Embed Size (px)
Citation preview

Vous recevez aux urgences Pierre âgé de 62 ans, adressé par sa famille pour troubles de la conscience. Sa femme vous signale avoir retrouvé son mari au domicile, inconscient, avec impossibilité de le réveiller. Le pa@ent a par ailleurs vomi à plusieurs reprises. Ses antécédents sont représentés par une hypertension artérielle et une fibrilla@on atriale. Son traitement comporte : APROVEL, COUMADINE. A l’examen, le pa@ent ouvre les yeux et gémit à la s@mula@on nocicep@ve sans réponse motrice. Les pupilles sont symétriques et réac@ves. T°=39,3°C, PA=90/40 mmHg, FC=110/min, SpO2 à 91% en AA, FR=30/min. Les bruits du cœur sont réguliers, sans souffle. Il existe une raideur de nuque. L’ausculta@on thoracique est sans par@cularité. L’examen cutané retrouve des marbrures des genoux, Il n’y a pas de lésion purpurique.
QUESTION 1 Quels diagnos@cs suspectez-‐vous ?
Cas clinique N°2, -‐ Pierre 62 ans

QUESTION 1 Quels diagnos@cs suspectez-‐vous ?
Ø Méningite bactérienne :
Ø Syndrome infec@eux avec sepsis sévère -‐ Fièvre -‐ hypotension artérielle, tachycardie, marbrures
Ø Une adeinte méningée
-‐ Raideur de nuque -‐ Vomissements
Ø Une adeinte encéphali@que
-‐ Coma (Score de Glasgow=5)
Mr G. Pierre âgé de 62 ans

Score de coma de Glasgow
Ouverture des yeux score Réponse motrice score Réponse verbale score
volontaire, spontanée 4 aux ordres 6 paroles orientées 5
sur ordres, au bruit 3 vers zone stimulée 5 paroles confuses 4
à la douleur 2 évitement 4 délire 3
pas de réponse 1 flexion MS-extension MI
3 capable deréponse simple/incompréhensible
2
extension MS etMI
2 pas de réponse 1
nulle 1

QUESTION 2 Détaillez votre prise en charge diagnos@que et thérapeu@que concernant la méningite au cours de la première heure ?
Ø An@biothérapie en urgence : -‐ Après réalisa@on d’hémocultures -‐ Après administra@on de Dexaméthasone 10mg (0,15 mg/kg) puis toutes les 6 heures -‐ Céphalosporine de 3ème généra@on à dose méningée :
-‐ Cekriaxone : 100mg/kg/j (en 2 injec@ons à12 heures) -‐ Cefotaxime : bolus 50mg/kg en une heure puis 300mg/kg/j IVSE
Ø Imagerie cérébrale (TDM) -‐ Recherche d’une contre-‐indica@on à la ponc@on lombaire
Ø
Méningite bactérienne :

Etiologie des méningites purulentes en fonction de l’âge



QUESTION 2 Détaillez votre prise en charge diagnos@que et thérapeu@que concernant la méningite au cours de la première heure ?
Ø Imagerie cérébrale (TDM) normale
Ø Ponc@on lombaire : -‐ Après antagonisa@on de la Coumadine (PPSB + vitamine K1)* -‐ Examen Cyto-‐bactériogique + Biochimique (protéinorachie et Glycorachie) -‐ Glycémie capillaire concomitante

QUESTION 3 Détaillez votre prise en charge symptoma@que ?
Ø Hospitalisa@on en réanima@on Ø Intuba@on et ven@la@on mécanique Ø Expansion volémique +/-‐ support vasopresseur Ø Neuroprotec@on – lude contre l’HTIC:
-‐ Séda@on -‐ Posi@on demi assise (30°C) -‐ Préven@on des ACSOS -‐ Monitorage éventuel de la PIC -‐ Isolement neuro-‐sensoriel
NB : hypothermie thérapeu@que délétère !
Mr G. Pierre âgé de 62 ans


Traitements associés • An@épilep@que en cas de crise convulsive
– Clonazepam ou Rivotril (1 ou 2 injec@ons) -‐ Réanima@on – Phenytoine ou phenobarbital IV, éventuellement mais risque hypotension
artérielle et hypoperfusion cérébrale
• Traitement de l’hypertension intracrânienne – correc@on d’une PA basse : remplissage vasculaire, drogues inotropes – réduc@on de la pression intracrânienne. Dans les formes sévères : suréléva@on de
la tête à 20-‐30°, séda@on, ven@la@on mécanique. – Le mannitol en bolus unique peut être proposé en situa@on immédiatement
menaçante.
• Lude contre les désordres hydro-‐électriques, la fièvre et l’hyperglycémie (ACSOS) : – Apports hydrosodés conven@onnels et surveillance natrémie et diurèse – Abaissement de la température si HIC sévère ou fièvre mal tolérée – Abaissement de la glycémie au dessous de 8,3 mmol/l après stabilisa@on de
l’hémodynamique d’un sepsis sévère de l’adulte par insuline IV – PCO2 entre 35 et 40 mmHg, oxygène correcte

QUESTION 4 A Vous recevez le résultat de la ponc@on lombaire : liquide trouble, 3500 éléments (98% PNN), protéinorachie=3g/l, glycorachie=0,1 mmol/l, ED : CGP diplocoques Recherche an@gène soluble pneumocoque (ou PCR) posi@ve. Modifiez-‐vous votre an@biothérapie ini@ale ?
Mr G. Pierre âgé de 62 ans
Ø NON Ø Car probable méningite à pneumocoque
-‐ Poursuite C3G : Cefotaxime 300mg/kg/j IVSE -‐ Poursuite dexaméthasone 10mg/6h pendant 4 jours

QUESTION 5A Quel est l’intérêt d’injecter des cor@coïdes avant ou même temps que les an@bio@ques dans la méningite à pneumocoque de l’adulte ? Ques@on 5B Vous voyez le pa@ent deux heures après l’injec@on d’an@bio@que, au retour du scanner. Il n’y a pas eu d’injec@on de cor@coïdes : que faites-‐vous ?
Mr G. Pierre âgé de 62 ans

Efficacité de la dexaméthasone
• DXM : – î Prod. cytokines pro
inflammatoires par monocytes, cellules dendri@ques, astrocytes, PN
– ì Prod. Cytokines an@-‐inflammatoires , IL-‐10
– Inhibe prod. ROS par les leucocytes
– î Adhérence leucocytaire – î Prod. TNF-‐α et IL-‐1 cellules
endothéliales microvasculaires et î expression ICAM-‐1 Modèle expérimental :
î TNF-α, lactate, NO î oedème cérébral et GB
B. Mook-Kanamori et al Clin Microbiol. Rev 2011,24:557

• Plan de l’étude • Randomisée
• 301 adultes avec méningite bactérienne
• Dexamethasone – 10 mg qid, 4j vs placebo
– Débutée avant ou lors de l’injection antibiotique • amoxicilline 2g x 6 (77 %)
• C3G injectable (8%)
The New England
Journal
of
Medicine
Copyr ight © 2002 by the Massachusett s Medical Society
VOLUME 347
N
OVEMBER
14, 2002
NUMBER 20
N Engl J Med, Vol. 347, No. 20
·
November 14, 2002
·
www.nejm.org
·
1549
DEXAMETHASONE IN ADULTS WITH BACTERIAL MENINGITIS
J
AN
DE
G
ANS
, P
H
.D.,
AND
D
IEDERIK
VAN
DE
B
EEK
, M.D.,
FOR
THE
E
UROPEAN
D
EXAMETHASONE
IN
A
DULTHOOD
B
ACTERIAL
M
ENINGITIS
S
TUDY
I
NVESTIGATORS
*
A
BSTRACT
Background
Mortality and morbidity rates are highamong adults with acute bacterial meningitis, espe-cially those with pneumococcal meningitis. In studiesof bacterial meningitis in animals, adjuvant treatmentwith corticosteroids has beneficial effects.
Methods
We conducted a prospective, randomized,double-blind, multicenter trial of adjuvant treatmentwith dexamethasone, as compared with placebo, inadults with acute bacterial meningitis. Dexametha-sone (10 mg) or placebo was administered 15 to 20minutes before or with the first dose of antibiotic andwas given every 6 hours for four days. The primaryoutcome measure was the score on the Glasgow Out-come Scale at eight weeks (a score of 5, indicating afavorable outcome, vs. a score of 1 to 4, indicating anunfavorable outcome). A subgroup analysis accordingto the causative organism was performed. Analyseswere performed on an intention-to-treat basis.
Results
A total of 301 patients were randomly as-signed to a treatment group: 157 to the dexametha-sone group and 144 to the placebo group. The base-line characteristics of the two groups were similar.Treatment with dexamethasone was associated witha reduction in the risk of an unfavorable outcome (rel-ative risk, 0.59; 95 percent confidence interval, 0.37 to0.94; P=0.03). Treatment with dexamethasone wasalso associated with a reduction in mortality (relativerisk of death, 0.48; 95 percent confidence interval, 0.24to 0.96; P=0.04). Among the patients with pneumo-coccal meningitis, there were unfavorable outcomesin 26 percent of the dexamethasone group, as com-pared with 52 percent of the placebo group (relativerisk, 0.50; 95 percent confidence interval, 0.30 to 0.83;P=0.006). Gastrointestinal bleeding occurred in twopatients in the dexamethasone group and in five pa-tients in the placebo group.
Conclusions
Early treatment with dexamethasoneimproves the outcome in adults with acute bacterialmeningitis and does not increase the risk of gastroin-testinal bleeding. (N Engl J Med 2002;347:1549-56.)
Copyright © 2002 Massachusetts Medical Society.
From the Department of Neurology, Academic Medical Center, Amster-dam. Address reprint requests to Dr. de Gans at the Academic Medical Cen-ter, University of Amsterdam, Department of Neurology H2, P.O. Box 22660,1100 DD Amsterdam, the Netherlands, or at [email protected].
*The investigators who participated in the European Dexamethasone inAdulthood Bacterial Meningitis Study are listed in the Appendix.
HE mortality rate among adults with acutebacterial meningitis and the frequency ofneurologic sequelae among those who sur-vive are high, especially among patients with
pneumococcal meningitis.
1,2
Unfavorable neurologicoutcomes are not the result of treatment with inappro-priate antimicrobial agents, since cerebrospinal fluidcultures are sterile 24 to 48 hours after the start of an-tibiotic therapy.
3
Studies in animals have shown thatbacterial lysis, induced by treatment with antibiotics,leads to inflammation in the subarachnoid space, whichmay contribute to an unfavorable outcome.
4,5
Thesestudies also show that adjuvant treatment with antiin-flammatory agents, such as dexamethasone, reducesboth cerebrospinal fluid inflammation and neurologicsequelae.
4,5
Many controlled trials have been performed to de-termine whether adjuvant corticosteroid therapy isbeneficial in children with acute bacterial meningitis.The results, however, do not point unequivocally to abeneficial effect. A meta-analysis of randomized con-trolled trials performed since 1988 showed a beneficialeffect of adjunctive dexamethasone therapy in terms ofsevere hearing loss in children with
Haemophilus influ-enzae
type b meningitis and suggested a protective ef-fect in those with pneumococcal meningitis if the drugwas given before or with parenteral antibiotics.
6
Thereare few data on the use of adjunctive dexamethasonetherapy in adults with bacterial meningitis. One large,prospective, randomized trial (neither placebo-con-trolled nor double-blind) showed a benefit of dex-amethasone therapy in a subgroup of patients withpneumococcal meningitis.
7
The paucity of data pre-cludes a recommendation that dexamethasone be ad-
T
The New England Journal of Medicine Downloaded from nejm.org on May 12, 2013. For personal use only. No other uses without permission.
Copyright © 2002 Massachusetts Medical Society. All rights reserved.
de Gans & van de Beek N Engl J Med 2002

de Gans & van de Beek N Engl J Med 2002
The New England
Journal
of
Medicine
Copyr ight © 2002 by the Massachusett s Medical Society
VOLUME 347
N
OVEMBER
14, 2002
NUMBER 20
N Engl J Med, Vol. 347, No. 20
·
November 14, 2002
·
www.nejm.org
·
1549
DEXAMETHASONE IN ADULTS WITH BACTERIAL MENINGITIS
J
AN
DE
G
ANS
, P
H
.D.,
AND
D
IEDERIK
VAN
DE
B
EEK
, M.D.,
FOR
THE
E
UROPEAN
D
EXAMETHASONE
IN
A
DULTHOOD
B
ACTERIAL
M
ENINGITIS
S
TUDY
I
NVESTIGATORS
*
A
BSTRACT
Background
Mortality and morbidity rates are highamong adults with acute bacterial meningitis, espe-cially those with pneumococcal meningitis. In studiesof bacterial meningitis in animals, adjuvant treatmentwith corticosteroids has beneficial effects.
Methods
We conducted a prospective, randomized,double-blind, multicenter trial of adjuvant treatmentwith dexamethasone, as compared with placebo, inadults with acute bacterial meningitis. Dexametha-sone (10 mg) or placebo was administered 15 to 20minutes before or with the first dose of antibiotic andwas given every 6 hours for four days. The primaryoutcome measure was the score on the Glasgow Out-come Scale at eight weeks (a score of 5, indicating afavorable outcome, vs. a score of 1 to 4, indicating anunfavorable outcome). A subgroup analysis accordingto the causative organism was performed. Analyseswere performed on an intention-to-treat basis.
Results
A total of 301 patients were randomly as-signed to a treatment group: 157 to the dexametha-sone group and 144 to the placebo group. The base-line characteristics of the two groups were similar.Treatment with dexamethasone was associated witha reduction in the risk of an unfavorable outcome (rel-ative risk, 0.59; 95 percent confidence interval, 0.37 to0.94; P=0.03). Treatment with dexamethasone wasalso associated with a reduction in mortality (relativerisk of death, 0.48; 95 percent confidence interval, 0.24to 0.96; P=0.04). Among the patients with pneumo-coccal meningitis, there were unfavorable outcomesin 26 percent of the dexamethasone group, as com-pared with 52 percent of the placebo group (relativerisk, 0.50; 95 percent confidence interval, 0.30 to 0.83;P=0.006). Gastrointestinal bleeding occurred in twopatients in the dexamethasone group and in five pa-tients in the placebo group.
Conclusions
Early treatment with dexamethasoneimproves the outcome in adults with acute bacterialmeningitis and does not increase the risk of gastroin-testinal bleeding. (N Engl J Med 2002;347:1549-56.)
Copyright © 2002 Massachusetts Medical Society.
From the Department of Neurology, Academic Medical Center, Amster-dam. Address reprint requests to Dr. de Gans at the Academic Medical Cen-ter, University of Amsterdam, Department of Neurology H2, P.O. Box 22660,1100 DD Amsterdam, the Netherlands, or at [email protected].
*The investigators who participated in the European Dexamethasone inAdulthood Bacterial Meningitis Study are listed in the Appendix.
HE mortality rate among adults with acutebacterial meningitis and the frequency ofneurologic sequelae among those who sur-vive are high, especially among patients with
pneumococcal meningitis.
1,2
Unfavorable neurologicoutcomes are not the result of treatment with inappro-priate antimicrobial agents, since cerebrospinal fluidcultures are sterile 24 to 48 hours after the start of an-tibiotic therapy.
3
Studies in animals have shown thatbacterial lysis, induced by treatment with antibiotics,leads to inflammation in the subarachnoid space, whichmay contribute to an unfavorable outcome.
4,5
Thesestudies also show that adjuvant treatment with antiin-flammatory agents, such as dexamethasone, reducesboth cerebrospinal fluid inflammation and neurologicsequelae.
4,5
Many controlled trials have been performed to de-termine whether adjuvant corticosteroid therapy isbeneficial in children with acute bacterial meningitis.The results, however, do not point unequivocally to abeneficial effect. A meta-analysis of randomized con-trolled trials performed since 1988 showed a beneficialeffect of adjunctive dexamethasone therapy in terms ofsevere hearing loss in children with
Haemophilus influ-enzae
type b meningitis and suggested a protective ef-fect in those with pneumococcal meningitis if the drugwas given before or with parenteral antibiotics.
6
Thereare few data on the use of adjunctive dexamethasonetherapy in adults with bacterial meningitis. One large,prospective, randomized trial (neither placebo-con-trolled nor double-blind) showed a benefit of dex-amethasone therapy in a subgroup of patients withpneumococcal meningitis.
7
The paucity of data pre-cludes a recommendation that dexamethasone be ad-
T
The New England Journal of Medicine Downloaded from nejm.org on May 12, 2013. For personal use only. No other uses without permission.
Copyright © 2002 Massachusetts Medical Society. All rights reserved.
The New England
Journal
of
Medicine
Copyr ight © 2002 by the Massachusett s Medical Society
VOLUME 347
N
OVEMBER
14, 2002
NUMBER 20
N Engl J Med, Vol. 347, No. 20
·
November 14, 2002
·
www.nejm.org
·
1549
DEXAMETHASONE IN ADULTS WITH BACTERIAL MENINGITIS
J
AN
DE
G
ANS
, P
H
.D.,
AND
D
IEDERIK
VAN
DE
B
EEK
, M.D.,
FOR
THE
E
UROPEAN
D
EXAMETHASONE
IN
A
DULTHOOD
B
ACTERIAL
M
ENINGITIS
S
TUDY
I
NVESTIGATORS
*
A
BSTRACT
Background
Mortality and morbidity rates are highamong adults with acute bacterial meningitis, espe-cially those with pneumococcal meningitis. In studiesof bacterial meningitis in animals, adjuvant treatmentwith corticosteroids has beneficial effects.
Methods
We conducted a prospective, randomized,double-blind, multicenter trial of adjuvant treatmentwith dexamethasone, as compared with placebo, inadults with acute bacterial meningitis. Dexametha-sone (10 mg) or placebo was administered 15 to 20minutes before or with the first dose of antibiotic andwas given every 6 hours for four days. The primaryoutcome measure was the score on the Glasgow Out-come Scale at eight weeks (a score of 5, indicating afavorable outcome, vs. a score of 1 to 4, indicating anunfavorable outcome). A subgroup analysis accordingto the causative organism was performed. Analyseswere performed on an intention-to-treat basis.
Results
A total of 301 patients were randomly as-signed to a treatment group: 157 to the dexametha-sone group and 144 to the placebo group. The base-line characteristics of the two groups were similar.Treatment with dexamethasone was associated witha reduction in the risk of an unfavorable outcome (rel-ative risk, 0.59; 95 percent confidence interval, 0.37 to0.94; P=0.03). Treatment with dexamethasone wasalso associated with a reduction in mortality (relativerisk of death, 0.48; 95 percent confidence interval, 0.24to 0.96; P=0.04). Among the patients with pneumo-coccal meningitis, there were unfavorable outcomesin 26 percent of the dexamethasone group, as com-pared with 52 percent of the placebo group (relativerisk, 0.50; 95 percent confidence interval, 0.30 to 0.83;P=0.006). Gastrointestinal bleeding occurred in twopatients in the dexamethasone group and in five pa-tients in the placebo group.
Conclusions
Early treatment with dexamethasoneimproves the outcome in adults with acute bacterialmeningitis and does not increase the risk of gastroin-testinal bleeding. (N Engl J Med 2002;347:1549-56.)
Copyright © 2002 Massachusetts Medical Society.
From the Department of Neurology, Academic Medical Center, Amster-dam. Address reprint requests to Dr. de Gans at the Academic Medical Cen-ter, University of Amsterdam, Department of Neurology H2, P.O. Box 22660,1100 DD Amsterdam, the Netherlands, or at [email protected].
*The investigators who participated in the European Dexamethasone inAdulthood Bacterial Meningitis Study are listed in the Appendix.
HE mortality rate among adults with acutebacterial meningitis and the frequency ofneurologic sequelae among those who sur-vive are high, especially among patients with
pneumococcal meningitis.
1,2
Unfavorable neurologicoutcomes are not the result of treatment with inappro-priate antimicrobial agents, since cerebrospinal fluidcultures are sterile 24 to 48 hours after the start of an-tibiotic therapy.
3
Studies in animals have shown thatbacterial lysis, induced by treatment with antibiotics,leads to inflammation in the subarachnoid space, whichmay contribute to an unfavorable outcome.
4,5
Thesestudies also show that adjuvant treatment with antiin-flammatory agents, such as dexamethasone, reducesboth cerebrospinal fluid inflammation and neurologicsequelae.
4,5
Many controlled trials have been performed to de-termine whether adjuvant corticosteroid therapy isbeneficial in children with acute bacterial meningitis.The results, however, do not point unequivocally to abeneficial effect. A meta-analysis of randomized con-trolled trials performed since 1988 showed a beneficialeffect of adjunctive dexamethasone therapy in terms ofsevere hearing loss in children with
Haemophilus influ-enzae
type b meningitis and suggested a protective ef-fect in those with pneumococcal meningitis if the drugwas given before or with parenteral antibiotics.
6
Thereare few data on the use of adjunctive dexamethasonetherapy in adults with bacterial meningitis. One large,prospective, randomized trial (neither placebo-con-trolled nor double-blind) showed a benefit of dex-amethasone therapy in a subgroup of patients withpneumococcal meningitis.
7
The paucity of data pre-cludes a recommendation that dexamethasone be ad-
T
The New England Journal of Medicine Downloaded from nejm.org on May 12, 2013. For personal use only. No other uses without permission.
Copyright © 2002 Massachusetts Medical Society. All rights reserved.

Pas d’intérêt de la dexaméthasone au cours de la méningite bactérienne au Malawi
• Double aveugle, randomisée • Déxaméthasone
– 16 mg 2x/j x4 jours
• + cekriaxone • Adultes
– 90% HIV + – Score de Glasgow moyen =10,4
+/-‐2,8
• Pneumocoque = 61 % – Cryptocoque 5%, – Pas de méningite bactérienne 8 %
• Mortalité globale = 54 %
Corticosteroids for Bacterial Meningitis in Sub-Sahar an Africa
n engl j med 357;24 www.nejm.org december 13, 2007 2447
at day 40 in the corticosteroid group becomes 1.09 (95% CI, 0.64 to 1.83).
The results of the intention-to-treat analysis and the predefined analyses for patients with proven and probable bacterial meningitis, proven bacte-rial meningitis, and pneumococcal meningitis in the corticosteroid trial are shown in Table 3. There were no differences in the rates of death, disability and death, or clinically detectable hearing loss at 40 days or in mortality at 10 days or at 6 months. Further exploratory analyses showed no evidence that corticosteroids were effective in any subgroup (Table S2 in the Supplementary Appendix). Pat-terns of hearing loss and of disability among sur-vivors are shown in Tables S3A and S3B in the Supplementary Appendix. As compared with pa-tients who received placebo, the temperatures of patients in the corticosteroid group were lower during treatment (mean difference, 0.49°C at day 4; P<0.001) (Fig. S1 in the Supplementary Appendix).
In the trial concerning the route of antibiotic administration, mortality at 40 days was 121 of 230 patients in the intravenous group (52.6%) and 128 of 229 patients in the intramuscular group (55.9%) (odds ratio, 0.88; 95% CI, 0.61 to 1.26) (Table 4). An on-treatment analysis, censoring events after premature discontinuation of ceftri-axone, shows a similar mortality of 119 of 225 patients in the intravenous group (52.9%) and 124 of 219 patients in the intramuscular group (56.6%). Given the actual 80% power of this study, a two-sided test excludes an increase or decrease in 40-day mortality in the intramuscular group of 25% and 24%, respectively. When an interaction term for the comparison of corticosteroid and pla-cebo administration is included, the odds ratio for mortality at 40 days in the intravenous group becomes 0.84 (95% CI, 0.5 to 1.14). In seven pa-tients, pain during intramuscular injection was sufficiently distressing for clinicians to switch to intravenous treatment. Only one isolate (S. pneu-moniae) showed reduced susceptibility to ceftriax-one (Table S4 in the Supplementary Appendix).
There were no differences in the rates of ad-verse events potentially related to corticosteroid therapy and none resulted in withdrawal of pa-tients from the trial (Table S5 in the Supplemen-tary Appendix). Nineteen patients had adverse events that were more likely to be due to antibi-otics than corticosteroids; nine patients had late fever (including seven patients in the corticoste-roid group), five had rash (including two in the
corticosteroid group), three had diarrhea (includ-ing one in the corticosteroid group), and two had jaundice (both of whom were in the corticosteroid group).
Discussion
The greatest burden of bacterial meningitis in adults occurs in developing countries where mor-tality rates are high. If effective, corticosteroids as adjuvant therapy would represent an affordable and appropriate intervention. The results of our study show that, in a setting where the majority of patients are likely to have advanced HIV infec-tion, where presentation tends to be late, and where S. pneumoniae is the predominant pathogen, adju-vant therapy with dexamethasone for bacterial meningitis in adults confers no advantage with re-gard to mortality or morbidity at 40 days.
In our study, mortality was substantially higher than in it is in industrialized settings, but it was typical for a low-resource setting in sub-Saharan Africa. It was lower than in previous studies in Malawi,3,5 probably due to the use of ceftriaxone (rather than penicillin plus chloramphenicol) and the effect of improved care as a result of the pa-tients’ inclusion in a clinical trial.
The negative findings from this study, pre-dominantly in patients with advanced HIV disease, contrast with those of a European trial of corti-costeroids involving 301 adults with meningitis.7 The European trial showed an overall reduction of mortality from 15% to 7% at 8 weeks (P=0.04), and the benefit of corticosteroids was most marked in patients with pneumococcal meningitis. The current findings are similar to those of a large
100
75
50
25
00 2010 30 40
Placebo
Corticosteroid
AUTHOR:
FIGURE:
JOB:
4-CH/T
RETAKEICM
CASE
EMail LineH/TCombo
Revised
REG F
Enon
1st2nd3rd
Scarborough
2 of 2
12-13-07
ARTIST: ts
35724 ISSUE:
22p3
Figure 2. Kaplan–Meier Estimates of Survival for 459 Patients through Day 40.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by CHRISTOPHE CAMUS MD on January 26, 2008 .
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;24 www.nejm.org december 13, 2007 2441
original article
Corticosteroids for Bacterial Meningitis in Adults in Sub-Saharan Africa
Matthew Scarborough, M.R.C.P., Stephen B. Gordon, M.D., Christopher J.M. Whitty, F.R.C.P., Neil French, Ph.D., Yasin Njalale, Dip.Med.Sci.,
Alex Chitani, Dip.Med.Sci., Timothy E.A. Peto, Ph.D., David G. Lalloo, F.R.C.P., and Eduard E. Zijlstra, Ph.D.
From the College of Medicine (M.S., S.B.G., C.J.M.W., N.F., Y.N., A.C., E.E.Z.) and the Malawi–Liverpool–Wellcome Pro-gramme of Clinical Tropical Research (S.B.G., N.F.) — both in Blantyre, Mala-wi; the Nuffield Department of Clinical Laboratory Science (M.S.) and the Nuf-field Department of Medicine (T.E.A.P.) — both at the University of Oxford, Oxford, United Kingdom; the Liverpool School of Tropical Medicine, Liverpool, United King-dom (M.S., S.B.G., N.F., D.G.L.); and the London School of Hygiene and Tropical Medicine, London (C.J.M.W.). Address re-print requests to Dr. Scarborough at the Nuffield Department of Clinical Labora-tory Science, John Radcliffe Hospital, Ox-ford OX3 9DU, United Kingdom, or at [email protected].
N Engl J Med 2007;357:2441-50.Copyright © 2007 Massachusetts Medical Society.
A bs tr ac t
BackgroundIn sub-Saharan Africa, bacterial meningitis is common and is associated with a high mortality. Adjuvant therapy with corticosteroids reduces mortality among adults in the developed world, but it has not been adequately tested in developing countries or in the context of advanced human immunodeficiency virus (HIV) infection.
Methods We conducted a randomized, double-blind, placebo-controlled trial of dexametha-sone (16 mg twice daily for 4 days) and an open-label trial of intramuscular versus in-travenous ceftriaxone (2 g twice daily for 10 days) in adults with an admission diag-nosis of bacterial meningitis in Blantyre, Malawi. The primary outcome was death at 40 days after randomization.
Results A total of 465 patients, 90% of whom were HIV-positive, were randomly assigned to receive dexamethasone (233 patients) or placebo (232 patients) plus intramuscular cef-triaxone (230 patients) or intravenous ceftriaxone (235 patients). There was no sig-nificant difference in mortality at 40 days in the corticosteroid group (129 of 231 patients) as compared with the placebo group (120 of 228 patients) by intention-to-treat analysis (odds ratio, 1.14; 95% confidence interval [CI], 0.79 to 1.64) or when the analysis was restricted to patients with proven pneumococcal meningitis (68 of 129 patients receiving corticosteroids vs. 72 of 143 patients receiving placebo) (odds ratio, 1.10; 95% CI, 0.68 to 1.77). There were no significant differences between groups in the outcomes of disability and death combined, hearing impairment, and adverse events. There was no difference in mortality with intravenous ceftriaxone (121 of 230 patients) as compared with intramuscular ceftriaxone (128 of 229 patients) (odds ratio, 0.88; 95% CI, 0.61 to 1.27).
Conclusions Adjuvant therapy with dexamethasone for bacterial meningitis in adults from an area with a high prevalence of HIV did not reduce mortality or morbidity. In this setting, intramuscular administration was not inferior to intravenous administra-tion of ceftriaxone for bacterial meningitis. (Current Controlled Trials number, ISRCTN31371499.)
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by CHRISTOPHE CAMUS MD on January 26, 2008 .
N. Engl. J Med 2007;357:2441

Efficacité de la déxaméthasone au cours de la méningite bactérienne au Vietnam
• Double aveugle, randomisée • > 14 ans • DXM : 0,4 mg/kg x 2/j X 4j • + CRO 2g x 2 x 10 à 14j • Évalua@on à 30 jours • Glasgow score médian 13 • HIV + 0,5 % • Pneumocoque 13 %
– S. Suis 26 % – S. aureus = 2%
• Mortalité globale 11 % (10,1% DXM versus 12,4% en ITT)
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;24 www.nejm.org december 13, 20072436
and 21 placebo) were treated with a combina-tion of ceftriaxone and vancomycin, and 26 pa-tients (11 receiving dexamethasone, and 15 pla-cebo) with a combination of ceftriaxone and rifampin. Of 55 S. pneumoniae isolates, 50 (90.9%) were susceptible to ceftriaxone (minimal inhibi-tory concentration [MIC], ≤0.5 µg per milliliter) and 5 (9.1%) had intermediate resistance to cef-triaxone (MIC, >0.5 to 1.0 µg per milliliter). The rest of the bacterial isolates, with the exception of Pseudomonas aeruginosa (in 1 patient), S. aureus (in 1), and Escherichia coli (in 1), were susceptible to cef-triaxone.
All but four patients were tested for HIV in-fection; only three were infected (Table 1). One of these three had tuberculous meningitis, one had cryptococcal meningitis, and one had S. pneu-moniae meningitis (the first two received dexa-methasone, and the third placebo).
Intention-to-Treat Analysis of Primary Outcome
Thirty days after randomization, 22 of the 217 patients in the dexamethasone group (10.1%) and 27 of the 218 patients in the placebo group (12.4%) had died (relative risk of death in the dexametha-sone group, 0.79; 95% confidence interval [CI], 0.45 to 1.39) (Fig. 2A). The study drug was with-drawn early in 10 patients in each group, in most cases because a diagnosis other than bacterial meningitis was made. Among these patients, all but one (who had received dexamethasone) sur-vived. The results of per-protocol analyses were similar to the results of intention-to-treat analy-ses for all primary and secondary outcomes.
Prespecified Subgroup AnalysisThe primary outcome was compared among sub-groups of patients defined according to the diag-nosis (definite bacterial meningitis, probable bac-terial meningitis, or a different diagnosis) (Table 2). There was significant heterogeneity of the treat-ment effect across these diagnostic groups, but
1.00
0.90
0.95
0.85
0.80
0.75
1.00
0.90
0.95
0.85
0.80
0.75
1.00
0.90
0.95
0.85
0.80
0.75
0.000 5 10 15 20 25 30
Placebo
Placebo
Dexamethasone
Dexamethasone
Dexamethasone
Placebo
P=0.42
0.000 5 10 15 20 25 30
P=0.03
DexamethasonePlacebo
217218
DexamethasonePlacebo
143157
210204
140146
208200
138143
202196
136142
201196
136142
200192
135139
199192
135139
0.000 5 10 15 20 25 30
P=0.14
DexamethasonePlacebo
6954
6552
6551
6149
6149
6049
6049
AUTHOR:
FIGURE:
JOB:
4-CH/T
RETAKEICM
CASE
EMail LineH/TCombo
Revised
REG F
Enon
1st2nd3rd
Mai (Farrar)
2 of 2
12-13-07
ARTIST: ts
35724 ISSUE:
22p3
Figure 2. Kaplan–Meier Survival Estimates According to Study Group.
Panel A shows survival estimates for all patients who underwent randomization (intention-to-treat analysis). Panel B shows survival estimates for patients with def-inite bacterial meningitis, and Panel C estimates for patients with probable bacterial meningitis. P values are based on the log-rank test.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by CHRISTOPHE CAMUS MD on January 26, 2008 .
n engl j med 357;24 www.nejm.org december 13, 2007 2431
The new england journal of medicineestablished in 1812 december 13, 2007 vol. 357 no. 24
Dexamethasone in Vietnamese Adolescents and Adults with Bacterial Meningitis
Nguyen Thi Hoang Mai, M.D., Tran Thi Hong Chau, M.D., Guy Thwaites, M.D., Ly Van Chuong, M.D., Dinh Xuan Sinh, M.D., Ho Dang Trung Nghia, M.D., Phung Quoc Tuan, M.D., Nguyen Duy Phong, M.D., Nguyen Hoan Phu, M.D., To Song Diep, M.D., Nguyen van Vinh Chau, M.D., Nguyen Minh Duong, M.D.,
James Campbell, Constance Schultsz, M.D., Chris Parry, M.D., M. Estee Torok, M.D., Nicholas White, F.R.C.P., Nguyen Tran Chinh, M.D., Tran Tinh Hien, M.D., Kasia Stepniewska, Ph.D., and Jeremy J. Farrar, F.R.C.P.
A bs tr ac t
From the Hospital for Tropical Diseas- es (N.T.H.M., T.T.H.C., L.V.C., D.X.S., H.D.T.N., N.H.P., T.S.D., N.V.C., N.M.D., N.T.C., T.T.H.); Oxford University Clinical Research Unit, Hospital for Tropical Dis-eases (G.T., P.Q.T., J.C., C.S., C.P., M.E.T., K.S., J.J.F.); and the University of Medi-cine and Pharmacy (N.D.P., N.W.) — all in Ho Chi Minh City, Vietnam; and the De-partment of Infectious Disease, Imperial College, London (G.T.); the Nuffield De-partment of Clinical Medicine, John Rad-cliffe Hospital, Oxford (C.S., M.E.T., K.S., J.J.F.); and the Department of Medical Microbiology, University of Liverpool, Liver-pool (C.P.) — all in the United Kingdom. Address reprint requests to Dr. Farrar at the Oxford University Clinical Research Unit, Hospital for Tropical Diseases, 190 Ben Ham Tu, Quan 5, Ho Chi Minh City, Vietnam, or at [email protected].
N Engl J Med 2007;357:2431-40.Copyright © 2007 Massachusetts Medical Society.
BackgroundIt is uncertain whether all adults with bacterial meningitis benefit from treatment with adjunctive dexamethasone.
MethodsWe conducted a randomized, double-blind, placebo-controlled trial of dexametha-sone in 435 patients over the age of 14 years who had suspected bacterial meningi-tis. The goal was to determine whether dexamethasone reduced the risk of death at 1 month and the risk of death or disability at 6 months.
ResultsA total of 217 patients were assigned to the dexamethasone group, and 218 to the placebo group. Bacterial meningitis was confirmed in 300 patients (69.0%), prob-able meningitis was diagnosed in 123 patients (28.3%), and an alternative diagno-sis was made in 12 patients (2.8%). An intention-to-treat analysis of all the patients showed that dexamethasone was not associated with a significant reduction in the risk of death at 1 month (relative risk, 0.79; 95% confidence interval [CI], 0.45 to 1.39) or the risk of death or disability at 6 months (odds ratio, 0.74; 95% CI, 0.47 to 1.17). In patients with confirmed bacterial meningitis, however, there was a signifi-cant reduction in the risk of death at 1 month (relative risk, 0.43; 95% CI, 0.20 to 0.94) and in the risk of death or disability at 6 months (odds ratio, 0.56; 95% CI, 0.32 to 0.98). These effects were not found in patients with probable bacterial men-ingitis. Results of multivariate analysis indicated that dexamethasone treatment for patients with probable bacterial meningitis was significantly associated with an increased risk of death at 1 month, an observation that may be explained by cases of tuberculous meningitis in the treatment group.
ConclusionsDexamethasone does not improve the outcome in all adolescents and adults with suspected bacterial meningitis; a beneficial effect appears to be confined to patients with microbiologically proven disease, including those who have received prior treat-ment with antibiotics. (Current Controlled Trials number, ISRCTN42986828.)
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by CHRISTOPHE CAMUS MD on January 26, 2008 .
n engl j med 357;24 www.nejm.org december 13, 2007 2431
The new england journal of medicineestablished in 1812 december 13, 2007 vol. 357 no. 24
Dexamethasone in Vietnamese Adolescents and Adults with Bacterial Meningitis
Nguyen Thi Hoang Mai, M.D., Tran Thi Hong Chau, M.D., Guy Thwaites, M.D., Ly Van Chuong, M.D., Dinh Xuan Sinh, M.D., Ho Dang Trung Nghia, M.D., Phung Quoc Tuan, M.D., Nguyen Duy Phong, M.D., Nguyen Hoan Phu, M.D., To Song Diep, M.D., Nguyen van Vinh Chau, M.D., Nguyen Minh Duong, M.D.,
James Campbell, Constance Schultsz, M.D., Chris Parry, M.D., M. Estee Torok, M.D., Nicholas White, F.R.C.P., Nguyen Tran Chinh, M.D., Tran Tinh Hien, M.D., Kasia Stepniewska, Ph.D., and Jeremy J. Farrar, F.R.C.P.
A bs tr ac t
From the Hospital for Tropical Diseas- es (N.T.H.M., T.T.H.C., L.V.C., D.X.S., H.D.T.N., N.H.P., T.S.D., N.V.C., N.M.D., N.T.C., T.T.H.); Oxford University Clinical Research Unit, Hospital for Tropical Dis-eases (G.T., P.Q.T., J.C., C.S., C.P., M.E.T., K.S., J.J.F.); and the University of Medi-cine and Pharmacy (N.D.P., N.W.) — all in Ho Chi Minh City, Vietnam; and the De-partment of Infectious Disease, Imperial College, London (G.T.); the Nuffield De-partment of Clinical Medicine, John Rad-cliffe Hospital, Oxford (C.S., M.E.T., K.S., J.J.F.); and the Department of Medical Microbiology, University of Liverpool, Liver-pool (C.P.) — all in the United Kingdom. Address reprint requests to Dr. Farrar at the Oxford University Clinical Research Unit, Hospital for Tropical Diseases, 190 Ben Ham Tu, Quan 5, Ho Chi Minh City, Vietnam, or at [email protected].
N Engl J Med 2007;357:2431-40.Copyright © 2007 Massachusetts Medical Society.
BackgroundIt is uncertain whether all adults with bacterial meningitis benefit from treatment with adjunctive dexamethasone.
MethodsWe conducted a randomized, double-blind, placebo-controlled trial of dexametha-sone in 435 patients over the age of 14 years who had suspected bacterial meningi-tis. The goal was to determine whether dexamethasone reduced the risk of death at 1 month and the risk of death or disability at 6 months.
ResultsA total of 217 patients were assigned to the dexamethasone group, and 218 to the placebo group. Bacterial meningitis was confirmed in 300 patients (69.0%), prob-able meningitis was diagnosed in 123 patients (28.3%), and an alternative diagno-sis was made in 12 patients (2.8%). An intention-to-treat analysis of all the patients showed that dexamethasone was not associated with a significant reduction in the risk of death at 1 month (relative risk, 0.79; 95% confidence interval [CI], 0.45 to 1.39) or the risk of death or disability at 6 months (odds ratio, 0.74; 95% CI, 0.47 to 1.17). In patients with confirmed bacterial meningitis, however, there was a signifi-cant reduction in the risk of death at 1 month (relative risk, 0.43; 95% CI, 0.20 to 0.94) and in the risk of death or disability at 6 months (odds ratio, 0.56; 95% CI, 0.32 to 0.98). These effects were not found in patients with probable bacterial men-ingitis. Results of multivariate analysis indicated that dexamethasone treatment for patients with probable bacterial meningitis was significantly associated with an increased risk of death at 1 month, an observation that may be explained by cases of tuberculous meningitis in the treatment group.
ConclusionsDexamethasone does not improve the outcome in all adolescents and adults with suspected bacterial meningitis; a beneficial effect appears to be confined to patients with microbiologically proven disease, including those who have received prior treat-ment with antibiotics. (Current Controlled Trials number, ISRCTN42986828.)
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by CHRISTOPHE CAMUS MD on January 26, 2008 .

Ne pas remedre en cause les recommanda@on de la conférence de consensus 2008, mais
Données pharmacocinétiques modèle lapin CS î CRO pénétration dans les méninges
Paris MM et al . AAC 1994; 38: 1320-4
Augmentation des lésions neuronales hippocampe par DXM Modèle rat NN + Altération des fonctions cognitives, mais non retrouvées chez l’adolescent, adulte, enfant
dexamethasone in patients with bacterial meningitis, thisprompted us to study the effect of the drug in our model ofpneumococcal meningitis in infant rats. Specifically, we exam-ined whether dexamethasone influenced apoptotic injury in thedentate gyrus and whether this was associated with an effect onlearning capacity after recovery from acute meningitis.
MATERIALS AND METHODS
Model of meningitis. The animal studies were approved bythe Animal Care and Experimentation Committee of the Can-ton of Bern, Switzerland, and followed National Institutes ofHealth guidelines for the performance of animal experiments.Nursing Sprague-Dawley rat pups were infected on postnatalday 11 (n ! 142) by intracisternal injection with 10 !L ofsaline containing an inoculum of log10 6.5 " 0.6 cfu/mLStreptococcus pneumoniae (17, 19, 24, 25). Uninfected ani-mals (n ! 62) were injected intracisternally with 10 !L ofsterile, pyrogen free saline. At 18 h after infection, animalswere weighed and assessed clinically. To document meningitis,10 !L of cerebrospinal fluid was obtained by puncture of thecisterna magna and cultured quantitatively.Treatment. All infected animals (n ! 142) received antibi-
otic treatment (ceftriaxone 100 mg/kg s.c. bid; Roche Pharma,Reinach, Switzerland) following CSF collection at 18 h. An-tibiotic treatment was continued for 2 doses in infected animalssubsequently examined histopathologically (n ! 38) and for5 d in animals subjected to learning testing (n ! 104). Animalsto be assessed histopathologically (n ! 38 for meningitis; n !14 for uninfected controls) were randomized for treatment withdexamethasone (0.7 mg/kg s.c. q8h from 18 to 34 h afterinfection; n ! 16 for meningitis; n ! 8 for controls) or vehicle(n ! 22 for meningitis; n ! 6 for controls). Animals to beassessed for learning performance were randomized for treat-ment with dexamethasone (0.7 mg/kg s.c. q8h for 4 d; n ! 34)or vehicle (n ! 70) concomitant with the first antibiotic dose.Data presented here combine two separate experiments usingthe same protocol. In the first trial, normal saline was admin-istered as vehicle to control animals (infected controls, n ! 31;uninfected controls, n ! 31). In the second trial, control
animals received PBS containing 1% Tween 80 (0.2 mL s.c.)as vehicle (infected controls, n ! 52; uninfected controls, n !32) because in this trial another drug was tested concomitantlywith dexamethasone, which had to be dissolved in PBS/Tween(17). Treatment with NaCl versus PBS/Tween did not result insignificant differences in hippocampal histopathology or learn-ing performance either in uninfected or in infected controlanimals. However, for both the infected and uninfected controlgroup, animals treated with NaCl or PBS/Tween had to becombined to make the differences between the three treatments(uninfected; infected vehicle treated; infecteddexamethasone treated) statistically significant.Effect of treatment on bacterial killing in CSF. In eleven
infected animals (dexamethasone, n ! 5; PBS/Tween, n ! 6)repeated cisternal punctures were performed at 18, 22, and 30 hpost-infection. CSF bacterial titers were determined quantita-tively by serial dilution to assess the influence of dexametha-sone therapy on the decline of bacterial titers in CSF followinginitiation of antibiotic therapy.Histopathology. At 34 h post-inoculation, infected animals
treated with dexamethasone (n ! 10), uninfected animalstreated with dexamethasone (n ! 8) and infected (n ! 19) anduninfected controls (n ! 6) were killed with an overdose ofpentobarbital. Animals dying spontaneously before 34 h (n !9) were not evaluated. Immediately after euthanasia, animalswere perfused via the left ventricle with 15 mL of 4% para-formaldehyde in PBS (pH 7.4). Brains were removed, post-fixed and snap-frozen at #60°C in methylbuthane and cut at45–60 !m intervals on a cryotome to obtain four coronalsections of the hippocampal region. Sections were mounted ongelatinized glass slides for staining. After dehydration, sectionswere Nissl stained with cresyl violet and coverslips were fixedwith Entellan® (Merck, Darmstadt, Germany). Neuronal in-jury in the dentate gyrus was evaluated as described previously(24). Apoptosis in the granule cell layer of the hippocampus,defined as cells showing markedly shrunken, condensed orfragmented nuclei (Fig. 1) was counted at 400x in 3 visualfields for each of the four blades of the dentate gyrus. Anaverage per dentate gyrus (six visual fields) per animal was
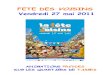
Figure 1. Hippocampal dentate gyrus histology of infant rats suffering from pneumococcal meningitis at 34 h after infection. A) In the dentate gyrus ofuninfected controls physiologic occurrence of neuronal apoptosis is sporadically visible by the formation of condensed and fragmented nuclei (arrowhead). B)In infected vehicle treated rats formation of apoptotic bodies is characteristically observed in the inner rim of the dentate gyrus (arrowheads) at 34 h afterinfection. C) Treatment with dexamethasone markedly increased the occurrence of apoptotic bodies (arrowheads) in the hippocampal dentate gyrus. Cresyl violet;original magnification $ 300; bar 50 !m.
354 LEIB ET AL.
dexamethasone in patients with bacterial meningitis, thisprompted us to study the effect of the drug in our model ofpneumococcal meningitis in infant rats. Specifically, we exam-ined whether dexamethasone influenced apoptotic injury in thedentate gyrus and whether this was associated with an effect onlearning capacity after recovery from acute meningitis.
MATERIALS AND METHODS
Model of meningitis. The animal studies were approved bythe Animal Care and Experimentation Committee of the Can-ton of Bern, Switzerland, and followed National Institutes ofHealth guidelines for the performance of animal experiments.Nursing Sprague-Dawley rat pups were infected on postnatalday 11 (n ! 142) by intracisternal injection with 10 !L ofsaline containing an inoculum of log10 6.5 " 0.6 cfu/mLStreptococcus pneumoniae (17, 19, 24, 25). Uninfected ani-mals (n ! 62) were injected intracisternally with 10 !L ofsterile, pyrogen free saline. At 18 h after infection, animalswere weighed and assessed clinically. To document meningitis,10 !L of cerebrospinal fluid was obtained by puncture of thecisterna magna and cultured quantitatively.Treatment. All infected animals (n ! 142) received antibi-
otic treatment (ceftriaxone 100 mg/kg s.c. bid; Roche Pharma,Reinach, Switzerland) following CSF collection at 18 h. An-tibiotic treatment was continued for 2 doses in infected animalssubsequently examined histopathologically (n ! 38) and for5 d in animals subjected to learning testing (n ! 104). Animalsto be assessed histopathologically (n ! 38 for meningitis; n !14 for uninfected controls) were randomized for treatment withdexamethasone (0.7 mg/kg s.c. q8h from 18 to 34 h afterinfection; n ! 16 for meningitis; n ! 8 for controls) or vehicle(n ! 22 for meningitis; n ! 6 for controls). Animals to beassessed for learning performance were randomized for treat-ment with dexamethasone (0.7 mg/kg s.c. q8h for 4 d; n ! 34)or vehicle (n ! 70) concomitant with the first antibiotic dose.Data presented here combine two separate experiments usingthe same protocol. In the first trial, normal saline was admin-istered as vehicle to control animals (infected controls, n ! 31;uninfected controls, n ! 31). In the second trial, control
animals received PBS containing 1% Tween 80 (0.2 mL s.c.)as vehicle (infected controls, n ! 52; uninfected controls, n !32) because in this trial another drug was tested concomitantlywith dexamethasone, which had to be dissolved in PBS/Tween(17). Treatment with NaCl versus PBS/Tween did not result insignificant differences in hippocampal histopathology or learn-ing performance either in uninfected or in infected controlanimals. However, for both the infected and uninfected controlgroup, animals treated with NaCl or PBS/Tween had to becombined to make the differences between the three treatments(uninfected; infected vehicle treated; infecteddexamethasone treated) statistically significant.Effect of treatment on bacterial killing in CSF. In eleven
infected animals (dexamethasone, n ! 5; PBS/Tween, n ! 6)repeated cisternal punctures were performed at 18, 22, and 30 hpost-infection. CSF bacterial titers were determined quantita-tively by serial dilution to assess the influence of dexametha-sone therapy on the decline of bacterial titers in CSF followinginitiation of antibiotic therapy.Histopathology. At 34 h post-inoculation, infected animals
treated with dexamethasone (n ! 10), uninfected animalstreated with dexamethasone (n ! 8) and infected (n ! 19) anduninfected controls (n ! 6) were killed with an overdose ofpentobarbital. Animals dying spontaneously before 34 h (n !9) were not evaluated. Immediately after euthanasia, animalswere perfused via the left ventricle with 15 mL of 4% para-formaldehyde in PBS (pH 7.4). Brains were removed, post-fixed and snap-frozen at #60°C in methylbuthane and cut at45–60 !m intervals on a cryotome to obtain four coronalsections of the hippocampal region. Sections were mounted ongelatinized glass slides for staining. After dehydration, sectionswere Nissl stained with cresyl violet and coverslips were fixedwith Entellan® (Merck, Darmstadt, Germany). Neuronal in-jury in the dentate gyrus was evaluated as described previously(24). Apoptosis in the granule cell layer of the hippocampus,defined as cells showing markedly shrunken, condensed orfragmented nuclei (Fig. 1) was counted at 400x in 3 visualfields for each of the four blades of the dentate gyrus. Anaverage per dentate gyrus (six visual fields) per animal was
Figure 1. Hippocampal dentate gyrus histology of infant rats suffering from pneumococcal meningitis at 34 h after infection. A) In the dentate gyrus ofuninfected controls physiologic occurrence of neuronal apoptosis is sporadically visible by the formation of condensed and fragmented nuclei (arrowhead). B)In infected vehicle treated rats formation of apoptotic bodies is characteristically observed in the inner rim of the dentate gyrus (arrowheads) at 34 h afterinfection. C) Treatment with dexamethasone markedly increased the occurrence of apoptotic bodies (arrowheads) in the hippocampal dentate gyrus. Cresyl violet;original magnification $ 300; bar 50 !m.
354 LEIB ET AL.
dexamethasone in patients with bacterial meningitis, thisprompted us to study the effect of the drug in our model ofpneumococcal meningitis in infant rats. Specifically, we exam-ined whether dexamethasone influenced apoptotic injury in thedentate gyrus and whether this was associated with an effect onlearning capacity after recovery from acute meningitis.
MATERIALS AND METHODS
Model of meningitis. The animal studies were approved bythe Animal Care and Experimentation Committee of the Can-ton of Bern, Switzerland, and followed National Institutes ofHealth guidelines for the performance of animal experiments.Nursing Sprague-Dawley rat pups were infected on postnatalday 11 (n ! 142) by intracisternal injection with 10 !L ofsaline containing an inoculum of log10 6.5 " 0.6 cfu/mLStreptococcus pneumoniae (17, 19, 24, 25). Uninfected ani-mals (n ! 62) were injected intracisternally with 10 !L ofsterile, pyrogen free saline. At 18 h after infection, animalswere weighed and assessed clinically. To document meningitis,10 !L of cerebrospinal fluid was obtained by puncture of thecisterna magna and cultured quantitatively.Treatment. All infected animals (n ! 142) received antibi-
otic treatment (ceftriaxone 100 mg/kg s.c. bid; Roche Pharma,Reinach, Switzerland) following CSF collection at 18 h. An-tibiotic treatment was continued for 2 doses in infected animalssubsequently examined histopathologically (n ! 38) and for5 d in animals subjected to learning testing (n ! 104). Animalsto be assessed histopathologically (n ! 38 for meningitis; n !14 for uninfected controls) were randomized for treatment withdexamethasone (0.7 mg/kg s.c. q8h from 18 to 34 h afterinfection; n ! 16 for meningitis; n ! 8 for controls) or vehicle(n ! 22 for meningitis; n ! 6 for controls). Animals to beassessed for learning performance were randomized for treat-ment with dexamethasone (0.7 mg/kg s.c. q8h for 4 d; n ! 34)or vehicle (n ! 70) concomitant with the first antibiotic dose.Data presented here combine two separate experiments usingthe same protocol. In the first trial, normal saline was admin-istered as vehicle to control animals (infected controls, n ! 31;uninfected controls, n ! 31). In the second trial, control
animals received PBS containing 1% Tween 80 (0.2 mL s.c.)as vehicle (infected controls, n ! 52; uninfected controls, n !32) because in this trial another drug was tested concomitantlywith dexamethasone, which had to be dissolved in PBS/Tween(17). Treatment with NaCl versus PBS/Tween did not result insignificant differences in hippocampal histopathology or learn-ing performance either in uninfected or in infected controlanimals. However, for both the infected and uninfected controlgroup, animals treated with NaCl or PBS/Tween had to becombined to make the differences between the three treatments(uninfected; infected vehicle treated; infecteddexamethasone treated) statistically significant.Effect of treatment on bacterial killing in CSF. In eleven
infected animals (dexamethasone, n ! 5; PBS/Tween, n ! 6)repeated cisternal punctures were performed at 18, 22, and 30 hpost-infection. CSF bacterial titers were determined quantita-tively by serial dilution to assess the influence of dexametha-sone therapy on the decline of bacterial titers in CSF followinginitiation of antibiotic therapy.Histopathology. At 34 h post-inoculation, infected animals
treated with dexamethasone (n ! 10), uninfected animalstreated with dexamethasone (n ! 8) and infected (n ! 19) anduninfected controls (n ! 6) were killed with an overdose ofpentobarbital. Animals dying spontaneously before 34 h (n !9) were not evaluated. Immediately after euthanasia, animalswere perfused via the left ventricle with 15 mL of 4% para-formaldehyde in PBS (pH 7.4). Brains were removed, post-fixed and snap-frozen at #60°C in methylbuthane and cut at45–60 !m intervals on a cryotome to obtain four coronalsections of the hippocampal region. Sections were mounted ongelatinized glass slides for staining. After dehydration, sectionswere Nissl stained with cresyl violet and coverslips were fixedwith Entellan® (Merck, Darmstadt, Germany). Neuronal in-jury in the dentate gyrus was evaluated as described previously(24). Apoptosis in the granule cell layer of the hippocampus,defined as cells showing markedly shrunken, condensed orfragmented nuclei (Fig. 1) was counted at 400x in 3 visualfields for each of the four blades of the dentate gyrus. Anaverage per dentate gyrus (six visual fields) per animal was
Figure 1. Hippocampal dentate gyrus histology of infant rats suffering from pneumococcal meningitis at 34 h after infection. A) In the dentate gyrus ofuninfected controls physiologic occurrence of neuronal apoptosis is sporadically visible by the formation of condensed and fragmented nuclei (arrowhead). B)In infected vehicle treated rats formation of apoptotic bodies is characteristically observed in the inner rim of the dentate gyrus (arrowheads) at 34 h afterinfection. C) Treatment with dexamethasone markedly increased the occurrence of apoptotic bodies (arrowheads) in the hippocampal dentate gyrus. Cresyl violet;original magnification $ 300; bar 50 !m.
354 LEIB ET AL.
Méningite PC
Méningite PC + DXM Leib S. Pediatric research 2003 ; 54:353-57

Résultats de la méta-analyse 2007 DXM et MB chez l’enfant
Devenir Nb. études
Nb. sujets
RR CI 95%
Mortalité globale 15 2074 0,99 [0.81 ; 1.20]
Surdité sévère 13 1383 0.61 [0.44 ; 0.86] Surdité sévère / Hib 9 663 0.37 [0.20 ; 0.68]
Surdité sévère / autres germes
11 660 0.86 [0.57 ; 1.30]
Surdité sévère / autres germes Malawi exclu
10 0.42 [0.20 ; 0.89]
van de Beek D et al. Cochrane Library 2007

Dexaméthasone et méningite bactérienne
Suspected or proven community-‐acquired bacterial meningi@s: 1. Dexamethasone 10 mg IV before or with first dose of an@bio@c 2. Low dose or no steroids if:
– Sep@c shock 3. No dexamethasone if:
– Pre-‐treatment with parenteral an@bio@cs – HIV-‐posi@ve or low-‐income countries – Recent head injury – CSF shunt
4. 4 day treatment – 40 mg/day
5. No dexamethasone if not HIB or pneumococcus méningi@s
van de Beek et al N Engl J Med 2006

« Timing » déxaméthasone
• 20 minutes avant ou en même temps que an@bio@ques
• Pneumocoque – Effet « protecteur » maintenu au cours de l’expérimenta@on de l’animal si administrée 1 hr après celle de l’an@bio@que
Aucune donnée chez l’adolescent, adulte

• Mis sous déxaméthasone avant l’injec@on an@bio@que
• Pneumocoque, – CMI à la pénicilline < 0,1 mmol/l :
• Switch amoxicilline 16 g IVSE /24hr + poursuite déxaméthasone 4 jours – Dosage amoxicilline ?
• Extuba@on J4 • Reste confus avec des périodes d’agita@on
– Glasgow 13, pas de signe de défaillance hémodynamique
Mr G. Pierre âgé de 62 ans

QUESTION 6 Malgré votre an@biothérapie, l’évolu@on est marquée par une aggrava@on de l’état neurologique au 7ème jour avec mise en évidence d’un état de mal épilep@que traité par Thiopental. Quelles complica@ons craignez-‐vous ? Comment les recherchez-‐vous ?
Ø Empyème, Ø vascularite cérébrale Ø Hydrocéphalie Ø Encéphalopathie Bétalactamine, métabolique
Mr G. Pierre âgé de 62 ans
Ø Réalisa@on d’une IRM cérébrale Ø +/-‐ Contrôle du LCR

Mr G. Pierre âgé de 62 ans

Mr Pierre – C.R. IRM
• présence de modifica@ons de signal en diffusion en faveur d’une adeinte ischémique récente, images compa@bles avec une vascularite infec@euse.
Conduite à tenir ?

• Mul@ples lésions évocatrices de vascularite,
• diffuse mais prédominantes en territoire cérébral moyen droite,
• comprenant des ischémies récentes
Michèle 49 ans – vascularite au cours d’une méningite à pneumocoque

Mr Pierre G.. Evolu@on J9 – J23 • Traitement
– Céfotaxime = 16g IV SE 5adeinte infec@euse ou post-‐infec@euse ?) – + cor@cothérapie 3 bolus de 500 mg puis 1 mg/kg pendant 15 jours et
diminu@on progressive
• Evolu@on clinique à J 7 (cor@sone) – conscience normale, – Mais persistance d’une légère altéra@on du fonc@onnement cogni@f
global
• La ponc@on lombaire à J7 : – 230 éléments nucléés/mm3 dont 99 % de lymphocytes, – glycorachie et protéinorachie sont normales
• Soins de suite et rééduca@on à J14

Vascularite et méningite à pneumocoque
• Très peu de papiers • Au cours de la méningite à pneumocoque
– 5-‐ 25 % infarctus cérébral* – 9% Thromboses veineuses – 9 % hémorragies cérébrales
• La vascularite – Autopsie : infiltrats inflammatoires des obstruc@on des artérioles et
veines cérébrales – Angio IRM : rétrécissement artériels, grêles – Quel est l’effet de la dexaméthasone ?
• Rare appari@on secondaire de l’expression de la vascularite
larite devant des sténoses artérielles multiples à l’artériogra-phie est une question délicate qui se pose fréquemment enpratique neurovasculaire. Si les données cliniques et paraclini-ques complémentaires ne permettent pas de trancher formel-lement, il faut alors envisager de répéter l’artériographie,l’évolutivité des lésions plaidant plutôt en faveur du diagnosticd’angéite, alors que les lésions athéromateuses sont fixées etstables dans le temps.
Examens de laboratoiresÀ ce jour, il n’existe aucun examen biologique spécifique devascularite cérébrale. Néanmoins, un bilan biologique de pre-mière intention est indispensable face à une suspicion de vas-cularite cérébrale et en l’absence d’éléments d’orientation(encadre 1). Ce bilan comprend une numération formule san-guine, un bilan d’hémostase, un ionogramme avec créatinine,une VS, une C-reactive protein (CRP), une électrophorèse desprotéines et un bilan hépatique. Le syndrome inflammatoireest inconstant et peut être absent. Une lymphopénie(CD4 notamment) doit être systématiquement cherchée, notam-ment lorsqu’une cause infectieuse opportuniste est suspectée.
D’autres examens sont effectués à la recherche de maladiesinflammatoires chroniques (connectivites, vascularites systé-miques), de maladies infectieuses, malignes et toxiques, quidoivent être écartées.Le bilan auto-immun de base comprend la recherche desanticorps antinucléaires (AAN), des anticorps anti-antigènesnucléaires solubles, des anticorps anti-DNA natifs, particulière-ment si le contexte évoque une connectivite. La recherched’anticorps anti-cytoplasme des polynucléaires neutrophiles(ANCA) est indispensable pour documenter une éventuellevascularite systémique associée aux ANCA. L’activité du facteurrhumatoïde est également explorée en première intention pourdépister un rhumatisme inflammatoire (polyarthrite rhuma-toïde, syndrome de Gougerot-Sjögren). Les explorationsimmunologiques doivent également comporter une recherched’anticorps antiphospholipides, de cryoglobulines, une analyse
1075
Miseau
point
Figure 4Artériographie cérébrale d’une patiente de 56 ans atteinte d’unevascularite cérébrale primitive, vue sagitale : multiples sténoses(flèches noires) des principales branches de division du polygonede Willis dont l’artère cérébrale antérieure droite
Encadre 1Bilan biologique minimal de première intention à effectuerdevant une suspicion de vascularite cérébrale et en l’absenced’élements d’orientation (liste non exhaustive établie par lesauteurs)
Biologie usuelle :! NFP, ionogramme sanguin, calcémie ;
! bilan hépatique ;
! CRP, électrophorèse des protéines plasmatiques ;
! TP, TCA, fibrinogène.Analyse urinaire :! protéinurie des 24 h.Bilan immunologique :
! FAN (avec anticorps anti-ADN et anti-antigènes nucléaires
solubles si positifs), ANCA, FR, ECA, anticorps anticardiolipine/
antiphospholipides ;
! complément (C3, C4, CH50), cryoglobulinémie.LCR :
! cytologie, biochimie et bactériologie ;
! PCR HSV, VZV ;
! recherche de bandes oligoclonales.Bilan infectieux :
! sérologies : VIH, Herpes virus (CMV, EBV, HSV, VZV), VHB, VHC,
VDRL-TPHA, Lyme ;
! hémocultures, ECBU ;
! IDR " Quantiferon.TP : taux de prothrombine ; TCA : temps de céphaline activée ; FAN :facteurs antinucléaires ; ANCA : anticorps anti-cytoplasme despolynucléaires neurtrophiles ; FR : facteur rhumatoïde ; ECA :enzyme de conversion de l’angiotensine ; IDR : intradermoréaction.‘
Vascularites cérébralesMedecine vasculaire/Medecine interne/Neurologie
tome 41 > n811 > novembre 2012
*Pfister et al, Durand et al. Dodge and scartz, Arditi et al

Vascularite et méningites bactériennes
• Méningites « purulente » – Pneumocoque, Méningocoque, Hemophilus influenzae
• Méningites « à liquide clair » – Tuberculose – Syphilis – Lyme – Bartonellose, rickedsiose, leptospirose, Whipple
• Endocardite bactérienne

Complica@ons cérébrales secondaires méningite bactérienne
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 December 2002 http://infection.thelancet.com 723
ReviewPneumococcal meningitis
of survivors have clinical sequelae,18,19
whereas the mortality and morbidityrates of this age group in industrialisedcountries are about 10% and 30%,respectively.13,16
These mortality and morbiditydata have prompted studies that have targeted the identification of risk factors for adverse outcome of bacterial meningitis.28,29 Therisk for sequelae or death is greatest for, but not confined to, those patients who had seizures,focal neurological signs, deterioratingconscious state in hospital,hypotension, and S pneumoniaeinfection.2,28 The high risk for adverse outcome of pneumococcalmeningitis may be, at least in part, due to a relatively low sterilisation of the cerebrospinal fluid (CSF). Inone study,30 with pneumococcalmeningitis, the first negative CSFcultures occurred at 4·3 h, whereas alllumbar punctures in patients withmeningococcal meningitis were sterileby 2 h. Likewise, delays in diagnosisand therapy are assumed to affect the prognosis adversely,31 but theclinical data are inconclusive. Morethan 20 such studies have beenpublished; in almost half, there was no correlation between the duration of symptoms and the outcome.32
By contrast, in a randomised trial comparing ceftriaxone withcefuroxime in the therapy of childrenwith bacterial meningitis, hearingimpairment was milder in theceftriaxone-treated group than in the cefuroxime-treated group. This beneficial effect wasassociated with a more rapid CSF sterilisation.33
Interpretation of these studies, however, is difficult because(1) remembered duration of symptoms may not exactlyindicate the actual duration of meningitis, and (2) the clinicaloutcome is affected by many variables (see above).31 To solvethis problem, appropriate multivariate analyses to assess theindependent effects of delayed diagnosis, therapy, andsterilisation are needed. Until these have been done, prompttherapy should be the standard of care.
The accuracy of reported mortality for bacterialmeningitis may be hindered by the crude measurement ofhospital mortality and by the assumption that all hospitaldeaths are attributable to the case of meningitis thatprompted admission. Incorrect determination of the cause of hospital death, however, is common.34 Recently,McMillan and colleagues35 published a study designed tocharacterise and correlate the causes and timing of hospitaldeath in a cohort of adults (n=74) hospitalised for bacterial
meningitis. In a substantial proportion (23%) of patientswith bacterial meningitis who died in the hospital,meningitis was not the cause of death. All these patientsdied after 14 days in the hospital. Of those patients inwhom meningitis was at least the underlying cause ofdeath, 50 of 57 (88%) patients died within 14 days of hospital admission. Thus, the 14-day survival time seems to be a good means of discriminating between deathsattributed to meningitis and those that have another cause.The spectrum of causes of deaths attributed to meningitis isknown to be broad,35–38 ranging from systemic (eg, septicshock) to several neurological complications (eg, brainoedema, hydrocephalus, cerebrovascular involvement, and intractable seizures) (figure 2). Thus, in future studiesof bacterial meningitis it should be checked whether use ofthe simple 14-day survival endpoint will facilitate greateraccuracy of epidemiological statistics and will be a goodmeasure in investigations of the effect of new therapeuticstrategies.
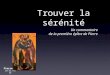
Figure 2. Major CNS complications secondary to acute bacterial meningitis. (A) Brain oedema. (B)Hydrocephalus. (C) Cerebral vasculitis with multiple cerebral infarctions. (D) Sinus thrombosis withvenous infarction and mild cerebral haemorrhage (black arrow). Brain oedema and hydrocephalusoccur, respectively, in 5–15% and about 10% of patients with community-acquired bacterialmeningitis. About 5–25% of patients with meningitis have cerebral infarction. Data are from Pfister etal,37 Durand et al,38 Dodge and Swartz,39 Arditi et al,13 and Westrate et al.40
Œdème cérébral
Vascularite cérébrale avec de multiples infarctus
Hydrocéphalie
Thrombophlébite avec infarctus d’origine veineuse et microhémorragies
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 December 2002 http://infection.thelancet.com 721
Reviews
Until the introduction of antibiotics in the 1930s and 1940s,acute bacterial meningitis was fatal in most cases. Sincethen it has become curable with a variable mortality andmorbidity rate for individual pathogens and patients.Neuropathological and clinical studies have shown that afatal outcome of the disease is often due to central nervoussystem (CNS) complications including cerebrovascularinvolvement, brain oedema formation, and hydrocephalusresulting in increased intracranial pressure and seizureactivity. During recent years, experimental studies withanimal models have substantially increased our knowledgeof the interactions of bacterial pathogens with mammaliancells and their entry into the CNS, and the complexpathophysiological mechanisms of brain dysfunction duringacute bacterial meningitis. There is now a substantial body of evidence that cytokines, chemokines, proteolyticenzymes, and oxidants are involved in the inflammatorycascade that leads to tissue destruction in bacterialmeningitis. Genetic targeting and/or pharmacologicalblockade of these pathways was beneficial in experimentalbacterial meningitis. Apart from dexamethasone, thesetreatment strategies hold major promise for the adjunctivetherapy of acute bacterial meningitis in clinical practice.
Lancet Infect Dis 2002; 2: 721–36
From its first description by Vieusseux in 1806 up to the early20th century, acute bacterial meningitis was uniformlyconsidered to be a fatal disease. Although the introduction ofsulfonamides and penicillins made bacterial meningitiscurable, mortality and morbidity from the disease remainunacceptably high.1 Neurological and neuropsychologicalsequelae are reported to affect up to half of survivors.2 Whileendemic bacterial meningitis remains a relatively rare disease,especially in developed countries, the potential occurrence ofepidemic bacterial meningitis in any part of the worldheightens its profile as a major infectious disease. Explosiveepidemics of meningococcal meningitis have periodicallycontinued to devastate sub-Saharan territories of Africa, theso-called meningitis belt. The most recent meningococcalmeningitis epidemic began in 1996 and has resulted in morethan 300 000 cases and 30 000 deaths being reported to theWorld Health Organization.3 Apart from epidemics, at least1·2 million cases of bacterial meningitis are estimated tooccur each year; 135 000 of them are fatal.4 These numbershave made bacterial meningitis a top-ten infectious cause ofdeath worldwide.
Clinical and neuropathological studies have clearlyshown that a fatal outcome of the disease is often caused by neurological complications secondary to bacterialmeningitis (eg, cerebral ischaemia, brain oedema formation,
hydrocephalus, or increased intracranial pressure). Duringthe past 15 years investigation has, therefore, focused on thepathophysiology of meningitis-associated brain dysfunction.5
It became evident that the host defence mechanisms withinthe brain are notably ineffective in eliminating majormeningitis pathogens, and that the inflammatory reaction tothe pathogen, rather than the pathogen itself, is largelyresponsible for the damage that results from bacterialmeningitis.6 A complicated series of interactions amongimmune, vascular, and central nervous system (CNS) cells, aswell as cytokines, chemokines, proteolytic enzymes, andoxidants seems to be ultimately responsible for meningitis-associated brain dysfunction. As a result, the therapeuticapproach to bacterial meningitis has to be widened fromeradicating the pathogen with antibiotics to prevention of the detrimental effects of the host immune response. In this article we highlight epidemiological trends andessential clinical aspects of acute bacterial meningitis. Wefurther review current notions of the pathogenesis andpathophysiology of acute bacterial meningitis, with anemphasis on promising targets for adjunctive therapy in acutebacterial meningitis.
Changing epidemiology of acute bacterialmeningitisDuring the past 15 years we have witnessed significantchanges in the epidemiology of acute bacterial meningitis.The most important change is the marked decline in theincidence of meningitis due to Haemophilus influenzae incountries that have introduced programmes for theimmunisation of infants with conjugate Hib vaccines,especially in North America and western Europe.1,7 Inthese countries, Streptococcus pneumoniae and Neisseriameningitidis are the most common causes of acute bacterialmeningitis, and bacterial meningitis is now a diseasepredominantly of adults rather than of infants and children.Most developing countries, however, have not added the Hib vaccine to their routine childhood immunisationprogrammes. Consequently, an estimated 350 000–700 000children worldwide still die from invasive Hib disease eachyear. The main barrier to adopting the Hib vaccine is its highcost relative to other routine immunisations (at least US$6,
Pathogenesis and pathophysiology ofpneumococcal meningitis
Uwe Koedel, William Michael Scheld, and Hans-Walter Pfister
UK and H-WP are at the Department of Neurology, KlinikumGrosshadern, Ludwig-Maximilians-University, Munich, Germany.WMS is at the Division of Infectious Diseases, Department of InternalMedicine, University of Virginia School of Medicine, Virginia, USA.
Correspondence: Professor Hans-Walter Pfister, Department ofNeurology, Klinikum Grosshadern, Ludwig-Maximilians-University,Marchioninistrasse 15, D-81377 Munich, Germany. Tel +49 89 7095 3676; fax +49 89 7095 6673; email [email protected]
Uwe Knodel, the lancet Infect. Dis 2002:722-34

Vascularite et méningite bactérienne : traitement
• Cor@sone 1 mg/kg avec une diminu@on très progressive (plusieurs mois) – Mais peu de données dans la lidérature
• Place des immunosuppresseurs ? (cyclophosphamide)

QUESTION 7 L’évolu@on neurologique est finalement sa@sfaisante après ré-‐intuba@on cor@coïdes, permedant l’extuba@on du pa@ent au 21ème jour. Quelles pathologies prédisposantes recherchez-‐vous ?
Ø Ethylisme chronique Ø Hémopathie (Myélome) Ø Diabète Ø Cirrhose Ø VIH
Ø Bilan : NFS, Calcémie, électrophorèse des pro@des, HbA1c, Bilan hépa@que, sérologie VIH

Méningite à Pneumocoque : recherche de facteurs de risque en fonc@on âge (2)
• Hypogammaglobulinémie – Recherche de Myélome mul@ple si âge > 50 ans
• Infec@on par le VIH – A rechercher systéma@quement en cas de facteur de risque ou si
infec@on invasive à pneumocoque récidivante • Chez le jeune enfant > 2 ans • Adolescent, jeune adulte sans facteur de risque autre d’infec@on invasive à pneumocoque
• Polymorphismes géné@ques – Mannose Binding lec@ne, autre …– discuté et en cours d’explora@on

Facteurs de risque évitables de méningite à bactérienne
• Méningites à pneumocoque – Implants cochléaires (Ree,uis J NEJM 2003, Wei BP. CID 2008)
• Vaccina@on an@-‐pneumococcique – Vaccin heptavalent conjugué si âge < 5 ans – Vaccin polysaccharidique, 23 valences si âge > 5 ans
– Splénectomie ou asplénie fonc@onnelle post-‐radiothérapie • Préven@on par vaccina@on et pénicilline orale
• Méningites induites à par@r de la flore cutanée (inocula@on) – Staphylocoques, streptocoques – Préven@on par le respect des règles d’hygiène de base et d‘asepsie lors des injec@ons para vertébrales ou intra rachidiennes

Méningite à Pneumocoque : recherche de facteurs de risque en fonc@on âge
• Asplénie congénitale ou hémoglobinopathie (drépanocytose) – Infec@ons invasives à pneumocoque dont méningites 20 à 1000 fois
plus fréquentes chez l’enfant < 5 ans.
• Déficit immunitaire congénitaux – Hypogammaglobulinémies congénitales, l’immunodéficience
commune variable, syndrome Wiskod-‐Aldrich – Rarement révélée par une méningite bactérienne à pneumocoque,
méningocoque ou hémophilus sp. – Evalua@on immunologique systéma@que après un 2e épisode
d’infec@on invasive à pneumocoque ou Méningite bactérienne?
• Traitement préven@f – Apport de gammaglobulines, vaccina@on, penicilline

Méningite à Staphylocoque ou autres Gram +
• Chez l’enfant peut être associé à un sinus dermique (dont risque méningite = 11 à 60 %) – Communica@on entre la peau, ses annexes et la moelle épinière – Anomalie rare de l’embryogénèse – A rechercher surtout si
• Hypertrichose cutanée, tâche de vin postérieures médianes
– IRM rachidienne • Chez l’adulte
– Méningite « d’inocula@on » : 6 % des méningites bactériennes (3/106 par an) – infec@on sévère

Selon Laurie L. Ackerman and Arnold H. Menezes Pediatrics 2003;112;641-647

QUESTION 8 Le pa@ent vous informe qu’il avait été vic@me d’un trauma@sme crânien grave à l'âge de 50 ans. L’imagerie réalisée confirme la présence d’une brèche ostéodurale. Quelle est votre a�tude thérapeu@que ?