Embed Size (px)
Citation preview

saint antoine
Toxicité cardiaque des chimiothérapies
Journée de l’AIH
24 Septembre 2016
Dr Stéphane Ederhy
Service de Cardiologie Hôpital Saint Antoine
Hôpitaux Universitaire Est Parisien
saint antoine Mr M, 62 ans
Vous recevez en consultation Mr M, 62 ans, que vous suivez pour un myélome multiple Il a bénéficié d’une chimiothérapie d’induction comportant 2 cycles ( Bortézomib , Dexamethasone et Thalidomide), en attente du 3 eme cycle ATCD médicaux : 0 ATCD chirurgicaux : 0 FDRCV : Dyslipidémie traitée, HTA traitée Traitement : Atorvastatine, Amlodipine Il se plaint depuis 1 semaine d’une dyspnée d’effort croissante et d’épisode de chute à répétitions survenant au lever
saint antoine
L’examen clinique retrouve : PA : 92 / 58 mm Hg ; FR = 25 /mn, Sat = 94 % en AA BDC irréguliers avec un SS 3/6 FA Crépitants aux bases OMI , RHJ , THJ
saint antoine Cardiotoxicity in Hematology
Peripheral Artery disease
Pulmonary Hypertension
saint antoine
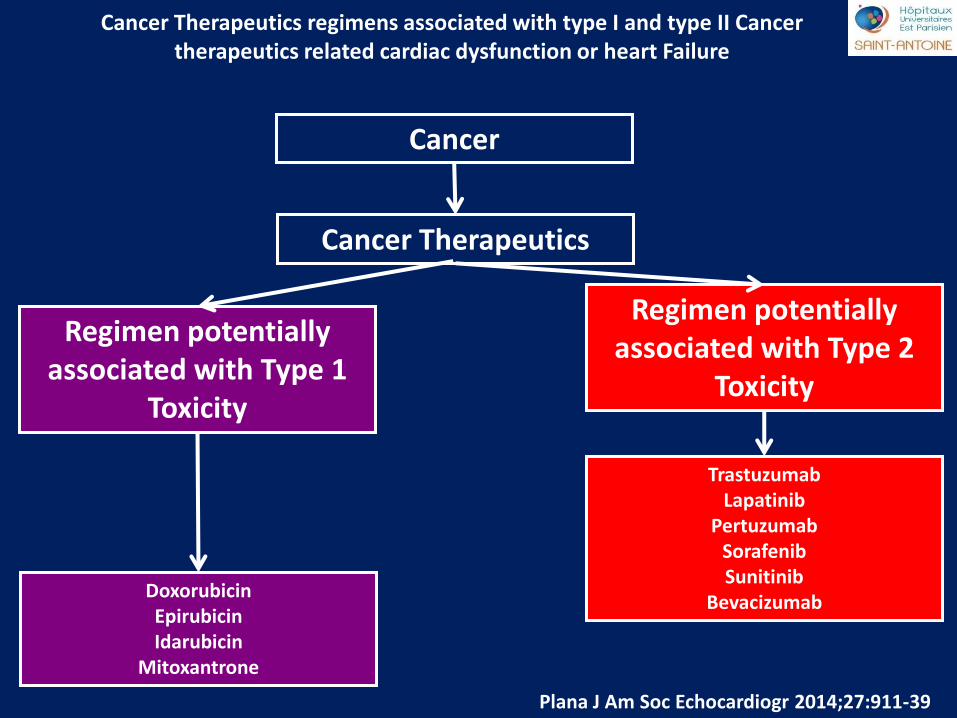
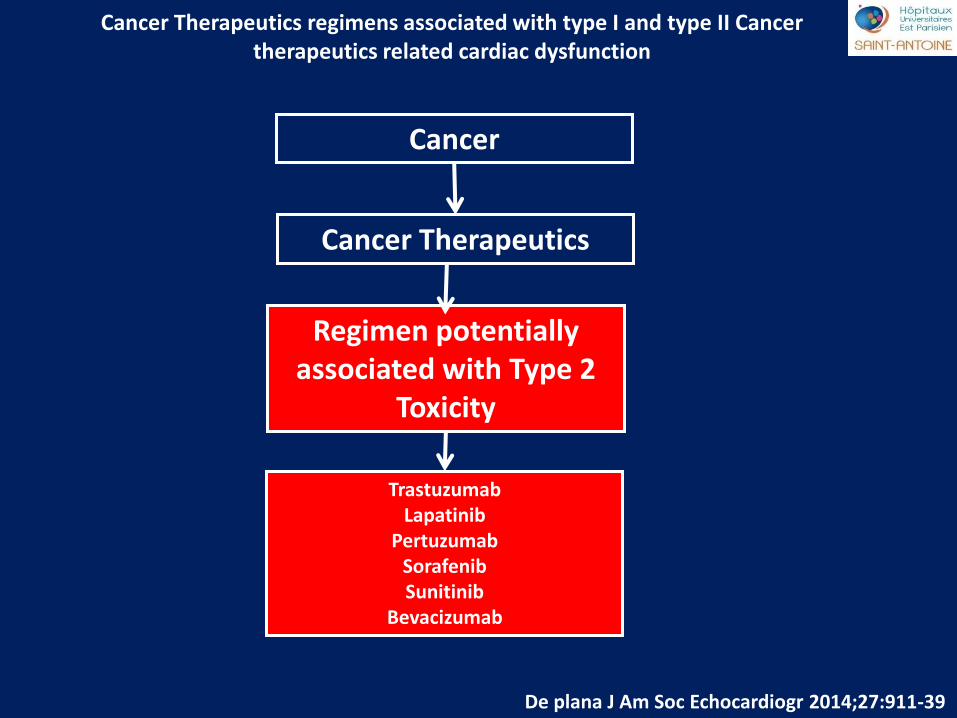
Cancer Therapeutics regimens associated with type I and type II Cancer therapeutics related cardiac dysfunction or heart Failure
Cancer
Cancer Therapeutics
Regimen potentially associated with Type 1
Toxicity
Doxorubicin Epirubicin Idarubicin
Mitoxantrone
Regimen potentially associated with Type 2
Toxicity
Trastuzumab Lapatinib
Pertuzumab Sorafenib Sunitinib
Bevacizumab
Plana J Am Soc Echocardiogr 2014;27:911-39
saint antoine
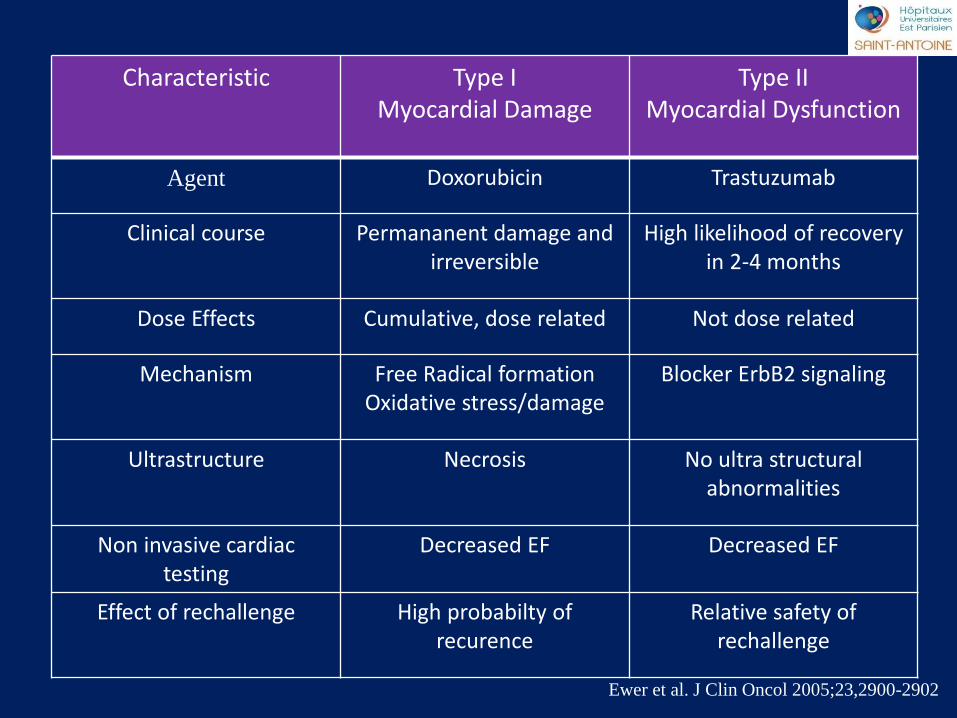
Ewer et al. J Clin Oncol 2005;23,2900-2902
Characteristic Type I Myocardial Damage
Type II Myocardial Dysfunction
Agent Doxorubicin Trastuzumab
Clinical course Permananent damage and irreversible
High likelihood of recovery in 2-4 months
Dose Effects Cumulative, dose related Not dose related
Mechanism Free Radical formation Oxidative stress/damage
Blocker ErbB2 signaling
Ultrastructure Necrosis No ultra structural abnormalities
Non invasive cardiac testing
Decreased EF Decreased EF
Effect of rechallenge High probabilty of recurence
Relative safety of rechallenge
saint antoine
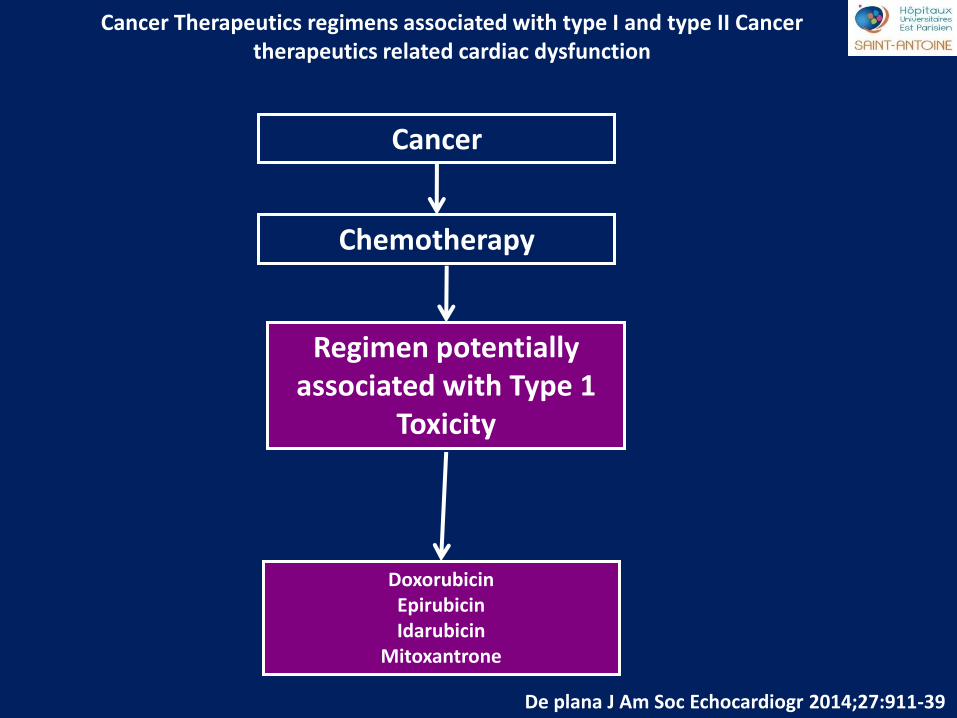
Cancer Therapeutics regimens associated with type I and type II Cancer therapeutics related cardiac dysfunction
Cancer
Chemotherapy
Regimen potentially associated with Type 1
Toxicity
Doxorubicin Epirubicin Idarubicin
Mitoxantrone
De plana J Am Soc Echocardiogr 2014;27:911-39
saint antoine
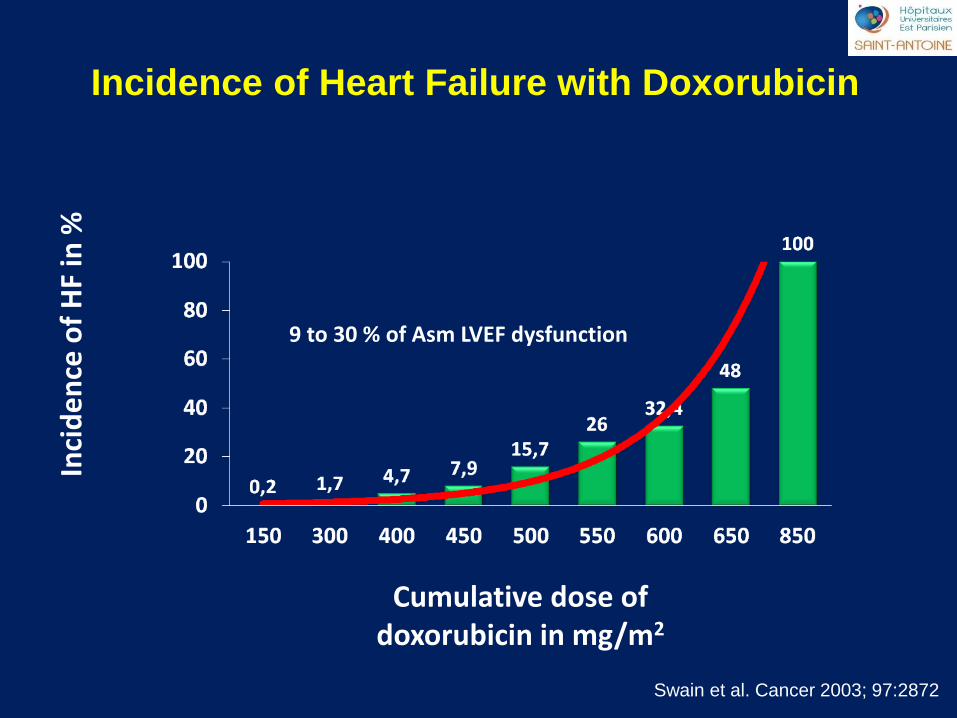
Swain et al. Cancer 2003; 97:2872
Incidence of Heart Failure with Doxorubicin
Cumulative dose of doxorubicin in mg/m2
Inci
de
nce
of
HF
in %
9 to 30 % of Asm LVEF dysfunction
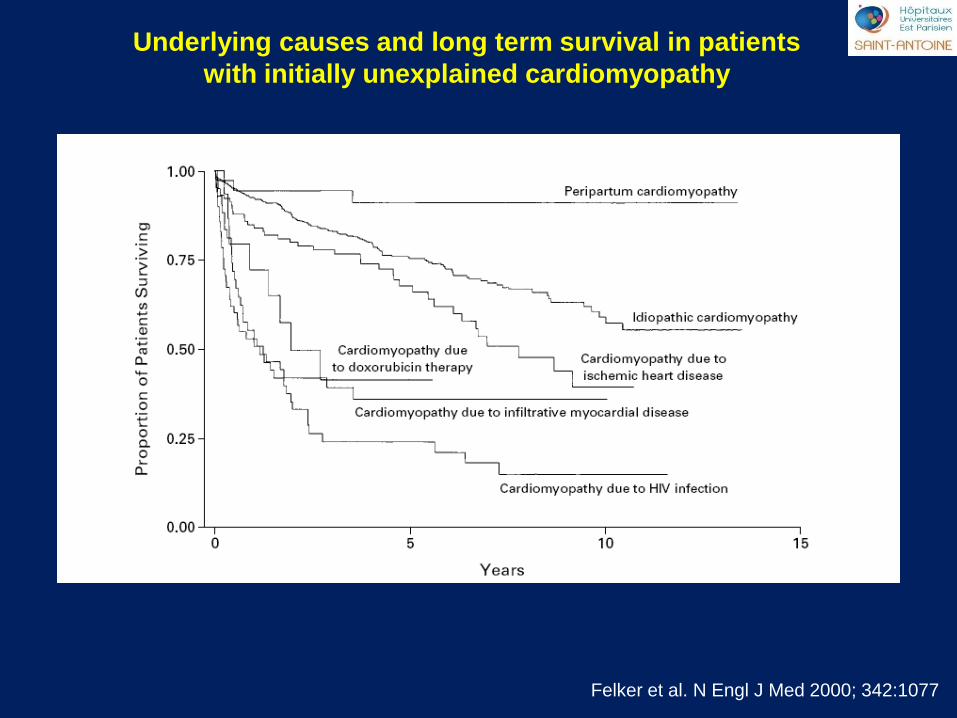
saint antoine Underlying causes and long term survival in patients
with initially unexplained cardiomyopathy
Felker et al. N Engl J Med 2000; 342:1077
saint antoine
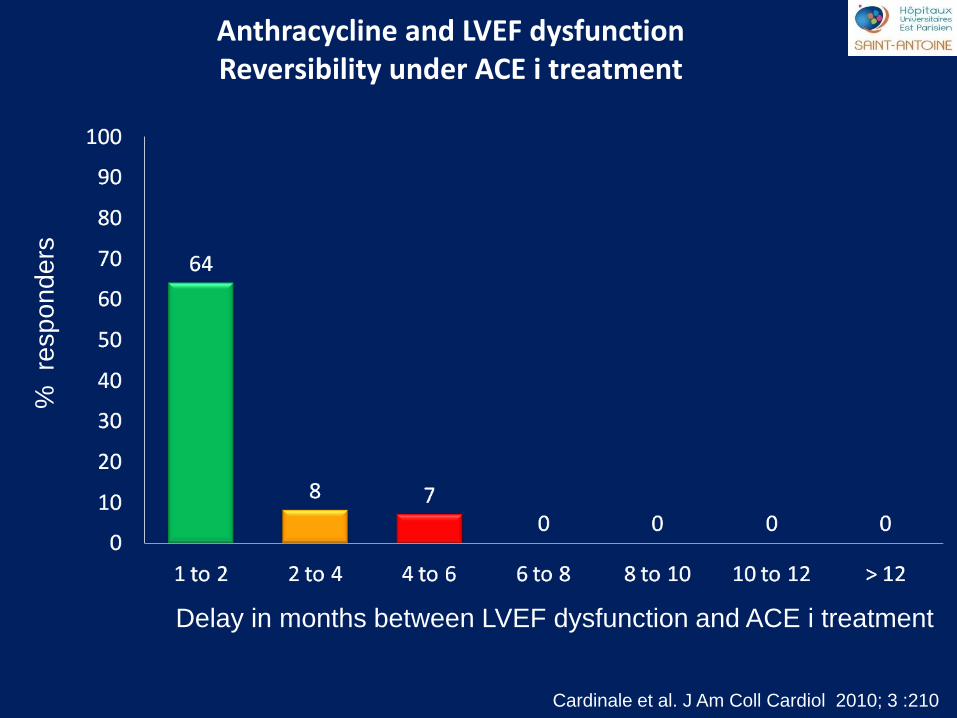
Cardinale et al. J Am Coll Cardiol 2010; 3 :210
Delay in months between LVEF dysfunction and ACE i treatment
% re
sp
on
de
rs
Anthracycline and LVEF dysfunction Reversibility under ACE i treatment
saint antoine
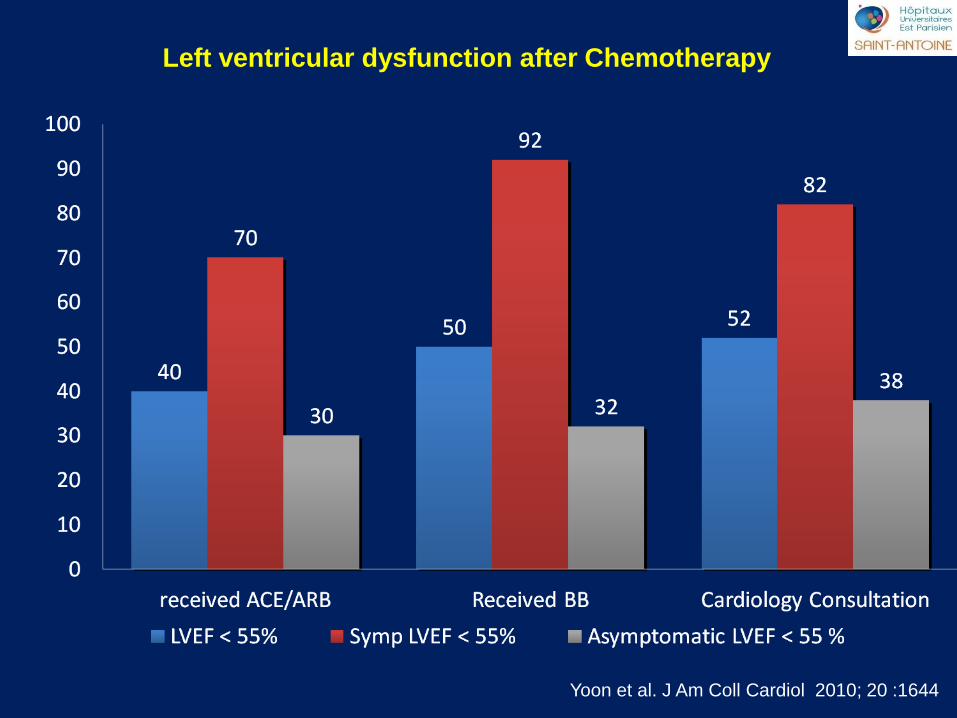
Left ventricular dysfunction after Chemotherapy
Yoon et al. J Am Coll Cardiol 2010; 20 :1644
saint antoine
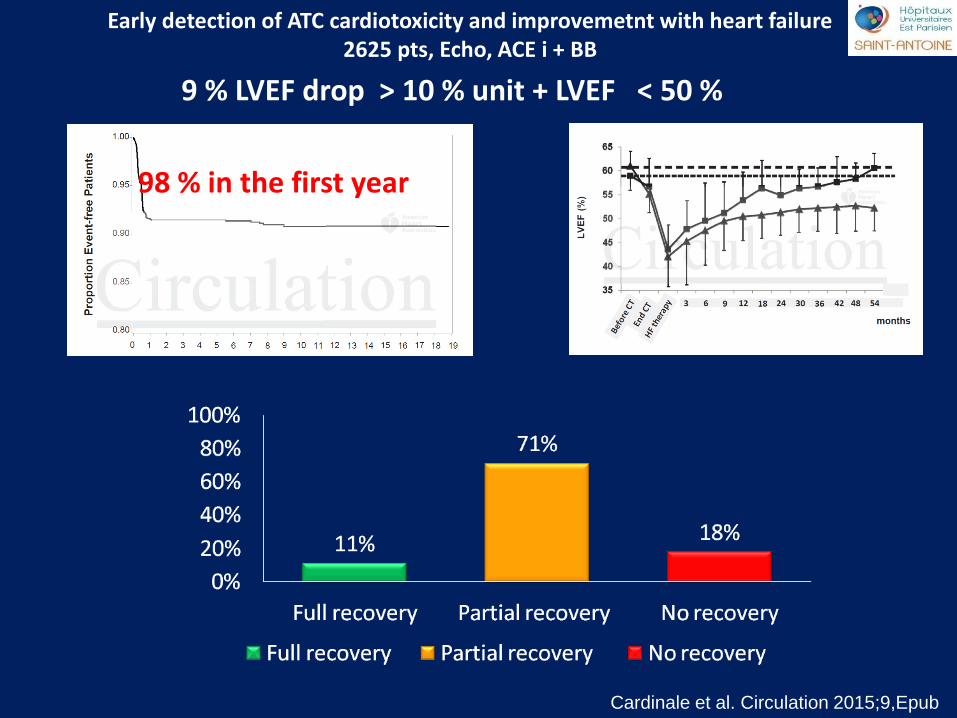
Cardinale et al. Circulation 2015;9,Epub
Early detection of ATC cardiotoxicity and improvemetnt with heart failure 2625 pts, Echo, ACE i + BB
9 % LVEF drop > 10 % unit + LVEF < 50 %
98 % in the first year
saint antoine
Pre-existing Risk Factors for
Cardiac Damages
Angina pectoris
Arterial hypertension
Valvulopathy
Radiotherapy < 6 months
Ethnicity
Age < 15 years ; Age > 70 years
Cumulative Dose
Combination with vincristine,
cyclophosphamide, mitomycin,
mithramycin, trastuzumab
saint antoine
Detecting cardiotoxicity
LVEF Other Echo tools ? TDI , STE
Biomarkers
saint antoine
Detecting cardiotoxicity
LVEF Other Echo tools ? TDI , STE
saint antoine
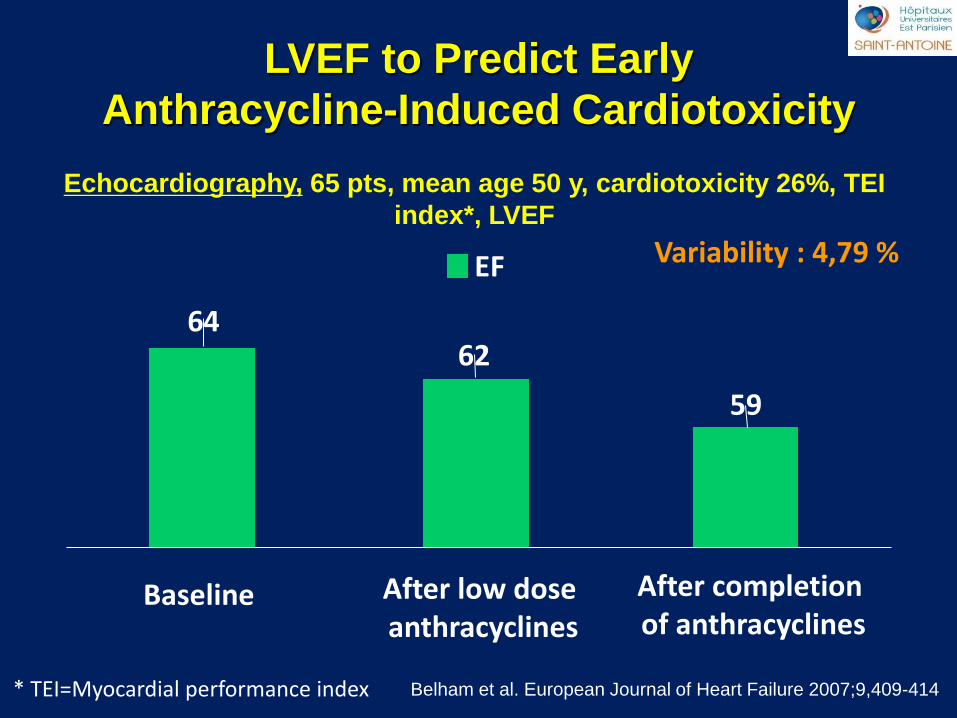
LVEF to Predict Early
Anthracycline-Induced Cardiotoxicity
Echocardiography, 65 pts, mean age 50 y, cardiotoxicity 26%, TEI
index*, LVEF
Variability : 4,79 %
Belham et al. European Journal of Heart Failure 2007;9,409-414 * TEI=Myocardial performance index
Baseline After low dose anthracyclines
After completion of anthracyclines
64 62
59
EF
saint antoine
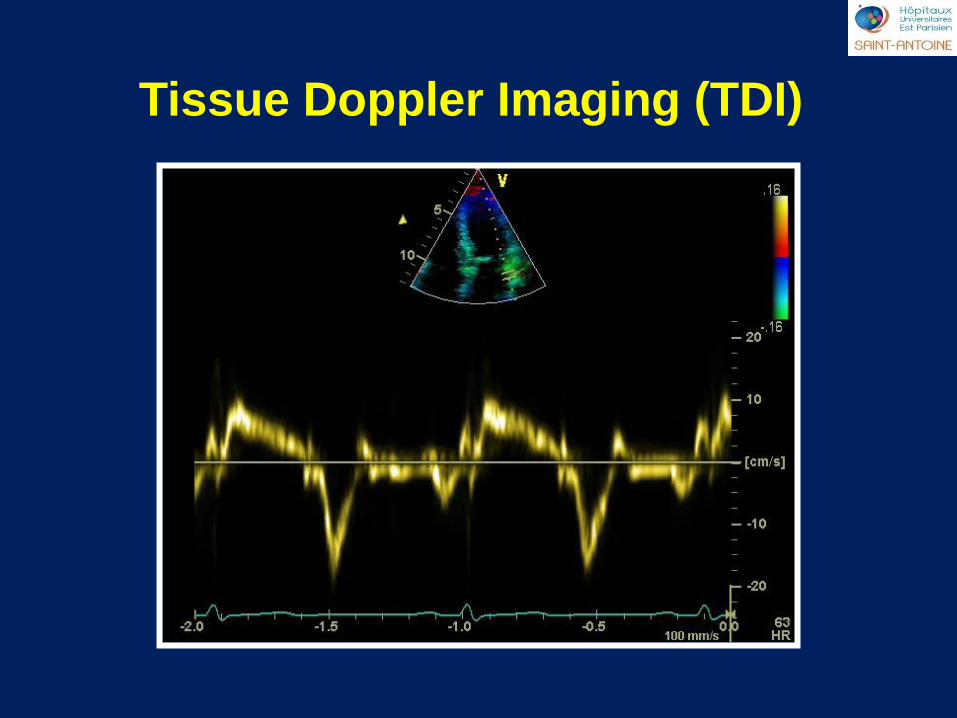
Tissue Doppler Imaging (TDI)
saint antoine
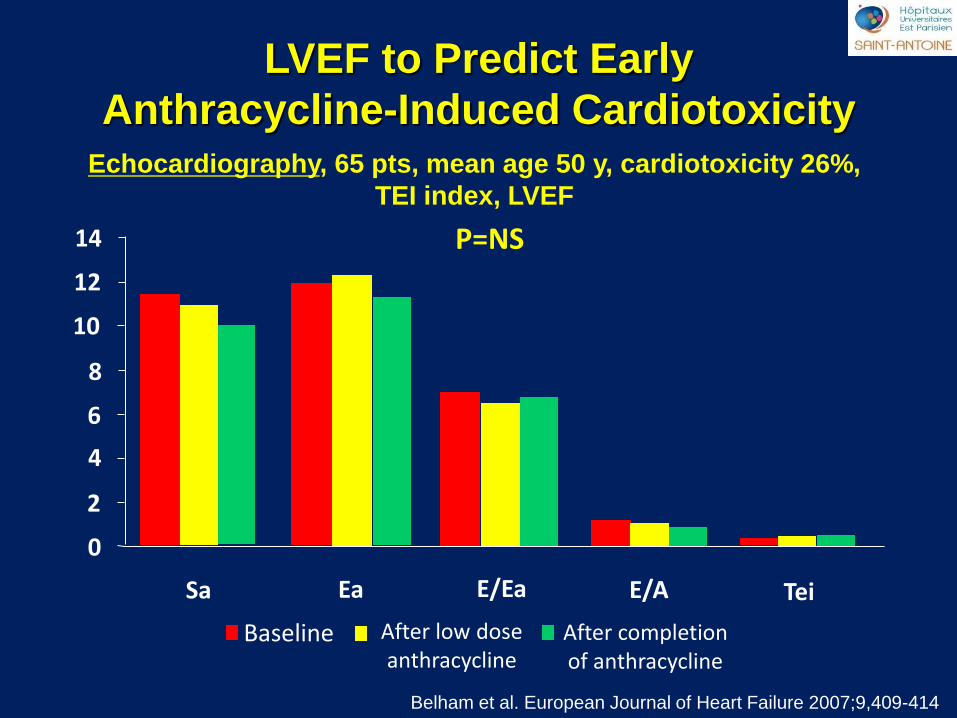
P=NS
Belham et al. European Journal of Heart Failure 2007;9,409-414
Echocardiography, 65 pts, mean age 50 y, cardiotoxicity 26%,
TEI index, LVEF
LVEF to Predict Early
Anthracycline-Induced Cardiotoxicity
0
2
4
6
8
10
12
14
Tei
Baseline After low dose anthracycline
After completion of anthracycline
Sa Ea E/Ea E/A
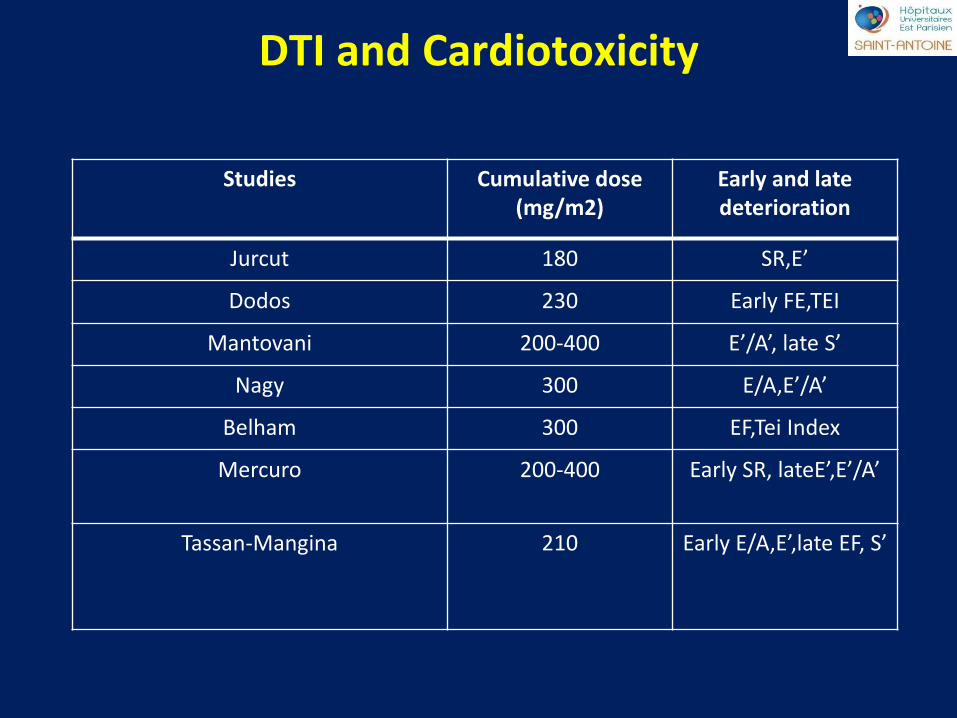
saint antoine DTI and Cardiotoxicity
Studies Cumulative dose (mg/m2)
Early and late deterioration
Jurcut 180 SR,E’
Dodos 230 Early FE,TEI
Mantovani 200-400 E’/A’, late S’
Nagy 300 E/A,E’/A’
Belham 300 EF,Tei Index
Mercuro 200-400 Early SR, lateE’,E’/A’
Tassan-Mangina 210 Early E/A,E’,late EF, S’
saint antoine
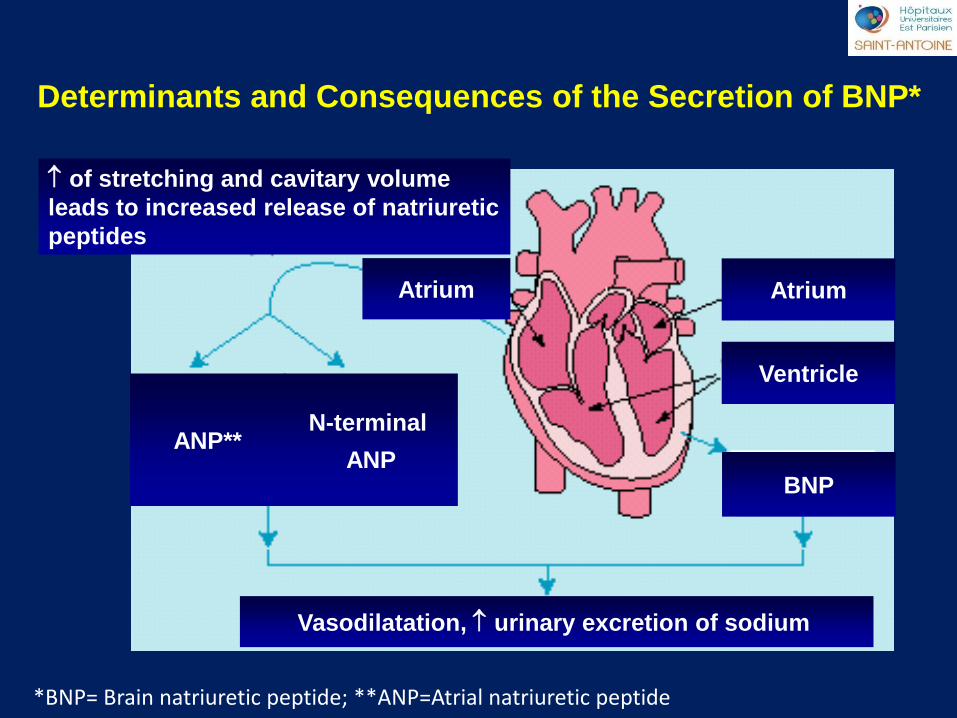
Atrium Atrium
Ventricle
BNP
ANP**
N-terminal
ANP
Vasodilatation, urinary excretion of sodium
of stretching and cavitary volume
leads to increased release of natriuretic
peptides
Determinants and Consequences of the Secretion of BNP*
*BNP= Brain natriuretic peptide; **ANP=Atrial natriuretic peptide
saint antoine
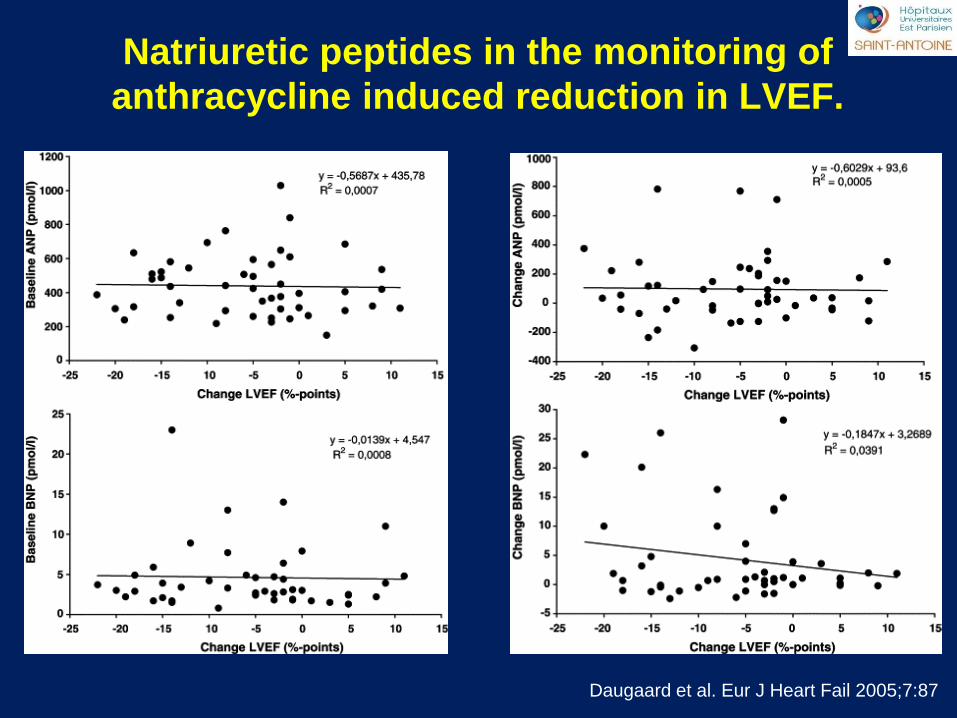
Natriuretic peptides in the monitoring of
anthracycline induced reduction in LVEF.
Daugaard et al. Eur J Heart Fail 2005;7:87
saint antoine
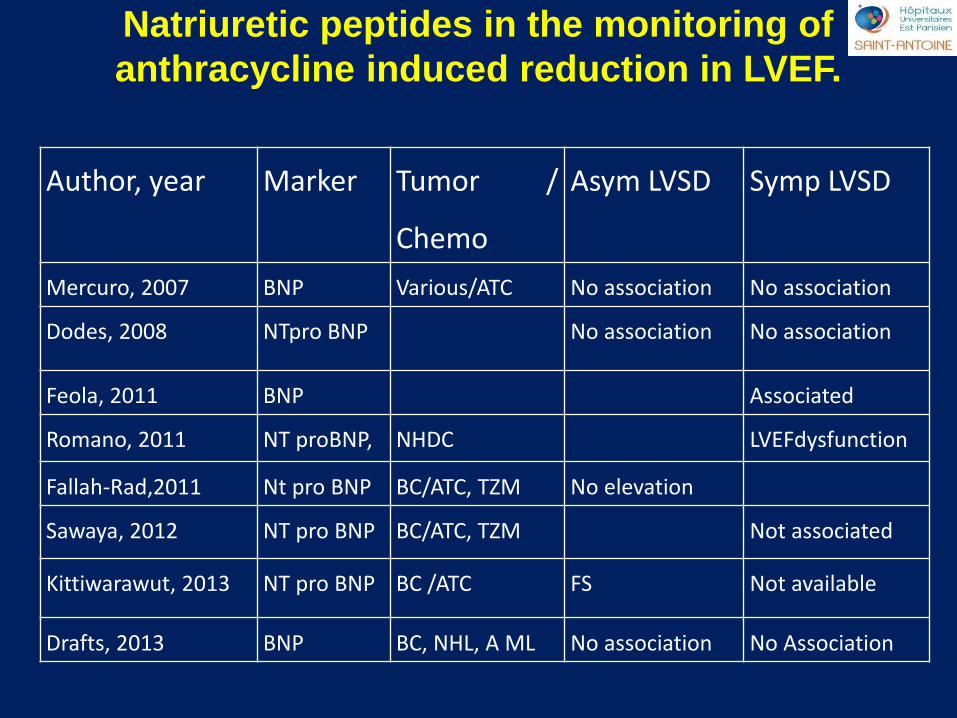
Author, year Marker Tumor /
Chemo
Asym LVSD Symp LVSD
Mercuro, 2007 BNP Various/ATC No association No association
Dodes, 2008 NTpro BNP No association No association
Feola, 2011 BNP Associated
Romano, 2011 NT proBNP, NHDC LVEFdysfunction
Fallah-Rad,2011 Nt pro BNP BC/ATC, TZM No elevation
Sawaya, 2012 NT pro BNP BC/ATC, TZM Not associated
Kittiwarawut, 2013 NT pro BNP BC /ATC FS Not available
Drafts, 2013 BNP BC, NHL, A ML No association No Association
Natriuretic peptides in the monitoring of
anthracycline induced reduction in LVEF.
saint antoine
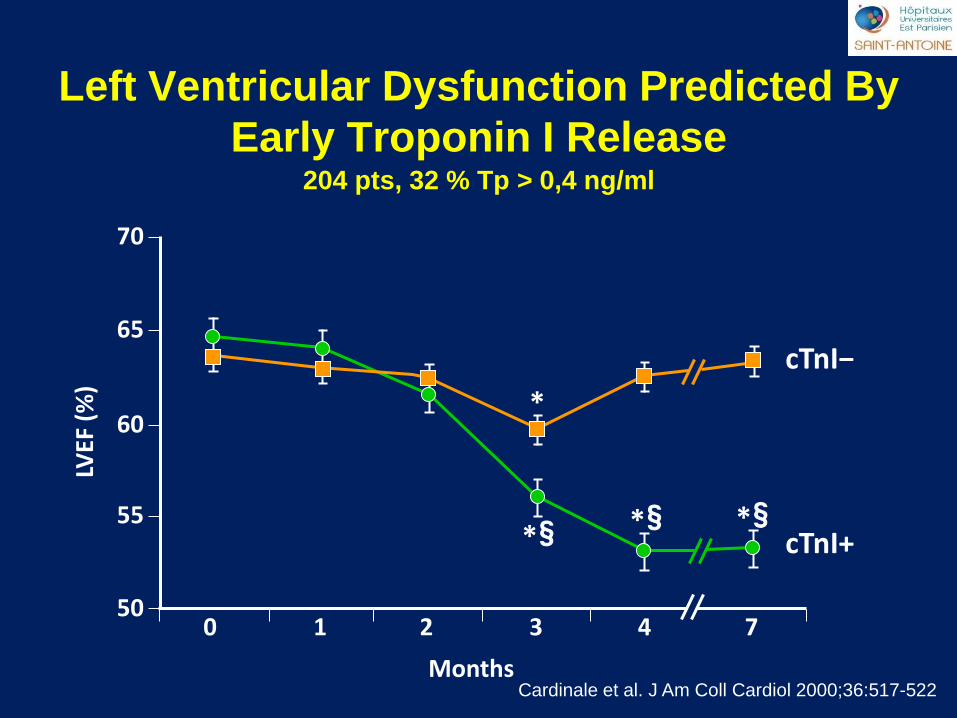
Left Ventricular Dysfunction Predicted By
Early Troponin I Release
Cardinale et al. J Am Coll Cardiol 2000;36:517-522
204 pts, 32 % Tp > 0,4 ng/ml
0 1 2 3 4 7
Months
LVEF
(%
)
50
55
60
65
70
*
§ * § * § *
cTnI−
cTnI+
saint antoine
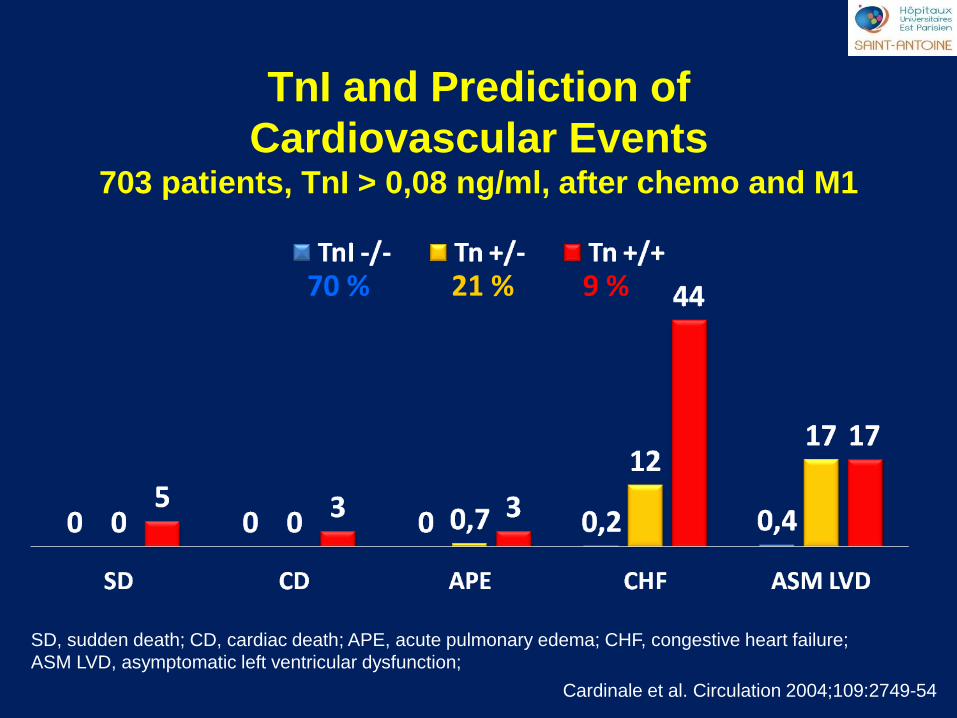
TnI and Prediction of
Cardiovascular Events 703 patients, TnI > 0,08 ng/ml, after chemo and M1
Cardinale et al. Circulation 2004;109:2749-54
SD, sudden death; CD, cardiac death; APE, acute pulmonary edema; CHF, congestive heart failure;
ASM LVD, asymptomatic left ventricular dysfunction;
70 % 9 % 21 %
saint antoine
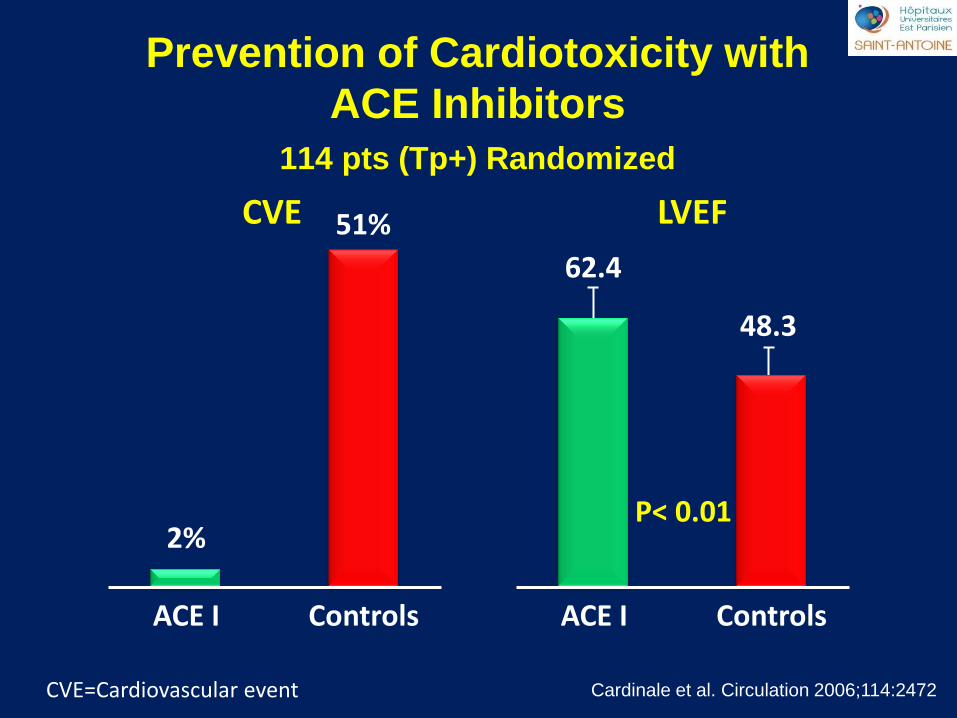
Prevention of Cardiotoxicity with
ACE Inhibitors
114 pts (Tp+) Randomized
Cardinale et al. Circulation 2006;114:2472
CVE
P< 0.01 2%
ACE I
51%
Controls ACE I Controls
62.4
48.3
LVEF
CVE=Cardiovascular event
saint antoine
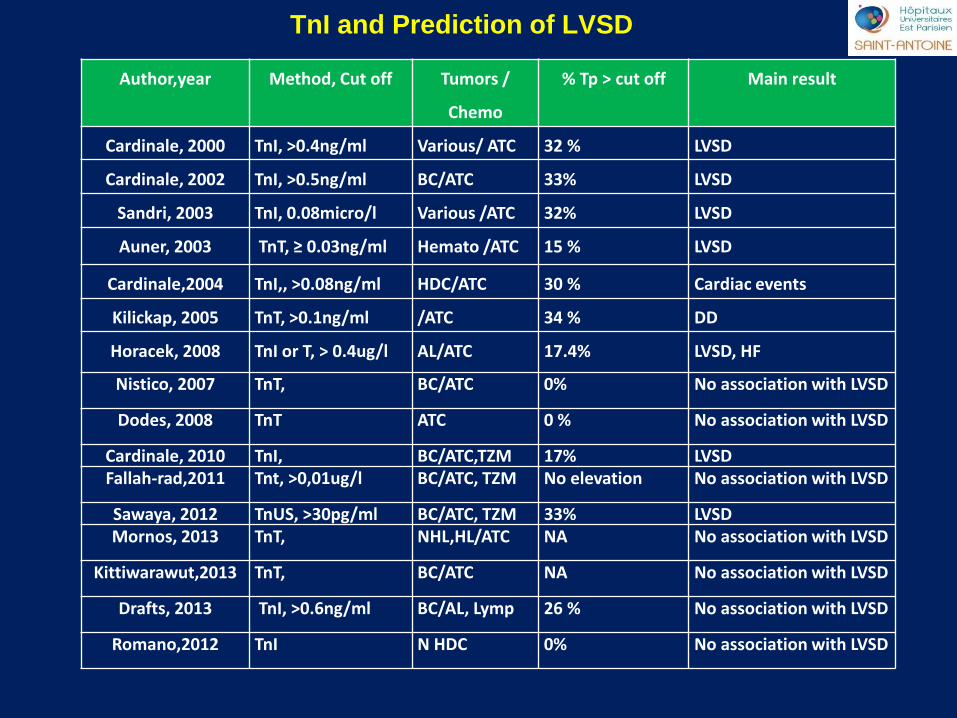
Author,year Method, Cut off Tumors /
Chemo
% Tp > cut off Main result
Cardinale, 2000 TnI, >0.4ng/ml Various/ ATC 32 % LVSD
Cardinale, 2002 TnI, >0.5ng/ml BC/ATC 33% LVSD
Sandri, 2003 TnI, 0.08micro/l Various /ATC 32% LVSD
Auner, 2003 TnT, ≥ 0.03ng/ml Hemato /ATC 15 % LVSD
Cardinale,2004 TnI,, >0.08ng/ml HDC/ATC 30 % Cardiac events
Kilickap, 2005 TnT, >0.1ng/ml /ATC 34 % DD
Horacek, 2008 TnI or T, > 0.4ug/l AL/ATC 17.4% LVSD, HF
Nistico, 2007 TnT, BC/ATC 0% No association with LVSD
Dodes, 2008 TnT ATC 0 % No association with LVSD
Cardinale, 2010 TnI, BC/ATC,TZM 17% LVSD
Fallah-rad,2011 Tnt, >0,01ug/l BC/ATC, TZM No elevation No association with LVSD
Sawaya, 2012 TnUS, >30pg/ml BC/ATC, TZM 33% LVSD
Mornos, 2013 TnT, NHL,HL/ATC NA No association with LVSD
Kittiwarawut,2013 TnT, BC/ATC NA No association with LVSD
Drafts, 2013 TnI, >0.6ng/ml BC/AL, Lymp 26 % No association with LVSD
Romano,2012 TnI N HDC 0% No association with LVSD
TnI and Prediction of LVSD
saint antoine
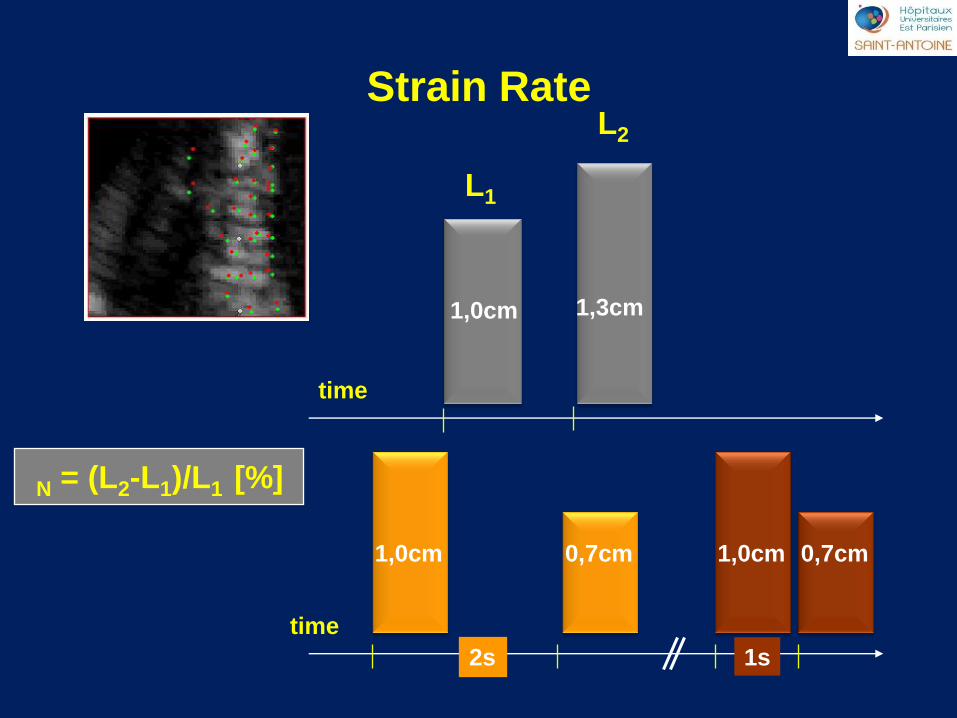
N = (L2-L1)/L1 [%]
Strain Rate
1,3cm
1,0cm 0,7cm
L2
L1
1,0cm
time
1,0cm 0,7cm
2s 1s
time
saint antoine
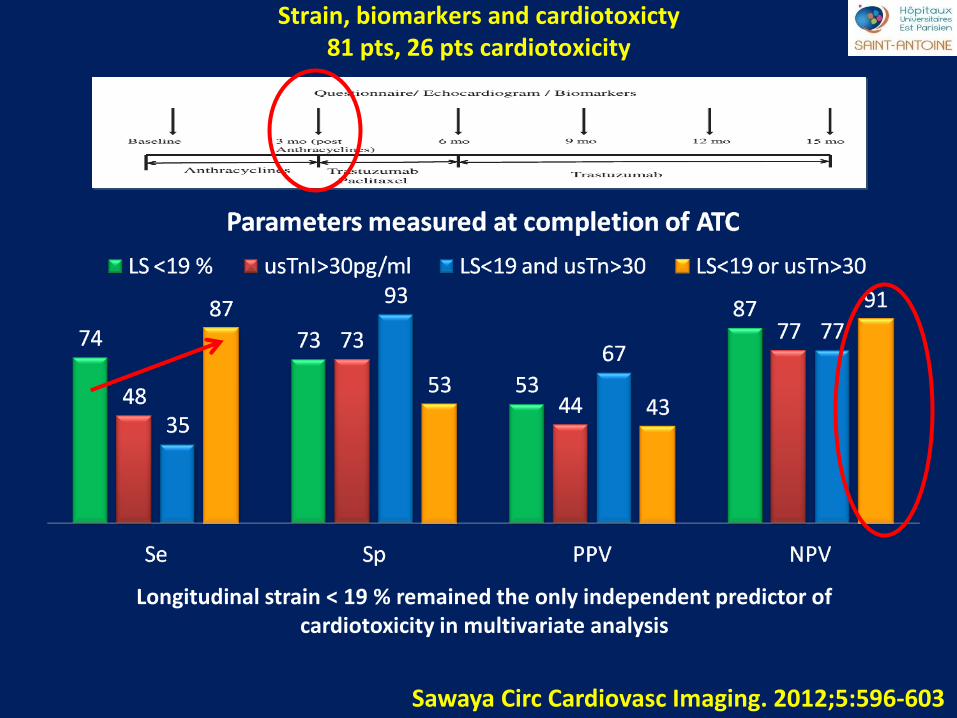
Sawaya Circ Cardiovasc Imaging. 2012;5:596-603
Strain, biomarkers and cardiotoxicty 81 pts, 26 pts cardiotoxicity
Longitudinal strain < 19 % remained the only independent predictor of cardiotoxicity in multivariate analysis
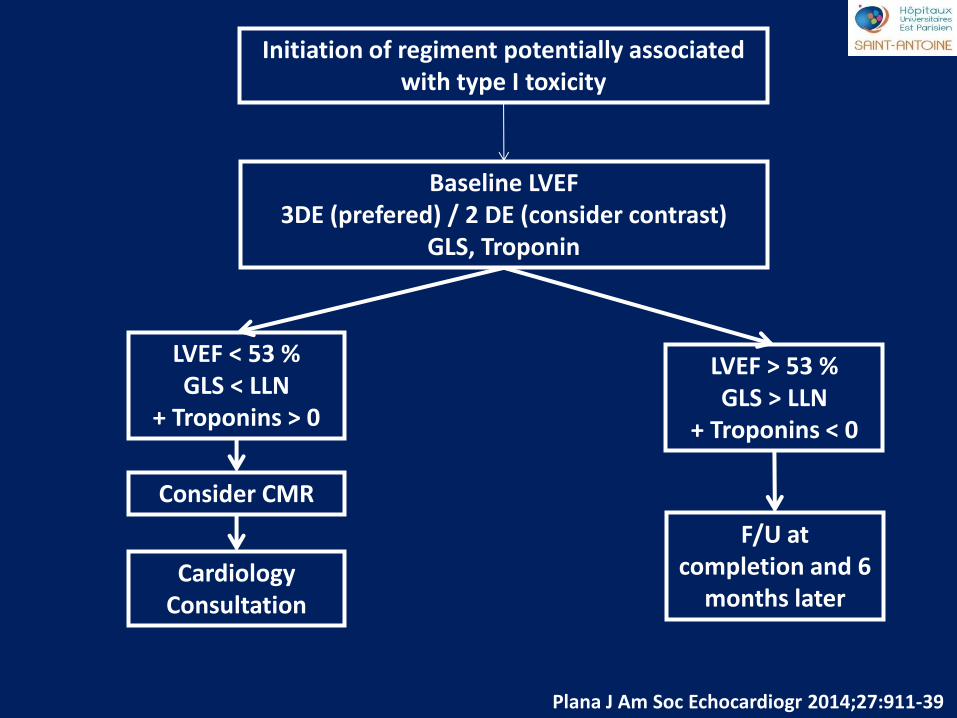
saint antoine
Initiation of regiment potentially associated with type I toxicity
Baseline LVEF 3DE (prefered) / 2 DE (consider contrast)
GLS, Troponin
LVEF < 53 % GLS < LLN
+ Troponins > 0
LVEF > 53 % GLS > LLN
+ Troponins < 0
F/U at completion and 6
months later Cardiology
Consultation
Consider CMR
Plana J Am Soc Echocardiogr 2014;27:911-39
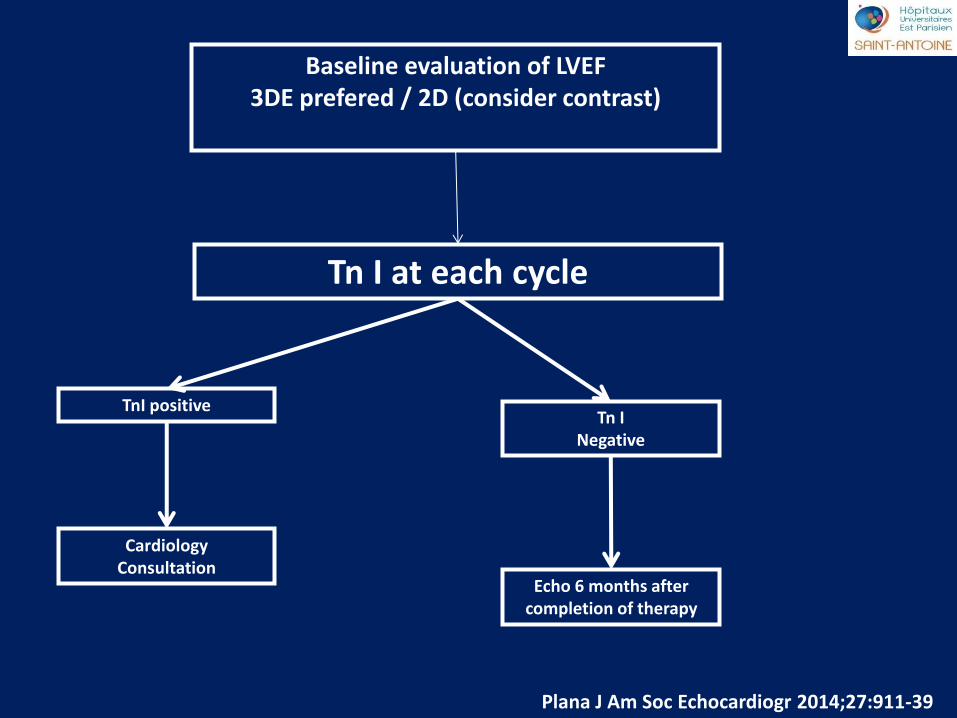
saint antoine
Baseline evaluation of LVEF 3DE prefered / 2D (consider contrast)
Tn I at each cycle
TnI positive Tn I
Negative
Echo 6 months after completion of therapy
Cardiology Consultation
Plana J Am Soc Echocardiogr 2014;27:911-39
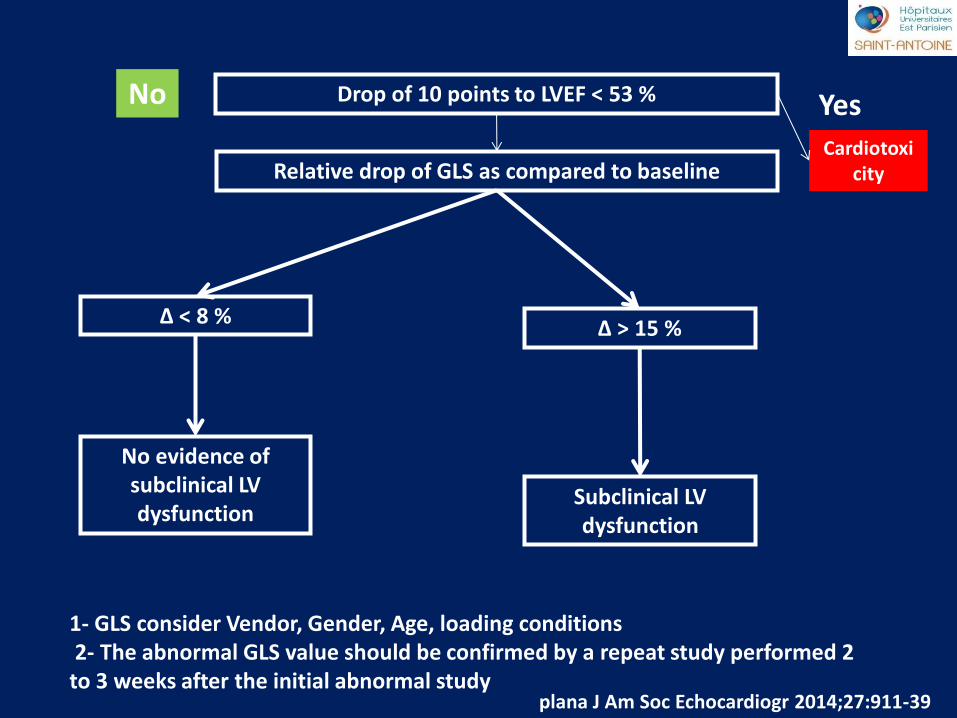
saint antoine
Drop of 10 points to LVEF < 53 %
Relative drop of GLS as compared to baseline
Δ < 8 % Δ > 15 %
Subclinical LV dysfunction
No evidence of subclinical LV dysfunction
plana J Am Soc Echocardiogr 2014;27:911-39
Cardiotoxicity
Yes No
1- GLS consider Vendor, Gender, Age, loading conditions 2- The abnormal GLS value should be confirmed by a repeat study performed 2 to 3 weeks after the initial abnormal study
saint antoine
Cancer Therapeutics regimens associated with type I and type II Cancer therapeutics related cardiac dysfunction
Cancer
Cancer Therapeutics
Regimen potentially associated with Type 2
Toxicity
Trastuzumab Lapatinib
Pertuzumab Sorafenib Sunitinib
Bevacizumab
De plana J Am Soc Echocardiogr 2014;27:911-39
saint antoine
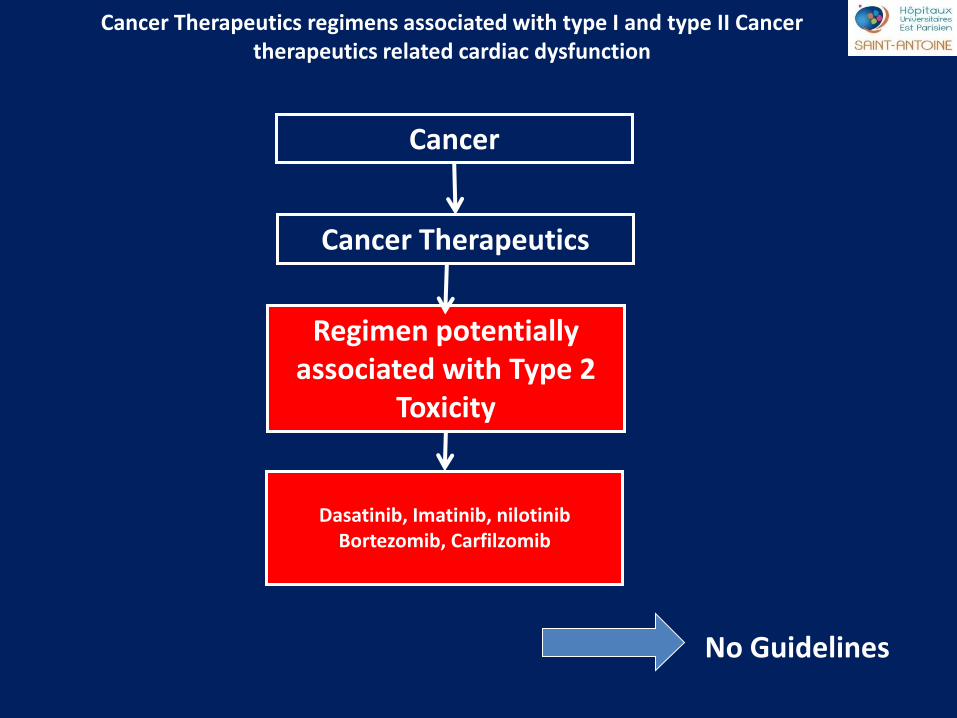
Cancer Therapeutics regimens associated with type I and type II Cancer therapeutics related cardiac dysfunction
Cancer
Cancer Therapeutics
Regimen potentially associated with Type 2
Toxicity
Dasatinib, Imatinib, nilotinib
Bortezomib, Carfilzomib
No Guidelines
saint antoine
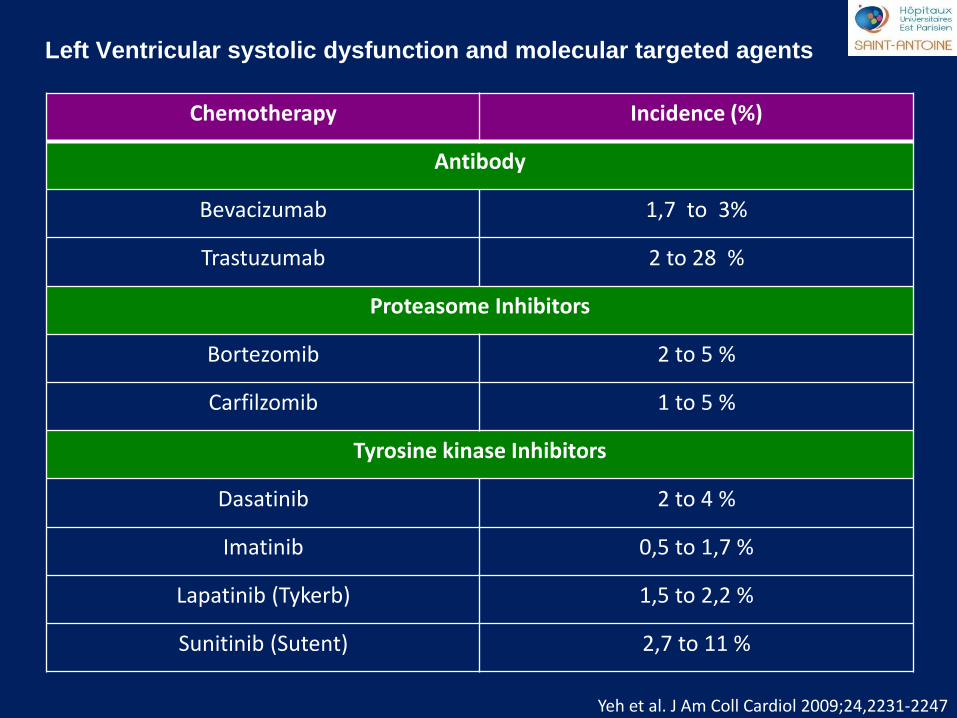
Left Ventricular systolic dysfunction and molecular targeted agents
Chemotherapy Incidence (%)
Antibody
Bevacizumab 1,7 to 3%
Trastuzumab 2 to 28 %
Proteasome Inhibitors
Bortezomib 2 to 5 %
Carfilzomib 1 to 5 %
Tyrosine kinase Inhibitors
Dasatinib 2 to 4 %
Imatinib 0,5 to 1,7 %
Lapatinib (Tykerb) 1,5 to 2,2 %
Sunitinib (Sutent) 2,7 to 11 %
Yeh et al. J Am Coll Cardiol 2009;24,2231-2247
saint antoine
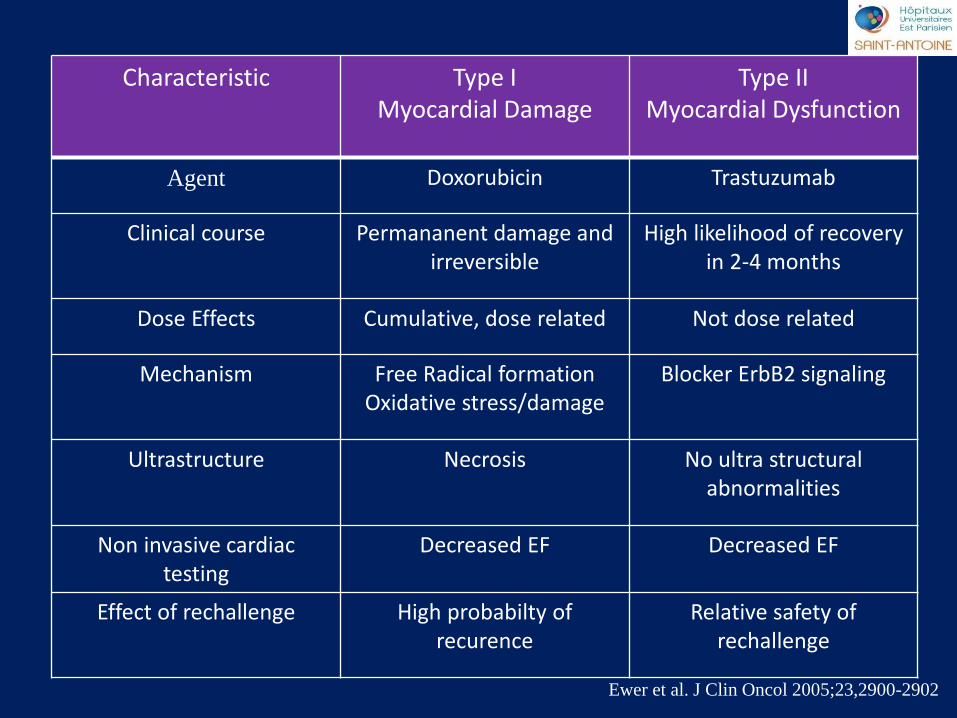
Ewer et al. J Clin Oncol 2005;23,2900-2902
Characteristic Type I Myocardial Damage
Type II Myocardial Dysfunction
Agent Doxorubicin Trastuzumab
Clinical course Permananent damage and irreversible
High likelihood of recovery in 2-4 months
Dose Effects Cumulative, dose related Not dose related
Mechanism Free Radical formation Oxidative stress/damage
Blocker ErbB2 signaling
Ultrastructure Necrosis No ultra structural abnormalities
Non invasive cardiac testing
Decreased EF Decreased EF
Effect of rechallenge High probabilty of recurence
Relative safety of rechallenge
saint antoine
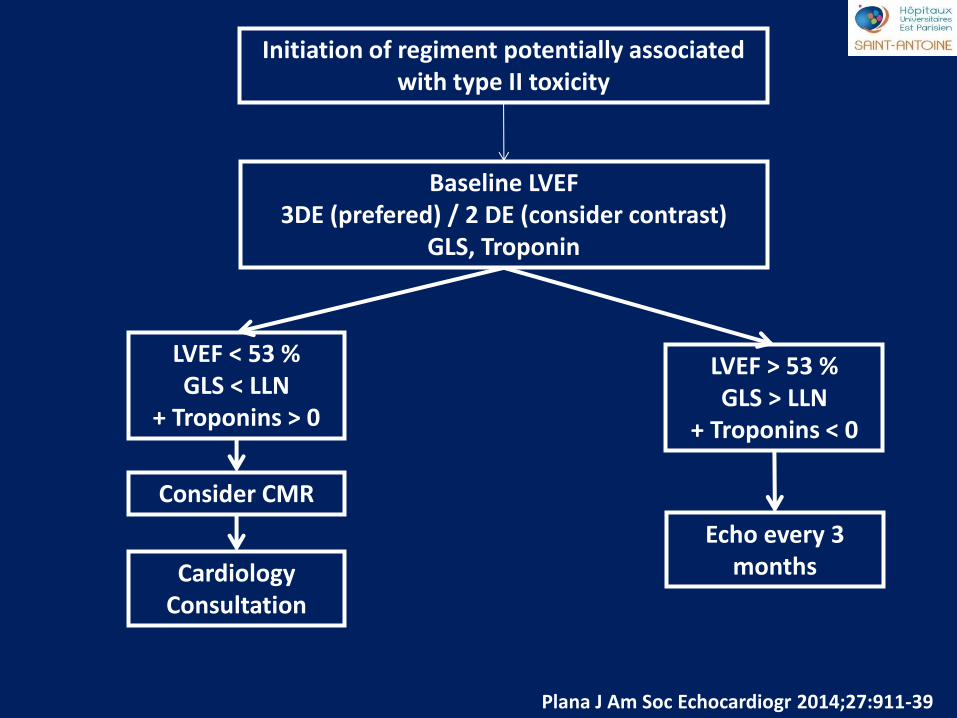
Initiation of regiment potentially associated with type II toxicity
Baseline LVEF 3DE (prefered) / 2 DE (consider contrast)
GLS, Troponin
LVEF < 53 % GLS < LLN
+ Troponins > 0
LVEF > 53 % GLS > LLN
+ Troponins < 0
Echo every 3 months Cardiology
Consultation
Consider CMR
Plana J Am Soc Echocardiogr 2014;27:911-39
saint antoine
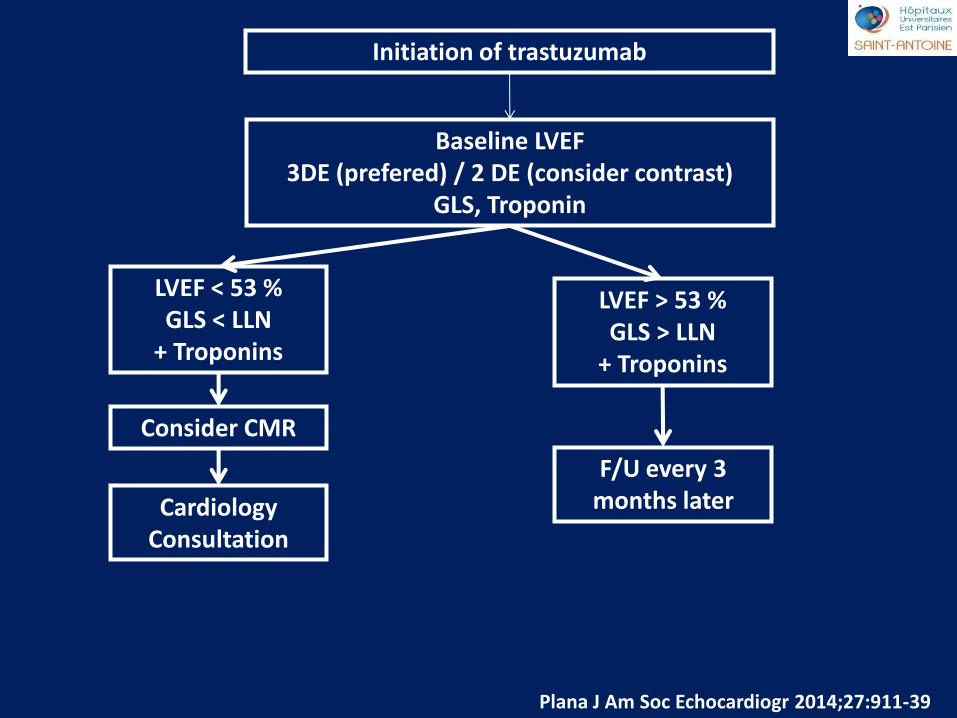
Initiation of trastuzumab
Baseline LVEF 3DE (prefered) / 2 DE (consider contrast)
GLS, Troponin
LVEF < 53 % GLS < LLN
+ Troponins
LVEF > 53 % GLS > LLN
+ Troponins
F/U every 3 months later Cardiology
Consultation
Consider CMR
Plana J Am Soc Echocardiogr 2014;27:911-39
saint antoine
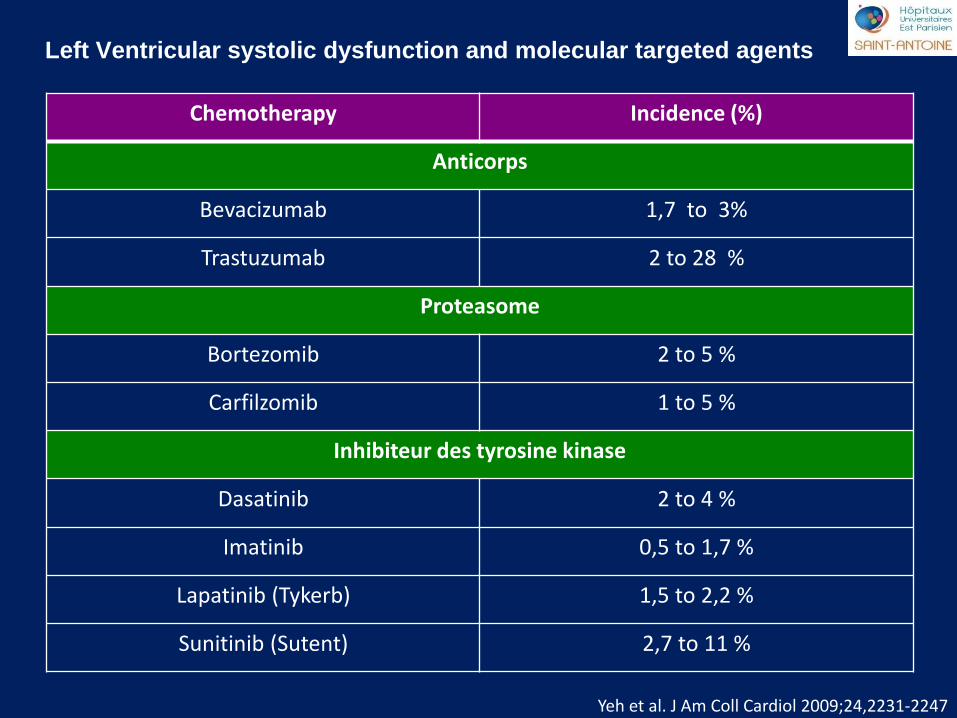
Left Ventricular systolic dysfunction and molecular targeted agents
Chemotherapy Incidence (%)
Anticorps
Bevacizumab 1,7 to 3%
Trastuzumab 2 to 28 %
Proteasome
Bortezomib 2 to 5 %
Carfilzomib 1 to 5 %
Inhibiteur des tyrosine kinase
Dasatinib 2 to 4 %
Imatinib 0,5 to 1,7 %
Lapatinib (Tykerb) 1,5 to 2,2 %
Sunitinib (Sutent) 2,7 to 11 %
Yeh et al. J Am Coll Cardiol 2009;24,2231-2247
saint antoine
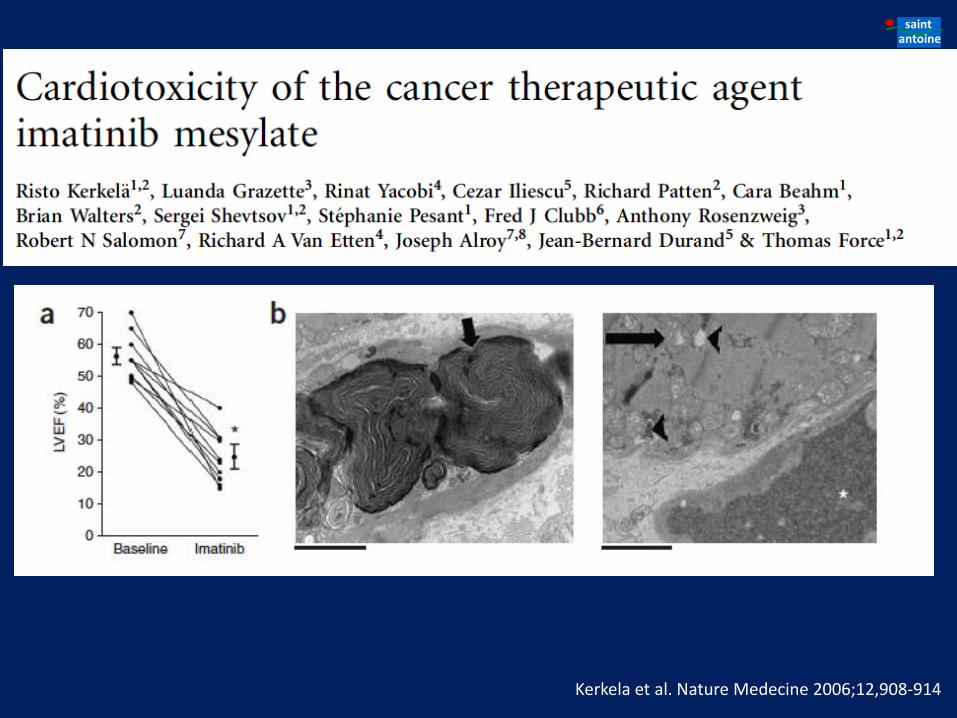
Kerkela et al. Nature Medecine 2006;12,908-914
saint antoine
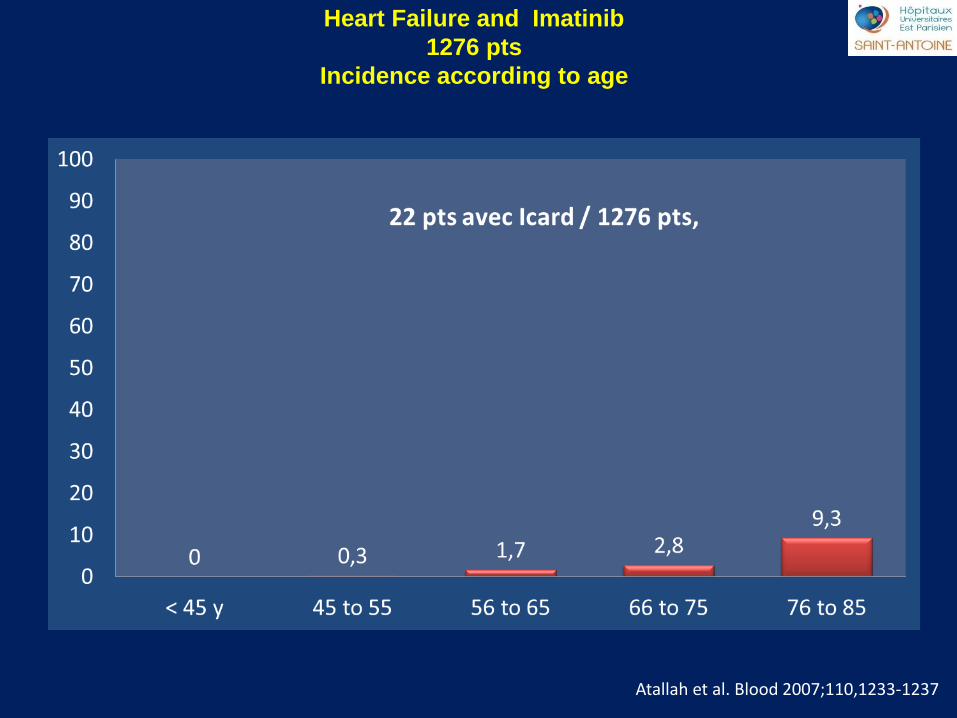
Heart Failure and Imatinib
1276 pts
Incidence according to age
Atallah et al. Blood 2007;110,1233-1237
saint antoine
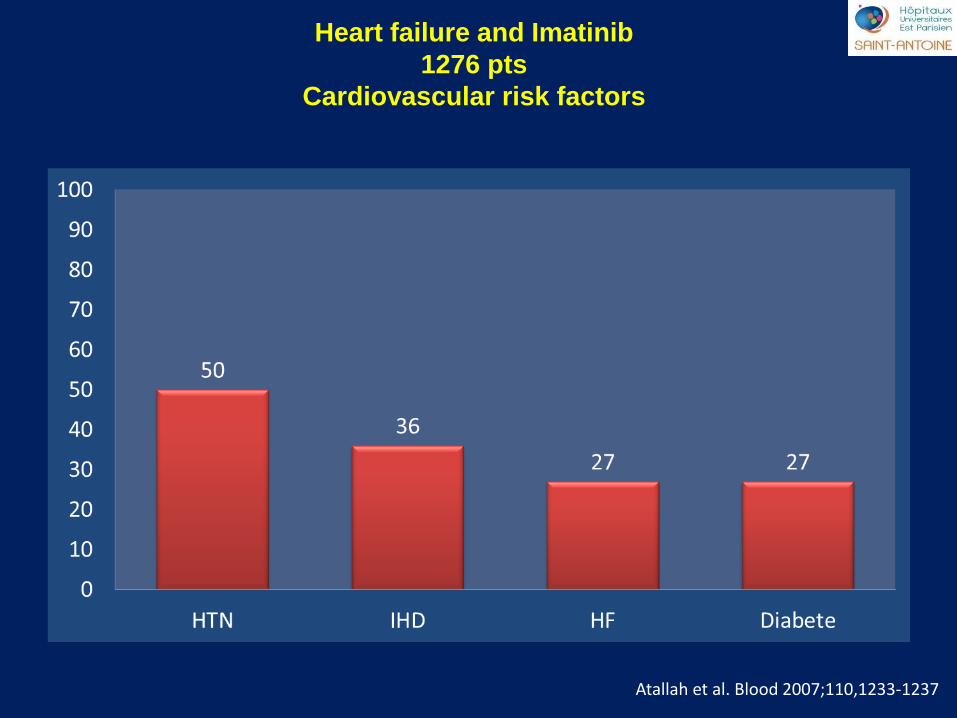
Atallah et al. Blood 2007;110,1233-1237
Heart failure and Imatinib
1276 pts
Cardiovascular risk factors
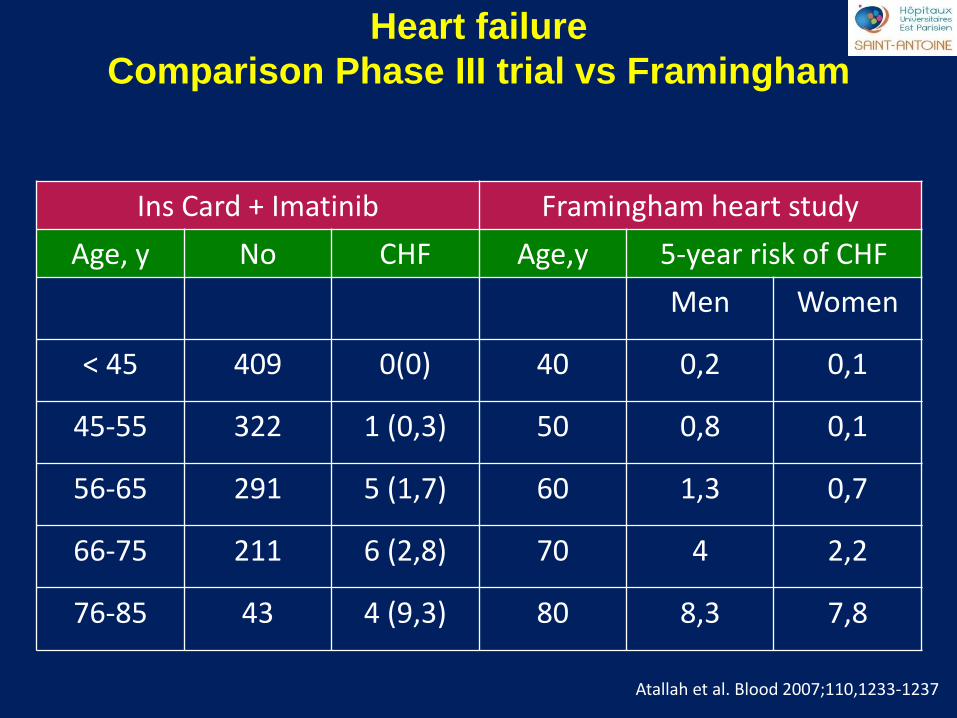
saint antoine Heart failure
Comparison Phase III trial vs Framingham
Ins Card + Imatinib Framingham heart study
Age, y No CHF Age,y 5-year risk of CHF
Men Women
< 45 409 0(0) 40 0,2 0,1
45-55 322 1 (0,3) 50 0,8 0,1
56-65 291 5 (1,7) 60 1,3 0,7
66-75 211 6 (2,8) 70 4 2,2
76-85 43 4 (9,3) 80 8,3 7,8
Atallah et al. Blood 2007;110,1233-1237
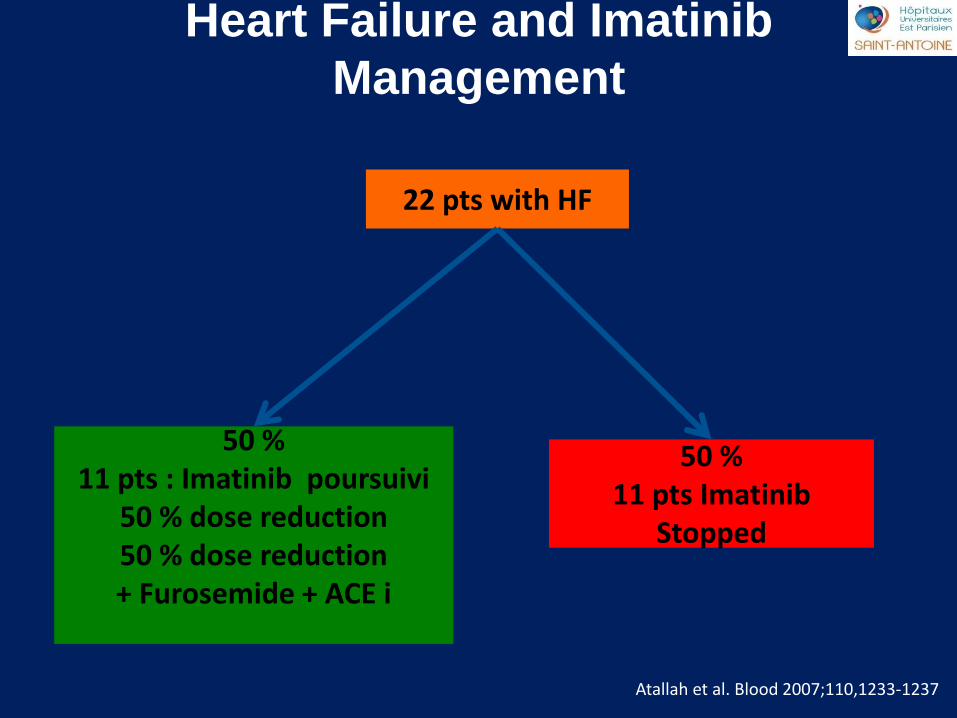
saint antoine Heart Failure and Imatinib
Management
Atallah et al. Blood 2007;110,1233-1237
22 pts with HF
50 % 11 pts : Imatinib poursuivi
50 % dose reduction 50 % dose reduction + Furosemide + ACE i
50 % 11 pts Imatinib
Stopped
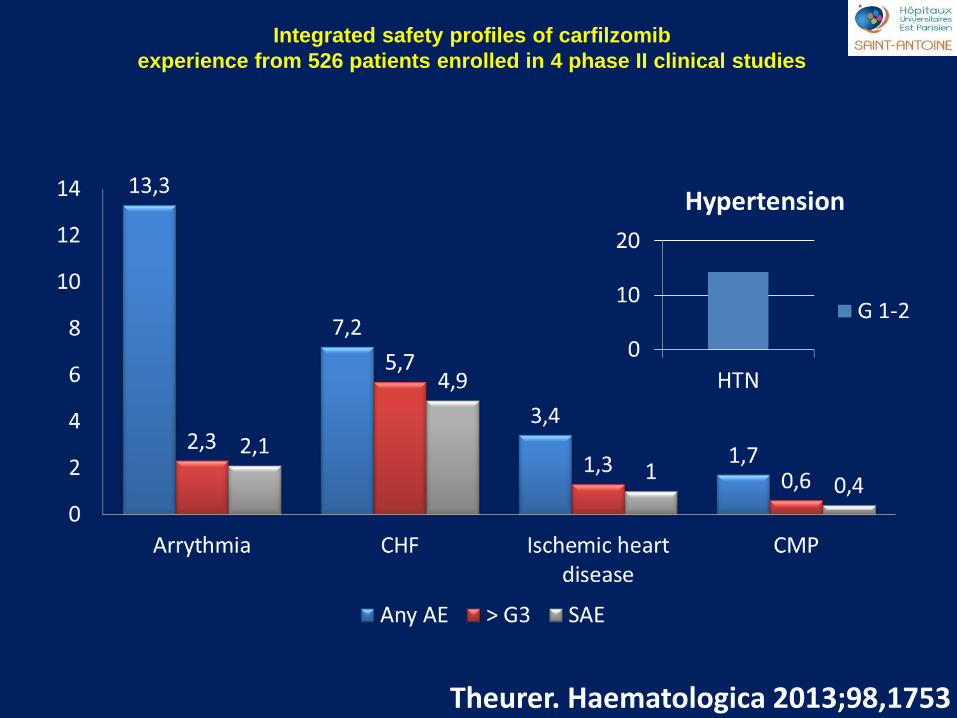
saint antoine Integrated safety profiles of carfilzomib
experience from 526 patients enrolled in 4 phase II clinical studies
Theurer. Haematologica 2013;98,1753
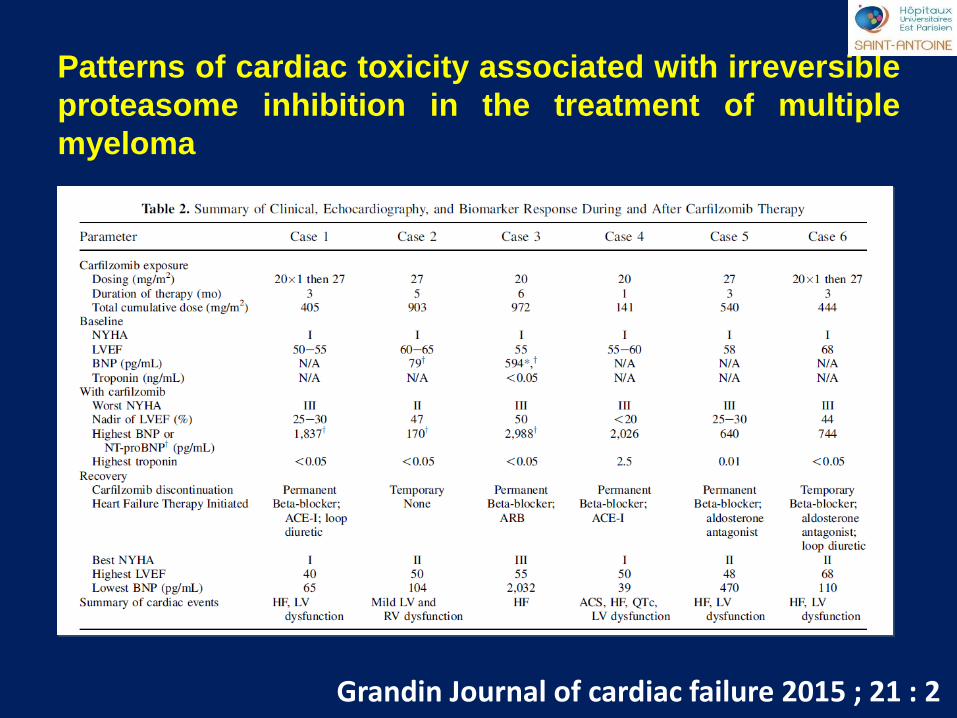
saint antoine
Patterns of cardiac toxicity associated with irreversible
proteasome inhibition in the treatment of multiple
myeloma
Grandin Journal of cardiac failure 2015 ; 21 : 2
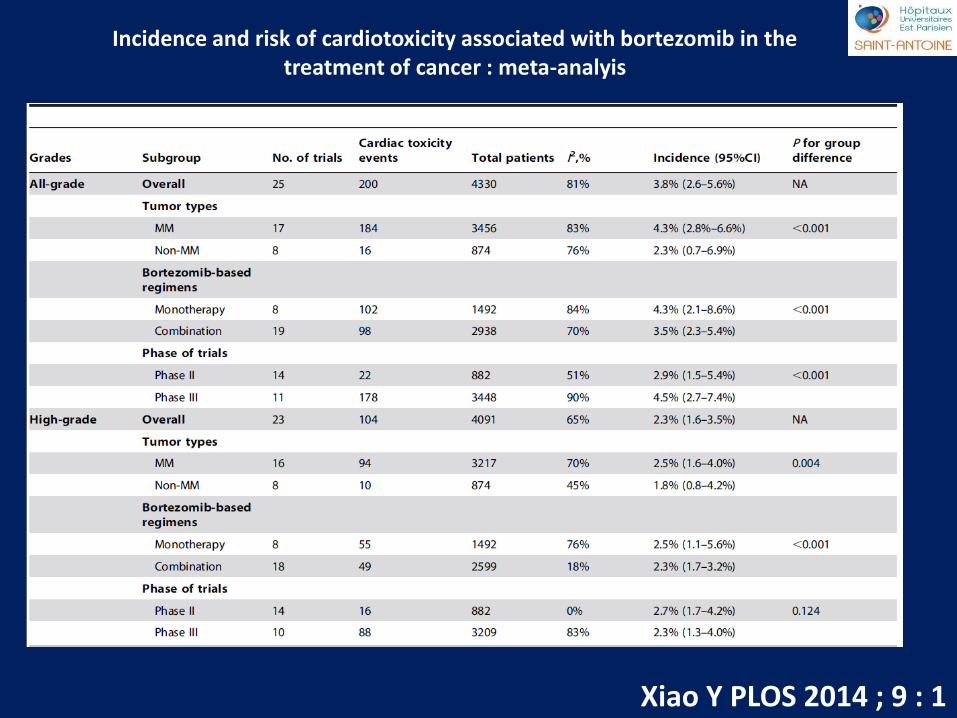
saint antoine Incidence and risk of cardiotoxicity associated with bortezomib in the
treatment of cancer : meta-analyis
Xiao Y PLOS 2014 ; 9 : 1
saint antoine TKI / IP
1.Prise en charge : Réversible et sensible au TTT par IEC + Diurétique
2.Indentification rapide des signes et symptômes d’IC = > Echographie
cardiaque
3.Echographie cardiaque ne peut être proposée en pré traitement
4.Echographie cardiaque : pas de monitoring systématique
5.Myelome et atteinte cardiaque
saint antoine Cardiotoxicity in Hematology
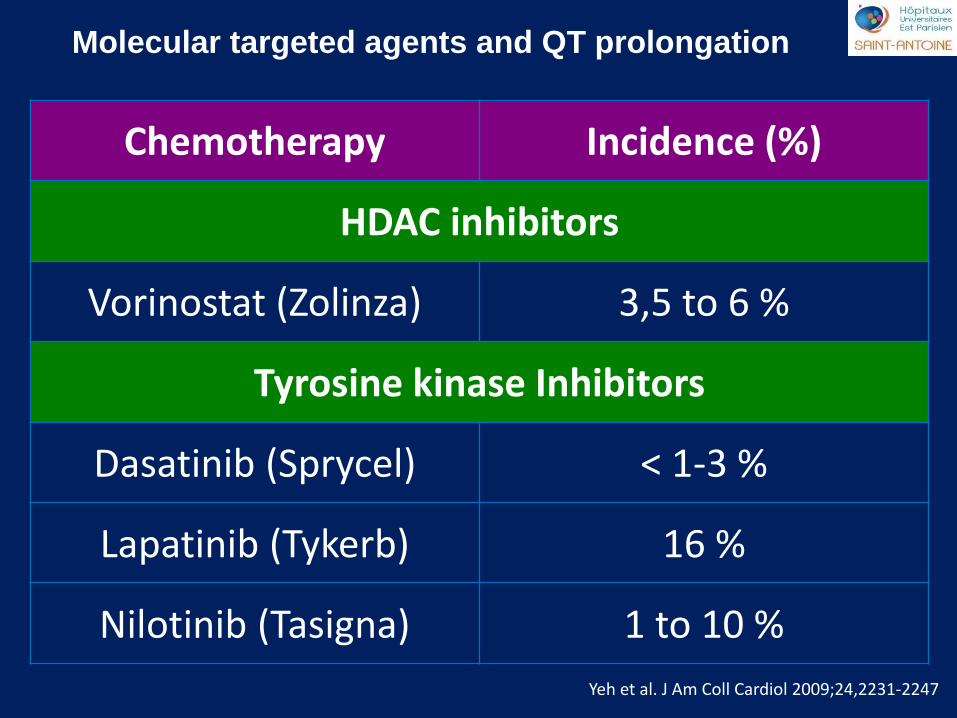
saint antoine Molecular targeted agents and QT prolongation
Yeh et al. J Am Coll Cardiol 2009;24,2231-2247
Chemotherapy Incidence (%)
HDAC inhibitors
Vorinostat (Zolinza) 3,5 to 6 %
Tyrosine kinase Inhibitors
Dasatinib (Sprycel) < 1-3 %
Lapatinib (Tykerb) 16 %
Nilotinib (Tasigna) 1 to 10 %
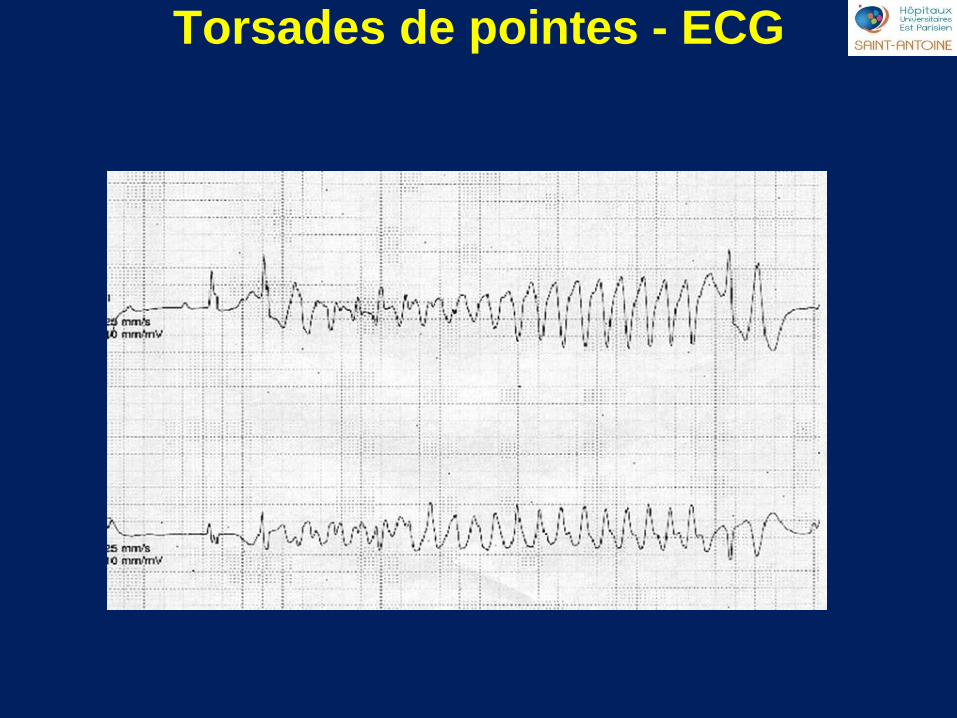
saint antoine Torsades de pointes - ECG
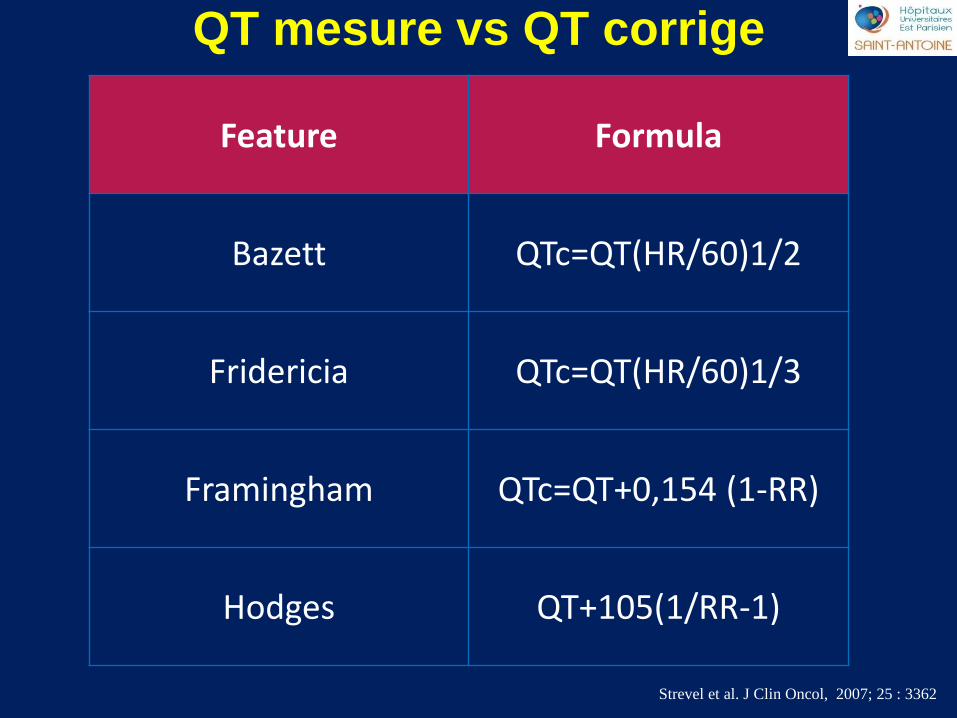
saint antoine QT mesure vs QT corrige
Strevel et al. J Clin Oncol, 2007; 25 : 3362
Feature Formula
Bazett QTc=QT(HR/60)1/2
Fridericia QTc=QT(HR/60)1/3
Framingham QTc=QT+0,154 (1-RR)
Hodges QT+105(1/RR-1)
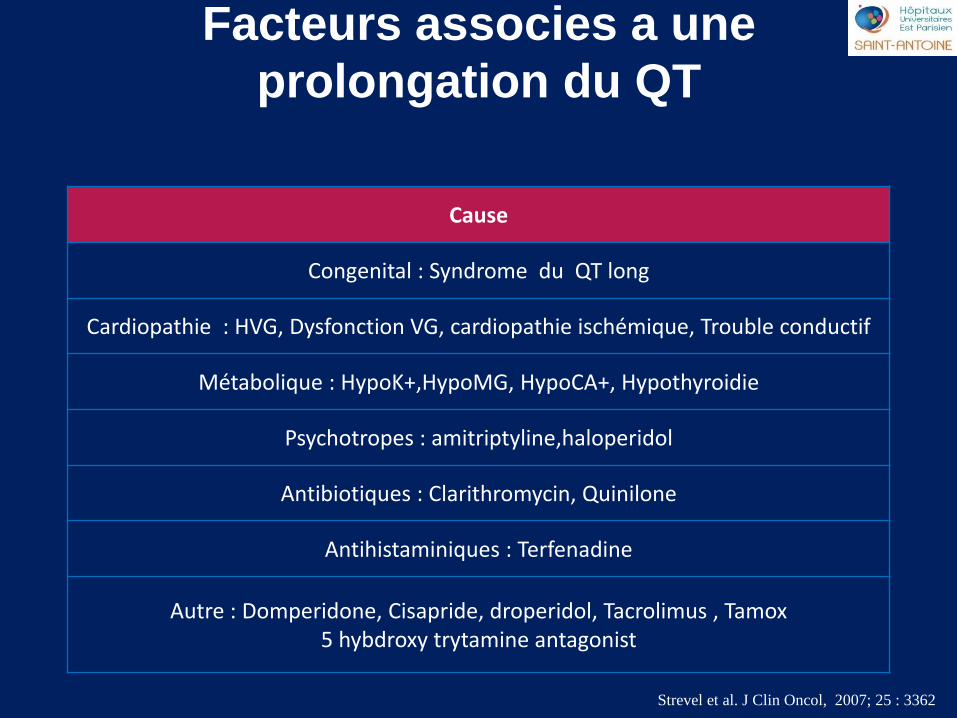
saint antoine Facteurs associes a une
prolongation du QT
Strevel et al. J Clin Oncol, 2007; 25 : 3362
Cause
Congenital : Syndrome du QT long
Cardiopathie : HVG, Dysfonction VG, cardiopathie ischémique, Trouble conductif
Métabolique : HypoK+,HypoMG, HypoCA+, Hypothyroidie
Psychotropes : amitriptyline,haloperidol
Antibiotiques : Clarithromycin, Quinilone
Antihistaminiques : Terfenadine
Autre : Domperidone, Cisapride, droperidol, Tacrolimus , Tamox 5 hybdroxy trytamine antagonist
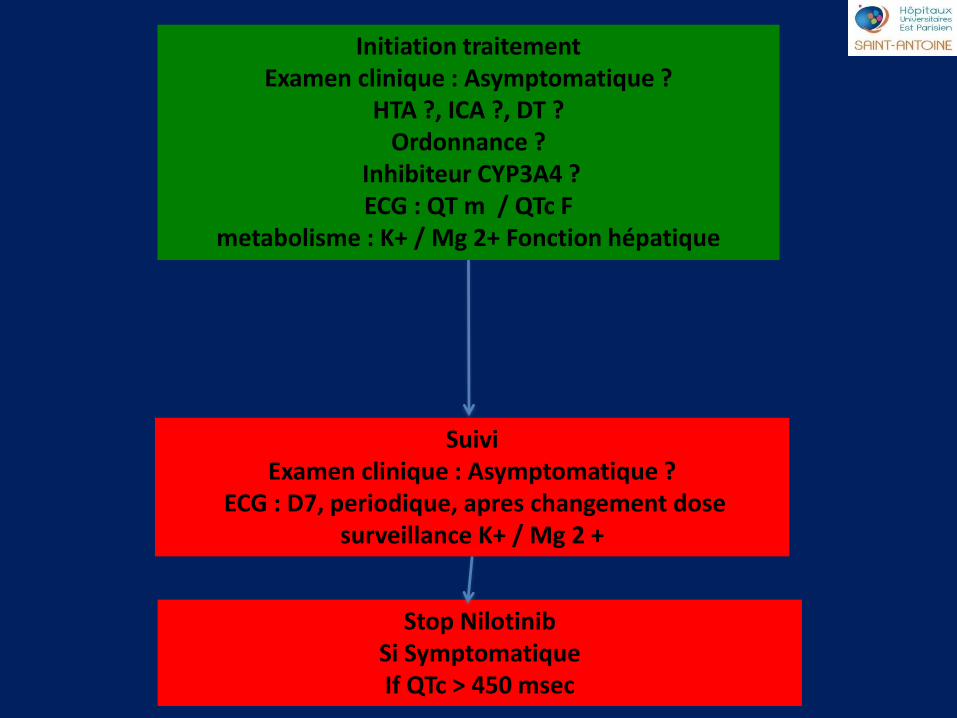
saint antoine Initiation traitement
Examen clinique : Asymptomatique ? HTA ?, ICA ?, DT ?
Ordonnance ? Inhibiteur CYP3A4 ? ECG : QT m / QTc F
metabolisme : K+ / Mg 2+ Fonction hépatique
Suivi Examen clinique : Asymptomatique ?
ECG : D7, periodique, apres changement dose surveillance K+ / Mg 2 +
Stop Nilotinib Si Symptomatique If QTc > 450 msec
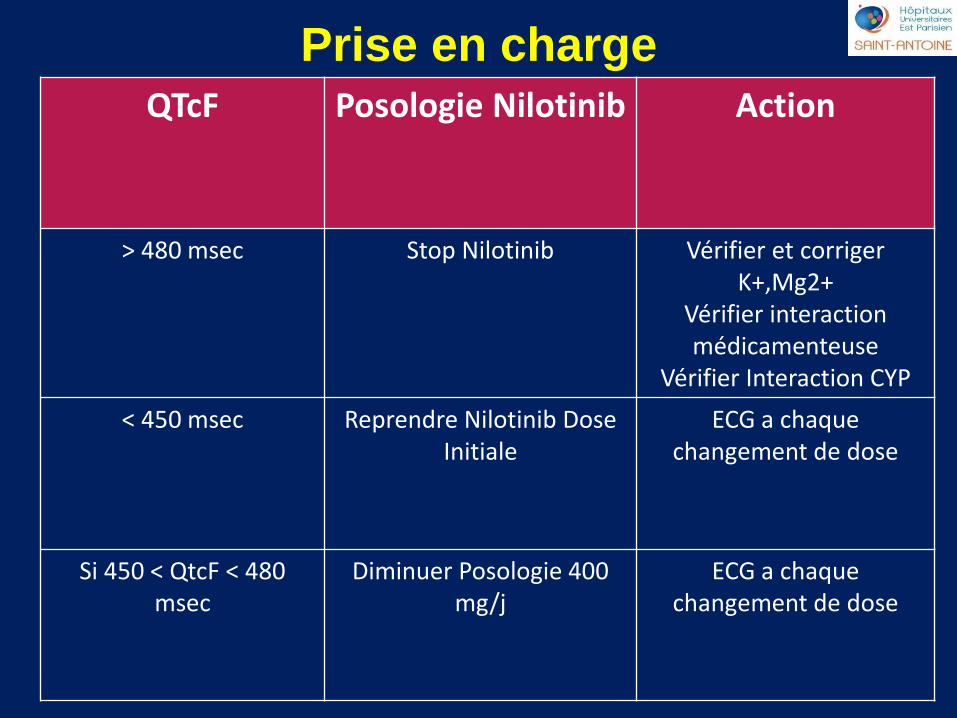
saint antoine
QTcF Posologie Nilotinib Action
> 480 msec Stop Nilotinib Vérifier et corriger K+,Mg2+
Vérifier interaction médicamenteuse
Vérifier Interaction CYP
< 450 msec Reprendre Nilotinib Dose Initiale
ECG a chaque changement de dose
Si 450 < QtcF < 480 msec
Diminuer Posologie 400 mg/j
ECG a chaque changement de dose
Prise en charge
saint antoine Cardiotoxicity in Hematology
Peripheral Artery disease
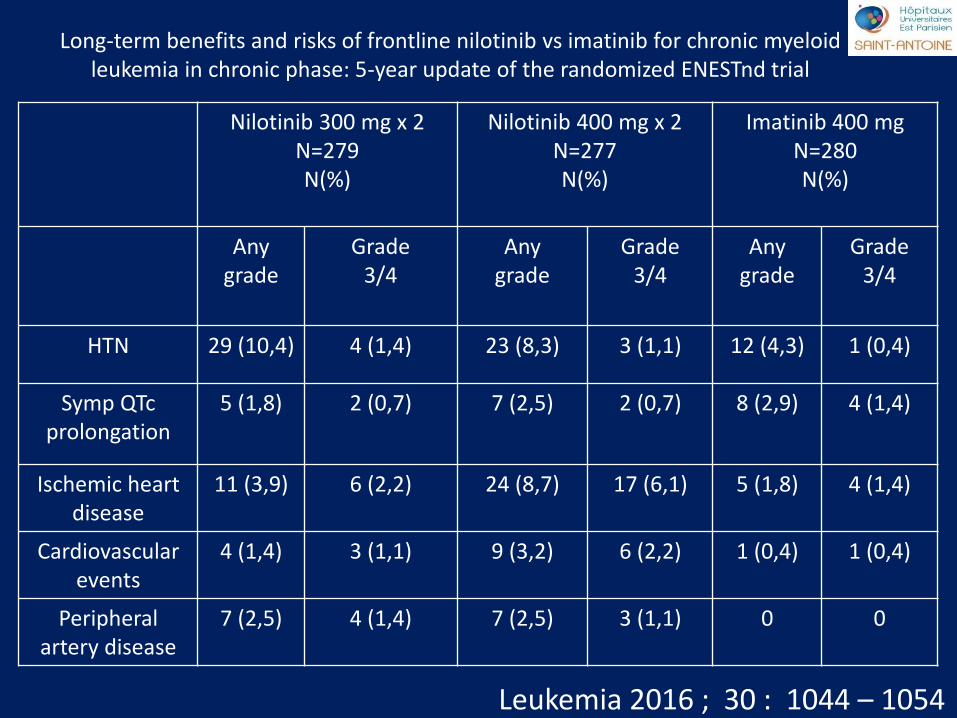
saint antoine Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid
leukemia in chronic phase: 5-year update of the randomized ENESTnd trial
Leukemia 2016 ; 30 : 1044 – 1054
Nilotinib 300 mg x 2 N=279 N(%)
Nilotinib 400 mg x 2 N=277 N(%)
Imatinib 400 mg N=280 N(%)
Any grade
Grade 3/4
Any grade
Grade 3/4
Any grade
Grade 3/4
HTN 29 (10,4) 4 (1,4) 23 (8,3) 3 (1,1) 12 (4,3) 1 (0,4)
Symp QTc prolongation
5 (1,8) 2 (0,7) 7 (2,5) 2 (0,7) 8 (2,9) 4 (1,4)
Ischemic heart disease
11 (3,9) 6 (2,2) 24 (8,7) 17 (6,1) 5 (1,8) 4 (1,4)
Cardiovascular events
4 (1,4) 3 (1,1) 9 (3,2) 6 (2,2) 1 (0,4) 1 (0,4)
Peripheral artery disease
7 (2,5) 4 (1,4) 7 (2,5) 3 (1,1) 0 0
saint antoine
saint antoine
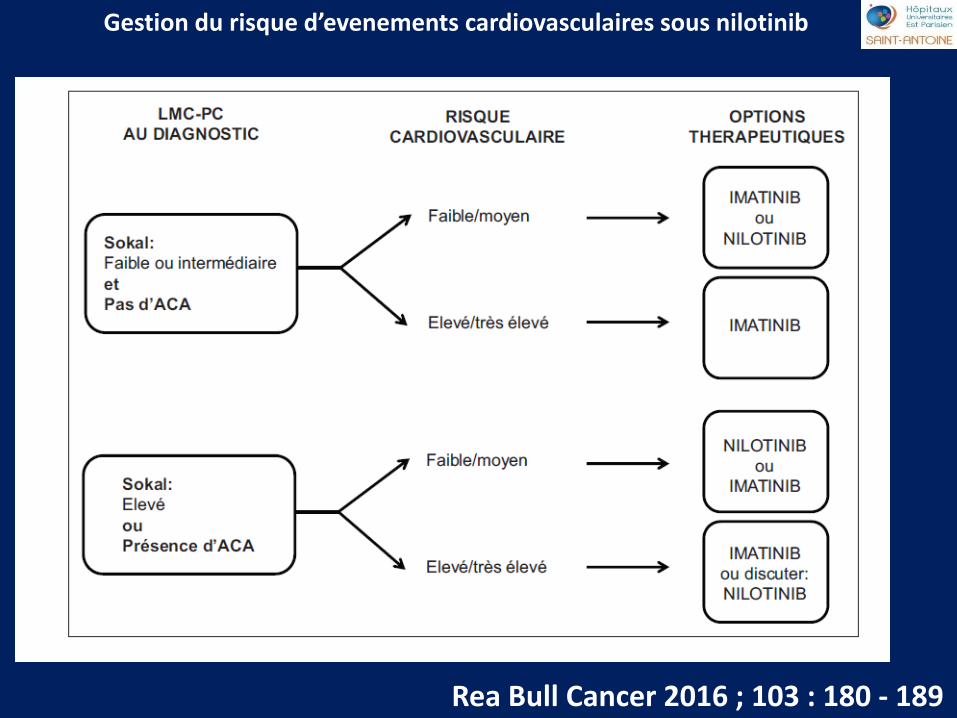
Rea Bull Cancer 2016 ; 103 : 180 - 189
Gestion du risque d’evenements cardiovasculaires sous nilotinib
saint antoine
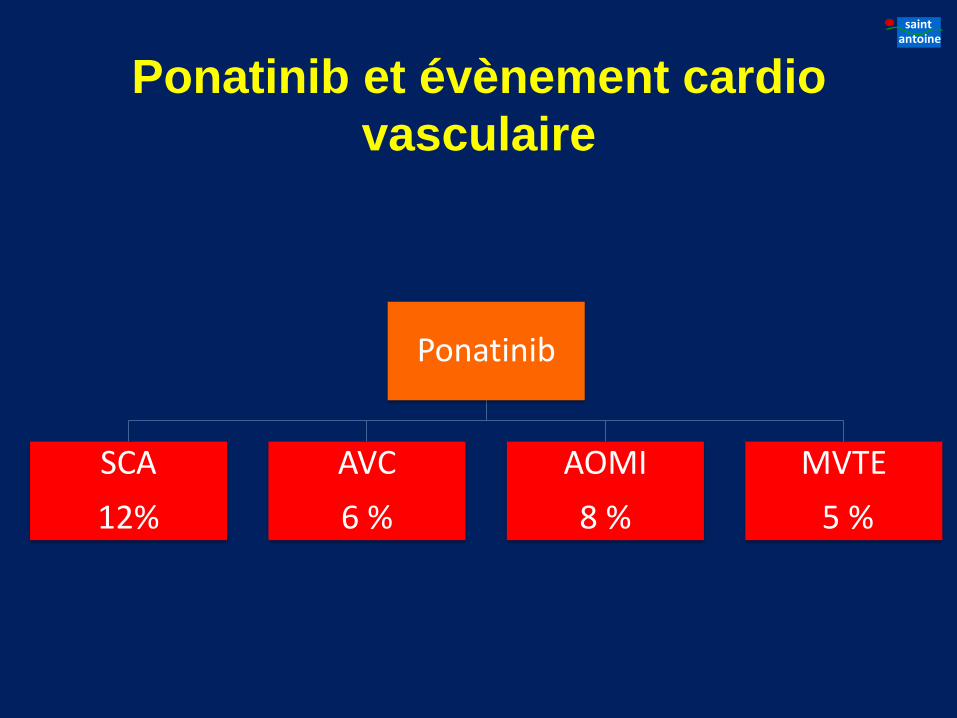
Ponatinib et évènement cardio
vasculaire
Ponatinib
SCA
12%
AVC
6 %
AOMI
8 %
MVTE
5 %
saint antoine Cardiotoxicity in Hematology
Pulmonary Hypertension
saint antoine Conclusions
1- Anthracycline : Stratégie de depistage et de prevention 2- Thérapies moléculaires ciblées : Reversibilite, Modulation de la posologie 3- Toxicités emergentes : AOMI, HTP
saint antoine
A vos boitiers ! 4 questions
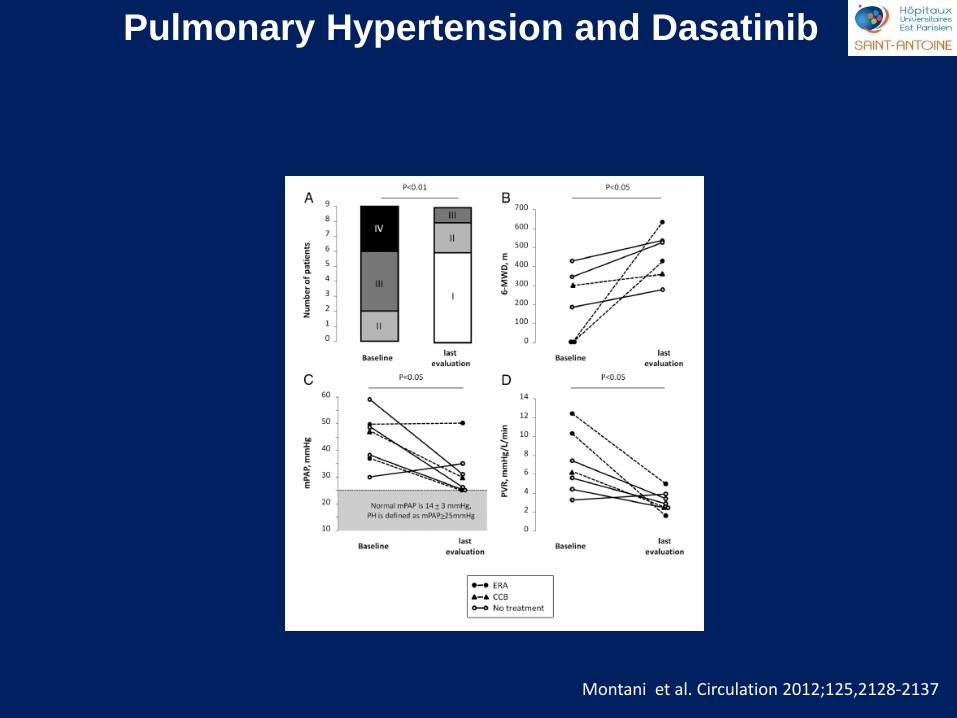
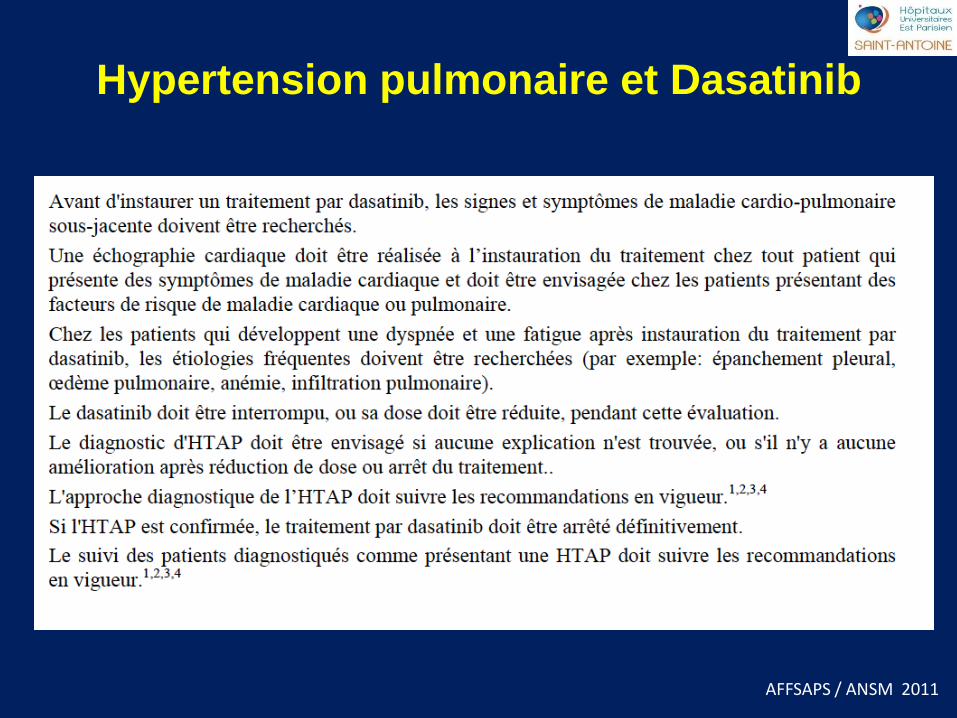
saint antoine Pulmonary Hypertension and Dasatinib
Montani et al. Circulation 2012;125,2128-2137
saint antoine
AFFSAPS / ANSM 2011
Hypertension pulmonaire et Dasatinib
saint antoine
saint antoine
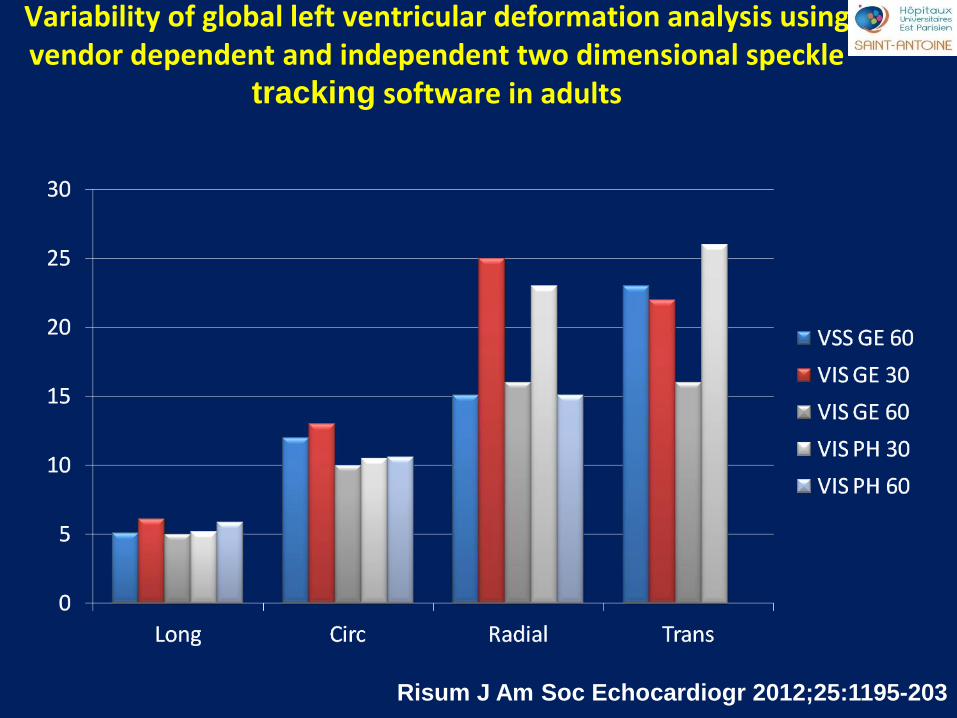
Variability of global left ventricular deformation analysis using vendor dependent and independent two dimensional speckle
tracking software in adults
Risum J Am Soc Echocardiogr 2012;25:1195-203
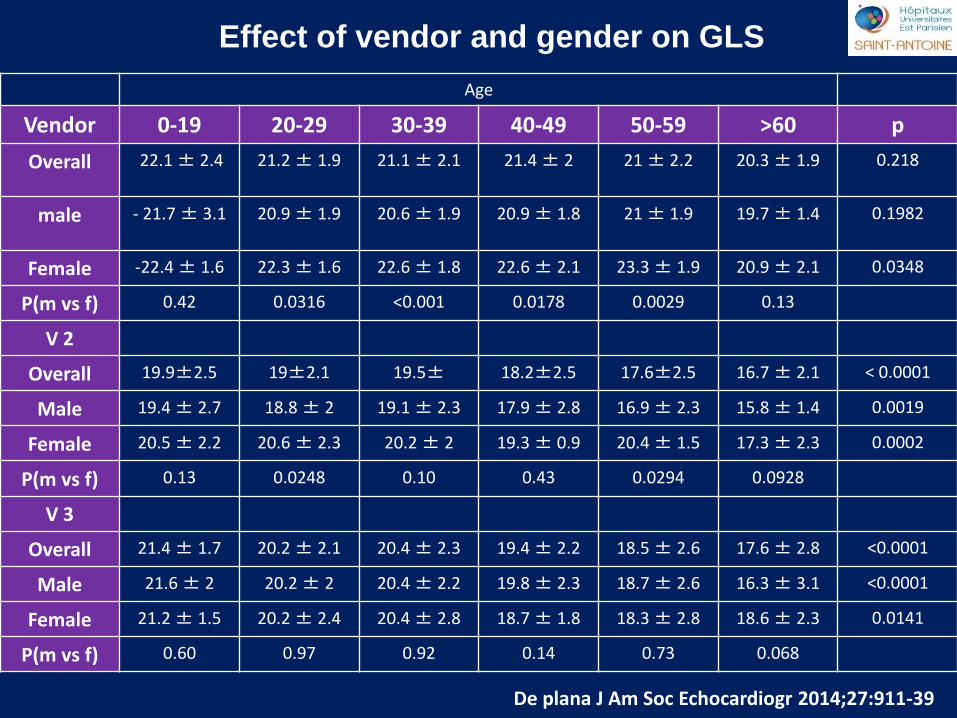
saint antoine Effect of vendor and gender on GLS
De plana J Am Soc Echocardiogr 2014;27:911-39
Age
Vendor 0-19 20-29 30-39 40-49 50-59 >60 p
Overall 22.1 ± 2.4 21.2 ± 1.9 21.1 ± 2.1 21.4 ± 2 21 ± 2.2 20.3 ± 1.9 0.218
male - 21.7 ± 3.1 20.9 ± 1.9 20.6 ± 1.9 20.9 ± 1.8 21 ± 1.9 19.7 ± 1.4 0.1982
Female -22.4 ± 1.6 22.3 ± 1.6 22.6 ± 1.8 22.6 ± 2.1 23.3 ± 1.9 20.9 ± 2.1 0.0348
P(m vs f) 0.42 0.0316 <0.001 0.0178 0.0029 0.13
V 2
Overall 19.9±2.5 19±2.1 19.5± 18.2±2.5 17.6±2.5 16.7 ± 2.1 < 0.0001
Male 19.4 ± 2.7 18.8 ± 2 19.1 ± 2.3 17.9 ± 2.8 16.9 ± 2.3 15.8 ± 1.4 0.0019
Female 20.5 ± 2.2 20.6 ± 2.3 20.2 ± 2 19.3 ± 0.9 20.4 ± 1.5 17.3 ± 2.3 0.0002
P(m vs f) 0.13 0.0248 0.10 0.43 0.0294 0.0928
V 3
Overall 21.4 ± 1.7 20.2 ± 2.1 20.4 ± 2.3 19.4 ± 2.2 18.5 ± 2.6 17.6 ± 2.8 <0.0001
Male 21.6 ± 2 20.2 ± 2 20.4 ± 2.2 19.8 ± 2.3 18.7 ± 2.6 16.3 ± 3.1 <0.0001
Female 21.2 ± 1.5 20.2 ± 2.4 20.4 ± 2.8 18.7 ± 1.8 18.3 ± 2.8 18.6 ± 2.3 0.0141
P(m vs f) 0.60 0.97 0.92 0.14 0.73 0.068
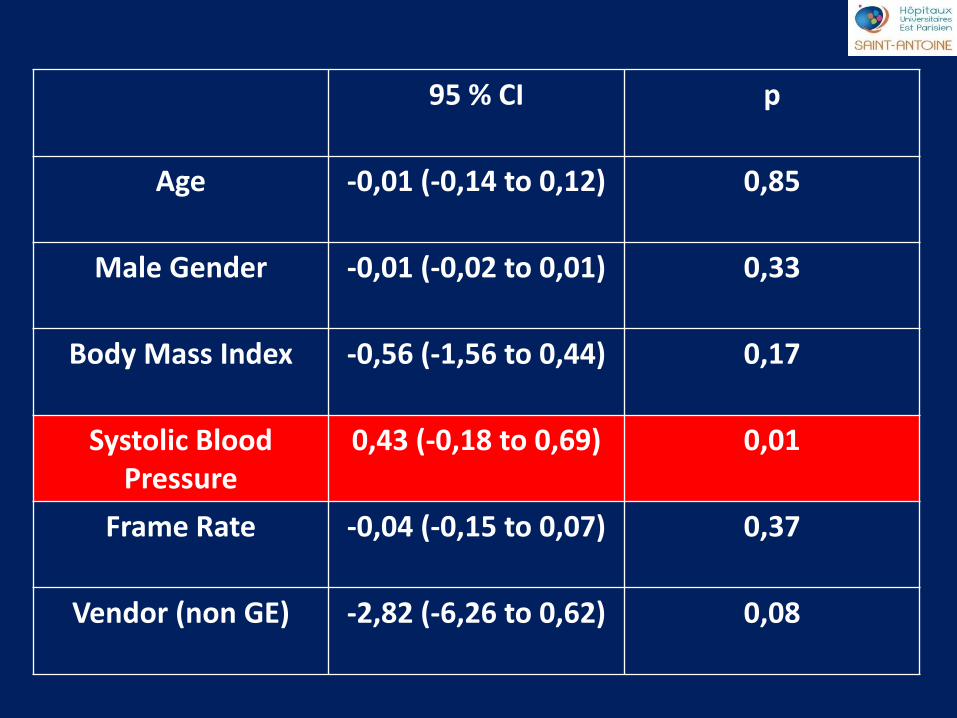
saint antoine
95 % CI p
Age -0,01 (-0,14 to 0,12) 0,85
Male Gender -0,01 (-0,02 to 0,01) 0,33
Body Mass Index -0,56 (-1,56 to 0,44) 0,17
Systolic Blood Pressure
0,43 (-0,18 to 0,69) 0,01
Frame Rate -0,04 (-0,15 to 0,07) 0,37
Vendor (non GE) -2,82 (-6,26 to 0,62) 0,08
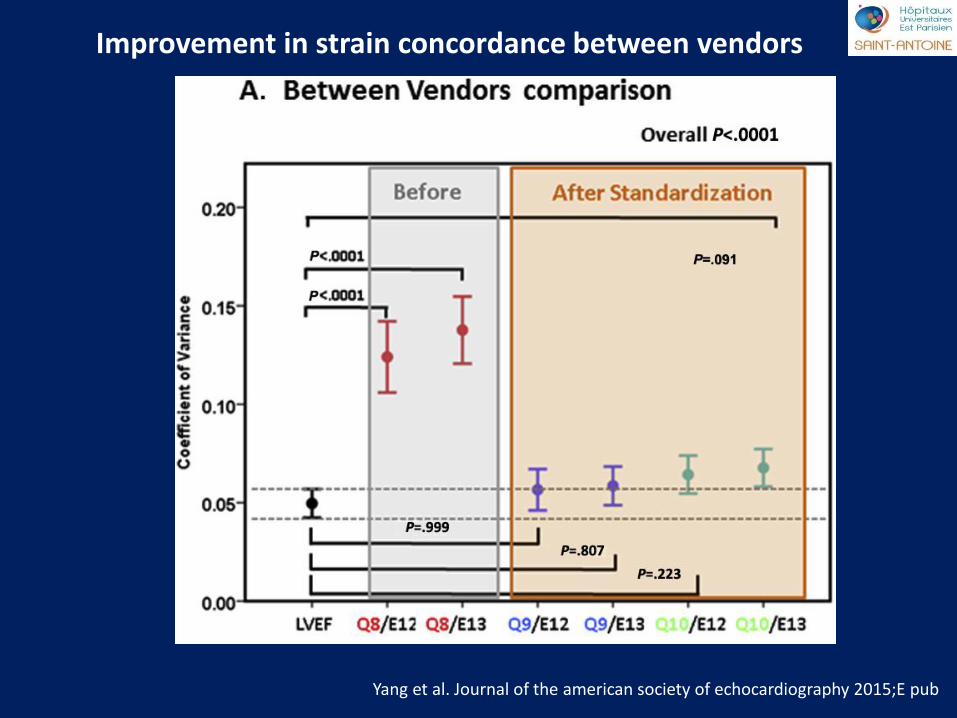
saint antoine
Yang et al. Journal of the american society of echocardiography 2015;E pub
Improvement in strain concordance between vendors
saint antoine
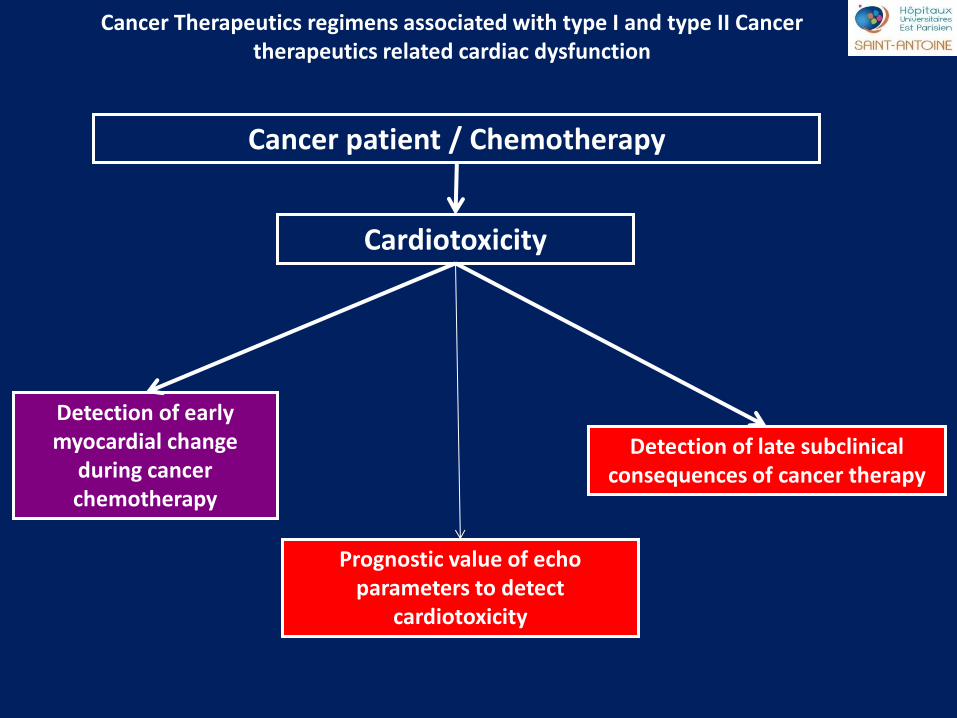
Cancer Therapeutics regimens associated with type I and type II Cancer therapeutics related cardiac dysfunction
Cancer patient / Chemotherapy
Cardiotoxicity
Detection of early myocardial change
during cancer chemotherapy
Detection of late subclinical consequences of cancer therapy
Prognostic value of echo parameters to detect
cardiotoxicity
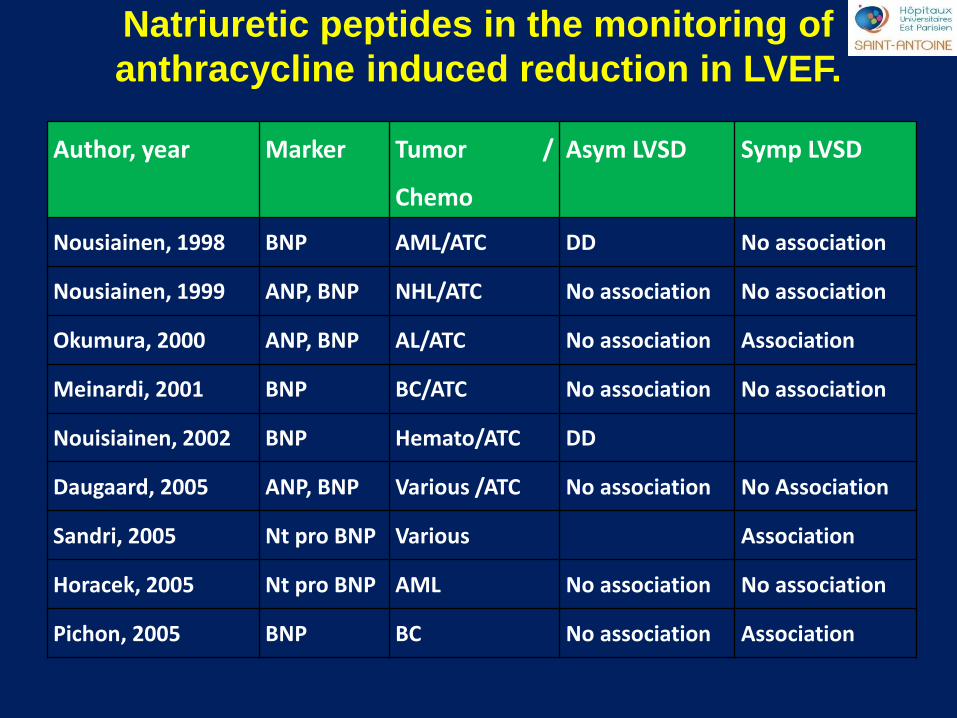
saint antoine
Author, year Marker Tumor /
Chemo
Asym LVSD Symp LVSD
Nousiainen, 1998 BNP AML/ATC DD No association
Nousiainen, 1999 ANP, BNP NHL/ATC No association No association
Okumura, 2000 ANP, BNP AL/ATC No association Association
Meinardi, 2001 BNP BC/ATC No association No association
Nouisiainen, 2002 BNP Hemato/ATC DD
Daugaard, 2005 ANP, BNP Various /ATC No association No Association
Sandri, 2005 Nt pro BNP Various Association
Horacek, 2005 Nt pro BNP AML No association No association
Pichon, 2005 BNP BC No association Association
Natriuretic peptides in the monitoring of
anthracycline induced reduction in LVEF.
saint antoine
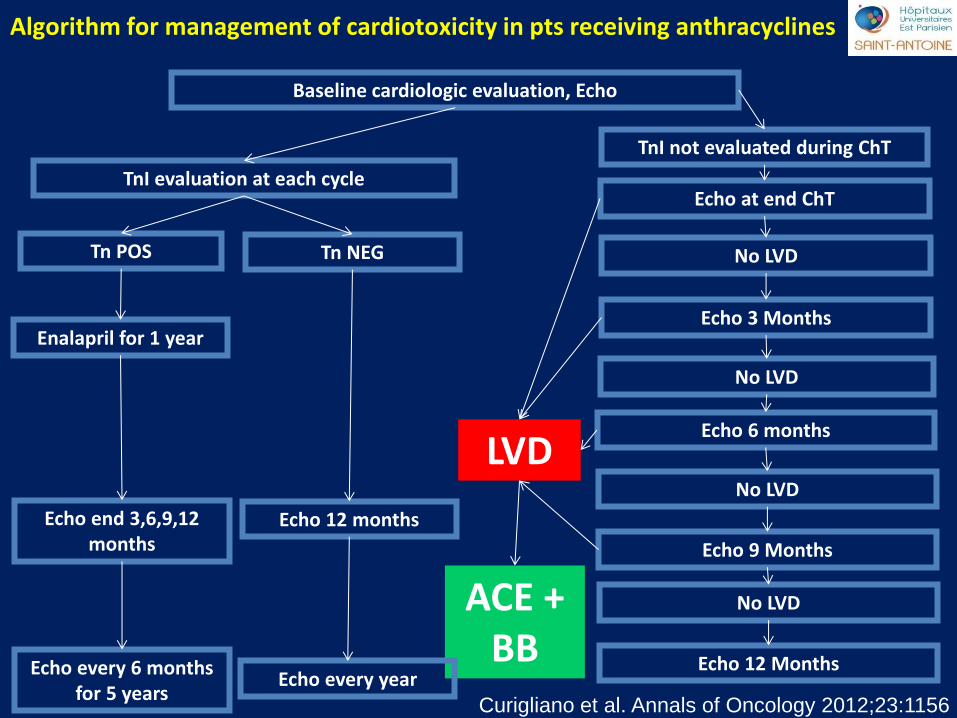
Algorithm for management of cardiotoxicity in pts receiving anthracyclines
Curigliano et al. Annals of Oncology 2012;23:1156
Baseline cardiologic evaluation, Echo
TnI evaluation at each cycle
TnI not evaluated during ChT
No LVD
Echo 3 Months
Echo at end ChT
No LVD
No LVD
Echo 9 Months
Echo 6 months
LVD
ACE + BB
No LVD
Echo 12 Months
Tn NEG Tn POS
Enalapril for 1 year
Echo end 3,6,9,12 months
Echo every 6 months for 5 years
Echo 12 months
Echo every year
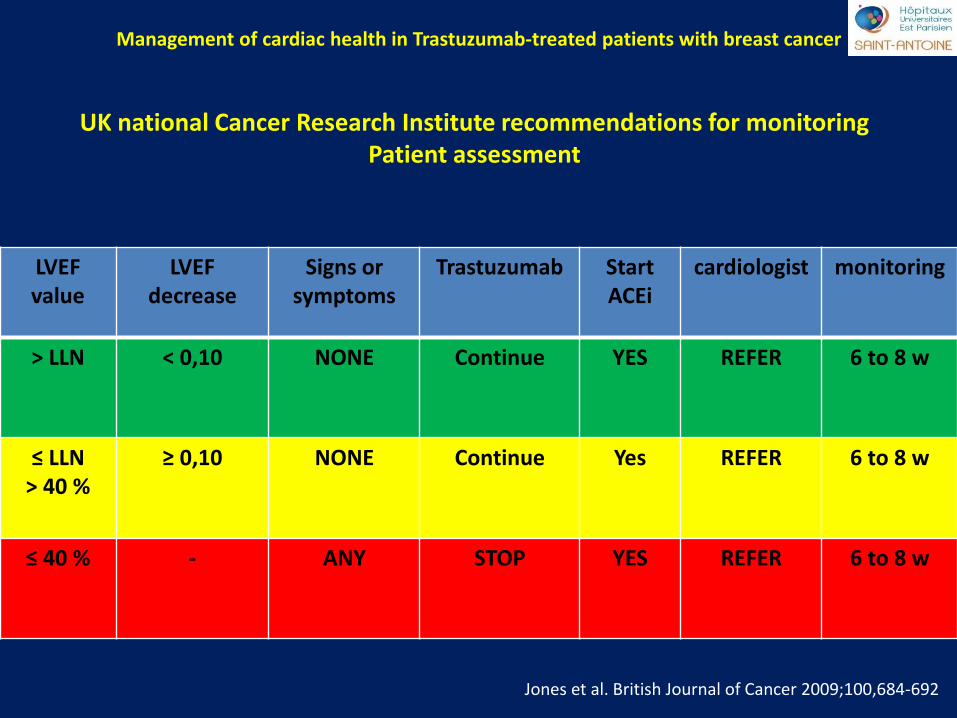
saint antoine Management of cardiac health in Trastuzumab-treated patients with breast cancer
UK national Cancer Research Institute recommendations for monitoring Patient assessment
Jones et al. British Journal of Cancer 2009;100,684-692
LVEF value
LVEF decrease
Signs or symptoms
Trastuzumab Start ACEi
cardiologist monitoring
> LLN < 0,10 NONE Continue YES REFER 6 to 8 w
≤ LLN > 40 %
≥ 0,10 NONE Continue Yes REFER 6 to 8 w
≤ 40 % - ANY STOP YES REFER 6 to 8 w