Embed Size (px)
Citation preview

ESTEFANIA ECHEVERRY
PROLIFERATION DES CELLULES GLIALES DANS LA MOELLE ÉPINIÈRE ET DOULEUR
NEUROPATHIQUE.
Mémoire présenté à la Faculté des études supérieures de l'Université Laval
dans le cadre du programme de Maîtrise en Neurobiologie pour l'obtention du grade de maître es sciences (M.Sc)
FACULTE DE MEDECINE UNIVERSITÉ LAVAL
QUÉBEC
2007
© Estefania Echeverry, 2007

i
RÉSUMÉ
Négligées pendant des siècles, les cellules gliales révolutionnent notre conception du
système nerveux. En effet, ces cellules pourraient être des éléments clés dans le
développement de plusieurs maladies et depuis quelques années elles apparaissent
comme des modulateurs importants dans la transmission des signaux nociceptifs. Ces
cellules une fois « activées » pourraient contribuer à l'initiation et au maintien de la
douleur neuropathique. Dans la présente étude, nous avons caractérisé le patron temporel
et spatial de la prolifération gliale, l'une des plus marquantes caractéristiques de
l'activation gliale, dans le cadre d'un modèle neuropathique induit par la lésion d'un nerf
périphérique. En se servant du bromodeoxyuridine (BrdU) comme marqueur mitotique,
nous avons analysé la prolifération des cellules dans la moelle épinière, identifié le
phénotype des cellules en division, et retracé leur destinée cellulaire, en faisant une
corrélation avec les phénomènes comportementaux typiques chez les animaux présentant
une douleur neuropathique. Nos résultats ont démontré qu'une lésion de nerf périphérique
induit une prolifération cellulaire précoce et transitoire dans la moelle épinière du côté
ipsilatéral à la lésion. La majorité des cellules en prolifération sont des microglies Iba-1+,
de concert avec quelques progéniteurs d'oligodendrocytes NG2+, et quelques astrocytes
GFAP+. On a observé une étroite corrélation temporelle et spatiale entre cette
prolifération microgliale dans la corne dorsale de la moelle épinière et les réponses de
douleur anormalement exagérées, ce qui suggère une importante contribution de la
nouvelle microglie à la genèse des symptômes présents dans les cas de douleur
neuropathique.

ii
ABSTRACT
Neglected for centuries, glial cells are revolutionizing our understanding of the nervous
system. Indeed, thèse cells could be key players in the development of many diseases and
in récent years they hâve appeared as important modulators in the transmission of
nociceptif signais. Thèse cells once "activated" could contribute to the initiation and
maintenance of neuropathic pain. In this study, we characterized the temporal and spatial
pattern of glial prolifération, one of the most striking features of glial activation, in the
context of a neuropathic pain model induced by peripheral nerve injury. Using
bromodeoxyuridine (BrdU) as a mitotic marker, we analyzed cell prolifération in the
spinal cord, identified the phenotype of dividing cells, and traced their fate, and
correlated thèse phenomena with behavioral assays of the neuropathic pain syndrome.
Our results demonstrated that peripheral nerve injury induced an early and transient cell
prolifération, on the spinal cord ipsilateral to the nerve lésion. The majority of
proliferating cells are microglia Iba-1+, together with a few progenitors of
oligodendrocytes NG2+, and a few GFAP+ astrocytes. There was a close temporal
corrélation between microglial prolifération in the spinal cord dorsal horn and the
abnormal pain responses, suggesting a contribution of the new microglia to the genesis of
neuropathic pain symptoms.

iii
Avant-propos
Le présent mémoire, témoigne du fruit de mes études de deuxième cycle en
neurobiologie. Pour les amateurs de cellules gliales, il s'avérera particulièrement
intéressant, car c'est de ces petites cellules dont il a été question au cours de mes travaux
de recherche. Je dois bien cela à ma directrice de recherche Dr. Ji Zhang, sa passion
pour les cellules gliales s'est avérée en effet, fort contagieuse. Il est difficile dans la vie
de trouver des gens qui te font confiance et qui sont prêts à te montrer généreusement la
voie et les outils pour atteindre tes objectifs ; je suis profondément reconnaissante d'avoir
une directrice de recherche avec ces qualités.
Ce mémoire, est divisé en trois parties. La première partie comprend une introduction au
sujet des cellules gliales et douleur. La deuxième partie comprend un article publié
récemment, qui expose les résultats du projet que j'ai entrepris au cours de ma maîtrise.
Finalement, dans la troisième partie, je fais le point sur les résultats exposés dans le
chapitre II, je discute du lien entre cette étude et l'étude présentée en annexe et je parle
des possibles avenues futures dans ce domaine de recherche. L'annexe I, est en fait un
article publié cette année aussi. J'ai pu participer à un moindre degré à ce projet et les
résultats présentés sont importants à mentionner dans ce mémoire.
Je ne pourrais pas terminer la présentation de ce mémoire sans remercier toutes les
personnes qui ont rendu possible l'atteinte de cet objectif. D'abord mes parents, Gabriel
et Patricia. Leur amour et leur constant appui, me permettent d'avancer chaque jour, alors
que je me retrouve si loin d'eux. Être dans un pays étranger peut résulter parfois très
difficile, mais la lumière que mes parents m'ont donnée me pousse vers l'avant pour aller
plus loin à chaque fois. J'ai la chance aussi d'avoir des amis merveilleux qui me

iv
encouragement à persévérer, quand je pense à Mireya et Carlos; Agnès; Hélène et Stella,
je n'ai que de bons souvenirs.
Je tiens à remercier à nouveau, ma directrice de recherche Dr. Ji Zhang pour sa
gentillesse, sa générosité et disponibilité et pour m'avoir accueilli à bras ouverts dans son
laboratoire pour mes études de deuxième cycle et pour mon futur doctorat ! Je voudrais
remercier aussi, nos collaborateurs Dr. Yves De Konick et Dr. Serge Rivest qui nous
inspirent énormément dans le monde de l'étude de la douleur et de la neuroimmunologie
respectivement.
Au centre de recherche Robert-Giffard, où mon travail de laboratoire a eu lieu, j'ai eu
l'occasion aussi de rencontrer des collègues et des amis fantastiques : Walter, Rémy,
Guillaume, Danny, Xiang, Judy-Fay, Sirisha, Albert et Daniel parmi d'autres. Merci à
tous pour votre amitié, surtout les trois derniers, qui ont fait de ma maîtrise une
expérience inoubliable, j'espère vous garder comme amis pour la vie. Merci aussi à mes
amies et à ma famille en Colombie. Merci à toi aussi, Ludovic, merci de m'encourager,
de me soutenir, de m'aimer. Ton amour est une source d'inspiration qui remplit mon
cœur de joie. Merci à tous de faire de moi ce que je suis aujourd'hui, je vous garde pour
toujours dans mon cœur et si j'avais à faire un article sur ma vie, probablement que vous
en seriez les mots-clés.

V
Je dédie ce mémoire à mes parents, Patricia et Gabriel, pour tout le support apporté au cours des
années, pour tous leurs encouragements et pour toute la confiance et l'amour qu 'ils me
témoignent

vi
Table des matières
RÉSUMÉ i
ABSTRACT ii
AVANT-PROPOS iii
LISTE DES FIGURES viii
LISTE DES ABRÉVIATIONS ix
CHAPITRE I
INTRODUCTION 2
LES CELLULES GLIALES ET LA DOULEUR 4
1. De la douleur en général 4
1.1 Caractéristiques de la douleur 4 1.2 Les mécanismes fondamentaux de la douleur 9
1.2.1 De la périphérie à la moelle épinière 9 1.2.2 De la moelle au cerveau 18
2. Des Cellules Gliales en général : 20
2.1. Rôle des cellules gliales de la moelle épinière dans le développement de la douleur neuropathique 24
3. Problématique 29
CHAPITRE II : Characterization of cell prolifération in rat spinal cord following
peripheral nerve injury and the Relationship with Neuropathic Pain 31
2.1 RÉSUMÉ 32 2.2 ABSTRACT 33 2.3 INTRODUCTION 34 2.4 MATERIALS AND METHODS 36 2.5RESULTS 42

vii
2.6 DISCUSSION 55 2.7 ACKNOWLEDGEMENTS 60 2.8 Référence List 61
CHAPITRE III
CONCLUSIONS ET PERSPECTIVES 67
BIBLIOGRAPHIE: 71
ANNEXE I : Expression of CCR2 in Both Résident and Bone Marrow-Derived
Microglia Plays a Critical Rôle in Neuropathic Pain 80

viii
LISTE DES FIGURES
Figure 1.1. Douleur Nociceptive, Inflammatoire et neuropathique 8
Figure 1.2.Voies de transmission des messages douloureux 13
Figure. 1.3 - Tronçon de moelle : segment de la région cervicale 14
Figure 1.4. Coupe horizontale d'une hémi-moelle (Albe-Fessard D.) 15
Figure 1.5. Les cellules gliales du système nerveux central 23
Figure 1.6. Activation microgliale suite à la lésion d'un nerf périphérique 26
Figure 1.7. L'effet du BDNF sur l'homéostasie neuronale dans la lamina I 28
Figure II.l 44
Figure II.2 46
Figure II.3 48
Figure II.4 50
Figure II.5 53
Figure II.6 54
Figure III.l. Les composantes de l'activation microgliale 69

ix
LISTE DES ABREVIATIONS
BrdU
NG2
OX-42
Iba-1
GFAP
DH
VH
GM-CSF
NO
PGs
EAA
BDNF
IL-ip
TNF-a
MCP-1
IL-6
P2X4
TLR4
GABA
Bromodeoxyuridine
A chondroitin sulphate proteoglycan
Complément receptor C3bi
lonized Calcium-Binding Adapter Molécule 1
Glial Fibrillary Acidic Protein
Dorsal Horn
Ventral Horn
Granulocyte-macrophage colony-stimulating
factor
Nitric Oxyde
Prostaglandins
Excitatory Amino Acids
Brain derived neurotrophic factor
Interleukine l-|i
Tumor necrosis factor a
Monocyte chemoattractant protein-1
Interleukine-6
Purinergic receptor-4
Toll like receptor-4
Gamma-amino-butyric acid

2
CHAPITRE I
INTRODUCTION
La douleur neuropathique est un état de douleur chronique avec des options de
traitements limités (Scholz et al. 2002). Elle est provoquée entre autres, par des
dommages aux nerfs qui transmettent l'information sensorielle (toucher, douleur,
température etc.). Les patients éprouvent une douleur intense en réponse à des stimuli qui
ne sont pas généralement douloureux et éprouvent également des douleurs spontanées et
exagérées. L'examen retrouve le plus souvent des signes d'hypersensibilité comme :
• L'allodynie : Qui correspond à la réduction d'un seuil douloureux ; un stimulus
normalement non nociceptif va donc être perçu comme douloureux par le patient.
Une allodynie doit toujours être caractérisée également par la modalité de
stimulation (mécanique, thermique, chimique) et le type de stimulus utilisé
(mécanique : toucher, pression, piqûre, distension ; thermique : chaud, froid ;
chimique : type de substance).
• L'hyperalgésie : Qui correspond à une perception douloureuse anormalement
intense à un stimulus normalement douloureux. Là encore la nature du stimulus
utilisé doit être précisée.
• L'hyperpathie : réaction excessive et durable après une stimulation répétée et (ou)
d'hypo sensibilité comme :
> L'hypoalgésie : diminution de la sensibilité à une stimulation nociceptive,
dans une zone spontanément douloureuse. On peut d'ailleurs parfois parler
d'anesthésie douloureuse.

3
La recherche sur la douleur neuropathique a toujours eu tendance à se concentrer sur les
changements induits par l'endommagement des nerfs sensoriels et les changements
secondaires au niveau des neurones de la moelle épinière qui reçoivent et analysent
l'information sensorielle avant qu'elle ne soit transmise au cerveau pour être « perçue ».
Cependant, des travaux récents montrent que les lésions de nerf activent également
d'autres cellules faisant partie du système nerveux : les cellules gliales de la moelle
épinière, et impliquent ces cellules dans la genèse et le maintien de la douleur
neuropathique.
C'est dans le cadre de cette problématique, que mes travaux de recherche au cours de ma
maîtrise se sont développés. J'ai pu constater que les cellules gliales sont en effet
impliquées dans les cas de douleur neuropathique suivant un processus
multidimensionnel appelé « activation gliale » dont les caractéristiques de forte
prolifération cellulaire ont particulièrement réveillé notre intérêt. Dans cette étude donc,
on reporte une description détaillée d'un des attributs les plus marquants de l'activation
gliale : la prolifération cellulaire dans la moelle épinière ; ce phénomène contribue
significativement au processus d'activation gliale, et donc à l'initiation et au maintien des
états de douleur neuropathique.

■I
LES CELLULES GLIALES ET LA DOULEUR
1. De la douleur en général
1.1 Caractéristiques de la douleur
Selon la définition de Y International Association for the Study of Pain (IASP), la douleur
est : « une expérience sensorielle et émotionnelle désagréable liée à des lésions tissulaires
réelles ou potentielles ou décrites en des termes évoquant de telles lésions ».
Il y a une dichotomie extraordinaire dans le domaine de la douleur. Un progrès
passionnant est accompli en identifiant les mécanismes moléculaires et cellulaires qui
opèrent dans les voies sensorielles pour produire des signaux neuraux que nous
interprétons finalement comme de la douleur (Julius et al. 2001; Woolf et al. 2000).
Cependant, pour nombreux patients, la douleur continue à produire une grave détresse,
qui perturbe la qualité de leurs vies. La majorité des traitements cliniques qui sont
actuellement disponibles sont partiellement efficaces et peuvent être accompagnés
d'effets secondaires affligeants ou avoir un potentiel d'abus important (Sindrup et al.
1999). L'augmentation du nombre de personnes du troisième âge dans la population
implique une augmentation des conditions douloureuses relatives à l'âge, comme
l'ostéoarthrite, qui exigent des traitements efficaces contre la douleur (Lynch et al, 2000).
Les améliorations dans la gestion du cancer augmentent l'espérance de vie, mais sont
accompagnées d'une élévation de l'incidence cumulative des syndromes chroniques de
douleur reliés aux tumeurs aussi bien que de la douleur liée à la thérapie, telle que la
polyneuropathie douloureuse induite par la chimiothérapie. Le besoin clinique insatisfait,
la douleur individuelle et les coûts économiques et sociaux de la douleur sont

5
substantiels. Pour établir le lien entre l'avancement de la neurobiologie de la douleur et le
manque de succès dans la thérapie clinique, un effort plus grand et plus sophistiqué doit
être dirigé vers la découverte de nouveaux analgésiques.
On peut caractériser la douleur par son profil évolutif en:
• Douleur aiguë : Elle est d'évolution brève et souvent de forte intensité. Elle a un
début et une fin bien précise. C'est un symptôme, une sensation déclenchée par le
système nerveux pour alerter l'ensemble de l'organisme et évoluant depuis moins
de trois mois. Elle s'accompagne de manifestations physiques, psychiques et
comportementales du domaine du stress. C'est un signal d'alarme utile qui appelle
un diagnostic et un traitement étiologique.
• Douleur chronique : Elle est sans limite dans le temps et évolue depuis 3 à 6
mois, persistante et rebelle aux traitements usuels. D'intensité variable, elle
s'accompagne de modifications émotionnelles du registre de l'anxiodépression et
de modifications du comportement social, familial et professionnel. Alors que la
douleur aiguë est plus considérée comme une « douleur-symptôme », la douleur
chronique se définit comme une entité propre, véritable « douleur-maladie ». La
douleur chronique atteint tout l'individu, elle n'a plus aucune fonction, ni objectif
biologique. Elle envahit la vie de l'individu, l'univers affectif, le vécu quotidien,
qu'il soit professionnel, social et personnel.
La douleur chronique peut être liée à une maladie ou à une déficience, ou se manifester
après un accident. Son origine peut être variable (cancéreuse, séquellaire etc.). Avec
certains types de douleurs chroniques, comme les migraines, la douleur est à répétition
plutôt que constante. Il existe de nombreux autres types de douleurs chroniques, comme

6
les douleurs post-chirurgicales chroniques, la cellulomyalgie, le syndrome temporo-
mandibulaire, etc. Pour le patient, cette douleur devient la composante la plus critique de
sa maladie.
La douleur comme sensation peut être divisée en catégories distinctes
La douleur normalement sert comme dispositif d'avertissement, un système d'alarme
activé en réponse aux dommages imminents dans l'organisme. Cette douleur
nociceptive est activée seulement par des stimuli nocifs agissant sur un appareillage
sensoriel spécialisé à seuil élevé (Fig. I.la) (Scholz et Wolf 2002). La nociception est
essentielle pour la survie des organismes dans un environnement potentiellement hostile.
Une fois que le tissu a été endommagé mécaniquement ou par infection, ischémie, la
croissance d'une tumeur ou par un processus auto-immun, des médiateurs chimiques
multiples sont libérés à partir des cellules endommagées et inflammatoires. «La soupe
inflammatoire» résultante est riche en cytokines, facteurs de croissance, kinines, purincs,
aminés, prostanoïdes et ions, y compris des protons (Boddeke et al. 2001 ; Mantyh et al.
2002). Quelques médiateurs inflammatoires activent directement des nocicepteurs,
évoquant la douleur. D'autres agissent ensemble pour produire une sensibilisation du
système nerveux somatosensoriel, ce qui caractérise la douleur inflammatoire,
permettant une activation plus facile de la voie nociceptive jusqu'à ce que le tissu
guérisse (Fig. I.lb). Une plasticité mésadaptée représente des changements qui produisent
de la douleur spontanée et exagérée sans avoir un rôle protecteur ou réparateur
discernable. Cette douleur nommée douleur neuropathique, est générée typiquement
par l'intermédiaire de dommages du système nerveux central ou périphérique ou de son
dysfonctionnement (Fig. I.le).

7
En effet, les douleurs neuropathiques peuvent être dues à des lésions du système nerveux,
que ce soit au niveau périphérique (à la suite d'une amputation, de la section d'un nerf,
d'un zona, d'une neuropathie diabétique ou alcoolique etc.) ou central (après un
traumatisme médullaire, sclérose en plaque etc.). Ces douleurs peuvent être spontanées,
se manifestant ainsi en l'absence de tout stimulus et sont :
• permanentes (fourmillements, brûlure, piqûre, broiement etc.)
• ou paroxystiques (douleurs fulgurantes en décharge électrique, élancement, coup
de poignard etc.).
Cependant, elles peuvent aussi se manifester après un stimulus normalement non
douloureux, comme un courant d'air ou un effleurement, ou d'un stimulus peu
douloureux qui est perçu de façon exagérée. Dans tous les cas, ce sont des douleurs très
invalidantes s'accompagnant parfois, surtout quand elles sont chroniques, d'anxiété et de
dépression. (Lynch et al. 1998). C'est à ce type de douleur que nous nous intéresserons
dans cette étude.

8
Dotileui Réaction «mo t i ve
Réflexe <l>nleveiiient
l> Doiilem infl.imimitohe
,F v. ..<*jr, U * t ï Y » ;
(ri'-'' ° W W
^id^.: ~ " * Ô „ NeuIropM . ^ j . . . ~ , _ 0 / ' nf,initor.t
m Y
Jp o • • J
0 O HmlMrfno SkVQtgrtn
H-N«ivo (jrowlh lactof
iln.iii*;-!!.-. INI.. PiXtttualilfKlinJ EWfWholins Al'P Inlurimikins
c Douleiii Nemoptithiqiie L»ilon<tolamo«M»plnlM
..
Accliltnt C»I*I>I o-va •culnli*
■• .n. ii oui » du canal cmpian
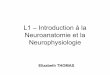
Figure 1.1. Douleur Nociceptive, Inflammatoire et neuropathique.
a. Les stimuli nociceptifs sont traduits en activité électrique dans les terminaux périphériques des fibres C, par des nocicepteurs ou par des canaux ioniques sensibles à la chaleur, à des stimuli mécaniques, aux protons et au froid. Cette activité est acheminée à la moelle épinière et ensuite au cortex, où la sensation de douleur est perçue, b. Du tissu endommagé, des cellules inflammatoires ou tumorales libèrent des médiateurs chimiques qui activent ou modifient les propriétés de réponse aux stimuli, des nocicepteurs afférents, c. La douleur neuropathique résulte d'un dysfonctionnement ou des lésions du système nerveux. Des conditions affectant le système nerveux périphérique, comme le syndrome du canal carpien, la lésion de la moelle épinière ou les traumatismes au cerveau après un accident cérébro-vasculaire, peuvent tous provoquer des douleurs neuropathiques, qui se caractérisent par une combinaison de déficits neurologiques et une douleur amplifiée. (Adapté d'après Scholz et Wolf, 2002).

9
1.2 Les mécanismes fondamentaux de la douleur
René Descartes, le philosophe et scientifique, peut être crédité comme le premier à avoir
essayé de comprendre la douleur, de façon documentée. Il a donné naissance en effet, à la
théorie qui décrit que la transmission de la douleur se fait par un canal simple qui
connecte la peau au cerveau. Cet arrangement simplifié du réflexe, édité en 1664 dans le
«Traité de l'Homme», était le commencement du développement de la doctrine moderne
des réflexes (Descartes R. 1972).
La théorie de Ronald Melzack et Patrick Wall a intensément contesté celle de Descartes.
Leur théorie du portillon ou «gâte control theory», proposée en 1965, révolutionna l'étude
de la douleur et ouvra les portes à la recherche sur les phénomènes de plasticité dans la
sensibilisation spinale et dans le système nerveux central, des phénomènes
pathophysiologiques causant la douleur chronique (Melzack R. et Wall PD 1965) Le
traitement de la douleur a lieu dans une matrice intégrée tout le long de l'axe neuronale et
se produit sur au moins trois niveaux : dans les domaines périphériques, médullaire, et
supra-spinale (Fig. 1.2). (DeLeo et al. 2006).
1.2.1 De la périphérie à la moelle épinière
Le circuit neurobiologique complexe qu'emprunte l'influx douloureux depuis les nerfs
périphériques jusqu'au cerveau comporte schématiquement trois parties :
- En périphérie, des terminaisons sensorielles spécialisées reçoivent des stimuli
physiques, thermiques ou chimiques provenant de la peau, des muscles ou des viscères.

10
- Ces fibres sensorielles provenant des tissus cutanés s'associent aux fibres motrices pour
former des troncs nerveux mixtes souvent regroupés en plexus avant d'atteindre la
moelle.
- Ces plexus se subdivisent pour entrer de façon étagée dans le canal vertébral (appelé
aussi canal rachidien). (Fig. 1.2.)
Les fibres sensorielles cutanées et musculaires se séparent des fibres motrices avant leur
entrée dans le canal rachidien. À ce niveau on retrouve les ganglions rachidiens qui
contiennent les corps cellulaires de neurones jouant un rôle sensitif, c'est-à-dire assurant
la sensibilité de la partie du corps innervée par le nerf rachidien auquel elles
appartiennent. Les fibres motrices se trouvent dans les racines ventrales. Les racines
dorsales ont donc un rôle purement afférent, les ventrales un rôle essentiellement efférent
(Stein C. 1995).
En périphérie, les messages nociceptifs sont générés au niveau des terminaisons
nerveuses libres amyéliniques constituant des arborisations plexiformes dans les tissus
cutanés, musculaires et articulaires. Ces terminaisons sont considérées aujourd'hui
comme les récepteurs habituels de la douleur ou nocicepteurs. Les messages nociceptifs
sont ensuite véhiculés dans les nerfs par les fibres Aô et les fibres C. On distingue trois
modalités de nocicepteurs :
• Unimodaux: Activés que par stimulation nociceptive mécanique (=
mécanonocicepteurs); ils sont en relation avec les fibres Aô.
• Multimodaux: Activés indifféremment par des stimulations nociceptives
mécaniques ou thermiques.

I l
• Polymodaux: Activés aussi bien par stimulation physique, mécanique ou
thermique, que par nature chimique. (= chimiorécepteurs). Ils sont en relation
avec les fibres C.
Les lésions périphériques peuvent sensibiliser ces nocicepteurs, causant la libération de
médiateurs algésiques tels que les prostaglandines, le potassium, l'histamine, les
leukotriènes, la bradykinine, et la substance P. C'est le pourquoi de l'usage systémique de
drogues anti-inflammatoires nonsteroidalles et de l'aspirine, qui diminuent la production
de prostaglandines sensibilisatrices chez les patients qui présentent une douleur
inflammatoire.
Les terminaisons nerveuses libres se prolongent par des fibres dans les nerfs
périphériques. Il existe deux types de fibres :
• Fibres myélinisées (groupe A) à seuil d'excitation bas, dissociées en fonction de
leur calibre et de leur vitesse de conduction en sous-groupe: a, p\ 8 (peu
myélinisées).
-A8, transmettent les douleurs aiguës de courte durée à type de piqûre ; elles assurent
la conduction de la douleur rapide, épicritique
• Fibres non-myélynisées (groupe C), à seuil d'excitation bas, de très petit calibre.
Les fibres de gros calibre, de conduction rapide, ne conduisent pas la douleur, mais
conduisent des messages sensitifs. Les fibres de petit calibre, de conduction très lente,
conduisent la douleur.

12
- Les fibres C, transmettent les douleurs plus diffuses à type de brûlure ; c'est la
conduction de la douleur lente, protopathique. Ces fibres font synapse dans la corne
dorsale de la moelle épinière, où la modulation spinale se produit (Fig.1.2.)
L'influx suit un neurone périphérique ou protoneurone dont le corps cellulaire est situé
dans le ganglion rachidien. Après leur trajet dans les nerfs périphériques, les fibres
afférentes rejoignent le système nerveux central par les racines rachidiennes postérieures
ou leurs équivalents au niveau des nerfs crâniens. Les fibres Aô et C se terminent de
façon massive au niveau des couches superficielles de la corne dorsale de la moelle
(couche I, zone marginale et couche II, qui correspond à la substance gélatineuse) (Fig.
1.2., voir aussi Fig. 1.4.). Les fibres A de gros calibre forment deux collatérales primaires
dans la moelle, l'une monte et rejoint les fibres des colonnes dorsales pour atteindre
l'étage bulbaire, l'autre descend pendant quelques segments. De ces deux collatérales
primaires partent des collatérales secondaires dont certaines prennent contact avec les
motoneurones ce qui correspond au réflexe médullaire (réflexe d'extension, phénomène
médullaire sans intégration corticale), les autres connectent avec les interneurones
médullaires qui reçoivent déjà les terminaisons des fibres afférentes de plus fin diamètre
(C et un peu de Aô).

13
Région bulbo-mésencéphalique
I
Structures supra-spinales
V Contrôles descendants
(5-HT, NA, CCK, SP...)
Ganglions rochidions dorsaux
Neurones sensoriels primaires
Périphérie
5-HT PG NGF
Bradykinine Cytokines...
Interneurones
Enképhalines, GABA, SP, CCK...
Moelle epinière
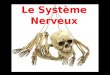
Figure 1.2.Voies de transmission des messages douloureux.
Les neurones sensoriels primaires, dont les corps cellulaires sont localisés dans les ganglions rachidiens dorsaux, transmettent les signaux nociceptifs vers leur premier relais central, la corne dorsale de la moelle epinière. Les signaux nociceptifs sont ensuite acheminés, au travers de certaines structures supraspinales «relais», vers le cortex cérébral ou l'information «douloureuse» est intégrée. Dans la moelle epinière, la transmission des signaux est modulée, entre autres, par des neurones descendants (notamment à partir de la région bulbomésencéphalique) et des interneurones spinaux, mettant en jeu de nombreux neuromédiateurs: sérotonine (5-HT), noradrénaline (NA), cholécystokinine (CCK), acide y-aminobutyrique (GABA). Lors d'une inflammation périphérique, certaines molécules présentes dans «la soupe inflammatoire»: prostaglandines (PG), nerve growth factor (NGF), cytokines, bradykinine peuvent agir directement sur les terminaisons des neurones sensoriels pour les sensibiliser et même pour modifier, à plus long terme, leur phénotype. (Meunier et al. 2004).

14
1.2.1.1 Organisation de la moelle épinière : IM moelle épinière, porte d'entrée
des fibres sensitives dans le système nerveux central.
Un segment de moelle est constitué de deux parties :
• la substance grise, zone centrale contenant des corps cellulaires ;
• la substance blanche, région où ne se trouvent que des fibres entourant cette
substance grise. Celle-ci contient les fibres afférentes et efférentes et les faisceaux
spinaux de conduction (Fig. 1.3.).
Figure. 1.3 - Tronçon de moelle correspondant à un segment de la région cervicale, région dorsale vers le haut. (Albe-Fessard D. 1996)
La substance blanche médullaire
Les fibres contenues dans une racine dorsale pénètrent dans la moelle du côté où elles
sont entrées dans le canal rachidien. Elles le font avec une organisation médio-latérale.
Les fibres de plus grand diamètre (AaP et une partie des AS) entrent le plus médialement.
Les fibres de plus fin diamètre, en majorité non myélinisées (une partie des fibres A8 et
les fibres C) entrent plus latéralement. Sur la figure 1.4., sont représentés l'entrée des
fibres apportées par une radicelle ainsi que leurs terminaisons. Les contingents médian et

15
latéral sont représentés par des traits de grosseurs différentes permettant de suivre sur le
schéma le trajet des fibres qu'ils apportent.
Contingent médian
Zone marginale
Subst. gélatineuse Contingent
latéral
Noyau propre
Figure 1.4. Coupe horizontale d'une hémi-moelle (Albe-Fessard D.)
Les fibres conduites par chaque contingent sont signalées, ainsi que les niveaux où elles
se terminent. Les couches de Rexed sont indiquées en chiffres romains (I, II, III, etc.) et
les noms des régions équivalentes (zone marginale, substance gélatineuse, ...) dans la
nomenclature de Ramon y Cajal sont notées à droite.

16
1.2.1.2 Rôle de la moelle épinière dans la conduction des messages
nociceptifs :
Des fibres nociceptives, peu ou pas myélinisees, conduisent à des vitesses variables le
message douloureux jusqu'à un premier relais : la corne postérieure de la moelle épinière.
Comme on l'a déjà mentionné, les fibres de petit calibre transmettent beaucoup plus
lentement des stimuli nociceptifs intenses (mécaniques, thermiques ou chimiques). Dans
la moelle épinière, ces petites fibres stimulent notamment la libération de la substance P,
une molécule intervenant dans la transmission du signal de douleur (Julius et al, 2001).
La moelle épinière traite et module le message nociceptif, qu'elle transmet ensuite au
tronc cérébral puis au thalamus et à d'autres structures du cerveau. Très schématiquement,
à partir de la moelle épinière, deux grands types de faisceaux ascendants véhiculent le
message nociceptif jusqu'au cerveau : une voie latérale, rapide, spécialisée dans la
composante sensitive de la douleur, et une voie médiane, plus lente, qui intervient dans
ses composantes affective et émotionnelle. Fait remarquable, il existe au niveau de la
moelle épinière un système d'inhibition qui « filtre » la douleur. Les fibres de gros calibre
(Aap) jouent un rôle clé dans cette inhibition (Porreca et al, 2002).
♦ La théorie du « Gâte control »
Les fibres sensitives de gros calibre A8 et A(î inhibent la propagation de l'influx
nociceptif en excitant un système interneuronal inhibiteur. L'influx algique est lui
véhiculé par les fibres AS et C. L'interneurone est situé dans la couche II ou substance
gélatineuse de Rolando d'après hypothèse, les influx en provenance des grosses fibres
entretiendraient un tonus inhibiteur, lequel serait fixé par l'arrivée « suffisante » d'une

17
volée nociceptive (entraînant l'ouverture de portillon) tonus qui au contraire, serait
renforcé par une activation supplémentaire des Aô(3. Cela explique notamment pourquoi,
en cas de brûlure par exemple, on se sent soulagé lorsqu'on se frotte à l'endroit où l'on
vient de se brûler : le stimulus tactile léger, transmis rapidement par les grosses fibres,
inhibe le stimulus douloureux intense qui est lui transmis lentement par les petites fibres.
Dans la moelle épinière il semble y avoir aussi l'amplification secondaire, qui
contrairement à l'amplification primaire siège en dehors de la lésion et relève de
mécanismes beaucoup plus complexes. Tout en nécessitant la présence des influx
nociceptifs périphériques (puisqu'elle disparaît lors d'une anesthésie locale appliquée au
niveau de la lésion), cette amplification secondaire semble liée à un accroissement de la
réactivité de certains neurones du système nerveux central qui ont été « sensibilisés » par
l'activation initiale des nocicepteurs. Ainsi «sensibilisés», certains neurones de la corne
dorsale de la moelle, sur lesquels convergent des messages conduits non seulement par
des fibres fines mais aussi par des fibres de grand diamètre Aap, pourraient présenter des
réponses exagérées aux stimulations tactiles de faible intensité et être ainsi à l'origine des
phénomènes d'allodynie et d'hyperalgésie.
Enfin, dans certains cas de lésion du nerf, quand la régénération fait suite à la
dégénérescence, certaines fibres AaP établissent de nouveaux contacts synaptiques avec
des neurones qui initialement, n'étaient activés que par des stimulations nociceptives
(Woolf C.J. et al. 1992). C'est justement au niveau de la moelle épinière la où la
sensibilisation secondaire a lieu, que les cellules gliales ont été perçues comme ayant un
comportement particulier, et potentiellement nocif en ce qui concerne la douleur
chronique, comme on le verra plus loin.

18
1.2.2 De la moelle au cerveau
♦ Voies ascendantes impliquées
Les voies ascendantes antéro-latérales jouent un rôle majeur dans la transmission des
messages nociceptifs vers les centres supérieurs.
- faisceaux spino-réticulaires
- faisceaux spino-ponto-mésencephaliques
- faisceau spino-thalamique.
De la moelle vers le thalamus, les fibres se regroupent en faisceaux, déterminant :
• La voie lemniscale : Elle est composée de fibres myéliniques Aa de gros calibre ;
cette voie est le support de la sensibilité discriminative (sensibilité tactile fine,
etc.).
• La voie extra-lemniscale : Elle est composée de fibres myéliniques Aô et
amyéliniques de petit calibre, elle est celle de la sensibilité discriminative
(perceptions tactiles grossières, thermiques, douloureuses).
♦ Du thalamus vers le cortex
Après leur trajet dans les nerfs périphériques, les fibres afférentes font synapse dans le
thalamus, relais fondamental de la nociception. A partir du thalamus, les projections se
font sur les aires sensitives du cortex. La sensation douloureuse brute est fournie par le
thalamus ; le cortex intervient pour y ajouter des composantes : l'algognosie (prise de
conscience d'une douleur) et l'algothymie (répercussion affective de la douleur).
En effet, dans le cerveau les systèmes de modulation et d'intégration du message
douloureux sont extrêmement complexes. Toutes les données de la neurophysiologie
actuelle s'inscrivent contre l'idée ancienne d'un centre cérébral unique de la douleur.

19
L'imagerie cérébrale a même révélé que de nombreuses régions du cerveau participent à
la perception de la douleur. Pour schématiser, le thalamus qui reçoit le message
douloureux projette deux groupes de neurones dans le cerveau : le premier se dirige vers
le cortex pariétal, qui décrypte la sensation douloureuse pour en déterminer la
localisation, l'intensité, la durée et le type (brûlure, piqûre etc.) ; le second se dirige vers
le cortex frontal, lequel analyse et définit la part émotionnelle du message douloureux.
(Hofbauer et al. 2001)
Comme on l'a déjà vu, tout au long des circuits nociceptifs interviennent des systèmes de
modulation et d'inhibition notamment dans la moelle épinière, mais aussi par des voies
descendantes issues de la région postérieure du cerveau.
♦ Contrôles d'origine supra-spinale
Us s'exercent essentiellement depuis le tronc cérébral. Expérimentalement, la stimulation
électrique de la substance grise péri-aqueducale (SGPA) au niveau du mésencéphale ou
de certains noyaux du raphé (au niveau du bulbe) entraîne des effets antalgiques
importants. Elle bloque la transmission spinale de l'influx nociceptif en mettant en jeu
des voies descendantes inhibitrices qui sont surtout sérotoninergiques et
noradrénergiques. D'autres systèmes ont été identifiés : dopaminergiques, cholinergiques
(avec la CCK ou cholécystokinine), etc.

20
2. Des Cellules Gliales en général :
Le terme glie (du mot grecque signifiant «colle») reflète la présomption du dix-neuvième
siècle voulant que ces cellules servent exclusivement à soutenir le système nerveux d'une
manière quelconque. Le mot a survécu, en dépit du manque d'évidence qui supporte
l'idée que «coller» des cellules est une des fonctions des glies. Les rôles gliales qui sont
bien établis incluent : le maintien du milieu ionique des cellules nerveuses ; la modulation
du taux de propagation des signaux nerveux ; la modulation synaptique en contrôlant la
prise de neurotransmetteurs dans la synapse ; fournir un échafaudage dans quelques
aspects du développement neural, et faciliter (ou empêcher, parfois) le rétablissement de
dommages neuraux. Il y a trois types de cellules gliales dans le système nerveux central
mature : les astrocytes, les oligodendrocytes, et les microglies (Fig. 1.5) (Zigmond et al.
1999).
Les astrocytes, résidents exclusivement du cerveau et de la moelle épinière, ont des
ramifications raffinées qui donnent à ces cellules un aspect d'étoile, (d'où le préfixe
«astro»). Les astrocytes, comme la plupart de cellules gliales, ont longtemps été
considérés essentiellement pour leur rôle de support et d'entretien du tissu nerveux. Mais
de plus en plus d'évidences plaident en faveur d'une implication beaucoup plus
importante des astrocytes dans la communication nerveuse.
On connaît depuis longtemps leur rôle de pourvoyeur du glucose nécessaire à l'activité
nerveuse. Grâce à leurs «pieds» apposés contre la paroi des capillaires sanguins
cérébraux, le glucose peut pénétrer dans les astrocytes où il est partiellement métabolisé
et retransmis aux neurones. Il semble même qu'une activité synaptique plus intense

21
favorise un apport plus élevé de glucose en activant le travail des astrocytes (Holash et
Stewart 1993).
On sait aussi que les astrocytes sont couplés les uns aux autres par des «gap-jonctions» à
travers lesquels peuvent circuler divers métabolites. C'est par ces jonctions que les
astrocytes évacuent vers les capillaires le potassium extracellulaire excédentaire généré
par une intense activité neuronale. Mais ce qu'on découvre de plus en plus, c'est que ce
réseau d'astrocytes communiquant, forme un véritable syncytium, c'est-à-dire qu'ils se
comportent comme un seul et même élément. À travers ce réseau se propageraient par
exemple des vagues d'ions calcium dont l'effet régulateur pourrait se faire sentir dans un
grand nombre de synapses en même temps.
Une fonction importante des astrocytes est aussi de maintenir, par une multitude de
moyens, un environnement chimique approprié pour garantir une bonne signalisation
neuronale.
Les oligodendrocytes, qui sont également limités au système nerveux central, fixent un
emballage riche en lipides appelé myéline autour d'une grande proportion d'axones. Le
motif très particulier de cet enroulement accélère la conduction nerveuse. (Kettenman et
Ransom 1995)
Finalement, les cellules microgliales, la première ligne de défense contre les
envahisseurs étrangers, et considérées comme les macrophages du cerveau, sont dérivées
principalement de précurseurs hématopoïétiques. Elles partagent beaucoup de propriétés
avec les macrophages retrouvés dans d'autres tissus, et sont principalement des cellules
phagocytaires qui enlèvent les débris cellulaires des emplacements où il y a eu une lésion
ou un renouvellement cellulaire naturel (Sykova et al. 2000). En outre, les microglies,

22
tout comme les macrophages, sécrètent des molécules de signalisation en particulier un
éventail de cytokines, qui sont également produits par des cellules du système
immunitaire, et qui peuvent moduler l'inflammation locale et influencer la survie ou la
mort cellulaire.
Après des lésions au cerveau, le nombre de microglies à l'emplacement des dommages
augmente considérablement. Certaines de ces cellules en prolifération correspondent à
des microglies résidentes du cerveau, alors que d'autres viennent des macrophages qui
émigrent dans les secteurs blessés et entrent dans le cerveau par des de ruptures locales
dans la vascularisation cérébrale (McMahon et al. 2006).
Différents types de cellules gliales assurent donc, chacune à sa façon, le bon
fonctionnement des neurones du système nerveux central. Des noms différents sont
donnés aux cellules gliales qui assument ces fonctions dans le système nerveux
périphérique. On parle alors de cellules satellites pour le support mécanique des neurones
et de cellules de Schwann pour la fabrication de la myéline.

23
Astrocytes Oligodendrocytes Microglie
Figure 1.5. Les cellules gliales du système nerveux central. L'astrocyte tire son nom de sa forme étoilée : d'une petite masse cytoplasmique partent des prolongements diversement ramifiés qui, au contact des autres cellules, s'élargissent en pied astrocytaire L'oligodendrocyte est une cellule de petite taille dont les prolongements s'enroulent en plusieurs feuillets autour des axones voisins pour former la gaine de myéline. Celle-ci est régulièrement interrompue entre chaque prolongement oligodendritique par de brefs espaces appelés nœuds de Ranvier. La cellule microgliale au repos, ou microglie ramifiée, est une petite cellule ovoïde dotée de prolongements épineux plus ou moins longs. (D'après Jones et Cowan 1983)

24
2.1. Rôle des cellules gliales de la moelle épinière dans le
développement de la douleur neuropathique.
Il y a quelques années présentant ses études faites à l'université du Colorado, Linda
Watkins avait proposé que les cellules gliales contribuent à la douleur chronique
résultante des lésions du système nerveux périphérique (Watkins et al. 2001). Cela était
en désaccord avec la pensée prééminente dans le domaine, qui soutenait que la douleur
était due purement à un malentendu entre les neurones. Cette conférence avait contrarié
plusieurs neuroscientifiques qui se trouvaient dans l'assistance.
De nos jours de tels mécontentements deviennent plus rares. L'idée autrefois hérétique
que les cellules gliales sont les joueurs principaux dans la douleur neuropathique dirige
maintenant, nombreuses recherches sur la douleur. La découverte de l'importance des
cellules gliales a donné une nouvelle vie à une idée longtemps mise aux marges de la
neurologie : les cellules gliales peuvent avoir un rôle principal au cœur des désordres
affectant le système nerveux, y compris la douleur neuropathique (Miller et al. 2005).
Les cellules gliales ont été considérées pour la première fois comme un facteur important
dans les cas de douleur chronique, par Garrison et ses collègues (Garrison et al. 1994). Us
ont fait des marquages par immunohistochimie afin d'examiner l'expression d'un
marqueur spécifique d'activation astrocytaire, la protéine GFAP (glial fibrillary acidic
protein). Ils ont trouvé que : (1) les manipulations qui créent une douleur exagérée
activent également les astrocytes de la moelle épinière du côté ipsilatéral à la lésion, et
(2) une drogue qui bloque cette douleur exagérée bloque également l'activation des
astrocytes. Depuis lors, chaque modèle animal de douleur pathologique (impliquant une

25
lésion nerveuse) étudié jusqu'ici, a indiqué une corrélation positive entre la «douleur
exagérée» et l'activation gliale dans la moelle épinière (DeLeo JA. 2001 ).
Mais, qu'est-ce que l'activation gliale exactement ? Qu'on parle d'astrocytes ou de
microglies il s'agit toujours d'un processus multidimensionnel. Les microglies s'activent
suite à plusieurs événements affectant le système nerveux central notamment l'invasion
microbienne, la lésion de la moelle épinière et les lésions de nerf. La cellule microgliale
au repos, ou microglie ramifiée, est une petite cellule ovoïde dotée de prolongements
épineux plus ou moins longs. Lorsqu'elle est activée, la cellule microgliale subit des
modifications morphologiques qui la transforment en microglie amiboïde, où les
prolongements disparaissent et le corps cellulaire s'agrandit (Tsuda et al. 2001) (Fig. I.6.).
Une fois activées les microglies relâchent des substances pro-inflammatoires telles que
des cytokines et des chimiokines et d'autres facteurs pouvant faciliter la douleur
(McMahon 2005). Une des meilleures façons d'étudier l'impact des microglies sur la
douleur c'est de suivre ce processus complexe d'activation.
En effet, après une lésion, des processus pro-inflammatoires se mettent en place pour
faciliter la réparation du tissu endommagé, et même combattre des possibles infections.
La douleur neuropathique qui résulte d'une lésion périphérique n'implique pas seulement
des processus inflammatoires au niveau de la lésion mais aussi au niveau de la moelle
épinière. Étant donné que la moelle elle-même ne présente aucun dommage, le fait que
des processus inflammatoires puissent y avoir lieu, est remarquable

26
Figure 1.6. Activation microgliale suite à la lésion d'un nerf périphérique. A. Une forte immunoreactivité au marqueur microglial Iba-1 apparaît après une lésion périphérique causant de la douleur neuropathique. B. Cette activation a lieu surtout du côté ipsilatéral à la lésion où on observe une augmentation de la densité cellulaire et des changements brusques dans la morphologie de la microglie. (D'après Zhang et al.2006 et Echeverry et al. 2007).
Ainsi les questions suivantes se posent naturellement. L'activation gliale est-elle
nécessaire pour l'induction et le maintien de la douleur neuropathique ? L'activation gliale
est-elle suffisante pour induire cette douleur ?
Dans les dernières années, plusieurs études ont tenté de répondre à ces questions en
utilisant des inhibiteurs gliaux tels que le fluorocitrate ou la minocycline. Le premier, un
bloqueur du métabolisme microglial et astrocytaire, administré avant ou après la lésion,
inhibe l'apparition de douleur neuropathique (Milligan 2000, 2003 ; et Meller 1994);
alors que la minocycline (inhibiteur spécifique des microglies) arrive à prévenir
l'apparition de la douleur mais pas à la réduire une fois celle-ci s'est établie
(Raghavendra 2003). Ces études indiquent que, alors que les astrocytes auraient un rôle
important au niveau du maintien de la douleur, les microglies seraient davantage

27
impliquées dans les phases initiales de cette condition. De plus, l'implantation de
microglies «activées» in vitro dans la moelle épinière de rongeurs naïfs, provoque des
signes de douleur neuropathique (d'allodynie mécanique) chez ces animaux. (Tsuda et al.
2003). Comment ces petites microglies arrivent elles à déclencher cette pathologie?
Quelques études récentes se sont penchées sur la question, est sont arrivées à proposer
des mécanismes plausibles pour expliquer les détails de ce phénomène.
Coull et collaborateurs par exemple, ont découvert un lien critique entre l'activation
microgliale et l'altération neurosensorielle provoquant la douleur neuropathique (Coull et
al. 2005) Ils ont démontré que les microglies bouleversent le contrôle inhibiteur de le
moelle épinière, et que la molécule clé derrière ce phénomène est le facteur
neurotrophique BDNF (Brain Derived Neurotrophic Factor) relâché par les microglies.
Cette équipe, sous la direction du Dr. Yves De Koninck, avait déjà démontré que la
douleur neuropathique est directement reliée à des altérations neuronales (causées par des
lésions périphériques) dans la région de la couche I de la moelle épinière, l'origine des
voies nociceptives qui vont vers le cerveau (Coull et al. 2003). Normalement le
tamponnage inhibiteur se fait dans la moelle par l'intermédiaire des neurotransmetteurs
GABA et glycine qui en se liant à des canaux ioniques, permettent l'entrée massive
d'ions Cf. Ces ions, hyperpolarisent les neurones de la couche I, inhibant du même coup
cette voie nociceptive. Mais après la lésion, le nombre de transporteurs de C1"(KCC2) est
réduit, ce qui cause une accumulation d'ions Cl" à l'intérieur des neurones. Quand le
GABA se lie aux récepteurs-canaux Cl" alors, les ions au lieu d'entrer pour
hyperpolariser, ils sortent pour dépolariser et l'inhibition est interrompue (Fig. 1.7.).
Comment les microglies sont impliquées dans cette situation ? Les auteurs ont observé

28
que le relâchement de BDNF par les microglies cause directement ce virage
d'hyperpolarisation vers dépolarisation car lorsque cette relâche est interrompue, la
dépolarisation anormale l'est aussi et la douleur est abolie. De plus, lorsque le BDNF est
injecté de façon locale près des neurones, il cause l'accumulation d'ions chlorures dans
les cellules nerveuses de la moelle (Fig. 1.7.)
Avant lésion Après lésion
Doulaur pathologique
Transmission du lignai th douleur
au carvaau
Au cerveau /mtcmçjf / activé* ,
Figure 1.7. L'effet du BDNF sur l'homéostasie neuronale dans la couche I. (D'après
De Koninck Y. 2006).

29
3. Problématique
À la lumière de ce que l'on connaît à propos de l'activation microgliale, quelques
questions suscitent encore beaucoup de débats.
1- Quel est le facteur déclencheur de cette activation ? Il y a plusieurs candidats: Le
récepteur surexprimé chez les microglies activées, P2X4 et son ligand l'ATP. (Tsuda et
al. 2003) ; Des cytokines comme le TNF-alpha, et IL-6 (Klein et al. 1997) ; La Fractalkine
qui en se liant à son récepteur induit l'activation in vitro et in vivo (Verge et al. 2004) ; Le
récepteur TLR4 (Tanga et al. 2005) ; et la chimiokine MCP-1 (Abbadie et al. 2003). En
effet cette dernière protéine, est exprimée après la lésion du nerf sciatique dans les
ganglions rachidiens, se présente aussi dans la moelle épinière et est suive par l'activation
des microglies et des astrocytes (Zhang et al.2006). Notre équipe présente maintenant de
nouveaux résultats qui confirment le rôle critique de cette chimiokine dans le
déclenchement de l'activation microgliale (Annexe 1 : Zhang et al. 2007)
2- Quelle est l'origine de ces cellules activées ? On sait que les cellules résidentes de
la moelle se transforment et deviennent «actives» suite à des manipulations qui causent
de la douleur neuropathique. Ce qui est moins clair est la participation d'autres
populations telles que des cellules nouvellement formées ou des macrophages dérivés de
la moelle osseuse pouvant infiltrer la moelle épinière. Dans l'étude présentée en annexe
nous apportons de nouveaux indices montrant la contribution des cellules dérivées de la
moelle osseuse; alors que dans l'étude présentée dans le chapitre suivant, on s'est
intéressés aux possibles contributions d'une population de cellules activées, générée par
prolifération cellulaire.

30
La prolifération cellulaire, est en effet, plutôt rare dans le système nerveux en général et
la moelle épinière n'en est pas l'exception. Plusieurs études ont observé une forte
prolifération dans les cas de lésion de la moelle épinière (Liu et al, 2000 ; Horky et al,
2006). Dans notre cas nous avons analysé cette prolifération alors que la moelle épinière
est intacte, mais toujours dans le cadre d'une forte activation gliale. En d'autres mots,
nous nous sommes intéressés dans cette étude, à comprendre plus en détail une des
caractéristiques de cette activation : la prolifération cellulaire dans la moelle épinière.
Est-ce que l'activation est une transformation exclusive des cellules dormantes de la
moelle ? Est-ce que cette activation comprend aussi le démarrage d'une forte génération
cellulaire afin d'incorporer plus de cellules activées ? Et si c'est le cas, quelle est la
contribution de cette nouvelle population au processus d'activation, et même, quelle
serait la contribution de cette nouvelle population à la douleur neuropathique? Dans le
chapitre suivant, nous essayons de répondre à ces questions.

31
CHAPITRE II
Characterization of cell prolifération in rat spinal cord following
peripheral nerve injury and the relationship with neuropathic pain
Stefania Echeverry, Xiang Qun Shi, Ji Zhang
Unité de Neurobiologie Cellulaire, Centre de Recherche Université Laval Robert-Giffard,
Université Laval, 2601, Chemin de la Canardière, Québec, QC, Canada Gl J 2G3
Received 3 January 2007; received in revised form 10 April 2007; accepted 1 May 2007
* Pain (2007), doi:10.1016/j.pain.2007.05.002

M
2.1 RÉSUMÉ
L'activation gliale est une réaction du système nerveux central aux lésions nerveuses.
Dans la présente étude, nous avons caractérisé temporelle et spatialement la prolifération
gliale, l'une des plus visibles caractéristiques de cette activation, et sa relation avec la
douleur neuropathique induite par la lésion d'un nerf périphérique. En utilisant le
bromodeoxyuridine (BrdU) comme marqueur mitotique, nous avons analysé la
prolifération cellulaire dans la moelle épinière, identifié le phénotype des cellules en
division et tracé leur destinée, tout en faisant une corrélation avec les phénomènes
comportementaux typiques de la douleur neuropathique. Nos résultats ont démontré que
la blessure d'un nerf périphérique induit une forte prolifération cellulaire, dans la moelle
épinière du côté ipsilatéral à la lésion nerveuse, qui atteint un pic 3 jours après la lésion.
La majorité des cellules proliférantes étaient des microglies Iba-1+, de concert avec
certains progéniteurs d'oligodendrocytes NG2+, et quelques astrocytes GFAP+. Ces
cellules nouvellement générées continuent à se diviser dans le temps et la réponse atteint
son sommet 14 jours après la blessure. Les microglies demeurent toujours le phénotype
principal, et plus de 60% des microglies activées proviennent de cette population de
cellules nouvellement produites. Il existe une étroite corrélation temporelle entre cette
prolifération microgliale dans la corne dorsale de la moelle épinière et les réponses de
douleur exagérées, suggérant une contribution de cette nouvelle population de microglies
à la genèse des symptômes associés à la douleur neuropathique

33
2.2 ABSTRACT
Glial activation is a typical response of the central nervous system to nerve injury.
In the current investigation, we characterized the temporal and spatial pattern of glial
prolifération, one of the most conspicuous features of glial activation, in relation to nerve
injury-induced neuropathic pain. Using bromodeoxyuridine (BrdU) as a mitotic marker,
we analyzed cell prolifération in the spinal cord, identified the phenotype of dividing
cells, traced their fate, and correlated thèse phenomena with behavioral assays of the
neuropathic pain syndrome. Our results demonstrated that peripheral nerve injury
induced an early and transient cell prolifération, on the spinal cord ipsilateral to the nerve
lésion which peaked at day 3 post-surgery. The majority of the proliferating cells were
Iba-1+ microglia, together with some NG2+ oligodendrocyte progenitors, and GFAP+
astrocytes. Thèse newly generated cells continued to divide over time with the response
peaking at day 14 post-injury. Microglia were always the prédominant phenotype which
made up over 60% of activated microglia derived from this newly generated cell
population. There was a close temporal corrélation between microglial prolifération in
the spinal cord dorsal horn and the abnormal pain responses, suggesting a contribution of
the new microglia to the genesis of the neuropathic pain symptoms.

34
2.3 INTRODUCTION
Glial cells réside in the healthy central nervous system (CNS) as a ubiquitously
distributed quiescent cell population that responds to changes in the CNS environrnent
and react swiftly to pathological events. Glial activation is a characteristic of the CNS
response to injury in the peripheral and central nervous system, stroke, and inflammatory
and neurodegenerative disease. Peripheral nerve injury induced glial responses in the
spinal cord dorsal horn hâve been demonstrated in différent animal models of painful
peripheral neuropathy (Colburn, Rickman et al. 1999;Fu, Light et al. 1999;Zhang, Hoffert
et al. 2003).
Activated microglia are characterized by a spécifie morphology, prolifération,
increased expression of cell surface markers and receptors, and changes in function, such
as migration to areas of damage, phagocytosis, and production/release of pro-
inflammatory substances (Gehrmann, Matsumoto et al. 1995). The same conditions that
activate microglia also activate astrocytes; this response can be recognized by
hypertrophy and increased production of glial fibrillary acidic protein (GFAP).
Functionally this activation is characterized by the increased production of a variety of
trophic factors and a very spécifie class of cytokines (gpl30 ligands, such as IL-6, CNTF,
etc.). There is évidence that both activated microglia and astrocytes contribute to
neuropathic pain following peripheral nerve injury (Watkins, Milligan et al.
2001;Watkins and Maier 2002;Tsuda, Inoue et al. 2005).
An unanswered question is whether activation is a property of only those cells
that already existed in the spinal cord, or whether thèse cell populations are increased due
to prolifération or recruitment. The current study was performed to provide a detailed

:*5
characterization of the temporal and spatial pattern of glial cell prolifération in the spinal
cord following a peripheral nerve injury that gives rise to a neuropathic pain syndrome.
We conducted a chronic constriction injury on the left sciatic nerve of animais (Mosconi
and Kruger 1996). With the thymidine analog, bromodeoxyuridine (BrdU) as index, we
investigated non-neuronal cell prolifération around central terminais of injured sensory
neurons in the dorsal horn and proliferative response of perineuronal glial cells in the
ventral horn. We traced the fate of cells incorporating BrdU at 3 days and at 7 days after
nerve injury until one month post-surgery. In addition, we monitored animal nociceptivc
response following nerve constriction to détermine the corrélation between the
development of neuropathic pain and the génération of new glial cell population.

36
2.4 MATERIALS AND METHODS
Animais
Adult maie Sprague-Dawley rats (Charles River, Québec, Canada) were used and
weighed 170-200g (post natal day > 45) at the time of surgery. Prior to surgery, they
were acclimated to standard laboratory conditions (14-h light, 10-h dark cycle) and given
free access to rat chow and water. Ail protocols were performed in accordance with
guidelines from the Canadian Council on Animal Care and were approved by Laval
University Animal Care committee.
Peripheral nerve injury
Rats were anaesthetized with a mixture of ketamine and xylazine (100 mg/kg
intraperitoneally). The left common sciatic nerve was exposed via blunt dissection
through the biceps femoris muscle. The nerve was isolated from surrounding connective
tissue using glass probes. Approximately 4-6 mm of the nerve was elevated minimally
and held in place using a sterilized glass probe to place a 2 mm section of split PE-60
polyethylene tubing (Intramedic PE-60, fisher Scientific Ltd, Montréal, Québec) around
the nerve. The muscle and skin layers were closed under aseptic conditions (Mosconi
and Kruger 1996). Sham-operated rats underwent the same surgical procédure as
described above but without implantation of the polyethylene tubing.
BrdU injection paradigms:
The thymidine analog bromodeoxyuridine (BrdU) was used to label proliferating
cells in the spinal cord after sciatic nerve injury.

37
Experiment 1: To détermine temporal and spatial profile of cell prolifération in
the lumbar spinal cord following sciatic nerve injury, animais were given
intraperitoneally a single dose of BrdU (100 mg/kg, 20 mg/ml in 0.007 N NaOH/0.9%
NaCl) at day 1, day 3, day 7, day 14 and day 61 after injury (n=6 per group). Three naïve
rats and two sham-operated rats each for day 3 and day 7 were included in the analysis.
Animais were perfused two hours after BrdU injection for histological analysis.
Experiment 2: To détermine the fate of cells newly generated at day 3 post-
injury, rats were injected with BrdU (100 mg/kg) at day 3 and perfused at day 7, day 14
or day 29 post-injury (n=6 per group).
Experiment 3: To détermine the fate of cells incorporated BrdU at day 7 post-
injury, rats were injected with BrdU (100 mg/kg) at day 7 and perfused at day 14 post-
injury (n=6 per group).
Tissue préparation
Rats were deeply anaesthetized with ketamine/xylazine, and then perfused
transcardially with 0.9% saline, followed by 4% paraformaldehyde (PFA) in 0.1 M
sodium phosphate buffer (pH 7.4). The lumbar spinal cords were removed (some
cervical spinal cords were also collected to serve as control) and placed in the same
fixative overnight, then transferred to 30% sucrose for cryoprotection. Frozen spinal
cords were eut transversely into 30-|0,m-thick sections on a sliding microtome, collected
in an anti-freeze solution [0.05M sodium phosphate buffer (pH 7.3) containing 30%
ethylene glycol and 20% glycerol] and stored at -20°C until use.

38
Multiple immunofluorescent labelling
To label cells incorporated with BrdU, free-floating sections were pretreated with
50% formamide in 2x standard saline citrate (SSC) for 2h at 65°C; followed by 15 min in
2x SSC at room température, 30 min in 2N HCl at 37°C, 10 min in 0.1 M borate buffer
and three times rinses in Tris-buffered saline (TBS), pH 7.6, at room température. Non
spécifie labelling was blocked with TBS + 0.25% Triton X-100, 1% BSA and 3% normal
goat sérum for lh. A monoclonal goat anti-rat antibody against BrdU (1:250, Accurate
Chemicals, Westbury, NY) was incubated with tissue sections for 48h at 4°C. After
primary antibody incubation, sections were rinsed in TBS and incubated in Alexa 488-
conjugated goat anti-rat IgG (in TBS containing 0.25% Triton X-100, 1% BSA and 3%
normal goat sérum, 1:250; Molecular Probes, Eugène, OR) for lh. After rinses in TBS,
sections were mounted onlo slides and coverslipped with Vectashield Mounting médium
(Vector Lab, Burlingame, CA).
To identify the phenotypes and the fate of newly born cells, double fluorescent-
immunolabeling was performed, combining BrdU labelling with one of the cell spécifie
phenotypic markers listed below. Sections were pretreated with 50% formamide and HCl
as described above and incubated with BrdU antibody mixed with one of the following
antibodies at 4°C for 48 h: mouse anti-neuron-specific nuclear protein (NeuN)
monoclonal antibody (for neurons, 1:1000; Chemicon, Temecula, CA), rabbit anti-Iba-1
polyclonal antibody (ionizing calcium-binding adaptor molécule, for microglia and
macrophages, 1:1000; Wako, Richmond, VA), rabbit anti-glial fibrillary acid protein
(GFAP) polyclonal antibody (for astrocytes, 1:1000; Dako, Carpinteria, CA), rabbit anti-
NG2 polyclonal antibody (chondroitin sulphate proteoglycan, for oligodendrocyte

39
progenitors and macrophages, 1:250; Chemicon, Temecula, CA). Sections were
developed using a mixture of Alexa 488-conjugated goat anti-rat IgG and Alexa 594-
conjugated goat anti-rabbit or goat anti-mouse IgG. Double labelling of OX-42 (1:1000;
Cedarlane, Burlington, ON) with NG2 (1:500) was also conducted to verify the
expression of NG2 in macrophage/microglial cells.
Image processing and quantitative analysis:
Single or multiple immunofluorescent images were acquired and quantified using
an Olympus microscope (AX-70) equipped with a Spot Caméra or a Zeiss LSM 510
confocal laser-scanning microscope. Images were processed, cropped and optimized in
Photoshop 7.0 by making minor adjustments and arranged in montage.
Quantification of proliferating cells: The total number of BrdU labeled cells was
quantified in the lumbar spinal cord using stereological methods. The gray matter in four
régions [dorsal horn (DH)-ipsi, DH-contra, ventral horn (VH)-ipsi, and VH-contra] of
lumbar spinal cord (at the level of L4-L6) was examined and quantified (5-6
sections/animal, 3-4 animals/group). BrdU nuclei exhibited punctuate staining in part of
the nucleus were excluded from the study. Only uniformly BrdU labeled nuclei were
considered for quantification. The complète cell nucleus was followed through the z-
axis and a defined volume (460|xm x 460 |xm x 15|xm) was used for BrdU positive cell
counting. Cell density per région was then extrapolated to the number of cells per cubic
millimeter.
Quantification of double labelling of BrdU and phenotypic cell markers: The
specificity of each label was first verified using single-channel scans that were then

40
merged into multiple channel-views. To confirm double-labeling, confocal Z-stacks were
generated at 1 |im intervais and visualized in three dimensional orthogonal planes. Only
a well-defined BrdU-labeled nucleus associated with a well-circumscribed,
immunopositive cell body was considered as a proliferating cell with a particular
phenotype. For quantification, sections were scanned using 488 and 594 dual-laser
channels. BrdU single-labeled cells and cells double-labelled for BrdU and another
spécifie marker, were recorded at 20x magnification. The quantification of double
labelled cells was conducted in the same defined volume (460(im x 460 jam x 15|im) as
for BrdU single labelled cells in the four différent régions described above.
Nociceptive behavior assessment:
The hind paw (ipsilateral and contralateral to the site of nerve injury) withdrawal
threshold to mechanical stimulus was measured using von Frey hairs. Rats were placed
on a rack with a mesh bottom which permitted easy access to the plantar surface of the
paws. The animais were given 30 minutes to acclimatize prior to testing. The filaments
were applied to the mid-plantar région of the left hind paw, perpendicular to the plantar
surface, with sufficient force to cause a slight buckling against the paw, and held in place
for approximately 6-8 seconds. A positive response was recorded if the paw was sharply
withdrawn. A séries of 8 von Frey filaments of logarithmically incrémental stiffness
(0.41 to 15.14 grams) (Stoelting) were applied in either ascending or descending order as
necessary to détermine the response threshold (Chaplan, Bach et al. 1994). Based on the
response pattern and the force of the final filament, the 50% response threshold was
calculated using Dixon's "up-down" method (Dixon 1980).

41
Thermal sensitivity was assessed by measuring paw withdrawal latencies to a
radiant heat stimulus using the Hargreaves apparatus (IITC Life Sciences, Woodland
Hills, CA) (Hargreaves, Dubner et al. 1988). Rats were placed within a plastic
compartment atop a warm tempered glass surface kept at a constant température and a
light beam (65% intensity) beneath the surface was aimed at the skin of the flat part of
the heel. The time to remove the paw was recorded as the withdrawal latency (seconds).
A cut-off latency of 20 seconds was imposed to prevent tissue damage.
Statistical analysis:
Ail data are presented as mean ± SEM. Significance was determined using (1)
one-way ANOVA followed by Dunnett's post hoc analysis for the temporal profile of
cell prolifération in the DH and in the VH respectively, in Fig. 1B; (2) paired student's t-
tests for the différences of cell numbers between ipsi- and contralateral side in the DH or
in the VH, respectively, in Fig. 2B; (3) repeated measures ANOVA followed by
Dunnett's post hoc for behavioral analysis in Fig 6; P was considered significant at <
0.05.

42
2.5 RESULTS
Survey of cell prolifération in the lumbar spinal cord following peripheral nerve
injury
Cell prolifération was determined by BrdU incorporation into DNA of the cells
undergoing S-phase. We injected a single dose of BrdU into animais at différent time
points post-injury (day 1-day 61). Animais were perfused at 2 hours post-injection
(experiment 1). The 2 hr post-injection time point labels cells that are undergoing DNA
replication but do not hâve time to migrate and differentiate. In naïve lumbar spinal
cords and cervical spinal cords of sciatic nerve injured rats, few sparse BrdU labeled cells
were found within the parenchyma. In sham-operated lumbar spinal cord, only at early
stage, e.g. day 3 post-injury, there was a slight, non-significant increase of BrdU positive
cells on the ipsilateral side to compare with that in the contralateral side (Fig. 1 A).
Chronic constriction of the left sciatic nerve resulted in vast numbers of newly
dividing cells on the ipsilateral side of lumber spinal cord (Fig. 1). Cell prolifération was
minimum on day 1 post-injury, peaked on day 3 with a mean of 15368 ± 826/mm3 cells
in the DH and 7888 ± 712/mm3 cells in the VH (24 fold and 11 fold increases,
respectively, compared to intact rat). This increase of BrdU labeled cells was
substantially decreased afterwards, to a mean of 3982 ± 654/mm3 cells in the DH and
4208 ± 262/mm3 cells in the VH at day 7; and 1841 ± 175/mm3 cells in the DH and 2031
± 232/mm3 cells in the VH at day 14. There was a return to basai levels (703 ± 74/mm3
cells in the DH and 685 ± 73/mnr cells in the VH) two months after nerve lésion (day
61). The left sciatic nerve injury induced an increase in cell prolifération on the

43
contralateral side of lumbar spinal cord, but this was much less intense than that on the
ipsilateral side, and not statistically significant when compared to intact rat (Fig. 1).
To identify the phenotypes of thèse newly generated cells on day 3, cellular
double-labeling was conducted with différent cellular markers; colocalization was always
verified by thin-plane (I |im) confocal microscopy in x, y, z planes. NeuN
immunoreactivity was used to assess the number of dividing neurons. Despite the high
density of BrdU labeled cells in the ipsilateral DH and VH lumbar spinal cord at day 3, a
careful search for BrdU and NeuN colocalization yielded no association of thèse two
markers (Fig. 2A). Therefore, no évidence for neurogenesis could be found in the lumbar
spinal cord following peripheral nerve injury.

Figure II. 1
44
naïve dl d3 d7 d14 1I61 Time posMnjury(days)
Figure 1.
Fig.lA. Représentative examples of BrdU labelling in spinal cord at différent time points after nerve injury. A single dose of BrdU (100 mg/kg) was administrated at day 1, day 3, day 7, day 14 and day 61 post-injury and rats were perfused two hours post-injection. Comparisons were made between naïve rats, sham-operated rats, and nerve-injured rats, in addition to the cervical spinal cord where only sparse BrdU labelling was observed. The increase of BrdU labelled cells was found at ail time points post-injury with a peak at day 3. Peripheral nerve injury-induced spinal cord cell prolifération was restricted to the ipsilateral side in both dorsal and ventral horns (DH and VH). The proliferating cell density in the DH is higher than that in the VH at day 3. (Scale bar = 1mm) Fig.lB. A quantitative analysis of BrdU labelling demonstrated that peripheral nerve injury-induced spinal cord cell prolifération on the ipsilateral side peaked (both DH and VH) at day 3 and declined thereafter (***P<0.001, **<P<0.01, *P<0.05 compared to their respective counterparts in naïve rats). Note that at day 3 significantly more cells were présent in the ipsi-DH (16316 cells/mm ) than in the ipsi-VH (8879 cells/mm3). Data are means ± SEM.

45
A large portion of BrdU labeling was associated with the microglial marker, Iba-1. Three
days after injury, many reactive microglia in the ipsilateral DH and VH were found
colocalized with BrdU+ nuclei (Fig. 2A), Iba-1 co-labeling was found in 72% of the total
BrdU+ cells in the ipsilateral DH and 59% in the ipsilateral VH. There were 7 fold and 6
fold increases in the DH-ipsi and the VH-ipsi, respectively, relative to the DH-contra and
the VH-contra counts (Fig. 2B).
The présence of glial progenitor cells was determined by colocalization with the
proteoglycan marker NG2. NG2 was expressed by some BrdU-incorporating cells in ail
four examined régions, 4 times more in the ipsi-DH than in the contra-DH, and 2.5 times
more in the ipsi-VH than in the contra-VH. BrdU-positive cells co-labeled with GFAP
were found in ail four régions, 3 and 1.5 times more in the ipsi-DH and ipsi-VH relative
to the contralateral quadrants. Thus, spinal cord microglia manifested the most
prominent proliferative response, followed by NG2 positive progenitors, whereas the
reaction of astrocytes was relatively minor (Fig.2A and 2B).

46
Figure II.2
NeuN/Bi GFAP/Bi NG2/Bi Iba-l/Bi
DU
VH
B „ IttOOOi * * * E 1600» M 14000-| 12000-•e 10000-3 8000 1 6000 3 40O0
20O0 0
■ DH-ipsi ■ DH-contra a VH-ipsi o VH-contra
BrdU> iba-1+/BidU+ NG2+/BrdLK OFAP+/BrdU<
Figure 2.
Fig. 2A. Différent cellular markers (NeuN, GFAP, NG2 and Iba-l ) were used to identify the phenotypes of dividing cells at day 3 post-injury in the ipsi-DH and ipsi-VH. For both DH and VH, none of NeuN+ neurons were found colocalized with BrdU+ nuclei. Only rare cells were double labelled for BrdU and GFAP. Few BrdU+ nuclei were found within the NG2 producing cells. The majority of BrdU labelled cells were Iba-l+
microglia. (Scale bar=100|lm) Fig. 2B. A quantitative analysis of BrdU labelling and colocalization with différent cellular markers at day 3 post-injury. Note that in response to peripheral nerve injury, spinal cord microglia manifested the most prominent proliferative response, followed by NG2 positive progenitors, whereas the reaction of astrocytes was relatively minor. Note also that at day 3 the cell prolifération rate is higher in the DH than in the VH. Data are means ±SEM. (***P<0.00l, **<P<0.01, *P<0.05 compared to their respective contralateral sides).

47
Chronic fate of cells incorporating BrdU at day 3 and at day 7 post-injury
The chronic fate of cells dividing at day 3 post-injury was determined by
administrating BrdU on day 3 after surgery, and perfusing the animais at day 7, day 14
and day 29 (experiment 2). Using immunohistochemistry, the tissue was analyzed for
BrdU+ cells and for cells double-labeled with BrdU and Iba-1, NG2, or GFAP.
As in experiment 1, we found a large increase of BrdU-labeled cells in the ipsi-
DH, on day 3 (15368 ± 826/mm3) post-injury. This increase remained relatively stable
until day 7 (14600 ± 785/mm3), then doubled by day 14 (27390 ± 1160/mm3), and
declined rapidly (12490 ± 2026/mm3) at day 29. In the ipsi-VH, newly generated cells
on day 3 (7888 ± 712/mm3) continued to divide over time and peaked at day 14 (28740 ±
1994/mm3), then rapidly decreased (8150 ± 742/mm3) at day 29. In the contra-DH and
contra-VH, there was a slight increase of BrdU positive cells at day 7 and day 14 (larger
on day 7), with a return to the day 3 level by day 29 (Fig. 3).

48
Figure II.3
DH-ipsilateral side
%
.'.::: i<: M >
day 3 day? day 14 day29
Time post-injury (day)
VH-ipsilatoral side
30000
£ 25000
. ' : : : : : : ; i
2 15000
K::::HÎ
!::::KI
day 3 day7 dayt4 day29
Time post-injury {day)
È E
S r r
ai o
E F
Q) S E n C
S
DH-contralateral side
30000 /
25000J
20000■
15000
10000
5000 9 0 9 9/
aGFAP+.'BrdU+ □ NG2+/BrdU* niba-1*/BrdU+ Nlln n-
day 3 day7 day 14 day29
Time post-injury (day)
VH-con t ra la te ra l s ide
30000
25000-
20000
15000
10000
5000- 99 mm.. day 3 day7 day14 day29
Time post-irijury(day)
Figure 3.
Fig. 3. Density (cells numbers per mm ) of total BrdU labeled-cells, BrdU labeled-GFAP+ cells, BrdU labelled-NG2+ cells and BrdU labelled Iba-l+ cells in four régions of lumbar spinal cord. BrdU was administrated once at day 3 post-sciatic nerve injury and animais were killed at day 3, day 7, day 14 and day 29 post-injury. Cells incorporating BrdU at day 3 continued to divide and to differentiate. Cell division peaked at day 14. The prédominant phenotype of newly generated cells is Iba-1+ microglia at ail time points examined. GFAP-labeled dividing astrocytes were a minor population with a slight increase over time. The increase of NG2+ dividing cells was transient; it declined sharply after the peak at day 14.

49
At ail time points examined, the dominant phenotype of newly generated cells
was always Iba-1 positive microglia (Fig. 3). As we demonstrated in our previous report
(Zhang and De Koninck 2006) with OX-42 staining, at day 7 and day 14 post-nerve
injury Iba-1 positive microglia were dramatically increased in the ipsilateral lurnbar
spinal cord (Fig. 4A). Double labeling of BrdU with Iba-1 was verified by rotating cells
in orthogonal planes (Fig.4B) and by z-stack (1 |im intervais) analysis (Fig. 4C),
indicating that the colocalization of BrdU and Iba-1 was not, instead, two closely
apposed, single labeled cells. As demonstrated in Fig.4D-4E, activated microglial cells
had extensive cytoplasm and short processes, and some were located in perineuronal
positions. Among thèse activated microglia, a significant proportion were newly formed
(evidenced by colocalization with BrdU+ nuclei) and represented 60% of ail Iba-1
labeled cells in the ipsi- DH (Fig. 4D) and 65% in the ipsi- VH (Fig. 4E).
To a lesser extent, NG2 was expressed by BrdU incorporating cells (Fig. 5A).
Both in the ipsi-DH and the ipsi-VH, NG2/BrdU expressing cells tended to increase in
number from day 3 to day 14, and were significantly reduced during the later stage (day
29). On the contralateral side, the number of NG2/BrdU expressing cells was relatively
stable, except a temporary increase on day 7 (Fig. 3). No statistically significant up-
regulation of NG2 expression was observed on the ipsilateral side versus the contralateral
side (data not shown). Most NG2+ cells displayed a complex, highly branched
morphology (Fig. 5B, small arrow). A few NG2+ cells with elongated cell bodies were
found on the ipsilateral side; they were co-labeled with the macrophage/microglia
marker, OX-42 (Fig. 5B). Thus the NG2/BrdU positive population may hâve included
macrophages/microglia.

Figure II.4
50
BrdU lba-1/BrdU
»!■ H BRI
Figure 4.
Fig. 4. BrdU colocalization with microglial marker Iba-l. 4A: Microglial activation in the lumbar spinal cord 14 days after sciatic nerve lésion. Note the robust increase of Iba-1 immunoreactivity in the ipsilateral DH and VH. 4B: Confocal images of two cells in the ipsilateral DH double labelled with Iba-1 (red cytoplasmic stain) and BrdU (green nucleus stain) rotated in orthogonal planes (x,y,z) and, 4C: z-sectioned to verify double-labeling throughout its extent. A large portion of activated microglia in the ipsi-DH (D) and the ipsi-VH (E) are indeed newly generated microglia as they colocalized with BrdU+ nuclei. The rats were perfused 14 days after injury (11 days after BrdU injection). Scale bars: 1 mm in A; 10 |xm in B and C, 200 |im in D and E.

51
GFAP-labeled astrocytes comprised a relatively small population of cells that
were incorporated with BrdU within gray matter at day 3 (911 ± 182/mm3 in the DH and
577 ± 78/mm3 in the VH), however, the number of GFAP/BrdU expressing cells
increased progressively over time on the ipsilateral side, reaching 3150 ± 520/mm3 cells
in the DH and 3290 ± 478/mm3 cells in the VH at day 14; this increase was sustained
until at least day 29 (Fig. 3).
As the number of BrdU labeled cells at day 7 post-injury was also significantly
increased (Fig. IB), we equally verified the fate of thèse cells born at 7 days post-injury
(experiment 3). In contrast to what we observed at day 3 post-injury where newly
generated cells continued to divide and peaked at day 14 (Fig 3), the number of cells
incorporated BrdU at day 7 slightly decreased after one week (day 14 post-injury), from
3982 ± 654/mm3 to 2484 ± 339/mm3 in the DH and 4208 ± 262/mm3 to 2668 ± 402/mm3
in the VH, ispilateral side to the injury, whereas microglia always predominated: 64% -
57% (day 7-day 14), followed by oligodendrocyte progenitors: 11 % - 35% (day 7-day 14)
and astrocytes: 11% - 18% (day 7-day 14) in the DH; and 57% - 73% (day 7-day 14),
followed by oligodendrocyte progenitors: 25% - 26% (day 7-day 14) and astrocytes: 14%
- 9% (day 7-day 14) in the VH.
Relationship between nociceptive response and microglial cell prolifération
following peripheral nerve injury:
Von Frey threshoJds for contralateral hind paws did not vary over a prolonged
testing period. In contrast, nerve injured rats showed a significant decrease in mechanical
threshold on the ipsilateral side, starting from 4 days after surgery, 5.69 ± 0.84 g

52
compared to 14.5 ± 0.5 g before surgery (baseline). Thresholds continued to décline,
reaching 2.12 ± 0.33 g on day 12 and this persisted until the last time point tested, 25
days (data not shown) after the implantation of polyethylene tube (Fig. 6A). Nociceptive
withdrawal latencies to noxious heat for the ipsilateral paw of nerve injured rats also
decreased shortly after the lésion: 15 ± 0.34 seconds before surgery (baseline) to 9.7 ±
2.08 seconds at d3, and 8.9 ± 2.1 seconds at d5, and this persisted for the entire 2 weeks
of testing (Fig. 6B).
To compare the relationship of nociceptive response to the spinal microglial cell
prolifération induced by peripheral nerve injury, by adding up the lba-l+/BrdU+ cells
derived from microglia originally born at day 3 and at day 7, we observed that the massif
increase of newly formed microglia at day 3 corresponds to the initiation of both
mechanical allodynia and thermal hyperalgesia, and the second burst of this cell
population at day 14 matches the time point where mechanical allodynia reached its
lowest level around two weeks after injury (Fig 6C).

53
Figure II.5
N
/
A
BrdU
\
/
/BrdU
/
M ^^^^^ mmmmÊmm
j BrdU /B
C " _ mm _
Figure 5.
Fig. 5. Confocal laser scanning microscope images showing colocalization of NG2 and GFAP with BrdU+ cells at 14 days after nerve injury (11 days after BrdU injection). A. Two NG2 producing cells double labelled with BrdU in the ipsi-DH. B. The population of newly generated NG2+ cells represents oligodendrocytes progenitors, but some could be activated microglia/macrophages because a few NG2+ cells colocalized with OX-42 (arrowhead), a macrophages/microglia marker. *: motor neurons in the VH. The majority of NG2+ cells exhibited multipolar, stellate morphologies resembling normal oligodendrocyte progenitors (small arrow). C. An astrocyte double-labeled with BrdU and GFAP (arrow). Scale bars = 10 |im in A and C, 100 |im in B.

Figure II.6
.vl
C n 25000
E | 20000
E c 15000
1 + 10000
3 ■p Ç 5000 i— râ ^ n
-Ipsilateral
-contralaleral
□ derived from cells born on d3
O derived from cells born on d7
Ipsl Ipsl
I contra
2 4 6 8 10 12 14
Time post-injury (days)
Figure 6.
Fig. 6. Time course of mechanical allodynia (A) and thermal hyperalgesia (B) in the ipsilateral and contralateral hind paws of nerve-injured rats determined by paw withdrawal threshold to calibrated Von Frey hair stimulation and paw withdrawal latency to noxious heat, respectively. In the contralateral side, withdrawal thresholds to mechanical stimuli and to heat stimuli did not change over the testing period. Both nociceptive responses in injured-animal ipsilateral hind paws (n=6) were significantly reduced, starting from d3 onwards (** P<0.01, *<0.05 from baseline). C. Temporal profile of microglial prolifération in the spinal cord dorsal horn induced by sciatic nerve injury.

55
2.6 DISCUSSION
Our findings indicate that a proliferative burst of glial cells occurs in the
ipsilateral dorsal horn and ventral horn following peripheral nerve injury. The majority
of the dividing cells were microglia, and thèse newly generated cells continued to divide
for at least two weeks. Proliferating microglia were the prédominant phenotype at ail
time points examined. The time course of microglia prolifération closely correlated with
the development of neuropathic pain, which suggests the prolifération of microglia may
hâve a rôle in the pathogenesis of pain hypersensitivity.
Spinal cord injury (SCI) causes not only neuronal loss, but also the death of
approximately 50% of the astrocytes and oligodendrocytes in the spared white matter
adjacent to the site of injury (Grossman, Rosenberg et al. 2001). Ependymal cells and
non-ependymal cells proliferate in injured spinal cord and the dividing cell population
differentiates into oligodendrocytes and astrocytes that migrate toward the injury site and
contribute to the formation of scar tissue over a period of several weeks (Johansson,
Momma et al. 1999;Yamamoto, Yamamoto et al. 2001). In several différent spinal cord
injury models, a significant increase of the BrdU-incorporating cells in the border zone of
the lésion has been observed over 24 hours to one week post-injury (McTigue, Wei et al.
2()0l;Zai and Wrathall 2005). The most abundant phenotype was reactive to NG2, a
chondroitin sulfate proteoglycan found on the surface of oligodendrocyte progenitors
(Dawson, Levine et al. 2000;Jones, Yamaguchi et al. 2002). When NG2/BrdU
colocalization declined, there was an increase in the number of cells that express
oligodendrocyte markers, and to a lesser degree, astrocytes antigens (Horky, Galimi et al.
2006). Thus, direct injury to the spinal cord with a significant initial cell loss stimulâtes

56
the prolifération of glial progenitors, which participate in the repair of demyelination
lésions and the formation of scar tissue.
With a peripheral nerve injury, where there is little or no cell loss in the spinal
cord and the blood-brain barrier is physically intact, with probably a local sélective and
temporary increase of blood-spinal cord barrier permeability (Gordh, Chu et al. 2006), we
also identified a strong and rapid stimulation of cell prolifération in both ipsi-DH and
VH. This proliferative response consisted of a striking increase in microglial cells, which
is contrast to what is seen after a direct injury to the spinal cord. Our results extend and
confirm previous observations (Liu, Rudin et al. 2000;Narita, Yoshida et al. 2006) and
add a detailed description of the spatial and temporal pattern of cell prolifération. Thèse
observations suggest that peripheral nerve injury induces a microglia-mediated
neuroinflammatory response within the DH and the VH of the spinal cord. There exist
common motor and sensory neuronal "signais" in the médiation of microglial cell
prolifération induced by peripheral nerve injury, although the intensity and temporal
profile of glial reaction from DH and VH are différent. The proliferative response in the
DH was much stronger than that in the VH at day 3. In the DH, the response was stable
until day 7 and then BrdU+ cells doubled in number at day 14, which suggests that there
were two bursts of prolifération. In contrast, prolifération in the VH progressively
increased and reached a peak at day 14. Thèse phenomena suggested that the release of
neuron-glial signaling molécules from primary afférents in the DH and from motor
neuron cell bodies in the VH might be in a différent pattern.
We also observed a moderate and progressive prolifération of NG2+ progenitors,
which could mature into oligodendrocytes, and a limited astrocyte prolifération. Synergy

57
between immune cells, such as microglia in the CNS, and adult glial progenitor cells may
promote functional recovery from CNS injury (Ziv, Avidan et al. 2006). None of the
BrdU+ cells in our study expressed neuronal markers. This finding is consistent with
previous studies showing that the spinal cord is not a neurogenic région in either the
injured or uninjured state (Horner, Power et al. 2000;Yamamoto, Yamamoto, Kitamura,
Nakamura, and Nakafuku 2001).
Induction of prolifération is one of the first steps in the activation of microglia,
and it has been well documented in vivo, in models of Alzheimer's disease, multiple
sclerosis and CNS trauma (Gehrmann, Schoen et al. 1991;Matsumoto, Ohmori et al.
1992;Chao, Hu et al. 1994). Our results provided a well-defined spatial and temporal
profile of microglial prolifération in the spinal cord following sciatic nerve injury. The
signais that induce microglial prolifération in response to nerve injury hâve remained
elusive. Granulocyte-macrophage colony-stimulating factor (GM-CSF) is a growth
factor that stimulâtes the prolifération and maturation of myeloid progenitors, giving rise
to neutrophils, monocytes and macrophages. One study has shown that facial nerve
axotomy increases GM-CSF binding to areas of neurodegeneration, indicating an
increase in the number of receptors. This increase temporally coincides with microglial
activation in the area of neurodegeneration (Raivich, Gehrmann et al. 1991). Likewise,
studies using cultured microglia hâve shown that GM-CSF induces prolifération of
microglia, both of neonatal and adult origins (Suzumura, Sawada et al. 1990;Lee, Liu et
al. 1994). A récent study revealed that prolifération of microglia can be stimulated by
several proinflammatory mediators, such as IL-1(3 and TNF-oc, that are able to directly
stimulate microglial NADPH oxidase, leading to subséquent hydrogen peroxide

58
production, which acts as a mitogenic signal for microglia (Mander and Brown 2005).
Jak/STAT and MAP kinase pathways are known to be important in controlling cellular
prolifération. Drugs that block thèse pathways may become tools to control
inflammation in the CNS by limiting microglial prolifération (Liva, Kahn et al. 1999).
Rapid microglial prolifération in the spinal cord following peripheral nerve injury
leads us to speculate on its functional significance. The development of mechanical
allodynia and thermal hyperalgesia is characteristic of the animal model used hère
(Mosconi and Kruger 1996). Récent findings highlight the active participation of glial
cells in the initiation and/or maintenance of chronic pain in différent pathological
conditions. The fact that peripheral nerve injury can induce spinal microglial/astrocytic
activation has been demonstrated in several chronic neuropathic pain models (Colburn,
Rickman, and DeLeo 1999;Fu, Light, Matsushima, and Maixner 1999;Zhang, Hoffert,
Vu, Groblewski, Ahmad, and O'Donnell 2003). Récent study also showed that a majority
of activated microglia was found within the territory occupied by peripherally
axotomised primary afférents with some of spread into "spared" régions (Beggs and
Salter 2006) Activated microglia release pain-enhancing substances such as pro-
inflammatory cytokines, nitric oxide (NO), prostaglandins (PGs), and excitatory amino
acids (EAA) (Hashizume, DeLeo et al. 2000), that excite spinal pain responsive neurons
either directly or indirectly, and promote the release of other transmitters that can act on
nociceptive neurons (Watkins, Milligan et al. 2003). Several drugs that disrupt glia
signalling by targeting glial activation (Raghavendra, Tanga et al. 2003;Milligan,
Twining et al. 2003), inhibiting the synthesis of cytokines (Sweitzer, Schubert et al.
2001), blocking pro-inflammatory cytokine receptors , or disrupting pro-inflammatory

59
cytokine signalling pathway with inhibitors of p38MAP kinase (Sweitzer, Medicherla et
al. 2004) hâve reduced neuropathic pain in animal models. Ail thèse data strongly
suggest that spinal cord glia are important pain modulators.
As reported hère and in our previous work (Zhang and De Koninck 2006) a
significant microglial response starts by day 3 and peaks at day 14. On day 14 post-
injury, when both the microglial response and the development of allodynia peak, over
60% of the activated microglia are newly generated cells. In contrast, the proliferative
response of astrocytes to nerve injury is characterized by a slight increase in the cell
number that continues in a moderate and progressive manner. This temporal pattern
matches the up-regulation of GFAP, which starts around day 7 and is sustained (Zhang
and De Koninck 2006). Our behavioral data showed that both paw withdrawal threshold
to mechanical stimuli and paw withdrawal latency to heat stimuli were significantly
reduced by day 3 and the hypersensitivity was maintained at least for one month. It is
thus possible that activated microglia (including the newly generated microglia) make an
important contribution to the initiation of neuropathic pain. Activated astrocytes (a minor
proportion of which were newly formed) might contribute to the maintenance of
neuropathic pain. It remains to be determined whether the dividing microglia came from
the prolifération of résident microglia and/or from the recruitment of bone marrow
derived cells.

60
2.7 ACKNOWLEDGEMENTS
Dr. Gary Bennett (McGilJ University) is gratefully acknowledged for his insight review
and helpful comments during the préparation of the manuscript. The study was supported
by Canadian Institutes for Health Research (CIHR) grant MOP-77624 to J.Z.

61
2.8 Référence List
1. Beggs,S. and Salter,M.W., Stereological and somatotopic analysis of the spinal
microglial response to peripheral nerve injury, Brain Behav.Immun., (2006).
2. Chao,C.C, Hu,S., Kravitz,F.H., Tsang,M., Anderson,W.R., and Peterson,P.K.,
Transforming growth factor-beta protects human neurons against beta-amyloid-
induced injury, Mol.Chem.Neuropathol., 23 (1994) 159-178.
3. Chaplan,S.R., Bach,F.W., Pogrel,J.W., ChungJ.M., and Yaksh,T.L„ Quantitative
assessment of tactile allodynia in the rat paw, J.Neurosci.Methods, 53 (1994) 55-63.
4. Colburn,R.W., Rickman,A.J., and DeLeoJ.A., The effect of site and type of nerve
injury on spinal glial activation and neuropathic pain behavior, Exp.Neurol., 157
(1999) 289-304.
5. Dawson,M.R., LevineJ.M., and Reynolds,R., NG2-expressing cells in the central
nervous system: are they oligodendroglial progenitors?, J.Neurosci.Res., 61 (2000)
471-479.
6. Dixon,W.J., Efficient analysis of expérimental observations,
Annu.Rev.Pharmacol.Toxicol., 20 (1980) 441-462.
7. Fu,K.Y., Light,A.R., Matsushima,G.K., and Maixner,W., Microglial reactions after
subcutaneous formalin injection into the rat hind paw, Brain Res., 825 (1999) 59-
67.

62
8. GehrmannJ., Matsumoto,Y., and Kreutzberg,G.W., Microglia: intrinsic
immuneffector cell of the brain, Brain Res.Brain Res.Rev., 20 (1995) 269-287.
9. Gehrmann,J., Schoen,S.W., and Kreutzberg,G.W., Lésion of the rat entorhinal
cortex leads to a rapid microglial reaction in the dentate gyrus. A light and électron
microscopical study, Acta Neuropathol.(Berl), 82 (1991) 442-455.
10. Gordh,T., Chu,H., and Sharma,H.S., Spinal nerve lésion alters blood-spinal cord
barrier function and activâtes astrocytes in the rat, Pain, 124 (2006) 211-221.
11. Grossman.S.D., Rosenberg,L.J., and WrathallJ.R., Temporal-spatial pattern of
acute neuronal and glial loss after spinal cord contusion, Exp.Neurol., 168 (2001)
273-282.
12. Hargreaves,K., Dubner,R., Brown,F., Flores,C, and JorisJ., A new and sensitive
method for measuring thermal nociception in cutaneous hyperalgesia, Pain, 32
(1988)77-88.
13. Hashizume,H., DeLeoJ.A., Colburn,R.W., and WeinsteinJ.N., Spinal glial
activation and cytokine expression after lumbar root injury in the rat, Spine, 25
(2000) 1206-1217.
14. Horky,L.L., Galimi,F., Gage,F.H., and Horner,PJ., Fate of endogenous
stem/progenitor cells following spinal cord injury, J.Comp Neurol., 498 (2006) 525-
538.

63
15. Horner,P.J., Power,A.E., Kempermann.G., Kuhn,H.G., Palmer,T.D., Winkler,J.,
Thal,L.J., and Gage,F.H., Prolifération and differentiation of progenitor cells
throughout the intact adult rat spinal cord, J.Neurosci., 20 (2000) 2218-2228.
16. Johansson,C.B., Momma,S., Clarke,D.L., Risling,M., Lendahl,U., and Frisen,J.,
Identification of a neural stem cell in the adult mammalian central nervous System,
Cell, 96 (1999) 25-34.
17. Jones,L.L., Yamaguchi,Y., Stallcup,W.B., and Tuszynski.M.H., NG2 is a major
chondroitin sulfate proteoglycan produced after spinal cord injury and is expressed
by macrophages and oligodendrocyte progenitors, J.Neurosci., 22 (2002) 2792-
2803.
18. Lee,S.C, Liu,W., Brosnan,C.F., and Dickson,D.W., GM-CSF promotes
prolifération of human fetal and adult microglia in primary cultures, Glia, 12 (1994)
309-318.
19. Liu,L., Rudin,M., and Kozlova,E.N., Glial cell prolifération in the spinal cord after
dorsal rhizotomy or sciatic nerve transection in the adult rat, Exp.Brain Res., 131
(2000) 64-73.
20. Liva,S.M, Kahn,M.A., Dopp,J.M., and De Vellis,J., Signal transduction pathways
induced by GM-CSF in microglia: significance in the control of prolifération, Glia,
26(1999)344-352.

64
21. Mander,P. and Brown,G.C, Activation of microglial NADPH oxidase is synergistic
with glial iNOS expression in inducing neuronal death: a dual-key mechanism of
inflammatory neurodegeneration, J.Neuroinflammation., 2 (2005) 20.
22. Matsumoto,Y., Ohmori,K., and Fujiwara,M., Microglial and astroglial reactions to
inflammatory lésions of expérimental autoimmune encephalomyelitis in the rat
central nervous System, J.Neuroimmunol., 37 (1992) 23-33.
23. McTigue,D.M., Wei,P., and Stokes,B.T., Prolifération of NG2-positive cells and
altered oligodendrocyte numbers in the contused rat spinal cord, J.Neurosci., 21
(2001)3392-3400.
24. Milligan,E.D., Twining,C, Chacur,M., Biedenkapp,J., 0'Connor,K., Poole,S.,
Tracey,K., Martin,D., Maier,S.F., and Watkins,L.R., Spinal glia and
proinflammatory cytokines médiate mirror-image neuropathic pain in rats,
J.Neurosci., 23 (2003) 1026-1040.
25. Mosconi,T. and Kruger.L., Fixed-diameter polyethylene cuffs applied to the rat
sciatic nerve induce a painful neuropathy: ultrastructural morphometric analysis of
axonal altérations, Pain, 64 (1996) 37-57.
26. Narita,M., Yoshida,T., Nakajima,M., Narita,M., Miyatake,M., Takagi.T.,
Yajima,Y., and Suzuki,T., Direct évidence for spinal cord microglia in the
development of a neuropathic pain-like state in mice, J.Neurochem., 97 (2006)
1337-1348.

65
27. Raghavendra,V., Tanga,F., and DeLeoJ.A., Inhibition of inicroglial activation
atténuâtes the development but not existing hypersensitivity in a rat model of
neuropathy, J.Pharmacol.Exp.Ther., 306 (2003) 624-630.
28. Raivich,G., GehrmannJ., and Kreutzberg,G.W., Increase of macrophage colony-
stimulating factor and granulocyte-macrophage colony-stimulating factor receptors
in the regenerating rat facial nucleus, J.Neurosci.Res., 30 (1991) 682-686.
29. Suzumura,A., Sawada.M., Yamamoto.H., and Marunouchi,T., Effects of colony
stimulating factors on isolated microglia in vitro, J.Neuroimmunol., 30 (1990) 111-
120.
30. Sweitzer,S.M., Medicherla,S., Almirez,R., Dugar,S., Chakravarty,S., ShumillaJ.A.,
Yeomans,D.C, and Protter,A.A., Antinociceptive action of a p38alpha MAPK
inhibitor, SD-282, in a diabetic neuropathy model, Pain, 109 (2004) 409-419.
31. Sweitzer.S.M., Schubert,P., and DeLeoJ.A., Propentofylline, a glial modulating
agent, exhibits antiallodynic properties in a rat model of neuropathic pain,
J.Pharmacol.Exp.Ther., 297 (2001) 1210-1217.
32. Tsuda,M., Inoue,K., and Salter.M.W., Neuropathic pain and spinal microglia: a big
problem from molécules in "small" glia, Trends Neurosci., 28 (2005) 101-107.
33. Watkins,L.R. and Maier,S.F., Beyond neurons: évidence that immune and glial cells
contribute to pathological pain states, Physiol Rev., 82 (2002) 981-1011.

66
34. Watkins,L.R., Milligan,E.D., and Maier,S.F., Glial activation: a driving force for
pathological pain, Trends Neurosci., 24 (2001) 450-455.
35. Watkins,L.R., Milligan,E.D., and Maier,S.F., Glial proinflammatory cytokines
médiate exaggerated pain states: implications for clinical pain, Adv.Exp.Med.Biol.,
521 (2003) 1-21.
36. Yamamoto,S., Yamamoto,N., Kitamura,T., Nakamura,K., and Nakafuku,M.,
Prolifération of parenchymal neural progenitors in response to injury in the adult rat
spinal cord, Exp.Neurol., 172 (2001) 115-127.
37. Zai,L.J. and WrathallJ.R., Cell prolifération and replacement following contusive
spinal cord injury, Glia, 50 (2005) 247-257.
38. Zhang,J. and De Koninck,Y., Spatial and temporal relationship between monocyte
chemoattractant protein-1 expression and spinal glial activation following
peripheral nerve injury, J.Neurochem., 97 (2006) 772-783.
39. Zhang,J., Hoffert,C, Vu,H.K., Groblewski,T., Ahmad,S., and 0'Donnell,D.,
Induction of CB2 receptor expression in the rat spinal cord of neuropathic but not
inflammatory chronic pain models, Eur.J.Neurosci., 17 (2003) 2750-2754.
40. Ziv,Y., Avidan,H., Pluchino,S., Martino,G., and Schwartz,M., Synergy between
immune cells and adult neural stem/progenitor cells promotes functional recovery
from spinal cord injury, Proc.Natl.Acad.Sci.U.S.A, 103 (2006) 13174-13179.

67
CHAPITRE III
CONCLUSIONS ET PERSPECTIVES
Depuis quelques années, les cellules gliales apparaissent comme des modulateurs
importants dans la transmission des signaux nociceptifs. En effet, lorsqu'un nerf
périphérique est endommagé (ce qui produit des réponses nociceptives anormalement
intenses), souvent les microglies et les astrocytes sont activés. Une fois « activées », les
cellules gliales relâchent une variété de substances neuroexcitatrices qui peuvent
potentialiser la transmission de douleur par les neurones. Dans le cas des glies,
l'activation est multidimensionnelle, les cellules acquièrent donc de multiples nouvelles
caractéristiques dont la prolifération et migration cellulaires. Au cours de cette étude, on
s'est intéressé à analyser la relation entre la réponse des cellules gliales à la lésion d'un
nerf périphérique et l'établissement de la douleur chronique en s'attardant surtout sur
l'étude de la gliogénèse dans la moelle épinière, en utilisant le BrdU comme marqueur de
prolifération cellulaire.
On a constaté que la lésion d'un nerf périphérique induisant un grave état neuropathique,
déclenche une augmentation du niveau de prolifération cellulaire qui atteint son sommet à
d3, dans la moelle épinière, du côté ipsilatéral à la lésion. La majorité de ces cellules en
prolifération sont des microglies activées.
• Ces cellules nouvellement générées continuent à se diviser et à se différencier au
fil du temps pour atteindre un nouveau sommet à dl4. Le phénotype prédominant
est toujours Iba-1+ marqueur de microglie.

68
• Cette forte prolifération cellulaire est cruciale dans le développement du
phénomène d'activation microglial, puisque la formation de nouvelles microglies
représente 60% du phénomène d'activation globale.
• Cette nouvelle population n'est pas seulement le fruit de la prolifération des
cellules microgliales résidentes de la moelle épinière. En fait, 20 % des cellules
nouvellement formées proviennent de la périphérie, de la division des
macrophages dérivés de la moelle osseuse qui pénètrent dans la moelle épinière
suite à la lésion, pour se transformer en microglies activées. (Annexe 1.)
• Il existe une corrélation temporelle et spatiale importante entre la prolifération des
cellules microgliales de la moelle épinière dans la corne dorsale, et les réponses
nociceptives induites par la lésion du nerf sciatique. Ce qui suggère la
contribution potentielle de ces nouvelles microglies au sein du processus
d'activation microgliale global, critique dans les états de douleur neuropathique.
Somme toute, les études présentées dans ce mémoire apportent de nouveaux indices
concernant la dynamique des cellules gliales dans les cas de douleur neuropathique. La
protéine MCP-1 semble être un déclencheur important de l'activation microgliale et du
chimiotactisme qui provoque l'infiltration de cellules dérivées de la moelle osseuse dans
la moelle épinière. Et la forte prolifération cellulaire, propriété des cellules résidentes et
des cellules provenant de la périphérie, apporte une contribution majeure au phénomène
d'activation dans la moelle épinière. (Figure. III. 1).

69
Lésion périphérique M H M H M Ganglions rachidiens "T MCP-1
Activation microgliale
Infiltration, transformation
Transformation Prolifération prolifération delamicroglie de la microglie de dérivées de la résidente résidente moelle osseuse
Figure III.l. Les composantes de l'activation microgliale. Le mot transformation
fait référence aux changements cellulaires autres que la prolifération.
Les hypothèses présentées dans cette étude ouvrent différentes avenues intéressantes. En
effet, dans le cadre de l'activation giiale après une lésion périphérique on commence à
peine à s'intéresser aux mécanismes cellulaires et moléculaires impliqués dans tout ce
processus; et spécialement les mécanismes modulant la prolifération des microglies (et
des cellules gliales en général) dans la moelle épinière intacte, sont méconnus. Il est donc
pertinent de concentrer nos efforts dans cette direction.
Tout d'abord, l'utilisation d'inhibiteurs du cycle cellulaire tels que l'ara-C (cytosine
arabinoside) (Mansour et al. 1995), nous permettraient de mieux élucider l'implication au
niveau fonctionnel de la prolifération cellulaire. En injectant ce composant de façon
intrathécale et systémique, il serait possible de différencier les contributions relatives des

70
deux populations en prolifération : les macrophages et les cellules gliales. De la même
façon, l'exploration des effets cellulaire et systémiques (comportement neuropathique)
induits par des modulateurs de la prolifération cellulaires tels que le TGF-P
(Transforming growth factor-p1), connu pour être un agent anti-inflammatoire et anti
prolifération important (Kitisin et al. 2007); et le GM-CSF (granulocyte-macrophage
colony-stimulating factor) une cytokine qui fomente la prolifération de macrophages in
vitro (Lee et al. 1994), pourrait nous apporter des nouvelles pistes en ce qui concerne les
mécanismes cellulaires sous-jacents à la prolifération cellulaire, critique dans l'activation
gliale qui accompagne la douleur neuropathique.
Les cellules gliales révolutionnent tout ce que l'on connaît sur le système nerveux, et sont
maintenant perçues comme des modulateurs importants de l'homéostasie neuronale,
pouvant être impliquées dans beaucoup de pathologies affectant le système nerveux. La
douleur neuropathique n'en est pas l'exception, mais au fur et à mesure qu'on élargit nos
connaissances sur l'activation gliale et sur la biologie gliale en général, de nouveaux
horizons thérapeutiques plus prometteurs s'ouvrent à nous.

71
Bibliographie:
1. Abbadie, C. et al. Impaired neuropathic pain responses in mice lacking the
chemokine receptor CCR2. Proc. Natl Acad. Sci. USA 100, 7947-7952 (2003)
2. Albe-Fessard, D., La douleur. Paris: Masson. (1996)
3. Alice Meunier, Joao Braz, François Cesselin, Michel Hamon, Michel Pohl.
Inflammation et douleur: thérapie génique expérimentale. Médecine/sciences;
20 : 325-30 M/S n° 3, vol. (2004)
4. Besson JM. Bases physiologiques de la nociception. In : Boureau F, Ed. Pratique
du traitement de la douleur. Paris : Doin ; p. 19-38. (1998)
5. Besson, J.M., et al. Physiologie de la nociception. J. Physiol. (Paris),. 78(1): p. 7-
107.(1982)
6. Boddeke, E.W. Involvement of chemokines in pain. Eur. J. Pharmacol. 429, 115-
119(2001).
7. Colburn RW, Rickman AJ, DeLeo JA. The effect of site and type of nerve injury
on spinal glial activation and neuropathic pain behavior. Exp Neurol 157:289 -
304.(1999)
8. Coull JA, Beggs S, Boudreau D, Boivin D, Tsuda M, Inoue K, Gravel C, Salter
MW, De Koninck Y. BDNF from microglia causes the shift in neuronal anion
gradient underlying neuropathic pain. Nature 438:1017-1021. (2005)

72
9. Coull JA, Boudreau D, Bachand K, Prescott SA, Nault F, Sik A, De Koninck P,
De Koninck Y. Trans-synaptic shift in anion gradient in spinal lamina I neurons
as a mechanism of neuropathic pain. Nature. 424(6951):938-42. (2003)
10. De Léo JA, Jesierski RP. The rôle of neuroinflammation and neuroimmune
activation in persistent pain. Pain; 90: 1-6. (2001)
11. Descartes R. Treatise of man. Hall TS, translator. Cambridge, MA: Harvard
University Press; (1972).
12. Echeverry S, Shi XQ, Zhang J Characterization of cell prolifération in rat spinal
cord following peripheral nerve injury and the relationship with neuropathic pain.
Pain, Doi: 10.1016. In press. (2007)
13. Fairbanks CA, Schreiber KL, Brewer KL, Yu CG, Stone LS, Kitto KF, et al.
Agmatine reverses pain induced by inflammation, neuropathy, and spinal cord
injury. Proc Natl Acad Sci USA; 97: 10584-9. (2000)
14. Fields, H.L. Pain modulation: expectation, opioid analgesia and virtual pain. Prog.
Brain Res. 122, 245-253 (2000).
15. Fu Ky, Light AR, Maixner W. Relationship between nociceptor activity,
peripheral edema, spinal microglial activation and longterm hyperalgesia induced
by formalin. Neuroscience; 101(4): 1127-35. (2000)
16. Fu Ky, Light AR, Matsushima GK, Maixner W. Microglial reactions after
subcutaneous formalin injection into the rat hind paw. Brain Res; 825: 59-67.
(1999)

73
17. Gebhart GF, Sandkuhler J, Thalhammer JG, Zimmermann M. Inhibition of spinal
nociceptive information by stimulation in midbrain of the cat is blocked by
lidocaine microinjected in nucleus raphe magnus and medullary reticular
formation. J Neurophysiol. 50:1446-59. (1983)
18. Gebhart GF. Descending modulation of pain. Neurosci Biobehav Rev.; 27:729-
37.(2004)
19. Hofbauer RK, Rainville P, Duncan GH, Bushnell MC. Cortical représentation of
the sensory dimension of pain. J Neurophysiol. 86:402-11. (2001)
20. Horky,L.L., Galimi.F., Gage,F.H., and Horner.P.J., Fate of cndogenous
stem/progenitor cells following spinal cord injury, J.Comp Neurol., 498 525-538.
(2006).
21. Horner,P.J., Power,A.E., Kempermann,G., Kuhn,H.G., Palmer,T.D., Winkler,J.,
Thal,L.J., and Gage,F.H., Prolifération and ditïerentiation of progenitor cells
throughout the intact adult rat spinal cord, J.Neurosci., 20: 2218-2228. (2000).
22. Holash JA. and Stewart, PA. The relationship of astrocyte-like cells to the vessels
that contribute to the blood ocular barriers. Brain Res. 629: 218-224. (1993).
23. Hunt, S.P. & Mantyh, P.W. The molecular dynamics of pain control. Nat. Rev.
Neurosci. 2, 83-91.(2001).
24. Julius, D. & Basbaum, A.I. Molecular mechanisms of nociception. Nature 413,
203-210(2001).
25. Kettenman H. and Ransom B.R. Neuroglia. Oxford University Press. (1995)

74
26. Kitisin K, Saha T, Blake T, Deng M, Kim C, Tang Y, Shetty K, Mishra B, and
Mishra L, TGF-beta signaling in Development. Sci, STKE (399), DOI: 10.1126
(2007).
27. Klein, M. A. et al. Impaired neuroglial activation in interleukin-6 déficient mice.
Glia 19,227-233 (1997).
28. Kondo I, Marvizon JC, Song B, Salgado F, Codeluppi S, Hua XY, Yaksh TL.
Inhibition by spinal mu- and delta-opioid agonists of afferent-evoked substance P
release. J Neurosci. 25:3651-60. (2005)
29. Lee,S.C, Liu,W., Brosnan,C.F., and Dickson,D.W., GM-CSF promotes
prolifération of human fetal and adult microglia in primary cultures, Glia, 12 309-
318.(1994)
30. Liu,L., Rudin,M., and Kozlova,E.N., Glial cell prolifération in the spinal cord
after dorsal rhizotomy or sciatic nerve transection in the adult rat, Exp.Brain Res.,
131:64-73.(2000)
31. Lynch, D. in Practical Management of Pain 3rd edn. (éd. Raj, P.P.) (1998)
32. Mansour TS, Jin H, Wang W, et al. Anti-human immunodeficiency virus and anti-
hepatitis-B virus activities and Troxacitabine in leukemia toxicities of the
enantiomers of 20-deoxy-30-oxa-40-thiocytidine and their 5-fluoro analogues in
vitro. J Med Chem.; 38:1-^1. (1995).
33. Mantyh PW, DeMaster E, Malhotra A, Ghilardi JR, Rogers SD, Mantyh CR, Liu
H, Basbaum AI, Vigna SR, Maggio JE, Simone DA. Receptor endocytosis and

75
dendrite reshaping in spinal neurons after somatosensory stimulation. Science.
268:1629-32.(1995)
34. Mantyh, P.W., Clohisy, D.R., Koltzenburg, M. & Hunt, S.P. Molecular
mechanisms of cancer pain. Nature Rev.Cancer 2, 201-209 (2002).
35. McMahon, S. B., Bennett, D. L. H. & Bevan S. in Textbook of Pain (eds
McMahon, S. B. & Koltzenburg, M.) Chapter 3 (Elsevier, London, 2006).
36. McMahon, S. B., Cafferty, W. B. & Marchand, F. Immune and glial cell factors
as pain mediators and modulators.Exp. Neurol. 192, 444-462 (2005)
37. Melzack R, Wall PD. Pain mechanisms: a new theory. Science; 150:971-9.
(1965).
38. Milligan ED, O'Connor KA, Armstrong CB, Martin D, Tracey KJ, Maier SF,
Watkins LR. Systemic administration of CNI-1493, a p 38 MAP kinase inhibitor,
blocks HIV-1 gp 120-induced enhanced pain states in rats. J Pain; 2: 326-33
(2001).
39. Milligan ED, O'Connor KA, Nguyen KT, Armstrong CB, Twining C, Gaykema
R, et al. Intrathecal HIV-1 envelope glycoprotein gp 120 enhanced pain states
mediated by spinal proinflammatory cytokines. J Neurosci; 21: 2808-19. (2001)
40. Milligan, E. D. et al. Evidence that exogenous and endogenous fractalkine can
induce spinal Nociceptive facilitation in rats. Eur. J. Neurosci. 20, 2294-2302
(2004).

76
41. Porreca F, Burgess SE, Gardell LR, Vanderah TW, Malan TP Jr, Ossipov MH,
Lappi DA, Lai J. Inhibition of neuropathic pain by sélective ablation of brainstem
medullary cells expressing the mu-opioid receptor. J Neurosci; 21:5281-8. (2001)
42. Porreca, F., Ossipov, M.H. & Gebhart, G.F. Chronic pain and medullary
descending facilitation. Trends Neurosci. 25, 319-325 (2002).
43. Reynolds DV. Surgery in the rat during electrical analgesia induced by focal brain
stimulation. Science; 164:444-5.(1969)
44. Ribeiro, R. A. et al. Involvement of résident macrophages and mast cells in the
writhing nociceptive response induced by zymosan and acetic acid in mice. Eur. J.
Pharmacol. 387, 111-118 (2000).
45. Roberts, L. & McColl, G. J. Tumor necrosis factor inhibitors: risks and benefits in
patients with rheumatoid arthritis. Intern. Med. J. 34, 687-693 (2004).
46. Rutkowski MD, Winkelstein BA, Hickey WF, Pahl JL, DeLeo JA. Lumbar nerve
root injury induces central nervous system neuroimmune activation and
neuroinflammation in the rat: relationship to painful radiculopathy. Spine;
27:1604-13.(2002)
47. Schafers, M., Svensson, C. L, Sommer, C. & Sorkin, L. S. Tumor necrosis factor-
a induces mechanical allodynia after spinal nerve ligation by activation of p38
MAPK in primary sensory neurons. J. Neurosci. 23, 2517-2521 (2003).
48. Scholz, J. & Woolf, C. J. Can we conquer pain? Nature Neurosci. 5, 1062-1067
(2002) 270-293 (2002).

77
49. Sindrup, S.H. & Jensen, T.S. Efficacy of pharmacological treatments of
neuropathic pain: an update and effect related to mechanism of drug action. Pain
83,389^100(1999).
50. Stein C. The control of pain in peripheral tissue by opioids. N Engl J Med.;
332:1685-90.(1995).
51. Svensson, CI. & Yaksh, T.L. The spinal phospholipase-cyclooxygenase-
prostanoid cascade in nociceptive processing. Annu. Rev. Pharmacol. Toxicol. 42,
553-583 (2002).
52. Sweitzer S, Martin A, De Léo JA. Intrathecal IL-1 receptor antagonist in
combination with soluble tumor necrosis factor receptor exhibits an anti-allodynic
action a rat model of neuropathic pain. Neuroscience; 103: 529-39. (2001)
53. Sweitzer SM, Hickey WF, Rutkowski MD, Pahl JL, DeLeo JA. Focal peripheral
nerve injury induces leukocyte trafficking into the central nervous System:
potential relationship to neuropathic pain. Pain; 100:163-70. (2002)
54. Sweitzer SM, Schubert P, De Léo JA. Propentofylline, a glial modulating agent,
exhibits antiallodynic properties in a rat model of neuropathic pain. J Pharmacol
ExpTher;297: 1210-7.(2001)
55. Sykova E, Chvatal A. Glial cells and volume transmission in the CNS.
Neurochem Int; 36: 397-409. (2000)
56. Tanga FY, Nutile-McMenemy N, DeLeo J A. The CNS rôle of Toll-like receptor 4
in innate neuroimmunity and painful neuropathy. Proc Natl Acad Sci USA.;
102:5856-61.(2005)

78
57. Tsuda M, Inoue K, Salter MW. Neuropathic pain and spinal microglia: a big
problem from molécules in "small" glia. Trends Neurosci. 28:101-107. (2005)
58. Tsuda, M. et al. P2X4 receptors induced in spinal microglia gâte tactile allodynia
after nerve injury. Nature 424, 778-783 (2003).
59. Tsuda, M., Mizokoshi, A., Shigemoto-Mogami, Y., Koizumi, S. & Inoue, K.
Activation of p38 mitogenactivated protein kinase in spinal hyperactive microglia
contributes to pain hypersensitivity following peripheral nerve injury. Glia 45,
89-95 (2004).
60. Verge, G. M. et al. Fractalkine (CX3CL1) and fractalkine receptor (CX3CR1)
distribution in spinal cord and dorsal root ganglia under basai and neuropathic
pain conditions. Eur. J. Neurosci. 20, 1150-1160 (2004).
61. Watkins LR, Maier SF. Implications of immune-to-brain communications for
sickness and pain. Proc Natl Acad Sci USA; 96: 7710-3. (1999).
62. Watkins LR, Maier SF. The pain of being sick: implications of immune-to-brain
communication for understanding pain. Ann Rev Psychol; 51: 29-57. (2000)
63. Watkins LR, Martin D, Ulrich P, Tracey KJ, Maier SF. Evidence for the
involvement of spinal cord glia in subcutaneous formalin induced hyperalgesia in
the rat. Pain; 71: 225-35. (1997)
64. Watkins LR, Milligan ED, Maier SF. Glial activation: a driving force for
pathological pain. TINS; 24: 450-5. (2001)
65. Watkins LR, Milligan ED, Maier SF. Spinal cord glia: new players in pain. Pain;
93:201-5.(2001)

79
66. Willis W. Hyperalgesia and allodynia. New York: Raven Press; 400 p. ( 1992)
67. Winkelstein, B. A., Rutkowski, M. D., Sweitzer, S. M., Pahl, J. L. & DeLeo, J. A.
Nerve injury proximal or distal to the DRG induces similar spinal glial activation
and sélective cytokine expression but differential behavioral responses to
pharmacologie treatment. J. Comp. Neurol. 439, 127-139 (2001).
68. Woolf, C.J. & Mannion, R.J. Neuropathic pain: aetiology, symptoms,
mechanisms, and management. Lancet 353, 1959-1964 (1999).
69. Woolf, C.J. & Max, M.B. Mechanism-based pain diagnosis: issues for analgésie
drug development. Anesthesiol. 95, 241-249 (2001). |
70. Woolf, C.J. & Salter, M.W. Neuronal plasticity—increasing the gain in pain.
Science 288, 1765-1768(2000).
71. Woolf, C.J., P. Shortland, and R.E. Coggeshall, Peripheral nerve injury triggers
central sprouting of myelinated afférents. Nature, 355(6355): p. 75-8. (1992)
72. Zhang J, De Koninck Y. Spatial and temporal relationship between monocyte
chemoattractant protein-1 expression and spinal glial activation following
peripheral nerve injury. J Neurochem 97:772-783. (2006)
73. Zhang J, Shi XQ, Echeverry S, Mogil J, De Koninck Y, Rivest S. Expression of
CCR2 in both résident and bone marrow derived microglia plays a critical rôle in
neuropathic pain. J. Neuroscience in press (2007).
74. Zigmond MJ, Bloom FE, Landis SC, Roberts JL, Squire LR. Fundamental
Neuroscience. Académie Press, Chapter 3. (1999).

80
ANNEXE I
Expression of CCR2 in Both Résident and Bone Marrow-Derived Microglia Plays a Critical Rôle in Neuropathic Pain
Ji Zhang,' Xiang Qun Shi,' Stefania Echeverry,1 Jeffrey S. Mogil,2 Yves De Koninck,1
and Serge Rivest3
'Unité de Neurobiologie Cellulaire, Centre de Recherche Université Laval Robert-Giffard, Québec, Québec, Canada GIJ 2G3, 2 Department of Psychology and The Alan Edwards Centre for Research on Pain, McGill University, Montréal, Québec, Canada and ' Laboratoire d'endocrinologie Moléculaire et Oncologique, Centre de Recherche du Centre Hospitalier de l'Université Laval, Québec, Québec, Canada.
*The Journal of Neuroscience, November 7,2007 • 27(45): 12396 -12406

12396 • The Journal of Neuroscience, November 7,2007 ■ 27(45):12396-12406
Cellular/Molecular
Expression of CCR2 in Both Résident and Bone Marrow-Derived Microglia Plays a Critical Rôle in Neuropathic Pain
Ji Zhang,1 Xiang Qun Shi,1 Stefania Echeverry,1 Jeffrey S. Mogil,2 Yves De Koninck,1 and Serge Rivest* 'Unité de Neurobiologie Cellulaire, Centre de Recherche Université Laval Robert-Giffard, Québec, Québec, Canada Gl] 2G3, ■'Department of Psychology and The Alan Edwards Centre for Research on Pain, McGill University, Montréal, Québec, Canada H3A 2T5, and 'Laboratoire d'endocrinologie Moléculaire et Ontologique, Centre de Recherche du Centre Hospitalier de l'Université Laval, Québec, Québec, Canada Gl V 4G2
Neuropathic pain resulting from damage to or dysfunction of peripheral nerves is not well understood and difficult to treat. Although CNS hyperexcitability is a critical component, récent findings challenge the neuron-centric view of neuropathic pain etiology and pathology. Indeed, glial cells were shown to play an active rôle in the initiation and maintenance of pain hypersensitivity. However, the origins of thèse cells and the triggers that induce their activation hâve yet to be elucidated. Hère we show that, after peripheral nerve injury induced by a partial ligation on the sciatic nerve, in addition to activation of microglia résident to the CNS, hematogenous macrophage/monocyte infiltrate the spinal cord, proliferate, and differentiate into microglia. Signaling from chemokine monocyte chemoattractant protein-1 (MCP-1, CCL2) to its receptor CCR2 is critical in the spinal microglial activation. Indeed, intrathecal injection of MCP-1 caused activation of microglia in wild-type but not in CCR2-deficient mice. Furthermore, treatment with an MCP-1 neutralizing antibody prevented bone marrow-derived microglia (BMDM) infiltration into the spinal cord after nerve injury. In addition, using sélective knock-out of CCR2 in résident microglia or BMDM, we found that, although total CCR2 knock-out mice did not develop microglial activation or mechanical allodynia, CCR2 expression in either résident microglia or BMDM is sufficient for the development of mechanical allodynia. Thus, to effectively relieve neuropathic pain, both CNS résident microglia and blood-borne macrophages need to be targeted. Thèse findings also open the door for a novel therapeutic strategy: to take advantage of the natural ability of bone marrow-derived cells to infiltrate selectively affected CNS régions by using thèse cells as vehicle for targeted drug delivery to inhibit hypersensitivity and chronic pain.
Key words: nerve injury; leukocyte infiltration; allodynia; spinal cord; chemokine; glial activation
Introduction The pathophysiological processes underlying the etiology of neuropathic pain involve molecular and cellular changes in neuronal plasticity and anatomical reorganization at various levels of the peripheral nervous System and CNS (Marx, 2004; Baron, 2006; Campbell and Meyer, 2006). Récent findings hâve highlighted the active involvement of glial cells in the pathogenesis of nerve injury-induced neuropathic pain and uncover new targets for potential painkilling drugs (Marchand et al., 2005; Tsuda et al., 2005).
Peripheral nerve injury induces activation of spinal microglial cells (Coyle, 1998; Colburn et al., 1999; Fu et al., 1999; Zhang et al., 2003). Activated microglia contribute to neuropathic pain syniptomology through the release of molécules that act as direct
Received May 9,2007; revised Sept. 17,2007; accepted Sept. 18,2007.
Eh s work was supporter! by a Canadian Intitules of Health research tjrant (J.Z.) and a team grant from Neuro-
seienre Canada (Brain Repair program). I.S.M. holds a Canada Research Chair in the Genetics of Pain. V.O.K is a
Chercheur National of the fonds de la Recherche en Santé du Québec. S.R. holds a Canada Research Chair in Neuro-
immunology. We thank Martine tessard for technkal assistance for the génération of the chimeric mice.
Coi respondence should be addressed to Dr. Ji 7hang at her présent address: îhe Alan Edwards Centre for Research
on Pain, McGill University, 740, Dr. Penfield Avenue, Suite 3200C, Montréal, Québec, Canada H3A 2B2. E-mail:
ji.zlialigti'mcgilUa.
X. Q. Shi's and S. Echeverry's présent address: The Alan Edwards Centre for Research on Pain, McGill University,
Montréal, Québec, Canada H3A2B2.
DOI:10.1523/JNEUROSCI.3016-07.2007
Copyright O 2007 Society for Neuroscienre 0270-6474/07/2712396-11 SI 5.00/0
modulators of neuronal excitability (Tsuda et al., 2003; Coull et al, 2005). A major question remains unanswered: where do thèse activated microglial cells corne from and is there a spécifie population involved in pain? The normal CNS is characterized by t wo major monocyte-related populations: highly ramified CNS résident microglia and hematopoietic perivascular macrophages (Raivich and Banati, 2004). The renewal of microglia in adult-hood occurs not only through the prolifération of preexisting cells but also through the recruitment of precursors that dérive from bone marrow (BM), because the perivascular macrophages replenished by circulating monocyte could migrate through basai membrane into the CNS parenchyma, a process enhanced in différent forms of inflammatory neuropathology (Streit et al., 1989; Lawson et al., 1992; Priller et al., 2001; Sweitzeret al., 2002). The relative contribution of résident and invading microglia to the pathogenesis may vary depending on the setting and severity of the injury, as is evidenced by the différent dynamics of BM-derived cell accumulation (Furuya et al., 2003; Priller et al., 2006; Solomon et al., 2006; Denker et al., 2007). An understanding of the distinct contribution of cells of the monocytic lineage in injury-induced neuropathic pain is important for directing the search for novel therapeutic targets.
Whenever neurons are injured, microglia become activated, both at the primary lésion sites and remote from primary damage, at sites where the damaged neurons project (Kreut/.berg,

Zhang et al. • Microglia and Macrophages in Neuropathic Pain J. NeuroscL, November 7,2007 • 27(45):12396-12406 • 12397
1996). Thus, microglial activation is likely to be controlled by endangered neurons. The identity of the molécules involved in neuron-microglia signaling in différent injury conditions remains an active subject of investigation. Chemokines and their receptors constitute an elaborate signaling System that plays an important rôle in cell-to-cell communication not only in the pe-ripheral immune System but also in the CNS (Ransohoff and Tani, 1998; Ambrosini and Aloisi, 2004; Moser et al., 2004; Rot and von Andrian, 2004). Monocyte chemoattractant protein-1 (MCP-1 ), also named CCL2, is a member of the CC family che-mokine that specifically attracts and activâtes monocytes to the sites of inflammation (Léonard et al., 1991). Absent in normal CNS, MCP-1 was found to be induced in facial nucleus neurons by facial nerve transection (Flugel et al., 2001), in sympathetic ganglion neurons after postganglionic axotomy (Schreiber et al., 2001 ), and in DRG sensory neurons and spinal cord motor neurons by chronic constriction of the sciatic nerve (Tanaka et al., 2004; Zhang and De Koninck, 2006). CCR2, the receptor for MCP-1, isexpressedselectivelyon cellsof monocyte/macrophage lineage in periphery (Rebenko-Moll et al., 2006) and can be induced in spinal microglia by peripheral nerve injury (Abbadie et al., 2003). We also demonstrated that, both spatially and tempo-rally, MCP-1 induction is closely correlated with the subséquent surrounding microglial activation (Zhang and De Koninck, 2006). We predicted that the induced neuronal MCP-1 could be the signaling molécule that activâtes résident spinal microglial and/or attracts peripheral macrophages into the spinal cord. Also, it could contribute to peripheral sensitization by attracting macrophages to the injured nerve and DRG. It has been demonstrated that mice lacking the CCR2 [CCR2 knock-out (KO)] had impaired nociceptive response typically associated with neurop-athy (Abbadie et al., 2003), but the exact contribution of CCR2 in résident and bone marrow-derived microglia has yet to be clearly defined.
In the présent study, we identified the origins of activated microglia by using chimeric mice in which their bone marrow was replaced by one that expresses green fluorescent protein (GFP). We show that, after peripheral nerve injury, in addition to activation of microglia résident to the spinal cord, b lood-bome macrophages hâve the ability to infiltrate the spinal cord, prolif-erate, and differentiate into activated microglia. We also showed that infiltration of peripheral macrophages into the spinal cord after nerve injury involves direct MCP-1/CCR2 signaling from the CNS to the periphery. The fact that both résident microglia and bone marrow-derived macrophages participate in the modulation of central sensitization in neuropathic pain indicates that inhibition of either résident microglia or of peripheral macrophages may not be an efficient approach to relieve neuropathic pain. Both need to be targeted.
Materials and Methods Animais Adult (7- to 12-week-old) maie C57BL/6 mice were purchased from The Jackson Laboratory (Bar Harbor, ME). Hemizygous transgenic mice expressing GFP under the control of the chicken 0-actin promoter and cytomegalovirus enhancer and CCR2 knock-out mice were initially ob-tained from the same vendor. Local colonies of GFP and CCR2KO mice were then established and maintained on a C57BL/6 background, respec-tively. Mice were housed four per cage after weaning in a temperature-and humidity-controlled vivarium, on a 14/10 h light/dark cycle (lights on at 6:00 A.M. and off at 8:00 P.M.), with access to rodent chow and water ad libitum. Behavioral experiments were conducted from 8:00 A.M. to 4:00 P.M. Ail protocols were conducted according to the Cana-
dian Council on Animal Care guidelines, as administrated by the Laval University Animal Welfare Committee.
Génération ofbone marrow-chimeric mice Récipient mice were exposée! to 10-gray total-hody irradiation using a cobalt-60 source (Theratron-780 model; MUS Nordion, Ottawa, Ontario, Canada). A few hours later, the animais were injected via tail vein with ~ 5 X 106 bone marrow cells freshly collected from donor mice. The cells were aseptically harvested by flushing fémurs with Dulbecco's PBS (DPBS) containing 2% fetal bovine sérum. The samples were combinée!, filtered through a 40 jim nylon mesh, centrifuged, and passed through a 25 gauge needle. Recovered cells were resuspended in DPBS at a concentration of 5 X 106 vial nucleated cells per 200 /ni. Irradiated mice trans-planted with this suspension were housed in autoclaved cages and treated with antibiotics (0.2 mg of trimethoprim and 1 mg of sulfamethoxazole per milliliter of drinking water given for 7 d before and 2 weeks after irradiation). Animais were subjected to partial sciatic nerve ligation 3-5 months after transplantation.
GFP chimeric mice. GFP-positive (GFP ' ) transgenic mice were used as BM donors. C57BL/6 mice were irradiated and transplantée! with GFP ' cells via the tail vein.
Central CCR2KO chimeric mice. CCR2KO mice were used as BM récipients. GFP+ transgenic BM cells were transplantée! into irradiated CCR2KO mice.
Peripheral CCR2KU chimeric mice. GFP ' transgenic mice were used as BM récipients. Bone marrow cells collected from CCR2KO mice were transplantée! into irradiated GFP ' transgenic mice.
The présence of GFP ' donor-derived cells in the peripheral circulation of transplant récipients in each chimeric group was analyzed 8 weeks after transplantation by fluorescence-activated cell sorting. The GFP chimeric mice and central CCR2KO chimeric mice used in the protocol had ail >80% (83.6 ± 5.03%; n = 50) of GFP + peripheral blood leukocytes, and peripheral CCR2KO chimeric mice had only 1.53 ± 0.03% {n = 10) GFP ' cells in the blood.
Irradiation bone marrow chimeric mouse génération is currently widely used to distinguish blood-derived and GNS résident microglia. To exclueie the possibility that the cell recruitment is an artifact of irradiation or bone marrow transplantation, some additional approaches, such as intrasplenic injection of 6-carboxylfluorescein diacetate, a long-lasting intracellular fluorescent tracer, and using unirradiated parabionts with surgically anatomosed vasculature hâve been reported. As seen in GFP bone marrow chimeras, monitoring invasion of blood dérivée! cells in the absence of previous irradiation and bone marrow transplantation clearly revealed that recruitment of leukocytes across the blood-brain barrier contributes to the accumulation of ionizing calcium-binding adaptor molécule-positive (Iba-1 ' ) cells within the CNS parenchyma in différent pathological conditions (Bechmann et al., 2005; Massengale et al., 2005). More importantly, irradiation does not affect the ability of résident cells to proliferate after spinal cord injury (Horky et al., 2006).
Nerve injury model and behavioral studies Partial sciatic nerve ligation was conducted according to the method of Seltzeret al. (1990) as adaptée! to mice (Malmbergand Basbaum, 1998). Briefly, under isoflurane anesthesia and aseptic conditions, the left sciatic nerve was exposed at high-thigh level. The dorsum of the nerve was carefully freed from surrounding connective tissues at a site near the trochanter. A 8-0 suture was inserted into the nerve with a 3/a curved, reversed-cutting mini-needle (Tyco Health Care, Mississauga, Ontario, Canada) and tightly ligated so that the dorsal one-third to one-half of the nerve thickness was trapped in the ligature. The wound was then closed with two muscle sutures (4-0) and two to three skin sutures (4-0). In sham-operated mice, the nerve was exposed and left intact. The wound was closed as in injured mice.
Ail animais were assessed for mechanical sensitivity before surgery and from days 2-3 after injury until they were killed for histological studies. The investigator was totally blinded to the treatments the mice received. Paw-withdrawal threshold was measured with calibrated von Frey fibers using the up-down method (Chaplan et al., 1994), as described previ-ously (Mogil et al., 1999). Mice were placed on a métal mesh floor with

12398 • J. Neurosci., November 7,2007 • 27(451:12396-12406 Zhang et al. • Microglia and Macrophages in Neuropathic Pain
small Plexiglas cubides (9 X 5 X 5 cm high), and a set of eight calibrated von Frey fibers (ranging from 0.008 to 1.40 g of force) were applied to the plantar surface of the hindpaw until they bent. The threshold force re-quired to elicit withdrawal of the paw (médian 50% paw withdrawal) was determined on two tests separated by at least 1 h. Ail animais were habit-ualed for at least 2 h to their individual Plexiglas observation chamber before testing. Baseline data (day 0) was obtained by averaging measure-ments made 1-2 d before surgery.
Intrathecal injections In a subset of animais, recombinant mouse (rm) MCP-1 (R 8c D Systems, Minneapolis, MN) or neutralizing antibody against mouse MCP-1 (R & D Systems) were injectée! by intrathecal punctions at the level of L5-L6 under isoflurane anesthesia. The rmMCP-1 was delivered every 2 d (2 jxg in 10 JLLI of saline per injection) in adult naive CCR2KO and wild-type (C57BL/6) mice, and the animais were killed at day 6 after the first injection and processed for immunohistochemistry as described below. The MCP-1 neutralizing antibody was delivered in adult GFP chimeric mice with nerve injury. Starting from the day of surgery, mice received an injection of the antibody every 2 d until day 13 after injury (4 /xg in 10 /xl of saline per injection). Animais were then perfused for visualization of GFP cell infiltration at day 14 after injury. Mice in the control groups received intrathecal injections of an equal volume of saline.
Immunohistochemistry In wild-type (C57BL/6) and GFP chimeric mice, bromodeoxyuridine (BrdU) (50 mg/kg; Sigma, St. Louis, MO) was injected intraperitoneally at day 3 after injury, and animais were killed 2 h, 4 d, Il d, and 27 d after injection. To collect the spinal cord tissues of ail animais used in the current study, mice were deeply anesthetized via an intraperitoneal injection of a mixture of ketamine hydrochloride and xylazine and then rapidly perfused transcardially with 0.9% saline, followed by 4% parafor-maldehyde in sodium phosphate buffer. Lumbar spinal cords were re-moved and postfixed overnight. Lumbar spinal cord (L4-L5 segments) were eut into 30 (xm sections, then collected in a cold cryoprotectant solution (0.05 M sodium phosphate buffer, pH 7.3, 30% ethylene glycol, and 20% glycerol), and stored at —20°C.
To allow the détection for BrdU-labeled cells, free-floating sections were pretreated with 50% formamide in 2X SSC for 2 h at 65°C, followed by 15 min in 2X SSC at room température, 30 min in 2N HCI at 37°C, 10 min in 0.1 M borate buffer at room température. Nonspecific labeling was blocked with TUS plus 0.25% Triton X-100, 1% BSA, and 3% normal goat sérum for 1 h. A polyclonal goat anti-rat antibody against BrdU (1:250; Accurate Chemicals, Westbury, NY) was incubated with tissue sections for 48 h at 4°C. After primary antibody incubation, sections were rinsed in TBS and incubated in Alexa 488-conjugated goat anti-rat IgG (in TBS containing 0.25% Triton X-100, 1% BSA, and 3% normal goat sérum, 1:250; Invitrogen, Carlsbad, CA) for 1 h. After rinses in TBS, sections were mounted onto slides and coverslipped with Vectashield mounting médium (Vector Laboratories, Burlingame, CA).
Regular immunofluorescent staining was performed to identify the phenotypes of infiltrated BM cells and spinal microglia reaction to the penpheral nerve injury. Free-floating sections were first treated in TBS containing 3% normal sérum, I % BSA, and 0.25 Triton X-100 for 1 h at room température and then 30 /xm spinal cord sections were incubated overnight at 4°C with antibodies listed below: mouse anti-neuron-specific nuclear protein (NeuN) monoclonal antibody (for neurons, 1:1000; Chemicon, Temecula, CA), rabbit anti-Iba-1 polyclonal antibody (for microglia and macrophages, 1:1000; Wako Chemicals, Rich-mond, VA), rabbit anti-glial fibrillary acid protein (GFAP) polyclonal antibody (for astrocytes, 1:1000; DakoCytomation, Carpinteria, CA), rabbit anti-NG2 polyclonal antibody (chondroitin sulfate proteoglycan, for oligodendrocyte progenitors, 1:250; Chemicon), and monoclonal rat anti-CD31 (for endothelial cells, 1:1000; BD Biosciences PharMingen, San Diego, CA), respectively, followed by a 60 min incubation at room température in fluorochrome-conjugated goat secondary antibody. The sections were then mounted onto SuperFrost slides (Fisher Scientific, Nepean, Ontario, Canada) and coverslipped with Vectashield mounting médium (Vector Laboratories). In some cases, to better identify the an-
atomical distribution of infiltrated cells, additional immunostaining was performed using a polyclonal antibody against GFP ( 1:1000; Invitrogen), revealed by a DAB-based en/.ymatic method; the tissue was then coun-terstained with thionin to identify the parenchyma.
Image analysis Images were acquired either using an Olympus Optical (Tokyo, Japan) microscope (AX-70) equipped with a Spot Caméra or a Zeiss (Oberkochen, Germany) LSM 510 confocal laser-scanning microscope. Colocalization was ensured with confocal Z stacks at 1 /xm intervais and visualization in three-dimensional orthogonal planes. Quantitative analysis of the immunofluorescence intensity was performed on images dig-itized using a constant set of parameters (exposure time, gain, and postimage processing) with spécial care to avoid signal saturation. We measured the intensity of Iba-1 immunofluorescence as the average pixel intensity within a rectangle (197 X 533 pixels) on the dorsal horn (DH) (lamina I—IV) and a rectangle (224 X 294 pixels) on the ventral horn (VH) (lamina IX), on both sides relative to the side of injury (Meta-Morph, version 6.2r6; Universal Imaging, Downingtown, PA). GFP ' cells, BrdU ' cells, and Iba-1 f microglia! cells were counted by two independent investigators in four différent régions of interest [ipsilateral DH (DHi), contralateral DH (DHc), VHi, and VHc]. Only ramified GFP ' /Iba-1 cells within parenchyma] gray matter were included.
Statistics AH data are presented as means ± SEM. Statistical analysis was based on the following: (1) repeated-measures ANOVA followed by Dunnett's case-comparison post hoc test for behavioral analyses; (2) paired i test for the différence in intensity of Iba-1 signal between ipsilateral and contralateral side in the DH and VH, respectively; (3) unpaired t test for the différence in intensity of Iba-1 signal between groups (peripheral/central CCR2KO DHi vs GFP chimera DHi; peripheral/central CCR2KO VHi vs GFPchimeraVHi).
Results Infiltration of bone marrow-derived cells into spinal cord after peripheral nerve injury To identify the origins of the activated microglia observed in the spinal cord after peripheral nerve injury, we transplanted GFP-expressing bone marrow stem cells into irradiated C57BL/6 mice (GFP chimeric mice). We found that, in naive animais, GFP^ cells were virtually absent in the spinal cord parenchyma, and the few GFP + cells found in the spinal cord had an elongated shape and were restricted to blood vessels (Fig. 1 A). We then subjected the mice to either a sham surgery of the thigh or a partial sciatic nerve ligation injury. Insham-operated mice, the numbero fGFP cells was slightly higher in the spinal cord, but there was no sig-nificant différence between the ipsilateral and contralateral sides (Fig. \A). In contrast, many ramified GFP-expressing cells were présent in the DHi and VHi of the L4-L5 spinal cord after nerve injury (Fig. \A). The différent morphologies of G F P + cells are depicted in Figure 1 B-D. The results were confirmed by immu-nolabeling with a polyclonal antibody against GFP for infiltrated cells. Counterstaining with thionin helped better identify the an-atomical localization of GFP ' cells (Fig. \E-H).
To identify the phenotype of thèse ramified GFP ' donor cells, we used an antibody directed against Iba-1 to label microglia. Confocal microscope analysis on x, y, and z orthogonal planes provided direct évidence that virtually ail G F P + cells présent within the spinal cord parenchyma were Iba-1-positive ramified cells (Fig. 2A-C). Double immunolabeling of GFP with other cellular markers, NeuN for neurons, GFAP for astrocytes, NG2 for oligodendrocyte progenitors, and CD31 for endothelial cells, were also conducted. No évidence of GFP colocalization with the above markers has been observed (Fig. 2D).
To détermine the temporal profile of BM-derived cell infiltra-

Zhang et al. • Microglia and Macrophages in Neuropathic Pain J. Neurosci., November7,2007 • 27(45):12396-12406 -12399
Naive Sham Nerve-injured-d14 —
DHI
VHI
"'.lé*:
«**# S 4
Figure 1 . Infiltration of bone marrow-derived cells into the spinal cord after sciatic nerve injury. A, BM-derived cells in the lumbar spinal cord of naive, sham-operated and sciatic nerve-injured mice. No ramified GFP ' cells were found in the spinal parenchyma of non-injured animais. In contrast, GFP + cell infiltration was remarkable in injured animais, which was restricted in the ipsilateral side of the injury (scale bar, 1 mm). B-D, Meningeal GFP ' cells had a round shape (S), they were elongated when associated with blood vessels (0 , and ramified within the parenchyma (D) (scale bar, 100 /i,m).£-«,lmmunolabelingof infiltrated cells with a polyclonal antibody against GFP, counterstained by thionin, revealed theiranatomical localization in DHi and VHi(day14after injury) (£) and différent cellular shapes depending on the distribution in the méninges (F), within vessels (G), and parenchyma (H ) (scale bar, 50 ^m).
lba-1
GFP
Meige
DHi UHc VHI VHc
■ ■1 c
Figure 2. Phenotype identification of infiltrated BM-derived cells in the lumbarspinal cord. A, Intense lba-1 labeling was found in activated microglia in the ipsilateral side spinal cord (DH/VH), whereas lba-1 immunofluorescence was weak (red) in the contralateral DH/VH. Ramified GFP ' cells (green) overlapped with the lba-1 immunoreactive signal in the ipsilateral DH/VH. Almost ail ramified GFP f cells within the parenchyma were lba-1 ' (merge) (scale bar, 200 /n.m), which was confirmed by confocal microscopic analysis in thex,y, and /orthogonal planes in DH (B) and VH (O (scale bar, 10 /u,m). D, No colocalization of GFP with other cellular markers (NeuN, GFAP, NG2, and CD31) was observed in the lumbarspinal cord dorsal horn 14 d after injury (scale bar, 100/j,m).
tion and its relationship with CNS résident microglia, we quan-tified the number of ramified GFP-expressing cells among ail lba-1 immunoreactive microglia in four différent régions of in-terest: DHi, DHc, VHi, and VHc. Three days after nerve lésion, an average of 9% of microglia in the DHi and 22% in the VHi ex-pressed GFP (DHi, 3.6 ± 0.6 GFP ' cells; VHi, 8.0 ± 2.3 GFP +
cells). At days 7-14 after injury, 25-27 and 41-42% of microglia in the DHi and the VHi were found tobe GFP ' , respectively. One
month after the injury, the number of GFP ' cells decreased to 6 and 16% in the DHi and the VHi, respectively (Fig. 3). The time course of the increase in GFP * cell number in the lumbar spinal cord paral-leled that of microglial activation (Fig. 3).
Prolifération and differentiation of bone marrow-derived cells within the spinal cord parenchyma We then assessed the plasticity of thèse infil-trating cells by determining their capacity to proliferate and differentiate into microglia. Animais were injected with UrdU 3 d after injury and perfused at différent time points afterward (days 3-30). Immunofluorescence staining of incorporated lîrdU revealed that peripheral nerve injury induced cell prolifération in the spinal cord, ipsilateral to the side of nerve injury, from days 3 to 14 (Fig. 4A). Nerve injury increased the number of BrdU ' cells in both irradiated GFP chimeric mice and non-irradiated con-trol C57DL/6 mice equally (data not shown). Double immunolabeling of BrdU with GFP demonstrated that both résident cells (red arrow) and BM-derived hematopoietic cells (yellow arrow) proliferated within the spinal cord parenchyma (Fig. 4B), in which 19.7 and 22.3% of BrdU ' cells derived from peripheral macrophages in the DHi and the VHi, respectively (Fig. 4C).
We next analyzed morphological changes in thèse infiltrated GFP + cells. Al-though they had a round shape when lin-
ing the méninges, they developed broad and short processes once they infiltrated the parenchyma (day 3). At later time points (days 7-30), most GFP + cells were highly ramified microglial cells with relatively small cell bodies, resembling their résident counter-parts (Fig. AC). Thus, newly recruited hematogenous macrophages invaded the spinal cord parenchyma proliferated and dif-ferentiated gradually into highly ramified microglia.

12400 • J. Neurosci., November 7,2007 • 27(45):12396-12406 Zhang et al. • Microglia and Macrophages in Neuropathic Pain
70
c 60 O Ç» 0) 1.0
40
30
20
10
DH VH
Naive
DHi DHc VHi VHc
day3
Rôle of CCR2 in mediating microglial chemotaxis in the spinal cord To test the hypothesis that CCR2 is critical in résident microglial activation and peripheral macrophage infiltration, we first com-pared Iba-1 immunofluores-cence in sections of L4-L5 spinal cord taken from wild-type (C57BL/6) and CCR2-deficient (CCR2KO) mice. Although nerve injury induced a striking increase of Iba-1 immunoreac-tivity in the DHi and VHi of wild-type (C57BL/6) mice at day 14 af-ter nerve injury, such an increase was almost completely abolished in CCR2KO mice (Fig. 5A,B). This finding suggests that CCR2 expression is necessary for both activation of résident microglia and chemotaxis of BM-derived cells af-ter peripheral nerve injury.
Chemotaxis of BM-derived cells may, however, occur sec-ondarily to activation of résident microglia expressing CCR2. To test for this possibility, we next generated two other groups of chimeric mice by transplanting BM cells collected from GFP transgenic mice into irradiated CCR2KO mice (central CCR2KO chimera) and by transplanting CCR2KO bone marrow cells into irradiated GFP transgenic mice (peripheral CCR2KO chimera). The expression pattern of Iba-1 was similar in wild-type non-irradiated mice and GFP chimeric mice, showing that irradiation and bone marrow cell transplantation did not modify the ability of résident microglia and BM-derived cells to respond to nerve injury (Fig. 5A). We quantified the mean inten-sity of Iba-1 immunoreactive signal in defined régions of the dorsal and ventral horns, in which microglial activation was considered to be the most prominent. Ail groups of chimeric mice exhibited sig-nificant différences in Iba-1 staining between ipsilateral and contracterai sides after injury (Fig. 55). In addition, the Iba-1 signal was significantly lower on the side ipsilateral to the injury in both groups of CCR2KO chimeric mice when compared with the ipsilateral side in GFP chimeric mice (Fig. 5A,B).
The same resuit was obtained by counting Iba-1 ' cells (Table 1). When CCR2 was absent in the periphery, the decrease in Iba-1 ' cell number (Table 1, A minus C) corresponded to that of infiltrated cells in the GFP chimeric mice (Table 1, B). Similarly, when CCR2 was absent in the CNS, the différence in Iba-1 ' cell number between central CCR2 KO and total CCR2KO (Table 1, D minus E) corresponded to the number of infiltrated cells in the GFP chimeric mice (Table 1, B). The loss in Iba-1 staining in each condition thus reflected the contribution of activated résident microglia and bone marrow-derived infiltrated macrophages, respectively. The results thus indicate that CCR2 expression is not only necessary for the activation of résident microglia but is also directly responsible for recruitment of BM-derived cells to the CNS.
MCP-1 is the trigger for macrophage infiltration and activation of résident microglia via its cognate receptor CCR2 To identify the ligand that activated the CCR2 receptor, we injectée! intrathecally rmMCP-1 in wild-type and in CCR2KO
I I
□ lba-1
c i p
X
JL xPi
i
DHc VHi VHc
day 7
DHi DHc VHi VHC
day 14
DHi DHc VHi VHc
day 30
Time post-injury (days)
Figure 3. Temporal profile of BM-derived cell infiltration in the spinal cord parenchyma. The numbers of lba-1 ' microglia (white bars) and GFP +/ lba-1 ' BM-derived microglia (gray bars) were determined in fours régions of the spinal cord ( 4 - 6 sections per mouse, 6 mice per group). Note the significant increase of BM-derived microglia in the ipsilateral side DH/VH starting from day 3 and peaking at day 14. Corre-spondingly, the number of microglia in the ipsilateral side, including BM-derived microglia increased also from day 3 to day 14 (data are expressed as mean ± SEM).
mice. Exogenous MCP-1 induced an increase in the size of microglial cell bodies as shown by Iba-1 immunostaining in intact wild-type mice, and thèse changes were abolished in CCR2-deficient mice (Fig. 6A). In addition, we injected intrathecally an antibody against mouse MCP-1 in GFP chimeric mice having nerve injury to verify whether neutralization of MCP-1 could prevent peripheral macrophage infiltration. In four of seven animais, GFP ' cell infiltration was completely abolished. Overall, the number of ramified GFP + cells was significantly reduced in mice injected with the MCP-1 neutralizing antibody compared with mice that received control saline injection (Fig. 6B,C).
CCR2 in either CNS microglia or in bone marrow-derived macrophages is sufficient for the development of mechanical allodynia Development of mechanical hypersensitivity (allodynia) is a clin-ically relevant characteristic of nerve injury. To address the rela-tionship between mechanical allodynia and the chemotaxis of résident and BM-derived microglia, we measured paw-withdrawal threshold to mechanical stimuli in ail animais before and after injury. Before nerve injury, the withdrawal threshold was not affected by the CCR2 gène deletion nor by the irradiation and bone marrow cell transplantation (Fig. 7). Wild-type C57BL/6 mice showed a robust decrease in withdrawal threshold from 0.35 ± 0.01 g before surgeryto 0.09 ± 0.01 g ( p < 0 . 0 1 ) a t day 3 after surgery and maintained this hypersensitivity to the end of the testing period (day 14) (Fig. 7A). Mechanical allodynia was significantly attenuated in CCR2KO mice (Fig. 75) and in GFP chimeric mice treated with MCP-1 antibody (58 ± 3.8% réduction compared with saline treated mice at day 12 after injury; n = 7 per group), indicating that MCP-1/CCR2 signaling plays a critical rôle in the development of the hypersensitivity. In contrast, however, neither sélective peripheral CCR2KO nor sélective central CCR2 KO mice had their allodynia significantly attenuated (Fig. 7D,£). This resuit indicates that expression of CCR2 in either résident or BM-derived cells is sufficient for the

Zhang et al. • Microglia and Macrophages in Neuropathic Pain J. Neurosci., November 7,2007 • 27(45):12396-12406 • 12401
development of mechanical allodynia after peripheral nerve injury.
Discussion Hère we demonstrate that BM-derived macrophages hâve the ability to infiltrate the spinal parenchyma after peripheral nerve injury. In-terestingly, in contrast to spinal cord injury, the blood-spinal cord barrier (BSCB) remains physically intact after peripheral nerve injury, yet our results show that chemotaxis occurs across the BSCB. Thèse infiltrated macrophages proliferate and differentiate into microglia and, together with their résident coun-terparts, contribute to CNS microgliosis in response to peripheral nerve injury. We re-ported previously that MCP-1, the endoge-nous ligand for CCR2 receptors, is produced by injured neurons (Zhang and De Koninck, 2006). In the current study, we demonstrated that exogenous MCP-1 could induce spinal microglial activation and this activation is lost in CCR2KO mice. In addition, neutralization of MCP-1 prevented peripheral macrophage infiltration after nerve injury. Together, thèse findings imply a neuron-to-microglia and neuron-to-macrophage signaling mechanism underlying the central component of neuro-pal hic pain pathogenesis. The fact that both résident and BM-derived microglia participate in the development of the pathology has direct clinical importance. Inhibiting either résident microglia or BM-derived macrophages may not be an effective approach to relieve neuropathic pain.
Recruitment of circulating leukocytes into the CNS in normal physiological conditions and in pathological states supports the essen-tial functions of immunosurveillance and host
Figure 4. Prolifération and differentiation of infiltrated bone marrow-derived cells. A, Représentative BrdU staining in the lumbar spinal cord of GFP chimeric mice (14 d after injury, 11 d after BrdU injection). Note the increase of BrdU-positive cells in the lumbar spinal cord, ipsilateral to the injury (scale bar, 1 mm). 8, Z-sectioned scan with confocal microscope (Zeiss LSM 510) through the extent of Brdll-positive nucleus to verify the double labeling with GFP ' cells. BrdU and GFP colocalization showing cell prolifération within BM-derived microglia (yellow arrow); BrdU single labeling showing cell prolifération m résident cells (red arrowhead) (scale bar, 20 i im). C, Quantitative analysis of the number of GFP ' /BrdU ' cells over total BrdU ' cells (14 d after injury, n = 3 , 3 - 4 sections per animal, total of 277 BrdU ' cells in DH and 201 BrdU ' cells in VH were counted) indicating that, 14 d after injury, when microglial activation on the ipsilateral side reached its peak, —20% of proliferating cells derived from peripheral macrophages (data are presented as mean ± SEM). D, Photomicro-graphs showing the morphological plasticity of BM-derived cells over time Until they were recruited intothe parenchyma, they were round/ oval shaped on the endothelium; shortly after their pénétration (day 3 after injury), BM-derived GFP ' cells displayed few short branches with a large cell body; during days 7-14, they developed into ramified cells; 30 d after injury, thèse infiltrated BM-derived cells differentiated into highly ramified microglia (scale bar, 100 ^.m).
BrdU
ipsilateral contralateral M e r g e r g l on the méninges
in the parenchyma -d3
m the parenchyma -d7
m the parenchyma -d14
m the parenchyma -d30
80.3% DHi
VHi 77.7%
19.7%
22.3%
I BrdU+
BrdU+/GFP+

12402 • J. Neurosci., November7,2007 • 27(451:12396-12406 Zhang et al. • Microglia and Macrophages in Neuropathic Pain
B
défense. Although the molecular signais and detailed mechanisms responsible for the migration of spécifie inflammatory cells into the CNS compartment are not completely identified, accumulating évidence suggests that chemokines, in concert with adhésion molécules, are essen-tial for the process (Charo and Ransohoff, 2006). MCP-1, identified originally as monocyte, memory T lymphocytes and NK cell-specific chemoat-tractant (Valenteet al., 1988; Yoshimura et al., 1989) has been attributed a key rôle in regulating the infiltration of monocytes during inflammation. MCP-1 knock-out mice exhibited déficient monocyte recruitment in expérimental autoimmune encephalomyelitis (Lu et a l , 1998;Huangetal„ 2001). En-torhinodentate axotomy induces leuko-cyte infiltration in the denervated hippocampus (Bechmann et al., 2005; Ladeby et al., 2005) in which induced MCP-1 expression by glial cells has been considered as critical in directing leuko-cytes to sites of axonal injury in the CNS (Babcock et al., 2003). It is interesting to note that, although numerous GFP cells were found in multiple régions of normal brain (the current study; data not shown) (Vallieres and Sawchenko, 2003; Simard and Rivest, 2004), such a process remains rare in the spinal cord of intact mice. However, bone marrow-derived cells infiltrated massively the affected régions ipsilateral to the peripheral nerve damage. This chemotaxis is dépendent on MCP-1, because MCP-1 antibody treatment successfully reduced the num-ber of infiltrated cells. This is also dépendent on the MCP-1 receptor CCR2, because CCR2-deficient mice no longer exhibited such an accumulation of mi-croglial cells. MCP-1 has the ability to alter expression of tight junction-associated proteins in endothelial cells of the brain vascular System (Stamatovic et al., 2003; Song and Pachter, 2004), which results in a local and temporary increase of BSCB permeability (Gordh et al., 2006). This may explain why MCP-1 and CGR2 play such a critical rôle in such a cell influx in the affected spinal cord. We then took advantage of this model to détermine the respective contribution of BM-derived versus résident microglia in generating chimeric mice and found that both types of cells participate in this process. MCP-1 production by damaged neurons after peripheral nerve injury (Zhang and De Koninck, 2006) may then trigger chemotaxis through its cognate receptor CCR2 expressed in résident and bone marrow-derived microglia.
In response to peripheral nerve injury, spinal glial cells, especially microglia, proliferate (Echeverry et al., 2007). The results from the current study showed that both résident cells
Wild-type-naive Wilcl-type iniured CCR2KO injured
GFP chimera injurod Perlph CCR2KO chl Iniured Cent.CCR2KO chl injurod
Figure 5. Rôle of CCR2 in mediating microglial chemotaxis in the spinal cord. A, Photomicrographs depicting représentative lba-1-positive cells in mouse L5 régions 14 d after the sham opération or injury. Partial sciatic nerve ligation induced a striking increase of lba-1 immunoreactivity (ir) in the ipsilateral side DH/VH in wild-type C57BL/6 mice; this increase in lba-1 immunore-active signal was almost completely abolished in CCR2K0 mice, whereas both groups of CCR2K0 chimeric mice exhibited partial atténuation when compared with GFP chimeric mice after sciatic nerve ligation (scale bar, 1 mm). B, Intensity of lba-1 signal determined as the average pixel intensity on spécifie régions ofinterest on L5 sections at14dafterinjury(4-6sectionsper mouse, 4 mice per group; data are expressed as mean ± SEM; *p < 0.05, **p < 0.01, ipsilateral vs contracterai; *p < 0.05, peripheral/ central CCR2K0 DHi vs GFP DHi; M p < 0.01, peripheral CCR2K0 VHi vs GFP VHi).
Table 1. Quantification of l b a - 1 + cell numbers in the lumber spinal cord of mice with différent CCR2 genetic background 14 d after peripheral nerve injury
GFP chimeric mice Peripheral CCR2K0mice
lba-1 ' cells B
GFP ' cells lba-1 C cells
Central CCR2K0 IIIKC
D lba-1+ cells
CCR2K0 mice
E lba-1 + cells
DHi DHc VHI Vile
59.7 ± 2.75 25.2 ± 3.83
56.55 ± 6.03 28.65 ± 2.95
16 ± 4.72 3 ± 0.26
21.3 ± 8.1 4 ± 1.67
41.65 ± 2.09* 22,80 ± 1.56 33.05 ± 4.37* 26.80 ± 0.43
42.50 ± 3.63* 20.90 ± 3.53 42.20 ± 2.42* 25.40 ± 2.92
27.72 ± 2.1** 23.78 ± 1.33 26.02 ± 3.56* 26.94 ± 0.98
The numberof lba-1'' microglia was determined in four régions (DHI, DHc, VHI, and VHc) of thesplnal cord (4—6 sections per mouse, 4 mice per group) in four groups (GFP chimeric, peripheral CCR2K0 chimeric, central CCR2K0 chimeric, and CCPJK0) of mice al 14 d afler injury. Note that, on the ipsilateral side, the number of lba-1 ' cells was significantly less in mice lacking peripherally, centrally, or totally CCR2 receptor than that in GFP chimeric mice (data are expressed as mean ± SEM,"p < 0.05, "p < 0.01, peripheral, central, and total CCIÎ2K0 DHI/VHI VS GFP DHi/VHI, respeclively).
and blood-derived microglia retain their capacity to divide, in which 20% of proliferating cells derived from peripheral macrophages. We also observée! that infiltrated blood-borne cells can differentiate into highly ramified lba-1 ' résident microglia but not in any other types of cells at ail tested time points after injury (days 3-30). The potential plasticity of hemato-poietic stem cells raised the questions on the trans-lineage differentiation. Several independent groups hâve provided évidence that bone marrow-derived cells participate in adult neurogenesis and angiogenesis by giving rise to neurons (Mezey et al., 2000; Priller et al., 2001), endothelial cells

Zhang et al. • Microglia and Macrophages in Neuropathic Pain J. Neurosci., November7,2007 • 27(45)12396-12406 • 12403
1. Wild type with il rmMCP-1 3. CCR2KOwilhlt rmMCP-
Figure 6. Rôle of MCP-1 in stimulating résident microglial activation and peripheral macrophage infiltration via its cognate receptor CCR2. A, Intrathecal (it) delivery of rmMCP-1 (3 injections, 2 /tig in 10 /xl of saline per injection over 6 d) stimulated microglia in the spinal cord of intact wild-type mice as seen by the increase in size of their cell bodies (AI) when compared with that in mice which did not receive MCP-1 stimulation (A2). Thèse changes were not observed in CCR2-deficient mice: microglial size and shape remained similar in CCR2K0 mice either treated (A3) or not (A4) with MCP-1 (scale bar, 200 /n,m). Note the morphological changes highlighted in the insets. B, Infiltrated ramified GFP H cells were no longer présent in the ipsilateral side OH and VH of injured mice treated with MCP-1 antibody (ab). Only few elongated and scattered GFP ' cells were found in blood vessels, although the number of meningeal GFP ' cells significantly increased (scale bar, 1 mm). C, Quantitative analysis of GFP +
cells in the spinal cord of GFP chimeric mice after sciatic nerve injury and MCP-1 neutralization (data are shown as mean ± SEM; n = 7 mice/group; **p < 0.01, mice treated with MCP-1 antibody vs mice treated with saline). MCP-1 antibody significantly reduced the number of GFP ' cells within the spinal cord parenchyma.
A. Wild-type mice 1).!,
B. CCR2KO mice
11.4
0.3
0.3
0.1 ** Cl
2 4 6 8 10 12 Time post-ln|ury (days)
D. Periph.CCR2KO chimera 0.6-,
2 4 6 8 10 12 Time post-injury (days)
2 4 6 8 10 12 Time post-injury (days)
Figure 7. Mechanical allodynia in response to partial sciatic nerve ligation. Injured paw-withdrawal thresholds decreased from baseline (—0.35 g) to below 0.1 g in ail groups, except for CCR2K0 mice. Significant decrease in withdrawal threshold occurred in ail chimeric groups, indicating that CCR2 expression in either résident or bone marrow-derived microglia is sufficient to cause mechanical allodynia. Data are shown as mean ± SEM; *p < 0.05; **p < 0.01; n = 4 - 6 mice per group. Baseline data (day 0) was obtained by an average of two measurements, 1-2 d before surgery.
(Bailey et al., 2006), and astrocytes (Kopen et al., 1999). Consistent with some other studies (Simard and Rivest, 2004; Mas-sengale et al., 2005), our findings indicated that bone marrow-derived stem cells and their progeny maintain lineage fidelity within the spinal cord parenchyma in the pathology of neuropathic pain induced by peripheral nerve injury. The discrep-
ancy may be explained by technical problems (specificity of cellular markers and sensitivity of histochemical meth-ods) but most likely the différence may resuit from anatomical distributions, because the BM-derived cells exhibiting the characteristic morphology of cere-bellar Purkinje neurons has been observed more frequently (Priller et al., 2001; Wright et al., 2001) and also from différent pathophysiological conditions.
The contribution of glia and glia-neuron communication in enhancing nociceptive transmission has been well documented. Every animal model of nerve injury-induced exaggerated pain is associated with the activation of glia within the pain-responsive régions of the spinal cord (Tsuda et a l , 2005). Such exaggerated pain states are mediated by glial activation, because they are blocked by drugs (e.g., fluorocitrate and minocy-cline) that block glial activation (Milli-gan et al., 2003; Raghavendra et al., 2003), by sélective proinflammatory cy-tokine antagonists (Sweitzer et al., 2001), and by disrupting proinflammatory cytokine signaling pathway (Sweitzer et al., 2004). We revealed in this study that nerve injury induced microglial activation comprises the activation of preexisting résident microglia, as well as the recruitment of BM-derived peripheral macrophages. Of important impact is that both populations are in-volved in the central component of sen-sitization to enhance spinal neuronal ex-citability by dynamic glial modulators, such as ATP and BDNF (Tsuda et a l , 2003; Coull et al., 2005). Either résident microglia (central sensitization) or peripheral macrophages (central sensitization by infiltration into the spinal cord and peripheral sensitization by their ac-tivity at the injured site) is sufficient to cause the neuropathic pain. The fact that Iba-1 staining was significantly reduced in both central and peripheral CCR2KO chimeric mice (compared with GFP chimeric mice) while neuropathic pain be-havior remained identical in ail three lines of mice suggest that there may be a floor effect on the behavior, i.e., that the amount of microglia activation in the wild type is supramaximal, in other words, more than enough to produce a full effect. Rutkowski et al. (2000) dem-
onstrated that mechanical allodynia was not altered by either deactivation of macrophages with CNI-1493 or by depletion of circulating macrophages using lisosome-encapsulated clo-dronate before peripheral nerve injury. They concluded that macrophages hâve limited rôle in génération of nerve injury-induced mechanical allodynia. It was also reported that mac-
- Injured-left - Injured-rlght - .i i. . i11 i. 11
- sham-rlght
Cent.CCR2KO chimera
0 2 4 6 8 10 12 Time post-injury (days)

12404 • J. Neurosci., November 7,2007 • 27(45):12396-12406 Zhang et al. • Microglia and Macrophages in Neuropathic Pain
rophage depletion by intravenous injection of l iposome-encapsulated clodronate reduced thc number of macrophages in the injured nerve and alleviated slightly thermal hyperalge-sia (Liu et a l , 2000). The discrepancy with our results may stem from différences in the behavioral ou tcomes measured (mechanical allodynia vs thermal hyperalgesia). In light of our current findings, we suggested that peripheral macrophages hâve significant cont r ibut ion not only in peripheral but also in central sensitization. However, blockade of only circulating macrophages is not enough to a t tenuate hypersensitivity, be-cause the involvement of spinal cord résident microglia in the central componen t is not negligible.
Our results not only implicated MCP-I as a necessary me-diator for spinal microglia] activation, they point to the che-mokine as being a major player for the development of mechanical allodynia. Thèse data are consistent with another study showing an essential rôle of CCR2 in mediat ing neuropathic pain in mice (Abbadie et al., 2003). We further revealed the critical rôle of CCR2 in peripheral macrophages and résident microglia through neuron- to-macrophages and neuron-to-microglia interaction in the genesis of ongo ingneuropa th i c pain. In addit ion, MCP-1 was reportée! to depolarize sensory neurons after chronic compress ion of the dorsal root ganglion (White et al., 2005), which implicates a direct neu ron- to -neuron interaction of the ligand with its receptor. Some other mediators for neuron-to-gl ia communica t ion that could lead to glial activation and conséquent enhancement of pain hâve been suggested. ATP activâtes glia and the release of pro in-flammatory cytokines (Hide et al., 2000; Shigemoto-Mogami et al., 2001). Mice lacking either purinergic P2X4 or P2X7
receptors show an impaired ability to develop neuropathic pain (Tsuda et al., 2003; Chessell et al., 2005). The chemokinc fractalkine lias also been suggested to cont r ibute to the hypersensitivity evoked by nerve injury through microglial activation (Verge et al., 2004). Mice that bear a muta t ion in the gène encoding toll-like receptor 4 (TLR4) hâve a reduced microglial activation and do not develop thermal and mechanical allodynia after peripheral nerve injury (Tanga et al., 2004). Heat shock protein 27 was proposed to be the potential endogenous ligand forTLR4 (Costigan et al., 1998). Although considérable redundancy may exist, microglial activation and recrui tment through MCP-1/CCR2 seem a critical componen t for the pathogenesis of neuropathic pain.
The ability of macrophages to infiltrate and differentiate into fully functional microglia in the CNS parenchyma opens the door for new therapeutic stratégies to treat neuropathic pain. Indeed, thèse cells are innately and specifically attracted to injured and diseased régions and may thus be used as effective and sélective vehicles to deliver molécules that prevent neurodegenerat ion (Scholz et al., 2005), cl iminate toxic p ro teins or pronociceptive signaling molécules (Shubayev and Myers, 2002; Coull et al., 2005), or deliver ant i - inf lammatory agents (Ledeboer et al., 2007). BM-derived cells will be able to follow the chemoat t ract ing gradient provided by the dis-tressed neurons (e.g., MCP-1) early after injury and specifically in the affected région and deliver the necessary molécules to limit microgliosis and neuronal hypersensitivity. A similar approach can be envisaged to treat neurodegenerat ive dis-eases, such as Alzheimer's disease (Simard et al., 2006), amyo-trophic latéral sclerosis (Solomon et al., 2006), pr ion disease (Priller et al., 2006), and mult iple sclerosis (Raivich and Ba-nati, 2004) in which BM-derived cells massively infiltrate the affected régions.
Références Abbadie C, Lindia IA, Cumiskey AM, Peterson Llî, Mudgett JS, lîayne EK,
DeMartino )A, Maclntyre UE, Forrest M( (2003) Impaired neuropathic pain responses in mice lacking the chemokinc receptor CCR2. Proc Natl Acad Sci USA 100:7947-7952.
Ambrosini E, Aloisi F (2004) Chemokines and glial cells: a complex network in the central nervous System. Neurochem Res 29:1017-1038.
Babcock A A, Kuziel WA, Rivest S, Owens T (2003) Chemokine expression by glial cells directs leukocytes to sites of axonal injury in the CNS. ) Neurosci 23:7922-7930.
Bailey AS, Willenbring H, liang S, Anderson IM, Schroeder DA, Wong MH, Grompe M, Fleming WH (2006) Myeloid lineage progenitors give lise to vascular endothelium. Proc Natl Acad Sci USA 103:13156-13161.
lîaron R (2006) Mechanisms of disease: neuropathic pain—a clinical perspective. Nat Clin Pract Neurol 2:95-106.
Bechmann 1, Goldmann 1, Kovac AD, Kwidzinski E, Simburger E, Naftolin F, Dirnagl U, Nitsch R, Priller I (2005) Circulating monocytic cells infiltrate layers of anterograde axonal degeneration wherc they transform into microglia. FASEB J 19:647-649.
Campbell JN, Meyer RA (2006) Mechanisms of neuropathic pain. Neuron 52:77-92.
Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL ( 1994) Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Methods 53:55-63.
Charo I F, Ransohoff RM (2006) The many rôles of chemokines and chemokine receptors in inflammation. N Engl J Med 354:610-621.
Chessell IP, Hatcher JP, Bountra C, Michel AU, Hughes JP, Green P, Egerton ], Murfin M, Richardson 1, Peck WL, Grahames CB, Casula MA, Yiangou Y, Birch R, Anand P, Buell GN (2005) Disruption of the P2X7 purino-ceptor genc abolishes chronic intlammatory and neuropathic pain. Pain 114:386-396.
Colburn RW, Rickman AJ, UeLeo JA (1999) The effect ofsite and type of nerve injury on spinal glial activation and neuropathic pain behavior. Exp Neurol 157:289-304.
Costigan M, Mannion RJ, Kendall G, Lewis SE, Campagna IA, Coggeshall RE, Meridith-Middleton J, Tate S, Woolf CJ (1998) Heat shock protein 27: developmental régulation and expression after peripheral nerve injury. ) Neurosci 18:5891-5900.
Coull IA, Beggs S, Boudreau U, Boivin D, Tsuda M, Inoue K, Gravel C, Salter MW, De Koninck Y (2005) BDNF from microglia causes the shift in neuronal anion gradient underlying neuropathic pain. Nature 438:1017-1021.
Coylc UE (1998) Partial peripheral nerve injury leadsto activation ofastro-glia and microglia which parallels the development of allodynic behavior. Glia 23:75-83.
Denker SP, Ji S, Uingman A, Lee SY, Uerugin N, Wendland MF, Vexler ZS (2007) Macrophages are comprised of résident brain microglia not infil-trating peripheral monocytes acutely after neonatal stroke. J Neurochem 100:893-904.
Echeverry S, Shi XQ, Zhang J (2007) Characterization of cell prolifération in rat spinal cord following peripheral nerve injury and the relationship with neuropathic pain. Pain, in press.
Flugel A, Hager G, Horvat A, Spitzer C, Singer GM, Graeber MB, Kreutzberg GW, Schwaiger FW (2001) Neuronal MCP-1 expression in response to remote nerve injury. J Cereb lllood Flow Metab 21:69-76.
Fu KY, Light AR, Matsushima GK, Maixner W (1999) Microglial reactions after subeutaneous formalin injection into the rat hind paw. Brain Res 825:59-67.
Furuya T, Tanaka R, Urabe T, Hayakawa I, Migita M, Shimada T, Mizuno Y, Mochizuki H (2003) Establishment of modified chimeric mice using GFP bone marrow as a model for neurological disorders. NeuroRcport 14:629-631.
Gordh T, Chu H, Sharma HS (2006) Spinal nerve lésion alters blood-spinal cord barder mnetion and activâtes astrocytes in the rat. Pain 124:211-221.
Hide I, Tanaka M, Inoue A, Nakajima K, Kohsaka S, Inoue K, Nakata Y (2000) Extracellular ATP triggers tumor necrosis factor-alpha release from rat microglia. I Neurochem 75:965-972.
Horky LL, Galimi F, Gage FH, Homer P] (2006) Fate of endogenous stem/ progenitor cells following spinal cord injury. J Comp Neurol 498:525-538.

Zharig et al. • Microglia and Macrophages in Neuropathic Pain J. Neurosci.,November7,2007 • 27(45):12396-12406 • 12405
Huang DR, Wang ), Kivisakk P, Rollins BJ, Ransohoff RM (2001 ) Absence of monocyte chemoattractant protein I in mice leads to decreased local macrophage recruitment and antigen-specific T helpcr cell type 1 im-mune response in expérimental autoimmune encephalomyelitis. J Exp Med 193:713-726.
Kopen GC, Prockop DJ, Phinney DG (1999) Marrow stromal cells migrate throughout forebrain and cerebellum, and they differentiate into astro-cytes after injection into neonatal mouse brains. Proc Natl Acad Sci USA 96:10711-10716.
Kreutzberg GW (1996) Microglia: a sensor for pathological events in the CNS. Trends Neurosci 19:312-318.
Ladeby R, Wirenfeldt M, Dalmau I, Gregersen R, Garcia-Ovejero D, Babcock A, Owens T, Finsen B (2005) Proliferating résident microglia express the stem cell antigen CD34 in response to acute neural injury. Glia 50:121-131.
Lawson LJ, Perry VH, Gordon S (1992) Turnover of résident microglia in the normal adult mouse brain. Neuroscience 48:405-415.
Ledeboer A, Jekich BM, Sloane EM, MahoneyJH, Langer S J, Milligan ED, Martin D, Maier SF, Johnson KW, Leinwand LA, Chavez RA, Watkins LR (2007) Intrathecal interleukin-10 gène therapy atténuâtes paditaxel-induced me-chanical allodynia and proinflammatoiy cytokine expression in dorsal root ganglia in rats. Brain Behav Immun 21:686-698.
Léonard EJ, Skeel A, Yoshimura T (1991) Biological aspects of monocyte chemoattractant protein-) (MCP-I). Adv Exp Med liiol 305:57-64.
Liu T, van Rooijen N, Tracey DJ (2000) Depletion of macrophages reduces axonal degeneration and hyperalgesia following nerve injury. Pain 86:25-32.
Lu B, Rutledge BJ, Gu L, Fiorillo J, Lukacs NW, Kunkel SL, North R, Gérard C, Rollins BJ (1998) Abnormalities in monocyte recruitment and cytokine expression in monocyte chemoattractant protein I -déficient mice. J Exp Med 187:601-608.
Malmberg AU, Basbaum Al (1998) Partial sciatic nerve injury in the mouse as a model of neuropathic pain: behavioral and neuroanatomical corre-lates. Pain 76:215-222.
Marchand F, PerrettiM.McMahonSB (2005) Rôle of the immune System in chronic pain. Nat Rev Neurosci 6:521-532.
Marx J (2004) Pain research. Prolonging the agony. Science 305:326-329.
Massengale M, Wagers AJ, Vogel H, Weissman IL (2005) Hematopoietic cells maintain hematopoietic fates upon entering the brain. J Exp Med 201:1579-1589.
Mezey E, Chandross KJ, Harta G, Maki RA, McKercher SR (2000) Turning blood into brain: cells bearing neuronal antigens generated in vivo from bone marrow. Science 290:1779-1782.
Milligan ED, Twining C, Chacur M, Biedenkapp J, O'Connor K, Poolc S, Tracey K, Martin D, Maier SF, Watkins LR (2003) Spinal glia and proin-flammatory cytokines médiate mirror-image neuropathic pain in rats. J Neurosci 23:1026-1040.
Mogil JS, Wilson SG, Bon K, Lee SE, Chung K, Raber P, Pieper JO, Hain HS, Belknap JK, Hubert L, Elmer Gl, Chung JM, Devor M (1999) Heritabil-ity ofnociception I: responsesof 11 inbred mouse strains on 12 measures of nociception. Pain 80:67-82.
Moser B, Wolf M, Walz A, Loetscher P (2004) Chemokines: multiple levels of leukocyte migration control. Trends Immunol 25:75-84.
Priller J, Flugel A, WehnerT, Boentert M, HaasCA, Prinz M, Fernandez-Klett F, Prass K, Bechmann 1, de Boer BA, Frotscher M, Kreutzberg GW, Perdons DA, Dirnagl U (2001) Targeting gene-modiiied hematopoietic cells to the central nervous System: use of green fluorescent protein un-covers microglial engraftment. Nat Med 7:1356-1361.
Priller J, Prinz. M, Heikenwalder M, Zeller N, Schwarz P, Heppner FL, Aguzzi *\ (2006) Early and rapid engraftment of bone marrow-derived microglia in scrapie. J Neurosci 26:11753-11762.
Raghavendra V, Tanga F, DeLeo JA (2003) Inhibition of microglial activa-don atténuâtes the development but not existing hypersensitivity in a rat model of neuropathy. J Pharmacol Exp Ther 306:624-630.
Raivich G, Banati R (2004) Brain microglia and blood-derived macrophages: molecular profiles and functional rôles in multiple sclerosis and animal models of autoimmunedemyelinating disease. Brain Res Brain Res Rev 46:261-281.
Ransohoff RM, Tani M (1998) Do chemokines médiate leukocyte recruitment in post-traumatic CNS inflammation? Trends Neurosci 21:154-159.
Rebenko-Moll NM, Liu L, Cardona A, Ransohoff RM (2006) Chemokines,
mononuclear cells and the nervous System: heaven (or hell) is in the détails. CurrOpin Immunol 18:683-689.
Rot A, von Andrian UH (2004) Chemokines in innate and adaptive host défense: basic chemokinesegrammar for immune cells. Annu Rev Immunol 22:891-928.
Rutkowski MD, Pahl JL, SweitzerS, van Rooijen N, Deleo JA (2000) Limited rôle of macrophages in génération of nerve injury-induced mechanical allodynia. Physiol Behav 71:225-235.
Scholz J, Broom DC, Youn DH, Mills CD, Kohno T, Suter MR, Moore KA, Decosterd I, Coggeshall RE, Woolf CJ (2005) Blocking caspase activity prevents transsynaptic neuronal apoptosis and the loss of inhibition in lamina II of the dorsal horn after pcripheral nerve injury. J Neurosci 25:7317-7323.
Schreiber RC, Krivacic K, Kirby B, Vaccariello SA, Wei T, Ransohoff RM, Zigmond RE (2001) Monocyte chemoattractant protein (MCP)-l is rapidly expressed by sympathetic ganglion neurons following axonal injury. NeuroReport 12:601-606.
Seltzer Z, Dubner R, Shir Y (1990) A novel behavioral model of neuropathic pain disorders produced in rats by partial sciatic nerve injury. Pain 43:205-218.
Shigemoto-Mogami Y, Koizumi S, Tsuda M, Ohsawa K, Kohsaka S, Inoue K (2001) Mechanisms underlying extracellular ATP-evoked interleukin-6 release in mouse microglial cell line, MG-5. I Neuro-chem 78:1339-1349.
Shubayev VI, Myers RR (2002) Anterograde TNF alpha transport from rat dorsal root ganglion to spinal cord and injured sciatic nerve. Neurosci Lett 320:99-101.
Simard AR, Rivest S (2004) Bone marrow stem cells hâve the ability to pop-ulate the entire central nervous System into fully differentiated parenchy-mal microglia. FASEB J 18:998-1000.
Simard AR, Soulet D, Gowing G, Julien JP, Rivest S (2006) Bone marrow-derived microglia play a critical rôle in restrictingsenile plaque formation in Alzheimer's disease. Neuron 49:489-502.
Solomon JN, Lewis CA, Ajami B, Corbel SY, Rossi FM, Krieger C (2006) Origin and distribution of bone marrow-derived cells in the central nervous System in a mouse model of amyotrophic latéral sclerosis. Glia 53:744-753.
Song L, Pachter JS (2004) Monocyte chemoattractant protcin-1 alters expression of tight junction-associated proteins in brain microvascular en-dothelial cells. Microvasc Res 67:78-89.
Stamatovic SM, Keep RF, Kunkel SL, Andjelkovic AV (2003) Potential rôle of MCP-1 in endothelial cell tight jonction "opening:" signaling via Rho and Rho kinase. J Cell Sci 116:4615-4628.
Streit WJ, Graeber MB, Kreutzberg GW (1989) Expression ofla antigen on perivascular and microglial cells after sublethal and lethal motor neuron injury. Exp Neurol 105:115-126.
Sweitzer S, Martin D, DeLeo JA (2001) Intrathecal interleukin-1 receptor antagonist in combination with soluble tumor necrosis factor receptor exhibits an anti-allodynic action in a rat model of neuropathic pain. Neuroscience 103:529-539.
Sweitzer SM, Hickey WF, Rutkowski MD, Pahl JL, DeLeo JA (2002) Focal pe-ripheral nerve injury induces leukocyte trafficking into the central nervous System: potential relationship to neuropathic pain. Pain 100:163-170.
Sweitzer SM, Medicherla S, Almirez R, Dugar S, Chakravarty S, Shumilla 1A, Yeomans DC, Frotter AA (2004) Antinociceptive action of a p.38alpha MAPK inhibitor, SD-282, in a diabetic neuropathy model. Pain 109:409-419.
Tanaka T, Minami M, Nakagawa T, Satoh M (2004) Enhanced production of monocyte chemoattractant protein-1 in the dorsal root ganglia in a rat model of neuropathic pain: possible involvement in the development of neuropathic pain. Neurosci Res 48:463-469.
Tanga FY, Raghavendra V, DeLeo JA (2004) Quantitative real-time RT-PCR assessment of spinal microglial and astrocytic activation markers in a rat model of neuropathic pain. Ncurochem Int 45:397-407.
Tsuda M, Shigemoto-Mogami Y, Koizumi S, Mizokoshi A, Kohsaka S, Salter MW, Inoue K (2003) P2X4 receptors induced in spinal microglia gale tactile allodynia after nerve injury. Nature 424:778-783.
Tsuda M, Inoue K, Salter MW (2005) Neuropathic pain and spinal microglia: a big problem from molécules in "small" glia. Trends Neurosci 28:101-107.
Valente AJ, Graves DT, Vialle-Valentin CE, Delgado R, Schwartz CJ (1988)

12406 • J. Neurosci., November 7,2007 • 27(45):12396-12406 Zhang et al. • Microglia and Macrophages in Neuropathic Pain
Purification of a monocyte chemotactic factor secreted by noniiuman primate vascular cells in culture. Biochemistry 27:4162-4168.
Valiieres L, Sawchenko PE (2003) Bone marrow-derived cells that populate tbc adult mouse brain préserve their hematopoietic identity. J Neurosci 23:5197-5207.
Verge GM, Milligan ED, Maier SF, Watkins LR, Naeve GS, Foster AC (2004 ) Fractalkine (CX3CL1) and fractalkine receptor (CX3CR1) distribution in spinal cord and dorsal root ganglia under basai and neuropathic pain conditions. Eur | Neurosci 20:1150-1160.
White FA, Sun J, Waters SM, Ma C, Ren U, Ripsch M, Steflik J, Cortright DN, Lamotte RH, Miller RJ (2005) Excitatory monocyte chemoattractant protein-1 signaling is up-regulated in sensory neurons after chronic compression of the dorsal root ganglion. Proc Natl Acad Sci USA 102:14092-14097.
Wright DE, Wagers Al, Gulati AP, Johnson FL, Weissman IL (2001) Physi-ological migration ot hematopoietic stem and progenitor cells. Science 294:1933-1936.
YoshimuraT, Robinson EA, AppellaE, Matsushima K,ShowalterSD,Skeel A, Léonard EJ (1989) Thrce forms of monocyte-derived neutrophil chemotactic factor (MDNCF) distinguished by différent lengths of the amino-terminal séquence. Mol Immunol 26:87-93.
Zhang |, De Koninck Y (2006) Spatial and temporal relationship between monocyte chemoattractant protein-1 expression and spinal glial activation following peripheral nerve injury. J Neurochem 97:772-783.
Zhang J, Hoffert C, Vu HK, Groblewski T, Ahmad S, O'Donnell D (2003) Induction of CB2 receptor expression in the rat spinal cord of neuropathic but not inflammatory chronic pain models. Eur | Neurosci 17: 2750-2754.