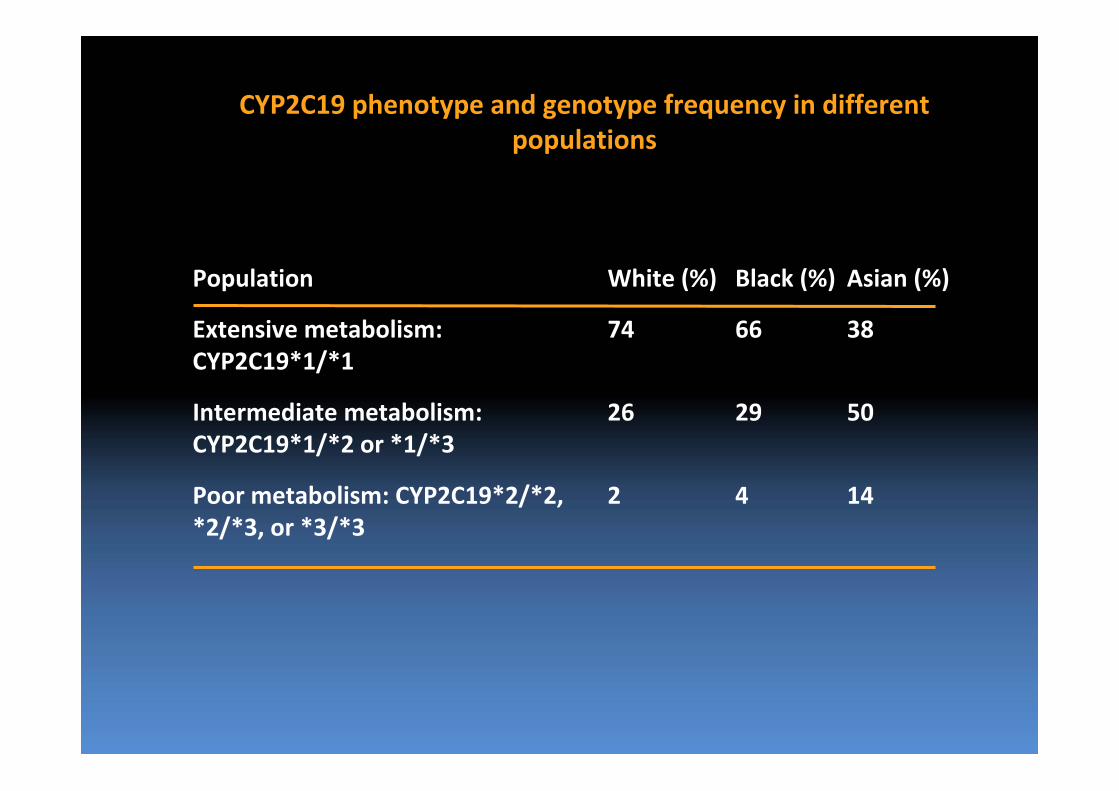
Population White (%) Black (%) Asian (%)
Extensive metabolism: CYP2C19*1/*1
74 66 38
Intermediate metabolism: CYP2C19*1/*2 or *1/*3
26 29 50
Poor metabolism: CYP2C19*2/*2, *2/*3, or *3/*3
2 4 14
CYP2C19 phenotype and genotype frequency in different populations
Clopidogrel et polymorphismes
• 30% de la population est porteuse d’une allèle occasionnant une réduction de la biotransformation du clopidogrel– Associé à une augmentation (2x) d’événements cliniques
• 2C19*2 = 25‐30%• 2C9*3 = 10%• 2B6 = 10%• 2C19*3 = 1‐25 % selon l’ethnie
• 40% de la population serait porteuse d’une allèle associée àune bio‐transformation accrue du clopidogrel– Associé à un risque hémorragique accru
• 2C19*17
• Les polymorphismes ne semblent expliquer que 12% de la variabilité au clopidogrel
Clopidogrel et polymorphisme
• Période de question
Interactions médicamenteuses
• Interactions suggérées et/ou prouvées– IPP
– BCC
– Certaines statines
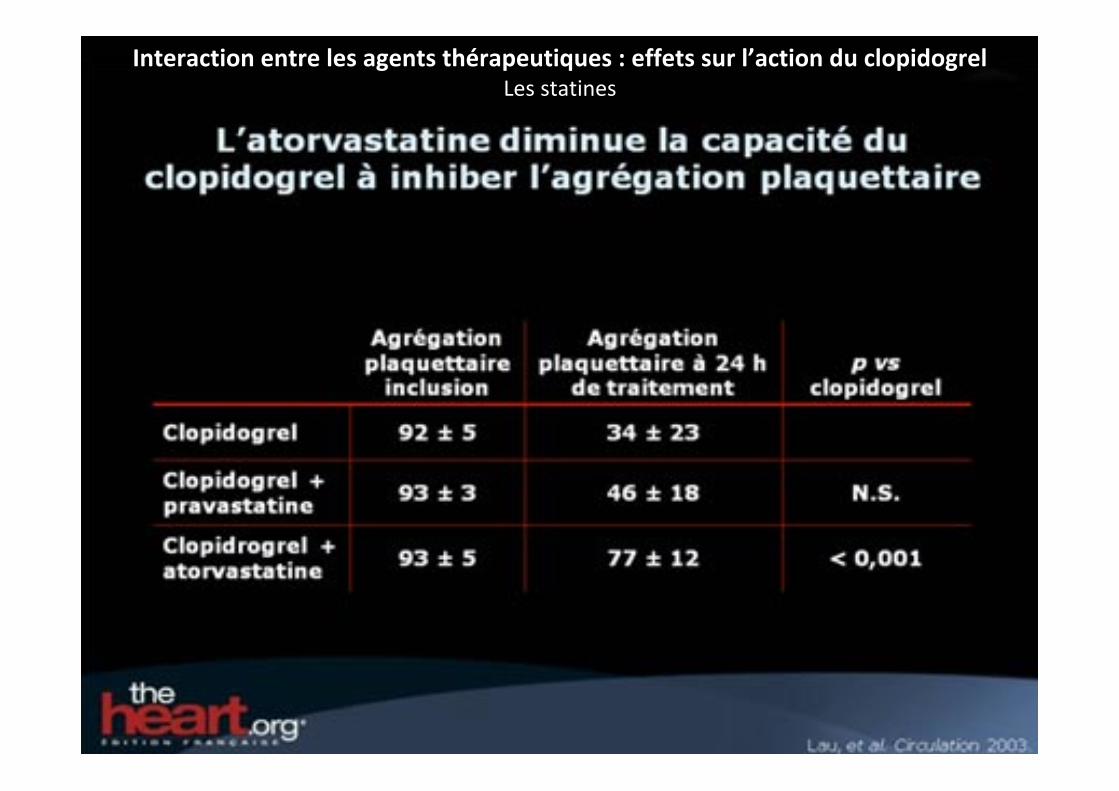
Interaction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes statines
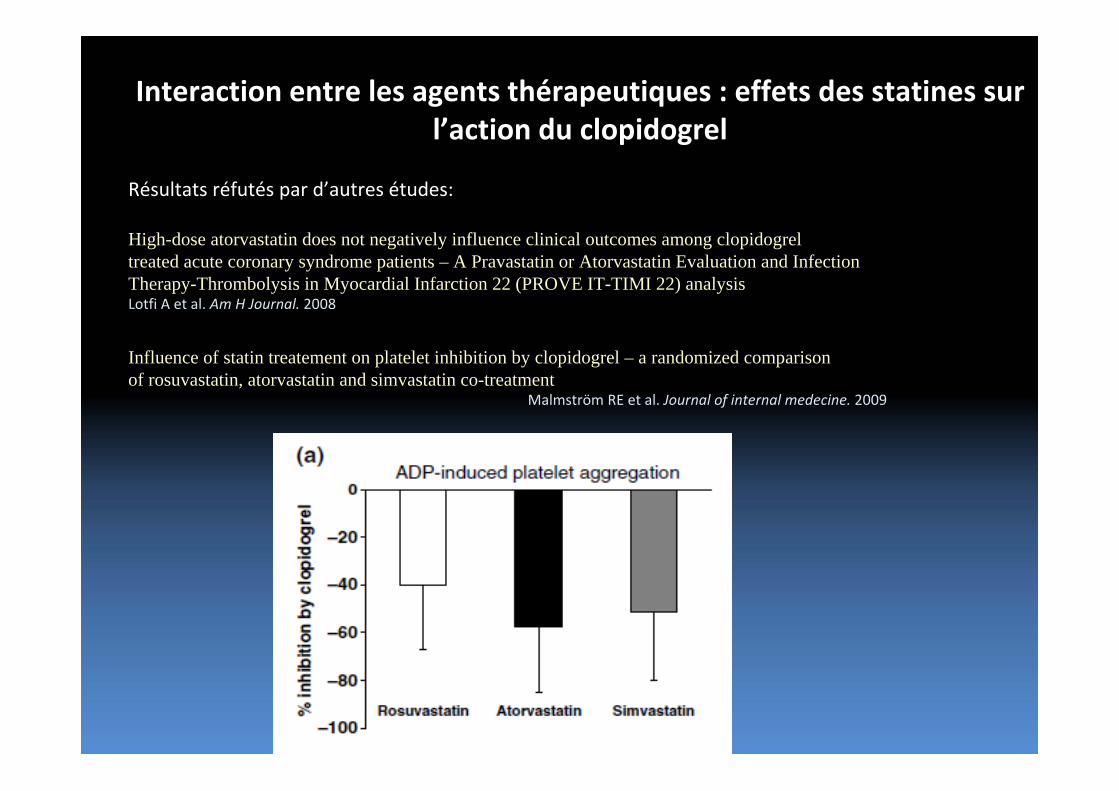
Interaction entre les agents thérapeutiques : effets des statines sur l’action du clopidogrel
Résultats réfutés par d’autres études:
High-dose atorvastatin does not negatively influence clinical outcomes among clopidogrel treated acute coronary syndrome patients – A Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT-TIMI 22) analysisLotfi A et al. Am H Journal. 2008
Influence of statin treatement on platelet inhibition by clopidogrel – a randomized comparison of rosuvastatin, atorvastatin and simvastatin co-treatment
Malmström RE et al. Journal of internal medecine. 2009
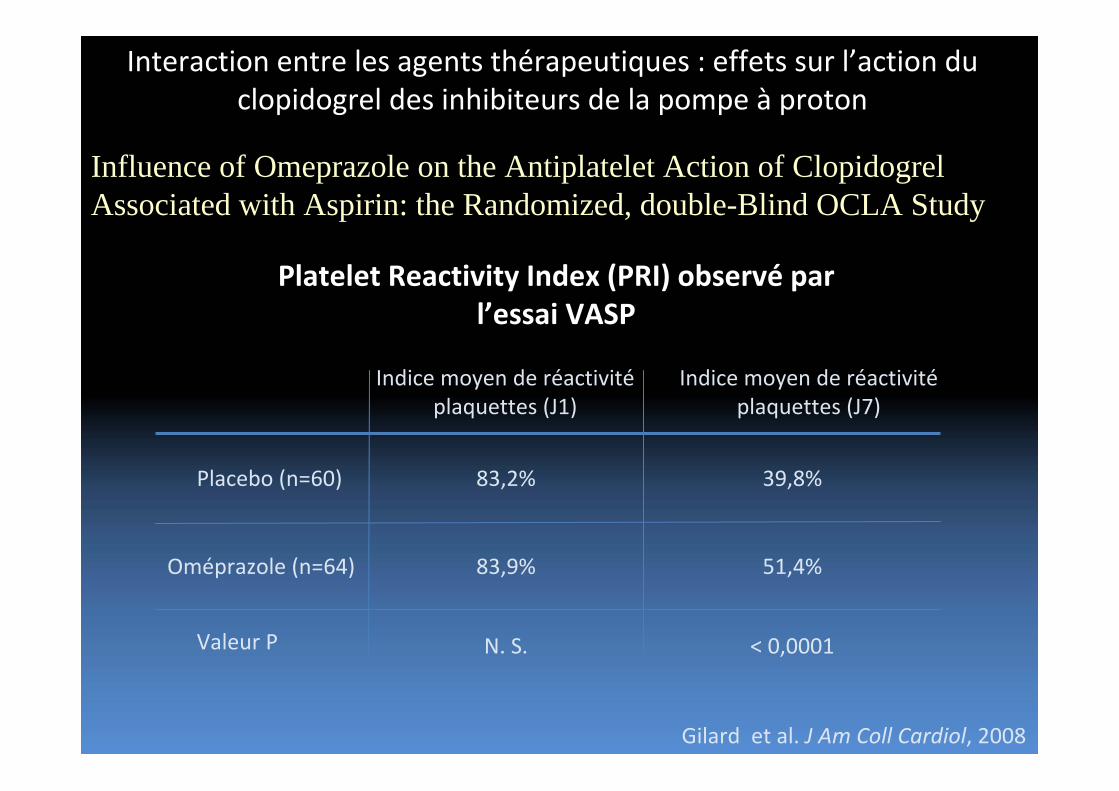
Interaction entre les agents thérapeutiques : effets sur l’action du clopidogrel des inhibiteurs de la pompe à proton
Influence of Omeprazole on the Antiplatelet Action of Clopidogrel Associated with Aspirin: the Randomized, double-Blind OCLA Study
Platelet Reactivity Index (PRI) observé par l’essai VASP
Oméprazole (n=64)
Indice moyen de réactivitéplaquettes (J1)
83,2% 39,8%
83,9% 51,4%
Indice moyen de réactivitéplaquettes (J7)
Placebo (n=60)
Valeur P N. S. < 0,0001
Gilard et al. J Am Coll Cardiol, 2008
OCLA: conclusions
• Clopidogrel “poor” responders (defined as PRI >50%)
were more common in the Omp group 60.9% vs. 26.7%
in the placebo group (p < 0.0001).
• The odds ratio of being a clopidogrel “poor” responder
when treated with Omp was 4.31 (95% CI 2.0 to 9.2).
Interaction entre les agents thérapeutiques : effets sur l’action du clopidogrel par Les inhibiteurs de la pompe à proton
Sibbing et al. Thromb Haemost, 2009
Impact of proton pump inhibitors on the antiplatelet effects of clopidogrel
Étude d’observation sur 1000 patients avec Plavix
L’aggregation plaquettaire est mesurée pas Multiple Electrode platelet Aggregation
La population est divisée en quatre groupes selon l’IPP prise par le patient:Sans IPP (n=732)
Pantoprazole (n=162)Omeprazole (n=64)Esomeprazole (n=42)
Les caractéristiques cliniques des quatres groupes ne diffèrent pas de façon significative
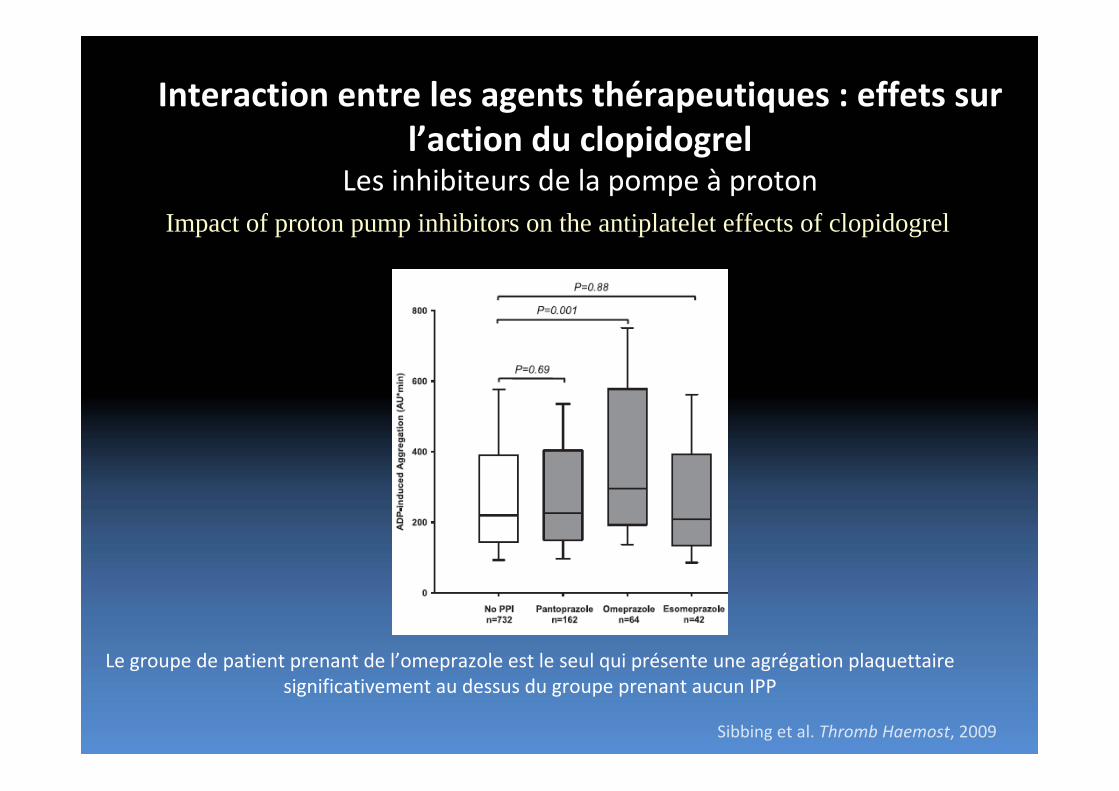
Interaction entre les agents thérapeutiques : effets sur l’action du clopidogrel
Les inhibiteurs de la pompe à protonImpact of proton pump inhibitors on the antiplatelet effects of clopidogrel
Le groupe de patient prenant de l’omeprazole est le seul qui présente une agrégation plaquettaire significativement au dessus du groupe prenant aucun IPP
Sibbing et al. Thromb Haemost, 2009
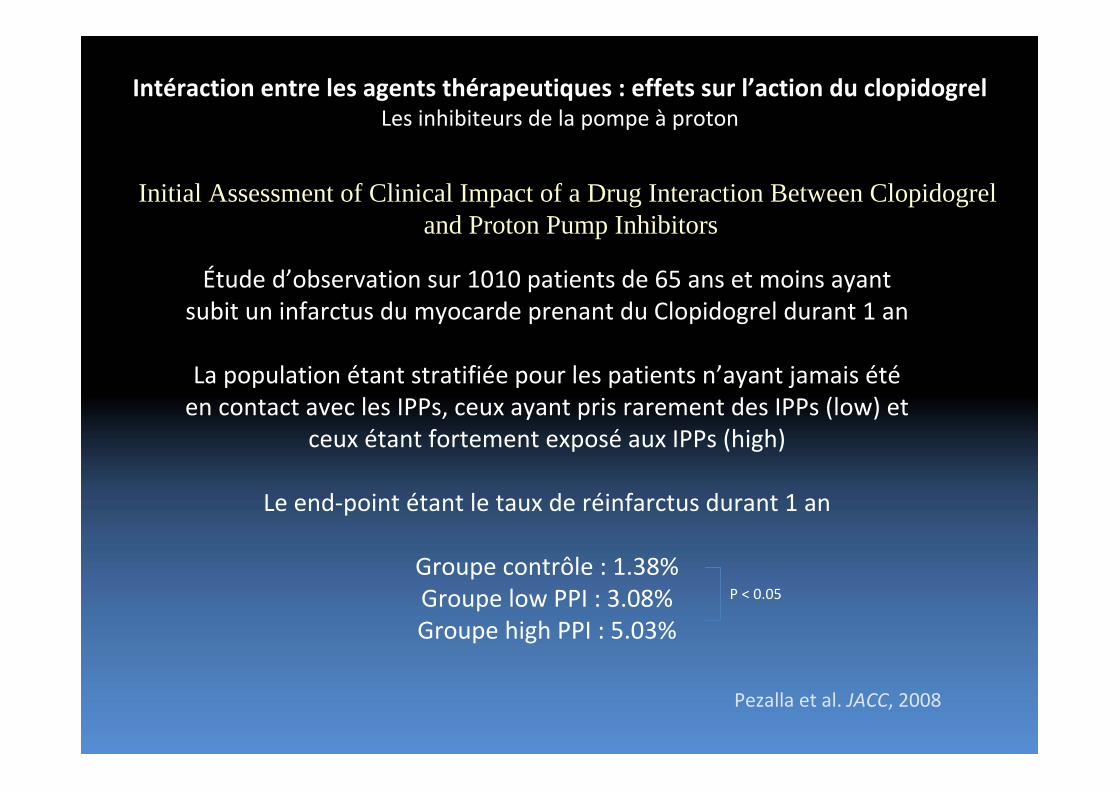
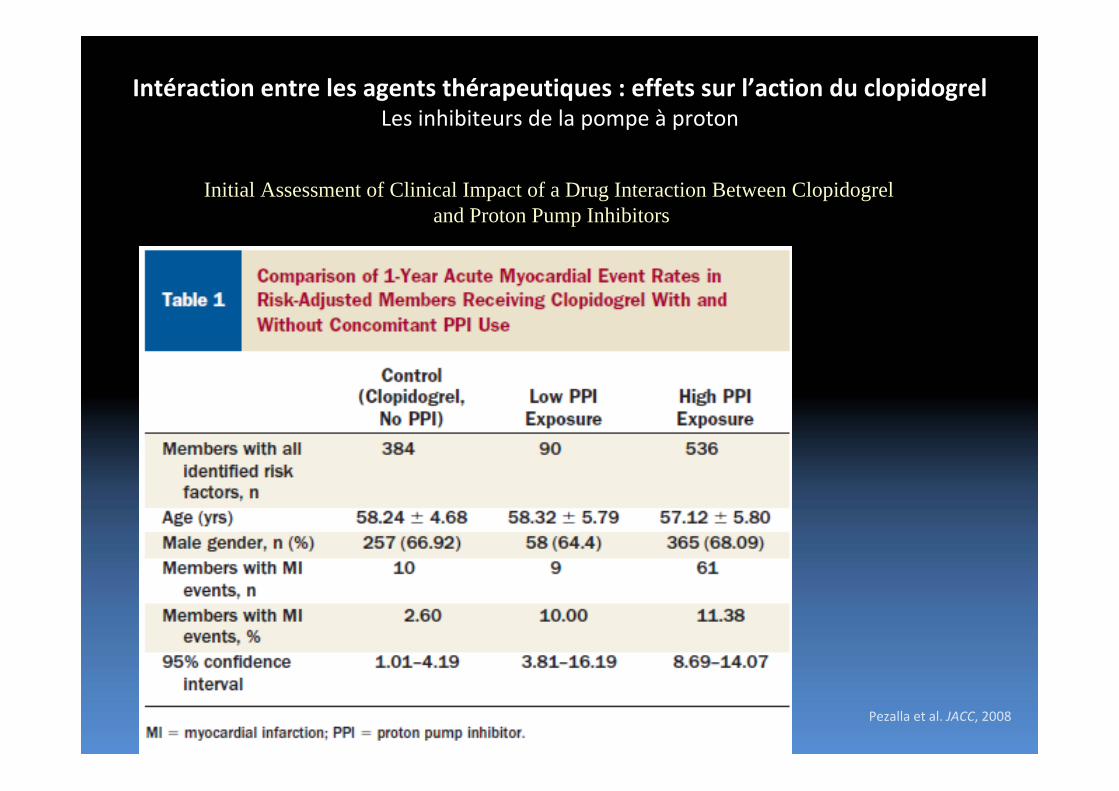
Intéraction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes inhibiteurs de la pompe à proton
Initial Assessment of Clinical Impact of a Drug Interaction Between Clopidogrel and Proton Pump Inhibitors
Pezalla et al. JACC, 2008
Étude d’observation sur 1010 patients de 65 ans et moins ayant subit un infarctus du myocarde prenant du Clopidogrel durant 1 an
La population étant stratifiée pour les patients n’ayant jamais étéen contact avec les IPPs, ceux ayant pris rarement des IPPs (low) et
ceux étant fortement exposé aux IPPs (high)
Le end‐point étant le taux de réinfarctus durant 1 an
Groupe contrôle : 1.38%Groupe low PPI : 3.08%Groupe high PPI : 5.03%
P < 0.05
Intéraction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes inhibiteurs de la pompe à proton
Initial Assessment of Clinical Impact of a Drug Interaction Between Clopidogrel and Proton Pump Inhibitors
Pezalla et al. JACC, 2008
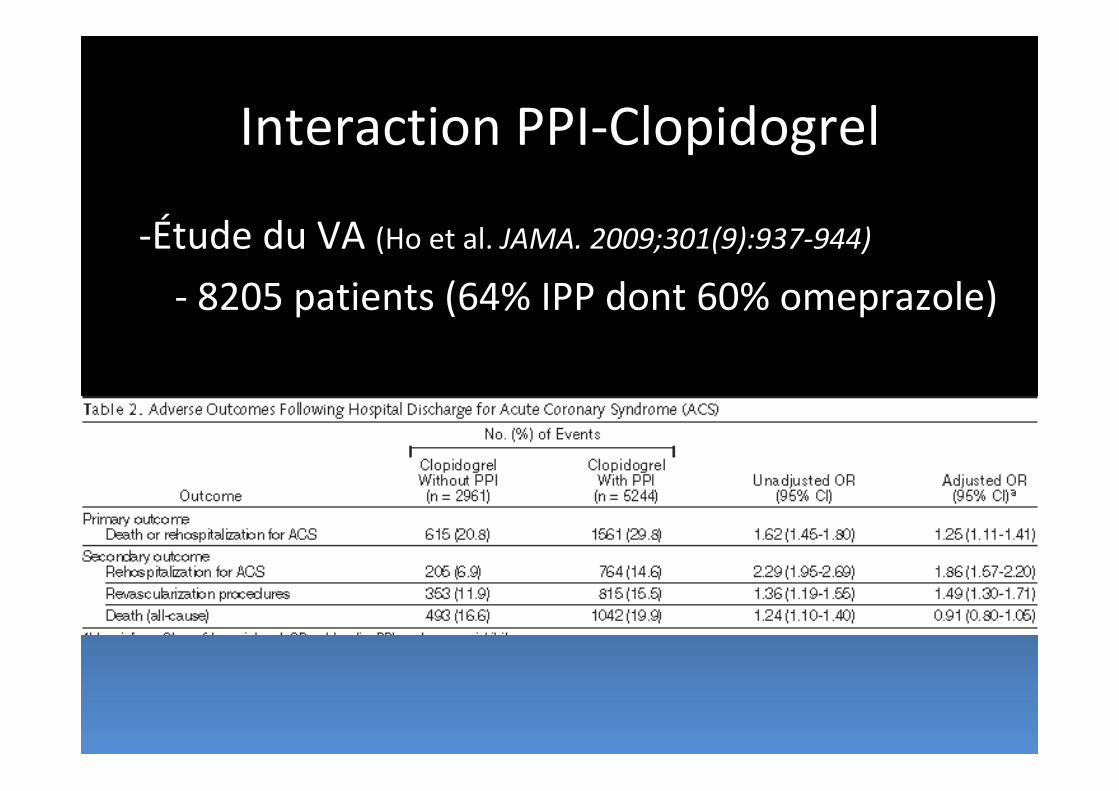
Interaction PPI‐Clopidogrel
‐Étude du VA (Ho et al. JAMA. 2009;301(9):937‐944)
‐ 8205 patients (64% IPP dont 60% omeprazole)
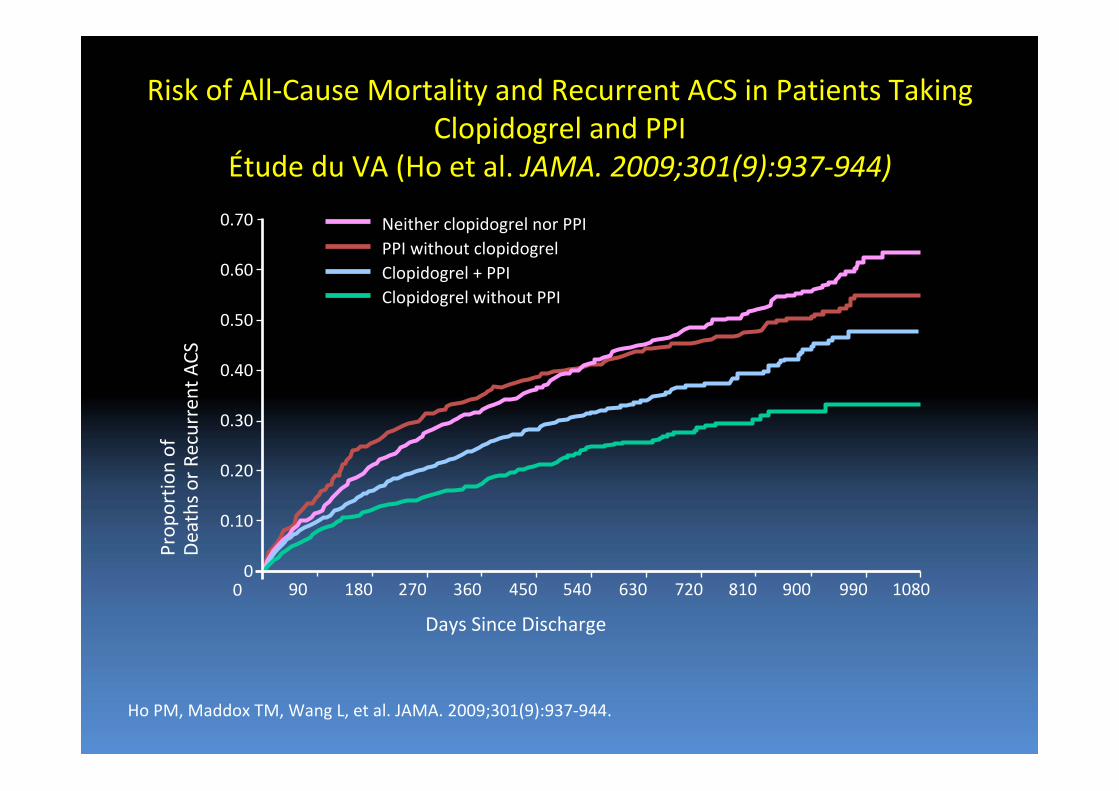
Risk of All‐Cause Mortality and Recurrent ACS in Patients Taking Clopidogrel and PPI
Étude du VA (Ho et al. JAMA. 2009;301(9):937‐944)
Ho PM, Maddox TM, Wang L, et al. JAMA. 2009;301(9):937‐944.
0.70
0.60
0.50
0.40
0.30
0.20
0.10
00 90 180 270 360 450 540 630 720 810 900 990 1080
Days Since Discharge
Prop
ortio
n of
Deaths or Recurrent ACS
Neither clopidogrel nor PPIPPI without clopidogrelClopidogrel + PPIClopidogrel without PPI
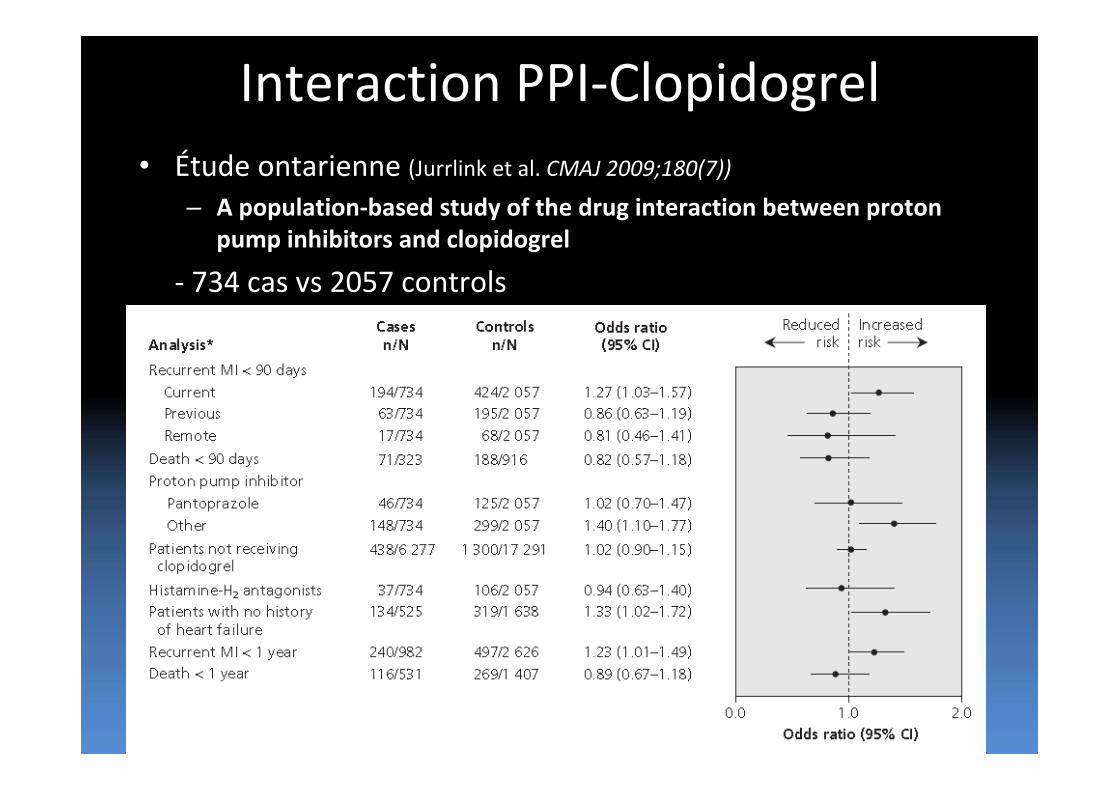
Interaction PPI‐Clopidogrel• Étude ontarienne (Jurrlink et al. CMAJ 2009;180(7))
– A population‐based study of the drug interaction between proton pump inhibitors and clopidogrel
‐ 734 cas vs 2057 controls
Autres études cliniques (abstracts)• Aubert et al. 6 (Abstract)
• Patients who received a stent from the National Medco Database
• Observational Cohort
• 14383 pts
• Started plavix after stent placement and who were at least 80% compliant
• PPI (4521) vs. no PPI (9862)
•• One‐year incidence of major CV events: Hosp. from stroke, MI, angina or CABG
• Rate of 1° endpoint
•• 1) PPI group 32.5%
• vs 21.2% in Non‐ PPIsgroup
• (none of these patients had prior CV event)
• Adjusted OR 1.79
•• 2) PPI group 39.8%
• vs 26.2% in Non‐ PPIs group
• (prior CV event)
• Adjusted OR 1.86
Autres études cliniques (abstracts)
• Kreutz et al.7
• (Abstract)
• Patients undergoing PCI with stenting from the National Medco Database
• Observational
• Cohort
• 16690
• Clopidogrel therapy alone (9862) vs clopidogrel + PPI (6828)
• One year incidence of hosp. for MI, unstable angina, stroke/TIA,PCI/CABG, or CV death
• Rate of 1° endpt. 17.9% in non‐PPI group vs 25.1% PPI group (p<0.001)
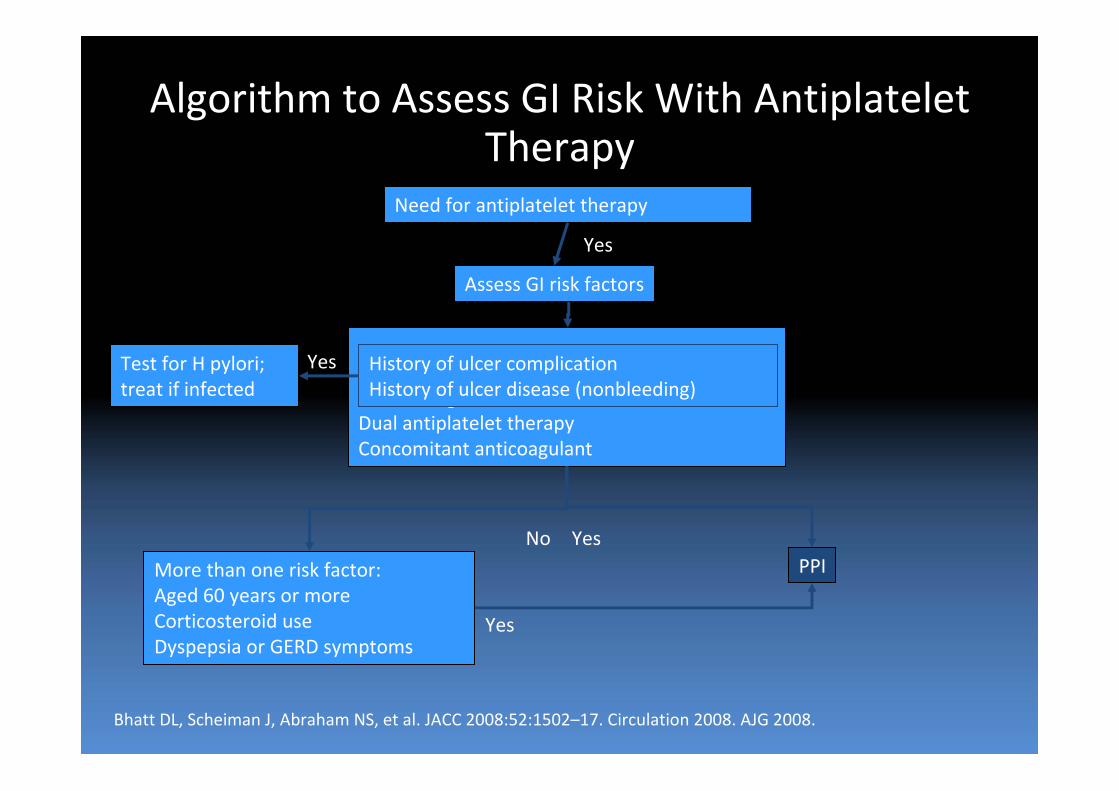
GI bleedingDual antiplatelet therapyConcomitant anticoagulant
Algorithm to Assess GI Risk With Antiplatelet Therapy
Assess GI risk factors
History of ulcer complication History of ulcer disease (nonbleeding)
Test for H pylori; treat if infected
More than one risk factor:Aged 60 years or moreCorticosteroid useDyspepsia or GERD symptoms
Need for antiplatelet therapy
Yes
Yes
NoPPI
Yes
Yes
Bhatt DL, Scheiman J, Abraham NS, et al. JACC 2008:52:1502–17. Circulation 2008. AJG 2008.
Réaction des organismes
• FDA– “Healthcare providers should re‐evaluate the need for starting or continuing treatment with a PPI, including Prilosec OTC, in patients taking clopidogrel.”
• Santé‐Canada (août 2009)– L'utilisation d'inhibiteurs de la pompe à protons de même que d'autres médicaments qui inhibent l'isoenzyme CYP2C19 est déconseillée chez les patients recevant Plavix® (clopidogrel). Le médecin prescripteur devrait soupeser les risques et les bienfaits de la poursuite du traitement par un inhibiteur de la pompe à protons, tout en tenant compte de l'existence d'autres agents gastroprotecteurs.
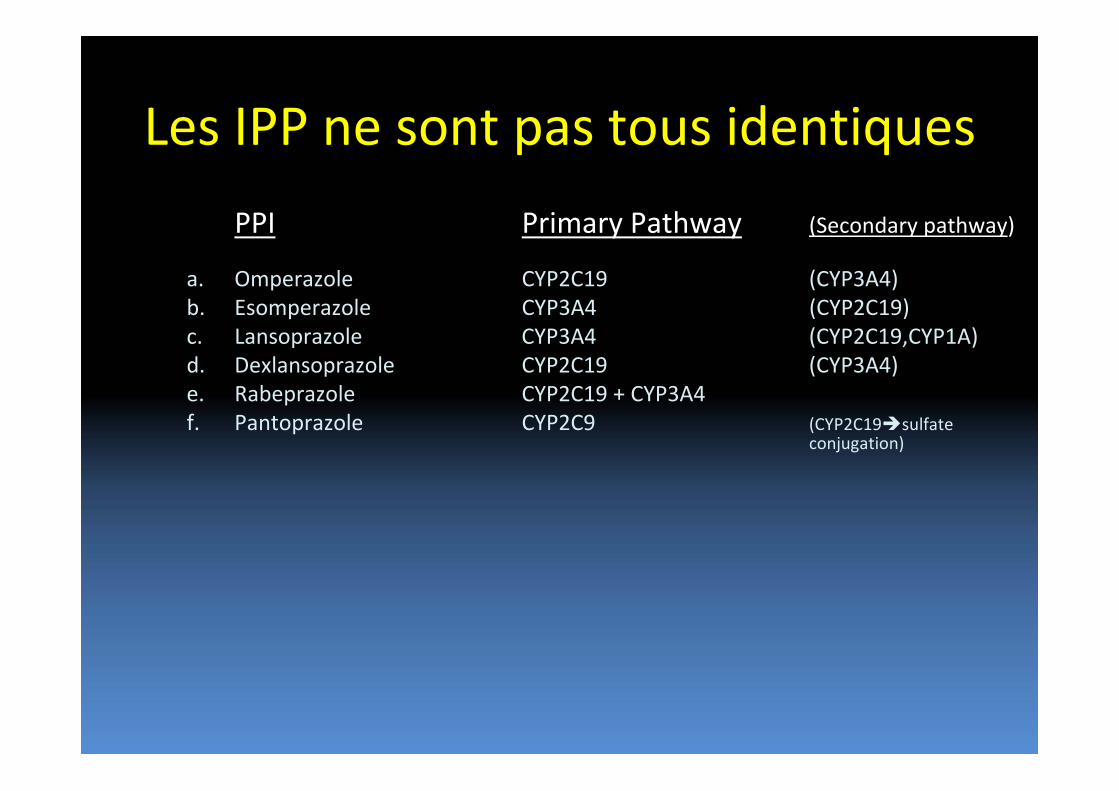
Les IPP ne sont pas tous identiques
PPI Primary Pathway (Secondary pathway)
a. Omperazole CYP2C19 (CYP3A4)b. Esomperazole CYP3A4 (CYP2C19)c. Lansoprazole CYP3A4 (CYP2C19,CYP1A)d. Dexlansoprazole CYP2C19 (CYP3A4)e. Rabeprazole CYP2C19 + CYP3A4f. Pantoprazole CYP2C9 (CYP2C19 sulfate
conjugation)
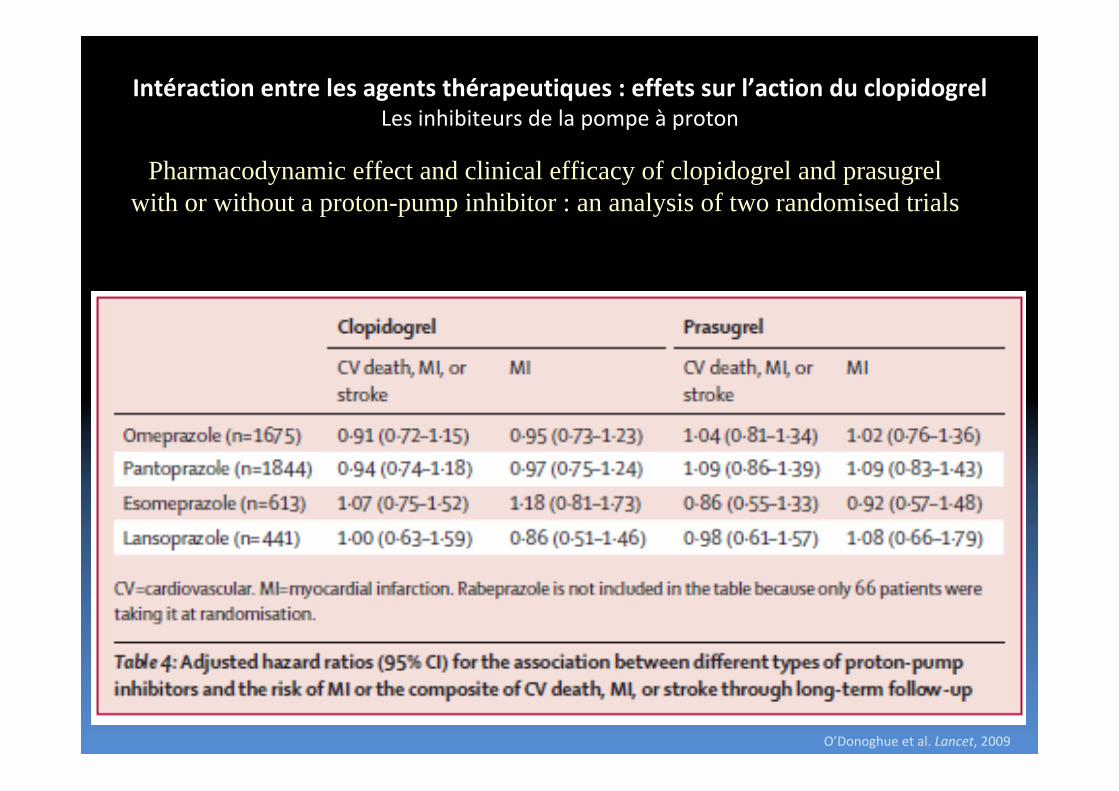
Intéraction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes inhibiteurs de la pompe à proton
Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor : an analysis of two randomised trials
O’Donoghue et al. Lancet, 2009
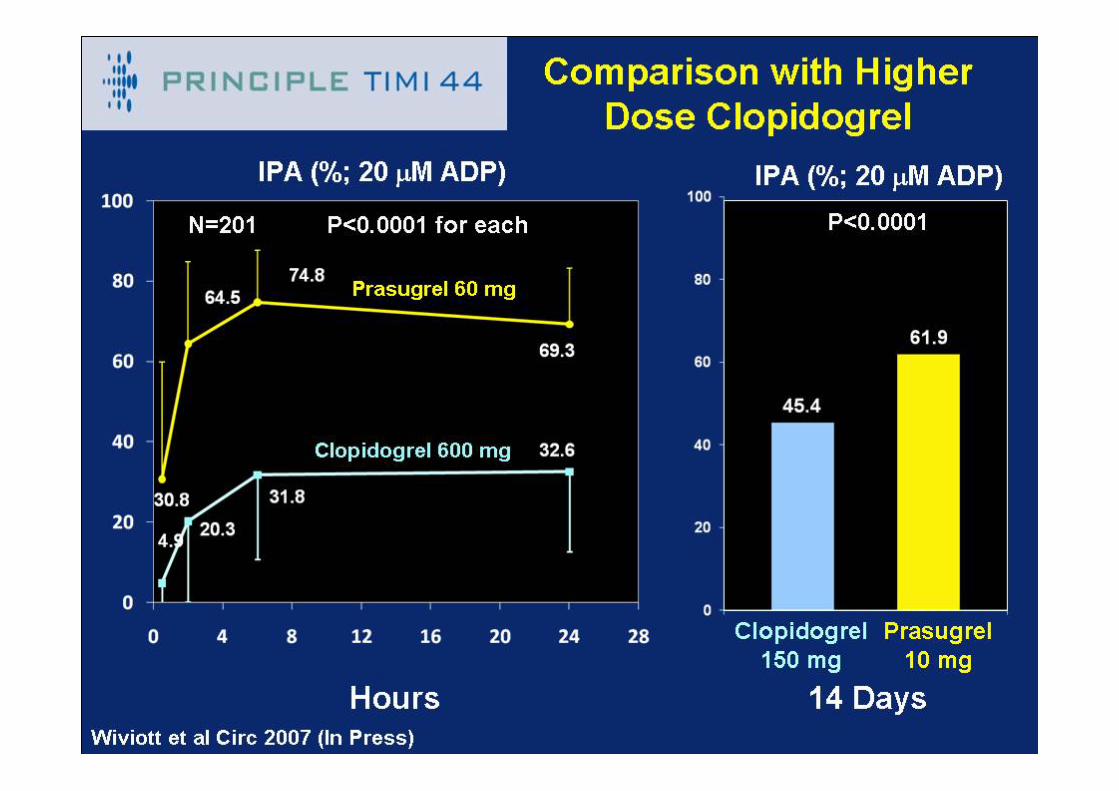
1er étude: Basée sur le PRINCIPLE‐TIMI 44 Trial (201 patients) avec comme end‐point primaire l’inhibition de l’agrégation plaquettaire, 6 heures après la dose de charge de clopidogrel (600mg) ou de Prasugrel (60mg).
2e étude: Basée sur le TRITON‐TIMI 38 Trial (13608 patients) avec comme end‐point primaire les événements cardiovasculaires, mort, infarctus et AVC.
*L’utilisation des IPPs dans ces études était à la discrétion des médecins traitants.
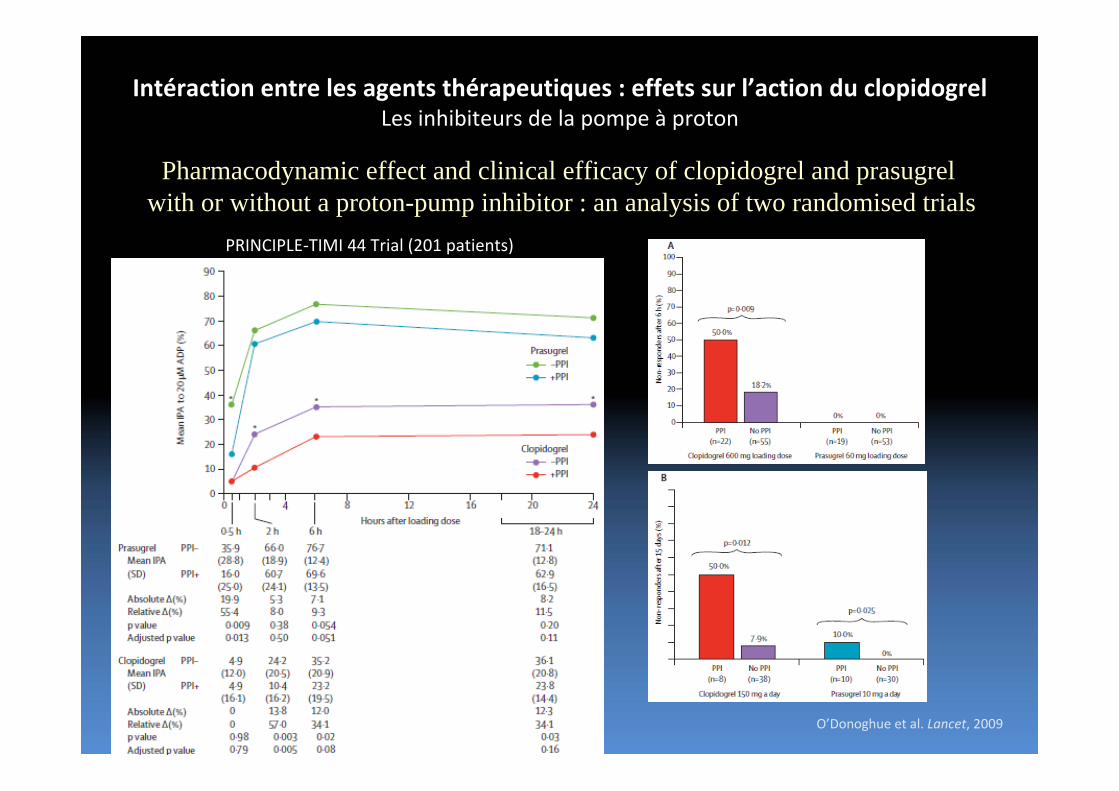
Intéraction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes inhibiteurs de la pompe à proton
Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor : an analysis of two randomised trials
O’Donoghue et al. Lancet, 2009
PRINCIPLE‐TIMI 44 Trial (201 patients)
CV death, M
I or stroke
Days
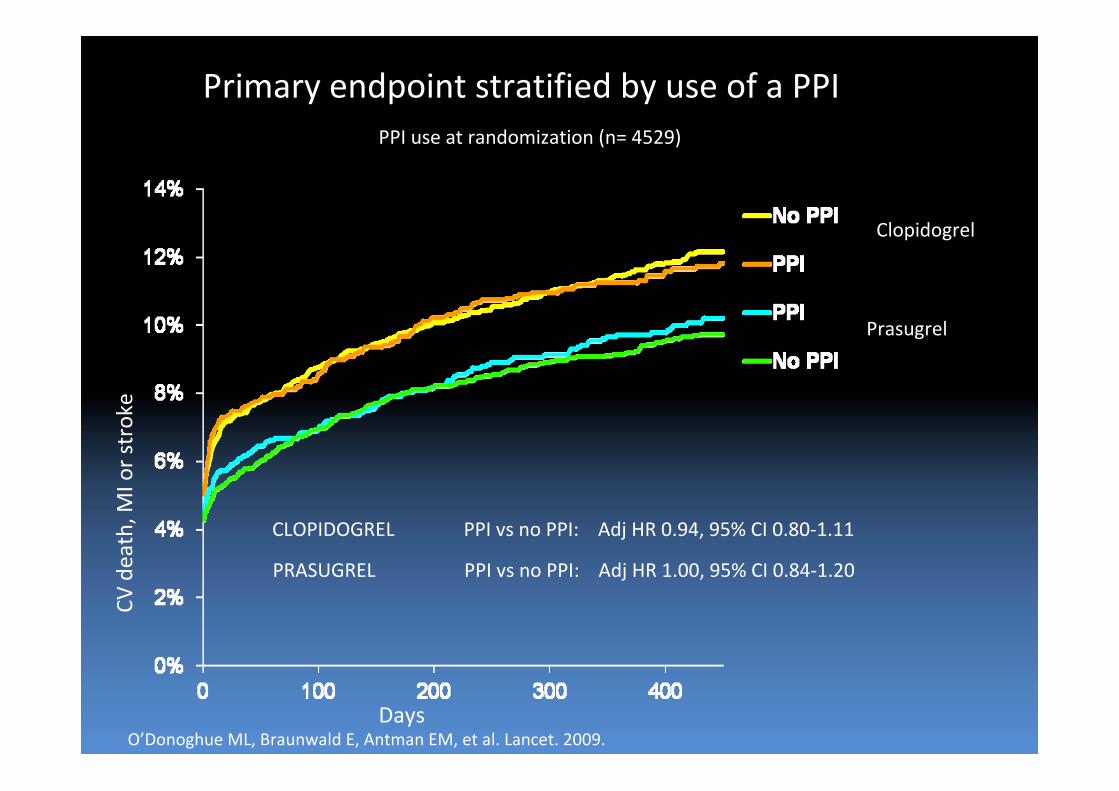
CLOPIDOGREL PPI vs no PPI: Adj HR 0.94, 95% CI 0.80‐1.11
PPI use at randomization (n= 4529)
Clopidogrel
Prasugrel
PRASUGREL PPI vs no PPI: Adj HR 1.00, 95% CI 0.84‐1.20
Primary endpoint stratified by use of a PPI
O’Donoghue ML, Braunwald E, Antman EM, et al. Lancet. 2009.
Intéraction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes inhibiteurs de la pompe à proton
Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor : an analysis of two randomised trials
O’Donoghue et al. Lancet, 2009
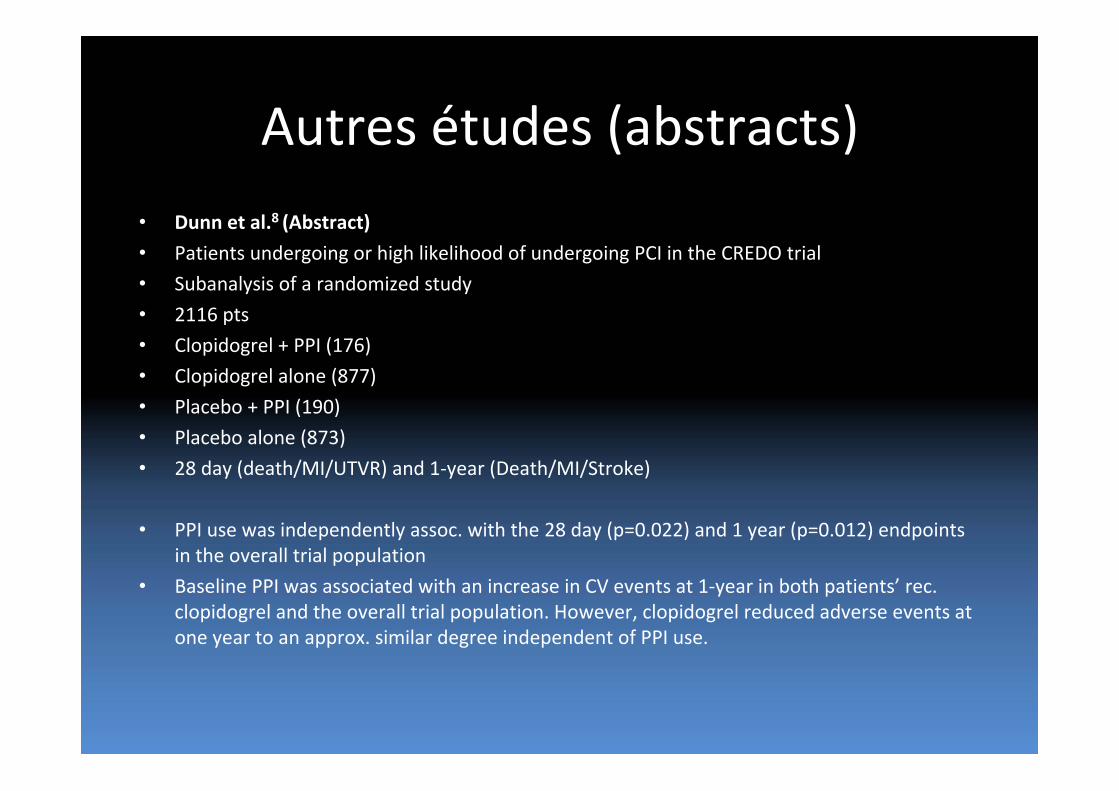
Autres études (abstracts)
• Dunn et al.8 (Abstract)
• Patients undergoing or high likelihood of undergoing PCI in the CREDO trial
• Subanalysis of a randomized study
• 2116 pts
• Clopidogrel + PPI (176)
• Clopidogrel alone (877)
• Placebo + PPI (190)
• Placebo alone (873)
• 28 day (death/MI/UTVR) and 1‐year (Death/MI/Stroke)
• PPI use was independently assoc. with the 28 day (p=0.022) and 1 year (p=0.012) endpoints in the overall trial population
• Baseline PPI was associated with an increase in CV events at 1‐year in both patients’ rec. clopidogrel and the overall trial population. However, clopidogrel reduced adverse events at one year to an approx. similar degree independent of PPI use.
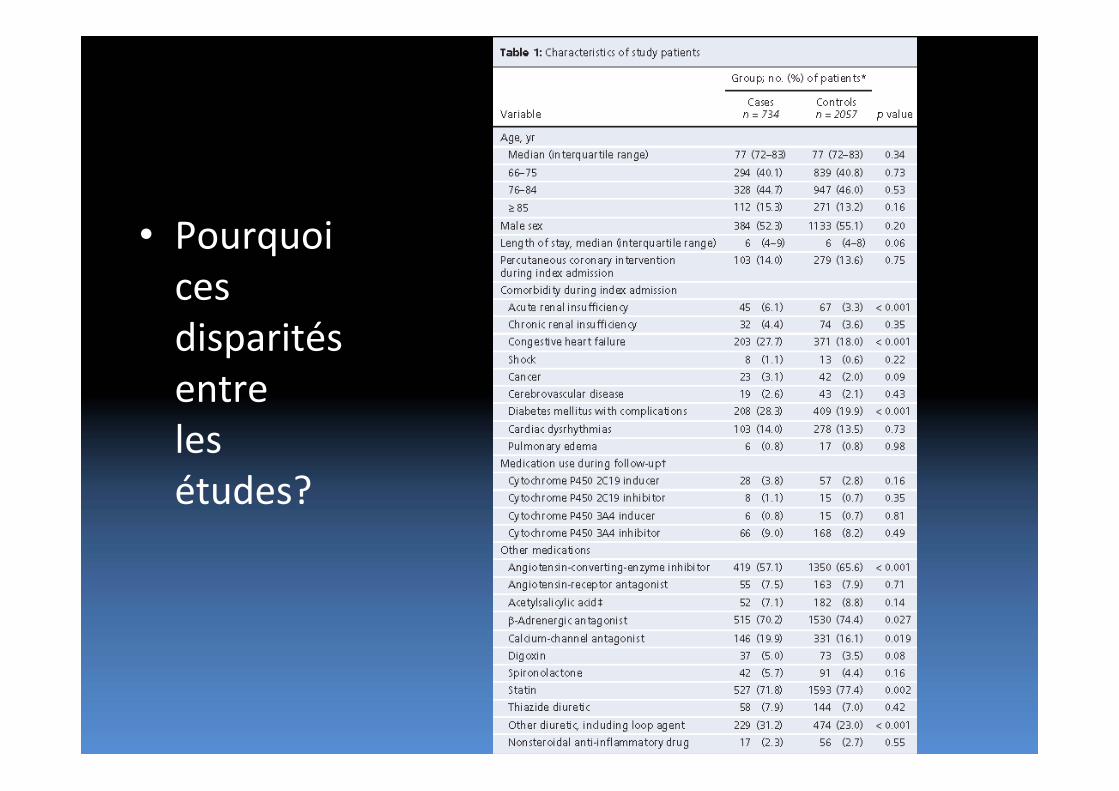
• Pourquoicesdisparitésentrelesétudes?
The COGENT TrialThe COGENT Trial
Deepak L. Bhatt MD, MPH, Byron Cryer MD, Charles F. Contant PhD, Marc Cohen MD, Angel Lanas MD, DSc, Thomas J. Schnitzer MD, PhD, Thomas L. Shook MD, Pablo Lapuerta MD, Mark A. Goldsmith, MD, PhD, Benjamin M. Scirica MD, Robert P. Giugliano MD, Christopher P. Cannon MD, on Behalf of the COGENT Investigators
Aims
• To determine whether PPI versus placebo reduced important GI events in patients on dual antiplatelet therapy
• To determine if there was any cardiovascular interaction between clopidogrel and PPI
Methods
• Multicenter, international, randomized, double‐blind, double‐dummy, placebo‐controlled, parallel group, phase 3 efficacy and safety study of CGT‐2168, a fixed‐dose combination of clopidogrel (75 mg) and omeprazole (20 mg), compared with clopidogrel.
• Patients were stratified based on two baseline factors: H. pylori serology (positive or negative) and concomitant use of any NSAID.
• All patients were to receive enteric coated aspirin at a dose of 75 to 325 mg.
Methods
• The GI endpoint was upper GI bleeding, bleeding of presumed occult GI origin with decrease in hemoglobin of ≥ 2 g/dL or decrease in hematocrit ≥ 10%, symptomatic gastroduodenal ulcer confirmed by endoscopy or radiography, pain of presumed GI origin with underlying multiple erosive disease confirmed by endoscopy, obstruction, or perforation.
• The cardiovascular endpoint was the composite of cardiovascular death, non‐fatal MI, CABG or PCI, or ischemic stroke.
• Adjudication of events was performed by an independent committee of cardiologists and gastroenterologists.
• The initial planned sample size was 3200 patients, an accrual period of 1 year, and maximum follow up of 2 years. As a low rate of gastrointestinal events was observed as the trial was ongoing, the sample size target was increased to 4200 and then ~5000 (143 GI events). The study ended when the sponsor declared bankruptcy.
Inclusion Criteria
• Patients ≥ 21 years of age• Clopidogrel therapy with concomitant aspirin was anticipated for at least the next 12 months
– acute coronary syndrome
–undergoing placement of a coronary stent
Exclusion Criteria
• Hospitalized patients for whom discharge was not anticipated within 48 hours of randomization
• Requirement for current or chronic use of a proton pump inhibitor, H2 receptor blocker, sucralfate or misoprostol
• Erosive esophagitis, esophageal, or gastric variceal disease, or non‐endoscopic gastric surgery
• Receipt of > 21 days of clopidogrel or another thienopyridine prior to randomization
• Oral anticoagulation that cannot be safely discontinued for duration of study
• Recent fibrinolytic therapy
• Scheduled PCI or recent (< 30 days prior to randomization) CABG
• Active bleeding or a history of a hemostatic disorder
• Systemic corticosteroids except low‐dose oral corticosteroids equivalent to prednisone ≤ 5 mg/day
Results
• 3627 patients (above the initial target of 3200)
• 393 sites
• Median follow‐up 133 days (maximum 362 days)
• 136 adjudicated cardiovascular events (preliminary)
• 105 adjudicated GI events (preliminary)
–143 had been planned
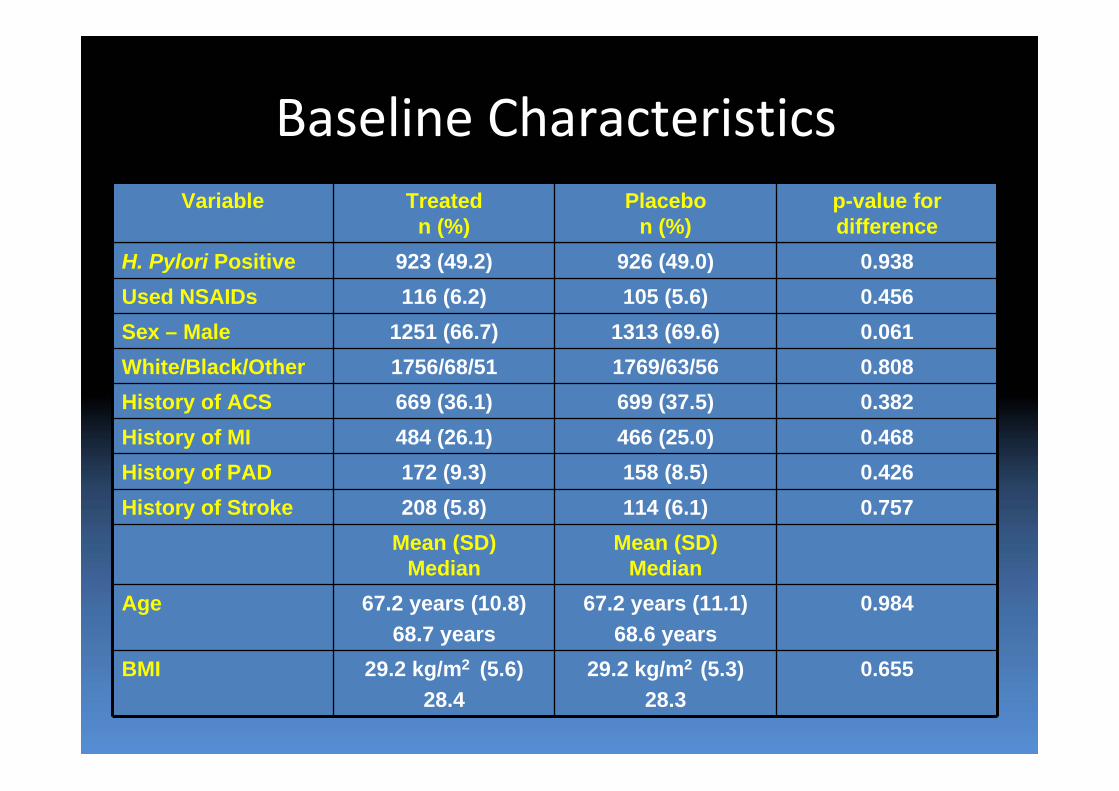
Baseline CharacteristicsVariable Treated
n (%)Placebo
n (%)p-value for difference
H. Pylori Positive 923 (49.2) 926 (49.0) 0.938Used NSAIDs 116 (6.2) 105 (5.6) 0.456Sex – Male 1251 (66.7) 1313 (69.6) 0.061White/Black/Other 1756/68/51 1769/63/56 0.808History of ACS 669 (36.1) 699 (37.5) 0.382History of MI 484 (26.1) 466 (25.0) 0.468History of PAD 172 (9.3) 158 (8.5) 0.426History of Stroke 208 (5.8) 114 (6.1) 0.757
Mean (SD)Median
Mean (SD)Median
Age 67.2 years (10.8)68.7 years
67.2 years (11.1)68.6 years
0.984
BMI 29.2 kg/m2 (5.6)28.4
29.2 kg/m2 (5.3)28.3
0.655
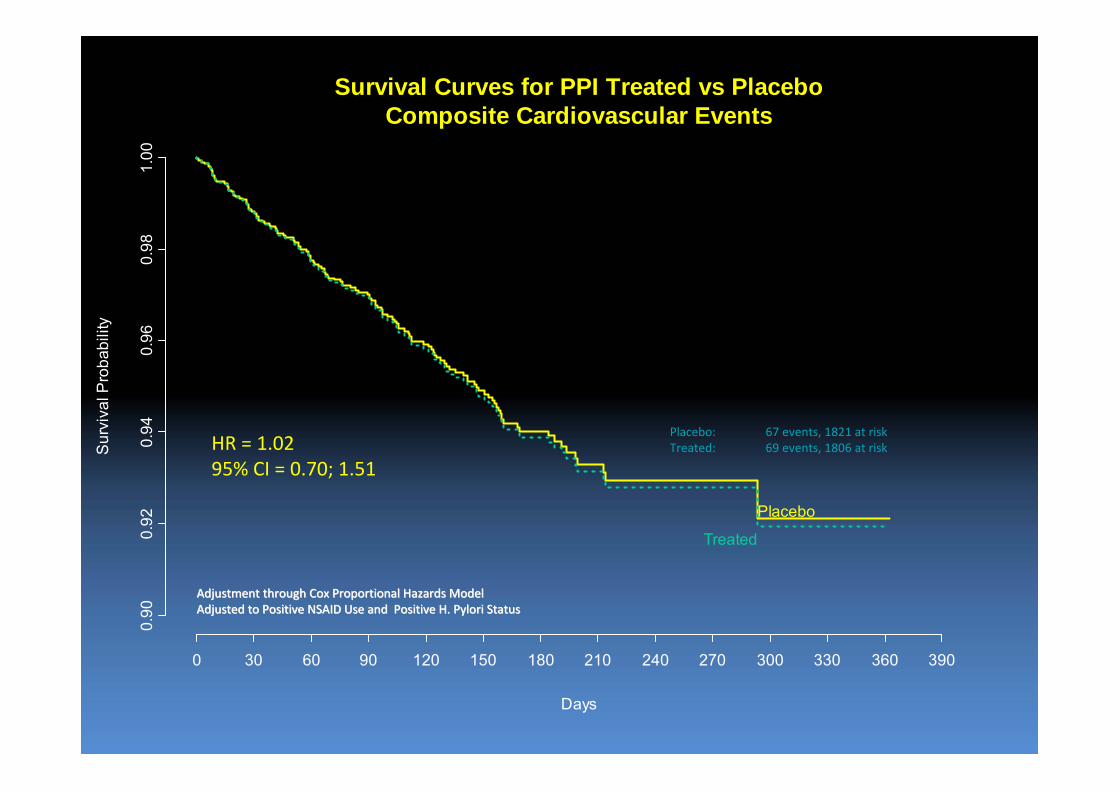
Days
Sur
viva
l Pro
babi
lity
0 30 60 90 120 150 180 210 240 270 300 330 360 390
0.90
0.92
0.94
0.96
0.98
1.00
Placebo
Treated
Survival Curves for PPI Treated vs PlaceboComposite Cardiovascular Events
Adjustment through Cox Proportional Hazards ModelAdjustment through Cox Proportional Hazards ModelAdjusted to Positive NSAID Use and Positive H. Pylori StatusAdjusted to Positive NSAID Use and Positive H. Pylori Status
HR = 1.0295% CI = 0.70; 1.51
Placebo: 67 events, 1821 at riskTreated: 69 events, 1806 at risk
Days
Sur
viva
l Pro
babi
lity
0 30 60 90 120 150 180 210 240 270 300 330 360 390
0.90
0.92
0.94
0.96
0.98
1.00
PlaceboTreated
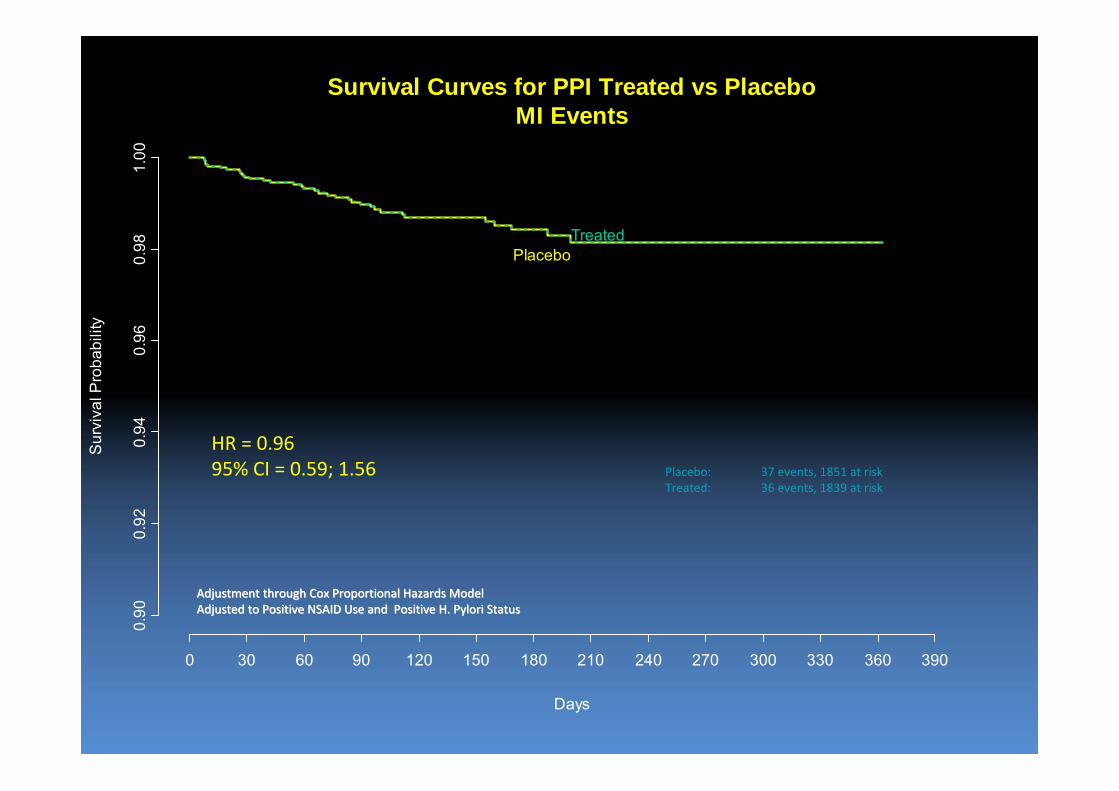
Survival Curves for PPI Treated vs PlaceboMI Events
Adjustment through Cox Proportional Hazards ModelAdjustment through Cox Proportional Hazards ModelAdjusted to Positive NSAID Use and Positive H. Pylori StatusAdjusted to Positive NSAID Use and Positive H. Pylori Status
HR = 0.9695% CI = 0.59; 1.56 Placebo: 37 events, 1851 at risk
Treated: 36 events, 1839 at risk
Days
Sur
viva
l Pro
babi
lity
0 30 60 90 120 150 180 210 240 270 300 330 360 390
0.90
0.92
0.94
0.96
0.98
1.00
PlaceboTreated
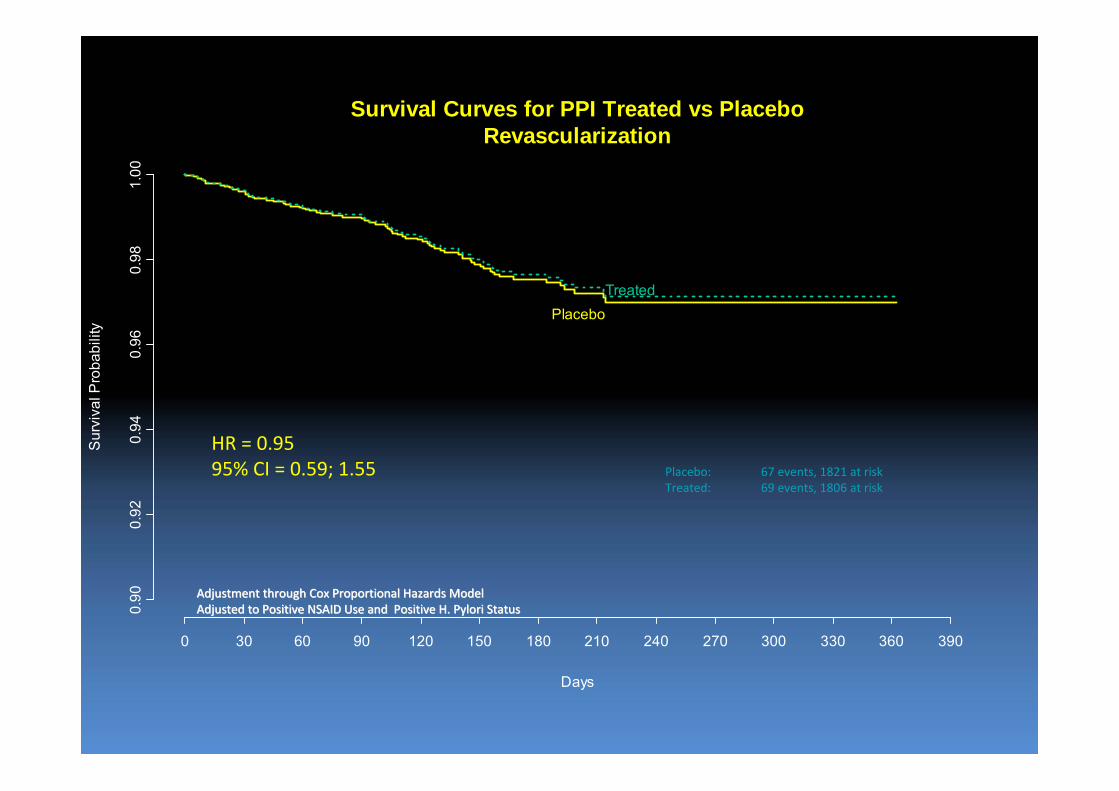
Survival Curves for PPI Treated vs PlaceboRevascularization
Adjustment through Cox Proportional Hazards ModelAdjustment through Cox Proportional Hazards ModelAdjusted to Positive NSAID Use and Positive H. Pylori StatusAdjusted to Positive NSAID Use and Positive H. Pylori Status
HR = 0.9595% CI = 0.59; 1.55 Placebo: 67 events, 1821 at risk
Treated: 69 events, 1806 at risk
Hazard Ratio
0 2 4 6 8 10
H. pylori Positive or Indeterminate
H. pylori Negative
No NSAIDs Used
NSAIDs Used
Male
Female
Other Race
Black
White
Age <= 70
Age > 70
BMI <= 30
BMI > 30
Overall
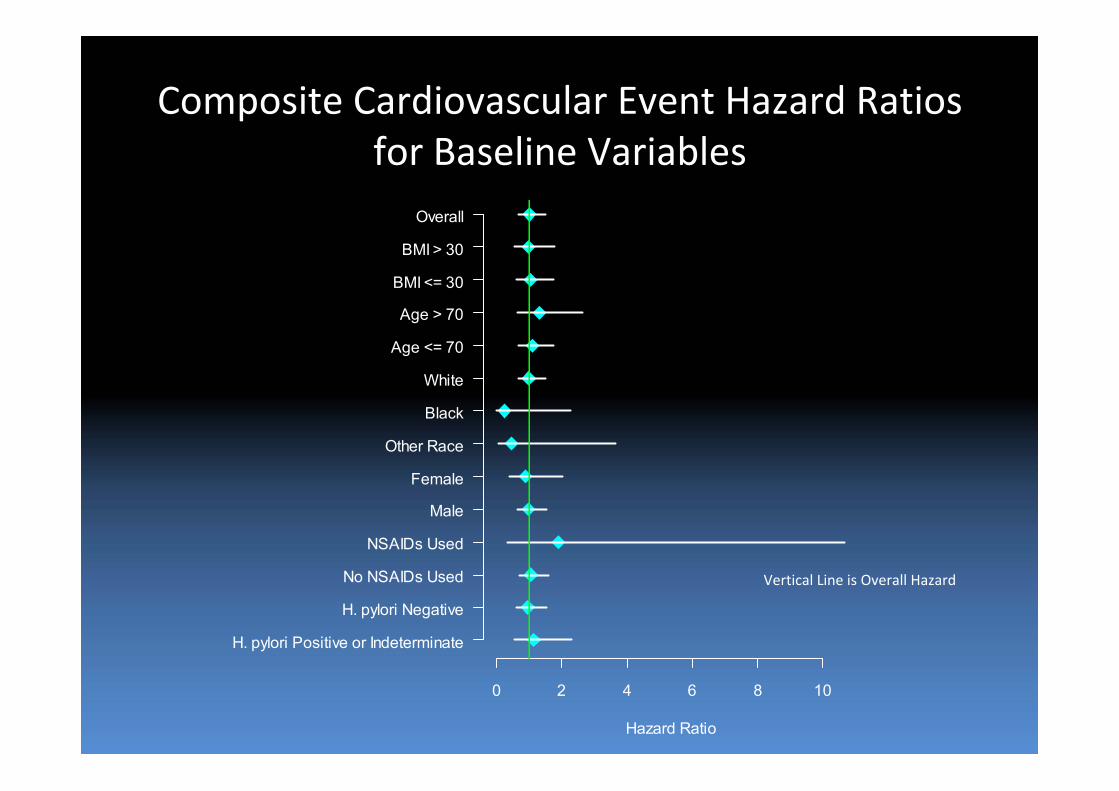
Composite Cardiovascular Event Hazard Ratios for Baseline Variables
Vertical Line is Overall Hazard
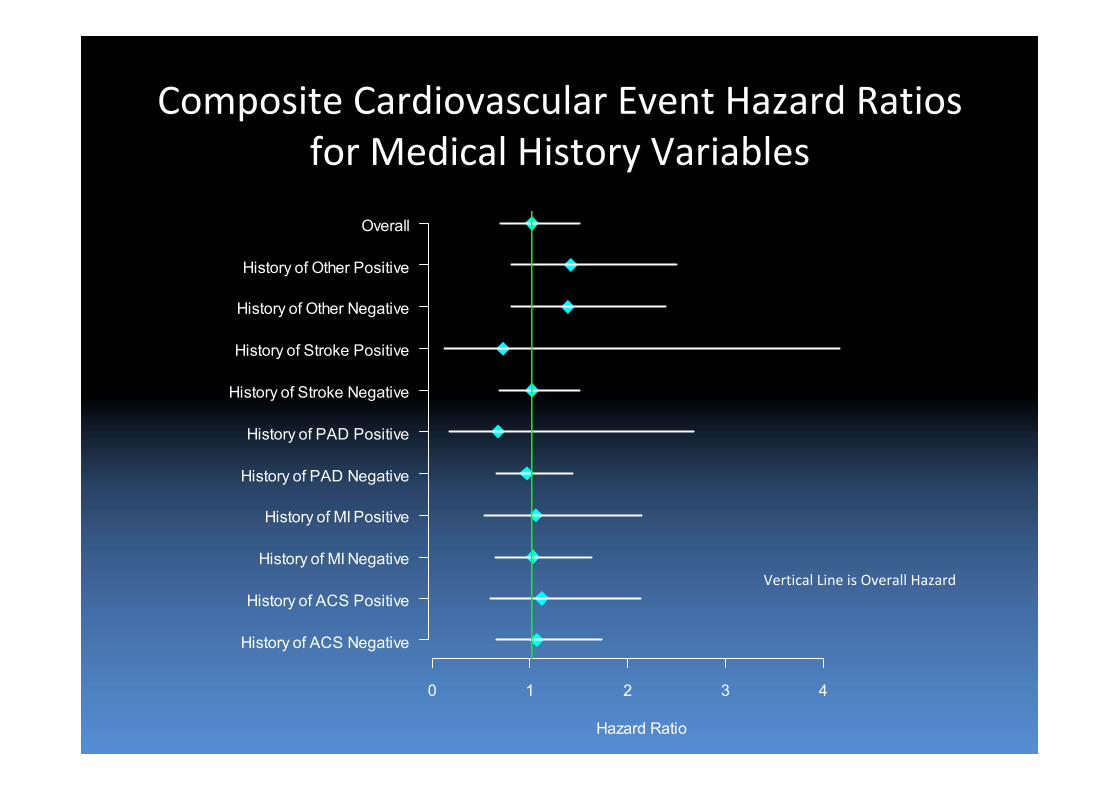
Composite Cardiovascular Event Hazard Ratios for Medical History Variables
Hazard Ratio
0 1 2 3 4
History of ACS Negative
History of ACS Positive
History of MI Negative
History of MI Positive
History of PAD Negative
History of PAD Positive
History of Stroke Negative
History of Stroke Positive
History of Other Negative
History of Other Positive
Overall
Vertical Line is Overall Hazard
Days
Sur
viva
l Pro
babi
lity
0 30 60 90 120 150 180 210 240 270 300 330 360 390
0.90
0.92
0.94
0.96
0.98
1.00
Placebo
Treated
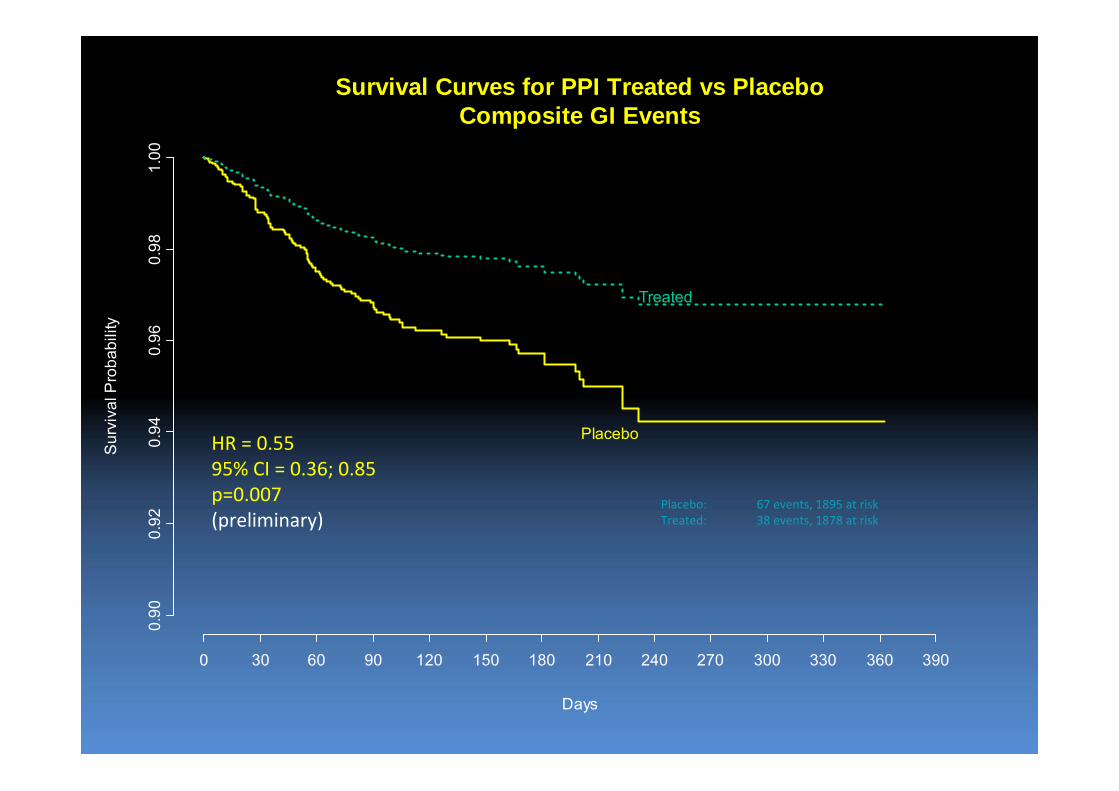
Survival Curves for PPI Treated vs PlaceboComposite GI Events
HR = 0.5595% CI = 0.36; 0.85p=0.007(preliminary)
Placebo: 67 events, 1895 at riskTreated: 38 events, 1878 at risk
Limitations • Due to premature termination of trial, limited follow‐up
– However, most relevant for GI events, as most cardiac events early after ACS or PCI
– No current PPI/clopidogrel data set has more adjudicated CV endpoints
• May not be directly applicable to PPIs other than omeprazole
– Most commonly used PPI
– One most indicted by ex vivo studies
• Special formulation of clopidogrel/PPI with different release kinetics, so may not be the same as taking clopidogrel and omeprazole off the shelf
– If a major concern, then take the clopidogrel in the morning and the PPI at night
Conclusions
• COGENT is the first, randomized assessment of clopidogrel and PPIs on clinical events
• The data provide strong reassurance that there is no clinically relevant adverse cardiovascular interaction between clopidogrel and PPIs
• The results call into question the exact relationship between ex vivo platelet assays and clinical outcomes, especially with respect to assessing drug interactions
– Platelet assays and observational data are not a substitute for RCT data
• Further research is needed to define the optimal strategy to reduce GI events in patients on antithrombotic therapy, though prophylactic PPIs seem very promising
Nouvelles réactions
• FDA (Nov 2009)– "New data show that when clopidogrel and omeprazole are taken together, the effectiveness of clopidogrel is reduced. Patients at risk for heart attacks or strokes who use clopidogrel to prevent blood clots will not get the full effect of this medicine if they are also taking omeprazole.“
– FDA suggest not to use: esomeprazole (nexium), lanzoprazole (prevacid), or omeprazole (losec)
– Espacer les doses ne suffit pas
IPP‐ Résumé
• Une étude pharmacodynamique prospective randomisée à double insu a démontré une diminution de l’effet anti‐plaquettaire du clopidogrel lorsque associé à l’omeprazole
• Aucune étude pharmacodynamique randomisée avec d’autres IPP
• Deux études non‐randomisées suggère que l’esomeprazole et le pantoprazole n’auraient pas d’effet néfaste
IPP ‐ Résumé
• Seulement les études rétrospectives sur des bases de données médico‐administratives ont démontré une augmentation du risque lorsque les IPP sont precrits avec le clopidogrel.
• Le pantoprazole a aussi été incriminé dans quelques unes de ces études.
• L’augmentation du risque d’événements semble démesuré par rapport a l’efficacité prouvée du clopidogrel dans les études antérieures
• Les patients sous IPP présentent plus de comorbidités
IPP‐Résumé
• Les études prospectives non‐randomisées n’ont pas démontré de risque clinique accru (TRITON, CREDO, CURRENT; n>35,000)
• La seule étude clinique randomisée (COGENT) n’a pas démontré de risque ischémique avec omeprazole avec une diminution significative du risque de saignement (étude non publiée)
Interaction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes antagonistes calciques
Gremmel et al. Heart, Aug 2009
Calcium-channel blockers decrease clopidogrel-mediated platelet inhibition
Étude d’observation sur 162 patients sur Clopidogrel suites à une intervention percutanée
Une analyse par light Transmitance Aggregometry (LTA) et par l’essai VerifyNow P2Y12 est fait 24 heures suivant la procédure
L’attribution d’un antagoniste calcique était laissé à la discrétion du Cardiologue traitant
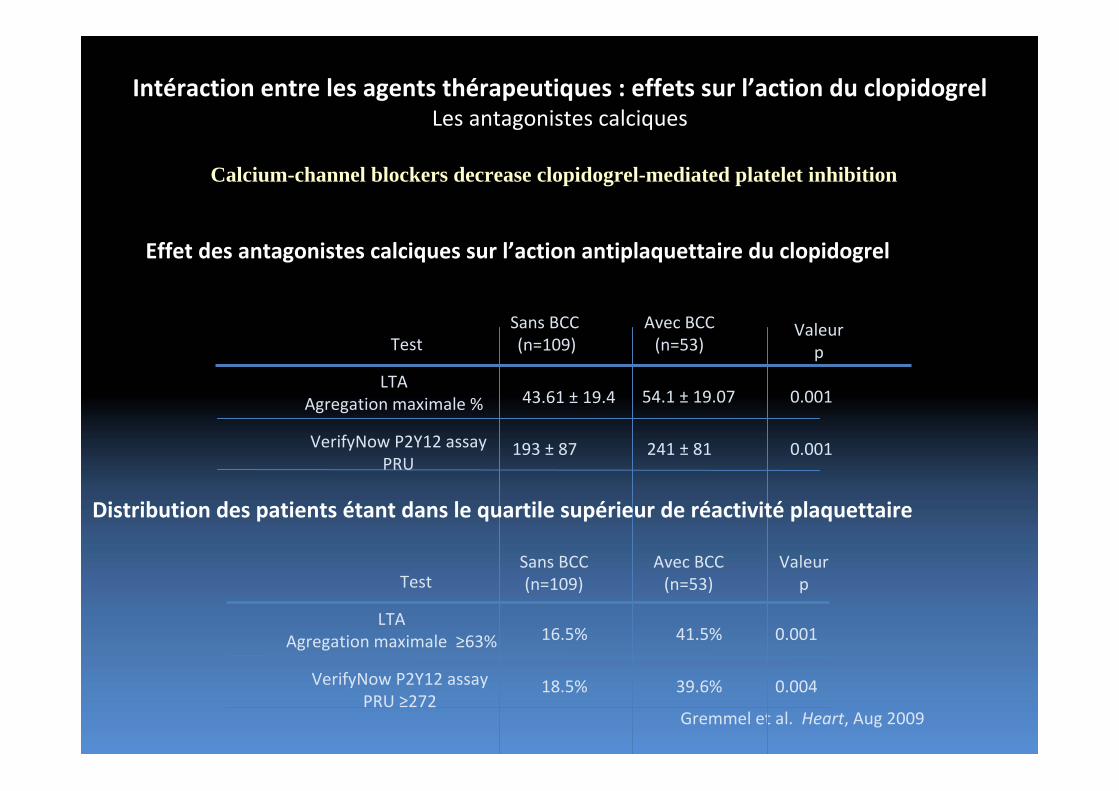
Intéraction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes antagonistes calciques
Gremmel et al. Heart, Aug 2009
Effet des antagonistes calciques sur l’action antiplaquettaire du clopidogrel
Test
LTAAgregation maximale %
VerifyNow P2Y12 assayPRU
Avec BCC(n=53)
Sans BCC(n=109)
43.61 ± 19.4 54.1 ± 19.07
193 ± 87 241 ± 81
0.001
0.001
Valeur p
Distribution des patients étant dans le quartile supérieur de réactivité plaquettaire
Test
LTAAgregation maximale ≥63%
VerifyNow P2Y12 assayPRU ≥272
Avec BCC (n=53)
Sans BCC(n=109)
Valeur p
41.5%16.5%
39.6%18.5%
0.001
0.004
Calcium-channel blockers decrease clopidogrel-mediated platelet inhibition
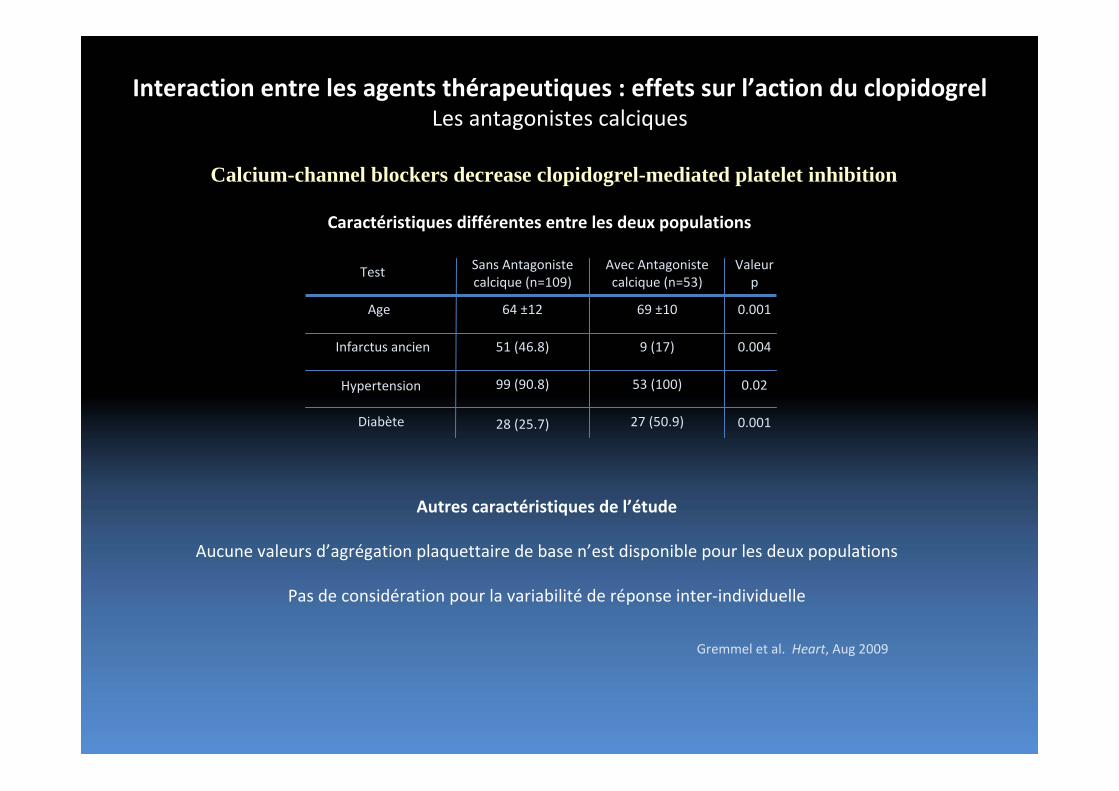
Interaction entre les agents thérapeutiques : effets sur l’action du clopidogrelLes antagonistes calciques
Caractéristiques différentes entre les deux populations
Test
Age
Infarctus ancien
Avec Antagoniste calcique (n=53)
Sans Antagoniste calcique (n=109)
Valeur p
64 ±12 69 ±10
51 (46.8) 9 (17)
0.001
0.004
Hypertension
Diabète
Autres caractéristiques de l’étude
Aucune valeurs d’agrégation plaquettaire de base n’est disponible pour les deux populations
Pas de considération pour la variabilité de réponse inter‐individuelle
Gremmel et al. Heart, Aug 2009
99 (90.8) 53 (100)
28 (25.7) 27 (50.9)
Calcium-channel blockers decrease clopidogrel-mediated platelet inhibition
0.02
0.001
Étude SPICEévaluation des Statines et des inhibiteurs de la Pompe à protons et leur Influence sur le Clopidogrel et ses
Effets antiplaquettaires
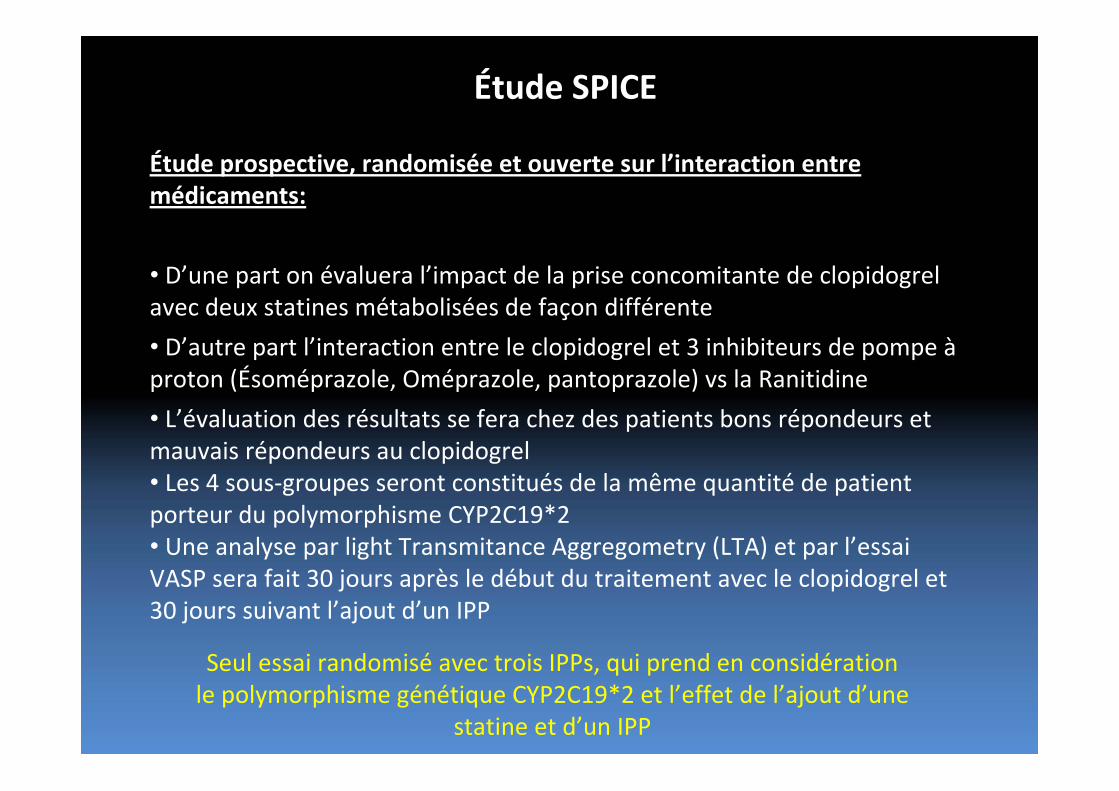
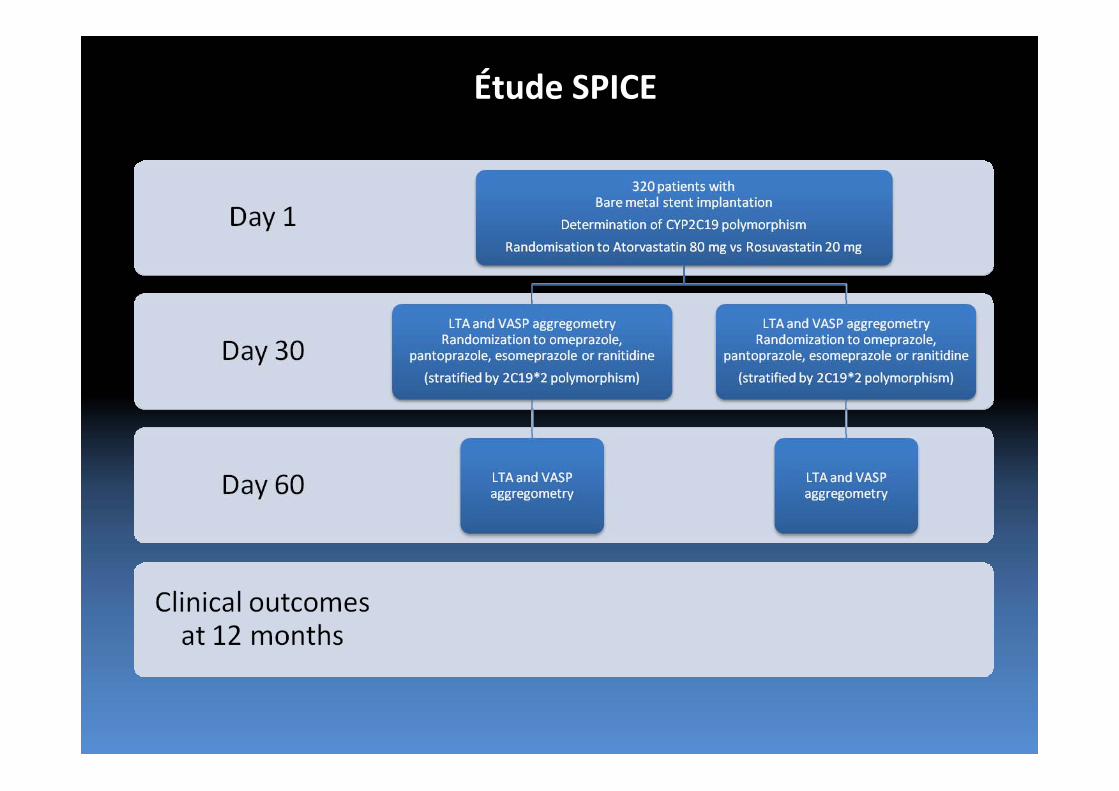
Étude SPICE
Étude prospective, randomisée et ouverte sur l’interaction entre médicaments:
• D’une part on évaluera l’impact de la prise concomitante de clopidogrel avec deux statines métabolisées de façon différente
• D’autre part l’interaction entre le clopidogrel et 3 inhibiteurs de pompe àproton (Ésoméprazole, Oméprazole, pantoprazole) vs la Ranitidine
• L’évaluation des résultats se fera chez des patients bons répondeurs et mauvais répondeurs au clopidogrel • Les 4 sous‐groupes seront constitués de la même quantité de patient porteur du polymorphisme CYP2C19*2• Une analyse par light Transmitance Aggregometry (LTA) et par l’essai VASP sera fait 30 jours après le début du traitement avec le clopidogrel et 30 jours suivant l’ajout d’un IPP
Seul essai randomisé avec trois IPPs, qui prend en considération le polymorphisme génétique CYP2C19*2 et l’effet de l’ajout d’une
statine et d’un IPP
Étude SPICE
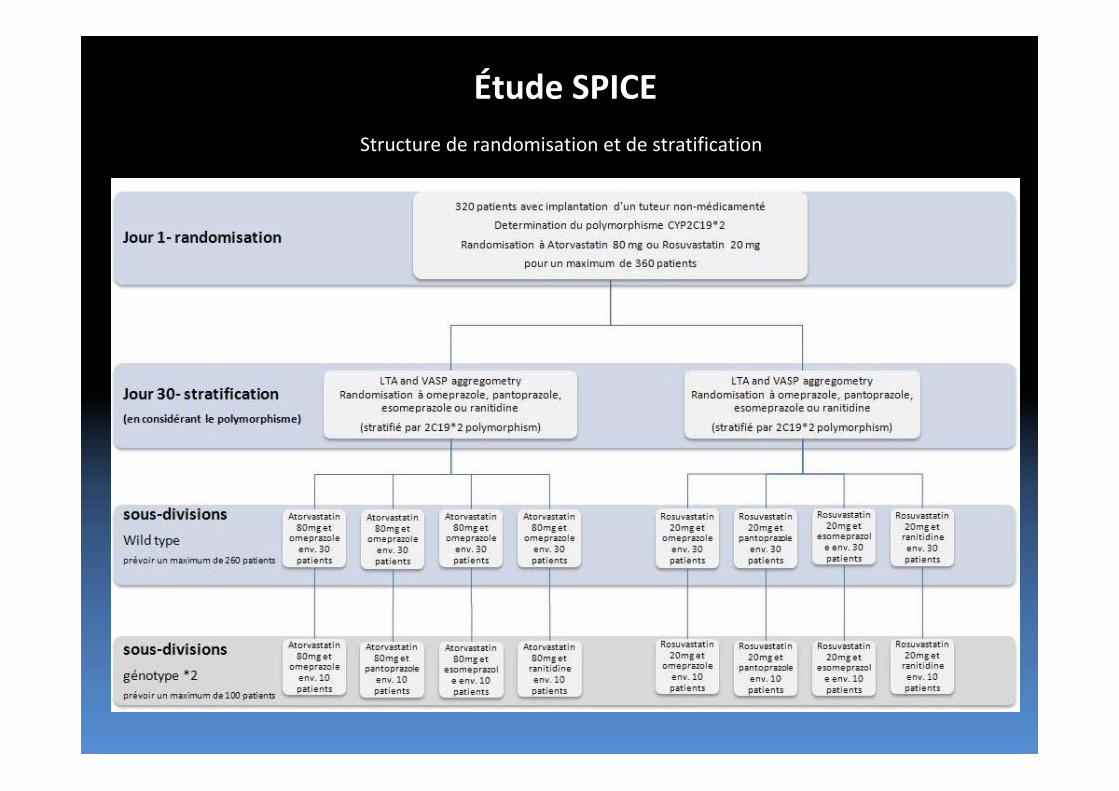
Étude SPICEStructure de randomisation et de stratification
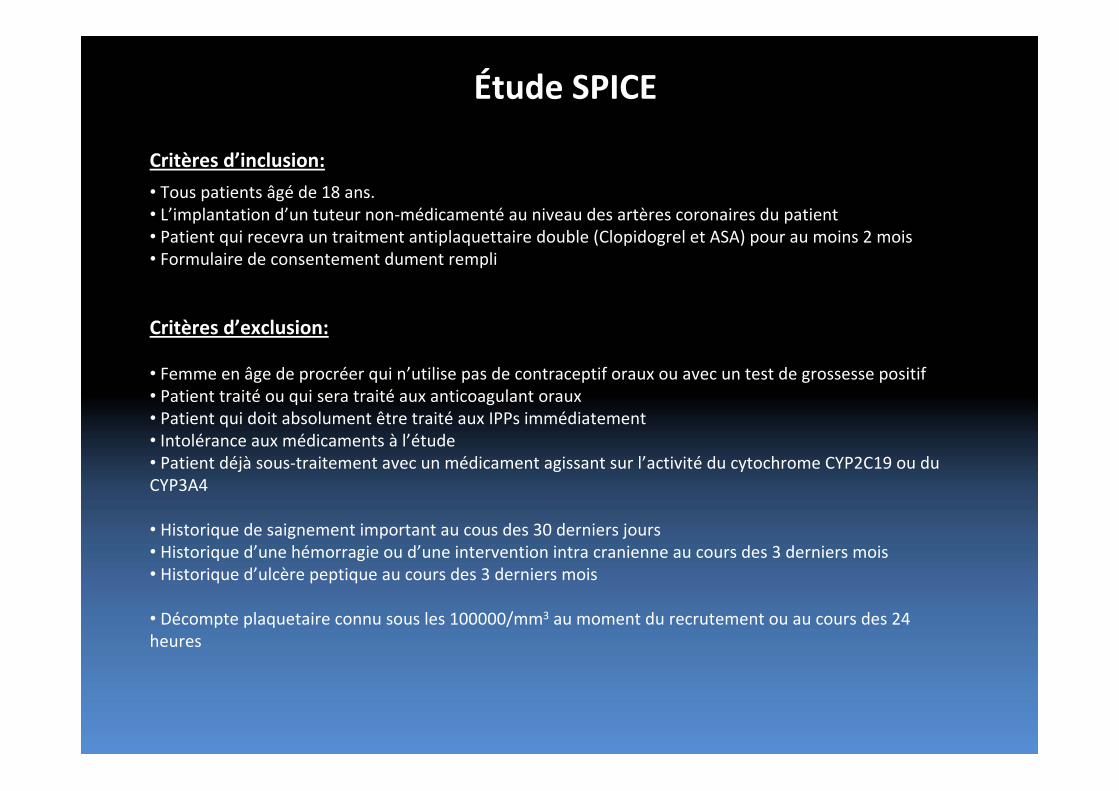
Étude SPICE
Critères d’inclusion:
• Tous patients âgé de 18 ans.• L’implantation d’un tuteur non‐médicamenté au niveau des artères coronaires du patient• Patient qui recevra un traitment antiplaquettaire double (Clopidogrel et ASA) pour au moins 2 mois• Formulaire de consentement dument rempli
Critères d’exclusion:
• Femme en âge de procréer qui n’utilise pas de contraceptif oraux ou avec un test de grossesse positif• Patient traité ou qui sera traité aux anticoagulant oraux• Patient qui doit absolument être traité aux IPPs immédiatement • Intolérance aux médicaments à l’étude• Patient déjà sous‐traitement avec un médicament agissant sur l’activité du cytochrome CYP2C19 ou du CYP3A4
• Historique de saignement important au cous des 30 derniers jours• Historique d’une hémorragie ou d’une intervention intra cranienne au cours des 3 derniers mois• Historique d’ulcère peptique au cours des 3 derniers mois
• Décompte plaquetaire connu sous les 100000/mm3 au moment du recrutement ou au cours des 24 heures
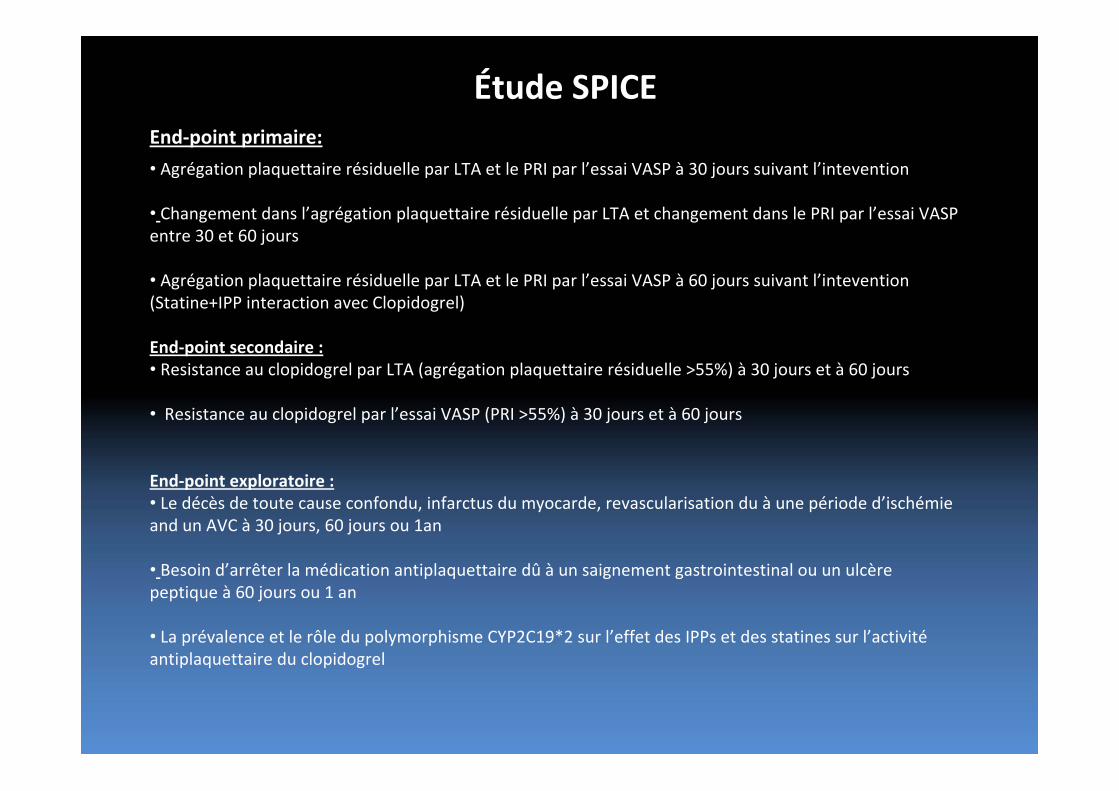
Étude SPICEEnd‐point primaire:
• Agrégation plaquettaire résiduelle par LTA et le PRI par l’essai VASP à 30 jours suivant l’intevention
• Changement dans l’agrégation plaquettaire résiduelle par LTA et changement dans le PRI par l’essai VASP entre 30 et 60 jours
• Agrégation plaquettaire résiduelle par LTA et le PRI par l’essai VASP à 60 jours suivant l’intevention (Statine+IPP interaction avec Clopidogrel)
End‐point secondaire :• Resistance au clopidogrel par LTA (agrégation plaquettaire résiduelle >55%) à 30 jours et à 60 jours
• Resistance au clopidogrel par l’essai VASP (PRI >55%) à 30 jours et à 60 jours
End‐point exploratoire :• Le décès de toute cause confondu, infarctus du myocarde, revascularisation du à une période d’ischémie and un AVC à 30 jours, 60 jours ou 1an
• Besoin d’arrêter la médication antiplaquettaire dû à un saignement gastrointestinal ou un ulcère peptique à 60 jours ou 1 an
• La prévalence et le rôle du polymorphisme CYP2C19*2 sur l’effet des IPPs et des statines sur l’activitéantiplaquettaire du clopidogrel
Interactions médicamenteuses
• Période de question
Nouveaux antagonistes des récepteurs de l’ADP
• Limitations du clopidogrel
• Avantages et inconvénients des nouveaux antagonistes – Prasugrel (Effient)
– Ticagrelor (Brillinta)
• Perspectives futures– Thérapie individualisée
– Point‐of‐care assays
Clopidogrel
• Pro‐drug• Activation par CYP450 2C19 et 3A4
– Potentiel d’interaction médicamenteuse
• Long délai d’action: 2h (600mg) à 12h (300mg)– Nécessité de pré‐traiter
• Variabilité interindividuelle importante– Résistance chez 25‐30% de la population
• Liaison irréversible = longue durée d’action• Degré d’inhibition plaquettaire faible (45%)

Antiplaquettaire idéal
• Inhibition directe
• Réversible
• Inhibition compétitrice
• Début d’action rapide
• Pas d’interactions médicamenteuses
• Pas de variabilité interindividuelle (résistance)
• Plus puissant que plavix (?)

Nouveaux agents
• Prasugrel (Effient), Eli Lilly
• Ticagrelor (Brillanta), Astra
• Cangrelor
• Elinogrel
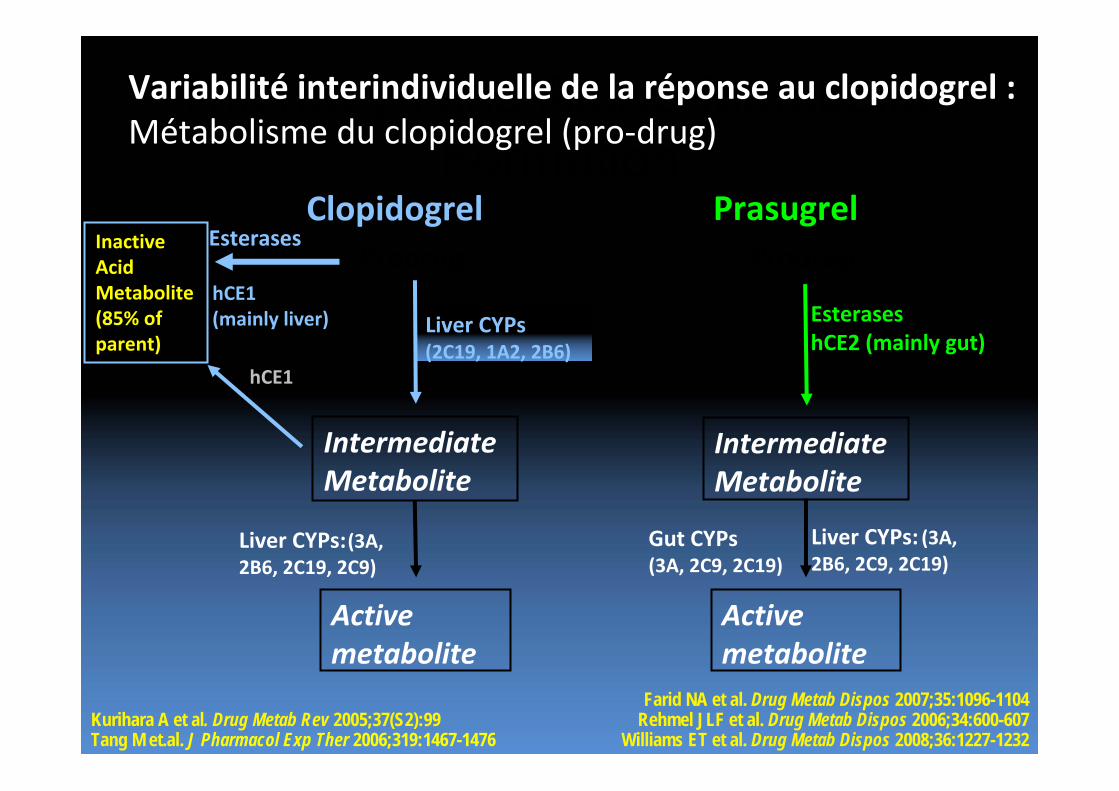
Thienopyridine Active Metabolite Formation
Farid NA et al. Drug Metab Dispos 2007;35:1096-1104Rehmel JLF et al. Drug Metab Dispos 2006;34:600-607
Williams ET et al. Drug Metab Dispos 2008;36:1227-1232Kurihara A et al. Drug Metab Rev 2005;37(S2):99 Tang M et.al. J Pharmacol Exp Ther 2006;319:1467-1476
PrasugrelClopidogrel
Gut CYPs (3A, 2C9, 2C19)
Prodrug
IntermediateMetabolite
Liver CYPs(2C19, 1A2, 2B6)
Activemetabolite
Liver CYPs:(3A,2B6, 2C19, 2C9)
EsterasesInactive Acid Metabolite(85% of parent)
hCE1(mainly liver) Esterases
hCE2 (mainly gut)
Prodrug
Activemetabolite
IntermediateMetabolite
hCE1
Liver CYPs: (3A, 2B6, 2C9, 2C19)
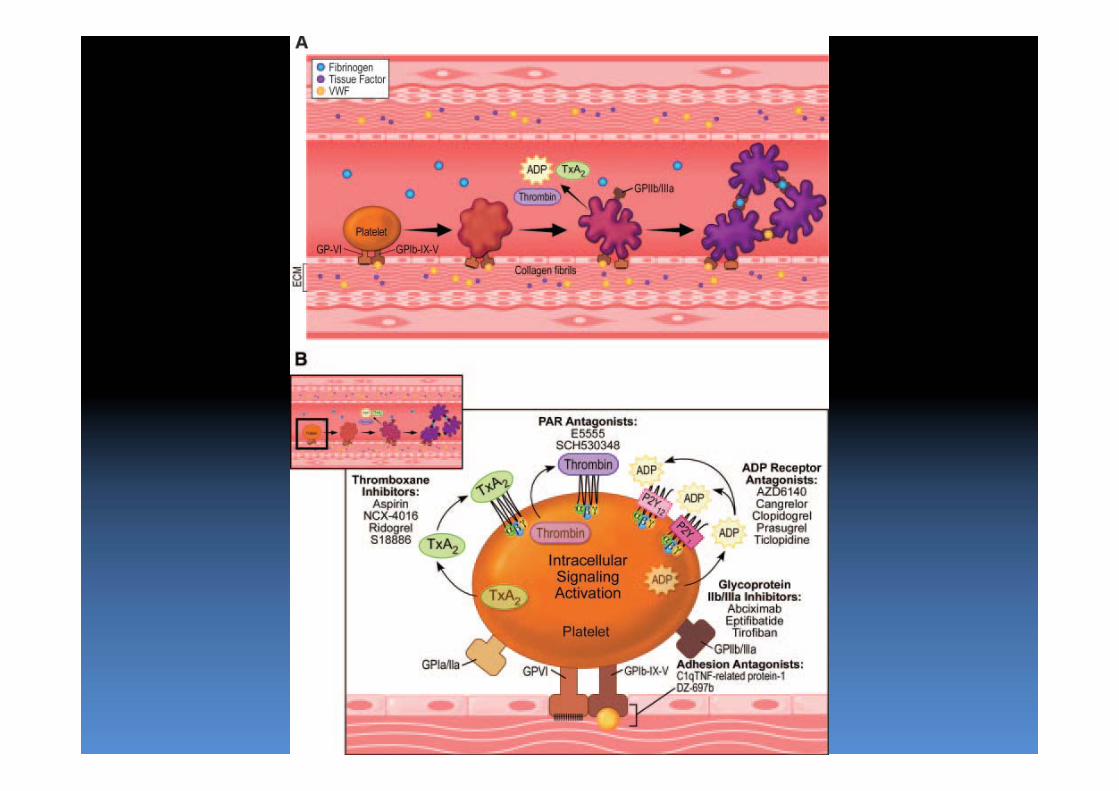
Variabilité interindividuelle de la réponse au clopidogrel :Métabolisme du clopidogrel (pro‐drug)
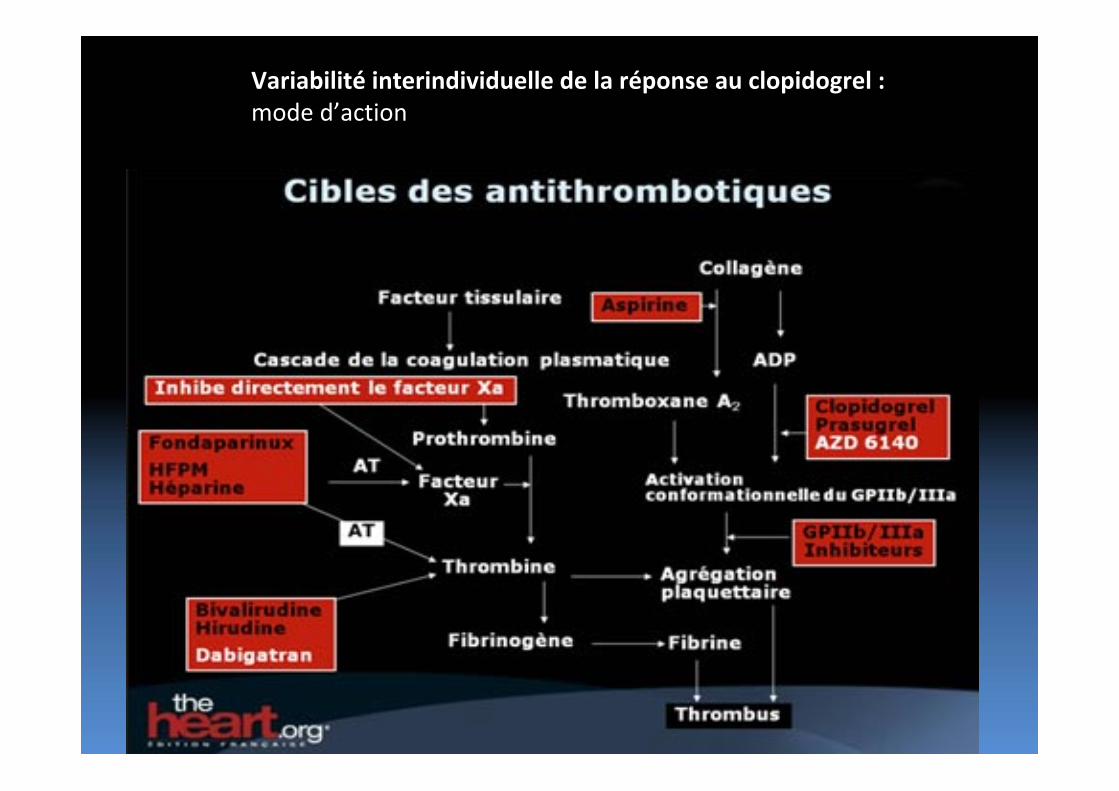
Variabilité interindividuelle de la réponse au clopidogrel :mode d’action
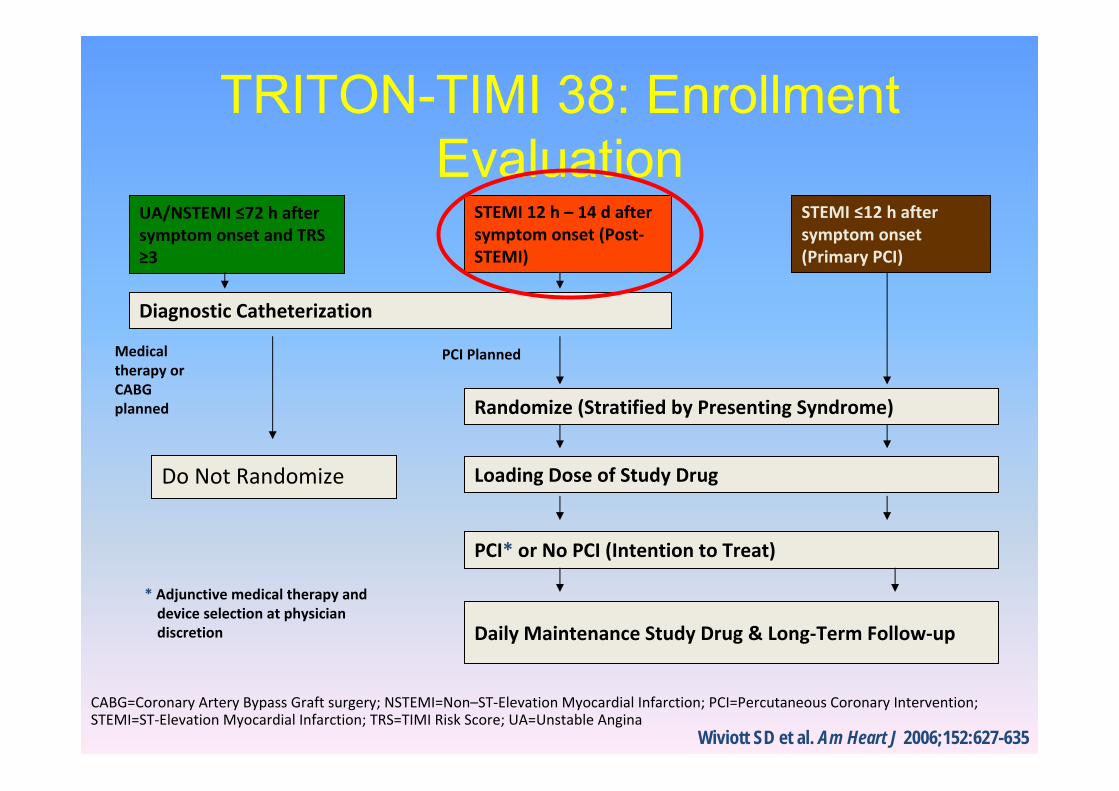
TRITON-TIMI 38: Enrollment Evaluation
UA/NSTEMI ≤72 h after symptom onset and TRS ≥3
STEMI 12 h – 14 d after symptom onset (Post‐STEMI)
STEMI ≤12 h after symptom onset (Primary PCI)
Diagnostic Catheterization
Randomize (Stratified by Presenting Syndrome)
Loading Dose of Study Drug
Daily Maintenance Study Drug & Long‐Term Follow‐up
* Adjunctive medical therapy and device selection at physician discretion
Medical therapy or CABG planned
PCI Planned
PCI* or No PCI (Intention to Treat)
Wiviott SD et al. Am Heart J 2006;152:627-635
CABG=Coronary Artery Bypass Graft surgery; NSTEMI=Non–ST‐Elevation Myocardial Infarction; PCI=Percutaneous Coronary Intervention; STEMI=ST‐Elevation Myocardial Infarction; TRS=TIMI Risk Score; UA=Unstable Angina
Do Not Randomize
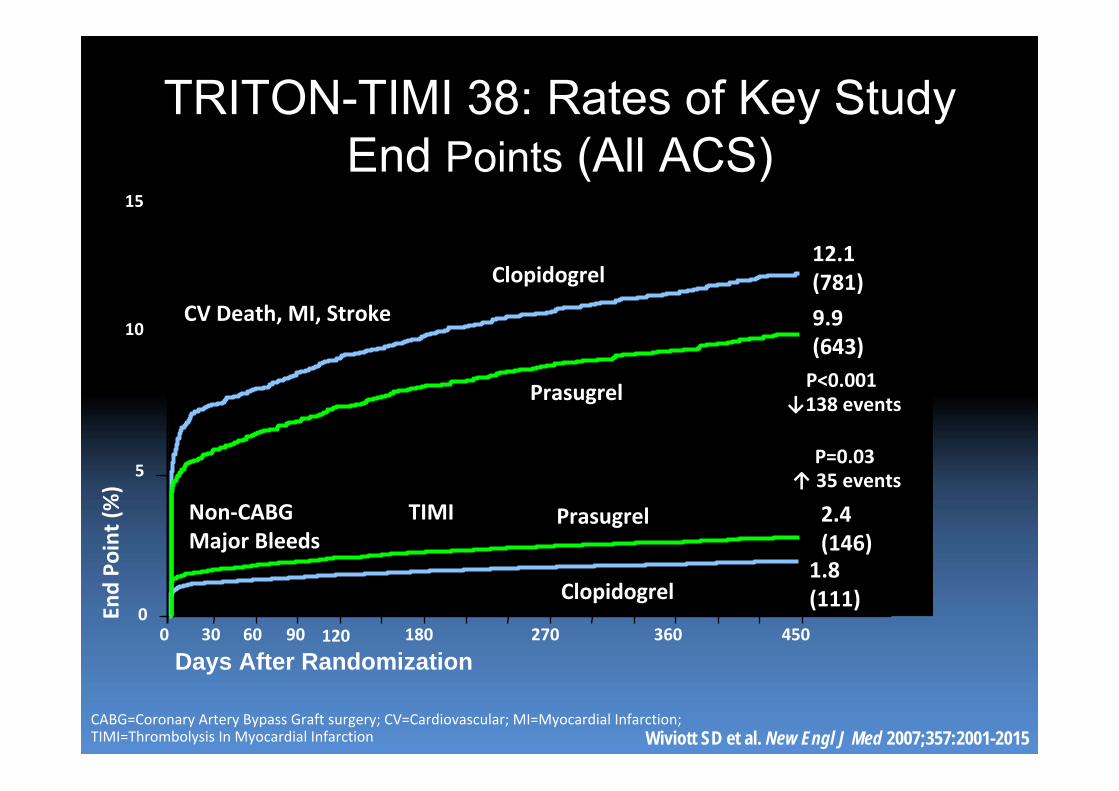
CABG=Coronary Artery Bypass Graft surgery; CV=Cardiovascular; MI=Myocardial Infarction; TIMI=Thrombolysis In Myocardial Infarction
Prasugrel
Clopidogrel
TRITON-TIMI 38: Rates of Key Study End Points (All ACS)
Wiviott SD et al. New Engl J Med 2007;357:2001-2015
5
10
15
00 30 60 90 180 270 360 450
Days After Randomization
End Po
int (%)
120
1.8 (111)
2.4(146)
Non‐CABG TIMI Major Bleeds
CV Death, MI, Stroke
P=0.03
P<0.001↓138 events
↑ 35 events
12.1(781)
9.9 (643)
Prasugrel
Clopidogrel
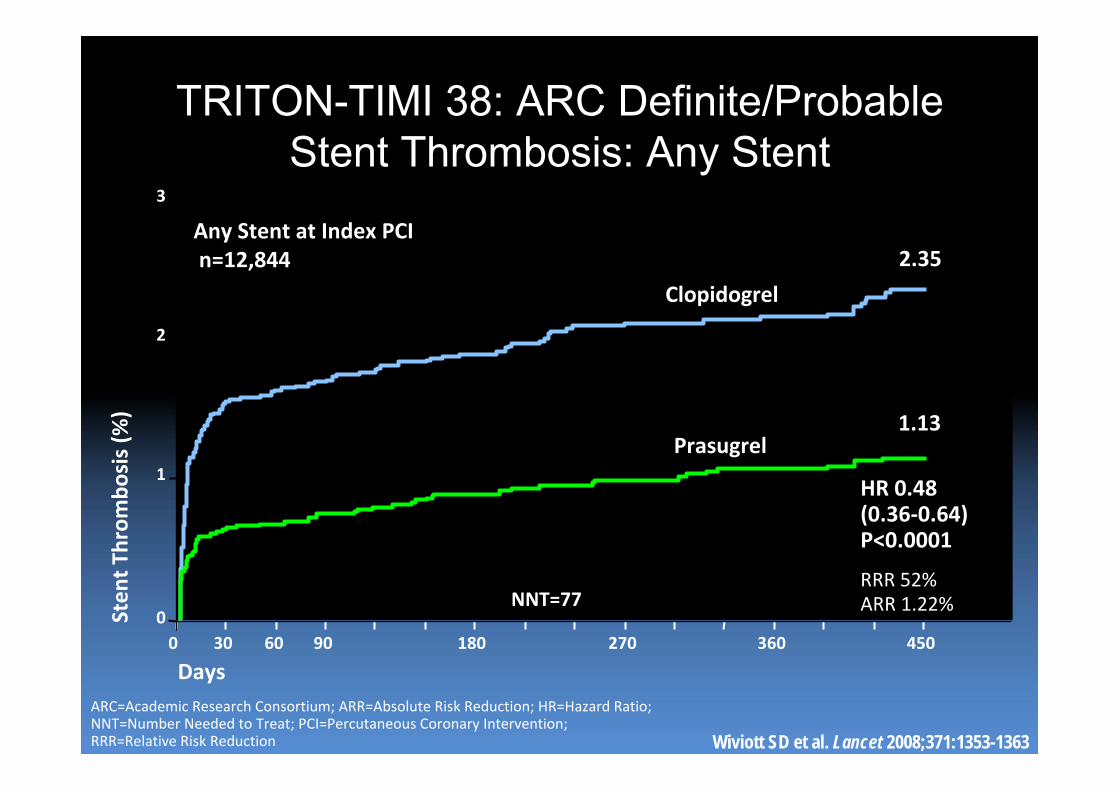
TRITON-TIMI 38: ARC Definite/Probable Stent Thrombosis: Any Stent
ARC=Academic Research Consortium; ARR=Absolute Risk Reduction; HR=Hazard Ratio; NNT=Number Needed to Treat; PCI=Percutaneous Coronary Intervention; RRR=Relative Risk Reduction Wiviott SD et al. Lancet 2008;371:1353-1363
0 30 60 90 180 270 360 450
HR 0.48 (0.36‐0.64)P<0.0001
RRR 52%ARR 1.22%
Prasugrel
Clopidogrel
2.35
1.13
Days
Sten
t Throm
bosis (%
)
Any Stent at Index PCIn=12,844
0
1
2
3
NNT=77
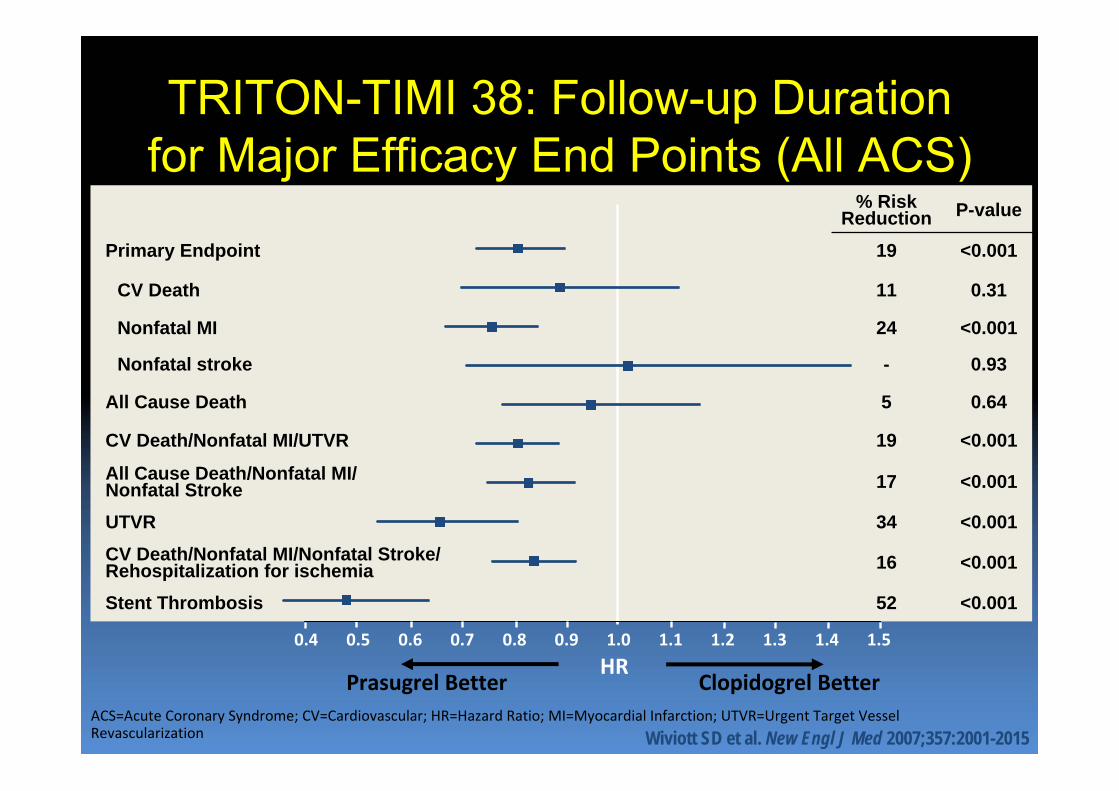
TRITON-TIMI 38: Follow-up Duration for Major Efficacy End Points (All ACS)
ACS=Acute Coronary Syndrome; CV=Cardiovascular; HR=Hazard Ratio; MI=Myocardial Infarction; UTVR=Urgent Target Vessel Revascularization
0.5
Prasugrel Better Clopidogrel BetterHR
0.4 0.6 0.7 0.8 0.9 1.1 1.2 1.3 1.41.0 1.5
Wiviott SD et al. New Engl J Med 2007;357:2001-2015
% Risk Reduction P-value
Primary Endpoint 19 <0.001
CV Death 11 0.31
Nonfatal MI 24 <0.001
Nonfatal stroke - 0.93
All Cause Death 5 0.64
CV Death/Nonfatal MI/UTVR 19 <0.001
All Cause Death/Nonfatal MI/Nonfatal Stroke 17 <0.001
UTVR 34 <0.001CV Death/Nonfatal MI/Nonfatal Stroke/Rehospitalization for ischemia 16 <0.001
Stent Thrombosis 52 <0.001
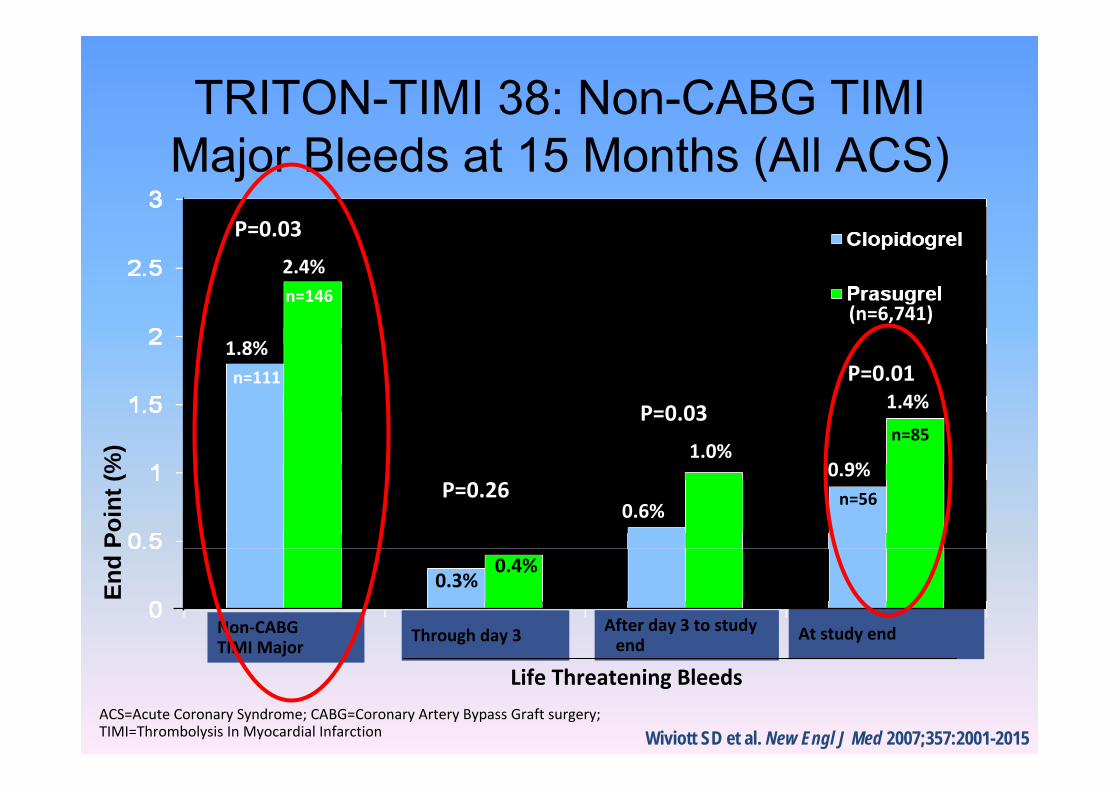
TRITON-TIMI 38: Non-CABG TIMI Major Bleeds at 15 Months (All ACS)
ACS=Acute Coronary Syndrome; CABG=Coronary Artery Bypass Graft surgery; TIMI=Thrombolysis In Myocardial Infarction
End
Poin
t (%
)
Non‐CABGTIMI Major
Through day 3 At study endAfter day 3 to study end
(n=6,716)
(n=6,741)
Life Threatening Bleeds
1.8%
0.4%0.3%
1.0%
0.6%
n=111
2.4%n=146
0.9%n=56
1.4%
n=85
P=0.03
P=0.26
P=0.03
P=0.01
Wiviott SD et al. New Engl J Med 2007;357:2001-2015
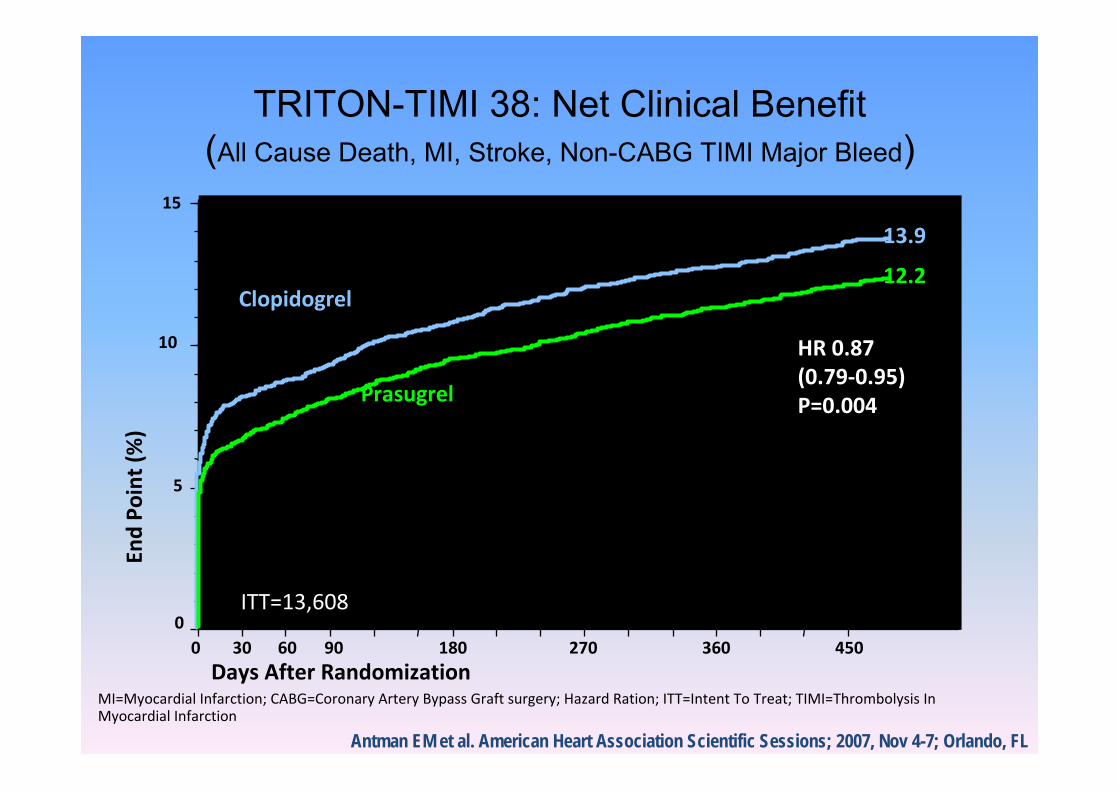
Days After RandomizationMI=Myocardial Infarction; CABG=Coronary Artery Bypass Graft surgery; Hazard Ration; ITT=Intent To Treat; TIMI=Thrombolysis In Myocardial Infarction
Antman EM et al. American Heart Association Scientific Sessions; 2007, Nov 4-7; Orlando, FL
0
5
10
15
0 30 60 90 180 270 360 450
End Po
int (%)
HR 0.87 (0.79‐0.95)P=0.004
13.9
12.2
ITT=13,608
Prasugrel
Clopidogrel
TRITON-TIMI 38: Net Clinical Benefit(All Cause Death, MI, Stroke, Non-CABG TIMI Major Bleed)
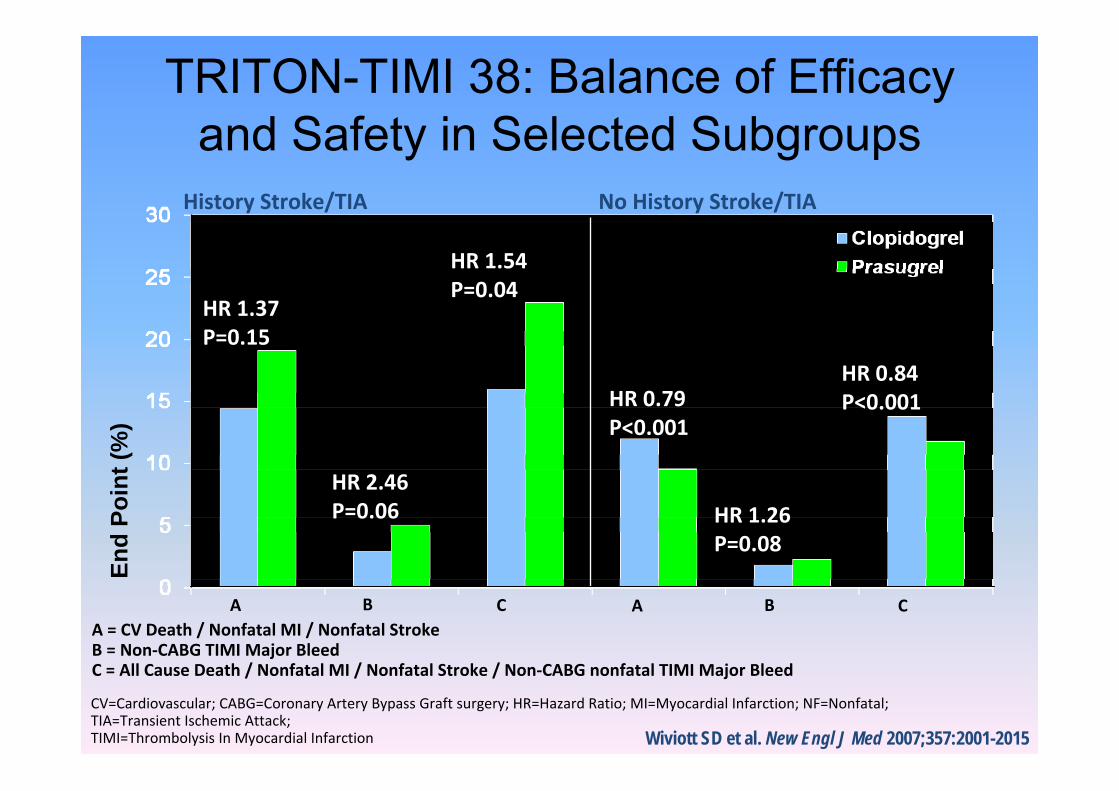
CV=Cardiovascular; CABG=Coronary Artery Bypass Graft surgery; HR=Hazard Ratio; MI=Myocardial Infarction; NF=Nonfatal; TIA=Transient Ischemic Attack; TIMI=Thrombolysis In Myocardial Infarction
A = CV Death / Nonfatal MI / Nonfatal StrokeB = Non‐CABG TIMI Major BleedC = All Cause Death / Nonfatal MI / Nonfatal Stroke / Non‐CABG nonfatal TIMI Major Bleed
History Stroke/TIA No History Stroke/TIA
End
Poin
t (%
)
A B C A B C
TRITON-TIMI 38: Balance of Efficacy and Safety in Selected Subgroups
Wiviott SD et al. New Engl J Med 2007;357:2001-2015
HR 2.46 P=0.06
HR 1.37 P=0.15
HR 0.79 P<0.001
HR 1.26 P=0.08
HR 1.54 P=0.04
HR 0.84 P<0.001
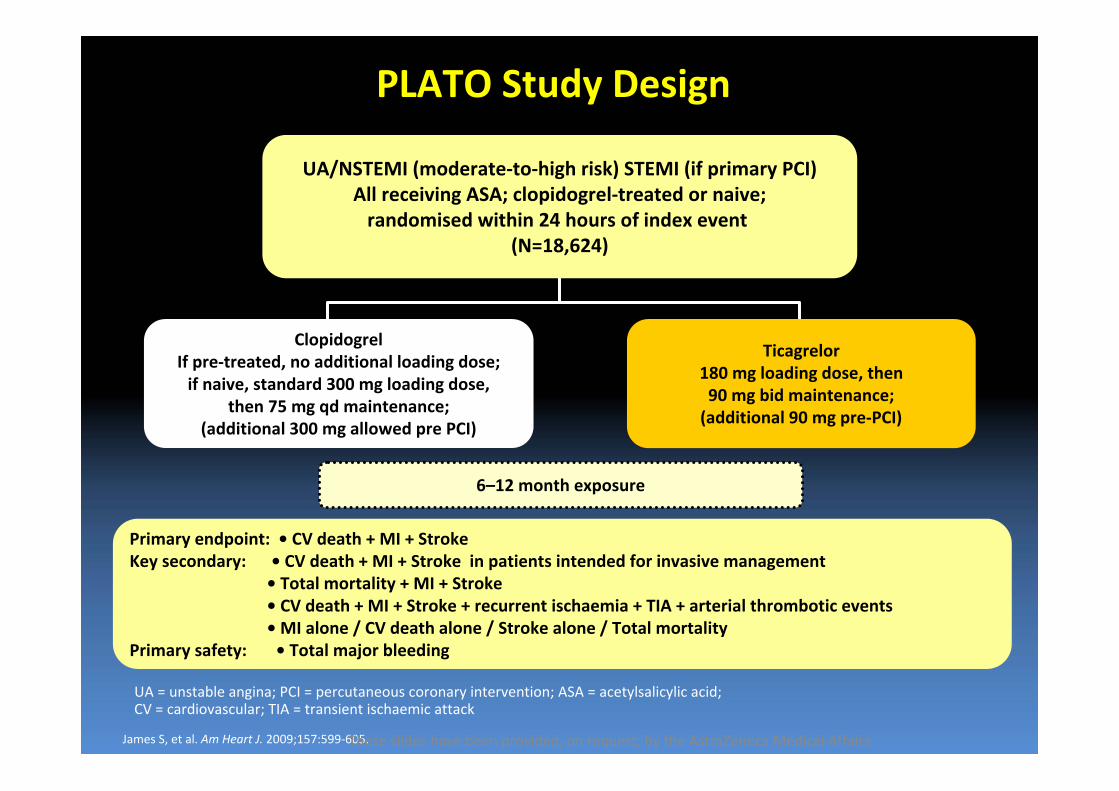
PLATO Study Design
Primary endpoint: • CV death + MI + Stroke Key secondary: • CV death + MI + Stroke in patients intended for invasive management
• Total mortality + MI + Stroke • CV death + MI + Stroke + recurrent ischaemia + TIA + arterial thrombotic events• MI alone / CV death alone / Stroke alone / Total mortality
Primary safety: • Total major bleeding
6–12 month exposure
ClopidogrelIf pre‐treated, no additional loading dose;if naive, standard 300 mg loading dose,
then 75 mg qd maintenance;(additional 300 mg allowed pre PCI)
Ticagrelor180 mg loading dose, then90 mg bid maintenance;(additional 90 mg pre‐PCI)
UA/NSTEMI (moderate‐to‐high risk) STEMI (if primary PCI)All receiving ASA; clopidogrel‐treated or naive;randomised within 24 hours of index event
(N=18,624)
UA = unstable angina; PCI = percutaneous coronary intervention; ASA = acetylsalicylic acid; CV = cardiovascular; TIA = transient ischaemic attack
James S, et al. Am Heart J. 2009;157:599‐605.These slides have been provided, on request, by the AstraZeneca Medical Affairs
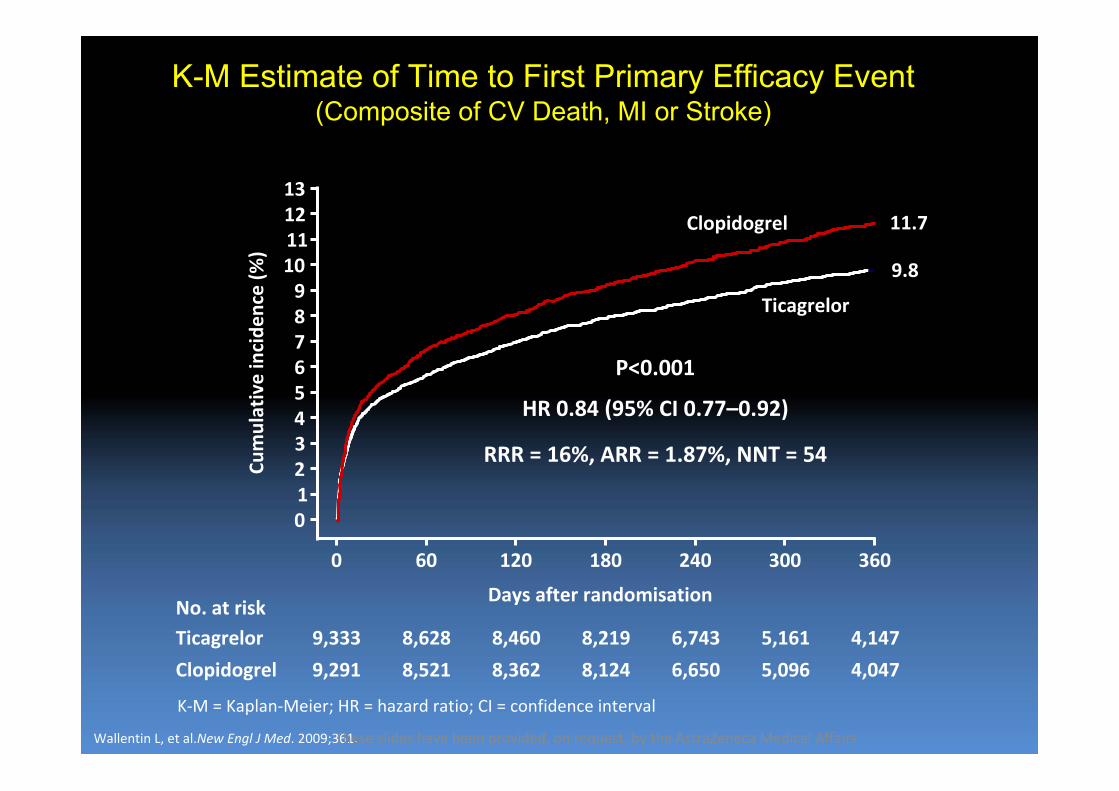
K-M Estimate of Time to First Primary Efficacy Event (Composite of CV Death, MI or Stroke)
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,521
8,628
8,362
8,460
8,124
Days after randomisation
6,650
6,743
5,096
5,161
4,047
4,147
0 60 120 180 240 300 360
1211109876543210
13
Cumulative incide
nce (%
)9.8
11.7
8,219
P<0.001
HR 0.84 (95% CI 0.77–0.92)
RRR = 16%, ARR = 1.87%, NNT = 54
Clopidogrel
Ticagrelor
K‐M = Kaplan‐Meier; HR = hazard ratio; CI = confidence interval
Wallentin L, et al.New Engl J Med. 2009;361.These slides have been provided, on request, by the AstraZeneca Medical Affairs
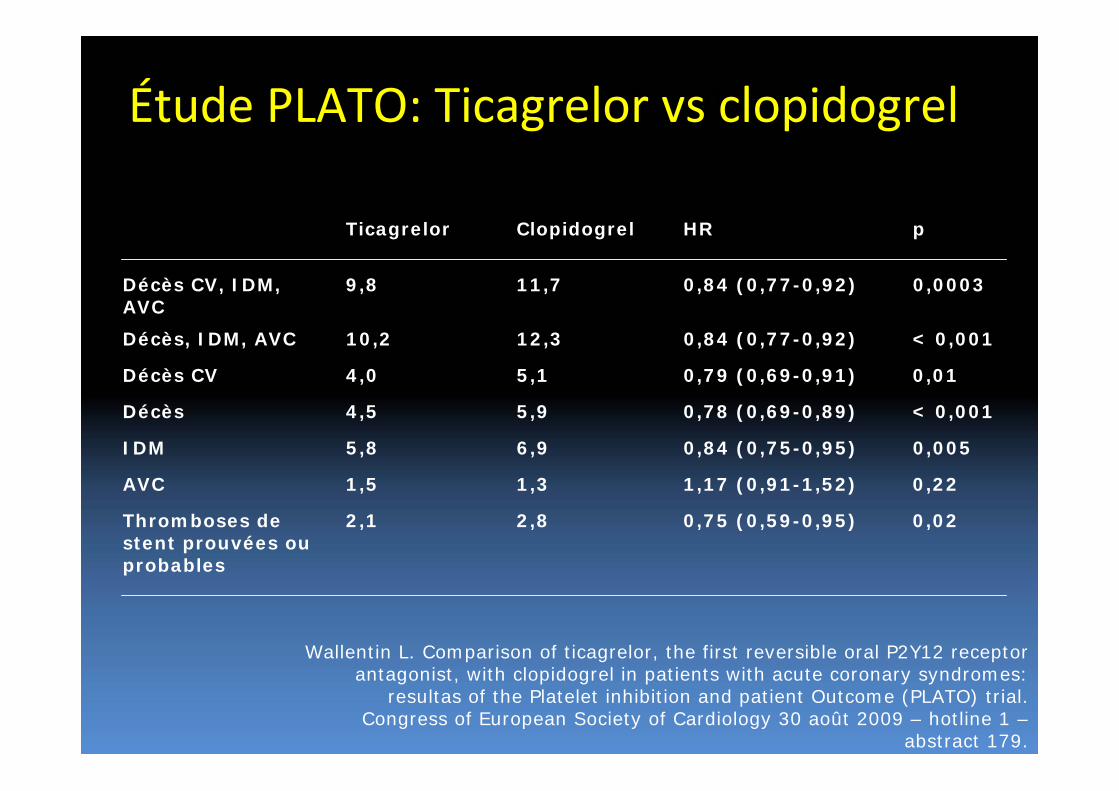
Étude PLATO : principaux critères de jugement
Wallentin L. Comparison of ticagrelor, the first reversible oral P2Y12 receptor antagonist, with clopidogrel in patients with acute coronary syndromes:
resultas of the Platelet inhibition and patient Outcome (PLATO) trial. Congress of European Society of Cardiology 30 août 2009 – hotline 1 –
abstract 179.
Ticagrelor Clopidogrel HR p
Décès CV, IDM, AVC
9,8 11,7 0,84 (0,77-0,92) 0,0003
Décès, IDM, AVC 10,2 12,3 0,84 (0,77-0,92) < 0,001
Décès CV 4,0 5,1 0,79 (0,69-0,91) 0,01
Décès 4,5 5,9 0,78 (0,69-0,89) < 0,001
IDM 5,8 6,9 0,84 (0,75-0,95) 0,005
AVC 1,5 1,3 1,17 (0,91-1,52) 0,22
Thromboses de stent prouvées ou probables
2,1 2,8 0,75 (0,59-0,95) 0,02
Étude PLATO: Ticagrelor vs clopidogrel
132
133
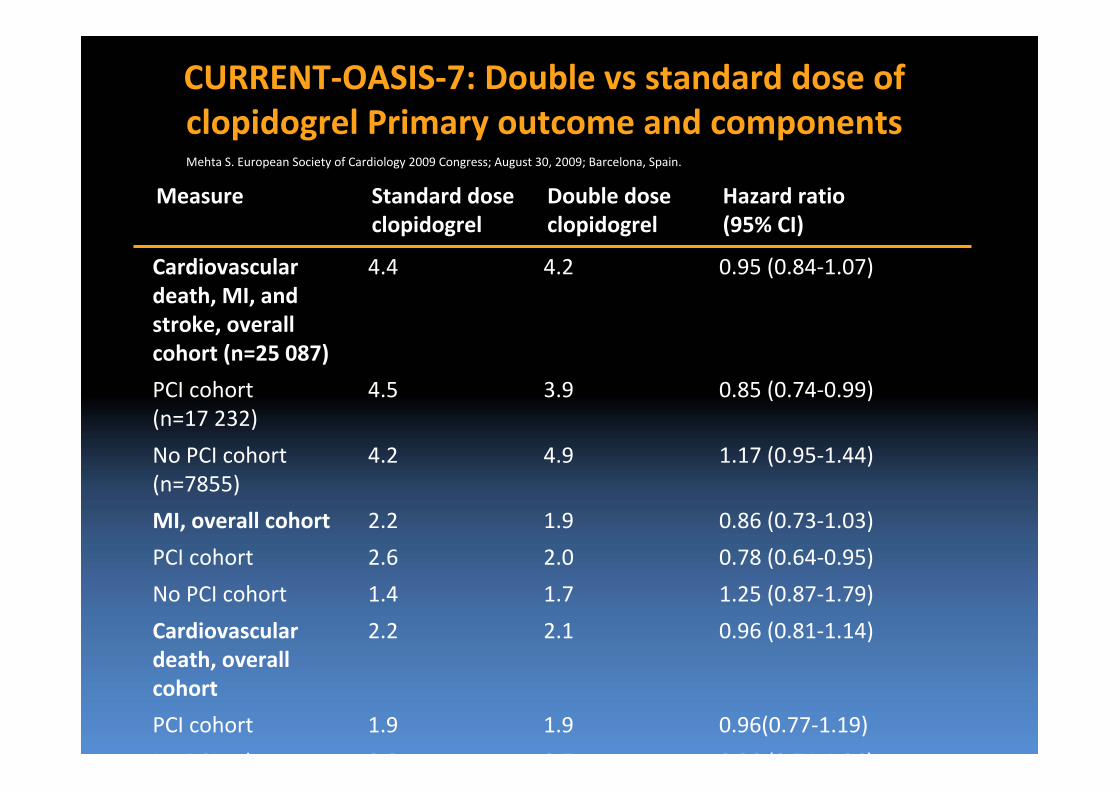
Measure Standard dose clopidogrel
Double dose clopidogrel
Hazard ratio(95% CI)
Cardiovascular death, MI, and stroke, overall cohort (n=25 087)
4.4 4.2 0.95 (0.84‐1.07)
PCI cohort (n=17 232)
4.5 3.9 0.85 (0.74‐0.99)
No PCI cohort (n=7855)
4.2 4.9 1.17 (0.95‐1.44)
MI, overall cohort 2.2 1.9 0.86 (0.73‐1.03)
PCI cohort 2.6 2.0 0.78 (0.64‐0.95)
No PCI cohort 1.4 1.7 1.25 (0.87‐1.79)
Cardiovascular death, overall cohort
2.2 2.1 0.96 (0.81‐1.14)
PCI cohort 1.9 1.9 0.96(0.77‐1.19)
N PCI h 2 8 2 7 0 96 (0 74 1 26)
CURRENT‐OASIS‐7: Double vs standard dose of clopidogrel Primary outcome and componentsMehta S. European Society of Cardiology 2009 Congress; August 30, 2009; Barcelona, Spain.
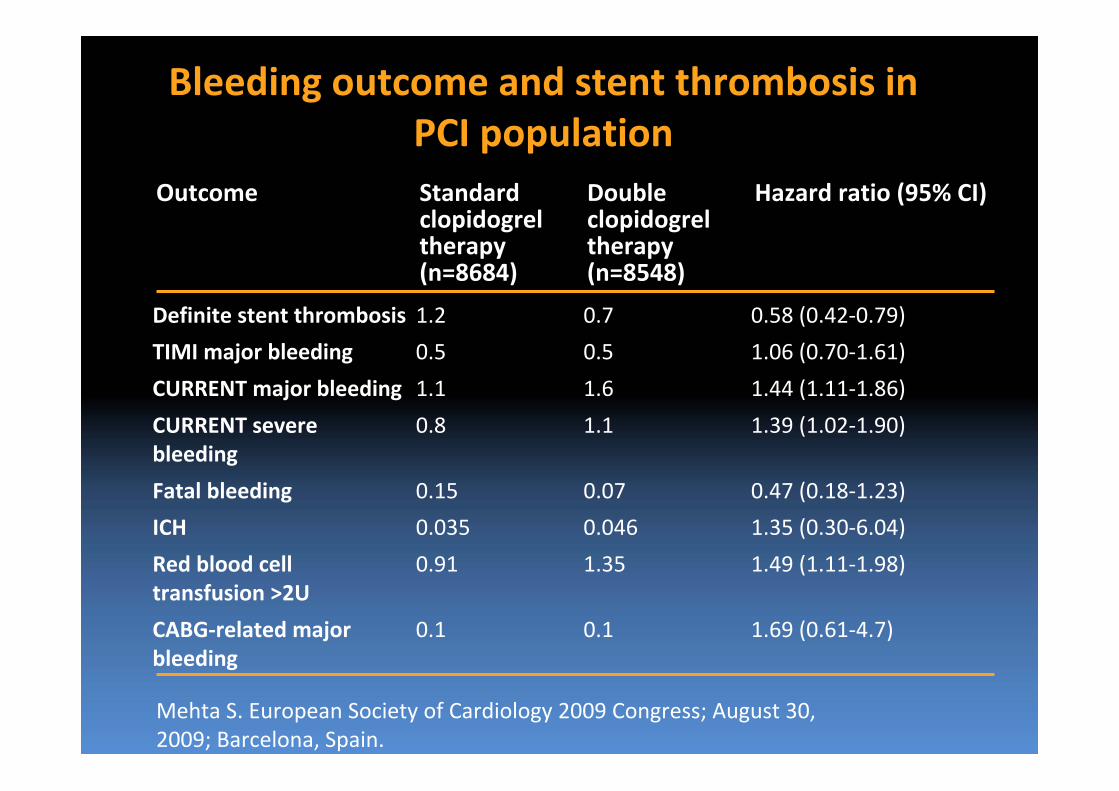
Outcome Standard clopidogrel therapy (n=8684)
Double clopidogrel therapy (n=8548)
Hazard ratio (95% CI)
Definite stent thrombosis 1.2 0.7 0.58 (0.42‐0.79)
TIMI major bleeding 0.5 0.5 1.06 (0.70‐1.61)
CURRENT major bleeding 1.1 1.6 1.44 (1.11‐1.86)
CURRENT severe bleeding
0.8 1.1 1.39 (1.02‐1.90)
Fatal bleeding 0.15 0.07 0.47 (0.18‐1.23)
ICH 0.035 0.046 1.35 (0.30‐6.04)
Red blood cell transfusion >2U
0.91 1.35 1.49 (1.11‐1.98)
CABG‐related major bleeding
0.1 0.1 1.69 (0.61‐4.7)
Bleeding outcome and stent thrombosis in PCI population
Mehta S. European Society of Cardiology 2009 Congress; August 30, 2009; Barcelona, Spain.
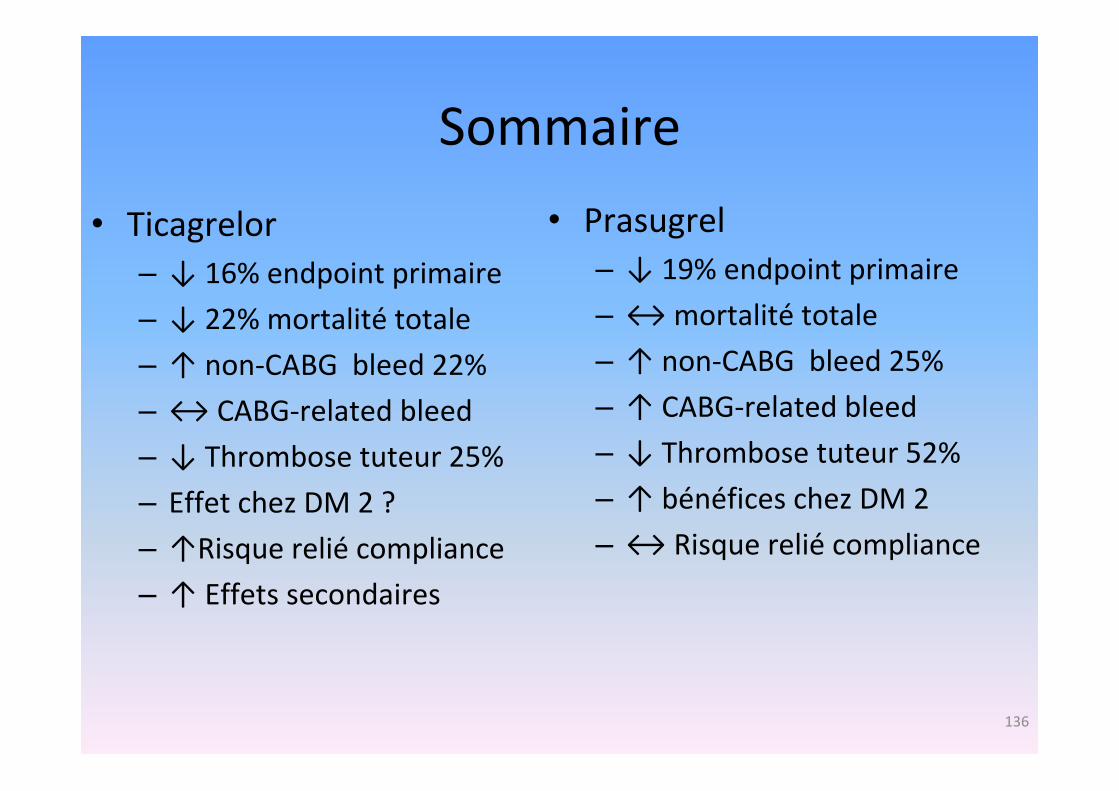
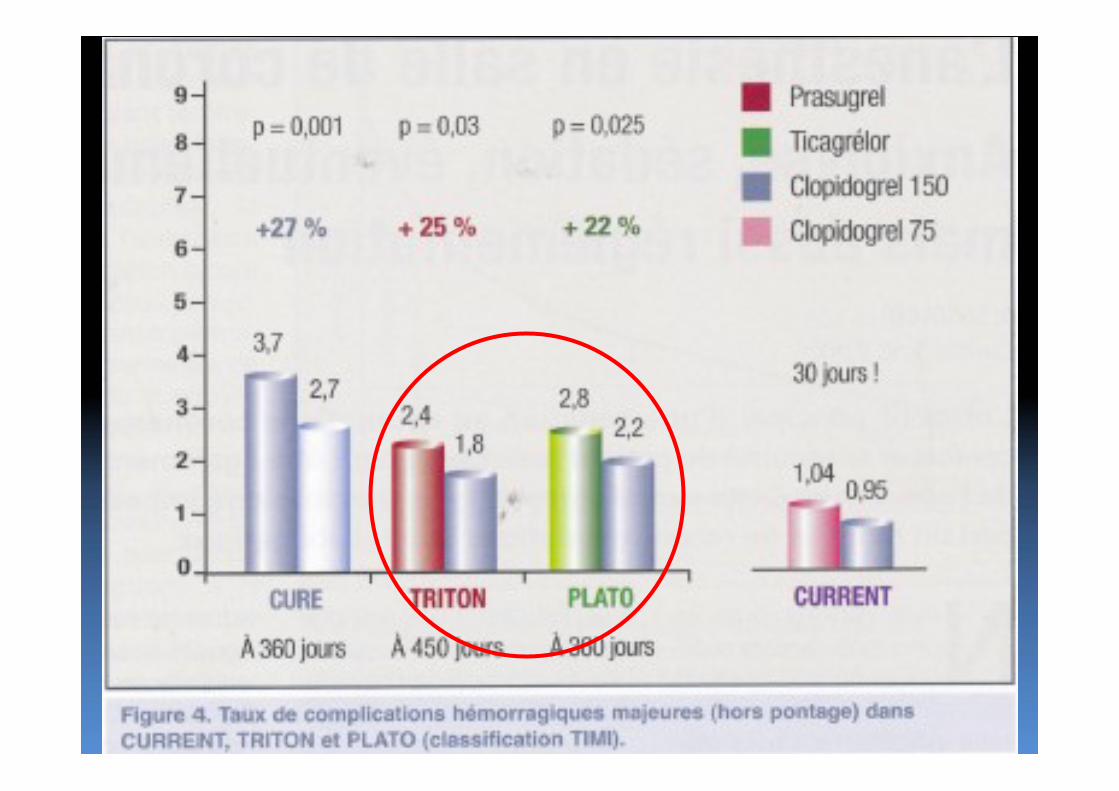
Sommaire
• Ticagrelor– ↓ 16% endpoint primaire
– ↓ 22% mortalité totale
– ↑ non‐CABG bleed 22%
– ↔ CABG‐related bleed
– ↓ Thrombose tuteur 25%
– Effet chez DM 2 ?
– ↑Risque relié compliance
– ↑ Effets secondaires
• Prasugrel– ↓ 19% endpoint primaire
– ↔mortalité totale
– ↑ non‐CABG bleed 25%
– ↑ CABG‐related bleed
– ↓ Thrombose tuteur 52%
– ↑ bénéfices chez DM 2
– ↔ Risque relié compliance
136
L’AVENIR…
• Thérapie antiplaquettaire personnalisée– Le degré d’agrégation plaquettaire sous traitement prédit les événements cliniques
• Light transmittance aggregometry• VASP• Verify now
– Une partie des non‐répondeurs au clopidogrel répondent à une dose plus haute de clopidogrel
– La majorité répondent au ticagrelor • étude RESPOND
Étude à surveiller
• GRAVITAS– Clopidogrel 150mg vs 75mg chez non répondeurs
– Environ 4000 patients suivis 6 mois suite àimplantation d’un tuteur pharmacoactif
Études originales à venir à l’IUCPQ
• Étude BADCOP– Better Antiplatelet effect with Double dose Clopidogrel Or Prasugrel in patients with high platelet reactivity under standard dose clopidogrel
• Étude de l’effet antiplaquettaire du ticagrelor et du clopidogrel chez les obèses morbides avant et après une chirurgie bariatrique
• Étude PREPPIE– Prasugrel to REduce Peri‐Procedural Ischemic Events
Nouveaux anti‐plaquettaires
• Période de question

![h patites autoimmunes [Mode de compatibilit ] - SNFMI · Disclosures • Dr P. Cacoub has received consulting and lecturing fees from : Astra Zeneca, Bristol-Myers Squibb, Gilead,](https://img.pdfslide.fr/doc/110x75/5e121f51f2bce03f5b3a7cf6/h-patites-autoimmunes-mode-de-compatibilit-disclosures-a-dr-p-cacoub-has.jpg)