Embed Size (px)
Citation preview

Samah Chiry, R1

Objectifs1. Chez un patient qui a du sang dans ses selles et dont l’état hémodynamique est
instable, tenez compte des antécédents pour distinguer entre un saignement gastro-intestinal
supérieur et un saignement inférieur, car l’examen sera alors différent.
2. Chez un patient chez qui vous soupçonnez la présence de sang dans les selles, explorez d’autres causes possibles (p. ex. ingestion de betteraves, de fer, de Pepto-Bismol) avant de procéder à un examen général.
3. Recherchez les patients à risque plus élevé de saignement GI (p. ex. saignement GI antérieur, séjour aux soins intensifs, anti-inflammatoires non stéroïdiens, alcool) afin de modifier le traitement pour diminuer le risque de saignement GI (p. ex. cytoprotection)
4. Chez les patients souffrant d’un saignement GI évident, identifiez ceux qui pourraient nécessiter un traitement en temps opportun même s’ils ne sont pas encore en état de choc.
5. Chez un patient stable atteint d’un saignement GI inférieur, recherchez des causes sérieuses (p.
ex. tumeur, maladie intestinale inflammatoire, ulcère, varices) même quand le saignement
semble avoir une cause évidente (p. ex. n’attribuez pas un saignement rectal aux hémorroïdes
ou à un anticoagulant oral).
6. Chez un patient souffrant d’un saignement GI supérieur : a) incluez le saignement de varices dans votre diagnostic différentiel; b) utilisez les antécédents et l’examen physique pour évaluer la probabilité d’un
saignement variqueux, car sa prise en charge est différente.

Anatomie
saignement GI superieur vs inferieur determine par le ligament de treitz (LT).
Superieur: proximal au LT: Oesophage, estomac, 2eme / 3eme portion du duodenum
inferieur : distal au LT: petit intestin et colon

Saignement GI superieur Saignement GI inferieur
Incidence : 48-160 cas/100.000 adultes / annee
Mortalite : 10 a 14%La moyenne pour le sejour
a l’hopital (n’incluant pas les varices) avec ou sans complications est de 2.7 a 4.4 jours.
Mortalite a diminue de 23% aux EU (1998 a 2006), de 40% en Bretagne (1993 a 2007), inchange au Canada (1993 a 2003)
20-33% des episodes de saignement GI
Mortalite: 10 a 20% surtout avec les patients ages et ceux avec comorbidites
Plus frequent chez les personnes agees a cause de la haute incidence de la diverticulose et la maladie vasculaire chez ce groupe.
♂ > ♀

Saignement aigu:- moins de trois jours
- Instabilite hemodynamique et/ou besoin de
transfusion sanguine

Evaluation initiale Le premier point dans la prise en charge d’un
saignement digestif est de definir le site et la cause du saignement:
Est ce que le saignement GI est superieur ou inferieur?

L’histoireLa nature du saignement :1. Hematemese (vx du sang): origine superieure- Coffee ground emesis- Rouge frais- Caillots de sang - Apres des vomissements excessifs2. Melena - Selles noires (verifier avec le TR)- A besoin d’au moins 50cc de sang dans le tractus GI- Typiquement survient d’une origine superieure, mais 5%
peuvent etre d’origine inferieure- Occasionnellement la source est le petit intestin ou le colon
proximal3. Hematoschezia (sang rouge per rectum)- d’habitude suggere un saignement distal au LT- A considerer un saignement superieur si instabilite
hemodynamique

Les points importants dans l’histoire La duree du saignement, la frequence Les sx associes: douleur abd, un nouveau chgt dans les
habitudes de selles, fievre, urgence/tenesme, perte de poids, anorexie, N/V, satiete precoce, dysphagie/odynophagie, epistaxis/hemoptysie
Antcds: - Saignement anterieur - Trauma- Hx de radiation a l’abd et au pelvis- Ulcere peptique anterieur- Hx de maladie inflammatoire de l’intestin- Comorbidites : MCAS, ins cardiaque, maladie hepatique- Chx anterieure: AAA- Endoscopies anterieures : les rapports Medication: - NSAIDs- ASA- Anticoagulants

LaboratoireFSC Base : E, Cr, Uree (uree peut augmenter sans augmentation de
la Cr du a l’absorption des proteines du sang et a la dehydratation)
PT/PTTType et crossmatchECG chez les patients > 50 ans, ou ayant une
hx de MCAS ou arrythmie, ou ayant une DRS/palpitations associees avec le saignement

Diagnostic differentiel : saignement GI superieur
Les causes rares: ulcere de stress,ulcere de Dieulafoy, malformation AV, Fistule aorto-enterique, anastomose chirurgicale..

Saignement variqueuxSx de la maladie
hepatique Antecedants
Faiblesse, anorexie et malaise Nausee et vomissement Perte de poids Discomfort ou douleur
abdominal (QSD, epigastre et QSG)
Jaunisse et urine foncee Oedeme et ascite Prurit Ecchymoses (easy bruising) Impotence et dysfonction
sexuel Crampes musculaires
Hx de jaunisse suggerant une hepatite anterieure infectieuse ou medicamenteuse
Hx de transfusionHx de drogues IVPrise d’alcool ou AINSHx de cirrhose

Saignement variqueuxPaleurHypertrophie des parotides (reliee a l’alcolisme et/ou
malnutrition) JaunisseTelangiectasis ( peau, levres, doigts).Gynecomastie chez les hommes Fetor hepaticus erytheme palmaireAscitesCirculation collaterale autour de l’ombilic, venous hums
(bruit audible du flot turbulent dans les veines collaterales)SlenomegalieAtrophie testiculaireAngiome stellare Caput medusahemorrhoides

Diagnostic differentiel : saignement GI inferieur

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux
A. Resuscitation, risk assessment, and preendoscopy management A1. Immediately evaluate and initiate appropriate resuscitation. A2. Prognostic scales are recommended for early stratification of patients
into low- and high-risk categories for rebleeding and mortality.† A3. Consider placement of a nasogastric tube in selected patients because
the findings may have prognostic value.* A4. Blood transfusions should be administered to a patient with a
hemoglobin level 70 g/L. A5. In patients receiving anticoagulants, correction of coagulopathy is
recommended but should not delay endoscopy. A6. Promotility agents should not be used routinely before endoscopy to
increase the diagnostic yield. A7. Selected patients with acute ulcer bleeding who are at low risk for
rebleeding on the basis of clinical and endoscopic criteria may be discharged promptly
after endoscopy.† A8. Preendoscopic PPI therapy may be considered to downstage the
endoscopic lesion and decrease the need for endoscopic intervention but should not delay

Determiner l’urgence de la situation clinique: 1.Est ce que le patient est en choc? - Tachypnee, tachycardie, agitation, diminution
de l’etat de conscience, palleur indiquent une perte de sang > 1500 mL ( 30% du volume circulatoire)
- Att aux beta-bloqueurs2. Est ce que le patient est orthostatique? - SV avec TA couche et debout - Une ↓ de > 10 mmhg ou une ↑ de > 10
batt/min indiquent une perte de sang > 800 mL (15% du volume circulatoire)

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux A. Resuscitation, risk assessment, and preendoscopy management A1. Immediately evaluate and initiate appropriate resuscitation. A2. Prognostic scales are recommended for early stratification of patients
into low- and high-risk categories for rebleeding and mortality. A3. Consider placement of a nasogastric tube in selected patients because
the findings may have prognostic value.* A4. Blood transfusions should be administered to a patient with a
hemoglobin level 70 g/L. A5. In patients receiving anticoagulants, correction of coagulopathy is
recommended but should not delay endoscopy. A6. Promotility agents should not be used routinely before endoscopy to
increase the diagnostic yield. A7. Selected patients with acute ulcer bleeding who are at low risk for
rebleeding on the basis of clinical and endoscopic criteria may be discharged promptly
after endoscopy.† A8. Preendoscopic PPI therapy may be considered to downstage the
endoscopic lesion and decrease the need for endoscopic intervention but should not delay

Les predicteurs cliniques pour resaignement ou mortaliteAge > 65 ansChocComorbiditesHb initialement basMelenaBesoin de transfusionSang rouge frais au TR, dans le Vx, ou le TNGSepsis↑ uree, creat, AST, ALT

Glasgow- Blatchford Bleeding score Uree (mmol/L)
6·5-7·9 = 2 points 8·0-9·9 = 3 points 10·0-25·0 = 4 points >25·0 = 6 points
Haemoglobin pour les hommes (g/L) 120-129 =1 points 100-119 = 3 points <100 = 6 points
Haemoglobin pour les femmes (g/L) 100-119 =1 point <100 = 6 point
Pression systolique(mm Hg) 100-109 =1point 90-99 =2 point <90 =3 point
D’autres marqueurs: Pouls ≥ 100/min =1 point presentation avec melena = 1 point presentation avec syncope = 2 point Maladie hepatique= 2 point Insuffisance cardique=2 point

Rockall scoring system the most widely used, gives estimates of the risks of recurrent
bleeding and death. It is based on the three clinical factors mentioned above and on two endoscopic ones, awarding points for:
Age—0 points if less than 60; 1 point if 60 to 79; or 2 points if 80 years or older
Shock—1 point if the pulse is more than 100; 2 points if the systolic blood pressure is less than 100 mm Hg
Comorbid illness—2 points for ischemic heart disease, congestive heart failure, or other major comorbidity; 3 points for renal failure, hepatic failure, or metastatic disease
Endoscopic diagnosis—0 points if no lesion found or a Mallory-Weiss tear; 1 point for peptic ulcer, esophagitis, or erosive disease; 2 points for GI malignancy
Endoscopic stigmata or recent hemorrhage—0 points for a clean-based ulcer or flat pigmented spot; 2 points for blood in the upper GI tract, active bleeding, a nonbleeding visible vessel, or adherent clot.
The Rockall score can thus range from 0 to 11 points, with an overall score of 0, 1, or 2 associated with an excellent prognosis.

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux
A. Resuscitation, risk assessment, and preendoscopy management A1. Immediately evaluate and initiate appropriate resuscitation. A2. Prognostic scales are recommended for early stratification of patients
into low- and high-risk categories for rebleeding and mortality. A3. Consider placement of a nasogastric tube in selected patients because
the findings may have prognostic value. A4. Blood transfusions should be administered to a patient with a
hemoglobin level 70 g/L. A5. In patients receiving anticoagulants, correction of coagulopathy is
recommended but should not delay endoscopy. A6. Promotility agents should not be used routinely before endoscopy to
increase the diagnostic yield. A7. Selected patients with acute ulcer bleeding who are at low risk for
rebleeding on the basis of clinical and endoscopic criteria may be discharged promptly
after endoscopy.† A8. Preendoscopic PPI therapy may be considered to downstage the
endoscopic lesion and decrease the need for endoscopic intervention but should not delay

Tube NasoGastriqueIndication : - Devant tout saignement superieur ou saignement
indetermineBenefices therapeutiques et diagnostiquesPositive evidence que le saignement est superieur sang rouge frais endoscopie en urgence coffee ground endoscopie ds prochains
24hNegative n’exclut pas un saignement superieur
(saignement intermittent, spasme pylorique, oedeme empechant le reflux du sang duodenal)
Contraindications:- Varices oesophagiennes ne sont pas une
contraindication- Trauma facial/ fracture de l’os nasal

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux
A. Resuscitation, risk assessment, and preendoscopy management A1. Immediately evaluate and initiate appropriate resuscitation. A2. Prognostic scales are recommended for early stratification of patients
into low- and high-risk categories for rebleeding and mortality. A3. Consider placement of a nasogastric tube in selected patients because
the findings may have prognostic value. A4. Blood transfusions should be administered to a patient with a
hemoglobin level 70 g/L. A5. In patients receiving anticoagulants, correction of coagulopathy is
recommended but should not delay endoscopy. A6. Promotility agents should not be used routinely before endoscopy to
increase the diagnostic yield. A7. Selected patients with acute ulcer bleeding who are at low risk for
rebleeding on the basis of clinical and endoscopic criteria may be discharged promptly
after endoscopy.† A8. Preendoscopic PPI therapy may be considered to downstage the
endoscopic lesion and decrease the need for endoscopic intervention but should not delay

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux A. Resuscitation, risk assessment, and preendoscopy management A1. Immediately evaluate and initiate appropriate resuscitation. A2. Prognostic scales are recommended for early stratification of patients
into low- and high-risk categories for rebleeding and mortality. A3. Consider placement of a nasogastric tube in selected patients because
the findings may have prognostic value. A4. Blood transfusions should be administered to a patient with a
hemoglobin level 70 g/L. A5. In patients receiving anticoagulants, correction of coagulopathy is
recommended but should not delay endoscopy. A6. Promotility agents should not be used routinely before endoscopy to
increase the diagnostic yield. A7. Selected patients with acute ulcer bleeding who are at low risk for
rebleeding on the basis of clinical and endoscopic criteria may be discharged promptly
after endoscopy.† A8. Preendoscopic PPI therapy may be considered to downstage the
endoscopic lesion and decrease the need for endoscopic intervention but should not delay

Warfarin peut precipite un saignement Le risque de saignement GI chez les patients
ayant du coumadin est de 2.3 a 4.9 fois plus grand que ceux qui n’ont pas.
Malgre que le nbre de plaquettes n’est pas un predicteur de la mortalite, un INR > 1.5 a la presentation est un predicteur significatif de la mortalite chez les patients avec saignement superieur.
Endoscopie peut se faire avec un INR entre 2-3
Si INR supratherapeutique, il faut le corriger avant.

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux
A. Resuscitation, risk assessment, and preendoscopy management
A1. Immediately evaluate and initiate appropriate resuscitation. A2. Prognostic scales are recommended for early stratification of
patients into low- and high-risk categories for rebleeding and mortality.
A3. Consider placement of a nasogastric tube in selected patients because the findings may have prognostic value.
A4. Blood transfusions should be administered to a patient with a hemoglobin level 70 g/L.
A5. In patients receiving anticoagulants, correction of coagulopathy is recommended but should not delay endoscopy.
A6. Promotility agents should not be used routinely before endoscopy to increase the diagnostic yield.
A7. Selected patients with acute ulcer bleeding who are at low risk for rebleeding on the basis of clinical and endoscopic criteria may be discharged promptly
after endoscopy.† A8. Preendoscopic PPI therapy may be considered to downstage
the endoscopic lesion and decrease the need for endoscopic intervention but should not delay endoscopy.

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux
B. Endoscopic management B1. Develop institution-specific protocols for multidisciplinary management.
Include access to an endoscopist trained in endoscopic hemostasis. B2. Have available on an urgent basis support staff trained to assist in
endoscopy. B3. Early endoscopy (within 24 hours of presentation) is recommended for most
patients with acute upper gastrointestinal bleeding. B4. Endoscopic hemostatic therapy is not indicated for patients with low-risk
stigmata (a clean-based ulcer or a nonprotuberant pigmented dot in an ulcer bed).
B5. A finding of a clot in an ulcer bed warrants targeted irrigation in an attempt at dislodgement, with appropriate treatment of the underlying lesion.
B6. The role of endoscopic therapy for ulcers with adherent clots is controversial. Endoscopic therapy may be considered, although intensive PPI therapy alone may be sufficient.
B7. Endoscopic hemostatic therapy is indicated for patients with high-risk stigmata (active bleeding or a visible vessel in an ulcer bed).
B8. Epinephrine injection alone provides suboptimal efficacy and should be used in combination with another method.
B9. No single method of endoscopic thermal coaptive therapy is superior to another.
B10. Clips, thermocoagulation, or sclerosant injection should be used in patients with high-risk lesions, alone or in combination with epinephrine injection.
B11. Routine second-look endoscopy is not recommended. B12. A second attempt at endoscopic therapy is generally recommended in
cases of rebleeding.

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueuxPharmacologic managementC1. Histamine-2 receptor antagonists are not
recommended for patients with acute ulcer bleeding.C2. Somatostatin and octreotide are not routinely
recommended for patients with acute ulcer bleeding.C3. An intravenous bolus followed by continuous-
infusion PPI therapy should be used to decrease rebleeding and mortality in patients with high-risk stigmata who have undergone successful endoscopic therapy.
C4. Patients should be discharged with a prescription for a single daily-dose oral PPI for a duration as dictated by the underlying etiology.

IPP
La dose recommendee d’omeprazole: 80 mg bolus suivi d’une perfusion de 8 mg/h pour 72 h diminue le resaignement , l’indication pour la chirurgie et la mortalite.
Apres le traitement de l’evenement aigu, un IPP est recommende pour 6 a 8 semaines, plus long si test positif pour H.pylori ou s’il prend l’ASA ou un AINS.

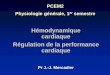
Algorithm for patients with acute upper gastrointestinal bleeding.
ALBELDAWI M et al. Cleveland Clinic Journal of Medicine 2010;77:131-142
©2010 by Cleveland Clinic

Endoscopic stigmata of bleeding peptic ulcer (arrows) and risk of recurrent bleeding and death. Upper endoscopy is 90% to 95% diagnostic for acute upper GI
bleeding.
ALBELDAWI M et al. Cleveland Clinic Journal of Medicine 2010;77:131-142
©2010 by Cleveland Clinic

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueux
D. Nonendoscopic and nonpharmacologic in-hospital management
D1. Patients at low risk after endoscopy can be fed within 24 hours.
D2. Most patients who have undergone endoscopic hemostasis for high-risk stigmata should be hospitalized for at least 72 hours thereafter.
D3. Seek surgical consultation for patients for whom endoscopic therapy has failed.
D4. Where available, percutaneous embolization can be considered as an alternative to surgery for patients for whom endoscopic therapy has failed.
D5. Patients with bleeding peptic ulcers should be tested for H. pylori and receive eradication therapy if it is present, with confirmation of eradication.
D6. Negative H. pylori diagnostic tests obtained in the acute setting should be repeated.

Preferred therapies for Helicobacter pylori infection
1. Triple therapy : - Proton pump inhibitor twice a day + Clarithromycin
(Biaxin) 500 mg twice a day + Amoxicillin 1,000 mg twice a day
- 10–14 days - 70%–85% - Proton pump inhibitor twice a day + Clarithromycin 500
mg twice a day + Metronidazole (Flagyl) 500 mg twice a day
- 10–14 days - 75%–85% - Consider in penicillin-allergic patients who have not
previously received a macrolide or who cannot tolerate bismuth quadruple therapy
2. Quadruple therapy - Proton pump inhibitor twice a day + Bismuth subsalicylate
525 mg twice a day + Metronidazole 250 mg four times a day + Tetracycline 500 mg four times a day
- 10–14 days - 75%–90% - Consider in penicillin-allergic patients

Recommendations de la prise en charge des patients avec saignement GI superieur non variqueuxE. Postdischarge, ASA, and NSAIDsE1. In patients with previous ulcer bleeding who
require an NSAID, it should be recognized that treatment with a traditional NSAID plus PPI or a COX-2 inhibitor alone is still associated with a clinically important risk for recurrent ulcer bleeding.
E2. In patients with previous ulcer bleeding who require an NSAID, the combination of a PPI and a COX-2 inhibitor is recommended to reduce the risk for recurrent bleeding from that of COX-2 inhibitors alone.
E3. In patients who receive low-dose ASA and develop acute ulcer bleeding, ASA therapy should be restarted as soon as the risk for cardiovascular complication is thought to outweigh the risk for bleeding.
E4. In patients with previous ulcer bleeding who require cardiovascular prophylaxis, it should be recognized that clopidogrel alone has a higher risk for rebleeding than ASA combined with a PPI.

ASA
The higher the aspirin dose, the higher the risk. Aspirin doubles the risk of upper GI bleeding at daily doses of 75 mg , and quadruples it at doses of 300 mg.
The most important risk factor for upper GI bleeding in patients taking aspirin is a history of peptic ulcer bleeding.
Approximately 15% of aspirin users who have bleeding from ulcers have recurrent bleeding within 1 year.
When considering whether to discontinue antiplatelet therapy, a cardiologist should be consulted along with a gastroenterologist to weigh the risks of GI bleeding vs thrombosis.

Clopidogrel (Plavix)
Clopidogrel (Plavix) is recommended for hospitalized patients with acute coronary syndrome who cannot tolerate the GI side effects of aspirin.
This recommendation was largely based on the safety data from the CAPRIE (Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events) trial, in which the incidence of major GI bleeding was lower in the clopidogrel group (0.52%) than in the aspirin group (0.72%; P < .05).

In a recent double-blind randomized controlled trial in patients with a history of aspirin-induced bleeding, the combination of low-dose aspirin plus esomeprazole (Nexium) twice a day was superior to clopidogrel by itself in terms of the rate of recurrent bleeding (0.7% vs 8.6%; P < .05).
A similar trial showed nearly identical results: 0% upper GI bleeding in the group receiving aspirin plus esomeprazole 20 mg daily, vs 13.6% in the clopidogrel group (P = .0019).
These studies suggest that a once-daily proton pump inhibitor combined with aspirin is a safer alternative than clopidogrel alone

Clopidogrel plus a proton pump inhibitorInterestingly, recent studies have shown that
omeprazole (Losec) decreases the antiplatelet effect of clopidogrel, possibly by inhibiting the CYP2C19 enzyme.
However, concomitant use of , lansoprazole (Prevacid), and esomeprazole (Nexium) did not have this effect, suggesting that although all proton pump inhibitors are metabolized to a varying degree by CYP2C19, the interaction between proton pump inhibitors and clopidogrel is not a class effect.
Therefore, pantoprazole, lansoprazole, and esomeprazole may be the appropriate proton pump inhibitors to use with clopidogrel in patients who have a clear indication for the medication, consistent with current guideline recommendations.


Indications pour la chirurgie Emergency surgery is required in about 10-
25% of patients with lower gastrointestinal bleeding (LGIB).
The indications for surgery :1. Persistent hemodynamic instability with
active bleeding2. Persistent, recurrent bleeding3. Transfusion of more than 4 units packed red
bloods cells in a 24-hour period, with active or recurrent bleeding


Take Home message The first priority is to ensure that the patient is
hemodynamically stable, which often requires admission to the intensive care unit for monitoring and fluid resuscitation.
Peptic ulcers account for most cases of upper GI bleeding, but bleeding from varices has a much higher case-fatality rate and always demands aggressive treatment.
Patients with ulcer disease should be tested and treated for Helicobacter pylori infection.
Patients with a history of bleeding ulcers who need long-term treatment with aspirin or a nonsteroidal anti-inflammatory drug should also be prescribed a proton pump inhibitor.

Bibliographie
International Consensus Recommendations on the Management of Patients With Nonvariceal Upper Gastrointestinal Bleeding, Annals of Internal Medicine, 2010; 152: 101-113.
Management of the Adult Patient With Acute Lower Gastrointestinal Bleeding, American Journal of Gastroenterology (1998) 93, 1202–1208






















![Epuration extra rénale.ppt [Mode de compatibilité] › pdf_ppt_docs › college2014 › epurationextrarenale.pdf‐IRA avec instabilité hémodynamique sévère ‐Désordres hydroéléctrolytiquesmettant](https://img.pdfslide.fr/doc/110x75/60d94fa14677cd24300cee43/epuration-extra-rnaleppt-mode-de-compatibilit-a-pdfpptdocs-a-college2014.jpg)