Embed Size (px)
Citation preview

Okihiro syndrome is caused by SALL4 mutations
Jurgen Kohlhase1,*, Marielle Heinrich1, Lucia Schubert1, Manuela Liebers1, Andreas Kispert2,
Franco Laccone1, Peter Turnpenny3, Robin M. Winter4 and William Reardon5
1Institut fur Humangenetik, Universitat Gottingen, Heinrich-Duker-Weg 12, 37073 Gottingen, Germany,2Institut fur Molekularbiologie, Medizinische Hochschule Hannover, Carl-Neuberg-Str. 1, 30625 Hannover, Germany,3Clinical Genetics, Royal Devon and Exeter Hospital, Barrack Rd, Exeter, 4Dept Clinical and Molecular Genetics,
Institute of Child Health, 30 Guilford Street, London WC1N 1EH, UK and 5National Centre for Medical Genetics,
Our Lady’s Hospital for Sick Children, Crumlin, Dublin 12, Ireland
Received July 26, 2002; Revised and Accepted September 11, 2002
Okihiro syndrome refers to the association of forearm malformations with Duane syndrome of eye retraction.Based on the reported literature experience, clinical diagnosis of the syndrome can be elusive, owing to thevariable presentation in families reported. Specifically, there is overlap of clinical features with otherconditions, most notably Holt–Oram syndrome, a condition resulting from mutation of the TBX5 locus andTownes–Brocks syndrome, known to be caused by mutations in the SALL1 gene. Arising from ourobservation of several malformations in Okihiro syndrome patients which are also described in Townes–Brocks syndrome, we postulated that Okihiro syndrome might result from mutation of another member of thehuman SALL gene family. We have characterized the human SALL4 gene on chromosome 20q13.13–q13.2.Moreover, we have identified literature reports of forelimb malformations in patients with cytogeneticallyidentifiable abnormalities of this region. We here present evidence in 5 of 8 affected families that mutation atthis locus results in the Okihiro syndrome phenotype.
INTRODUCTION
Duane anomaly, a congenital disorder of ocular motility, is acommon condition and accounts for up to 1% of all cases ofstrabismus (1). It consists of limitation of eye abductionassociated with retraction of the eye globe and narrowing of thepalpebral fissure on adduction. Although it may occasionally beseen as a familial feature, usually transmitted in autosomaldominant fashion, most patients with Duane anomaly aresporadic cases. Loci for Duane anomaly have been mapped tochromosomes 2q (2), 4q (3), 8q (4,5) and 22 (6). However,gene mutations resulting in Duane anomaly have not beendefined.
Careful examination of patients with Duane anomalyfrequently uncovers associated anomalies, most commonlyinvolving the external ear, hearing dysfunction, spinal andvertebral malformations, renal malformation and variabledegrees of upper limb hypoplasia (7,8). Consequently, severalclinical conditions have been delineated involving patients withDuane syndrome and associated malformations. However, it isunclear at present whether these conditions are truly distinct orwhether several ‘overlap syndromes’ exist, representing vari-able expression of a single genetic entity. The LondonDysmorphology Database lists 12 clinically distinct conditions
with Duane anomaly (9). Okihiro syndrome is one suchcondition.
Okihiro syndrome refers to the familial occurrence of radialsided hand malformations in association with Duane anomalyand has been observed in several reports (10–15). The range ofassociated features among the families described is broad,encompassing anal stenosis, pigmentary disturbance, atrialseptal defect, hearing impairment, renal abnormalities, externalear malformations and facial asymmetry in affected indivi-duals. Significant intrafamilial variability is a feature ofreported pedigrees.
SALL genes encode putative zinc finger transcription factorsknown to be important in human malformation syndromes, inthat mutation at the SALL1 locus causes Townes–Brockssyndrome (16). Until recently, three genes had been identifiedwithin this gene family, but SALL2 and SALL3 have not yetbeen associated with disease phenotypes (17,18). SALL4 is anew member of this gene family, which has been localized tochromosome 20q13.13–q13.2 (19). We hypothesized thatOkihiro syndrome might be the result of mutations of a humanSALL gene. This hypothesis was based on the observation ofoccasional clinical features of Okihiro syndrome in patientswith established mutations of human SALL1 as the cause oftheir malformations—specifically Duane anomaly, anal
*To whom correspondence should be addressed at: Institute for Human Genetics, University of Gottingen, Heinrich-Duker-Weg 12, 37073 Gottingen,Germany. Email: [email protected]
# 2002 Oxford University Press Human Molecular Genetics, 2002, Vol. 11, No. 23 2979–2987
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

stenosis, deafness and external ear anomalies (20). Theidentification of SALL4 and the localization of that gene tohuman chromosome 20 strengthened our hypothesis, in thatlimb malformations have been reported in patients withchromosomal deletions which are likely to encompass theSALL4 region of chromosome 20 (21,22). Moreover, aphenotype with cardiac and limb anomalies, thought torepresent a Holt–Oram presentation, has been reported witha de novo pericentric inversion of chromosome 20 involvinga break point at q13.2 (23).
In this communication we report the characterization of thehuman SALL4 gene. To rest the hypothesis that mutation at thislocus might cause Okihiro syndrome, we sought mutations ineight families. The study was specifically confined to familieswith Duane anomaly associated with radial limb malformation.We now present evidence that mutation at this locus causesOkihiro syndrome in 5 of the 8 families tested.
RESULTS
SALL4 consists of 4 exons (3159 bp of coding sequence) andencodes three C2H2 double zinc finger domains of the SAL-type, the second of which has a single C2H2 zinc fingerattached at its carboxy-terminal end, as well as an N-terminalC2HC zinc finger motif typical for vertebrate SAL-likeproteins. Comparison of the amino acid sequences of SALL1,
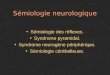
2, and 3 with SALL4 suggests that SALL3 and 4 might haveseparated after duplication of a common ancestor gene (datanot shown). While SALL3 encodes a fourth double zinc fingerdomain which seems to be spliced out preferentially from themRNA (18), the corresponding coding sequence is replaced byintron 2 in SALL4. A schematic comparison of the humanSALL proteins is shown in Figure 1.
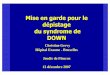
Multiple tissue northern blot analysis with poly(A)þ RNAfrom various human adult organs revealed expression of a5.5 kb transcript exclusively in adult testis but not in spleen,thymus, prostate, uterus, small intestine, colon, and peripheralblood lymphocytes (Fig. 2A). Expression was also not detectedin adult pancreas, kidney, skeletal muscle, liver, lung, placenta,heart and brain tissue as determined by multiple tissue northernblot analysis (data not shown). RT–PCR confirmed expressionin adult testis as well as lack of expression in brain, heart, lung,liver, kidney, and skeletal muscle but revealed faint SALL4expression in ovary and spleen (Fig. 2C). Northern blotanalysis with total RNA furthermore revealed SALL4 mRNAexpression in embryonal carcinoma cell lines H12.1 and 2102EP (24), respectively (Fig. 2B), but not in Jurkat, HeLa, andPC-3 cells (data not shown). In both SALL4 expressing celllines but not in non-expressing tissues (data not shown), asecond transcript of about 4 kb was observed (Fig. 2B). SinceRT–PCR with primers positioned in exons 2 and 4 as well as inexons 1 and 2 suggested that there is no alternative splicing inSALL4 (data not shown), the second transcript might result
Figure 1. Schematic comparison of the four human SALL proteins. Note that all four human SALL proteins share the typical SAL structure (36) with at least threewidely spaced C2H2 double zinc finger (DZF) motifs (zinc fingers are indicated as oval symbols) with a single C2H2 zinc finger attached to the second domain. Inaddition, all human SALL proteins share an additional N-terminal C2HC zinc finger characteristic for vertebrate SALL proteins. The carboxyterminal DZF ofSALL2 (black) is different from other SALL DZF domains. SALL4 encodes three C2H2 DZF domains and contains two carboxyterminal introns. SALL4 is mostsimilar to the most abundant SALL3 isoform (18) lacking the third DZF domain (splice sites indicated by arrows).
2980 Human Molecular Genetics, 2002, Vol. 11, No. 23
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

from alternative polyadenylation. This hypothesis is strenghtenedby the presence of two polyadenylation signals 198 bp and 1906bp 30 of the stop codon in the SALL4 genomic sequence.Comparison of 4000 bp sequence 30 to the SALL4 stop codonwith the human EST database revealed presence of highlyhomologous EST sequences only for the first 1906 bp, suggestingthat the longest SALL4 transcript contains a 30UTR of this size.
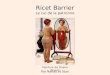
Eight unrelated families with Okihiro syndrome wereanalysed for SALL4 mutations (Fig. 3A–E) by amplificationof the coding sequences of exons 1–4 and direct sequencing ofSALL4 PCR products. In family 1 (14) the heterozygousnonsense mutation 1954C!T (Q652X) was detected whichsegregated with the clinical phenotype (Fig. 3A and B) inaffected individuals (II.2, II.3, II.5, III.3, III.4, III.5) and wasnot observed in clinically unaffected individuals (I.2, II.1, II.4,II.6, III.1, III.2). Patient III.6 is clinically unaffected but doescarry the mutation, being a non-manifesting heterozygote(Fig. 3A). Segregation of the mutation in the family wasanalysed by direct sequencing and confirmed by independentPCR and sequencing (data not shown).
In family 2 (unpublished), a heterozygous single base pairdeletion 1053delG was found which leads to a frameshift and apreterminal stop codon 4 bp 30 of the deletion (Fig. 3B). Thismutation, if not leading to nonsense-mediated decay of themRNA of the mutant allele, would result in a putativeprematurely terminated SALL4 protein lacking all double zincfingers. Sequencing of PCR products showed that all affectedfamily members carried the mutation. No samples were available
from unaffected family members. Results were confirmed byindependent PCR and sequencing (data not shown).
In patient III.1 of family 3 (Fig. 3C), direct sequencinganalysis (data not shown) showed a heterozygous 842delGmutation also causing a frameshift and a premature stop codon23 bp 30 to the deletion possibly resulting in a truncated SALL4protein lacking all double zinc finger domains. The mutationcreates a novel NlaIV restriction site and segregation of themutation was analysed by restriction digest of a 639 bp(mutant) and 640 bp (wild-type) internal PCR fragment of exon2. The mutation results in two novel fragments of 91 and 81 bpinstead of the wild-type fragment of 173 bp. All affected but nounaffected family members from whom DNA was availableshowed the mutation (Fig. 3C). The limb malformations in thisfamily were more severe than observed in the other familiesstudied (Fig. 4C–F).
In family 4, direct sequencing showed a 2288C!A transitioncreating a preterminal stop codon (S763X) (Fig. 3D). Themutation was found in all three affected but not in theunaffected family members as determined by direct sequen-cing. Results were confirmed by independent PCR andsequencing (data not shown).
In family 5, the 940–941insC insertion was detected only inthe affected girl but not in her unaffected mother (Fig. 3E). Thefather was unavailable. This mutation causes a frameshift with apremature stop codon after 112 bp. Results were confirmed byindependent PCR and sequencing (data not shown). Allmutations reported were not found in 100 control chromosomes
Figure 2. SALL4 expression analysis. (A) Multiple tissue northern blot (Amersham Biosciences) containing 2mg poly Aþ RNA per lane from eight different humanadult tissues. The blot was hybridized with DNA probes for SALL4 (upper) and human beta-actin cDNA as control (lower part). Tissues are: peripheral bloodleukozytes (lane 1), colon (lane 2), small intestine (lane 3), uterus (lane 4), testis (lane 5), prostate (lane 6), thymus (lane 7), spleen (lane 8). Note detection ofa SALL4 transcript of �5.5 kb (arrow) only in testis tissue. (B) Northern blot containing human total RNA of embryonal carcinoma cell lines H12.1 (lane 1)and 2102 EP (lane 2) showing a prominent transcript of �5.5 kb and a weaker signal at �4 kb (upper part). Lower part: beta actin control hybridization.(C) Upper: RT–PCR with total RNA from adult human tissues (brain (lane 1), heart (lane 2), lung (lane 3), liver (lane 4), kidney (lane 5), spleen (lane 6), ovary(lane 7), testis (lane 8) and skeletal muscle (lane 9)) showing a 929 bp SALL4 cDNA fragment strongly amplified from testis RNA and faintly from spleen andovary. Lower: amplification of a 352 bp HPRT cDNA fragment as control. C: control amplification without template.
Human Molecular Genetics, 2002, Vol. 11, No. 23 2981
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

2982 Human Molecular Genetics, 2002, Vol. 11, No. 23
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

as determined by direct sequencing of PCR products. No SALL4mutations were found in the remaining three families analysed.
DISCUSSION
Our results demonstrate that Okihiro syndrome is caused bytruncating mutations of the gene SALL4 (Fig. 5). Based onthe nature of the mutations we postulate that haploinsuffi-ciency for SALL4 is underlying the malformations seen inOkihiro syndrome. Confirmation of haploinsufficiency as theunderlying mechanism would require the observation ofOkihiro syndrome in a patient with confirmed deletion of the
SALL4 gene. However, in the absence of such a patient, adominant or dominant-negative effect of the mutations or aresidual activity of some mutant protein is still possible.Nonetheless, the available evidence favours haploinsuffi-ciency for several reasons. Truncating mutations likely resultin nonsense-mediated mRNA decay (25,26). Also, the limbmalformations seen in patients with cytogenetic deletions ofchromosome 20q, which probably encompass the SALL4locus, would be consistent with this (21,22). Finally thenature of the sequence changes we report and the predictedeffects of these are very similar to the spectrum of SALL1mutations seen in Townes–Brocks syndrome (TBS), whereonly truncating mutations of SALL1 have been found in TBSpatients (27). However, the mouse knock-out for thehomologous Sall1 gene did not reveal a phenotypemimicking TBS (28). Instead, bilateral hypoplasia or aplasiaof the kidneys were the only observed malformationssuggesting that the pathogenic effect of truncating humanSALL1 mutations could be different from haploinsufficiency.Alternatively, the different Sall genes could fulfill differentfunctions between mouse and human.
The most severe limb phenotype observed, in Family 3, iscaused by the most 50 positioned mutation (842delG), possiblyleading to proteins without double zinc finger domains. Asimilar outcome in terms of protein structure would be expectedof the 1053delG mutation. On the other hand, the limbphenotype of the 1053delG mutation is quite similar to thephenotype caused by mutations 1954C!T and 2288C!A,resulting in proteins lacking only the third double zinc fingerdomain. Consequently, it is not possible to reach firmconclusions with respect to the limb phenotype in terms ofmutation position, at this stage. Further families with SALL4mutations and protein studies are needed to investigate anypossible association between functional severity of mutationand the limb phenotype.
In the forelimb, SALL4 mutation in the most severe casesleads to phocomelic limbs (Family 3; Fig. 3B, Fig. 4C–F).However the limb phenotype observed in most of our patientsis milder, often involving the forearm, especially on the radialside, with associated thumb hypoplasia or reduplication. In afew instances, we have observed normal first metacarpal andcarpal formation and the condition is manifest only by absenceor hypoplasia of the thenar muscles (Fig. 4B). Additionalclinical features seen in our patient cohort include anal stenosis(Families 4 and 5), external ear malformations (Families 2, 4and 5), deafness (Families 2, 4 and 5), unilateral renal agenesis(Family 2), choanal stenosis (Family 2) and ventricular septaldefect (Family 3). In addition to a key role in upper limbmorphogenesis, these clinical features argue for SALL4function during normal development in several other tissues,including the ear, cloacal membrane, heart and kidney.However, the relatively high frequency of unilateral renalagenesis and ventricular septal defects in the normal populationmust be borne in mind while interpreting this observation.
We present confirmation of SALL4 mutations as the basis ofOkihiro syndrome. With one exception all patients reportedhave Duane retraction anomaly as a signal feature of thecondition. The exception, case III.6 of Family 1, we interpret asa non-manifesting carrier of the condition. Study of publishedpedigrees establishes that non-manifesting obligate gene
Figure 3. Mutations in 5 families with Okihiro syndrome. (A) Mutation1954C!T segregating in Family 1. The pedigree has already been reported(14). Note the nonmanifesting gene carrier III.6. Limb malformations are con-fined to the hands, the upper arm and forearms being normal. (B) Family 2,showing the 1053delG mutation, which segregates with the affected phenotype.The phenotype in this family included thumb hypoplasia, triphalangeal thumb,unilateral deafness, choanal atresia and unilateral renal agenesis as well asDuane anomaly. (C) Family 3, showing segregation of the 824delG mutationby NlaIV restriction digest. Note presence of the 81 and 91 bp mutant fragmentsin affected persons only. Clinically, due to the severity of the limb malforma-tions (Fig. 3B) and the observation of a ventricular septal defect in patientIII.1, an initial diagnosis of Holt–Oram syndrome was considered likely.However, the observation of Duane anomaly in several affected individuals inthe family suggested the true diagnosis. The limb phenotype in affected indivi-duals varied from phocomelia to very mild. (D) Family 4, demonstrating a2282C!A nonsense mutation associating with the affected phenotype. Thephenotype in this family comprised Duane anomaly, thumb malformations in-cluding reduplication, external ear malformations, deafness and anal stenosis.(E) Family 5, demonstrating a 940–941C insertion in affected individual II.1(absent in her mother I.1). The father was unavailable. The phenotype in thiscase comprises Duane anomaly, absence of the external ear, deafness, triphalan-geal thumbs and anal stenosis requiring surgery.
Human Molecular Genetics, 2002, Vol. 11, No. 23 2983
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

Figure 4. Clinical features of Okihiro syndrome patients. (A) Family 1 demonstrating Duane retraction anomaly. The patient is unable to abduct the left eye uni-laterally and on adducting the same eye there is retraction of the globe and narrowing of the palpebral fissure. (B) Patient II.3, family 1 demonstrating left thenarhypoplasia. (C–F) Limb malformations in three affected individuals of family 3. (C) I.2 has bilateral radial club hands with absence of the thumbs. (F) II.4 shows avery rudimentary upper limb, with absence of the thumb and forearm and a short humerus. (D) III.1 has a normal humerus but short forearm and absence of thethumb. (E) There is radiological fusion of the ulna and radius, which are foreshortened. The first metacarpals are absent.
2984 Human Molecular Genetics, 2002, Vol. 11, No. 23
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

carriers are known in this disorder (8), thus supporting ourview of the data in respect to this patient, in whose case theabsence of Duane anomaly has been confirmed on formalexamination. Moreover, the cosegregation of mutations withphenotype in the other families, the absence of mutations incontrol populations and the truncating nature of all mutationsdetected argue for a causal relationship between SALL4mutations and Okihiro syndrome. There were no identifiableclinical differences between the five families in whommutations were established and the three in whom we wereunable to demonstrate mutation of SALL4, one of which hasalso been the subject of a previous report (13).
The London Dysmorphology Database (9) lists 12 clinicallydistinct conditions with Duane anomaly, Okihiro syndromebeing one. However, dysmorphologists will recognizethe overlap phenotypes among our patient cohort and it mayprove instructive to seek SALL4 mutations in a wider patientpopulation. Foremost among such syndromes might be Holt–Oram syndrome, a developmental anomaly characterized byradial forelimb anomalies, congenital heart malformations andassociated features (29). Despite the identification of acausative locus for Holt–Oram syndrome at the TBX5 gene,only about 30% of clinically identified cases with this diagnosishave mutations of TBX5 (30). It is also noteworthy that a caseof Holt–Oram syndrome has already been reported in asso-ciation with a de novo pericentric inversion of chromosome 20,involving q13.2 (23). In light of the findings we present here,we would speculate that the subject of that report may have hadOkihiro syndrome, arising from disruption of the SALL4 gene.Other clinical disorders which might be considered ascandidates for mutation studies at SALL4 would be acro-reno-ocular syndrome (31), SALL1 mutation-negative Townes–Brocks syndrome as well as patients with isolated Duaneanomaly. Additionally, the identification of malformationsassociated with SALL4 will facilitate the investigation of thatgroup of patients with limb/cardiac anomalies originallyconsidered to represent examples of Thalidomide embryopathybut in whose offspring the observation of similar anomalies hasled to claims that Thalidomide is a mutagen as opposed to ateratogen (32).
MATERIALS AND METHODS
Patients
Genomic DNA was collected from patients with Okihirosyndrome and unaffected relatives after obtaining their informedconsent and with the approval of the Research Ethics Committee
of Great Ormond Street Hospital for Children, London.The diagnosis of Okihiro syndrome was based on presence ofDuane anomaly and upper limb malformations.
Northern blotting
For expression analysis of SALL4 a 32P-labelled probe of theIMAGE (33) clone 752642 (836 bp) was generated by useof rediprimeTM II labelling system (Amersham Biosciences,Freiburg, Germany) and hybridized to multiple tissue northernblots RPN4801 and RPN4803 containing polyAþ RNA ofdifferent adult human tissues (Amersham Biosciences) accord-ing to manufacturer’s protocols and to northern blots with totalRNA of human cell lines. RNA extraction, northern blottingand hybridization were carried out as described (34).
RT–PCR
2 mg of total RNA from adult human tissues (brain, heart, lung,liver, kidney, spleen, ovary, testis, skeletal muscle) were reversetranscribed using Ready-To-GoTM You-Prime First StrandBeads (Amersham Biosciences PeqLab, Erlangen, Germany)and 20 pmol each of primers SA4RTS2 and HPRTR (50-GTCAAGGGCATATCCTACAAC-AAAC-30) according to themanufacturers instructions. 1 ml of each first strand reactionwas used as a template in two subsequent PCR reactions withprimers 1) SA4E2S6N and SA4RTR2 (amplifying a 929 bpSALL4 fragment), and 2) HPRTF (50-CCTGCTGGATTACATCAAAGCACTG-30) and HPRTR.Primer sequences for HPRT were derived from the HPRTcDNA sequence (35). Fragments were amplified in 1�polymerase buffer with 1.5 mM MgCl2, 10 mM Tris pH 8.0,50 mM KCl using 1 ml of template cDNA, 100 mM dNTPs,primers 0.5 mM each, and 1 U Platinum Taq polymerase(Invitrogen, Karlsruhe, Germany). Cycling conditions were:95�C for 4 min followed by 35 cycles of amplification (1 min,94�C; 1 min, 64�C; 1 min, 72�C) and a final elongation step at72�C for 3 min on a Perkin Elmer/Cetus (Weiterstadt,Germany) thermocycler. Amplification products were visua-lized on agarose gels. The DNA sequence of the SALL4amplification product was verified by direct sequencing.
Genetic analysis
Genomic DNA was prepared from peripheral lymphocytes byroutine procedures. Primers for amplification and directsequencing of exons 1–4 are shown in Table 1. A 1560 bpfragment encompassing exon 1 was amplified with primersSA4E1F3 and SA4E1R3. Exon 2 was amplified with primers
Figure 5. Schematic representation of the SALL4 protein and localization of mutations identified.
Human Molecular Genetics, 2002, Vol. 11, No. 23 2985
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

SA4E2F6 and SA4E2R3 (5095 bp) followed by a nestedamplification with primers SA4E2F5 and SA4E2R2 resultingin a fragment of 4051 bp (Table 1). Exon 3 was amplified withSA4E3F1 and SA4E3R1 primers (456 bp fragment), exon 4(coding region; 660 bp fragment) with primers SA4E4F1 andSA4E4R1. Exons 1 and 2 were amplified using the SAWADYMid Range PCR system (PeqLab) according to the manufac-turer’s instructions (annealing temperature 64�C; Perkin Elmer/Cetus thermocycler). Exons 3 and 4 were amplified in 1�polymerase buffer with 1.5 mM MgCl2, 10 mM Tris pH 8.0,50 mM KCl using 100 ng of template genomic DNA, 100 mM
dNTPs, primers 0.5 mM each, and 1 U Platinum Taq polymerase(Invitrogen). The cycling parameters were: 95�C for 4 minfollowed by 35 cycles of amplification (1 min, 94�C; 1 min,64�C; 40 sec, 72�C) and a final elongation step at 72�C for3 min on a Perkin Elmer/Cetus thermocycler. PCR productswere analysed on 0.7% (exons 1 and 2) or 1% (exons 3 and 4)agarose gels, the fragments gel purified using the QIAquick gelextraction system (Qiagen, Hilden, Germany), cycle sequenced(primers see Table 1) using the ET Terminator Kit (AmershamBiosciences) and analysed on a MegaBace automated sequencer(Amersham Biosciences) following the manufacturer’s protocol.
Mutations in family 1 (1954C!T) and family 4 (2288C!A)were detected by direct sequencing of exon 2 with primersSA4E2S5N and SA4E2S6N (Table 1), respectively. Mutationsin families 2 and 5 (1053delG, family 2; 940–941insC,family 5) were detected by direct sequencing of exon 2 withprimers SA4E2S3N (Table 1). The mutation in family 3(842delG) was confirmed and analysed for segregation byinternal amplification of exon 2 (640 bp, wild-type; 639 bp,mutant) with primers SA4F581 and SA4R1281 (Table 1). PCRproducts were ethanol precipitated and restriction digested withNlaIV according to the manufacturers instructions (NewEngland Biolabs, Beverly, MA, USA). Restriction fragmentswere separated on a 2.5% agarose gel and visualized byethidium bromide staining.
GenBank accession numbers
SALL4 mRNA, NM_020436. Genomic contig NT_011362.
ACKNOWLEDGEMENTS
We would like to thank the families for their participation,generosity and patience. We would also like to thank H.-U.Pauer and P. Burfeind for discussion and comments, W. Engelfor review and support and M. Moschner and U. Teske fortechnical assistance. W.R. wishes to specifically acknowledgeM. Bitner for phlebotomy in family 1. Family 4 was brought toour attention by Richard Trembath. W.R. is supported by TheChildren’s Medical and Research Foundation at Our Lady’sHospital for Sick Children. This work was funded by theWilhelm-Sander-Stiftung (grant 98.075.2 to J.K.).
REFERENCES
1. Kirkham, T.H. (1970) Inheritance of Duane’s syndrome. Br. J. Ophthalmol.,54, 323–329.
2. Appukuttan, B., Gillanders, E., Juo, S.H., Freas-Lutz, D., Ott, S., Sood, R.,Van Auken, A., Bailey-Wilson, J., Wang, X., Patel, R.J. et al. (1999)Localization of a gene for Duane retraction syndrome to chromosome 2q31.Am. J. Hum. Genet., 65, 1639–1646.
3. Chew, C.K., Foster, P., Hurst, J.A. and Salmon, J.F. (1995) Duane’sretraction syndrome associated with chromosome 4q27–31 segmentdeletion. Am. J. Ophthalmol., 119, 807–809.
4. Vincent, C., Kalatzis, V., Compain, S., Levilliers, J., Slim, R., Graia, F.,Pereira, M.L., Nivelon, A., Croquette, M.F., Lacombe, D. et al. (1994) Aproposed new contiguous gene syndrome on 8q consists of Branchio–Oto–Renal (BOR) syndrome, Duane syndrome, a dominant form ofhydrocephalus and trapeze aplasia; implications for the mapping of theBOR gene. Hum. Mol. Genet., 3, 1859–1866.
5. Rickard, S., Parker, M., van’t Hoff, W., Barnicoat, A., Russell-Eggitt, I.,Winter, R.M. and Bitner-Glindzicz, M. (2001) Oto–facio–cervical (OFC)syndrome is a contiguous gene deletion syndrome involving EYA1 :molecular analysis confirms allelism with BOR syndrome and furthernarrows the Duane syndrome critical region to 1 cM. Hum. Genet., 108,398–403.
6. Cullen, P., Rodgers, C.S., Callen, D.F., Connolly, V.M., Eyre, H., Fells, P.,Gordon, H., Winter, R.M. and Thakker, R.V. (1993) Association of familialDuane anomaly and urogenital abnormalities with a bisatellited markerderived from chromosome 22. Am. J. Med. Genet., 47, 925–930.
7. Pfaffenbach, D.D., Cross, H.E. and Kearns, T.P. (1972) Congenital anomaliesin Duane’s retraction syndrome. Arch. Ophthalmol., 88, 635–639.
Table 1. SALL4 primer sequences
Exon Forward 50–30 Name Reverse 50–30 Name
Exon 1 GGTCCCCCTCTGATTTCGTC SA4E1F3* gaaaaccgcctcgctcctaaa SA4E1R3*ATTACTGGGACATGCGCGTTC SA4E1F1
Exon 2 aggcattgttctcagcagtcc SA4E2F6* ggctgctaacaaaggggtcat SA4E2R3*cttaggggtgtgccgacttg SA4E2F5# ccaggctcctttttgatgacc SA4E2R2#CACAGGGAGAATGGCGGCAG SA4E2S2N ACACAAGATCTGCTCGAGGAC SA4E2SR1CACATGTCTCAGCAGGTTTCTG SA4E2S3N ACACAAGATCTGCTCGAGGAC SA4E2SR2CCCAGCTGTTTGCCGAGTTC SA4E2S4N TGGGGATGTCGGTGAAAGTGC SA4R1281GGGTGGGACCAAACTATAATTC SA4E2S5NCAGAGAATCCCTGTGACTTTAC SA4E2S6NATCAGCGGAGCGCGGATGC SA4F581CTCACGCCAACATCCCTTCTG SA4F884
Exon 3 tacaaagccagctccagactc SA4E3F1* gaagacacctggtgcctagc SA4E3R1*Exon 4 ttgccagtgagcttcaaatctc SA4E4F1* AAGCAGCATAGCAACAATCGTG SA4E4R1*
AGACCGCCATTGAGC SA4RTS2CACAACAGGGTCCACATTCAC SA4RTR2
All primers were used for direct sequencing except for SA4E1F3, SA4E2F5, SA4E2F6, SA4E2R2 and SA4E2R3. Primers marked with * were also used forprimary PCR amplification, primers marked by # for nested amplification. Primers located in introns are lower case, whereas exonic primers are capitalized.
2986 Human Molecular Genetics, 2002, Vol. 11, No. 23
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from

8. Hayes, A., Costa, T. and Polomeno, R.C. (1985) The Okihiro syndrome ofDuane anomaly, radial ray abnormalities, and deafness. Am. J. Med. Genet.,22, 273–280.
9. Winter, R.M. and Baraitser, M. (2001) London Dysmorphology Database.Oxford University Press, Oxford.
10. Ferrell, R.L., Jones, B. and Lucas, R.V. Jr. (1966) Simultaneous occurrenceof the Holt–Oram and the Duane syndromes. J. Pediatr., 69, 630–634.
11. Okihiro, M.M., Tasaki, T., Nakano, K.K. and Bennett, B.K. (1977) Duanesyndrome and congenital upper-limb anomalies. A familial occurrence.Arch. Neurol., 34, 174–179.
12. Temtamy, S.A. and McKusick, V.A. (1978) The genetics of handmalformations. Birth Defects Orig. Artic. Ser., 14, 1–619.
13. MacDermot, K. and Winter, R. (1987) Radial ray defect and duaneanomaly: report of a family with autosomal dominant transmission.Am. J. Med. Genet., 27, 313–319.
14. Collins, A., Baraitser, M. and Pembrey, M. (1993) Okihiro syndrome:thenar hypoplasia and Duane anomaly in three generations. Clin.Dysmorphol., 2, 237–240.
15. Chun, B.B., Mazzoli, R.A. and Raymond, W.R. (2001) Characteristicsof Okihiro syndrome. J. Pediatr. Ophthalmol. Strabismus, 38, 235–239.
16. Kohlhase, J., Wischermann, A., Reichenbach, H., Froster, U. and Engel, W.(1998) Mutations in the SALL1 putative transcription factor gene causeTownes–Brocks syndrome. Nat. Genet., 18, 81–83.
17. Kohlhase, J., Schuh, R., Dowe, G., Kuhnlein, R.P., Jackle, H., Schroeder, B.,Schulz-Schaeffer, W., Kretzschmar, H.A., Kohler, A., Muller, U. et al.(1996) Isolation, characterization, and organ-specific expression of twonovel human zinc finger genes related to the Drosophila gene spalt.Genomics, 38, 291–298.
18. Kohlhase, J., Hausmann, S., Stojmenovic, G., Dixkens, C., Bink, K.,Schulz-Schaeffer, W., Altmann, M. and Engel, W. (1999) SALL3, a newmember of the human spalt-like gene family, maps to 18q23. Genomics, 62,216–222.
19. Deloukas, P., Matthews, L.H., Ashurst, J., Burton, J., Gilbert, J.G.,Jones, M., Stavrides, G., Almeida, J.P., Babbage, A.K., Bagguley, C.L.et al. (2001) The DNA sequence and comparative analysis of humanchromosome 20. Nature, 414, 865–871.
20. Kohlhase, J., Taschner, P., Burfeind, P., Pasche, B., Newman, B., Blanck, C.,Breuning, M., ten Kate, L., Maaswinkel-Mooy, P., Mitulla, B. et al. (1999)Molecular analysis of SALL1 mutations in Townes–Brocks syndrome.Am. J. Hum. Genet., 64, 435–445.
21. Fraisse, J., Bertheas, M.F., Frere, F., Lauras, B., Rolland, M.O. andBrizard, C.P. (1981) Un nouveau syndrome: del (20) (q13–qter).Localisation segmentaire de gene de l’adenosine deaminase (ADA). Ann.Genet., 24, 216–219.
22. Shabtai, F., Ben-Sasson, E., Arieli, S. and Grinblat, J. (1993) Chromosome 20long arm deletion in an elderly malformed man. J. Med. Genet., 30, 171–173.
23. Yang, S., Sherman, S., Derstine, J. and Schonberg, S. (1990) Holt–Oramgene may be on chromosome 20. Pediatr. Res., 27, 137A.
24. Casper, J., Schmoll, H.-J., Schnaidt, U. and Fonatsch, C. (1987) Cell linesof human germinal cancer. Int. J. Androl., 10, 105–113.
25. Culbertson, M.R. (1999) RNA surveillance. Unforeseen consequences forgene expression, inherited genetic disorders and cancer. Trends Genet., 15,74–80.
26. Hentze, M.W. and Kulozik, A.E. (1999) A perfect message: RNAsurveillance and nonsense-mediated decay. Cell, 96, 307–310.
27. Kohlhase, J. (2000) SALL1 mutations in Townes–Brocks syndrome andrelated disorders. Hum. Mut., 16, 460–466.
28. Nishinakamura, R., Matsumoto, Y., Nakao, K., Nakamura, K., Sato, A.,Copeland, N., Gilbert, D., Jenkins, N., Scully, S., Lacey, D. et al. (2001)Murine homolog of SALL1 is essential for ureteric bud invasion in kidneydevelopment. Development, 128, 3105–3115.
29. Newbury-Ecob, R.A., Leanage, R., Raeburn, J.A. and Young, I.D. (1996)Holt–Oram syndrome: a clinical genetic study. J. Med. Genet., 33,300–307.
30. Cross, S.J., Ching, Y.H., Li, Q.Y., Armstrong–Buisseret, L., Spranger, S.,Lyonnet, S., Bonnet, D., Penttinen, M., Jonveaux, P., Leheup, B. et al.(2000) The mutation spectrum in Holt–Oram syndrome. J. Med. Genet., 37,785–787.
31. Becker, K., Beales, P.L., Calver, D.M., Matthijs, G. and Mohammed, S.N.(2002) Okihiro syndrome and acro-renal-ocular syndrome: clinical overlap,expansion of the phenotype, and absence of PAX2 mutations in two newfamilies. J. Med. Genet., 39, 68–71.
32. McBride, W.G. (1994) Thalidomide may be a mutagen. Br. Med. J., 308,1635–1636.
33. Lennon, G., Auffray, C., Polymeropoulos, M. and Soares, M.B. (1996) TheI.M.A.G.E. Consortium: an integrated molecular analysis of genomes andtheir expression. Genomics, 33, 151–152.
34. Buck, A., Archangelo, L., Dixkens, C. and Kohlhase, J. (2000)Molecular cloning, chromosomal localization, and expression ofthe murine SALL1 ortholog Sall1. Cytogenet. Cell Genet., 89,150–153.
35. Jolly, D.J., Okayama, H., Berg, P., Esty, A.C., Filpula, D., Bohlen, P.,Johnson, G.G., Shively, J.E., Hunkapillar, T. and Friedmann, T. (1983)Isolation and characterization of a full-length expressible cDNA for humanhypoxanthine phosphoribosyl transferase. Proc. Natl Acad. Sci. USA., 80,477–481.
36. Kuhnlein, R.P., Frommer, G., Friedrich, M., Gonzalez-Gaitan, M.,Weber, A., Wagner-Bernholz, J.F., Gehring, W., Jackle, H. andSchuh, R. (1994) spalt encodes an evolutionary conserved zincfinger protein of novel structure which provides homeotic genefunction in the head and tail region of the Drosophila embryo.EMBO J., 13, 168–179.
Human Molecular Genetics, 2002, Vol. 11, No. 23 2987
by guest on May 3, 2013
http://hmg.oxfordjournals.org/
Dow
nloaded from