Embed Size (px)
Citation preview
Jean-Charles Preiser
Service des soins intensifs
Hôpital Universitaire Erasme – Bruxelles
Congrès de diététique thérapeutique et de support nutritionnel
28 mars 2015 - Bruxelles
IMPACT DE NOUVELLES ETUDES
D’INTERVENTIONS NUTRITIONNELLES SUR NOTRE
PRATIQUE
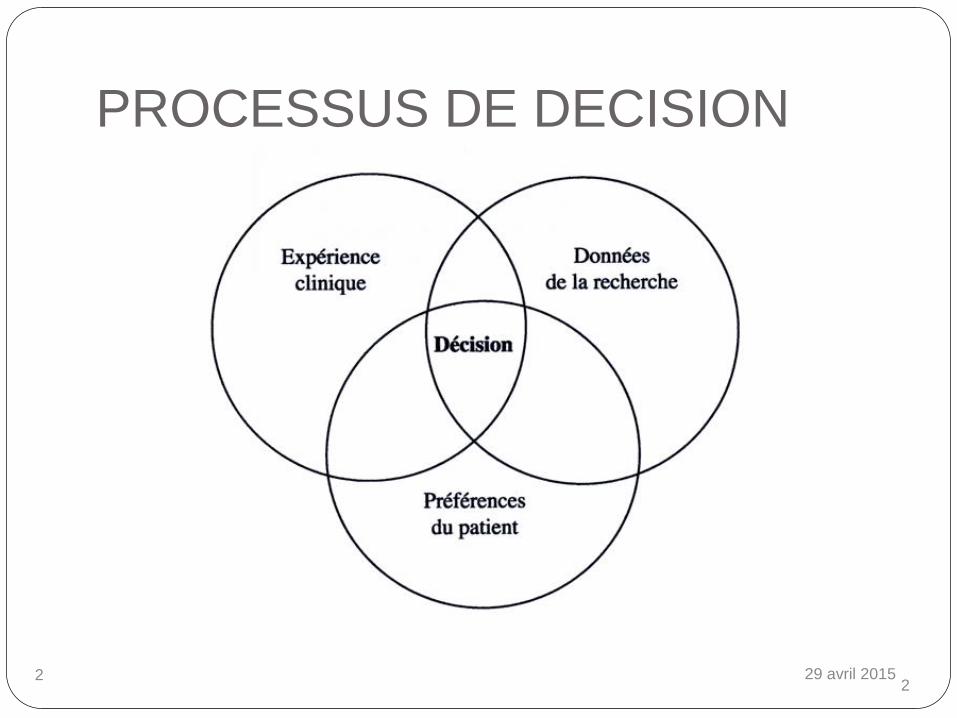
PROCESSUS DE DECISION
29 avril 2015 2 2
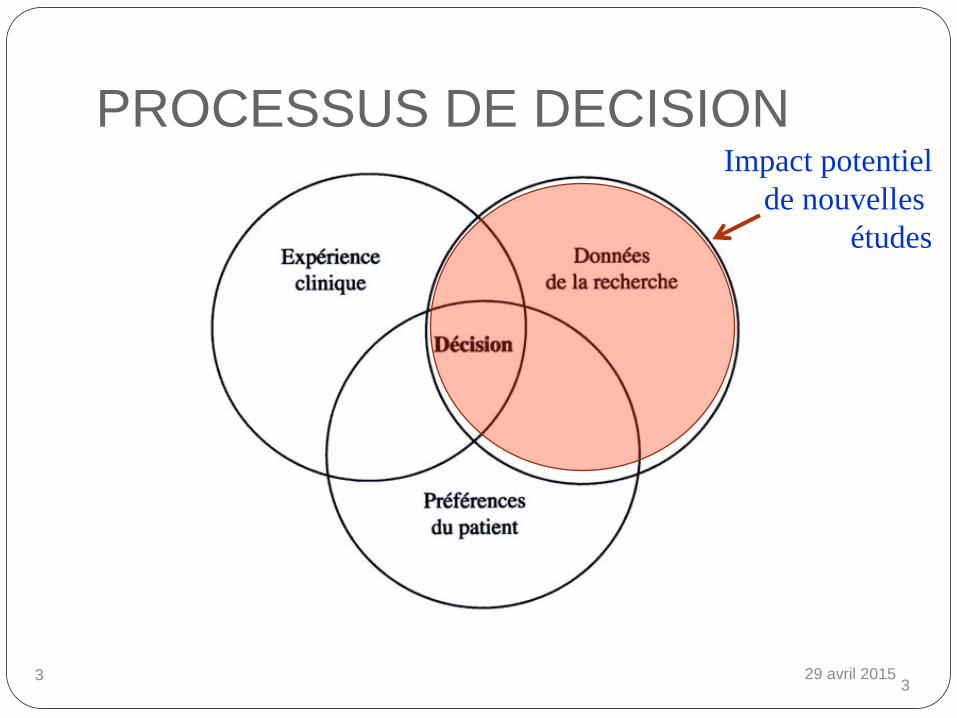
PROCESSUS DE DECISION
29 avril 2015 3 3
Impact potentiel
de nouvelles
études

INFLUENCE DES LEADERS
D’OPINION!
29 avril 2015 5
29 avril 2015 6
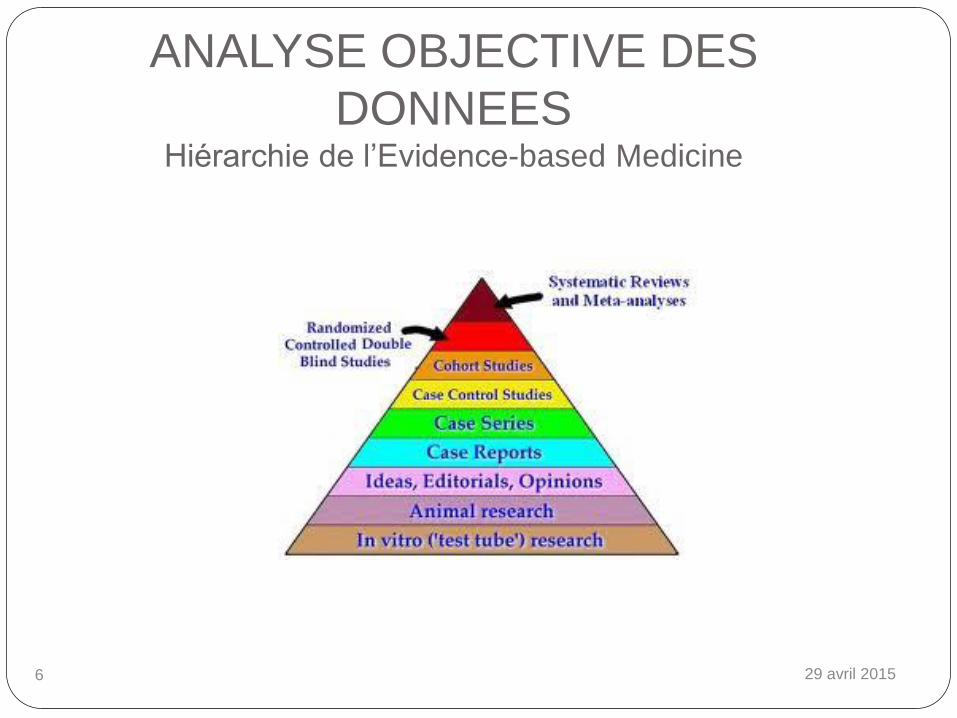
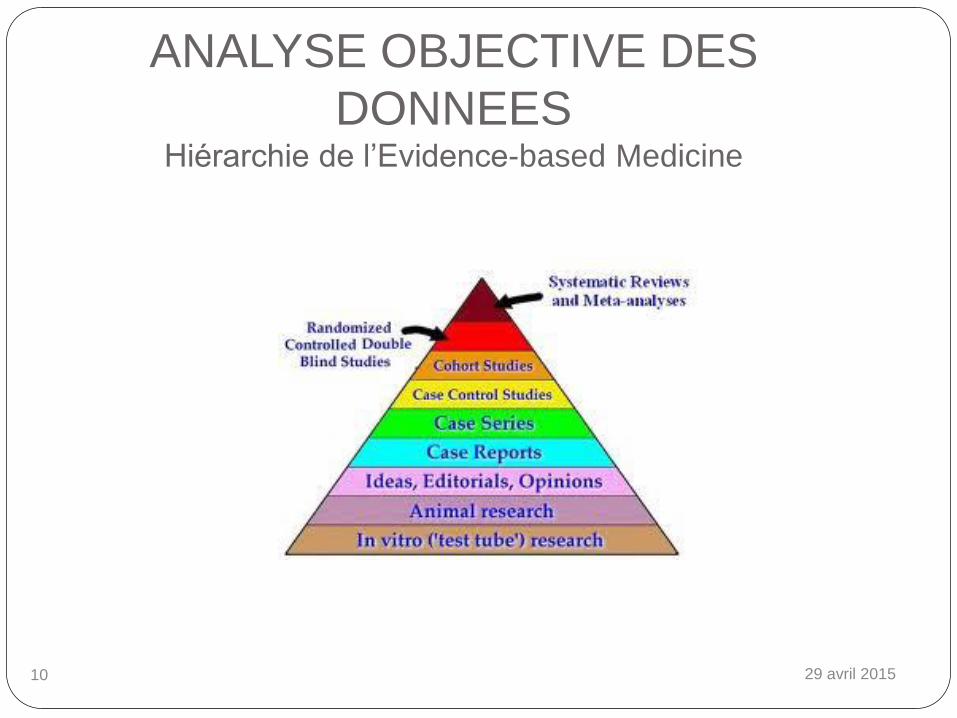
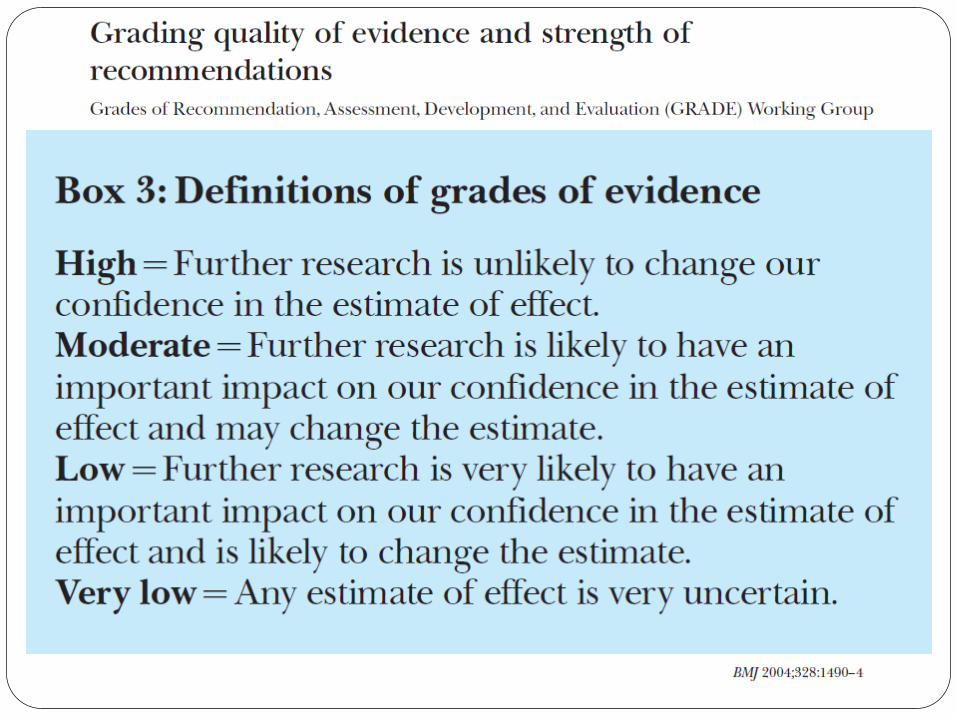
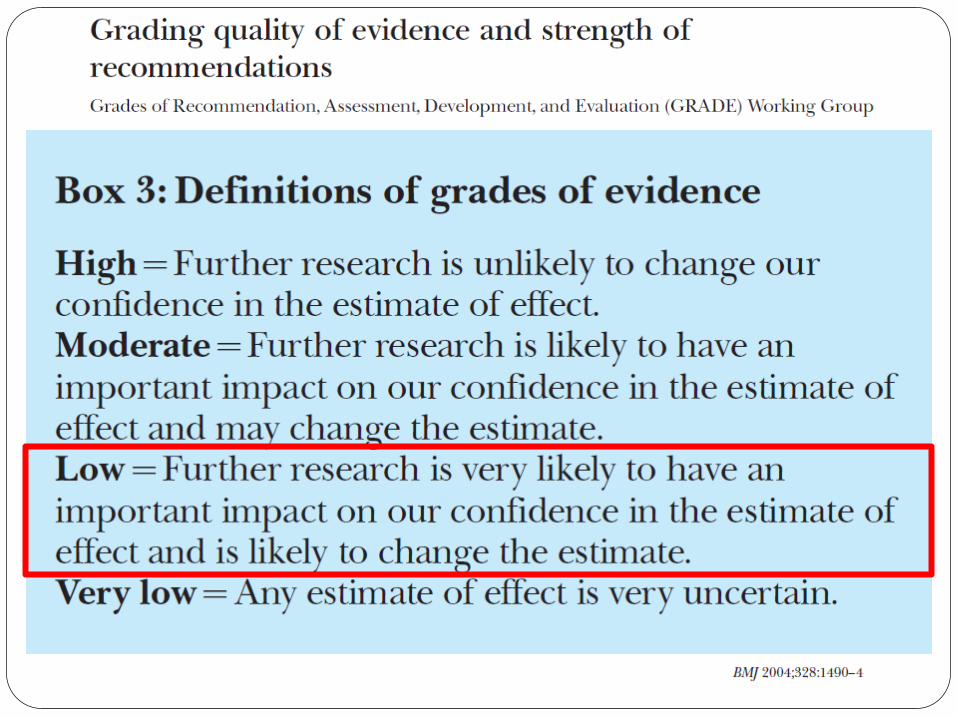
ANALYSE OBJECTIVE DES
DONNEES Hiérarchie de l’Evidence-based Medicine
29 avril 2015 7 29 avril 2015 7
29 avril 2015 8 29 avril 2015 8
29 avril 2015 9
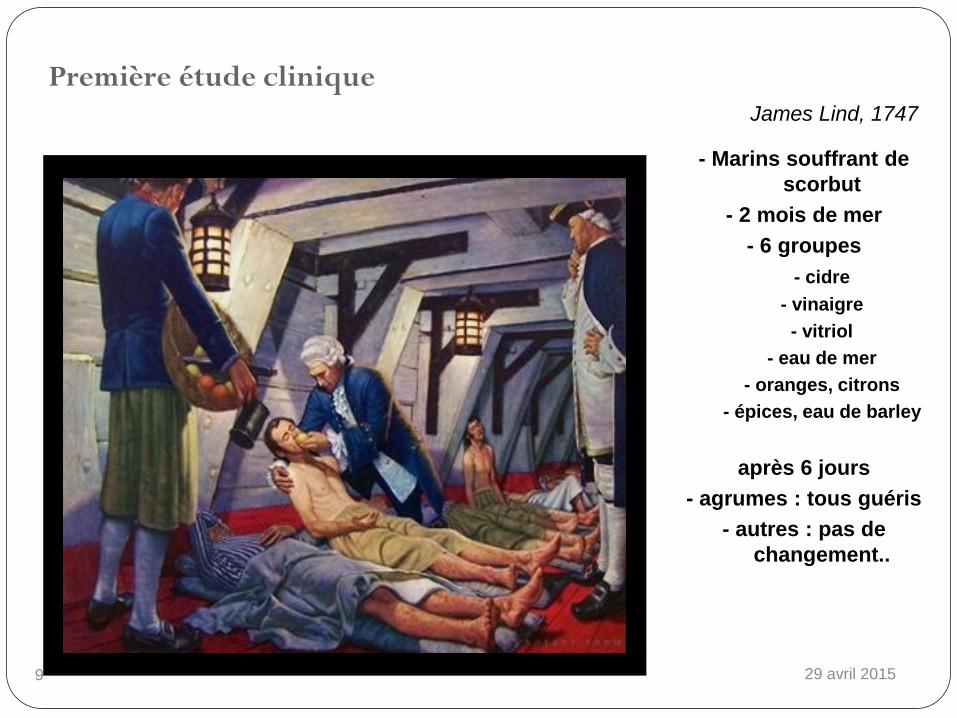
Première étude clinique
- Marins souffrant de
scorbut
- 2 mois de mer
- 6 groupes
- cidre
- vinaigre
- vitriol
- eau de mer
- oranges, citrons
- épices, eau de barley
après 6 jours
- agrumes : tous guéris
- autres : pas de
changement..
James Lind, 1747
29 avril 2015 10
ANALYSE OBJECTIVE DES
DONNEES Hiérarchie de l’Evidence-based Medicine
29 avril 2015 11
Guidelines
Guidelines
Sont Des constats (statements) et
recommandations pour la
pratique clinique basées sur
l’état actuel des connaissances
dans un domaine spécifique
Un moyen de mettre évidence
les différences entre notre
pratique et l’état actuel des
connaissances
Ne sont pas Des contraintes légales
Des garanties de réussite
Un substitut au jugement
clinique
Par nature, les guidelines évoluent!
Très bien,
mais sont-elles applicables
ou réalisables avec les
ustensiles, outils et
ingrédients actuels?
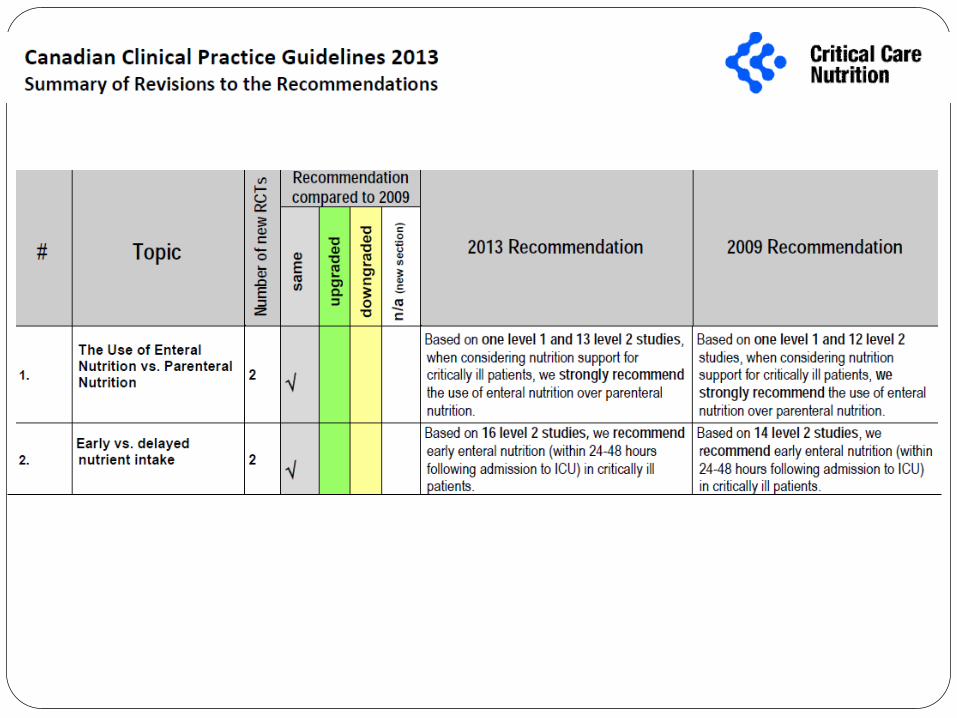
Deux exemples d’application
Péri-opératoire
Soins intensifs – réanimation
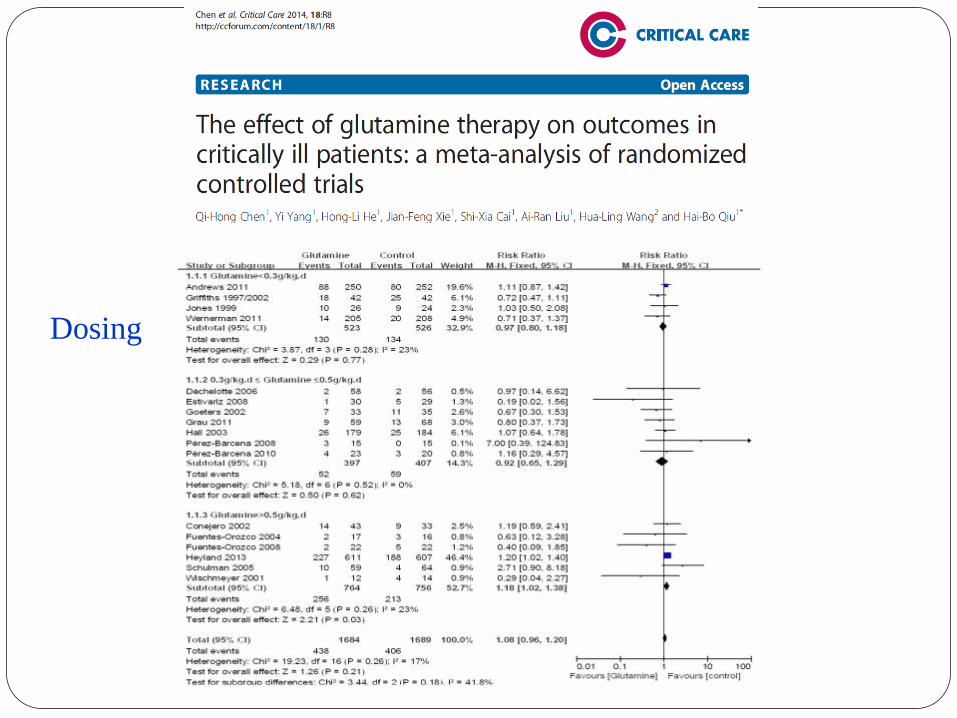
Suppléments en glutamine
Mesure du résidu gastrique
Deux exemples d’application
Péri-opératoire
Soins intensifs – réanimation
Suppléments en glutamine
Mesure du résidu gastrique
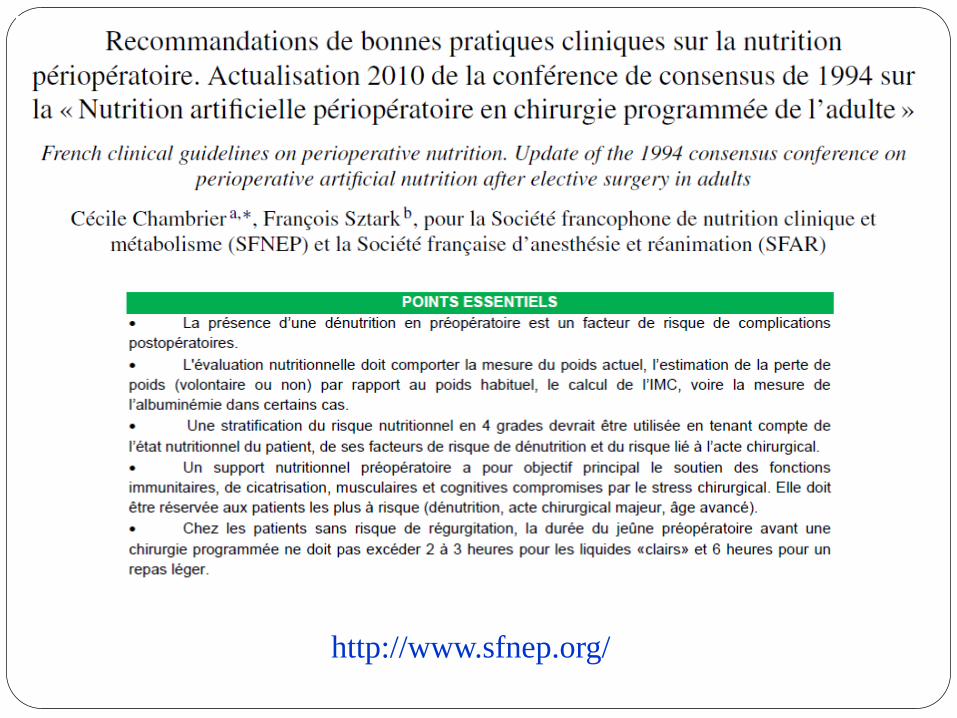
http://www.sfnep.org/
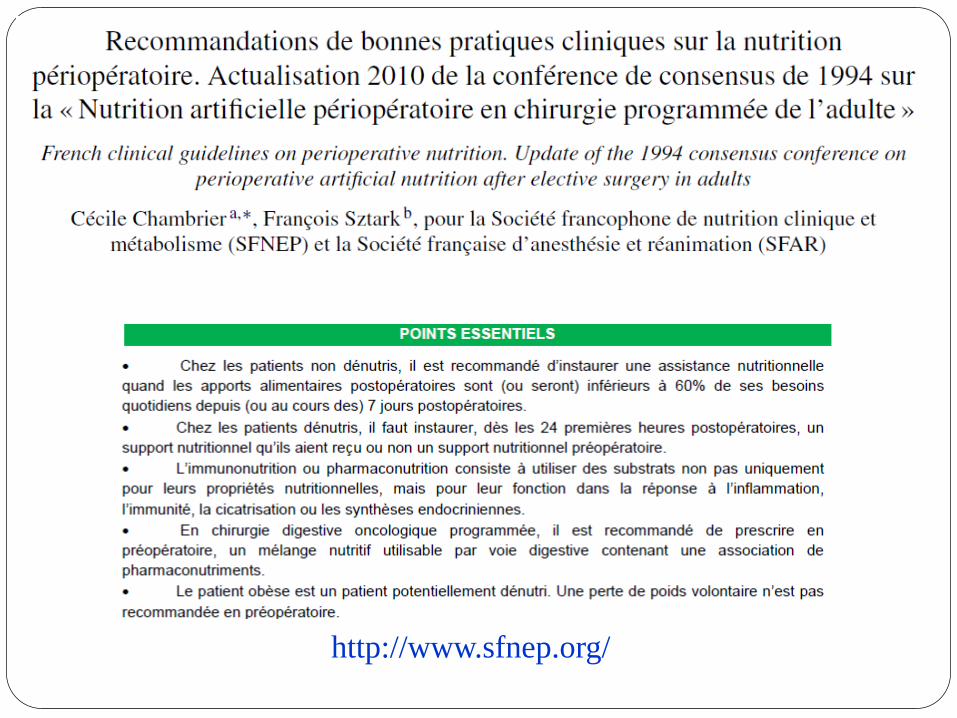
http://www.sfnep.org/
Deux exemples d’application
Péri-opératoire
Soins intensifs – réanimation
Suppléments en glutamine
Mesure du résidu gastrique
Deux exemples d’application
Péri-opératoire
Soins intensifs – réanimation
Suppléments en glutamine
Mesure du résidu gastrique
Did glutamine switch from angel to devil?
The REDOXS© Study REducing Deaths due to OXidative Stress
The REDOXS© Study REducing Deaths from OXidative Stress
Study Chair
Dr. Daren Heyland, MD, FRCPC
Project Leader
Rupinder Dhaliwal, BASc, RD
Can
a
dia
n C
rit
ical Ca
re
Tria
ls G
r
oup
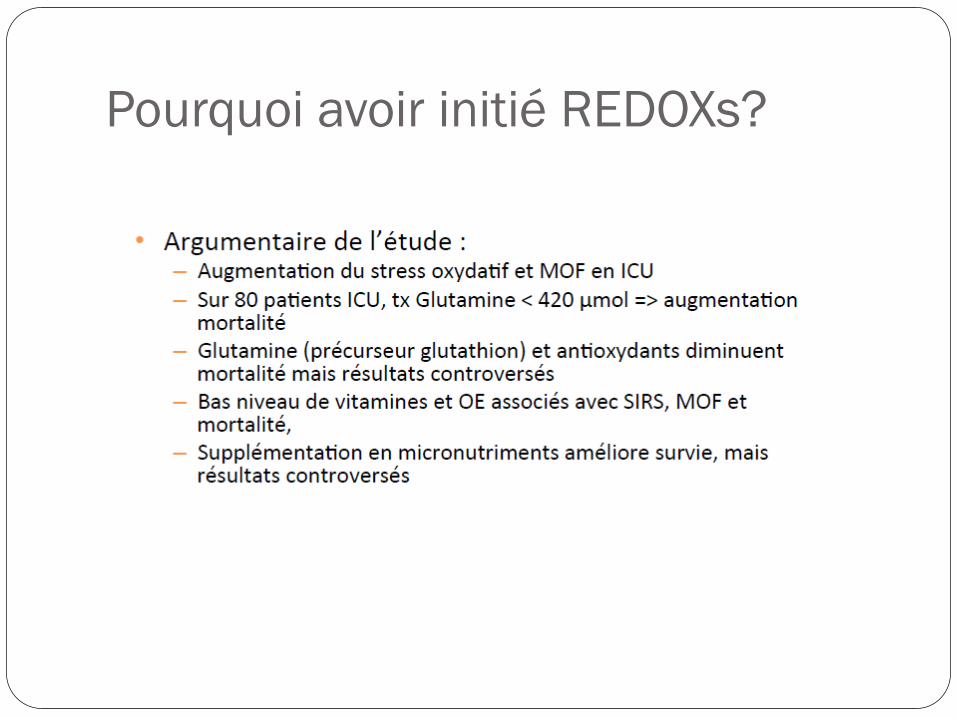
Pourquoi avoir initié REDOXs?
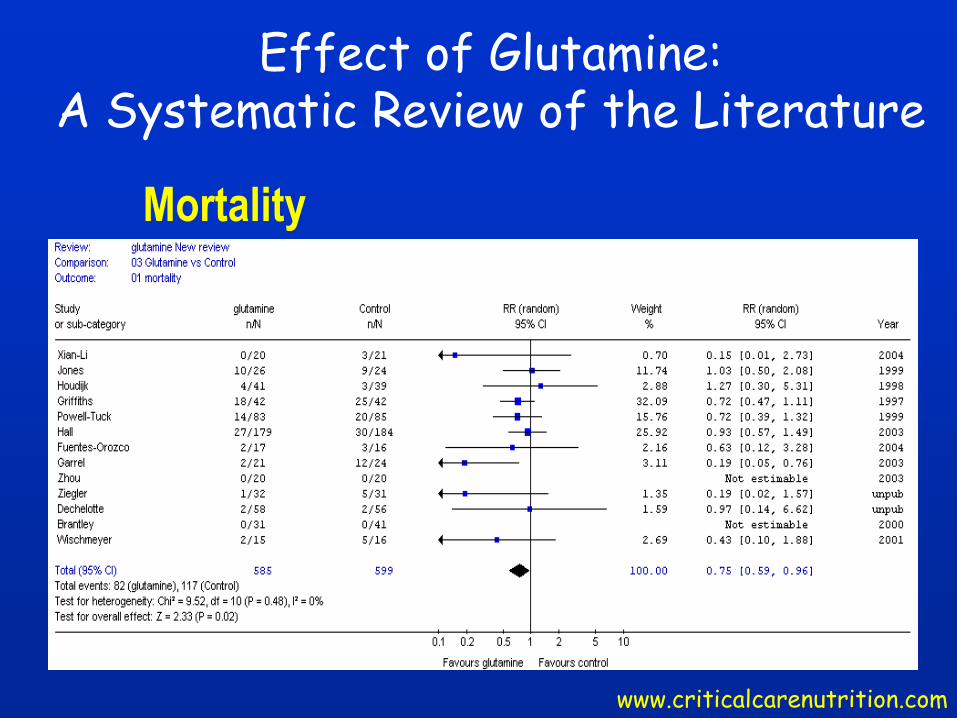
Effect of Glutamine: A Systematic Review of the Literature
www.criticalcarenutrition.com
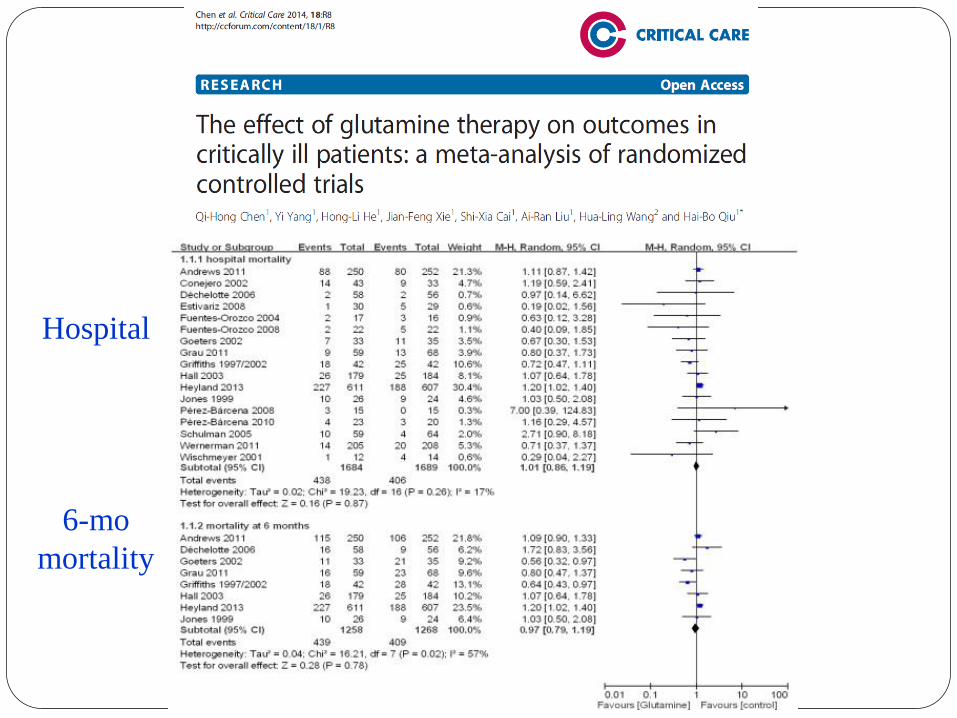
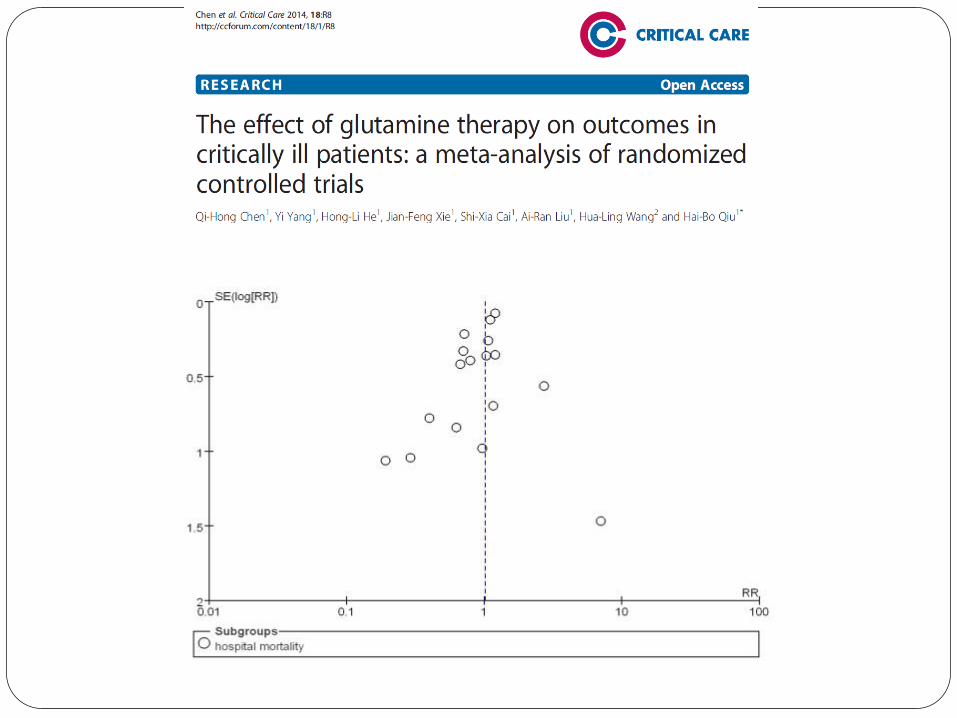
Mortality
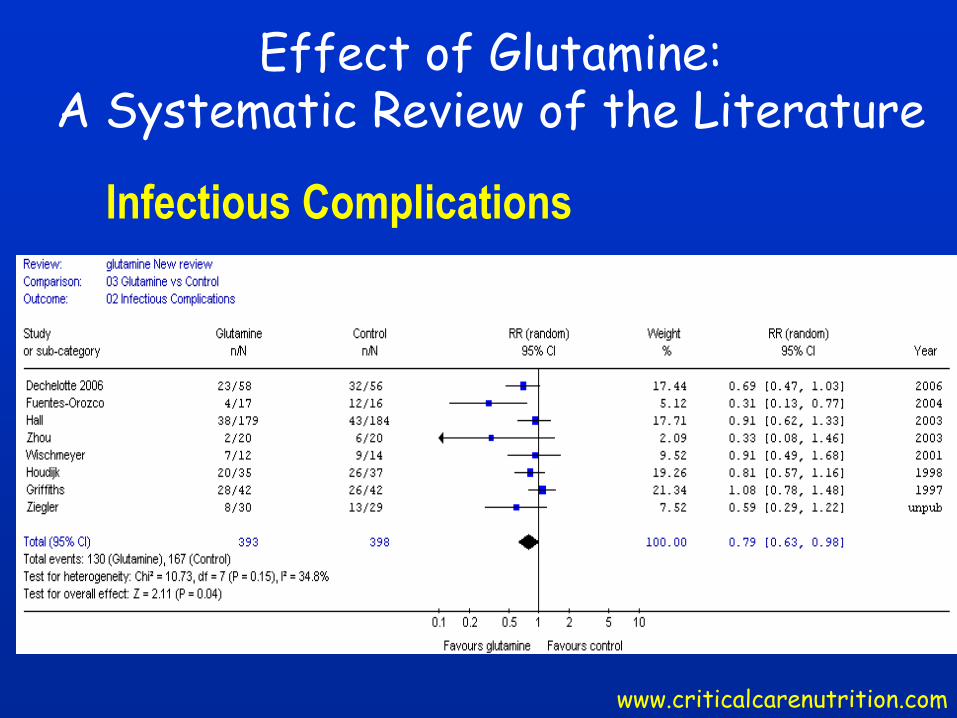
Effect of Glutamine: A Systematic Review of the Literature
www.criticalcarenutrition.com
Infectious Complications
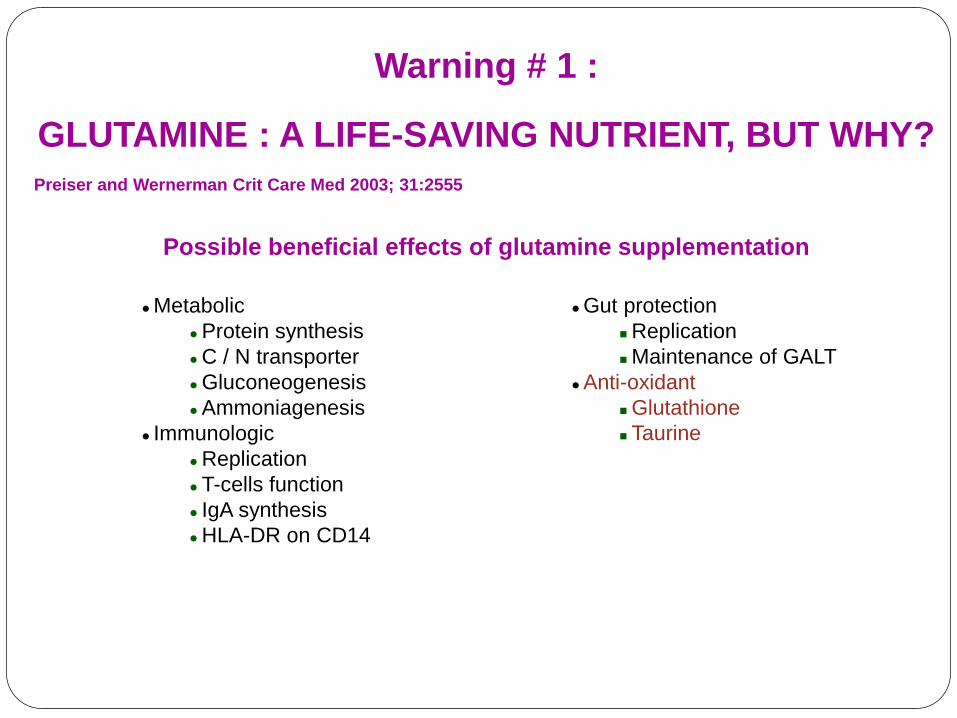
Warning # 1 :
GLUTAMINE : A LIFE-SAVING NUTRIENT, BUT WHY?
Preiser and Wernerman Crit Care Med 2003; 31:2555
Possible beneficial effects of glutamine supplementation
Metabolic
Protein synthesis
C / N transporter
Gluconeogenesis
Ammoniagenesis
Immunologic
Replication
T-cells function
IgA synthesis
HLA-DR on CD14
Gut protection
Replication
Maintenance of GALT
Anti-oxidant
Glutathione
Taurine
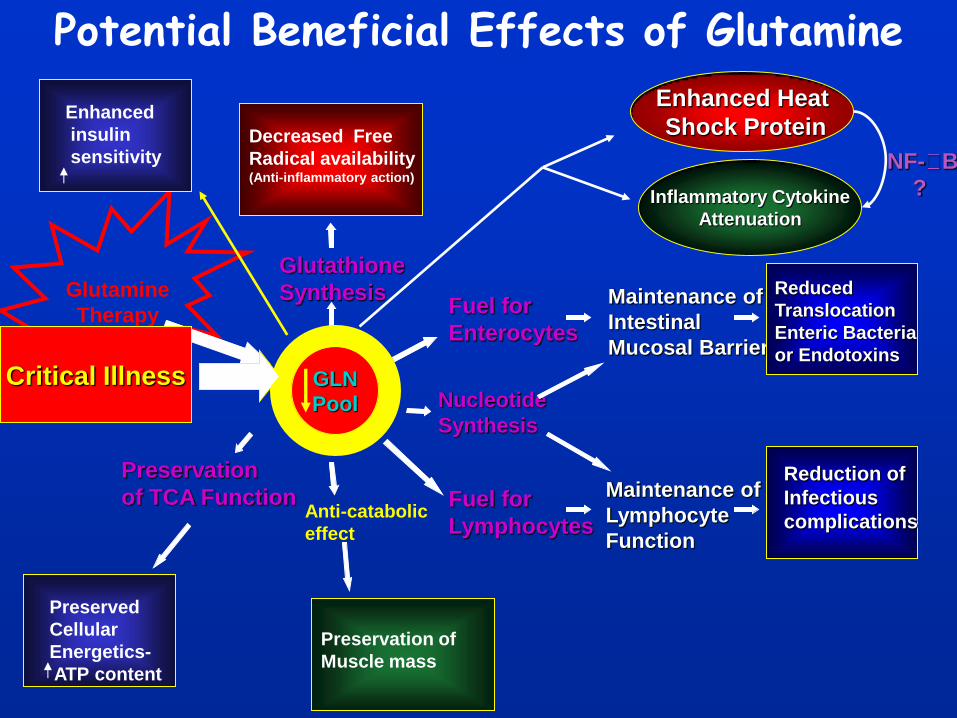
Potential Beneficial Effects of Glutamine
Fuel for
Enterocytes
Fuel for
Lymphocytes
Nucleotide
Synthesis
Maintenance of
Intestinal
Mucosal Barrier
Maintenance of
Lymphocyte
Function
Preservation
of TCA Function
Decreased Free
Radical availability (Anti-inflammatory action)
Glutathione
Synthesis
GLN
pool
Glutamine
Therapy
Enhanced Heat
Shock Protein
Anti-catabolic
effect
Preservation of
Muscle mass
Reduced
Translocation
Enteric Bacteria
or Endotoxins
Reduction of
Infectious
complications
Inflammatory Cytokine
Attenuation
NF- B
?
Preserved
Cellular
Energetics-
ATP content
GLN
Pool Critical Illness
Enhanced
insulin
sensitivity
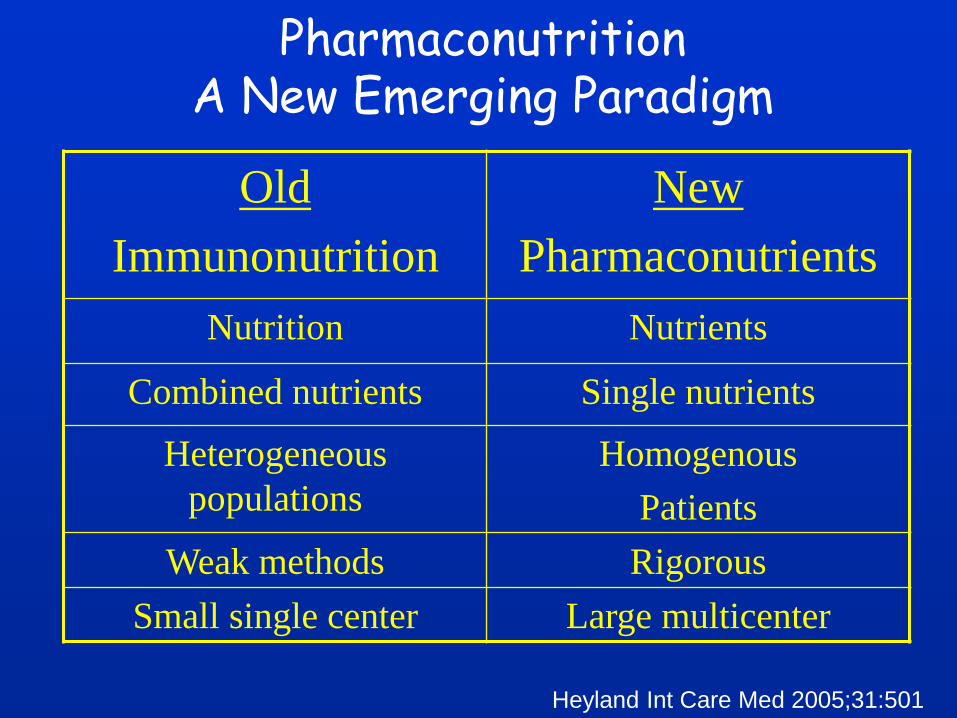
Pharmaconutrition A New Emerging Paradigm
Old
Immunonutrition
New
Pharmaconutrients
Nutrition Nutrients
Combined nutrients Single nutrients
Heterogeneous
populations
Homogenous
Patients
Weak methods Rigorous
Small single center Large multicenter
Heyland Int Care Med 2005;31:501
Research Questions
In critically ill patients with severe organ
dysfunction, what is the effect of:
1) Glutamine supplementation compared to
placebo on 28-day mortality?
2) Antioxidant supplementation compared to
placebo on 28-day mortality?
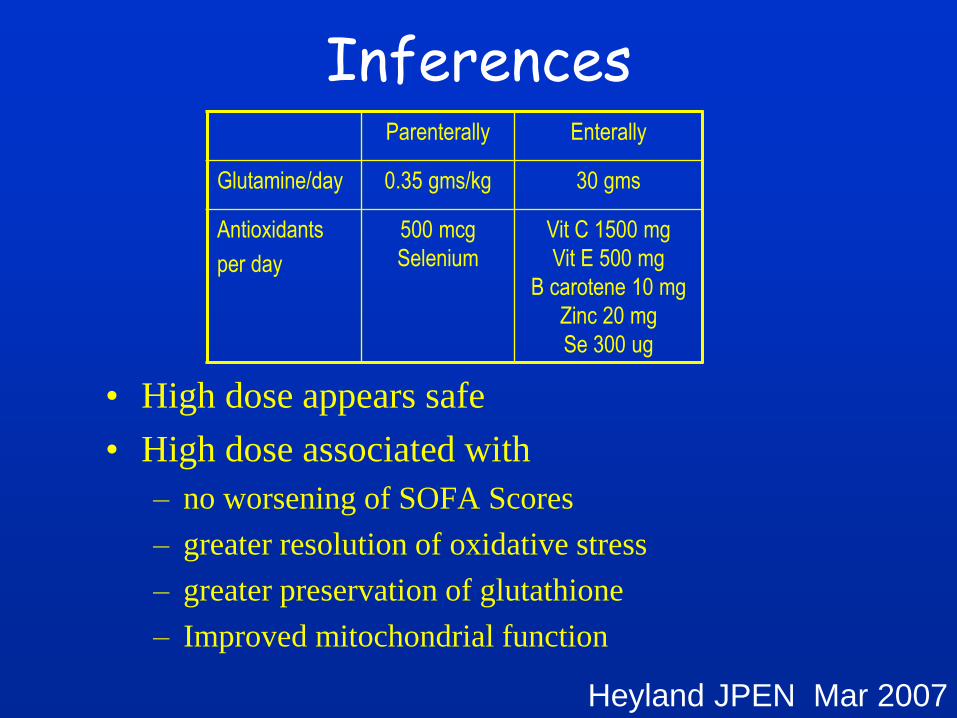
Inferences
• High dose appears safe
• High dose associated with
– no worsening of SOFA Scores
– greater resolution of oxidative stress
– greater preservation of glutathione
– Improved mitochondrial function
Heyland JPEN Mar 2007
Parenterally Enterally
Glutamine/day 0.35 gms/kg 30 gms
Antioxidants
per day
500 mcg
Selenium
Vit C 1500 mg
Vit E 500 mg
B carotene 10 mg
Zinc 20 mg
Se 300 ug
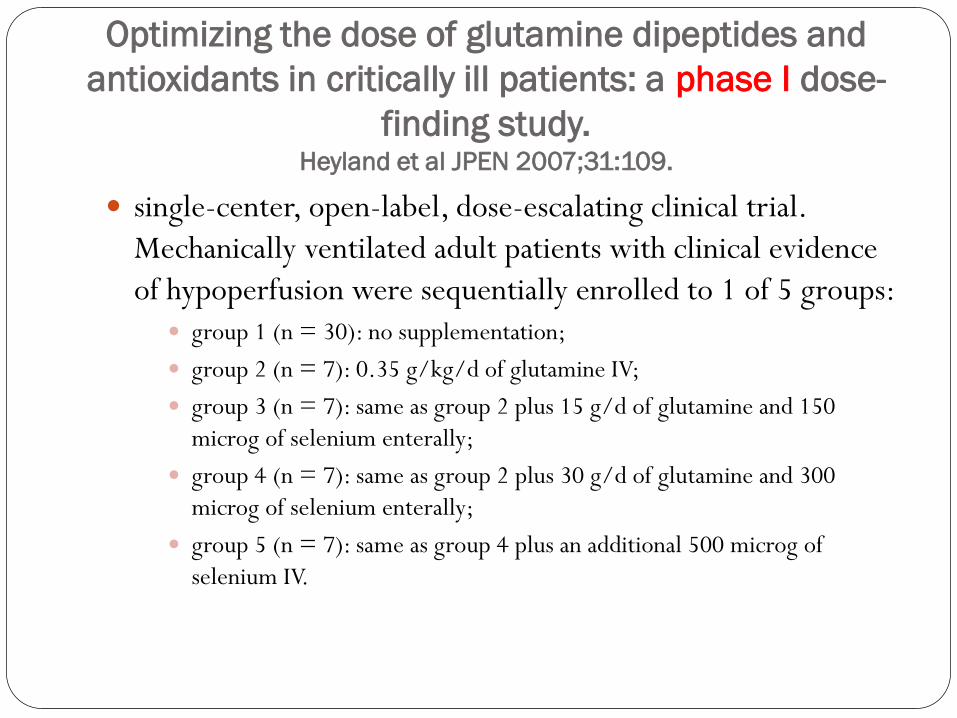
Optimizing the dose of glutamine dipeptides and
antioxidants in critically ill patients: a phase I dose-
finding study. Heyland et al JPEN 2007;31:109.
single-center, open-label, dose-escalating clinical trial.
Mechanically ventilated adult patients with clinical evidence
of hypoperfusion were sequentially enrolled to 1 of 5 groups: group 1 (n = 30): no supplementation;
group 2 (n = 7): 0.35 g/kg/d of glutamine IV;
group 3 (n = 7): same as group 2 plus 15 g/d of glutamine and 150
microg of selenium enterally;
group 4 (n = 7): same as group 2 plus 30 g/d of glutamine and 300
microg of selenium enterally;
group 5 (n = 7): same as group 4 plus an additional 500 microg of
selenium IV.
KNOWN POSSIBLE TOXICITY OF
GLUTAMINE
Related to metabolites (ammonia, glutamate?):
Hepatic encephalopathy / ammonium production
Lower glutamate levels
Precusor of arginine => NO
Ranges of doses used in critically ill patients: 0.35 g/kg.day
IV and/or 30 – 60 g orally/enterally
J Nutr 2001.
The unsolved issue is:
How safe were we with this phase I trial?
N = 7 per group
Relevance of outcome variables selected, in terms of safety?
Duration of follow-up
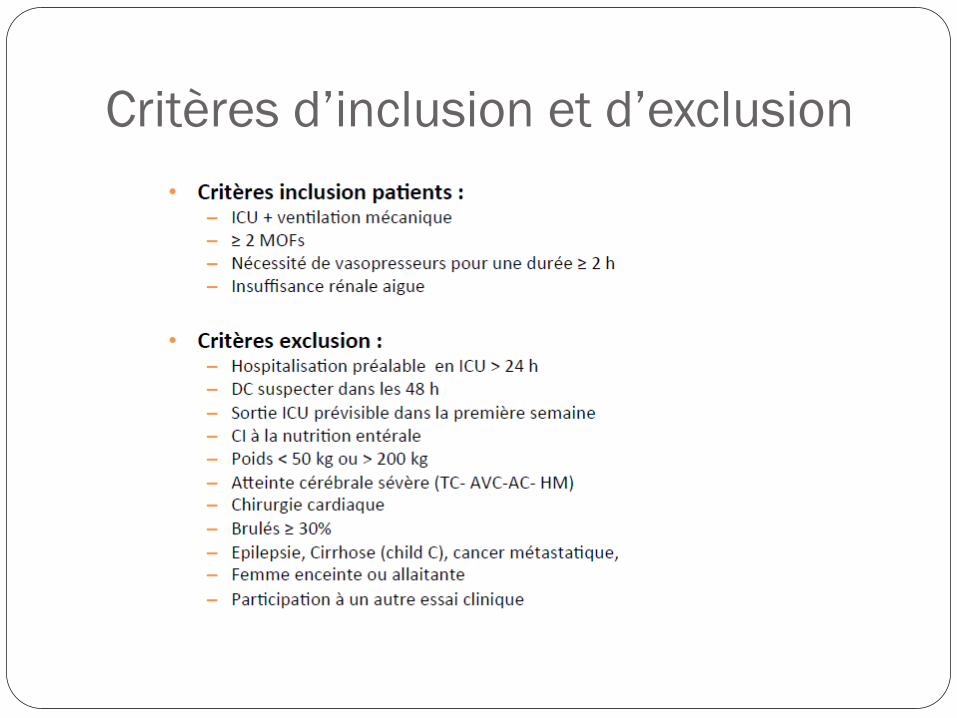
Critères d’inclusion et d’exclusion
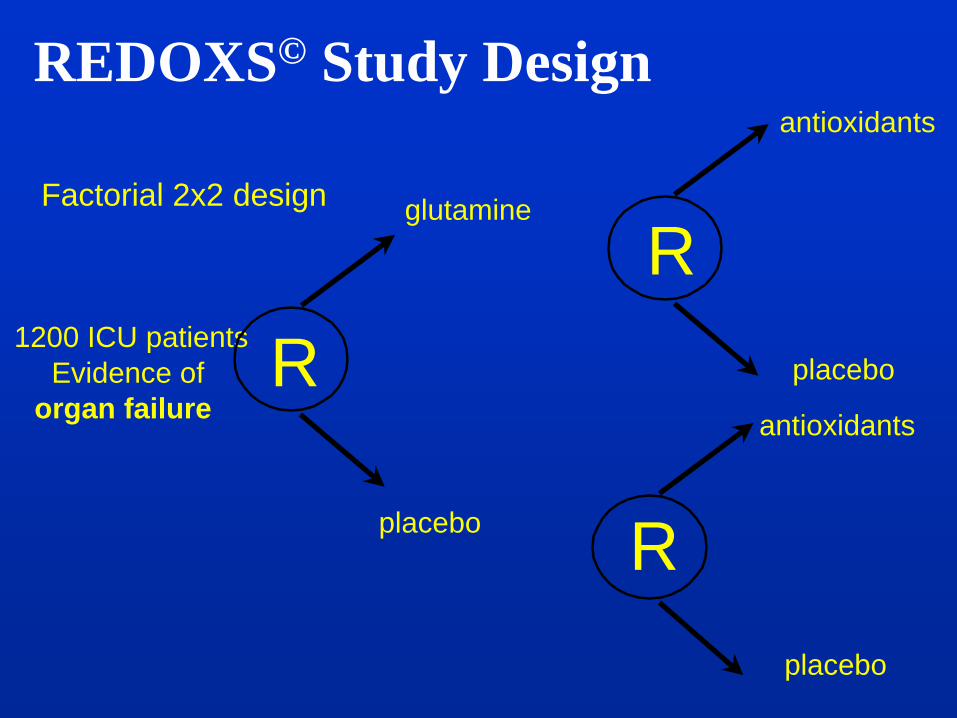
1200 ICU patients
Evidence of
organ failure R
glutamine
placebo
R
R
antioxidants
placebo
Factorial 2x2 design
placebo
antioxidants
REDOXS© Study Design
Start of Supplements
Start ASAP within 24 hrs of admission to ICU within 2 hrs of randomization
Duration: 28 days or death or discharge min of 5 days
Parenteral supplements as soon as patient resuscitated 10 ml/hr dedicated central port (eg. one of a triple lumen) can run peripherally if needed (watch for phlebitis) Do NOT infuse with medications; IV fluids, albumin, nutrition OK
Enteral supplement NG tube OK or feeding tube 20 ml/hr, can be given via Y connector start regardless of whether docs want to start enteral nutrition
nutrients vs.
nutrition
SS Manual p 4-10
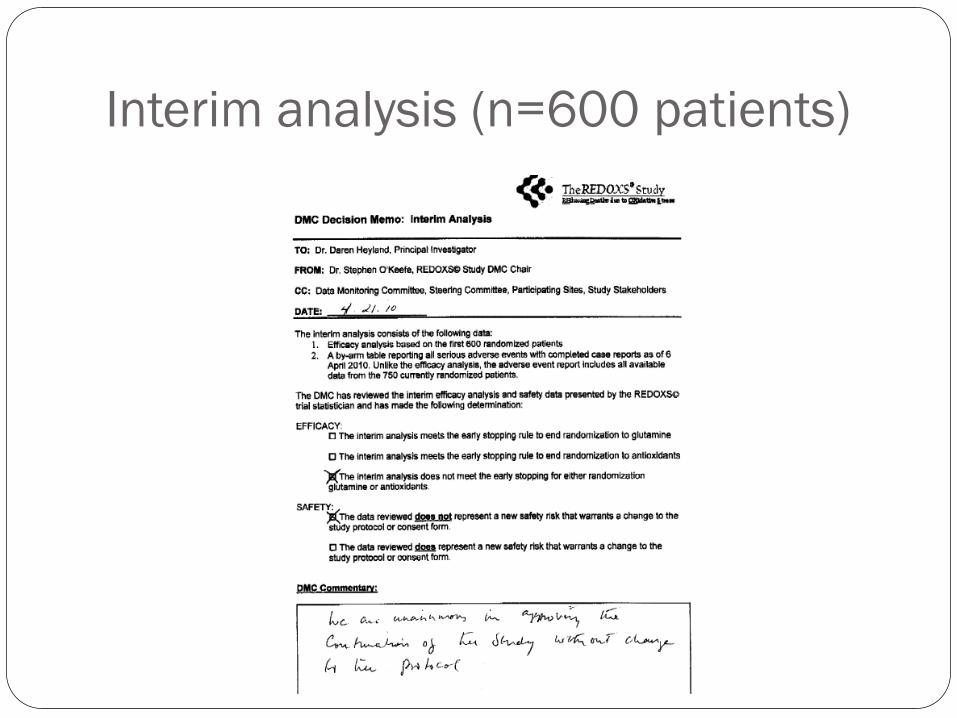
Interim analysis (n=600 patients)
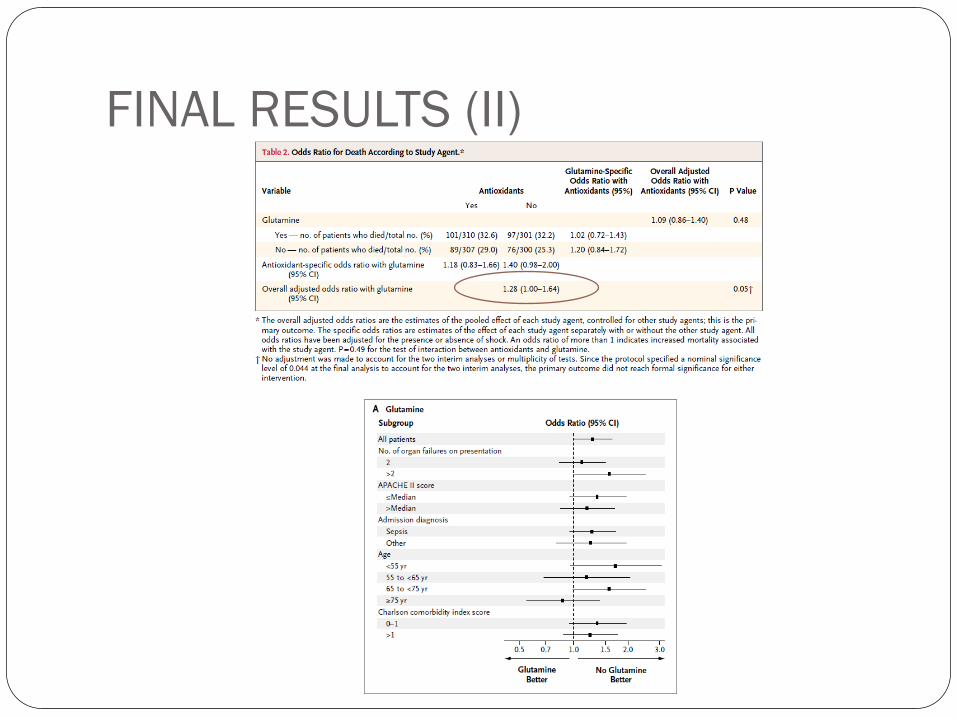
FINAL RESULTS (II)
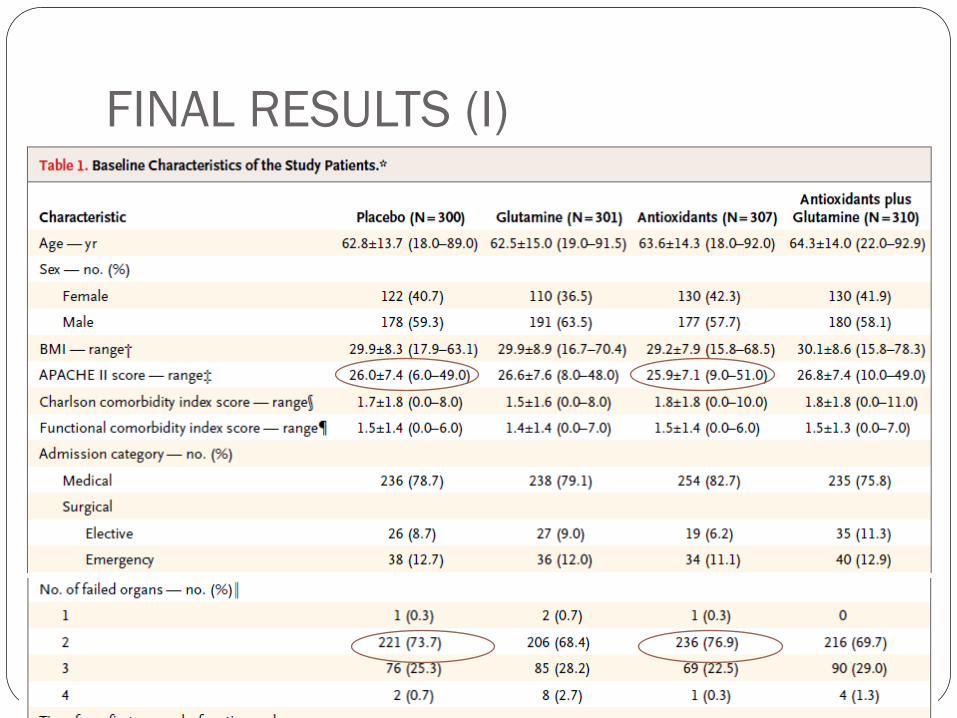
FINAL RESULTS (I)

POST-HOC ANALYSIS
45
Metaplus
European PRCT (14 centres)
Mechanically ventilated adults
Comparison of an immune-modulating formula enriched
in glutamine, vitamins C and E, selenium, zinc and
omega-3 fatty acids (EPA and DHA) with a control
isocaloric isonitrogenous solution
Van Zanten et al JAMA 2014; 312:514
46
Aims of the study
Primary outcome variable :
Incidence of nosocomial infections
Secondary outcome variables :
Score SOFA (Sepsis-related Organ Failure Assessment)
Length of ventilation,
Length of stay
Insulin requirements
ICU, hospital, 28-day and 6-mo mortality
Plasma concentrations of glutamine, Vit C, vit E, Sélénium, Zinc, DHA
at days 0,4 and 8.
Van Zanten et al JAMA 2014; 312:514
47
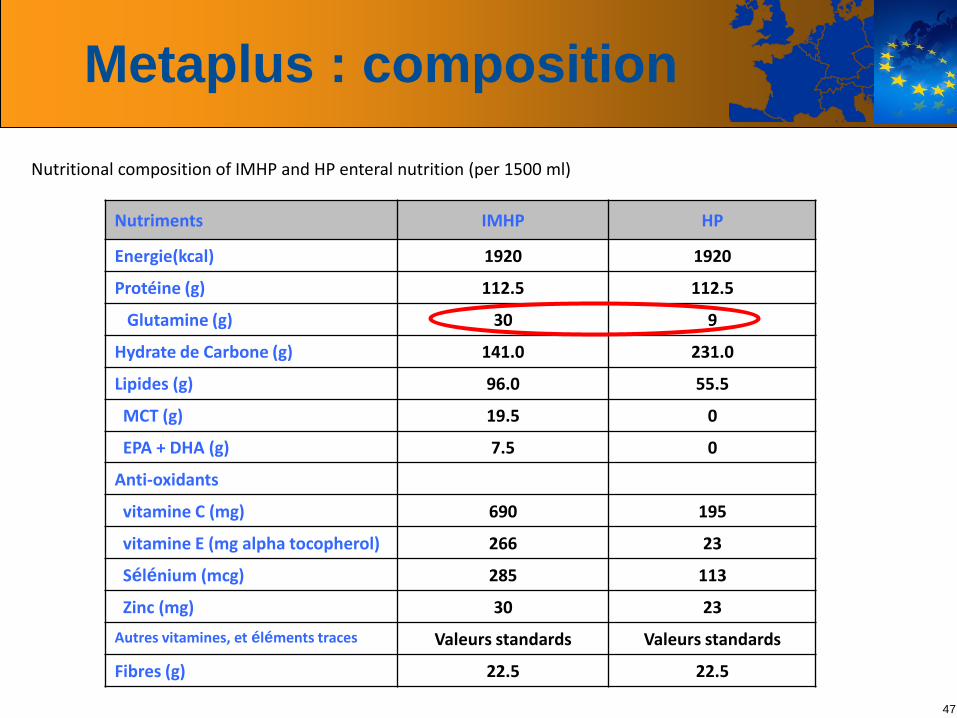
Metaplus : composition
Nutritional composition of IMHP and HP enteral nutrition (per 1500 ml)
Nutriments IMHP HP
Energie(kcal) 1920 1920
Protéine (g) 112.5 112.5
Glutamine (g) 30 9
Hydrate de Carbone (g) 141.0 231.0
Lipides (g) 96.0 55.5
MCT (g) 19.5 0
EPA + DHA (g) 7.5 0
Anti-oxidants
vitamine C (mg) 690 195
vitamine E (mg alpha tocopherol) 266 23
Sélénium (mcg) 285 113
Zinc (mg) 30 23
Autres vitamines, et éléments traces Valeurs standards Valeurs standards
Fibres (g) 22.5 22.5
48
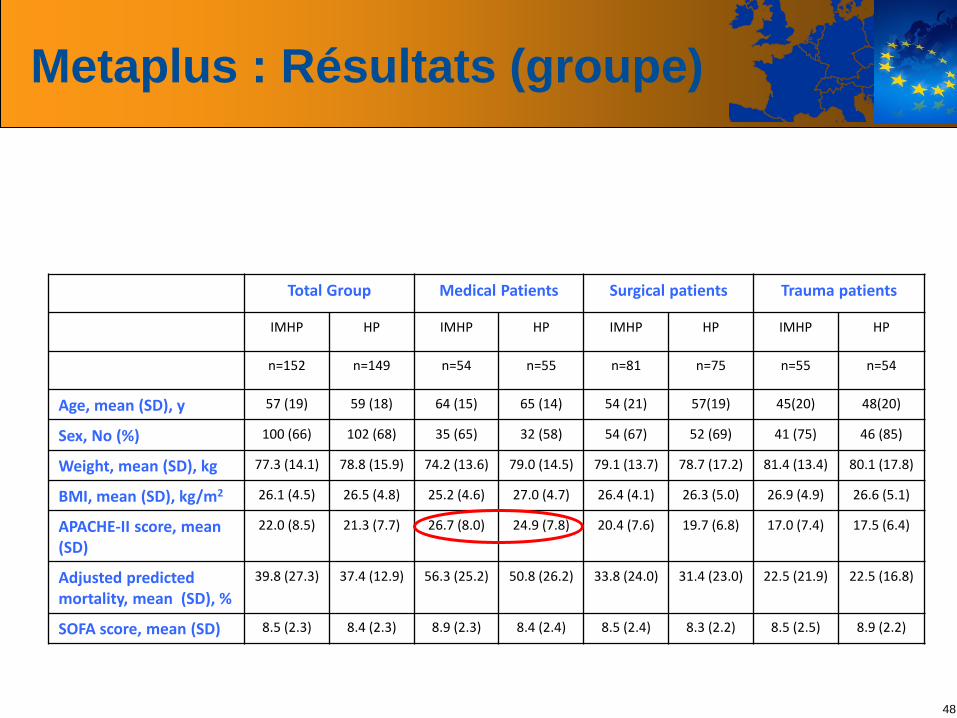
Metaplus : Résultats (groupe)
Total Group Medical Patients Surgical patients Trauma patients
IMHP HP IMHP HP IMHP HP IMHP HP
n=152 n=149 n=54 n=55 n=81 n=75 n=55 n=54
Age, mean (SD), y 57 (19) 59 (18) 64 (15) 65 (14) 54 (21) 57(19) 45(20) 48(20)
Sex, No (%) 100 (66) 102 (68) 35 (65) 32 (58) 54 (67) 52 (69) 41 (75) 46 (85)
Weight, mean (SD), kg 77.3 (14.1) 78.8 (15.9) 74.2 (13.6) 79.0 (14.5) 79.1 (13.7) 78.7 (17.2) 81.4 (13.4) 80.1 (17.8)
BMI, mean (SD), kg/m2 26.1 (4.5) 26.5 (4.8) 25.2 (4.6) 27.0 (4.7) 26.4 (4.1) 26.3 (5.0) 26.9 (4.9) 26.6 (5.1)
APACHE-II score, mean (SD)
22.0 (8.5) 21.3 (7.7) 26.7 (8.0) 24.9 (7.8) 20.4 (7.6) 19.7 (6.8) 17.0 (7.4) 17.5 (6.4)
Adjusted predicted mortality, mean (SD), %
39.8 (27.3) 37.4 (12.9) 56.3 (25.2) 50.8 (26.2) 33.8 (24.0) 31.4 (23.0) 22.5 (21.9) 22.5 (16.8)
SOFA score, mean (SD) 8.5 (2.3) 8.4 (2.3) 8.9 (2.3) 8.4 (2.4) 8.5 (2.4) 8.3 (2.2) 8.5 (2.5) 8.9 (2.2)
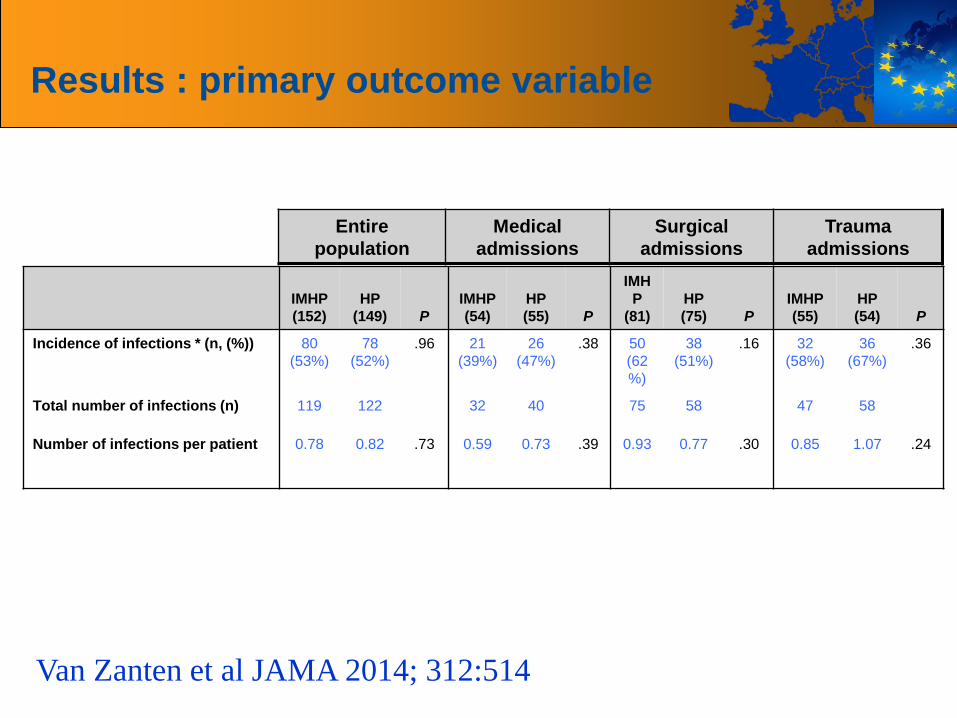
Results : primary outcome variable
IMHP
(152)
HP
(149) P
IMHP
(54)
HP
(55) P
IMH
P
(81)
HP
(75) P
IMHP
(55)
HP
(54) P
Incidence of infections * (n, (%)) 80
(53%)
78
(52%)
.96 21
(39%)
26
(47%)
.38 50
(62
%)
38
(51%)
.16 32
(58%)
36
(67%)
.36
Total number of infections (n) 119 122 32 40 75 58 47 58
Number of infections per patient 0.78 0.82 .73 0.59 0.73 .39 0.93 0.77 .30 0.85 1.07 .24
Entire
population
Medical
admissions
Surgical
admissions
Trauma
admissions
Van Zanten et al JAMA 2014; 312:514
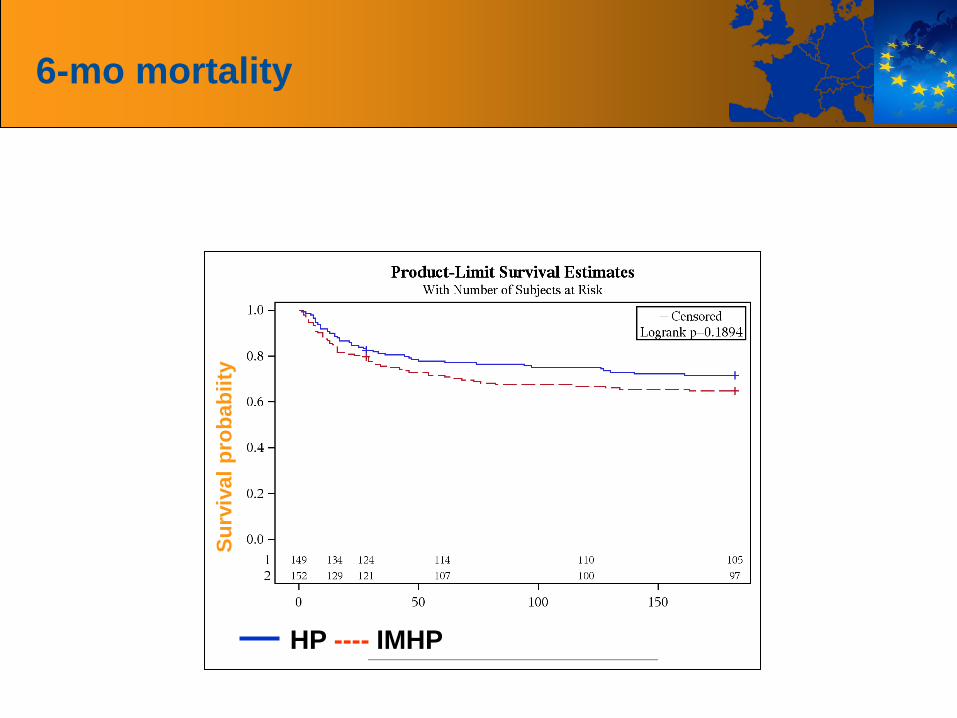
6-mo mortality
Su
rviv
al
pro
bab
iity
HP ---- IMHP
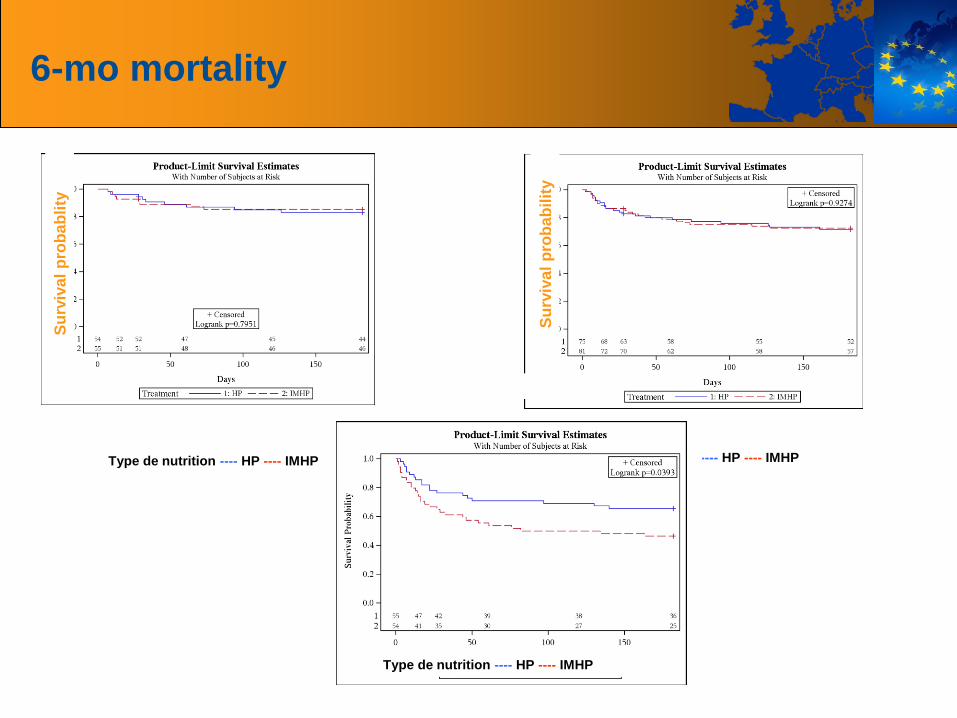
6-mo mortality S
urv
iva
l p
rob
ab
lity
Su
rviv
al
pro
bab
ilit
y
Type de nutrition ---- HP ---- IMHP Type de nutrition ---- HP ---- IMHP
Type de nutrition ---- HP ---- IMHP
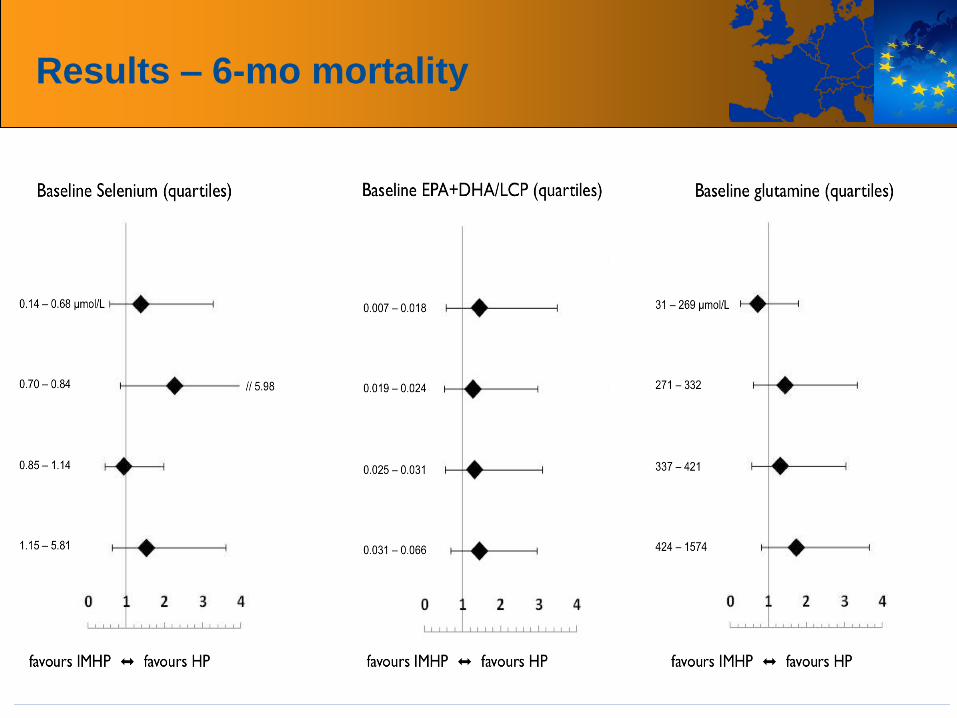
Results – 6-mo mortality
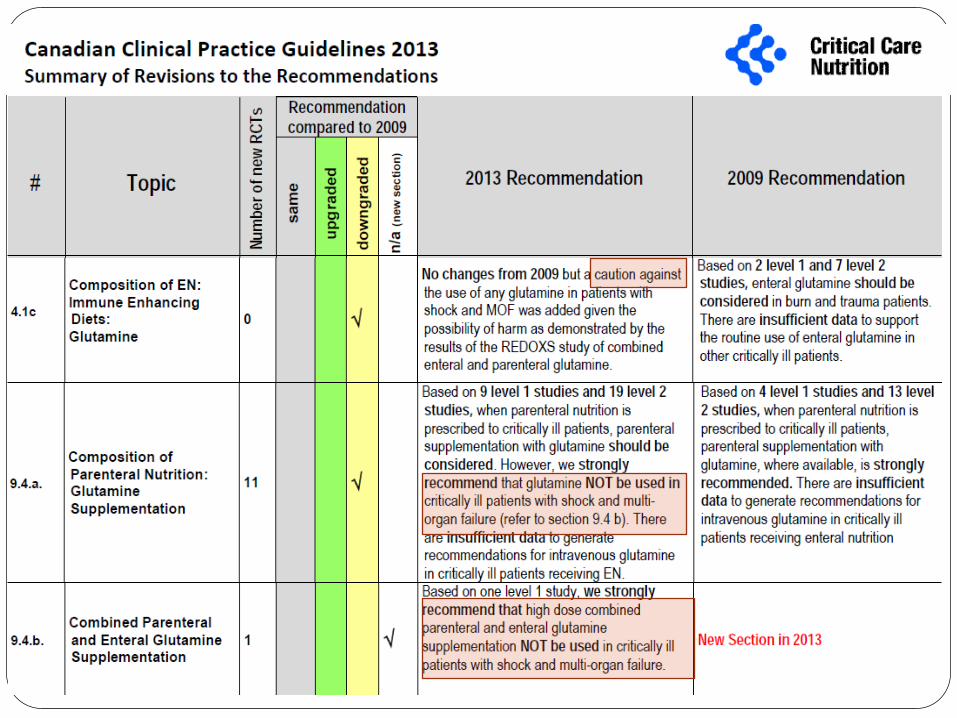
Warning # 2:
REDOXS and META-PLUS :
more questions than answers Preiser JC, Wernerman J.
JPEN J Parenter Enteral Nutr. 2013 Sep;37(5):566-7
Hope to confirm the beneficial
effect of glutamine replaced by a
frightening discovery
of potential toxicity!!!
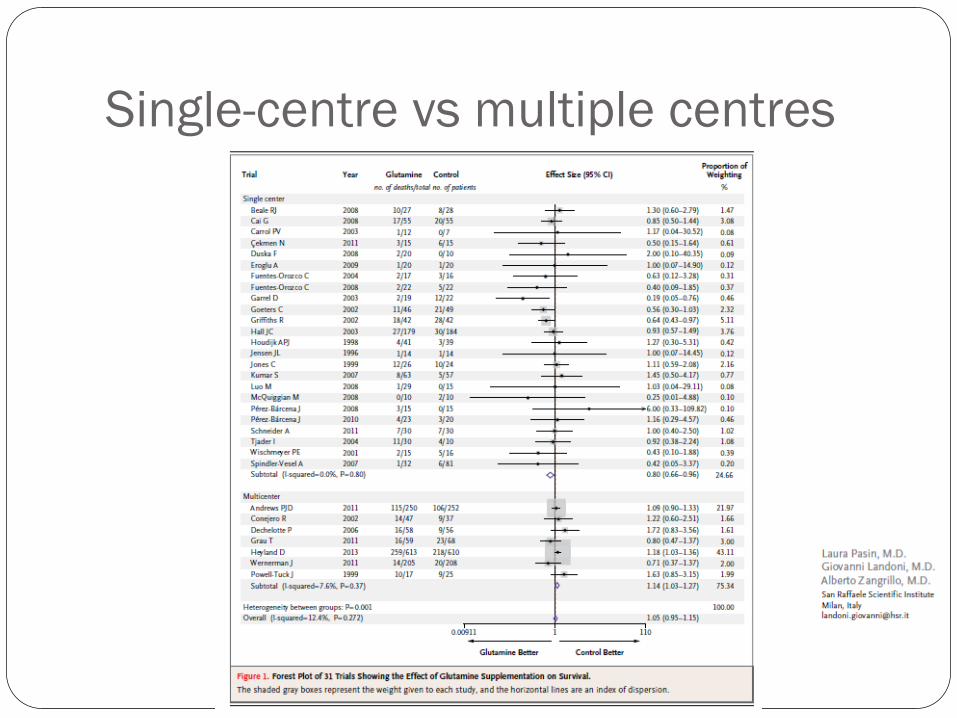
Single-centre vs multiple centres
FROM MARTIN LUTHER KING BACK TO
HIPPOCRATES
Primum non nocere
Glutamine is THE
life-saving
pharmaconutrient
First check
its safety
Au nom du principe de
précaution…
Deux exemples d’application
Péri-opératoire
Soins intensifs – réanimation
Suppléments en glutamine
Mesure du résidu gastrique
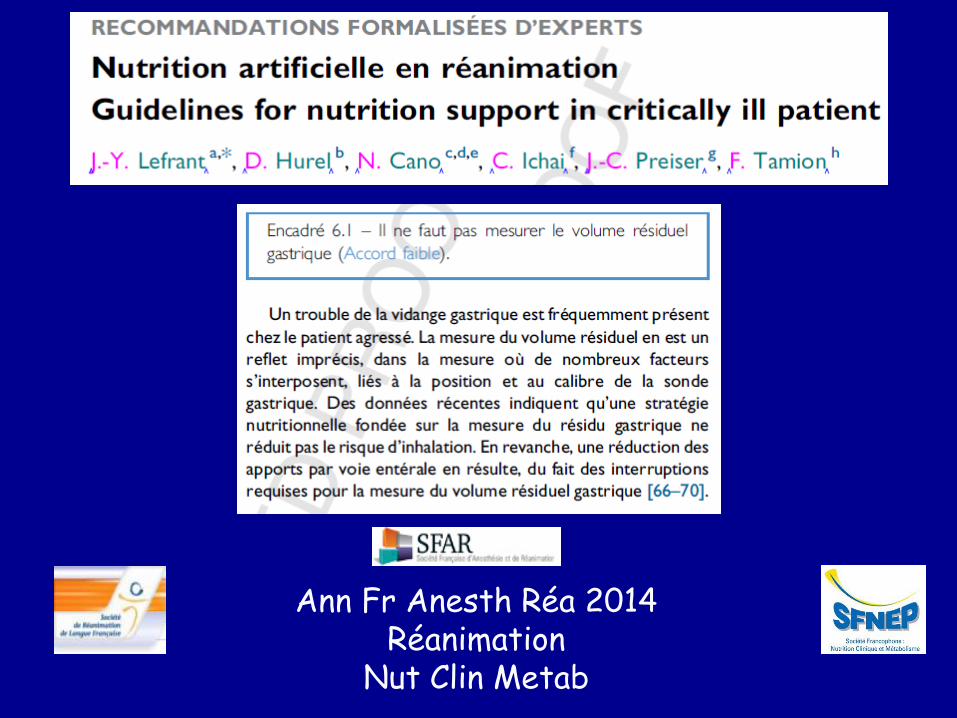
Ann Fr Anesth Réa 2014 Réanimation
Nut Clin Metab
0
50
100
150
200
250
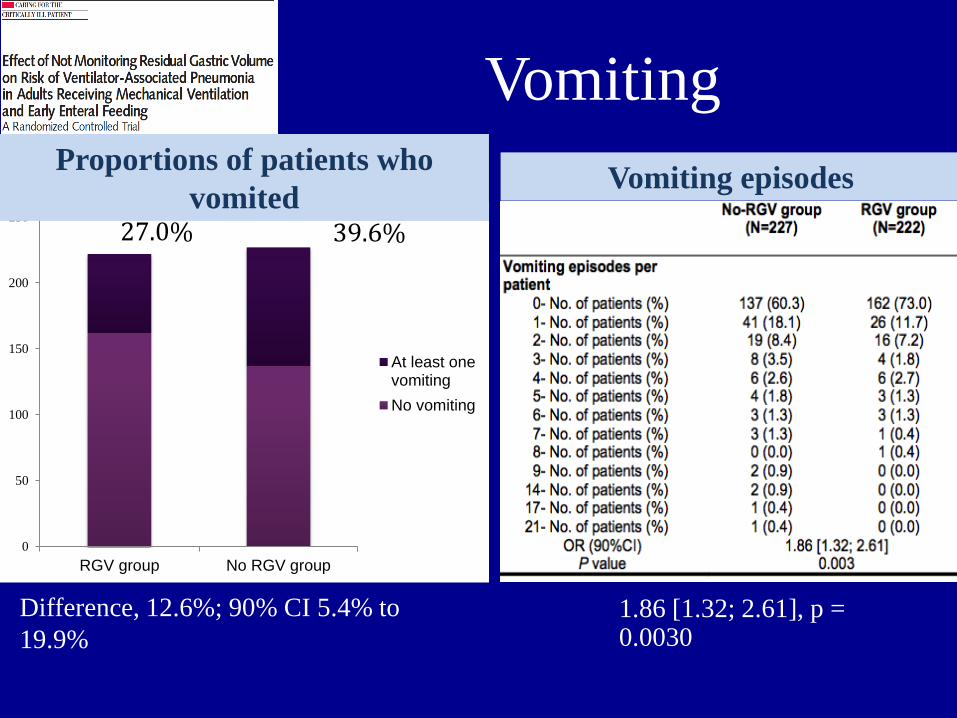
RGV group No RGV group
At least onevomiting
No vomiting
Vomiting
27.0% 39.6%
N patients
1.86 [1.32; 2.61], p = 0.0030
Difference, 12.6%; 90% CI 5.4% to
19.9%
Proportions of patients who
vomited Vomiting episodes
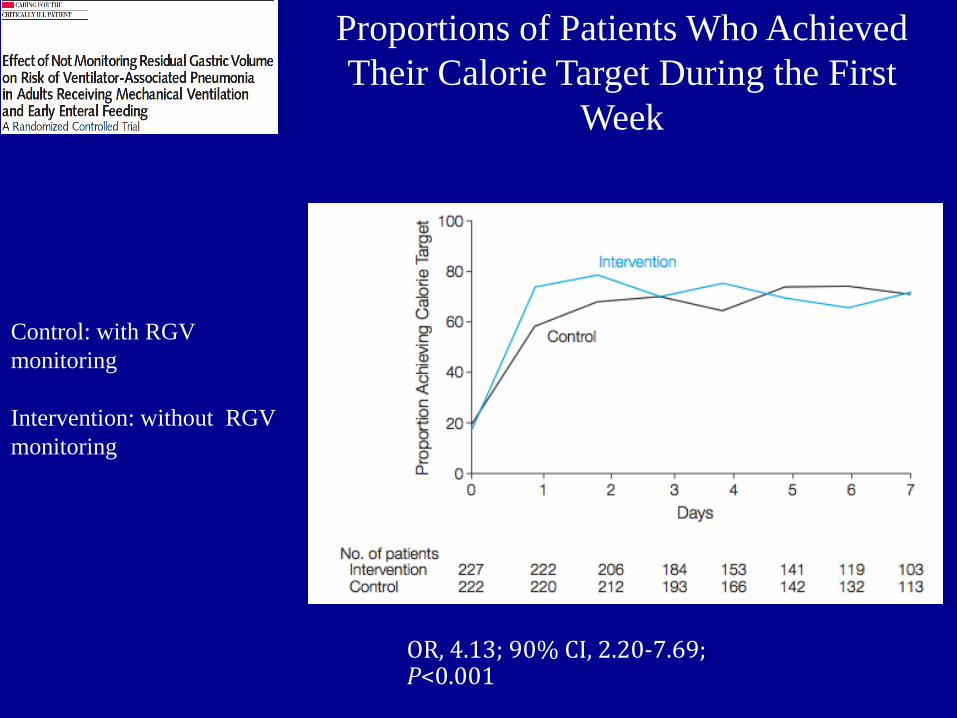
Proportions of Patients Who Achieved
Their Calorie Target During the First
Week
OR, 4.13; 90% CI, 2.20-7.69; P<0.001
Control: with RGV
monitoring
Intervention: without RGV
monitoring
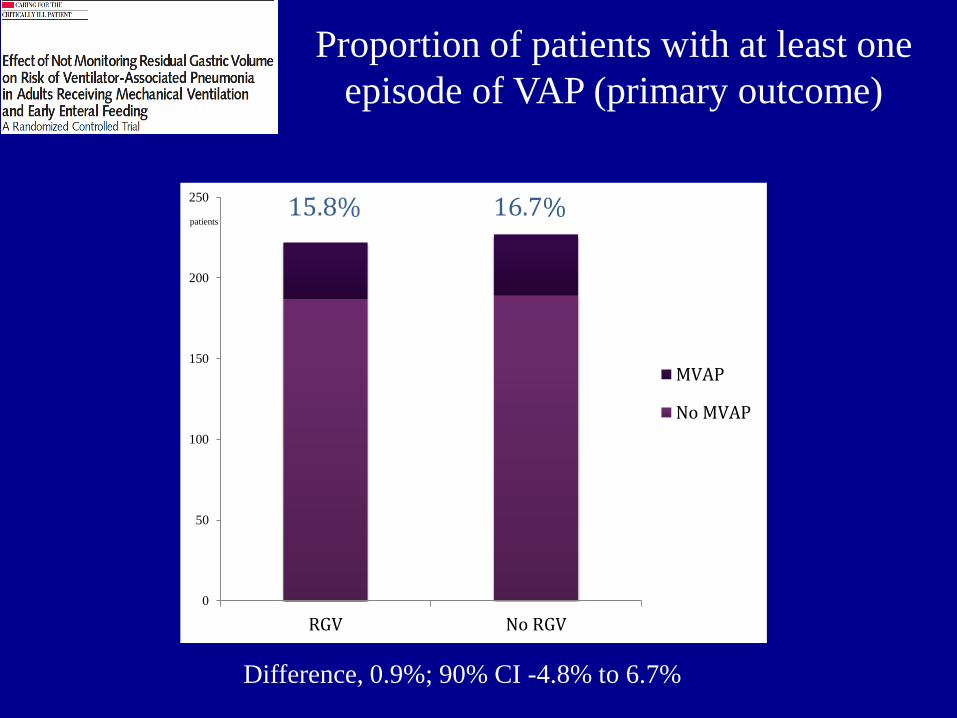
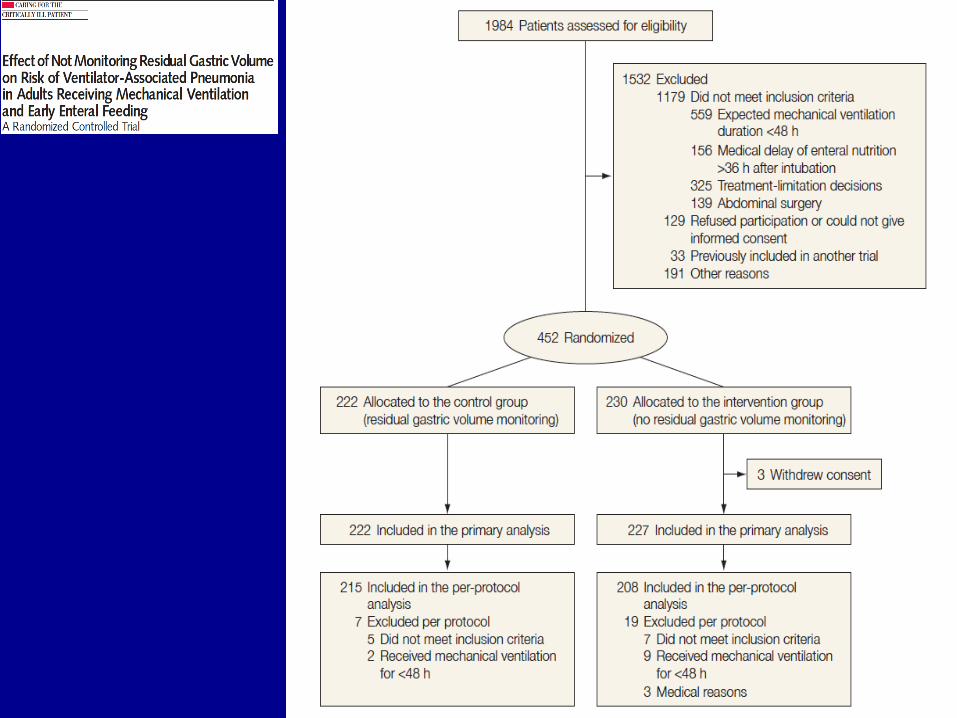
Proportion of patients with at least one
episode of VAP (primary outcome)
0
50
100
150
200
250
RGV No RGV
MVAP
No MVAP
15.8% 16.7%
Difference, 0.9%; 90% CI -4.8% to 6.7%
patients
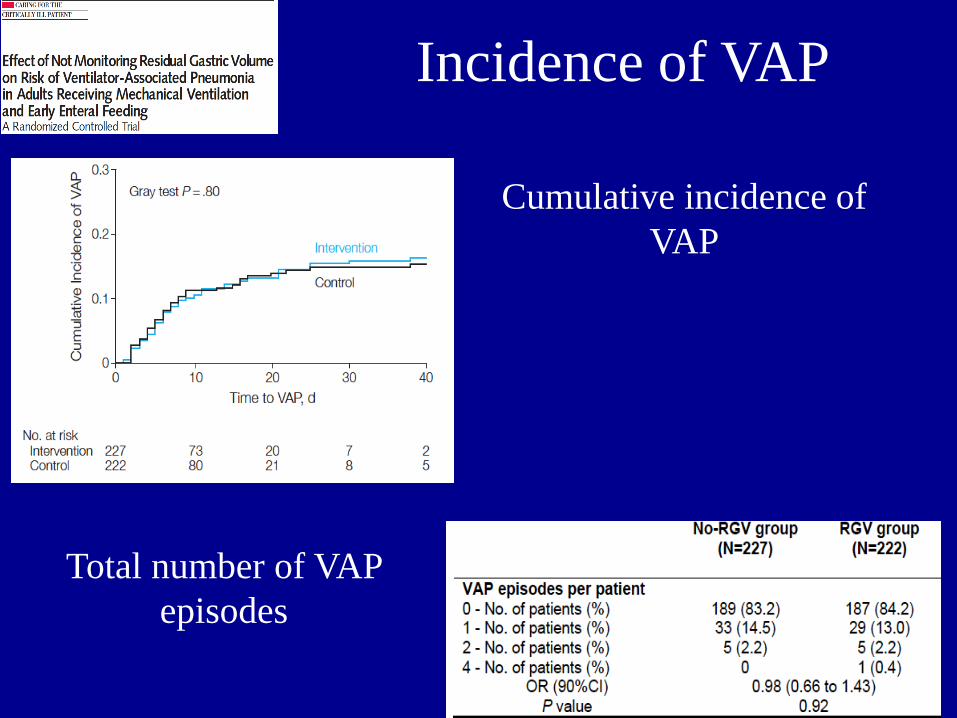
Incidence of VAP
Total number of VAP
episodes
Cumulative incidence of
VAP
Ou
« Ce qui était considéré comme
Vrai hier n’est plus forcément
La Vérité aujourd’hui »

Ou
« Ce qui était considéré comme
Vrai hier n’est plus forcément
La Vérité aujourd’hui »
Mais
efforçons-nous de la regarder
en face, quelles que soient
nos convictions