Embed Size (px)
Citation preview

soumis pour publication le 12 décembre 2010accepté pour publication le 16 mars 2011 151
Revue d’Odonto-Stomatologie/Septembre 2011
La position de la canine, son environnement gingival fragile et ses tables osseuses fines la rendent vulnérable auxagressions mécaniques. À cause de son volume, les mouvements orthodontiques qui l’éloignent de son enveloppeparodontale risquent d’engendrer des lésions. La chirurgie plastique intervient activement pour préserver ces paramètresanatomiques. Sa situation stratégique, sa proprioception et sa morphologie palatine (canine maxillaire) interviennent dansla cinématique mandibulaire. Au niveau esthétique, sa gencive marginale participe au dessin de la ligne gingivale et sonanatomie en fait une dent difficile à restaurer. Son remplacement implique un choix thérapeutique délicat face auxparamètres de mutilation, de pérennité ou de contraintes techniques. Ses caractéristiques interviennent lors des choix deremplacements des incisives latérales (agénésies), amenant systématiquement à des compromis. Pour ces raisons, lorsquela clinique ne l’impose pas, il faut y toucher le moins possible, implanter avec prudence et surtout anticiper les éventuelsproblèmes par des thérapeutiques ortho-parodontales préventives.
Virginie MONNET-CORTI*, Caroline FOUQUE-DERUELLE**, Bernard MAGNEVILLE**.*Maître de Conférences des Universités, Faculté d’Odontologie de Marseille, Praticien Hospitalier, APHM.**Ancien Assistant Hospitalo-Universitaire, Faculté d’Odontologie de Marseille - Exercice privé à Marseille.
La canine une dent pas commeles autres : considérationsparodontales et prothétiques.
Mots clés :CanineParodonteProthèseOrthodontieChirurgie plastique parodontale
PARODONTIE
Canine, a tooth unlikethe others: periodontaland prosthetic considerations.
Rev Odont Stomat 2011;40:151-172
Keywords:CaninePeriodontalProstheticOrthodonticPeriodontal plastic-surgery
R É S U M É
Canines are vulnerable to mechanical attacks due to its position, fragile gingival environment and thin cortical bone tables.Because of its large size, any orthodontic action moving the tooth away from the supporting tissues may cause periodontallesions. Plastic surgery has been actively performed to protect these anatomical parameters. Its strategic position,proprioception and palatal morphology (in maxillary canines) are involved in the mandible kinematics. In esthetics, thecanine marginal gingiva is used to draw the gingival line and its particular anatomy is difficult to restore. When a caninemust be replaced, a treatment choice must be decided by taking into account several parameters such as tissue damage,longevity or technical constraints. In presence of lateral incisor agenesis, a treatment decision may be a compromise byusing a canine for a replacement with certain tooth modifications. Consequently, when the clinical condition does not require,the canines should be the least altered. An implant placement in this position must be performed with caution. Treatmentsof impacted canines must be especially anticipated with preventive orthodontic/periodontal approaches.
A B S T R A C T

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
La canine est fréquemment impliquée dans différentstraitements simples ou complexes faisant intervenir lesdiverses disciplines odontologiques.Son éruption et, par conséquent, la mise en fonctionocclusale sont tardives, induisant une immaturitéparodontale bien après l’adolescence, a fortiori suite àune mise en place orthodontique après son âge d’éruptionavec ou sans dégagement chirurgical.Au niveau parodontal, lorsqu’elle présente une lésionsuperficielle ou profonde, il faut souvent considérer uneétiologie pluri-factorielle : anatomique, bactérienne,occlusale, et/ou traumatique.Au niveau prothétique, le cumul des paramètres àrespecter impose une vigilance particulière.Observons ce qui la distingue des autres dents.
Éruption et données parodontales :
Le parodonte immature de l’enfant et de l’adolescentprésente de nombreuses différences anatomiques parrapport à celui de l’adulte.- Développement de l’ensemble des tissus de soutien enétroite corrélation avec la croissance osseuse faciale.Celle-ci débute lentement chez l’enfant à partir de 2 ans,s’arrête à 8 ans après la poussée de croissance juvénilepour reprendre avec la poussée de croissance adolescente(12 ans chez les filles et 14 ans chez les garçons) et seterminer ou ralentir fortement à la fin de la croissancedes os longs (15 ans chez les filles et 17 ans chez lesgarçons) (Sauvan et coll., 2008).- Croissance de l’os alvéolaire (premier pilier des tissusdentaires et parodontaux).On sait que la croissance des procès alvéolaires estproportionnelle à l’éruption dentaire ainsi qu’à la fonctionmusculaire. Pendant l’enfance, elle est plus importantedans le sens vertical que dans les sens antéro-postérieuret transversal. Cette activité appositionnelle verticalesur la crête osseuse alvéolaire est observée jusqu’à 21ans environ, ce qui correspond à la fin de l’éruptionpassive et à la stabilisation de l’espace biologiqueparodontal (Gargiuolo et coll., 1961).Compte tenu de sa date d’éruption, la canine bénéficiedonc tardivement de cette activité appositionnelle.- Chez l’adolescent le cément est plus épais et plus denseet le desmodonte moins large que chez l’enfant, ces deuxtissus présentent ainsi des caractéristiques histologiqueset anatomiques d’un tissu jeune immature.- Quant à la gencive, au début de l’éruption fonction-nelle, elle est le siège d’une inflammation transitoire :elle est épaisse, ourlée et rouge. Secondairement, la qualitéet la quantité de tissu gingival chez l’enfant et chezl’adolescent sont étroitement corrélées à la position del’émergence dentaire tandis que la position de la lignemuco-gingivale est déterminée génétiquement par rap-
Canines are frequently involved in various simple orcomplex treatments involving diverse dental disciplines.A delayed eruption and consequently late developmentinto occlusion of canines can result in a periodontalimmaturity long after adolescence and when its age oferuption is exceeded, an orthodontic intervention is àfortiori required with or without surgical exposure.When the tooth presents a superficial or deep periodontallesion, a multi-factorial etiology must be considered:anatomical, bacterial, occlusal and\or traumatic.When a prosthetic reconstruction is indicated on thistooth, several parameters must be taken into accountwith particular attention.Several characteristics can distinguish this tooth fromthe others.
Eruption and periodontal data:
Immature periodontium in children and adolescentspresents numerous anatomical differences with regardto that of adults:- Development of all tooth supporting tissues in closerelationship with facial bone growth. Facial bone growthbegins slowly in children from 2 years old then arrestsat 8 years old after the juvenile growth spurt before startingagain with the adolescent growth spurt (12 years old ingirls and 14 years old in boys) to end or considerablyslows down at the end of long bone growth (15 years oldin girls and 17 years old in boys). (Sauvan et al., 2008).- Growth of alveolar bone as a (first support of dentaland periodontal tissues).The growth of alveolar bone processes is known to berelated to and affected by tooth eruption and muscularfunction. During childhood, it is more pronounced invertical than antero-posterior and transverse directions.This vertically appositional activity of the alveolar bonecrest is observed until approximately 21 years old,corresponding to the final stage of passive eruption andthe stabilization of the periodontal biological space(Gargiuolo et al., 1961).Considering its date of eruption, the canine thus benefitslately from this appositional activity.- Histologically and anatomically, the cementum and theperiodontal ligament present characteristics of animmature young tissue in children and adolescents.However, the latter have thicker and denser cementumwith a narrower periodontal ligament space.- At the beginning of functional eruption, a transitorygingival inflammation is observed resulting in a thick,swollen and red tissue. The quality and quantity of gingivaltissue in children and adolescent are closely related tothe position of tooth emergence whereas the position ofthe muco-gingival junction is genetically determinedwith regard to the basal bone borders of the maxilla and
152

Revue d’Odonto-Stomatologie/Septembre 2011
port aux bords basilaires maxillaires et mandibulaires. Lahauteur de tissu kératinisé en denture temporaire croîten même temps que la croissance des procès alvéolaires.Le sulcus est plus profond jusqu’à la fin des phénomènesd’éruption passive.Lorsque, chez l’adulte, les tissus parodontaux de lacanine sont devenus des tissus matures et fonctionnels,la sensibilité et la finesse de la proprioception du ligamentparodontal (desmodonte) de la canine en font une« dent-clé » pour le guidage lors des mouvements delatéralité fonctionnels ou para-fonctionnels.La quantité et la qualité de la gencive sont alors stableset présentent des valeurs moyennes facilement mesura-bles qu’il est utile de connaitre afin de s’y référer avanttout traitement : d’après Müller et Eger (1997), la valeurmoyenne normale de hauteur de tissu kératinisé de lacanine est d’environ 4,5 mm au maxillaire et de 3,5 mmà la mandibule. La valeur moyenne normale d’épaisseurde la gencive vestibulaire de la canine est d’environ 0,8mm au maxillaire et à la mandibule. Il est important denoter que l’épaisseur gingivale de la canine maxillairereprésente la valeur la plus faible par rapport à toutes lesautres dents maxillaires.La table osseuse vestibulaire autour des canines maxil-laire et mandibulaire est très fine, parfois il y a contactdirect entre la paroi radiculaire et l’os alvéolaire sansinterposition de ligament parodontal.Parfois même, cette racine très volumineuse émerge endehors de l’os alvéolaire créant des déhiscences et desfenestrations, et la mettant ainsi en contact direct avecle tissu conjonctif gingival vestibulaire (lui-même debiotype très fin).De plus, l’anatomie globuleuse de cette racine est souventbordée de concavités osseuses proximales très prononcées.
Afin d’aider les cliniciens à dépister les anatomiesparodontales fragiles, quelques auteurs (Ochsenbein etMaynard, 1974) travaillant en collaboration étroite avecdes orthodontistes, ont proposé de répertorier les différentsbiotypes parodontaux au travers de classifications.Certaines s’appliquent aux enfants et adolescents (Korbendauet Guyomard, 1998) (figure 1AB), d’autres aux adultes(Maynard et Wilson, 1980). Selon Benoit et Genon en1985 qui ont évalué les différents types de parodontechez 400 patients traités orthodontiquement, la classedes parodontes fins et fragiles dits « à risque » concerneenviron 30 % de leurs patients enfants et adolescents.En présence d’un biotype parodontal fin et fragile(figure 2), l’apparition de lésions parodontales sembleinéluctable. Ces lésions sont déclenchées essentiellementpar la mise en œuvre d’un brossage traumatique (Wennstromet Zucchelli, 1996). En effet, les canines étant situées auniveau du changement d’angulation de la courbure d’arcadedentaire et étant en situation proéminentes (bosse canine),
mandible. During primary dentition, the height ofkeratinized tissue grows at the same time as the alveolarbone processes. The gingival sulcus remains moreprofound until the end of the passive eruption.
In adults with mature and functional periodontal tissues,the sensitivity of the canine periodontal ligament’sproprioceptive function makes this tooth a “key-tooth”for guiding during functional or parafunctional lateralexcursions.
The quantity and quality of the gingiva are then stableand presenting mean values that are simple to measureand can be used as a reference prior to any treatment.According to Müller and Eger (1997), the normal meanheight of the canine keratinized gingival tissue is about4.5 mm in the maxilla and 3.5 mm in the mandible. Thenormal mean thickness of the canine labial gingiva isabout 0.8 mm in both maxilla and mandible. It must benoted that the gingival thickness of the maxillary caninerepresents the least value compared to that of the othermaxillary teeth.
The labial cortical bone around maxillary and mandibularcanines is very thin and the root surface can sometimesbe in direct contact with the alveolar bone withoutinterposition of periodontal ligament.Moreover, this very voluminous root can appear outsidethe bony limits of the alveolus creating alveolar bonedehiscences and fenestrations resulting in a directcontact of the root with the labial gingival connectivetissue of very thin biotype).Furthermore, the globuleuse anatomy of the canine rootis often lined with highly pronounced proximal boneconcavities.To help clinicians detecting fragile periodontal anatomies,some authors (Ochsenbein and Maynard, 1974) workingin close collaboration with orthodontists suggested aclassification into different periodontal biotypes. Thisclassification has been applied to children and adolescents(Korbendau and Guyomard, 1998) (figure 1AB), oradults (Maynard and Wilson, 1980). According to Benoitand Genon (1985) who evaluated various types ofperiodontium in 400 orthodontically-treated patients,the class of thin and fragile, called “at risk”, periodontiumconcerns approximately 30% of the patients (childrenand adolescents).In the presence of a thin and fragile periodontal biotype(figure 2), periodontal lesions inevitably appear. Theselesions are essentially caused by traumatic toothbrushing(Wennstrom and Zucchelli, 1996). Indeed, being situated atthe turning angle of the dental arch curvature and in theprominent situation (canine prominence), canines areoften the first to present marks of a vigorous toothbrushing
153

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
ce sont souvent les premières à présenter les stigmatesd’un brossage vigoureux avec une brosse dure. Ces lésionsse présentent sous la forme d’érosion gingivale, de fentede Stillman (Stillman 1921) (figure 3), ou de récessiongingivale voire d’abrasion cervicale.Ainsi, il faut savoir dépister des manœuvres d’hygiènebucco-dentaire agressives et traumatogènes pour éduquerles patients à un brossage non traumatique et en surveillerla pérennité.Plus que toute autre dent, la canine doit faire son éruptionau centre des tissus parodontaux dans l’espace laissé parla dent lactéale pour s’envelopper d’un manchon deparodonte de bonne dimension capable de résister auxagressions mécaniques.
with a hard toothbrush. These lesions appear under theform of gingival erosion, Stillman’s cleft (Stillman 1921)(figure 3), or gingival recession. Cervical abrasion can alsobe observed.
Aggressive and traumatic oral hygiene operationsshould therefore be detected and the patients must beinstructed to a non-traumatic toothbrushing with a long-term follow-up.It is also more essential than in other teeth that the caninemust emerge in the center of periodontal tissue spaceleft by its deciduous tooth creating a periodontiumsleeve of proper dimension capable of resisting mechanicalaggressions.
154
1A
Fig. 1 : classification de Korbendau et Guyomard, 1998.A : le type A, le procès alvéolaire est épais, son bord marginal estproche de la jonction amélo-cémentaire (1 mm). La gencive estépaisse et de hauteur supérieure à 2 mm ; le type A correspond auparodonte idéal, qui résiste bien à l’agression bactérienne et aux stressmécaniques.B : le type C, le procès alvéolaire est mince, son bord marginal est àdistance de la jonction amélo-cémentaire. La gencive est mince ettendue, de hauteur supérieure à 2 mm. Ce type représente unparodonte fragile avec la présence d’une déhiscence osseuse et d’unegencive mince. Il peut évoluer vers une vraie récession gingivale.
1B
Fig. 1: classification of Korbendau and Guyomard (1998).A: type A, thick alveolar bone with the marginal bone close tothe cemento-enamel junction (1 mm). The gingiva is thick with aheight superior to 2 mm. The type A corresponds to the idealperiodontium, which resists well bacterial aggression andmechanical stress.B: type C, thin alveolar bone with the marginal margin remotefrom the cemento-enamel junction. The gingiva is thin and tightwith a height superior to 2 mm. This type represents a fragileperiodontium with a presence of bone dehiscence and thin gingiva.It can evolve towards a real gingival recession.
2 3
Fig. 2 : chez l’adulte : biotype parodontal fin et fragile.In adult: thin and fragile periodontal biotype.
Fig. 3 : fente de Stillman (1921) et érosion gingivale due au Bros-sage traumatique qui est le facteur majeur du déclenchement desrécessions gingivales (Wennstrom et Zucchelli, 1996).Stillman’s cleft (1921) and gingival erosion due to traumatictoothbrushing which is the major triggering factor of gingivalrecessions (Wennstrom and Zucchelli, 1996).

Revue d’Odonto-Stomatologie/Septembre 2011
Mouvements orthodontiqueset données parodontales :
La canine, à cause de ses dimensions importantes, doitcheminer dans un couloir d’éruption confortable(Korbendau et Guyomard, 1998) et à distance raisonnabledes autres dents. En effet, si son éruption en malpositionn’est pas interceptée, elle peut créer des dommagesirréparables sur les dents adjacentes (nécrose pulpaire,destruction desmodontale et osseuse voire résorptionradiculaire)(figure 4 AB).
Parmi les mouvements orthodontiques qui risquentd’engendrer des lésions sur le parodonte fragile on peutnoter :- les versions corono-linguale ou corono-vestibulaire
des incisives mandibulaires,- la translation vestibulaire,- les mouvements de torque radiculo-vestibulaires,- les déplacements mésio-distaux d’une dent dans une
zone édentée étroite,- l’expansion transversale (Detienville et coll., 1993 ;
Fontenelle 1982 ; Maynard 1998).
Orthodontic movements andperiodontal data:
Due to its voluminous size, the canine must proceed duringits eruption through a spacious eruption path (Korbendauand Guyomard, 1998) and at a reasonable distance fromthe other teeth. Indeed, when its eruption in malpositionis not intercepted, an irreparable damage can be causedon the neighboring teeth such as pulp necrosis, periodontalligament and bone destruction or even root resorption)(figure 4 AB).
Following orthodontic movements present a risk ofengendering lesions on fragile periodontium:
- lingual or labial tippings of mandibular incisors,- buccal/labial translation,- labial/buccal root torque movements,- mesio-distal movements of a tooth in a narrowedentulous area,
- transversal expansion (Detienville et al., 1993;Fontenelle 1982; Maynard 1998).
155
4A
4B
Fig. 4 : éruption en ectopie palatine de la 13 avec atteintesparodontales sur 12 et 11.Palatally ectopic eruption of tooth 13 with periodontal affectionson teeth 12 and 11.A : aspect clinique de l’abcès parodontal.Clinical view of a periodontal abscess.B : aspect radiologique des lésions au niveau des racines des 12 et 11et du parodonte environnant.Radiography of lesions on the roots of 12 and 11 and surroundingperiodontium.

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
Tant que la dent est déplacée au sein de l’enveloppe duprocès alvéolaire, le risque d’effets secondaires défavorablessur les tissus mous est minimal (Wennström et coll.,1987) et la plupart des traitements orthodontiques n’ontpas d’effet néfaste sur le parodonte.Mais une canine avec un parodonte fin (ou en vestibulo-position) qui est déplacée distalement dans une zoneédentée plus étroite vestibulo-lingualement (par exemplele site d’extraction d’une 1ère prémolaire dont les paroisosseuses vestibulaires et linguales sont perdues)présentera souvent une perte d’attache et une dénudationradiculaire. Une hauteur adéquate de gencive attachéediminue la probabilité d’apparition de récession tissulaire.
En résumé, lors du déplacement mésio-distal d’une dent,l’orthodontiste doit évaluer la dimension vestibulo-lingualede la zone vers laquelle elle va être placée, sa positionvestibulo-linguale et la quantité de gencive attachée quil’entoure. Les mouvements orthodontiques qui éloignentles dents de l’enveloppe osseuse prédéterminée généti-quement risquent d’engendrer des lésions muco-gingivales,surtout au sein d’un morphotype fin.Au cours de l’expansion frontale et latérale des arcades,des tensions et compressions peuvent amincir les tissusmous. Si l’expansion aboutit à la formation d’une déhiscenceosseuse, la finesse des tissus mous de recouvrementdevient un facteur favorable à une récession gingivale(Zachrisson 1998).Les effets de l’expansion transversale ont été comparésselon la technique orthodontique employée sur despatients (âgés de 8 à 13 ans) de deux cabinets d’orthodontie(Vanarsdall et Herberger, 1987) :- 55 patients ont eu une expansion palatine rapide de10 à 10,5 mm en 3 semaines obtenue par un expanseurde Haas et les 30 autres patients ont été traités par unetechnique d’Edgewise sans expansion.Les données ont été évaluées entre 8 et 10 ans après lestraitements sur modèles, diapositives, céphalogrammesantérieurs et postérieurs, en pré- et post-traitementorthodontique.Les résultats à 10 ans indiquent que dans les casd’expansions stabilisées, 20 % présentaient des réces-sions vestibulaires sur une ou plusieurs dents (figure 5 AB),les patients traités par technique d’Edgewise présentaient6 % de récessions. Ainsi, chez les adolescents qui ontun petit maxillaire, le traitement orthodontique mobiliseprobablement les dents à travers l’enveloppe alvéolaireosseuse et prédispose à la récession gingivale. Cependant,des adultes non traités pour ce type de défauts transversauxprésentent souvent des récessions gingivales.Un traitement orthodontique précoce en denture lactéaleou mixte est donc idéal pour corriger orthopédiquementles anomalies squelettiques transversales car la croissanceest active et la séparation palatine est alors plus facile.
As long as a tooth is moved within the alveolar boneenvelope, the risk of unfavorable side effects on softtissues is minimal (Wennström et al., 1987) and mostorthodontic treatments have no fatal effect on periodontium.
When a canine with thin periodontium (or in buccalposition) is moved distally in a more labio-lingually narrowedentulous zone (for example the extraction site of a 1st
premolar whose buccal and lingual bones are lost), thetooth will often present an attachment loss and rootdenudation. An attached gingival of adequate heightdecreases the probability of tissue recession.
In summary, during mesio-distal movement of a tooth,the orthodontist must evaluate the bucco-lingualdimension of the area towards where the tooth will beplaced, its bucco-lingual position and the quantity ofsurrounding attached gingiva. Any orthodontic actionwhich moves away the teeth from the geneticallypredetermined supporting bone may cause muco-gingival lesions, especially within a thin morphotype.During frontal and lateral expansion of the arches, tensionand compression forces can result in thin soft tissues.While the expansion may lead to the formation of a bonedehiscence, thin covering soft tissue is a favorable factorcausing gingival recession (Zachrisson 1998).
The effects of transverse expansion were compared de-pending on the orthodontic technique used (on 8 to 13year-old patients) in two orthodontic clinics (Vanarsdalland Herberger, 1987):- 55 patients were treated with Haas expansion ap-pliances to obtain a rapid palatal expansion of 10-10.5mm in 3 weeks and 30 patients were treated by theEdgewise technique without expansion.The data were evaluated on models, slides and antero-posterior cephalograms and the pre-orthodontic treatmentresults were compared with those of post-orthodontictreatment between 8 and 10 years.The results at 10 years showed 20% of the cases withstabilized expansions presenting buccal or labial reces-sions on one or several teeth (figure 5AB) and 6% ofrecessions were found in the patients treated with theEdgewise technique. Therefore, in adolescents with asmall maxilla, the orthodontic treatment probably movesteeth through the supporting alveolar bone and predisposesto gingival recession. However, gingival recessions arealso often present in adults untreated for transverse defects.
An early orthodontic treatment in the primary or mixeddentition periods is thus ideal to orthopedically correctthe transverse skeletal anomalies because the palatalseparation is easier during active growth.
156

Revue d’Odonto-Stomatologie/Septembre 2011
Notion d’espace biologiqueet éruption passive :
Le respect de l’espace biologique parodontal est aussiune notion fondamentale que toutes les disciplinesodontologiques partagent. Ainsi, en orthodontie cetespace sera évalué afin de rétablir sa position et sa santé.
Les dimensions de l’espace biologique ont été mesuréespour la première fois par Gargiulo et coll. (1961). Ils ontanalysé les dimensions de la jonction dento-gingivaleselon les quatre stades de l’éruption passive. L’espacebiologique mesure en moyenne 2 mm. Ces notions s’ap-pliquent bien sûr à la canine. Chaque fois que cet espacebiologique sera altéré autour d’une canine, la positionparticulière de cette dent et la finesse de son systèmed’attache rendront plus difficiles et délicates les techniqueschirurgicales de reconstruction de cet espace et onfavorisera les techniques orthodontiques de reconstruction(égression, ingression associées ou non à une fibrotomiecirconférentielle).Si l’éruption passive s’interrompt, il s’agit alors d’uneanomalie de développement. Cette éruption passiveincomplète se manifeste cliniquement par le recouvrementd’une partie des couronnes dentaires par la gencive. Celamodifie l’harmonie dento-faciale car la partie visible desdents présente une forme carrée inesthétique. L’excès detissu mou tend à dépasser le bord inférieur de la lèvresupérieure, provoquant ainsi un sourire gingival prononcé.L’éruption passive altérée a été classée en deux typesdistincts (Coslet et coll., 1977) :- type I : hauteur excessive de gencive attachée
mesurée à partir de la gencive marginale libre à laligne muco-gingivale;
Biologic width andpassive eruption:
The respect for the biologic width is fundamental forpractices in all dental disciplines. In orthodontics, thiswidth must also be evaluated to restore to its positionand health.
The dimensions of the biologic width were measured forthe first time by Gargiulo et al. (1961) who analyzed thedimensions of the dentogingival junction during the fourstages of the passive eruption. The biologic width is onaverage 2 mm. in all teeth including canines. When thebiologic width around a canine is altered, a correctionwith surgical reconstruction techniques is more difficultand delicate due to the tooth particular position and thinperiodontal attachment system. Orthodontic reconstructiontechniques such as extrusion and intrusion associated ornot to circumferential supracrestal fibrotomy are thereforeprivileged.
An incomplete passive eruption occurs, due to aninterruption by an anomaly in development, resultingin clinically manifestations as a partial coverage of thetooth crowns by gingiva. The dento-facial harmony ismodified and the teeth are visible as unsightly square-shaped. The soft tissue excess extending beyond thelower border of the upper lip provokes therefore apronounced gingival smile.Two types of altered passive eruption can be distinguished(Coslet et al., 1977):- type I: excessive height of attached gingivameasured from the free marginal gingiva to themuco-gingival line;
157
5A
Fig. 5 : chez cette patiente âgée de 22 ans, 5 ans après le traitementorthodontique on peut voir :A : des récessions gingivales sur 23 et 64 (agénésie unique de la24) sur un parodonte fragile en présence d’un brossage vigoureux.B : résultat à 3 mois psot-opératoire du recouvrement radiculaire pargreffe de tissu conjonctif sous lambeau positionné coronairement.
5B
Fig. 5: 22-year-old patient, 5 years after orthodontic treatment.A: gingival recessions, probably due to strong toothbrushing, on teeth23 and 64 (unique agenesis of tooth 24) on a fragile periodontium.B: post-operative result at 3 months following to root coverageprocedure with connective tissue graft and coronally positionedflap.

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
- type II : hauteur normale de gencive attachéemesurée à partir de la gencive marginale librejusqu’à la ligne muco-gingivale.
Canine maxillaire etesthétique du sourire :
Sur le plan parodontal, nous savons qu’au cours d’un sourireforcé, la gencive est visible chez 89,06 % des patients(Cl I +II + III)(Liébart et coll., 2004). Aussi faut-ilintégrer cette notion dans l’esthétique finale du sourireaussi bien de face (figure 6A) que de profil (figure 6B).La gencive marginale de la canine sert aussi à dessinerla ligne gingivale qui est une tangente passant par lespoints les plus déclives des gencives marginales de l’incisivecentrale et de la canine maxillaire. L’angle mesuré entrecette tangente et la ligne inter incisive est d’environ 85°+/- 5° (Charruel et coll., 2008).Il est aussi important de noter que, dans les limites decette étude portant sur 103 adultes sains et jeunes, il aété montré une asymétrie systématique de cet angleentre le côté droit et le côté gauche. De plus, par rapportà cette ligne gingivale, la position du bord gingival del’incisive latérale maxillaire se situe toujours en retraitcoronaire d’environ 0,6 mm en moyenne. Les festonsgingivaux qui suivent la ligne des collets sont visibleschez environ 40 % des patients au cours d’un sourireforcé (Liébart et coll., 2004) et cela presque jusqu’auxpremières molaires maxillaires.
- type II: normal height of attached gingivameasured from the free marginal gingiva up to themuco-gingival line.
Maxillary canine andthe esthetics of a smile:
According to one of our studies, during a forced smile,the gingiva is visible in 89.06% of the participatedpatients (indicated as Classes I, II, III in the publication)(Liébart et al., 2004). This observation must thereforebe taken into account in the final esthetics of the smileboth on facial view (figure 6A) and profile view (figure6B) The gingival line is a slightly tangent line drawnconnecting the zenith of the marginal gingiva of themaxillary central incisors and canines. In a study on 103healthy young adults, the angle formed between the gin-gival line and the maxillary midline is about 85° +/- 5°(Charruel et al., 2008).
Moreover, within the studied population, an asymmetryof this angle between the right and left sides was shownto be systematic. Furthermore, the gingival margin zenithof the maxillary lateral incisors is always situated coronallyto this gingival line about 0.6 mm.The gingival embrasuresfollowing the cervical line are visible almost up to themaxillary first molars in approximately 40% of the studiedpatients during a forced smile (Liébart et al., 2004).
158
6A
Fig. 6 : le parodonte marginal de la canine est visible au cours d’unsourire forcé.A : de face un bandeau continue de 3 mm de gencive est visible,classes I de Parodontia (Liébart et al. 2004).B : de profil.
6B
Fig. 6: the canine marginal periodontium is visible during aforced smile.A: facial view, a continuous gingival band of 3 mm is visible,periodontium class I (Liébart et al. 2004).B: profile view.

Revue d’Odonto-Stomatologie/Septembre 2011
159
7A
Fig. 7 : la ligne gingivale est une tangente passant par le zénith desfestons gingivaux de l’incisive centrale et de la canine.A : en présence de fente de Stillman et de récessions gingivales,l’effet est dysharmonieux.B : après greffe de conjonctif enfoui sous un tunnel la ligne gingivaleredevient harmonieuse.
7B
Fig. 7: the gingival line is a tangent passing from the zenith ofscalloped gingival of central incisors and canines.A: dysharmonious gingival line in the presence of Stillman’scleft and gingival recessions.B: after buried tunnel connective tissue graft, the gingival linebecomes again harmonious.
Le tracé de ces festons gingivaux dessine une lignecontinue qui doit être harmonieuse à l’état naturel avecdes formes rondes et festonnées. Si les traitementsorthodontiques agissent sur la forme des festons gingivaux,ils doivent toujours respecter cette harmonie (figure7A). De plus, les techniques de recouvrement radiculairepeuvent participer à cette harmonie (figure 7B).L’esthétique des papilles de part et d’autre des caninesest fondamentale, leur absence (« trou noir ») étant trèsvisible surtout du côté mésial. Or la présence et la formedes papilles sont étroitement corrélées à la position dela dent dans les 3 sens de l’espace et ainsi à la positiondes points de contact proximaux (Tarnow et coll., 1992 ;Magne et Belser, 2004). Il faudra donc y apporter uneattention particulière lors de la mise en place orthodontique,de la réalisation de meulages proximaux pré-orthodon-tiques, mais aussi dans le cadre de toutes restaurationsconservatrice ou prothétique dento ou implanto-portée.
Application au traitementde la canine dystopique :
La connaissance du bien-fondé d’une architectureparodontale fonctionnelle et esthétique autour de la caninependant l’éruption, la croissance, la puberté et le traitementorthodontique motive de nombreuses interventions dechirurgie plastique parodontale chez l’enfant et l’adolescent(Monnet-Corti et Borghetti, 2000).L’indication majeure est la dent incluse et retenue enposition dystopique après avoir essayé de favoriser lesconditions d’éruption spontanée (extraction dent lactéale,espace sur l’arcade) (Richardson et Russell, 2000 ; Olive2002 ; Leite et coll., 2005) . Mais l’indication peut êtreétendue à l’interception d’éruption dystopique dans la
The tracing of gingival contour forms a continuous linewhich must be harmonious in natural appearance withround and scalloped pattern. Any orthodontic treatmentacting on the shape of the gingival contour must alwaysrespect this harmony (figure 7A). Furthermore, rootcoverage techniques can be used to improve this harmony(figure 7B).The mesial and distal interdental papillae of the caninesare fundamental to the esthetics since an absent papillawill form a highly visible (“black triangle”) especiallyon the mesial of the tooth. The presence and shape ofinterdental papillae are highly dependent on the toothposition in 3 dimensions and also to the position ofproximal contact points (Tarnow et al., 1992; Magne andBelser, 2004). A particular attention must be paid to thisstructure during orthodontic treatment, pre-orthodonticproximal stripping and also during any conservativerestorations or tooth- or or implant-supported prosthesis.
Application to the treatmentof ectopic canines:
The valid knowledge on function and esthetics of theperiodontal architecture surrounding the canine duringtooth eruption, growth, puberty and orthodontic treatmentshas lead to numerous procedures of periodontal plasticsurgery in children and adolescents (Monnet-Corti andBorghetti, 2000).The major indication for treatment with periodontalplastic surgery is impacted teeth retained in ectopicposition after attempts have been made to favor spontaneouseruption (extraction of deciduous tooth, creation ofspaces on the arch) (Richardson and Russell, 2000;Olive 2002; Leite et al., 2005). However, periodontal

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
muqueuse alvéolaire (vestibulaire au maxillaire etvestibulaire ou linguale à la mandibule) ou aux dépensdes racines des dents voisines (Monnet-Corti et Borghetti,2003). Il a été montré que 0,71 % des enfants de 10 à13 ans présentent des résorptions des racines des incisivespermanentes provoquées par une éruption ectopique descanines maxillaires (Ericson et Kurol, 1986 et 1987). Prèsde 80 % des dents concernées sont des incisives latérales(Bishara 1992).
L’inclusion peut être unilatérale ou bilatérale. La prévalenced’inclusion des canines est de l’ordre de 1 à 2 % de lapopulation (Bishara 1992 ; Dachi et Howell, 1961 ; Eric-son et Kurol, 1987b ; McKay 1978 ; Grover et Lorton,1985).Les inclusions touchent plus fréquemment la populationféminine (2 sur 3) que masculine, surtout pour les caninesmaxillaires (Becker et coll., 1983 ; Kuftinec et Shapira,1995a ; McKay 1978). Pour la canine maxillaire, l’inclusionpalatine (85 %) est plus fréquente que l’inclusion vestibulaireet 8 % de ces inclusions sont bilatérales (Bishara 1992 ;Quirynen et coll., 2000).En général, le dégagement chirurgical ne sera programméque lorsque l’arcade aura été préparée par un traitementorthodontique. La préparation concerne l’aménagementde l’espace nécessaire de la dent (Park et coll., 2004).
La préservation de la dent lactéale peut être motivée pardes demandes esthétiques de la part du patient (adolescentet adulte) et pour des raisons biomécaniques (maintiende l’espace mésio-distal et de la largeur vestibulo-palatinede la crête alvéolaire). Dans certaines circonstances, ilpeut s’avérer nécessaire d’extraire cette dent lactéale etde ménager l’espace suffisant pour laisser la possibilitéà la dent définitive de réaliser son éruption naturelle,son positionnement orthodontique et de disposer d’unezone de tissu kératinisé transposable par lambeaupositionné apicalement (LPA) ou lambeau positionnéapicalement et latéralement (LPLA).Pour la préparation de l’espace, les avulsions des prémolairesdoivent être différées jusqu’à l’évaluation de la probabilitéde réussite de la mise en place de la canine, de la duréedu traitement et de la motivation du patient (Thomine etcoll., 1995).L’objectif de l’orthodontiste est de réaliser l’éruption sansdistorsion du plan d’occlusion ni récession gingivale.Les objectifs du parodontiste sont de procurer un accèsdirect à la couronne clinique, d’effectuer un dégagementostéo-muqueux suffisant pour le collage du verrou or-thodontique, de déplacer les tissus pour recréer une ana-tomie parodontale normale et/ou compatible avec lemaintien de la santé parodontale et ainsi de provoquerchirurgicalement une émergence dans un site dystopique.Les lambeaux d’accès font référence aux travaux de
plastic surgery is indicated for an interception of ectopiceruption in alveolar soft tissue (buccal/labial in themaxilla and buccal/labial or lingual in the mandible) orwhen the impaction causes root resorption on the adjacentteeth (Monnet-Corti and Borghetti, 2003). It was shownthat 0.71% of 10 to 13-year-old children presentresorptions on the roots of permanent incisors causedby an ectopic eruption of the maxillary canines (Ericson andKurol, 1986 and 1987). About 80% of the concernedteeth are lateral incisors (Bishara 1992).The impaction can be unilateral or bilateral. The preva-lence of impacted canines is in the order of 1-2% of thepopulation (Bishara 1992; Dachi and Howell, 1961;Ericson and Kurol, 1987b; McKay 1978; Grover andLorton, 1985).The impaction occurs more frequently in female (2 outof 3) than male, especially for maxillary canines(Becker et al., 1983; Kuftinec and Shapira, 1995a;McKay 1978). For maxillary canines, palatal impaction(85%) is more frequent than buccal impaction and 8% ofthese impactions are bilateral (Bishara 1992; Quirynen etal., 2000).Generally, a surgical exposure will be scheduled onlywhen the dental arch is already prepared by an orthodontictreatment. The preparation concerns the management ofthe space required for the tooth (Park et al., 2004).
The retained deciduous tooth can be preserved foresthetic reason requested by the patient (adolescent andadult) and for biomechanical reasons (maintenance ofthe mesio-distal space and the bucco-palatal width ofthe alveolar crest).In certain circumstances, the deciduous tooth must beextracted to obtain a space suff icient for a naturaleruption and orthodontic positioning of the permanenttooth and a keratinized tissue transposable by apicallypositioned flap (APF) or laterally and apically positionedflap (LAPF).
For space preparation, the extraction of premolars mustbe postponed until obtaining an evaluation result on thesuccess of the canine positioning, treatment durationand patient’s motivation (Thomine et al., 1995).
The treatment goal of the orthodontist is to achieve theeruption without altering the occlusion or creating gingivalrecession. The periodontist’s roles are to obtain a directaccess to the clinical crown, perform a bone-soft tissueexposure sufficient for bonding of an orthodonticbracket to the tooth crown, transpose soft tissue torecreate a normal periodontal anatomy compatible withperiodontal health maintenance and also surgically exposethe tooth crown in an ectopic site.The access flaps can refer to (font référence aux) the
160

Revue d’Odonto-Stomatologie/Septembre 2011
Korbendau et Guyomard (1980 et 1998). Les différentestechniques de dégagement chirurgical d’une dent inclusesont :- en vestibulaire : la gingivectomie, le lambeau
vestibulaire repositionné, le lambeau positionnéapicalement (LPA) (Borghetti et Monnet-Corti, 2008),le lambeau positionné latéralement et apicalement(LPLA)(figure 8 ABCDE);
works of Korbendau and Guyomard (1980 and 1998).Different surgical exposure techniques of an impactedtooth are:- buccal approach: gingivectomy, repositionedvestibular flap, apically positioned flap (APF)(Borghetti and Monnet-Corti, 2008), laterally andapically positioned flap (LAPF) (figure 8 ABCDE);
161
8A
Fig. 8 : patiente âgée de 14 ans. La canine maxillaire droite estincluse et retenue en position vestibulaire entre la racine de la 12et de la 11. Dégagement chirurgical 13 incluse et retenue endystopie haute par lambeau positionné apicalement et latéralement( LPLA).14-year-old patient. The right maxillary canine is impacted andretained in buccal position between the roots of teeth 12 and 11.Surgical exposure of the impacted 13 retained in a high ectopicposition using a laterally and apically positioned flap (LAPF).A : vue clinique.Clinical aspect.B : aspect radiologique sur orthopantomogramme.Orthopantomogram.C : élimination d’un volet de muqueuse alvéolaire permettantd’accéder à la couronne clinique de la 13.A soft tissue window is made through alveolar mucosa to accessthe clinical crown of tooth 13.D : dissection d’un lambeau d’épaisseur partielle situé en distl dela 12 au niveau du site d’extraction de la 53.Dissection of a partial-thickness flap situated on the distal of tooth12 at the extraction site of tooth 53.E : déplacement apical et latéral et sutures résorbables du lambeau.Apical and lateral displacement and flap closure with resorbablesutures.F : Après 18 mois, mise en place de la dent avec un parodontesain.After 18 months, the tooth is repositioned with a healthyperiodontium.
8B 8C
8D 8E
8F

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
- en palatin : le lambeau palatin repositionné fenêtré(figure 9ABCDEF) ou non.
- palatal approach: repositioned palatal flap with(figure 9ABCDEF) or without soft tissue window.
162
Fig. 9 : patiente âgée de 14 ans. Les deux canines maxillaires sontincluses et retenues en position palatine pour la 13 et alvéolairepour la 23.14-year-old patient. Both maxillary canines are impacted, palatalposition for tooth 13 and alveolar position for tooth 23.A : les 53 et 63 sont toujours en place.Teeth 53 and 63 are still in position.B : élévation d’un lambeau d’épaisseur totale palatin de 14 à 24.Noter la proximité de la face vestibulaire de 23 avec la paroiradiculaire palatine de la 22.Elevation of a full-thickness flap from teeth 14 to 24. The proximityof the buccal surface of tooth 23 with the palatal root of tooth 22 isnoted..C : le dégagement minutieux à l’aide d’instrument manuel se faitsans risque parodontal aux dépends de l’os palatin péri-coronaire.A meticulous exposure using a manual instrument is made withoutperiodontal risk by removing the palatal bone surrounding the toothcrown.D : sutures du lambeau et réalisation de fenêtres muqueuses permet-tant l’accès direct aux couronnes cliniques des 13 et 23.Sutures of the flap and soft tissue removal creating windows fora direct access to the crowns of teeth 13 and 23.E : aspect de la santé parodontale autour de 22 et 23 au cours dumouvement orthodontique.Periodontal health surrounding teeth 22 and 23 in the courseof orthodontic movement.F : qualité du parodonte autour de la 23 à la fin de sa mise en placeet en fonction.Quality of the periodontium around tooth 23 at the end of itsrepositioning and in function.
9A 9B
9C 9D
9E
9F

Revue d’Odonto-Stomatologie/Septembre 2011
Le dégagement par lambeau positionné apicalement estl’abord de choix dans de nombreuses situations. Le LPAa pour objectif de créer ou de maintenir du tissu kératiniséautour de la dent à dégager par déplacement apical dutissu kératinisé existant. Les indications du LPLA sontles mêmes que celles du LPA sauf que la position de ladent est latérale par rapport à la gencive kératiniséedisponible sur la crête édentée ou autour d’une dentadjacente. Le site donneur peut être une crête édentée(cas le plus simple) ou les tissus vestibulaires des dentsadjacentes.La technique recommandée en présence d’inclusionpalatine est le lambeau palatin repositionné. Le succèsde la mise en place des dents incluses repose sur un bonaccès à la couronne clinique, en respectant la jonctionamélo-cémentaire, la présence de tissus de soutien sainset de bonne qualité et, enfin, un bon positionnementsur l’arcade.Certaines études ont recherché les effets de l’alignementde canines incluses au maxillaire sur l’état parodontal etont montré la présence de récessions gingivales pour lesinclusions vestibulaires (Wisth et coll., 1976) et de perted’attache pour les inclusions palatines (Becker 1984 ;Kohavi et coll.,1984). L’expérience clinique montre quele tissu marginal ainsi recréé par les techniques dechirurgie plastique parodontale résiste au sondage et eststable dans le temps (figure 9F). Selon Korbendau etGuyomard (1983), la gencive attachée suit la dent dansses déplacements. La gencive est située au même niveauque les dents voisines, ne présente pas de modificationde hauteur et conserve des épaisseurs et qualités d’unparodonte en bonne santé en fin de traitement ortho-dontique (Caminiti et coll., 1998 ; Ling et coll., 2007).
Dans certains cas, la dent est immobile. Cela peut être dûà un dégagement osseux insuffisant, une tractionorthodontique inadéquate ou une ankylose. Fleury etcoll. (1985) ont rencontré 28 % de dents ankylosées sur224 canines maxillaires incluses. Cependant, 77 % de cesdents ont été traitées après l’âge de 21 ans. L’absence demouvement de la dent soumise aux forces orthodontiquesest plus fréquente lors d’inclusions palatines.
Quatre étiologies peuvent l’expliquer (Park et coll., 2004) :
- une élimination chirurgicale de l’os péricoronaireinsuffisante;
- une orientation inappropriée des forces orthodontiques;- une ankylose;- un collage de l’attache à la surface osseuse.Face à ces situations, la plupart du temps, l’extractions’impose avec plus ou moins de difficulté liée à l’ampleurde l’ankylose et à la volonté de minimiser les dégâts pa-rodontaux per et post-opératoires.
A surgical exposure by apically positioned flap is theaccess of choice in numerous situations. APF is used tocreate or maintain some keratinized tissue around thetooth to be exposed by apical displacement of the existingkeratinized tissue. The indications of LAPF are the sameas those of APF except that the tooth position is lateralwith regard to the keratinized gingiva available on theedentulous crest or around an adjacent tooth. The donorsite can be an edentulous crest, which is the simplestcase, or the buccal/labial tissues of adjacent teeth.
The recommended technique in the presence of palatalimpaction is a repositioned palatal flap. The successrepositioning of an impacted tooth is based on an adequateaccess to the tooth crown respecting the cemento-enamel junction, the presence of healthy and good qualitysupporting tissues and, finally, a proper tooth positioningon the arch.Certain studies evaluated the effects of the alignment ofimpacted canines in the maxilla on the periodontal statusand showed the presence of gingival recessions for buccal ?impactions (Wisth et al., 1976) and loss of attachmentfor palatal impactions (Becker 1984; Kohavi et al.,1984). From clinical experience, it has been shown thatthe marginal tissue recreated by periodontal plastic surgerytechniques resists probing and is stable over time(figure 9F). According to Korbendau and Guyomard(1983), the attached gingiva will follow the tooth in itsmovements (displacements) to be situated at the samelevel as that of the neighboring teeth. It does not presentany modification of height and preserves the thicknessesand qualities of a healthy periodontium at the end oforthodontic treatment (Caminiti et al., 1998; Ling et al.,2007).In certain cases, the impacted tooth cannot be moveddue to an insufficient bone exposure, an inadequateorthodontic traction or an ankylosis. Fleury et al. (1985)found 28% of ankylosed teeth on 224 impacted maxil-lary canines. However, 77% of these teeth were treatedafter the age of 21 years. An absence of tooth movementsubjected to orthodontic forces is more frequent in palatalimpactions.
Four etiologies can explain it-the failure of tooth movement(Park et al. 2004):- insufficient surgical removal of the bone surroundingthe tooth crown;
- inappropriate orientation of orthodontic forces;- ankylosis of deciduous teeth;- bonding of an attachment on the bone surface.Facing to this situation, most of the time, an extraction(of which tooth? Deciduous or permanent tooth) is obli-gatory with more or less difficulty related to the extentof ankylosis and the operator’s will to minimize per andpost-operative periodontal damages.
163

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
Restauration ou remplacementde la canine, les contraintes cliniques :
Le remplacement d’une canine absente implique un choixthérapeutique qu’il faudra décider en équipe et avec leconsentement éclairé du patient majeur ou des parentsd’un mineur.La restauration peut être conservatrice (coronoplastie,restauration plastique, facette) ou prothétique (coiffe,bridge ou implant).Ce remplacement relève d’une problématique globale car,outre sa position stratégique dans la courbure de l’arcadeentre secteur antérieur et postérieur, cette dent présentedes particularités dans tous les domaines.
• Morphologie fonctionnelle (figure 10) :La fonction cinématique de guidage latéral mandibulairedépend de la morphologie de la face palatine de la caninemaxillaire.
Si l’on note une nette stabilité de la morphologie vestibulaire,il existe une variabilité de la morphologie linguale de lacanine. Ces variations d’une zone essentielle sur le planfonctionnel sont suffisamment importantes pour en tenircompte sur le plan clinique (El Zoghby et coll., 2010).On sait que l’inclinaison des faces linguales, par rapportau plan axio-orbitaire, diminue nettement de 10º en allantde l’incisive centrale (57º) à la canine (47º) (El Zoghbyet coll., 2010).Ces données, initiées par les travaux de Slavicek en 1983,permettent au clinicien généraliste ou orthodontiste des’appuyer sur des bases anatomiques pour la restitutionde cette fonction.Il y aura fonction canine lorsque seule la canine assure
Restoration or replacement ofa canine, clinical constraints:
Replacement of an absent canine is a treatment choicewhich must be decided in a teamwork approach andinformed consent must be obtained from patients over18 years old or parents of the patients under 18 years old.A restoration involving canines or on canine positions can beconservative (tooth crown reduction and recontouring,composite resin restoration, veneer) or prosthetic (crown,bridge or implant).Its replacement is globally problematic. Besides its strategicposition in the arch curvature between anterior and posteriorsegments, this tooth presents several specificities.
• Functional morphology (figure 10):The kinematics during lateral translation of the mandibledepends on the palatal surface morphology of the maxil-lary canines.
Although a constant buccal morphology of the caninescan be evidently noted, there is a variability of thelingual/palatal morphology. From a functional point ofview, these variations are sufficiently significant to beclinically taken into account (El Zoghby et al., 2010).The slope angulations of the palatal surfaces of maxil-lary anterior teeth with regard to the axio-orbital planeevidently decreases by 10º from central incisors (57º) tocanines (47º) (El Zoghby et al., 2010).These data, initiated by the works of Slavicek in 1983,allow general clinicians or orthodontists to use anatomicalbases for the restoration of its guiding function.An occlusion is called canine-guided function or canineprotectionwhen only the canines ensure lateral excursions of
164
10
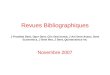
Fig. 10 : paramètres généraux prothétiques de la canine : anatomiede la face palatine, âge, carrefour entre les contraintes postérieureset antérieures (1), profil d’émergence (2), embrasure occlusale (3),position de la pointe (4), ligne des collets (5).General prosthetic parameters of the canine: palatal surfaceanatomy, age, junctions between posterior and anterior stresses (1),emergence profile (2), occlusal embrasure (3), position of the cusptip (4), cervical line (5).

Revue d’Odonto-Stomatologie/Septembre 2011
la fonction latérale et fonction de groupe lorsque d’autresdents participent à cette fonction (ce type de guidageest d’autant plus fréquent que le système dentaire vieil-lit), et, c’est l’analyse clinique des différents paramètresfonctionnel, biologique et esthétique qui induira le choixde la morphologie à restituer ou à créer.
• Position de la pointe, profil d’émergence et naturedu parodonte (figure 11ABCDE) :
L’anatomie fonctionnelle de la face palatine déterminantla position de la pointe, celle-ci se trouve souvent lingualéepar rapport au bord libre des incisives latérales maxillaireset des pointes cuspidiennes des premières prémolaires.Il en découle une forme aplatie de la face vestibulaire enrapport avec un profil d’émergence présentant un faiblebombé cervical, provoquant une contrainte directe dubol alimentaire sur un parodonte de biotype fragile(figure 12 ABC). La bosse canine est une constanteparodontale qui repose essentiellement sur le volume dela racine et non pas sur une quantité excessive des tis-sus parodontaux vestibulaires (la table externe osseuse,
the mandible, and called group function when the otherteeth participate in this movement. This latter type ofocclusion is all the more frequent in ageing dentition. Aclinical analysis of various functional, biological andesthetic parameters will then lead to the choice of themorphology to be restored or to be created.
• Position of the canine cusp tip, emergence profileand nature of the surrounding periodontium (figure11ABCDE):
The functional anatomy of the palatal surface determiningthe position of the cusp point which is often located linguallywith regard to the incisal edge of maxillary lateral incisorsand the cusp tips of maxillary first premolars.A flat buccal surface with an emergence profile of slightcervical convexity of the canines provokes a directcontact of the food bolus on a fragile periodontal biotype(figure 12 ABC). The canine prominence is a periodontalcharacteristic which is essentially based on the canineroot size and not an excessive quantity of buccal periodontaltissues since the external cortical bone, periodontalligament and gingiva are found to be the thinnest at this
165
Fig. 11 : anatomie de la face palatine de lacanine maxillaire. AB : réduction enrespectant les différents plans. C : réductionhomothétique mise en évidence par la cléen silicone.D : profil d’émergenceet positionde la pointe. E : réduction homothétiquepermet une épaisseur constante céramo-métallique reconstruisant l’anatomienaturellede la caninePalatal surface anatomy of the maxillarycanine.AB: reduction by respecting differentplanes.C: homothetic reduction shown by asilicone index. D: emergence profile andposition of the cusp tip. E: homotheticreduction allows a proper metal-ceramicthickness reconstructing the natural anatomyof the canine.
11A 11B 11C
11D 11E

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
le ligament et la gencive présentent les épaisseurs lesplus fines à cet endroit). Les effets du vieillissementparodontal seront visibles à cause de la possible migrationapicale du bord gingival libre. La position de la gencivemarginale prédispose à l’harmonie de la ligne des collets(figure 13).Pour toutes ces raisons et selon le biotype parodontalinitial, les difficultés cliniques de reconstruction pourrontindiquer des préparations corono-périphériquesscrupuleusement homothétiques ainsi qu’une augmentationde l’épaisseur des tissus parodontaux.
place. The effects of periodontal ageing will be visibledue to possible apical migration of the free gingival margin.The position of the marginal gingiva participates in theharmony of the gingival cervical line (figure 13).
These above-mentioned reasons together with the initialperiodontal biotype present clinical diff iculties inreconstruction of canines. Scrupulous preparations ofhomothetic full crowns as well as an increase of theperiodontal tissue thickness can be indicated.
166
Fig. 12 : Mr C. 27 ans, souhaite une réhabilitation occluso-fonc-tionnelle et esthétique. A : il présente les symptômes d’une amé-logènèse « imparfaite » associée à une hygiène bucco-dentaireinsuffisante. B : les préparations respectent l’homothétie et laposition des pointes canines. C : l’ anatomie des faces vestibulairespeut être respectée grâce à l’homothétie des restaurations. CoiffesImpress Laboratoire W. Pertot.Mr C., 27 years old, requests for an occluso-functional andesthetic rehabilitation. A: oral examination showing an amelo-genesis“imperfecta” associated with insufficient oral hygiene.B:tooth homothetic preparations and the canine cusp tip position arerespected. C: the anatomy of buccal surfaces is respected withhomothetic restorations. Impress crowns, LaboratoryW. Pertot.
12A
12B
12C
13
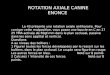
Fig. 13 : paramètres prothétique de l’environnement parodontal :âge, biotype parodontal (1), bosse canine (2), table externe (3), lignedes collets (4), embrasure et papille (5).Prosthetic parameters of the periodontal environment: age,periodontal biotype (1), canine prominence (2), external corticalbone (3), cervical line (4), embrasure and interdental papilla(5).

Revue d’Odonto-Stomatologie/Septembre 2011
• Problématique du remplacement de la canine absenteou déplacée :Le remplacement d’une canine absente par un bridge surdents naturelles pose le problème de sa pérennité en rap-port avec sa destruction tissulaire. Le bridge collé sur leslatérales et les prémolaires peut être une solution d’at-tente pendant la croissance jusqu’à l’âge adulte mais enaucun cas une solution durable.
La réalisation de préparation corono-périphérique surdents vitales s’avère mutilante et moins indiquéeaujourd’hui. De plus, sur le plan biomécanique, l’incisivelatérale présente un indice de Le Huche et une surfaceradiculaire beaucoup plus défavorable que la premièreprémolaire (Ogolnik 1993).Ainsi, en présence d’organes dentaires sains, la solutionde choix réside dans la mise en place d’un implant(figure 14 ABCD).Cependant, c’est une solution quipeut s’avérer complexe à mettre en œuvre du fait del’anatomie osseuse résiduelle, de la présence de concavitéosseuse maxillaire, de la finesse de la table osseuseexterne. La dimension de la crête édentée va permettrela stabilité primaire de l’implant et va guider le position-
• Problematic replacement of a missing or displacedcanine:The replacement of a missing canine with a bridge onnatural teeth raises the problem of its longevity relatedto natural tooth tissue destruction. A bonded bridge onlateral incisors and premolars can be a temporary solutionduring the growth until the adulthood (pendant la crois-sance jusqu’à l’âge adulte) but on no account a long-term solution.
Full crown preparation on vital teeth is considereddamaging to tooth tissue and presently less indicated.Furthermore, biomechanically (from a biomechanicalpoint of view), lateral incisors present a Le Huche’sindex and radicular surface much less favorable thanfirst premolars (Ogolnik 1993).In the presence of healthy tooth tissue, the solution ofchoice is therefore an implant placement (figure 14ABCD). However, this solution can be complex tooperate because of the residual bone anatomy, the presenceof maxillary bone concavity and thin external corticalbone. The dimension of the edentulous bone crestinfluences the primary implant stability and will guidethe implant positioning for the proper emergence profile.
167
Fig. 14A : patiente âgée de 45 ans, avec un biotype parodontal fin et fragile, a reçuune greffe gingivale libre sur 13 quelques années auparavant. Elle souhaitel’alignement des collets dentaires et présente des problèmes endodontiquesmajeurs. L’esthétique des céramiques très opaques ne lui convient plus. La 13présente une fracture verticale totale. B : extraction de la 13 et mise en place d’unimplant (FNT Biomet 3i de diamètre 4mm et de longueur 13mm) immédiatementavec un inlay core Zi-RéAl Biomet 3i. C : céramiques sur Zircon, laboratoire J.LKraft. Noter la difficulté du positionnement cervical au sein de la gestion des tis-sus.D : la patiente ne découvre pas la totalité de ses festons gingivaux au cours dusourire.A: 45-year-old patient, with a thin and fragile periodontal biotype, treatedwith a free gingival graft 13 years ago. She requested for a treatment for thealignment of the cervical line and endodontic problems. Highly opaque porcelainrestorations are not esthetic to her and need a correction. Tooth 13 presentsa total vertical fracture.B: extraction of tooth 13 and placement of an implant (FNTBiomet 3i, 4mm diameter and 13mm length) and an immediate Zi-Real abutment(Biomet 3i). C: zircon-based ceramics, laboratory J.L Kraft. The difficulty ofcervical positioning in the prepared soft tissues is noted. D: the totality ofscalloped gingival is not shown during the smile.
14A 14B 14C
14D

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
nement pour le profil d’émergence. De plus, l’esthétiquedu parodonte devra s’approcher le plus possible des dentsadjacentes en terme de couleur, forme de contour, positionde la gencive marginale ainsi que la présence souhaitablede papille. Enfin la bosse canine, particularité anatomiquede cette dent devra être recréée par des greffes de tissusosseux (préalables à l’implantation) et /ou de tissu mou(figure 15ABCD).
• Traitement de l’agénésie de la latérale : cas particulierdes canines mésialées (figure 16 ABCDE).
Le traitement prothétique des agénésies pose souventd’importants problèmes et notamment des problèmesesthétiques.
Furthermore, the periodontium esthetics must approachas much as possible that of adjacent teeth in terms ofcolor, contour, position of the marginal gingiva as wellas a desirable presence of interdental papilla. Finally thecanine prominence, the anatomical specificity of thistooth, must be recreated by bone grafts (prior to implantplacement) and/or tissue grafts (figure 15ABCD).
• Treatment of maxillary lateral incisior agenesis:particular case ofmesialized canines (figure 16ABCDE).
A prosthetic treatment of ageneses often presents pro-blems particularly in esthetics.
168
Fig. 15A : Mme G. 64 ans, suivie depuis 20 ans. Souhaite rétablirl’esthétique des collets dentaires.Mrs G., 64 years old, followed for 20 years, requests for an estheticrestoration of the tooth cervical.
15A 15B
15C 15D
Fig. 15B : elle présente une parodontite chronique stabilisée avec denombreuses récessions parodontales sur parodonte de type III deMaynard et Wilson, 1980 et des lésions cervicales d’usure.An oral examination shows a stabilized chronic periodontitis withnumerous periodontal recessions on type III periodontium accordingto the classification by Maynard andWilson (1980) and cervicalabrasions.
Fig. 15CD : après une greffe de tissu conjonctif enfoui et la mise enplace de céramiques sur Zircon, Laboratoire JL Kraft.After a buried connective tissue graft and placement of Zircon-based ceramic Laboratory JL Kraft.

Revue d’Odonto-Stomatologie/Septembre 2011
Le maintien de la canine en « normoposition » obligerale clinicien à remplacer prothétiquement l’incisive latéralemanquante. Ceci pourra se faire par :- la prothèse conjointe traditionnelle, ce qui ne manquerapas de poser des problèmes de mutilation et d’esthétiqueà long ou moyen terme ;
If the canine must be maintained in its “normal position”,the clinician will be obliged to prosthetically replace themissing lateral incisor by:- conventional fixed prosthesis, what will create problemsof tooth tissue destruction and esthetics at middle orlong term;
169
Fig. 16A : agénésie des incisives latérales maxillaires et remplacéespar les canines maxillaires. Fin du traitement orthodontique (Dr. JSSimon).Agenesis of the maxillary lateral incisors replaced by maxillarycanines. End of orthodontic treatment (Dr. JS Simon).
16A
Fig. 16B : la transformation des canines en incisives latérales consisteà couper les pointes canines, construire à la résine composite des an-gles mésial et distal du bord libre, réduire le bombé vestibulaire, ré-duire le cingulum et réduire la cuspide palatine de la premièreprémolaire.The transformation of canines into lateral incisors consists in grin-ding the canine cusp tips, building of the mesial and distal angles ofthe incisal edge with composite resin, reducing the buccal convexity,reducing the cingulum and reducing the palatal cusp of the first pre-molar.
16B
16C
Fig. 16C : aspect final de face.Final facial view.
16D
Fig. 16DE : de profil.Profile view.
16E

Revue d’Odonto-Stomatologie/Septembre 2011
PARODONTIE
- la prothèse implantaire, qui semble très séduisante aupremier chef, mais qui peut poser un grand nombre dedifficultés liées à l’anatomie de l’os résiduel, du parodontemarginal ou à l’esthétique.La mésialisation de la canine qui va permettre la fermeturedes espaces va, quant à elle poser des problèmes esthétiquesliés à l’anatomie particulière de la canine, ainsi que desproblèmes occlusaux liés à l’altération de la « fonctioncanine » (Manière-Ezvan et coll. 2006).Quelle que soit la décision thérapeutique multifactorielle(esthétique, fonctionnelle, économique, psychologique),la notion de compromis demeure omniprésente.La présentation de différentes situations cliniques mettraen évidence les résultats esthétiques et fonctionnels quesont en droit d’attendre nos patients. Lorsque l’optionde mésialer des canines a été retenue, des odontoplastiesadditives et soustractives permettront de transformer laprémolaire en canine par meulage de la pointe cuspidiennepalatine, la fermeture des embrasures occlusales, laréduction du bombé vestibulaire, et enfin la réductiondu cingulum de la canine afin de pouvoir organiser lesrapports d’occlusion.
- implant-supported prosthesis, which primarily seemsvery attractive but can put a large number of difficultiesrelated to the residual bone anatomy, marginal periodontiumor esthetics.Space closure with canine mesialization, however, cancause esthetic problems due to the particular canine anatomyand problems of occlusion from a modif ication of“canine-guided function” (Manière-Ezvan et al. 2006).
Although a treatment decision for canines must be basedonmultifactorial approaches (esthetic, functional, economic,psychological), a compromise attitude remains ubiquitous.A presentation of different clinical situations willdemonstrate the esthetic and functional results that thepatients can expect.When canine mesialization is adopted,additive and subtractive odontoplasties will transformthe premolars into canines by grinding the palatal cusptip, closing occlusal embrasures, reducing the buccalconvexity, and finally reducing the canine cingulum inorder to adjust occlusal relationships.
170
Toutes les techniques de reconstruction mises en œuvre présenteront des compromis esthétiques etfonctionnels tant il est complexe de restaurer ou de reproduire à l’identique une canine absente, perdue ou lésée.C’est pour cette raison que, lorsque la clinique ne l'impose pas, il faut y toucher le moins possible, implanter avecprudence et surtout anticiper par des thérapeutiques ortho-parodontales préventives.
A restoration or reproduction of a missing, lost or destructed canine to its original form is so complex thatany reconstruction techniques will present esthetic and functional compromises. Consequently, when the clinicalcondition does not require, the canines should be the least altered.An implant placement in this position must beperformed with caution. Treatments of impacted canines must be especially anticipated with preventiveorthodontic/periodontal approaches.
Traduction : Ngampis SIX
Conclusion
Demande de tirés-à-part :Virginie Monnet-Corti - 44, Bd Tristan Corbière - 13012 Marseille

BECKERA., KOHAVI D., ZILBERMANY.Periodontal status following the aligment of palatallyimpacted canine teeth. Amer J Ortho 1983;84:332-336. Cat 1
BECKERA.Etiology of maxillary canine impactions.Amer J Ortho 1984;86:437-438. Cat 4
BENOIT R., GENON P.Indications des thérapeutiques muco-gingivales chez l’enfantet l’adolescent. Rev Dent Stomato 1985;3:173-196. Cat 3
BISHARA S.E.Impacted maxillary canines: a review.Amer J Ortho Dentofac Orthop 1992;101:159-171. Cat 3
BORGHETTI A. ET MONNET-CORTI V.Lambeau positionné apicalement. In : Chirurgie Plastiqueparodontale. Borghetti A et Monnet-Corti V, Ed: CdP Paris,2008:143-160. Cat 3
CAMINITI M.F., SANDOR G.K., GIAMBATTISTINI C.,TOMPSON B.Outcomes of the surgical exposure, bonding and eruption of82 impacted maxillary canines.J Canad Dent Ass 1998;64:572-579. Cat 1
CHARRUEL S., PEREZ C., FOTI B., CAMPS .,MONNET-CORTI V.Gingival contour assessment: clinical parameters useful foresthetic diagnosis and treatment.J Periodont 2008;79:795-801. Cat 1
COSLET J.G., VANARSDALL R., WEISGOLDA.Diagnosis and classification of delayed passive eruption ofthe dentogingival junction in the adult. Alpha Omega1977;70:24-28. Cat 3
DACHI S.F., HOWELL F.V.A survey of 3,874 routine full mouth radiographs.Oral Surg 1961;14:1165-1169. Cat 1
DETIENVILLE R., SAUVAN J.L., JEANNE C.Chirurgie muco-gingivale et éruption dentaire.J Parodont 1993;12:163-174. Cat 3
EL ZOGHBYA., RÉ J.P., PEREZ C., GIRAUDEAUA.,ORTHLIEB J.D.Canine et incisive maxillaires : mieux connaître lamorphologie pour optimiser la fonction.Rev Orthop Dentofac 2010;11:47-61. Cat 4
ERICSON S., KUROL J.Longitudinal study and analysis of clinical supervision ofmaxillary canine eruption.Commun Dent Oral Epidem 1986;14:172-176. Cat 1
ERICSON S., KUROL J.Incisor resorption caused by maxillary cuspids.A radiographic study. Angle Orthodont 1987a;57:332-346.Cat 1
ERICSON S., KUROL J.Radiographic examination of ectopically erupting maxillarycanines. Amer J Ortho Dentofac Orthop 1987b;91: 483-492.Cat 1
Revue d’Odonto-Stomatologie/Septembre 2011
171
FLEURY J.E., DEBOETS D., ASSAD-AUCLAIR C.,MAFFRE N., SULTAN P.La canine incluse : mise au point à propos de 212 observations.Principes généraux de traitement.Rev Stomato Chir Maxillofac 1985;86:122-131. Cat 4
FONTENELLEA.Une conception parodontale du déplacement dentaireprovoqué : vers une application clinique raisonnée.J Parodont 1982;1:131-155. Cat 4
GARGIULOA.W., WENTZ F.M., ORBAN B.Dimensions and relations of the dentogingival junction inhumans. J Periodont 1961;32:261-267. Cat 1
GROVER P., LORTON L.The incidence of unerupted permanent teeth and relatedclinical cases. Oral Surg 1985;59:420-424. Cat 4
KOHAVI D., BECKERA., ZILBERMANY.Surgical exposure, orthodontic movement, and final toothposition as factors in periodontal breakdown of treatedpalatally impacted canines. Amer J Ortho 1984;85:72-77.Cat 1
KOKICH V.G.Surgical and orthodontic management of impacted maxillarycanines. Amer J Ortho Dentofac Orthop 2004;126: 278-283.Cat 3
KORBENDAU J.M., GUYOMARD F.Apport de la chirurgie parodontale à la mise en place descanines en dystopie vestibulaire.Rev Orthop Dentofac 1980;14:459-477. Cat 3
KORBENDAU JM, GUYOMARD F.Mise en place des incisives retenues : problèmesmuco-gingivaux et remaniements tissulaires.J Parodont 1983;2:7-29. Cat 3
KORBENDAU J.M., GUYOMARD F.Chirurgie parodontale orthodontique.Ed: CdP Paris, 1998:65-218. Cat 3
KUFTINEC M.M., SHAPIRAY.The impacted maxillary canine. I. Review of concept.J Dent Child 1995a;62:317-324. Cat 3
LEITE H. DE R., OLIVEIRAG.S., BRITO H.H.Labially displaced ectopically erupting maxillary permanentcanine: interceptive treatment and long-term results.Amer J Orthod Dentofacial Orthop 2005;128:241-251. Cat 4
LIEBART MF, FOUQUE-DERUELLE C, SANTINI A,DILLIER F.L., MONNET CORTI V., GLISE, J.M.,BORGHETTI A.Smile line and periodontium visibility.Periodont Pract today 2004;1:17-25. Cat 1
LING K.K., HO C.T., KRAVCHUK O., OLIVE R.J.Comparison of surgical and non-surgical methods of treatingpalatally impacted canines. I. Periodontal and pulpaloutcomes. Aust Ortho J 2007;23:1-7. Cat 1
MAGNE P., BELSER U.Novel porcelain laminate preparation approach driven by adiagnostic mock-up. J esthet restor dent 2004;16(1):7-16.Cat 4
Bi
bl
io
gr
ap
hi
e

MANIERE-EZVAN D., BROCARD J., SCHITTLY J.-D.,ORTHLIEB J. D.Occlusodontie pratique. Une approche clinique rationnelle.EDP Sciences – Ed: SID 2006. Cat 3
MAYNARD J.G., OSCHENBEIN C.Mucogingival problems, prevalence and therapy in children.J Periodont 1975;46:543-552. Cat 4
MAYNARD J.G., WILSON R.D.Diagnosis and management of mucogingival problems inchildren. Dent Clin N Amer 1980;24:683-703. Cat 4
MAYNARD J.G.Mucogingival considerations for the adolescent patient.In: Nevins M, Mellonig JT (eds). Periodontal therapy:clinical approaches and evidence of success.Quintes Pub Co Chicago, 1998:291-303. Cat 3
MCKAY C.The unerupted maxillary canine, an assessment of the role ofsurgery in 2 500 treated cases. Brit dent J 1978;145:207-210.Cat 1
MONNET-CORTI V., BORGHETTI A.Canines incluses et chirurgie plastique parodontale.Rev Odontostomat 2003;32:259-277. Cat 3
MONNET-CORTI V., BORGHETTI A.Chirurgie plastique parodontale et orthodontie.J Parodont Impl Orale 2000;19:253-266. Cat 3
MONNET-CORTI V., BORGHETTI A.Dégagement chirurgical des dents incluses. In : ChirurgiePlastique parodontale. Borghetti A et Monnet-Corti V,Ed: CdP 2008:433-445. Cat 3
MÜLLER H.P., EGER T.Gingival phenotypes in young males adults.J Clin Periodont 1997;24:65-71. Cat 1
OCHSENBEIN C., MAYNARD J.G.The problem of attached gingiva in children.J dent Child 1974;41:263-270. Cat 3
OGOLNIK R., VIGNON M., TAIEB F.Prothèse fixée principes et pratique.Ed: Masson Paris, 1993;4:54-59. Cat 3
OLIVE R.J.Orthodontic treatment of palatally impacted maxillarycanines. Aust Ortho J 2002;18:64-70. Cat 1
PARK H.S., KWON O.W., SUNG J.H.Micro-implant anchorage for forced eruption of impactedcanines. J Clin Ortho 2004;38:297-302. Cat 4
QUIRYNEN M., OP HEIJ D.G., ADRIANSENSA.,OPDEBEECK H.M., VAN STEENBERGHE D.Periodontal health of orthodontically extruded impactedteeth. A split-mouth, long-term clinical evaluation.J Periodont 2000;71:1708-1714. Cat 1
RICHARDSON G., RUSSELL K.A.A review of impacted permanent maxillary cuspids.Diagnosis and prevention.J Canad Dent Ass 2000;66:497-501. Cat 3
PARODONTIE
Revue d’Odonto-Stomatologie/Septembre 2011
SAUVAN J.L., MILLER P.D., AZZI R.I.L’adulte jeune. In : Chirurgie Plastique parodontale. Bor-ghetti A et Monnet-Corti V. Ed: CdP Paris, 2008:383-387.Cat 3
SAUVAN JL, MILLER PD, AZZI R. II.Indications et spécificités de la chirurgie plastiqueparodontale chez l’enfant, l’adolescent et l’adulte jeune.In : Chirurgie Plastique parodontale. Borghetti A. etMonnet-Corti V., Ed: CdP Paris, 2008:405-421. Cat 3
SLAVICEK R.Les principes de l’occlusion.Rev Ortho Dentofac 1983;17:449-490. Cat 4
STILLMAN P.R.Early clinical evidences of disease in the gingiva andpericementum. J dent Res 1921;3:25-31. Cat 4
TARNOW D.P., MAGNERA.W., FLETCHER P.The effect of the distance from the contact point to the crestof bone on the presence of the interproximal dental papilla.J Periodont 1992;63:995-996. Cat 1
THOMINE F., KORBENDAU J.M., MARTINEAU C.Mise en place chirurgico-orthodontique des dents retenues.Real Clin 1995;6:351-369. Cat 4
VANARSDALL R.L., HERBERGER T.A.Rapid palatal expansion: long-term stability and periodontalimplications. Thèse. Philadelphie : University ofPennsylvania, 1987. Cat 3
WENNSTRÖM J.L., ZUCCHELLI G.Increased gingival dimensions: a significant factor for suc-cessful outcome of root coverage procedures? A 2-year pros-pective clinical study. J Clin Periodont 1996;23:770-777.Cat 1
WENNSTRÖM J., LINDHE J., SINCLAIR F.,THILANDER B.Some periodontal tissue reactions to orthodontic toothmovements in monkeys. J Clin Periodont 1987;14:121-129.Cat 2
WISTH P.J., NODERVAL K., BOE O.E.Periodontal status of orthodontically treated impacted maxil-lary canines. Angle Orthod 1976;46:69-76. Cat 1
ZACHRISSON B.U.Orthodontics and periodontitis 1998. In: Lindhe J., KarringT., Lang N.P. (eds). Clinical periodontology and implantdentistry. Copenhagen: Munksgaard 1998;741-793. Cat 3
Bi
bl
io
gr
ap
hi
e
172