Embed Size (px)
Citation preview

Cas clinique
DOI of or1Discipline
Davila’’ Univ2Departme
and Pharmacy3Discipline
‘‘Carol DavilRoumanie.
4DepartmeHygiene and P
Trois variantes anatomiques tr�es rares del’art�ere h�epatique
Mugurel Constantin Rusu,1 Adelina Maria Jianu,2 Dorina Sztika,2 Dragos Cuzino,3
Carla Loreto,4 Bucarest et Timisoara, Roumanie; et Catane, Italie
De nombreuses variantes anatomiques de l’art�ere h�epatique, mais pas toutes, sont connues. Denouvelles ou extremement rares variantes anatomiques des art�eres h�epatiques peuvent cepen-dant etre rencontr�ees en pratique courante. Le premier cas rapport�e a �et�e document�e par lescanner et correspond �a une variante rare : une art�ere h�epatique propre r�etroporte anastomos�eeavec l’art�ere m�esent�erique sup�erieure par un arc de B€uhler. Le deuxi�eme cas pr�esente lesr�esultats d’une �etude de dissection, o�u une art�ere h�epatique moyenne (MHA) s’est av�er�ee naıtred’un tronc commun gastroh�epatique avec l’art�ere gastrique droite, du tronc de l’art�ere h�epatiquepropre ; cette MHA passait au-dessus de l’art�ere h�epatique gauche, la cachant. Par ailleurs,dans le cas 2, une art�ere h�epatique droite accessoire naissait de l’art�ere m�esent�eriquesup�erieure. Dans le troisi�eme cas rapport�e dans cet article, une boucle art�erielle associaitl’art�ere h�epatique commune et l’art�ere gastroduod�enale et envoyait une branche ascendante,diagnostiqu�ee comme MHA, et descendante, consid�er�e comme une art�ere gastroduod�enaledouble. Nous n’avons pas ne trouv�e de rapport pr�ec�edent de variantes comme celles des cas 2et 3, que nous consid�erons comme extremement rares. Cependant, les chirurgiens et lesradiologues doivent se rendre compte de telles possibilit�es morphologiques rares de l’art�ereh�epatique.
Hepatic artery variations are very important in sur-
gical and radiological procedures concerning the
liver.1 Therefore, rare or extremely rare anatomic
variants of the hepatic arteries still remain impor-
tant and should further be presented, even though
there are available studies performed on large lots.
For example, in a recent study performed using
spiral computed tomography (CT) and digital sub-
traction angiography, the celiac axis and common
hepatic artery (CHA) variations were documented
iginal article: 10.1016/j.avsg.2011.03.011.
of Anatomy, Faculty of Dental Medicine, ‘‘Carolersity of Medicine and Pharmacy, Bucarest, Roumanie.
nt of Anatomy, ‘‘Victor Babes’’ University of Medicine, Timisoara, Roumanie.
of Radiology and Medical Imaging, Faculty of Medicine,a’’ University of Medicine and Pharmacy, Bucarest,
nt of Anatomy, Diagnostic Pathology, Forensic Medicine,ublic Health, University of Catania, Catane, Italie.
in 5,002 patients.2 In more than 50% of cases,
arterial hepatic vascularization is not limited to a
single artery arising from the celiac trunk (CelT).3
Still new or extremely rare anatomical variations of
the hepatic arteries can be encountered in the cur-
rent practice.
The arch theory by Mac Kay and Tandler’s longi-
tudinal arterial anastomosis theory account for the
genesis of the arterial trunk anastomoses and the
main anatomic variations.3 According to these
Correspondance : Mugurel Constantin Rusu, Discipline of Anatomyand Embryology, Faculty of Dental Medicine, University of Medicineand Pharmacy, ‘‘Carol Davila’’ 8, Blvd. Eroilor Sanitari, RO-76241,Bucarest, Roumanie, E-mail: [email protected]
Ann Vasc Surg 2011; 25: 1138.e1-1138.e7http://dx.doi.org/10.1016/j.acvfr.2012.12.003� Annals of Vascular Surgery Inc.�Edit�e par ELSEVIER MASSON SAS
1212.e1
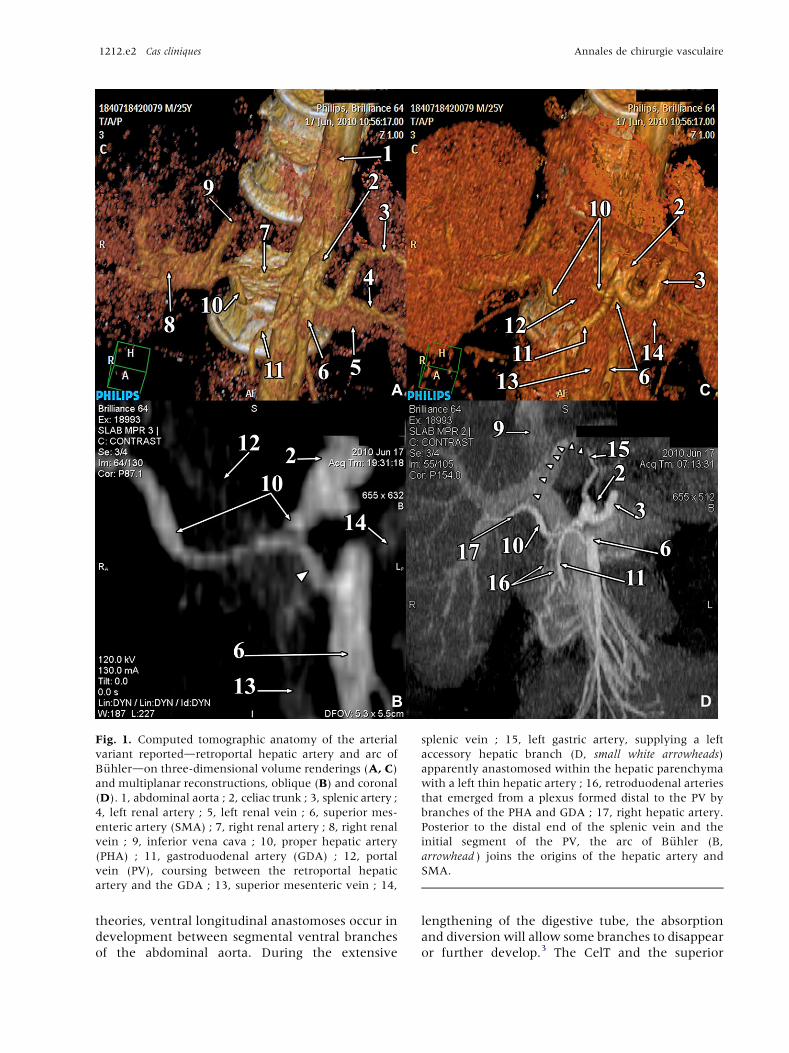
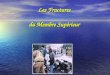
Fig. 1. Computed tomographic anatomy of the arterial
variant reporteddretroportal hepatic artery and arc of
B€uhlerdon three-dimensional volume renderings (A, C)
and multiplanar reconstructions, oblique (B) and coronal
(D). 1, abdominal aorta ; 2, celiac trunk ; 3, splenic artery ;
4, left renal artery ; 5, left renal vein ; 6, superior mes-
enteric artery (SMA) ; 7, right renal artery ; 8, right renal
vein ; 9, inferior vena cava ; 10, proper hepatic artery
(PHA) ; 11, gastroduodenal artery (GDA) ; 12, portal
vein (PV), coursing between the retroportal hepatic
artery and the GDA ; 13, superior mesenteric vein ; 14,
splenic vein ; 15, left gastric artery, supplying a left
accessory hepatic branch (D, small white arrowheads)
apparently anastomosed within the hepatic parenchyma
with a left thin hepatic artery ; 16, retroduodenal arteries
that emerged from a plexus formed distal to the PV by
branches of the PHA and GDA ; 17, right hepatic artery.
Posterior to the distal end of the splenic vein and the
initial segment of the PV, the arc of B€uhler (B,
arrowhead ) joins the origins of the hepatic artery and
SMA.
1212.e2 Cas cliniques Annales de chirurgie vasculaire
theories, ventral longitudinal anastomoses occur in
development between segmental ventral branches
of the abdominal aorta. During the extensive
lengthening of the digestive tube, the absorption
and diversion will allow some branches to disappear
or further develop.3 The CelT and the superior
Vol. 25, No. 8, 2011 Cas cliniques 1212.e3
mesenteric artery (SMA) are joined together
through the pancreaticoduodenal arcades and the
arc of B€uhler. These anastomoses are divided during
pancreatic resections but are well represented in the
case of CelT stenosis.3 The anastomosis (arc, arcade)
of B€uhler between the CelT and the SMA, first
described in 1904, is a rare finding and is explained
by failure of regression of the ventral segmental
anastomoses between the 10th and 13th segmental
arteries during embryonic life.4 There are only a few
reports of the arc of B€uhler in current scientific
literature,4 and the collateral development of this
anastomosis relates to a different hemodynamic in
the upper visceral arteries.5
Fig. 2. The hepatic arterial variation in case report 1. 1,
PV ; 2, celiac trunk ; 3, SMA ; 4, splenic artery ; 5, left
gastric artery ; 6, PHA ; 7, GDA. The left main (arrow) and
accessory (double arrow) hepatic arteries are indicated.
The arc of B€uhler (arrowhead ) joins the SMA and the
PHA. *right hepatic artery.
CASE REPORT 1
A CT angiography performed on a 26-year-old male
patient revealed several rare anatomic variants that were
better detailed by use of both multiplanar reconstructions
and three-dimensional volume renderings instead of any
of these two alone (Fig. 1). The CelT was identified,
sending off the splenic artery and further dividing into the
proper hepatic artery (PHA) and the gastroduodenal
artery (GDA). The portal vein (PV) was found on three-
dimensional volume renderings coursing between the
PHA and the GDA. Therefore, a retroportal course of the
PHA was diagnosed, with that artery being continued on
the right posterior side of the PV toward the hepatic hilum.
From the PHA left, a large right hepatic artery (RHA) and a
thin left hepatic artery (LHA) entering the hepatic
parenchyma and anastomosing with a left accessory
hepatic branch emerged from the left gastric artery. On
multiplanar reconstructions, we identified retroportal and
retropancreatic anastomosis between the origins of the
PHA and the SMA, which was diagnosed as the arc of
B€uhler. These arterial variations are summarized in
Figure 2. Anastomoses of the PHA and the GDA were
identified distal to the PVdfrom that arterial network
were leaving retroduodenal arteries. Anastomoses of the
pancreaticoduodenal arteries, superior and inferior, were
also identified. An additional variation of the right renal
arteries was identified (Fig. 3), represented by a main or
hilar right renal artery (RRA) and a right inferior polar
artery, both with aortic origins. The hilar RRA left the side
of the aorta at an intermediate level between the origins of
the CelT and SMA, and had an initial course at the level of
the retroportal PHA, being separated from it by the infe-
rior caval vein.
Fig. 3. The variation of the right renal arteries in casereport 1. The abdominal aorta (1) sends off a main hilar
(2) and a lower polar (3) renal artery. (4) SMA ; com-
puted tomographic angiography, oblique multiplanar
reconstruction.
CASE REPORT 2
A second anatomical case study was performed in a
formalin-fixed adult cadaver, 59-year-old man. The CHA
was divided anterior to the left border of the PV into an
ascending branch, the PHA, and a descending one, the
GDA. Soon after its origin, the PHA split in two
trunksdone posterior (the PHA proper) and the other
anterior, anatomically uncommon. Because the latter sent
off the right gastric artery and a supernumerary hepatic
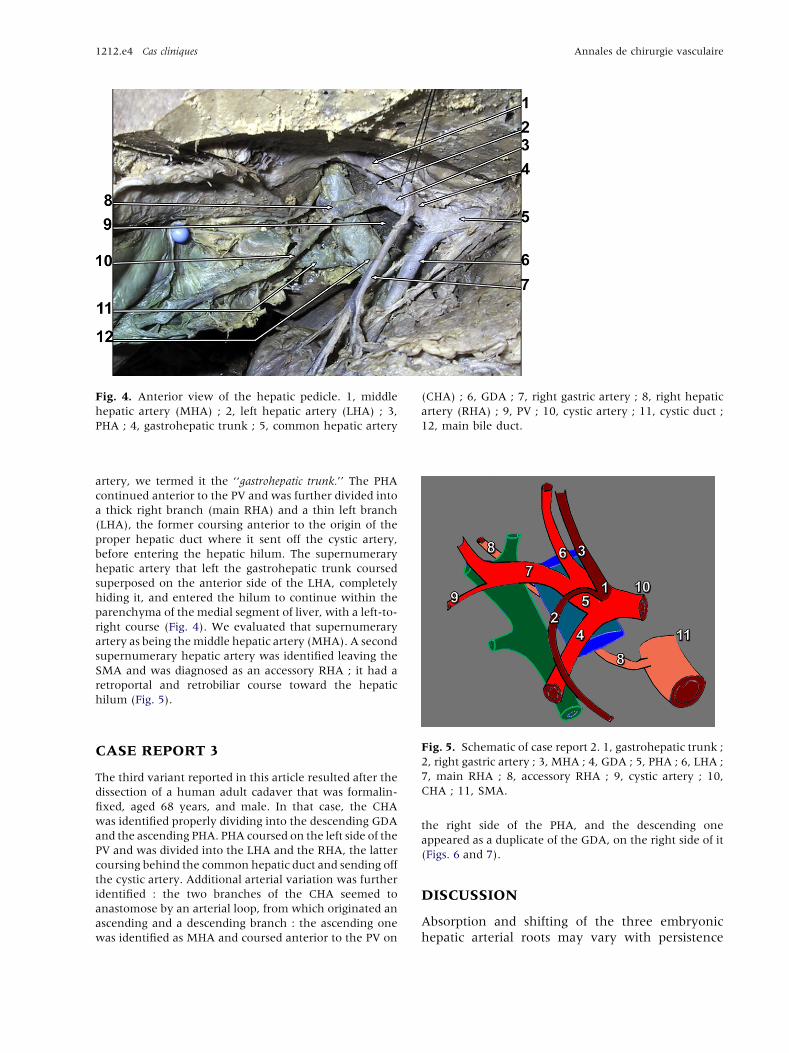
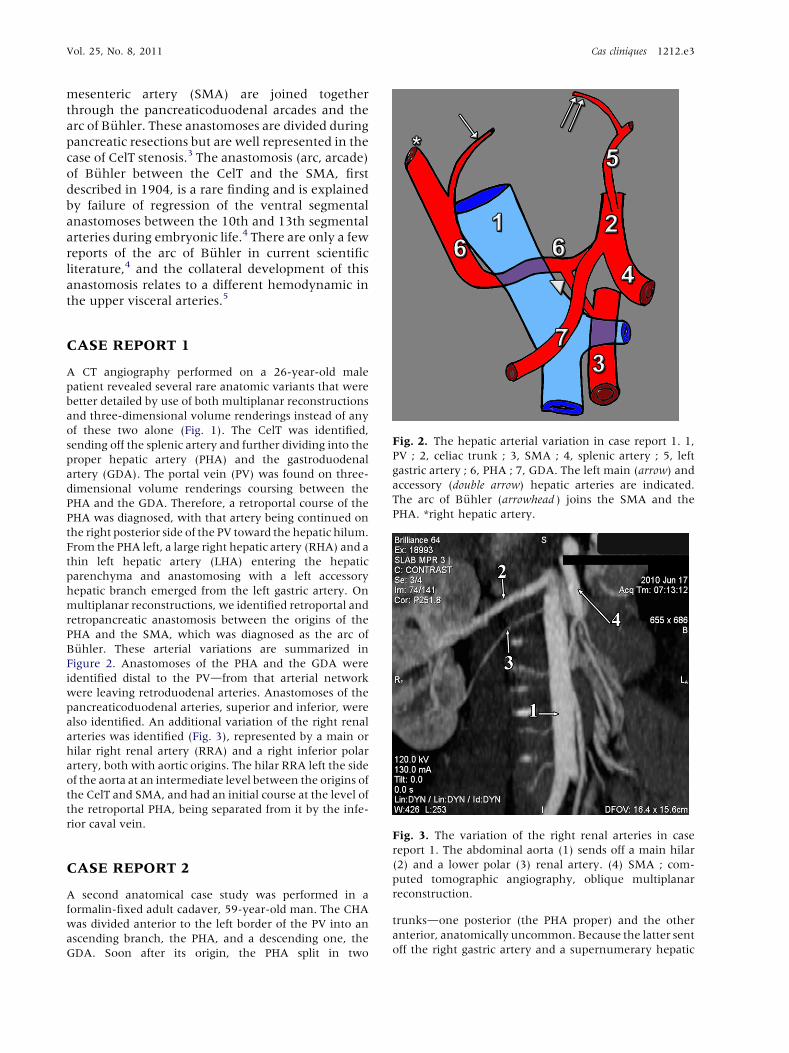
Fig. 4. Anterior view of the hepatic pedicle. 1, middle
hepatic artery (MHA) ; 2, left hepatic artery (LHA) ; 3,
PHA ; 4, gastrohepatic trunk ; 5, common hepatic artery
(CHA) ; 6, GDA ; 7, right gastric artery ; 8, right hepatic
artery (RHA) ; 9, PV ; 10, cystic artery ; 11, cystic duct ;
12, main bile duct.
1212.e4 Cas cliniques Annales de chirurgie vasculaire
artery, we termed it the ‘‘gastrohepatic trunk.’’ The PHA
continued anterior to the PV and was further divided into
a thick right branch (main RHA) and a thin left branch
(LHA), the former coursing anterior to the origin of the
proper hepatic duct where it sent off the cystic artery,
before entering the hepatic hilum. The supernumerary
hepatic artery that left the gastrohepatic trunk coursed
superposed on the anterior side of the LHA, completely
hiding it, and entered the hilum to continue within the
parenchyma of the medial segment of liver, with a left-to-
right course (Fig. 4). We evaluated that supernumerary
artery as being themiddle hepatic artery (MHA). A second
supernumerary hepatic artery was identified leaving the
SMA and was diagnosed as an accessory RHA ; it had a
retroportal and retrobiliar course toward the hepatic
hilum (Fig. 5).
Fig. 5. Schematic of case report 2. 1, gastrohepatic trunk ;
2, right gastric artery ; 3, MHA ; 4, GDA ; 5, PHA ; 6, LHA ;
7, main RHA ; 8, accessory RHA ; 9, cystic artery ; 10,
CHA ; 11, SMA.
CASE REPORT 3
The third variant reported in this article resulted after the
dissection of a human adult cadaver that was formalin-
fixed, aged 68 years, and male. In that case, the CHA
was identified properly dividing into the descending GDA
and the ascending PHA. PHA coursed on the left side of the
PV and was divided into the LHA and the RHA, the latter
coursing behind the common hepatic duct and sending off
the cystic artery. Additional arterial variation was further
identified : the two branches of the CHA seemed to
anastomose by an arterial loop, from which originated an
ascending and a descending branch : the ascending one
was identified as MHA and coursed anterior to the PV on
the right side of the PHA, and the descending one
appeared as a duplicate of the GDA, on the right side of it
(Figs. 6 and 7).
DISCUSSION
Absorption and shifting of the three embryonic
hepatic arterial roots may vary with persistence
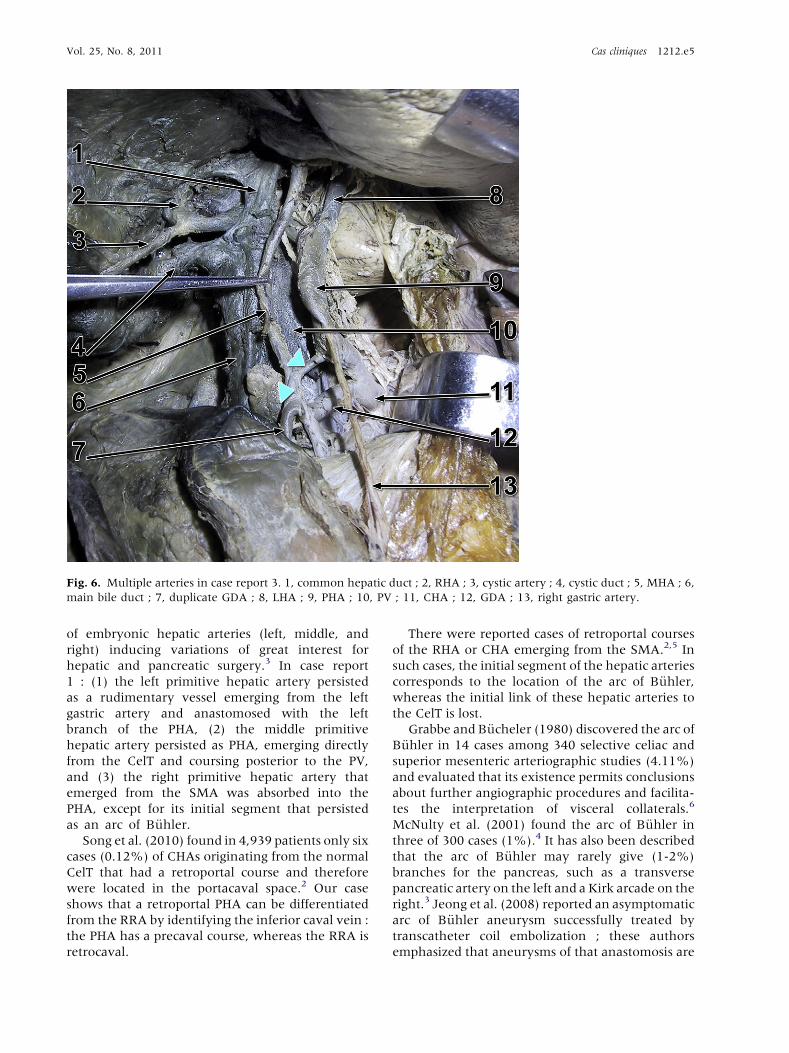
Fig. 6. Multiple arteries in case report 3. 1, common hepatic duct ; 2, RHA ; 3, cystic artery ; 4, cystic duct ; 5, MHA ; 6,
main bile duct ; 7, duplicate GDA ; 8, LHA ; 9, PHA ; 10, PV ; 11, CHA ; 12, GDA ; 13, right gastric artery.
Vol. 25, No. 8, 2011 Cas cliniques 1212.e5
of embryonic hepatic arteries (left, middle, and
right) inducing variations of great interest for
hepatic and pancreatic surgery.3 In case report
1 : (1) the left primitive hepatic artery persisted
as a rudimentary vessel emerging from the left
gastric artery and anastomosed with the left
branch of the PHA, (2) the middle primitive
hepatic artery persisted as PHA, emerging directly
from the CelT and coursing posterior to the PV,
and (3) the right primitive hepatic artery that
emerged from the SMA was absorbed into the
PHA, except for its initial segment that persisted
as an arc of B€uhler.Song et al. (2010) found in 4,939 patients only six
cases (0.12%) of CHAs originating from the normal
CelT that had a retroportal course and therefore
were located in the portacaval space.2 Our case
shows that a retroportal PHA can be differentiated
from the RRA by identifying the inferior caval vein :
the PHA has a precaval course, whereas the RRA is
retrocaval.
There were reported cases of retroportal courses
of the RHA or CHA emerging from the SMA.2,5 In
such cases, the initial segment of the hepatic arteries
corresponds to the location of the arc of B€uhler,whereas the initial link of these hepatic arteries to
the CelT is lost.
Grabbe and B€ucheler (1980) discovered the arc of
B€uhler in 14 cases among 340 selective celiac and
superior mesenteric arteriographic studies (4.11%)
and evaluated that its existence permits conclusions
about further angiographic procedures and facilita-
tes the interpretation of visceral collaterals.6
McNulty et al. (2001) found the arc of B€uhler in
three of 300 cases (1%).4 It has also been described
that the arc of B€uhler may rarely give (1-2%)
branches for the pancreas, such as a transverse
pancreatic artery on the left and a Kirk arcade on the
right.3 Jeong et al. (2008) reported an asymptomatic
arc of B€uhler aneurysm successfully treated by
transcatheter coil embolization ; these authors
emphasized that aneurysms of that anastomosis are
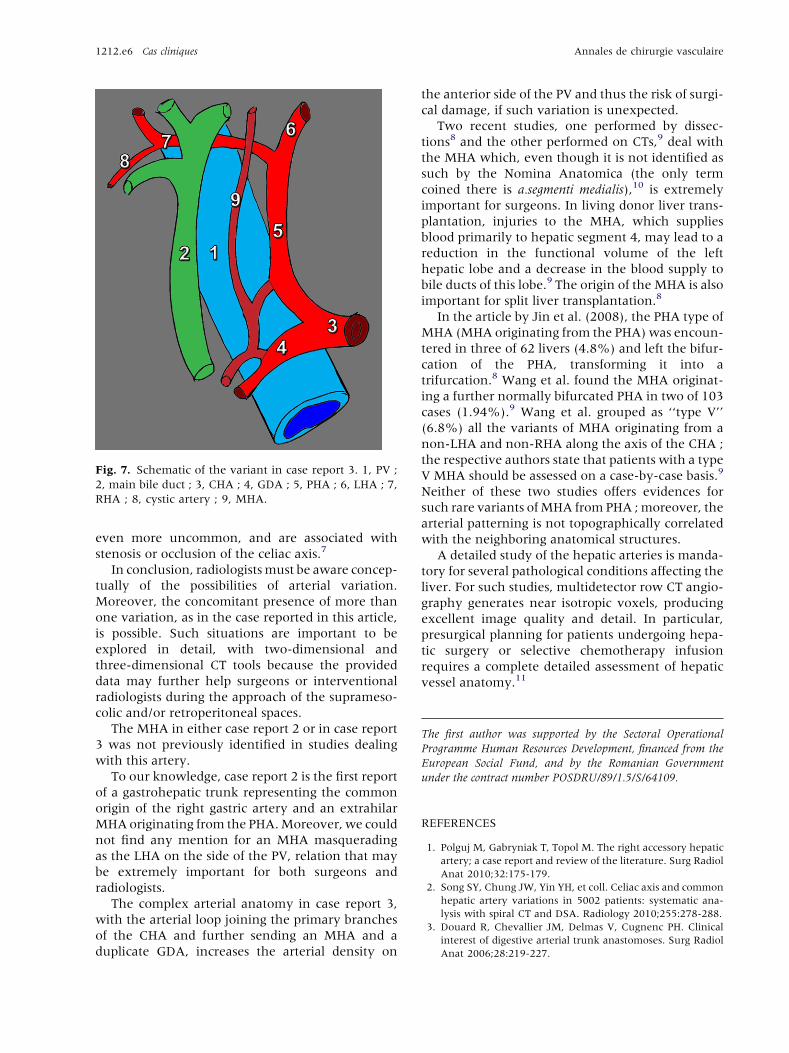
Fig. 7. Schematic of the variant in case report 3. 1, PV ;
2, main bile duct ; 3, CHA ; 4, GDA ; 5, PHA ; 6, LHA ; 7,
RHA ; 8, cystic artery ; 9, MHA.
1212.e6 Cas cliniques Annales de chirurgie vasculaire
even more uncommon, and are associated with
stenosis or occlusion of the celiac axis.7
In conclusion, radiologistsmust be aware concep-
tually of the possibilities of arterial variation.
Moreover, the concomitant presence of more than
one variation, as in the case reported in this article,
is possible. Such situations are important to be
explored in detail, with two-dimensional and
three-dimensional CT tools because the provided
data may further help surgeons or interventional
radiologists during the approach of the suprameso-
colic and/or retroperitoneal spaces.
The MHA in either case report 2 or in case report
3 was not previously identified in studies dealing
with this artery.
To our knowledge, case report 2 is the first report
of a gastrohepatic trunk representing the common
origin of the right gastric artery and an extrahilar
MHAoriginating from the PHA.Moreover, we could
not find any mention for an MHA masquerading
as the LHA on the side of the PV, relation that may
be extremely important for both surgeons and
radiologists.
The complex arterial anatomy in case report 3,
with the arterial loop joining the primary branches
of the CHA and further sending an MHA and a
duplicate GDA, increases the arterial density on
the anterior side of the PV and thus the risk of surgi-
cal damage, if such variation is unexpected.
Two recent studies, one performed by dissec-
tions8 and the other performed on CTs,9 deal with
the MHA which, even though it is not identified as
such by the Nomina Anatomica (the only term
coined there is a.segmenti medialis),10 is extremely
important for surgeons. In living donor liver trans-
plantation, injuries to the MHA, which supplies
blood primarily to hepatic segment 4, may lead to a
reduction in the functional volume of the left
hepatic lobe and a decrease in the blood supply to
bile ducts of this lobe.9 The origin of the MHA is also
important for split liver transplantation.8
In the article by Jin et al. (2008), the PHA type of
MHA (MHA originating from the PHA)was encoun-
tered in three of 62 livers (4.8%) and left the bifur-
cation of the PHA, transforming it into a
trifurcation.8 Wang et al. found the MHA originat-
ing a further normally bifurcated PHA in two of 103
cases (1.94%).9 Wang et al. grouped as ‘‘type V’’
(6.8%) all the variants of MHA originating from a
non-LHA and non-RHA along the axis of the CHA ;
the respective authors state that patients with a type
V MHA should be assessed on a case-by-case basis.9
Neither of these two studies offers evidences for
such rare variants ofMHA from PHA ;moreover, the
arterial patterning is not topographically correlated
with the neighboring anatomical structures.
A detailed study of the hepatic arteries is manda-
tory for several pathological conditions affecting the
liver. For such studies, multidetector row CT angio-
graphy generates near isotropic voxels, producing
excellent image quality and detail. In particular,
presurgical planning for patients undergoing hepa-
tic surgery or selective chemotherapy infusion
requires a complete detailed assessment of hepatic
vessel anatomy.11
The first author was supported by the Sectoral Operational
Programme Human Resources Development, financed from the
European Social Fund, and by the Romanian Government
under the contract number POSDRU/89/1.5/S/64109.
REFERENCES
1. Polguj M, Gabryniak T, Topol M. The right accessory hepatic
artery; a case report and review of the literature. Surg Radiol
Anat 2010;32:175-179.
2. Song SY, Chung JW, Yin YH, et coll. Celiac axis and common
hepatic artery variations in 5002 patients: systematic ana-
lysis with spiral CT and DSA. Radiology 2010;255:278-288.
3. Douard R, Chevallier JM, Delmas V, Cugnenc PH. Clinical
interest of digestive arterial trunk anastomoses. Surg Radiol
Anat 2006;28:219-227.

Vol. 25, No. 8, 2011 Cas cliniques 1212.e7
4. McNulty JG, Hickey N, Khosa F, O’Brien P, O’Callaghan JP.
Surgical and radiological significance of variants of B€uhler’sanastomotic artery: a report of three cases. Surg Radiol Anat
2001;23:277-280.
5. SponzaM, Pozzi Mucelli R, Pozzi Mucelli F. Arterial anatomy
of the celiac trunk and the superior mesenteric artery with
computerized tomography. Radiol Med 1993;86:260-267.
6. Grabbe E, B€ucheler E. B€uhler’s anastomosis. Rofo 1980;132:
541-546.
7. Jeong SJ, Lim NY, Jang NK, et coll. Transcatheter coil
embolization of an Arc of Buhler aneurysm. Korean J Radiol
2008;9(Suppl):S77-S80.
8. Jin GY, Yu HC, Lim HS, et coll. Anatomical variations of the
origin of the segment 4 hepatic artery and their clinical
implications. Liver Transpl 2008;14:1180-1184.
9. Wang S, He X, Li Z, et coll. Characterization of the middle
hepatic artery and its relevance to living donor liver trans-
plantation. Liver Transpl 2010;16:736-741.
10. Feneis H, Dauber W. Pocket Atlas of Human Anatomy Based
on the International Nomenclature. 4th ed. Stuttgart,
Germany: Thieme, 2000.
11. Saba L, Mallarini G. Multidetector row CT angiography in
the evaluation of the hepatic artery and its anatomical
variants. Clin Radiol 2008;63:312-321.