Embed Size (px)
Citation preview
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 1/19
Chronic disorder in which the heart can nolonger pump sufficient blood to meet
metabolic demands of the body.
CONGESTIVE HEART FAILURE
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 2/19

8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 3/19
H igh Output F ailure ² Occurs when condition causes the heart towork harder to met demands of the body
S ystolic F ailure ² leads to problem with contraction & ejection of blood
D iastolic F ailure ² leads to problem with the heart relaxing & fillingof blood
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 4/19
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 5/19
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 6/19
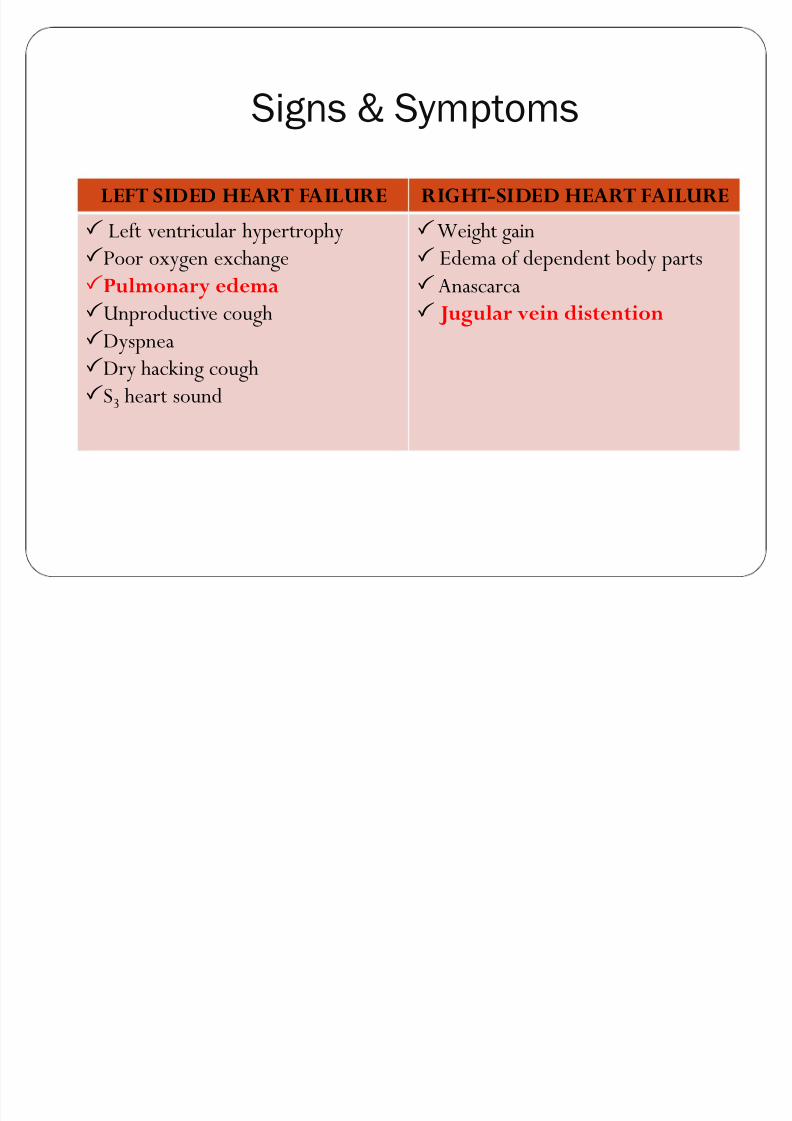
Signs & Symptoms
LEFT SIDED HEART FAILURE RIGHT-SIDED HEART FAILURE
L eft ventricular hypertrophyPoor oxygen exchangePulmonary edemaU nproductive coughDyspneaDry hacking coughS3 heart sound
Weight gainEdema of dependent body partsAnascarcaJugular vein distention
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 7/19
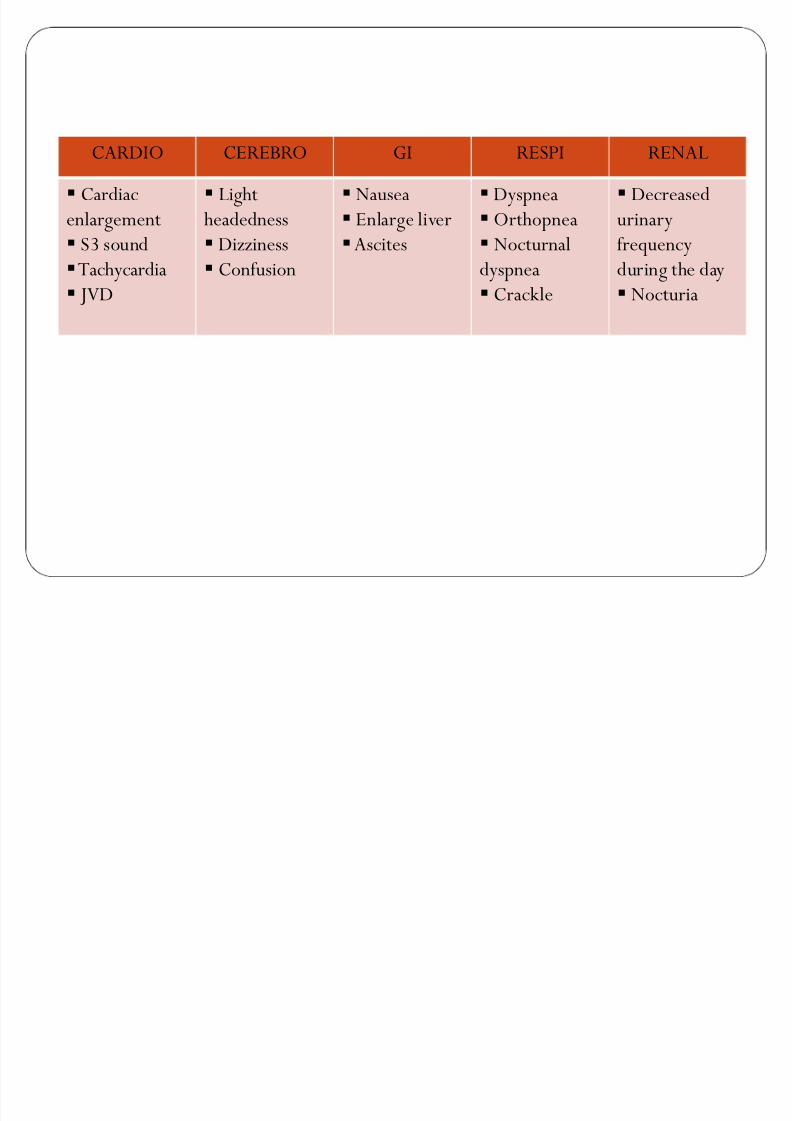
CARDIO CEREBRO GI RESPI RENAL
Cardiacenlargement
S3 sound
Tachycardia JVD
L ightheadedness
Dizziness
Confusion
NauseaEnlarge liverAscites
DyspneaOrthopneaNocturnal
dyspneaCrackle
Decreasedurinaryfrequency
during the dayNocturia
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 8/19
D IAGNOSTIC TEST
Chest X - rayE CG
E chocardiography
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 9/19
Coronary artery revascularization with percutaneous angioplasty orbypass surgery ² if patient have underlying coronary artery disease
Cardiac resynchronization ² involving the use of left ventricular and biventricularpacing,treatment for hf with electrical conduction defects
I nternal cardiac defibrillator ² use to prevent dangerous heart rhythm
H eart pump (ventricular assistive device)
M ED ICALM ANAGEM ENT
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 10/19
H eart valve replacementCoronary bypass surgeryH eart transplant
Myectomy
SURGICAL M ANAGEM ENT
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 11/19
I ntropicsD iuretics
T hiazide
L oopPotassium -S paring
VasodilatorsA CE I nhibitors
P HARM ACOLOGICALM ANAGEM ENT
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 12/19
IntropicsD igitalis ² increase force of myocardial contraction helpincrease cardiac output
Nursing ConsiderationsR ecognize therapeutic dose and toxic dose is narrowObserve signs of toxicity
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 13/19
D iuretics1. T hiazide D iuretics
o Chlorothiazide ( D iuril) & H ydrochlorothiazide(H ydro D iuril)
o Promote excretion of sodium, chloride and watero A dverse effects: H ypokalemia & H yperkalemia
2. L oop D iureticso F urosemide ( L asix)o Promote excretion of sodium and water by blocking
reabsorption in the L oop of H enleo A dverse E ffects: H ypokalemia, H yonatremia &
H yperglycemia
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 14/19
3. Potassium ² S paring D iuretics
o S pironolactone ( A ldactone)o I nhibits action of aldosterone in the distal tubule ²
leading to sodium excretion and potassiumretention
o A dverse E ffects: H yperkalemia
Nursing ConsiderationsM onitor intake, output, weight, and serum electrolytelevelsCaution patients to change positions slowlyA dminister diuretic in the morning
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 15/19
Vasodilatorso H ydralazine, Nitrates, Prazosino Vasodilator drugs: relax pulmonary arterial and
venous vessels, dilating vessels, causing pooling of blood & reducing resistance in the systemic arterialvessels.
Nursing ConsiderationA dvise patients taking nirates, may experience headachesR emind patient to change positions slowly to prevent
orthostatic hypotension
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 16/19
ACE Inhibitorso Captopril, B enazeprilo I nterrupt RAA cycleo T hese drugs promote vasodilation and diuresis by
decreasing afterload and preload
Nursing ConsiderationCarefully monitor patient for H yperkalemia
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 17/19
D ecreased cardiac output related to impaired inotropic state of the myocardium
I mpaired gas exchange related to increased pulmonarycongestion secondary to increased left ventricular and diastolicpressure
E xcess fluid volume related to fluid retention secondary todecreased renal perfusion
NURSING D IAGNOSIS
8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 18/19
Nursing M anagemento Providing supplemental oxygen at 2 to 4L /min
o maintain or improve oxygenationo Promote Rest and Activity
o minimize O2 demando Diet modification
a. Salt restriction b. For decompensated patient the water intake is restricted by 1.5 ² 2L per
day to avoid water retention and significant hyponatremia

8/3/2019 NCM1o6 - CHF
http://slidepdf.com/reader/full/ncm1o6-chf 19/19
c.Avoid alcohol-can interact with cardiac agent and maycause
cardiomyopathyo Stop Smoking
o causes vasoconstriction
o Adherence and compliance to medicationo Exercise should be base on the clinical condition and status as long as itwill not cause show symptoms of decompensationo Caution for driving and traveling airplane
o pressure changes o2 concentrationo Promote pulmonary hygiene
o reduce risk of atelectasis and pneumoniao Position the patient
o to maximize chest exersion
o Institute pressure ulcer prevention strategies





























