Embed Size (px)
Citation preview

Cas clinique
DOI of or
Pr�esent�e aucular Surgical
1Division oSurgery, Harb
2Asociaci�onUruguay.
CorrespondEndovascularson Street, Tor
Ann Vasc Surghttp://dx.doi.or� Annals of V�Edit�e par ELS
Traitement endovasculaire des traumatismesaortiques ferm�es avec une art�ere sous-clavi�eredroite aberrante associ�ee : Rapport de trois cas
Tyler S. Reynolds,1 Carlos E. Donayre,1 Carmelo Gastambide Somma,2 Walter Giossa Poggio,2
Karen M. Kim,1 Tien Nguyen,1 Rodney White,1 Torrance, California, USA, et Montevideo,
Uruguay
La rupture traumatique de l’aorte dans les cas rares d’art�ere sous-clavi�ere droite aberrante(ARSA) exige une attention sp�eciale pour empecher la survenue d’un AVC post�erieurd�evastateur. Nous pr�esentons trois cas trait�es en employant une approche endovasculaire,avec un examen des donn�ees pr�eop�eratoires et op�eratoires importantes. Trois patientsimpliqu�es dans des collisions de v�ehicule �a moteur avec des l�esions multiples ont �et�e trait�esdans deux �etablissements. Le scanner montrait une transsection de l’aorte et une ARSA. Cha-cun des trois cas a �et�e trait�e avec une approche diff�erente. Un patient n’a pas eu de pontagepr�eop�eratoire parce que l’imagerie confirmait une zone d’ancrage satisfaisante distale �a l’originede l’art�ere sous-clavi�ere gauche. Deux patients ont eu un pontage pr�eop�eratoire entre la caro-tide droite et la sous-clavi�ere devant la couverture pr�evue des deux art�eres sous-clavi�eres par lestentgraft pour pr�eserver un flux dans une art�ere vert�ebrale. Chez un patient, un dispositif endo-vasculaire d’occlusion a �et�e d�eploy�e dans l’ARSA avant d�eploiement aortique d’un stentgraft.Chez l’autre, l’occlusion de l’ARSA a �et�e effectu�ee 4 jours plus tard pour une endofuite persis-tante de type II. Le patient qui a eu un pontage et l’occlusion pr�eop�eratoire de l’ARSA a fait unAVC post�erieur mortel peu de temps apr�es la chirurgie. Les deux autres patients n’ont euaucune complication proc�edurale et n’ont eu besoin d’aucune r�einterventions avec un suivi de2 et 5 ans. Un patient est toujours en r�eadaptation apr�es 5 ans de suivi pour des l�esions trau-matiques c�er�ebrales ind�ependantes de la r�eparation par stentgraft. Bien que l’incidence del’ARSA soit tr�es limit�ee, l’imagerie et l’�evaluation pr�eop�eratoire du flux sanguin c�er�ebral sont cri-tiques pour empecher un AVC p�eriop�eratoire. La revascularisation, si elle est n�ecessaire pourobtenir une zone proximale sure de largage, doit etre effectu�ee avant le d�eploiement du stent-graft. La revascularisation sous-clavi�ere bilat�erale est indiqu�ee si des anomalies de la circulationc�er�ebrale sont pr�esentes.
iginal article: 10.1016/j.avsg.2011.05.001.
28�eme Annual Meeting de la Southern California Vas-Society, 30 avril e 1er mai 2010, Carlsbad, CA, USA.
f Vascular and Endovascular Surgery, Department ofor-UCLA Medical Center, Torrance, CA, USA.
Espa~nola Primera de Socorros Mutuos, Montevideo,
ance : Carlos E. Donayre, Division of Vascular andSurgery, Harbor-UCLA Medical Center, 1000 West Car-rance, CA 90502, USA, E-mail: [email protected]
2011; 25: 979.e7-979.e12g/10.1016/j.acvfr.2012.10.014ascular Surgery Inc.EVIER MASSON SAS
INTRODUCTION
Aortic transection occurs in only 0.8% of motor
vehicle collisions but accounts for 16% of associated
deaths.1 Endovascularmanagement of these injuries
is rapidly evolving and may soon become first-line
treatment for select patients. Sufficient landing
zone to avoid a type I endoleak often requires
coverage of the left subclavian artery. The absolute
and relative indications for selective revasculariza-
tion of the left subclavian artery are discussed.
Aberrant right subclavian artery (ARSA), also
referred to as arteria lusoria, is the most common
1043.e7

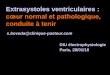
Fig. 1. Thoracic aortic transection with aortic hematoma,
left hemothorax, and aberrant right subclavian artery
(ARSA).
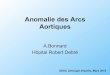
Fig. 2. Postoperative computed tomographic recon-
struction showing endograft in good position with a
patent left subclavian artery and exclusion of the ARSA.
1043.e8 Cas cliniques Annales de chirurgie vasculaire
intrathoracic arterial abnormality occurring in 0.45-
2% of the population. The abnormality is often
discovered incidentally on diagnostic imaging.2,3 To
our knowledge, the endovascular management of
transection of the thoracic aorta with ARSA has not
been previously reported. In the special setting of an
ARSA and a transected aorta, endograft coverage of
both subclavian vessels mandates revascularization
of one or possibly both vessels. We report manage-
ment of three such cases over a 5-year period at two
different institutions.
Case 1
A 21-year-old female asthmatic was struck laterally
by a truck while she was in her vehicle. She was
unconscious on arrival to the emergency room and
was intubated for respiratory depression with a
stable blood pressure. She had stigmata of facial and
blunt chest trauma. Computed tomography (CT)
showed a left maxillary and frontal skull fracture
with hemorrhagic brain injury. CT of the thorax
showed aortic injury, with a mediastinal hematoma
and hemothorax (Fig. 1). AnARSAoriginating distal
to the left subclavian artery was also noted. Trans-
esophageal ultrasound confirmed an aortic intimal
disruption with an associated pseudoaneurysm.
The patient was initially stabilized in the inten-
sive care unit and underwent thoracic endovascular
aortic repair (TEVAR) the following day.
A TALENT (Medtronic, Inc., Santa Rosa, CA),
26 mm in diameter and 150 mm in length, endo-
prosthesis was successfully deployed just distal to
the origin of the left subclavian artery with exclu-
sion of the transection and the ARSA.
She subsequently underwent tracheostomy
5 days later, followed by gastrostomy, and was dis-
charged 2 months after the incident with moderate
neurologic impairment secondary to traumatic
brain injury. At that time, a repeat CT showed no
evidence of endoleak and successful endovascular
exclusion of her transected aorta. CT scan at 1 and
5 years later confirmed the lack of endoleaks and
no migration (Fig. 2). She is still undergoing neu-
rologic rehabilitation while working as a secretary.
Case 2
A 40-year-old man was driving a semi-truck when
he struck another truck. After a 90-minute extri-
cation, he was brought to a local emergency
department in a hypotensive state with a blood
pressure of 85/52 mm Hg and required intubation.
Abdominal ultrasound demonstrated fluid in Mor-
rison’s pouch. He was given 4 U of packed red blood
cells and 4 U of fresh frozen plasma, and blood
pressure was restored to normal. CT scan revealed
an open-book pelvic fracture and a possible aortic
injury. The patient was airlifted to our institution
where CT angiogram confirmed aortic transection
and ARSA. CT angiogram of the brain demonstrated
questionable filling of the right posterior commu-
nicating artery of the circle ofWillis; however, it was
believed to be patent. The vertebral arteries were of
good caliber.
The patient was taken to the endovascular suite
immediately where transesophageal ultrasound
and intravascular ultrasound confirmed transection
located just distal to the left subclavian origin. A right
carotid to right axillary bypass was performed using
an 8-mm polytetrafluoroethylene to preserve flow

Fig. 3. Fluoroscopy demonstrating axillary to right
common carotid artery bypass graft followed by Amplat-
zer vascular plug placement to exclude the ARSA.
Fig. 4. Angiogram demonstrating site of traumatic aortic
transection with origin of associated aberrant right sub-
clavian artery (ARSA) (white arrow). RCCA, right com-
mon carotid artery; LCCA, left common carotid artery;
LSA, left subclavian artery.
Vol. 25, No. 7, 2011 Cas cliniques 1043.e9
to the right vertebral artery. A 14 mm Amplatzer
vascular plug (AGA Medical Corp., Minneapolis,
MN) was then deployed in the proximal right sub-
clavian artery (Fig. 3).
A TALENT (Medtronic, Inc.), 32 mm in diameter,
endoprosthesis was subsequently deployed exclud-
ing the right and left subclavian arteries.
Adenosine-induced temporary cardiac arrest was
performed to ensure proper placement of the
endoprosthesis, and postoperative angiogram con-
firmed good placement without endoleak.
The patient was transferred back to the intensive
care unit in stable condition; however, he began to
require increased ventilator support 6 hours later
and had decreased ocular reflexes. CT confirmed
posterior stroke with massive cerebral edema and
basilar artery thrombosis. The patient expired
shortly thereafter.
Case 3
A 47-year-old man involved in a motor vehicle
collision was found to have multiple pelvic fractu-
res, acute diaphragmatic hernia, and widened
mediastinum. He was hemodynamically stable;
however, CT confirmed aortic transection, and so
the patient was transferred to our institution. CT
angiogram revealed transection of the aorta with
incidental ARSA. It also demonstrated an intact
circle of Willis and normal vertebral arteries. The
patient was taken directly to the operating room.
Angiography revealed approximately 15 mm bet-
ween the lowermost edge of the left common
carotid and the beginning of the transaction and the
aberrant vessel could also be visualized (Fig. 4).
A right carotid to right axillary bypass using an
8-mm polytetrafluoroethylene was again per-
formed followed by device deployment. A 36-mm
Valiant endoprosthesis (Medtronic, Inc.) was selec-
ted. After full deployment of the thoracic endo-
prosthesis, IVUS interrogation and angiography
revealed full endoprosthesis expansion and good
placement just distal to the left common carotid
artery. Type II endoleak was visualized from the
ARSA, as expected (Fig. 5). Given the patient’s other
injuries, he was then taken for repair of the dia-
phragmatic injury, with a plan to return later for
occlusion of the proximal right subclavian artery.
Repeat CT the next day confirmed persistent type
II endoleak from retrograde filling of the ARSA, and
the patient was taken on postoperative day 4 for
endoluminal exclusion of the leak using a 12-mm
Amplatzer vascular plug. The patient has done
well 2 years later with no further interventions.
DISCUSSION
Endovascular repair may soon become the first-line
treatment for transection of the aorta. Traumatic
rupture of the aortic isthmus can occur with rapid
deceleration or extreme shear forces after blunt
chest trauma.4 Mechanisms include compression
and blast forces, especially in the vertical or hori-
zontal axis.5 Immediate death has been reported in
>75% of cases.4-7 In an autopsy series of all post-
mortem examinations over a 4-year period, trau-
matic rupture of the aorta was found in 16% of
automobile accidents resulting in death.6 This
patient population is younger than those with other
thoracic aortic pathology, including aneurysm and
dissection. The pathology and characteristics of the

Fig. 5. Final angiogram demonstrating type II endoleak
secondary to retrograde filling through ARSA.
1043.e10 Cas cliniques Annales de chirurgie vasculaire
aorta are quite different. Our institution has found
the aorta in these younger patients to be more
compliant than older patients (T. Reynolds et al.,
unpublished data, January 2011). This may be
related to normal aging or a physiologic change after
blunt aortic injury.
In a prospective study of blunt aortic injury by the
American Association for the Surgery of Trauma in
1996, the average time to open operative repair for
transection was just over 16 hours.8 However, the
average time taken to perform an endovascular
repair at our institution is less than 16 hours. In the
same study, reportedmortality rate with open repair
is 14.9-15.1%, depending on technique.
In an analysis by Tang et al. in 2008, endovascu-
lar repair was compared with open surgery.9 Mor-
tality rate is lower with endovascular repair at 7.6
versus 15.2%. Paraplegia rate was reported to be 0%
with endovascular repair and 5.6% for open repair.
Stroke is also lower at 0.8 versus 5.6%. A later study
by the American Association for the Surgery of
Trauma in 2008 showed similar rates of paraplegia
in both groups, and additionally reported device-
related complications, including vascular access
(4.8%) and endoleak (13.6%).10
Endovascular management of aortic transection
has been shown to be safe and effective in clinical
trials. The evolution of management of blunt aortic
injury is well summarized by Neschis et al. in
2008.11 Several advantages of endovascular repair
include decreased blood loss, operative time, hos-
pital stay, and most importantly, aortic clamping is
not necessary; therefore, risks associated with
shunting and bypass are avoided. Perioperative
mortality is decreased with endovascular repair at
6.8% compared with 16-31% for open repair.
Stroke and paraplegia rates have been shown to be
lower with endovascular repair when compared
with open repair.11
Anticoagulants are routinely administered dur-
ing stent-graft deployment. Systemic hepariniza-
tion is avoided in the setting of complex solid organ
injury, concern for head trauma/brain injury, or
significant pelvic fractures. In such cases, we con-
nect only access sheaths to a heparin solution to
prevent formation of thrombus within the sheaths.
The previously published data are limited in
regard to the timing of repair of aortic transection.
Patients without pseudoaneurysm formation and
minimal intimal disruptionmay be able to be mana-
ged with delayed treatment or nonoperative mana-
gement. However, if the transection is complex
(pseudoaneurysm, intra-aortic thrombus, or
hemothorax), then it should be treated emergently.
At this time, delayed repair may be a reasonable
alternative in carefully selected patients with long-
term follow-up and imaging.12,13 Serial radio-
graphic examinations during the first week are
necessary because of the potential for rapid pro-
gression of the aortic injury.14
Subclavian artery revascularization
Controversy exists regarding routine or selective
revascularization with the coverage of one subcla-
vian (left) artery during TEVAR without ARSA.
Selective revascularization, through carotid-to-
subclavian bypass or transposition of the sub-
clavian artery, for patients with unfavorable
anatomy has been shown to be safe. Reece et al.
reported on 27 patients who underwent TEVAR
requiring coverage of the left subclavian artery
(LSA) among 64 patients in the series.15 Seven
patients underwent selective preoperative revascu-
larization based on vascular anatomy. The indica-
tions for TEVAR for these patients were not
mentioned; however, indications for preemptive
revascularization included dominant left vertebral
artery (one patient), incomplete Circle ofWillis (two
patients), ARSA (three patients), and left internal
mammary artery-to-left anterior descending artery
bypass (one patient). The three patients with ARSA
underwent revascularization 1-3 days before
TEVAR. Among the 20 patients who were not
revascularized, three developed left arm claudica-
tion and one developed postoperative retrograde
aortic dissection and subclavian steal syndrome. All
four patients subsequently underwent post-
operative LSA revascularization with no further
symptoms. There was no perioperative mortality or
paraplegia in the series and no significant posterior
circulation strokes or permanent left arm deficits.
In a single-institution study by Botta et al. in
2008, management of the left subclavian artery was

Vol. 25, No. 7, 2011 Cas cliniques 1043.e11
addressed.7 Of 27 patients who underwent endo-
vascular repair for acute traumatic transection of the
descending aorta, eight had an aorta with a short
proximal neck (<5 mm), and four of these patients
underwent endovascular complete or partial LSA
coverage. The other four patients had pseudo-
aneurysm of the left subclavian or left carotid artery
and were treated with conventional open inter-
vention. A single patientwith LSA coverage suffered
a large cerebellar stroke despite the absence of any
alteration of the circle ofWillis. The properties of the
vertebral arteries on preoperative imaging, namely
dominance, are not reported.
Riesenman et al. reported outcomes of 28 of 112
patients who underwent complete or partial cove-
rage of the left subclavian artery.16 Debranching
was performed for zone 0 or 1 coverage. Three of
these patients underwent carotid-to-carotid bypass
and one of these underwent left carotid-to-
subclavian bypass for right vertebral artery
stenosis. One patient who did not undergo revas-
cularization developed positional claudication of the
left hand while turning his head. Fourteen of 24
patients who underwent zone 2 placement had
complete coverage of the left subclavian artery.
Three patients developed left upper extremity
symptoms but did not require intervention. One
patient who had been treated emergently for a
ruptured mycotic aneurysm developed rest pain
requiring revascularization was found to have
aberrant insertion and coverage of a left vertebral
artery. Three embolic strokes were reported
(12.5%), but none were attributed to vertebral-
basilar insufficiency ischemia. The authors conclu-
ded that prophylactic revascularization is not
necessary.
Options for maintaining subclavian artery
patency during TEVAR include carotid-to-
subclavian bypass or transposition, as well as
endovascular techniques including fenestrated and
branched grafts, and the ‘‘chimney procedure.’’17
The ‘‘chimney (snorkel) procedure’’ may be performed
to improve forward flow through the subclavian
artery with the placement of a subclavian stent at
the orifice of the subclavian artery. This allows
extension of the aortic endograft over a portion of
the subclavian artery. The anatomy must be favo-
rable, including an adequate neck distal to the left
subclavian to minimize risk of a type I endoleak
around the subclavian stent.
Aberrant right subclavian artery
The ARSA results from a developmental abnorma-
lity likely related to regression of the right fourth
aortic arch and persistence of the distal right dorsal
aorta. It usually travels posterior to the esophagus
and is usually asymptomatic. Less than 10% of
patients develop dysphagia lusoria and the origin
can become aneurysmal in 8% of patients (Komme-
rell’s Diverticulum).3,18 Other abnormalities com-
monly seen with this anomaly include a
nonrecurrent right inferior laryngeal nerve, a com-
mon origin of the common carotid arteries, a
replaced right or left vertebral artery, coarctation of
the aorta, a right-sided thoracic duct, and a dex-
troposed aortic arch.18 Symptoms of progressive
dysphagia or aneurysmal disease prompt surgical
intervention.
There are several case reports in the previously
published data describing surgical repair of sympto-
matic ARSA as well as special considerations in the
repair of type B dissection.19-22 Traumatic rupture
of an ARSA has also been reported.23 Bednarkiewicz
et al. emphasized the importance of preoperative
diagnosis of ARSA in a patient with blunt aortic
injury treated by open surgical approach.24 Clamp-
ing of the aorta proximal to both subclavian arteries
with inadvertent exclusion of both vertebral arteries
may lead to posterior circulation ischemia. Revas-
cularization is the mainstay of therapy.
We prefer right carotid-to-axillary bypass initially
because it eliminates the risk of aneurysm formation
later in the ARSA, similar to what happens with the
persistent sciatic artery. However, if the left verte-
bral artery is dominant, a left carotid-to-subclavian/
axillary bypass is indicated.
CONCLUSION
The devastating complications emphasize the
importance of careful preoperative planning. The
CT angiogram is essential in all patients not only to
characterize the nature of the aortic injury and asso-
ciated injuries in the stable trauma patient, but also
to detect any pertinent anomaly such as the ARSA.
A widened mediastinum on plain chest film and
transesophageal echocardiogram alone are not
sensitive for detection of ARSA. Failure to recognize
the surgical and clinical ramifications can have
drastic consequences. Carotid-to-subclavian arte-
rial bypass before endograft exclusion of the verte-
bral arteries has been shown to successfully
maintain posterior circulatory flow through the
vertebral artery.
The following principles are emphasized from the
cases discussed. First, preoperative CT angiography
or aortography is vital to assess aortic anatomy,
vertebral-basilar system, and cerebral vasculature.

1043.e12 Cas cliniques Annales de chirurgie vasculaire
Second, forward flow must be maintained through
the vertebral-basilar system to maintain posterior
cerebral perfusion. Indications for revascularization
include incomplete circle of Willis, exclusion of a
dominant vertebral artery, presence of internal
mammary coronary artery bypass, and ipsilateral
functioning hemodialysis access. Relative indica-
tions also include extensive aortic coverage, pre-
vious abdominal aortic aneurysm repair, and
aberrant left vertebral artery.
The landing zone is often proximal to both sub-
clavian arteries in the patient with ARSA. In this
setting, a unilateral revascularization procedure is
absolutely necessary to maintain perfusion of the
posterior circulation of the brain. Selective bilateral
revascularization in the setting of ARSA is then indi-
cated in the special settings discussed.
Bilateral revascularization is recommended in the
setting of incomplete Circle of Willis. In case 2, flow
in the right posterior communicating artery of the
circle of Willis was questionable. A left carotid-to-
subclavian or axillary bypass, subclavian-carotid
transposition, or endovascular technique, includ-
ing the ‘‘Chimney procedure,’’ are options for
revascularization.17 If both vertebral arteries need to
be revascularized, we prefer right carotid-to-
subclavian/axillary artery bypass and a ‘‘chimney’’
procedure to maintain perfusion of the left vertebral
artery.
Third, if revascularization is necessary, it must be
performed before endoluminal exclusion to pre-
serve flow through the vertebral-basilar system.
Carotid artery to axillary bypass is a rapid revascu-
larization procedure and is preferred by some sur-
geons in the setting of aortic transection. Finally, the
need for occlusion of the native ARSA in the setting
of type II endoleak is not urgent because associated
morbidity is low. In fact, acute changes in perfusion
through the vertebral arteries may be detrimental.
The anticipated type II endoleak in case 3 was
occluded 4 days later with no complications.
In conclusion, traumatic rupture of the aorta
with ARSA can be managed successfully with an
endovascular approach. As endovascular repair
continues to replace open repair as first-line treat-
ment for most patients, thorough preoperative
planning will improve outcomes and assist in the
development of innovative techniques for compli-
cated patients.
REFERENCES
1. Jahromi A, Kazemi K, Safar H, Doobay B, Cina C. Traumatic
rupture of the thoracic aorta: cohort study and systematic
review. J Vasc Surg 2001;34:1029-1034.
2. Felson B, Cohen S, Courter S, McGuire J. Anomalous right
subclavian artery. Radiology 1950;54:340-349.
3. Freed K, Low V. The aberrant subclavian artery. Am J
Roentgenol 1997;166:481-484.
4. Sevitt S. The mechanism of traumatic rupture of the thoracic
aorta. Br J Surg 1977;64:166-173.
5. Parmley LF, Mattingly TW, Mariom WC, Jahnke EJ. Non-
penetrating traumatic injury of the aorta. Circulation
1958;17:1086-1101.
6. Greendyke RM. Traumatic rupture of aorta. Special refe-
rence to automobile accidents. JAMA 1996;195:119-122.
7. Botta L, Russo V, Savini C, et coll. Endovascular treatment
for acute traumatic transaction of the descending aorta:
focus on operative timing and left subclavian artery
management. J Thorac Cardiovasc Surg 2008;136:
1558-1563.
8. Fabian T, Richardson J, Croce M, et coll. Prospective study of
blunt aortic injury: multicenter trial of the American Asso-
ciation for the Surgery of Trauma. J Trauma 1997;42:
374-383.
9. Tang G, Tehrani H, Usman A, Katariya K, Otero C, Perez E,
Eskandari M. Reduced mortality, paraplegia, and stroke with
stent graft repair of blunt aortic transections: a modern
meta-analysis. J Vasc Surg 2008;47:671-675.
10. Demetriades D, Velmahos G, Scalea T, et coll. Diagnosis and
treatment of blunt thoracic aortic injuries: changing per-
spectives. J Trauma 2008;64:1415-1419.
11. Neschis D, Scalea T, Flinn W, Griffith B. Blunt aortic injury.
N Engl J Med 2008;359:1708-1716.
12. Cafarelli A, Mallidi H, Maggio P, Spain D, Miller D,
Mitchell S. Early outcomes of deliberate nonoperative
management for blunt thoracic aortic injury in trauma.
J Thorac Cardiovasc Surg 2010;140:598-605.
13. Symbas P, Sherman A, Silver J, Symbas J, Lackey J. Trau-
matic rupture of the aorta: immediate or delayed repair?
Ann Vasc 2002;235:796-802.
14. Holmes J, Bloch R, Hall A, Carter Y, Karmy-Jones R. Natural
history of traumatic rupture of the thoracic aorta managed
nonoperatively: a longitudinal analysis. Ann Thorac Surg
2002;73:1149-1154.
15. Reece B, Gazoni L, Cherry K, et coll. Re-evaluating the need
for left subclavian artery revascularization with thoracic
endovascular aortic repair. Ann Thorac Surg 2007;84:
1201-1205.
16. Riesenman P, Farber M, Mendes R, Marston W, Fulton J,
Keagy B. Coverage of the left subclavian artery during
thoracic endovascular aortic repair. J Vasc Surg 2007;45:
90-95.
17. Criado F. A percutaneous technique for preservation of arch
branch patency during thoracic endovascular aortic repair
(TEVAR): retrograde catheterization and stenting. J Enco-
vasc Ther 2007;14:54-58.
18. Epstein D, Debord J. Abnormalities associated with aberrant
right subclavian arteries-a case report. Vasc Endovascular
Surg 2002;36:297-303.
19. Weinberger G, Randall A, Parker B, Kiefer A. Involvement
of an aberrant right subclavian artery in dissection of the
thoracic aorta: diagnostic and therapeutic implication. Am J
Roentgenol 1977;129:653-655.
20. Mosquera V, Marini M, Rodriguez F, Cao I, Juffe A. Com-
plicated acute type B aortic dissection with involvement of
an aberrant right subclavian artery and rupture of a thora-
coabdominal aortic aneurysm, Crawford type I: successful
emergency endovascular treatment. J Thorac Cardiovasc
Surg 2007;134:1055-1057.

Vol. 25, No. 7, 2011 Cas cliniques 1043.e13
21. Baccin C, Montegegro M, Mour~ao G. Thoracic aorta dis-
section associated with aberrant right subclavian artery:
treatment with endovascular stent-graft placement. Yale J
Biol Med 2004;77:59-62.
22. Syme J. Aortic dissection involving an aberrant right sub-
clavian artery studied by aortography. Aust Radiol 1973;17:
174-179.
23. Alcocer J, Spier L, Dyke C, Griffith B, Gammie J. Traumatic
rupture of an aberrant right subclavian artery. Ann Thorac
Surg 2000;69:621-623.
24. Bednarkiewicz M, Robert J, Khatchatourian G, Genin G,
IrmayF, Faidutti B. Traumatic rupture of the aortic isthmus in
a patientwith an aberrant right subclavian artery: therapeutic
implications. J Thorac Cardiovasc Surg 1999;118:1112-1113.