Embed Size (px)
Citation preview

Complications aiguës et chroniques liées aux nouveaux produits
H. Donnadieu-Rigole
Département d’addictologie
CHU Montpellier
Cet intervenant :
a déclaré ses liens d’intérêt
Tous les orateurs ont reçu une déclaration de liens d’intérêt.
Les NPS « New Psychoactive substances »
• Cathinones/Cannabis de synthèse/GHB/BZD/opiacés…
• 100 nouvelles substances /an
• Au moins 200 articles sur Pubmed de
janvier 2015 à avril 2016…
Plan
• Complications aigues somatiques
• Complications chroniques
• Complications liées au mode d’administration
Complications aiguesCathinones
Cannabis de synthèse
Synthetic Cathinones: A New Public Health Problem Current Neuropharmacology, 2015, Vol. 13, No. 1 13
Table 1. Molecular structure of the most spread synthetic cathinones.
Usual Names Equivalent Names Chemical Names Formula Structure
Butylone β-keto-N-
methylbenzodioxolylbutanamine,
bk-MBDB
1-(1,3-benzodioxol-5-yl)-2-
(methylamino)butan-1-one
C12H15NO3
Ethcathinone Ethylpropion, Eth-Cat (RS)-2-ethylamino-1-phenyl-
propan-1-one
C11H15NO
Ethylone 3,4-methylenedioxy-N-
ethylcathinone, MDEC,
bk-MDEA
(RS)-1-(1,3-benzodioxol-5-yl)-2-
(ethylamino)propan-1-one
C12H15NO3
3-Fluoromethcathinone 3-FMC (RS)-1-(3-Fluorophenyl)-2-
methylaminopropan-1-one
C10H12FNO
4-Fluoromethcathinone 4-FMC (RS)-1-(4-Fluorophenyl)-2-
methylaminopropan-1-one
C10H12FNO
Buphedrone α-methylamino-butyrophenone,
MABP
2-(methylamino)-1-phenylbutan-
1-one
C11H15NO
Mephedrone 4-methylmethcathinone, MMC,
4-MMC
(RS)-2-methylamino-1-
(4-methylphenyl)propan-1-one
C11H15NO
Methcathinone α-methylamino-propiophenone,
ephedrine, Cath, Jeff
(RS)-2-(methylamino)-1-phenyl-
propan-1-one
C10H13NO
Methedrone para-methoxymethcathinone,
4-methoxymethcathinone,
bk-PMMA, PMMC,
methoxyphedrine, meow meow
(RS)-1-(4-methoxyphenyl)-2-
(methylamino)propan-1-one
C11H15NO2
MDPV Methylenedioxypyrovalerone (RS)-1-(Benzo[d][1,3]
dioxol-5-yl)-2-(pyrrolidin-
1-yl)pentan-1-one
C16H21NO3
Methylone 3,4-
methylenedioxymethcathinone
(±)-2-Methylamino-1-
(3,4-methylenedioxyphenyl)
propan-1-one
C11H13NO3
Naphyrone Naphthylpyrovalerone, O-2482 (RS)-1-naphthalen-2-yl-2-
pyrrolidin-1-ylpentan-1-one
C19H23NO
Pentedrone 2-(methylamino)-1-
phenylpentan-1-one,
α-methylamino-valerophenone
(±)-1-phenyl-2-
(methylamino)pentan-1-one
C12H17NO
Pyrovalerone Centroton, 4-methyl-β-ketone-
prolintane, Thymergix, O-2371
(RS)-1-(4-methylphenyl)-2-
(1-pyrrolidinyl)pentan-1-one
C16H23NO
Karila et al. 2015
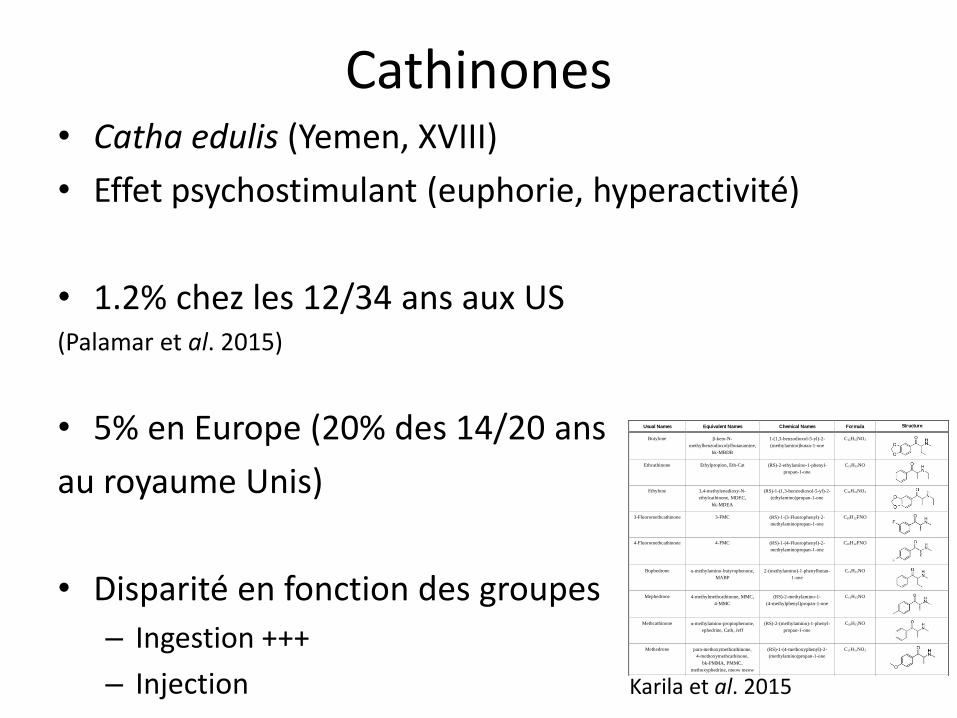
Cathinones• Catha edulis (Yemen, XVIII)
• Effet psychostimulant (euphorie, hyperactivité)
• 1.2% chez les 12/34 ans aux US (Palamar et al. 2015)
• 5% en Europe (20% des 14/20 ans
au royaume Unis)
• Disparité en fonction des groupes
– Ingestion +++
– Injection
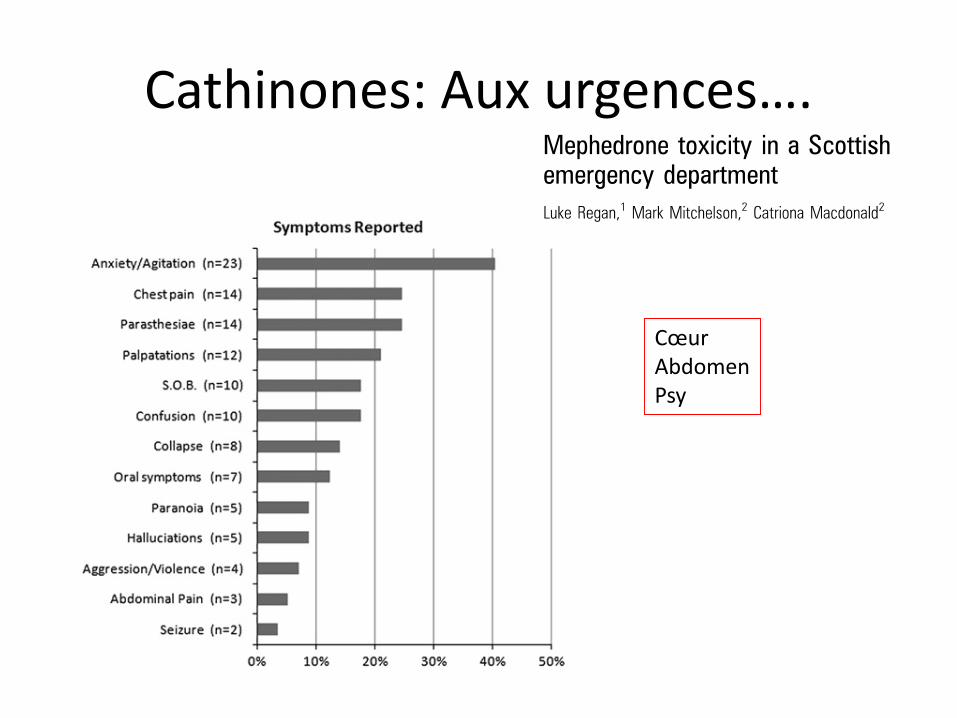
Cathinones: Aux urgences….
CœurAbdomenPsy
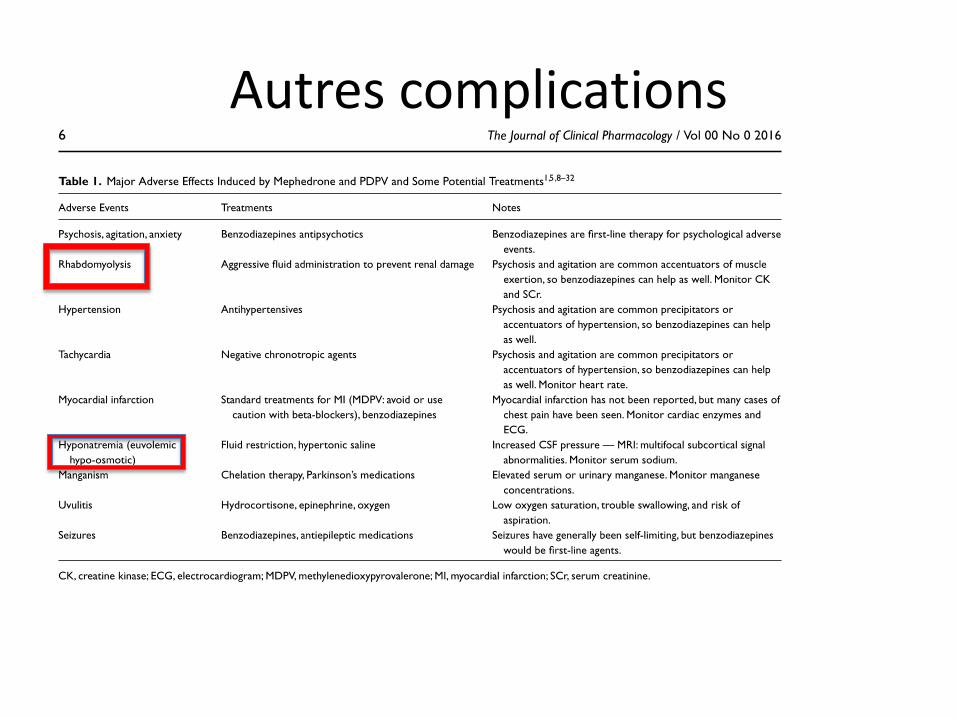
Autres complications
Hyponatrémie/Rhabdomyolyse
Hyponatrémié sévère avec épilepsie après LSD •SIADH (Médié par le système serotoninergique)•Rabdomyolyse
ReinionogrammeMuscles…
Et aussi….
• Hyper ou hypothermie/ en fonction de l’environnement thermique
• Cystites amicrobiennes destructrices
Cannabis de synthèse
• Plus d’affinité pour les récepteurs CB1
• Pas de tabac ou de THC
• <1% en population générale
• 4000 cas dans la littérature: 26 décès
– Effets psychiatriques
– Effets indésirables
– sympathomimétiques
– hallucinogènes
Karila et al. 2016 Tait et al. 2015
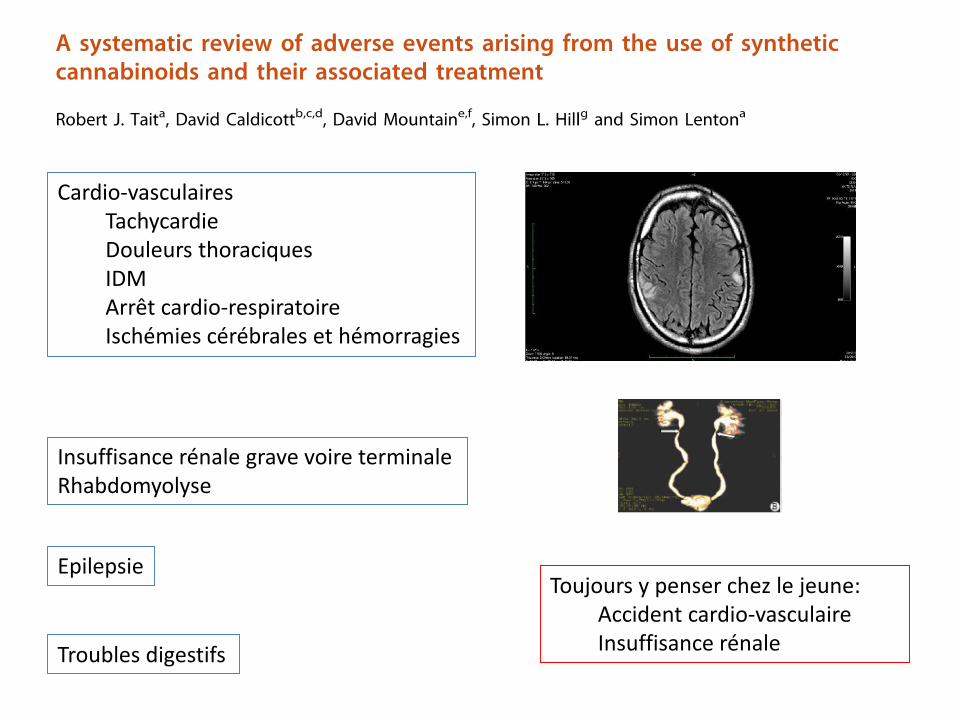
Cardio-vasculairesTachycardieDouleurs thoraciquesIDMArrêt cardio-respiratoireIschémies cérébrales et hémorragies
Toujours y penser chez le jeune:Accident cardio-vasculaireInsuffisance rénale
Insuffisance rénale grave voire terminaleRhabdomyolyse
Epilepsie
Troubles digestifs
Atteinte Uro-néphrologique
« Cystite amicrobienne ? (Chu et coll., 2009)
«Destruction app. urinaire inférieur» Kétamine «chronique»
Hydronéphrose bilatérale
Risque de diabète ?(Wong, 2012)
Dans l’avenir, quel risque d’insuffisance rénale terminale ?????
Phénacétine (produit de coupe) IV avec cocaïne IV
‘’
sniff
Messages
Toujours y penser
• Assurer les fonctions vitales– USI
– Remplissage
– BZD
– Traitements symptomatiques
Pièges
• Produit annoncé comme consommé par l’usager
• Associations fréquentes de différents produits– Alcool
– Cocaïne
– Sildenafil
– Produits de coupe

COMPLICATIONS CHRONIQUES
La dépendance
– Craving
– phénomène de tolérance aigue
– Un syndrome de sevrage (tremblements, frissons, hypothermie)
– Affaissement des relations sociales
– Impact sur la libido
Transmission hépatite C et B=Injection de NPS
HCV
• Usage de drogue par voie IV – Plus gros pourvoyeur de
transmission
– 10 millions dans le monde
– 40 à 80% de séroprévalence en fonction des pays
HBV
• 5 à 10 % de séroprévalence suivant les pays
• Ag HBS (0.3 à 2.7 millions)
The epidemiology of viral hepatitis among people who inject
drugs: Results of global systematic reviews
Paul Nelson, Bradley Mathers, Benjamin Cowie, Holly Hagan, Don Des Jarlais, Danielle
Horyniak, and Louisa Degenhardt
National Drug and Alcohol Research Centre, University of New South Wales, Sydney, NSW,
Australia (P K Nelson MHSc, B M Mathers MBChB); Victorian Infectious Diseases Reference
Laboratory, North Melbourne, VIC, Australia (B Cowie PhD); College of Nursing, New York
University, New York, NY, USA (H Hagan PhD); Beth Israel Medical Center, New York, NY, USA
(Prof D Des Jarlais PhD); Centre for Population Health, Burnet Institute, Melbourne, VIC,
Australia (D Horyniak BBioMedSci, Prof L Degenhardt PhD); and Centre for Health Policy,
Programs and Economics, School of Population Health, University of Melbourne, Melbourne, VIC,
Australia (L Degenhardt)
Abstract
Background—Injecting drug use (IDU) is an important risk for viral hepatitis transmission.
Detailed, transparent estimates of the scale of the problem at regional and global levels have never
been made. We report national, regional and global prevalence and population size estimates for
hepatitis C (HCV) and hepatitis B (HBV) among people who inject drugs.
Methods—Systematic search of peer-reviewed (Medline/Embase/PsycINFO) and grey literature
databases, conference abstracts and online resources, with a widely distributed call for additional
data. From 4386 peer-reviewed and 1019 grey literature sources, 1125 were reviewed in full.
Studies were extracted to a customised database and graded according their methods. Serological
reports of HCV antibodies/anti-HCV, HBV antibodies/anti-HBc, and/or HBV surface antigen/
HBsAg among IDUs samples with n>40 participants, <100% HIV-positive, and sampling frames
that did not exclude participants on the basis of age or sex were included. Using endorsed decision
rules, prevalence estimates were calculated with anti-HCV and anti-HBV as proxies for exposure
and HBsAg for current infection. These were combined with IDU population sizes to estimate the
number of HBV and HCV positive IDUs.
Findings—Eligible reports of anti-HCV among IDUs were located for 77 countries. Prevalence
was 60–80% in 26 countries and >80% in 12. We estimate worldwide about 10.0 million (range
6.0–15.2M) IDUs might be anti-HCV positive. China, (1.6M), the USA (1.5M) and the Russian
Correspondence to: Prof Louisa Degenhardt, Centre for Population Health, Burnet Institute, 85 Commercial Road, Melbourne, VIC3004, Australia, [email protected].
Contributions
PN & LD developed the overall methodology for use in the reviews. HH and DDJ developed the methodology and oversaw data
extraction for the HCV Synthesis Project, and provided this for use in this review. DH maintained the customised database. PN & DH
conducted literature searches, extracted data and provisionally selected reports for use in generating estimates. PN & LD decided on
the final set of reports, with advice from BC; these were reviewed by HH, DDJ, DH & BM. BM developed the methodology and
generated regional and global estimates; these were reviewed by PN & LD. PN & LD led the writing of the manuscript; HH, DDJ,
DH, BC & BM commented and contributed text. PN generated the maps. All authors had access to all data used in this review. All
authors gave approval for the manuscript to be submitted.
Conflicts of interest
LD and BM have received grant money and have acted as independent consultants to the World Health Organization, UNAIDS and
the United Nations Office on Drugs and Crime. DDJ has been funded by, and acted as a consultant to, the WHO. LD received an
untied educational grant (2006–2008) from Reckitt Benckiser to conduct a post-marketing surveillance study of buprenorphine-
naloxone in the treatment of heroin dependence in Australia.
NIH Public AccessAuthor ManuscriptLancet. Author manuscript; available in PMC 2012 August 13.
Published in final edited form as:
Lancet. 2011 August 13; 378(9791): 571–583. doi:10.1016/S0140-6736(11)61097-0.
NIH
-PA
Auth
or M
anu
scrip
tN
IH-P
A A
uth
or M
an
uscrip
tN
IH-P
A A
uth
or M
an
uscrip
t
The epidemiology of viral hepatitis among people who inject
drugs: Results of global systematic reviews
Paul Nelson, Bradley Mathers, Benjamin Cowie, Holly Hagan, Don Des Jarlais, Danielle
Horyniak, and Louisa Degenhardt
National Drug and Alcohol Research Centre, University of New South Wales, Sydney, NSW,
Australia (P K Nelson MHSc, B M Mathers MBChB); Victorian Infectious Diseases Reference
Laboratory, North Melbourne, VIC, Australia (B Cowie PhD); College of Nursing, New York
University, New York, NY, USA (H Hagan PhD); Beth Israel Medical Center, New York, NY, USA
(Prof D Des Jarlais PhD); Centre for Population Health, Burnet Institute, Melbourne, VIC,
Australia (D Horyniak BBioMedSci, Prof L Degenhardt PhD); and Centre for Health Policy,
Programs and Economics, School of Population Health, University of Melbourne, Melbourne, VIC,
Australia (L Degenhardt)
Abstract
Background—Injecting drug use (IDU) is an important risk for viral hepatitis transmission.
Detailed, transparent estimates of the scale of the problem at regional and global levels have never
been made. We report national, regional and global prevalence and population size estimates for
hepatitis C (HCV) and hepatitis B (HBV) among people who inject drugs.
Methods—Systematic search of peer-reviewed (Medline/Embase/PsycINFO) and grey literature
databases, conference abstracts and online resources, with a widely distributed call for additional
data. From 4386 peer-reviewed and 1019 grey literature sources, 1125 were reviewed in full.
Studies were extracted to a customised database and graded according their methods. Serological
reports of HCV antibodies/anti-HCV, HBV antibodies/anti-HBc, and/or HBV surface antigen/
HBsAg among IDUs samples with n>40 participants, <100% HIV-positive, and sampling frames
that did not exclude participants on the basis of age or sex were included. Using endorsed decision
rules, prevalence estimates were calculated with anti-HCV and anti-HBV as proxies for exposure
and HBsAg for current infection. These were combined with IDU population sizes to estimate the
number of HBV and HCV positive IDUs.
Findings—Eligible reports of anti-HCV among IDUs were located for 77 countries. Prevalence
was 60–80% in 26 countries and >80% in 12. We estimate worldwide about 10.0 million (range
6.0–15.2M) IDUs might be anti-HCV positive. China, (1.6M), the USA (1.5M) and the Russian
Correspondence to: Prof Louisa Degenhardt, Centre for Population Health, Burnet Institute, 85 Commercial Road, Melbourne, VIC3004, Australia, [email protected].
Contributions
PN & LD developed the overall methodology for use in the reviews. HH and DDJ developed the methodology and oversaw data
extraction for the HCV Synthesis Project, and provided this for use in this review. DH maintained the customised database. PN & DH
conducted literature searches, extracted data and provisionally selected reports for use in generating estimates. PN & LD decided on
the final set of reports, with advice from BC; these were reviewed by HH, DDJ, DH & BM. BM developed the methodology and
generated regional and global estimates; these were reviewed by PN & LD. PN & LD led the writing of the manuscript; HH, DDJ,
DH, BC & BM commented and contributed text. PN generated the maps. All authors had access to all data used in this review. All
authors gave approval for the manuscript to be submitted.
Conflicts of interest
LD and BM have received grant money and have acted as independent consultants to the World Health Organization, UNAIDS and
the United Nations Office on Drugs and Crime. DDJ has been funded by, and acted as a consultant to, the WHO. LD received an
untied educational grant (2006–2008) from Reckitt Benckiser to conduct a post-marketing surveillance study of buprenorphine-
naloxone in the treatment of heroin dependence in Australia.
NIH Public AccessAuthor ManuscriptLancet. Author manuscript; available in PMC 2012 August 13.
Published in final edited form as:
Lancet. 2011 August 13; 378(9791): 571–583. doi:10.1016/S0140-6736(11)61097-0.
NIH
-PA
Au
thor M
an
uscrip
tN
IH-P
A A
uth
or M
an
uscrip
tN
IH-P
A A
uth
or M
an
uscrip
t
Priorité pour le traitement anti HCV
Transmission HIV
Risque augmenté
• HSH
• Augmentation du risque si injection cathinones (Giese et
al.2015)
– Irlande
– Roumanie
– Grèce
Prévention
• Echanges de seringues
• Salles d’injections sécurisées
• ETP autour de la réduction des risques
(MacArthur et al. 2014)
Cannabis de synthèse
• Altération des fonctions cognitives (Bossong et al.
2010) , Cancers
• Augmentation du risque d’usage problématique du cannabis de synthèse (Blevins
et al. 2016)
– Augmentation de conséquences psycho-sociales
Complications liées au mode d’administration
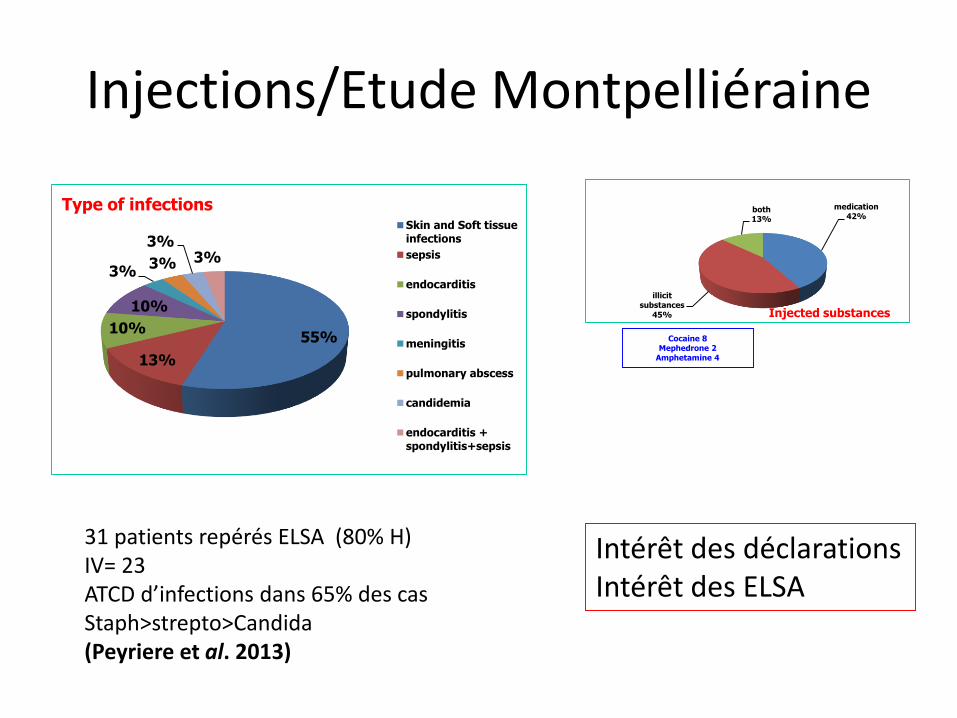
Injections/Etude Montpelliéraine
55%
13%
10%
10%
3%3%
3%3%
Type of infectionsSkin and Soft tissueinfections
sepsis
endocarditis
spondylitis
meningitis
pulmonary abscess
candidemia
endocarditis +spondylitis+sepsis
medication42%
illicit substances
45%
both13%
Injected substances
Cocaine 8Mephedrone 2
Amphetamine 4
31 patients repérés ELSA (80% H)IV= 23ATCD d’infections dans 65% des casStaph>strepto>Candida (Peyriere et al. 2013)
Intérêt des déclarations Intérêt des ELSA
Les injections
• Bactériémie à Staph. Aureus
– Augmentation avec les NPS depuis 2013
– Augmentation des abcès pulmonaires
– Augmentation des endocardites
Staphylococcus aureusbacteraemia associated with injected newpsychoactive substances
D . J. GRI FFI TH 1* , C. L . M A CK I N TOSH 1A N D D . I N VERA RI TY 2
1Regional Infectious Diseases Unit, Western General Hospital, Edinburgh, UK2Department of M icrobiology, Royal Infirmary of Edinburgh, UK
Received 4 July 2015; Final revision 14 October 2015; Accepted 14 October 2015;
first published online 9 November 2015
SUM M ARY
Injecting drug use is often associated with deep-seated infection. In Lothian in Scotland there has
been a recent increase in the use of injected new psychoactive substances (NPS). Patients who
have injected NPS have presented with Staphylococcus aureus bacteraemia (SAB) with life-
threatening complications. We describe a unique case-series of 14 episodes of SAB in ten
patients. Users of injected NPS had a significantly higher incidence of endocarditis and cavitating
pulmonary lesions (P < 0·05) compared to those who inject only opiates. Cases of SAB in people
who inject NPS have contributed to a significant rise in the overall incidence of SAB in people
who inject drugs (P < 0·05) which has in turn impacted on the ability of Lothian to meet national
targets for reducing the incidence of SAB.
Key words: Bloodstream infections, endocarditis, injecting drug use, pulmonary abscess
Staphylococcus aureus.
I NT RODUCT I ON
In recent yearstherehasbeen a rapid increasein theuse
of new psychoactive substances (NPS) by people who
inject drugs (PWID) in Scotland [1]. These includesev-
eral different classesof active ingredient, including syn-
thetic cannabinoids and synthetic cathinones [2].
Although some of these substances have been made il-
legal in certain jurisdictions, there remains a wide var-
iety of subtly altered variants that have not yet been
legislated against and have indeed been manufactured
deliberately to circumvent existing laws [3]. Prior to
2009, NPS were not reported as a factor, causative or
not, in any deaths related to drugs in Scotland. Since
then there has been an increasing number seen, with
113 deaths in 2013 mentioning NPS as a factor [1].
NPS can be purchased in Scotland through many
routes, including directly from dealers, internet mar-
keting and retail outlets (‘head shops’). They have
been adopted by many PWID as alternatives to
more traditional drugs of misuse such as opiates
owing to their availability, legality, relatively low
cost and perceived safety [2, 4, 5].
Among PWID, some NPS are referred to as ‘bath
salts’ due to their visual similarity to bathing salts
[2, 4]. One such substance known as ‘Burst’ is a
NPS that was popular in the Lothian area of South
East Scotland during the study period [Scottish
Drugs Forum (SDF), personal communication], a
population of about 830 000 served by NHS Lothian
[6]. Although ‘bath salts’ typically contain synthetic
cathinones, related to an amphetamine analogue
derived from the plant Catha edulis (khat) [2, 4, 7],
the ingredients found in ‘Burst’ tend to be more vari-
able. During the period of this study, methioprop-
amine (MPA), butylone and ethylphenidate were
known to be in local circulation in ‘Burst’ (SDF,
* Author for correspondence: Dr D. J. Griffith, Regional InfectiousDiseases Unit, Western General Hospital, Crewe Road, EdinburghEH4 2XU, UK.(Email: [email protected])
Epidemiol. Infect. (2016), 144, 1257–1266. © Cambridge University Press 2015
doi:10.1017/S095026881500271X
Epidemiol. Infect. (2016), 144, 1257–1266.
Parachutes ou « Body stuffing »
• Recherche d’effets prolongés = Effets retardés inattendus (Hendrickson et al. 2006)
• Methamphetamines dans un sachet (cavité corporelle) = effets secondaires majeurs
Le SLAM
• Augmentation du risque de transmission des MST
• Augmentation des hépatites C aigues
(Croi 2016, Abstract 675)
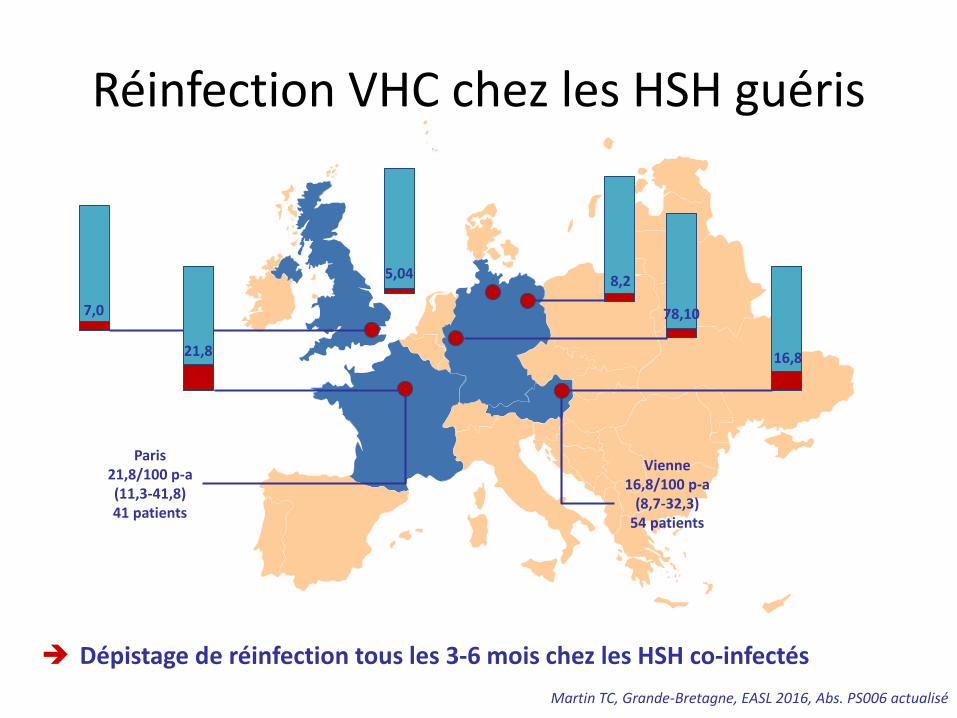
Réinfection VHC chez les HSH guéris
Dépistage de réinfection tous les 3-6 mois chez les HSH co-infectés
Martin TC, Grande-Bretagne, EASL 2016, Abs. PS006 actualisé
7,0
21,8
5,04 8,2
78,10
16,8
Vienne16,8/100 p-a
(8,7-32,3)54 patients
Paris21,8/100 p-a(11,3-41,8)41 patients
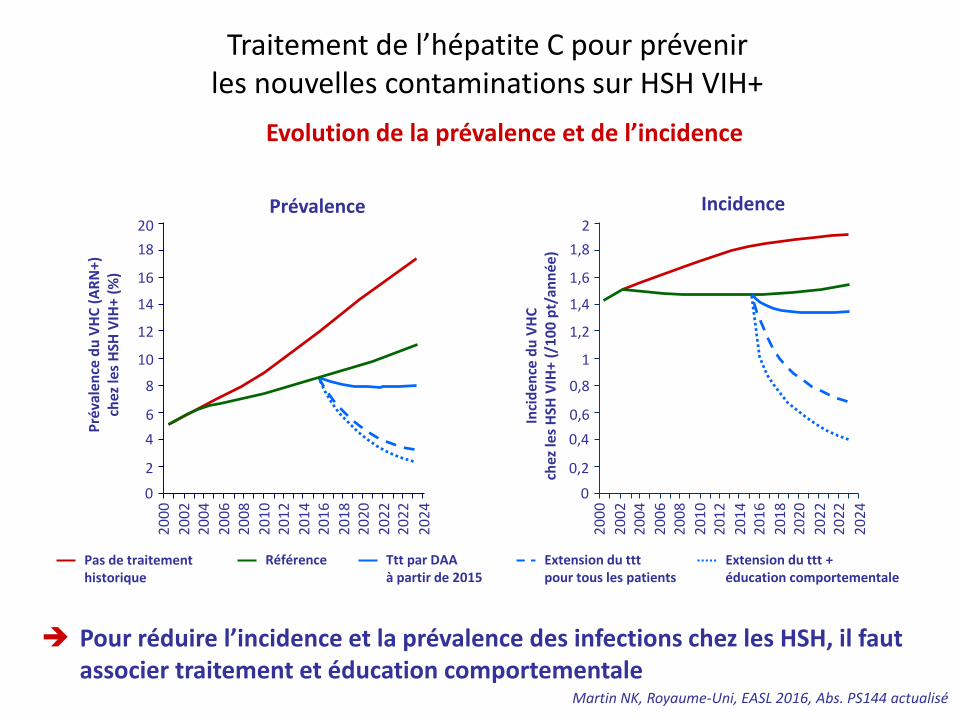
Traitement de l’hépatite C pour prévenir les nouvelles contaminations sur HSH VIH+
Martin NK, Royaume-Uni, EASL 2016, Abs. PS144 actualisé
Evolution de la prévalence et de l’incidence
Pour réduire l’incidence et la prévalence des infections chez les HSH, il faut associer traitement et éducation comportementale
Prévalence Incidence
Pré
vale
nce
du
VH
C (
AR
N+)
chez
les
HSH
VIH
+ (%
)
0
2
6
8
12
16
18
20
4
10
14
20
00
20
02
20
04
20
06
20
08
20
10
20
12
20
14
20
16
20
18
20
20
20
22
20
22
20
24
Inci
den
ce d
u V
HC
chez
les
HSH
VIH
+ (/
10
0 p
t/an
née
)
0
0,2
0,6
0,8
1,2
1,6
1,8
2
0,4
1
1,4
20
00
20
02
20
04
20
06
20
08
20
10
20
12
20
14
20
16
20
18
20
20
20
22
20
22
20
24
Pas de traitementhistorique
Référence Ttt par DAAà partir de 2015
Extension du tttpour tous les patients
Extension du ttt +éducation comportementale
Conclusion
• Toujours l’évoquer, le rechercher et le déclarer
• Suivi addictologique à préconiser
• Messages de prévention et d’information
Dominique A « vers le bleu »