Embed Size (px)
Citation preview
Hémostatiques
Charles Marc SAMAMAServices d’Anesthésie-Réanimation
Cochin - Hôtel-Dieu de Paris
DDAVP
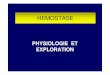
vWF Desmopressine (DDAVP)
• hémostatique
– passage du Willebrand dans la circulation plasmatique
– 200 à 300% du taux de base de vWF
– 300 à 400% du taux de base de facteur VIII
• libération de tPA par la cellule endothéliale
Desmopressine (DDAVP)
• demi-vie plasmatique : 1 h
• délai d’action : 30 min
• durée de l’effet : 8 h
• modes d’administration IV, IM, SC et IN
• forme IV (Minirin®): 0,3 µg/kg en 20 min (sérum salé)
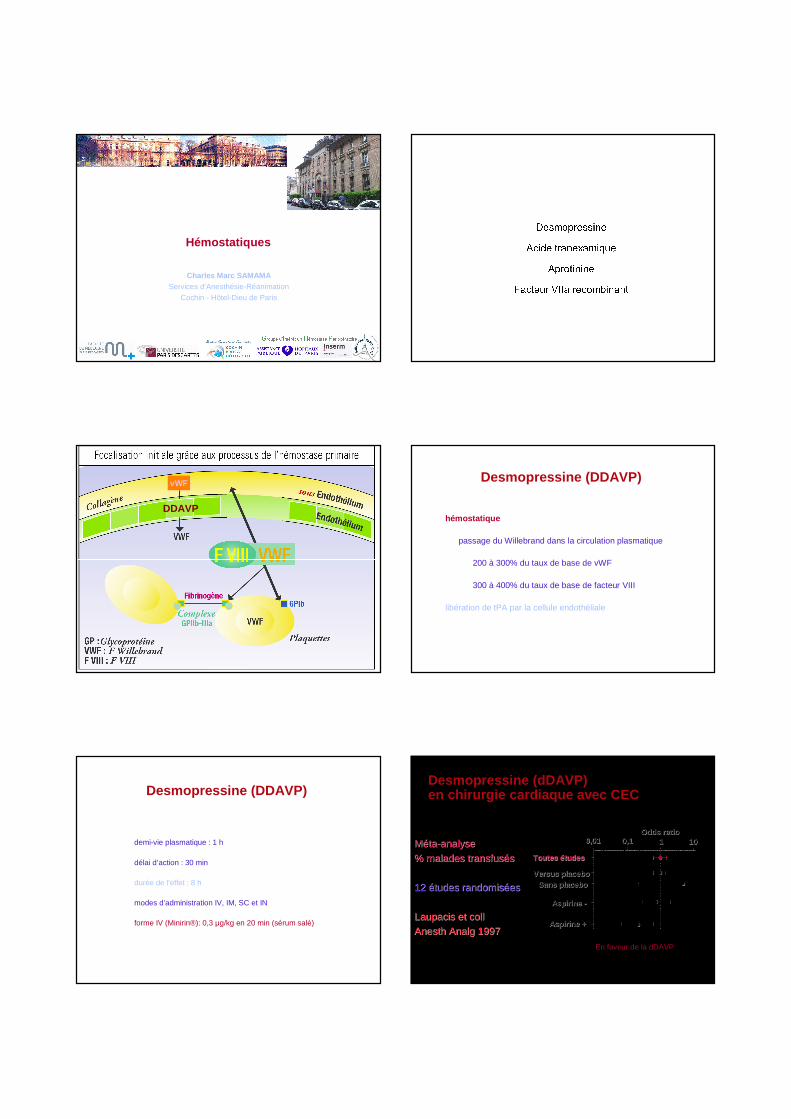
Desmopressine (dDAVP) en chirurgie cardiaque avec CEC
MMéétata--analyseanalyse
% malades transfus% malades transfusééss
12 12 éétudes randomistudes randomisééeses
Laupacis et collLaupacis et coll
Anesth Analg 1997Anesth Analg 1997
Toutes Toutes éétudestudes
Versus placeboVersus placeboSans placeboSans placebo
Aspirine Aspirine --
Aspirine +Aspirine +
0,010,01 0,10,1 11 1010Odds ratioOdds ratio
En faveur de la dDAVP
Mannucci P, Thromb Haemost 2001; 86: 149-53
Willebrand disease
•• Synthetic agentSynthetic agent
•• Low molecular weightLow molecular weight
• Binds to plasminogen and plasmin, and prevents
binding to the lysine binding sites of fibrinogen
•• No biotransformationNo biotransformation
• Short elimination half-life, but duration of the effect
unknown
• Low cost
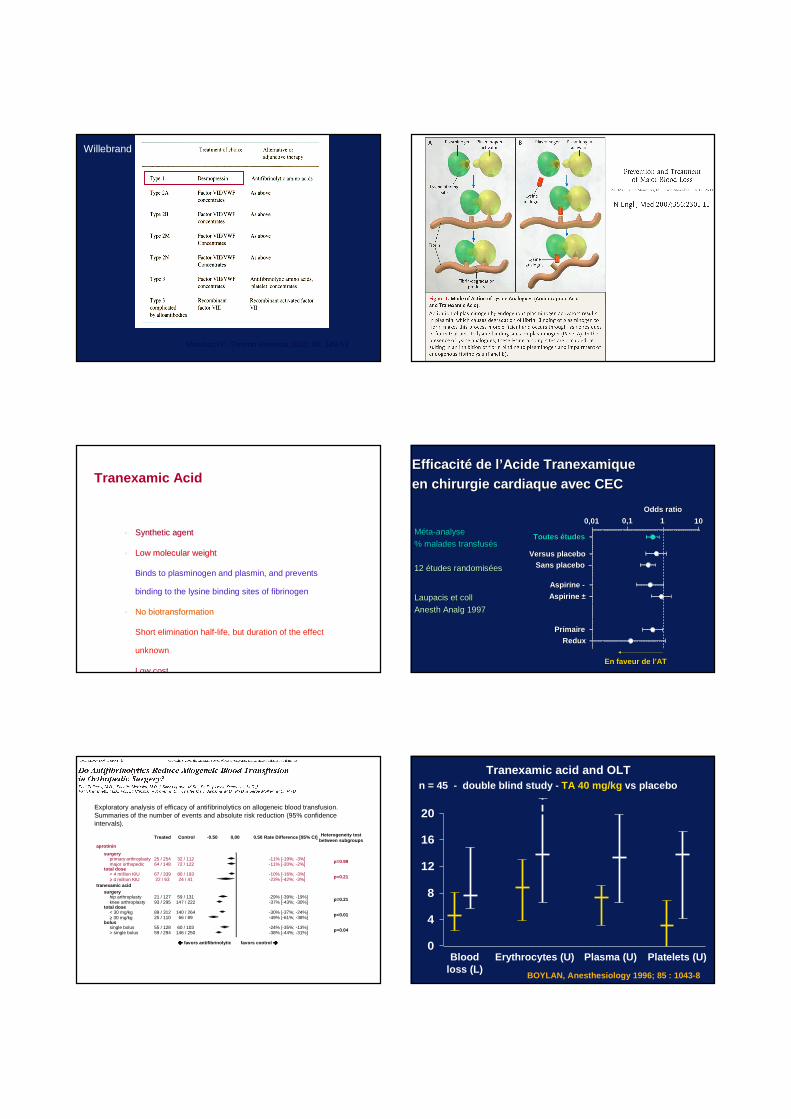
Tranexamic AcidEfficacitEfficacit éé de lde l ’’Acide Tranexamique Acide Tranexamique en chirurgie cardiaque avec CECen chirurgie cardiaque avec CEC
MMéétata--analyseanalyse
% malades transfus% malades transfusééss
12 12 éétudes randomistudes randomisééeses
Laupacis et collLaupacis et coll
Anesth Analg 1997Anesth Analg 1997
Toutes Toutes éétudestudes
Versus placeboVersus placebo
Sans placeboSans placebo
Aspirine Aspirine --
Aspirine Aspirine ±±
PrimairePrimaire
ReduxRedux
0,010,01 0,10,1 11 1010Odds ratioOdds ratio
En faveur de lEn faveur de l ’’ATAT
Treated Control Rate Difference [95% CI] Heterogeneity testbetween subgroups
p=0.99primary arthroplasty 25 / 254 32 / 112 -11% [-19%; -3%]major orthopedic 64 / 148 72 / 122 -11% [-20%; -2%]
p=0.21< 4 million KIU 67 / 339 80 / 193 -10% [-16%; -3%]≥ 4 million KIU 22 / 63 24 / 41 -23% [-42%; -3%]
-0.50 0,00 0.50
p=0.21
surgery
aprotinin
total dose
tranexamic acidsurgery
21 / 127 59 / 131 -29% [-39%; -19%]93 / 295 147 / 222 -37% [-43%; -30%]
hip arthroplastyknee arthroplasty
89 / 312 140 / 264 -30% [-37%; -24%]25 / 110 66 / 89 -49% [-61%; -38%]
< 30 mg/kg≥ 30 mg/kg
total dose
55 / 128 60 / 103 -24% [-35%; -13%]59 / 294 146 / 250 -38% [-44%; -31%]
single bolus> single bolus
bolus
+
p<0.01
p=0.04
���� favors antifibrinolytic favors control ����
Exploratory analysis of efficacy of antifibrinolytics on allogeneic blood transfusion. Summaries of the number of events and absolute risk reduction (95% confidence intervals).
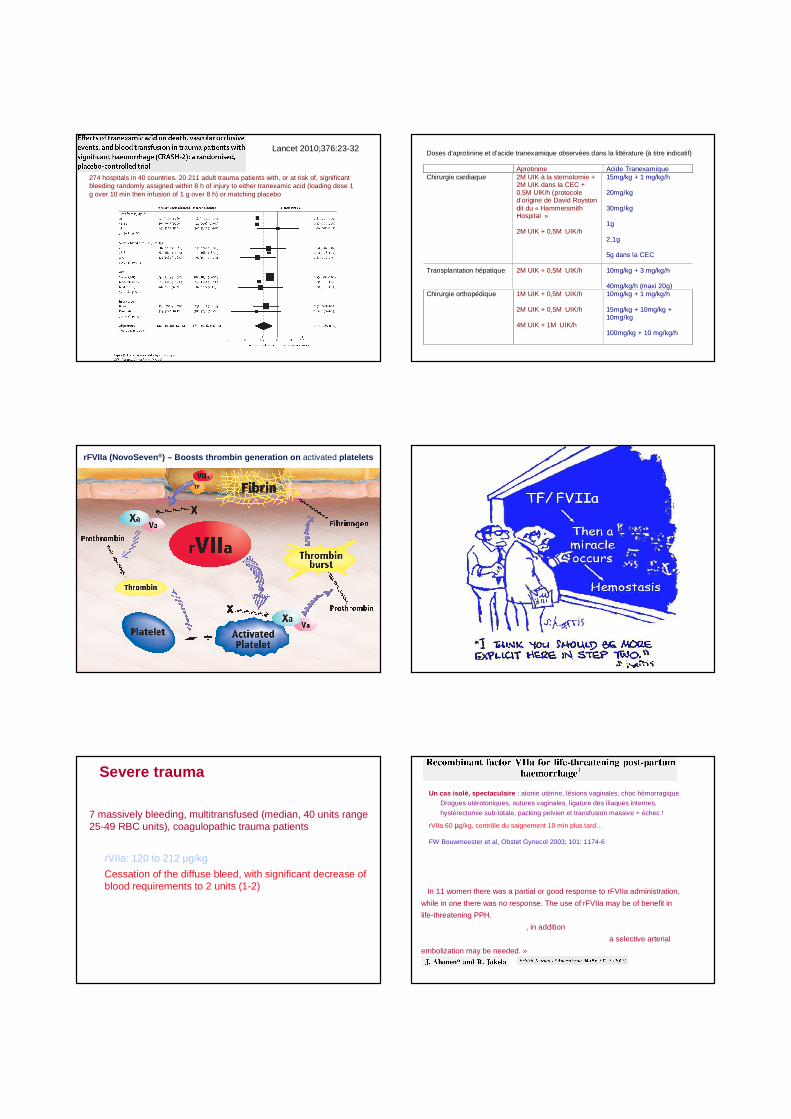
Tranexamic acid and OLT
0
4
8
12
16
20
Bloodloss (L)
Erythrocytes (U) Plasma (U) Platelets (U)
n = 45 - double blind study - TA 40 mg/kg vs placebo
BOYLAN, Anesthesiology 1996; 85 : 1043-8
Lancet 2010;376:23-32
274 hospitals in 40 countries. 20 211 adult trauma patients with, or at risk of, significant bleeding randomly assigned within 8 h of injury to either tranexamic acid (loading dose 1 g over 10 min then infusion of 1 g over 8 h) or matching placebo
Doses d’aprotinine et d’acide tranexamique observées dans la littérature (à titre indicatif) Aprotinine Acide Tranexamique Chirurgie cardiaque 2M UIK à la sternotomie +
2M UIK dans la CEC + 0,5M UIK/h (protocole d’origine de David Royston dit du « Hammersmith Hospital » 2M UIK + 0,5M UIK/h
15mg/kg + 1 mg/kg/h 20mg/kg 30mg/kg 1g 2,1g 5g dans la CEC
Transplantation hépatique 2M UIK + 0,5M UIK/h 10mg/kg + 3 mg/kg/h 40mg/kg/h (maxi 20g)
Chirurgie orthopédique 1M UIK + 0,5M UIK/h 2M UIK + 0,5M UIK/h 4M UIK + 1M UIK/h
10mg/kg + 1 mg/kg/h 15mg/kg + 10mg/kg + 10mg/kg 100mg/kg + 10 mg/kg/h
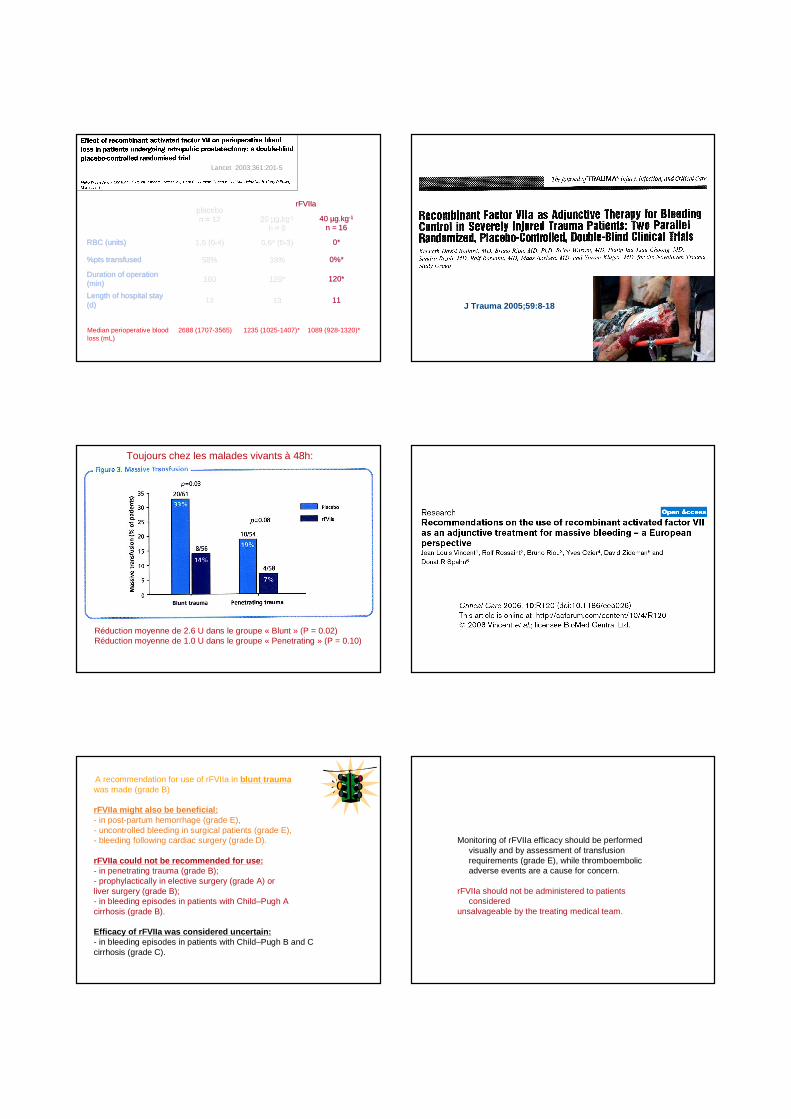
rFVIIa (NovoSeven ®) – Boosts thrombin generation on activated platelets
Severe traumaMartinowitz et al., J Trauma 2001;51 :431-39
7 massively bleeding, multitransfused (median, 40 units range 25-49 RBC units), coagulopathic trauma patients
rVIIa: 120 to 212 µg/kg
Cessation of the diffuse bleed, with significant decrease of blood requirements to 2 units (1-2)
Three of the seven patients died of reasons other than bleeding or thromboembolism
Un cas isolé, spectaculaire : atonie utérine, lésions vaginales, choc hémorragique.
Drogues utérotoniques, sutures vaginales, ligature des iliaques internes,
hystérectomie sub-totale, packing pelvien et transfusion massive = échec !
rVIIa 60 µµg/kg, contrôle du saignement 10 min plus tard…
FW Bouwmeester et al, Obstet Gynecol 2003; 101: 1174-6
« In 11 women there was a partial or good response to rFVIIa administration,
while in one there was no response. The use of rFVIIa may be of benefit in
life-threatening PPH.
However, treatment with rFVIIa, in addition to standard surgical and medical
interventions, may not be definitive in every patient and a selective arterial
embolization may be needed. »
placeboplacebon = 12n = 12
rFVIIarFVIIa
20 20 µµg.kgg.kg--11
n = 8n = 840 40 µµg.kgg.kg--11
n = 16n = 16
RBC (units)RBC (units) 1,5 (01,5 (0--4)4) 0,6* (00,6* (0--3)3) 0*0*
%pts transfused%pts transfused 58%58% 38%38% 0%*0%*
Duration of operation Duration of operation (min)(min) 180 180 126*126* 120*120*
Length of hospital stay Length of hospital stay (d)(d) 1212 1313 1111
Lancet 2003;361:201-5
Median perioperative blood 2688 (1707-3565) 1235 (1025-1407)* 1089 (928-1320)*loss (mL)
J Trauma 2005;59:8-18
Réduction moyenne de 2.6 U dans le groupe « Blunt » (P = 0.02)Réduction moyenne de 1.0 U dans le groupe « Penetrating » (P = 0.10)
Toujours chez les malades vivants à 48h:
A recommendation for use of rFVIIa in blunt traumawas made (grade B)
rFVIIa might also be beneficial:- in post-partum hemorrhage (grade E), - uncontrolled bleeding in surgical patients (grade E), - bleeding following cardiac surgery (grade D).
rFVIIa could not be recommended for use:- in penetrating trauma (grade B); - prophylactically in elective surgery (grade A) or liver surgery (grade B); - in bleeding episodes in patients with Child–Pugh A cirrhosis (grade B).
Efficacy of rFVIIa was considered uncertain:- in bleeding episodes in patients with Child–Pugh B and C cirrhosis (grade C).
Monitoring of rFVIIa efficacy should be performed visually and by assessment of transfusion requirements (grade E), while thromboembolic adverse events are a cause for concern.
rFVIIa should not be administered to patients considered
unsalvageable by the treating medical team.
• Every attempt should be made to control bleeding by conventionalmeans. rFVIIa should not replace and/or delay surgery or an y other methods used to control the source of bleeding, suc h as
angiography with embolization.
• Traditional use of blood products, including RBCs, platelets, FFP and cryoprecipitate/fibrinogen, should not be replaced by rFVIIa.
• To ensure maximal rFVIIa efficacy, attempts should be made to achieve the following:
· Platelets: > 50,000 x G/l · Fibrinogen: 0.5 to 1.0 g/l · pH: 7.20
· Hematocrit: > 24%
rVIIa en 2011
• Un hémostatique puissant , qui a potentiellement
sauvé des vies, après échec des traitements
conventionnels
• Peu d’évidences « Evidence based » pour l’instant
• Attention ++++ au risque thrombotique chez les
patients vasculaires ou âgés
• Coût élevé
• Toujours en collaboration avec les équipes
d’hémostase
Donc…
Desmopressine, inutile sauf pour le Willebrand
Acide Tranexamique moins efficace mais plus sûr
Facteur VIIa« Magic bullet »?? - efficacité mais prudence
« Pour arrêter le sang: mettre la main droite sur l'épaule droite du
malade, mouiller l'index droit de salive, faire un signe de croix avec cette
même main droite, la remettre ensuite sur l'épaule droite en disant: pain
n'a pas faim, feu n'a pas froid, sang arrête-toi »
Recette du Loir et Cher
in: B Edeine, La Sologne, Paris 1974
retrouvée par JF Schved, Montpellier