Embed Size (px)
Citation preview

Prise en charge des troubles Prise en charge des troubles sexuels masculinssexuels masculins
Béatrice Cuzin, GH E Herriot, Béatrice Cuzin, GH E Herriot, CLUB, LYONCLUB, LYON

épidémiologieépidémiologie
Lauman 1999:Lauman 1999: EnquEnquête chez 1410 ête chez 1410
hommes, prévalence hommes, prévalence 31% troubles sexuels: 31% troubles sexuels: 21% éjaculation 21% éjaculation rapide, 5% troubles rapide, 5% troubles érection, 5% troubles érection, 5% troubles du désirdu désir

étape diagnostiqueétape diagnostique
diagnostic positif des troubles sexuelsdiagnostic positif des troubles sexuels caractérisation de la dysfonction sexuellecaractérisation de la dysfonction sexuelle description de l’histoire sexuelle description de l’histoire sexuelle évaluation du retentissement de la dysfonction évaluation du retentissement de la dysfonction
sexuellesexuelle recherche des pathologies et facteurs pouvant recherche des pathologies et facteurs pouvant
favoriser ou aggraver une dysfonction sexuellefavoriser ou aggraver une dysfonction sexuelle examen cliniqueexamen clinique examens complémentaires à réaliser dans le examens complémentaires à réaliser dans le
bilan initial (Cour F 2005)bilan initial (Cour F 2005)

étape diagnostiqueétape diagnostique
diagnostic positif des troubles sexuelsdiagnostic positif des troubles sexuels caractérisation de la dysfonction sexuellecaractérisation de la dysfonction sexuelle description de l’histoire sexuelledescription de l’histoire sexuelle
Focus: Focus:
questionnaires: DE: IIEF 5, EHSquestionnaires: DE: IIEF 5, EHS

Echelle EHS : score de RigiditéEchelle EHS : score de Rigidité
Pénis élargi mais non
rigide
Pénis rigide mais pas assez
pour la pénétration
Pénis suffisamment rigide pour la pénétration mais pas complétement rigide
Pénis complétement dur et rigide
DE sevèreIIEF 6 - 10
DE Modérée IIEF 11 - 21
DE moyenneIIEF 22 - 25
Pas DEIIEF 26 - 30
MulhallJP, Goldstein I, Bushmakin AG, Cappelleri JC, and Hvidsten K. Validation of the Erection Hardness Score. J Sex Med 07
EHS : Erection Hardness Score

étape diagnostiqueétape diagnostique
évaluation du retentissement de la évaluation du retentissement de la dysfonction sexuelledysfonction sexuelle
Focus: Focus:
baisse estime de soi, bien baisse estime de soi, bien être émotionnel être émotionnel (althof 2002), augmentation score (althof 2002), augmentation score dépression (feldman 1994, Seidman 2002)dépression (feldman 1994, Seidman 2002)
partenaire (Chevret Méasson 2005)partenaire (Chevret Méasson 2005)

étape diagnostiqueétape diagnostique
recherche des pathologies et facteurs recherche des pathologies et facteurs pouvant favoriser ou aggraver une pouvant favoriser ou aggraver une dysfonction sexuelledysfonction sexuelle
Focus: facteurs de risque cardio-Focus: facteurs de risque cardio-vasculaires (prévalence des DE chez 30 à vasculaires (prévalence des DE chez 30 à 75 % chez les sujets à haut risque de 75 % chez les sujets à haut risque de maladie cardiovasculaire (Yusuf 2004, maladie cardiovasculaire (Yusuf 2004, Brownwyn GA 2007)Brownwyn GA 2007)

étape diagnostiqueétape diagnostique
examen cliniqueexamen cliniqueexamens complémentaires à réaliser examens complémentaires à réaliser
dans le bilan initialdans le bilan initialFocus:Focus:
Testostéronémie bio-disponibleTestostéronémie bio-disponible Pharmaco-echo-doppler VP: pas en Pharmaco-echo-doppler VP: pas en
première intention (Aversa 2007) première intention (Aversa 2007)

Etapes prise en chargeEtapes prise en charge
Évaluation de la demande du patient et coupleÉvaluation de la demande du patient et couple une information sexuelleune information sexuelle des conseils d’hygiène de viedes conseils d’hygiène de vie un changement éventuel des traitements en un changement éventuel des traitements en
cours cours Des traitements médicamenteux, Des traitements médicamenteux,
psychothérapies, approche sexo-corporelle, psychothérapies, approche sexo-corporelle, etc…..etc…..

Etapes prise en chargeEtapes prise en charge des conseils d’hygiène de viedes conseils d’hygiène de vie
Focus: Focus:
rrôle du régime, du poids sur la DE, duôle du régime, du poids sur la DE, du
rôle de l’exercice physique et de larôle de l’exercice physique et de la
perte de poids sur la récupérationperte de poids sur la récupération
(Esposito K 2006, 2009, Bacon CG 2006,(Esposito K 2006, 2009, Bacon CG 2006,
Hannan JL)Hannan JL)

Troubles de l’érectionTroubles de l’érection
L’approche pharmacologique: L’approche pharmacologique: les IPDE 5,les IPDE 5,traitement de première lignetraitement de première ligne
Adapter l’IPDE5 à l’utilisation:Adapter l’IPDE5 à l’utilisation:choix du patient (couple)choix du patient (couple)information sur la cinétique des information sur la cinétique des
molécules (action rapide/lente, à molécules (action rapide/lente, à la la demande/quotidien).demande/quotidien).
études spécifiquesétudes spécifiques

5%
7%
7%
22%
29%
47%Possibilit de prendre le traitement uniquement lorsque leژ
couple en a besoin
Fermet rection ژژ
Possibilit d صگژtre couvert plusieurs jours au risque de leگگprendre pour rien
Possibilit d ژژژصژˆ rieurگlai supگrection dans un dگ obtenir uneگ3 heures
Rapidit d صژ actionگ
NSP/ refus
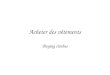
Les fondamentaux du traitementLes fondamentaux du traitement Quelles sont / seraient vos attentes Quelles sont / seraient vos attentes
par rapport au traitement ?par rapport au traitement ?
Attitude vis à vis de la sexualité et des troubles de l'érection. Étude Louis Harris 2005. Troubles de l’érection : le vécu des femmes. M. Chevret-Measson

3%
5%
8%
11%
23%
50%Sa dure ژ
Sa fermetژ
Sa rigiditژ
Son maintien vertical
Sa rapiditژdapparitionص
NSP/ refus
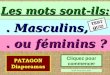
Qu'est ce qu'une bonne érection ?Qu'est ce qu'une bonne érection ?
Concernant l’érection proprement dite, quels sont les Concernant l’érection proprement dite, quels sont les critères qui définissent une érection de bonne qualité ?critères qui définissent une érection de bonne qualité ?
Attitude vis à vis de la sexualité et des troubles de l'érection. Étude Louis Harris 2005. Troubles de l’érection : le vécu des femmes. M. Chevret-Measson

Synthèse des résultatsSynthèse des résultats
Les femmes affirment être globalement satisfaites de leur sexualité même si une sur trois aimerait une fréquence des rapports plus élevée
Face aux pannes sexuelles, l'attitude des femmes indique des attentions dirigées vers les hommes, c'est en premier lieu son attitude, son énervement, son sentiment de culpabilité qui gênent les femmes loin devant leur propre absence de plaisir
Attitude vis à vis de la sexualité et des troubles de l'érection. Étude Louis Harris 2005. Troubles de l’érection : le vécu des femmes. M. Chevret-Measson

Mac Mahon 2004
troubles de l’éjaculation

Recommandations de l’AUA sur le traitement Recommandations de l’AUA sur le traitement pharmacologique de l’EPpharmacologique de l’EP
Définition: éjaculation qui se produit plus tDéfinition: éjaculation qui se produit plus tôt que désiré, ôt que désiré, avant ou peu après la pénétration causant une détresse avant ou peu après la pénétration causant une détresse à l’un ou les deux partenairesà l’un ou les deux partenaires
Critère diagnosticCritère diagnosticInterrogatoireInterrogatoire
Importance de voir la partenaireImportance de voir la partenaire
IELTIELT
Différentier des autres DSDifférentier des autres DS

Interrogatoire médical et psychosocialInterrogatoire médical et psychosocial
Evaluer la plainteEvaluer la plainte Degré de détresse patient/partenaireDegré de détresse patient/partenaire Perception du contrPerception du contrôle de l’éjauclationôle de l’éjauclation IELTIELT Début et durée de la PEDébut et durée de la PE Antécédents psychosociauxAntécédents psychosociaux Antécédents médicauxAntécédents médicaux

Buvat J, Tesfaye F, Rothman M, Rivas DA, Giuliano F.Buvat J, Tesfaye F, Rothman M, Rivas DA, Giuliano F.Dapoxetine for the treatment of premature ejaculation: results from a randomized,Dapoxetine for the treatment of premature ejaculation: results from a randomized,double-blind, placebo-controlled phase 3 trial in 22 countries. Eur Urol. 2009 Apr;55(4):957-67. double-blind, placebo-controlled phase 3 trial in 22 countries. Eur Urol. 2009 Apr;55(4):957-67.
BACKGROUND: Dapoxetine is being developed for the on-demand treatment of premature ejaculation (PE). BACKGROUND: Dapoxetine is being developed for the on-demand treatment of premature ejaculation (PE). Previous clinical trials have demonstrated its safety and efficacy. OBJECTIVE: To evaluate the long-term Previous clinical trials have demonstrated its safety and efficacy. OBJECTIVE: To evaluate the long-term efficacy and safety of dapoxetine in men with PE. DESIGN, SETTING, AND PARTICIPANTS: This efficacy and safety of dapoxetine in men with PE. DESIGN, SETTING, AND PARTICIPANTS: This randomized, double-blind, parallel-group, placebo-controlled, phase 3 trial, conducted in 22 countries, randomized, double-blind, parallel-group, placebo-controlled, phase 3 trial, conducted in 22 countries, enrolled men (N=1162) > or = 18 yr of age who met the Diagnostic andenrolled men (N=1162) > or = 18 yr of age who met the Diagnostic andStatistical Manual of Mental Disorders, fourth edition, text revision criteria for PE for > or = 6 mo, with an Statistical Manual of Mental Disorders, fourth edition, text revision criteria for PE for > or = 6 mo, with an intravaginal ejaculatory latency time (IELT) < or = 2 min in > or = 75% of intercourse episodes at baseline. intravaginal ejaculatory latency time (IELT) < or = 2 min in > or = 75% of intercourse episodes at baseline. INTERVENTION: Dapoxetine 30 mg or dapoxetine 60 mg or placebo on demand (1-3 h before intercourse) INTERVENTION: Dapoxetine 30 mg or dapoxetine 60 mg or placebo on demand (1-3 h before intercourse) for 24 wk. MEASUREMENTS: Stopwatch-measured IELT, Premature Ejaculation Profile (PEP), Clinical for 24 wk. MEASUREMENTS: Stopwatch-measured IELT, Premature Ejaculation Profile (PEP), Clinical Global Impression (CGI) of change, adverse events (AEs). RESULTS AND LIMITATIONS: The study was Global Impression (CGI) of change, adverse events (AEs). RESULTS AND LIMITATIONS: The study was completed by 618 men. Mean average IELT increased from 0.9 min at baseline (all groups) to 1.9 min, 3.2 completed by 618 men. Mean average IELT increased from 0.9 min at baseline (all groups) to 1.9 min, 3.2 min, and 3.5 min with placebo and dapoxetine 30 mg and dapoxetine 60 mg, respectively, at study end point; min, and 3.5 min with placebo and dapoxetine 30 mg and dapoxetine 60 mg, respectively, at study end point; geometric mean IELT increased from 0.7 min at baseline to 1.1min, 1.8 min, and 2.3 min, respectively, at geometric mean IELT increased from 0.7 min at baseline to 1.1min, 1.8 min, and 2.3 min, respectively, at study end point. All PEP measures and IELTs improved significantly with dapoxetine versus placebo at week study end point. All PEP measures and IELTs improved significantly with dapoxetine versus placebo at week 12 and week 24 (p<0.001 for all). The most common AEs were nausea, dizziness, diarrhea, and headache. 12 and week 24 (p<0.001 for all). The most common AEs were nausea, dizziness, diarrhea, and headache. AEs led to discontinuation in 1.3%, 3.9%, and 8.2% of subjects with placebo and dapoxetine 30 mg and AEs led to discontinuation in 1.3%, 3.9%, and 8.2% of subjects with placebo and dapoxetine 30 mg and dapoxetine 60 mg, respectively. Limitations of this study included the exclusion of men who were not in long-dapoxetine 60 mg, respectively. Limitations of this study included the exclusion of men who were not in long-term monogamous relationships. CONCLUSIONS: Dapoxetine significantly improved all aspects of PE and term monogamous relationships. CONCLUSIONS: Dapoxetine significantly improved all aspects of PE and was generally well tolerated in this broad population.was generally well tolerated in this broad population.

Priligy™ (Dapoxetine) Receives First Regulatory Approvals For The Priligy™ (Dapoxetine) Receives First Regulatory Approvals For The Treatment Of Premature Ejaculation (PE) In Finland And SwedenTreatment Of Premature Ejaculation (PE) In Finland And Sweden
17 Feb 2009 17 Feb 2009 Janssen-Cilag EMEA, a division of Janssen Pharmaceutica N. V., announced that Janssen-Cilag EMEA, a division of Janssen Pharmaceutica N. V., announced that Priligy™(dapoxetine) has received marketing authorisation in Finland and Sweden for Priligy™(dapoxetine) has received marketing authorisation in Finland and Sweden for the on-demand treatment of premature ejaculation (PE) in men 18 - 64 years of age. the on-demand treatment of premature ejaculation (PE) in men 18 - 64 years of age. These approvals follow the positive outcome of a decentralised marketing authorisation These approvals follow the positive outcome of a decentralised marketing authorisation procedure in seven European Union countries: Sweden, Austria, Finland, Germany, procedure in seven European Union countries: Sweden, Austria, Finland, Germany, Spain, Italy and Portugal. The procedure was finalised in December 2008, and Finland Spain, Italy and Portugal. The procedure was finalised in December 2008, and Finland and Sweden are the first countries worldwide to grant marketing authorisation for this and Sweden are the first countries worldwide to grant marketing authorisation for this compound. National approvals and licenses in the other five European countries are compound. National approvals and licenses in the other five European countries are expected to follow. Dapoxetine is not approved for marketing in the United States. expected to follow. Dapoxetine is not approved for marketing in the United States.
Dapoxetine is a drug specifically developed for the on-demand treatment of PE and is Dapoxetine is a drug specifically developed for the on-demand treatment of PE and is the first oral medication (tablet) to be approved for this condition. Dapoxetine has been the first oral medication (tablet) to be approved for this condition. Dapoxetine has been extensively evaluated in five randomised, placebo-controlled Phase III clinical trials extensively evaluated in five randomised, placebo-controlled Phase III clinical trials involving more than 6,000 men with PE and their partners. This is the largest and most involving more than 6,000 men with PE and their partners. This is the largest and most comprehensive clinical trial programme to date for a drug therapy to treat PE. comprehensive clinical trial programme to date for a drug therapy to treat PE. Dapoxetine is a unique, short-acting, selective serotonin reuptake inhibitor (SSRI) Dapoxetine is a unique, short-acting, selective serotonin reuptake inhibitor (SSRI) designed to be taken only when needed, that is 1-3 hours before sexual intercourse is designed to be taken only when needed, that is 1-3 hours before sexual intercourse is anticipated, rather than every day. Dapoxetine will be marketed by Janssen-Cilag, anticipated, rather than every day. Dapoxetine will be marketed by Janssen-Cilag, marking another significant advance in the company's commitment to developing marking another significant advance in the company's commitment to developing innovative, high quality treatments for unmet medical needs. innovative, high quality treatments for unmet medical needs.

TramadolTramadol
Salem EA, Wilson SK, Bissada NK, Delk JR II, Hellstrom WJ, and Cleves MA.Salem EA, Wilson SK, Bissada NK, Delk JR II, Hellstrom WJ, and Cleves MA.Tramadol HCL has promise in on-demand use to treat premature ejaculation. Tramadol HCL has promise in on-demand use to treat premature ejaculation. J SexMed 2008;5:188–193.J SexMed 2008;5:188–193.
Single-blind, placebo-controlled, crossover, stopwatch monitored two-period study was Single-blind, placebo-controlled, crossover, stopwatch monitored two-period study was conducted, on 60 patients with lifelong PE. PE was defined as IELT of < 2 minutes in 80% conducted, on 60 patients with lifelong PE. PE was defined as IELT of < 2 minutes in 80% of intercourse episodes. A total of 25 mg of Tramadol hydrochloride was given to one of intercourse episodes. A total of 25 mg of Tramadol hydrochloride was given to one group (30) prior to intercourse and placebo was supplied for the other group (30) for 8 group (30) prior to intercourse and placebo was supplied for the other group (30) for 8 weeks. Drugs were taken 1–2 hours before sexual activity and sexual intercourse was weeks. Drugs were taken 1–2 hours before sexual activity and sexual intercourse was required at least once per week. After the initial treatment period, the two groups took the required at least once per week. After the initial treatment period, the two groups took the alternate medication for another 2 months. The two 8-week treatment periods were alternate medication for another 2 months. The two 8-week treatment periods were separated by 1 week washout period. IELT was timed by a stopwatch at each intercourse separated by 1 week washout period. IELT was timed by a stopwatch at each intercourse and was reported by patients or partners. and was reported by patients or partners. Results. Results. The baseline (mean± SD) IELT for The baseline (mean± SD) IELT for patients before treatment was 1.17± 0.39 minutes. At the end of the treatment period patients before treatment was 1.17± 0.39 minutes. At the end of the treatment period utilizing the active drug, the mean IELT was increased significantly in patients on utilizing the active drug, the mean IELT was increased significantly in patients on Tramadol treatment to 7.37 ± 2.53 minutes. The same patients on placebo medication Tramadol treatment to 7.37 ± 2.53 minutes. The same patients on placebo medication had mean IELT of only 2.01±0.71 minutes. Patients uniformly reported satisfaction with had mean IELT of only 2.01±0.71 minutes. Patients uniformly reported satisfaction with their resulting control over ejaculation.their resulting control over ejaculation.Conclusions.Conclusions.Tramadol, a drug with a proven safety record as an anti-inflammatory Tramadol, a drug with a proven safety record as an anti-inflammatory agent, shows promise as a drug for treating rapid ejaculation.agent, shows promise as a drug for treating rapid ejaculation.

Aversa A, Pili M, Francomano D, Bruzziches R, Spera E, La Pera G, Spera G. Effects of vardenafil administration on intravaginal ejaculatory latency time in men with lifelong premature ejaculation. Int J Impot Res. 2009 Jul-Aug;21(4):221-7. Premature ejaculation (PE) is thought to be the most common male sexual dysfunction; however, the prevalence of lifelong (LL)-PE is relatively low. The aim of this study was to investigate the effects of on-demand vardenafil (10 mg) to modify the intravaginal ejaculatory latency time (IELT) in men with LL-PE without erectile dysfunction. Forty-two men (18-35 years) were enrolled in a 16-week, double-blind, placebo-controlled, cross-over study. Primary end point was the modification from baseline of IELT assessed by stopwatch technique; secondary end points were post-ejaculatory refractory time (PERT) and variations of scores at the Index of Premature Ejaculation questionnaire. The changes in geometric mean IELT were superior after taking vardenafil (0.6+/-0.3 vs 4.5+/-1.1 min, P<0.01), compared with placebo (0.7+/-0.3 vs 0.9+/-1.0 min, ns). PERT dropped significantly after vardenafil (16.7+/-2.0 vs 4.3+/-0.9 min, P<0.001), compared with placebo (15.3+/-2.2 vs 15.8+/-2.3 min). Patients who took vardenafil (vs placebo) reported significantly (P<0.01) increased ejaculatory control (6+/-2 vs 16+/-2), improved overall sexual satisfaction (7+/-2 vs 15+/-1) and distress (4+/-1 vs 8+/-1) scores, respectively. Multiple regression analysis (r(2)=0.86) for IELT by the number of attempts at sexual intercourse showed significant differences between the slopes of lines for placebo and vardenafil (P<0.0001). T he most common adverse events for vardenafil (vs placebo) were headache (10 vs 3%), flushing (12 vs 0%) and dyspepsia (10 vs 0%), which tended to disappear over the time. In conclusion, in our study, vardenafil increased IELT and reduced PERT in men with LL-PE. Besides, improvements in confidence, perception of ejaculatory control and overall sexual satisfaction were reported.
Vardenafil

Dinsmore WW, Wyllie MG. PSD502 improves ejaculatory latency, control and sexual satisfaction when applied topically 5 min before intercourse in men with premature ejaculation: results of a phase III, multicentre, double-blind, placebo-controlled study. BJU Int. 2009 Apr;103(7):940-9.
RESULTS: In all, 300 men with PE were randomized from 31 centres in Europe. The geometric mean (range) IELT over the 3-month treatment period increased from a baseline of 0.6 min in both groups to 3 .8 (0.3-57.8) and 1.1 (0 -15.0) min in the PSD502 and placebo groups, respectively. Adjusting for treatment-group imbalances, this represents a 6.3-fold and 1.7-fold increase in adjusted geometric means. There were significantly greater increases in the scores for the IPE domains of ejaculatory control and sexual satisfaction in the PSD502 group than in the placebo group, with a mean (sem) 7.0 (0.59)-point difference between treatments in change from baseline in the IPE domain for ejaculatory control and a 5.9 (0.57)- point difference in change from baseline in the IPE domain for sexual satisfaction (both P < 0.001). This was supported by improvements in all secondary endpoints. At the end of the treatment period 66% o f patients rated PSD502 as 'good' or 'excellent'. PSD502 was well tolerated and no systemic adverse events were reported. Localized treatment-related adverse events were reported by 2.6% and 3.1% of patients and partners, respectively. CONCLUSION: PSD502 applied topically 5 min before intercourse improved ejaculatory latency and significantly improved ejaculatory control and sexual satisfaction, factors relevant for acceptance of a PE treatment by both patient/physician and regulatory authorities. PSD502 was well tolerated by both patients and partners, with no systemic side-effects and a low incidence of localized effects, and was rated favourably by most users. PSD502 therefore appears to offer significant advantages over other therapies in development for the treatment of PE.
PSD 502/Tempe (Pletora)

PSD502 For Premature Ejaculation - Positive Outcomes From European Phase III Pivotal Trial
07 Nov 2008 Plethora Solutions Holdings PLC ("Plethora" or the "Company", AIM: PLE), the specialist developer of products for the treatment and management of urological disorders, announces that its European Phase III double-blind placebo controlled study of PSD502 for the treatment of premature ejaculation (PE) has met its three co-primary endpoints of Intra-vaginal Ejaculation Latency Time ('IELT') and Index of Premature Ejaculation ('IPE'; Ejaculatory Control and Sexual Satisfaction domains). The successful European study is one of two pivotal Phase III studies running in parallel with identical protocols. The second Phase III study is being conducted in North America and is expected to complete in the first half of 2009. Once the results from the US Phase III study become available, data from the two studies will be combined for submission for regulatory approval in the USA and Europe. European and US Phase III Study Details Each Phase III study is a multi-centre, randomised, double blind, placebo-controlled efficacy study and the programme is expected to recruit a total of 540 patients across the two studies. Patients are treated for a 12 week period with an optional open label phase of up to 9 months. The European study was conducted with 300 randomised patients across 32 investigational centres in 4 countries across Europe. Of these, 265 patients also entered the optional 9 month open label study.

Anorgasmies, anéjaculationAnorgasmies, anéjaculation Psychogéne: généralisé/situationnelle.Psychogéne: généralisé/situationnelle. Anatomique congénitale, acquise: TURP, incision colAnatomique congénitale, acquise: TURP, incision col Neurologique: diabète, PR, sympathectomie, curage, Neurologique: diabète, PR, sympathectomie, curage,
anévrysmesanévrysmes InfectieuseInfectieuse Endocrinienne: hypogonadisme, hypothyroidieEndocrinienne: hypogonadisme, hypothyroidie Médicamenteuse: antidépresseurs, Médicamenteuse: antidépresseurs,
antidépresseurs,alcool, alpha-bloquants antidépresseurs,alcool, alpha-bloquants Pas de traitement médicamenteux sauf TSH, Pas de traitement médicamenteux sauf TSH,
approche psychothérapique.approche psychothérapique.

Troubles du désirTroubles du désir
Généralisé/situationnelGénéralisé/situationnel Primaire/acquisPrimaire/acquis Troubles de l’identité sexuelle, difficultés Troubles de l’identité sexuelle, difficultés
lors de l’acquisition de la sexualité.lors de l’acquisition de la sexualité. Médicaments: IMAO, antidépresseurs TC, Médicaments: IMAO, antidépresseurs TC,
IRS, antipsychotiques, antiandrogènes.IRS, antipsychotiques, antiandrogènes. hypogonadismehypogonadisme

Troubles du désir: traitementTroubles du désir: traitement AndrogénothérapieAndrogénothérapie Changement médicamentsChangement médicaments PsychothérapiePsychothérapie
Focus: nombreuses études sur le rFocus: nombreuses études sur le rôle protecteur ôle protecteur de la testostérone, données rassurantes sur le de la testostérone, données rassurantes sur le cancer de prostate. Association possible avec cancer de prostate. Association possible avec les 5PDE5 (Isidori 2005, Bologna 2007, Legros les 5PDE5 (Isidori 2005, Bologna 2007, Legros 2008).2008).










![[exposition] Georges de La Tour Trois nuits pour une ... › ressources › 0 › 23 › 6161_dossier... · sensu, plus attaché au clair-obscur et au drame" (J. P. Cuzin et D. Salmon)](https://img.pdfslide.fr/doc/110x75/5f0d42847e708231d43975f7/exposition-georges-de-la-tour-trois-nuits-pour-une-a-ressources-a-0-a.jpg)