-
Acquis et perspectives des traitements
systémiques et thérapies ciblées
néoadjuvants
17 Octobre 2014
Jean-‐Yves Pierga Département d’Oncologie
médicale
Institut Curie
-
Définition d’un traitement néoadjuvant
(NCI)
• Traitement donné en première intention
pour réduire le volume d’une
tumeur avant le traitement principal
qui est habituellement la chirurgie
!
• Chimiothérapie, radiothérapie, hormonothérapie
• Traitement d’induction
National Cancer Institute. NCI
dictionary of cancer terms. Available
at: http://www.cancer.gov/dictionary?CdrID=45800.
Accessed April 25, 2014
http://www.uvp5.univ-paris5.fr/CAMPUS-GYNECO-OBST/cycle2/poly/2968ico.asp
-
Traitement néoadjuvant
• Historique • Conservation d’organe • Réponse
histologique • Evaluation de nouvelles
molécules • Hétérogénéité tumorale • Impact
sur la maladie micrométastatique
-
Objectifs du traitement néoadjuvant
➢Réduire le volume de la Tumeur
!
➢Commencer plus tôt le traitement
systémique : impact sur la
survie à long terme? !
➢Contrôler l’efficacité du protocole de
chimiothérapie
Chir conserv.
Chirurgie
-
Premières Indications!.$,'$&3(%0+2"&-@)'3(( (
A(/-01'&3()+1-)','04(-*-01"3(( (
Y.+"6/('-'DXQ%0B
( ( A(/-01'&3()+1-)','04(-*-01"3(
Y.+"6/('-'DXQ%0B
-
Historique• In 1956, neoadjuvant therapy
was used to treat choriocarcinoma.6,7
• In 1968, the concept of
perioperative chemotherapy for breast
cancer was introduced.8
• Neoadjuvant therapy for rectal cancer
was presented in 1986 and for
pancreatic cancer in 1990.9,10 6.Hertz
R, Li MC, Spencer DB. Effect
of methotrexate therapy upon
choriocarcinoma and chorioadenoma. Proc
Soc Exp
Biol Med. 1956;93(2):361-‐366. 7.Li MC,
Hertz R, Bergenstal DM. Therapy
of choriocarcinoma and related
trophoblastic tumors with folic acid
and purine antagonists. N Engl
J Med. 1958;259(2):66-‐74. 8. Fisher
B, Ravdin RG, Ausman RK, Slack
NH, Moore GE, Noer RJ. Surgical
adjuvant chemotherapy in cancer of
the breast: Results of a decade
of cooperative investigation. Ann
Surg. 1968;168(3):337-‐56. 9. Smith
DE, Muff NS, Shetabi H.
Combined preoperative neoadjuvant
radiotherapy and chemotherapy for
anal and rectal cancer. Am J
Surg. 1986;151(5):577-‐580. 10. Weese
JL, Nussbaum ML, Paul AR,
Engstrom PF, Solin LJ, Kawalynshyn
MJ, Hoffman JP. Increased
resectability of locally advanced
pancreatic and periampullary carcinoma
with neoadjuvant chemoradiotherapy. Int
J Pancreatol. 1990;7(1-‐3):177-‐185
-
Rationnel pour le traitement
néoadjuvant
• Réduire la taille tumorale avant
chirurgie • Faciliter la procédure
chirurgicale • Réduire le volume de
tissue devant être retiré • Réduire
ainsi la morbidité du geste
chirurgical • Effet sur les ganglions
loco-‐régionaux (stérilisation de certains
ganglions)
Bailey L Bulletin of American
College of Surgeons, JUN 2014
-
Conservation d ’organe
La réponse clinique permet-‐elle
d’améliorer le taux de conservation?
!
Utilisation dans les cancers
opérables
-
Sarcome d ’Ewing opéré
-
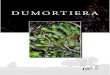
Osteosarcoma
Changing pattern of surgery
with time (by year of
diagnosis).
Dark shading represents
amputation/disarticulation; grey, rotation
plasty; and white, (limb-‐saving)
resection.
1,702 patients Treated on
Neoadjuvant Cooperative Osteosarcoma Study
Group Protocols
Stefan S. Bielack,
Journal of Clinical Oncology, Vol
20, 2002: 776-‐790
-
Mastectomie
http://www.ncbi.nlm.nih.gov.gate2.inist.fr/pubmed?term=NSCLC%20Meta-analysis%20Collaborative%20Group%5BCorporate%20Author%5D
-
L2'&-@)'(P&'-34(/-01'&
M4&-4%=%1-4%+0Q(R:'Q(/)%0%1-)(.$,+&(M%S'Q(/)%0%1-)(J+#-)(M4-4$3
L2'&-4%+0
T(.RU(%=(VWH(6&3?
R/(C(XT(.RU(%=(VWH(6&3?
R/(C(X
L2'&-4%+0
JMRPO(PAEY
Z[%3>'&F(P?F(\/LF(E]]GF(E]]Y^(
-
O(_(H?HE
O&'+2(/>',+
O+34+2(/>',+
PAEY!B$,2'14+,6(!-4'
`Ha`Ya
YHa
`Ha
XHa
IHa
H
-
Tumorectomie
-
C40601 (1)Schéma de l'étude
Stade II-‐III
HER2+
wT+L x 16 sem.
R wT+H x 16 sem.
wT+H+L x 16 sem. Recommandé :
Chimiothérapie AC
dose dense ➔ H x 34 sem.
ASCO® 2013 -‐ D'après Ollila DW
et al., abstr. 501 actualisé
C H I R U R G I
E
Prélèvement tissulaire
*wT = paclitaxel hebdomadaire, H =
trastuzumab, L = lapatinib
• Critère principal : réponse complète
histologique sein (*ASCO 2013) •
Critères secondaires :
– Cliniques : RC histologique sein
et ganglions*, tolérance*, survie
sans récidive, survie globale
– Recherche translationnelle*
Prélèvement tissulaire
-
Pré-‐traitement
C40601 (2)Eligibilité à la chirurgie
conservatrice mammaire (CCM)
305 patientes, 292 évaluables pour
TC (traitement conservateur)
ASCO® 2013 -‐ D'après Ollila DW
et al., abstr. 501 actualisé
Décision du chirurgien pour TC
?
Traitement néoadjuvant
Non 169 (58 %)
Oui 116 (94 %)
Non 7 (6 %)
Oui 72 (43 %)
Non 97 (57 %)
TC?
Oui 123 (42 %)
TC?
-
Chimiothérapie néo-‐adjuvante• Cancer du sein:
maladie loco-‐régionale ou systémique?
!
⬥Principes de Halsted !
⬥Dissémination précoce (B. Fisher) •En
dehors de la voie lymphatique
•Action sur la Maladie
Micrométastatique
-
].',(+&%60'-('V.5&)(-
-
!e=='14(+=(3$&:%1-)(&',+*-)(+0(4>'(:&+f4>(-0#(j%0'4%13(+=(&'3%#$-)(4$,+&!
N$0#$SF([%3>'&(P(/RJ/e!((!eMeR!/d(g]?(gY`EAgY`W?(E]G]
-
Impact sur la survie globale
-
Davide Mauri et al, Journal of the National Cancer Institute,
Vol. 97, 2005
Neoadjuvant Versus Adjuvant Systemic Treatment in Breast Cancer:
A Meta-Analysis
3946 patients Comparison
of neoadjuvant therapy with adjuvant
therapy no statistically or
clinically significant difference with
death, disease progression or distant
disease recurrence
-
Presurgical Chemotherapy Compared With
Immediate Surgery and Adjuvant
Chemotherapy for Nonmetastatic
Osteosarcoma: Pediatric Oncology Group
Study
POG-‐8651
Allen M. Goorin, JCO, 2003, 21,
1574 N=106
-
O&'+2'&-4%*'(1>',+4>'&-26(=+&(0+0A3,-))A1'))()$0:(1-01'&8(-(3634',-4%1(&'*%'f(-0#(,'4-A-0-)63%3(+=(%0#%*%#$-)(2-&4%1%2-04(#-4-!
IYF]F'^().?.0.51&%&'F655.46+.)%,('d+6$*N'].0"()N';
-
J'+-#K$*-04(/>',+4>'&-26(+&(O&%,-&6!M$&:'&6(%0(M4-:'(ccc/(+&(cl(L*-&%-0(/-01'&
j(+B6)('I'X0B5'>'^(-';
-
Réponse histologique
Quelle échelle d’évaluation ?
-‐ Evaluation de la réponse
histologique ?
-‐ Relation avec la survie
globale ?
-
PAEY!/)%0%1-)(-0#(O-4>+)+:%1(P&'-34(.$,+&(!'32+03'(4+(O&'+2(/>',+(Z`YW(243^
g`a
IHa
Xga
1/!(ZIX](243^
1O!(ZI]`(243^
1Mi(T(1Oi(ZEXH(243^
Iga
Xa
]a
2c0*(ZE`H(243^
2J+0Ac0*(ZI`(243^
2/!(Z`g(243^
-
PAEY!i%3'-3'A[&''(-0#(L*'&-))(M$&*%*-)!
R11+%0:(4+(!'32+03'
H
IHa
XHa
`Ha
YHa
EHHa
I X ` Yn'-&
OoH?HHHHW2cJl1O!1J!
2/!
I X ` Y
2cJl1O!1J!
2/!OoH?HHHY
k+),-&j(J8(/i/F(IHHH
-
d+0j++2('4(-)(ZE]]Y^*
[%3>'&('4(-)((ZE]]Y^
M-4-)+==!'4(-)!"E]]W#
p$'&'&('4(-)(ZE]]]^
/>'*-))%'&('4(-)(ZE]]g^*
O-4>+)+:%1-)(N&-#%0:(M634',3
U%))'&(q(O-60'('4(-)(ZE]]X^
*2/!(%01+&2+&-4'3()6,2>(0+#'3 O+34(1>',+
k%4>+$4(1>',+
-
EFS selon le volume et la réponse Histologique
EFS selon le volume de la
tumeur et la réponse histologique
à la chimiothérapie pour les
patients traités par chimiothérapie
seule avant chirurgie (données
regroupées de la SFOP et du
GPOH)
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6 7 8 9 10 Years
< 200 ml - < 10%, n = 168
>= 200 ml - < 10%, n = 73
< 200 ml - >= 10%, n = 66
>= 200 ml - >= 10%, n = 39
Volume - Cellules résiduelles
p < 10-5
Sarcome d’EwingSarcome d’Ewing
-
L*'&-))(3$&*%*-)(-11+%0:(4+(>%34+)+:%1-)(&'32+03'(%0(EFGHI(2-4%'043(.&'-4'#(+0(J'+-#K$*-04(/++2'&-4%*'(L34'+3-&1+,-(M4$#6(N&+$2(O&+4+1+)3(!
!'32+03'(:&-#'#(-11+%0:(4+(M-)S'&Ap$0431>%j('4(-)!!
Y)(G.0'YN'_%(5."fM''AB?2C05)BD)&56C6>05)'C>B5BEFAB?2C05)BD)&56C6>05)'C>B5BEFM'j65';
-
P. Cortazar Lancet 2014
-
P. Cortazar Lancet 2014 on line Feb
-
Méta-‐analyse des essais randomisés
néo-‐adjuvants
1,0
0,8
0,6
0,4
0,2
0,00 50 100 150 200
pCR (n = 2 131)Sans pCR (n
= 9 824)
HR = 0,48 ; p < 0,001
Mois
Survie sans événement
1,0
0,8
0,6
0,4
0,2
0,00 50 100 150 200
pCR (n = 2 131)Sans pCR (n
= 9 824)
HR = 0,36 ; p < 0,001
Mois
Survie globale
Survie en fonction de la pCR
P. Cortazar Lancet 2014 on line Feb
-
• The FDA may grant accelerated
approval • on the basis of a
surrogate end point that is •
“reasonably likely to predict clinical
benefit.” • For neoadjuvant breast-‐cancer
treatment, • we propose that the
rate of pathological • complete
response be used as this
surrogate.
Pathological Complete Response and
Accelerated Drug Approval in Early
Breast Cancer !Tatiana M. Prowell,
M.D., and Richard Pazdur, M.D.
n engl j med 366;26 june 28,
2012
-
.&-34$S$,-@('4(2'&4$S$,-@(3'()%'04(3$&(#%=="&'043("2%4+2'3('4(2'$*'04(-*+%&($0'(-14%*%4"(360'&:%7$'
K+.&)$\$/.4'-%&+$*)&'5%B.0-?%0-(*(0-(0)'VXW;?VXWb?AEbe'"6/*5(`'K+.&)$\$/.4'*+(,(0)&'VXW;'+("(*)6+'&3(--%0B'K+.&)$\$/.4'456"f&'VXW;'&%B0.5%0B'.0-'G5.B&'"(55&'G6+'-(&)+$")%60'41')3('%//$0('&1&)(/',%.'!CFF
de!I
.&-34$S$,-@O'&4$S$,-@ de!g
de!I
A?C99650)89)05:)&0C>82)&855:)"**GH+=IJ"G-JJ*H)KFC84)89)05:)L09)M8N)&0C>82:!"**=H=I,J+-,=J:)MBO6C4PF:)$CC?)M8N)Q8R:)"**JH==IJ,,-J=S:
A(+)$\$/.4'*+(,(0)&'5%B.0-?%0-$"(-'VXW;?VXWb'-%/(+%\.)%60'A(+)$\$/.4'-6(&'06)'*+(,(0)'VXW;'+("(*)6+'&3(--%0B'c5.B&'"(55&'G6+'-(&)+$")%60'41')3('%//$0('&1&)(/',%.'!CFF
M$@#+,-%0(cl(+=(de!I i%,'&%S-4%+0(#+,-%0(+=(de!I
-
/BeLOR.!R(8(M1>",-(#'()
-
0 10 20 30 40 50 60 700
10
20
30
40
50
60
70
80
90
100
Nb à risque402 371 318 268 226 104 28 1Ptz +
T + D
Temps (mois)
HR = 0,68
IC 95 % 0,56 –
0,84
p = 0,0002
Ptz + T + D Pla + T
+ D
Survie globale (%
)
D, docetaxel; Pla, placebo; Ptz,
pertuzumab; T, trastuzumab
406 350 289 230 179 91 23 0Pla + T +
D
ITT population, Stratified by geographic
region and neo/adjuvant chemotherapy
Analyse final de la survie
globale
Median follow-‐up 50 months
(range 0-‐70 months)
S. Swain et al., PPS, ESMO®
2014
40.8
mois
56.5
mois
Δ 15.7
mois
-
NeoSphere: design de l’étude
THP (n=107)
docetaxel + trastuzumab
+
pertuzumab
HP (n=107)
trastuzumab + pertuzumab
TP (n=96)
docetaxel + pertuzumab
!S
U
R
G
E
R
Y
docetaxel q3w x 4→FEC q3w x 3 trastuzumab q3w cycles 5–17
FEC q3w x 3 trastuzumab q3w cycles 5–17
FEC q3w x 3 trastuzumab q3w cycles 5–17
FEC q3w x 3 trastuzumab q3w cycles 5–21
Study dosing: q3w x 4
TH (n=107)
docetaxel + trastuzumab
Patients with operable or
locally
advanced /inflammatory*
HER2-‐positive BC
Chemo-‐naïve &
primary tumors
>2cm (N=417)
BC, breast cancer; FEC, 5-fluorouracil, epirubicin and
cyclophosphamide
*Locally advanced=T2–3, N2–3, M0 or T4a–c, any N,
M0; operable=T2–3, N0–1, M0; inflammatory = T4d, any N, M0
H,
trastuzumab; P, pertuzumab; T, docetaxel
3
-
H, trastuzumab; P, pertuzumab; T,
docetaxel
p values from
Cochran-‐Mantel-‐Haenszel test and adjusted
for multiplicity
p=0.0198
TH THP HP TP
p=0.014150
40
30
20
10
0
pCR, % ±
95%
CI
p=0.003
29.0
45.8
16.824.0
Gianni L, et al. Lancet
Oncol 2011 DOI:10.1016/S1470-‐2045(11)70336-‐9
L’association du pertuzumab au docetaxel
donne des résultats équivalents au
docetaxel traztuzumab
Le bras sans chimiothérapie avec
les deux anticorps montre une
activité biologique nette
La combinaison du pertuzumab au
trastuzumab avec le docetaxel
augmente de façon considérable le
taux de pCR
Réponse histologique
-
• FDA NEWS RELEASE • For Immediate
Release: Sept. 30, 2013
FDA approves Perjeta for neoadjuvant
breast cancer treatment
First drug
approved for use in preoperative
breast cancer
• The U.S. Food and Drug
Administration today granted accelerated
approval to Perjeta (pertuzumab) as
part of a complete treatment
regimen for patients with early
stage breast cancer before surgery
(neoadjuvant setting). Perjeta is the
first FDA-‐approved drug for the
neoadjuvant treatment of breast
cancer.
-
Rationale for drug development in
the neoadjuvant setting
• Rapid assessment of efficacy • Smaller
sample size • Biomarker development
and validation • Discovery of
mechanisms of resistance to
therapy
-
O-4%'04('0(1+$&3(#
-
Impact sur la maladie
micrométastatique
-
Klein, C. Science 2008Endométriose?
-
RECIRCULATION !Is cancer a disease of self-seeding?!
Larry Norton & Joan Massagué Nature Medicine, 12, 2006
Kim & Massagué, Cell Dec 2009
-
Self-‐Seeding: auto-‐ensemencement?
! Comen, E. et al. Nat. Rev. Clin. Oncol. 8, 369–377 (2011)
-
K$/6+'&(5G'&((-%0B
Kim & Massagué, Cell Dec 2009
K$/6+'&(5G'&((-%0B
Tumor-derived cytokines IL-6 and IL-8!act as CTC attractants
!whereas MMP1/collagenase-1!and the actin cytoskeleton component
fascin-1 are mediators of CTC infiltration into mammary tumors
-
Méthodes de détection des DTC au
niveau médullaire
Adapted from Pantel K, Nature
Cancer Reviews, 2004, 4, 448
1x10 6 CMN/cytospot X 3
slides
on EDTA
!Preoperative bilateral bone marrow
aspirations from both anterior iliac
crests (3 to 5 ml per
sample) Or one bone marrow
aspiration under local anesthesia
from posterior iliac crest or
sternum (3 to 5 ml per
sample)
Same number of control slides
-
YN'_+.$0M'IX>^';
-
Pooled Analysis of Bone Marrow Aspirations during
Recurrence-free Follow-up (n=676)
Overall Survival by Bone Marrow Status
Janni W et al, Clin Cancer Res 17(9); 2967–76 2011
-
A+6B06&)%"'Y%B0%G%".0"('6G'C%&&(/%0.)(-'K$/6+'F(55&'%0')3('_60('^.++6Q'6G'A+6&).)('F.0"(+'A.)%(0)&'K+(.)(-'g%)3'I(6.-7$,.0)'V6+/60('K+(.)/(0)!
A8C4)XY5582T0CC;)89)05)A&')"**Z
-
!Models, mechanisms and clinical evidence for cancer
dormancy"
Julio A. Aguirre-Ghiso, Nature Cancer Reviews, 2007
Dissémination métastatique!La dormance
-
56
Les cellules souches tumorales
Caractéristiques des cellules souches
1/ Auto-‐renouvellement
2/ Potentiel multiple
3/ Potentiel de prolifération
!
C.T. Jordan, NEJM sept 2006
-
Cellules souches du cancer du sein
(Breast cancer
initiating cells BrCA-‐IC)
•(Phénotype CD44+,CD24- /low, ESA+)
M. Wicha, Michigan, Ann Arbor
-
Change in CTC count during
therapy, by patient
Pierga et al, Lancet Oncol 2012
Non correlation with other parameters including pCR
BEVERLY 2
Inflammatory Breast cancer
HER2+
N=52
-
EFG'#**+/.($%'-+'3#?&=($&'!)!?'*#-&%+/1
Pierga ESMO 2014
-
EFG'#**+/.($%'-+'3#?&=($&'!)!?'*#-&%+/1'#$.'0!7'?-#-,?
Pierga ESMO 2014
-
@H-H/+%H$H(-H'-,>+/#=&
9#0'&-'#=2'M1%'01'.&-03)-4%+0-)U'#%1%0'I:JK:'6+='L'K:M0?KJ
-
N/*"(-&*-,/&'OH$+>(P,&'.&?'-,>&,/?
!'N/3+/&?*&$*&'Q-/+$*2'3/#$*"&?R
Shared!primary
Shared!metastasis
Private
Metastatic mutations (and allelic imbalances) are:!!• shared
between 1° and 2° tumours!• different between 1° and 2° tumours
Ubiquitous
Derived from Gerlinger et al., 2012 NEJM
-
@H-H/+%H$H(-H'-,>+/#=&
9#0'&-'#=2'M1%'01'.&-03)-4%+0-)U'#%1%0'I:JK:'6+='L'K:M0?KJ9#0'&-'#=2'M1%'01'.&-03)-4%+0-)U'#%1%0'I:JK:'6+='L'K:M0?KJ
-
@H-H/+%H$H(-H'-,>+/#=&
9#0'&-'#=2'M1%'01'.&-03)-4%+0-)U'#%1%0'I:JK:'6+='L'K:M0?KJ
-
Klein CA, Cell Cycle 3:29-‐31,
2004
-
T(O-1)%4-C')(YH(,:r,I
T(O-1)%4-C')(YH(,:r,I
T(O-1)%4-C')(YH(,:r,I
B&+SN8))T'Q4;O'KSJUR• BCLDD2'@57:A'Q=+*#=R2'V':'*>
W(**#/-SO&3"#/-'&-'05:2'GN4!G':JKX2'GKSJK
* Réduction posologie à 750 mg/jour avec le paclitaxel
(amendement oct 2008)
.&-34$S$,-@(X(,:rj:(! I(,:rj:
B-2-4%0%@(EWHH(,:rK
B-2-4%0%@(EHHH(,:rKs(T!.&-34$S$,-@(X(,:rj:(! I(,:rj:
R .&-34$S$,-@(Y(,:rj:(! `(,:rj:
B-2-4%0%@(EWHH(,:rK
B-2-4%0%@(EHHH(,:rK(T!.&-34$S$,-@(Y(,:rj:(! `(,:rj:
`(3',-%0'3 T(EI(3',-%0'3 gX(3',-%0'3
-
B&+N8))T'Y'0!7
Baselga J Lancet 2012
-
!"#$%&'()*&+&,-&./00123+4567123&53&18-9&16:32-&;
Toutes les patientes : radiothérapie si indiquée (concomitante
avec les thérapies ciblées). Patientes RH+ : hormonothérapie pour
au moins 5 ans. Shéma 2 A : w-P : paclitaxel hebdomadaire ; 3-w D:
docétaxel toutes les 3 sem. Shéma 2B: 3-w D : docétaxel/3 sem. ;
carbo : carboplatine !
Lapatinib
34 weeks6 wks12 weeks
Trastuzumab/3 sem
Toutes les patientes : radiothérapie si indiquée (concomitante
avec les thérapies ciblées). Patientes RH+ : hormonothérapie pour
au moins 5 ans. Shéma 2 A : w-P : paclitaxel hebdomadaire ; 3-w D:
docétaxel toutes les 3 sem.Shéma 2B: 3-w D : docétaxel/3 sem. ;
carbo : carboplatine
Shéma 1:
T!"#$%&%'$("'$#)*+,-(./01%'$#%2("3!4.(2"(56#$6/!"3#%(8'(9(:(;(!?56/&"(-@(A($!"#$%&%'$("'$#)*+,-(57'57$"'$("3!4.(BC(D(E".%(FG"'$6!"5H52#'%(8'(9(=(==I>(!?56/&"(-J(A($!"#$%&%'$("'$#)*+,-(57'57$"'$(D(1'%(56#$6/!"3#%(."'.("'$6!"5H52#'%(8'(9(:=((((!!!!!
34 weeks6 wks12 weeks Lapatinib + trastuzumab/3 sem.
LapatinibTrastuzumab hebdomadairewash!out
52 sem.
34 sem.6 sem.12 sem.
+$1F%(@KCCL(F%(36".%(MMM(57&3"!"'$(1'("'(F%($!"#$%&%'$("'$#(*+,-((3"!(2"3"$#'#E(.%12(8K>N(C!".$1O1&"E(.%12(8C>N(2%1!(./01%'5%(8K(C>(71((
2%1!(57&E#'"#.7'((8CPK>(F"'.(2%(5"'5%!(F1(.%#'(3!/575%(*+,-P
-
Suivi médian = 4,5 ans
* 97.5% CI
ASCO® 2014 -‐ M. Piccart-‐Gebhart
et al., abstr. LBA4 actualisé
Étude ALTTO (3) Survie sans
rechute (SSR)
Survivan
ts sa
ns m
alad
ie
Années
Bras Nb patients Nb EvtsTaux de SSR
à 4
ansHR
cf Tras* p
**
**p < 0,025 requis pour
significativité
-
ADN tumoral circulant
! H. Schwarzenbach, D S. B. Hoon K. Pantel Nature Reviews Cancer
2011
-
C Bettegowda et al ScienceTranslationalMedicine 19 February 2014
Vol 6 Issue 224 224ra24
-
MX
[/$%5$#7'(F%(&1$"$#7'(.3/5#Z#01%(F%($1&%1!(F"'.(2G@[\($1&7!"2(5#!512"'$(8@[\5$>A(3!/F#5$#7'(F%(2"(!/5#F#Q%("3!4.(56#$6/!"3#%(3!%!%(
BC1D2E:&F=2G52&H&53&18-9&16:32-&I))9&103=18/:>
]"$#%'$%.((3!/.%'$"'$(1'(5"'5%!(F1(.%#'(275"2#./(
F/E1$"'$(1'%(56#$6/!"3#%('/7"F^1Q"'$%
• 4(+0?(&'.(#%$+?-(P,&'.&'=#'-,>&,/'–
!"(/,/%(&'Q0+,/'=&?'0#-(&$-&?'#[&*',$&'>#=#.(&'/H?(.,&==&R'
• W=#?>#'0+,/'&\-/#*-(+$'.&'=
N̂EB'=(3/&'*(/*,=#$-'Q5E)NR'– 4#?&=($&'–
W+?-S*"(/,/%(&'–
)+,?'=&?'U'>+(?'0&$.#$-'=&'?,([(
B6#$6/!"3#%('/7"F^1Q"'$%( ]7.$(56#!1!Y#%
?1#Q#(.$"'F"!F!0/H=_[&>&$-'.&'?#$%'-+,?'=&?'U'
>+(?
!'@';'7'`'7'O';'5
-
ML
@'$#5#3"$#7'("Q"'$(2"(!/5#F#Q%(52#'#01%
KJ'JJJ'
K'JJJ'
KJJ'
KJ'
K'
BE
_1$
"'$(5
73#%
.`&
2
;$*=,?(+
$
!"(/,/%
(& U K: Ka :L
_7#.(37.$)56#!1!Y#%
)WDX'*IO'V')a:L
!"(>(+-"H/#0(&
)/#?-,b,>#3
8&-/+b+=&
KX2D>+(?'.
#̂$-(*(0#-(+$''.&'=#'/H*(.([&'*=($(P,&
!#$*&/'.,'?&($'7T'A[&'@57:'A'&$'/H0+$?&'*+>0=_-&''"(?-+=+%(P,&'>#>>#(/&'&-'%#$%=(+$$#(/&'#0/_?'*"(>(+-"H/#0(&''$H+#.c,[#$-&'&-'-/#?-,b,>#3
)&>0?'>H.(#$'.
#̂$-(*(0#-(+$'#[#$-''-+,-&?'=&?'/H*(.([&?'*=($(P,&?Y'a'>+(?
BC1D2E:&F=2G52&H&53&18-9&16:32-&I))9&103=18/:>
-
MD
]!/F#5$#7'(F%.(!/5#F#Q%.(3!/575%.(a(F/$%5$#7'(F%.(&1$"$#7'.?1
!Q#%
(."'.
(&"2
"F#%
J
:D
DJ
MD
KJJ
_7#.(37.$)56#!1!Y#%
J U K: Ka :L
NEB-*'&$'#,%>&$-#-(+$'
BH%#-([&
0'C'J2JJM
8#'.H-&*-(+$'.1$#>(P,&'.&'=
#̂00#/(-(+$''.&'>,-#-(+$'&?-'"#,-&>&$-'0/H.(*-([&'
'.&'/H*(.([&?'0/H*+*&?
\/7"F^1Q"'$(56#$6/!"3#% ]7.$(56#!1!Y#%
?$"'F"!F(Z7227b)13!3=++.'?#>0=&?'&[&/1'U'>+(?
L K
J KM
0'C'J2JJJM
L1#
\7'
PQ% )Q%!!
F/$%5$#7'([%(2G@[\$5!
,%561$%(3!/575%
@1Y&%'$"$#7'(F%(2G@[\$5("3!4.(56#!1!Y#%
BC1D2E:&F=2G52&H&53&18-9&16:32-&I))9&103=18/:>
B(*(M(,(c(,(d(M(+
-
Conclusions
• Réponse de la tumeur primitive
est un indicateur partiel d’impact
du traitement systémique sur la
maladie micrométastatique !
• Cette dissociation peut être plus
grande dans le cadre d’une
association radio-‐chimiothérapie
-
Conclusions• Corrélation entre pCR et
survie mais Différence de valeur
de la pCR selon le
sous-‐type histologique • pCR marqueur
intermédiaire d’efficacité d’un traitement
(Validation FDA) o Indications «
larges » de chimiothérapie
néo-‐adjuvante dans les cancer du
sein HER2+ ou triple négatif o
L’utilisation en préopératoire permet
une évaluation in vivo de
l’efficacité du traitement
(évaluation de la pCR) o Indication
de chimiothérapie adjuvante à partir
du T1bN0
o Indication dans les tumeurs luminales
B o En fonction de la
prolifération o Développement d’outils
prédictifs (DLD30, ….) o Objectifs de
conservation mammaire o Hétérogénéité
tumorale et problème de fiabilité
de la biopsie
-
Chimiothérapie néo adjuvante!
,/F1#!%(2%(Q721&%(F%(2"(C1&%1!(
!@1Y&%'$%!(2"(56#!1!Y#%(57'.%!Q"$!#5%(
!
B7&&%'5%!(321.($e$(2%($!"#$%&%'$(.H.$/%(!]".(FG"Q"'$"Y%(F/&7'$!/(%'(.1!Q#%(Y27E"2%`"F^1Q"'$(
!
B7'$!e2%!(2G%ZZ#5"5#$/(F1(3!7$7572%(F%(56#$6/!"3#%(!C!"#$%&%'$(F%(!"$$!"3"Y%f(
!
+Q"21%!(3!/575%&%'$(1'%('71Q%22%($6/!"3%1$#01%(!+'!%Y#.$!%&%'$(FG1'%('71Q%22%(&72/512%
?1!Y%!H ,%2"3.%?H.$%($6%!"3H
?H.$%($6%!"3H ?1!Y%!H 3B,
Adjuvant trial:
Neoadjuvant trial:Weeks
Years
BCS, breast-conserving surgery; pCR, pathological complete
response.!1. Fisher B, et al. J Clin Oncol 1997; 15:2483–2493; 2.
Wolmark N, et al. J Natl Cancer Inst Monogr 2001; (30):96–102;"3.
Kaufmann M, et al. Ann Surg Oncol 2012; 19:1508–1516; 4. Kaufmann
M, et al. J Clin Oncol 2006; 24:1940#1949;!5. Amos KD, et al. Int J
Breast Cancer 2012; 2012:385978; 6. Buzdar AU. Cancer 2007;
110:2394–2407.
-
Conclusions
• Double blocage dans les cancers
du sein HER2+ • Enregistrement
du pertuzumab? Programme d’accès
• Pas de bénéfice clairement démontré
du bevacizumab
• Place des sels de platine dans
les cancers triple négatifs ?
-
INSTITUT CURIE