Embed Size (px)
Citation preview

Traitement de la douleur chronique par radiofréquence
12
K N E E U S G U I D E D
1 • Patient in supine position, affected
knee elevated.• For Superior Lateral and Superior
Medial Genicular Nerve: align transducer in coronal orientation over the joint line.
• Move cephalad to metaphyseal/diaphyseal junction femur.
2 • Identify genicular nerve and artery,
located near the periosteum.• If neurovascular bundle is poorly
visualised, use metaphyseal/diaphyseal junction as bony land-mark for introducer placement.
• Mark skin at midpoint transducer.
3 • Turn transducer to an axial
orientation, confirm 50% depth of femur.
• Anaesthetise skin, advance introducer AP in plane to the nerve or 50%.
• Turn transducer in coronal plane and verify introducer tip is near nerve or junction.
4 • For Inferior Medial Genicular
Nerve: align transducer in coronal orientation over the joint line.
• Move caudal to metaphyseal/diaphyseal junction tibia.
5 • Identify genicular nerve and artery,
located near the periosteum. • If neurovascular bundle is poorly
visualised, use metaphyseal/diaphyseal junction as bony land-mark for introducer placement.
• Mark skin at midpoint transducer.
8 9
H I P
1 • Patient in supine position.• Obtain AP image with head of
femur in the center.
2 • Target femoral nerve is the
12 o’clock position on the superior osseous rim of the acetabulum.
• Overlay target with introducer, slide to entry point, lateral of the inguinal crease.
• Advance introducer to the target site where osseous acetabulum is contacted.
3 • Visualise incisura and ischial
tuberosity. • Place needle over the inferior
aspect of the ischium.• Enter at the 6 o’clock position,
relative to the incisura.
4 • Maintain intermittent contact
with the anterior ischial surface during advancement towards first lesion target for the obturator nerve.
• Avoid superficial direction of needle travel.
5 • Retract probe approximately
1 cm inferior.• Perform lesion at the second
obturator nerve target position.
10
S H O U L D E R
1 • Patient in prone position, hand
palm affected side pronated. • Obtain AP view to visualise
shoulder girdle. • Then rotate approximately
15°-40° ipsilateral oblique, decline approximately 15°-40° caudal to visualise spinoglenoid notch.
2 • Position introducer on the posterior
osseous rim of the glenoid fossa, lateral and superior to the spinoglenoid notch (first suprascapular nerve target).
• Stay in the upper ⅓ – ½ of the glenoid fossa on the most lateral border.
• Perform the testing and lesioning.
3 • Remove the probe from the intro-
ducer and replace with stylet. • Reposition the introducer inferiorly
3-4mm from 1st position, lateral and inferior to the spinoglenoid notch (second suprascapular nerve target).
• Perform testing and lesioning.
4 • Maintain C-arm angles and
translate to center over the head of the humerus.
• Place introducer inferior to the tubercle where it begins to taper into the humerus on the most lateral border (first axillary nerve target).
5 • Remove the probe from the
introducer and replace with the stylet.
• Reposition tip of introducer towards the most inferior and lateral border of the greater tubercle (second axillary nerve target).
6
L U M B A R
1 • Patient in prone position. • True AP image of treatment level,
tilt C-arm to square off superior end plates.
2 • Rotate ipsilateral oblique
(35°-40°) and place SAP in centre of disc space.
3 • Target location is the midpoint of
the base of the SAP, also referred to as “Scotty dog eye”.
4 • Insert introducer using a gun
barrel approach till bony contact. • AP view to check if not lateral on
the transverse process.
5 • Go to lateral view to confirm
depth and to assure tip is posterior to the z-joint lucency.

Traitement de la douleur chronique par radiofréquence
Dr Aissou HPPE, Champigny sur Marne
Conflits intérêts: Aucun

Recommandations SFETD
• Radiofréquence pulsée: Il existe une recommandation faible en faveur de l’utilisation de la radiofréquence pulsée dans les douleurs postzostériennes thoraciques. Il n’est pas possible de conclure concernant l’utilisation de la PRF pour les douleurs radiculaires.

Recommandations SFETD
• Radiofréquence pulsée: Il existe une recommandation faible en faveur de l’utilisation de la radiofréquence pulsée dans les douleurs postzostériennes thoraciques. Il n’est pas possible de conclure concernant l’utilisation de la PRF pour les douleurs radiculaires.

Recommandations SFETD
• Radiofréquence pulsée: Il existe une recommandation faible en faveur de l’utilisation de la radiofréquence pulsée dans les douleurs postzostériennes thoraciques. Il n’est pas possible de conclure concernant l’utilisation de la PRF pour les douleurs radiculaires.

Antalgiques, Local (Capsaïcine, Toxine botulique), kinésithérapie, ostéopathe, acupuncture
TENS, psychothérapie (Hypnose, TCC, sophrologie etc..), rTMS
Anesthésie locorégionale, infiltration
Radiofréquence continue ou pulsée, cryoneurolyse, SNPC
Stimulation médullaire, intra-crânienne
Chirurgie de dénervation
Moins invasif
Plus invasif
Stratégies thérapeutiques

Antalgiques, Local (Capsaïcine, Toxine botulique), kinésithérapie, ostéopathe, acupuncture
TENS, psychothérapie (Hypnose, TCC, sophrologie etc..), rTMS
Anesthésie locorégionale, infiltration
Stimulation médullaire, intra-crânienne
Chirurgie de dénervation
Moins invasif
Plus invasif
Stratégies thérapeutiques
Radiofréquence continue ou pulsée, cryoneurolyse, SNPC

Antalgiques 2 classes
Activité Physique et adaptative
TENS
Acupuncture, Hypnose etc.
Blocs diagnostics et neuromodulation
peripherique
Pompe intratechale et
neuromodulation centrale
Chirurgie denervation
Principes de prise en charge patients douloureux chroniques

Blocs diagnostics ou infiltrations
Radiofréquence continue
Radiofréquence Pulsée Cryoneurolyse
Neurostimulation périphérique
Principes de prise en charge patients douloureux chroniques

La radiofréquence est une thérapie non médicamenteuse qui utilise les propriétés antalgiques des courants électriques de haute fréquence (400 à 500 kHz).
L'application d'un courant sinusoïdal (400 à 500 kHz) provoque une agitation ionique autour de l’électrode et une augmentation de température locale. Cette augmentation de température est à l’origine des lésions tissulaires.
Radiofréquence Continue et Pulsée

Matériel radiofréquence
• Generateur
• Canule
• Electrode
• une terre

Radiofréquence Continue et Pulsée
Continue
Pulsée

CRF PRF
Conventionnelle Coolief
Température 70-90° 70-90° 42°
Types lesions Neurolyse Neurolyse Neuromodulation
Taille de la lésion + ++ -modification structurelle Interruption du nerf Interruption du nerf pas de modification
structurelle
Type de nerfs ciblés sensitifs pur sensitifs pur sensitifs pur ou mixtes
Durée de l’effet antalgique
2-3 ans 2-3 ans 4-24 mois
Radiofréquence Continue et Pulsée

Procédure
• Après identification du nerf ou de la zone cible sous échographie ou scopie, positionnement de la canule
• Introduction de l’electrode dans la canule
• Stimulation sensitive puis motrice
• Injection d’une solution AL à travers la canule
• Procédure de radiofréquence 90 à 300 sec selon le type de radiofréquence

Indications • zona
• Nevralgie d'Arnold
• Nevralgie du trijumeau
• Gonalgie
• Arthralgie hanche et épaule
• névrome, méralgie etc…
12
K N E E U S G U I D E D
1 • Patient in supine position, affected
knee elevated.• For Superior Lateral and Superior
Medial Genicular Nerve: align transducer in coronal orientation over the joint line.
• Move cephalad to metaphyseal/diaphyseal junction femur.
2 • Identify genicular nerve and artery,
located near the periosteum.• If neurovascular bundle is poorly
visualised, use metaphyseal/diaphyseal junction as bony land-mark for introducer placement.
• Mark skin at midpoint transducer.
3 • Turn transducer to an axial
orientation, confirm 50% depth of femur.
• Anaesthetise skin, advance introducer AP in plane to the nerve or 50%.
• Turn transducer in coronal plane and verify introducer tip is near nerve or junction.
4 • For Inferior Medial Genicular
Nerve: align transducer in coronal orientation over the joint line.
• Move caudal to metaphyseal/diaphyseal junction tibia.
5 • Identify genicular nerve and artery,
located near the periosteum. • If neurovascular bundle is poorly
visualised, use metaphyseal/diaphyseal junction as bony land-mark for introducer placement.
• Mark skin at midpoint transducer.
8 9
H I P
1 • Patient in supine position.• Obtain AP image with head of
femur in the center.
2 • Target femoral nerve is the
12 o’clock position on the superior osseous rim of the acetabulum.
• Overlay target with introducer, slide to entry point, lateral of the inguinal crease.
• Advance introducer to the target site where osseous acetabulum is contacted.
3 • Visualise incisura and ischial
tuberosity. • Place needle over the inferior
aspect of the ischium.• Enter at the 6 o’clock position,
relative to the incisura.
4 • Maintain intermittent contact
with the anterior ischial surface during advancement towards first lesion target for the obturator nerve.
• Avoid superficial direction of needle travel.
5 • Retract probe approximately
1 cm inferior.• Perform lesion at the second
obturator nerve target position.
10
S H O U L D E R
1 • Patient in prone position, hand
palm affected side pronated. • Obtain AP view to visualise
shoulder girdle. • Then rotate approximately
15°-40° ipsilateral oblique, decline approximately 15°-40° caudal to visualise spinoglenoid notch.
2 • Position introducer on the posterior
osseous rim of the glenoid fossa, lateral and superior to the spinoglenoid notch (first suprascapular nerve target).
• Stay in the upper ⅓ – ½ of the glenoid fossa on the most lateral border.
• Perform the testing and lesioning.
3 • Remove the probe from the intro-
ducer and replace with stylet. • Reposition the introducer inferiorly
3-4mm from 1st position, lateral and inferior to the spinoglenoid notch (second suprascapular nerve target).
• Perform testing and lesioning.
4 • Maintain C-arm angles and
translate to center over the head of the humerus.
• Place introducer inferior to the tubercle where it begins to taper into the humerus on the most lateral border (first axillary nerve target).
5 • Remove the probe from the
introducer and replace with the stylet.
• Reposition tip of introducer towards the most inferior and lateral border of the greater tubercle (second axillary nerve target).
6
L U M B A R
1 • Patient in prone position. • True AP image of treatment level,
tilt C-arm to square off superior end plates.
2 • Rotate ipsilateral oblique
(35°-40°) and place SAP in centre of disc space.
3 • Target location is the midpoint of
the base of the SAP, also referred to as “Scotty dog eye”.
4 • Insert introducer using a gun
barrel approach till bony contact. • AP view to check if not lateral on
the transverse process.
5 • Go to lateral view to confirm
depth and to assure tip is posterior to the z-joint lucency.

Cas clinique
• Patiente de 44 ans accident de la circulation avec écrasement sans fracture en 2011.
• Gonalgie chronique droite face interne avec flexion limité < 90°, périmètre de marche de 3 min avec canne.
• EVA 7/10 au repos et DN4 7. AT depuis 2011. Multiples traitements médicaux avec effets secondaires.
• Prise en charge durant 5 mois avec TENS, infiltration diagnostique suivi d’une radiofréquence des nerfs géniculés et saphène interne. Marche sans canne, reprise de la marche nordique. Reprise du travail.
12
K N E E U S G U I D E D
1 • Patient in supine position, affected
knee elevated.• For Superior Lateral and Superior
Medial Genicular Nerve: align transducer in coronal orientation over the joint line.
• Move cephalad to metaphyseal/diaphyseal junction femur.
2 • Identify genicular nerve and artery,
located near the periosteum.• If neurovascular bundle is poorly
visualised, use metaphyseal/diaphyseal junction as bony land-mark for introducer placement.
• Mark skin at midpoint transducer.
3 • Turn transducer to an axial
orientation, confirm 50% depth of femur.
• Anaesthetise skin, advance introducer AP in plane to the nerve or 50%.
• Turn transducer in coronal plane and verify introducer tip is near nerve or junction.
4 • For Inferior Medial Genicular
Nerve: align transducer in coronal orientation over the joint line.
• Move caudal to metaphyseal/diaphyseal junction tibia.
5 • Identify genicular nerve and artery,
located near the periosteum. • If neurovascular bundle is poorly
visualised, use metaphyseal/diaphyseal junction as bony land-mark for introducer placement.
• Mark skin at midpoint transducer.

Innervation du genou et RF • Branches nerf fémoral (saphène
interne, vaste latérale, vaste médiale et vaste interne)
• Branches nerf sciatique (nerf géniculé supero-mediale infero-mediale supero-laterale et infero-laterale)
FIGURE 5. Distal exposure of course of superior medial genicular nerve, medial views. A, Distal VM intact. B, Distal VM reflected.*Medial epicondyle. ADM indicates adductor magnus tendon; DGA, descending genicular artery; F, femur; FA, femoral artery; GR, gracilis;NVM, nerve to vastus medialis; P, patella; RF, rectus femoris; S, sartorius; SM, semimembranosus; SMGA, superior medial genicular artery.Reprinted with permission from Philip Peng Educational Series.
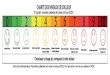
FIGURE 6. Frequency map of the innervation of the anterior knee joint. A, Lateral view. B, Anterior view. C, Medial view. Reprinted withpermission from Philip Peng Educational Series.
Tran et al Regional Anesthesia and Pain Medicine • Volume 43, Number 4, May 2018
6 © 2018 American Society of Regional Anesthesia and Pain Medicine
Copyright © 2018 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.
www.painphysicianjournal.com 141
Comparison Between 2 Methods for Genicular Nerve Block
ating table with a pillow under the popliteal fossa to reduce discomfort. After sterile preparation of the op-erative field and sterile cover wrapping of the 12-MHz linear transducer (XarioTM SSA-660A; Toshiba Medical Systems Corporation, Otawara-shi, Japan), the transduc-er was first placed on the junctions between the epicon-dyles and shafts of the femur and tibia. The transducer was then moved up or down to identify the genicular arteries, which were usually near the periosteal areas as confirmed by color Doppler ultrasound. Given that the superior lateral (12), superior medial (SM), and in-ferior medial (IM) genicular arteries travel along each genicular nerve (Fig. 1B), the location of the needle tip should be within the vicinity of each genicular artery. After identifying the genicular arteries, the skin and subcutaneous tissue were anesthetized with 1 mL of 1% lidocaine at each target point. The needle was inserted using the long-axis view of the ultrasound probe. After positioning the needle tip next to a genicular artery, a gentle aspiration was performed before administering 2 mL of the same injectate mentioned above at each nerve.
Measured Variables and Follow-upAll baseline values were assessed prior to the
procedure, whereas postprocedure outcome measure-ments were evaluated after 4 and 12 weeks. Demo-graphic data for all patients were collected through standard history-taking, as well as physical and radio-logical examinations. Pain intensity was assessed us-ing the single 11-point Numeric Rating Scale (NRS-11) in which 0 = no pain and 10 = worst pain perceivable. To measure subjective knee functionality, the Western Ontario and McMaster’s Universities Osteoarthritis Index (WOMAC) was used. The WOMAC consists of 5 questions measuring pain, 2 measuring joint stiffness, and 17 measuring functional limitation, with all ques-tions scored on a scale of 0 to 4. The total scores for pain, stiffness, and physical function, which ranged from 0 to 20, 0 to 8, and 0 to 68, respectively, were then determined. Accordingly, higher scores on the WOMAC indicate worse pain, stiffness, and functional limitation (13). To obtain valid baseline values and outcome measurements, all patients were instructed on how to appropriately fill out the NRS-11 and
Fig. 1. A. Anteroposterior fluoroscopic view after needle insertion into the junction between the shaft and epicondyle of the tibia and femur. B. Ultrasound images identifying genicular arteries and nerves using color Doppler mode. White arrows indicate genicular arteries, while arrowheads indicate genicular nerves appearing as a small rounded hypoechoic dot. C. Anteroposterior and lateral fluoroscopic images after ultrasound-guided needle insertion for genicular nerve block. The location of the needle tip was similar to that in Panel A. Contrast dye spread showed that the needle tips were positioned in the periosteal area, which is the junction between the shaft and epicondyle of long bones.
Pain Physician: March/April 2019: 22:139-146
144 www.painphysicianjournal.com
On the other hand, ultrasound guidance during GNB offers unique advantages over fluoroscopy. First, neither the patients nor clinicians are exposed to radiation dur-ing an ultrasound-guided procedure. This is deemed as the best advantage ultrasound has over fluoroscopy. Second, ultrasound can provide a real-time image of soft tissues (nerves, muscles, vessels, etc.), an image of needle tip advancement relevant to surrounding structures, and visualization of injectate spread (12). Third, it can both statically and dynamically guide diagnostic and therapeu-tic procedures. Another advantage of ultrasound-guided GNB includes the visualization of genicular arteries and even the occasional identification of genicular nerves,
Fig. 3. Proportion of successful responders in both groups at 1 and 3 months after procedure. Group U = ultrasound-guided genicular nerve block; Group F = fluoroscopy-guided genicular nerve block
Table 2. Comparison of pain intensity and functional outcomes between both groups after genicular nerve block.
Group U (n = 31) Group F (n = 30)P Value
Baseline 1 mo 3 mos Baseline 1 mo 3 mos
NRS-11 6.3 ± 1.6 3.8 ± 2.1* 4.3 ± 2.1* 6.7 ± 1.6 3.9 ± 1.9* 4.9 ± 1.9* 0.637WOMAC_Pain 10.8 ± 4.0 7.2 ± 4.0* 7.9 ± 4.2* 10.7 ± 4.5 6.9 ± 3.7* 9.3 ± 4.5 0.189WOMAC_Stiffness 4.4 ± 2.3 2.7 ± 1.7* 2.9 ± 1.8* 4.0 ± 2.3 2.8 ± 1.9* 3.5 ± 2.0 0.153WOMAC_Physical function 34.5 ± 16.6 23.3 ± 15.0* 25.0 ± 14.2* 34.3 ± 11.7 22.9 ± 11.5* 27.3 ± 13.0* 0.320WOMAC_Total 50.0 ± 20.6 34.2 ± 19.6* 35.6 ± 18.5* 48.7 ± 16.5 32.1 ± 16.0* 39.6 ± 18.1* 0.179
Data are expressed as means ± standard deviations.NRS-11, numeric rating scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. * P < .05 compared with baseline values in each group. P values comparing NRS-11 and WOMAC scores between both groups.
which may increase GNB precision. This led us to speculate that using ultrasound may be more effi-cient than using fluoroscopy when performing GNB.
The present study found no difference in efficacy between these imaging methods for GNB. Several studies have compared the effectiveness of fluoros-copy- vs ultrasound-guided blocks for chronic pain management (20-23). Consistent with our results, such studies reported no significant difference in postprocedural outcomes between the 2 modalities for an image-guided block. This similarity between both image guidance methods for GNB may be due to the anatomical properties of genicular nerves. Genicular nerves travel along each genicular artery. Such genicular neurovascular bundles extend across the junctions between the epicondyles and shafts of the femur and tibia (3,9,24). To demonstrate that GNB targets locate similarly regardless of the imaging device used, fluoroscopic images of the knee were obtained after ultrasound-guided needle insertion (Fig. 1C). The results showed that needle tips were lo-cated at the junctions between the epicondyles and shafts of the femur and tibia. Consequently, given the similarity in target positions during GNB regard-less of the imaging equipment used, we may surmise that the efficacy of both imaging devices might also be similar.
One previous report compared the efficacy of ultrasound- vs fluoroscopy-guided RFGN (25), and their results were similar to those found in this study. However, they failed to discuss why such similarity in efficacy existed between both imaging methods. As such, we believe that the current study may provide more valuable information compared to the previous study.
Considering the similar effects of both guidance modalities, we believe that ultrasound may be more
A Prospective Randomized Comparison of the Efficacy of Ultrasound- vs Fluoroscopy- Guided Genicular Nerve Block for Chronic Knee Osteoarthritis. Pain Physician 2019; 22:139-146 • ISSN 1533-3159

Innervation du genou et RF • Branches nerf fémorale
(saphene interne, vaste latérale, vaste médiale et vaste interne)
• Branches nerf sciatique (nerf géniculé supero-mediale infero-mediale supero-laterale et infero-laterale)
FIGURE 5. Distal exposure of course of superior medial genicular nerve, medial views. A, Distal VM intact. B, Distal VM reflected.*Medial epicondyle. ADM indicates adductor magnus tendon; DGA, descending genicular artery; F, femur; FA, femoral artery; GR, gracilis;NVM, nerve to vastus medialis; P, patella; RF, rectus femoris; S, sartorius; SM, semimembranosus; SMGA, superior medial genicular artery.Reprinted with permission from Philip Peng Educational Series.
FIGURE 6. Frequency map of the innervation of the anterior knee joint. A, Lateral view. B, Anterior view. C, Medial view. Reprinted withpermission from Philip Peng Educational Series.
Tran et al Regional Anesthesia and Pain Medicine • Volume 43, Number 4, May 2018
6 © 2018 American Society of Regional Anesthesia and Pain Medicine
Copyright © 2018 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.
www.painphysicianjournal.com 141
Comparison Between 2 Methods for Genicular Nerve Block
ating table with a pillow under the popliteal fossa to reduce discomfort. After sterile preparation of the op-erative field and sterile cover wrapping of the 12-MHz linear transducer (XarioTM SSA-660A; Toshiba Medical Systems Corporation, Otawara-shi, Japan), the transduc-er was first placed on the junctions between the epicon-dyles and shafts of the femur and tibia. The transducer was then moved up or down to identify the genicular arteries, which were usually near the periosteal areas as confirmed by color Doppler ultrasound. Given that the superior lateral (12), superior medial (SM), and in-ferior medial (IM) genicular arteries travel along each genicular nerve (Fig. 1B), the location of the needle tip should be within the vicinity of each genicular artery. After identifying the genicular arteries, the skin and subcutaneous tissue were anesthetized with 1 mL of 1% lidocaine at each target point. The needle was inserted using the long-axis view of the ultrasound probe. After positioning the needle tip next to a genicular artery, a gentle aspiration was performed before administering 2 mL of the same injectate mentioned above at each nerve.
Measured Variables and Follow-upAll baseline values were assessed prior to the
procedure, whereas postprocedure outcome measure-ments were evaluated after 4 and 12 weeks. Demo-graphic data for all patients were collected through standard history-taking, as well as physical and radio-logical examinations. Pain intensity was assessed us-ing the single 11-point Numeric Rating Scale (NRS-11) in which 0 = no pain and 10 = worst pain perceivable. To measure subjective knee functionality, the Western Ontario and McMaster’s Universities Osteoarthritis Index (WOMAC) was used. The WOMAC consists of 5 questions measuring pain, 2 measuring joint stiffness, and 17 measuring functional limitation, with all ques-tions scored on a scale of 0 to 4. The total scores for pain, stiffness, and physical function, which ranged from 0 to 20, 0 to 8, and 0 to 68, respectively, were then determined. Accordingly, higher scores on the WOMAC indicate worse pain, stiffness, and functional limitation (13). To obtain valid baseline values and outcome measurements, all patients were instructed on how to appropriately fill out the NRS-11 and
Fig. 1. A. Anteroposterior fluoroscopic view after needle insertion into the junction between the shaft and epicondyle of the tibia and femur. B. Ultrasound images identifying genicular arteries and nerves using color Doppler mode. White arrows indicate genicular arteries, while arrowheads indicate genicular nerves appearing as a small rounded hypoechoic dot. C. Anteroposterior and lateral fluoroscopic images after ultrasound-guided needle insertion for genicular nerve block. The location of the needle tip was similar to that in Panel A. Contrast dye spread showed that the needle tips were positioned in the periosteal area, which is the junction between the shaft and epicondyle of long bones.
Pain Physician: March/April 2019: 22:139-146
144 www.painphysicianjournal.com
On the other hand, ultrasound guidance during GNB offers unique advantages over fluoroscopy. First, neither the patients nor clinicians are exposed to radiation dur-ing an ultrasound-guided procedure. This is deemed as the best advantage ultrasound has over fluoroscopy. Second, ultrasound can provide a real-time image of soft tissues (nerves, muscles, vessels, etc.), an image of needle tip advancement relevant to surrounding structures, and visualization of injectate spread (12). Third, it can both statically and dynamically guide diagnostic and therapeu-tic procedures. Another advantage of ultrasound-guided GNB includes the visualization of genicular arteries and even the occasional identification of genicular nerves,
Fig. 3. Proportion of successful responders in both groups at 1 and 3 months after procedure. Group U = ultrasound-guided genicular nerve block; Group F = fluoroscopy-guided genicular nerve block
Table 2. Comparison of pain intensity and functional outcomes between both groups after genicular nerve block.
Group U (n = 31) Group F (n = 30)P Value
Baseline 1 mo 3 mos Baseline 1 mo 3 mos
NRS-11 6.3 ± 1.6 3.8 ± 2.1* 4.3 ± 2.1* 6.7 ± 1.6 3.9 ± 1.9* 4.9 ± 1.9* 0.637WOMAC_Pain 10.8 ± 4.0 7.2 ± 4.0* 7.9 ± 4.2* 10.7 ± 4.5 6.9 ± 3.7* 9.3 ± 4.5 0.189WOMAC_Stiffness 4.4 ± 2.3 2.7 ± 1.7* 2.9 ± 1.8* 4.0 ± 2.3 2.8 ± 1.9* 3.5 ± 2.0 0.153WOMAC_Physical function 34.5 ± 16.6 23.3 ± 15.0* 25.0 ± 14.2* 34.3 ± 11.7 22.9 ± 11.5* 27.3 ± 13.0* 0.320WOMAC_Total 50.0 ± 20.6 34.2 ± 19.6* 35.6 ± 18.5* 48.7 ± 16.5 32.1 ± 16.0* 39.6 ± 18.1* 0.179
Data are expressed as means ± standard deviations.NRS-11, numeric rating scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. * P < .05 compared with baseline values in each group. P values comparing NRS-11 and WOMAC scores between both groups.
which may increase GNB precision. This led us to speculate that using ultrasound may be more effi-cient than using fluoroscopy when performing GNB.
The present study found no difference in efficacy between these imaging methods for GNB. Several studies have compared the effectiveness of fluoros-copy- vs ultrasound-guided blocks for chronic pain management (20-23). Consistent with our results, such studies reported no significant difference in postprocedural outcomes between the 2 modalities for an image-guided block. This similarity between both image guidance methods for GNB may be due to the anatomical properties of genicular nerves. Genicular nerves travel along each genicular artery. Such genicular neurovascular bundles extend across the junctions between the epicondyles and shafts of the femur and tibia (3,9,24). To demonstrate that GNB targets locate similarly regardless of the imaging device used, fluoroscopic images of the knee were obtained after ultrasound-guided needle insertion (Fig. 1C). The results showed that needle tips were lo-cated at the junctions between the epicondyles and shafts of the femur and tibia. Consequently, given the similarity in target positions during GNB regard-less of the imaging equipment used, we may surmise that the efficacy of both imaging devices might also be similar.
One previous report compared the efficacy of ultrasound- vs fluoroscopy-guided RFGN (25), and their results were similar to those found in this study. However, they failed to discuss why such similarity in efficacy existed between both imaging methods. As such, we believe that the current study may provide more valuable information compared to the previous study.
Considering the similar effects of both guidance modalities, we believe that ultrasound may be more
A Prospective Randomized Comparison of the Efficacy of Ultrasound- vs Fluoroscopy- Guided Genicular Nerve Block for Chronic Knee Osteoarthritis. Pain Physician 2019; 22:139-146 • ISSN 1533-3159

RF sous échographie et douleurs chroniques du genou
www.painphysicianjournal.com 43
The Effect of Ultrasound-Guided Genicular Nerve Block with Adjuvant Corticosteroid
artery traveled along each genicular nerve. After using color Doppler to confirm the ge-nicular artery, the needle was inserted in the plane of the ultrasound probe in the long-axis view. After confirming the placement of the needle-tip next to a genicular artery, a gentle aspiration was performed and a 2 mL injection volume was administered. This method was used to inject a total of 6 mL of lidocaine or 6 mL of lidocaine plus 20 mg of triamcinolone (TA) at 3 separate target sites: the superior lateral, superior medial, and inferior medial genicular nerves (Table 2).
After the procedure, all of the patients were advised to continue using any previously prescribed medications when their symptoms were persisted, whereas, they were advised to stop or reduce current medication when their symptoms were alleviated. The patients were prohibited any additional medications or physiotherapy regimens at the 8-week post-procedure period.
Outcome Measurements and Follow-Up
An independent physician, who was blinded to the treatment allocations, per-formed all preoperative baseline and postpro-cedural outcome measurements (1, 2, 4, and 8 weeks) at the outpatient pain clinic. Baseline characteristics were recorded for all patients. Weight-bearing radiographs were reviewed at baseline, and the Kellgren-Lawrence system was used to grade the degree of OA. Outcome measures were assessed according to hospital visits at baseline and at 1, 2, 4, and 8 weeks after the procedure (Table 3). Before each procedure, the patients were instructed in the use of a 100 mm visual analog scale (VAS) (range: no pain to unbearable pain) and Ox-ford Knee Score (OKS, Table 3), and baseline values were obtained. OKSs were based on self-administered, joint-specific 12-item ques-tionnaires. Each question was scored from 1 to 5, with one representing either the best outcome and/or the fewest symptoms. The scores from each question were summed to yield overall scores ranging from 12–60, with 12 representing the optimal outcome (17). At 1, 2, 4, and 8 weeks after the procedure, each
Fig. 1. Ultrasound-guided identification of GNB target sites. Representative longitudinal images of the knee at the level of the distal femoral condyle and medial tibial metaphysis are shown. The superior lateral (A), superior medial (B), and inferior medial (C) genicular nerves (arrowhead) accompany each genicular artery (white arrow).
patient completed a written questionnaire that requested an estimation of these measurements. Additionally, these question-naires assessed global perceived effects on a 7-point scale (1 = worst ever, 2 = much worse, 3 = worse, 4 = not improved but not worse, 5 = improved, 6 = much improved, and 7 = best ever). To quantify changes in analgesics, the Medication Quantification Scale (MQS) was also measured (18). Pain data were expressed as absolute values.
Primary outcomes included the mean changes from base-line levels of knee pain to 1, 2, 4, and 8 weeks after GNB, as
www.painphysicianjournal.com 43
The Effect of Ultrasound-Guided Genicular Nerve Block with Adjuvant Corticosteroid
artery traveled along each genicular nerve. After using color Doppler to confirm the ge-nicular artery, the needle was inserted in the plane of the ultrasound probe in the long-axis view. After confirming the placement of the needle-tip next to a genicular artery, a gentle aspiration was performed and a 2 mL injection volume was administered. This method was used to inject a total of 6 mL of lidocaine or 6 mL of lidocaine plus 20 mg of triamcinolone (TA) at 3 separate target sites: the superior lateral, superior medial, and inferior medial genicular nerves (Table 2).
After the procedure, all of the patients were advised to continue using any previously prescribed medications when their symptoms were persisted, whereas, they were advised to stop or reduce current medication when their symptoms were alleviated. The patients were prohibited any additional medications or physiotherapy regimens at the 8-week post-procedure period.
Outcome Measurements and Follow-Up
An independent physician, who was blinded to the treatment allocations, per-formed all preoperative baseline and postpro-cedural outcome measurements (1, 2, 4, and 8 weeks) at the outpatient pain clinic. Baseline characteristics were recorded for all patients. Weight-bearing radiographs were reviewed at baseline, and the Kellgren-Lawrence system was used to grade the degree of OA. Outcome measures were assessed according to hospital visits at baseline and at 1, 2, 4, and 8 weeks after the procedure (Table 3). Before each procedure, the patients were instructed in the use of a 100 mm visual analog scale (VAS) (range: no pain to unbearable pain) and Ox-ford Knee Score (OKS, Table 3), and baseline values were obtained. OKSs were based on self-administered, joint-specific 12-item ques-tionnaires. Each question was scored from 1 to 5, with one representing either the best outcome and/or the fewest symptoms. The scores from each question were summed to yield overall scores ranging from 12–60, with 12 representing the optimal outcome (17). At 1, 2, 4, and 8 weeks after the procedure, each
Fig. 1. Ultrasound-guided identification of GNB target sites. Representative longitudinal images of the knee at the level of the distal femoral condyle and medial tibial metaphysis are shown. The superior lateral (A), superior medial (B), and inferior medial (C) genicular nerves (arrowhead) accompany each genicular artery (white arrow).
patient completed a written questionnaire that requested an estimation of these measurements. Additionally, these question-naires assessed global perceived effects on a 7-point scale (1 = worst ever, 2 = much worse, 3 = worse, 4 = not improved but not worse, 5 = improved, 6 = much improved, and 7 = best ever). To quantify changes in analgesics, the Medication Quantification Scale (MQS) was also measured (18). Pain data were expressed as absolute values.
Primary outcomes included the mean changes from base-line levels of knee pain to 1, 2, 4, and 8 weeks after GNB, as
www.painphysicianjournal.com 43
The Effect of Ultrasound-Guided Genicular Nerve Block with Adjuvant Corticosteroid
artery traveled along each genicular nerve. After using color Doppler to confirm the ge-nicular artery, the needle was inserted in the plane of the ultrasound probe in the long-axis view. After confirming the placement of the needle-tip next to a genicular artery, a gentle aspiration was performed and a 2 mL injection volume was administered. This method was used to inject a total of 6 mL of lidocaine or 6 mL of lidocaine plus 20 mg of triamcinolone (TA) at 3 separate target sites: the superior lateral, superior medial, and inferior medial genicular nerves (Table 2).
After the procedure, all of the patients were advised to continue using any previously prescribed medications when their symptoms were persisted, whereas, they were advised to stop or reduce current medication when their symptoms were alleviated. The patients were prohibited any additional medications or physiotherapy regimens at the 8-week post-procedure period.
Outcome Measurements and Follow-Up
An independent physician, who was blinded to the treatment allocations, per-formed all preoperative baseline and postpro-cedural outcome measurements (1, 2, 4, and 8 weeks) at the outpatient pain clinic. Baseline characteristics were recorded for all patients. Weight-bearing radiographs were reviewed at baseline, and the Kellgren-Lawrence system was used to grade the degree of OA. Outcome measures were assessed according to hospital visits at baseline and at 1, 2, 4, and 8 weeks after the procedure (Table 3). Before each procedure, the patients were instructed in the use of a 100 mm visual analog scale (VAS) (range: no pain to unbearable pain) and Ox-ford Knee Score (OKS, Table 3), and baseline values were obtained. OKSs were based on self-administered, joint-specific 12-item ques-tionnaires. Each question was scored from 1 to 5, with one representing either the best outcome and/or the fewest symptoms. The scores from each question were summed to yield overall scores ranging from 12–60, with 12 representing the optimal outcome (17). At 1, 2, 4, and 8 weeks after the procedure, each
Fig. 1. Ultrasound-guided identification of GNB target sites. Representative longitudinal images of the knee at the level of the distal femoral condyle and medial tibial metaphysis are shown. The superior lateral (A), superior medial (B), and inferior medial (C) genicular nerves (arrowhead) accompany each genicular artery (white arrow).
patient completed a written questionnaire that requested an estimation of these measurements. Additionally, these question-naires assessed global perceived effects on a 7-point scale (1 = worst ever, 2 = much worse, 3 = worse, 4 = not improved but not worse, 5 = improved, 6 = much improved, and 7 = best ever). To quantify changes in analgesics, the Medication Quantification Scale (MQS) was also measured (18). Pain data were expressed as absolute values.
Primary outcomes included the mean changes from base-line levels of knee pain to 1, 2, 4, and 8 weeks after GNB, as
Cómo citar este artículo: González Sotelo V, et al. Bloqueo ecoguiado de los nervios geniculados en el manejo analgésicode la artroplastia de rodilla: descripción de la técnica y resultados clínicos preliminares. Rev Esp Anestesiol Reanim. 2017.http://dx.doi.org/10.1016/j.redar.2017.04.001
ARTICLE IN PRESS+ModelREDAR-824; No. of Pages 9
4 V. González Sotelo et al.
1 2
Superomedial
Superolateral
Inferomedial
Inferolateral
3 4
Figura 1 Técnica de abordaje «fuera de plano» de los nervios geniculados en los pacientes. Imagen 1: nervio geniculado supe-romedial; imagen 2: nervio geniculado inferomedial; imagen 3: nervio geniculado superolateral; imagen 4: nervio geniculadoinferolateral.
trasladado al quirófano para realizar la ATR, bajo aneste-sia subaracnoidea a nivel L3-L4, en abordaje medial, conaguja punta de lápiz de 25-27 G. Se administraba bupiva-caína isobara al 0,5% 10-12,5 mg + fentanilo 10 !g. Duranteel intraoperatorio se realizó sedación mediante perfusióncontinua de propofol a las dosis necesarias para mantener elestado de consciencia en un nivel de Ramsay 3. Según el pro-tocolo, los pacientes recibieron paracetamol 1 g intravenosopreviamente al inicio de la isquemia y tramadol 1 mg/kg alretirar la isquemia. Tras finalizar la intervención, el pacienteera trasladado a la Unidad de Recuperación Postanestésica(URPA) hasta la reversión del bloqueo motor. Se indicó ala enfermera del área de recuperación (ciega en el trata-miento analgésico recibido) que anotara la hora de reversiónparcial del bloqueo motor (dorsiflexión del pie) y la horade reversión total (flexión de la rodilla contralateral). Seexplicaba al paciente la evaluación del dolor mediante laescala numérica (EN); una vez revertido el bloqueo motor,si el paciente refería un dolor en la EN ≥ 3, se administrabadexketoprofeno ajustado a función renal; si en la URPA eldolor en la EN era ≥ 5, el anestesiólogo realizaba un bloqueofemoral de rescate; se explicaba al paciente la evaluacióndel dolor a las 12 h del bloqueo genicular y se indicaba eluso de opioide de rescate si la EN era ≥ 5 (hidrocloruro depetidina 50 mg subcutáneo). En la habitación se continuabacon el tratamiento farmacológico establecido como proto-colo institucional (dexketoprofeno alterno con paracetamoliv/8 h). Al siguiente día se entrevistaba al paciente y se lepreguntaba acerca del descanso nocturno (bueno/malo) y lasatisfacción de la técnica (sí/no).
Se hizo una tabla de recolección de datos con las varia-bles demográficas: edad, peso, talla y sexo, también la horade inicio de la anestesia intradural, el tiempo de isque-mia, la hora de finalización de la intervención, la hora dela reversión parcial y total del bloqueo motor, la necesidadde rescate con AINE y/o bloqueo femoral por inadecuadocontrol del dolor, la valoración del dolor en la habitación alas 12 h de realizado el bloqueo de geniculados y el consumode fármacos de rescate en este periodo. Se realizó un análi-sis descriptivo de los datos. Estos se expresaron en medias ydesviación estándar, mediana y rangos, o número de pacien-tes y porcentajes, según las características de las variables.Dado el objetivo del estudio y las características de la mues-tra, no se realizaron análisis estadísticos comparativos de losdatos obtenidos.
Resultados
Estudio anatómico
El bloqueo de los nervios geniculados se realizó siguiendolas referencias óseas y/o musculares. El procedimiento eco-guiado fue realizado con abordaje fuera de plano en lapierna 1 y en plano en la pierna 2. La reconstrucción tridi-mensional de las piernas del cadáver realizada en el escánermostró a nivel de los nervios geniculados superiores una dis-tribución del volumen que se extendía en dirección cefálicay posterior (fig. 2A y B). En los geniculados inferiores la dis-tribución se mantuvo más localizada: el lado medial seguía

CRF et Douleurs chroniques du genou
• 50 patients, suivis sur 6 mois après RF
• Diminution EVA de 50% à 6 mois
• Amelioration score de qualité de vie
over time were evaluated using both classic statistical analysis andBayesian inference. P < 0.05 was considered significant. Dataanalysis was performed using Stata version 12 (StatCorp, CollegeDrive, Texas) andWinbugs version 1.4.3 (MRCBiostatistics Unit,Cambridge, United Kingdom).
RESULTSBetween December 2013 and March 2014, we enrolled 25
eligible patients for radiofrequency treatment to relieve the paincaused by chronic osteoarthritis of the knee joint. Both maleand female patients with the American Society of Anesthesiolo-gists physical status II and III suffering from intractable pain (VASscore ≥5 during > 6 months) associated with gonarthrosis grade3 to 4 according to the Kellgren-Lawrence classification (Table 1)were enrolled. Demographics and quantifiable characteristics ofthese patients are shown in Table 2. Most of them suffered fromsignificant comorbidities, that is, BMI 30 kg/m2 or greater (12/25), arterial hypertension (22/25), coronary insufficiency (7/25),and diabetes mellitus type 2 (4/25). Patients either refused surgery(17/25) or were not judged as a good candidate for knee replace-ment by the surgeon (7/25). One patient (1/25) continued suffer-ing from pain for more than 6 months after total knee replacement.Before radiofrequency therapy, patients were unsuccessfully treatedwith paracetamol (23/25), tramadol (9/25), opioids (3/25), nonste-roidal anti-inflammatory drugs (9/25), and other conservative ther-apies (5/25) including physiotherapy, articular injectionwith hyaluronicacids or steroids, or a combination of these.
Before therapy and at 1, 6, and 12 months following treat-ment, VAS, WOMACA,WOMAC B,WOMACC, andWOMAC
total scores were measured and compared (Table 3 and Figs. 3, 4).Normality (Shapiro-Wilk test) and sphericity (Mauchly test) wereconfirmed for all investigated categories. Results of repeated-measures analysis of variance, with post hoc pairwise comparisonof different levels of the investigated categories, were obtainedusing the Holm-Šídák approach to multiple comparisons and canbe found in Table 1. These outcomes are similar to those obtainedwith the Bayesian approach. On the basis of these results, the nullhypothesis, predicting no therapeutic effect at 1 year following theintervention, could be rejected.
Global evaluation of therapy consisted in assessing the pro-portion of patients with at least 50% improvement in VAS scoresin comparison to the baseline value at 1, 6, and 12 months follow-ing treatment. These values are 22/25 (88%), 16/25 (64%), and 8/25 (32%) at, respectively, 1, 6, and 12 months following interven-tion. Patient satisfaction scores at 6 months after the interventionwere poor (2/25), average (1/25), good (5/25), and very good(16/25). The outcomes of the patient, treated for persistent painfollowing total knee arthroplasty, were within the 95% confidenceinterval at 1, 6, and 12 months following treatment.
All patients were discharged within a few hours after comple-tion of the procedure. Although several patients experienced tem-porary touch pain from the radiofrequency cannula during theprocedure, the pain was tolerable and required no medication.Otherwise, no participant reported adverse events during the12 months following treatment. Most patients had rescue analge-sics for breakthrough pain in previously prescribed medication.
DISCUSSIONIn this prospective study, we found that radiofrequency
neurotomy of genicular nerves can reduce pain and disability inpatients with grade 3 to 4 gonarthrosis who did not respond toconservative treatment and who were at high risk for surgical ap-proaches, for example, because of cardiovascular comorbidity.Ultrasound-guided radiofrequency ablation of genicular nervesis a minimally invasive, cost-effective, and efficacious procedurethat can be performed in an outpatient setting without sedation.Patients can be discharged within a few hours after completionof the procedure. Analogous to radiofrequency denervation fortreatment of chronic pain from other causes, the beneficial effectof treatment started to decay after 6 months. At 1 year after the in-tervention, still 32% of patients reported at least 50% improve-ment in pretreatment VAS scores. If necessary, neurotomy canbe repeated in order to provide further relief.
TABLE 2. Demographic Data and Patient Characteristics
Patient Characteristics Median Value (Range) or Number
Age, y 75 (52–88)Male/female, n 3/22BMI, kg/m2 29 (23–38)ASA class (II/III) 20/5Severity of arthrosis (grade 3/4) 9/16
Severity of gonarthrosis graded according to the Kellgren-Lawrence scale.ASA indicates American Society of Anesthesiologists physical status
classification.
TABLE 3. Results of the Statistical Analysis
ParameterScore BeforeTreatment
Score at 1 mo FollowingTreatment
Score at 6 mo FollowingTreatment
Score at 12 mo FollowingTreatment
VAS 8.5 (8.2–8.8)* 2.5 (1.8–3.3)† 3.9 (3.1–4.9)‡ 5.8 (3.7–7.8)WOMAC A 14.0 (13.2–14.8)* 5.2 (3.9–6.6)† 6.4 (4.8–8.1)‡ 8.4 (6.4–10.4)WOMAC B 3.8 (3.1–4.3) 3.2 (2.8–3.7) 3.3 (2.8–3.8) 3.5 (2.9–4.0)WOMAC C 47.3 (44.9–49.8)* 31.4 (27.0–35.9)† 32.8 (27.8–37.8) 36.3 (31.8–40.8)WOMACTotal
65.2 (61.8–68.5)* 39.5 (33.5–45.6)† 40.7 (32.6–48.9)‡ 49.2 (38.5–60.0)
Results of the repeated-measures analysis of variance of the investigated categories, that is, VAS and WOMAC A, B, C, and total. Post hoc pairwisecomparison of different levels of the investigated categories was done using the Holm-Šídák approach to multiple comparisons Values are mean (95% con-fidence interval).
*Significantly different from the scores at 1, 6, and 12 months following treatment (P < 0.001).†Significantly different from the score at 12 months following treatment (P < 0.01).‡Significantly different from the score at 12 months following treatment (P < 0.01).
Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 Genicular Nerve Block for Gonarthrosis
© 2016 American Society of Regional Anesthesia and Pain Medicine 65
Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.
allowed to continue preintervention analgesic therapy followingthe treatment (real or sham). This might have represented a con-founding factor distorting the outcomes.
The purpose of our study was to reproduce radiofrequencygenicular neurotomy as described by Choi et al. This was doneto evaluate its long-term efficacy in reducing pain and incapacityassociated with advanced osteoarthritis of the knee. Our null hy-pothesis was that no significant difference would exist betweenscores for perceived pain and disability before treatment and at1 year following the intervention.
METHODS
Participant RecruitmentIn this single-center, prospective, observational, noncontrolled,
longitudinal trial, patients suffering from pain caused by osteoarthritisof the knee joint were considered to receive percutaneous radio-frequency denervation of genicular nerves. The research projectwas approved by the research ethics committee of the RegionalHealth Area of Cádiz, Spain, on November 11, 2013, and was reg-istered in ClinicalTrials.gov (NCT02688543). Written informedconsent was obtained from all participants.
Eligible patients suffered fromchronic pain (during>6months)of moderate to severe intensity (scoring ≥5 on a 0- to 10-pointcontinuous visual analog scale [VAS] ranging from none [0] toan extreme amount of pain [10]) due to advanced osteoarthritisof the knee (grades 3-4 according to the Kellgren-Lawrence clas-sification; Table 1). The pain proved to be resistant to conservativetreatments including physiotherapy, oral analgesics, and intra-articular injection with hyaluronic acids or steroids. In this study,genicular nerve ablation was applied as an alternative analgesicapproach for those who refused knee arthroplasty; were judgedby their surgeons as being inappropriate for surgical treatment,for example, because of cardiovascular or other comorbidities;or who had to be managed for persistent pain and stiffness aftertotal knee arthroplasty.
The exclusion criteria included knee-pain related disordersthatmight benefit fromother interventions, for example, patellofemoraldisorders, meniscal injuries, ligamentous laxity, and so on, acuteknee pain associated with radicular neuropathy or intermittentclaudication, connective tissue diseases, serious neurologic or
psychiatric disorders, mental deterioration impeding adequatecommunication or collaboration, anticoagulant medications, pace-makers, prior electroacupuncture treatment, and injection withsteroids or hyaluronic acids during the previous 3 months.
Anatomy of Genicular NervesThe afferent nerves supplying the knee joint can schemati-
cally be divided into a posterior and anterior group of innerva-tion.12,13 The posterior group originates from the sciatic nerve,mainly through its tibial branch, and in a variable amount of casesthrough contributions from the obturator nerve. The anterior groupsupplying the anteromedial and anterolateral capsule and associ-ated ligaments includes articular branches of the femoral (throughbranches to vastus medialis, vastus lateralis, and vastus intermediusmuscles), the common peroneal, and the saphenous nerves.
Literature review revealed a lack of agreement on the numberand origin of nerve branches supplying the anterior knee capsule.12–17
Recent investigation, however, allowed to establish definite pat-terns of innervation.11 The following 6 nerves could be demon-strated in all dissected specimens: the superolateral branch originatingfrom the innervation to vastus lateralis, the superomedial branchoriginating from the innervation to vastus medialis, the middlebranch originating from the innervation to the vastus intermedius,the inferolateral (recurrent) branch from the common peronealnerve, the inferomedial branch from the saphenous nerve, and alateral retinacular nerve branch from the common peroneal nerve.Furthermore, knee branches, that is, both nerves or vessels, are re-ferred to as “genicular” branches.
These genicular nerve endings showed variable proximal tra-jectories but consistent distal points of contact with femur andtibia. The fairly stable anatomical basis makes at least 3 of them,that is, the superior lateral, the superior medial, and the inferiormedial genicular nerves, accessible to percutaneous ablation.
ProcedureThe technique was performed in an outpatient setting, under
aseptic conditions, with basic monitoring (pulse oximetry and
TABLE 1. Radiological Assessment of the Severity of Osteoarthritisof the Knee
Grade Severity Radiological Features
0 None Absence of radiographic changesof osteoarthritis
1 Doubtful Possible osteophytic lipping, doubtfulnarrowing of joint space
2 Minimal Definitive osteophytes, possible jointspace narrowing on anteroposteriorweight-bearing radiograph
3 Moderate Multiple moderate-size osteophytes,definitive narrowing of joint space
4 Severe Large-size osteophytes, marked narrowingof joint space, severe sclerosis, anddeformity of bone contour
The Kellgren-Lawrence system is a method of classifying the severityof osteoarthritis using 5 grades.
Adapted from Kellgren JH, Lawrence JS. Radiological assessment ofosteo-arthrosis. Ann Rheum Dis. 1957;16:494–502.
FIGURE 1. Fluoroscopic image of anteroposterior view of the leftknee joint. Radiofrequency electrode tips were placed onperiosteal areas connecting the shaft of the femur to bilateralepicondyles and the shaft of the tibia to itsmedial epicondyle. Thesuperior medial (SM), superior lateral (SL), and inferior medial (IM)genicular nerves run down these areas.
Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 Genicular Nerve Block for Gonarthrosis
© 2016 American Society of Regional Anesthesia and Pain Medicine 63
Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.

• Diminution EVA de 50% à 6 mois
• Amelioration scores de qualité de vie
over time were evaluated using both classic statistical analysis andBayesian inference. P < 0.05 was considered significant. Dataanalysis was performed using Stata version 12 (StatCorp, CollegeDrive, Texas) andWinbugs version 1.4.3 (MRCBiostatistics Unit,Cambridge, United Kingdom).
RESULTSBetween December 2013 and March 2014, we enrolled 25
eligible patients for radiofrequency treatment to relieve the paincaused by chronic osteoarthritis of the knee joint. Both maleand female patients with the American Society of Anesthesiolo-gists physical status II and III suffering from intractable pain (VASscore ≥5 during > 6 months) associated with gonarthrosis grade3 to 4 according to the Kellgren-Lawrence classification (Table 1)were enrolled. Demographics and quantifiable characteristics ofthese patients are shown in Table 2. Most of them suffered fromsignificant comorbidities, that is, BMI 30 kg/m2 or greater (12/25), arterial hypertension (22/25), coronary insufficiency (7/25),and diabetes mellitus type 2 (4/25). Patients either refused surgery(17/25) or were not judged as a good candidate for knee replace-ment by the surgeon (7/25). One patient (1/25) continued suffer-ing from pain for more than 6 months after total knee replacement.Before radiofrequency therapy, patients were unsuccessfully treatedwith paracetamol (23/25), tramadol (9/25), opioids (3/25), nonste-roidal anti-inflammatory drugs (9/25), and other conservative ther-apies (5/25) including physiotherapy, articular injectionwith hyaluronicacids or steroids, or a combination of these.
Before therapy and at 1, 6, and 12 months following treat-ment, VAS, WOMACA,WOMAC B,WOMACC, andWOMAC
total scores were measured and compared (Table 3 and Figs. 3, 4).Normality (Shapiro-Wilk test) and sphericity (Mauchly test) wereconfirmed for all investigated categories. Results of repeated-measures analysis of variance, with post hoc pairwise comparisonof different levels of the investigated categories, were obtainedusing the Holm-Šídák approach to multiple comparisons and canbe found in Table 1. These outcomes are similar to those obtainedwith the Bayesian approach. On the basis of these results, the nullhypothesis, predicting no therapeutic effect at 1 year following theintervention, could be rejected.
Global evaluation of therapy consisted in assessing the pro-portion of patients with at least 50% improvement in VAS scoresin comparison to the baseline value at 1, 6, and 12 months follow-ing treatment. These values are 22/25 (88%), 16/25 (64%), and 8/25 (32%) at, respectively, 1, 6, and 12 months following interven-tion. Patient satisfaction scores at 6 months after the interventionwere poor (2/25), average (1/25), good (5/25), and very good(16/25). The outcomes of the patient, treated for persistent painfollowing total knee arthroplasty, were within the 95% confidenceinterval at 1, 6, and 12 months following treatment.
All patients were discharged within a few hours after comple-tion of the procedure. Although several patients experienced tem-porary touch pain from the radiofrequency cannula during theprocedure, the pain was tolerable and required no medication.Otherwise, no participant reported adverse events during the12 months following treatment. Most patients had rescue analge-sics for breakthrough pain in previously prescribed medication.
DISCUSSIONIn this prospective study, we found that radiofrequency
neurotomy of genicular nerves can reduce pain and disability inpatients with grade 3 to 4 gonarthrosis who did not respond toconservative treatment and who were at high risk for surgical ap-proaches, for example, because of cardiovascular comorbidity.Ultrasound-guided radiofrequency ablation of genicular nervesis a minimally invasive, cost-effective, and efficacious procedurethat can be performed in an outpatient setting without sedation.Patients can be discharged within a few hours after completionof the procedure. Analogous to radiofrequency denervation fortreatment of chronic pain from other causes, the beneficial effectof treatment started to decay after 6 months. At 1 year after the in-tervention, still 32% of patients reported at least 50% improve-ment in pretreatment VAS scores. If necessary, neurotomy canbe repeated in order to provide further relief.
TABLE 2. Demographic Data and Patient Characteristics
Patient Characteristics Median Value (Range) or Number
Age, y 75 (52–88)Male/female, n 3/22BMI, kg/m2 29 (23–38)ASA class (II/III) 20/5Severity of arthrosis (grade 3/4) 9/16
Severity of gonarthrosis graded according to the Kellgren-Lawrence scale.ASA indicates American Society of Anesthesiologists physical status
classification.
TABLE 3. Results of the Statistical Analysis
ParameterScore BeforeTreatment
Score at 1 mo FollowingTreatment
Score at 6 mo FollowingTreatment
Score at 12 mo FollowingTreatment
VAS 8.5 (8.2–8.8)* 2.5 (1.8–3.3)† 3.9 (3.1–4.9)‡ 5.8 (3.7–7.8)WOMAC A 14.0 (13.2–14.8)* 5.2 (3.9–6.6)† 6.4 (4.8–8.1)‡ 8.4 (6.4–10.4)WOMAC B 3.8 (3.1–4.3) 3.2 (2.8–3.7) 3.3 (2.8–3.8) 3.5 (2.9–4.0)WOMAC C 47.3 (44.9–49.8)* 31.4 (27.0–35.9)† 32.8 (27.8–37.8) 36.3 (31.8–40.8)WOMACTotal
65.2 (61.8–68.5)* 39.5 (33.5–45.6)† 40.7 (32.6–48.9)‡ 49.2 (38.5–60.0)
Results of the repeated-measures analysis of variance of the investigated categories, that is, VAS and WOMAC A, B, C, and total. Post hoc pairwisecomparison of different levels of the investigated categories was done using the Holm-Šídák approach to multiple comparisons Values are mean (95% con-fidence interval).
*Significantly different from the scores at 1, 6, and 12 months following treatment (P < 0.001).†Significantly different from the score at 12 months following treatment (P < 0.01).‡Significantly different from the score at 12 months following treatment (P < 0.01).
Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 Genicular Nerve Block for Gonarthrosis
© 2016 American Society of Regional Anesthesia and Pain Medicine 65
Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.
allowed to continue preintervention analgesic therapy followingthe treatment (real or sham). This might have represented a con-founding factor distorting the outcomes.
The purpose of our study was to reproduce radiofrequencygenicular neurotomy as described by Choi et al. This was doneto evaluate its long-term efficacy in reducing pain and incapacityassociated with advanced osteoarthritis of the knee. Our null hy-pothesis was that no significant difference would exist betweenscores for perceived pain and disability before treatment and at1 year following the intervention.
METHODS
Participant RecruitmentIn this single-center, prospective, observational, noncontrolled,
longitudinal trial, patients suffering from pain caused by osteoarthritisof the knee joint were considered to receive percutaneous radio-frequency denervation of genicular nerves. The research projectwas approved by the research ethics committee of the RegionalHealth Area of Cádiz, Spain, on November 11, 2013, and was reg-istered in ClinicalTrials.gov (NCT02688543). Written informedconsent was obtained from all participants.
Eligible patients suffered fromchronic pain (during>6months)of moderate to severe intensity (scoring ≥5 on a 0- to 10-pointcontinuous visual analog scale [VAS] ranging from none [0] toan extreme amount of pain [10]) due to advanced osteoarthritisof the knee (grades 3-4 according to the Kellgren-Lawrence clas-sification; Table 1). The pain proved to be resistant to conservativetreatments including physiotherapy, oral analgesics, and intra-articular injection with hyaluronic acids or steroids. In this study,genicular nerve ablation was applied as an alternative analgesicapproach for those who refused knee arthroplasty; were judgedby their surgeons as being inappropriate for surgical treatment,for example, because of cardiovascular or other comorbidities;or who had to be managed for persistent pain and stiffness aftertotal knee arthroplasty.
The exclusion criteria included knee-pain related disordersthatmight benefit fromother interventions, for example, patellofemoraldisorders, meniscal injuries, ligamentous laxity, and so on, acuteknee pain associated with radicular neuropathy or intermittentclaudication, connective tissue diseases, serious neurologic or
psychiatric disorders, mental deterioration impeding adequatecommunication or collaboration, anticoagulant medications, pace-makers, prior electroacupuncture treatment, and injection withsteroids or hyaluronic acids during the previous 3 months.
Anatomy of Genicular NervesThe afferent nerves supplying the knee joint can schemati-
cally be divided into a posterior and anterior group of innerva-tion.12,13 The posterior group originates from the sciatic nerve,mainly through its tibial branch, and in a variable amount of casesthrough contributions from the obturator nerve. The anterior groupsupplying the anteromedial and anterolateral capsule and associ-ated ligaments includes articular branches of the femoral (throughbranches to vastus medialis, vastus lateralis, and vastus intermediusmuscles), the common peroneal, and the saphenous nerves.
Literature review revealed a lack of agreement on the numberand origin of nerve branches supplying the anterior knee capsule.12–17
Recent investigation, however, allowed to establish definite pat-terns of innervation.11 The following 6 nerves could be demon-strated in all dissected specimens: the superolateral branch originatingfrom the innervation to vastus lateralis, the superomedial branchoriginating from the innervation to vastus medialis, the middlebranch originating from the innervation to the vastus intermedius,the inferolateral (recurrent) branch from the common peronealnerve, the inferomedial branch from the saphenous nerve, and alateral retinacular nerve branch from the common peroneal nerve.Furthermore, knee branches, that is, both nerves or vessels, are re-ferred to as “genicular” branches.
These genicular nerve endings showed variable proximal tra-jectories but consistent distal points of contact with femur andtibia. The fairly stable anatomical basis makes at least 3 of them,that is, the superior lateral, the superior medial, and the inferiormedial genicular nerves, accessible to percutaneous ablation.
ProcedureThe technique was performed in an outpatient setting, under
aseptic conditions, with basic monitoring (pulse oximetry and
TABLE 1. Radiological Assessment of the Severity of Osteoarthritisof the Knee
Grade Severity Radiological Features
0 None Absence of radiographic changesof osteoarthritis
1 Doubtful Possible osteophytic lipping, doubtfulnarrowing of joint space
2 Minimal Definitive osteophytes, possible jointspace narrowing on anteroposteriorweight-bearing radiograph
3 Moderate Multiple moderate-size osteophytes,definitive narrowing of joint space
4 Severe Large-size osteophytes, marked narrowingof joint space, severe sclerosis, anddeformity of bone contour
The Kellgren-Lawrence system is a method of classifying the severityof osteoarthritis using 5 grades.
Adapted from Kellgren JH, Lawrence JS. Radiological assessment ofosteo-arthrosis. Ann Rheum Dis. 1957;16:494–502.
FIGURE 1. Fluoroscopic image of anteroposterior view of the leftknee joint. Radiofrequency electrode tips were placed onperiosteal areas connecting the shaft of the femur to bilateralepicondyles and the shaft of the tibia to itsmedial epicondyle. Thesuperior medial (SM), superior lateral (SL), and inferior medial (IM)genicular nerves run down these areas.
Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 Genicular Nerve Block for Gonarthrosis
© 2016 American Society of Regional Anesthesia and Pain Medicine 63
Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.
CRF et Douleurs chroniques du genou

CLRF Vs IAS Douleurs chroniques du genou
• 151 patients inclus dont 76 groupe CLRF
• Gonalgie évoluant depuis plus de 10 ans
• score arthrose radiographique modéré à sévère
• Diminution EVA à 1, 3 et 6 mois groupe CLRF vs groupe IAS
Seventy-four percent (43/58) (95% CI, 62.9–85.4) of theCRFA group and 16% (11/68) (95% CI, 7.4–24.9) of the IASgroup met successful outcome criteria (≥50% reduction in NRSscore) at 6 months (P < 0.0001, χ2 test), whereas 25.9% (15/58)and 83.8% (57/68) of these study cohorts, respectively, were non-responders. None of the subjects in the CRFA group reportedworse pain at 6 months, whereas 15% (10/68) of the IAS cohortexperienced exacerbation of usual knee pain during the follow-up period (P < 0.0024, χ2 test). Twenty-two percent (13/58)(95% CI, 11.4–33.5) of the CRFA group and 4% (3/68) (95%CI, 0–9.4) of the IAS group reported “no pain” (100% reduction)6 months after treatment (P < 0.0026, χ2 test). In the CRFAgroup, 6.9% (4/58) of the population had no change in usual painfollowing the 6-month time point compared with 23.5% (16/68)of the IAS group (Fig. 4).
Oxford Knee Score
The mean OKS in each study cohort was equivalent at base-line (Table 2). MeanOKSs improved at all end points within bothstudy groups (P < 0.0001 at each data point, paired Student t test)relative to baseline scores. The mean OKSs were greater in theCRFA group than in the IAS group at 1, 3, and 6 months(Table 2). Increasingly higher OKSs in the CRFA group werenoted over the course of the 6-month time frame, whereasscores in the IAS group exhibited an opposite trend from 1 to6 months. Index knee function improved in the CRFA group,whereas it declined in the IAS group from 1 to 6 monthsafter treatment.
Interestingly, while the number of subjects in each studygroup considered to have “severe (knee) arthritis” symptoms werenot different at baseline, beginning at 1 month, more subjects inthe CRFA group than in the IAS group had “satisfactory jointfunction,” and at 3 and 6 months, more subjects in the CRFAhad “mild to moderate arthritis” or “satisfactory joint function”than in the IAS group. These latter OKS classifications were notapplicable to any study subjects at baseline (Table 3).
Global Perceived Effect
At 1 month, there was no difference (P = 0.1, χ2 test) in theproportions of subjects who reported perceived improvement as aconsequence of treatment for chronic knee pain between theCRFA (79% [53/67]; 95% CI, 69.1–89.1) and IAS (67% [46/69]; 95% CI, 55.3–78.1) groups. In contrast, at the 3-month timepoint, a higher proportion of the CRFA group reported improve-ment (80% [52/65]; 95% CI, 70.0–90.0) compared with the IASgroup (31% [21/68]; 95% CI, 19.6–42.1) (P < 0.0001). At6 months, 91% (53/58) (95% CI, 83.9–98.8) of the CRFA cohortversus 24% (16/67) (95% CI, 13.4–34.4) of the IAS group(P < 0.0001) reported improved global perceived effect.
FIGURE 3. Numeric Rating Scale—mean usual knee pain. MeanCRFA and IAS study group NRS scores are indicated by bars, andSDs are expressed as whiskers. *P < 0.05 and **P < 0.0001(Wilcoxon rank sum test) versus IAS means at same time points.
FIGURE 4. Numeric Rating Scale—changes in usual knee pain at 6 months. Changes in CRFA (A) and IAS (B) study group NRS scores frombaseline at 6 months are indicated by the horizontal black bars. The treatment “responder” qualification required an NRS score decreasefrom baseline of 50% or greater.
Davis et al Regional Anesthesia and Pain Medicine • Volume 43, Number 1, January 2018
88 © 2017 American Society of Regional Anesthesia and Pain Medicine
Prospective, Multicenter, Randomized, Crossover Clinical Trial Comparing the Safety and Effectiveness of Cooled Radiofrequency Ablation With Corticosteroid Injection in the Management of Knee Pain From Osteoarthritis. Reg Anesth Pain Med 2018;43: 84–91

• CLRF: 70% patients ont un benefice analgésique de plus de 50%.
• IAS: 16% patients ont un benefice analgésique de plus de 50%. 35% aucun benefice voir une aggravation de la douleur
Seventy-four percent (43/58) (95% CI, 62.9–85.4) of theCRFA group and 16% (11/68) (95% CI, 7.4–24.9) of the IASgroup met successful outcome criteria (≥50% reduction in NRSscore) at 6 months (P < 0.0001, χ2 test), whereas 25.9% (15/58)and 83.8% (57/68) of these study cohorts, respectively, were non-responders. None of the subjects in the CRFA group reportedworse pain at 6 months, whereas 15% (10/68) of the IAS cohortexperienced exacerbation of usual knee pain during the follow-up period (P < 0.0024, χ2 test). Twenty-two percent (13/58)(95% CI, 11.4–33.5) of the CRFA group and 4% (3/68) (95%CI, 0–9.4) of the IAS group reported “no pain” (100% reduction)6 months after treatment (P < 0.0026, χ2 test). In the CRFAgroup, 6.9% (4/58) of the population had no change in usual painfollowing the 6-month time point compared with 23.5% (16/68)of the IAS group (Fig. 4).
Oxford Knee Score
The mean OKS in each study cohort was equivalent at base-line (Table 2). MeanOKSs improved at all end points within bothstudy groups (P < 0.0001 at each data point, paired Student t test)relative to baseline scores. The mean OKSs were greater in theCRFA group than in the IAS group at 1, 3, and 6 months(Table 2). Increasingly higher OKSs in the CRFA group werenoted over the course of the 6-month time frame, whereasscores in the IAS group exhibited an opposite trend from 1 to6 months. Index knee function improved in the CRFA group,whereas it declined in the IAS group from 1 to 6 monthsafter treatment.
Interestingly, while the number of subjects in each studygroup considered to have “severe (knee) arthritis” symptoms werenot different at baseline, beginning at 1 month, more subjects inthe CRFA group than in the IAS group had “satisfactory jointfunction,” and at 3 and 6 months, more subjects in the CRFAhad “mild to moderate arthritis” or “satisfactory joint function”than in the IAS group. These latter OKS classifications were notapplicable to any study subjects at baseline (Table 3).
Global Perceived Effect
At 1 month, there was no difference (P = 0.1, χ2 test) in theproportions of subjects who reported perceived improvement as aconsequence of treatment for chronic knee pain between theCRFA (79% [53/67]; 95% CI, 69.1–89.1) and IAS (67% [46/69]; 95% CI, 55.3–78.1) groups. In contrast, at the 3-month timepoint, a higher proportion of the CRFA group reported improve-ment (80% [52/65]; 95% CI, 70.0–90.0) compared with the IASgroup (31% [21/68]; 95% CI, 19.6–42.1) (P < 0.0001). At6 months, 91% (53/58) (95% CI, 83.9–98.8) of the CRFA cohortversus 24% (16/67) (95% CI, 13.4–34.4) of the IAS group(P < 0.0001) reported improved global perceived effect.
FIGURE 3. Numeric Rating Scale—mean usual knee pain. MeanCRFA and IAS study group NRS scores are indicated by bars, andSDs are expressed as whiskers. *P < 0.05 and **P < 0.0001(Wilcoxon rank sum test) versus IAS means at same time points.
FIGURE 4. Numeric Rating Scale—changes in usual knee pain at 6 months. Changes in CRFA (A) and IAS (B) study group NRS scores frombaseline at 6 months are indicated by the horizontal black bars. The treatment “responder” qualification required an NRS score decreasefrom baseline of 50% or greater.
Davis et al Regional Anesthesia and Pain Medicine • Volume 43, Number 1, January 2018
88 © 2017 American Society of Regional Anesthesia and Pain MedicineProspective, Multicenter, Randomized, Crossover Clinical Trial Comparing the Safety and Effectiveness of Cooled Radiofrequency Ablation With Corticosteroid Injection in the Management of Knee Pain From Osteoarthritis. Reg Anesth Pain Med 2018;43: 84–91
CLRF Vs IAS Douleurs chroniques du genou

• CLRF: 70% patients ont un benefice analgésique de plus de 50%.
• IAS: 16% patients ont un benefice analgésique de plus de 50%. 35% aucun benefice voir une aggravation de la douleur
Seventy-four percent (43/58) (95% CI, 62.9–85.4) of theCRFA group and 16% (11/68) (95% CI, 7.4–24.9) of the IASgroup met successful outcome criteria (≥50% reduction in NRSscore) at 6 months (P < 0.0001, χ2 test), whereas 25.9% (15/58)and 83.8% (57/68) of these study cohorts, respectively, were non-responders. None of the subjects in the CRFA group reportedworse pain at 6 months, whereas 15% (10/68) of the IAS cohortexperienced exacerbation of usual knee pain during the follow-up period (P < 0.0024, χ2 test). Twenty-two percent (13/58)(95% CI, 11.4–33.5) of the CRFA group and 4% (3/68) (95%CI, 0–9.4) of the IAS group reported “no pain” (100% reduction)6 months after treatment (P < 0.0026, χ2 test). In the CRFAgroup, 6.9% (4/58) of the population had no change in usual painfollowing the 6-month time point compared with 23.5% (16/68)of the IAS group (Fig. 4).
Oxford Knee Score
The mean OKS in each study cohort was equivalent at base-line (Table 2). MeanOKSs improved at all end points within bothstudy groups (P < 0.0001 at each data point, paired Student t test)relative to baseline scores. The mean OKSs were greater in theCRFA group than in the IAS group at 1, 3, and 6 months(Table 2). Increasingly higher OKSs in the CRFA group werenoted over the course of the 6-month time frame, whereasscores in the IAS group exhibited an opposite trend from 1 to6 months. Index knee function improved in the CRFA group,whereas it declined in the IAS group from 1 to 6 monthsafter treatment.
Interestingly, while the number of subjects in each studygroup considered to have “severe (knee) arthritis” symptoms werenot different at baseline, beginning at 1 month, more subjects inthe CRFA group than in the IAS group had “satisfactory jointfunction,” and at 3 and 6 months, more subjects in the CRFAhad “mild to moderate arthritis” or “satisfactory joint function”than in the IAS group. These latter OKS classifications were notapplicable to any study subjects at baseline (Table 3).
Global Perceived Effect
At 1 month, there was no difference (P = 0.1, χ2 test) in theproportions of subjects who reported perceived improvement as aconsequence of treatment for chronic knee pain between theCRFA (79% [53/67]; 95% CI, 69.1–89.1) and IAS (67% [46/69]; 95% CI, 55.3–78.1) groups. In contrast, at the 3-month timepoint, a higher proportion of the CRFA group reported improve-ment (80% [52/65]; 95% CI, 70.0–90.0) compared with the IASgroup (31% [21/68]; 95% CI, 19.6–42.1) (P < 0.0001). At6 months, 91% (53/58) (95% CI, 83.9–98.8) of the CRFA cohortversus 24% (16/67) (95% CI, 13.4–34.4) of the IAS group(P < 0.0001) reported improved global perceived effect.
FIGURE 3. Numeric Rating Scale—mean usual knee pain. MeanCRFA and IAS study group NRS scores are indicated by bars, andSDs are expressed as whiskers. *P < 0.05 and **P < 0.0001(Wilcoxon rank sum test) versus IAS means at same time points.
FIGURE 4. Numeric Rating Scale—changes in usual knee pain at 6 months. Changes in CRFA (A) and IAS (B) study group NRS scores frombaseline at 6 months are indicated by the horizontal black bars. The treatment “responder” qualification required an NRS score decreasefrom baseline of 50% or greater.
Davis et al Regional Anesthesia and Pain Medicine • Volume 43, Number 1, January 2018
88 © 2017 American Society of Regional Anesthesia and Pain Medicine
CLRF Vs IAS Gonalgie
Prospective, Multicenter, Randomized, Crossover Clinical Trial Comparing the Safety and Effectiveness of Cooled Radiofrequency Ablation With Corticosteroid Injection in the Management of Knee Pain From Osteoarthritis. Reg Anesth Pain Med 2018;43: 84–91

EPAULE et RF
Capsulite retractile Arthrose SDRC postopératoire

Innervation de l’épaule
Acromioclavicular jointVangsness et al52 noted the presence of mechanoreceptorsin the acromioclavicular joint; however, no paperstudying acromioclavicular joint nociceptors could beidentified.
Nerves and articular branches
The articular nerve branches innervating the shoulder jointwere found to arise from the suprascapular (SSN), LPN,lower subscapular (LSN), radial, and axillary (AN) nerves(Fig. 2; Table I).
Suprascapular nerveGardner16 described a lateral AB of the SSN in 1948, whichprovided innervation to the coracoclavicular ligaments andterminated its course in the superior aspect of the GHcapsule. Aszmann and Dellon4 described this branch as amedial AB innervating the coracoclavicular and cor-acohumeral ligaments and SAB. They also identified distaland lateral ABs terminating within the posterior jointcapsule. Vorster et al54 provided data to support this medialAB course and described the course of a new branch,splitting off from the parent nerve just proximal to thescapular neck and running on the scapula deep to thesupraspinatus before entering the infraspinatus near itstendon. Ebraheim et al13 confirmed that the medial ABturns laterally along the base of the coracoid process andterminated in the acromioclavicular joint and SAB. They
also described a second branch running laterally proximalto the infraspinous fossa and entering the posterior aspectof the capsule deep to the infraspinatus. Eckmann et al14
classified ABs with respect to the spinoglenoid notch (su-perior and inferior). These ABs were reported to courselaterally in the supraspinous (superior branch) and infra-spinous (inferior branch) fossae of the scapula to innervatethe posterior GH capsule, SAB, and posterior fascia of thehead and neck of the humerus. The authors did not describea discrete anatomic area of innervation in their paper.14 In2019, Laumonerie et al31 described a lateral subacromialbranch, which arose from the SSN distal to the supra-scapular notch and terminated over the supraspinatusmuscle in the medial portion of the SAB and the acromialinsertion of the acromioclavicular ligament. This studyelucidated previously undescribed anatomy of the SSN andits 3 distinct AB courses: 2 subacromial branches (medialand lateral) and 1 posterior GH branch to the shoulder joint.This arrangement, allowing for bipolar innervation of theSAB, was consistent with the bipolar distribution of thenociceptors in the medial and lateral part of the SABdescribed by Ide et al.24
Axillary nerveGardner16 initially described the ABs as arising from 3sites: the main trunk, as well as the anterior and posteriordivisions. After the AN entered the quadrangular space, 1or 2 ABs take off from the main trunk. These ABs traveledwith the anterior circumflex humeral artery and coursed
Figure 2 Schematic diagram of sensory innervation of the shoulder joint. (A) Anterior view; (B) posterior view.
e502 P. Laumonerie et al.
Sensory innervation of the human shoulder joint: the three bridges to break. P Laumonerie. J Shoulder Elbow Surg (2020) 29, e499–e507

Branche coracoidienne du nerf pectoral

Branche coracoidienne du nerf pectoral

Nerf Axillaire
assessment with US while maintaining the tip perpendic-ular to the nerve, thus allowing an optimal field of lesionfor the PRF. Furthermore, we target the nerve lateral tothe quadrangular space, thus benefitting from the hu-merus as an anterior border protecting from unwantedanterior needle penetration.
Although the only previous report we found of a PRFon both the SSN and AN for chronic pain treatment usedthree cycles of PRF of two minutes’ duration, we optedfor a single cycle. The optimal settings of PRF are still amatter of debate and are beyond the scope of this
technical report. We chose to use a safer stimulation mo-dality as repetitive PRF cycles could lead to a surge in tiptemperature that could produce ablative thermocoagula-tion on nervous fibers.
Simultaneous pulsed radiofrequency on the suprascap-ular and axillary nerves for the treatment of the chroniccondition of the painful shoulder has been scarcely stud-ied, with very few references in the literature. The ulti-mate efficacy of this combined technique has to beconfirmed or disproved by future trials. We are currentlyconducting a randomized controlled study to investigate
Figure 2. Position of the patient and ultrasound transducer for the realization of the suprascapular nerve block and its correlationwith the ultrasound image. PCHA ¼ posterior circumflex humeral artery.
Figure 1. Position of the patient and ultrasound transducer for the realization of the suprascapular nerve block and its correlationwith the ultrasound image.
Suprascapular, Axillary, US-Guided, Pulsed Radiofrequency 3
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/advance-article-abstract/doi/10.1093/pm/pny311/5301761 by EKU
Libraries user on 26 January 2019
Gofeld M, Restrepo-garces CE, Theodore R, Faclier G. Pulsed radiofrequency of suprascapular nerve for chronic shoulder pain: A randomized double-blind ac- tive placebo-controlled study. Pain Pract 2013;13 (2):96–103.

Innervation de l’épaule
Acromioclavicular jointVangsness et al52 noted the presence of mechanoreceptorsin the acromioclavicular joint; however, no paperstudying acromioclavicular joint nociceptors could beidentified.
Nerves and articular branches
The articular nerve branches innervating the shoulder jointwere found to arise from the suprascapular (SSN), LPN,lower subscapular (LSN), radial, and axillary (AN) nerves(Fig. 2; Table I).
Suprascapular nerveGardner16 described a lateral AB of the SSN in 1948, whichprovided innervation to the coracoclavicular ligaments andterminated its course in the superior aspect of the GHcapsule. Aszmann and Dellon4 described this branch as amedial AB innervating the coracoclavicular and cor-acohumeral ligaments and SAB. They also identified distaland lateral ABs terminating within the posterior jointcapsule. Vorster et al54 provided data to support this medialAB course and described the course of a new branch,splitting off from the parent nerve just proximal to thescapular neck and running on the scapula deep to thesupraspinatus before entering the infraspinatus near itstendon. Ebraheim et al13 confirmed that the medial ABturns laterally along the base of the coracoid process andterminated in the acromioclavicular joint and SAB. They
also described a second branch running laterally proximalto the infraspinous fossa and entering the posterior aspectof the capsule deep to the infraspinatus. Eckmann et al14
classified ABs with respect to the spinoglenoid notch (su-perior and inferior). These ABs were reported to courselaterally in the supraspinous (superior branch) and infra-spinous (inferior branch) fossae of the scapula to innervatethe posterior GH capsule, SAB, and posterior fascia of thehead and neck of the humerus. The authors did not describea discrete anatomic area of innervation in their paper.14 In2019, Laumonerie et al31 described a lateral subacromialbranch, which arose from the SSN distal to the supra-scapular notch and terminated over the supraspinatusmuscle in the medial portion of the SAB and the acromialinsertion of the acromioclavicular ligament. This studyelucidated previously undescribed anatomy of the SSN andits 3 distinct AB courses: 2 subacromial branches (medialand lateral) and 1 posterior GH branch to the shoulder joint.This arrangement, allowing for bipolar innervation of theSAB, was consistent with the bipolar distribution of thenociceptors in the medial and lateral part of the SABdescribed by Ide et al.24
Axillary nerveGardner16 initially described the ABs as arising from 3sites: the main trunk, as well as the anterior and posteriordivisions. After the AN entered the quadrangular space, 1or 2 ABs take off from the main trunk. These ABs traveledwith the anterior circumflex humeral artery and coursed
Figure 2 Schematic diagram of sensory innervation of the shoulder joint. (A) Anterior view; (B) posterior view.
e502 P. Laumonerie et al.
Sensory innervation of the human shoulder joint: the three bridges to break. P Laumonerie. J Shoulder Elbow Surg (2020) 29, e499–e507

Nerf suprascapulaire
assessment with US while maintaining the tip perpendic-ular to the nerve, thus allowing an optimal field of lesionfor the PRF. Furthermore, we target the nerve lateral tothe quadrangular space, thus benefitting from the hu-merus as an anterior border protecting from unwantedanterior needle penetration.
Although the only previous report we found of a PRFon both the SSN and AN for chronic pain treatment usedthree cycles of PRF of two minutes’ duration, we optedfor a single cycle. The optimal settings of PRF are still amatter of debate and are beyond the scope of this
technical report. We chose to use a safer stimulation mo-dality as repetitive PRF cycles could lead to a surge in tiptemperature that could produce ablative thermocoagula-tion on nervous fibers.
Simultaneous pulsed radiofrequency on the suprascap-ular and axillary nerves for the treatment of the chroniccondition of the painful shoulder has been scarcely stud-ied, with very few references in the literature. The ulti-mate efficacy of this combined technique has to beconfirmed or disproved by future trials. We are currentlyconducting a randomized controlled study to investigate
Figure 2. Position of the patient and ultrasound transducer for the realization of the suprascapular nerve block and its correlationwith the ultrasound image. PCHA ¼ posterior circumflex humeral artery.
Figure 1. Position of the patient and ultrasound transducer for the realization of the suprascapular nerve block and its correlationwith the ultrasound image.
Suprascapular, Axillary, US-Guided, Pulsed Radiofrequency 3
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/advance-article-abstract/doi/10.1093/pm/pny311/5301761 by EKU
Libraries user on 26 January 2019
Gofeld M, Restrepo-garces CE, Theodore R, Faclier G. Pulsed radiofrequency of suprascapular nerve for chronic shoulder pain: A randomized double-blind ac- tive placebo-controlled study. Pain Pract 2013;13 (2):96–103.

PRF et capsulite retractile

PRF nerf supra scapulaire et capsulite retractile

PRF et capsulite retractile
Diminution des EVA de l’ordre de 50 % à 1,3 et 6 mois
Amélioration du Quick Dash
Figure 3. Pain numeric rating scale post-treatment follow-up (last observation carried forward).
Figure 4. Shoulder Pain and Disability Index post-treatment follow-up (last observation carried forward).
Figure 5. Constant–Murley Score post-treatment follow-up.
Pulsed Radiofrequency of Suprascapular Nerve • 5
Figure 3. Pain numeric rating scale post-treatment follow-up (last observation carried forward).
Figure 4. Shoulder Pain and Disability Index post-treatment follow-up (last observation carried forward).
Figure 5. Constant–Murley Score post-treatment follow-up.
Pulsed Radiofrequency of Suprascapular Nerve • 5
Gofeld M, Restrepo-garces CE, Theodore R, Faclier G. Pulsed radiofrequency of suprascapular nerve for chronic shoulder pain: A randomized double-blind ac- tive placebo-controlled study. Pain Pract 2013;13 (2):96–103.

Merci de votre attention

Traitement de la douleur chronique par radiofréquence
Dr Aissou HPPE, Champigny sur Marne