Embed Size (px)
Citation preview
Pourquoi pas l’AIVOC ?Pourquoi pas l’AIVOC ?
S. Martinez DAR Timone 09/09/09
• Concept récent (20 ans)
• buts :
– Concentration constante (fenêtre cible)
• Plasma• Plasma
• « Site effet »
– Diminution des effets secondaires
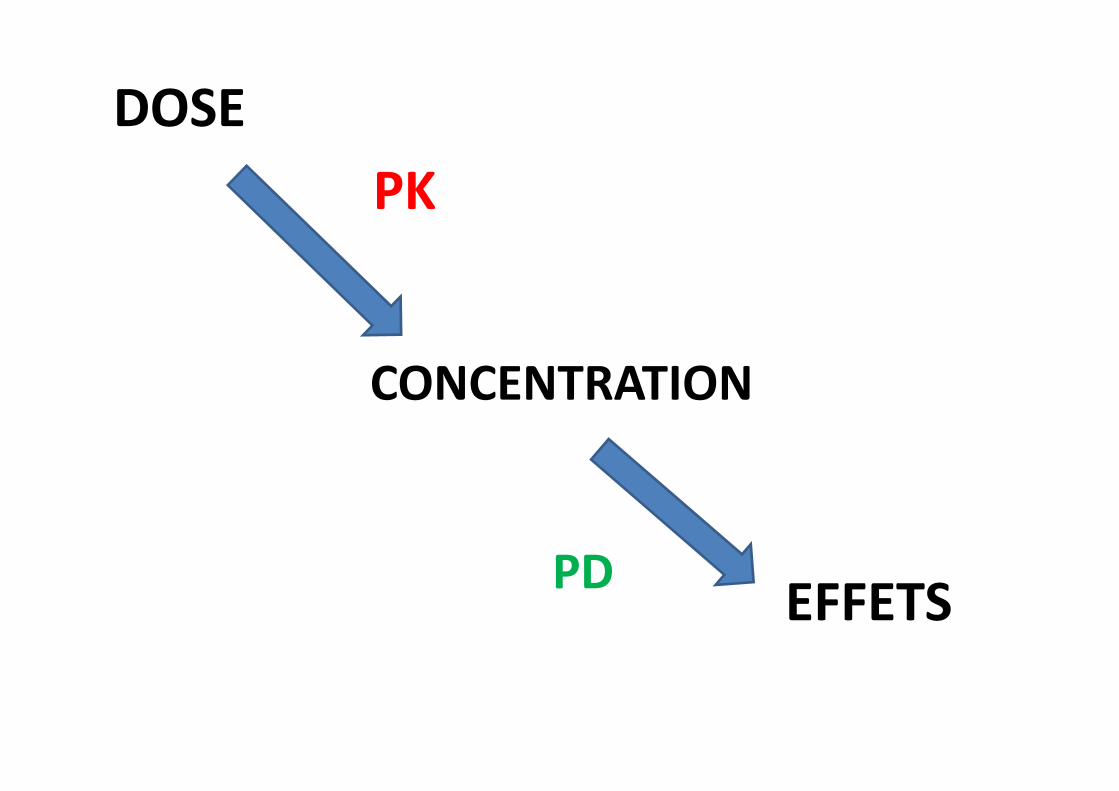
DOSE
CONCENTRATION
PK
CONCENTRATION
EFFETSPD
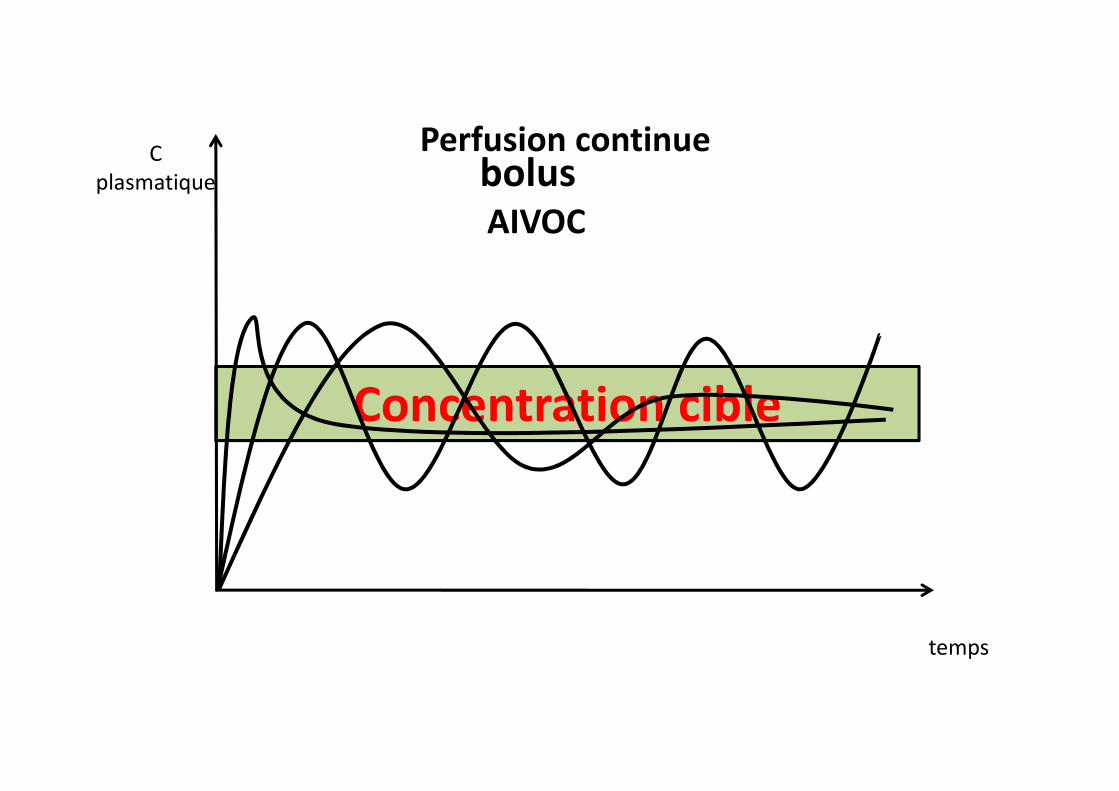
C plasmatique bolus
Perfusion continue
AIVOC
Concentration cible
temps
Concentration cible
Principe
• Modèle pharmaco-cinétique
• Compartiments
• Somme d’exponentielles décroissantes – Distribution – Distribution
– Élimination (notion de demi-vie contextuelle)
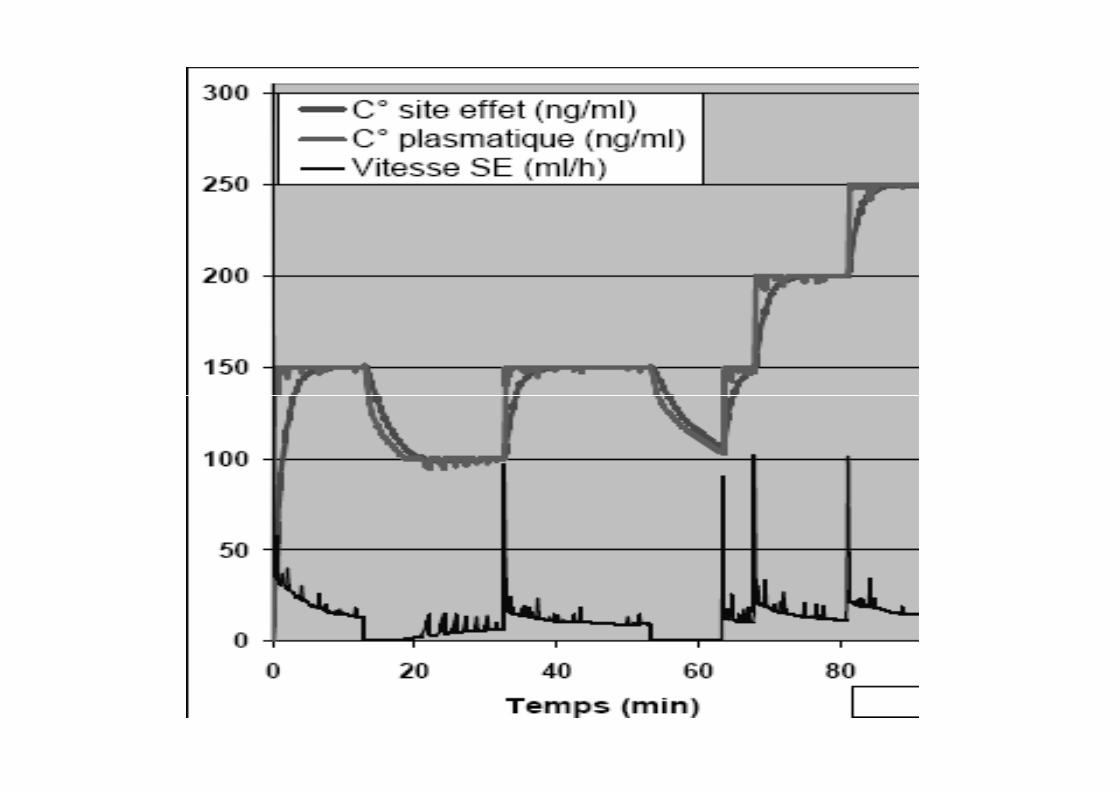
• Concentration plasmatique cible (t)
• Concentration au « site effet » (t)
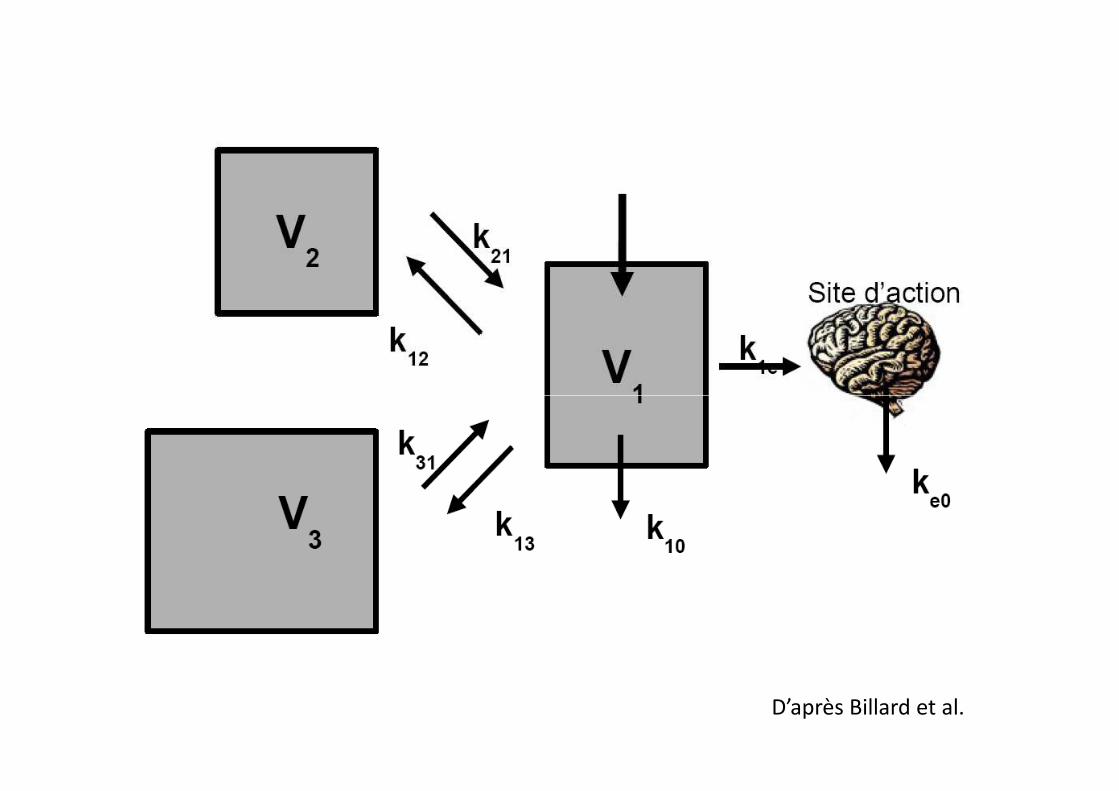
D’après Billard et al.
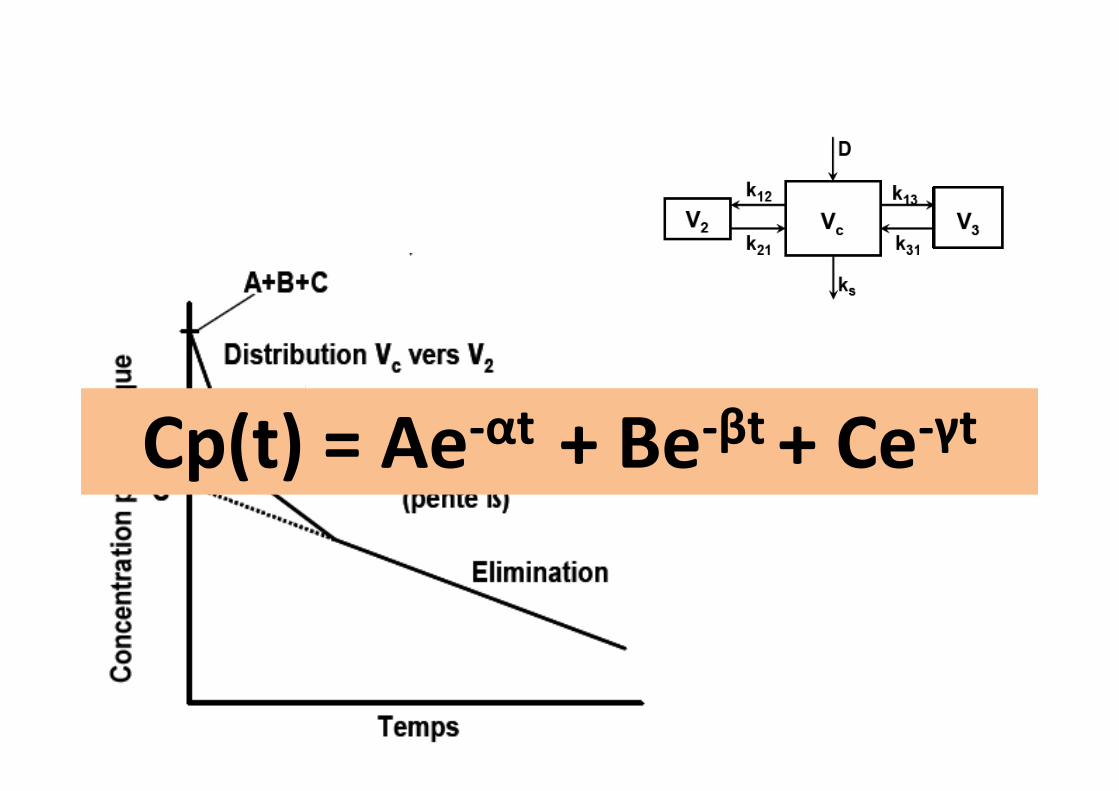
Cp(t) = Ae-αt + Be-βt + Ce-γtCp(t) = Ae-αt + Be-βt + Ce-γt
Modèles pharmacocinétiques
• Molécules utilisées– Morphiniques– Hypnotiques
• Mesures/ population • Cible plasmatique • Cible plasmatique • Cible au site effet (determination du ke0)
– Imprécisions– Connaissance des modèles – S’adapter
• Patient• Chirurgie
Limites des modèles
• Populations étudiées (extrapolation)
• AIVOC titrée (réponse HD, BIS…)
• Biais et erreurs :
Site effet ���� ke0
• Cible effet
• Études doses-effets
– BIS
– Réponses HD– Réponses HD
• Déterminant (bolus initial)
????
• Quelles molécules ?
• Quels modèles ?• Quels modèles ?
• Quels patients ?
• Quelles chirurgies ?
théoriquement
• Ensemble des molécules
• En pratique :
• Morphiniques
– Remifentanil– Remifentanil
– Sufentanil
• Hypnotiques
– Propofol
AIVOC et morphiniques
- Importance de la PK
- Fentanyl : peu maniable
- Sufentanil, Alfentanil
- Remifentanil : le plus souple d’utilisation - Remifentanil : le plus souple d’utilisation
AIVOC au sufentanil
• Modèles GEPS
• Poulation : sujet de 14 à 68 ans, poids de 47 à 94 kg
• Concentration cible (délai du pic à 6 min)• Concentration cible (délai du pic à 6 min)
• Reprise VS à 0,15 ng/ml
AIVOC au Remifentanil
• Modèle Minto
• Population : 20 à 85 ans, 85 à 110 kg
• Pic rapide (plasma ou cible)
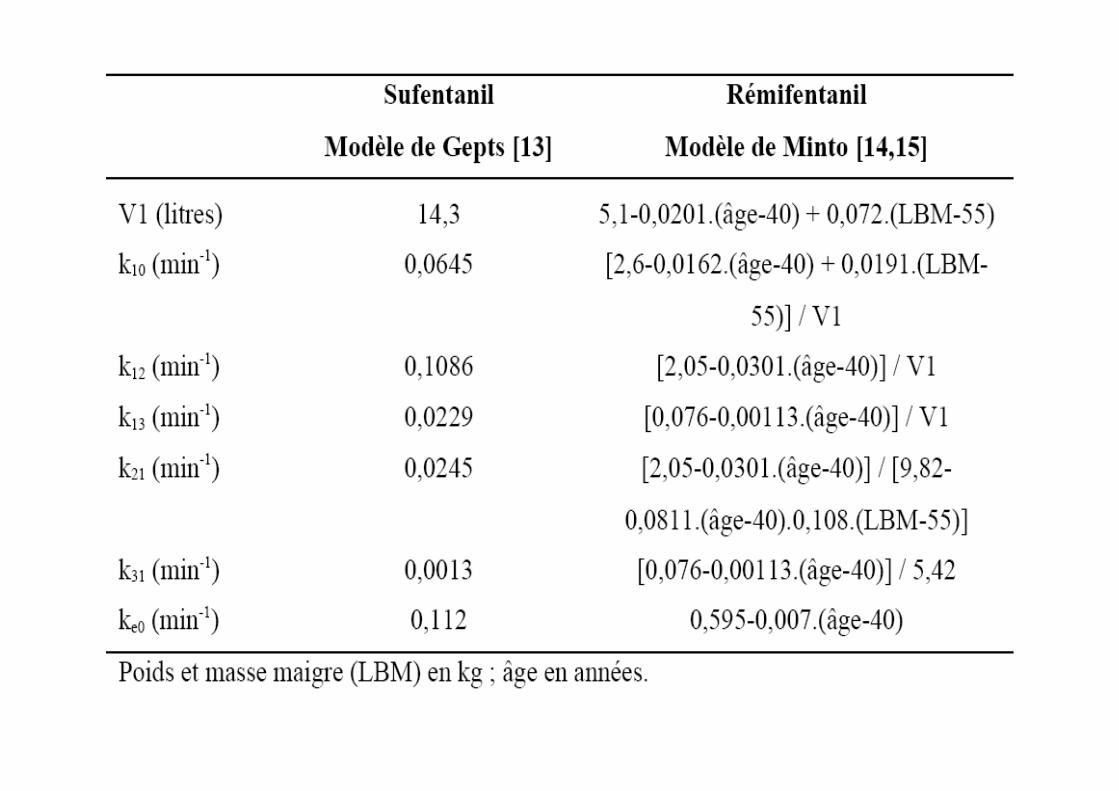
• Importance des covariables (Cf. tableau) • Importance des covariables (Cf. tableau)
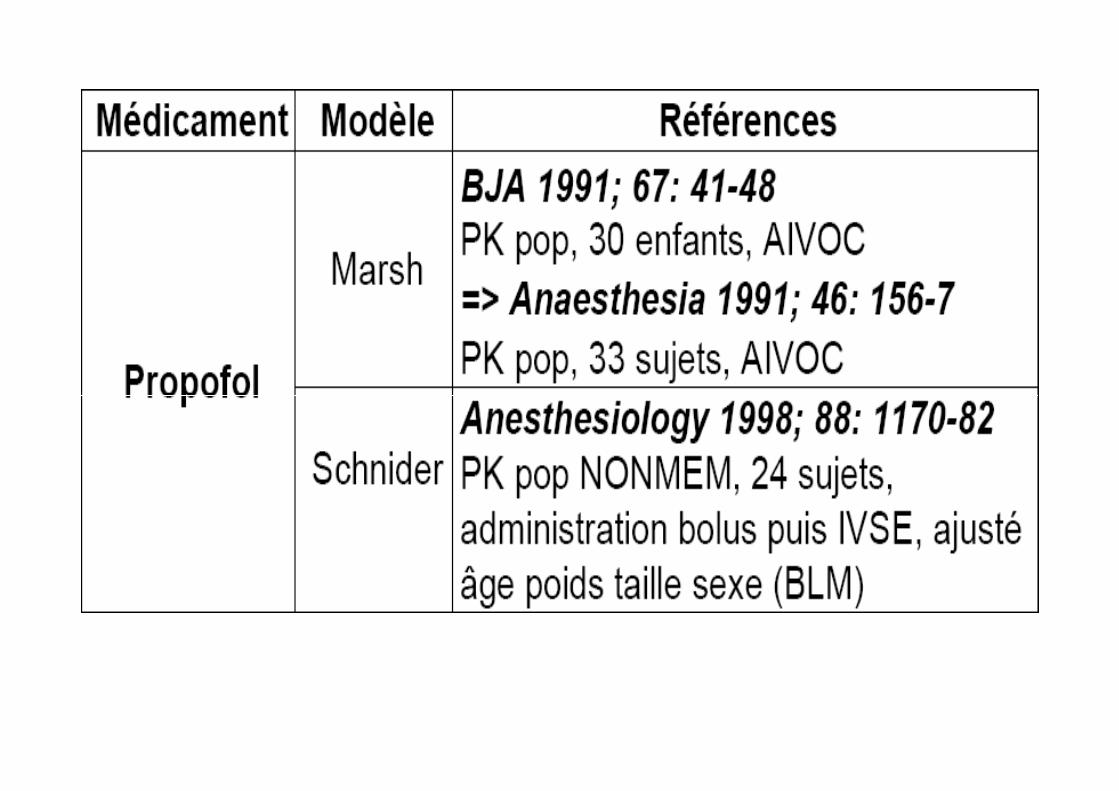
AIVOC au Propofol
• Seul hypnotique en pratique
• Réduction des effets HD
• 2 modèles PK :
– Marsh– Marsh
– Schnider
Marsh
• Premier modèle
• Deux versions :
– Diprifusor
– Primea– Primea
• Diffèrence du Ke0
• Seule covariable : poids
• Possible chez le sujet agé : cible adaptée.
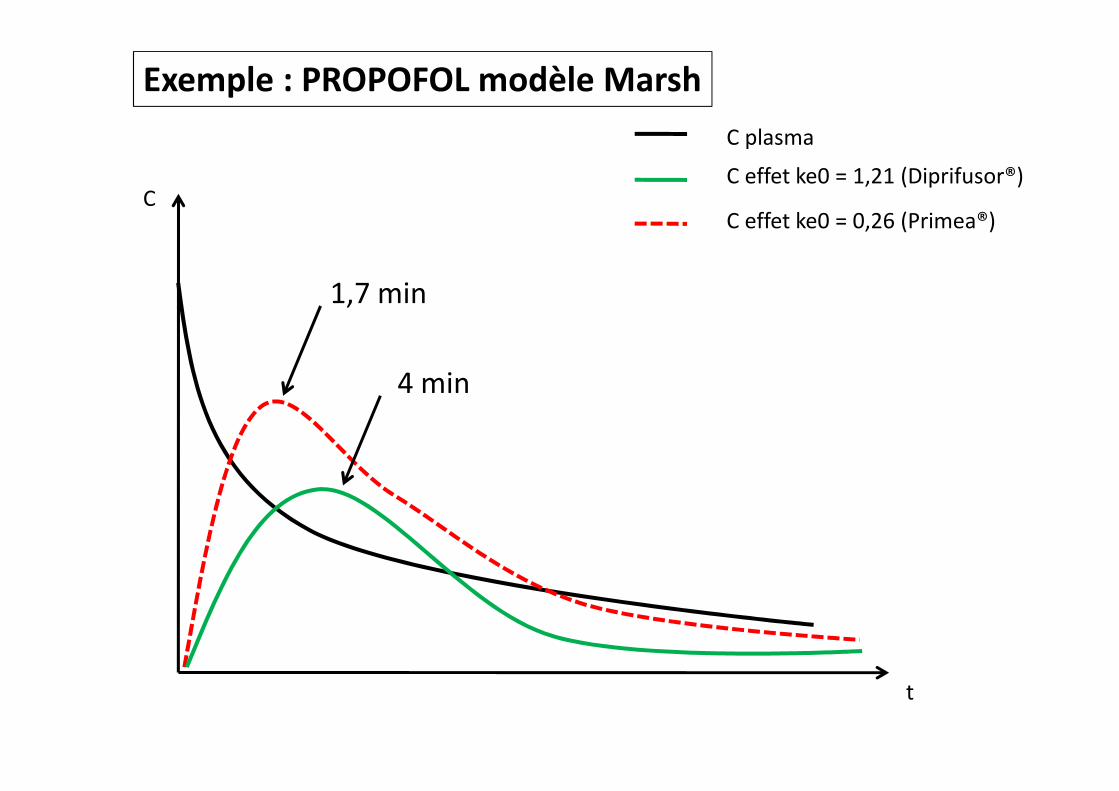
C plasma
C effet ke0 = 1,21 (Diprifusor®)
C effet ke0 = 0,26 (Primea®)
1,7 min
4 min
C
Exemple : PROPOFOL modèle Marsh
4 min
t
Schnider
• Plus récents
• Prise en compte des covariables :
– Àge
– Poids, taille – Poids, taille
– sexe
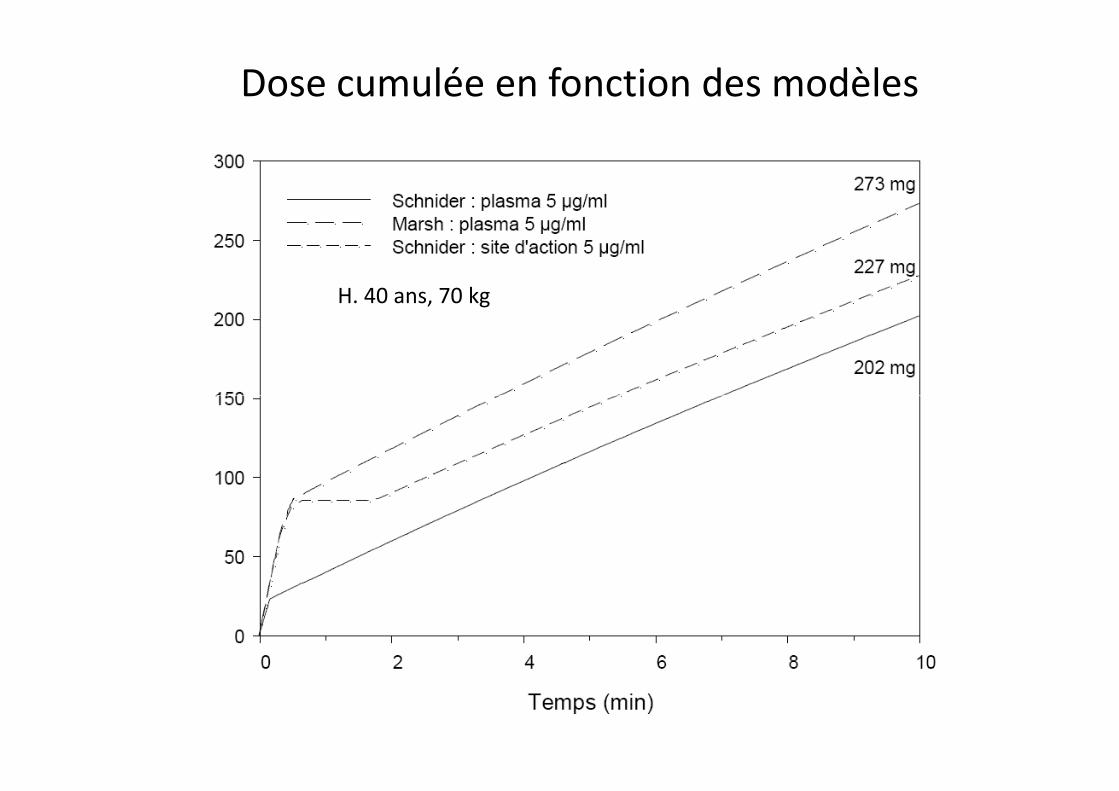
Dose cumulée en fonction des modèles
H. 40 ans, 70 kg
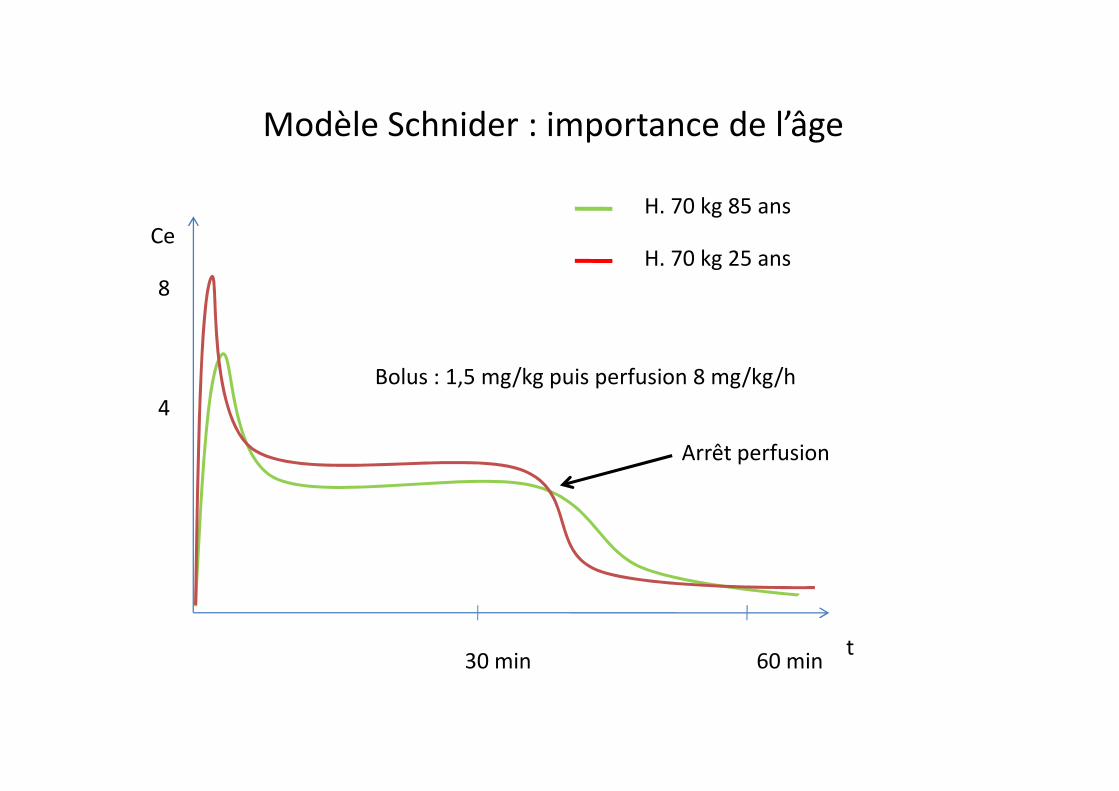
8
4
CeH. 70 kg 85 ans
H. 70 kg 25 ans
Modèle Schnider : importance de l’âge
Bolus : 1,5 mg/kg puis perfusion 8 mg/kg/h
4
t30 min 60 min
Arrêt perfusion
En pratique
• Utilisé pour :
– Terrains fragiles (moindres effets II HD)
– Tout type de chirugie :
• Anesthésie profonde • Anesthésie profonde
• Sédation
– Anesthésie précise :
• Induction
• Réveil
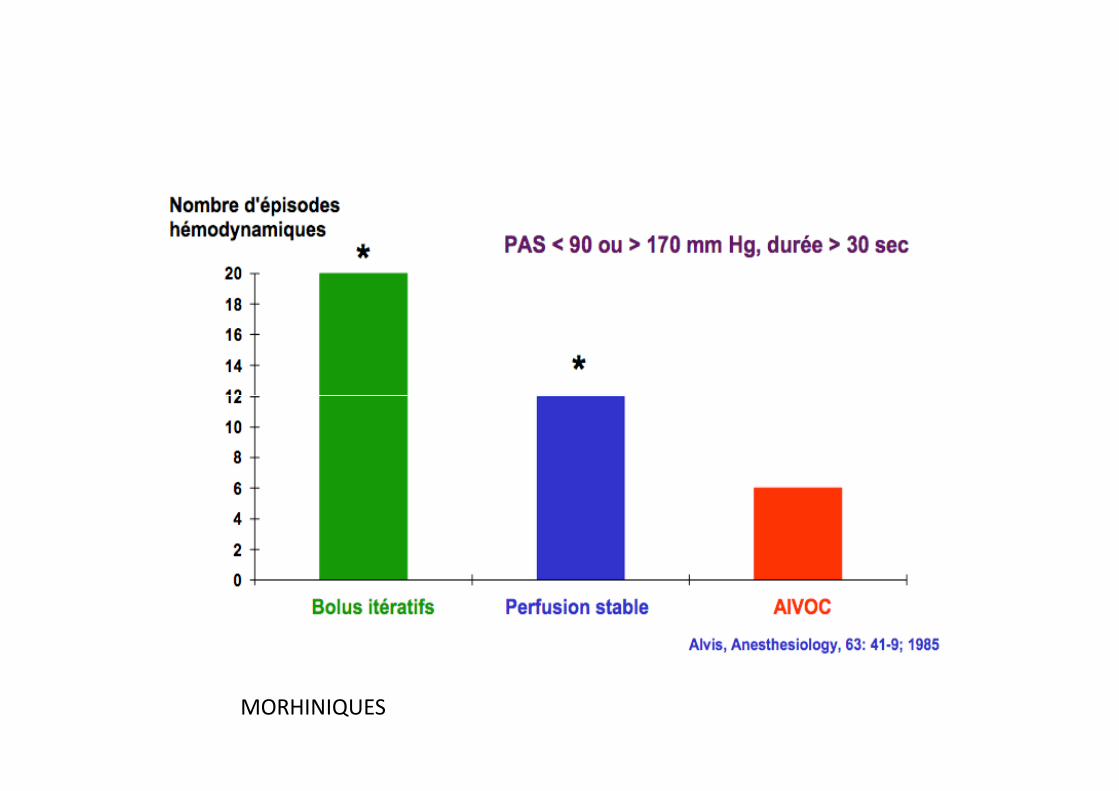
MORHINIQUES
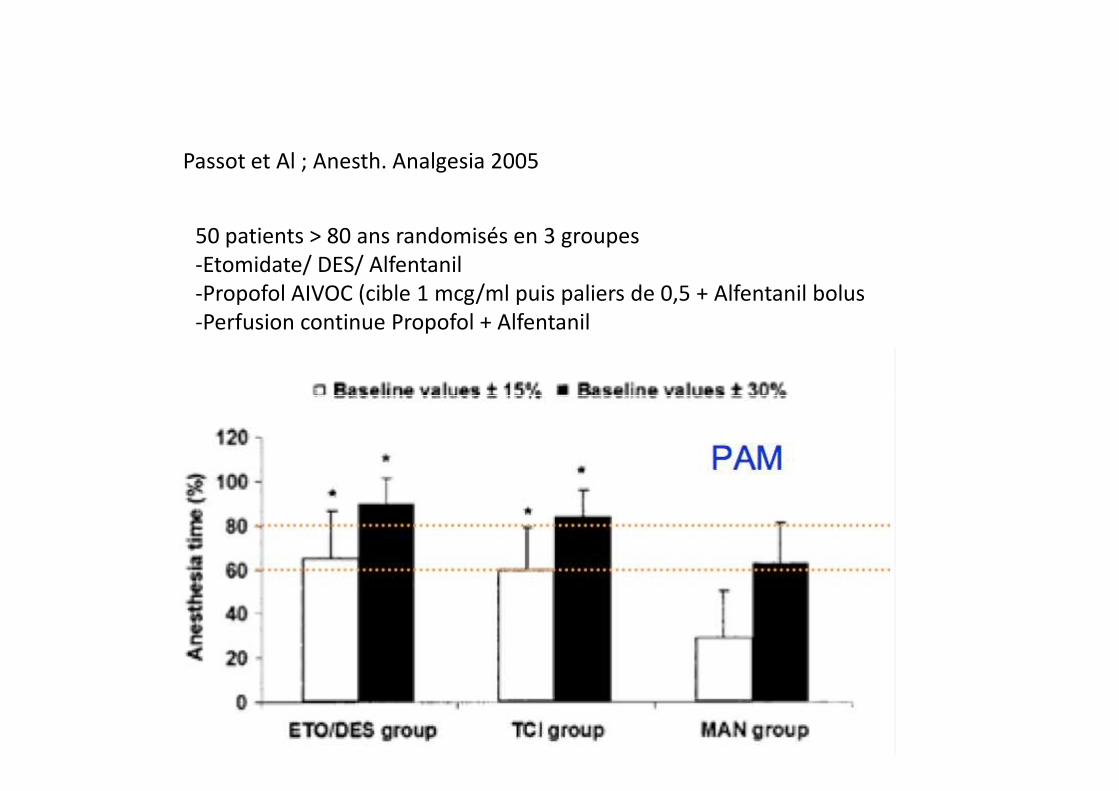
Passot et Al ; Anesth. Analgesia 2005
50 patients > 80 ans randomisés en 3 groupes-Etomidate/ DES/ Alfentanil-Propofol AIVOC (cible 1 mcg/ml puis paliers de 0,5 + Alfentanil bolus-Perfusion continue Propofol + Alfentanil
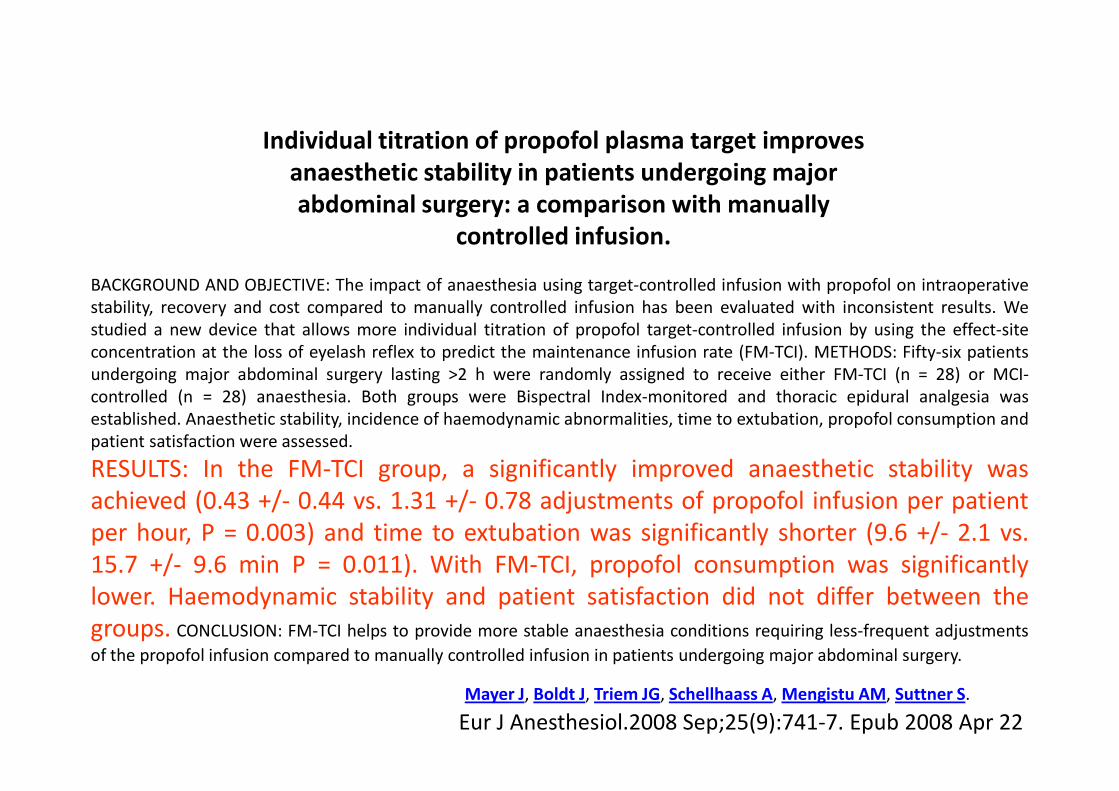
Individual titration of propofol plasma target improves anaesthetic stability in patients undergoing major abdominal surgery: a comparison with manually
controlled infusion.
BACKGROUND AND OBJECTIVE: The impact of anaesthesia using target-controlled infusion with propofol on intraoperativestability, recovery and cost compared to manually controlled infusion has been evaluated with inconsistent results. Westudied a new device that allows more individual titration of propofol target-controlled infusion by using the effect-siteconcentration at the loss of eyelash reflex to predict the maintenance infusion rate (FM-TCI). METHODS: Fifty-six patientsundergoing major abdominal surgery lasting >2 h were randomly assigned to receive either FM-TCI (n = 28) or MCI-controlled (n = 28) anaesthesia. Both groups were Bispectral Index-monitored and thoracic epidural analgesia was
Eur J Anesthesiol.2008 Sep;25(9):741-7. Epub 2008 Apr 22Mayer J, Boldt J, Triem JG, Schellhaass A, Mengistu AM, Suttner S.
controlled (n = 28) anaesthesia. Both groups were Bispectral Index-monitored and thoracic epidural analgesia wasestablished. Anaesthetic stability, incidence of haemodynamic abnormalities, time to extubation, propofol consumption andpatient satisfaction were assessed.
RESULTS: In the FM-TCI group, a significantly improved anaesthetic stability wasachieved (0.43 +/- 0.44 vs. 1.31 +/- 0.78 adjustments of propofol infusion per patientper hour, P = 0.003) and time to extubation was significantly shorter (9.6 +/- 2.1 vs.15.7 +/- 9.6 min P = 0.011). With FM-TCI, propofol consumption was significantlylower. Haemodynamic stability and patient satisfaction did not differ between thegroups. CONCLUSION: FM-TCI helps to provide more stable anaesthesia conditions requiring less-frequent adjustments
of the propofol infusion compared to manually controlled infusion in patients undergoing major abdominal surgery.
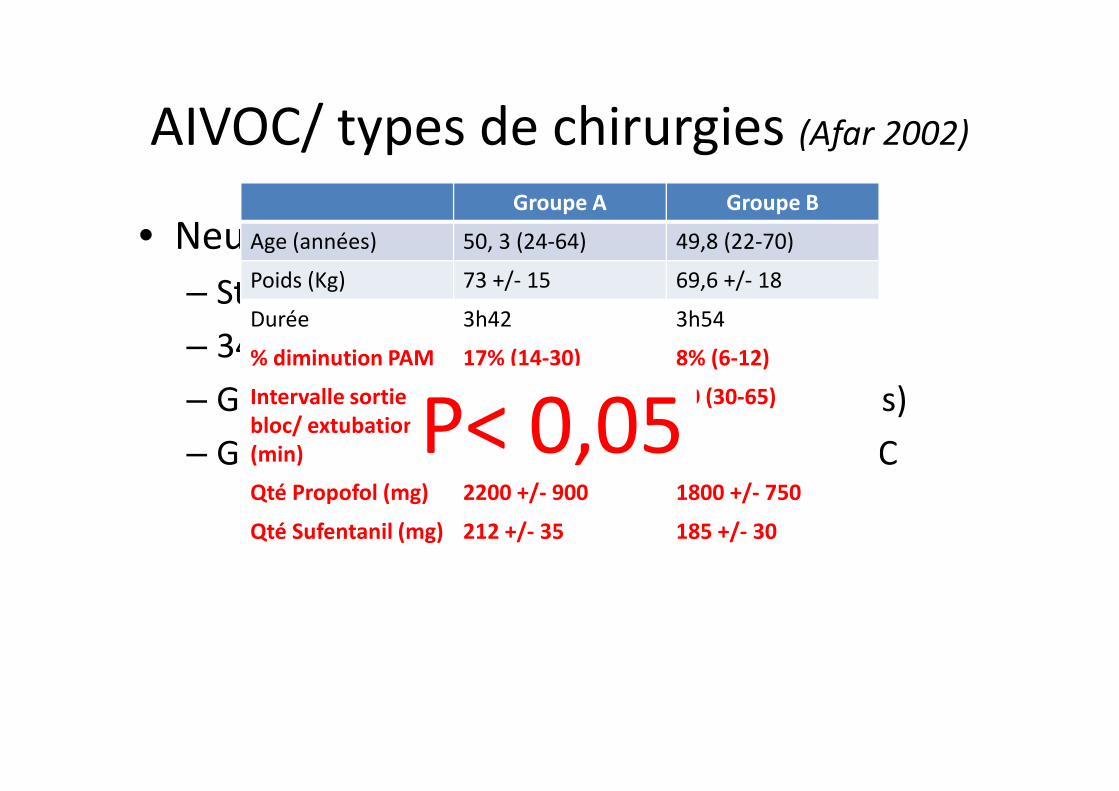
AIVOC/ types de chirurgies (Afar 2002)
• Neurochirurgie (Siao, Afar 2002) :
– Stabilité HD, réveil
– 34 adultes, ASA 2/3, craniectomie
– Groupe A (n=16) : propofol/ sufentanil (bolus)
Groupe A Groupe B
Age (années) 50, 3 (24-64) 49,8 (22-70)
Poids (Kg) 73 +/- 15 69,6 +/- 18
Durée 3h42 3h54
% diminution PAM 17% (14-30) 8% (6-12)
Intervalle sortie 73 (55-123) 40 (30-65)
P< 0,05– Groupe A (n=16) : propofol/ sufentanil (bolus)
– Groupe B (n=18) : propofol/ sufentanil AIVOC
Intervalle sortiebloc/ extubation(min)
73 (55-123) 40 (30-65)
Qté Propofol (mg) 2200 +/- 900 1800 +/- 750
Qté Sufentanil (mg) 212 +/- 35 185 +/- 30
P< 0,05
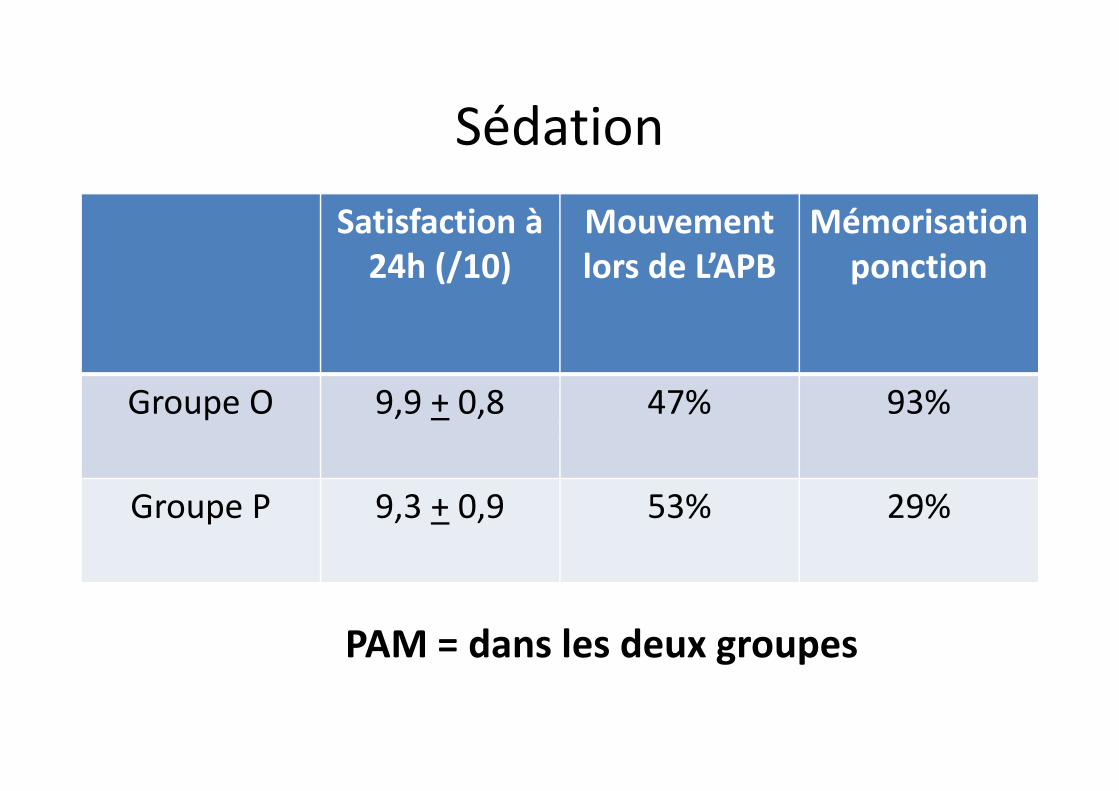
Sédation
• Sédation pour anésthésie péribulbaire (Chiron B.
Afar 2002) :
– 30 patients :
• Groupe sans sédation (O)
Satisfaction à 24h (/10)
Mouvement lors de L’APB
Mémorisationponction
Groupe O 9,9 + 0,8 47% 93%•• Groupe Propofol AIVOC (cible à 0,9 mcg/ml) (P)
Groupe O 9,9 + 0,8 47% 93%
Groupe P 9,3 + 0,9 53% 29%
PAM = dans les deux groupes
Anesthésie pour bronchoscopie
Anesthesiology 2001 (Bruyère M.)
30 patients
Groupe P (propofol manuel)
Groupe P (propofol AIVOC + Remifentanil IVSE)
Resultats :
HD, temps de réveil : idem dans les 2 groupes
Posologies : X 2 dans le groupe P manuel
Absence de mémorisation dans les 2 groupes
Conclusion (1)
• Modèles mathématiques complexes et imparfaits
• Utilisation simple
• Résultats probants• Résultats probants
– Qualité d’anesthésie
– Réduction des posologies
– Diminution des effets secondaires
Anesthésie intraveineuse à objectif de concentration (Aivoc)
avec le propofol.Évaluation des formations et pratiques au
bloc opératoirebloc opératoireC. Écoffey1*, X. Viviand2, V. Billard3, J.B.
Cazalaà4, S. Molliex5, F. Servin6, M.C. Laxenaire7
Ann Fr Anesth Réanim 2001 ; 20 : 228-45
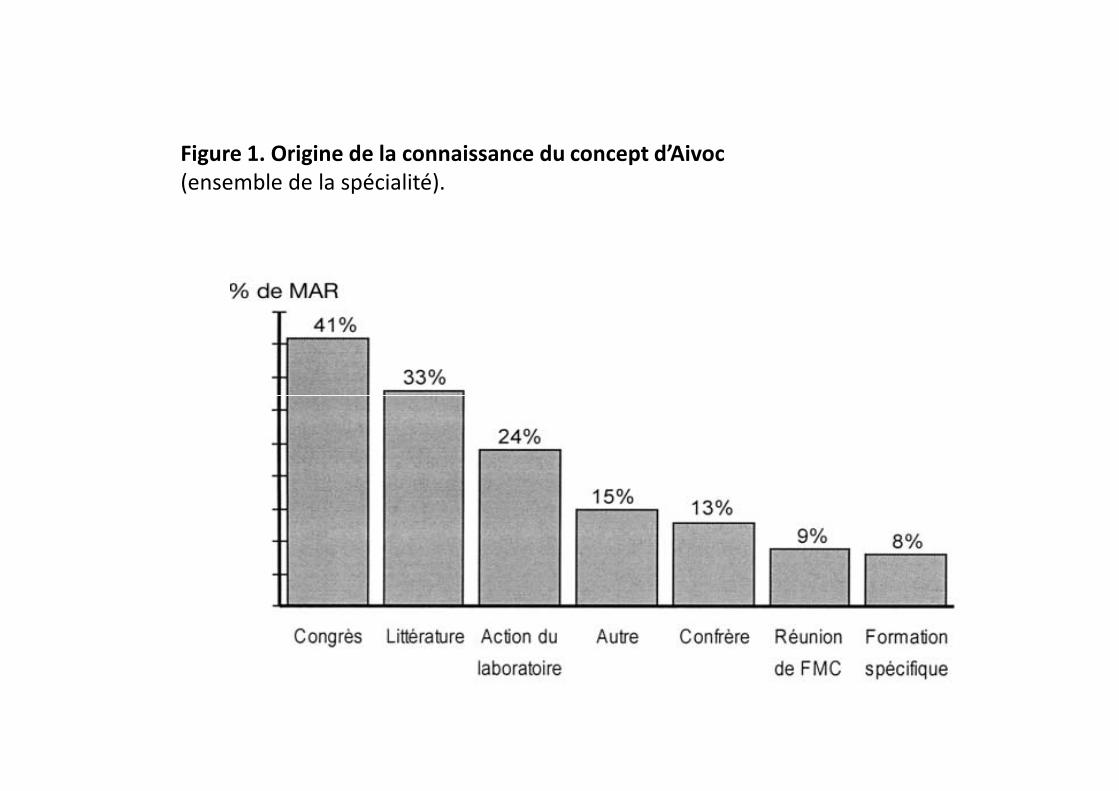
Figure 1. Origine de la connaissance du concept d’Aivoc(ensemble de la spécialité).
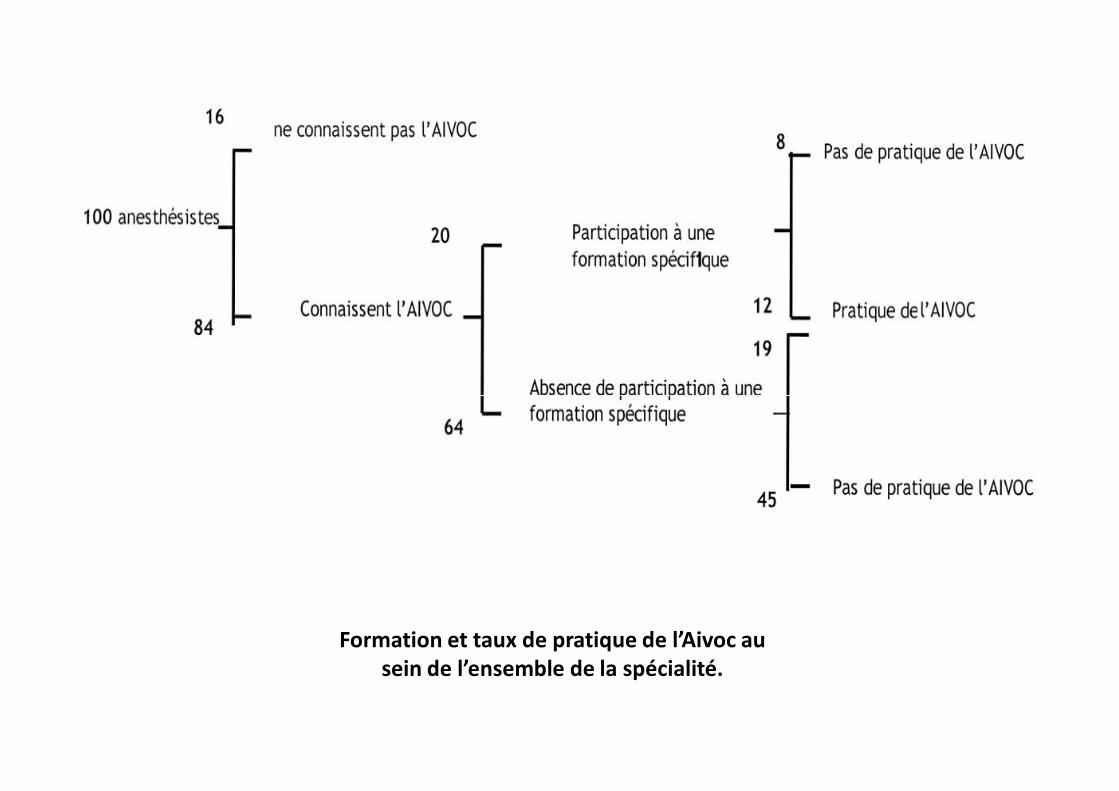
Formation et taux de pratique de l’Aivoc au sein de l’ensemble de la spécialité.
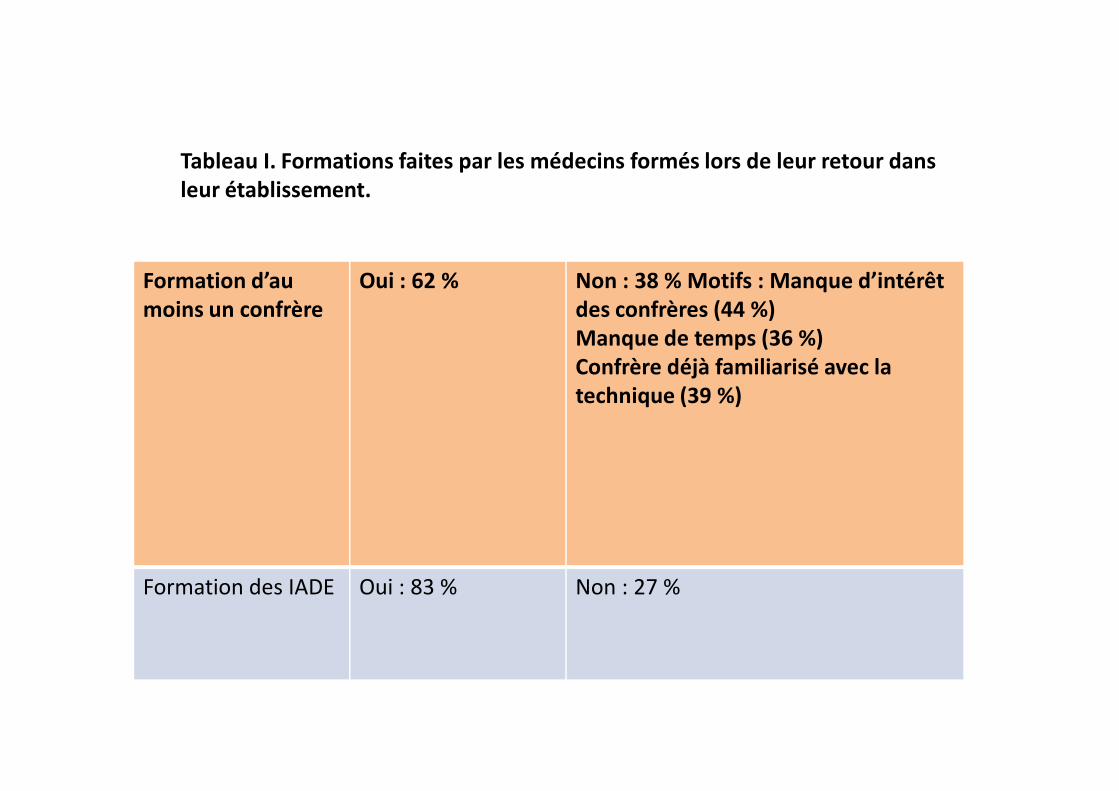
Tableau I. Formations faites par les médecins formés lors de leur retour dans leur établissement.
Formation d’au moins un confrère
Oui : 62 % Non : 38 % Motifs : Manque d’intérêt des confrères (44 %)Manque de temps (36 %)Confrère déjà familiarisé avec la technique (39 %)technique (39 %)
Formation des IADE Oui : 83 % Non : 27 %
Conclusion (2)
• De la théorie à la pratique
• Technique simple à utiliser mais …
• Probable nécessité de formation
• Nécessité de convaincre • Nécessité de convaincre – Les futur MAR
– Ses collègues…
• Outils complémentaires comparables pour les halogénés (anesthésie par inhalation à objectif de concentration).
















![Utilisation intraveineuse de la lidocaïne pour l'analgésie ... · 3 des douleurs viscérales à l’effet analgésique de la lidocaïne [8]. Une autre explication résiderait dans](https://img.pdfslide.fr/doc/110x75/5e4f8a7b739e07224027336a/utilisation-intraveineuse-de-la-lidocane-pour-lanalgsie-3-des-douleurs.jpg)











![[Product Monograph Template - Standard] · électrolytes. Une surveillance spéciale est requise au début de toute perfusion intraveineuse. En cas de signes anormaux, il faut cesser](https://img.pdfslide.fr/doc/110x75/5b9e5cfe09d3f204248b9b0c/product-monograph-template-standard-electrolytes-une-surveillance-speciale.jpg)