Embed Size (px)
Citation preview
3
Prise en charge d’un patient infecté par le VIH :
une nécessaire approche multidisciplinaire
Pr Corinne Isnard Bagnis, Paris
Lille janvier 2012

4
l Il consulte pour découverte récente d’une séropositivité
Monsieur X....53 ans
à dernière sérologie négative il y a 6 ans à 130 000 copies, CD4 350/ml, génotype sensible
a tous les ARV à ATCD familiaux : une mère diabétique de type 2
hypertendue multicompliqué récemment dialysée à ATCD personnels : une colique néphrétique droite
à 33 ans, une syphilis traitée il y a 9 ans (VDRL neg, TPHA 40)
à pas de co-infection VHB ou VHC à créatinine 87 micromôles/L, pas de protéinurie
l Que feriez vous comme examens complémentaires dans le bilan initial ?
1m68, 85 kg, BMI 31
caucasien, MSM, vit avec son compagnon séronégatif
Manager dans la finance

5
l Examens complémentaires pour l’infection VIH : à examen clinique complet à pression artérielle à tour de taille à vaccinations à NFS, TGO, TGP, PA, calcémie, phosphatémie, glycémie à jeun, sérologie
toxoplasmose, HAV, bilan lipidique (LDL, HDL, TG), HLA B5701, tropisme
l Examens complémentaires pour la fonction rénale : à bandelette urinaire pour protéinurie, leucocyturie, glycosurie à ECBU (confirmation si hématurie et leucocyturie) à estimation du débit de filtration glomérulaire (créatinine et formules)

4
LE RISQUE RENAL
Evaluation du risque rénal chez le patient infecté par le VIH Antécédents familiaux de maladie rénale Origine ethnique Taux des CD4-nadir des CD4 Charge virale Traitement néphrotoxiques ARV ou autres AINS ++++ Comorbidités cardiovasculaires et métaboliques
HTA Diabète
Co infection VIHC
28
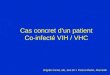
1 2 4 8
16 32 64
128
> 60 30 -59 < 30
Athe
rosc
lero
tic C
V Ev
ents
(per
100
0 Pe
rson
-Yea
rs)
Estimated Glomerular Filtration Rate (mL/min/1.73m2)
Albuminuria 0 mg/dL 30 mg/dL > 100 mg/dL
1 2 4 8
16 32 64
128
> 60 30 -59 < 30 H
eart
Fai
lure
Eve
nts
(per
100
0 Pe
rson
-Yea
rs)
Estimated Glomerular Filtration Rate (mL/min/1.73m2)
Albuminuria 0 mg/dL 30 mg/dL > 100 mg/dL
A B
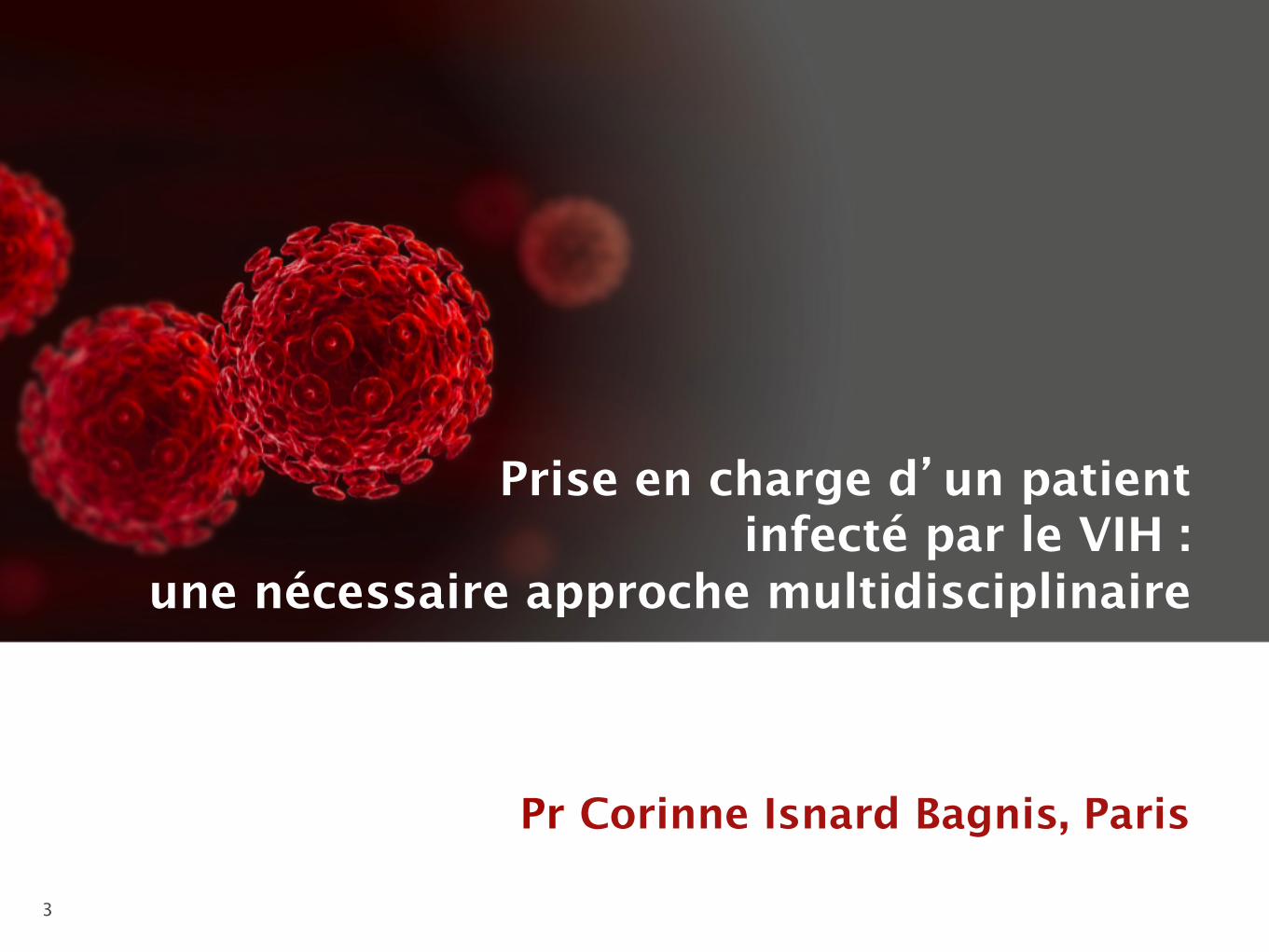
Incidence rates of atherosclerotic cardiovascular (CV) events (A) and heart failure (B),
stratified by eGFR and dipstick albuminuria level.
6
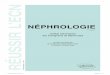
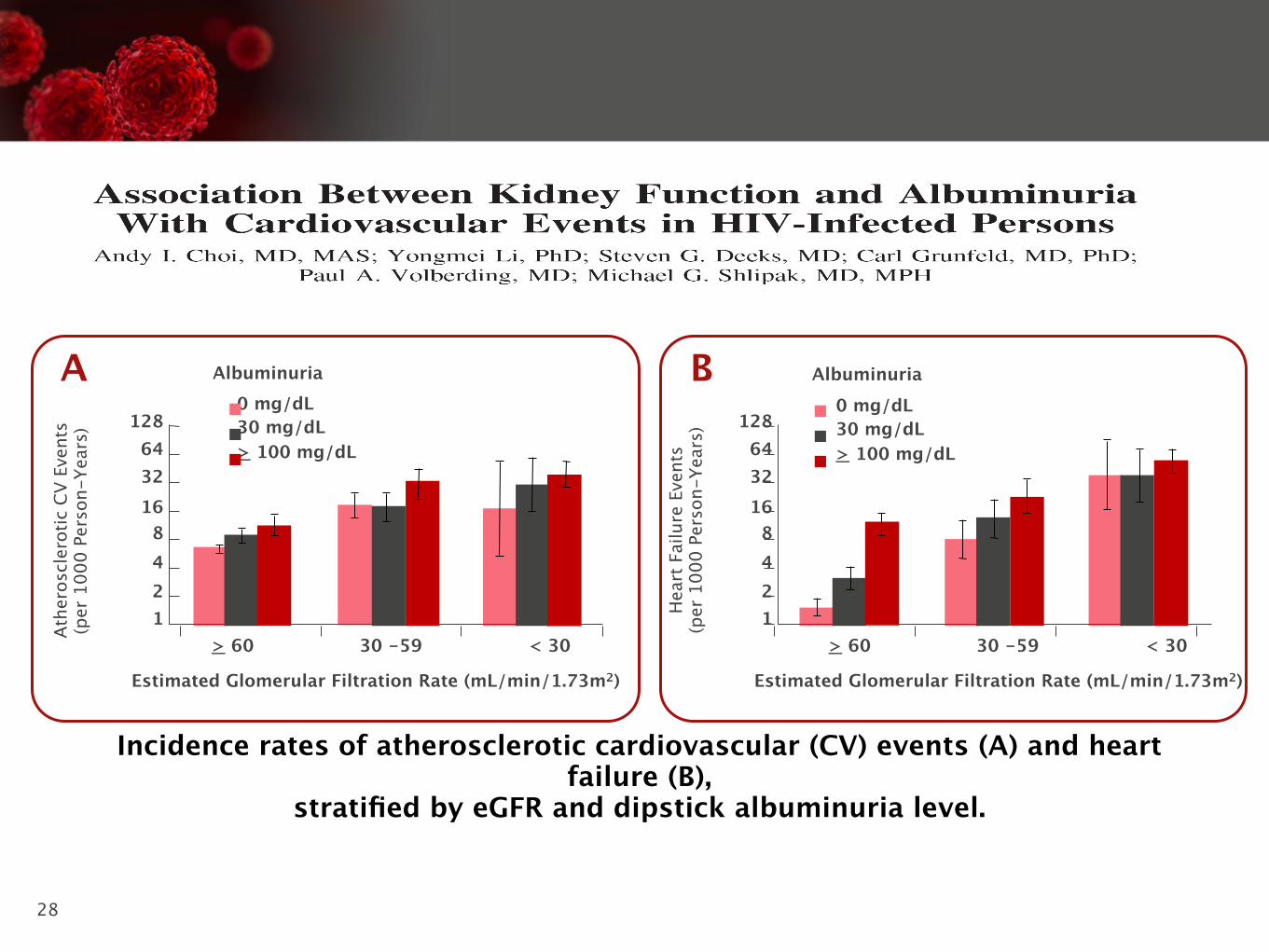
Recommandations 2011 EACS http://www.europeanaidsclinicalsociety.org/guidelines.asp
EACS Guidelines / 37
.LGQH\�GLVHDVH��GLDJQRVLV
eGFR (i)
�����P/�PLQ 30-59 mL/min < 30 mL/min
Prot
einu
ria (ii
)
83�&�(iii)������ 5HJXODU�)ROORZ�XS���&KHFN�ULVN�IDFWRUV�IRU�
CKD and nephrotoxic medication including ART (iv)
��'LVFRQWLQXH�RU�DGMXVW�drug dosages where appropriate (v)
��3HUIRUP�UHQDO�XOWUDVRXQG���8UJHQW�UHIHUUDO�WR�
nephrologist
83�&�(iii) 50-100
��&KHFN�ULVN�IDFWRUV�IRU�&.'�DQG�QHSKURWR[LF�PHGLFDWLRQ�including ART (iv)
��'LVFRQWLQXH�RU�DGMXVW�GUXJ�GRVDJHV�ZKHUH�DSSURSULDWH�(v) ��3HUIRUP�UHQDO�XOWUDVRXQG���,I�KDHPDWXULD�SUHVHQW�ZLWK�DQ\�OHYHO�RI�SURWHLQXULD�UHIHU�WR�QHSKURORJLVW�
��5HIHU�WR�QHSKURORJLVW�LI�QHZ�&.'�RU�SURJUHVVLYH�GHFOLQH�LQ�eGFR
83�&�(iii) > 100
Management of HIV-associated renal disease (vi)
Prevention of progressive renal disease Comment1� Antiretroviral therapy 6WDUW�$57�LPPHGLDWHO\�ZKHUH�+,9�DVVRFLDWHG�QHSKURSDWK\�
�+,9$1��(vii)�RU�+,9�LPPXQH�FRPSOH[�GLVHDVH�VWURQJO\�VXVSHFWHG��5HQDO�ELRSV\�WR�FRQ¿UP�KLVWRORJLFDO�GLDJQRVLV�UHFRPPHQGHG�
2� Start ACE inhibitors or angiotensin-II receptor antagonists if: D��+\SHUWHQVLRQ��DQG�RU�E��3URWHLQXULD�
Monitor eGFR and K+ level closely on starting treatment or increasing dose D��%ORRG�SUHVVXUH�WDUJHW������������PP+J
3� General measures: D��$YRLG�QHSKURWR[LF�GUXJV�E��/LIHVW\OH�PHDVXUHV��VPRNLQJ��ZHLJKW��GLHW��F��7UHDW�G\VOLSLGDHPLD�(viii)�DQG�GLDEHWHV�(ix)
G��$GMXVW�GUXJ�GRVDJHV�ZKHUH�QHFHVVDU\�
&.'�DQG�SURWHLQXULD�DUH�LQGHSHQGHQW�ULVN�IDFWRUV�IRU�&9'�
L� H*)5�� XVH� D0'5'� EDVHG� RQ� VHUXP� FUHDWLQLQH�� JHQGHU�� DJH� DQG�HWKQLFLW\��,I�QRW�SUHYLRXVO\�NQRZQ�WR�KDYH�&.'��UHDVVHVV�ZLWKLQ���ZHHNV
LL� 8ULQDO\VLV��XVH�XULQH�GLSVWLFN�WR�VFUHHQ�IRU�KDHPDWXULD��7R�VFUHHQ�IRU�SURWHLQXULD��XVH�XULQH�GLSVWLFN�DQG�LI������FKHFN�83�&��RU�VFUHHQ�ZLWK�83�&��3URWHLQXULD�GH¿QHG�DV�SHUVLVWHQW�LI�FRQ¿UPHG�RQ�����RFFDVLRQV�!�����ZHHNV�DSDUW��,I�83�&�QRW�DYDLODEOH��XVH�8$�&��VHH�QRWH�iii)
LLL� 83�&� LQ� VSRW� XULQH� �PJ�PPRO�� LV� SUHIHUUHG� WR�8$�&�DV�GHWHFWV� WRWDO�XULQDU\�SURWHLQ� VHFRQGDU\� WR�JORPHUXODU�$1'� WXEXODU�GLVHDVH��8$�&�ODUJHO\�GHWHFWV�JORPHUXODU�GLVHDVH�DQG�FDQ�EH�XVHG�IRU�VFUHHQLQJ�IRU�+,9�DVVRFLDWHG�UHQDO�GLVHDVH�ZKHUH�83�&�LV�QRW�DYDLODEOH��EXW�LV�QRW�DSSURSULDWH� IRU� VFUHHQLQJ� IRU� WXEXODU� SURWHLQXULD� VHFRQGDU\� WR� GUXJ�QHSKURWR[LFLW\� �H�J�� WHQRIRYLU���6FUHHQLQJ�YDOXHV� IRU�8$�&�DUH��������������DQG�!�����8$�&�VKRXOG�EH�PRQLWRUHG�LQ�SDWLHQWV�ZLWK�GLDEHWHV�PHOOLWXV��83&�UDWLR�LV�FDOFXODWHG�DV�XULQH�SURWHLQ��PJ�/����XULQH�FUHDWLQLQH��PPRO�/���PD\�DOVR�EH�H[SUHVVHG�DV�PJ�PJ��&RQYHUVLRQ�IDFWRU�IRU�PJ�WR�PPRO�FUHDWLQLQH�LV�[�����������
LY� &KHFN� ULVN� IDFWRUV� IRU�&.'��DQG� UHSHDW�H*)5�DQG�XULQDO\VLV�DV�SHU�VFUHHQLQJ�WDEOH��VHH�S��6)
Y� 'RVH�PRGL¿FDWLRQ�RI�$59V�LQ�FDVH�RI�LPSDLUHG�UHQDO�IXQFWLRQ��VHH�RQOLQH�WDEOH�IRU�“Indications and tests for proximal renal tubulopathy”
YL� -RLQW�PDQDJHPHQW�ZLWK�D�QHSKURORJLVWYLL� +,9$1� VXVSHFWHG� LI� EODFN� HWKQLFLW\� � 83�&� !� ���� PJ�PPRO� � QR�
KDHPDWXULDYLLL�6HH�S��31L[� 6HH�S��29

7

16
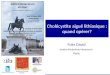
l Protéinurie > 300 mg/24 heures l Albuminurie normale <30 mg/24 heures
l Anomalies du sédiment urinaire : à Hématurie pathologique : GR>10/mm3 ou 10 000/ml à Leucocyturie pathologique : GB>10/mm3 ou 10 000/ml
l Quel que soit le DFG, la persistance pendant plus de 3 mois de marqueurs d’atteinte rénale témoigne d’une maladie rénale qui impose un diagnostic étiologique et/ou une surveillance néphrologique (stade 1 classification NKF).

17
l La mesure d’une protéinurie à 0.3 g/L équivaut à une excrétion protéique de 600 mg par 24hsi la diurèse est de 2L
Bandelettes
Trace < 0.3 g/L
+ 0.3-1 g/L
++ 1-3 g/L
+++ 3-10 g/L
++++ >10 g/L

18
Ratio protéine/ créatinine
Protéine (mg/L)/créatinine (g/L) sur échantillon
Proteine (mg/L)/créatinine (mmol/L)
Urines 24 h (mg/24 h)
Normal <30 mg/g < 2mg/mmol < 30 mg/J
Microalbuminurie 30-300 mg/g 2-22 mg/mmol 30-300
mg/J
Protéinurie ≥ 300 mg/g ≥ 22 mg/mmol ≥ 300 mg/J

19
l Il vous apporte un bilan biologique
Monsieur X....55 ans
à CD4 330, CV 70 000 copies/ml à créatinine : 105 micromôles/L, protéinurie 0,4
gr/L, MDRD 72 ml/min/1.73 m2
à hématurie microscopique à la bandelette à glycémie à jeun normale, LDL 1.8 gr/L, HDL 0,45
gr/L, TG 2 gr/L, CH Tot 2.6 gr/L à pas de co-infection VHB ou VHC
l Que faites vous pour explorer l’hématurie microscopique ?
1m78, 83 kg, BMI 26
moins 5 kg
PA 145/95 mmHG assis à droite

Hématies à l’ECBU
Echographie anormale Echographie normale
Lithiase è ASP
Tumeur è scanner
Kystes
Hématome
Malformation(+ autre cause ?)
Thrombose veine rénale(nouveau-né,maladie
thrombogène)
Infection urinaire
Bactérienne : cystite, urétrite…(+ autre cause)
Bilharziose ?Pays d’endémie oeufs dans les
urines
Protéinurie ou microalbuminurie Hématies dysmorphiques
Pas de protéinurie Hématies normales
Syndrome “néphrétique”(HTA, oedème, oligurie…)
C3 bas, évolutionbrève : GN aiguë
C3 nul ou bas, évolution prolongée è PBR
ATCD familiaux, surdité : Alport è biopsie cutanée, PBR
Contexte cliniqueè purpura rhumatoïde è LED, SHU
Hématuries récidivantes è GN à IgA ? è PBR
Protéinurie-hématurie isolée permanemie è PBR
Lithiase ? : cristallurie calciurie, oxalurie
échographie répétées
Drépanocytose ? Ethnie électrophorèse Hb
Coagulopathie ? (+ autre cause) è hémostase
Pas de cause probable Hématurie abondante ou répétée sang rouge ou caillots è cystoscopie
Saignement vésical ou urétral
Saignement urétéral unilatéral : cause
vasculaire ? è scanner artériographie 20
21
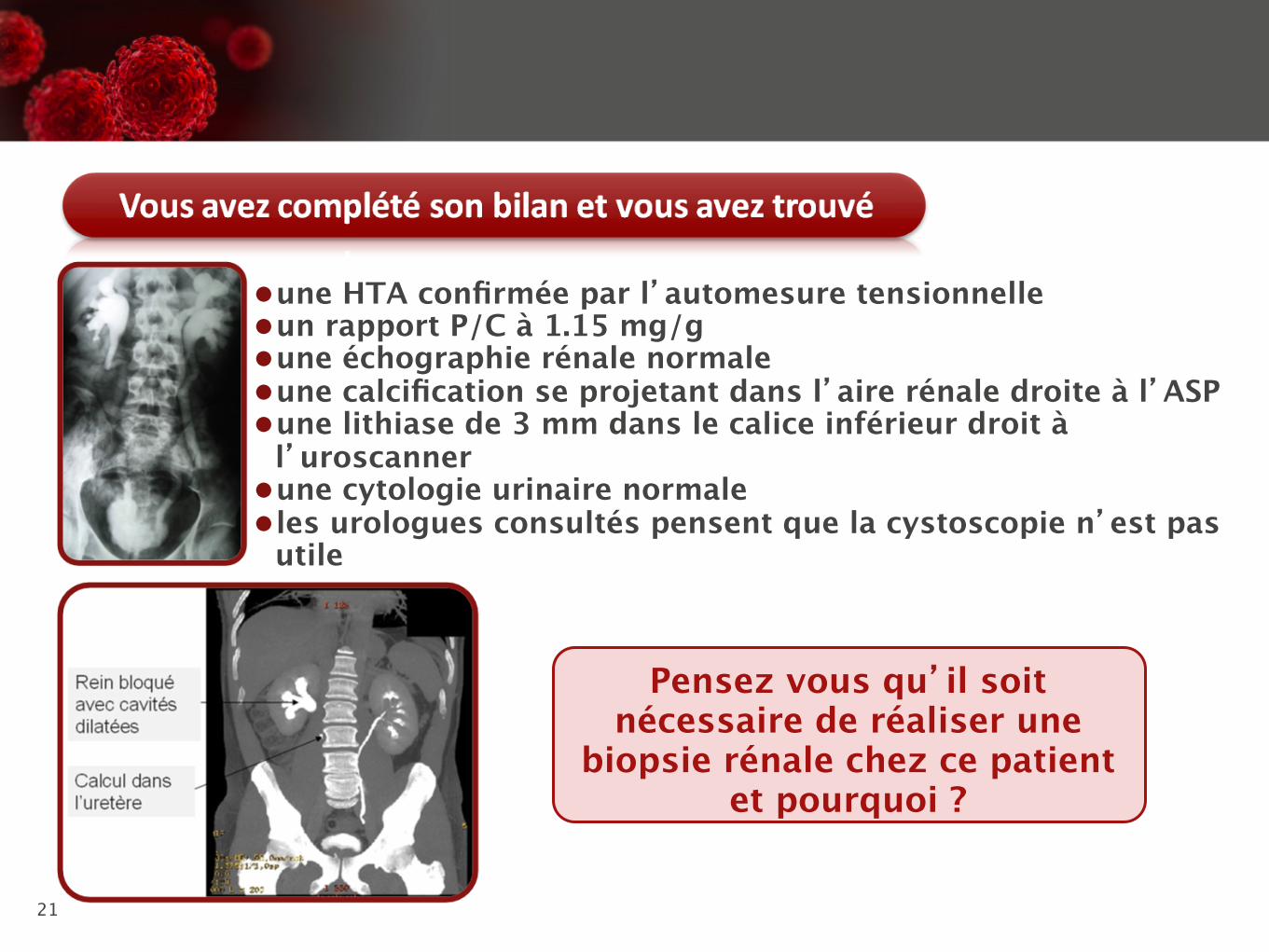
l une HTA confirmée par l’automesure tensionnelle l un rapport P/C à 1.15 mg/g l une échographie rénale normale l une calcification se projetant dans l’aire rénale droite à l’ASP l une lithiase de 3 mm dans le calice inférieur droit à
l’uroscanner l une cytologie urinaire normale l les urologues consultés pensent que la cystoscopie n’est pas
utile
Pensez vous qu’il soit nécessaire de réaliser une
biopsie rénale chez ce patient et pourquoi ?

Lithiases et VIH

Lithiases dans la population générale
• 10% de la population française adulte a fait ou fera une colique néphrétique au cours de sa vie - taux de récidive 50%
• augmentation de la prévalence depuis 30 ans • Deux hommes pour une femme (10 à 15% de hommes et
3 à 5% des femmes) • 1 à 2% des entrées d’un service d’urgence - 120 000
épisodes par an (interventions urologiques, arrêts de travail)
• 5.3 billions de dollars/an aux USA • 200 000 patients ont une maladie lithiasique sévère • 2% des dialysés ont perdu leur fonction rénale à cause
d’une maladie lithiasique
• douleur brutale intense lombaire ou lomboabdominale à type de colique intermittente, irradiation vers les OGE • hématurie • nausées, vomissements • dysurie, pollakiurie, impériosité, brulûres
urinaires (calcul ureteral, sable) • anxiété, agitation • pas de fièvre
la colique «frénétique»

17
Recommandations de prise en charge de la CN
• bandelettes +/- ECBU • créatininémie, hémogramme • traitement antalgique : AINS IV +/- paracétamol ou morphiniques
(morphine titrée intraveineuse) • ketoprofène 100 mg dans 100 ml de SG5% ou de serum
physiologique en 20 minutes trois fois par jour • si la douleur persiste à 20 mins, refaire un bolus si elle persiste à
40 mins 5 mg de morphine • boissons libres • femmes enceinte (AINS CI au 3eme trim, morphiniques sauf si
travail) • IRC pas d’AINS • antispasmodiques non conseillés • avis urologique surtout si CN hyperalgique, fébrile, anurique,
rupture de la voie excrétrice ... Recommandations de la Société Française de Médecine d’Urgence

18
CAT devant une lithiase
• découverte en consultation – Uroscanner basse dose +++ – pas de symptômes et calcul < 5 mm :
surveillance, exploration métabolique et diététique – pas de symptômes et calcul > 5 mm : traitement
urologique du calcul – symptômes : traitement urologique du calcul
PIerre Conort et Isabelle Tostivint, La revue du Praticien, 2011

19
CAT devant une lithiase • Découverte aux urgences (CN)
– pyélonéphrite aigue obstructive ou anurie : TDM basse dose non injecté • drainage en urgence • traitement urologique
– CN simple • AINS morphine • ASP/écho ou TDM basse dose non injecté
– douleur OK : élimination – douleur OK calcul persistant : traitement urologique – persistance de la douleur : drainage en urgence :
traitement urologique du calcul
19 PIerre Conort et Isabelle Tostivint, La revue du Praticien, 2011
20
Que devient le calcul ? • l’avenir du calcul est déterminé par sa taille et sa localisation • taux d’évacuation du calcul :
– 12, 22 et 445% pour un calcul situé dans la partie proximale, médiane ou distale de l’uretère
– 55, 35 et 8% pour des calculs de <4, 4-6 et >6 mm de diamètre • traitement favorisant l’évacuation du calcul : AINS, stéroides, inhibiteurs
calciques (diminue la contraction musculaire et le spasme urétéral), alpha bloquants (tamsulosine Josir, terazosin, Dysalfa, doxazosine Zoxan) (diminue le tonus musculaire urétéral et la force/fréquence du péristaltisme)
• métanalyse 9 essais randomisés : recevoir un ICC ou A- (avec ou sans stéroides et contre rien ou placebo) augmente de 65% de risque d’émission du calcul
• en France pas d’AMM pour la tamsulosine dans cette indication • si le calcul est < 10 mm et que la douleur est contrôlée, le traitement
«vasodilatateur» est conseillé par les recommandations américaines (surtout si calcul «distal»)
Moe et al, Pharmacotherapy of Urolithiasis, Kidney Int 2011.

Composition des lithiases
• lithiases oxalo calciques – Wedellite : oxalate de calcium dihydraté
(hypercalciurie++) oxalate dependant – Whewellite : oxalate de calcium monohydraté
forme oxalodépendante (hyperoxalurie++) • Phosphate • Phosphoammoniacomagnésien - struvite • Cystine • Acide urique

Prévalence relative des lithiases en fonction de leur composition
• Oxalate de calcium pur ou avec un faible composant de phosphate de calcium 59% • Phosphate de calcium prédominant 10% • Acide urique 17% • Struvite 12% • Cystine ou autres 2% • plaques de Randall* 22%
Johri et al, Nephron Clin Pract, 2010 * plaque de Randall dépôts de phosphate dans la médulllaire profonde mais peuvent s’étendre jusqu’à la papille ou ils servent de support de cristallisation

23
homme femme
jeune whedellite : 45% des calculs
whewellite ++ et phosphocalciques,
wedellite+
moyen whewellite 59% entre 50-59 ans
whewellite 54% entre 40 et 49 ans
agé acide urique 31% après 70 ans
acide urique 20% après 70 ans
24
Facteurs de risque
• multifactoriel nutritionnels • augmentation de la concentration des urines • apports en protéine • apports en sel • excès de sucres raffinés • aliments riches en oxalate • hyperparathyroidie secondaire (femme âgée) • tubulopathies • infections à répétitions • malformations de l’appareil urinaires • maladies inflammatoires du tube digestif • ileostomie • immobilisation prolongée
24

Pourquoi des lithiases ? • Facteurs génétiques (Dent, bartter, acidose tubulaire distale,
cystinurie, polymorphismes de CFEX, biochimiques, diététiques, sociétaux
• Déséquilibre entre facteur lithogènes (calcium, oxalate, acide urique dans les urines) et facteurs protecteurs (magnésium, citrate dans les urines)
• Facteurs de risque : – âge (hypercalciurie et sujet jeune, diabète et
hyperparathyroïdie primaire et sujet âgé), – obésité (40% des hommes obèses ont une lithiase urique)
par insulinoresistance et diminution de l’ammoniogénèse rénale conduisant à un abaissement du pH urinaire – ATCD familiaux x par 3 ou 4 le risque

26
Bilan métabolique des lithiases

27
Bilan métabolique des lithiases
B40
la présence d’une anomalie biologique n’est pas la preuve qu’elle est responsable de la lithiase...
La présence d’une anomalie biologique n’est pas la preuve qu’elle est la cause de la lithiase…

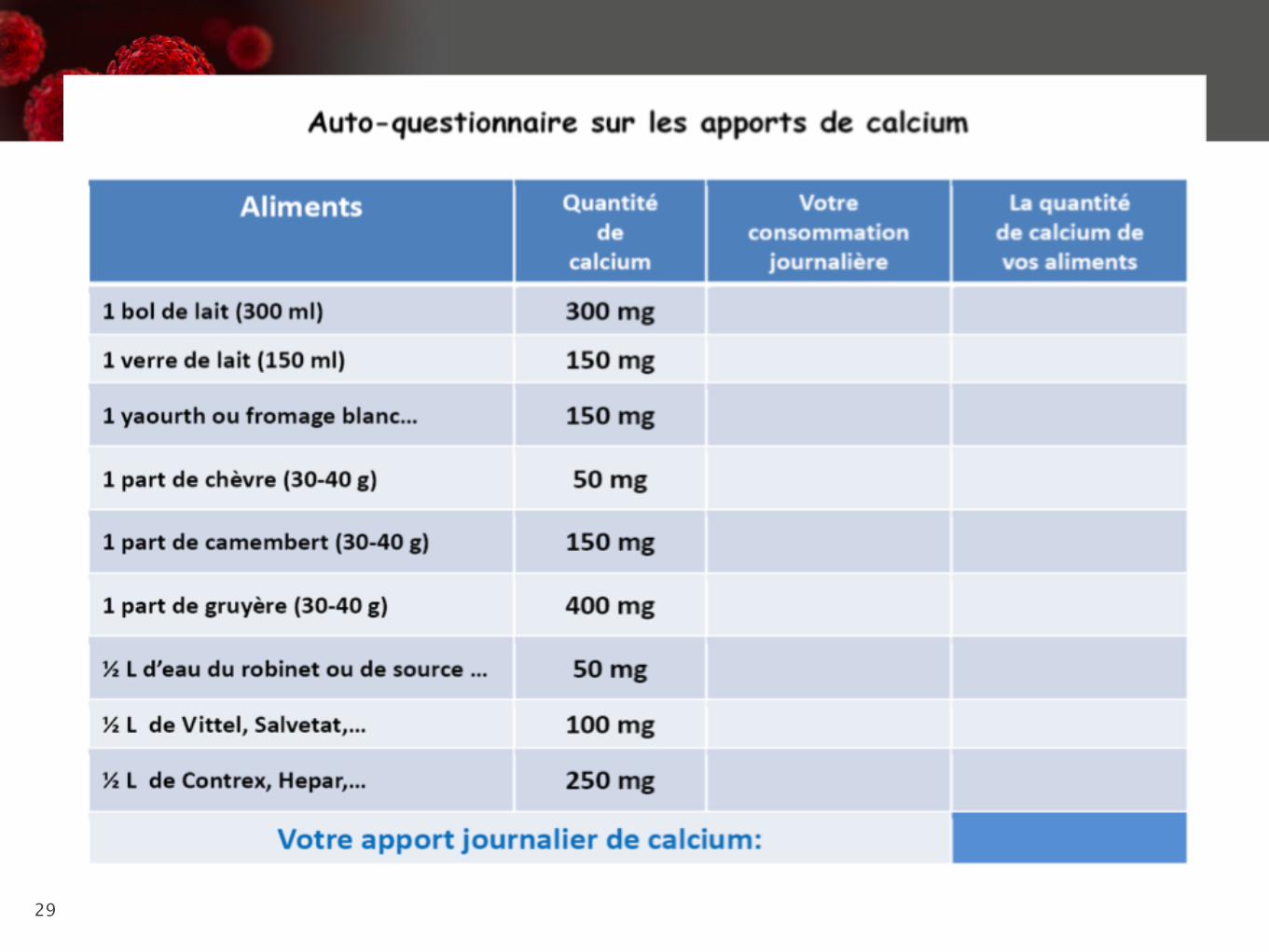
28
Zone de risque cristallogène
• CaU > 3.8 mmol/L • CaU> 1 mmol/10 kg de poids sur 24H • PhU > 24 mmol/L • oxalurie > 0.3 mmol/L • Citraturie < 1 mmol/L • magnesurie< 1.5 mmol/L • densité urinaire > 1012
28
29

Lithiases médicamenteuses
1% des lithiases en France
calculs constitués en tout ou en partie d’un médicament ou de ses
métabolites urinaires
calculs métaboliques induits par les effets des médicaments sur l’excrétion de solutés lithogènes
ou sur le pH urinaire (médicament absent de la lithiase)
0.4% IP+++++ 0.25% ?
découverte tardive parfois à distance de l’arrêt du traitement

Nature et fréquence des constituants lithiasiques identifiés dans les calculs urinaires (laboratoire Cristal, Necker)
Famille de médicaments Nombre de cas (%) Constituants identifiés dans les calculs
Antiprotéases Indinavir Atazanavir
64 (49.2%) 36 28
Indinavir monohydraté Atazanavir
Antinucléosidiques Efavirenz
2 (1.5%) 2
Métabolites de l’Efavirenz
Antihypertenseur Triamtérène
21 (16.2%) 21
Triamtérène et métabolites
Sulfamides Sulfadiazine
18 (13.3%) 18
N-acétylsulfadiazine
Antibiotiques Ceftriaxone Amoxicilline Ciprofloxacine
9 (6.9%) 6 2 1
Ceftriaxone de calcium Amixicilline trihydratée Ciprofloxacine, sel de magnésium
Trisilicate de magnésium (antiacides) 15 (11.2%) Silice opaline
Allopurinol 1 (0.8%) Oxypurinol (+ xanthine)
Total 130 (100%)
Daudon M et Knebelmann B, Dossier lithiase de la Revue du Praticien, mars 2011, vol 31, 374.
Facteurs de risque de lithiase médicamenteuse
• Lié au patient : – Notion de lithiase antérieure
• Lié au médicament : – Surdosage
• Présence d’un calcul in situ • Faibles apports hydriques
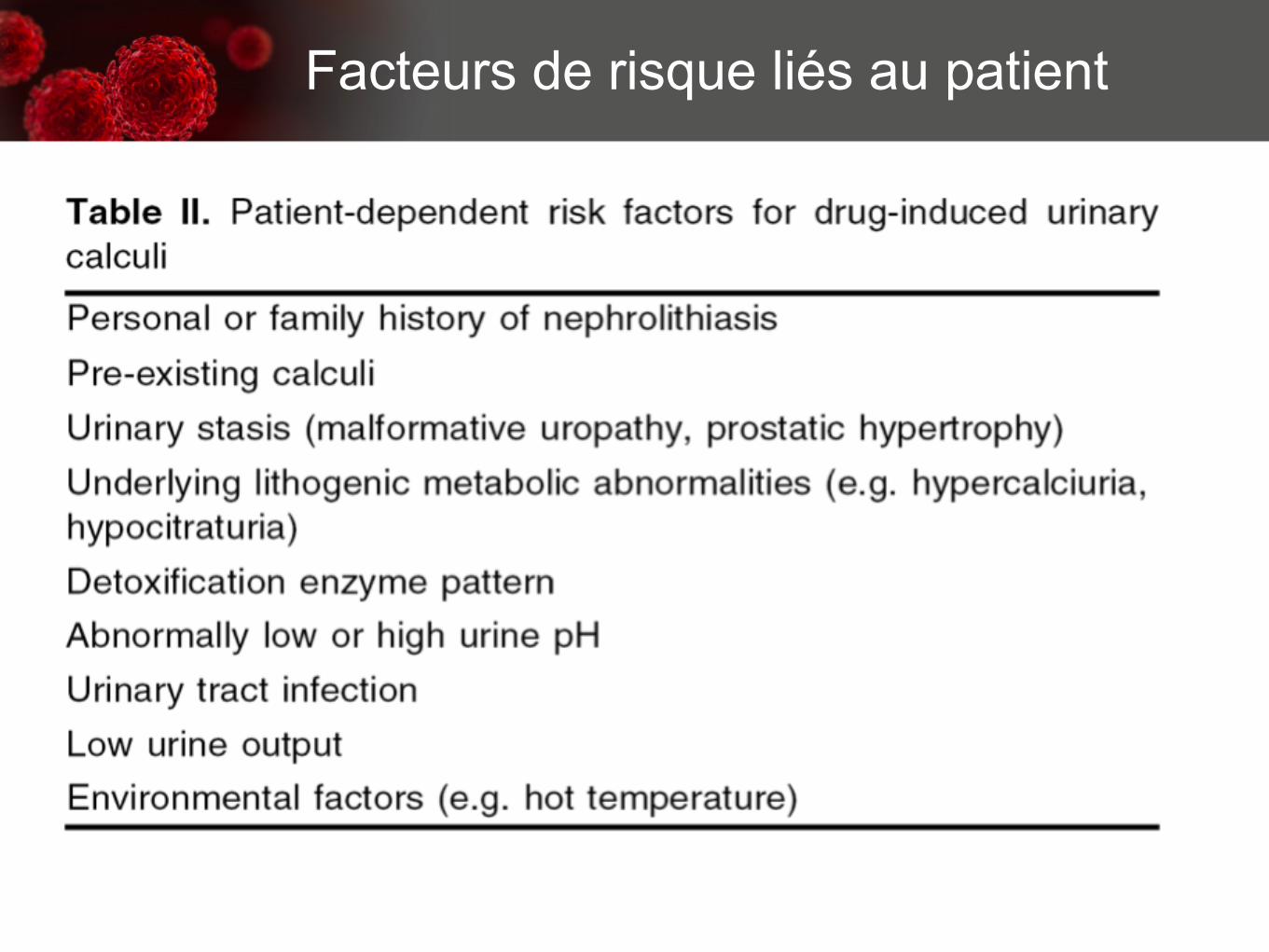
Facteurs de risque liés au patient
Daudon et al, Drug-induced renal calculi, Drugs 64(3), 245-275, 2004.

Facteurs de risque liés au médicament

Facteur de risque lié au médicament : Exemple de l’indinavir
• Fréquence des lithiases : 9 à 36% • Présentation clinique : colique néphrotique, douleur
lombaire, dysurie • Calcul pur d’indinavir = radiotransparent à la RX et au
scanner sans injection (échographie, UIV, scanner injecté)
• Élimination spontanée du calcul ou intervention urologique mais pas de traitement par ultrasons (nature protéique du calcul) sauf si lithiase mixte contenant du calcium
• Complications : IRA (néphropathie interstitielle avec cristaux dans les tubes collecteurs corticaux et médullaires (reversible à l’arrêt du traitement)

• Le calcul est beige, irrégulier, 2-6 mm • Contiennent de l’indinavir monohydrate de 3 à 97% • 2/3 des calculs sont purement constitués d’indinavir
• L’indinavir est présent dans 97% des cas dans le noyau • 30% des calculs contiennent de l’oxalate/phosphate de Ca
• L’indinavir est absorbé rapidement et 20% de la dose est éliminée dans les urines dans les 24h (11% sous forme inchangée)
• La solubilité de l’indinavir dans les urines est très dépendante du pH (10 fois supérieure à pH 5 qu’à pH 6 en solution aqueuse)
• Pour une administration de 800 mg chez un patient dont le volume urinaire est de 1500 ml/jour, la concentration urinaire d’indinavir attendue est d’environ 200-300 mg/L ce qui est à la limite de la solubilité
• Les principaux facteurs de risque de lithiase à l’indinavir sont : – pH>5.5 – Les épisodes de déshydratation (chaleur, diarrhée) – Prise concomitante d’acyclovir ou de cotrimoxazole – Co infection VHC (diminution du catabolisme hépatique de l’indinavir et augmentation de l’excretion rénale) – Concentrations plasmatiques élevées d’indinavir
• Prévention : – acidification des urines (difficile à réaliser à long terme et favorise les lithiases uriques) – Augmentation des apports hydriques (150 ml après chaque prise et chaque heure pendent deux heures) – Coca cola®, acide phosphorique
Exemple de l’indinavir

37
Nelfinavir et amprénavir
• 1er cas en 2002 • lithiase 99% constituée de médicament • 1 à 2% de la dose ingérée est retrouvée dans
les urines • la même patiente en 2008 expulse une lithiase
composée d’amprénavir 95% et ritonavir 5%
37 Engeler et al, J of Urology, 2002. Feicke et al, Antiviral Therapy, 2008

38
Lopinavir
• 4 cas cliniques peu documentés
38
39
ATAZANAVIR • premier cas français ! • cirrhose B • ATCD de lithiases oxalocalciques en 1988 et 2000 • sept 2003 DDI, TNF, EFV • Sept 2004 EMT, TNF, ATZr • CN une fois par mois à partir d’oct 2005 et tous les
15 jours à partir de mars 2006 • non calmées par les AINS et l’alcalinisation • calculs à droite - urétéroscopie et JJ en juin 2006 • lithiases d’ATZ pur
Pacanowski et al, AIDS 2006

40
ATAZANAVIR
• 11 cas français • étude rétrospective dans 7 centres • entre 2004 et 2007 • 1134 patients traités - 11 lithiases (0.97%) • 4 patients avaient un ATCD de lithiase • 23 mois en moyenne après le début du
traitement • taux résiduels d’ATZ normaux • 8 calculs pur d’ATZ et 4 mélangés (oxalate de
Ca) • radiotransparents, friables, beiges 40

41
Couzigou et al CID 2007

42
ATAZANAVIR
• très lié aux protéines • métabolisée par le CYP 3A4 en dérivés libres et
glucuroconjugués dans la bile • 7% de la dose est excrétée inchangée dans les
urines • la solubilité de l’ATZ est augmenté à pH acide

Atazanavir Exposure is Associated With Increased Rate of Renal Stones Compared With Efavirenz, Lopinavir and Darunavir
• étude monocentrique, 45 mois • comparaison de la prévalence des calculs rénaux
chez les patients infectés par le VIH traités par une combinaison associant ATZ/r versus EFV,LPV/r et DRV/r • diagnostic de calcul radiologique même si pas de
lithiase visualisée (echo, Rx, CT, UIV en excluant ou non les patients ayant reçu antérieurement un traitement par IDV ou ATZ)
• As ARV-associated renal stones are often radiolucent, abnormalities in the collecting systems compatible with obstruction or dilation secondary to a recently passed stone, were included as evidence of stones in the context of an appropriate clinical history
Rockwood et al, IAS 2011
44
Atazanavir Exposure is Associated With Increased Rate of Renal Stones Compared With Efavirenz, Lopinavir and Darunavir
• les patients exposés à l’ATZ et ayant eu une lithiase avaient un taux de bilirubine moyen supérieur à celui des patients n’ayant pas de lithiase et traités par ATZ : prédisposition génétique pour les métaboliseurs lents ?
37
45
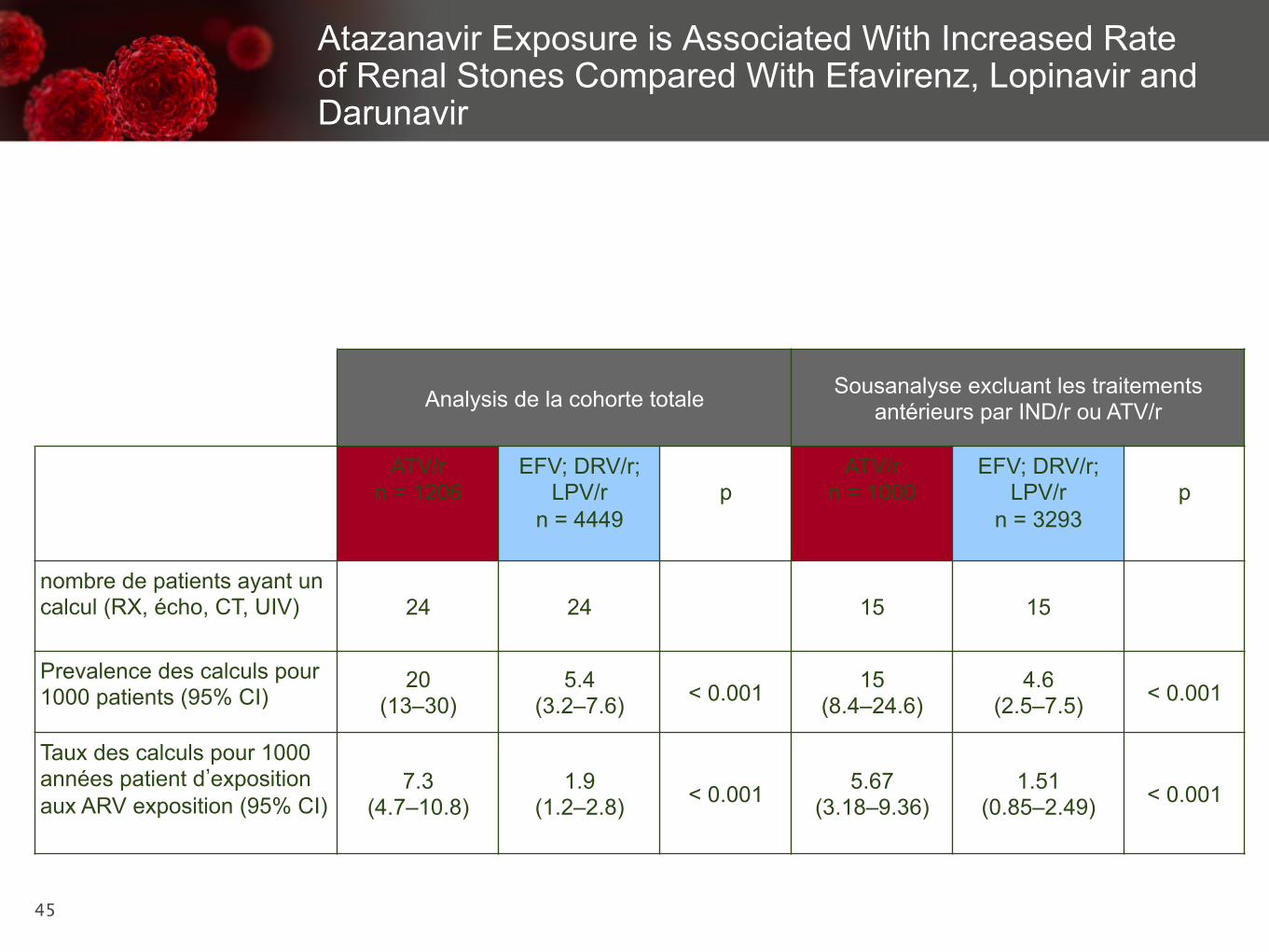
Atazanavir Exposure is Associated With Increased Rate of Renal Stones Compared With Efavirenz, Lopinavir and Darunavir
Analysis de la cohorte totale Sousanalyse excluant les traitements antérieurs par IND/r ou ATV/r
ATV/r n = 1206
EFV; DRV/r; LPV/r
n = 4449
p
ATV/r n = 1000
EFV; DRV/r; LPV/r
n = 3293
p
nombre de patients ayant un calcul (RX, écho, CT, UIV) 24 24 15 15
Prevalence des calculs pour 1000 patients (95% CI)
20 (13–30)
5.4 (3.2–7.6) < 0.001 15
(8.4–24.6) 4.6
(2.5–7.5) < 0.001
Taux des calculs pour 1000 années patient d’exposition aux ARV exposition (95% CI)
7.3 (4.7–10.8)
1.9 (1.2–2.8) < 0.001 5.67
(3.18–9.36) 1.51
(0.85–2.49) < 0.001
46
ATAZANAVIR
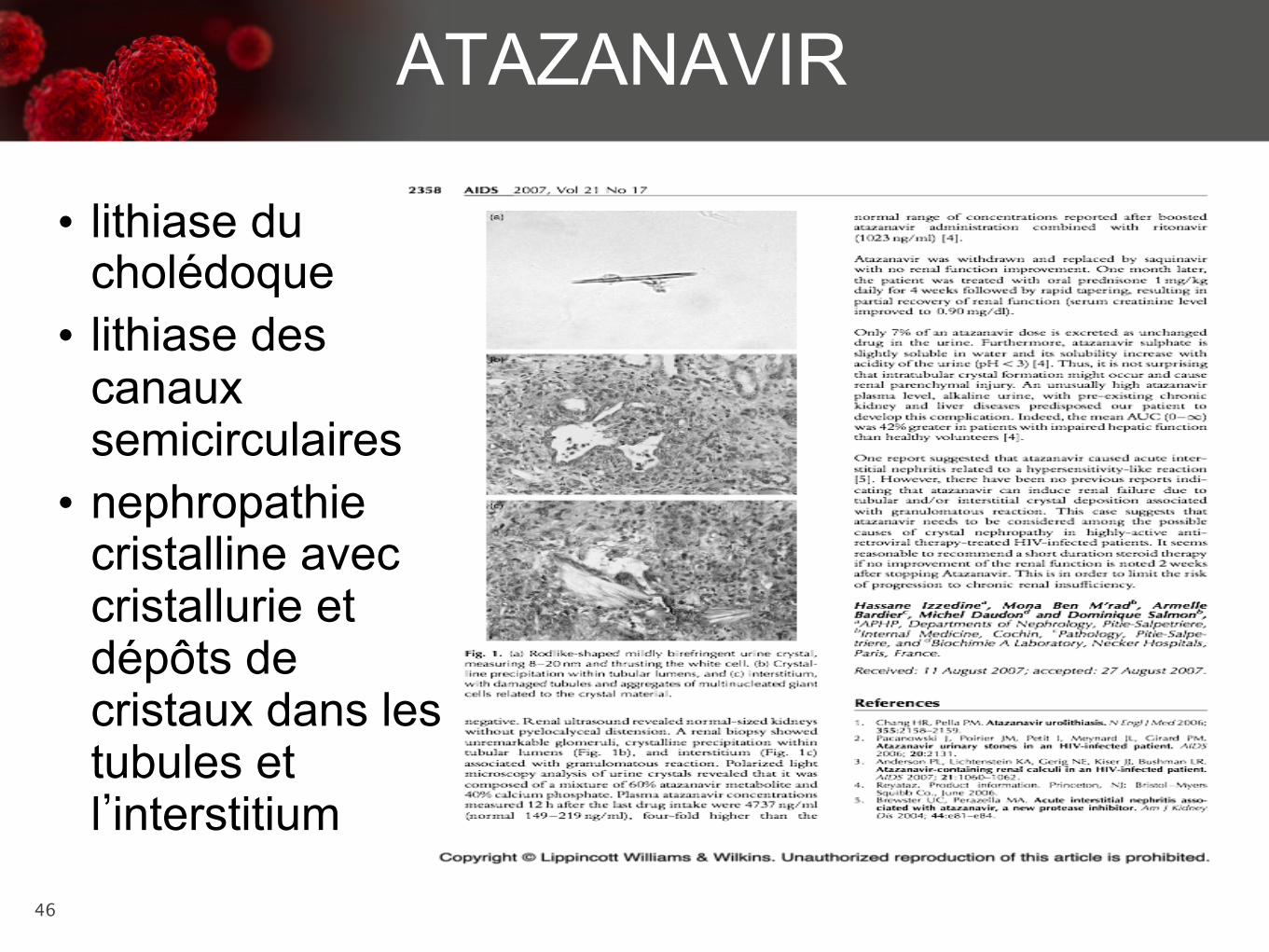
• lithiase du cholédoque • lithiase des
canaux semicirculaires • nephropathie
cristalline avec cristallurie et dépôts de cristaux dans les tubules et l’interstitium
Jacques et al, Annals Pharmacother, 2010. Pastori et al, AIDS 2009, Izzedine et al, AIDS 2007

Lien entre cristallurie et calculs
• L’analyse de la cristallurie est un examen non standardisé • Les résultats rendus par les laboratoires
habituels sont peu fiables • 3 cristalluries sur 6 mois (urines fraîches,
transport immédiat au labo, lecture par quelqu’un qui connait...)
Le patient infecté par le VIH est-il à haut risque de lithiase ?
• Etude rétrospective (Chicago, Illinois): tous les patients infectés par le VIH sous IP ayant une colique néphrétique entre juin 1996 et janvier 2001 • 24 patients 22 hommes/2 femmes
– Indinavir 14 âge moyen 29.2
– Ritonavir 3 durée exp IP 14 mois (2-40)
– Nelfinavir 2
– Indeterminée :5 (essai aveugle)
Nadler et al J of Urol 2003

49
• Présentation clinique habituelle • Hydratation, antalgique, arrêt transitoire de l’IP • 41.6% des patients ont eu besoin d’une urétéroscopie
+extraction du calcul (n=4), lithotripsie (n=4), nephrolithotomie percutanée (n=1), cystoscopie avec stent (n=1)
• Sur 14 patients sous Indinavir (11 calculs analysables): 36% seulement avaient un calcul contenant de l’indinavir
• Pour les autres (sous indinavir ou non) : – oxalate de calcium mono et dihydraté – Urate d’Ammonium (diarrhée chronique/dénutrition) – Acide urique
Le patient infecté par le VIH est-il à haut risque de lithiase ?
Nadler et al J of Urol 2003
50
• 10 patients ont eu une exploration métabolique • 80% avaient des anomalies
– Hypocitraturie 5 (3 sous indinavir) – Hyperoxalurie 4 ( 2 sous indinavir) – Hypomagnesurie 4 (2 sous indinavir) – Hypercalciurie 3 (1 sous indinavir) – Sursaturation en oxalate de Ca 3 (1 sous indinavir) – augmentation de la calciurie par Kg et par créatinine – Hyperuricosurie 2 – Anomalies de l’excrétion des phosphates et du sodium
4
Le patient infecté par le VIH est-il à haut risque de lithiase ?
Nadler et al J of Urol 2003

51
therapy were retrieved. Serum electrolytes, urinalysis withmicroscopy, urine culture, stone analysis, and 24-hour urinecollections were documented. The primary insurance carrierwas used for purposes of analysis, because the company(Dianon Systems, Shelton, CT) that processes our 24-hoururine collections only bills the primary insurance carrier.Descriptive statistics and analysis of variance were used withstatistical significance set at P < 0.05.
Results
A total of 436 HIV-positive patients were identified and 46(11%, 95% confidence interval 9–15%) of these demonstratedimage-proven kidney and/or ureteral urolithiasis. Mean agewas 54 years (range 34–78 y), and mean body mass index was27 (range 22–35). Patient demographics are shown in Table 2.None of the patients were instructed to stop HAART afterdiagnosis of nephrolithiasis. In the vast majority of cases, CTurography was the imaging modality (n = 39, 85%), whereasultrasonography alone (n = 5, 11%) and plain kidneys-ureters-bladder radiography alone (n = 2, 4%) were less commonlyused. Mean time of patients with a HIV diagnosis was 24months (range 12–36 mos), and mean time to nephrolithiasisdiagnosis while receiving HAART was 13.5 months (range 9–18 mos) (P < 0.05).
The characteristics of the stones, including their treatment,are listed in Table 3. Mean stone size was 8 mm (range 2–24 mm – 2.8 standard deviation). Seven subjects had multiplekidney calculi ( ‡ 2), and only one had bilateral kidney calculi.Ureteral obstruction secondary to obstructive ureteral calculideveloped in 30 patients. A total of 23 patients had kidneycalculi, 28 had ureteral calculi, and 42/46 were symptomatic—among these, 10 patients underwent shockwave lithotripsy(SWL), 13 underwent ureteroscopy/lithotripsy, and 23 weretreated with medical expulsive therapy with spontaneouspassage of stones. Two patients needed repeated surgery,including one SWL and one ureteroscopy/lithotripsy. Despitethe immunocompromised status of these HIV-positive pa-tients, there were limited complications as a result of treat-ment for nephrolithiasis. These complications includedurinary tract infection (3) and cystitis (2) that was treated withoutpatient oral antibiotics. The third patient had sepsis afterureteroscopy/lithotripsy despite a preoperative negative ur-ine culture. He recovered without sequelae.
Only eleven (24%) patients underwent 24-hour urine col-lections. Among these 11 patients, 10 had urinary abnormal-ities detected in their 24-hour urine collection includinghypocitraturia, hypercalciuria, hyperuricosuria, hyperpho-sphaturia, or hypernatriuria (Fig. 1). Hypercalciuria (35%)and hypocitraturia (29%) were the two most common urinaryabnormalities identified, followed by hypernatriuria (18%),hyperuricosuria (12%), and hyperphosphaturia (6%). Themean urinary pH among this group of patients was 6.2. Thesepatients had varied insurance coverage: five had Medicare,three had private, two had Medi-Cal, and one was uninsured.The insurance coverage among the 35 patients who did notundergo 24-hour urine collections also varied: 16 had Medi-care, 12 had Medi-Cal, 6 had private, and 2 had Ryan White.Twenty-four patients had a history of recurrent ne-phrolithiasis, but only four of these patients underwent acomprehensive metabolic evaluation.
Seven (14%) patients underwent chemical analysis of theurinary calculi: Four had calcium oxalate monohydrate, one
Table 2. Demographics of Patients
No. of patients 46Mean age, y (range) 54 (34–78)Sex
- Male 41Body mass index (range) 27 (22–35)Race
- Caucasian 36- Hispanic 9- African-American 1
Insurances*- Medicare 21- Medi-Cal 12- Private 10- Ryan White 3
*Only the primary insurance is listed and used for the purposes ofthis study.
Table 1. Frequency of Nephrolithiasis in OurHighly Active Antiretroviral Therapy Cohort
Antiretroviral Rx n
Efavirenz/emtricitabine/tenofovir 9Abacavir/emtricitabine/lopinavir/ritonavir/tenofovir 8Raltegravir/ritonavir/darunavir/tenofovir 6Abacavir/lamivudine/zidovudine 4Lopinavir/zidovudine/tenofovir 4Ritonavir/atazanavir/emtricitabine/tenofovir 4Darunavir/ritonavir/emtricitabine/tenofovir 3Combivir/lamivudine/zidovudine/efavirenz 2Nevirapine/tenofovir 2Ritonavir/emtricitabine/tenofovir 2Norvir/ritonavir/atazanavir/tenofovir 1Nelfinavir/emtrictabine/tenofovir 1
Table 3. Details of Stone Characteristics
No. of subjects 46Mean stone size, mm (range) 8 (2–24 – 2.8 SD)Stone location
- Kidney 23- Ureter 28
Imaging modality- CT 39- Ultrasonography 5- Plain radiography (KUB) 2
Nonsurgical management(medical expulsive therapy)
23
Surgical management 23- Shockwave lithotripsy 10- Ureteroscopy/lithotripsy 13
Repeated surgery- Shockwave lithotripsy 1- Ureteroscopy/lithotripsy 1
Family history of urolithiasis 6Recurrence of urolithiasis 24
SD = standard deviation; CT = computed tomography; KUB = kid-neys, ureters, and bladder.
2 RAHEEM ET AL.
Prevalence of Nephrolithisis in HIV patient with ART Rahem, Journal of Endo Urology 2012

52
therapy were retrieved. Serum electrolytes, urinalysis withmicroscopy, urine culture, stone analysis, and 24-hour urinecollections were documented. The primary insurance carrierwas used for purposes of analysis, because the company(Dianon Systems, Shelton, CT) that processes our 24-hoururine collections only bills the primary insurance carrier.Descriptive statistics and analysis of variance were used withstatistical significance set at P < 0.05.
Results
A total of 436 HIV-positive patients were identified and 46(11%, 95% confidence interval 9–15%) of these demonstratedimage-proven kidney and/or ureteral urolithiasis. Mean agewas 54 years (range 34–78 y), and mean body mass index was27 (range 22–35). Patient demographics are shown in Table 2.None of the patients were instructed to stop HAART afterdiagnosis of nephrolithiasis. In the vast majority of cases, CTurography was the imaging modality (n = 39, 85%), whereasultrasonography alone (n = 5, 11%) and plain kidneys-ureters-bladder radiography alone (n = 2, 4%) were less commonlyused. Mean time of patients with a HIV diagnosis was 24months (range 12–36 mos), and mean time to nephrolithiasisdiagnosis while receiving HAART was 13.5 months (range 9–18 mos) (P < 0.05).
The characteristics of the stones, including their treatment,are listed in Table 3. Mean stone size was 8 mm (range 2–24 mm – 2.8 standard deviation). Seven subjects had multiplekidney calculi ( ‡ 2), and only one had bilateral kidney calculi.Ureteral obstruction secondary to obstructive ureteral calculideveloped in 30 patients. A total of 23 patients had kidneycalculi, 28 had ureteral calculi, and 42/46 were symptomatic—among these, 10 patients underwent shockwave lithotripsy(SWL), 13 underwent ureteroscopy/lithotripsy, and 23 weretreated with medical expulsive therapy with spontaneouspassage of stones. Two patients needed repeated surgery,including one SWL and one ureteroscopy/lithotripsy. Despitethe immunocompromised status of these HIV-positive pa-tients, there were limited complications as a result of treat-ment for nephrolithiasis. These complications includedurinary tract infection (3) and cystitis (2) that was treated withoutpatient oral antibiotics. The third patient had sepsis afterureteroscopy/lithotripsy despite a preoperative negative ur-ine culture. He recovered without sequelae.
Only eleven (24%) patients underwent 24-hour urine col-lections. Among these 11 patients, 10 had urinary abnormal-ities detected in their 24-hour urine collection includinghypocitraturia, hypercalciuria, hyperuricosuria, hyperpho-sphaturia, or hypernatriuria (Fig. 1). Hypercalciuria (35%)and hypocitraturia (29%) were the two most common urinaryabnormalities identified, followed by hypernatriuria (18%),hyperuricosuria (12%), and hyperphosphaturia (6%). Themean urinary pH among this group of patients was 6.2. Thesepatients had varied insurance coverage: five had Medicare,three had private, two had Medi-Cal, and one was uninsured.The insurance coverage among the 35 patients who did notundergo 24-hour urine collections also varied: 16 had Medi-care, 12 had Medi-Cal, 6 had private, and 2 had Ryan White.Twenty-four patients had a history of recurrent ne-phrolithiasis, but only four of these patients underwent acomprehensive metabolic evaluation.
Seven (14%) patients underwent chemical analysis of theurinary calculi: Four had calcium oxalate monohydrate, one
Table 2. Demographics of Patients
No. of patients 46Mean age, y (range) 54 (34–78)Sex
- Male 41Body mass index (range) 27 (22–35)Race
- Caucasian 36- Hispanic 9- African-American 1
Insurances*- Medicare 21- Medi-Cal 12- Private 10- Ryan White 3
*Only the primary insurance is listed and used for the purposes ofthis study.
Table 1. Frequency of Nephrolithiasis in OurHighly Active Antiretroviral Therapy Cohort
Antiretroviral Rx n
Efavirenz/emtricitabine/tenofovir 9Abacavir/emtricitabine/lopinavir/ritonavir/tenofovir 8Raltegravir/ritonavir/darunavir/tenofovir 6Abacavir/lamivudine/zidovudine 4Lopinavir/zidovudine/tenofovir 4Ritonavir/atazanavir/emtricitabine/tenofovir 4Darunavir/ritonavir/emtricitabine/tenofovir 3Combivir/lamivudine/zidovudine/efavirenz 2Nevirapine/tenofovir 2Ritonavir/emtricitabine/tenofovir 2Norvir/ritonavir/atazanavir/tenofovir 1Nelfinavir/emtrictabine/tenofovir 1
Table 3. Details of Stone Characteristics
No. of subjects 46Mean stone size, mm (range) 8 (2–24 – 2.8 SD)Stone location
- Kidney 23- Ureter 28
Imaging modality- CT 39- Ultrasonography 5- Plain radiography (KUB) 2
Nonsurgical management(medical expulsive therapy)
23
Surgical management 23- Shockwave lithotripsy 10- Ureteroscopy/lithotripsy 13
Repeated surgery- Shockwave lithotripsy 1- Ureteroscopy/lithotripsy 1
Family history of urolithiasis 6Recurrence of urolithiasis 24
SD = standard deviation; CT = computed tomography; KUB = kid-neys, ureters, and bladder.
2 RAHEEM ET AL.
Prevalence of Nephrolithisis in HIV patient with ART Rahem, Journal of Endo Urology 2012

53
Prevalence of Nephrolithisis in HIV patient with ART Rahem, Journal of Endo Urology 2012
therapy were retrieved. Serum electrolytes, urinalysis withmicroscopy, urine culture, stone analysis, and 24-hour urinecollections were documented. The primary insurance carrierwas used for purposes of analysis, because the company(Dianon Systems, Shelton, CT) that processes our 24-hoururine collections only bills the primary insurance carrier.Descriptive statistics and analysis of variance were used withstatistical significance set at P < 0.05.
Results
A total of 436 HIV-positive patients were identified and 46(11%, 95% confidence interval 9–15%) of these demonstratedimage-proven kidney and/or ureteral urolithiasis. Mean agewas 54 years (range 34–78 y), and mean body mass index was27 (range 22–35). Patient demographics are shown in Table 2.None of the patients were instructed to stop HAART afterdiagnosis of nephrolithiasis. In the vast majority of cases, CTurography was the imaging modality (n = 39, 85%), whereasultrasonography alone (n = 5, 11%) and plain kidneys-ureters-bladder radiography alone (n = 2, 4%) were less commonlyused. Mean time of patients with a HIV diagnosis was 24months (range 12–36 mos), and mean time to nephrolithiasisdiagnosis while receiving HAART was 13.5 months (range 9–18 mos) (P < 0.05).
The characteristics of the stones, including their treatment,are listed in Table 3. Mean stone size was 8 mm (range 2–24 mm – 2.8 standard deviation). Seven subjects had multiplekidney calculi ( ‡ 2), and only one had bilateral kidney calculi.Ureteral obstruction secondary to obstructive ureteral calculideveloped in 30 patients. A total of 23 patients had kidneycalculi, 28 had ureteral calculi, and 42/46 were symptomatic—among these, 10 patients underwent shockwave lithotripsy(SWL), 13 underwent ureteroscopy/lithotripsy, and 23 weretreated with medical expulsive therapy with spontaneouspassage of stones. Two patients needed repeated surgery,including one SWL and one ureteroscopy/lithotripsy. Despitethe immunocompromised status of these HIV-positive pa-tients, there were limited complications as a result of treat-ment for nephrolithiasis. These complications includedurinary tract infection (3) and cystitis (2) that was treated withoutpatient oral antibiotics. The third patient had sepsis afterureteroscopy/lithotripsy despite a preoperative negative ur-ine culture. He recovered without sequelae.
Only eleven (24%) patients underwent 24-hour urine col-lections. Among these 11 patients, 10 had urinary abnormal-ities detected in their 24-hour urine collection includinghypocitraturia, hypercalciuria, hyperuricosuria, hyperpho-sphaturia, or hypernatriuria (Fig. 1). Hypercalciuria (35%)and hypocitraturia (29%) were the two most common urinaryabnormalities identified, followed by hypernatriuria (18%),hyperuricosuria (12%), and hyperphosphaturia (6%). Themean urinary pH among this group of patients was 6.2. Thesepatients had varied insurance coverage: five had Medicare,three had private, two had Medi-Cal, and one was uninsured.The insurance coverage among the 35 patients who did notundergo 24-hour urine collections also varied: 16 had Medi-care, 12 had Medi-Cal, 6 had private, and 2 had Ryan White.Twenty-four patients had a history of recurrent ne-phrolithiasis, but only four of these patients underwent acomprehensive metabolic evaluation.
Seven (14%) patients underwent chemical analysis of theurinary calculi: Four had calcium oxalate monohydrate, one
Table 2. Demographics of Patients
No. of patients 46Mean age, y (range) 54 (34–78)Sex
- Male 41Body mass index (range) 27 (22–35)Race
- Caucasian 36- Hispanic 9- African-American 1
Insurances*- Medicare 21- Medi-Cal 12- Private 10- Ryan White 3
*Only the primary insurance is listed and used for the purposes ofthis study.
Table 1. Frequency of Nephrolithiasis in OurHighly Active Antiretroviral Therapy Cohort
Antiretroviral Rx n
Efavirenz/emtricitabine/tenofovir 9Abacavir/emtricitabine/lopinavir/ritonavir/tenofovir 8Raltegravir/ritonavir/darunavir/tenofovir 6Abacavir/lamivudine/zidovudine 4Lopinavir/zidovudine/tenofovir 4Ritonavir/atazanavir/emtricitabine/tenofovir 4Darunavir/ritonavir/emtricitabine/tenofovir 3Combivir/lamivudine/zidovudine/efavirenz 2Nevirapine/tenofovir 2Ritonavir/emtricitabine/tenofovir 2Norvir/ritonavir/atazanavir/tenofovir 1Nelfinavir/emtrictabine/tenofovir 1
Table 3. Details of Stone Characteristics
No. of subjects 46Mean stone size, mm (range) 8 (2–24 – 2.8 SD)Stone location
- Kidney 23- Ureter 28
Imaging modality- CT 39- Ultrasonography 5- Plain radiography (KUB) 2
Nonsurgical management(medical expulsive therapy)
23
Surgical management 23- Shockwave lithotripsy 10- Ureteroscopy/lithotripsy 13
Repeated surgery- Shockwave lithotripsy 1- Ureteroscopy/lithotripsy 1
Family history of urolithiasis 6Recurrence of urolithiasis 24
SD = standard deviation; CT = computed tomography; KUB = kid-neys, ureters, and bladder.
2 RAHEEM ET AL.

54
had cystine, one had uric acid, and one had an atazanavirmetabolite stone. In addition, six patients had a family historyof urolithiasis.
Discussion
We believe this is the first article to report both the preva-lence and etiology of nephrolithiasis in an HIV-positive cohortof patients taking no indinavir in the HAART era. Despite therecent shift toward less lithogenic HIV therapy, the 11%prevalence of nephrolithiasis in our cohort still exceeded thatof the non-HIV population (5.2%).2,3 Similar to previous re-ports, our study confirms that HIV patients share an equalrisk of nephrolithiasis that is not necessarily related toindinavir-based therapy.4 The medications in this study in-cluded PIs, but only one stone analysis demonstrated evi-dence of a PI-contained calculi. These findings are of criticalimportance, because it demonstrates that HIV-infected pa-tients are at an equal risk for nephrolithiasis, which ultimatelysignificantly contributes to the annual United States health-care expenditures.5
Medical management is the foundation of kidney and/orureteral calculi prevention, with algorithms dependent onboth serum studies and 24-hour urine studies as the corner-stone of a comprehensive metabolic evaluation. Un-fortunately, both previous reports and our current studydocument low utilization of the 24-hour urine study in theevaluation of nephrolithiasis. Recurrence rates in non-HIVpatients are 50% over 5 to 10 years, while medical manage-ment can identify specific urinary abnormalities in approxi-mately 97% of analyses, potentially reducing recurrencerates.6
More than half of our patients had recurrent nephrolithiasisand may well have benefited from medical intervention as apreventative measure. Furthermore, more than half of ourcohort needed surgical intervention with its attendant risksand financial burden to an already diseased population. Thesefindings add credence to performance of a comprehensivemetabolic evaluation as a means of reducing risk of recurrentnephrolithiasis. Generally, the evaluation for nephrolithiasisin the HIV patient should be no different from that of the non-HIV patient. Stone analysis, however, is particularly useful,because it discriminates metabolic stone from drug-inducedstone and subsequently reinforces the utility of a metabolicevaluation when a metabolic component exists in the stoneanalysis. A metabolic evaluation should also be considered,especially if a stone analysis is not available or if there is ahistory of recurrent metabolic stone disease.
We suspect that poor utilization of 24-hour urine studies ismost likely because of one of four possibilities: (1) provider
decision to recommend nonoperative therapy (increase fluidintake, decrease salt and protein) in low-risk nephrolithiasisformers or first-time nephrolithiasis formers; (2) providerdisbelief in the utility of the comprehensive metabolic testingand evaluation; (3) poor patient compliance in undergoingthis testing; or (4) insurance obstacles. Regarding the latter,we discovered a proportion (6%) of HIV patients were noteligible for 24-hour urine studies because of their specificfederal insurance, the Ryan White program, which only re-imburses this specific test on a case by case basis. Our data,however, do not support the supposition that insurance is anobstacle to metabolic evaluation.
The prevalence of nephrolithiasis is estimated to be 3% to22% for HIV-positive patients receiving indinavir.2,4,7–10 In-dinavir is a PI of which approximately 20% is not metabolizedand is excreted by the kidneys. Indinavir is most soluble atpH < 5, and therefore it tends to precipitate in alkaline urine.Hence, indinavir calculi typically tend to be radiolucent butmay act as a nidus for the formation of kidney and/or ureteralcalculi containing calcium oxalate and phosphate, which areradiopaque.2,11–13
The newer antiretroviral therapies in the form of HAARThave made a significant impact on the morbidity and mor-tality of patients with HIV infection. Antiretroviral drug re-sistance can develop rapidly through mutations; therefore, acombination of at least three drugs from at least two differentclasses is now used, coined HAART. Two NRTIs are usuallycombined with either NNRTIs or a PI. The primary aim ofHAART is to suppress a viral load below detectable levels,and thereby increase the CD4 cell count and decrease mor-bidity and mortality.9,10 Reports of kidney calculi made of adegraded PI other than indinavir exist with atazanavir,however.14–18 In addition, nephrolithiasis case reports asso-ciated with nonindinavir-based HAART exist (Table 4).
Notwithstanding the risk of PI composed stones, we reporta risk of nephrolithiasis in HIV patients that mimics the non-HIV population. We acknowledge the limitations/bias of thisretrospective study, which limits data collection, such asmissing data. In addition, we acknowledge that certainmedications such as thiazide diuretics may affect kidneystone formation, and therefore our analysis may
FIG. 1. Details of the etiology of nephrolithiasis amongpatients who underwent 24-hour urine collection.
Table 4. Current Literature Reports of HighlyActive Antiretroviral Therapy Associated
With Nephrolithiasis14–30
Stoneformation
Stonecharacteristics
Drug (Yes/No) (radiopaque)
NRTIsZidovudine No NoLamivudine Emtricitabine No NoStavudine No NoTenofovir Yes Yes
PisNelfinavir Yes YesAmprenavir Yes YesSaquinavir Yes YesLopinavir/ritonavir Yes YesAtazanavir Yes No
NRTIs = nucleoside reverse transcriptase inhibitors; PIs = proteaseinhibitors.
NEPHROLITHIASIS AMONG HIV-INFECTED PATIENTS 3
Prevalence of Nephrolithisis in HIV patient with ART Rahem, Journal of Endo Urology 2012

55
Prevalence of Nephrolithisis in HIV patient with ART Rahem, Journal of Endo Urology 2012
had cystine, one had uric acid, and one had an atazanavirmetabolite stone. In addition, six patients had a family historyof urolithiasis.
Discussion
We believe this is the first article to report both the preva-lence and etiology of nephrolithiasis in an HIV-positive cohortof patients taking no indinavir in the HAART era. Despite therecent shift toward less lithogenic HIV therapy, the 11%prevalence of nephrolithiasis in our cohort still exceeded thatof the non-HIV population (5.2%).2,3 Similar to previous re-ports, our study confirms that HIV patients share an equalrisk of nephrolithiasis that is not necessarily related toindinavir-based therapy.4 The medications in this study in-cluded PIs, but only one stone analysis demonstrated evi-dence of a PI-contained calculi. These findings are of criticalimportance, because it demonstrates that HIV-infected pa-tients are at an equal risk for nephrolithiasis, which ultimatelysignificantly contributes to the annual United States health-care expenditures.5
Medical management is the foundation of kidney and/orureteral calculi prevention, with algorithms dependent onboth serum studies and 24-hour urine studies as the corner-stone of a comprehensive metabolic evaluation. Un-fortunately, both previous reports and our current studydocument low utilization of the 24-hour urine study in theevaluation of nephrolithiasis. Recurrence rates in non-HIVpatients are 50% over 5 to 10 years, while medical manage-ment can identify specific urinary abnormalities in approxi-mately 97% of analyses, potentially reducing recurrencerates.6
More than half of our patients had recurrent nephrolithiasisand may well have benefited from medical intervention as apreventative measure. Furthermore, more than half of ourcohort needed surgical intervention with its attendant risksand financial burden to an already diseased population. Thesefindings add credence to performance of a comprehensivemetabolic evaluation as a means of reducing risk of recurrentnephrolithiasis. Generally, the evaluation for nephrolithiasisin the HIV patient should be no different from that of the non-HIV patient. Stone analysis, however, is particularly useful,because it discriminates metabolic stone from drug-inducedstone and subsequently reinforces the utility of a metabolicevaluation when a metabolic component exists in the stoneanalysis. A metabolic evaluation should also be considered,especially if a stone analysis is not available or if there is ahistory of recurrent metabolic stone disease.
We suspect that poor utilization of 24-hour urine studies ismost likely because of one of four possibilities: (1) provider
decision to recommend nonoperative therapy (increase fluidintake, decrease salt and protein) in low-risk nephrolithiasisformers or first-time nephrolithiasis formers; (2) providerdisbelief in the utility of the comprehensive metabolic testingand evaluation; (3) poor patient compliance in undergoingthis testing; or (4) insurance obstacles. Regarding the latter,we discovered a proportion (6%) of HIV patients were noteligible for 24-hour urine studies because of their specificfederal insurance, the Ryan White program, which only re-imburses this specific test on a case by case basis. Our data,however, do not support the supposition that insurance is anobstacle to metabolic evaluation.
The prevalence of nephrolithiasis is estimated to be 3% to22% for HIV-positive patients receiving indinavir.2,4,7–10 In-dinavir is a PI of which approximately 20% is not metabolizedand is excreted by the kidneys. Indinavir is most soluble atpH < 5, and therefore it tends to precipitate in alkaline urine.Hence, indinavir calculi typically tend to be radiolucent butmay act as a nidus for the formation of kidney and/or ureteralcalculi containing calcium oxalate and phosphate, which areradiopaque.2,11–13
The newer antiretroviral therapies in the form of HAARThave made a significant impact on the morbidity and mor-tality of patients with HIV infection. Antiretroviral drug re-sistance can develop rapidly through mutations; therefore, acombination of at least three drugs from at least two differentclasses is now used, coined HAART. Two NRTIs are usuallycombined with either NNRTIs or a PI. The primary aim ofHAART is to suppress a viral load below detectable levels,and thereby increase the CD4 cell count and decrease mor-bidity and mortality.9,10 Reports of kidney calculi made of adegraded PI other than indinavir exist with atazanavir,however.14–18 In addition, nephrolithiasis case reports asso-ciated with nonindinavir-based HAART exist (Table 4).
Notwithstanding the risk of PI composed stones, we reporta risk of nephrolithiasis in HIV patients that mimics the non-HIV population. We acknowledge the limitations/bias of thisretrospective study, which limits data collection, such asmissing data. In addition, we acknowledge that certainmedications such as thiazide diuretics may affect kidneystone formation, and therefore our analysis may
FIG. 1. Details of the etiology of nephrolithiasis amongpatients who underwent 24-hour urine collection.
Table 4. Current Literature Reports of HighlyActive Antiretroviral Therapy Associated
With Nephrolithiasis14–30
Stoneformation
Stonecharacteristics
Drug (Yes/No) (radiopaque)
NRTIsZidovudine No NoLamivudine Emtricitabine No NoStavudine No NoTenofovir Yes Yes
PisNelfinavir Yes YesAmprenavir Yes YesSaquinavir Yes YesLopinavir/ritonavir Yes YesAtazanavir Yes No
NRTIs = nucleoside reverse transcriptase inhibitors; PIs = proteaseinhibitors.
NEPHROLITHIASIS AMONG HIV-INFECTED PATIENTS 3
Prévention des récidives : moyens spécifiques aux lithiases médicamenteuses
• Adaptation de la dose du médicament • ????? • adaptation de la dose si atteinte et hépatique
et modification du métabolisme rénal?

Adaptation du pH urinaire en fonction du médicament
Médicaments cristallisant préférentiellement à pH
alcalin acide
Antiprotéases Ciprofloxacine Ceftriaxone Silice opaline
Aminopenicillines (amoxicilline) Sulfamides+++ Triamtérène

58
Conclusions
• Lithiase fréquent – mal pris en charge – diagnostics non faits • Chez le patient infecté par le VIH, augmentation
du risque métabolique de lithiase • Augmentation du risque avec les IP ?
Atazanavir ? • Importance de bien documenter les épisodes de
lithiase/prévenir la récidive

Etude CALVI : facteur de risque de CAlcul chez le patient infecté par le VIh
• Exploration prospective clinique, radiologique, métabolique des patients ayant fait un épisode de lithiase • Comparaison des données entre patients traités
par ATZ et sans ATZ
60
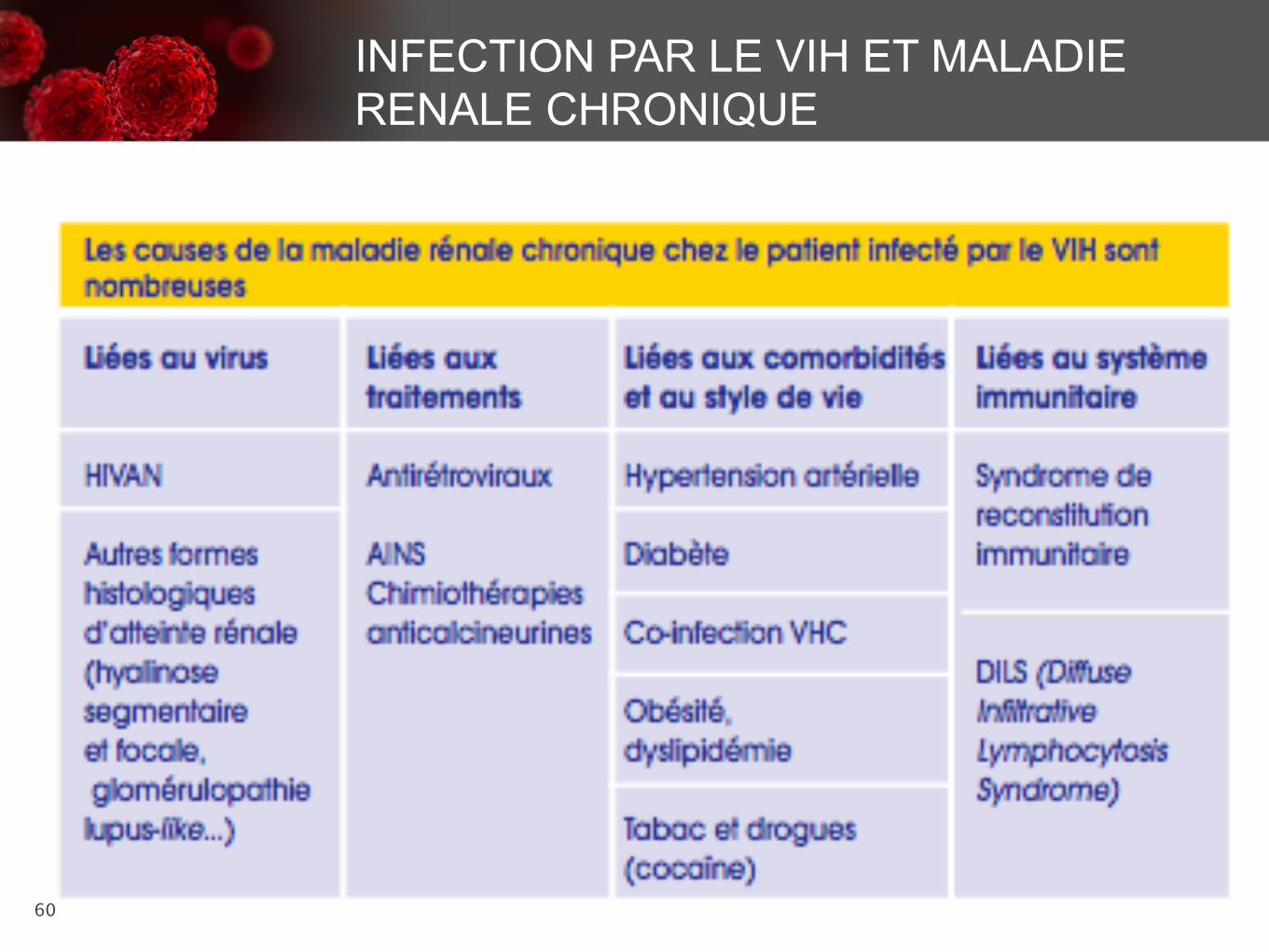
INFECTION PAR LE VIH ET MALADIE RENALE CHRONIQUE

61
Texte
MALADIE RENALE CHRONIQUE ET VIH
22
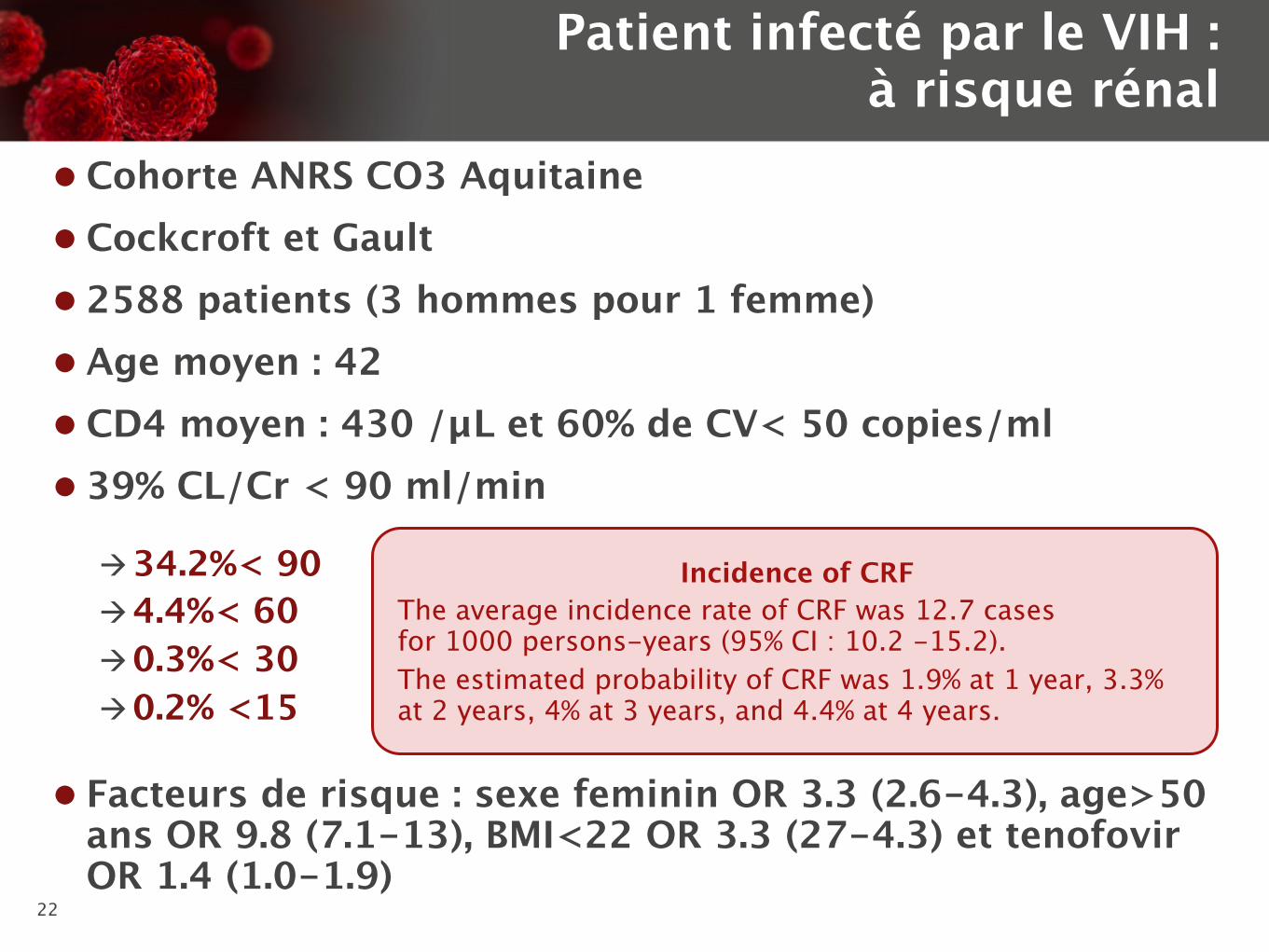
l Cohorte ANRS CO3 Aquitaine l Cockcroft et Gault l 2588 patients (3 hommes pour 1 femme) l Age moyen : 42 l CD4 moyen : 430 /µL et 60% de CV< 50 copies/ml l 39% CL/Cr < 90 ml/min
Patient infecté par le VIH : à risque rénal
à 34.2%< 90 à 4.4%< 60 à 0.3%< 30 à 0.2% <15
l Facteurs de risque : sexe feminin OR 3.3 (2.6-4.3), age>50 ans OR 9.8 (7.1-13), BMI<22 OR 3.3 (27-4.3) et tenofovir OR 1.4 (1.0-1.9)
Incidence of CRF The average incidence rate of CRF was 12.7 casesfor 1000 persons-years (95% CI : 10.2 -15.2). The estimated probability of CRF was 1.9% at 1 year, 3.3% at 2 years, 4% at 3 years, and 4.4% at 4 years.

63

64 64

• Cohorte Eurosida: Follow-up: 21,482 person-years; median 3.7 (IQR 2.8–5.7) years 225 (3.3%) progressed to CKD; overall incidence: 1.05 × 100 PYFU (0.91–1.18) ARV associated with risk of CKD: TDF, LPV/r, ATV/r • Cohorte Aquitaine: 2693 pts > 60 ml/mn; Mean follow-up (2004–2008): 3.4 years
86 pts progressed to CKD (defined as 2 consecutive CC < 60 mL/min/1.73 m2 ≥ 3 months apart) during 8477 PYFU
Average incidence rate of CKD: 1.01% PYFU
ARV associated with risk of CKD: TDF
• Cohorte Nadis: 7378 pts
N= 349 CKD; 4,7%
ARV associated with risk of CKD: TDF, ABC, IDV
1. Mocroft A, et al., for the EuroSIDA Study Group. AIDS. 2010 Jul 17;24(11);1667-1678. 2. Flandre P, et al. The New AIDS Data Group. Clin J AM SOC Nephrol. 2011 Jul;6(7):1700-1707.
3. Morlat P, et al IAS 2011; Poster WEPDB0104
CKD and HIV

66
Infection par le VIH et atteinte rénale : LE VIRUS

67
Texte
Bigé et al, 2011

68
69
Infection par le VIH et atteinte rénale : LE VIRUS

70

71

25
La seule meta analyse
Cooper et al, CID, 2010
- 20 - 10 0 10 20 Nephrotoxicity more likely Nephrotoxicity less likely
MD [95% CI], mL/ min Study or subcategory RCT
Total MD [95% CI], mL/ min
ART naive BICOMBO 2009 De Jesus 2009
333 300
- 0.70 [-2.73, 1.33] - 0.60 [-1.71, 0.51]
ART experienced HEAT 2009 Arribas 2008 Gallant 2004
672 458 600
- 3.00 [-9.06, 3.06] -3.00 [-6.77, 0.77]
-5.00 [-8.80, -1.20] Subtotal -1.50 [2.96, -0.005]
Cohort ART naive
Kinai 2009 Goicoechea 2008 NNRTI Goicoechea 2008 RPI HOPS 2007 Winston 2006
63 62 84 736 948
- 17.00 [-31.35, -2.65] -0.22 [-11.18, 10.74]
-7.88 [-18.66, 2.90] -4.40 [-6.97, -1.83] -6.33 [-14.85, 2.19]
ART experienced Fux 2007 Fux 2007 N Gallant 2005
284 569 658
-4.90 [-8.58, -1.22] -8.20 [-13.13, -3.27]
-5.80 [-8.70, -2.90] Subtotal -5.45 [-7.02, -3.89] Total -3.90 [-5.66, -2.14]

73
74
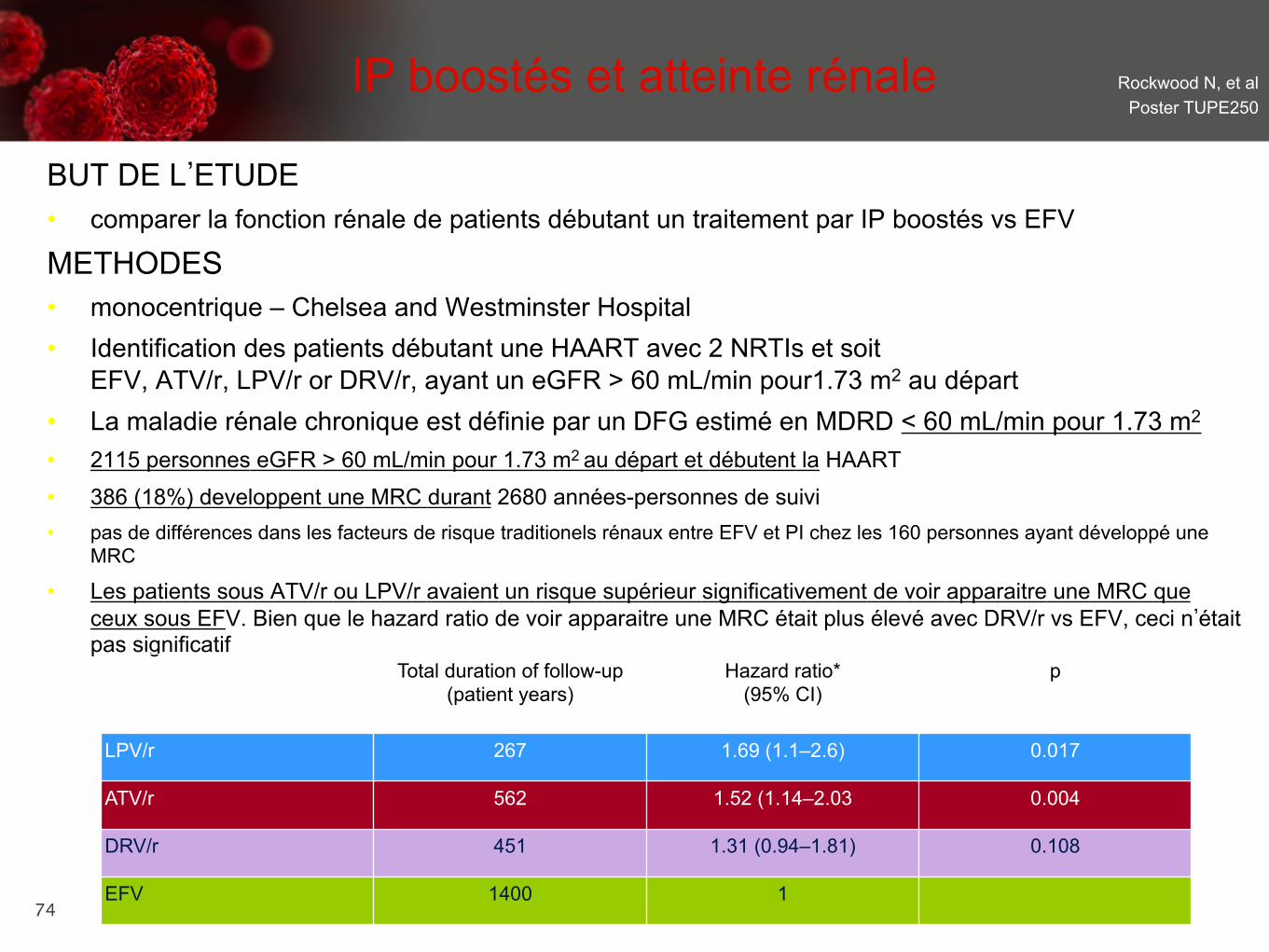
IP boostés et atteinte rénale Rockwood N, et al Poster TUPE250
BUT DE L’ETUDE • comparer la fonction rénale de patients débutant un traitement par IP boostés vs EFV
METHODES • monocentrique – Chelsea and Westminster Hospital • Identification des patients débutant une HAART avec 2 NRTIs et soit
EFV, ATV/r, LPV/r or DRV/r, ayant un eGFR > 60 mL/min pour1.73 m2 au départ • La maladie rénale chronique est définie par un DFG estimé en MDRD < 60 mL/min pour 1.73 m2 • 2115 personnes eGFR > 60 mL/min pour 1.73 m2 au départ et débutent la HAART • 386 (18%) developpent une MRC durant 2680 années-personnes de suivi • pas de différences dans les facteurs de risque traditionels rénaux entre EFV et PI chez les 160 personnes ayant développé une
MRC • Les patients sous ATV/r ou LPV/r avaient un risque supérieur significativement de voir apparaitre une MRC que
ceux sous EFV. Bien que le hazard ratio de voir apparaitre une MRC était plus élevé avec DRV/r vs EFV, ceci n’était pas significatif
Total duration of follow-up (patient years)
Hazard ratio* (95% CI)
p
LPV/r 267 1.69 (1.1–2.6) 0.017
ATV/r 562 1.52 (1.14–2.03 0.004
DRV/r 451 1.31 (0.94–1.81) 0.108
EFV 1400 1

75
• une proportion non négligeable de patients débutant la HAART voient leur fonction rénale diminuer.
• LPV/r et ATV/r, sont associés à un risque augmenté quelquesoit la fonction rénale de base, l’âge, l’exposition préalable au TDF ou la durée totale d’exposition au TDF
• le DRV/r n’est pas significativement associé à une atteinte rénale • La fonction rénale des patients sous HAART peut
rester stable, s’aggraver ou s’améliorer • 49% de ceux qui s’aggravent, améliorent leur fonction rénale en 12
mois.
IP boostés et atteinte rénale Rockwood N, et al Poster TUPE250

76

77

78

79
80

81
0.5 1 2
0.5 1 2
Background and Objective
• Background – Tenofovir (TDF), atazanavir (ATV), and other ARVs have been associated with
renal impairment,1-5 but the extent of such adverse drug reactions in HIV+ persons with normal baseline renal function is unknown
• Objective – Evaluate and compare the exposure to antiretrovirals and the risk of renal
impairment among HIV+ persons with normal baseline renal function
Ryom L, et al. Poster 865
1. Mocroft A, et al., for the EuroSIDA Study Group. AIDS. 2010 Jul 17;24(11);1667-1678. 2. Flandre P, et al. The New AIDS Data Group. Clin J AM SOC Nephrol. 2011 Jul;6(7):1700-1707. 3. Campo R, et al. The SWIFT Study, Abstract H2-786. 51st ICAAC, 2011. 4. Scherzer R, et al. AIDS. 2012 Feb 4. [Epub ahead of print] 5. Rockwood N, et al. AIDS. 2011;25:1671-1673.

Baseline Characteristics N, All Included (%) [IQR] N, ceGFR ≤70 (%) [IQR] N, CKD (%) [IQR]
All 22,603 (100) 468 (2) 131 (0.6)
Gender Male 16,438 (73) 340 (73) 89 (68)
Race White Unknown
10,573 (47) 9714 (43)
309 (66) 129 (28)
88 (67) 37 (28)
Median age (years) 39 [33-44] 46 [41-52] 46 [40-51]
HIV risk homosex. 10,006 (44) 176 (38) 39 (30)
Prior AIDS 4553 (20) 154 (33) 48 (37)
cART exposed 14,263 (63) 346 (74) 94 (72)
CD4 (count/mm3) 440 [290-624] 380 [217-568] 380 [221-585]
HIV-RNA (log10 copies/mL) 2.1 [1.7-4.2] 1.8 [1.7-4.0] 2.3 [1.7-4.0]
Years HIV+ 5.2 [1.2-11.1] 10.0 [5.3-14.9] 10.8 [4.5-15.5]
HBV (HBsAg or HBeAg or DNA pos./anti-HBe pos.) 2773 (12) 64 (14) 17 (13)
HCV (seropos. & RNA pos./unknown) 2765 (12) 93 (20) 37 (28)
Hypertension 1761 (8) 53 (11) 20 (15)
Diabetes 664 (3) 43 (9) 14 (11)
Prior CV event 336 (2) 17 (4) 6 (5)
Ryom L, et al. Poster 865
Results
Of 22,603 persons included with a normal baseline renal function:
• 468 (2.1%) progressed to ceGFR ≤70 (incidence rate [IR] 4.78/1000 PY [95% CI 4.35-5.22])
• 131 (0.6%) to CKD (1.33/1000 PY [1.10-1.56]) during a median follow-up (FU) of 4.5 years (IQR 2.7-6.1).
• eGFR decline of at least 20 mL/min (from eGFR >90 to ≤70) during 4.5 years equals an annual decline of at least 4-5 mL/min
Ryom L, et al. Poster 865

ARV Discontinuation Rates and eGFR Levels
Ryom L, et al. Poster 865
Adjusted for baseline eGFR, age, gender, race, HIV risk group, CD4 nadir, enrollment cohort and baseline date. AIDS, HBV/HCV status, smoking status, hypertension, diabetes, CV event, CD4, VL and cumulative exposure (per year) to indinavir, unboosted atazanavir and other boosted PIs (darunavir, tipranavir, [fos]amprenavir) (included as time-updated variables)
Persons with eGFR levels between 60 and 70 had significantly higher rates of discontinuing TDF (adjusted IR ratio [aIRR] 1.72 [1.38-2.14]), but not of other ARVs tested, compared to persons with eGFR >90
Dis
cont
inua
tion
IRR
(9
5% C
l)
>90
80.1
-90
70.1
-80
60.1
-70
<60 0.5
1
2
4
Tenofovir
Dis
cont
inua
tion
IRR
(9
5% C
l)
>90
80.1
-90
70.1
-80
60.1
-70
<60 0.5
1
2
4
Atazanavir/r
Dis
cont
inua
tion
IRR
(9
5% C
l)
>90
80.1
-90
70.1
-80
60.1
-70
<60 0.5
1
2
4
Lopinavir/r
Dis
cont
inua
tion
IRR
(9
5% C
l)
>90
80.1
-90
70.1
-80
60.1
-70
<60 0.5
1
2
4
Abacavir
eGFR
eGFR
eGFR
eGFR
Univariate Multivariate

ARV Exposure (Per Year) and Incidence Rate Ratios of ceGFR ≤70 and CKD From eGFR >90 Ryom L, et al.
Poster 865
Adjusted for baseline eGFR, age, gender, race, HIV risk group, CD4 nadir, enrollment cohort, and baseline date. AIDS, HBV/HCV status, smoking status, hypertension, diabetes, CV event, CD4, VL and cumulative exposure (per year) to indinavir included as time-updated variables. Other PI/r include darunavir, tipranavir, and (fos)amprenavir.
• Cumulative TDF (aIRR 1.18 [1.12-1.25] per year) and ATV/r (1.19 [1.09-1.32]) use were independently associated with increased rates of ceGFR ≤70 from eGFR >90, but not with CKD, whereas lopinavir/r (LPV/r) use was associated with both endpoints (1.11 [1.05-1.17]) and 1.22 [1.16-1.28] respectively. Inconsistent trends were seen with abacavir use
ceGFR ≤70 IRR (95% Cl) 0.5 1 2
Tenofovir
Lopinavir/r
Atazanavir/r
Atazanavir
Other Pl/r
Abacavir
Multivariate Univariate
CKD IRR (95% Cl) 0.5 1 2
1.18
1.11
1.19
1.22

Investigators’ Conclusions • In HIV+ persons with normal baseline renal function, cumulative use of TDF, ATV/r, and
LPV/r were each associated with a fast eGFR decline, as more traditional renal risk factors and HIV-related factors in adjusted models
• Rates of ARV-associated deteriorations in renal function from normal function were low over the 4.5 years of FU available, but may represent significant issues for lifelong use should the rates remain constant or even increase with age. For instance, after 5 years of TDF use, the incidence rate of progression to ceGFR ≤70 from levels >90 will be twice as high in TDF-exposed compared to unexposed persons
• Increased discontinuation rates of TDF, but not of other ARVs in persons with decreasing eGFR, suggest that drug switches are occurring more commonly for certain ARVs in relation to declining eGFR, and the switches may have prevented further deterioration to CKD. Closer monitoring of renal function may be appropriate for persons also on ATV/r and LPV/r
Ryom L, et al. Poster 865
88

89
Recommandations 2011 EACS http://www.europeanaidsclinicalsociety.org/guidelines.asp
EACS Guidelines / 37
.LGQH\�GLVHDVH��GLDJQRVLV
eGFR (i)
�����P/�PLQ 30-59 mL/min < 30 mL/min
Prot
einu
ria (ii
)
83�&�(iii)������ 5HJXODU�)ROORZ�XS���&KHFN�ULVN�IDFWRUV�IRU�
CKD and nephrotoxic medication including ART (iv)
��'LVFRQWLQXH�RU�DGMXVW�drug dosages where appropriate (v)
��3HUIRUP�UHQDO�XOWUDVRXQG���8UJHQW�UHIHUUDO�WR�
nephrologist
83�&�(iii) 50-100
��&KHFN�ULVN�IDFWRUV�IRU�&.'�DQG�QHSKURWR[LF�PHGLFDWLRQ�including ART (iv)
��'LVFRQWLQXH�RU�DGMXVW�GUXJ�GRVDJHV�ZKHUH�DSSURSULDWH�(v) ��3HUIRUP�UHQDO�XOWUDVRXQG���,I�KDHPDWXULD�SUHVHQW�ZLWK�DQ\�OHYHO�RI�SURWHLQXULD�UHIHU�WR�QHSKURORJLVW�
��5HIHU�WR�QHSKURORJLVW�LI�QHZ�&.'�RU�SURJUHVVLYH�GHFOLQH�LQ�eGFR
83�&�(iii) > 100
Management of HIV-associated renal disease (vi)
Prevention of progressive renal disease Comment1� Antiretroviral therapy 6WDUW�$57�LPPHGLDWHO\�ZKHUH�+,9�DVVRFLDWHG�QHSKURSDWK\�
�+,9$1��(vii)�RU�+,9�LPPXQH�FRPSOH[�GLVHDVH�VWURQJO\�VXVSHFWHG��5HQDO�ELRSV\�WR�FRQ¿UP�KLVWRORJLFDO�GLDJQRVLV�UHFRPPHQGHG�
2� Start ACE inhibitors or angiotensin-II receptor antagonists if: D��+\SHUWHQVLRQ��DQG�RU�E��3URWHLQXULD�
Monitor eGFR and K+ level closely on starting treatment or increasing dose D��%ORRG�SUHVVXUH�WDUJHW������������PP+J
3� General measures: D��$YRLG�QHSKURWR[LF�GUXJV�E��/LIHVW\OH�PHDVXUHV��VPRNLQJ��ZHLJKW��GLHW��F��7UHDW�G\VOLSLGDHPLD�(viii)�DQG�GLDEHWHV�(ix)
G��$GMXVW�GUXJ�GRVDJHV�ZKHUH�QHFHVVDU\�
&.'�DQG�SURWHLQXULD�DUH�LQGHSHQGHQW�ULVN�IDFWRUV�IRU�&9'�
L� H*)5�� XVH� D0'5'� EDVHG� RQ� VHUXP� FUHDWLQLQH�� JHQGHU�� DJH� DQG�HWKQLFLW\��,I�QRW�SUHYLRXVO\�NQRZQ�WR�KDYH�&.'��UHDVVHVV�ZLWKLQ���ZHHNV
LL� 8ULQDO\VLV��XVH�XULQH�GLSVWLFN�WR�VFUHHQ�IRU�KDHPDWXULD��7R�VFUHHQ�IRU�SURWHLQXULD��XVH�XULQH�GLSVWLFN�DQG�LI������FKHFN�83�&��RU�VFUHHQ�ZLWK�83�&��3URWHLQXULD�GH¿QHG�DV�SHUVLVWHQW�LI�FRQ¿UPHG�RQ�����RFFDVLRQV�!�����ZHHNV�DSDUW��,I�83�&�QRW�DYDLODEOH��XVH�8$�&��VHH�QRWH�iii)
LLL� 83�&� LQ� VSRW� XULQH� �PJ�PPRO�� LV� SUHIHUUHG� WR�8$�&�DV�GHWHFWV� WRWDO�XULQDU\�SURWHLQ� VHFRQGDU\� WR�JORPHUXODU�$1'� WXEXODU�GLVHDVH��8$�&�ODUJHO\�GHWHFWV�JORPHUXODU�GLVHDVH�DQG�FDQ�EH�XVHG�IRU�VFUHHQLQJ�IRU�+,9�DVVRFLDWHG�UHQDO�GLVHDVH�ZKHUH�83�&�LV�QRW�DYDLODEOH��EXW�LV�QRW�DSSURSULDWH� IRU� VFUHHQLQJ� IRU� WXEXODU� SURWHLQXULD� VHFRQGDU\� WR� GUXJ�QHSKURWR[LFLW\� �H�J�� WHQRIRYLU���6FUHHQLQJ�YDOXHV� IRU�8$�&�DUH��������������DQG�!�����8$�&�VKRXOG�EH�PRQLWRUHG�LQ�SDWLHQWV�ZLWK�GLDEHWHV�PHOOLWXV��83&�UDWLR�LV�FDOFXODWHG�DV�XULQH�SURWHLQ��PJ�/����XULQH�FUHDWLQLQH��PPRO�/���PD\�DOVR�EH�H[SUHVVHG�DV�PJ�PJ��&RQYHUVLRQ�IDFWRU�IRU�PJ�WR�PPRO�FUHDWLQLQH�LV�[�����������
LY� &KHFN� ULVN� IDFWRUV� IRU�&.'��DQG� UHSHDW�H*)5�DQG�XULQDO\VLV�DV�SHU�VFUHHQLQJ�WDEOH��VHH�S��6)
Y� 'RVH�PRGL¿FDWLRQ�RI�$59V�LQ�FDVH�RI�LPSDLUHG�UHQDO�IXQFWLRQ��VHH�RQOLQH�WDEOH�IRU�“Indications and tests for proximal renal tubulopathy”
YL� -RLQW�PDQDJHPHQW�ZLWK�D�QHSKURORJLVWYLL� +,9$1� VXVSHFWHG� LI� EODFN� HWKQLFLW\� � 83�&� !� ���� PJ�PPRO� � QR�
KDHPDWXULDYLLL�6HH�S��31L[� 6HH�S��29
EACS Guidelines / 37
.LGQH\�GLVHDVH��GLDJQRVLV
eGFR (i)
�����P/�PLQ 30-59 mL/min < 30 mL/min
Prot
einu
ria (ii
)
83�&�(iii)������ 5HJXODU�)ROORZ�XS���&KHFN�ULVN�IDFWRUV�IRU�
CKD and nephrotoxic medication including ART (iv)
��'LVFRQWLQXH�RU�DGMXVW�drug dosages where appropriate (v)
��3HUIRUP�UHQDO�XOWUDVRXQG���8UJHQW�UHIHUUDO�WR�
nephrologist
83�&�(iii) 50-100
��&KHFN�ULVN�IDFWRUV�IRU�&.'�DQG�QHSKURWR[LF�PHGLFDWLRQ�including ART (iv)
��'LVFRQWLQXH�RU�DGMXVW�GUXJ�GRVDJHV�ZKHUH�DSSURSULDWH�(v) ��3HUIRUP�UHQDO�XOWUDVRXQG���,I�KDHPDWXULD�SUHVHQW�ZLWK�DQ\�OHYHO�RI�SURWHLQXULD�UHIHU�WR�QHSKURORJLVW�
��5HIHU�WR�QHSKURORJLVW�LI�QHZ�&.'�RU�SURJUHVVLYH�GHFOLQH�LQ�eGFR
83�&�(iii) > 100
Management of HIV-associated renal disease (vi)
Prevention of progressive renal disease Comment1� Antiretroviral therapy 6WDUW�$57�LPPHGLDWHO\�ZKHUH�+,9�DVVRFLDWHG�QHSKURSDWK\�
�+,9$1��(vii)�RU�+,9�LPPXQH�FRPSOH[�GLVHDVH�VWURQJO\�VXVSHFWHG��5HQDO�ELRSV\�WR�FRQ¿UP�KLVWRORJLFDO�GLDJQRVLV�UHFRPPHQGHG�
2� Start ACE inhibitors or angiotensin-II receptor antagonists if: D��+\SHUWHQVLRQ��DQG�RU�E��3URWHLQXULD�
Monitor eGFR and K+ level closely on starting treatment or increasing dose D��%ORRG�SUHVVXUH�WDUJHW������������PP+J
3� General measures: D��$YRLG�QHSKURWR[LF�GUXJV�E��/LIHVW\OH�PHDVXUHV��VPRNLQJ��ZHLJKW��GLHW��F��7UHDW�G\VOLSLGDHPLD�(viii)�DQG�GLDEHWHV�(ix)
G��$GMXVW�GUXJ�GRVDJHV�ZKHUH�QHFHVVDU\�
&.'�DQG�SURWHLQXULD�DUH�LQGHSHQGHQW�ULVN�IDFWRUV�IRU�&9'�
L� H*)5�� XVH� D0'5'� EDVHG� RQ� VHUXP� FUHDWLQLQH�� JHQGHU�� DJH� DQG�HWKQLFLW\��,I�QRW�SUHYLRXVO\�NQRZQ�WR�KDYH�&.'��UHDVVHVV�ZLWKLQ���ZHHNV
LL� 8ULQDO\VLV��XVH�XULQH�GLSVWLFN�WR�VFUHHQ�IRU�KDHPDWXULD��7R�VFUHHQ�IRU�SURWHLQXULD��XVH�XULQH�GLSVWLFN�DQG�LI������FKHFN�83�&��RU�VFUHHQ�ZLWK�83�&��3URWHLQXULD�GH¿QHG�DV�SHUVLVWHQW�LI�FRQ¿UPHG�RQ�����RFFDVLRQV�!�����ZHHNV�DSDUW��,I�83�&�QRW�DYDLODEOH��XVH�8$�&��VHH�QRWH�iii)
LLL� 83�&� LQ� VSRW� XULQH� �PJ�PPRO�� LV� SUHIHUUHG� WR�8$�&�DV�GHWHFWV� WRWDO�XULQDU\�SURWHLQ� VHFRQGDU\� WR�JORPHUXODU�$1'� WXEXODU�GLVHDVH��8$�&�ODUJHO\�GHWHFWV�JORPHUXODU�GLVHDVH�DQG�FDQ�EH�XVHG�IRU�VFUHHQLQJ�IRU�+,9�DVVRFLDWHG�UHQDO�GLVHDVH�ZKHUH�83�&�LV�QRW�DYDLODEOH��EXW�LV�QRW�DSSURSULDWH� IRU� VFUHHQLQJ� IRU� WXEXODU� SURWHLQXULD� VHFRQGDU\� WR� GUXJ�QHSKURWR[LFLW\� �H�J�� WHQRIRYLU���6FUHHQLQJ�YDOXHV� IRU�8$�&�DUH��������������DQG�!�����8$�&�VKRXOG�EH�PRQLWRUHG�LQ�SDWLHQWV�ZLWK�GLDEHWHV�PHOOLWXV��83&�UDWLR�LV�FDOFXODWHG�DV�XULQH�SURWHLQ��PJ�/����XULQH�FUHDWLQLQH��PPRO�/���PD\�DOVR�EH�H[SUHVVHG�DV�PJ�PJ��&RQYHUVLRQ�IDFWRU�IRU�PJ�WR�PPRO�FUHDWLQLQH�LV�[�����������
LY� &KHFN� ULVN� IDFWRUV� IRU�&.'��DQG� UHSHDW�H*)5�DQG�XULQDO\VLV�DV�SHU�VFUHHQLQJ�WDEOH��VHH�S��6)
Y� 'RVH�PRGL¿FDWLRQ�RI�$59V�LQ�FDVH�RI�LPSDLUHG�UHQDO�IXQFWLRQ��VHH�RQOLQH�WDEOH�IRU�“Indications and tests for proximal renal tubulopathy”
YL� -RLQW�PDQDJHPHQW�ZLWK�D�QHSKURORJLVWYLL� +,9$1� VXVSHFWHG� LI� EODFN� HWKQLFLW\� � 83�&� !� ���� PJ�PPRO� � QR�
KDHPDWXULDYLLL�6HH�S��31L[� 6HH�S��29
L’atteinte rénale chez un patient HIV+ est une indication à la tri thérapie*
* Gupta S CID 2005
Recommendations EACS 2011
90
EACS Guidelines / 36
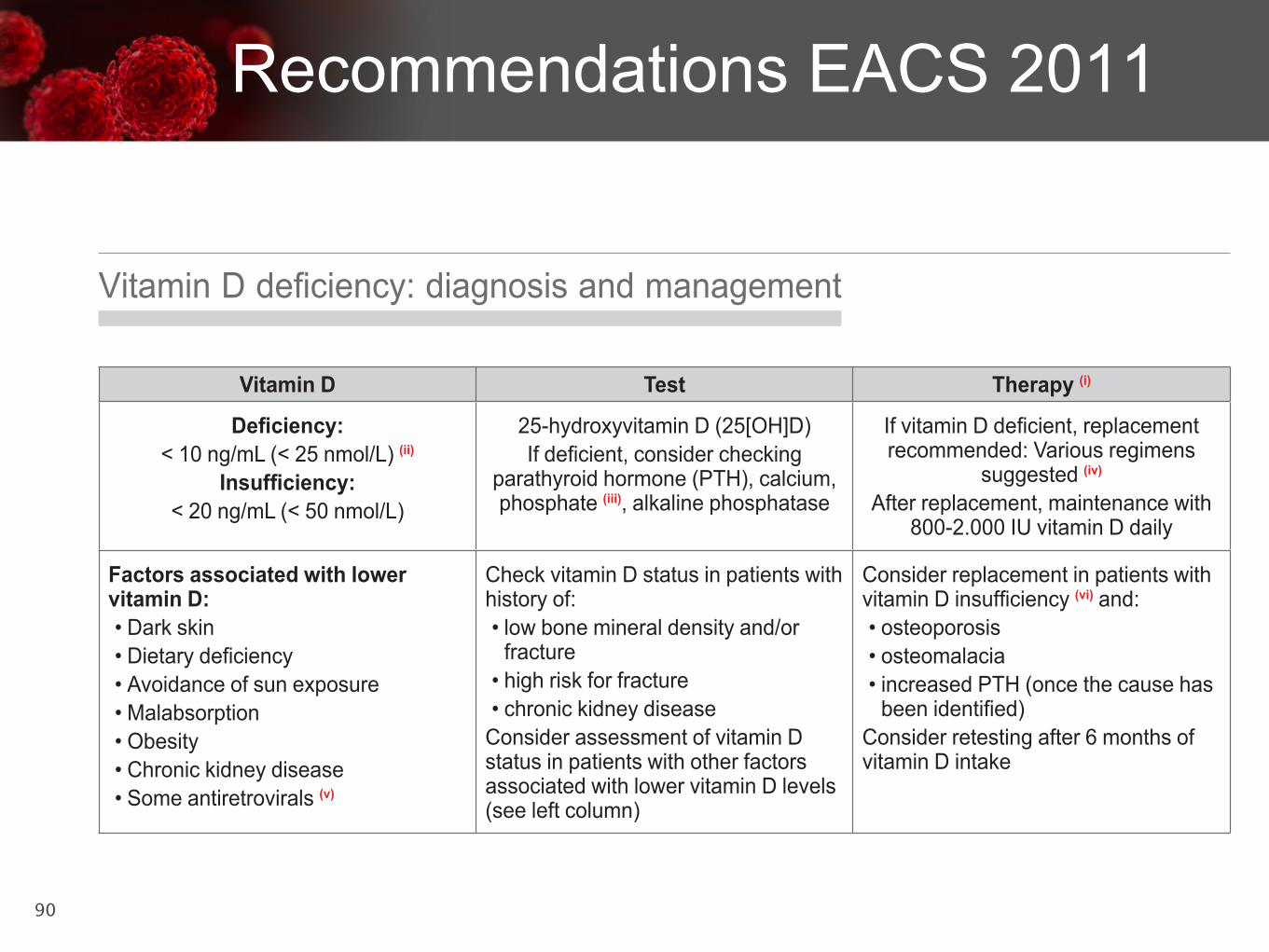
9LWDPLQ�'�GH¿FLHQF\��GLDJQRVLV�DQG�PDQDJHPHQW
Vitamin D Test Therapy (i)
'H¿FLHQF\������QJ�P/�������QPRO�/��(ii)
,QVXI¿FLHQF\������QJ�P/�������QPRO�/�
���K\GUR[\YLWDPLQ�'����>2+@'�,I�GH¿FLHQW��FRQVLGHU�FKHFNLQJ�
SDUDWK\URLG�KRUPRQH��37+���FDOFLXP��phosphate (iii)��DONDOLQH�SKRVSKDWDVH
,I�YLWDPLQ�'�GH¿FLHQW��UHSODFHPHQW�UHFRPPHQGHG��9DULRXV�UHJLPHQV�
suggested (iv)
$IWHU�UHSODFHPHQW��PDLQWHQDQFH�ZLWK�����������,8�YLWDPLQ�'�GDLO\
Factors associated with lower vitamin D:��'DUN�VNLQ��'LHWDU\�GH¿FLHQF\��$YRLGDQFH�RI�VXQ�H[SRVXUH��0DODEVRUSWLRQ��2EHVLW\��&KURQLF�NLGQH\�GLVHDVH��6RPH�DQWLUHWURYLUDOV�(v)
&KHFN�YLWDPLQ�'�VWDWXV�LQ�SDWLHQWV�ZLWK�KLVWRU\�RI���ORZ�ERQH�PLQHUDO�GHQVLW\�DQG�RU�
fracture��KLJK�ULVN�IRU�IUDFWXUH��FKURQLF�NLGQH\�GLVHDVH&RQVLGHU�DVVHVVPHQW�RI�YLWDPLQ�'�VWDWXV�LQ�SDWLHQWV�ZLWK�RWKHU�IDFWRUV�DVVRFLDWHG�ZLWK�ORZHU�YLWDPLQ�'�OHYHOV��VHH�OHIW�FROXPQ�
&RQVLGHU�UHSODFHPHQW�LQ�SDWLHQWV�ZLWK�YLWDPLQ�'�LQVXI¿FLHQF\�(vi)�DQG���osteoporosis��RVWHRPDODFLD��LQFUHDVHG�37+��RQFH�WKH�FDXVH�KDV�EHHQ�LGHQWL¿HG�
&RQVLGHU�UHWHVWLQJ�DIWHU���PRQWKV�RI�YLWDPLQ�'�LQWDNH
L� &DQ�EH�SURYLGHG�DFFRUGLQJ�WR�QDWLRQDO�UHFRPPHQGDWLRQV�DYDLODELOLW\�RI�SUHSDUDWLRQV��RUDO�DQG�SDUHQWHUDO�IRUPXODWLRQV���&RPELQH�ZLWK�FDOFLXP�ZKHUH�WKHUH�LV�LQVXI¿FLHQW�GLHWDU\�FDOFLXP�LQWDNH��&RQVLGHU�WKDW�LQ�VRPH�FRXQWULHV�IRRG�LV�DUWL¿FLDOO\�IRUWL¿HG�ZLWK�YLWDPLQ�'�
LL� 6RPH�H[SHUWV�FRQVLGHU�D�YDOXH�RI������QJ�P/�DV�YLWDPLQ�'�GH¿FLHQF\��/RZ� YLWDPLQ�'�KDV� D� SUHYDOHQFH� RI� XS� WR� ����� LQ�+,9� FRKRUWV� DQG�ZDV�DVVRFLDWHG�ZLWK�LQFUHDVHG�ULVN�IRU�RVWHRSRURVLV��W\SH���GLDEHWHV��PRUWDOLW\�DQG�$,'6�HYHQWV��&RQVLGHU�VHDVRQDO�GLIIHUHQFHV��GXULQJ�ZLQWHU�DSSUR[LPDWHO\������ORZHU�WKDQ�GXULQJ�VXPPHU��
LLL� &RQVLGHU� WKDW� K\SRSKRVSKDWDHPLD� FDQ� EH� DVVRFLDWHG� ZLWK� 7')�WKHUDS\�� 7KLV� SKRVSKDWH� ORVV� WKURXJK� SUR[LPDO� UHQDO� WXEXORSDWK\�PD\� EH� LQGHSHQGHQW� RI� ORZ� YLWDPLQ�'� �VHH� WDEOH� ³Drug-associated nephrotoxicity´��� $� FRPELQDWLRQ� RI� ORZ� FDOFLXP� �� ORZ� SKRVSKDWH�����KLJK�DONDOLQH�SKRVSKDWDVH�PD\�LQGLFDWH�RVWHRPDODFLD�DQG�ODFN�RI�YLWDPLQ�'��
LY� ([SHFW� WKDW�����8�YLWDPLQ�'�GDLO\� OHDGV� WR�DQ� LQFUHDVH�RI���QJ�P/��6RPH�H[SHUWV�SUHIHU�D� ORDGLQJ�GRVH�RI�H�J��������8�YLWDPLQ�'�GDLO\�IRU������ZHHNV�LQ�SDWLHQWV�ZLWK�YLWDPLQ�'�GH¿FLHQF\��7KH�SULQFLSDO�JRDO�LV�WR�DFKLHYH�D�VHUXP�OHYHO�!����QJ�P/�DQG�WR�PDLQWDLQ�QRUPDO�VHUXP�37+�OHYHOV��7KH�WKHUDSHXWLF�DLP�LV�WR�PDLQWDLQ�VNHOHWDO�KHDOWK��YLWDPLQ�'�VXSSOHPHQWDWLRQ�KDV�QRW�EHHQ�SURYHQ�WR�SUHYHQW�RWKHU�FR�PRUELGLWLHV�LQ�+,9�SDWLHQWV�
Y� 7KH�UROH�RI�+,9�WKHUDS\�RU�VSHFL¿F�GUXJV�UHPDLQV�XQFOHDU��6RPH�VWXGLHV�VXJJHVW�DQ�DVVRFLDWLRQ�RI�HIDYLUHQ]�ZLWK�UHGXFWLRQV�LQ�YLWDPLQ�'�
YL� 7KH� LPSOLFDWLRQV�RI�YLWDPLQ�'� OHYHOV� WKDW�DUH�EHORZ�WKH�SK\VLRORJLFDO�UHIHUHQFH� UDQJH� EXW� QRW� PDUNHGO\� UHGXFHG� DQG� WKH� YDOXH� RI�VXSSOHPHQWDWLRQ�DUH�LQFRPSOHWHO\�XQGHUVWRRG�