Embed Size (px)
Citation preview

Inhalation Toxicology, 2009; 21(13): 1077–1091
R E S E A R C H A R T I C L E
Determination of carboxyhaemoglobin in humans following low-level exposures to carbon monoxide
Nathalie H. Gosselin1, Robert C. Brunet2, and Gaétan Carrier3,4
1Pharsight, Montreal, Quebec, Canada, 2Département de Mathématiques et de Statistique and Centre de Recherches Mathématiques, Faculté des arts et des sciences, Université de Montréal, Montréal, Québec, Canada, 3Département de santé environnementale et santé au travail and Groupe de recherche interdisciplinaire en santé, Faculté de Médecine, Université de Montréal, Montréal, Québec, Canada, and 4Institut national de santé publique, Montréal, Québec, Canada
Address for Correspondence: Nathalie Gosselin, 2000 Peel Street, Suite 570, Montreal, Quebec H3A 2W5, Canada. E-mail: [email protected]
(Received 21 September 2008; revised 5 January 2009; accepted 13 January 2009)
Introduction
Carbon monoxide (CO) is a ubiquitous air contaminant derived from anthropogenic processes and human activ-ities. The principal cause of the outdoor pollution is the internal combustion engines of motor vehicles, whereas the CO contamination in indoor environments principally occurs by heaters fuelled with oil, gas, and kerosene and by tobacco smoking.
CO impairs the oxygen (O2) carrying capacity of blood
by combining with haemoglobin (Hb) to form carboxy-haemoglobin (COHb). For concentrations of CO as high as 1000 ppm, at normal atmospheric pressure, the partial oxygen pressures in aveoli and arterial blood will not be significantly reduced. Hence, Hb saturation from com-bination with either CO or O
2 remains near 100% (West,
2003). Since the affinity of CO for Hb is about 200 to 250
times greater than that of O2, small amounts of CO can
tie up a large proportion of the Hb in blood that would otherwise be available for carrying O
2. A COHb level
lower than 10% does not generally result in CO symptoms such as headache, dizziness weakness, nausea, confu-sion, disorientation, or visual disturbances (ICPS, 1999). However, patients with atherosclerotic cardiovascular disease may be adversely affected during exercise by the presence of carboxyhaemoglobin, even at concentrations as low as 2% (Allred et al., 1989). In order to protect people with established coronary diseases from ischemic heart attacks and to prevent hypoxic effects in foetuses, Health Canada, the U.S. Environmental Protection Agency (US EPA), and the World Health Organisation (WHO) propose maximum levels of COHb that should not be exceeded: 1.5% (Health Canada, 1989), 2% (US EPA, 2000), and 2.5% (IPCS, 1999).
ISSN 0895-8378 print/ISSN 1091-7691 online © 2009 Informa UK LtdDOI: 10.3109/08958370902744848
AbstractThis study proposes to estimate carboxyhaemoglobin (COHb) levels in the blood of men and women of various ages exposed to common concentrations of carbon monoxide (CO) using a model with only one free parameter while integrating alveoli–blood and blood–tissue CO exchanges. The model retained is essentially that of Coburn et al. (1965) with two important additions: an alveoli compartment for the dynamics of CO exchanges between alveoli and blood, and a compartment for the significant amounts of CO bound to heme proteins in extravascu-lar spaces. The model was validated by comparing its simulations with various published data sets for the COHb time profiles of volunteers exposed to known CO concentrations. Once the model was validated, it was used to simulate various situations of interest for their impact on public health. This approach yields reliable estimations of the time profiles of COHb levels resulting from different levels of CO exposure over various periods of time and under various conditions (resting, exercise, working, and smoking). The non-linear kinetics of CO, observed experimentally, were correctly reproduced by simulations with the model. Simulations were also carried out iteratively to determine the exposure times and CO concentrations in ambient air needed to reach the maximum levels of COHb recommended by Health Canada, the U.S. Environmental Protection Agency (EPA), and the World Health Organisation (WHO) for each age group of the general population. The lowest CO concentrations leading to maximum COHb levels of 1.5, 2, and 2.5% were determined.
Keywords: Carbon monoxide; carboxyhaemoglobin; risk assesment; toxicokinetic modeling; public health
http://www.informahealthcare.com/iht
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

1078 N. H. Gosselin et al.
Although there has been concern about the levels of car-bon monoxide in ambient air, little is known about COHb levels and their determinants in the general population. Whincup et al. (2006) examined these issues in a study of older British men, 60–79 yr old; that cross-sectional study reported on 4252 men who attended for examination at a socially representative general practice in each of 24 British towns between 1998 and 2000. Blood samples were meas-ured for COHb, and information on social, household, and individual factors was assessed by questionnaire. The geometric mean level of COHb was 0.46% and the median 0.50%; 9.2% of men had a COHb level of 2.5% or more and 0.1% of subjects had a level of 7.5% or more.
The US EPA, WHO, and Health Canada propose differ-ent CO concentrations in ambient air for different exposure durations likely to lead to these COHb levels. These max-imum air concentrations are recommended for a healthy adult doing light or moderate exercises; however, the level of COHb attained for a given CO concentration depends strongly on the values of several physiological parameters, and these vary importantly according to gender, age and activity levels. To assess these differences, a simple kinetic model that can link COHb levels to CO concentrations, while taking into account the intra- and intercondition variability of the population under various exposure conditions, would be useful. CO concentrations associated with a safe COHb level could thus be determined for the different age and gender groups under different exposure scenarios (acute, chronic and intermittent) and undergoing various effort levels.
Many models of the kinetics of CO in the human body have already been proposed. Coburn et al. (1965) developed a kinetic model describing the human response to endogen-ous production and environmental exposure to CO under transient and steady-state conditions. Using a single differ-ential equation for simulations, their model describes the temporal evolution of COHb during and after exposure to CO but does not incorporate either alveoli–blood or blood–tissue CO exchanges. This differential equation, commonly referred to as the CFK model, depends on the major physio-logical parameters governing the absorption and elimination of CO: the alveolar ventilation rate, the diffusing capacity of lungs for CO, the blood volume, the oxygen pressure in lung capillaries, the CO endogenous production, and the affinity ratio of haemoglobin (Hb) for oxygen (O
2) and CO.
The CFK model was modified by Smith et al. (1994) to simulate the observed difference between arterial and ven-ous blood COHb by incorporating the perfusion rates of the arms and that of the quickly and slowly perfused tissues. This expanded model better simulated the data of the experi-mental studies than did the original CFK model. However, since the values of two parameters had to be determined by adjustments between the simulations and experimen-tal data for each subject, Smith et al. (1994) remarked that this expanded CFK model was not adequately validated. Other mathematical approaches to modelling the uptake and elimination of CO in humans were proposed by Sharan
et al. (1990), Singh et al. (1991), and Selvakumar et al. (1992, 1993). None of these models described the diffusion of CO between blood and tissues in which CO is bound to heme proteins other than Hb, although that fact is well documented (Luomanmaki & Coburn, 1969; Caughey, 1970; Coburn, 1970; Cooper et al., 1970).
Bruce and Bruce (2003) developed a model for the kin-etics of CO in humans that includes the affinity of CO for myoglobin, a heme protein. The structure of this model is of the physiologically based pharmacokinetic type (PBPK). Two tissue compartments were used (i.e., muscle and non-muscle), in combination with arterial and venous blood compartments and a lung compartment. This model was validated using published data sets from human volun-teers exposed to CO and is able to simulate the differences between the arterial and venous COHb levels under envir-onmental or intoxicating exposures. However, for each data set, some parametric values needed to be estimated anew through best visual fits on each COHb profile; this was the case, in particular, for the blood flows in each tissue com-partment since these cannot be measured directly.
The inclusion of a compartment for the extravascular binding of CO was shown to be significant in the model of Cronenberger et al. (2007), where these authors developed a population PK analysis based on the time profiles of the COHb levels measured in smokers.
For the purpose of linking the COHb levels in humans to the concentrations of CO in ambient air under various envir-onmental or occupational exposure conditions, a variant of the CFK model is proposed in this study. This model incor-porates alveoli–blood and blood–tissue CO exchanges that were not included in the original CFK model. It also ensures mass conservation of CO at all times during and after expos-ure. This model incorporates the essentials of the kinetics of CO and allows the integration of the appropriate physio-logical values in the simulations of COHb levels in men and women of various ages, exposed to different CO concen-trations in ambient air over various periods of time while subject to diverse effort levels. It has a single free parameter whose value is estimated from one data set, and that value is applied to the simulations of all other data sets. All other parameters used, chemical and physiological, are accessible from experimental and physiological data reported in the literature.
Methods
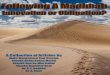
Proposed model for the kinetics of COThe schematic representation of absorption, distribution, and elimination of CO in the human body is depicted in Figure 1 (see Table 1 for definitions of the variables and parameters). Compartments represent the amounts of CO as a function of time in the alveoli, in the blood, and in tissues capable of capturing CO. The arrows represent amounts of CO transferred per unit of time. The temporal evolution of compartment amounts is described through the following system of differential equations.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Determination of carboxyhaemoglobin in humans 1079
kCO2BCO_Hb(t)
BCO_free(t)Amounts of free
CO in blood
BCO_Hb(t)Amounts of CO
bounded tohaemoglobin
Endo
SCO(t)Amounts of
CO bounded to heme
proteins inextravascular
spacekHbf·BCO_Hb(t)kfHb·BCO_free(t)
kHbS·BCO_Hb(t)
kSf·SCO(t)
BCO(t)Amounts of CO in blood
DLco·PALV(t)
DLco·PBL(t)
QALV·CEXT(t)
QALV·CALV(t)
ACO(t)Amounts of
CO in alveoliwith bloodexchanges
Figure 1. Model of the kinetics of carbon monoxide.
dA (t)dt
Q (C (t) C (t))
D (P (t) P (t))
COALV EXT ALV
Lco ALV BL
= ⋅ −
− ⋅ − (1)
dB (t)dt
D (P (t) P (t))
k B (t) k
CO_freeLco ALV BL
fHb CO_free Hbf
= ⋅ −
− ⋅ + ⋅⋅+ ⋅ +
B (t)
k S (t) EndoCO_Hb
Sf CO
(2)
dB (t)dt
k B (t)
k k k B (t)
CO_HbfHb CO_free
Hbf HbS CO2 CO_Hb
= ⋅
− + + ⋅( ) (3)
dS (t)dt
k B (t)
k S (t) k S t
COHbS CO_Hb
Sf CO CO2 CO
= ⋅
− ⋅ − ⋅ ( ) (4)
The inhaled CO amount (QALV
· CEXT
) enters compartment A
CO(t), which establishes the exchange between the CO in
ambient air and in the blood circulation. CO is absorbed into the organism by diffusing through the alveoli to the blood stream. This absorption depends on the gradient between alveolar and blood CO partial pressures (P
ALV–P
BL), as well as
on the diffusing capacity of lungs for CO (DLCO
).Though for both COHb and free CO, concentrations differ
slightly in arterial and venous bloods, for simplicity, global blood amounts are used, one for the COHb amount in blood, B
CO_Hb and one for the free CO amount, B
CO_free. The endog-
enous production of CO from the catabolism of hemoproteins
was taken into account through the input “Endo” into the free CO compartment. The compartment S
CO(t) represents the
amount of CO bound to molecules in tissues containing all heme structures that can reversibly bind to CO and O
2, such as
myoglobulin and cytochromes. Although this compartment represents mostly the CO bound to myoglobin in muscle tis-sues, it also includes the CO bound to other tissues such as the myocardium, the skeleton, and the liver (Coburn, 1970). COHb enters the extravascular spaces in a fashion similar to the oxyhaemoglobin transferred to extravascular spaces. This occurs very rapidly by diffusion from blood to tissues, and it is thus reasonable to assume that this CO rate of transfer is proportional to the B
CO_Hb amount (i.e., k
HbS·B
CO_Hb).
The elimination of CO from the body occurs principally through the pulmonary route (Q
ALV · C
ALV(t), though a small
amount is oxidized into CO2 (Tobias et al., 1945; Luomanmäki
& Coburn, 1969). Since this biotransformation occurs from dissociation of the CO bound to heme proteins followed by an oxidation reaction, the oxidation rates in extravascular spaces and in blood are taken to be equal; i.e., the oxidation rate k
CO2
was applied to both the BCO_Hb
and SCO
compartments.The pressures of free CO in alveoli and in pulmon-
ary blood, PALV
(t) and PBL
(t), are linked to the state vari-ables A
CO(t) and B
CO_Hb(t), respectively. On the one hand,
PALV
(t) is proportional to ACO
(t) by the law of perfect gases: P
ALV(t) · V
ALV = A
CO(t) · R · T, in which T = 310K and R=2.55
(mmHg · mLair
)/(Kelvin · mLco
). On the other hand, the par-tial pressure of gaseous CO in blood, P
BL(t), can be linked to
the fraction of Hb bound to CO (fCO_Hb
(t), the fraction of Hb bound to O
2 (f
O2_Hb(t), and the oxygen blood pressure (P
O2)
through Haldane’s equation (Roughton, 1970): (fCO_Hb
(t)/f
O2_Hb(t)) = M.(P
BL(t)/P
O2). This Haldane equation is valid
near complete Hb saturation, as is usually the case in the
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

1080 N. H. Gosselin et al.
blood of lung capillaries in healthy individuals (West, 995). Because the presence of CO does not reduce the P
O2 pres-
sure in pulmonary blood, Hb is nearly all bound, either to CO or O
2; it follows that f
CO_Hb(t) + f
O2_Hb(t) = 1. Here, f
CO_Hb(t)=
BCO_Hb
(t)/ BCO_HbMax
, where BCO_HbMax is the maximum amount of
CO that can be bound to Hb.Summing Eqs. (2) and (3), to obtain a differential equa-
tion for the total (free and bound to Hb) CO blood amount, B
CO(t), eliminates and renders superfluous the determin-
ation of the two constants kfHb
and kHbf
. Thus,
dB (t)dt
D (P (t) P (t))
k B (t) k S (t)
COLco ALV BL
HbS CO_Hb Sf CO
= ⋅ −
− ⋅ + ⋅− kk B EndoCO2 CO_Hb⋅ +
(5)
Further, reasonable simplifications can be obtained by replacing B
CO_Hb(t) by B
CO(t) in Eq. (5), since B
CO_free(t) is very
small compared to BCO_Hb
(t), a ratio of about 10−4, based on Henry’s law, which establishes the partial pressure of a gas dissolved in a liquid. This, with the use of Haldane’s equation, yields the following reduced system with three differential equations on three state variables, A
CO(t), B
CO(t), and S
CO(t).
dA (t)dt
Q C (t)A (t)V
DA (t)V
R
COALV EXT
CO
ALV
LcoCO
ALV
= ⋅ −
− ⋅ ⋅ ⋅ TTB (t) P
M B B (t)CO O2
CO_HbMax
CO
−⋅
⋅ −( )
(6)
dB (t)dt
DA (t)V
R TB (t) P
M B B (t)CO
LcoCO
ALV
CO O2
CO_HbMax
CO
= ⋅ ⋅ ⋅ −⋅
⋅ −(( )
− ⋅ + ⋅ − ⋅ +k B (t) k S (t) k B (t) EndoHbS CO Sf CO CO2 CO
(7)
dS (t)dt
k B (t)
k S (t) k S (t)
COHbS CO
Sf CO CO2 CO
= ⋅
− ⋅ − ⋅
(8)
Table 1. Variables and parameters used in model simulations.
Variables and parameters Descriptions
Variables ACO
(t) Amount of carbon monoxide in alveoli as a function of time (mlCO
)
BCO
(t) Total amount of carbon monoxide in blood as a function of time (mlCO
)
BCO_Hb
(t) Amount of carbon monoxide bound to haemoglobin as a function of time (mlCO
)
BCO_free
(t) Amount of free carbon monoxide in blood as a function of time (mlCO
)
SCO
(t) Amount of carbon monoxide bound to heme proteins in the extravascular spaces as a function of time (mlCO
)
CALV
(t) Concentration of carbon monoxide in alveoli as a function of time (mlCO
/mlair
)
PALV
(t) Pressure of carbon monoxide in alveoli as a function of time (mm Hg)
PBL
(t) Pressure of carbon monoxide in lung capillaries as a function of time (mm Hg)
CEXT
(t) Concentration of carbon monoxide in ambient air as a function of time (mlCO
/mlair
)
fCO_Hb
(t) Fraction of haemoglobin bound to carbon monoxide as a function of time
fO2_Hb
(t) Fraction of haemoglobin bound to oxygen as a function of time
Parameters QALV
Alveolar ventilation rate of inhaled air (mlair
/min)
DLco
Diffusing capacity of lungs for carbon monoxide (mlCO
/min/mm Hg)
kfHb
Bounding rate of carbon monoxide to haemoglobin in blood (min−1)
kHbf
Rate of carbon monoxide released to blood from haemoglobin (min−1)
kHbS
Capture rate of carbon monoxide from blood to heme proteins in extravascular spaces (min−1)
kSf
Release rate of carbon monoxide from heme proteins in extravascular spaces to blood (min−1)
kCO2
Oxidizing rate of carbon monoxide (min−1)
Endo Rate of endogenous production of carbon monoxide (mlCO
/min)
PO2
Partial pressure of oxygen in lung capillaries (mm Hg)
VALV
Alveolar volume (mlair
)
R Avogadro’s constant (mm Hg·mlair
/Kelvin · mlCO
)
T Temperature BTPS (Kelvin)
M Haldane’s coefficient which quantifies the relative affinity of CO and O2 for Hb
BCO_HbMax Maximum amount of carbon monoxide bound to haemoglobin (ml
CO)
fR
Respiratory frequency (min−1)
VT
Tidal volume (mlair
)
VD
Physiological dead space (mlair
)
VD_ana
Anatomical dead space (mlair
)
VD_alv
Alveolar dead space (mlair
)
Conversion factor: STPD conditions (standard temperature and pressure and dry gas) to BTPS conditions (body temperature and pressure, saturated water vapour)
VBL
Blood volume (mlblood
)
bCO_HbMax Maximum amount of carbon monoxide bound to one gram of haemoglobin (ml
CO/g
Hb)
CHb
Concentration of haemoglobin in blood (gHb
/mlblood
)
BW Body weight (kg)
Note. The units for amounts of carbon monoxide are in the BTPS conditions (body temperature and pressure, saturated water vapour).
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Determination of carboxyhaemoglobin in humans 1081
Table 2. Numerical values of parameters.
Parameters Values
QALV
See Table A1
VALV
See Table A1
DLco
See Table A1
kHbS
0.002 min−1
kSf
0.01 min−1
kCO2
3.33 × 10−5 min −1
BCO_HbMax b Hb V mlCO_Hb
MaxBL co× ×
bCO_HbMax 1.68 ml
CO/g
Hba
CHb
Newborns 170 gHb
/Lblood
1 to 2 yr old 115 gHb
/Lblood
12 to 13 yr old 145 gHb
/Lblood
Adults 150 gHb
/Lblood
VBL
0.079 × BW Lblood
Endo 1.21 × 10−4 × BW mlCO
/mina
M 240
PO2
Newborns 104.7 mm Hg
1 yr old 104.5 mm Hg
5 yr old 103.5 mm Hg
10 yr old 102.3 mm Hg
15 yr old 101.1 mm Hg
Adults 97 mm Hg
Note. The description of the parameters is given in Table 1. The explanation for each parametric value is given in the Appendix.aThe units for amounts of carbon monoxide are in the BTPS conditions (body temperature and pressure, saturated water vapour).
The principal differences between the proposed model and the standard Coburn–Forster–Kane (CFK) model lie with the addition of an alveoli compartment to describe the dynamics of CO exchanges between alveoli and blood and a compart-ment to account for the significant amounts of CO bound to heme proteins in extravascular spaces (myoglobin of the muscular cells and other heme-containing compounds, such as cytochromes and metalloenzymes). It is a simple matter to obtain the CFK model from the proposed model by first neutralizing the CO access to the extravascular space compartment (i.e., k
HbS = 0) and by steadying the short-term
dynamics of the alveolar compartment (i.e., dACO
/dt = 0).
Determination of parametersDetails on the determination of parametric values present in the model are found in the Appendix. When available in the literature, the subject’s characteristics were used to deter-mine these values. For instance, the alveolar ventilation rate (Q
ALV) varies as a function of age, gender, and workload
levels, as does the diffusing capacity of lungs for CO (DLco
), which also depends on height, a surrogate for alveolar sur-face. Only one free parameter, k
Sf, was determined through a
best fit to a single data set (Tikuisis et al., 1987a); that value was used recurrently in all other simulations,
The numerical values of all parameters used in model simulations are summarized in Tables 2, A1, and A2. Once the parameters of the model were determined, simulations of the time profiles of COHb were carried out by solving numerically the differential Eqs. (6), (7), and (8) using the fourth order Runge–Kutta method incorporated in MathCad 2001 Professional (Mathsoft). Simulations of different tem-poral exposure scenarios (acute, chronic, and intermittent) were performed by introducing time-varying inputs for the exposure variable C
EXT(t) (see Eq. (6)).
Experimental data for model validationThe scientific literature offers a number of studies reporting the COHb time profiles of volunteers exposed to CO in con-trolled environments. In order to validate the proposed model, simulations were compared to the experiments carried out by Stewart et al. (1970) and Tikuisis et al. (1987a, 1987b, 1992). These experimental studies were selected among others because they offered detailed time profiles of COHb under a variety of exposure scenarios (i.e., levels and periods of CO exposure as well as the effort levels of volunteers). In the study of Stewart et al. (1970), the mean COHb time profiles of only 6 experiments amongst 25 (i.e., experiments 14–17, 23, and 25) were presented in tables. These were retained for the purpose of validating our model because they pertain to subjects who did not receive any oxygen treatments. To make use of the graphic data from the study of Tikuisis et al. (1987a, 1987b, 1992), the COHb–time graphs were scanned using Sigma Plot Graphing Software (Jandel Corporation, San Rafael, CA).
The system of differential equations with the input func-tion (C
EXT(t) describing the experimental conditions was
solved to generate COHb time profiles. The physiological parametric values related to sex, age, and workload levels
used in the simulations were the ones measured during the experiments when provided. When not so provided, the values used were those proposed for an adult male in Tables 2, A1, and A2 according to the workload level reported in the study. To test the goodness of fit between model simulations and data set, a linear regression was car-ried out (y = m · x) between the observed (y) and simulated values (x) for COHb. A unit slope (i.e., m = 1), with a null confidence interval, implies a perfect fit; the slope m with its 95% confidence interval (IC95%) was thus estimated for each data set simulated.
Sensitivity analysisSince the parametric values in Tables 2, A1, and A2 are experimental group averages and are subject to wide varia-tions from one human to another, an analysis was designed to measure the impacts of these variations on the simu-lated values for COHb. To this effect, COHb levels were first simulated using the average values for the parameter set (COHb
default); then by varying the parametric values one at
a time, according to likely physiological ranges, new levels (COHb
new) were obtained. For each simulation, the vari-
ation for each output was calculated using the following equation:
Variation =−
×COHb COHb
COHbnew default
default100 (9)
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

1082 N. H. Gosselin et al.
In order to assess the impact of parameter variations for realistic situations, two typical scenarios were consid-ered: (i) a 40-yr-old man exposed during his 8-h working day to 35 ppm of CO during a 5-day week and exposed to 3 ppm of CO the rest of the time, and (ii) another 40-yr-old man exposed throughout the week to 3 ppm. The latter value is a realistic level observed for non-smoking individuals indoors with good air exchange (IPCS, 1999), whereas 35 ppm is the 8-h time-weighted average (TWA) concentration that is recommended by the Commission de la santé et sécurité du travail (CSST) (Québec, 2001).
Model simulationsOnce the model was validated and parametric sensitivity was assessed, it was used to address various CO exposure situations of interest for public health. Simulations were carried out to estimate the levels of COHb during and after environmental, occupational and smoking exposures. Through iteration of simulations, it was also possible to determine the CO concentrations in ambient air needed to reach the maximum recommended COHb levels of 1.5%, 2.0%, and 2.5% after 1-h, 8-h, and 24-hr\ exposure periods. These concentrations were determined for each age group, assuming a light workload level.
Results
Model validationThe time profiles of COHb simulated by the model were com-pared with those observed in different experimental studies (Stewart et al., 1970; Tikuisis et al., 1987a, 1987b, 1992). To illustrate this, comparisons between the model simulations and some of the data of Stewart et al. (1970) are graphically presented in Figure 2. There, three volunteers were exposed to 50 ppm levels of CO continuously for each of the 4 different time periods: 1, 3, 8, and 24 h (experiments 14–17 of Stewart et al., 1970). For this experimental study, the estimated slope of the linear regression on observed data versus simulations is 0.97 (IC95% = 0.95–0.99). Since no values for the individ-ual physiological parameters of these subjects were reported in that experimental study, simulations were implemented using average physiological parameters for men at rest.
In general, the model simulated closely the time profiles of COHb measured in volunteers who were exposed to a wide range of CO levels (50–4000 ppm) under several tem-poral scenarios. Figure 3 presents a comparison between the observed values of COHb reported in all experimental studies and those obtained from the model. Table 3 sum-marizes the results of linear regressions on the observed data versus simulated values for each data time profile. The goodness-of-fit slopes between simulated values and experimental data for each data set are always close to unity within a small confidence interval (0.95–1.04). This is a good indication of the validity of the model.
All the exposure scenarios used to validate the model were also re-simulated using the standard CFK model and
the results are presented in Table 3. The slope between the observed and predicted data (150 points) using the CFK model was generally lower than 1 and the 95% CI did not include the value 1 (e.g., m = 0.917, CI95% = (0.906–0.927). This illustrates the improvements brought about by the use of the proposed modified CFK model.
Sensitivity analysisSensitivity of the predicted COHb to the variation of model parameters was estimated through simulations of various exposure scenarios. The simulated COHb time profiles used as default values are presented in Figure 4. All parametric values were varied, one at a time, within likely physiological ranges, to assess their impact on COHb levels. For safety’s sake, the ranges of the parameters used in the sensitiv-ity tests are large, though the physiological variations in a group of healthy adults are likely narrower.
The results of this sensitivity analysis are presented in Table 4, where the levels of COHb and their variations are reported at relevant time points. The parameters {Hb, Endo, k
CO2, M} and the ratio k
HbS/k
Sf were taken to range over the
minimum and maximum values quoted in the literature for healthy adults (see Appendix). The range of values for the transfer rate k
Sf was arbitrarily taken to vary ±50% from
the default value. The alveolar ventilation rate, QALV
, and the diffusing capacity of lungs for CO, D
Lco, were taken to
range ±20% from the default value specific to each workload status for a 40-yr-old man. Since there are no available data about the inter- and intra-individual variability of partial pressure of oxygen in lung capillaries, P
O2, for healthy 40-yr-
old men, the sensitivity analysis used the normal range observed in individuals aged from 0 to 80 yr living at sea level (85– 105 mm Hg).
Table 4 shows that the most important parameter influ-encing the level of COHb is Haldane’s coefficient (M). In vitro experiments showed that this coefficient can vary from 200 to 260, possibly representing as much experimental uncertainty as genuine inter- and intra-individual variabil-ity (Roughton, 1970). A decrease of 20% in the default value of M results in a reduction of 13 to 26% from the default COHb value, depending on the sample periods. The next most important parameter is P
O2, where a decrease of 12%
leads to a 24% increase of the COHb level.For work exposure, say an 8-h workday at 35 ppm CO
concentrations in ambient air, realistic intersubject vari-ations (± 20%) of the alveolar ventilation rate (Q
ALV) show
that these variations have a negligible impact on the COHb levels at the end of the occupational exposure period per se (see Friday 4 PM in Table 4), but the impact is important up to 16 h after the work period (see Saturday 8 AM). This stems from the fact that during high exposure a person with a larger ventilation rate absorbs CO more rapidly but con-comitantly eliminates it more rapidly by exhalation; the two tend to balance out. However, during the after-work period, the subject is assumed to be exposed to low CO concentra-tions, 3 ppm; there, elimination of the accumulated CO by exhalation greatly surpasses the ongoing absorption.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Determination of carboxyhaemoglobin in humans 1083
4
3
2
1
00
Car
boxy
haem
olob
in (p
erce
nt)
4 6 8 10 12 142
(A)
4
3
2
1
00
Car
boxy
haem
olob
in (p
erce
nt)
Time (hours)10 15 20 25 30 35 40 455
(B)
Figure 2. Comparison of model simulations (lines) with the mean experi-mental data of Stewart et al. (1970) (experiments 14–17) for the time pro-files of COHb measured in male volunteers during and after exposure to 50 ppm of carbon monoxide (symbols): (A) during 1 h (□) and 3 h (×), and (B) during 8 h (□) and 24 h (×) (n = 3 per exposure group).
Overall, intra- and inter-individual variations of the physi-ological parameters do not lead to a wide variation in the COHb simulations.
Model simulationsCO absorption and elimination The impact of different workload levels on COHb levels was first assessed through the simulation of the buildup of COHb in a worker during a typical workday at 35 ppm CO in ambient air (Figure 5A). In a second simulation, the impact of different activity levels on CO elimination was assessed during the recuperation period after a CO exposure that had led to a COHb level of 6% at the end of the 8-h work period (Figure 5B). The graphs in Figure 5 show that exercise increases both the absorp-tion and the elimination of CO through higher ventilation rates. In the exposure phase (Figure 5A), exercise promotes absorption more than it promotes concomitant elimination, resulting in a higher buildup.
Model simulations with different inhaled CO concentra-tions (3, 30, or 300 ppm) during 24 h followed by zero exposure show that the absorption and elimination processes are gov-erned by non-linear kinetics (Figure 6). This non-proportional COHb response to inhaled CO concentrations stems from the
competition between CO and O2 for Hb. In Figure 6, it is seen
that: (i) the 10-fold increases in inhaled CO concentrations, 3, 30, and 300 ppm, do not result in 10-fold increases in the maximum COHb, which are respectively equal to 0.7%, 5.6%, 36.9%; and (ii) the COHb time profiles during the decreasing phase are not parallel on this semi-log plot, as they would be if the kinetics were linear.
The slopes of the COHb time profiles in Figure 6 vary with the time elapsed since the end of exposure. One can see from these profiles that the slopes that represent the instantane-ous elimination rate at each moment decrease with time because of the capture–release mechanism. Furthermore, because of the non-linear kinetics, a subject with a higher initial COHb will at all times detoxify more rapidly. This is illustrated in Figure 6 by the larger slopes immediately after the end of exposure as one goes from 0.206 to 0.344 h−1 for 3 to 300 ppm exposure concentrations. Again, if the kinetics were linear, these initial slopes would all be equal.
Realistic exposure scenarios In the province of Québec, the Commission de la santé et de la sécurité du travail (CSST) imposes maximum CO average exposure levels of 35 ppm for 8-h TWA, including a maximum of four 15-min peak exposure periods at 200 ppm (Québec, 2001). Figure 7 illus-trates an occupational exposure scenario corresponding to this maximum exposure standard.
According to IPCS (1999), each smoking period corresponds to a CO exposure of 400–500 ppm during 6 min. In order to
0
2
4
6
8
10
12
0 2 4 6 8 10 12
Tikuisis et al. (1987)Stewart et al. (1970) (Experiments #14-17)Tikuisis et al. (1987a)Tikuisis et al. (1992)O
bser
ved
Car
boxy
haem
oglo
bin
(mea
n)
Simulated Carboxyhaemoglobin (mean) (percent)
0
5
10
15
20
25
30
35
0 5 10 15 20 25 30 35
Stewart et al. (1970)(Experiments #23 and #25)
Obs
erve
d C
arbo
xyha
emog
lobi
n (m
ean)
Simulated Carboxyhaemoglobin (mean) (percent)
Figure 3. Comparison between observed COHb (percent) of male vol-unteers exposed to carbon monoxide and simulated COHb obtained using the model (see description of the studies at Table 3). The line (—) represents the linear equation y = x.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

1084 N. H. Gosselin et al.
assess the impact of cigarette smoking on COHb levels, the model was also used to simulate two typical smoking scenarios: 9 and 23 cigarettes per day (see Figure 8). The wash-out period is an important factor in assessing COHb levels. Assuming a smoking rate of 1 cigarette per hour, simulations indicate that a COHb level of 9% would be reached just at the end of smok-ing a cigarette, but would have decreased to 7.2% just before the next cigarette. For 2 cigarettes per hour, the correspond-ing figures would be 15.2% and 13.1%. For a light smoker, the COHb level would reach 5.9% at the end of smoking a cigarette and would have decreased to 3.5% at 2 h after smoking. These results are consistent with observed COHb levels in moderate and heavy smokers for whom the COHb levels are known to reach 8% and 15%, respectively (ICPS, 1999).
The two exposure scenarios just described and presented in Figures 7 and 8 lead to COHb levels much higher than
does the exposure to CO under normal environmental con-ditions. According to simulations, an individual, whatever his or her age, continuously exposed to 3 ppm CO would never exceed 0.85% COHb levels.
Links between COHb and ambient CO concentrations In order to determine CO exposure levels associated with the guideline values of Health Canada, the U.S. EPA, and WHO (COHb of 1.5%, 2%, and of 2.5%, respectively), simulations were carried out iteratively to determine the CO concen-trations needed to reach these values for different time exposure periods (see Table 5). These CO concentrations vary from 17.5 to 62 ppm for a 1-h exposure, from 8.2 to 16.6 ppm for an 8-h exposure, and from 7.1 to 13.2 ppm for a daily exposure. According to model simulations, babies 3 mo could in theory be exposed to the higher CO concentra-tion in the ambient air before reaching the guideline values. However, for 1-yr-old infants, the lowest CO concentrations are in order, i.e., 31.2 ppm, 14.1 ppm, and 12.6 ppm, dur-ing 1 h, 8 h, and 24 h, respectively, for a maximum COHb of 2.5%.
Table 4. Sensitivity analysis on the variations of parametric values through simulations of COHb at different times following occupational and environmental exposure to carbon monoxide (see Figure 4 for the description of the exposure and workload scenarios).
Model parameters
Variations in
parametric values
Carboxyhaemoglobin (percent) and variation (percent)a
Time following the beginning of exposure
High occupational exposure
Low occupational exposure
Friday 4 h PM
Saturday 8 h AM
Friday 4 h PM
Saturday 8 h AM
Default values 5.91 1.81 0.72 0.85
QALV
(of default values)
–20% 5.79 (–2.0) 2.13 (18) 0.75 (4.2) 0.85 (0.0)
+ 20% 6.00 (1.5) 1.58 (–13) 0.70 (–2.8) 0.82 (–3.5)
DLco
(of default values)
–20% 5.83 (–1.4) 1.86 (2.8) 0.74 (2.8) 0.86 (1.2)
+ 20% 5.97 (1.0) 1.78 (–1.7) 0.71 (–1.4) 0.84 (–1.2)
VBL
(L
blood)
4.98 6.01 (1.7) 1.68 (–7.2) 0.72 (0.0) 0.85 (0.0)
6.08 5.82 (–1.5) 1.94 (7.2) 0.73 (1.4) 0.84 (–1.2)
CHb
(g
HB/L
blood)
135 6.01 (1.7) 1.68 (–7.2) 0.72 (0.0) 0.85 (0.0)
170 5.79 (–2.0) 1.97 (8.8) 0.73 (1.4) 0.84 (–1.2)
Endo (ml
CO/min)
7.03 × 10−3 5.89 (–0.3) 1.77 (2.2) 0.70 (–2.8) 0.80 (–5.9)
1.15 × 10−2 5.96 (0.85) 1.91 (5.5) 0.77 (6.9) 0.95 (12)
kCO2
(min−1)
0 5.95 (0.7) 1.87 (3.3) 0.73 (1.4) 0.86 (1.2)
2.6 × 10−4 5.66 (–4.2) 1.51 (17) 0.68 (–5.6) 0.76 (11)
M 200 5.10 (–14) 1.34 (–26) 0.60 (17) 0.72 (–15)
260 6.30 (6.6) 2.07 (14) 0.78 (8.3) 0.91 (7.0)
PO2
(mm Hg)
85 6.56 (11) 2.24 (24) 0.83 (15) 0.96 (13)
105 5.55 (6.0) 1.59 (–12) 0.67 (6.9) 0.79 (–7.0)
kHbSkSf
b 0.1 6.01 (1.7) 1.70 (–6.1) 0.72 (0.0) 0.85 (0.0)
0.3 5.82 (–1.5) 1.91 (5.5) 0.73 (1.4) 0.83 (–2.4)
kSf
c (min−1)
5 × 10−3 5.93 (0.3) 1.80 (–0.6) 0.72 (0.0) 0.85 (0.0)
1.5 × 10−2 5.92 (0.2) 1.82 (0.6) 0.72 (0.0) 0.85 (0.0)
Note. The default values of model parameters are presented in Table 2 and in Appendix. The body weight used in simulations was 70 kg.a Variation = (New value – Default value)/Default value × 100.b The value of k
Sf was kept constant.
c The ratio kHbS
/kSf
is set equal to 0.2.
Table 3. Linear regressions (y = m · x) between the COHb values simulated by the model (x) and the observed values (y) in the different studies.
Experimental studies
Estimated slope (m) 95% Confidence interval Number of
pointsModified
CFK modelCFK
modelModified
CFK modelCFK
model
Stewart et al. (1970)a
0.98 0.91 0.95–0.99 0.89–0.93 37
Stewart et al. (1970)b
1.00 0.92 0.98–1.01 0.91–0.93 28
Tikuisis et al. (1987a)c
0.97 0.95 0.96–0.99 0.93–0.96 24
Tikuisis et al. (1987b)d
0.95 0.94 0.88–1.02 0.87–1.01 9
Tikuisis et al. (1987b)e
1.00 0.87 0.95–1.04 0.83–0.91 24
Tikuisis et al. (1992)f
1.04 1.02 1.02–1.06 1.01–1.04 28
All experiments
0.996 0.917 0.986–1.001 0.906–0.927 150
Note. Model simulations for the studies of Tikuisis et al. (1987a, 1992) were performed with parametric values of Q
alv, f
R, and D
Lco reported in
the articles and for Stewart et al. (1970) and Tikuisis et al. (1987b) were those reported in Table 2 and in Table A1. The values of other parameters included in the model were those presented in Table 2 for male adults.aMale volunteers exposed to 50 ppm CO during 1, 3, 8, or 24 h (n = 3 per exposure group) (experiments 14–17).bMale volunteers exposed to CO during a 2.3-h exposure period to 494 ppm CO or for a gradually increasing exposure to CO from 1 ppm to 1000 ppm over 2 h followed by a 30-min exposure at 1000 ppm (n = 2 per exposure group) (experiments 23 and 25).cMale volunteers at rest exposed to 1500 ppm CO during 5 periods of 5 minutes separated by 3-min unexposed periods or to 7500 ppm during 5 periods of 1 minute separated by 7-min unexposed periods (n = 11 per exposure group).dMale volunteers at rest exposed to CO during 4.5 min at varying levels: 500 ppm for the first minute followed by consecutive 30-s periods at 1000, 2000, 4000, 2000, and 1000 ppm and by a 1-min period at 500 ppm (n = 9).eMale volunteers exposed to 1000 ppm CO during 2 or 3 exercise periods of 5 min separated by 15-min unexposed periods intervals without exposure (n = 4) or to 4000 ppm CO during 2 exercise periods of 45-s separated by 20-min unexposed periods (n = 2).fMale volunteers exposed, while at rest, to 3000 ppm CO followed by a 10 min exercise period (45 watts) without exposure and by exposure periods of 3, 1, and 2 min separated by 2 min without exposure. The CO levels during the 3 latter periods were respectively 1000, 3000, and 1500 ppm (n = 10).
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Determination of carboxyhaemoglobin in humans 1085
Discussion
This study presents a systematic approach to estimating blood carboxyhaemoglobin levels following exposure to CO concentrations commonly found in general and occupa-tional environments. The proposed model, a variant of the CFK model developed by Coburn et al. (1965), insures mass conservation of CO at all times during and after exposure and an adequate body distribution of the CO amount. It takes into account the variations of the alveolar ventilation rate (Q
ALV) due to age, gender, and activity levels and the var-
iations in the diffusing capacity of CO between alveoli and blood (D
Lco). The model has a single free parameter, k
Sf; its
value is determined once from a single data set, and is then used in all simulations. All the other parametric values of the model were taken directly from the literature, including
the ranges for the values of physiological parameters that depend on age, gender, and activity level. The simulations of experimental data used to validate the model were carried out using only a single set of values for some basic physi-ological parameters (e.g., M, P
O2, k
Sf and k
HbS).
The proposed model differs from the standard CFK model in two ways. First, it includes the dynamics of alveoli–blood exchanges to obtain a better understanding of CO in the alveolar tissues, but this does not influence the simulation outcomes substantially. On the other hand, the inclusion of a compartment for the amount of heme proteins in extravas-cular spaces greatly improves the fit to data. Contrary to the standard CFK model, the proposed model does not system-atically over- or under-estimate the experimental data.
The proposed model was shown to simulate with good accuracy a great variety of experimental data for male
Car
oxyh
aem
oglo
bin
(per
cent
)
0.5 1 1.5 2 2.5 3 3.5 4 4.5 50
1
2
3
4
5
6
7
.
Car
oxyh
aem
oglo
bin
(per
cent
)
0
0.2
0.4
0.6
0.8
1
Monday Tuesday Wednesday Thursday Friday
Time (days)
Carbon m
onoxide concentration (ppm)
8
16
24
32
40
48
Carbon m
onoxide concentration (ppm)1.2
2.4
3.6
4.2
Sleeping Sitting
Light exercise
Sleeping Sitting
Light exercise
A
B
Figure 4. Simulations of the time profiles of COHb for two typical situations where a 40-yr-old man is exposed to carbon monoxide during a typical 5-day work week. The 24-h day consists of 3 consecutive 8-h periods: sleeping from 12 h PM to 8 h AM, working (light exercise) from 8 h AM to 4 h PM, and sitting from 4 h PM to 12 h PM. (A) High exposure: work period at 35 ppm and the rest of the time at 3 ppm. (B) Low daily exposure at 3 ppm. The CO exposure periods are represented by dotted lines (----) and the COHb simulations by solid lines (—).
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

1086 N. H. Gosselin et al.
subjects exposed to controlled exposures to CO for concen-trations varying from 3 to more than 300 ppm. Unfortunately, no time profiles of COHb levels in women from controlled experiments were available in the literature to test model simulations for women. Nevertheless, in all model simula-tions, for a given CO exposure, the values taken for the three main determinant factors (V
ALV, Q
ALV, and D
LCO) were specific
to the relevant age and gender groups and to the effort levels. Hence, the simulations reported for women are likely repre-sentative of their exposure. Another argument favoring that gender as such is not a significant variable stems from the population pharmacokinetic analysis of Cronenberger et al. (2007), where the effect of gender on the PK parameters of COHb was not deemed statistically significant.
The sensitivity analysis carried out for each parameter, allowed to vary within its physiological range, showed that in extreme cases the highest absolute variation of COHb is no more than 0.5%. These low variations indicate that the model is stable and that with a good knowledge of the exposure conditions (e.g., inhaled CO concentrations and effort levels), the model can simulate correctly the COHb level. The results of the sensitivity analysis presented in Table 4 are consistent with those obtained by McCartney (1990) with the CFK model. This author demonstrated that
with a CO concentration of 100 ppm in the ambient air, the haemoglobin blood concentration, the blood volume, and the initial COHb (equivalent to the Endo in the proposed model) have little effects on the COHb levels, whereas the parameters that mostly depend on the workload (Q
ALV,
DLCO
) and the CO affinity coefficient (M) affect strongly the COHb levels.
Once the model was validated on experimental data, it was used to simulate various situations of interest for their impact on public health. Among these are the CO concentra-tions in ambient air needed to reach some specified COHb levels that should not be exceeded in the general population. This is achieved through iterated simulations with different CO concentrations and for different exposure periods at light effort levels (Table 5). These CO concentrations were com-pared to the guideline values recommended by regulatory organizations. For a 2.5% COHb level, the CO concentrations obtained in this study are slightly higher than those recom-mended by WHO (IPCS, 1990) (i.e., 26 ppm for a 1-h exposure and 9 ppm for an 8-h exposure), whereas the CO concentra-tions obtained for a 1.5% COHb level were slightly lower than those recommended by Health Canada (1989) (i.e., 25 ppm for a 1-h exposure and 11 ppm for an 8-h exposure).
Regarding CO concentrations associated with recom-mended COHb guideline values, sensitivity analysis showed that the effort level and the value retained for Haldane’s coefficient (M) are the major determinants, especially over long periods of exposure. Model simulations for CO expo-sure under heavy exercise and under sleeping conditions show that during an 8-h exposure period, the CO concentra-tions needed to reach the 2.5% COHb level are 13.4 ppm and 21.5 ppm, respectively. Also, if Haldane’s coefficient (M), the most influential parameter, is varied from 200 to 260, the concentration of CO required for an adult to reach the 2.5% COHb level during exposure under light exercise decreases
5 10 15 20 25 30 350
1
2
3
4
5
6
Time (hours)
Car
boxy
haem
oglo
bin
(per
cent
)
1 2 3 4 5 6 7 80
1
2
3
4
5
6
7
Time (hours)
Car
boxy
haem
oglo
bin
(per
cent
)
A
B
Figure 5. Simulations of the COHb time profiles of a 40-yr-old man doing light exercise (—) or sitting (----): (A) COHb buildup during an 8-h expos-ure period to 35 ppm CO. (B) COHb elimination after an exposure to CO that led to a 6% COHb level.
0 10 20 30 40 50 600.1
1
10
100
Time (hours)
Car
boxy
haem
oglo
bin
(per
cent
) 0.344 hr−1
0.206 hr−1
0.266 hr−1
Figure 6. Simulations of the time profiles of COHb in a 40-yr-old man doing light exercise, exposed to carbon monoxide during 24 h at 3 ppm (-·-·-), 30 ppm (----), and 300 ppm (—). The arrows represent the elimin-ation rates at the end of exposure, i.e., the first-order derivative of COHb relative to time.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Determination of carboxyhaemoglobin in humans 1087
from 16.7 to 13.7 ppm for an 8-h exposure and from 15.2 to 11.6 ppm for a 24-h exposure, while the effect of that varia-tion is negligible for a 1-h exposure.
In assessing occupational exposures, simulations indi-cate that a 40-yr-old man exposed continuously to 35 ppm of CO for 8 h would reach COHb levels between 4 to 6% depending on the activity level (see Figure 5), while for an 8-h exposure period at 10 ppm plus four 15-min exposure periods at 200 ppm separated by 1 h (TWA of 33.75 ppm), the maximum COHb attained is higher, nearly 8% (see Figure 7). Further, results of simulations show that, during light exer-cise, so-called moderate smokers (1 cigarette every 2 h) may reach COHb levels comparable to a non-smoking worker exposed continuously to 35 ppm for 8 h (see Figure 8).
Simulations also render explicit the non-linearity of CO kinetics; i.e., multiplying CO concentrations does not result
in proportional increases in COHb levels. The non-linearity stems from the competition between CO and O
2 for Hb and
has a profound physiological impact. As a result, a subject with a higher initial COHb will at all times detoxify more rap-idly (see Figure 6). Also the non-linearity prevents the defi-nition of a single half-life for the elimination of CO because the elimination rate is not constant but rather depends on the instantaneous CO body amount. This may explain why the literature reports a wide range of values for the elimination half-life (i.e., 2–6.5 h; IPCS, 1999).
Overall, the proposed method provides a unified way of estimating the results of common environmental and occupational exposures to CO for men and women of all ages undergoing different effort levels. However, it is well to remember that the model, in its present form, cannot describe adequately the links between CO concentrations and COHb
0 2 4 6 8 10 120
2
4
6
8
10
Carbon m
onoxide concentration (ppm)
Time (hours)
Car
boxy
haem
oglo
bin
(per
cent
)
200
150
100
50
Figure 7. Simulations of the time profiles of COHb following the onset of occupational exposure to carbon monoxide in a 40-yr-old man doing light exercise during 8 h at a background level of 10 ppm plus four 15-min peak exposure periods at 200 ppm, each separated by 1 h. Exposure is rep-resented by a dotted line (----) and the COHb profile by a full line (—).
0 5 10 15 200
2
4
6
8
10
12
14
16
Car
boxy
haem
oglo
bin
(per
cent
)
Time (hours)
Figure 8. Simulations of the time profiles of COHb for a 40-yr-old man: (i) smoking a cigarette every hour during 10 h and then, every 30 min during 6 h (—), (ii) smoking a cigarette every 2 h during 16 h (----). The background environmental exposure to CO is taken to be 2 ppm and each cigarette exposure equivalent to 450 ppm during 6 min. The alveolar ven-tilation rate and diffusing capacity of lungs for CO used in these simula-tions correspond to a light exercise.
Table 5. Concentrations of carbon monoxide in ambient air needed to reach 1.5%, 2.0%, and 2.5% COHb after 1-h, 8-h, and 24-h exposure periods as a function of age.
Age
Concentrations of CO in ambient air (ppm)
Exposure 1 h Exposure 8 h Exposure 24 h
COHb 1.5% COHb 2.0% COHb 2.5% COHb 1.5% COHb 2.0% COHb 2.5% COHb 1.5% COHb 2.0% COHb 2.5%
3 month 34.2 48.1 62.0 9.4 13.1 16.6 7.2 9.9 12.6
1 yr old 17.5 24.4 31.2 8.2 11.1 14.1 7.3 10.1 12.6
5 yr old 20.4 28.5 36.5 8.2 11.2 14.3 7.1 9.8 12.5
10 yr old
Boys 20.5 28.5 36.5 8.2 11.2 14.2 7.4 10.0 12.7
Girls 20.7 28.8 36.9 8.2 11.2 14.2 7.4 10.0 12.7
15 yr old
Boys 23.9 33.5 43.0 8.4 11.4 14.5 7.6 10.4 13.2
Girls 25.2 35.2 45.3 8.4 11.4 14.7 7.6 10.4 13.2
Adults
Men 40 yr old 26.6 37.2 48.0 8.3 11.4 14.5 7.2 9.9 12.6
Women 40 yr old 26.6 37.2 48.0 8.3 11.4 14.5 7.2 9.9 12.6
Note. The parametric values are presented in Table 2 and in Appendix. The values of QALV, V
ALV, and D
Lco used in simulations corresponded to a light
workload level.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

1088 N. H. Gosselin et al.
levels under extreme conditions such as low O2 pressures at
high altitudes or at intoxicating CO concentrations. This is so because the model presented assumes complete Hb satura-tion by either O
2 or CO and that the PO
2 partial pressure is
independent of CO concentrations, assumptions that are only valid under normal atmospheric pressures and relatively low CO concentrations. To cope with extreme or very acute condi-tions, several important modifications would be necessary.
Appendix
Determination of parametric valuesAlveolar ventilation rate (Q
ALV) and alveolar volume (V
ALV)
QALV
was obtained by multiplying VALV
and the respiratory fre-quency (f
R) (i.e., Q
ALV = f
R . V
ALV) . V
ALV is obtained by subtract-
ing the physiological dead space (VD
) from the tidal volume (V
T) (i.e., V
ALV = V
T – V
D), and V
D is the sum of the anatomical
dead space (VD_ana
) (mouth, pharynx, larynx, trachea, and bronchi) and the volume of gas that reaches the alveoli but has no exchange with blood (V
D_alv) (i.e., V
D = V
D_ana+V
D_alv).
ICRP (1994) proposed reference values for VT and f
R as a
function of age, gender, and workload level (see Table A1). ICRP (1994) also determined the value of V
D_ana for each
group through dimensional estimates of the upper respira-tory tract, regardless of the effort status. Baker and Burki (1987) observed that the contribution of V
D_alv to V
D for
sitting subjects was about 16% of VD_ana
. Moreover, these authors showed that the increase in V
D, measured for dif-
ferent workload levels, amounted to approximately 0.182 of the increase in V
T, with or without increase in f
R. These rela-
tions were incorporated in the determination of VD
for each workload level, group of age and gender (see Table A1).
Diffusing capacity of lungs for carbon monoxide (DLco
) The equation of Paoletti et al. (1985) that expressed D
Lco at rest
(DLco_rest
) as a function of age and height was retained for the purpose of this study. The average heights for each age and sex group from the anthropometry report of Demirjian (1980) were used. To measure the effect of workload level on D
Lco, Zavorsky et al. (2004) measured D
Lco in combination
with the workload in 8 healthy men of ages around 27 yr; their results were summarized by a linear regression for D
Lco
according to the workload (w) expressed in watts:
D = 46.9 + 0.06 wLco ⋅
The workload level in the study of Zavorsky et al. (2004) is measured assuming w = 0 at rest. To use this regression in concert with the energy consumption (W) convention of ICRP (1994), an algebraic transformation was done: w = W – W
rest, with W
rest = 30 watts for men at rest. Further, the preced-
ing intercept, equal to 46.9 mlCO
/min/mm Hg, is close to the mean value (i.e., 46.2 ml
CO/min/mm Hg) measured while sit-
ting in the study of Zavorsky et al. (2004). To obtain a general formula encompassing age and sex differences as well as dif-ferent workload levels, it is thus reasonable to substitute for the intercept the appropriate age and sex diffusing capacity at rest (D
Lco_rest) calculated from Paoletti et al. (1985). Hence,
D D 0.06 W W )Lco Lco_rest rest= + × ( (A3)
where Wrest
is the workload level at rest according to the ICRP convention. Table A2 shows the values of D
Lco for various age
and sex groups taking in the workload levels used to infer V
ALV and Q
ALV in Table A1.
The lack of details in experimental studies with children was made up for with the following approximations: For children aged 3 mo, 1 yr, and 5 yr, the values of D
Lco were
taken, respectively, equal to 1.70, 5.82, and 11.79 mlCO
/mm Hg/min−1 regardless of workload levels. These values are based on the results of Knudson et al. (1987) and Paoletti et al. (1985), which observed that the ratio “D
Lco/V
ALV” is prac-
tically constant with age. The values for the DLco
of children were thus obtained using this age-independent ratio and the V
ALV values are presented in Table A1.
All the preceding values of DLco
are given under STPD conditions (standard temperature and pressure and dry gas), as is usual in the literature. Since the kinetics model is build to cope with BTPS conditions (body temperature and pressure, saturated water vapour), a conversion factor is introduced in the model simulations to convert the D
Lco from
STPD to BTPS as follows:
D DLcoBTPS
LcoSTPD= ×β (A4)
This conversion factor is equal to 1.21 for a barometric pressure of 760 mm Hg and a water vapour pressure of 47 mm Hg (West, 1995).Maximum haemoglobin capacity for CO (BCO_Hb
Max ) The maxi-mum Hb capacity for CO (BCO_Hb
Max ) is obtained from the fol-lowing equation:
B b C VCO_HbMax
CO_HbMax
Hb BL= ⋅ ⋅
where the maximum amount of CO that can bind to 1 g of Hb (bCO_Hb
Max ) is equal to 1.389 mlCO
/gHb
, based on STPD con-ditions (IPCS, 1999). Under BTPS conditions, this value is equal to 1.68 ml
CO/g
Hb using the conversion factor .
In spite of the wide variability in the concentration of Hb (C
Hb) in blood (i.e., 135–170 g
Hb/L
blood for adults; Oser,
1965) and the gender difference (mean values of 165 and 145 g
Hb/L
blood for adult man and woman respectively; ICRP,
2002), Hb concentrations equal to 150 gHb
/Lblood
were used in model simulations for men and women to conform to the usual value quoted in the scientific literature (West, 1995; IPCS, 1999). The Hb concentrations for the other age groups were based on ICRP (2002), which gives values of 170, 115, and 145 g
Hb/L
blood for newborns, children 1 to 2 yr old, and
children 12 to 13 yr old, respectively.In model simulations, the blood volume (V
BL) was consid-
ered equal to 7.9% of body weight as proposed by Brown et al. (1997). The reference body weight was taken equal to 70 kg for men and 58 kg for women. The anthropometry report of Demirjian (1980) was used to determine the reference body weight for children as a function of age and gender.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Determination of carboxyhaemoglobin in humans 1089
Haldane’s coefficient Haldane’s coefficient (M) was obtained from in vitro experiments where human blood samples were exposed in turn to CO alone and to O
2 alone (Roughton,
1970). When almost all Hb is saturated, as is usually the case in healthy individuals, M values range from 200 to 260 (Roughton, 1970). The default value for M in the model sim-ulations was kept constant at 240 for adults and children.
Partial pressure of oxygen in lung capillaries (PO2
) Oxygen pressure in blood changes during blood passage through the lung capillaries: When blood enters into the capillaries,
oxygen pressure corresponds to the venous blood pressure (i.e., ≈ 40 mm Hg), whereas, as blood exits the lung capillar-ies, oxygen pressure is about 100 mm Hg. Since the maxi-mum oxygen pressure is rapidly attained, i.e., during the first third of blood’s 0.75-second passage in a lung capillary, the O
2 pressure in lung capillaries (P
O2) was taken as similar to
the one in arteries.Cotes (1975) proposed a relationship between this pres-
sure and age: PO2
= –0.24 · Age + 104.7. This yields a range of 85–104. 7 mm Hg when age is varied from 0 to 80 yr. In model
Table A2. Diffusing capacity of lungs for CO (DLco
) for different workloads, ages, and sex.
Age group
Sleeping At rest Light exercise Heavy exercise
Work wattsa
DLco
mlCO
/min/mm Hgb Work wattsa
DLco
mlCO
/min/mm Hgb Work wattsa
DLco
mlCO
/min/mm Hgb Work wattsa
DLco
mlCO
/min/mm Hga
10 yr old
Boys 13.8 14.5 21.1 17.9 59.7 20.3 118.4 23.8
Girls 13.8 18.5 21.1 18.9 59.7 21.2 98.2 23.5
15 yr old
Boys 18.7 34.1 26.7 34.6 73.6 37.4 155.8 42.3
Girls 15.6 27.2 22.2 27.6 69.4 30.5 137.0 34.5
Adults
Men
20 yr old 20 41.1 30 41.7 80 44.7 160 49.5
40 yr old 20 37.2 30 37.8 80 40.8 160 45.6
60 yr old 20 33.3 30 33.9 80 36.9 160 41.7
Women
20 yr old 14.2 28.3 21.7 28.8 66.7 31.5 144.0 36.1
40 yr old 14.2 27.0 21.7 27.4 66.7 30.1 144.0 34.8
60 yr old 14.2 25.3 21.7 26.1 66.7 28.8 144.0 33.4
Note. The amounts of CO are given in the STPD conditions (standard temperature and pressure and dry gas).aThe workloads are determined assuming that the ratio “alveolar ventilation rate/workload” of each age group is equal to the ratio for men presented in Table A1.bThe diffusing capacities of lungs for CO are calculated using the equations of Paoletti et al. (1985) and Zavorsky et al. (2004). The heights used before age 19 yr are the averages obtained by Demirjian (1980) for different age groups; the heights are 174. 4 cm for adult men and 159. 8 cm for adult women.
Table A1. Reference values for the respiratory parameters of a general population (adapted from ICRP, 1994).
Age group
Sleeping, 8% of maximum workloada
At rest, 12% of maximum workloada
Light exercise, 32% of maximum workloada
Heavy exercise, 64% of maximum workloada
VT
fR
VD
c QALV
d VT
fR
VD
b QALV
d VT
fR
VD
c QALV
d VT
fR
VD
c QALV
d
3 month 39 38 16 869 NAe NAe NAe NAe 66 48 21 2158 NAe NAe NAe NAe
1 yr old 74 34 18 1906 102 36 23 2843 127 46 28 4573 NAe NAe NAe NAe
5 yr old 174 23 46 2946 213 25 53 4000 244 39 59 7229 NAe NAe NAe NAe
10 yr old
Boys 304 17 85 3730 333 19 90 4620 583 32 135 14,325 841 44 182 28,982
Girls 304 17 85 3730 333 19 90 4620 583 32 135 14,325 667 46 151 23,752
15 yr old
Boys 500 14 144 4987 533 15 150 5749 1000 23 235 17,601 1352 36 299 37,915
Girls 417 14 131 3999 417 16 131 4571 903 24 220 16,397 1127 38 261 32,925
Adults
Men 625 12 145 5755 750 12 168 6982 1250 20 259 19,816 1923 26 382 40,074
Women 444 12 139 3658 464 14 143 4496 992 21 239 15,814 1364 33 307 34,893
Note. VT = tidal volume (ml
air)
; f
R = respiratory frequency (min−1); V
D = physiological dead space (ml
air); Q
ALV = alveolar ventilation rate (ml
air/min). Volumes
are given in the BTPS conditions (body temperature and pressure, saturated water vapour).a According to ICRP (1994), the maximal workload is 250 watts for an adult man.b Values of V
D are the anatomical dead space proposed by ICRP (1994) multiplied by a factor of 1.152 to account for the alveoli dead space.
c Values of VD
during sleeping, light and heavy exercises are calculated considering that the VD
variation amounts to 0.182 of the VT variation.
d QALV
= fR · (V
T – V
D).
e NA, not available.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

1090 N. H. Gosselin et al.
simulations, oxygen pressure in the lung capillaries of adults was kept constant at 97 mm Hg, corresponding to an adult 30 yr of age. For all other age groups considered, the P
O2
value was calculated according to Cotes formula.
Endogenous production rate of carbon monoxide (Endo) Coburn et al. (1963a) measured the endogenous produc-tion of CO in 10 healthy men; the measured values ranged from 0.0058 to 0.0095 ml
CO(STPD)/min with a mean value of
0.0070 mlCO
/min. The latter value was also observed in other studies with healthy male volunteers (Coburn et al., 1964, 1965). For children, it is expected that the endogenous pro-duction of CO is lower because the amount of heme pro-teins is lower than in adults, being virtually proportional to their body weight. Consequently, in model simulations, CO endogenous formation was set to be proportional to body weight. Knowing that the mean body weight of the volunteers in Coburn et al. (1963a) was 69.5 kg, the appropriate value for the mean endogenous production of CO can be expressed as follows:
Endo BW/69.5kgSTPD = ×0 0070. mLCO (A5)
The following formula converts Endo into BTPS conditions:
Endo E doBTPS STPD= ×β n (A6)
Oxidizing rate of carbon monoxide (kCO2
) The oxidization rate (k
CO2) value used, 3.33 × 10−5/min, applied to the total body
amount of CO corresponds to the mean values obtained by Tobias et al. (1945) and Luomanmäki and Coburn (1969) in experiments on volunteers exposed to labelled CO. This value for the oxidizing rate was also proposed by Coburn (1970).
Capture and release rates IPCS (1999) reported that 10% to 50% of the CO in body can be bound to metallopro-teins other than Hb based on the study of Luomanmäki and Coburn (1969) in which 5 human volunteers and 31 anesthetised dogs were exposed to 14CO. These authors, however, reported that the 50% value was only observed in the exposed dogs and came about from a high exposure to CO provoking severe hypoxemia. For humans, under non-poisonous conditions of exposure to CO, a range of 10% to 30% for the part of the total CO body amount located in extravascular spaces seems coherent with the reported data. From the differential equations [Eqs. (6), (7), and (8)], it can be shown that, in steady state, the fraction of body amount in extravascular tissues is equal to the parameter ratio k
HbS/k
Sf. Congruent with the 10–30% range observed in
experiments, this ratio was set equal to the median value of 0.2 in simulations.
Once the preceding ratio is set, it remains to determine either k
HbS or k
Sf. The value for k
Sf was determined by the
method of least square fit between model simulations and an experimental data set. The data set retained for this purpose was that of Tikuisis et al. (1987a) for the volunteers exposed
to 1500 ppm CO because these authors reported several physiological parametric values for these volunteers, values that were incorporated in the simulations, thus minimising uncertainties. The value estimated for the transfer rate k
Sf
was 0.01 min−1; consequently, using the ratio discussed ear-lier, the value used for k
HbS was taken to be 0.002 min−1.
Declaration of interest: This study was commissioned by Health Canada, Air Health Effects Division. The authors thank Health Canada for providing financial support. The authors alone are responsible for the content and writing of the paper.
ReferencesAllred, E. N., Bleecker, E. R., Chaitman, B. R., Dahms, T. E.,
Gottlieb, S. O., Hackney, J. D., Pagano, M., Selvester, R. H., Walden, S. M., Warren, J. 1989. Short-term effects of carbon monoxide exposure on the exercise performance of subjects with coronary artery disease. N. Engl. J. Med. 321:1426–1432.
Baker, R. W., Burki, N. K. 1987. Alterations in ventilatory pattern and ratio of dead-space to tidal volume. Chest 92:1013–1017.
Benignus, V. A. 1995. A model to predict carboxyhemoglobin and pulmonary parameters after exposure to O2, CO2, and CO. Aviat. Space Environ. Med. 66:369–374.
Bernard, T. E., Duker, J. 1981. Modeling carbon monoxide uptake during work. Am. Ind. Hyg. Assoc. J. 42:361–364.
Brown, R. P., Delp, M. D., Lindstedt, S. L., Rhomberg, L. R., Beliles, R. P. 1997. Physiological parameters values for physiologically based pharmacokinetics model. Toxicol. Ind. Health 13:407–484.
Bruce, E. N., Bruce, M. C. 2003. A multicompartment model of carboxyhemoglobin and carboxymyoglobin responses to inhalation of carbon monoxide. J. Appl. Physiol. 95:1235–1247.
Caughey, W. S. 1970. Carbon monoxide binding in heme proteins. Ann. NY Acad. Sci. 170:148–153.
Coburn, R. F., Blakemore, W. S., Forster, R. E.1963a. Endogenous carbon monoxide production in man. J. Clin. Invest. 42:1172–1178.
Coburn, R. F., Williams, W. J., Kahn, S. B., Forster, R. E.1963b. Endogenous carbon monoxide production in patients with hemolytic anemia (abstr.). J. Clin. Invest. 42:924.
Coburn, R. F., Williams, W. J., Foster, R. E. 1964. Effect of erythrocyte destruction on carbon monoxide production in man. J. Clin. Invest. 43:1098–1103.
Coburn, R. F., Forster, R. E., Kane, P. B. 1965. Considerations of the physiological variables that determine the blood carboxyhemoglobin concentration in man. J. Clin. Invest. 44:1899–1910.
Coburn, R. F. 1970. The carbon monoxide body stores. Ann. NY Acad. Sci. 174:11–22.
Cooper, D. Y., Schleyer, H., Rosenthal, O. 1970. Some chemical properties of cytochrome P-450 and its carbon monoxide coumpound (P-450 CO). Ann. NY Acad. Sci. 174:205–217.
Cotes, J. E. 1975. Lung function, Assessment and application in medicine, 3th ed. Osney Mead, Oxford: Blackwell Scientific Publications.
Cronenberger, C., Mould, D. R., Roethig, H.-J., Sarkar, M. 2007. Population pharmacokinetic analysis of carboxyhaemoglobin concentrations in adult cigarette smokers. Br. J. Clin. Pharmacol. 65:30–39.
Demirjian, A. 1980. Anthropometry report: Height, weight and body dimensions. Ottawa: Nutrition Canada. Santé et Bien-être social Canada.
Health Canada. 1989. Exposure guidelines for residential indoor air quality. Ottawa: Environmental Health Directorate Health Protection Branch.
International Programme on Chemical Safety. 1999. Environmental health criteria 213, Carbon monoxide, 2th ed. Geneva: World Health Organization, International Programme on Chemical Safety.
International Commission on Radiological Protection. 1994. Human respiratory tract model for radiological protection. ICRP Publication 66. Ann. ICRP 24:1–3.
International Commission on Radiological Protection. 2002. Basic anatomical and physiological data for use in radiological protection: Reference values. ICRP Publication 89. Ann. ICRP 32:3–4.
Kudson, R. J., Kaltenborn, W. T., Knudson, D. E., Burrows, B. 1987. The single-breath carbon monoxide diffusing capacity. Am. Rev. Respir. Dis. 135:805–811.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.

Determination of carboxyhaemoglobin in humans 1091
Luomanmaki, K., Coburn, R. F. 1969. Effects of metabolism and distribution of carbon monoxide on blood and body stores. Am. J. Physiol. 217:354–363.
Lynch, S. R., Moede, A. L. 1972. Variation in the rate of endogenous carbon monoxide production in normal human beings. J. Lab. Clin. Med. 79:85–95.
McCartney, M. L. 1990. Sensitivity analysis applied to Coburn-Foster-Kane models of carboxyhemoglobin formation. Am. Ind. Hyg. Assoc. J. 51:169–177.
National Institute for Occupational Safety and Health. 1972. Criteria for a recommended standard. Occupational exposure to carbon monoxide. Rockville: NIOSH.
Oser, B. 1965. Hawk’s physiological chemistry, 14th ed. New York: Blakiston Division, McGraw-Hill.
Paoletti, P., Viegi, G., Pistelli, G., Di Pede, F., Fazzi, P., Polato, R., Saetta, M., Zambon, R., Carli, G., Giuntini, C., Lebowitz, M. D., Kudson, R. J. 1985. Reference equations for the single-breath diffusing capacity. Am. Rev. Respir. Dis. 132:806–813.
Quanjer, P. H. 1983. Transfer factor (diffusing capacity). Bull. Eur. Physiopathol. Respir. 19:39–44.
Québec. 2001. Gouvernement du Québec: Règlement sur la santé et la sécurité du travail. Gazette officielle du Québec, Partie 2, Lois et règlements 133:5020–5133.
Roughton, F. J. W. 1970. The equilibrium of carbon monoxide with human hemoglobin in whole blood. Ann. NY Acad. Sci. 174:177–188.
Selvakumar, S., Sharan, M., Singh, M. P. 1992. Mathematical model for the exchange of gases in the lungs with special reference to carbon monoxide. Med. Biol. Eng. Comput. 30:525–532.
Selvakumar, S., Sharan, M., Singh, M. P. 1993. A mathematical model for the elimination of carbon monoxide in humans. J. Theor. Biol. 162:321–336.
Sharan, M., Selvakumar, S., Singh, M. P. 1990. Mathematical model for the computation of alveolar partial pressure of carbon monoxide. Int. J. Biomed. Comput. 26:135–147.
Singh, M. P., Sharan, M., Selvakumar, S. 1991. A mathematical model for the computation of carboxyhemoglobin in human blood as a function of exposure time. Philos. Trans. R. Soc. Lond. B Biol. Sci. 334:135–147.
Smith, M. V., Hazucha, M. J., Benignus, V. A., Bromberg, P. A. 1994. Effect of regional circulation patterns on observed HbCO levels. J. Appl. Physiol. 77:1659–1665.
Stewart, R. D., Peterson, J. E., Baretta, E. D., Bachand, R. T., Hosko, M. J., Herrmann, A. A. 1970. Experimental human exposure to carbon monoxide. Arch. Environ. Health 21:154–164.
Tikuisis, P., Buick, F., Kane, D. M. 1987a. Percent carboxyhemoglobine in resting humans exposed repeatedly to 1,500 and 7,500 ppm CO. J. Appl. Physiol. 63:820–827.
Tikuisis, P., Madill, H. D., Gill, B. J., Lewis, W. F., Cox, K. M., Kane, D. M. 1987b. A critical analysis of the use of the CFK equation in predicting COHb formation. Am. Ind. Hyg. Assoc. J. 48:208–213.
Tikuisis, P., Kane, D. M., McLellan, T. M., Buick, F., Fairburn, S. M. 1992. Rate of formation of carboxyhemoglobin in exercising humans exposed to carbon monoxide. J. Appl. Physiol. 72:1311–1319.
Tobias, C. A., Lawrence, J. H., Roughton, F. J. W., Root, W. S., Gregersen, M. I. 1945. The elimination of carbon monoxide from the human body with reference to the possible conversion of CO to CO2. Am. J. Physiol. 145:253–263.
U.S. Environmental Protection Agency. 2000. Air quality criteria for carbon monoxide. EPA 600/P-99/001F. Washington, DC: U.S. Environmental Protection Agency.
West, J. B. 1998. Pulmonary pathophysiology. The essentials, 5th ed. Baltimore, MD: Williams & Wilkins.
West, J. B. 2003. Respiratory physiology. The essentials, 6th ed. Baltimore, MD: Williams & Wilkins.
Whincup, P., Papacosta, O., Lennon, L., Haines, A. 2006. Carboxyhaemoglobin levels and their determinants in older British men. BMC Public Health 18(6):189.
White, P. 1970. Carbon monoxide production and heme catabolism. Ann. NY Acad. Sci. 174:23–31.
Zavorsky, G. S., Quiron, K. B., Massarelli, P. S., Lands, L. C. 2004. The relationship between single-breath diffusion capacity of the lung for nitric oxide and carbon monoxide during various exercise intensities. Chest 125:1019–1027.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wat
erlo
o on
11/
06/1
4Fo
r pe
rson
al u
se o
nly.