Embed Size (px)
Citation preview
Diagnostic evaluation of a
symptomatic cerebrovascular
accident in a neonate with
focal convulsions
SWISS SOCIETY OF NEONATOLOGY
July 2013

2
Anderson S, Rimensberger P, Service de Néonatologie et des
Soins Intensifs Pédiatriques, Département de l’Enfant et de
l’Adolescent, Hôpitaux Universitaires de Genève
© Swiss Society of Neonatology, Thomas M Berger, Webmaster
3
Focal neonatal convulsions are usually related to peri-
natal asphyxia with hypoxic ischemic encephalopathy
or cerebrovascular accidents which include hemor-
rhagic lesions (including hemorrhagic periventricular
leukomalacia), arterial ischemic stroke or sinus venous
thrombosis.
With an estimated incidence of 1 in 4’000 delive-
ries, ischemic infarction is a rare cause of neurologi-
cal symp toms in the neonatal period (1). Occlusion of
a major cerebral artery can be due to an embolic or
thrombotic event. Clinically, patients typically present
with focal seizures and no altered consciousness bet-
ween the episodes. Standard techniques such as ce-
rebral ultrasound, electroencephalograms (EEGs) and
magnetic resonance imaging (MRI) aid in early dia-
gnosis (2). Additional information from cerebral blood
flow velocity measurements using transcranial Doppler
examinations might be useful for early differentiati-
on between perinatal arterial stroke and other types
of cerebral vascular lesions. Thus, diagnostic MRI may
not be required as an emergency examination.
INTRODUCTION
4
CASE REPORT This male patient was born by Cesarean section be-
cause of failure of labor progression at 37 weeks and
3 days of gestation with a birth weight of 3050 g.
Neonatal adaption was normal with Apgar scores of
9, 10, and 10 at 1, 5, and 10 minutes, respectively.
Family history revealed no convulsive, hematologic or
neurologic disorders.
On day 3 of life, there were three episodes of convul-
sions, which were initially focal with cloni of the right
arm and eye deviation to the upper right, then gene-
ralized secondarily with symmetric cloni and nystag-
mus. Each episode lasted for 2-3 minutes, and was
accompanied by tachycardia and falling oxygen satu-
rations. Adequate behavior was observed between the
episodes. Serum concentrations of glucose and elec-
trolytes were normal. After the third episode, pheno-
barbital treatment was started with a loading dose of
10 mg/kg followed by a maintenance dose of 5 mg/
kg/d. No more clinical episodes of convulsion were re-
corded thereafter.
Initial laboratory analyses of blood and cerebrospinal
fluid showed normal values for electrolytes, ammoni-
um, pyruvate, coagulation factors as well as infectious
parameters. Common metabolic disorders were exclu-
ded with normal newborn screening results (Guthrie
test).
5
Within 30 min after admission to NICU, cerebral ar-
tery flow velocity (CAFV) measured with transcranial
Doppler ultrasound of the left middle cerebral artery
(MCA) was diminished compared to the right MCA.
Peak systolic blood flow velocities were more than
25% higher (45 cm/s vs. 35 cm/s), and the end-diasto-
lic blood flow velocities were more than 60% (20 cm/s
vs. 12 cm/s) higher in the right MCA when compared
to the left MCA. There were also marked differences
in the resistance index values between the right and
left MCA (0.55 vs. 0.66) (Fig. 1). In addition, thalamic
hyperechogenic signals were detected on the initial
cerebral ultrasound.
Magnetic resonance imaging (MRI) 2 days after the
convulsions showed extensive acute ischemic lesions
in the left temporal lobe, as well as involvement of the
left thalamus, the posterior part of the left internal
capsula, and the left peduncle of the splenium of the
corpus callosum. No thrombus could be detected on
MR angiography (Fig. 2-4).
The EEG on day 3 of life showed no abnormalities. Fur-
ther laboratory analysis did not reveal an underlying
coagulation disorder (antithrombin III, factors II and V,
protein C and S). Maternal anticardiolipin antibodies,
lupus anticoagulants, ac-ß2-microglobulin could not
be detected.
6
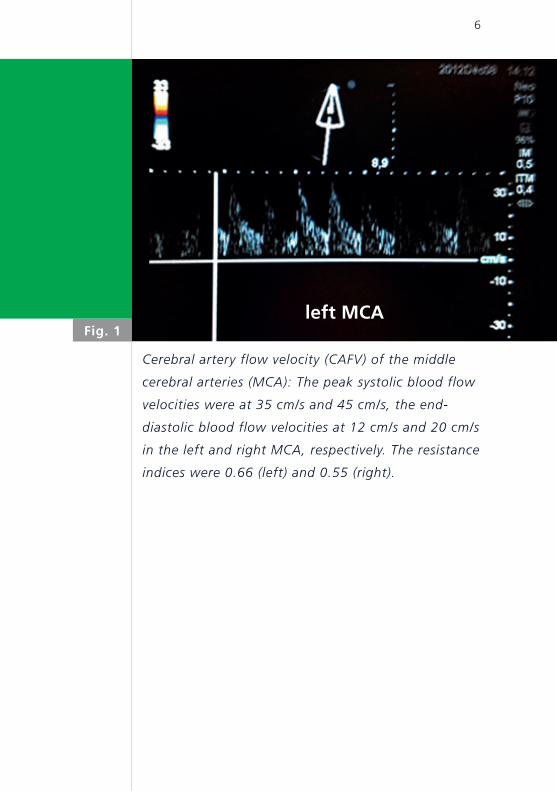
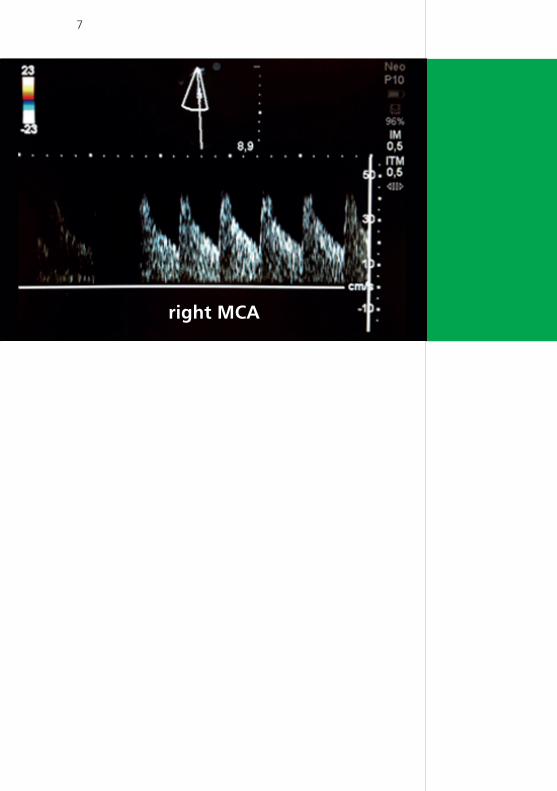
Fig. 1
Cerebral artery flow velocity (CAFV) of the middle
cerebral arteries (MCA): The peak systolic blood flow
velocities were at 35 cm/s and 45 cm/s, the end-
diastolic blood flow velocities at 12 cm/s and 20 cm/s
in the left and right MCA, respectively. The resistance
indices were 0.66 (left) and 0.55 (right).
left MCA
7
right MCA
8
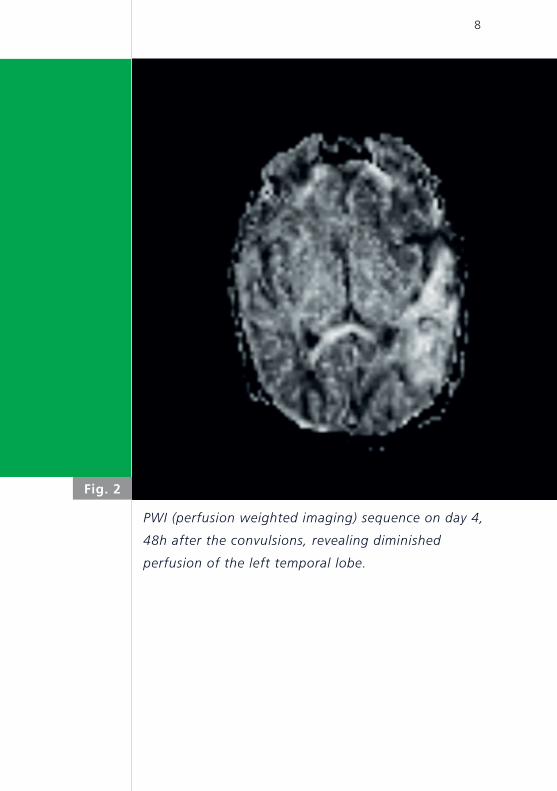
Fig. 2
PWI (perfusion weighted imaging) sequence on day 4,
48h after the convulsions, revealing diminished
perfusion of the left temporal lobe.
9
Neonatal seizures, one of the most common clinical
manifestations of central nervous system disorders
in the neonatal period, with a reported incidence of
1.5–14/1000 live births, can be either symptomatic or
idiopathic. Perinatal hypoxic ischemic insults (reported
seizure incidence of 40%-60%) and cerebrovascular
accidents (reported seizure incidence of 8%-20%),
birth trauma, perinatally acquired infections and me-
tabolic disturbances can be the cause of early sym-
ptomatic neonatal seizures. Furthermore, although
rare, congenital brain anomalies, inborn errors of me-
tabolism and genetic disorders can lead to neonatal
seizures (3). Cerebrovascular accidents can be divided
into either non-hemorrhagic arterial ischemic strokes,
or hemorrhagic insults. The latter are often related
to sinus venous thrombosis (SVT). Perinatal arterial
ischemic stroke is the second most common under-
lying etio logy of neonatal seizures in the full-term
newborn. The prognosis of arterial ischemic stroke is
generally better than of SVT.
Most cases of infants with neonatal cerebral infarction
present with focal and clonic convulsions, few present
with generalized and clonic, or even subtle seizures.
The onset of seizure activity is between 12 and 76
hours after birth. Infants tend to be alert and respon-
sive between episodes and are not encephalopathic.
Focal convulsions are to be evaluated in their perinatal
context. As a first step, in addition to standard labora-
tory tests to exclude possible metabolic causes, a
DISCUSSION
10
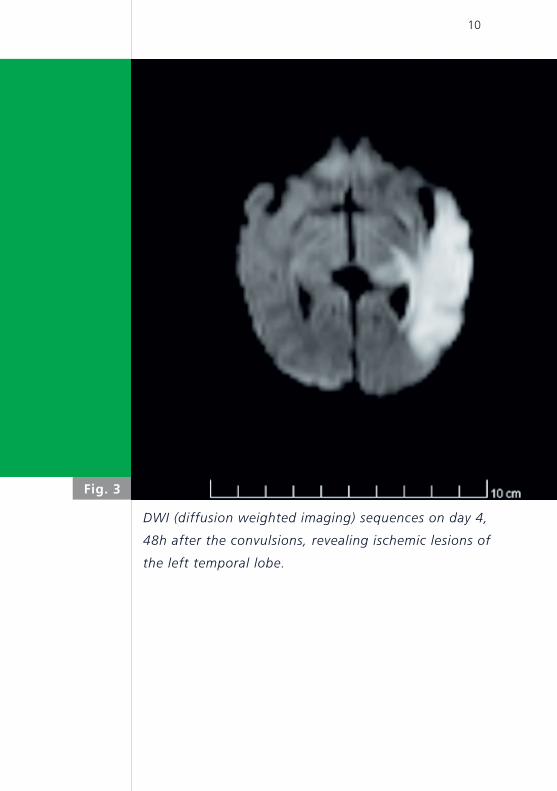
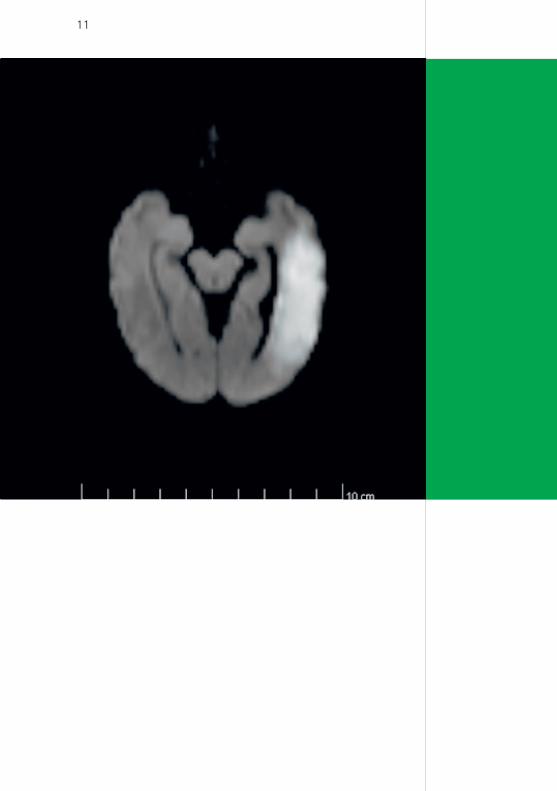
Fig. 3
DWI (diffusion weighted imaging) sequences on day 4,
48h after the convulsions, revealing ischemic lesions of
the left temporal lobe.
11
12
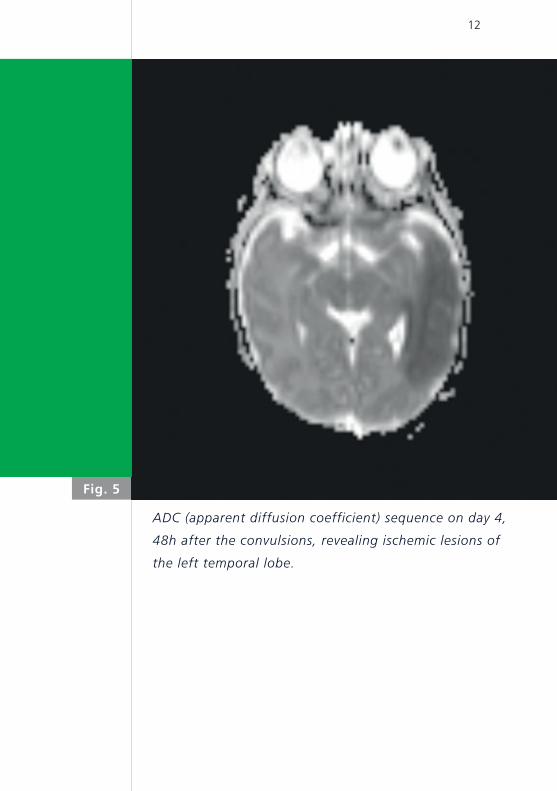
Fig. 5
ADC (apparent diffusion coefficient) sequence on day 4,
48h after the convulsions, revealing ischemic lesions of
the left temporal lobe.
13
detailed neurological and clinical evaluation of the ne-
onate between the episodes of convulsions is crucial.
With hemorrhagic lesions (including the hemorrhagic
PVL in preterm infants) patients show often an alte-
red level of consciousness, whereas patients with an
arterial ischemic stroke often display normal interic tal
behavior. Patients with SVT present with apneas (18%)
altered consciousness (2%), agitation (6%) or sepsis-
like symptoms (5%) (4).
Therapy of perinatal ischemic stroke is supportive
(5). SVT in the perinatal period is often associated
with hemorrhagic lesions (reported in 48-79% of the
cases). Nevertheless, anticoagulation with low mole-
cular-weight heparin has been proven to be safe (6)
and several case reports have documented successful
thrombolytic therapy. Therefore, early anticoagulation
and/or thrombolysis may have to be considered rapid-
ly. However, whether such treatment leads to a better
short- and long-term outcomes is unclear.
Cerebral ultrasound with high frequency transducers
enables examinations of high-risk neonates at the bed-
side. However, ischemic cerebral insults can be difficu-
lt to detect (7). Transcranial Doppler ultrasound is a
flexible, accessible, routinely used tool for the assess-
ment of several vascular pathologies (ie. vasospasm,
stenosis etc.) in the adult intensive care setting. In
the neonatal unit, transcranial Doppler ultrasound is
14
still used only rarely. Fukuda et al. (8), using this tech-
nique, described lower CAFVs in all cerebral arteries
of neonates who went on to develop PVL when com-
pared with control infants; this difference was found
from day 0 onwards. In another study, Basu et al. (9)
demonstrated higher CAFVs in the MCA in septic neo-
nates with high complication and mortality rates. They
consider the assessment of CAFVs early after birth as
an adjunct bedside, non-invasive investigation, which
may have immediate diagnostic and prognostic impli-
cations. Several case reports have described an asym-
metry of CAFV and RI measurements in the MCA in
neonates with cerebral infarcts (10-12). Finally, in a re-
cent study, color Doppler ultrasound has been shown
to be highly specific for ruling out SVT and therefore
being useful as part of a clinical-laboratory-imaging
algorithm (13).
Magnetic resonance imaging (MRI) has been
established as the imaging modality of choice for the
detection and evaluation of ischemic brain injury in
adults, because of its high sensitivity and specificity. In
the early phase of cerebral infarction of neonates, se-
veral reports have revealed the importance of diffusi-
on-weighted imaging (DWI) MRI to detect focal ische-
mic brain injury in neonates (14, 15). This sequence
can be used with high sensitivity during the first 2
days after a stroke. It has to be recognized that DWI
alterations in do not persist for more than one week.
After 5 days, diagnosis relies mainly on T2-weighted
images (16).
15
REFERENCES1. Estan J, Hope P. Unilateral neonatal cerebral infarction in full
term infants. Arch Dis Child 1997;76:F88-93
2. Mercuri E, Rutherfort M, Cowan F, et al. Early prognostic indi-
cators of outcome in infants with neonatal cerebral infarction:
A clinical, electroencephalogram, and magnetic resonance
imaging study. Pediatrics 1999;103:39-46
3. Ronen GM, Penney S, Andrews W. The epidemiology of clinical
neonatal seizures in Newfoundland: a population-based study.
J Pediatr 1999;134:71-75
4. Berfelo FJ, Kersbergen KJ, van Ommen CH, et al. Neonatal
cerebral sinovenous thrombosis from symptom to outcome.
Stroke 2010;41:1382-1388
5. Chabrier S, Husson B, Dinomais M, et al. New insights (and
new interrogations) in perinatal arterial ischemic stroke.
Thromb Res 2011;127:13-22
6. Pergami P, Abraham L. Impact of anticoagulation on the
short-term outcome in a population of neonates with cerebral
sinovenous thrombosis: a retrospective study. J Child Neurol
2011;26:844-850
7. Van Wezel-Meijler G, Steggerda SJ, Leijser LM. Cranial ultra-
sonography in neonates: role and limitations. Semin Perinatol
2010;34:28-38
8. Fukuda S, Kato T, Kakita H, et al. Hemodynamics of the
cerebral arteries of infants with periventricular leukomalacia.
Pediatrics 2006;117:1-8
9. Basu S, Dewangan S, Shukla RC, et al. Cerebral blood flow ve-
locity in early-onset neonatal sepsis and its clinical significance.
Eur J Pediatr 2012;171:901-909
16
10. Messer J, Haddad J, Casanova R. Transcranial Doppler evalu-
ation of cerebral infarction in the neonate. Neuropediatrics
1991;22:147-151
11. Perlman JM, Rollins NK, Evans D. Neonatal stroke: clinical
characteristics and cerebral blood flow velocity measurements.
Pediatr Neurol 1994;11:281-284
12. Nishimaki S, Seki K, Yokota S. Cerebral blood flow velocity in
two patients with neonatal cerebral infarction. Pediatr Neurol.
2001;24:320-323
13. Miller E, Daneman A, Doria AS, et al. Color Doppler US of
normal cerebral venous sinuses in neonates: a comparison with
MR venography. Pediatr Radiol 2012;42:1070-1079
14. Brasseur-Daudruy M, Bordarier C, Cellier C, et al. Cerebral
infarction in full-term newborns: MR imaging features. J Radiol
2008;89:1085-1093
15. Ramenghi LA, Bassi L, Fumagalli M, et al. Neonatal stroke.
Minerva Pediatr 2010;62:177-179
16. Küker W, Möhrle S, Mader I, et al. MRI for the management
of neonatal cerebral infarctions: importance of timing. Childs
Nerv Syst 2004;20:742-748


SUPPORTED BY
CONTACT
Swiss Society of Neonatology
www.neonet.ch
con
cep
t &
des
ign
by
mes
ch.c
h





























