Embed Size (px)
Citation preview

Quels traitements Quels traitements antithrombosants antithrombosants
dans les SCA ?dans les SCA ?
G de GevigneyG de Gevigney Hôpital CardiologiqueHôpital Cardiologique
Lyon, FranceLyon, France
Journées de l’AFL Journées de l’AFL BeyrouthBeyrouth
11-12 mai 200711-12 mai 2007

IntroductionIntroduction
Aspirine Aspirine
Héparine Héparine
Clopidogrel Clopidogrel
HBPMHBPM
ThrombolytiquesThrombolytiques
Anti GP2B3AAnti GP2B3A
FondaparinuxFondaparinux
BivalirudineBivalirudine

Best-of 2004 des Best-of 2004 des valvulopathiesvalvulopathies
Les acquis Les acquis dans les SCA dans les SCA
ST+ et ST-ST+ et ST-

6/046/04
00 1.01.0 2.02.0 Favors PlaceboFavors Aspirin
Cairns
Lewis
Theroux
Wallentin
Pooled
Cairns
Lewis
Theroux
Wallentin
Pooled
Relative Risk — Death or MIRelative Risk — Death or MI
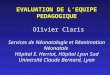
Acute Coronary Syndromes Without ST Acute Coronary Syndromes Without ST Evidence for Evidence for AspirinAspirin

6/046/04Oler A, JAMA 1996Oler A, JAMA 1996Oler A, JAMA 1996Oler A, JAMA 1996
Acute Coronary Syndromes without ST Acute Coronary Syndromes without ST Evidence for Evidence for HeparinHeparin Use (UFH + ASA versus ASA) Use (UFH + ASA versus ASA)
Relative Risk of Death or MIRelative Risk of Death or MIRelative Risk of Death or MIRelative Risk of Death or MI
Theroux (n = 243)
RISC (n = 399)
Cohen (n = 69)
Cohen (n = 214)
Holdright (n = 185)
Gurfinkel (n = 143)
Overall (n = 1353)
Theroux (n = 243)
RISC (n = 399)
Cohen (n = 69)
Cohen (n = 214)
Holdright (n = 185)
Gurfinkel (n = 143)
Overall (n = 1353)
0.50.5 11 1.51.5 22ASA + UFH BetterASA + UFH Better ASA BetterASA Better
00
2.662.66
6.876.87
P = 0.06P = 0.06

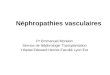
Clopidogrel Critère de jugement principal tous patients
20% RRR20% RRRpp=0.00009=0.00009n=12 562n=12 562
20% RRR20% RRRpp=0.00009=0.00009n=12 562n=12 562
Le bénéfice apparait dès les premières Le bénéfice apparait dès les premières heures et continue de croître à 12 moisheures et continue de croître à 12 mois
00 11 22 33 44 55 66 77 88 99 1010 1111 1212Suivi en moisSuivi en mois
% de patients présentant un événement ischémique% de patients présentant un événement ischémique( décès vasculaire, IDM, AVC)( décès vasculaire, IDM, AVC)
00
1010
1414
1212
44
88
66
22
Traitement standardTraitement standardClopidogrel + traitement standardClopidogrel + traitement standard
The CURE Investigators. The CURE Investigators. N Eng J Med N Eng J Med August 2001August 2001

Résultats à long terme de la randomisation à la fin du suivi
0.150.15
0.100.10
0.050.05
0.00.0
10100 4040 100100 200200 300300 400400
Cumulative hazard ratesCumulative hazard rates
31% RRR31% RRRpp=0.002=0.002n=2658n=2658
31% RRR31% RRRpp=0.002=0.002n=2658n=2658
Jours de suiviJours de suiviaa bb
a = délais médian randomisation /ACP (10 jours)a = délais médian randomisation /ACP (10 jours)b = 30 jours aprés ACPb = 30 jours aprés ACP
Tt conventionnelTt conventionnelClopidogrel + tt conventionnelClopidogrel + tt conventionnel
12.6%12.6%
8.8%8.8%
CritéreCritére: IDM + décès vasculaire: IDM + décès vasculaire
PCI-PCI-

Les acquis dans les SCALes acquis dans les SCA
ThrombolytiquesThrombolytiques
SCA ST +SCA ST +
échec dans SCA ST -échec dans SCA ST -
AntiGP-IIB-IIIAAntiGP-IIB-IIIA
SCA ST -SCA ST -

Best-of 2004 des Best-of 2004 des valvulopathiesvalvulopathiesHBPMHBPM

IDM ST+EXTRACT TIMI 25
HBPMHBPM
Antmann EM NEJM 2006 354
IDM ST+
20056 pts
fibrinolyse
HNFdurant 48H
ENOXAPARINE Bolus IV puis 1mg/kg SC 2 fois par jour si
< 75ans pas bolus et 0.75mg/kg si >75ansdurant toute l’hospitalisation
randomisée, double aveugle
30 joursCritères 1aires: décès et IDM
Critères IIaires : hémorragies majeures
Exclusion : chocExclusion : choccréatcréat>220>220

0
3
6
9
12
15
0 5 10 15 20 25 30
Pri
ma
ry E
nd
Po
int
(%)
Pri
ma
ry E
nd
Po
int
(%)
ENOX
UFH
Days Days
9.9%(1017)
12.0%(1223)
4.7%
5.2%
RRRR0.90 0.90
(0.80 to 1.01)(0.80 to 1.01)
P=0.08P=0.08
48 h48 h
UFH ENOX
206 events
Relative RiskRelative Risk0.83 (0.77 to 0.90)0.83 (0.77 to 0.90)
P<0.0001P<0.0001
ST + : Primary End Point ST + : Primary End Point Death or Nonfatal MIDeath or Nonfatal MI

Bleeding Endpoints (TIMI) Bleeding Endpoints (TIMI) 30 Days30 Days
1,4 0,9 0,7
2,11,3 0,8
0
2
4
6
8
10 UFHUFHENOXENOX
%
% E
ven
tsE
ven
ts
Major BleedMajor Bleed(fatal + nonfatal)(fatal + nonfatal)
ICH ICH
ARD 0.7%ARD 0.7%RR 1.53RR 1.53
P<0.0001P<0.0001
ARD 0.1%ARD 0.1%RR 1.27RR 1.27
P = 0.14P = 0.14
NonfatalNonfatalMajor BleedMajor Bleed
ARD 0.4%ARD 0.4%RR 1.39RR 1.39
P = 0.014P = 0.014

Méta analyse HBPM vs HNF: ST+ thrombolysé
Eikelboom JW et Al Circulation 2005

Méta analyse HBPM vs HNF ST+ thrombolysé
Eikelboom JW et Al Circulation 2005
Outcomes during hospitalization/at 7 days with
LMWH vs UFH End point LMW
HUFH Odd
s ratio
95% CI
Reinfarction (%) 3.0 5.2 0.57 0.45-0.73
Death (%) 4.8 5.3 0.92 0.74-1.13
Major bleeding (%)
3.3 2.5 1.30 0.98-1.72
Minor bleeding (%)
22.8 19.4 1.26 1.12-1.43

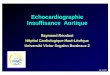
SCA ST- décès ou infarctus à 30 jours
saignements majeurs : pas de différence significative
HBPMHBPM
Elkelboom Lancet 2000; 355: 1936

SCA ST- SYNERGY9978 patients SCA ST- randomisés HNF vs enoxaparine avec 92% patients
coronarographiés
HBPMHBPM
Ferguson J JAMA 2004 252 :45-54
Décès et IDM à30 jours
0 5 10 15 20 25 300.8
0.85
0.9
0.95
1.0
% p
atie
nts
sans
déc
ès n
i ID
M
Jours après randomisation
UFHUFHEnoxaparinEnoxaparin
30-Day Death/MI30-Day Death/MI
0.80.8 11 1.21.2
Hazard Ratio (95% CI)
Enoxaparin
Better
UFH
Better

15,913,3
0
5
10
15
20
Death or MI at 30 Days
UFH
ENOXAPARIN
Efficacy and Safety Outcomes With Consistent Therapy (Including
Crossovers)
18%18% RRRRRR
Pat
ien
ts (
%)
Pat
ien
ts (
%)
HR [95%]HR [95%]0.82 [0.73-0.95]0.82 [0.73-0.95]
®
SYNERGY Trial Investigators. JAMA. 2004;292:45-54.
HR=hazard ratio.
UFH ENOX

SCA ST- SYNERGYComplications hémorragiques
HBPMHBPM
Ferguson J JAMA 2004 252 :45-54
Enoxaparin UFH(n = 4993) (n = 4985) P-
value
GUSTO severe 2.9 2.40.106
TIMI major - clinical: 9.1 7.60.008 CABG-related 6.8 5.90.081 Non-CABG-related 2.4 1.80.025 H/H drop - algorithm 15.2 12.50.001
Any RBC transfusion 17.0 16.00.155
ICH < 0.1 < 0.1 NS

Chez patients avec SCA ST- HBPM au moins aussi efficace qu’HNF; avantages :
. administration SC
. pas surveillance coagulation
. meilleure prédictibilité et stabilité traitement
Chez Patients avec IDM ST+ avant 75 ans utilisation possible
HBPMHBPM

Best-of 2004 des Best-of 2004 des valvulopathiesvalvulopathiesAntiGP IIB III AAntiGP IIB III A


Best-of 2004 des Best-of 2004 des valvulopathiesvalvulopathiesFondaparinuxFondaparinux

Rappels
AnticoagulantsAnticoagulants
XIIa
XIa
IXa
Voie intrinsèque
Xa
Voie extrinsèque(facteur tissulaire)
VIIa
Thrombine (IIa)
Héparine / HBPMAT-III dépendant)
Hirudine/Hirulogbivalirudine
Antithrombine exclusifs polysaccharidesfondaparinux
Agents anti Xa exclusifs
Thrombine-Fibrine

Fondaparinux
pentasaccharide synthétique
élimination rénale
demi-vie d’élimination 17-21H
contre-indication : insuffisance rénale sévère
pas de cas de thrombopénie induite décrite pas de
surveillance numération plaquettaire
Anti-XaAnti-Xa

Patients with NSTE ACS, Chest discomfort < 24 hours2 of 3: Age>60, ST Segment Δ, cardiac markers
Patients with NSTE ACS, Chest discomfort < 24 hoursPatients with NSTE ACS, Chest discomfort < 24 hours2 of 3: Age>60, ST Segment 2 of 3: Age>60, ST Segment ΔΔ, , cardiac markerscardiac markers
Fondaparinux2.5 mg sc once daily
FondaparinuxFondaparinux2.5 mg sc once daily2.5 mg sc once daily
Study Design: Randomized, Double Blind
ASA, Clop, GP IIb/IIIa, planned Cath/PCI as per
local practice
ASA, Clop, GP ASA, Clop, GP IIb/IIIaIIb/IIIa, , planned planned CathCath/PCI as per /PCI as per
local practicelocal practice
RandomizeRandomize
Enoxaparin1 mg/kg sc twice daily
EnoxaparinEnoxaparin1 mg/kg sc twice daily1 mg/kg sc twice daily
Primary: Efficacy: Death, MI, refractory ischemia at 9 days Safety: Major bleeding at 9 daysRisk benefit: Death, MI, refractory ischemia, major bleeds 9 days
Secondary: Above & each component separately at day 30 & 6 monthsHypothesis: First test non-inferiority, then test superiority
Primary:Primary: EfficacyEfficacy:: Death, MI, refractory ischemiaDeath, MI, refractory ischemia at 9 days at 9 days SafetySafety:: Major bleeding at 9 daysMajor bleeding at 9 daysRisk benefitRisk benefit:: Death, MI, refractory ischemia, major bleeds 9 daysDeath, MI, refractory ischemia, major bleeds 9 days
SecondarySecondary:: Above & each component Above & each component separatelyseparately at day 30 & 6 monthsat day 30 & 6 monthsHypothesisHypothesis:: First test nonFirst test non--inferiority, then test superiorityinferiority, then test superiority
Outcomes
PCI< 6 hPCI< 6 h,, No additional UFHNo additional UFHPCI >6 hPCI >6 h,, IV UFHIV UFHWith With IIb/IIIaIIb/IIIa 65 U/kg65 U/kgWithout Without IIb/IIIaIIb/IIIa 100 U/kg100 U/kg
PCI <6 hPCI <6 h:: IV Fonda 2.5 mgIV Fonda 2.5 mgwithout without IIb/IIIaIIb/IIIa, 0 with , 0 with IIb/IIIaIIb/IIIaPCI> 6 hPCI> 6 h:: IV Fonda 2.5 mg withIV Fonda 2.5 mg withand 5.0 mg without and 5.0 mg without IIb/IIIaIIb/IIIa
ExcludeAge < 21Any contra-ind to EnoxHem stroke< 12 mo.Creat> 3 mg/dL/265 umol/L
N=20,000

Death/MI/RI: Day 9
Days
Cum
ulat
ive
Haz
ard
0.0
0.01
0.02
0.03
0.04
0.05
0.06
0 1 2 3 4 5 6 7 8 9
Enoxaparin
Fondaparinux
HR 1.01 95% CI 0.90-1.13

Major Bleeding: 9 Days
Days
Cu
mu
lati
ve H
azar
d
0.0
0.01
0.02
0.03
0.04
0 1 2 3 4 5 6 7 8 9
HR 0.53 95% CI 0.45-0.62
P<<0.00001
Enoxaparin
Fondaparinux

Death or MI: 6 Months
Days
Cu
mu
lati
ve H
aza
rd
0.0
0.02
0.04
0.06
0.08
0.10
0.12
0 20 40 60 80 100 120 140 160 180
HR 0.91HR 0.9195% CI 0.8495% CI 0.84--0.990.99
P=0.036P=0.036
Enoxaparin
Fondaparinux

FondaparinuxFondaparinux
CONCLUSION OASIS 5
• efficacité similaire fondaparinux/enoxaparine
• réduction hémorragies avec fondaparinux entrainant diminution mortalité
• limites : seulement 60% patients coronarographiés, 33% population a eu une ATL
groupe enoxaparine a reçu HNF pour angioplastie 65% patients sous clopidogrel lors angioplastie cas thrombus dans cathéter
YUSUF S NEJM 2006 1464-76

12,000 Patients with STEMI < 12 h of symptom onsetInclusion: ST 2 mm prec leads or 1 mm limb leads
Exclusion: Contra-ind. for anticoagulant, INR>1.8, pregnancy, ICH<12 mo.
12,000 Patients with STEMI < 12 h of symptom onsetInclusion: ST 2 mm prec leads or 1 mm limb leads
Exclusion: Contra-ind. for anticoagulant, INR>1.8, pregnancy, ICH<12 mo.
UFH UFH notnot indicated indicatedUFH UFH notnot indicated indicated
OASIS 6: Randomized, Double Blind, Double Dummy
Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion (eg. late)Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion (eg. late)Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion (eg. late)Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion (eg. late)
StratificationStratificationStratificationStratification
UFH indicatedUFH indicatedUFH indicatedUFH indicated
Randomization Randomization
Fondaparinux2.5 mg Placebo
Fondaparinux2.5 mg UFH

Primary Efficacy OutcomeDeath/MI at 30 Days
Days
Cum
ulat
ive
Haz
ard
0.0
0.02
0.04
0.06
0.08
0.10
0.12
0 3 6 9 12 15 18 21 24 27 30
UFH/Placebo
Fondaparinux
HR 0.86 95% CI 0.77-0.96
P = 0.008

Death at Study End (3 or 6 months)
Days
Cum
ulat
ive
Haz
ard
0.0
0.02
0.04
0.06
0.08
0.10
0.12
0 18 36 54 72 90 108 126 144 162 180
UFH/Placebo
Fondaparinux
HR 0.88 95% CI 0.79-0.99
P = 0.029

Severe hemorrhage at 30 days

FondaparinuxFondaparinux
YUSUF S JAMA 2006 1519-30
OASIS 6
randomisation complexe
fondaparinux pas supérieure à l’HNF
plus complications lors angioplastie groupe fondaparinux
intérêt fondaparinux si pas de revascularisation par angioplastie envisagée

Best-of 2004 des Best-of 2004 des valvulopathiesvalvulopathiesBivalirudineBivalirudine

Rappels
AnticoagulantsAnticoagulants
XIIa
XIa
IXa
Voie intrinsèque
Xa
Voie extrinsèque(facteur tissulaire)
VIIa
Thrombine (IIa)
Héparine / HBPMAT-III dépendant)
Hirudine/Hirulogbivalirudine
Antithrombine exclusifs polysaccharidesfondaparinux
Agents anti Xa exclusifs
Thrombine-Fibrine

Moderateand highrisk ACS
(n=13,819)
Study Design – First RandomizationStudy Design – First Randomization
An
gio
gra
ph
y w
ith
in 7
2h
Aspirin in allClopidogrel
dosing and timingper local practice
Aspirin in allClopidogrel
dosing and timingper local practice
UFH/Enox+ GP IIb/IIIa(n=4,603)
Bivalirudin+ GP IIb/IIIa(n=4,604)
BivalirudinAlone
(n=4,612)
R*
*Stratified by pre-angiography thienopyridine use or administration*Stratified by pre-angiography thienopyridine use or administration
Moderate and high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,819)
Moderate and high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,819)
Medicalmanagement
PCI
CABG
56%
11%
33%

Study Design – Second RandomizationStudy Design – Second Randomization
UFH/Enox+ GP IIb/IIIa(N=4,603)
Bivalirudin+ GP IIb/IIIa(N=4,604)
BivalirudinAlone
(N=4,612)
R*
GPI upstream (N=2294)
GPI CCL for PCI (N=2309)
GPI upstream (N=2311)
GPI CCL for PCI (N=2293)
Aspirin in allClopidogrel
dosing and timingper local practice
Aspirin in allClopidogrel
dosing and timingper local practice
*Stratified by pre-angiography thienopyridine use or administration*Stratified by pre-angiography thienopyridine use or administration
Moderateand highrisk ACS(n=13,819
Moderate and high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,819)
Moderate and high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,819)

0 30 60 90 120 150 180 210 240 270 300 330 360 3900
5
15
25
Isch
emic
Co
mp
osi
te (
%)
Days from Randomization
10
20 UFH/Enoxaparin + IIb/IIIaBivalirudin + IIb/IIIa
Bivalirudin alone
EstimateP
(log rank)
30 day
7.4%0.367.8%0.347.9%
—
EstimateP
(log rank)
16.3%0.3816.5%0.3116.4%
1 year
—
p=0.55
Bivalirudin alone vs. Hep+GPIHR [95% CI] = 1.05 (0.95-1.17)
Bivalirudin+GPI vs. Hep+GPIHR [95% CI] = 1.05 (0.94-1.16)
Ischemic Composite Endpoint(Death, MI, unplanned revascularization for ischemia)
Ischemic Composite Endpoint(Death, MI, unplanned revascularization for ischemia)
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone

Myocardial InfarctionMyocardial Infarction
0 30 60 90 120 150 180 210 240 270 300 330 360 3900
5
10
15
Days from Randomization
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone
UFH/Enoxaparin + IIb/IIIaBivalirudin + IIb/IIIa
Bivalirudin alone
EstimateP
(log rank)
30 day
4.4%0.694.6%0.364.8%
—
EstimateP
(log rank)
6.2%0.636.4%0.107.1%
1 year
—
p=0.24
MI
(%)

0 30 60 90 120 150 180 210 240 270 300 330 360 3900
4
5
Mo
rtal
ity
(%)
Days from Randomization
2
1
Mortality: 524 total deaths at 1-yearMortality: 524 total deaths at 1-yearUFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone
UFH/Enoxaparin + IIb/IIIaBivalirudin + IIb/IIIa
Bivalirudin alone
EstimateP
(log rank)
1.4%0.531.6%0.391.6%
—
EstimateP
(log rank)
4.4%0.934.2%0.663.8%
1 year
—
p=0.90
Bivalirudin+GPI vs. Hep+GPIHR [95% CI] = 0.99 (0.80-1.22)
30 day
3
Bivalirudin alone vs. Hep+GPIHR [95% CI] = 0.95 (0.77-1.18)

Mo
rtal
ity
(%)
Days from Randomization
0 30 60 90 120 150 180 210 240 270 300 330 360 3900
5
15
30
10
25
20
1 yearEstimate
Major Bleed only (without MI) (N=551) 12.5%28.9%Both MI and Major Bleed (N=94)
3.4%No MI or Major Bleed (N=12,557)MI only (without Major Bleed) (N=611) 8.6%
Impact of MI and Major Bleeding (non-CABG) in the First 30 Days on Risk of Death Over 1 Year
28.9%
12.5%
8.6%
3.4%

ConclusionsConclusions• In patients with moderate and high risk ACS
undergoing an early invasive strategy with the use of GP IIb/IIIa inhibitors
• Bivalirudin is an acceptable substitute for either unfractionated heparin or enoxaparin
• Compared to either UFH/enoxaparin with GP IIb/IIIa inhibitors or bivalirudin with GP IIb/IIIa inhibitors
• A bivalirudin alone strategy results in marked reduction of bleeding at 30 days, and similar rates of mortality and composite ischemia at 1-year
• The results of this study further establish the important relationship between iatrogenic bleeding complications and subsequent mortality in patients with ACS

Recommandations actuellesRecommandations actuelles
Maladie
coronarienneIDM ST+ACC ESC
SCA ST-ACC ESC
HNF 1C 1B 1A 1B
HBPM 2B - 1A 1A
HBPM préférée à
HNF - - 2A 2A
si enoxaparine

ConclusionsConclusions
• pas de recommendations par rapport fondaparinux et bivalirudine
• important de prendre en compte le risque hémorragique

Best-of 2004 des Best-of 2004 des valvulopathiesvalvulopathiesCONCLUSIONSCONCLUSIONS

Prise en charge des SCA sans élévation du segment ST