Embed Size (px)
Citation preview

URGENCES ET NOUVEAUX ANTICOAGULANTS ORAUX (NOACS)
Professeur Cedric HERMANS MD MRCP (Lon) FRCP (Edin) PhD
Haemostasis and Thrombosis Unit
Haemophilia Clinic
Division of Haematology
Cliniques Universitaires Saint-Luc
Catholic University of Louvain
1200 Brussels, Belgium
Cedric HERMANS

• 18h00 – 19h00 Mécanismes d’action des nouveaux anticoagulants, comment et quand (Sujet 517) doser leur efficacité : la vision du laboratoire. Pr. Anne DEMULDER, Laboratoire d’Hématologie et de la Coagulation, CHU Brugmann, Bruxelles
• 19h00 – 20h00 Indications des nouveaux anticoagulants oraux, revue de l’EBM (Sujet 518) Pr. Jean-Luc VANDENBOSSCHE, Service de Cardiologie, CHU Saint-Pierre, Bruxelles
• 20h00 – 21h00 Urgences et nouveaux anticoagulants oraux (Sujet 519) Pr. Cédric HERMANS, Clinique d’Hématologie et de la Coagulation, CU Saint-Luc, Bruxelles

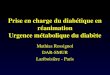
Les nouveaux anticoagulants oraux Inhibition directe et ciblée du FXa ou du FIIa (thrombine)
Fibrinogène Fibrine
IIa Prothrombine
Xa + Va
X
Tissue Factor-VIIa
IXa IX
VIIIa Rivaroxaban (Xarelto) (Bayer)
Apixaban (Eliquis) (BMS / PFIZER)
- Xaban
Dabigatran Etexilate (Pradaxa) (Boehringer-Ingelheim)
Pradaxa / Dabigatran : anti-thrombine
E Liqui S : E pour equilibrium - Liqui pour liquid and S pour Stability
Xarelto : Xa, RELiable, Treatment, Oral Cedric HERMANS UCL 2012

Comparaison des Nouveaux Anticoagulants
Apixaban
ELIQUIS
Rivaroxaban
XARELTO
Dabigatran
PRADAXA
Mechanism of action direct FXa inhibitor direct FXa inhibitor direct FIIa inhibitor
Oral availability ~50 % 80 % 6.5 %
Route of administration oral oral oral
Dosing 2x/day in all
indications
1x/day (AF, DVT and
PE)
1x/day (DVT
prevention)
2x/day (VTE, AF)
Pro-drug No No Yes
Food effect No No No
Renal Clearance ~27 % 36 % 85 %
Mean Half-Life (T1/2) ~12h 7–11 h 14–17 h
Tmax 3 h 2–4 h 0.5–2 h
Drug interactions
CYP 3A4 and P-gp
inhibitors
CYP 3A4 inducers
CYP 3A4 and P-gp
inhibitors
CYP 3A4 inducers
P-gp inhibitors
P-gp inducers
Eikelboom et al. Circulation 2010;121:1523

Risk of bleeding with NOACs

BIB
E 1
2/1
2/5
64 F
R
BIB
E 1
2/1
2/5
64 F
R
Pradaxa et FA : RE-LY study design1
Les patients ont été repartis en 3 groupes de manière randomisée sans tenir compte de l’âge, de la fonction rénale, d’un traitement concomitant, etc….
FA avec 1 facteur de risque •1/3 CHADS2: 0-1
•1/3 CHADS2: 2
•1/3 CHADS2: 3-6
Pradaxa
110 mg 2x/j
n=6076
Warfarine
(INR 2.0–3.0)
n=6015
Pradaxa
150 mg 2x/j
n=6022
1. Ezekowitz MD et al. Am Heart J 2009;157:805–10; Connolly SJ et al. N Engl J Med 2009;361:1139–5
Objectif primaire : démontrer la non-infériorité du Pradaxa® par rapport à la warfarine en terme de prévention des AVC et des embolies systémiques

BIB
E 1
2/1
2/5
64 F
R
BIB
E 1
2/1
2/5
64 F
R
RELY STUDY : Major bleeding and components
Characteristic Dabigatran 150 mg bid
Dabigatran 110 mg bid
Warfarin p-value
110 vs. W p-value
150 vs. W
Number of patients (n) 6,076 6,015 6,022
Major bleeding rate per year (%)
3.32 2.87 3.57 0.003 0.32
Life threatening (%) Non-life threatening (%) Gastrointestinal (%)
1.49
2.06 1.56
1.24
1.83 1.15
1.85
1.92 1.07
<0.001
0.65 0.52
0.03
0.39 0.001
Data represents %/year Connolly SJ, et al. N Engl J Med 2009;361:1139-1151
Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation

BIB
E 1
2/1
2/5
64 F
R
BIB
E 1
2/1
2/5
64 F
R
Facteurs pouvant augmenter le risque hémorragique du PRADAXA 1
AAS = Acide acétylsalicylique
AINS = Anti-inflammatoire non stéroïdien
ISRS = Inhibiteur sélectif de la recapture de la sérotonine
IRSNA = Inhibiteur de la recapture de la sérotonine-noradrénaline
Général • Age ≥ 75 ans
• Insuffisance rénale modérée (ClCr 30-50 mL/min) • Faible poids (< 50 kg)
Interactions médicamenteuses
• Inhibiteurs de la P-gp: vérapamil, amiodarone,quinidine, clarithromycine, dronédarone • Anti-aggrégants: AAS, Clopidogrel… • Autres traitements susceptibles d’altérer l’hémostase: AINS, ISRS ou IRSNA
Pathologies / interventions associées à des risques hémorragiques particuliers
• Troubles congénitaux ou acquis de la coagulation • Thrombocytopénie ou anomalies fonctionnelles des plaquettes • Biopsie récente, traumatisme majeur • Endocardite bactérienne • Oesophagite, gastrite ou reflux gastro-oesophagien
1. RCP Pradaxa®

BIB
E 1
2/1
2/5
64 F
R
BIB
E 1
2/1
2/5
64 F
R
Un effet anticoagulant continu grâce à deux prises par jour1
La pharmacocinétique ne soutient pas le dosage en prise unique. La FDA a évoqué la possibilité qu'un dosage deux fois par jour aurait été plus adapté 4
1. D’après Van Ryn et al., Thromb Haemost 2012; 103(6):1116-1127
2. D’après Kreutz et al., Fundamental and clinical pharmacology 2012; 26:27-32
3. Xarelto: Résumé des caractéristiques du produit (RCP)
4. N Engl J Med; 2011; 365: 1557-1559

Pradaxa® 150 mg, 2 x/jour, versus warfarine Efficacité
Réduction significative de l’AVC/embolie systémique
Sécurité
Taux d’hémorragies majeures comparable
Réduction significative de:
Hémorragies intracrâniennes,
Hémorragies menaçant le pronostic vital
Hémorragies totales
RE-LY® – RÉSUMÉ DES RÉSULTATS
Connolly SJ, et al. N Engl J Med 2009;361:1139-1151.
Pradaxa® 110 mg, 2 x/jour, versus warfarine Efficacité
Taux comparable d'AVC/embolie systémique
Sécurité
Réduction significative de :
Hémorragies majeures
Hémorragies intracrâniennes,
Hémorragies menaçant le pronostic vital
Hémorragies totales

Warfarin INR 2.5 (INR range 2–3) En
d o
f s
tud
y
Rivaroxaban 20 mg/jour
CrCL 30–49 mL/min:
Rivaroxaban 15 mg/jour
Fo
llo
w-u
p
AF non valvulaire et antécédents d’AVC, AIT, d’embolie systémique
Ou au moins deux des facteurs de risque:
Décompensation cardiaque Hypertension Age ≥ 75 ans Diabète
Mois
12–32
Mois
13–33
R
N = 14 000
Xarelto et Fibrillation Auriculaire Etude ROCKET AF
CrCL, creatine clearance
INR, international normalized ratio
Critère primaire d’effiacité
• AVC + embolie systémique
Crirère primaire de sécurité
• Hémorragie majeure + saignement relevant non majeur
Cedric HERMANS Dec 2011

Rivaroxaban Warfarin
Event Rate
or N (Rate)
Event Rate
or N (Rate)
HR
(95% CI)
P-
value
Major
>2 g/dL Hgb drop
Transfusion (> 2 units)
Critical organ bleeding
Bleeding causing death
3.60
2.77
1.65
0.82
0.24
3.45
2.26
1.32
1.18
0.48
1.04 (0.90, 1.20)
1.22 (1.03, 1.44)
1.25 (1.01, 1.55)
0.69 (0.53, 0.91)
0.50 (0.31, 0.79)
0.576
0.019
0.044
0.007
0.003
Intracranial Hemorrhage 55 (0.49) 84 (0.74) 0.67 (0.47, 0.94) 0.019
Intraparenchymal 37 (0.33) 56 (0.49) 0.67 (0.44, 1.02) 0.060
Intraventricular 2 (0.02) 4 (0.04)
Subdural 14 (0.13) 27 (0.27) 0.53 (0.28, 1.00) 0.051
Subarachnoid 4 (0.04) 1 (0.01)
Event Rates are per 100 patient-years
Based on Safety on Treatment Population
ROCKET-study Primary Safety Outcomes

APIXABAN - ARISTOTLE: Study design and objectives1
The primary objective of the trial was to determine if apixaban was non-inferior to warfarin for the prevention of stroke and systemic embolism.
If non-inferiority was met, the following endpoints were tested for superiority1,3
• Stroke or systemic embolism (primary efficacy endpoint)
• ISTH major bleeding (primary safety endpoint)
• Death due to any cause (key secondary endpoint)
14
1. Granger et al. N Engl J Med 2011;365:981-992. 2. Lopes et al. Am Heart J 2010;159:331-9. 3. Apixaban SmPC 2012.
*448 primary study events were needed. †≥ 2 of the following: age ≥ 80 years, weight ≤ 60 kg, serum creatinine level ≥ 1.5 mg/dL (133 µmol/L)
Patient Population2
Aged ≥ 18 years
Patients with NVAF and ≥ 1 risk factors for stroke
Apixaban 5.0 mg oral BD
(2.5 mg oral BD in select patients† [4.7%])
Warfarin
(adjusted to an INR of 2-3)
Event Driven*
Randomised, double-blind,
double-dummy

ARISTOTLE: Apixaban significantly reduced the rate of bleeding irrespective of the bleeding definition used
Outcome Apixaban
(n=9,088)
Event Rate (%/yr)
Warfarin
(n=9,052)
Event Rate (%/yr)
HR (95% CI) P value
Primary safety outcome: ISTH major bleeding
2.13 3.09 0.69 (0.60, 0.80) < 0.001
Intracranial 0.33 0.80 0.42 (0.30, 0.58) < 0.001
Other location 1.79 2.27 0.79 (0.68, 0.93) 0.004
Gastrointestinal 0.76 0.86 0.89 (0.70, 1.15) 0.37
Major or clinically relevant non-major bleeding
4.07 6.01 0.68 (0.61, 0.75) < 0.001
GUSTO severe bleeding 0.52 1.13 0.46 (0.35, 0.60) < 0.001
TIMI major bleeding 0.96 1.69 0.57 (0.46, 0.70) < 0.001
Any bleeding 18.1 25.8 0.71 (0.68, 0.75) < 0.001
Adapted from Granger et al. N Engl J Med 2011;365:981-92.

Concomitant use of apixaban with antiplatelet agents increases the risk of bleeding
ARISTOTLE APPRAISE II
In a clinical trial of patients with AF,
concomitant use of ASA increased
the major bleeding risk:
On apixaban from 1.8% to 3.4% per year
On warfarin from 2.7% to 4.6% per year
There was limited (2.1%) use of
concomitant dual antiplatelet therapy
In a clinical trial of high-risk post ACS
patients, characterised by multiple cardiac
and non-cardiac comorbidities, who
received ASA or the combination of ASA
and clopidogrel:
A significant increase in risk of ISTH major
bleeding was reported:
Apixaban: 5.13% per year
Placebo: 2.04% per year
Apixaban SmPC 2012.
Apixaban SmPC recommendations
In patients with AF and a condition that warrants mono or dual antiplatelet therapy,
a careful assessment of the potential benefits against the potential risks should be made
before combining this therapy with apixaban.
Apixaban should be used with caution when co-administered with NSAIDs (including
ASA) because these medicinal products typically increase the bleeding risk

Comparaison des 3 NOACs dans la FA
TE events/yr Maj. bleeds/yr
RE-LY D110 : 1.5 D110 : 2.7%*
CHADS2 2.1±1.1 D150 : 1.1%* D150 : 3.1%
VKA : 1.7% VKA : 3.4%
ROCKET-A RIV onT : 1.7%* RIV : 3.6%
CHADS2 3.5±1.1 VKA onT : 2.2% VKA : 3.4%
ARISTOTLE API : 1.3%* API : 2.1%*
CHADS2 2.1±1.1 VKA : 1.6% VKA : 3.1%
IC bleed ↓ significantly (not RIV) but ↑ GI bleed (not API)

Management of overdose without bleeding and bleeding complications in patients treated with NOACs

Hémorragies et AVK
AVK
Test biologique INR
Etiologie Interactions médicamenteuses
Traitement STOP VKA Vitamin K (Konakion) PPSB (II, VII, IX, X) FFP
Cedric HERMANS Dec 2011

Nombre de flacons de PPSB (20ml) à administrer pour obtenir un INR de 1.5
INR 7.5 6.0 5.0 4.0 3.5 3.0
50 Kg 3.0 3.0 3.0 3.0 3.0 2.0
60 Kg 4.0 4.0 3.5 3.0 3.0 3.0
70 Kg 4.5 4.0 4.0 4.0 3.5 3.0
80 Kg 5.0 5.0 4.5 4.5 4.0 3.5
90 Kg 5.0 5.0 5.0 5.0 4.5 4.0
100 Kg 5.0 5.0 5.0 5.0 5.0 4.5
Poids Flacons

Concentrations des FII, VII, IX, X après traitement par PPSB (40 ml) et Vit K (2 mg) chez une patiente surdosée en sintrom
Pre 10’ 24 h
INR >7 1,72 1,29
FII 8 53 69
FVII >3 22 56
FIX 9 28 90
FX 5 40 55


Hémorragies et anticoagulants oraux
AVK Xarelto Pradaxa
Test biologique INR Prothrombin time Anti-Xa
TT (Haemoclot) ECT APTT
Etiologie Interactions médicamenteuses
Dysfonction rénale Dysfonction rénale
Traitement STOP VKA Vitamin K PPSB (II, VII, IX, X) FFP
STOP Xarelto PPSB ? PFC ? FEIBA ?
STOP Pradaxa PFC ? Hemodialysis ? PPSB ? FEIBA ?
Cedric HERMANS Dec 2011

Influence des nouveaux anticoagulants sur les tests de coagulation
Pradaxa Anti-IIa
Xarelto Anti-Xa
Temps de prothrombine (QUICK)
+ ++ (Influence des réactifs +++)
TCA ou APTT ++ +
Temps de thrombine ou temps d’écarine (ECT)
++ -
Anti-Xa - ++
Anti-IIa ++ -
- Les perturbations des tests de coagulation sont influencées par le délai entre l’administration
de l’anticoagulant et les anomalies observées

APIXABAN : Management of overdose (without bleeding)
There is no antidote to apixaban
Overdose of apixaban may result in a higher risk of bleeding
In controlled clinical trials, orally administered apixaban in healthy subjects at
doses up to 10 times the daily maximum recommended human dose had no
clinically relevant adverse effects
Administration of activated charcoal may be useful in the management of
apixaban overdose or accidental ingestion
Apixaban SmPC 2012.
2 hours after 20 mg apixaban 6 hours after 20 mg apixaban
Apixaban AUC 50% 27%
Cmax No impact No impact
Mean half-life decrease From 13.4 h to 5.3 h From 13.4 h to 4.9 h
In healthy subjects, administration of activated charcoal 2 and 6 hours after ingestion of a 20-mg dose of apixaban resulted in:

APIXABAN : Management of bleeding complications
1. Apixaban SmPC 2012
2. Escolar et al. Thromb Res 2012;130 (Suppl 1):S113, abstract no. C0122
First measures1:
1. Treatment must be discontinued
2. The source of bleeding must be investigated
3. The initiation of appropriate treatment, e.g. surgical haemostasis or the transfusion of fresh frozen plasma, should be considered
4. Administration of activated charcoal may be useful in the management of apixaban overdose or accidental ingestion.
If life-threatening bleeding cannot be controlled by the above measures,
administration of recombinant factor VIIa (rFVIIa) may be considered1.
− However, there is currently no experience with the use of rFVIIa in individuals receiving apixaban.
− Re-dosing of rFVIIa could be considered and titrated depending on improvement of bleeding
An in vitro study suggests that PCC or activated PCC reverses the anticoagulant action of apixaban.2
PCC= Prothrombin Complex Concentrate

PRADAXA : GESTION DE
COMPLICATIONS HÉMORRAGIQUES
1. Interrompre le traitement et rechercher l’origine du saignement. Si
dans les 1-2 heures après surdosage: charbon actif
2. Maintenir une diurèse suffisante et initier un traitement
symptomatique standard
Hémostase chirurgicale
Remplacement du volume sanguin (ex. sang complet, plasma
frais congelé)
Utilisation de concentrés de facteurs de coagulation (sur base de
données pré-cliniques)
• Concentrés de complexe prothrombique (PCC; non-activé ou
activé)
• Facteur VIIa recombinant
Pradaxa®: RCP
Van Ryn J et al. Thromb Haemost. 2010;103(6):1116-27.

PRADAXA : GESTION DE
COMPLICATIONS HÉMORRAGIQUES
3. L’utilisation de concentrés de plaquettes peut être envisagée lorsque :
Une thrombocytopénie est présente
Des anti-agrégants plaquettaires à longue durée d’action ont été utilisés
4. Finalement, comme la liaison du dabigatran aux protéines plasmatiques est relativement faible (~35%), une hémodialyse peut être envisagée
Pradaxa®: RCP
Van Ryn J et al. Thromb Haemost. 2010;103(6):1116-27.

PRADAXA : GESTION DE
COMPLICATIONS HÉMORRAGIQUES
Van Ryn J et al. Thromb Haemost. 2010;103(6):1116-27.

EXPERT PAPER www.thrombosisguidelinesgroup.be

AVC CHEZ UN PATIENT SOUS PRADAXA®
• En présence d’hémorragie intracrânienne (HIC)
– Consulter un neurochirurgien
– Traiter comme n’importe quelle autre hémorragie sévère ou
menaçant le pronostic vital sous Pradaxa®
• AVC ischémique
– Traiter selon la pratique clinique courante
– L’administration de fibrinolytiques doit être envisagée lorsque le
patient présente un TT dilué, un ECT ou un TCA ne dépassant
pas la limite supérieure de la normale selon les fourchettes de
référence de chaque laboratoire.
Expert opinion RCP Pradaxa


XARELTO : gestion des complications hémorragiques

XARELTO : Gestion des complications hémorragiques

Possible measures to take in the case of bleeding with NOACs (EHRA practical guide of the NOACs – EHJ 2013)

Management of bleeding in patients taking NOACs (EHRA practical guide of the NOACs – EHJ 2013)

Management of NOACs before invasive procedures

Classification of elective surgical intervention acording to bleeding
risk

APIXABAN : Guidance on discontinuing apixaban before surgical or invasive procedures
Elective procedures
Urgent procedures Low risk
of bleeding*
Moderate or high risk
of bleeding**
At least 24h prior to
surgery or procedure*
At least 48h prior to
surgery or procedure**
Appropriate caution should be
exercised, taking into
consideration an increased risk
of bleeding.
This risk of bleeding should be
weighed against the urgency
of intervention.
*Interventions for which any bleeding that occurs is expected to be minimal, non-
critical in its location or easily controlled
**Interventions for which the probability of clinically significant bleeding cannot be
excluded or for which the risk of bleeding would be unacceptable
Apixaban SmPC 2012.

PRADAXA et INTERVENTIONS
CHIRURGICALES
• Les interventions chirurgicales peuvent imposer une interruption
temporaire de la prise du Pradaxa®
• Règles d’interruption avant une chirurgie élective
Fonction rénale
(CLCr )
Demi-vie
estimée
(h)
Arrêter la prise de Pradaxa avant une chirurgie
programmée
Risque de saignement
élevé
ou chirurgie majeure
Risque standard
≥ 80 ml/min ~ 13 2 jours avant 24 heures avant
≥ 50-< 80ml/min ~ 15 2-3 jours avant 1-3 jours avant
≥ 30-< 50ml/min ~ 18 4 jours avant 2-3 jours avant (> 48
heures)
RCP Pradaxa®
En général, pas besoin de bridging avec HBPM

PRADAXA et INTERVENTIONS
CHIRURGICALES
• Les interventions telles qu'une rachianesthésie – anesthesie péridurale –
ponction lombaire peuvent nécessiter une hémostase complète. Cfr colonne «risque de saignement élevé»
• Intervention urgente
Il convient de retarder si possible un acte chirurgical/une intervention au minimum 12 heures après la dernière dose.
Si l'intervention ne peut pas être retardée, le risque hémorragique peut être augmenté. Ce risque d’hémorragie doit être mesuré par rapport à l'urgence de l’intervention.
RCP Pradaxa®
RCP Pradaxa®

XARELTO : Recommandations en cas de procédures invasives

Interruption du traitement par Xarelto en cas de geste invasif

Last intake of drug before elective surgical intervention

NOACs et antidote(s)

Existe-t-il un antidote des NOACs?
• Aucun des nouveaux anticoagulants oraux n’a un antidote validé
pour le moment1
• Tous ont cependant une demi-vie courte
• En cas de saignements: mêmes mesures que pour les AVK (y
compris administration de facteurs de coagulation*) sauf Vit K
• Comme la liaison protéique est faible, le Pradaxa® peut être dialysé
(caractéristique unique)*
1. RCP Pradaxa, Xarelto, Eliquis
2. * données cliniques limitées

Existe-t-il un antidote?
D 110 BID D 150 BID Warfarin
Patients needing corrective measures 394 484 475
Patients having survived 369 456 435
Patients having died 25 28 40
FDA Clinical review Pradaxa® (dabigatran etexilate) - Nhi Beasley and Aliza Thompson.
Mesures correctrices utilisées dans RE-LY:
• Vit K (uniquement dans le groupe warfarine)
• FFP, PCC ou facteur VIIa recombinant
Les résultats positifs de Pradaxa® dans l’étude RE-LY ont été obtenus
en l’absence d’antidote



Conclusions
• L’utilisation des NOACs est associée à moins de complications hémorragiques (hormis digestives) que les AVKs, du moins dans les études cliniques.
• La gestion des complications hémorragiques sous NOACs est de mieux en mieux définie mais doit être validée.
• Le rôle des agents hémostatiques (PCCs, APCCs, RVIIa) doit être défini.
• La gestion des NOACs lors de gestes invasifs est en théorie plus facile que celle des AVKs.
• Des antidotes des NOACs sont en cours de validation et semblent prometteurs.
• Une bonne éducation de l’utilisation des NOACs est indispensable pour valoriser au mieux ces molécules prometteuses et réduire les complications.