Embed Size (px)
Citation preview

Respiratory DiseasesRespiratory Diseases(呼吸系统疾病)(呼吸系统疾病)JI WanshengJI WanshengDept. of Internal medicineDept. of Internal medicineTel: 2602375, mobile: Tel: 2602375, mobile: 1315360980513153609805

Pleural diseasesPleural diseases
1.1. Pleural effusionPleural effusion2.2. PneumothoraxPneumothorax

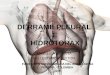
Pleural effusionPleural effusion Pleural space lies between the lung Pleural space lies between the lung
and chest wall, which formed by the and chest wall, which formed by the folding of visceral and parietal pleura folding of visceral and parietal pleura and normally, a thin layer of fluidand normally, a thin layer of fluid
A pleural effusionA pleural effusion is an excessive is an excessive quantity of fluid in the pleural spacequantity of fluid in the pleural space

Etiology & pathogenesisEtiology & pathogenesis
Pleural fluid circulation Pleural fluid circulation 1.1. Exudation or transudation Exudation or transudation
of Systemic vessels (red)of Systemic vessels (red)2.2. Reabsorption via Reabsorption via
lymphatic vessels (white)lymphatic vessels (white)3.3. Formation of pleural Formation of pleural
effusion by circulatory effusion by circulatory imbalanceimbalance

1.1. Static hydrate pressure increasedStatic hydrate pressure increased2.2. Increased permeability of pleural Increased permeability of pleural
capillarycapillary3.3. Colloid pressure reduced in pleural Colloid pressure reduced in pleural
capillarycapillary4.4. Drainage obstructed via lymphatic Drainage obstructed via lymphatic
vessels in parietal pleuravessels in parietal pleura5.5. Pleural injuriesPleural injuries6.6. FormationFormation>drainage >drainage →effusion→effusion

Symptoms and signsSymptoms and signs
Dyspnea—most commonDyspnea—most common Chest pain and coughChest pain and cough History of heart failure, hepatitis, liver History of heart failure, hepatitis, liver
cirrhosis, etccirrhosis, etc Signs –related to the quantity of pleural fluidSigns –related to the quantity of pleural fluid

Laboratory testingLaboratory testing

ColorColor DensityDensity Protein Protein RivaltRivaltaa
CellsCells
TT Light Light yellow or yellow or clearclear
<1.018<1.018 10 10 ~30~30 -- -- <300/uL, Lym<300/uL, Lym
ExEx Light Light yellow or yellow or whitewhite
1.027 1.027 ~ ~ 1.0451.045
41 41 ~85~85 ++ RBC and WBCRBC and WBC
EE Foggy, Foggy, purulentpurulent
1.021 1.021 ~1.033~1.033
30 30 ~55~55 ---- N, toxic N, toxic granules in granules in cellscells
HH RedRed 1.030 1.030 ~1.045~1.045
---- Like Like peripheral peripheral blood blood
CC Chylous or Chylous or fattyfatty
---- Plentiful L, Plentiful L, few RBCfew RBC
T: transudation, Ex: exudation, E: empyema, H: haemothorax, C: chylous pleural effusion

1. Transudation: cell counting<100-300/ul, L2. Exudation: WBC> 500/ul, 3. Empyema: WBC > 10,000/ul4. Haemothorax: 5,000/ul, caused by TB,
pulmonary infarction & malignancy.5. Chylous pleural effusion6.6. Examination Examination forfor malignant cells & malignant cells &
pathogens

ProteinsProteins1.1. E: >30g/L, PF/serum >0.5; Rivalta (+)E: >30g/L, PF/serum >0.5; Rivalta (+)2.2. T: <30g/L, albumin, Rivalta testing (-)T: <30g/L, albumin, Rivalta testing (-) Lipids: chylous effusion, not Lipids: chylous effusion, not
precipitated after centrifuge, Sudan precipitated after centrifuge, Sudan III staining: red, triglyceride III staining: red, triglyceride >1.24mmol/L, normal cholesterol. >1.24mmol/L, normal cholesterol. caused by injury of thoracic duct caused by injury of thoracic duct
Glucose: similar as serumGlucose: similar as serum LDH: E LDH: E >>200U/L, PF/serum >0.6 , 200U/L, PF/serum >0.6 ,
LDH>500U/L LDH>500U/L →malignancy or →malignancy or accompanied with infectionaccompanied with infection
Tumor markers: CEATumor markers: CEA

X-rayX-ray1.1. Slight free effusion Slight free effusion →blunted →blunted
costodiaphragmatic anglecostodiaphragmatic angle2.2. Large quantity of effusion Large quantity of effusion →arc effusion →arc effusion
shadow pointed upward and outwardshadow pointed upward and outward3.3. Gas-liquid thorax: gas-liquid planeGas-liquid thorax: gas-liquid plane4.4. Wrapped effusion Wrapped effusion →not changed with →not changed with
positionspositions

Ultrasound & other Ultrasound & other examinationsexaminations
1.1. Ultrasound-- Ultrasound-- guide thoracentesis for small guide thoracentesis for small amount or enveloped (wrapped) effusionamount or enveloped (wrapped) effusion
2.2. Pleural biopsy: Pleural biopsy: gained by thoracentesis or gained by thoracentesis or open surgery for tumor, TB or other pleural Dopen surgery for tumor, TB or other pleural D
3.3. BronchoscopyBronchoscopy

DiagnosisDiagnosis1.1. Effusion or not ?Effusion or not ?2.2. Transudate or exudate ? Transudate or exudate ? Any of Any of
following met? following met? PF/serum protein >0.5, PF/serum protein >0.5, PF/serum LDH >0.6, PF LDH >2/3 upper PF/serum LDH >0.6, PF LDH >2/3 upper serum limitserum limit
3.3. Etiology? Etiology?

EtiologyEtiology Transudate: Transudate: common in congestive heart common in congestive heart
failure, liver cirrhosis, nephrotic syndrome, failure, liver cirrhosis, nephrotic syndrome, hypoalbuminemia, etchypoalbuminemia, etc
Exudate: Exudate: most common in TB pleurisy, other: most common in TB pleurisy, other: pneumonia, lung abscess, bronchiectasis, etcpneumonia, lung abscess, bronchiectasis, etc
Malignant effusion: Malignant effusion: by malignancy from by malignancy from neighboring organs (LC, breast cancer) , or neighboring organs (LC, breast cancer) , or distal organs (GI or urinoprogenitive system)distal organs (GI or urinoprogenitive system)

Essentials of DiagnosisEssentials of Diagnosis
Asymptomatic; pleuritic chest pain; Asymptomatic; pleuritic chest pain; dyspnea if effusion is largedyspnea if effusion is large
↓↓vocal fremitus, dullness, distant breath vocal fremitus, dullness, distant breath sounds; bronchophony if effusion is largesounds; bronchophony if effusion is large
Laboratory testingLaboratory testing Radiographic evidence of pleural effusionRadiographic evidence of pleural effusion Findings depend on Findings depend on thoracocentesis, thoracocentesis,
pleural biopsy, or thoracoscopepleural biopsy, or thoracoscope

Approach to diagnosisApproach to diagnosis
Pleural effusion
Thoracentesis, measure PF protein and LDHAny of following met?PF/serum protein >0.5PF/serum LDH >0.6PF LDH >2/3 upper serum limit
Exudates
Transudate
Yes No
Continued

Exudates
Measure G, amylase, cytology, differential cell count,Culture, stain, tumor or TB markers
Amylase :Esophageal rupturePancreatic Dmalignancy
G<60mg/dl:MalignancyBacterial infectionRheumatoid pleuritisNo diagnosis
Consider pulmonary embolus
Continued

No
Consider pulmonary embolus
Helical CT or lung scan
PF marker for TB
Symptoms improving
observeConsider thoracoscopy or open pleural biopsy
Treat for PE
Yes
Yes
Treat for TBYesNo

Effusion secondary toEffusion secondary to1.1. Heart failureHeart failure2.2. Liver cirrhosisLiver cirrhosis3.3. Bacterial pneumoniaBacterial pneumonia4.4. Malignancy: metastatic tumor or Malignancy: metastatic tumor or
mesotheliomamesothelioma5.5. Pulmonary embolizationPulmonary embolization6.6. Viral infectionViral infection7.7. AIDSAIDS

Tuberculous pleuritisTuberculous pleuritis Chylothorax: rupture of thoracic ductChylothorax: rupture of thoracic duct Hemothorax: hematocritHemothorax: hematocrit>50 that of the >50 that of the
peripheral blood: caused by trauma, peripheral blood: caused by trauma, rupture of a blood vessel or tumorrupture of a blood vessel or tumor

TreatmentTreatment On etiologyOn etiology1.1. Tuberculous pleuritis: anti-TB Tuberculous pleuritis: anti-TB
chemotherapychemotherapy2.2. Parapneumonic effusion: antibioticsParapneumonic effusion: antibiotics3.3. CHF, liver cirrhosis, nephrotic CHF, liver cirrhosis, nephrotic
syndrome: improving systemic syndrome: improving systemic functionsfunctions
4.4. Malignant effusion: metheliomaMalignant effusion: methelioma5.5. Pulmonary embolizationPulmonary embolization6.6. etcetc

Treatment on large quantity of Treatment on large quantity of effusioneffusion
1.1. Reduce effusion quantity by aspiration. Not Reduce effusion quantity by aspiration. Not over 700ml 1over 700ml 1stst time, not over 1000ml every time, not over 1000ml every time, time, because rapid & excessive reduction because rapid & excessive reduction →abrupt →abrupt of thoracic pressure → of thoracic pressure → pulmonary edema or acute edema or acute heart failureheart failure -- --pleural reactionpleural reaction
2.2. PresentationsPresentations: : dizziness, sweating, and throbdizziness, sweating, and throb3.3. Stop aspiration at once, in prostrate position, Stop aspiration at once, in prostrate position,
0.1% epinephrine 0.5ml subcutaneously0.1% epinephrine 0.5ml subcutaneously

PneumothoraxPneumothorax DefinitionDefinition1.1. In normal status, no gas in pleural cavityIn normal status, no gas in pleural cavity2.2. Gas accumulation in pleural cavityGas accumulation in pleural cavity3.3. Common emergency of internal medicineCommon emergency of internal medicine

ClassificationClassification
1.1. Spontaneous: primary or secondarySpontaneous: primary or secondary2.2. Traumatic: direct or indirect trauma Traumatic: direct or indirect trauma
of chest wallof chest wall3.3. Nosocomial: caused by diagnostic Nosocomial: caused by diagnostic
or therapeutic operationsor therapeutic operations

Etiology & pathogenesisEtiology & pathogenesis
1.1. Rupture of peripheral Rupture of peripheral alveoli, esp. bullaalveoli, esp. bulla
2.2. Injury of chest wallInjury of chest wall3.3. Aerogenous bacterial in Aerogenous bacterial in
pleural cavity –pleural cavity –rare etiologyrare etiology
Main reasons

1.1. Large quantity of gas accumulation Large quantity of gas accumulation → disappearance of pleural negative → disappearance of pleural negative pressure →increased pressure on pressure →increased pressure on heart & large blood vessels →reduce heart & large blood vessels →reduce cardiac output, rapid arrhythmia, cardiac output, rapid arrhythmia, hypotension, even shockhypotension, even shock
2.2. Tension pneumothorax → shift of Tension pneumothorax → shift of mediastinum →circulatory disorders, mediastinum →circulatory disorders, even death of suffocationeven death of suffocation

Primary pneumothoraxPrimary pneumothorax1.1. Thin, tall, male youth and adultsThin, tall, male youth and adults2.2. X-ray: bulla neighboring pleura, more X-ray: bulla neighboring pleura, more
common on apexcommon on apex3.3. Formation of bulla is unclear, may related Formation of bulla is unclear, may related
to smoking, height or bronchiolitisto smoking, height or bronchiolitis Secondary pneumothorax: Secondary pneumothorax: To other To other
pulmonary D, which cause the incomplete pulmonary D, which cause the incomplete obstruction of bronchioles, then bulla obstruction of bronchioles, then bulla formedformed

Menstrual pneumothorax: Menstrual pneumothorax: occurred occurred 24~72 Hrs before menstruation, which 24~72 Hrs before menstruation, which may caused by rupture of ectopic may caused by rupture of ectopic endometriumendometrium
Pregnancy pneumothorax Pregnancy pneumothorax occurred occurred with pregnancy (may be related to with pregnancy (may be related to hormone and thoracic compliance)hormone and thoracic compliance)

Clinical classification of Clinical classification of spontaneous pneumothoraxspontaneous pneumothorax
1.1. Closed: smaller orifice, closed with Closed: smaller orifice, closed with retraction of the lung, inner pressure of retraction of the lung, inner pressure of pleural cavity (+) or (-)pleural cavity (+) or (-)
2.2. Open: or communicated. Bigger orifice or Open: or communicated. Bigger orifice or caused by adhesion between 2 layer of caused by adhesion between 2 layer of pleura. Inner pressure of pleural cavity pleura. Inner pressure of pleural cavity waved around zero cmH2Owaved around zero cmH2O
3.3. TensionTension

Tension or pressure pneumoniaTension or pressure pneumonia1.1. Valve opened to single directionValve opened to single direction2.2. In inspiratory phase, gas enter into In inspiratory phase, gas enter into
pleural cavity with thoracic expansion, pleural cavity with thoracic expansion, but not expelled with thoracic retraction but not expelled with thoracic retraction in expiratory phasein expiratory phase
3.3. So gas accumulated So gas accumulated →→lung pressed, and lung pressed, and mediastinum shifted to opposite sidemediastinum shifted to opposite side
4.4. Shift of mediastinum influence on blood Shift of mediastinum influence on blood reflux, which , in turn influence reflux, which , in turn influence cardiopulmonary functionscardiopulmonary functions
5.5. A common emergencyA common emergency

Clinical manifestationClinical manifestation SymptomsSymptoms1.1. History of exertional activities: taking sth History of exertional activities: taking sth
heavy, breath holding, etc.heavy, breath holding, etc.2.2. Abrupt onset, characterized as a sudden Abrupt onset, characterized as a sudden
lateral cutting or probing chest pain, followed lateral cutting or probing chest pain, followed by chest oppression and dyspnea, or by chest oppression and dyspnea, or stimulant coughstimulant cough
3.3. For tension pneumothorax, severe For tension pneumothorax, severe cardiopulmonary dysfunction may appear, cardiopulmonary dysfunction may appear, characterized by fidgety, dysphoria, cyanosis, characterized by fidgety, dysphoria, cyanosis, cold sweat, rapid pulse, arrhythmia, even cold sweat, rapid pulse, arrhythmia, even comacoma

SignsSigns None if less quantityNone if less quantity Typical signs when large quantityTypical signs when large quantity1.1. Trachea shifted to opposite side, bulging Trachea shifted to opposite side, bulging
half thorax (affected side)half thorax (affected side)2.2. Respiratory movement & fremitus reducedRespiratory movement & fremitus reduced3.3. Hyperresonance, disappearance of cardiac Hyperresonance, disappearance of cardiac
or hepatic dullnessor hepatic dullness4.4. Breath sound may disappear or reduceBreath sound may disappear or reduce

Sinus phrenicostalis

X-rayX-ray Typical charactersTypical characters Arc linear shadow (oppressed margin)Arc linear shadow (oppressed margin) Evaluation of accumulated gasEvaluation of accumulated gas1.1. Distance between lateral chest wall and Distance between lateral chest wall and
lung margin: large amount if lung margin: large amount if ≥≥2cm, small 2cm, small amount if <2cmamount if <2cm
2.2. Distance between apex and top of thoracic Distance between apex and top of thoracic top: large amount if top: large amount if ≥≥3cm, small amount if 3cm, small amount if <3cm<3cm


DiagnosisDiagnosis
Large amount of gas Large amount of gas accumulation could be accumulation could be determined by typical symptoms, determined by typical symptoms, signs and X-ray presentationssigns and X-ray presentations
Small amount of gas Small amount of gas accumulation lack symptom or accumulation lack symptom or signs, which should be alertsigns, which should be alert

Differential diagnosisDifferential diagnosis1.1. AsthmaAsthma2.2. Obstructive emphysemaObstructive emphysema3.3. Acute myocardial infarctionAcute myocardial infarction4.4. Pulmonary thromboembolismPulmonary thromboembolism5.5. Pulmonary bullaPulmonary bulla6.6. OthersOthers

TreatmentTreatment Aim: help to restore lung expansion, eAim: help to restore lung expansion, eradicate etiology, reduce collapseradicate etiology, reduce collapse1.1. Conservative therapyConservative therapy2.2. Closed thoracic drainageClosed thoracic drainage3.3. Sclerification with chemical hardening agentSclerification with chemical hardening agent4.4. SurgerySurgery5.5. Treatment on complicationsTreatment on complications

MethodMethod: : Gas ejection by thoracentesisGas ejection by thoracentesis IndicationIndication: small amount of gas, slight dysp: small amount of gas, slight dyspnea, good cardiopulmonary function, and clnea, good cardiopulmonary function, and closed pneumothoraxosed pneumothorax Amount for every ejection Amount for every ejection << 1000ml, qd or qo 1000ml, qd or qodd
1. Conservative therapy1. Conservative therapy

For tension pneumothoraxFor tension pneumothorax Resolve thoracic positive pressure in emergenResolve thoracic positive pressure in emergency, or else, severe complications may occurcy, or else, severe complications may occur Thoracentesis at once, emergent gas ejection Thoracentesis at once, emergent gas ejection should be performed, in order to reduce thorashould be performed, in order to reduce thoracic pressurecic pressure

IndicationsIndications1.1. Unstable pneumothoraxUnstable pneumothorax2.2. Significant dyspneaSignificant dyspnea3.3. Severe lung collapse Severe lung collapse 4.4. Communicated or tension pneumothoraxCommunicated or tension pneumothorax5.5. Recurrent frequentlyRecurrent frequently6.6. Any one of the above met, whatever the Any one of the above met, whatever the
amount of gas accumulationamount of gas accumulation
2. Closed thoracic drainage2. Closed thoracic drainage

In order to avoid recurrence, chemical In order to avoid recurrence, chemical hardening agent was injected to pleural hardening agent was injected to pleural cavitycavity
The production of aseptic inflammation The production of aseptic inflammation caused the adhesion of visceral and caused the adhesion of visceral and parietal pleura to close the cavityparietal pleura to close the cavity
3. Chemical pleural sclerification3. Chemical pleural sclerification

Indications for Closed thoracic draiIndications for Closed thoracic drainagenage1.1. Persistent or recurrentPersistent or recurrent2.2. Bilateral pneumothoraxBilateral pneumothorax3.3. Accompanied with bullaAccompanied with bulla4.4. Pulmonary dysfunction, not endure the sPulmonary dysfunction, not endure the surgeryurgery Common hardening agents: Common hardening agents: 多西环素、多西环素、 tatalc powder (lc powder ( 滑石粉滑石粉 ), etc; diluted by norm), etc; diluted by normal saline 60~100ml, then injected by draial saline 60~100ml, then injected by drainage duct, occluded for 1~2 Hrs; sprinkle nage duct, occluded for 1~2 Hrs; sprinkle hardening agent under thoracoscopehardening agent under thoracoscope
Refuse surgery

4. Surgery4. Surgery IndicationsIndications1.1. Ineffective by medical methodsIneffective by medical methods2.2. Persistent, bilateral, recurrent Persistent, bilateral, recurrent
pneumothoraxpneumothorax3.3. Tension pneumothorax, failed in Tension pneumothorax, failed in
drainagedrainage4.4. Thickened pleura Thickened pleura →→atelectasisatelectasis5.5. Or multiple bullaOr multiple bulla More success, low recurrenceMore success, low recurrence Methods: via thoracoscope or open Methods: via thoracoscope or open
surgerysurgery

5. Treatment on complications5. Treatment on complications