Embed Size (px)
Citation preview

Co-infections VIH/hépatites
Eric RosenthalEric Rosenthal
Service de Médecine InterneHôpital Archet, CHU de Nice, [email protected]

Orateur : GSK, BMS, Tibotec/Janssen Cilag, Gilead, Roche, MSD, Abbvie
Conflits d’intérêt
Membre de groupes de travail : BMS, Gilead, MSD, Abbvie, GSK

� Vaccinations anti-VHA et VHB
� Hépatites virales C aigües
3 points en 30 minutes …
� Hépatites virales C aigües
� Hépatites virales C chroniques

• Vacciner les patients anti-VHA -� Co-infection VHB, VHC et hépatopathies chroniques
� Risque d’exposition (HSH, UDI), voyage en zone d’endémie
• Vacciner tous les patients anti -VHB -
Recommandations vaccinales
VHA et VHB chez les PVVIH
• Vacciner tous les patients anti -VHB -� Vaccin double dose (40 µg) et schéma renforcé (M0, M1, M2, M6)
� Patients non-répondeurs
• Intégrer le ténofovir aux ARV à titre de prévention
• Sérologie annuelle
� Ac anti-HBc + isolés: injection de rappel et le cas échéant vaccination complète
http://www.sante.gouv.fr/IMG/pdf/Rapport_Prise_en_charge_Hepatites_2014.pdf
http://www.sante.gouv.fr/IMG/pdf/Rapport_Morlat_2013_Mise_en_ligne.pdf

Marqueurs sérologiques VHA et VHB et facteurs
associés à la vaccination chez les PVVIH
VHA VHB
Dépistés 31% 90%
Non immuns 48% 25%
Cohorte ANRS CO13 HEPAVIH, n = 1175 VIH/VHC
• Facteur pour vaccination VHA :
- haut niveau d’éducation (OR 3.6, 95% CI 1.03–12.4; p = 0,045)
• Facteurs pour vaccination VHB : - haut niveau d’éducation (OR 2.5, 95% CI 1.3–4.5; p = 0.003)- genre masculin (OR 2.0, 95% CI 1.1–3.8; p = 0.02)- nadir CD4 élevé (OR 1.05, 95%, CI 1.009–1.103; p = 0.018)- absence de cirrhose (OR 2.7, 95% CI 1.2–6.4; p = 0.02)
Winnock M et al. Vaccine 2011
Non immuns 48% 25%
Vaccinés 6% 11%

� Vaccinations anti-VHA et VHB
� Hépatites virales C aigües
En bref …
� Hépatites virales C aigües
� Hépatites virales C chroniques

Hépatites aiguës C chez les homosexuels
masculins VIH+
Serpaggi J et al. AIDS 2006; Vogel M et al. J Antimicrobial Chem 2009

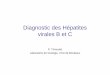
Evolution de l’incidence de l’infection VHC
chez les PVVIH
• HCV incidence in MSM:• Reached 4.1 cases per 100
PY in 2011 (18‐fold increase since 1998)
• HCV incidence in IDU:• Decreased from 13.9 to 2.2
cases per 100 PY
Swiss HIV Cohort Study: HCV yearly incidence rate by transmission group*
HET IDU MSM
Inci
denc
e ra
te (
per
100
py)
5
101520
• HCV incidence in heterosexuals• Remained <1 per 100 PY
throughout the study period
Wandeler G, et al. CROI 2012, Poster 106
Predictors of HCV seroconversion in MSM:
• History of unsafe anal sex• Past syphilis• Chronic hepatitis B
2002
Calendar year
1998 2000 2004 2006 2008 2010
Inci
denc
e ra
te (
per
100
py)
0.1
1
Shaded: 95% confidence intervals

� Vaccinations anti-VHA et VHB
� Hépatites virales C aigües
Et en détail …
� Hépatites virales C aigües
� Hépatites virales C chroniques

Aspects épidémiologiques
des co-infections VIH/VHC des co-infections VIH/VHC

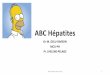
North: 359 = 18.3%
Prévalence des anti-VHC chez les PVVIH
Rockstroh J, et al. J Inf Dis 2005; 192:992–1002
South: 695 = 35.5%
Central: 293 = 15.0%
East: 613 = 31.3%

• Prevalence of HCV seropositivity in EuroSIDA is 33%1
• Of 1940 HCV Ab positive patients, 77% were serum HCV RNA-positive
(95% CI: 75–79)2
Distribution of HCV by genotype (1–4) in European regions2
60
Distribution génotypique du VHC chez les PVVIH
Northern Europe
0
20
40
1 2 3 4Southern
EuropeCentral Europe
Eastern Europe
1 2 3 4 1 2 3 4 1 2 3 4Genotype
1. Rockstroh J, et al. J Infect Dis 2005; 192:99–1002;
2. Soriano V, et al. J Infect Dis 2008; 198:1337–1344.

UK CHIC: Improved treatment outcomes and life expec tancy in patients starting HAART
UK CHIC: Life expectancy from age 20 to 65 of people starting cART (2000–2008) b by CD4 count at cART initiation, compared with UK
population (2000–2006) 2
UK population
Women Men (ye
ars)
70
60
50
UK CHIC: Observed a and projected proportion of patients with a current CD4 count < 200
cells/mm 3 and proportion of patients on ART with HIV-1 RNA <50 copies/mL in the UK 1
VL <50 copie s/ml, mode lled pat
ient
s
100 90 80 70
Evolution de l’espérance de vie des PVVIH
débutant un traitement
SLIDES FOR TRAINING PURPOSES ONLY 1. Adapted from Bansi L, et al. HIV Med 2010;11:432-438; 2. Adapted from May M, et al. BMJ. 2011;343:d6016 doi: 10.1136/bmj.d6016.
Women Men
HIV+ patients by CD4 count (cells/mm 3)
200–350 100–199 <100 Life
exp
ecta
ncy
50
40
30
20
10
0 20 25 30 35 40 45 50 55 60 65
Age (years)
Based on the UK CHIC study, standardized to risk-group status in the Survey of Prevalent HIV Infections Diagnosed (SOPHID) study. Error bars illustrate uncertainty bounds.
N = 9,657 HIV-infected patients with CD4 count recorded at baseline.
VL <50 copies/ml, observed VL <50 copie s/ml, mode lled
CD4<200 cells/mm, observed CD4<200 cells/mm, modelled
Pro
port
ion
of
p
2000 2002 2004 2006 2008 2010 2012
Year under follow-up
60 50 40 30 20 10 0

VIRAL HEPATITIS C IN HIV-INFECTED PATIENTSEric Rosenthal
Rosenthal et al, HIV Med 2009

Mortalité de 69.913 adultes français vivant avec le VIH
VIH/VHB
VIH
Mortalité chez les PVVIH
Ajusté sur âge, sexe, alcoolisme, cirrhose décompensée, SIDA
VIH/VHC
VIH/VHB
Mallet V et al. JFHOD 2013

Causes de décès chez les adultes co-infectés VIH/VHC
43 %
12 %
8 %
5 %
Cohorte ANRS CO13 HEPAVIH (Juin 2012)
5 %
4 %
4 %
4 %
2 %
6 %
7 %

Causes de décès chez les PVVIH (Mortavic 2010)
Rosenthal E, et al. J Hepatol 2012:56(Suppl 2) S12

Les patients VIH/VHC ont des CHC plus avancés que les patients VHC
Carcinome hépato-cellulaire (CHC)
http://www.sante.gouv.fr/IMG/pdf/Rapport_Morlat_2013_Mise_en_ligne.pdf

Contamination
Guérison
<20%
Infection
>80%
Hépatite
aiguë
Histoire naturelle de l’infection virale C
Lymphome
Guérison chronique> 95%
Hépatite
chronique
Cirrhose
>20%
CHC
Hépatopathie“Inflammationchronique”
1 à 2%
Lymphotropisme
Cryoglobulinémie
40%
Vascularite
Cryoglobulinémie

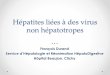
20
18
20
18
Hepatic causes Extrahepatic causes
Anti-HCV Ab positive, HCV-RNA undetectable
Anti-HCV Ab negative
19,8%
p<0,001 for intergroup comparison
Anti-HCV Ab positive, HCV-RNA detectable
The REVEAL HCV Cohort Study• 23 820 adults, Taiwan• 1095 anti-HCV positive ; 69.4% HCV-RNA detectable
HCV infection and global mortality risk
Lee MH et al. J Infect Dis 2012;206:469–477
18
16
14
12
10
8
6
4
2
0
18
16
14
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20
Mo
rta
lité
cu
mu
lée
(%
)
Mo
rta
lité
cu
mu
lée
(%
)
12,8%
1,6%
0,7%
12,2%
11,0%
p<0,001 for intergroup comparison p<0,001 for HCV-RNA detectable vs undetectable
Follow-up (years) Follow-up (years)
p<0,001 for intergroup comparison p<0,001 for HCV-RNA detectable vs undetectable

Circulatory diseases (A)
HCV infection and mortality risk from circulatory and renal diseases
Nephritis, nephrotic syndrome, and nephrosis (B)
Lee MH et al. J Infect Dis 2012;206:469–477

Interferon-based therapy and stroke-free survival
in HCV patients
Log-rank test,-f
ree
su
rviv
al
rate
0.95
0.90
100
Non-
IBT
IBT
Hazard ratio95% confidence
intervalP-value*
IBT 0.28 0.12 - 0.69 0.005
Non IBT 1
IBT ‡ 0.38 0.16 - 0.93 0.033
1
IBT, interferon based therapy
test,p = 0.003
Str
oke
-
0.80
0.85
0 1 2 3 4 5Time (years)
Hsu CS et al, Aliment Pharmacol Ther 2013; 38: 15-23
Non IBT 1
IBT † 0.39 0.16 - 0.95 0.039
Non IBT 1
† Adjusted for age, sex, hyperlipidaemia, DM, IHD, hypertension, alcohol-related illness, COPD, aspirin use, clopidogrel use,
warfarin use, dipyridamole use, ticlopidine use, statin use, ACE inhibitors use and influenza vaccination.
‡ Adjusted for age, DM, aspirin use and ACE inhibitors use.

Mortalité
hépatiqueToute cause
de mortalité
Bénéfices associés à la RVS
chez les patients co-infectés VIH/VHC
Mortalité
extra-hépatique
Mortalité
extra-hépatique
et non-VIH
Berenguer M et al. CID 2012

ARN VHC+ initial:
N= 2036 (81%)
• Guérison spontanée: n= 475 (19%)
• Guérison après traitement:
n= 644 (25%)
Prise en charge thérapeutique des patients
Co-infectés VIH/VHC en France
Sérologie VHC +:
N= 2511
• 17 776 PVVIH venus au moins une fois en 2012 dans 10 centres .
• 703 pts naïfs (52%)
• 493 pts en échec de TRT (37%)
• 132 en cours de traitement (10%)
• Recontamination: n= 14
N= 2036 (81%)
ARN VHC + au
31/12/2012*:
N= 1342 (54%)* Statut inconnu: n= 50
1283 (63%) patients ont reçu au
moins un traitement !
n= 644 (25%)
Génotype 1: 61%
Génotype 4: 24%
Génotype 3: 14%
Génotype 2: 2%
ARN VHC + :
Poizot Martin I et al.Hepadat’s AIDS study group. 14th European AIDS Conference 16-19 Octobre 2013

Les nouveaux traitements
anti-VHCanti-VHC

2011 : la bombe sofosbuvirElectron, Proton, Neutrino, Atomic, Fission, Fusion …

ELECTRON: PSI-7977 ± RBV ± PegIFN in Genotype 2/3 Treatment-Naive Patients
� Nucleotide analogue PSI-7977 400 mg QD + RBV for 12 wks
– PegIFN included for 0, 4, 8, or 12 wks
� All patients in all arms had
100
80
60
Pat
ient
s (%
)
100 100 100 100
SVR12 Outcomes
� All patients in all arms had undetectable HCV RNA by Wk 4
� 100% SVR12 in all RBV-containing arms
– SVR24 in 100% of patients with evaluable data (n = 20)
� PSI-7977 monotherapy (RBV free) arm added; 60% SVR4
Gane EJ, et al. AASLD 2011. Abstract 34.
60
40
20
0
Pat
ient
s (%
)
PSI-7977/RBV
+ 0 Wks PegIFN
(IFN Free)
PSI-7977/RBV
+ 4 WksPegIFN
PSI-7977/RBV
+ 8 WksPegIFN
PSI-7977/RBV
+ 12 WksPegIFN
n/N = 10/10 9/9 10/10 11/11

� Traitements AVEC interféron
� Traitements SANS interféron

AR
N V
HC
in
dé
tect
ab
les
(%)
42,2
59,4
73,465,6
60,760
80
100 PR B/PR
Efficacité de la trithérapie BOC + PR
chez les co-infectés naïfs VIH/VHC A
RN
VH
C i
nd
éte
cta
ble
s (%
)
3/34 3/64 5/34 27/64 8/34 38/64 11/34 47/64 10/34 9/3442/64 37/61
� La trithérapie par Boceprevir guérit 61 % des co-infectés naïfs
de traitement anti-VHC
8,814,7
23,532,4 29,4 26,5
4,7
42,2
0
20
40
4 8 12 24 Fin de
Traitement
RVS12
Semaines
Sulkowski M et al. Lancet ID 2013

AR
N V
HC
in
dé
tect
ab
le (
%)
60
80
10086
75 7167
5055
75
Telaprevir et co-infection: naïfs G1
Résultats virologiques S24
Résultats comparables dans l’étude de
AR
N V
HC
in
dé
tect
ab
le (
%)
Sans ART EFV/TDF/FTC ATV/r/TDF/FTC Total
0
20
40
6/7 11/16 10/15 27/38n/N = 2/6
33
4/8 6/8 12/22
T/PR PR
Résultats comparables dans l’étude de phase III Insight (AASLD 2013)
Sulkowski M, et al. Ann Intern Med 2013

Telaprevir, boceprevir et co-infection VIH :
patients prétraités
BocepreVIH, ANRS HC27TelapreVIH, ANRS HC26
Cotte L. et al., CROI 2014, P668; Poizot-Martin I. et al., CROI 2014, abstract P659 LB
La co-infection VIH ne doit plus être considérée
comme un facteur de mauvaise réponse au traitement !

Trithérapies anti-VHC avec IP chez 41 patients co-infectés
VIH/VHC traités hors essai thérapeutique (1)
80
100
70%
85% 84%G1a 78%
Naqvi A et al, SNFMI, Bastia 2014
0
20
40
60
80
JO S4 S12 S24 S48 RVS12
70% 67%
53%
Prétraités 66%
Non répondeurs 34%
F4 42%

Trithérapies anti-VHC avec IP chez 41 patients co-infectés
VIH/VHC traités hors essai thérapeutique (2)
13 patients (32%): échec virologique 5/41, décision dupatient 3/41, effets indésirables 5/41
Rash 10 (25%)AnémieAnémie sévère (Hb <9 g/dl ou baisse >3 g/dl)
36 (90%)34 (85%)
Réduction posologique de ribavirine 22 (55%)Utilisation d’EPO 22 (55%)Transfusion 2 (5%)
Naqvi A et al, SNFMI, Bastia 2014

Boceprévir et Télaprévir chez les patients
cirrhotiques dans la cohorte ANRS CO13 Hepavih
Gilbert C et al, IWHOD 2014

Boceprévir et Télaprévir chez les patients
cirrhotiques dans la cohorte ANRS CO13 Hepavih
Gilbert C et al, IWHOD 2014

Siméprévir + PEG-IFN/RBV
chez les co-infectés VHC/VIH : essai C212
RVS12 (%), ITT
7480
8996
79
6471 68
87
6170
5760
80
100%
179
Dieterich D, CROI 2014, Abs. 24
0
20
40
Ensemble des patients
Naïfs F3/F4
F0/F2
RechuteursRépondeurs partiels
Répondeurs nuls
G1a et autres
G1b
CTCC
TT
Génotype IL28B
27/28
40/59
11/18
16/18
62/88
36/45
14/22
42/53
13/15
7/10
16/28
78/106
(pas d’influence du polymorphisme Q80K)

Critères CUPIC : contre indications
à l’interféron
FacteursPlaquettes
> 100.000/mm3
Plaquettes
≤ 100.000/mm3
Sur risque d’EIs avec Peg-IFN/RBV+ TPV ou BOC
Albuminémie ≥ 35 g/l 3,4% (10/298) 4,3% (3/69)
Albuminémie < 35 g/l 7,1% (2/28) 44,1% (15/34)
Hezode C et al. J Hepatol 2013
Paramètres OR IC 95% p
Plaquettes < 100
000/mm3 3,11 1,30-7,41 0,0105
Albumine < 35 g/L 6,33 2,66-15,07 0,0001

� Traitements AVEC interféron
� Traitements SANS interféron

96100
7680
100
GT 1
HC
V R
NA
< 2
5 I
U/m
L (%
)
96 9688
80
100
GT 2
HC
V R
NA
< 2
5 I
U/m
L (%
)
100 98
6780
100
GT 3
HC
V R
NA
< 2
5 I
U/m
L (%
)
SOF + RBV x24 weeks SOF + RBV x12 weeks SOF + RBV x12 weeks
SOF + RBV chez les patients co-infectés
VIH/VHC (Photon 1)
0
20
40
60
Week 4 EOT SVR12
HC
V R
NA
< 2
5 I
U/m
L (%
)
110/114 87/114
0
20
40
60
Week 4 EOT SVR12
HC
V R
NA
< 2
5 I
U/m
L (%
)
25/26 23/2622/23
Sulkowski MS, et al. AASLD 2013. Oral #212
♦ No HCV resistance (S282T) was observed in virologic failures via deep sequencing
♦ Two patients had HCV breakthrough; both had documented non-adherence to SOF
♦ Two patients had transient HIV breakthrough; both had documented non-adherence to ART
0
20
40
60
Week 4 EOT SVR12
HC
V R
NA
< 2
5 I
U/m
L (%
)
41/41 28/42100/100 39/40

GT 1
SOF + RBV
24 weeks
GT 2
SOF + RBV
12 weeks
GT 3
SOF + RBV
12 weeks
SOF + RBV: comparaison mono-infectés VHC vs
co-infectés VIH/VHC
GT 3
SOF + RBV
24 weeks
687680
100 9388
80
100
56
6780
100
SV
R1
2 (
%)
85
80
100
Osinusi A, et al. JAMA. 2013;310(8):804-811.SulkowskiMS, et al. AASLD 2013. #212.ZeuzemS, et al. AASLD 2013#1085.LawitzE, et al. N Engl J Med. 2013 May 16;368(20):1878-87.
SV
R1
2 (
%)
0
20
40
60
SPARE PHOTON-1
SV
R1
2 (
%)
0
20
40
60
VALENCE PHOTON-1
SV
R1
2 (
%) 56
0
20
40
60
FISSION PHOTON-1
SV
R1
2 (
%)
0
20
40
60
VALENCE

Réponses virologiques soutenues
Ledipasvir/sofosbuvir à dose fixe chez les
patients co-infectés VIH/VHC G 1
EASL 2014 - D’après Osinusi A et al., abstract O14, actualisé
ARV- 13/13 13/13 13/13 12/12 10/10 10/10
ARV+ 37/37 37/37 30/30 22/22
LIQ : limite inférieure de quantification.

Ledipasvir/sofosbuvir à dose fixe chez les
patients VHC G1 pré-traités (ION-2)
• Etude de phase III: 440 patients VHC G1 en échec (F4 20%),
y compris aux inhibiteurs de protéase du VHC
Réponse virologique soutenue
24 semaines12 semaines
102/109 107/111 108/109 110/111
EASL 2014 - D’après Afdhal N et al., abstract O109, actualisé, N Engl J Med 2014

ANRS HC31 SOFTRIHANRS HC31 SOFTRIH
Pilot study to assess efficacy and safety ofPilot study to assess efficacy and safety ofSofosbuvirSofosbuvir//LedipasvirLedipasvir (GS(GS--5885) fixed5885) fixed--dose combination in dose combination in
treatmenttreatment--experienced subjects withexperienced subjects withHCV genotype 1 infection and HIV coHCV genotype 1 infection and HIV co--infectioninfection
Coordinating investigator : Pr Eric Rosenthal Service de Médecine interne, Hôpital Archet 1, Nice
Center for methodology and management : Pr Eric Bel lissantService de pharmacologie clinique – CIC Inserm 0203 Hôpital de Pontchaillou, Rennes

Virologic Responses (per-protocol population)
MK-5172 + MK-8742 ± RBV chez les patients
mono et co-infectés VIH/VHC G 1 (C-Worthy)
• Patients excluded from the per protocol population
– Mono-infected: 7 patients excluded
• 4 patients received wrong RBV dose; all achieved SVR12
• 3 patients discontinued early (Day 3, 22, 35) they are included in analysis up to time of discontinuation
– Co-infected: 1 patient excluded
• lost to follow-up after TW4 Adapted from: Mark Sulkowsky et al CROI 2014 #654LB

Recommandations
thérapeutiquesthérapeutiques


Génotype 1a
AASLD EASL Allemagne AFEF
Naïfs
Recommandé
alternative
SOF+ PR 12s
SIM 12S+PR 24s
SOF+ SIM 12s
SOF+ PR 12s
SOF+DCV 12 s ±R(cirrh)
SOF+ SIM 12 s
SOF+ PR 12s
24 s si facteurs neg
SOF+ PR 12s
SOF+DCV 12 s
SOF+ SIM 12 salternative SOF+ SIM 12s
SOF+R 24s
SOF+ SIM 12 s
±R(cirrh)
SIM 12S+PR 24s Q80K-
SOF+R 24s
SOF+ SIM 12 s
Rechuteurs
Recommandé
alternative
SOF+ PR 12s
SIM 12S+PR 24s
SOF+ SIM 12s
SOF+R 24s
SOF+ PR 12s
SOF+DCV 24 s ±R(cirrh)
SOF+ SIM 12 s ±R(cirrh)
SIM 12S+PR 24s Q80K-
SOF+R 24s
SOF+ PR 12s
SOF+DCV 12s
SOF+ SIM 12s
SOF+ PR 12s
SOF+DCV 12s
SOF+ SIM 12s
Non répondeurs SOF+SIM 12s
SOF+PR 12s
SIM12s+PR 24s
SOF+ PR 12s ou plus?
SOF+DCV 24 s ±R
SOF+ SIM 12 s ±R
SOF+ PR 12s
SOF+DCV 12s
SOF+ SIM 12s
SOF+DCV 12s
SOF+ SIM 12s

Co-infection VIH/VHC
• AASLD: Indications for HCV treatment in HCV/HIV co-infected persons are
identical to those in patients with HCV mono-infection. The same treatment
regimens can be used in HIV-co- infected patients as in patients without HIV
infection, as the virological results of therapy are identical
• EASL: Indications for HCV treatment in HCV/HIV co-infected persons are
identical to those in patients with HCV mono-infection (A1). The same treatment identical to those in patients with HCV mono-infection (A1). The same treatment
regimens can be used in HIV-co- infected patients as in patients without HIV
infection, as the virological results of therapy are identical (A1)
• Allemagne: Data with SOF + PegIFN + RBV x 12 weeks are limited, and
based on the Photon 1 study (SOF+R), there is no reason why SVR rates should not
be similar to SVR rates in mono-infected HCV patients
• AFEF: Les même schémas thérapeutiques que ceux proposés chez les
malades mono-infectés par le VHC peuvent être utilisés. Une attention toute
particulière doit être portée aux interactions médicamenteuses

G 1
Fibrose hépat que
F0/F1
et
pas de
manifestat ons extra-
hépat ques
G 2
Fibrose hépat que ≥ F2
ou
manifestat ons extra-hépat ques (vascularites, …)
ou
risque de transmission du VHC
G 3 G 4
Décision et choix de traitement ant -VHC chez les PVVIH
G 5,6
-At ente
décision au
cas /cas
S = semaines
DCV = daclatasvir; PR = Interféron pégylé+ribavirine; RBV = ribavirine; SMV = simeprevir; SOF = sofosbuvir
TGR = traitement guidé par la réponse (si ARN VHC < 25 UI/ml à S4 traitement 24S, sinon 48S)
Pour les pat ents cirrhot ques, le nombre de pat ents traités dans les essais est souvent faible et doit inciter à traiter ces pat ents dans le cadre
d’essais ou de cohortes observat onnelles lorsque cela est possible
NaifsPrétraités
bithérapie
1er choix
SOF+PR 12S
SOF+RBV 24S
alternat ves
SMV 12S+PR TGR 24/48S
SOF+DCV 24S
SOF+SMV 12S
Choix possibles
SMV 12S+ PR 48S
SOF+SMV 12S
SOF+DCV 24S
Prétraités
trithérapie
1er choix
essai
thérapeut que
alternat ve
SOF+DCV 24S
1er choix
essai thérapeut que
alternat ve
SOF+PR 12S
SOF+RBV 24S
SMV 12S+PR 24
(naïfs) /48S (pré-
traités)
Naifs ou
Prétraités
1er choix
SOF+RBV 12S
Naifs ou
Prétraités
1er choix
SOF+RBV 24S
alternat ves
SOF+PR12S
SOF+DCV24S
(cirrhot ques pré-
traités)
Naifs ou
Prétraités
Naifs ou
Prétraités
1er choix
essai
thérapeut que
alternat ve
SOF+PR 12S
http://www.sante.gouv.fr/IMG/pdf/Rapport_Prise_en_charge_Hepatites_2014.pdf

FranceCOMMENT TRAITER ?
Sofobuvir est recommandépour tous les génotypes
SOF + RIBA 24 semaines non recommandé chez les G1
Aucune spécificité pour lesPatients co -infectés VIH/VHCPatients co -infectés VIH/VHC

Interactions médicamenteuses

Le Futur en 2015
Interferon Free
Sofosbuvir
G2/3 +
Asunaprevir*
Daclatasvir*±
Sofosbuvir+ Ledipasvir
FDC*
Ombitasvir*
Dasabuvir*
+
ABT-450*/r
RBV
+
±
IFN
-fre
e
European approvals
Protease inhibitor
Nuc inhibitors
NS5A
NS5B inhibitor
Jul–Dec Jan–Jun Jul–Dec Jan–Jun Jul–Dec Jan–Jun Jul–Dec Jan–Jun Jul–Dec
Telaprevir
Boceprevir
Triple therapy
Sofosbuvir(G1,4,5,6)
+
RBV
±
BMS-325*
Daclatasvir*(G1, 2, 3, 4)
FDC*
2011 2012 2013 2014 2015
IFN
-bas
ed
Simeprevir*(G1, 4)
RBV
±
Nuc: nucleotide polymerase inhibitor; NS5A: hepatitis C virus non-structural protein 5a protease inhibitor*Not yet approved in Europe

Les aspects économiques

AMM européennes en 2014
JANVIER MAI SEPTEMBRE
SOFOSBUVIR
19 000 €/mois
SIMEPREVIR
11 600 €/mois
DACLASTAVIR
11 800 €/mois


� La vaccination contre le VHA et le VHB doit êtrerenforcée
Messages personnels …
� L’impact du VHC sur la morbi/mortalité estsignificatif. Les progrès thérapeutiques sontmajeurs et le VIH n’est plus une limite à la guérison
� Les principaux défis : le dépistage et l’accès au traitement pour le plus grand nombre