Embed Size (px)
Citation preview

Turkish Neurosiirgery 10: 126 - 130, 2000 Çolak: Tliree-le"d ccrvical disCt'ctolllY
Three-Level Cervical Discectomy and FusionWithout Internal Fixation
Internal FiksasyonsuzServikal Diskektomi
Uç Seviyelive Füzyon
AHMET ÇOLAK, MURAT KUTLAY, LEVENT TOSYALI, MEHMET NUSRET DEMIRCAN
GATA Haydarpasa Teaching Hospital, Department of Neurosurgery, (AÇ, MK, LT, MND) IstanbuL, Turkey
Received : 14.12.1998 ~ Accepted : 4.2.1999
Abstract: it is generally believed that the rate ofpseudoarthrosis rises as the number of operatiye levels ofanterior cervical discectomy and fusion increases. Thisretrospective study evaluated bone union status in 13patients who underwent three-level anterior cervicaldiscectomy and fusion with the Cloward technique. Noallografts or internal fixators were used in any of theprocedures. Pseudoarthrosis developed in four patients,each with one level affected, and three of these individualswere cigarette smokers. None of the 13 patients neededsubsequent surgery, and there were no majorpostoperative complications. The Cloward technique iseffective for three-level anterior cervk"l discectomy andfusion, but the associated 30% pseudoarthrosis rate in thegroup of patients in this study was unacceptable. In allcases, the cervical level that developed pseudoarthrosiswas the lowest motion segment that had been operated.
Key words: Anterior cervical discectomy and fusion,autograft, internal fixation, pseudoarthrosis
INTRODUCTION
Anterior eervieal diseeetomy and fusion is awidely aeeepted method of treating symptomatie diseherniation and degenerative disorders of the eerviealspine (1,2,7). it can be diffieult to aehieve good resultsin individuals who undergo multiple-Ievel surgerybeeause these patients are at high risk for developing
126
Özet: Genellikle anterior servikal diskektomi ve füzyonseviye sayisi arttikça psödoartroz oraninin arttigi kabuledilmektedir. Bu retrespektif çalismada üç seviyelianterior servikal diskektomi ve Cloward teknigi ile füzyonyapilan 13 hastada kemik birlesmesi degerlendirilmistir.Ameliyatlarin hiçbirinde allogreft ya da internal fiksatörkullanilmamistir. Dört hastada her birinde birer seviyeolmak üzere psödoartroz gelismistir ve bu hastalardanüçü sigara kullaniyordu. 13 hastadan hiçbirinde ikinci birameliyata gereksinim duyulmamis ve hiçbirinde majorpostoperatif komplikasyon görülmemistir. Üç seviyelianterior diskektomi ve füzyon için Cloward teknigi etkinbir yöntemdir, fakat bu grup hastada görülen % 30oranind"ki psödoartroz orani kabul edilebilir degildir.Psödoartrozis dört olguda da opere edilen en alt hareketsegmentinde olusmustur.
Anahtar kelimeler: Anterior servikal diskektomi ve
füzyon, internal fiksasyon, otograft, psödoartroz
pseudoarthrosis. Although not all pseudoarthrosesare symptomatie, the overall outeome is superiorwhen solid fusion is aehieved. We prefer to use theCloward teehnique beeause of our familiarity withthis method for fusion operations. In this study, weanalyzed our results in patients who underwent theCloward surgieal teehnique for three-Ievel anteriordiseectomy and fusion, and assessed the quality of

T/lrkisJi Ne/lros/lrgery 10: 126 - 130, 2000
vertebral fusion and overall outcome in this group.
PATIENTS AND METHODS
Between 1992and 1996,60 patients at our centerunderwent surgery for cervical disc herniation. Ofthese patients, 44 had one-Ievel, 2 had two-Ievel, and14 had three-Ievel herniation. One of the 14 three
level operated patients was lost to follow-up, thusour series included 13 patients, specifically 7 malesand 6 females. The mean patient age was 51.5 years(range, 21 to 72 years). Although all 13 individualscomplained of neck and arm pain that did notrespond to conservative treatment, their main clinicalproblems at presentation were radiculopathy in 8patients, and cervical spondylotic myelopathy in 5patients. None of the patients had had previoussurgery in the cervical region. Three individuals werecigarette smokers.
Prior to 1994, we evaluated four patients usingcomputerized tomography, but magnetic resonanceimaging was used to assess the nine most recentpatients. We documented all herniated discs andi orosteophytes preoperatively by one or the other ofthese methods. Anterior cervical discectomy andfusion were performed using the Cloward techniqueat alllevels in all patients, with autografts harvestedfrom each patient's iliac crest. No allografts orinternal fixators were used. We obtained immediatepostoperative radiographs to confirm that the graftswere correctly positioned. Each individual wore arigid cervical collar for 8 weeks postoperatively, andpatients were followed clinically and radiologicallyfor a mean of 41.3 months (range, 22 to 72 months).
Pre- and postoperative pa in status was gradedas mild, moderate, or severe, in accordance withRobinson's criteria (7). In all patients, radiographicfusion was determined based on plain lateral cervicalradiographs and flexion-extension views. The criteriafor fusion were bridging of the disc space withtrabecular bone, and 1 mm or less change measuredbetween spinous processes on flexion-extensionviews.
The disc pathology documented at the 39cervicallevels that required surgery was as follows:posterior protrusion of the disc (22Ievels), extrusionof a disc fragment below the posterior edge ofthe vertebra (8 levels), and herniation of discmaterial through the posterior longitudinalligament(9 levels).
Çolak: TJiree-level cervical discectoniy
RESULTS
The eight patients with radiculopathy recoveredfull motor function postsurgery, and noneexperienced worsening of their neurologicalsymptoms. In addition, none of these patientsdeveloped cervical disc herniation at any other levelin the postoperative course. Two patients weredysphagic in the immediate postoperative period,but this resolved within 2 weeks of the surgery. Therewere no cases of wound or graft infection. Seven ofthe eight patients experienced pain at the donor site,but this resolved before suture removal in all cases.
There was no graft displacement, and none of thepatients needed further surgery.
Of the 13 patients in this series, 9 developedsolid fusion at all operated levels. Seven of the ninebecame symptom-free, and two patients experiencedoccasional mild cervical pain during follow-up, butthis did not cause any significant functionallimitation(Figure 1). Four of the 13 patients were diagnosedwith pseudoarthrosis, with one level affected in eachindividual (Figure 2). We noted that three of the fourpatients with pseudoarthrosis smoked prior to andfollowing their operations, but the smaIl number ofpatients in this series was insufficient for statisticalanalysis of any possible association between smokingand pseudoarthrosis (Table 1). In each case,pseudoarthrosis developed at the lowest motionsegment that had been operated. Two of the fourindividuals with pseudoarthrosis had mild pain, onehad moderate pain, and one was asymptomatic.
DISCUSSION
Anterior cervical discectomy and fusion arewidely accepted as safe and effective treatment forcervical disc herniation and cervical spondylosis.With regard to clinical outcome, pa in resolves first,then motor function returns, and sensory function isrestored last (2). In addition to removing herniateddi ses and bone spurs, the aim of these procedures isto achieve bone union at every level of vertebralfusion. Creating a solid arthrodesis is considered vitalto obtaining good results with fusion surgery (6). ifthe fusion fails and pseudoarthrosis develops, theusual outcome is long-term pain.
Patients who undergo these procedures mustbe followed until radiological studies confirm boneunion. The use of lateral flexion and extension
radiographs is advised for assessing union because,although plain lateral radiographs may indicate solid
127

Turkis/i Neurosiirgery 10: 126 - 130, 2000 Çolak: Tliree-level cervical discectolll!l
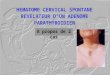
Figure 1: A patient's lateral hyperextension (a) and hyperflexion (b) radiographs show solid fusion at all three operated levels.
Table i: Age (years) and gender, clinical presentation, levels operated, follow-up periods (months) andpseudoarthrosed levels of patients.
Patient Age &ClinicalOperatedFollow-UpPseudoarthrosis
No.
GenderPresentationLevelsPeriodLevel
1
46M* RC 3-4,4-5,5-634C 5/6
2
42F RC 4-5,5-6,6-772-3
58F SMC 3-4,4-5,5-626-4
38F RC 3-4,4-5,5-642-5
44M RC 3-4,4-5,5-622-6
61F* SMC 4-5,5-6,6-745C 6/7
7
72M SMC 3-4,4-5,5-636-8
66M* RC 4-5,5-6,6-739C 6/7
9
51F RC 4-5,5-6,6-742-10
71M* SMC 3-4,4-5,5-655-11
21M* RC 3-4,4-5,5-638-12
42F RC 3-4,4-5,5-626C 5/6
13
58M SMC 3-4,4-5,5-660-
Abbreviations*: smoker, R; radiculopathy, SM: spondylitic myelopathy.
128

Turkish Neurosurgery 10: 126 - 130, 2000
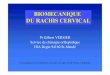
Figure 2: A lateral radiograph of a patient demonstratessolid fusion at the upper two levels, andpseudoarthrosis at the third level at whichsurgery was performed
fusion, luceney can often be deteeted at the vertebralinterface. Further, long-term follow-up is important,since some authors have reported that fusions thatappeared solid on radiographic studies done 3 to 4months postsurgery later developed pseudoarthroses(2).
A number of factors are thought to influencethe success of vertebral fusion surgery. Brown et aL.demonstrated in their series that the lumbar fusionrate in smokers was statisticaIIy lower than that innonsmokers (3). In their prospective series of 132anterior cervical interbody-fused patients, Bishopand colleagues found that cigarette smoking wasdetrimental to successful bone fusion (1). Asmentioned, three of the four patients with fusionfailure in our series were smokers. We advised these
individuals to stop smoking as soon as possible, andstressed the importance of doing so at least, after thesurgery. Regarding other influences, as Table 1shows, two of our four pseudoarthrosis patients were
Çolak: Three-level ceriJica/ discectol1lY
males, and we found no significant differencebetween the pseudarthrosis group and the rest ofthe 13 patients in the series with regard to agedistribution. it appears that smoking is the only factorthat we can control preoperatively which isknown to have a negatiye influence onpseudoarthrosis.
In their retrospective study, Bohlman andcoworkers found a positive correlation between thenumber of operated levels and the rate ofpseudoarthrosis. Although they stated thatmultiple vertebrectomy and one long strut graft fixedin place following multiple level discectomy mightlower the number of healing surfaces and reduceproblems with pseudoarthrosis, neither their teamnor ours chose to attempt this technique (2). Emeryet aL.suggested that the number of operatiye levelsshould not affect the local blood supply becauseof the highly vascular nature of the vertebralbody. it is likely that altered biomechanics playsthe most important role at graft-body interfaceswhen the number of operative levels is relatively high(5).
As an alternative to the procedure we use, theRobinson technique is also a popular method, butwe have performed the Cloward technique safely for15 years without any major complications. Anteriorcervical fixation has been suggested as an effectiveoption for multiple-le vei operations (4). Regardingpostsurgical assessment, the follow-up period forthese patients must be long enough to confirm solidfusion, but it seems reasonable to accept x-rayconfirmation of bone union as the last necessaryrecheck.
CONCLUSION
Although use of the Cloward technique withoutinternal fixation is perhaps not the ideal procedurefor multiple-level fusions, we have used this methodsafely and successfully for three-level anteriorcervical discectomy and fusion. The clinical problemsin our patients who developed pseudoarthroses wereso mild that no further surgery was required. it isessential that every patient be followed until solidfusion is confirmed at all operated levels, but wesuggest there is no need to continue with furtherrechecks in asymptomatic patients. In addition to theneed to confirm bone union, close follow-up· isrequired to monitor for common complications, suchas infection and deformity.
129

Turkis/i Neiirosurgenj 10: 126 - 130, 2000
Correspondence: Dr. Ahmet ÇOLAK
GATA Haydarpasa Egitim HastanesiBeyin ve Sinir Cerrahisi Servisi 81327Üsküdar - Istanbul
Phone: 216-3462600 ext. 2658 or 2657
Fax: 216-348 78 80
REFERENCES
1. Bishop RC, Moore KA, Hadley MN; Anterior CervicalInterbody Fusion Using Autogenic Bone GraftSubstrate: A Prospective Comparatiye Analysis. JNeurosurg 85: 206-210, 1996
2. Bohlman HH, Emery SE, Goodfellow DB, Jones PK;Robinson Anterior Cervical Oiscectomy and Arthrosisfor Cervical Radiculopathy. J. Bone and Joint Surg. 75-
130
Çolak: T/iree-levcl cerviciil discccto11lY
A: 1298-1307, 19933. Brown CW, Orme TL, Richardson HO; The Rate of
Pseudoarthrosis (Surgical Union) in Patients Who areSmokers and Patients Who are Nonsmokers: A
Comparison Study. Spine. 11: 942-943, 19864. Connolly PI, Esses SI, Kostuik JP: Anterior Cervical
Fusion: Outcome Analysis of Patients Fused with and
without Anterior Cervical Plates. J Spinal Oisord 9; 202206, 1996
5. Emery SE, Fisher RS, Bohlman; Three-Level AnteriorCervical Oiscectomy and Fusion. Spine 22: 2622-2625,1997
6. Newman M.: The Outcome of Pseudoarthrosis after
Cervical Anterior Fusion. Spine 18; 2380-2382, 19937. Robinson RA, Walker AE, FerHc OC, Wiecking DK;
The Results of Anterior Interbody Fusion of theCervical Spine. J Bone and Joint Surg [Am] 44: 15691587, 1962