Embed Size (px)
Citation preview

Original articleArticle original
� 2014 CEOPublished by / Edite par Elsevier Masson SAS
All rights reserved / Tous droits reserves
Treatment of infra-occluded primary molarsin patients with dental ageneses
Traitement des molaires temporaires eninfraclusion chez des patients qui pr�esentent desag�en�esies dentaires
Marie MEDIOa,*, Muriel DE LA DURE MOLLAb
aD�epartement d’orthodontie, hopital Piti�e-Salpetri�ere, AP–HP, universit�e Paris 7Denis-Diderot, 5, rue Thomas-Mann, 75205 Paris cedex 13, FrancebCentre de r�ef�erence des malformations rares de la face et de la cavit�e buccale, hopital Rothschild,AP–HP, 5, rue Santerre, 75012 Paris, France
Available online: 03 August 2014 / Disponible en ligne : 03 aout 2014
SummaryWhen dental agenesis is encountered, several treatment solu-tions can be considered: extraction of the primary tooth andclosure of the space or, alternatively, conservation of the spacewith the primary tooth still on the arch until a prosthesis can beplaced. In the presence of premolar agenesis, the correspondingprimary molar may be infra-occluded relative to the occlusalplane. This situation complicates the treatment plan.Depending on the clinical setting, it can be useful to restoreocclusal contacts using composite overlays. We will demonstratethis treatment option via two clinical cases. Tooth conservationhelps maintain the bone volume that will later facilitate place-ment of an implant and limit extrusion of the antagonists aswell as tipping of the neighboring teeth.
� 2014 CEO. Published by Elsevier Masson SAS. All rightsreserved
Key-words
·Infra-occlusion.
·Dental agenesis. ·Primary molar. ·Ankylosis.International Orthodontics 2014 ; 12 : 291-302http://dx.doi.org/10.1016/j.ortho.2014.06.004
R�esum�e
En pr�esence d’ag�en�esie dentaire, plusieurs solutions th�era-peutiques peuvent etre envisag�ees : extraction de la denttemporaire et fermeture de l’espace, ou maintien de l’espace,en conservant la dent temporaire sur l’arcade jusqu’a cequ’elle soit remplac�ee proth�etiquement. Lorsqu’il y aag�en�esie d’une pr�emolaire, la molaire temporaire correspon-dante peut se trouver en infraposition par rapport au pland’occlusion ce qui complique le plan de traitement. Suivantla situation clinique, il est int�eressant de r�etablir des contactsocclusaux avec des overlays en composite. Ce choix th�era-peutique sera illustr�e a travers deux cas cliniques. La conser-vation de ces dents permet de maintenir le volume osseux quifacilitera par la suite la mise en place d’un implant et limitel’�egression des dents antagonistes ainsi que la version desdents adjacentes.� 2014 CEO. Edite par Elsevier Masson SAS. Tous droitsreserves
Mots-cl�es
·Infraclusion.
·Ag�en�esie dentaire.·Molaire temporaire.
·Ankylose.
*Correspondence and reprints / Correspondance et tir�es a part :
Marie MEDIO, 14, rue Le Brun, 75013 Paris, France.e-mail address / Adresse e-mail : [email protected] (Marie MEDIO)
291

Marie MEDIO et al.
Dental agenesis is the most widespread hereditary pathologyin Europe with a prevalence of 5.45% [1]. Missing teeth canaffect all units, both primary and permanent, and can be foundin isolation or in association with multi-malformational syn-dromal forms of agenesis. Genetic mutations of genes MSX1,PAX 9 and AXIN 2 have been described in these isolated formsbut do not account for all cases of agenesis.
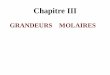
The meta-analysis performed by Polder et al. in 2004 reportedon the distribution of dental ageneses showing the most fre-quently missing and those more often preserved. Thus, thelower second premolars (41%) are the teeth most frequentlymissing followed by the upper lateral incisors (23%). The thirdmolars were not taken into account (fig. 1). The first molarsappear to be the least frequently absent teeth. When they aremissing, multiple ageneses are observed.
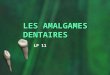
Premolar agenesis is often associated with other forms ofdental development anomaly, e.g. microdontia of the upperlateral incisors, palatal impaction of the upper canines andinfra-occlusion of the primary molars [2]. According to Peck,these manifestations constitute a “dental anomaly pattern”and are found more often in combination than in isolation onaccount of their shared genetic origin [3].Infra-occlusion of the primary molars can be observed in thepresence, or absence, of the germ of the subjacent permanenttooth [4]. Agenesis of the successional tooth has been observedin 17% of cases [5]. When the germ of the second premolar ispresent, it can be distally tipped and form an acute angle withthe mandibular plane [6](fig. 2). For Garib, distal ectopia ofthe lower second molars is a weak expression of the genes thatdetermine their agenesis [7].
The main hypothesis regarding the etiology of primary molarinfra-occlusion points to dental ankylosis [8]. Alveolar growthcontinues on either side of the adjacent teeth making the toothappear more and more “submerged” [9]. Infra-occlusion ofprimary molars is also accompanied by root resorption.
[(Fig._1)TD$FIG]
Fig. 1: Distribution of dental agenesis in EuFig. 1 : R�epartition des ag�en�esies dentaires
292
L’ag�en�esie dentaire est la pathologie h�er�editaire la plusfr�equente en Europe avec une pr�evalence de 5,45 % [1].L’absence de dents peut affecter toutes les dents (tempor-aires et permanentes) et peut etre soit isol�ee soit associ�eea des formes syndromiques polymalformatifs. Des mutationsg�en�etiques des g�enesMSX1, PAX9 etAXIN2 ont �et�e d�ecritesdans ces formes isol�ees mais n’expliquant pas tous les casd’ag�en�esies.Lam�eta-analyse dePolder et collaborateurs en 2004 rapportela r�epartition des ag�en�esies dentaires avec des dentsfr�equemment absentes et d’autres plus conserv�ees : lesdeuxi�emes pr�emolaires mandibulaires (41 %) sont le plussouvent absentes puis les incisives lat�erales maxillaires(23 %) en excluant les troisi�emes molaires (fig. 1). Les pre-mi�eres molaires semblent etre les dents le moins souventmanquantes. Lorsqu’elles sont absentes, le nombre d’ag�en�e-sies est alors �elev�e.Les ag�en�esies de pr�emolaires sont souvent associ�ees a d’au-tres anomalies du d�eveloppement dentaire : microdontie desincisives lat�erales maxillaires, inclusion palatine des caninesmaxillaires, infraclusion des molaires temporaires [2]. PourPeck, cesmanifestations constituent un « sch�ema d’anomaliedentaire » et apparaissent plus souvent associ�ees que demani�ere isol�ees de par leur origine g�en�etique commune [3].L’infraclusion des molaires temporaires peut etre observ�ee enpr�esence ou en l’absence du germe de la dent permanentesous-jacente [4]. L’ag�en�esie de la dent successionnelle a �et�eobserv�ee dans 17 % des cas [5]. Lorsque le germe de ladeuxi�eme pr�emolaire est pr�esent ce dernier peut etre en dis-toversion et former un angle aigu par rapport au plan mandi-bulaire [6] ; (fig. 2). Pour Garib, l’ectopie distale des deux-i�emes pr�emolaires mandibulaires est une expression faibledes g�enes qui d�eterminent leur ag�en�esie [7].La principale hypoth�ese de l’�etiologie de l’infraclusion desmolaires temporaires serait l’ankylose dentaire [8], la crois-sance alv�eolaire se poursuivant de part et d’autre au niveaudes dents adjacentes ; la dent apparaıt ainsi de plus en plus« submerg�ee » [9]. L’infraclusion des molaires temporairess’accompagne d’une r�esorption radiculaire.
rope (Polder et al., 2004).en Europe (Polder et al., 2004).
International Orthodontics 2014 ; 12 : 291-302

[(Fig._2)TD$FIG]
Fig. 2: Dental panorex showing tip-back of the germ of 45 andmoderate to severe infra-occlusion of 55-65-75-85.Fig. 2 : Panoramique dentaire montrant la distoversion du germe de
45 et l’infraclusion mod�er�ee a s�ev�ere de 55-65-75-85.
Treatment of infra-occluded primary molars in patients with dental agenesesTraitement des molaires temporaires en infraclusion chez des patients qui pr�esentent des ag�en�esies dentaires
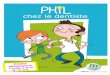
A simplified classification according to severity has beendescribed [10](fig. 3):— mild: the occlusal table is situated 1 mm below the occlusalplane;— moderate: the occlusal table coincides with the point ofcontact of the adjacent tooth;— severe: the occlusal table is situated below the point ofcontact, at gingival level.When a primary molar is infra-occluded, problems can occurto complicate the orthodontic treatment [11]:
— tipping of the adjacent teeth;— extrusion of the antagonist teeth;— shorter arch length;— disruption of the posterior occlusion;— lateral tongue thrusting.
[(Fig._3)TD$FIG]
Fig. 3: a: mild 1 mm infra-occlusionsion; c: severe 5 mm infra-occlusioteeth.Fig. 3 : a : infraclusion l�eg�ere de 1 m
3 mm ; c : infraclusion s�ev�ere de
adjacentes.
International Orthodontics 2014 ; 12 : 291-302
Une classification simple suivant la s�ev�erit�e a �et�e d�ecrite [10](fig. 3) :— l�eg�ere : la table occlusale se situe a 1 mm en dessous duplan d’occlusion ;— mod�er�ee : la table occlusale arrive au niveau du point decontact de la dent adjacente ;— s�ev�ere : la table occlusale est situ�ee sous le point decontact, au niveau de la gencive.Lorsqu’une molaire temporaire est en infraclusion, des com-plications peuvent apparaıtre, ce qui complique le traitementd’orthodontie [11] :— version des dents adjacentes ;— �egression des dents antagonistes ;— r�eduction de la longueur de l’arcade ;— perturbation de l’occlusion post�erieure ;— interposition lat�erale de la langue.
; b: moderate 3 mm infra-occlu-n with tipping of the adjacent
m ; b : infraclusion mod�er�ee de
5 mm avec version des dents
293

Marie MEDIO et al.
When these primary molar infra-occlusions are correlatedwith ageneses, the orthodontic treatment plan does not neces-sarily include extractions of the primary molars (PM) andsubsequent space closure. The treatment decision will dependon several factors, notably the facial type [12], skeletal anddental disorders and the number of ageneses (fig. 4):
— if the practitioner decides to perform space closure, extrac-tion of the primary molar can be done very early and physio-logic space closure will ensue. Joodelph and McNeill sug-gested extracting the primary molar before the age of 11(before eruption of the second molar) in order to ensure spon-taneous closure [13]. Other authors advocate performing ahemisection of the distal segment of the primary tooth as afirst step in order to encourage mesialization and avoid tippingbefore going on to extract the mesial segment [14]. In order toimprove the occlusal relationships, we are sometimes obligedto extract contralateral teeth to achieve symmetry, or antago-nists to obtain better molar relationships. Spaces due to man-dibular agenesis are often difficult to close, particularly inhypodivergent subjects;
— if the treatment plan is to maintain the agenesis spaces, thebest solution is to maintain the primary molar on the arch aslong as possible [15,16]. The longitudinal study by Bjerklin’steam in 99 patients presenting with agenesis of the premolarsshowed that more than 90% of primary molars were kept on thearch into adulthood [17]. Several alternative solutions can
[(Fig._4)TD$FIG]
Fig. 4: Decision-making when faced with premolar aFig. 4 : Prise de d�ecision face a une ag�en�esie pr�emol
294
Lorsque ces infraclusions des molaires temporaires sontcorr�el�ees a des ag�en�esies, le plan de traitement orthodon-tique ne comporte pas n�ecessairement les extractions desmolaires temporaires (MT) avec la fermeture des espaces.La d�ecision th�erapeutique va d�ependre de plusieurs fac-teurs notamment la typologie faciale [12], les troubles sque-lettiques et dentaires ainsi que le nombre d’ag�en�esies (fig. 4) :— si la d�ecision th�erapeutique est la fermeture d’espace,l’extraction de la molaire temporaire peut se faire tr�es pr�eco-cement, et on peut observer une fermeture physiologique del’espace. Joodelph et Mc Neill sugg�erent d’extraire la molairetemporaire avant 11 ans (avant l’�eruption de la deuxi�ememolaire) afin d’observer une fermeture spontan�ee [13]. Desauteurs pr�econisent �egalement de faire une h�emisection de lapartie distale de la dent temporaire dans un premier temps afinde favoriser sa m�esialisation en �evitant la version puis d’extra-ire la partie m�esiale [14]. Afin d’am�eliorer les rapports occlu-saux, nous sommes parfois contraints d’extraire en contro-lat�eral (pour sym�etriser) ou en antagoniste (pour obtenir demeilleurs rapports au niveau des molaires. Les espacesd’ag�en�esie a la mandibule sont souvent difficiles a fermer,surtout si le sujet est hypodivergent) ;— si la d�ecision th�erapeutique est le maintien des espacesd’ag�en�esies, la meilleure solution est de garder la molairetemporaire le plus longtemps possible sur l’arcade [15,16].L’�etude longitudinale de l’�equipe de Bjerklin sur 99 patientspr�esentant des ag�en�esies de pr�emolaires a montr�e que plusde 90 % des molaires temporaires ont �et�e conserv�ees sur
genesis.aire.
International Orthodontics 2014 ; 12 : 291-302

Treatment of infra-occluded primary molars in patients with dental agenesesTraitement des molaires temporaires en infraclusion chez des patients qui pr�esentent des ag�en�esies dentaires
then be envisaged, e.g. a tooth-supported bridge, whichinvolves impairing the teeth adjacent to the edentulous space;an auto-transplant of the third upper molar can be indicated insome clinical circumstances [18]; and, finally, the most fre-quent solution is an implant-borne crown when growth iscomplete;
— maintaining primary molars makes it possible to preservebone volume until such time as an implant can be inserted. Itis sometimes necessary to reduce the mesiodistal diameter ofthe primary molar, which is wider than a premolar, in order tocreate sufficient space for the future prosthetic restoration[19]. This reduction will be determined by the distancebetween the roots and by the size of the pulp in order to avoidany inflammatory reaction [20];
— if the primary molar has been extracted because of severelyresorbed roots, it becomes necessary to fabricate a spacemaintainer (band/crown loop, Nance arch, lingual archwire,or a splint) until the future prosthetic restoration can be per-formed. A pediatric prosthesis could also be made. If a tem-porary molar is infra-occluded, it is useful to preserve this
[(Fig._5)TD$FIG]
Fig. 5: a–c: intra-oral views in occlusion showing a bilateral infra-occviews of the maxillary and mandibular arches during development phas55-64-65-74-75-85 and agenesis of the successional teeth.Fig. 5 : a–c : vues intra-orales en occlusion montrant une infraclusion bil
vues intra-orales des arcades maxillaire et mandibulaire en phase de co
sion de 54-55-64-65-74-75-85 et ag�en�esies des dents successionelles.
International Orthodontics 2014 ; 12 : 291-302
l’arcade jusqu’a l’age adulte [17]. Plusieurs solutions deremplacement seront ensuite envisageables : le bridgedentoport�e, qui n�ecessite le d�elabrement des dents bordantl’�edentement ; l’autotransplantation de la troisi�eme molairemaxillaire peut etre indiqu�ee dans certaines situations clini-ques [18] et enfin la solution la plus fr�equente est la couronneimplantoport�ee en fin de croissance ;— le maintien de la molaire temporaire permet en effet deconserver le volume osseux en attendant la pose de l’implant.Il est parfois n�ecessaire de diminuer le diam�etre m�esiodistalde la molaire temporaire qui est plus large qu’une pr�emolaire,afin de m�enager un espace adapt�e a la future restaurationproth�etique [19] ; cette r�eduction va etre guid�ee par la diver-gence des racines ainsi que par la taille de la pulpe afin d’�eviterune r�eaction inflammatoire [20]. Si la molaire temporaire a �et�eextraite car les racines �etaient trop r�esorb�ees, il faut alorsr�ealiser un mainteneur d’espace en attendant la future restau-ration proth�etique : band/crown loop, arc de Nance, arc lin-gual, goutti�ere ; on peut �egalement r�ealiser une proth�esep�ediatrique ;— si la molaire temporaire est en infraclusion, il est int�eres-sant de conserver ces dents sur l’arcade afin d’�eviter la fonteosseuse et donc d’optimiser la mise en place de l’implant.Plusieurs options th�erapeutiques ont �et�e propos�eesdans la litt�erature pour remettre ces dents en fonction et�eviter des complications secondaires [21] : des coiffes
lusion with lingual interposition and left crossbite; d, e: intra-orale of adolescent dentition; f: panorex showing infra-occlusion of 54-
at�erale avec interposition linguale et invers�e d’articul�e gauche ; d, e :
nstitution de la denture adolescente ; f : panoramique avec infraclu-
295

Marie MEDIO et al.
tooth on the arch in order to avoid bone resorption and thusensure optimal implant placement. Several treatment options,such as a preformed pedodontic coping or direct or indirecttechnique composites, have been suggested in the literature torestore these teeth to normal function and avoid secondarycomplications [21].We will illustrate our paper with two clinical cases in which weplaced composite overlays by the indirect technique in orderto restore occlusal contact. The composites were made in thelaboratory on articulator-mounted plaster models. The over-lays were tried and then bonded and the occlusion waschecked using articulating paper.
[(Fig._6)TD$FIG]
Fig. 6: a: Quad helix for transverse expansion anwith composites on 55,65,75,85 using the indireoverlays and labial brackets on 11 and 21 to clomonths after placement of the overlays.Fig. 6 : a : Quad h�elix pour expansion transversa
platre avec composites r�ealis�es enm�ethode indire
des overlays coll�es et attaches vestibulaires sur 1
panoramique de controle 6 mois apr�es la pose d
296
p�edodontiques pr�eform�ees, des composites en m�ethodedirecte ou indirecte.
Deux cas cliniques ou nous avons r�ealis�e des overlays encomposite en m�ethode indirecte afin de r�etablir un contactocclusal illustrent nos propos. Les composites ont �et�efabriqu�es au laboratoire sur des mod�eles en platre mont�esen articulateur. Les overlays ont �et�e essay�es puis coll�es etl’occlusion a �et�e v�erifi�ee avec du papier articul�e.
d derotation of 16 and 26; b: plaster modelsct technique; c–e: intra-oral views of bondedse the median diastema; f: control panorex 6
le et d�erotation de 16 et 26 ; b : mod�eles en
cte sur 55 65, 75, 85 ; c–e : vues intra-orales
1 et 21 pour fermer le diast�emem�edian ; f :
es overlays.
International Orthodontics 2014 ; 12 : 291-302

Treatment of infra-occluded primary molars in patients with dental agenesesTraitement des molaires temporaires en infraclusion chez des patients qui pr�esentent des ag�en�esies dentaires
Clinical case no 1
A young girl aged 12.5 years in good general health consultedat the reference center for rare diseases on account of dentalageneses. Her clinical and radiologic records revealed severeoligodontia with agenesis of 18 teeth: the upper lateral incisors(12-22), the upper canines (13-23), the upper premolars (14-15-24-25), the left upper second molar (27), a lower incisor(41), three lower premolars (34-35-45), the left lower secondmolar (37) and the third molars (18-28-38-48).
She also displayed a narrow maxillary dental base with left-side mandibular laterodeviation, a 2 mm Class II on the rightand a 5 mmClass II on the left, a right and left lateral open bitewith lingual interposition, mesio-palatal rotation of 16 and 26andmoderate to severe infra-occlusion of 54-55-64-65-74-75-85 with partial root resorption (fig. 5).
[(Fig._7)TD$FIG]
Fig. 7: a–c: intra-oral views at end of orthodoreplace 12-13-14, 22-23. The prosthesis was sewith the overlays; d: occlusal view of the maxprosthetic restoration of 34 extending to 75.Fig. 7 : a–c : vues intra-orales en fin de traitem
pour remplacer 12-13-14, 22-23. La r�etention de
sur 55 et 65 r�ehabilit�es avec les overlays : d : v
arcade mandibulaire avec restauration proth�etiq
International Orthodontics 2014 ; 12 : 291-302
Cas clinique no 1
Une jeune fille ag�ee de 12 ans et 5 mois en bonne sant�eg�en�erale consulte au centre de r�ef�erence des maladies rares,pour ses ag�en�esies dentaires. Les examens clinique et radi-ologique r�ev�elent une oligodontie s�ev�ere avec ag�en�esie de18 dents : les incisives lat�erales maxillaires (12-22), lescanines maxillaires (13-23), les pr�emolaires maxillaires (14-15-24-25), la deuxi�eme molaire maxillaire gauche (27), uneincisive mandibulaire (41), trois pr�emolaires mandibulaires(34-35-45), la deuxi�eme molaire mandibulaire gauche (37) etles troisi�emes molaires (18-28-38-48).Elle pr�esente une endoalv�eolie maxillaire avec lat�erod�eviationmandibulaire a gauche, une Classe II de 2 mm a droite et5 mm a gauche, une b�eance lat�erale droite et gauche avecinterposition de la langue, une rotation m�esiopalatine de 16 et26 et une infraclusion mod�er�ee a s�ev�ere de 54-55-64-65-74-75-85 avec une r�esorption partielle des racines (fig. 5).
ntic treatment with pediatric prosthesis tocured to hooks on 55 and 65 reconstructedillary prosthesis; e: mandibular arch with
ent orthodontique avec proth�ese p�ediatrique
la proth�ese est assur�ee grace a des crochets
ue occlusale de la proth�ese maxillaire ; e :
ue de 34 en extension sur 75.
297

Marie MEDIO et al.
Treatment plan
Stage one:— maxillary transverse expansion using a quad helix to recen-ter the mandible and closure of the median diastema with twobrackets on 11 and 21;— prosthetic rehabilitation of the primary second molars bymeans of composite overlays in order to restore masticationand occlusion and prevent the lateral lingual interposition(fig. 6).Stage 2:— bimaxillary multibracket treatment to reduce the deep bite,coordinate the arches and achieve satisfactory intercuspation;
— a pediatric prosthesis was made at the end of treatment tocompensate for the edentulous spaces while waiting for thegrowth peak to terminate before placing implant-borne pros-theses (fig. 7).
Clinical case no 2
The patient was a young boy, 12 years old and in goodgeneral health, who was seen at the orthodontic unit of the
[(Fig._8)TD$FIG]
Fig. 8: a: panoramic radiography at 12 years wit46-48; b, c: right and left intra-oral view: bilatmandibular arch showing mild infra-occlusion ofFig. 8 : a : radiographie panoramique a 12 ans ave
38-45-46-48 ; b, c : vues intra-orales droite et gau
de l’arcade mandibulaire montrant l’infraclusion l�e
298
Plan de traitement
Dans un premier temps :— expansion transversale maxillaire avec un quad h�elix pourrecentrer la mandibule et fermeture du diast�eme m�edian avecdeux attaches sur 11 et 21 ;— r�ehabilitation proth�etique des deuxi�emes molaires tempor-aires avec des overlays en composite afin de r�etablir la mas-tication et l’occlusion et �eviter l’interposition linguale lat�erale(fig. 6).Dans un deuxi�eme temps :— traitement multiattache maxillaire et mandibulaire afin der�eduire la supraclusion, coordonner les arcades et obtenir unengr�enement des arcades satisfaisant ;— une proth�ese p�ediatrique est r�ealis�ee en fin de traitementpour compenser les �edentements et attendre la fin de crois-sance pour r�ealiser des proth�eses implantoport�ees (fig. 7).
Cas clinique no 2
Il s’agit d’un jeune homme ag�e de 12 ans en bonne sant�eg�en�erale, suivi en consultation dans le service d’orthodontie
h no visibility of 17-18-27-28-35-36-38-45-eral non-occlusion; d: occlusal view of the75 and 85 and rotation of 37 and 47.c absence de visibilit�e de 17-18-27-28-35-36-
che : inocclusion bilat�erale ; d : vue occlusale
g�ere de 75 et 85 et les rotations de 37 et 47.
International Orthodontics 2014 ; 12 : 291-302

[(Fig._9)TD$FIG]
Fig. 9: a: panoramic x-ray at 13 years showing moderate infra-occlusion of 75 and 85; b:lateral headfilm in occlusion with normal facial pattern.Fig. 9 : a : radiographie panoramique a 13 ans avec infraclusion mod�er�ee de 75 et 85 ; b :
t�el�eradiographie de profil en occlusion avec une typologie normodivergente.
Treatment of infra-occluded primary molars in patients with dental agenesesTraitement des molaires temporaires en infraclusion chez des patients qui pr�esentent des ag�en�esies dentaires
Piti�e-Salpetri�ere hospital in Paris for dental ageneses. Theclinical examination revealed agenesis of 6 teeth: two uppermolars (17-27), two lower premolars (35-45), and two lowermolars (36-46). Slow growth was associated with the latedevelopment of the germs at 18-28-38-48.
[(Fig._10)TD$FIG]
Fig. 10: a: panoramic x-ray at 14 years showingright and left Class I canine and intercuspating omandibular arch showing the restoration with aFig. 10 : a : radiographie panoramique a 14 an
germe ; b, c : Classe I canine D et G et occlusio
occlusale de l’arcade mandibulaire montrant la re
75 et 85.
International Orthodontics 2014 ; 12 : 291-302
de la Piti�e-Salpetri�ere pour des ag�en�esies dentaires. Al’examen clinique, il pr�esente une oligodontie avec ag�en�esiede 6 dents : deux molaires maxillaires (17-27), deux pr�emo-laires mandibulaires (35-45), et deux molaires mandibulaires(36-46). L’apparition des germes de 18-28-38-48 est tardiveassoci�ee a un retard de d�eveloppement.
visibility of 18-28-38-48 at germ stage; b, c:cclusion at 75 and 85; d: occlusal view of thecomposite overlay on 75 and 85.s avec visibilit�e de 18-28-38-48 a l’�etat de
n engr�enante au niveau de 75 et 85 ; d : vue
stauration avec un overlay en composite sur
299

Marie MEDIO et al.
From the skeletal viewpoint, he presented a Class I in anormodivergent facial pattern. From the dental perspective,he displayed a 2 mm Class II on both right and left sides with a2 mm overbite (fig. 8) and a mild infra-occlusion of 75 and 85with partially resorbed roots.The orthodontic treatment plan was to maintain the agenesisspaces on the arch at 75 and 85, to mesialize 37 and 47 to thesite of 36 and 46, to reduce the overjet and overbite and tocorrect the Class II by means of multibracket appliances onboth maxilla and mandible. During orthodontic treatment, 75and 85 became more and more infra-occluded and their rootshad been virtually totally resorbed (fig. 9).
Infra-occluded overlays were bonded on 75 and 85 in order toincrease crown height and restore occlusal contact (fig. 10).
[(Fig._11)TD$FIG]
Fig. 11: a: panorex x-ray at 15 years: almost cand 85; b, c: right and left canine Class I; 75 andmandibular arch with intra-arch alignment of 75Fig. 11 : a : radiographie panoramique a 15 ans
85 r�ehabilit�ees ; b, c : Classe I canine droite et g
occlusale de l’arcade mandibulaire avec alignem
300
Sur le plan squelettique, il pr�esente une Classe I sur unsch�ema normodivergent. Sur le plan dentaire, on note uneClasse II molaire de 2 mm droite et gauche avec une supra-clusion incisive de 2 mm (fig. 8) et une infraclusion l�eg�ere de75 et 85 avec des racines partiellement r�esorb�ees.Le plan de traitement orthodontique a consist�e a maintenir lesespaces d’ag�en�esies de 75 et 85 sur l’arcade, a m�esialer37 et 47 a la place de 36 et 46, a diminuer le surplomb et lerecouvrement et a corriger la Classe II avec un appareil multi-attache maxillaire et mandibulaire. Au cours du traitementd’orthodontie, 75 et 85 apparaissent de plus en plus en infra-clusion et leurs racines sont pratiquement totalementr�esorb�ees (fig. 9).Des overlays ont �et�e coll�es sur 75 et 85 en infraclusion afind’augmenter la hauteur coronaire et de r�etablir un contactocclusal (fig. 10).
omplete root resorption of reconstructed 7585 are in occlusion; d: occlusal view of theand 85.
: r�esorption quasi totale des racines de 75 et
auche, 75 et 85 sont en occlusion ; d : vue
ent intra-arcade de 75 et 85.
International Orthodontics 2014 ; 12 : 291-302

Treatment of infra-occluded primary molars in patients with dental agenesesTraitement des molaires temporaires en infraclusion chez des patients qui pr�esentent des ag�en�esies dentaires
Follow-up was scheduled one year after placement of theoverlays. Despite major root resorption at 75 and 85, therestored teeth were still in occlusion (fig. 11).
Conclusion
Preservation of the milk teeth made it possible to maintainsufficient bone volume to facilitate subsequent implant place-ments. Restoration of function and the composite reconstruc-tion of the entire crown maintained the mesiodistal diameter ofthe agenesic tooth and prevented extrusion of the antagonistsand tipping of the adjacent units as well as the lateral lingualinterposition.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
AcknowledgementsDr Vi-Fane, Dr Garrec, Dr Castaneda, Dr Nham, Dr Paulme.
References/R�ef�erences
1. Polder BJ, Van’t Hof MA, Vaprevalence of dental agene2004;32(3):217–26.
2. Baccetti T. A controlled s68(3):267–77.
3. Peck S. Dental anomaly pat4. Kula K, Tatum BM, Owen D
children with ankylosis of p5. Winter GB, Gelbier MJ, Goo
uous molars associated withdentition: a report of 28 sele
6. Shalish M, Peck S, Wasserassociated with infraocclusi
7. Garib DG, Peck S, Gomes Ssecond-premolar agenesis. A
8. Kurol J. Infraocclusion of prical and histological study. S
9. Noble J, Karaiskos N, Wiltprimary molar. Br Dent J 20
10. Brearley LJ, McKibben Jr.characteristics. ASDC J Den
11. Ekim SL, Hatibovic-Kofmaprimary molars. Int J Paedia
International Orthodontics 2014 ; 12 : 291-302
Un suivi r�egulier a �et�e r�ealis�e, 1 an apr�es la mise en place desoverlays. Malgr�e une importante r�esorption radiculaire de75 et 85, les dents restaur�ees sont toujours en occlusion(fig. 11).
Conclusion
La conservation de ces dents lact�eales permet de maintenirun volume osseux qui facilitera par la suite la mise en placedes implants. La remise en fonction avec une r�ehabilitation aucomposite de toute la couronne maintient le diam�etrem�esiodistal de la dent et permet ainsi d’�eviter des �egressionsdes dents antagonistes, des versions des dents adjacentesmais �egalement l’interposition lat�erale de la langue.
D�eclaration d’int�erets
Les auteurs d�eclarent ne pas avoir de conflits d’int�erets enrelation avec cet article.
RemerciementsDr Vi-Fane, Dr Garrec, Dr Castaneda, Dr Nham, Dr Paulme.
n der Linden FP, Kuijpers-Jagtman AM. Ameta-analysis of thesis of permanent teeth. Community Dent Oral Epidemiol
tudy of associated dental anomalies. Angle Orthod 1998;
tern (DAP). Angle Orthod 2009;79(5):1015–6., Smith RJ, Rule J. An occlusal and cephalometric study ofrimary molars. J Pedod 1984;8:146–59.dman JR. Severe Infra-occlusion and failed eruption of decid-eruptive and developmental disturbances in the permanentcted cases. Br J Orthod 1997;24(2):149–57.stein A, Peck L. Increased occurrence of dental anomalieson of deciduous molars. Angle Orthod 2010;80(3):440–5.C. Increased occurrence of dental anomalies associated withngle Orthod 2009;79(3):436–41.imary molars. An epidemiological familial, longitudinal clin-wed Dent J Suppl 1984;21:1-67.shire WA. Diagnosis and management of the infra-erupted07;203:632–4.DH. Ankylosis of primary molar teeth. I. Prevalence andt Child 1973;40(1):54-63.n S. A treatment decision-making model for infraoccludedtr Dent 2001;11(5):340–6.
301

12. Dias C, Closs LQ, Fontanella V, de Araujo FB. Vertical alveolar growth in subjects withinfraoccluded mandibular deciduous molars. Am J Orthod Dentofacial Orthop 2012;141(1):81–6.
13. Joondeph DR, McNeill RW. Congenitally absent second premolars: an interceptiveapproach. Am J Orthod Dentofacial Orthop 1971;59:50-66.
14. NorthwayWM. The nuts and bolts of hemisection treatment: managing congenitally missingmandibular second premolars. Am J Orthod Dentofacial Orthop 2005;127(5):606–10.
15. Bjerklin K, Bennett J. The long-term survival of lower second primary molars in subjectswith agenesis of the premolars. Eur J Orthod 2000;22(3):245–55.
16. Ith-Hansen K, Kjaer I. Persistance of deciduous molars in subjects with agenesis of thesecond premolars. Eur J Orthod 2000;22(3):239–43.
17. Bjerklin K, Al-Najjar M, Ka�restedt H, Andr�en A. Agenesis of mandibular second premolars
with retained primary molars: a longitudinal radiographic study of 99 subjects from 12 yearsof age to adulthood. Eur J Orthod 2008;30(3):254–61.
18. Lundberg T, Isaksson S. A clinical follow-up study of 278 autotransplanted teeth. Br J OralMaxillofac Surg 1996;34:181–5.
19. Kokich VG, Kokich VO. Congenitally missing mandibular second premolars: clinical Foptions. Am J Orthod Dentofacial Orthop 2006;130(4):437–44.
20. Sabri R. Management of over-retained mandibular deciduous second molars with andwithout permanent successors. World J Orthod 2008;9(3):209–20.
21. Kennedy DB. Treatment strategies for ankylosed primary molars. Eur Arch Paediatr Dent2009;10(4):201–10.
302 International Orthodontics 2014 ; 12 : 291-302
Marie MEDIO et al.