Embed Size (px)
Citation preview

Cas cliniques
DOI of or
DepartmenTrust, St. Mar
CorrespondLondon SW20rehman01@im
Ann Vasc SurDOI: 10.1016/� Annals of V�Edit�e par ELS
Un cas de kyste adventiciel ilio-f�emoralr�ecidivant
Syed Rehman, Louise Hancock, John Wolfe, Londres, Angleterre
Nous pr�esentons le cas d’un homme de 39 ans pr�esentant une claudication intermittenter�ecidivante 4 ans apr�es la mise en place d’un patch en Dacron au niveau de l’art�ere f�emoralecommune droite pour un kyste adventiciel. L’angiographie par r�esonance magn�etique n’�etait pascontributive, et l’art�eriographie conventionnelle retrouvait une st�enose �a 90% de l’art�eref�emorale commune droite. Le patient �etait trait�e par excision et remplacement de l’art�ereaffect�ee par une proth�ese en PTFE, et restait asymptomatique �a 6 mois. En cas dekyste adventiciel r�ecidivant, l’excision et le remplacement de l’art�ere affect�ee par interpositionproth�etique permet un r�esultat satisfaisant avec une faible probabilit�e de r�ecidive.
CASE REPORT
A 39-year-old man presented with progressive right leg
claudication that prevented him from walking 4 km to
work. He had cystic adventitial disease of the right
common femoral artery and, apart from a history ofmode-
rate smoking, he had no other risk factors for atheroscle-
rotic disease. Four years earlier, he underwent successful
Dacron patch repair of the right common femoral artery.
The cystic degeneration appeared to affect the anterior
two thirds of the artery, which was removed and replaced
with a large Dacron patch. The macroscopic disease was
removed. He remained asymptomatic for 4 years before
presenting with a recurrence of his symptoms.
Duplex ultrasound showed that the luminal diameter
of the right common femoral artery had narrowed,
although therewere reasonable velocities passing through
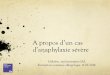
it and treadmill Doppler test was positive. Magnetic reso-
nance angiography (Fig. 1) showed signal loss in the distal
right common femoral artery and proximal superficial
femoral artery, indicating a degree of turbulence, but it
iginal article: 10.1016/j.avsg.2009.05.020.
t of Vascular Surgery, Imperial College Healthcare NHSy’s Hospital, Londres, Angleterre.
ence : Syed Rehman, 87 Grand Drive, Raynes Park,9DW, United Kingdom, E-mail addresses: syed.
perial.ac.uk, [email protected]
g 2010; 24: 550.e1-550.e3j.acvfr.2010.12.008ascular Surgery Inc.EVIER MASSON SAS
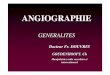
was multiplanar angiography (Fig. 2) that identified
extensive cystic adventitial disease of the posterior wall
causing 90% stenosis of the right common femoral artery
and origin of the right superficial femoral artery. The
patient’s worsening symptoms were considered to be due
to either aggressive myointimal hyperplasia or recurrence
of the cystic adventitial disease affecting the remaining
part of the common femoral artery that was previously
unaffected.
On the basis of the patient’s symptoms and the results
of the investigations, it was decided that it would be
appropriate to excise and replace the affected length of
common femoral artery. Intraoperatively, a large cystic
sac within the adventitia was compressing the right
common femoral artery and the origin of the right
superficial femoral artery. The termination of the external
iliac artery was transected, the profunda femoris was
transected just beyond its origin, and the superficial
femoral artery was transected 4 cm beyond its origin. An
8-mm PTFE externally supported graft was then anasto-
mosed to the external iliac artery end-to-end and the
distal anastomosis was performed end-to-end to the pro-
funda femoris artery. Following this, flow was restored to
the profunda femoris. An anastomosis was then per-
formed to the superficial femoral artery end-to-end and
the proximal anastomosis was end-to-side onto the PTFE
graft. Excellent flows were achieved as a result. Histology
revealed that the resection margins were free of cystic
adventitial disease. At 6-month follow-up, the patient’s
symptoms had completely resolved, he had a full com-
plement of peripheral pulses in the right leg, and treadmill
Doppler results were normal.
600.e1

Fig. 1. Magnetic resonance angiogram that is incon-
clusive for stenosis of the right common and superficial
femoral arteries.
Fig. 2. Multiplanar computed tomography angiogram
demonstrating severe stenosis of the right common
femoral artery and origin of the right superficial femoral
artery.
600.e2 Cas cliniques Annales de chirurgie vasculaire
DISCUSSION
Cystic adventitial disease is a rare cause of intermit-
tent claudication with an incidence of 1 : 1200 and
predominantly affecting males (male-to-female
ratio 15 : 1).1 The condition was first described by
Atkins and Key2 in 1947 involving the external iliac
artery in a 40-year-old man. Since then, approxi-
mately 320 cases have been reported.1 The majority
of these cases have involved the popliteal artery;
only 36 cases report iliofemoral artery
involvement.1,3
The etiology of this condition remains unclear.
Several theories have been suggested and were
most recently reviewed by Levien and Benn in
1998.4 These include the suggestions that cystic
adventitial disease is part of a myxomatous systemic
degenerative condition, caused by repeated micro-
trauma; the ganglion theory that adventitial cysts
originate as capsular synovial structures that involve
the adjacent blood vessel; and the developmental
theory that mucin-secreting cells from an adjacent
joint become included in the adventitia during
development. Levien and Benn suggested their own
unifying hypothesis that cystic adventitial disease is
a developmental condition caused by nonsynovial
less-differentiated joint-related mesenchymal cell
rests in nonaxial blood vessels. Cystic adventitial
disease should be suspected in patients with
intermittent claudication in the absence of peri-
pheral arterial disease or atherosclerotic risk factors.
It may present acutely but does not usually manifest
as rest pain. Clinically, there are diminished or
absent pulses, and a bruit may be audible over the
stenosed artery. The ankle-brachial pressure index
may also be reduced.
Investigations include duplex ultrasound, which
shows arterial stenosis and a cyst, with no flow,
appearing as anechoic or hypoechoic masses in the
vessel wall. Angiography demonstrates distinctive
stenosis of the arterial lumen, which has an ‘‘hour-
glass’’ appearance or demonstrates the ‘‘scimitar
sign’’ depending on the configuration of the cyst.
Magnetic resonance imaging (MRI) is said to be as
effective at diagnosing cystic adventitial disease as
conventional angiography. Cysts are hyperintense
on T2-weighted images and have variable signal
intensity on T1-weighted images due to the variable
amount of mucoid material within the cysts.5
However, in our patient, MRI (Fig. 1) was incon-
clusive, whereas multiplanar angiography (Fig. 2)
defined the severe stenosis.
Several treatment methods have been used in the
management of cystic adventitial disease. In a small
number of cases, conservative management has
resulted in spontaneous resolution of symptoms.6-9
However, the majority of patients require interven-
tion. Ultrasound- or computed tomography (CT)-
guided aspirationhas beenusedwith varying success.
Do et al.10 describe successful ultrasound-guided

Vol. 24, No. 4, 2010 Cas cliniques 600.e3
aspiration in seven patients without recurrence at a
mean follow-up of 14.8 months, while Sieunarine
et al.11 and Colombier et al.12 both report recurrences
following CT-guided aspiration requiring subsequent
surgical intervention. Our experience suggests that
recurrence is likely unless the segment of artery is
removed. Balloon angioplasty does not appear to be
successful as it does not affect the cystic compression
of the artery.13
Surgical intervention appears to provide the
most successful long-term outcome, which is of
particular relevance as cystic adventitial disease
affects relatively young patients. Cyst excision can
be performed without arterial reconstruction but
is associated with a 10% recurrence rate.14 We
have reported recurrence in a patient who origi-
nally had cyst excision performed with patch
repair. Ohta et al.15 reported a case of cystic
adventitial disease recurring within an interposed
autogenous saphenous vein graft.
In patients with recurrent cystic adventitial
disease, excision and replacement of the affected
artery with a prosthetic interposition graft provides
a successful outcome with minimum chance of
recurrence. However, it is still important to consider
the complications of prosthetic graft interposition.
In addition, it is vital that all patients receive
follow-up.
REFERENCES
1. Jindal R, Majed A, Hamady M, et coll. Cystic adventitial
disease of the iliofemoral artery: case reports and a short
review. Vascular 2006;14:169-172.
2. Atkins HJB, Key IA. A case of myxomatous tumour arising
in the adventitia of the left external iliac artery. Br J Surg
1947;34:426-427.
3. Gagnon J, Doyle DL. Adventitial cystic disease of common
femoral artery. Ann Vasc Surg 2007;21:84-86.
4. Levien LJ, Benn CA. Adventitial cystic disease: a unifying
hypothesis. J Vasc Surg 1998;28:193-205.
5. Wright LB, Matchett WJ, Cruz CP, et coll. Popliteal artery
disease: diagnosis and treatment. Radiographics 2004;24:
467-479.
6. Pursell R, Torrie EP, Gibson M, et coll. Spontaneous and
permanent resolution of cystic adventitial disease of the
popliteal artery. J.R Soc Med 2004;97:77-78.
7. Owen ER, Speechly-Dick EM, Kour NW, et coll. Cystic
adventitial disease of the popliteal artery: a case of sponta-
neous resolution. Eur J Vasc Surg 1990;4:319-321.
8. Furunaga A, Zempo N, Akiyama N, et coll. Cystic disease of
right popliteal artery with spontaneous resolution. Nippon
Geka Gakkai Zasshi 1992;93:1501-1503.
9. Soury P, Rivi�ere J, Watelet J, et coll. Spontaneous regression
of a sub-adventitial cyst of the popliteal artery. J Mal Vasc
1995;20:323-325.
10. Do DD, Braunschweig M, Baumgartner I, et coll. Adventitial
cystic disease of the popliteal artery: percutaneous US-
guided aspiration. Radiology 1997;203:743-746.
11. Sieunarine K, Lawrence-Brown MM, Kelsey P. Adventitial
cystic disease of the popliteal artery: early recurrence after
CT guided percutaneous aspiration. J Cardiovasc Surg
(Torino) 1991;32:702-704.
12. Colombier D, Elias A, Rousseau H, et coll. Cystic adventitial
disease: importance of computed tomography in the diag-
nostic and therapeutic management. J Mal Vasc 1997;22:
181-186.
13. Khoury M. Failed angioplasty of a popliteal artery stenosis
secondary to cystic adventitial disease: a case report. Vasc
Endovasc Surg 2004;38:277-280.
14. McAnespey D, Rosen RC, Cohen JM, et coll. Adventitial
cystic disease. J Foot Surg 1991;30:160-164.
15. Ohta T, Kato R, Sugimoto I, et coll. Recurrence of cystic
adventitial disease in an interposed vein graft. Surgery
1994;116:587-592.